BREAKING: Pfizer and its development partner BioNTech announced Wednesday that the Canadian government granted emergency approval for their vaccine, joining a short list of a countries that can now administer shots.
The day after the U.K.'s mass vaccination campaign began, Britain’s medical regulatory agency warned that “any person with a history of significant allergic reaction to a vaccine, medicine or food” should not receive the new Pfizer-BioNTech vaccine. The announcement came after two health-care workers reacted adversely to the shot.
In the United States, the Food and Drug Administration is moving ahead with its process to determine whether to approve the same Pfizer-BioNTech vaccine candidate for emergency use, after a review confirmed that it meets the standard for such authorization.
by ponchi101 That is exactly what Suliso posted a few days ago: if you vaccinate 10,000 people in one day, somebody will wake up the next day WITH SOMETHING. A tooth ache, vomiting, colics, a bad case of the blues.
I mean, when I got my flu shot they gave me a little pamphlet of the side effects. Some people simply will go through something.
Bad statistical understanding...
by ti-amieCDC director allegedly ordered deletion of email seeking to interfere with coronavirus guidance, House panel chair says
Robert Redfield is director of the Centers for Disease Control and Prevention. (Al Drago/Bloomberg)
By
Lenny Bernstein and
Lena H. Sun
Dec. 10, 2020 at 4:00 p.m. EST
The director of the Centers for Disease Control and Prevention allegedly ordered the destruction of an email written by a top Trump administration health official who was seeking changes in a scientific report on the coronavirus’s risk to children, the head of a congressional oversight subcommittee charged Thursday.
In a letter to CDC Director Robert R. Redfield and his superior, Health and Human Services Secretary Alex Azar, Rep. James E. Clyburn (D-S.C.) expressed “my serious concern about what may be deliberate efforts by the Trump Administration to conceal and destroy evidence that senior political appointees interfered with career officials’ response to the coronavirus crisis at the Centers for Disease Control and Prevention.”
The report was not altered or withdrawn. But Clyburn, chairman of the House Select Subcommittee on the Coronavirus Crisis, cited an interview three days ago with the editor of the CDC’s most authoritative publication, the Morbidity and Mortality Weekly Report, known as MMWR. Charlotte Kent, editor in chief of that report, told investigators that while on vacation in August, she received instructions to delete the email written by Paul Alexander, a senior adviser to Azar.
When Kent went to locate the email, it had already been deleted, she said, according to a transcript of the interview provided by Clyburn. When she inquired about who had ordered its deletion, she was told the instructions had come down from Redfield through the chain of command.
“I heard from [REDACTED], who, as I understood, heard from Dr. [Michael F.] Iademarco, who heard from Dr. Redfield to delete it,” Kent told the investigators, according to the transcript. Iademarco is director of the Center for Surveillance, Epidemiology and Laboratory Services at the CDC.
In a statement released Thursday afternoon through HHS, Redfield said, “Regarding the email in question, I instructed CDC staff to ignore Dr. Alexander’s comments. As I testified before Congress, I am fully committed to maintaining the independence of the MMWR, and I stand by that statement.”
The subcommittee’s ranking member, Rep. Steve Scalise (R-La.), issued a statement disputing Clyburn’s charges. Scalise said the letter “drastically mischaracterizes Dr. Kent’s interview,” and maintained that Democrats on the panel “continue to search for illusory evidence” of obstruction by Trump administration officials.
Clyburn’s letter also asserted that HHS has blocked other top CDC officials from testifying to the committee this week and delayed sending requested documents for many months.
Clyburn also charged that an edition of the MMWR on a coronavirus outbreak at a Georgia summer camp was held up for two days to allow Redfield to testify to Clyburn’s committee on July 31.
An HHS spokesperson said the “subcommittee’s characterization of the conversation with Dr. Kent is irresponsible. We urge the subcommittee to release the transcript in full, which will show that during her testimony Dr. Kent repeatedly said there was no political interference in the MMWR process.
“Moreover, during the interview referenced in the letter, a staff member on the subcommittee chose to violate basic common practices of attorney-client privilege that protect the interests of the department, but more importantly the witness. Despite HHS working diligently to accommodate the select subcommittee’s many requests, the subcommittee is not operating in good faith.”
Efforts by Alexander and his supervisor at HHS, Michael Caputo, to change, delay and block CDC advice to the public on the pandemic were reported this summer, during a period of intense battles between the Trump administration, which was seeking to reopen the country, and the career scientists at the CDC.
In the end, language in the MMWR was not altered, nor was the report taken down, according to a former CDC official with specific knowledge of the event, who spoke on the condition of anonymity to share internal deliberations at the time.
“That did not happen,” the former official said. Political appointees at HHS and the White House pressured CDC to change guidance and press releases, but “the MMWR is where the line was drawn.”
Alexander, in particular, was adamant that CDC scientists were reporting information to harm the administration’s efforts. According to Clyburn, the Aug. 8 email that Redfield allegedly sought to delete read, in part: “CDC tried to report as if once kids get together, there will be spread and this will impact school reopening. . . . Very misleading by CDC and shame on them. Their aim is clear. . . . This is designed to hurt this Presidnet [sic] for their reasons which I am not interested in.”
Alexander has left HHS, and Caputo is on medical leave.
The committee said it is seeking to interview Redfield by Dec. 17 and still wants to speak with the four other CDC officials: Anne Schuchat, principal deputy director; Nina Witkofsky, acting chief of staff; Trey Moeller, acting deputy chief of staff; and Kate Galatas, acting associate director for communications.
by ti-amie In other words, as the late Bob Marley sad "I shot the sheriff but I didn't shoot no deputy."
by ti-amieFrench President Macron tests positive for the coronavirus after showing symptoms
By
James McAuley and
Michael Birnbaum
Dec. 17, 2020 at 11:34 a.m. EST
PARIS — French President Emmanuel Macron tested positive for the coronavirus after beginning to show symptoms, the country's presidential palace announced Thursday.
The 42-year-old president will isolate for seven days but will continue his work, the statement declared. A spokeswoman for the palace told Reuters that all of the president’s upcoming trips — including a visit to Lebanon that was scheduled for next week — have been canceled.
Macron is the latest world leader to test positive for the virus, following President Trump, Britain’s Boris Johnson and Brazil’s Jair Bolsonaro — all of whom have recovered. In contrast with those leaders, who at least initially downplayed the threat of the virus, Macron was one of the first heads of state in the West to embrace mask-wearing, and in the spring he presided over one of the tightest lockdowns in Europe. Macron’s age also puts him in a lower risk category.
The Élysée did not provide details on his condition. A spokesperson said he would still preside over a Thursday meeting on development via videoconference from isolation.
Macron’s diagnosis put other European leaders on alert, since he interacted in the past week with multiple heads of state or government. Spanish Prime Minister Pedro Sánchez is now self-quarantining after dining Monday with Macron at the Élysée Palace in Paris, though El Pais newspaper reported Thursday he had tested negative. French Prime Minister Jean Castex, who has also been in contact with Macron, said he would also be self-quarantining, Agence France-Presse reported.
Macron also met in person with the leaders of 24 E.U. countries on Thursday and Friday last week at a summit in Brussels. (Two leaders were absent: Croatia’s was sick with the coronavirus, and Estonia’s was quarantining.) Ahead of the summit, some diplomats were concerned about the health risks of an in-person meeting. An E.U. spokesman didn’t immediately respond to a question about whether the leaders who were present would now quarantine.
French authorities have informed the European Union that they believe Macron was a contagion risk starting Monday evening, meaning that the leaders who attended last week’s summit are not considered contacts, an E.U. official said, speaking on the condition of anonymity to candidly discuss the health situation.
The official said sanitary measures were taken at the summit and that no other participant has tested positive. It was not immediately clear why France believed Macron was contagious starting Monday evening.
In any case, not all European leaders appeared to trust the Élysée’s assurances that Macron was not contagious last week. Belgian Prime Minister Alexander de Croo said he was being tested for the virus and would quarantine until he receives the result, after sitting in a room with Macron — along with most of the rest of Europe’s leaders — for almost 24 hours straight starting the afternoon of Dec. 10.
This week, in addition to Sánchez, Macron also met with European Council President Charles Michel on Monday and with Portuguese Prime Minister António Costa on Tuesday.
On Wednesday, the day before his diagnosis, Macron held a cabinet meeting, although it was not immediately clear whether it took place in person and, if so, whether all participants wore masks. The Élysée Palace did not immediately respond to questions about that meeting.
Michel will quarantine “as a matter of precaution,” his spokesman said, although he tested negative on Tuesday and “is not considered to be a close contact,” his spokesman, Barend Leyts, wrote on Twitter.
French first lady Brigitte Macron is likewise self-quarantining but currently has no symptoms, according to a statement from her office to AFP. She tested negative for the coronavirus as recently as Tuesday, her office said, in advance to a visit to a pediatric ward at a Paris hospital.
Macron’s diagnosis comes as France is still contending with a second wave of the virus.
In late October, a surge of infections prompted him to declare another national lockdown, the country’s second since the pandemic began. Nonessential shops began reopening late last month, bars and restaurants must stay closed into January, and the French government lifted France’s lockdown on Tuesday, although it imposed an 8 p.m. to 6 a.m. curfew.
While the number of new infections showed some improvement after the nearly month-long lockdown, hospitals appear to be more saturated than they were during a first wave in the spring. The government had hoped that the daily case load would be lower than 5,000 by the time it lifted the second lockdown, but on Wednesday the French Health Ministry reported 17,615 new cases in the previous 24 hours along with 264 new deaths. As of Wednesday, hospitals admitted 8,979 new patients, 1,205 of whom were admitted to intensive care units, according to the Health Ministry.
Vaccination in France is set to begin in late December or early January for high risk groups and health-care workers before expanding to the broader population between April and June. It will not be mandatory, Macron has said.
Macron’s diagnosis raised immediate questions about the handling of Brexit negotiations, which need to be concluded within days if there is any chance of Britain and the European Union ratifying a trade deal by Dec. 31, the day London will sever its final ties with the bloc. Leaders had previously floated the possibility of an additional in-person summit in the next two weeks to finalize a deal.
European policymakers have complained that negotiations about thorny issues are nearly impossible when they are conducted virtually, as has mostly been the case since March.
Macron has been one of the most stubborn European leaders during Brexit talks, and his sign-off is crucial to any Brexit deal.
Birnbaum reported from Brussels. Rick Noack in Berlin and Teo Armus in Washington contributed to this report.
by ti-amieWhite House Official Recovers From Severe Covid-19, Friend Says
By Jennifer Jacobs
December 14, 2020, 1:53 PM EST Updated on December 14, 2020, 4:30 PM EST
Crede Bailey spent three months in hospital with disease
Friend created GoFundMe account with details of illness
A White House official who fell ill with Covid-19 in September is recovering after three months in the hospital, though he lost his right foot and lower leg in his battle against the virus, according to a friend.
Crede Bailey, the director of the White House security office, was the most severely ill among dozens of Covid-19 cases known to be connected to the White House. Bailey’s family has asked the White House not to publicize his condition, and President Donald Trump has never publicly acknowledged his illness.
Bailey’s friends have raised more than $30,000 for his rehabilitation through a GoFundMe account. The White House declined to say whether Trump has contributed to the effort.
“Crede beat COVID-19 but it came at a significant cost: his big toe on his left foot as well as his right foot and lower leg had to be amputated,” Dawn McCrobie, who organized the GoFundMe effort for Bailey, wrote Dec. 7.
Bailey is now at a rehabilitation center and will be fitted for a prosthetic leg in the coming months, she wrote.
“His family has staggering medical bills from a hospital stay of 2+ months and still counting in the ICU and a long road ahead in rehab before he can go home,” McCrobie wrote Nov. 13, when she created the account. “When he does make it home there will be major changes necessary to deal with his new, and permanent, disability.”
Two people familiar with Bailey’s situation confirmed that McCrobie is a friend. They asked not to be identified because Bailey’s family has tried to keep his illness private.
McCrobie did not respond to messages and White House spokespeople declined to comment. Efforts to reach Bailey and multiple members of his family by phone, e-mail and social media have been unsuccessful.
After this story was published, McCrobie updated the GoFundMe page to advise Bailey’s friends to ignore messages from journalists. “Per Crede’s wishes, please let the media tell their story without your input,” she wrote.
Bailey’s office handles credentialing for access to the White House complex and works closely with the U.S. Secret Service on security measures. Bailey was known on the compound as a strong Trump supporter.
The president has repeatedly minimized the risk from Covid-19 since the beginning of the pandemic, both before and after he was hospitalized with the disease Oct. 2-5.
Doctors are still learning about the extent to which the coronavirus can damage the body, but loss of blood flow is one possible consequence. The virus is known to attack the vascular system and can cause deadly blood clots.
When she created the GoFundMe account, McCrobie wrote that “Crede will NOT be happy I’ve done this as he is a proud man who is the first to help everyone else but would never ask for help himself.”
She updated the post Dec. 7 with more details about his condition. He “is blown away by your generosity,” she said to donors.
“His house will need to be renovated to accommodate his disability; ramps to get in/out of the house, the bathroom shower will have to be modified, handrails will have to be installed, etc. etc.,” she wrote.
He’ll also need a new vehicle that can accommodate a wheelchair and that can be modified so the gas pedal can be operated with Bailey’s left leg, she wrote. “I could go on and on but you get the picture - there are a lot of adjustments ahead!”
(Updated with McCrobie post on GoFundMe in ninth paragraph.)
by Suliso I'm afraid situation is dire almost everywhere in Europe and Americas. Vaccines is the only solution at this stage, but their impact will take at least 2 more months to register. EU and Switzerland expected to start their campaigns from December 27th.
by ti-amie James Williams
@edujdw
Is this correct? We can gift £BILLIONS for a failing test and trace programme to a private company run by friens and Conservative supporters, but for testing in schools it has to be done by volunteers and already overworked teachers? Seriously?
by ti-amie
Kurt "Masks Save Lives" Eichenwald
@kurteichenwald
Now we know why the administration is cutting distrituon of the vaccine to states: Just like the Biden transition team leaked, they had no distribution plans. Pfizer explains in next tweet....
Suliso wrote: ↑Thu Dec 17, 2020 7:59 pm
I'm afraid situation is dire almost everywhere in Europe and Americas. Vaccines is the only solution at this stage, but their impact will take at least 2 more months to register. EU and Switzerland expected to start their campaigns from December 27th.
Indeed. The closing down here in Colombia is all but gone. Traffic up to the same volumes, people in the street just getting ready for Xmas.
Many places are installing hand-washing stations at their entrance. Sponsored by soap companies. Not a bad idea.
Colombia is expecting 10 MM doses starting Feb-Mar (Pfizer/BioNtech). As you say, the only way out. But that would cover only 10% of the population (around 50 million). I gather we will need the other companies to join the game soon.
by ti-amieInterior shuts Washington Monument after interior secretary tests positive for the coronavirus
Park Service staff say they may have been exposed when David Bernhardt led a private, after-hours tour
By
Juliet Eilperin,
Lisa Rein and
Darryl Fears
Dec. 18, 2020 at 12:18 p.m. EST
Add to list
Officials have taken the extraordinary step of closing the Washington Monument starting Friday as a precaution after Interior Secretary David Bernhardt — who had been giving private, nighttime tours to associates — tested positive for the coronavirus.
Interior spokesman Nicholas Goodwin confirmed the temporary closure, saying the department acted after consulting with federal health officials. Bernhardt had led other Trump DOI appointees on a tour earlier this week. Some National Park Service staff at the site said they had been exposed to the secretary during his after-hours tour and are now in quarantine, which has led to a staffing shortage at the monument, Goodwin said.
“As we do in all circumstances when an employee attests to having covid-19, we work with our public health officials to ensure all guidance from the CDC is followed, such as identifying close contacts and cleaning areas as appropriate,” Goodwin said. “The Secretary was recently at the Washington Monument. In working with our public officials and out of an abundance of caution, a couple of employees have quarantined resulting in a temporary workforce reduction at the monument and its temporary closure.”
The secretary’s diagnosis Wednesday forced the cancellation of a large Interior Department holiday party scheduled for Thursday night, and it is raising concerns about his deputy’s plans to visit two national parks next week. Deputy Secretary Katharine MacGregor, who is headed to Yellowstone and Grand Tetons National Parks starting Monday, has asked National Park Service staff to drive her between them and provide tours of Yellowstone for four days, according to several federal officials briefed on the plan who spoke on the condition of anonymity out of fear of retaliation. Depending on the route, the trip is 113 miles and should take roughly three hours by car.
MacGregor’s trip to Wyoming “will move forward as planned” because the department’s team of public health professionals had examined her recent activities and determined she “has not had close contact with Secretary Bernhardt as described by CDC guidance,” Goodwin said. He added, “the health and safety of the public and our employees is our top priority.”
“Interior has an incredible team of more than 60 public health professionals on staff that have been leading the Department’s pandemic response efforts with the Secretary and other members of leadership over the past year,” he said, adding that since the Washington Monument reopened Oct. 1, no Park Service staffer working there has tested positive for the coronavirus.
MacGregor will visit newly renovated staff housing in the park, officials said, which has been a major administration priority. Interior Assistant Secretary for Fish and Wildlife and Parks Rob Wallace, who lives in Wyoming and is working remotely, may accompany MacGregor on her park tour, officials said.
Bernhardt, who tested positive for the coronavirus before he was to attend a Cabinet meeting with President Trump on Wednesday, has been in proximity with several Interior officials in the past week. Political appointees had meetings Monday and Tuesday, according to two federal officials, which culminated with a reception with food and drink in the secretary’s office.
Several of the appointees walked through the building to the secretary’s office without wearing face coverings, according to one of the officials. Some of the highest-ranking officials at Interior — including Bernhardt and MacGregor — have not consistently worn masks, according to two individuals.
The shuttering of the Washington Monument, where visitors normally crowd into a small elevator to ascend to the top, has implications for D.C.'s tourist industry. The administration first closed it in mid-March, then reopened it in October. Under pandemic procedures, a limited number of people are allowed in the elevator at any one time, and they must be spaced six feet apart.
A notice posted on the Park Service’s website reads, “Consistent with Centers for Disease Control and Prevention guidance and in coordination with the NPS Office of Public Health, the Washington Monument is temporarily closed due to a reduction in its workforce resulting from a potential COVID-19 exposure.”
“NPS is working to staff the Washington Monument at the appropriate levels to maintain the safety of its operations for visitors and employees,” it adds.
Theresa Pierno, president and chief executive of the National Parks Conservation Association, a nonprofit group that supports the park system, said in an email that the move illustrates that “Bernhardt has been careless and reckless managing our national parks and public lands throughout this pandemic.”
“His irresponsible behavior has put countless park rangers in harm’s way, further demonstrating his failure to put the health and safety of park visitors and rangers at risk,” she added. “To use our parks as his own personal playground is shameful, and a slap in the face to the American people.”
Bernhardt is not the only interior secretary to lead private tours of the nation’s most famous park sites. His predecessor Ryan Zinke brought friends and family members on park trips across the country, touring everywhere from the basement of the Lincoln Memorial to California’s Channel Islands National Park.
With a month remaining before the Trump administration ends, MacGregor plans to visit two national parks in Wyoming. While department officials are now reassessing the activities she will do during the trip, the initial itinerary called for Park Service employees to pick her up in Bozeman, Mont., and drive her to the park, as well as provide transportation at times during her stay.
MacGregor has asked to go snowshoeing during her visit, as well as for transportation to be arranged between Yellowstone and Jackson Hole Airport. Transportation options include a snow coach or van, both of which would be enclosed, or a snowmobile, which is not.
Some employees at both Yellowstone and the Grand Tetons have expressed concerns about the possibility of coming in close contact with MacGregor during her trip, according to three officials. Bernhardt may travel to both parks early next month, these officials added, though those plans have not yet been finalized.
Coalition to Protect America’s National Parks Chair Phil Francis, whose group represents both Park Service retirees as well as current officials, noted that “while we hope the secretary will recover,” the fact that he visited staff at Great Smoky Mountains National Park in early May and “there was no sign of the secretary wearing a mask or social distancing” raises concerns.
“It’s truly unbelievable that Secretary Bernhardt and his staff would plan a trip to Yellowstone at a time when the pandemic is raging,” Francis said in an interview. “The lack of concern for others is astounding.”
MacGregor would not be the first high-ranking Interior official to visit Yellowstone under a lame-duck president. Then-Secretary Sally Jewell flew to the area just before Thanksgiving in 2016 to announce a two-year ban on new mining claims outside the park.
At the time the administration was racing to impose new restrictions on development near the park. Several proposals for gold exploration just north of Yellowstone had sparked opposition from business owners and environmentalists as a threat to tourism and outdoor recreation.
by ponchi101 Meanwhile, down here.
After a celebration called "Night of the candles" (people get together to light up candles in celebration of the Immaculate Conception), a very large surge of cases have brought daily new cases and deaths back to record numbers (nation wise).
The govt is asking people to stay away from large gatherings again. In the meantime, you can't walk down the supermarket aisles because both of the amount of products and people.
Very little analysis to do after the full year of virus.
The govt also established the vaccine protocol. Nothing major: health personnel first, risk groups second, then people over 60, then the rest of us...
by ti-amie
Rebekah Jones, MS, GISP
@GeoRebekah
Sweden has admitted that their strategy was a mistake, names schools as a major driver of spread, and closes all high schools until end of January.
Katrin Rabiei, MD PhD @DrKatrin_Rabiei
Press conference in Sweden by the Flag of Sweden government including @SwedishPM & head of the public health agency.
I will summarize what they said here Thread:
Spreading is going too fast in Sweden. We need harder restrictions
Government wants to thank those who have taken measures to minimize the spread (!).
Non essential business (pools, museums) to close until 24th of January
Vaccine is a new & sought after tool against #COVID19
Deputy PM takes over:
All non essential workers must work from home until 24th of January
From 24th of December:
only 4 persons can gather at a restaurant
No alcohol sale from 20.00
Maximum number of people at shopping centers, shops & gyms.
Use of Face with medical mask during certain hours in public transport
High schools closed until 24th of JanuaryEveryone who can work at home must work from home!
by ponchi101 Well. As an experiment, it was worth it. Now we really know that expecting for herd-immunity WAS not the way to go.
Would like to see a serious person from Brazil coming forth with their findings.
by ti-amieChristmas plans in chaos as Boris Johnson tells London and southeast to ‘stay home’
PM announces toughest measures yet for England as new virus strain causes surge in cases
Caroline Wheeler, Gabriel Pogrund | The Sunday Times
Christmas holiday plans for millions of families in southeast England will be plunged into chaos tonight as new restrictions are introduced to contain a new strain of the coronavirus.
Boris Johnson has unveiled tier 4 restrictions for London, the southeast and east of England, which will prevent households from mixing over Christmas.
The restrictions come into force at midnight, with all non-essential shops, including hairdressers, and indoor leisure centres and cinemas closed with immediate effect.
The prime minister told the 5.3 million people living under the toughest measures to stay at home. The only exceptions are for support bubbles, childcare and separated parents. Individuals will be able to socialise with one other person from another household in a public outdoor space.
In other areas in England, the lifting of restrictions to allow up to three households to mix will be limited to Christmas Day only. People will also be advised to “stay local”.
Mr Johnson cautioned people against visiting tier 4 areas and banned overnight stays.
He had previously said it would be “inhumane” to scrap plans to relax restrictions between December 23 and 27, but told a televised press conference today: “I know how disappointing this will be ... when the science changes, we must change our response. When the virus changes its method of attack, we must attack our method of defence. And as your prime minister, I sincerely believe there is no alternative open to me.”
The move is an attempt to reduce transmission after the government alerted the World Health Organisation to a new mutant strain that is up to 70% more infectious.
Officials have estimated the strain accounts for 60% of new infections in London, where intensive care units are operating at full capacity and all non-essential outpatient appointments are set to be cancelled.
No 10 has said it expects other countries to ban Britons, mirroring the action taken after the identification of a mutant strain linked to mink in Denmark. Those in tier 4 will be banned from holidaying abroad.
The change in policy came after ministers and scientific advisers met last night to discuss the current outbreak, which has seen daily deaths reach 534. More than 170,000 people have tested positive for the virus over the past week. The cabinet met to ratify the decision this afternoon.
Chris Whitty, the chief medical officer, said there was no evidence that the new strain of the virus, known as VUI2020/12/01, caused a higher mortality rate or was impervious to the vaccine.
However, he said the new and emerging respiratory virus threats advisory group, which advises ministers, considered it was more infectious.
The tier 4 restrictions will apply in all tier 3 areas in the southeast, covering Kent, Buckinghamshire, Berkshire, Surrey (excluding Waverley), Gosport, Havant, Portsmouth, Rother and Hastings.
It will also apply in London (all 32 boroughs and the City of London) and the east of England (Bedford, Central Bedford, Milton Keynes, Luton, Peterborough, Hertfordshire and Essex (excluding Colchester, Uttlesford and Tendring).
by ti-amieHow worried should we be about the new coronavirus mutation?
Scientists scramble to work out how it responds to vaccine
Andrew Gregory
, Health Editor
Saturday December 19 2020, 12.00pm GMT, The Sunday Times
Millions more people in England are entering the toughest coronavirus restrictions this weekend amid fears a new variant is accelerating the spread of the disease.
Boris Johnson held an unscheduled meeting of ministers on Friday night amid mounting concern about the threat posed by the mutant strain.
Scientists familiar with the new variant say it is spreading fastest in southeast England.
What is the new variant and why does it pose a threat?
It has been named VUI — 202012/01 — the first variant under investigation in December.
Public Health England (PHE) said that, as of December 13, 1,108 cases with this new variant had been identified, predominantly in southeast England, although that figure is understood to have risen since then.
PHE believes this new variant includes a mutation in the spike protein and that changes in this part of the spike protein may result in the virus becoming more infectious and spreading more easily between people.
What makes this new variant potentially so significant?
Professor Sir Mark Walport — a member of the Government’s Scientific Advisory Group for Emergencies (Sage) — said there was a real possibility that it could have a “transmission advantage”.
“What happens with viruses is they do naturally mutate all the time and the ones that are likely to do well are the ones that increase transmission,” he said. “We know that this is a new variant, it has been seen in other countries but it seems to be quite widespread which suggests that it has got a transmission advantage.”
There have been many mutations in the virus since it emerged in 2019.
This is to be expected — SARS-CoV-2 is an RNA virus and these viruses mutate and change. But this variant has sparked particular concern because it appears to be speeding up the spread of the virus.
“Scientists are working extremely hard to work out what is going on,” said Walport. “But it does definitely seem possible that this transmits more easily. It will make the social-distancing even more critical.”
Do we know for definite that the new variant is accelerating the spread of the virus?
No. Ewan Birney, deputy director general of European Molecular Biology Laboratory, said the new variant had been growing “very strongly in the south of England” but it was not possible to say definitively that it was transmitting faster than others or whether it was because the number of cases in general was growing.
However, he added that most scientists “think it is going faster — that it really is a property of the virus”.
How worried should we be?
Not enough is yet known about the new strain, but it is premature to make any claims about the potential impacts of virus mutation. However, if the virus spreads faster it will be much harder to control.
This one could potentially be serious, but not enough is known, and the surveillance and research is continuing this weekend.
The Covid-19 Genomics UK (COG-UK) consortium said it is difficult to predict whether any given mutation is important when it first emerges and that it would take “considerable time and effort to test the effect of many thousands of combinations of mutations”.
It said the biggest concern is any changes that lead to an increase in reinfections or vaccine failure and that most attention is on mutations in the gene that encodes the spike protein.
There are currently around 4,000 mutations in the spike protein gene.
Is it the first novel strain detected in the UK?
No. A number of variants have been detected using sequencing studies in the UK.
A specific variant (the D614G variant) has previously been detected in western Europe and North America which is believed to spread more easily but not cause greater illness.
But it is thought this is the first strain that will be investigated in such detail by PHE.
What examples are there of other virus strains?
The Danish government culled millions of mink after it emerged that hundreds of Covid-19 cases in the country were associated with SARS-CoV-2 variants associated with farmed minks — including 12 cases with a unique variant, reported on November 5.
In October a study suggested that a coronavirus variant that originated in Spanish farm workers spread rapidly throughout Europe and accounted for most UK cases.
The variant, called 20A.EU1, is known to have spread from farm workers to local populations in Spain in June and July, with people then returning from holiday in Spain most likely playing a key role in spreading the strain across Europe.
Are new variants always a bad thing?
Not necessarily. They could even be less virulent — which could be a positive thing.
There have already been various strains of Covid-19 with no real consequence.
However, if they spread more easily but cause the same disease severity, more people will end up becoming ill in a shorter period of time.
Will the virus become more harmful?
Probably not. Only changes that make viruses better for transmission are likely to be stable and result in new circulating strains. The pressure on the virus to evolve is increased by the fact that so many millions of people have now been infected.
Most of the mutations will not be significant or give cause for concern, but some may give the virus an evolutionary advantage which may lead to higher transmission or mean it is more harmful.
So what are the scientists doing now?
Scientists are scrambling to grow the new strain in labs to see how it responds.
This includes looking at whether it produces the same antibody response, how it reacts to the vaccine, and modelling the new strain.
It could take up to two weeks for this thorough process to be complete.
COG-UK is also carrying out random sequencing of positive samples across the UK to compile a sequencing coverage report, which is sent to each of the four public health agencies each week.
It said random sampling is important to capture regional coverage.
Will vaccines still work?
That is the big question. Matt Hancock, the health secretary, said the latest clinical advice is that it is highly unlikely that this new variant would fail to respond to a vaccine.
The vaccine produces antibodies against many regions in the spike protein, and it is unlikely a single change would make the vaccine less effective.
However, this could happen over time as more mutations occur, as is the case every year with flu.
Apart from any potential impact on vaccines, why else does a new variant that could be speeding up the spread of the virus matter?
The key point here is that if the variant does accelerate how quickly the virus is spreading, that could mean more people fall ill in a shorter period over the next few weeks.
That is worrying because hospitals are already filling up fast with Covid-19 patients.
The total number of Covid-19 patients in hospital in England stood at 15,465 on December 16, up from 13,467 a week earlier. This is higher than at any point during the second wave.
It puts the number on course to reach a new record for the pandemic in the first week of January, with the current peak of 18,974 virus patients in hospital reached in April. This would be before the NHS feels the effect of a five-day relaxation of restrictions over Christmas.
by ponchi101 Next person that even hints at doubting evolution should be executed in the spot.
by ti-amieMultiple European countries ban travel from UK over new Covid strain
WHO tells members to redouble efforts to stop spread as Israel turns away UK passport holders
Sam Jones in Madrid, Angela Giuffrida in Rome, Oliver Holmes in Jerusalem and agencies
Sun 20 Dec 2020 18.12 GMT
European countries have begun to close their doors to travellers from the UK after the discovery of a fast-spreading strain of Covid-19 in England.
As the World Health Organization called on its members in Europe to step up measures, countries including France, Germany, Ireland and the Netherlands announced bans on travel from the UK.
France said it was suspending passenger and human-handled freight transport for 48 hours from midnight, and that the time would be used to agree on a new testing regime in collaboration with its European Union partners.
Germany, which is suspending flights from midnight on Sunday, has not yet detected the new strain but is taking reports from the UK “very seriously”, its health minister Jens Spahn said.
A German government source told Agence France-Presse the restriction could be adopted by the entire 27-member EU and that countries were also discussing a joint response over sea, road and rail links with Britain.
Belgium is also suspending flight and Eurostar arrivals from Britain from midnight. The prime minister, Alexander De Croo, said the ban would initially be in place for at least 24 hours.
Italy’s foreign minister, Luigi Di Maio, said the government had decided to act after the UK raised the alarm about the new strain. “As a government we have the duty to protect Italians and for this reason, after having warned the British government, the health ministry will sign a provision for the suspension of flights with the UK,” he said. “Our priority is to protect Italy and our compatriots.”
Di Maio offered no more details, but flights arriving in Italy from the UK on Sunday are not thought to be affected. Austria is also planning to ban flights, but is still working out the details..
The Dutch ban, which came into effect from 6am local time on Sunday, will last until 1 January. Ireland will impose restrictions on flights and ferries from Britain from midnight, while Bulgaria is suspending flights from and to the UK from midnight until 31 January. Romania also said it banned all flights to and from the UK for two weeks starting on Monday afternoon.
The German chancellor Angela Merkel held a conference call with the French president, Emmanuel Macron, and the EU chiefs Ursula von der Leyen and Charles Michel about the matter.
The Spanish government said it had asked the European commission and the European council to come up with a “joint, coordinated response” to the situation, but that it would “act in defence of the interests and rights of Spanish citizens” if one was not forthcoming. The European commission has not said whether a prohibition on travellers from the UK would be recommended for all EU countries.
The WHO said it was in close contact with British officials, and that outside the UK nine cases of the new strain had been reported in Denmark, one in the Netherlands and one in Australia. “Across Europe, where transmission is intense and widespread, countries need to redouble their control and prevention approaches,” a spokeswoman for WHO Europe said.
Were it to continue into January, the travel disruption could exacerbate transport problems caused by Brexit as Britain leaves the EU’s single market, which guarantees movement within its borders.
Israel, too, imposed new measures on Sunday, barring entry to non-citizens arriving from the UK, Denmark and South Africa, citing fears about Covid variants. Israeli citizens arriving from those countries will have to enter isolation at state-run quarantine hotels for up to 14 days.
The hastily enacted decision led to confusing scenes at Israel’s international airport, where according to domestic media about 130 passengers on two flights from London were informed of the new quarantine requirements on arrival. Police were called to the scene after several people refused, Channel 12 news reported, and 12 decided to return to the UK.
Ellen Steel, a British–Israeli citizen on one of the flights, said she was ordered to board a crowded bus without being told where she was going. “At Luton, check-in was normal, but then they called boarding 1.5 hours early. At the gate, they turned everyone away [all non-Israelis] who had a British passport,” she told the Times of Israel.
“When we landed someone from the health ministry came on [the plane] and announced we’d all have to go to hotels. If we wanted to have a fight about it we could but only at the hotel and not before,” she said. Police escorted the buses, she added.
The UK government announced emergency restrictions after Public Health England said it had identified more than 1,100 cases of a new variant of coronavirus that may be speeding up the spread of the virus, particularly in south-east England.
AFP and the Associated Press contributed to this report
By
Yasmeen Abutaleb,
Ashley Parker,
Josh Dawsey and
Philip Rucker
Dec. 19, 2020
As the number of coronavirus cases ticked upward in mid-November — worse than the frightening days of spring and ahead of an expected surge after families congregated for Thanksgiving — four doctors on President Trump’s task force decided to stage an intervention.
After their warnings had gone largely unheeded for months in the dormant West Wing, Deborah Birx, Anthony S. Fauci, Stephen Hahn and Robert Redfield together sounded new alarms, cautioning of a dark winter to come without dramatic action to slow community spread.
White House Chief of Staff Mark Meadows, among the many Trump aides who were infected with the virus this fall, was taken aback, according to three senior administration officials with knowledge of the discussions. He told the doctors he did not believe their troubling data assessment. And he accused them of outlining problems without prescribing solutions.
The doctors explained that the solutions were simple and had long been clear — among them, to leverage the power of the presidential bully pulpit to persuade all Americans to wear masks, especially the legions of Trump supporters refusing to do so, and to dramatically expand testing.
“It was something that we were almost repetitively saying whenever we would get into the Situation Room,” said Fauci, who directs the National Institute of Allergy and Infectious Diseases. “Whenever we got the opportunity to say, ‘This is really going to be a problem because the baseline of infections was really quite high to begin with, so you had a lot of community spread.’ ”
On Nov. 19, hours after the Centers for Disease Control and Prevention advised against Thanksgiving travel, Vice President Pence, who chairs the coronavirus task force, agreed to hold a full news conference with some of the doctors — something they had not done since the summer. But much to the doctors’ dismay, Pence did not forcefully implore people to wear masks, nor did the administration take meaningful action on testing.
As for the president, he did not appear at all.
Trump went days without mentioning the pandemic other than to celebrate progress on vaccines. The president by then had abdicated his responsibility to manage the public health crisis and instead used his megaphone almost exclusively to spread misinformation in a failed attempt to overturn the results of the election he lost to President-elect Joe Biden.
“I think he’s just done with covid,” said one of Trump’s closest advisers who, like many others interviewed for this story, spoke on the condition of anonymity to candidly discuss internal deliberations and operations. “I think he put it on a timetable and he’s done with covid. . . . It just exceeded the amount of time he gave it.”
Now, a month later, the number of coronavirus cases in the United States is reaching records daily. The nation’s death count is rising steadily as well, this past week surpassing 300,000 — a total that had seemed unfathomable earlier this year. The dark winter is here, hospitalizations risk breaching capacities, and health professionals predict it will get worse before it gets better.
The miraculous arrival of a coronavirus vaccine this past week marks the first glimmer of hope amid a pandemic that for 10 months has ravaged the country, decimated its economy and fundamentally altered social interactions.
Yet that triumph of scientific ingenuity and bureaucratic efficiency does not conceal the difficult truth, that the virus has caused proportionately more infections and deaths in the United States than in most other developed nations — a result, experts say, of a dysfunctional federal response led by a president perpetually in denial.
“We were always going to have spread in the fall and the winter, but it didn’t have to be nearly this bad,” said Scott Gottlieb, a former FDA commissioner in the Trump administration. “We could have done better galvanizing collective action, getting more adherence to masks. The idea that we had this national debate on the question of whether masks infringed on your liberty was deeply unfortunate. It put us in a bad position.”
Maryland Gov. Larry Hogan, one of the few Republican elected officials who have criticized Trump’s handling of the pandemic, said many in the administration are working hard to control the alarming November-to-December surge, but not the man at the top.
“My concern was, in the worst part of the battle, the general was missing in action,” Hogan said of the recent surge.
The story of how America arrived at this final season of devastation, with the reported death toll some days surpassing 3,000 people — a new 9/11 day after day — is based on interviews over the past month with 48 senior administration officials, government health professionals, outside presidential advisers and other people briefed on the inner workings of the federal response.
The catastrophe began with Trump’s initial refusal to take seriously the threat of a once-in-a-century pandemic. But, as officials detailed, it has been compounded over time by a host of damaging presidential traits — his skepticism of science, impatience with health restrictions, prioritization of personal politics over public safety, undisciplined communications, chaotic management style, indulgence of conspiracies, proclivity toward magical thinking, allowance of turf wars and flagrant disregard for the well-being of those around him.
“There isn’t a single light-switch moment where the government has screwed up and we’re going down the wrong path,” said Kyle McGowan, who resigned in August as chief of staff at the CDC under Redfield, the center’s director. “It was a series of multiple decisions that showed a lack of desire to listen to the actual scientists and also a lack of leadership in general, and that put us on this progression of where we’re at today.”
P1
by ti-amie P2
‘Words matter’
Trump’s defenders say the president and his administration deserve credit not only for Operation Warp Speed — the public-private initiative to develop, test and now distribute vaccines — but also for their work early on to address a shortage of ventilators, ease supply-chain delays for personal protective equipment and set guidelines for businesses and other gathering places to reopen after the March and April shutdowns.
They also point to Trump’s decision in late January to restrict travel from China, where the virus originated. And they say they’re not sure what Trump should have done differently.
“President Trump has led a historic, whole-of-America coronavirus response — resulting in 100,000 ventilators procured, an abundance of critical PPE sourced for our frontline heroes, the largest testing regime in the world, groundbreaking treatments, and a safe and effective vaccine in record time with another to be approved in the coming days,” White House spokeswoman Sarah Matthews said in a statement. She went on to attribute the success of vaccines to Trump’s “bold and innovative leadership.”
Still, the administration’s overall response is likely to be scrutinized for years to come as a case study in crisis mismanagement. At the heart of the problem, experts say, have been Trump’s scrambled and faulty communications.
“Words matter a lot, and what we have here is a failure to communicate — and worse than that, the effective communication of policies, of myths, of confusion about masks, about hydroxychloroquine, about vaccines, about closures, about testing,” said Tom Frieden, a former CDC director in the Obama administration. “It’s stunning.”
Trump’s repeated downplaying of the virus, coupled with his equivocations about masks, created an opening for reckless behavior that contributed to a significant increase in infections and deaths, experts said.
“The central and most important thing we needed was national leadership from the president to be able to really lead with empathy,” said Anita Cicero, deputy director of the Johns Hopkins Center for Health Security. “It seemed much more focused on the administration as the lead character, rather than communities in need.”
A hallmark of the response has been the secrecy of some in the White House, including Meadows, whom other officials described as outright hostile in his denial of the virus and punitive toward colleagues who sought to follow public health guidelines or be transparent.
As the virus spread wildly among White House staff this fall, Meadows sought to conceal some cases from becoming public — including, at first, his own — and instructed at least one fellow adviser who sought to disclose an infection not to.
In addition, Meadows threatened to fire White House Medical Unit doctors, who fall below the chief of staff in the chain of command, if they helped release information about new infections, according to one official. Ben Williamson, an aide to Meadows, said it was “false” that the chief of staff ever threatened to terminate doctors.
Meadows argued internally, according to this official, that the White House was “under no obligation to tell the press or the public that Joe Schmo who works in the White House has tested positive.”
Despite shunning recommended protocols internally, Trump aides speak with pride about the actions they took on the pandemic and are incredulous that their work has been so widely panned.
One senior administration official involved in the response said what was accomplished in less than a year — from producing and distributing protective gear to creating vaccines — is nothing short of remarkable. But, this official acknowledged, “The way it was messaged, unfortunately, was flawed.”
A second senior administration official said, “I’m not clear on what Trump should have done different, but put me in the camp of, well, something, because it has not been a success.”
Olivia Troye, a former Pence adviser and task force aide who resigned in the summer and campaigned against Trump’s reelection, said the nation’s trauma is a result of the president’s mismanagement of the crisis early on, and is being prolonged by his disinterest in it now.
“I would love to say that I’m shocked, but I’m not,” Troye said. “This is in keeping with everything he has been.” She added: “People are still dying every day. There’s thousands of cases every day and yet he won’t do the right thing. . . . To see a sitting president directly refuse to help during a crisis is just flabbergasting to me.”
Paul A. Offit, who is director of the Vaccine Education Center at Children’s Hospital of Philadelphia, a professor of vaccinology at the University of Pennsylvania and a member of the FDA’s vaccine advisory council, said of Trump: “He’s a salesman, but this is something he can’t sell. So he just gave up. He gave up on trying to sell people something that was unsellable.”
On Friday morning, in a tableau orchestrated to provide hope to a beleaguered nation, Pence and second lady Karen Pence received the Pfizer vaccine — a needle in his left shoulder as they sat beneath a sign that read, “SAFE and EFFECTIVE,” broadcast live on national television.
Tucker Carlson arrived at Trump’s private Mar-a-Lago Club the first Saturday in March, before cities started shutting down, on an urgent mission: to convey to the president the seriousness of the coronavirus threat.
Carlson’s message was simple but pointed. He warned the president that the virus was real, that people he knew were going to get it, that the country might have already missed the point at which they could control it and, as he later told Vanity Fair, that “this could be really bad.”
But Carlson and the president ultimately talked past one another, said a person familiar with the conversation. Carlson told Trump he could lose the election because of the virus, and Trump argued that the virus was less deadly than people were claiming.
The scene at Mar-a-Lago that weekend underscored the concerns. Far from taking any precautions, Trump that Saturday dined with Brazilian President Jair Bolsonaro and his delegation — several of whom later tested positive for the virus — while Donald Trump Jr.’s girlfriend, Kimberly Guilfoyle, threw herself a lavish 51st birthday party at the club. The next day, Trump hosted a fundraising brunch with about 900 attendees.
As the country began to shut down in March, Trump and his administration found themselves in the early throes of denial and dysfunction. Despite the warnings of Carlson and others, Trump continued to downplay the severity of the virus, and turf wars and unclear chains of command roiled the administration’s fledgling response.
Public health advisers and other administration officials were left scrambling — scattershot, and with little clear direction — to recoup time squandered.
Jared Kushner, the president’s son-in-law and senior adviser who had spent the early days of 2020 focused on other challenges in his overly large portfolio — including a Middle East peace plan and overseeing Trump’s reelection campaign — turned his attention to the virus.
Kushner’s allies and even some of his critics say he was effective in helping cut through bureaucracy — ensuring, for instance, that states eventually had as many ventilators as they needed. A text or call to Kushner could yield a clear response or directive in just minutes, said one senior administration official, and shortly after Pence was appointed head of the coronavirus task force his chief of staff, Marc Short, enlisted Kushner’s help to streamline resources and speed up response times.
But the help Kushner provided was often ad hoc rather than part of a long-term strategy, according to people familiar with his role.
“It was entirely tactical troubleshooting and, to be fair, it was pretty successful, with the ventilators and this and that, but it was whack-a-mole,” said an outside Republican in frequent touch with the White House.
Part of Kushner’s coronavirus management approach was an ambitious effort to bring in a cadre of young consultants from the private sector as volunteers. The group was dismissively referred to as the “Slim Suit” crowd.
“[Kushner] is like, ‘I’m going to bring in my data and we’re going to MBA this to death and make it work,’ ” one senior administration official said.
But problems quickly emerged with Kushner’s team of volunteers. The group was not issued government laptops or emails, forcing them to use their personal Gmail addresses — a practice that often hindered their efforts to procure personal protective equipment from companies that were understandably skeptical of inquiries coming from nongovernment email accounts. The volunteers in charge of PPE procurement also did not know the Food and Drug Administration requirements for importing the protective equipment, and found themselves spending unnecessary time Googling basic questions and calling the FDA for guidance.
Max Kennedy Jr., a senior associate at a private growth equity firm when he joined Kushner’s effort as a volunteer, was so alarmed by what he witnessed that he initially filed an anonymous whistleblower report.
Among his complaints was a culture that prioritized tips and leads from VIPs, which consumed an inordinate amount of the volunteers’ time and energy. Kennedy wrote in his report that Jeanine Pirro, a Trump booster who hosts a Fox News show, “repeatedly called and emailed until 100,000 masks were sent to a particular hospital she favored. No checks were completed to ensure that the hospital was in particular need of PPE.”
Kennedy, a lifelong Democrat and a grandson of Robert F. Kennedy, later revealed his identity and, in an interview with The Washington Post, described a group of smart and earnest volunteers who were, at best, out of their depth and, at worst, asked to do things they felt uncomfortable doing.
Kennedy said that Brad Smith, the director of the Center for Medicare and Medicaid Innovation and a friend of Kushner, asked him and another volunteer to make a coronavirus model for 2020 that specifically projected a low casualty count. When Kennedy noted that he had no training in epidemiology and had never modeled a virus before, he recalled, Smith told him that it was just like making a financial model. The other models made by the health experts, Smith explained, were “too catastrophic.”
“‘They think 250,000 people could die and I want this model to show that fewer than 100,000 people will die in the worst-case scenario,’ ” Kennedy said Smith told him. “He gave us the numbers he wanted it to say.”
Kennedy and the other volunteer refused to make the model. But he said the incident left him discomfited.
“[Smith] said, ‘Look around. Does it look like 250,000 people are going to die? I don’t think so,’ ” Kennedy recounted. “And I remember thinking it was a weird thing to say because we were surrounded by military officers in the [Federal Emergency Management Agency] basement and it did look like a lot of people might die.”
In an emailed statement, Smith denied asking Kennedy and a fellow volunteer to create a low fatality model.
“The only model I asked the team to build in the three weeks Max volunteered was a model to project PPE needs through July 2020,” Smith said. “To calculate PPE needs, the model used hospitalizations and deaths as inputs. The mean version of the model assumed 169,000 deaths by July 2020 and the worst case version of the model assumed 312,000 deaths by July 2020. According to the CDC, there were approximately 160,000 deaths as of July 30, so the model’s assumptions proved to be very accurate.”
There were other problems too. Kushner’s initiative to stand up drive-through testing sites nationwide at retail stores such as CVS, Target and Walgreens, for instance, may have been a good idea in theory but almost instantly raised concerns. Government officials asked Kushner and his team whether they had fully considered the logistical and supply issues behind setting up the sites — including swabs and reagents for tests, and protective equipment for the clinicians administering them.
Kushner’s team responded that they had it covered, but it quickly became clear they did not. At a time when health-care workers were using garbage bags as gowns and reusing N95 masks because of severe shortages, roughly 30 percent of “key supplies,” including masks, in the national stockpile of emergency medical equipment went toward Kushner’s testing effort, according to an internal March planning document obtained by The Post and confirmed by one current and one former administration official.
Though Kushner had initially promised thousands of testing sites, only 78 materialized, the document said, and the national stockpile was used to supply more than half of those.
“The knock against Jared has always been that he’s a dilettante who will dabble in this and dabble in that without doing the homework or really engaging in a long-term, sustained, committed way, but will be there to claim credit if things go well and disappear if things go poorly,” a former senior administration official said. “And this is another example of that.”
By the summer, Trump had grown angry with Kushner over problems with testing, said current and former administration officials — a rare conflict between the president and his son-in-law.
Matthews defended Kushner’s testing initiative, saying there are now more than 6,000 retail testing sites and that the federal government has established more than 500 temporary surge testing sites in 17 states over the past 10 months.
At the beginning of the outbreak, the United States failed to deploy a coronavirus diagnostic test across the country so state and local officials could quickly detect and trace confirmed cases. And while the administration eventually scaled up testing considerably — more than 1.5 million tests a day are now being conducted — it still has not developed a national testing strategy. Even as more tests have become available, experts said, there have rarely been enough for the scale of the pandemic.
“Compared to other countries, the biggest mistake we made was in testing,” said Katrina Armstrong, a physician and chief of Massachusetts General Hospital who has been treating coronavirus patients. “It’s not even a hard test, and we whiffed it. There should be central leadership bringing everything together. For the clinical side, not having access to testing early on and through the summer was the biggest tragedy of what got us here.”
The best chance to control an outbreak is at the very beginning. But U.S. officials squandered that opportunity in February for two key reasons. The first was the CDC’s failure to deploy a working coronavirus test, and the second was the task force’s almost singular focus on repatriating Americans from China and cruise ships, rather than on preparing the United States for an inevitable outbreak.
A review of task force agendas from that time demonstrates a disproportionate focus on cruise ships, masks and other bureaucratic and logistical issues, rather than on more practical public health steps such as testing, contact tracing and targeted efforts to prevent the virus’s spread. That allowed the virus to spread undetected for all of February, several officials and experts said, as it seeded itself in New York, Washington state, California, New Orleans and other populous areas. And from then on, the country was perpetually behind the virus.
Kennedy said his experience volunteering in the White House left him disillusioned.
“I don’t think this has to be a politicized crisis,” Kennedy said. “This pandemic is incredibly tragic and, as someone who was in the room, it was very clear it wasn’t taken seriously. It was well understood what measures could be taken to save lives, to reduce the severity of the pandemic, and the administration and Jared Kushner made an active choice not to pursue those actions.”
As the virus began to rage across the United States, some of the nation’s health officials had a novel idea. Face coverings were emerging as one of the simplest tools available to control the contagion’s spread. So Robert Kadlec, the assistant secretary for preparedness and response at the Department of Health and Human Services, called Jerry Cook, an executive at the cotton clothing giant Hanes, on March 13 to discuss producing enough masks to send to every American household, according to two senior administration officials.
Cook pulled together a number of underwear makers, including Fruit of the Loom, SanMar, Beverly Knits and Delta Apparel, to figure out how to redirect their manufacturing operations to manufacture 650 million three-ply cotton masks — enough to send a packet of five to each household. The masks would bear an HHS logo, contain a microbiocide that would kill the virus, and say: “Do your part, help stop the spread.”
A command group at FEMA unanimously approved the plan, and the task force doctors did as well. Birx, the White House coronavirus response coordinator, saw the white prototypes and asked if they could be made in a neutral tone.
But when Kadlec’s boss, HHS Secretary Alex Azar, began to pitch it at a White House task force meeting in March, there was sharp dissent. Several on the task force generally did not have much confidence in Kadlec, and a senior administration official said his plan was half-baked and that he was unable to answer basic questions, like how much the effort would cost or how they would deliver all the masks.
Short abruptly stopped the conversation and told Pence the idea wasn’t ready and was being pulled off the agenda. Other officials complained that the masks looked like underwear, according to three current and former senior administration officials. Peter T. Gaynor, the FEMA administrator, compared them to jockstraps.
Then there was the issue of logistics. For months leading up to the pandemic, Trump had been attacking the U.S. Postal Service and airing grievances over its business relationship with Amazon. Some aides surmised that, for Trump, a private-public partnership involving the Postal Service as the distributor would be a nonstarter.
The mail-a-mask plan was killed. The Office of Management and Budget tried to cancel the contracts with the underwear makers, but the masks still were produced and distributed to health clinics, religious groups and states that requested them. Hanes did not respond to a request for comment.
Kadlec was so frustrated that he decided his time as preparedness and response chief was no longer best spent on preparing and responding, so he focused instead on vaccines and therapeutics.
Skepticism of masks became a hallmark of the Trump administration’s pandemic response. On April 3, when the CDC recommended that all Americans wear masks, Trump announced that he would not do so because he could not envision himself sitting behind the Resolute Desk with his face covered as he greeted visiting dignitaries. The president stressed that mask-wearing was “voluntary,” effectively permitting his legions of followers to disregard the CDC’s recommendation.
In the months that followed, Trump was only seen wearing a mask on rare occasions, instead following the advice of Stephen Miller, Johnny McEntee, Derek Lyons and other trusted aides to think of masks as a cultural wedge issue.
Pence covered his face with somewhat more regularity than the president, but after forgoing a mask during an April 28 visit to the Mayo Clinic in Minnesota, he drew a public rebuke from the hospital’s leaders. Short then yelled at a hospital official over it, a person with knowledge of the visit said.
“What the Trump administration has managed to do is they accomplished — remarkably — a very high-tech solution, which is developing a vaccine, but they completely failed at the low-tech solution, which is masking and social distancing, and they put people at risk,” Offit said.
Trump did not imagine the coronavirus would consume the fourth year of his presidency. When he established a task force in January, he assumed it would not last long and that the crisis would subside relatively quickly, according to two officials with knowledge of the situation. These officials said the president selected Pence, the favorite of then-acting White House chief of staff Mick Mulvaney, for chair of the task force over Gottlieb and former New Jersey governor Chris Christie.
In retrospect, according to a senior administration official, Trump’s biggest political miscalculation was basing the task force in the White House. “Once you put it in the Situation Room, the president owns every failure, leak, whatever, whereas this could have been an Azar, Redfield, Hahn problem,” this official said.
In the early weeks, Pence was the frontman at daily coronavirus news conferences. He provided top-line updates, including case and death counts, before turning it over to Fauci, Birx and other health professionals. Short advised the vice president against detailing such dire statistics, but Pence insisted, believing he was obligated to share such facts with the public, according to another official with knowledge of these discussions.
Over time, however, Trump decided he wanted to be the face of the government’s response, so he took over Pence’s role at the briefings. A number of Republican senators privately counseled the president to let the doctors be out front, according to a senior Republican congressional official, but “Trump just couldn’t let someone else get all that attention.”
Trump’s performances were riddled with misinformation, contradictions and indecorous boasts, while also predicting miracles and promoting cure-all therapeutics. Trump often said he was trying to be a “cheerleader” for the country, and a senior administration official explained that the president has said he drew lessons from Norman Vincent Peale’s “The Power of Positive Thinking.”
“What he’s saying there is, ‘I’m going to will the economy to success through mass psychology. We’re going to tell the country things are going great and it’s going to be a self-fulfilling prophecy,’ ” this official said of Trump.
But there were consequences for Trump’s often too-rosy takes. Hogan — who as chairman of the National Governors Association helped lead regular meetings among governors and task force members, sometimes including Trump — said there was “a huge disconnect” between what was agreed to by Pence and members of the task force and what the president told the public.
“We would have a great meeting that might have lasted an hour or two with all the top folks focused on the virus, and then the president would have one of those rambling press conferences that went on maybe an hour too long and he said the opposite of what others in the administration told us that day,” Hogan recalled.
The Maryland governor, one of the rare Republicans who seemed unafraid to challenge Trump, said he directly confronted the president in some of these sessions about what was not working.
“I pushed back very hard when there was no testing program and there was no availability of basic supplies, like swabs and tubes and testing agents and ventilators,” Hogan said. “There were a few times the president bristled when I wasn’t saying everything was great. . . . One time the president said on a call, ‘You’re not being very nice to me.’ I said, ‘No, Mr. President, I’m always nice. I’m just telling you what the governors see.’ ”
The White House also made governors’ jobs more difficult by interfering at the CDC, which was forced to water down reopening guidelines for businesses, schools, restaurants and other facilities after a cadre of White House and administration officials weighed in with suggestions that were not based on science.
By late spring — after he infamously suggested people ingest bleach to cure themselves of the virus — Trump stopped appearing at coronavirus briefings. Meadows is among those credited with pulling the plug.
“He felt it was a loser message,” said one senior administration official with knowledge of Meadows’s thinking. “So why message on covid?”
Scott Atlas found himself in Trump’s orbit the way so many do: through the television screen.
A neuroradiologist with no infectious-disease or public health background, Atlas joined the coronavirus response team in August as a special government employee, after a few senior Trump advisers — Kushner, McEntee and Hope Hicks — were impressed by his appearances on cable news.
Atlas began working out of Kushner’s office suite, and quickly scored a blue badge — the most coveted level of White House access — and a spot on the coronavirus task force. Though many were skeptical of him, the vice president’s team felt that if Atlas was going to be part of the virus response, then he needed to be a full-fledged member of the effort, said two people familiar with the decision.
Atlas pushed a controversial “herd immunity” strategy — of letting the virus spread freely among the young and healthy — and clashed with others on the task force, many of whom described him as combative and condescending. He lorded his seemingly unfettered access to the president over the group and, as one senior adviser said, “The science just got totally perverted with Scott in the room.”
Atlas, who resigned Nov. 30, defended his advice to Trump as “based on the best available science and data at the time” and said he sought to reduce both the virus spread and what he called “structural harms.” In a lengthy emailed statement, Atlas denied much of The Post’s reporting about his work in the administration, including that he had described those with the coronavirus in derisive or demeaning terms.
“I am very disappointed to see more totally false statements and patently absurd lies about me,” Atlas said. “Although I don’t intend to weigh-in on every false and defamatory story or allow myself to be endlessly used as a political piñata, I firmly deny the false accusations that, as a special advisor to the President, I advocated for ‘herd immunity’ via letting the infection spread as a scientific approach to the pandemic. Nothing could be further from the truth.”
Even those inclined to be sympathetic to Atlas’s coronavirus theory — that the virus mainly affected the most vulnerable, who were the only ones who truly needed protection — found his personal manner off-putting, said one senior administration official. And privately, Atlas often argued his case more crudely, bluntly saying coronavirus was a disease that only affected the overweight, the diabetic and the elderly, the other adviser said.
But Trump liked Atlas — and the shoddy science he was peddling seemingly bolstered the president’s optimism. Atlas’s appeal to Trump, this adviser explained, was that he “had a doctor title but a MAGA perspective,” referring to Trump’s “Make America Great Again” slogan.
Atlas’s presence, however, frustrated much of the rest of the group, especially the public health experts who feared he was undermining their hard-fought efforts to keep the public safe.
“If you ever wanted to spread confusion and give license to the people in the cities and states who did not want to abide by any of the public health measures, you gave them license to do it,” Fauci said. “They could say, ‘Look, this guy who’s a well-respected Stanford person who the president seems to like is saying this thing; why should we listen to Fauci?’ I think he was disruptive to what Birx and I were trying to do.”
The addition of Atlas to the coronavirus task force was just the latest iteration of the infighting that had plagued the virus response all along. He clashed with the other doctors, but especially with Birx.
One early dispute was over testing. At the time, the president was pushing to move away from the widespread testing recommended by health experts and toward more narrow surveillance testing in vulnerable communities. Atlas and Birx fought over the issue in the Oval Office, with Birx — who was backed up by Redfield — advising that widespread testing was the best way to catch new cases, a senior administration official said.
In August, the CDC put out revised testing guidelines that were more in line with Atlas’s view than Birx’s, only to walk them back after a public outcry.
During another task force meeting, Atlas argued that it would be reasonable to consider substantially fewer mitigation efforts, allowing people to become infected. Instead, Atlas said, officials should focus their efforts on protecting those in nursing homes. Birx retorted that the vulnerable were not only in nursing homes, prompting agreement by other doctors in the group.
“Dr. Scott Atlas has caused people to lose their lives because he stood at the White House podium and told people masks may not work and he told people we should get over it and build up herd immunity,” said McGowan, the former CDC chief of staff. “He’s telling the world lies from a bully pulpit, from a position of power, and I believe people died because of that.”
Some of Trump’s advisers tried to convey to the president how much his reelection might hinge on the pandemic. Being seen as a responsible, empathetic leader in a moment of crisis, they explained, would buoy his chances of victory.
For instance, internal campaign data from pollster Tony Fabrizio found that in July, just 40 percent of voters approved of Trump’s handling of the virus and 58 percent disapproved, a deficit of 18 percentage points. Among independents, the gap grew to 30 percentage points, according to a senior campaign adviser.
According to an internal polling memo obtained by The Post, more than 70 percent of voters in target states supported “mandatory masks at least indoors when in public, and even a majority of Republicans support this.”
Though Republicans were not keen on the idea of an executive order for mask-wearing, they were less opposed to an order that applied only indoors, the internal polling found. And, as one of the slides reviewed by The Post read, “Voters favor mask-wearing while keeping the economy open,” and also favor Trump “issuing an executive order mandating the use of masks in public places.”
Given those findings, Fabrizio, Kushner, then-campaign manager Brad Parscale and others urged Trump to model good behavior by wearing a mask, and to encourage his supporters to do so as well, several Trump advisers said. But the president was unreceptive, as was Meadows.
“He was of the opinion that it would hurt his base,” the senior campaign adviser said. “He listened and it just didn’t move him. The argument just didn’t move him.”
The president and some on his team were also increasingly frustrated with Fauci, who frequently appeared in the media offering what they viewed as an overly alarmist public health message. “Fauci was probably Joe Biden’s most effective campaign surrogate on the trail in 2020,” said Jason Miller, a senior campaign adviser.
Trump aides added that there also was little pushback to the idea of Trump resuming large rallies — without social distancing or mask requirements. The few advisers who did counsel caution were largely ignored, with allies arguing that rallies were key to the president’s brand and that the raucous events also helped improve his mood.
“My attitude was, how are voters going to take us seriously that we’re taking this seriously if we’re doing things where the perception is we’re putting people at risk?” the senior adviser said. “It surely undermines.”
As summer turned to fall, Birx — whose calming guidance and elegant scarves had inspired online memes — found herself silenced and increasingly minimized in the coronavirus response.
Atlas succeeded in sidelining her from Trump’s immediate orbit. Her national television appearances all but vanished. She traveled to dozens of states and had unfiltered conversations with governors and local officials, but was denied the time she wanted with the president to keep him abreast of the facts. And her warnings fell on deaf ears inside the West Wing.
“She would circulate her daily report, and more often than not, there would be no responses from anyone on the email,” a senior administration official recalled. “I remember there were times where she would flag something massive, like, we are within weeks of a massive remdesivir shortage, and no one would reply.”
Birx met either in person or virtually with Fauci and other doctors on the task force at least once a week to discuss the science and support each other as they were being ignored at the White House. They plotted alternative ways to get their messages to the public, including through Birx’s travels to states.
But Birx was undermined there, too. After she advised Florida’s political leaders in August to close bars and restrict indoor dining, Atlas visited the state and contradicted her. Atlas told Gov. Ron DeSantis (R) and other local leaders to focus less on widespread testing and instead to direct their efforts to opening the economy back up and opening schools, according to two senior administration officials.
As it became clear the pandemic was worsening and the country was headed for a disastrous winter, Atlas dismissed Birx’s projections in task force meetings and in private discussions with Trump and Pence. This pushed Birx to be more outspoken, especially in the reports she and her small team put together, some of which took on a grim tone, officials said.
“It was almost like she wanted to make sure she had a paper trail saying, ‘I, too, think we’re in trouble,’ ” another senior administration official said. “It was a combination of events that pushed her to change her tune and be much more realistic about the seriousness of what was going on.”
The rise in cases and deaths in November coincided with a drop in visibility from Trump and Pence. Following the Nov. 3 election, the two went many days without public appearances. Whenever the president did speak or weigh in on Twitter, it was usually about his desire to overturn the election results, not about the worsening pandemic.
As for Pence, one consistent criticism was his reluctance to deliver tough news and dire coronavirus statistics to the president. As one former senior administration official put it, “He knows, like everybody else knows, that covid is the last thing Trump wants to hear about or see anybody making news about. If not touting Operation Warp Speed, it’s the topic that shall not be spoken of.” A senior administration official and Pence ally, however, said Pence always shared the daily reality with Trump but, as a perpetual optimist, often did so with a positive spin.
The president and vice president did make a couple of appearances to tout vaccine breakthroughs. But much to the frustration of health officials, they did little to leverage their influence with the 74 million Americans who had just voted for them to persuade people to make sacrifices to stop the spread.
“There are tens of millions of people who fundamentally don’t have the same perception of reality when it comes to the virus,” Frieden said. “There are always going to be people who are suspicious and paranoid and believe in UFOs or whatever, but because we’re not on the same page on covid, it’s very hard to get people to act together.”
The week before Thanksgiving, health officials fanned out to plead with Americans not to travel over the holiday. Fauci practically begged people in an appearance on ABC’s “Good Morning America” to stay home and not interact with people outside their immediate household.
But even America’s most famous doctor, one with an approval rating well north of Trump’s, was unconvincing to many. More than 3 million people were screened at U.S. airports in a three-day period just before Thanksgiving, according to the Transportation Security Administration. AAA projected that an additional 48 million people would travel by car around the holiday.
That nonchalance about spreading the virus carried this month into the White House, where Trump and first lady Melania Trump hosted a traditional series of elaborate holiday parties.
Night after night, the Trumps had party guests congregate inside the White House residence to mix, mingle and hear the president speak — each clinking of champagne flutes a potential superspreader moment.
“Here, you have Fauci and Birx saying: wear a mask, keep your distance, avoid congregate settings and indoor crowds, particularly indoors,” a senior administration official said. “And then you have these events at the White House where nobody is wearing a mask, they’re having an event inside and then coming outside, if there ever was a complete confusion of messages.”
Pence and second lady Karen Pence also hosted holiday parties at the Naval Observatory, where pictures from one such event earlier this month showed hundreds of guests mingling mostly maskless underneath an enclosed tent. Even Pence himself, the head of the coronavirus task force, did not wear a mask.
Members of military bands, servers and others were forced to work and exposed for hours to guests who were not wearing masks, officials said.
At least one worker who got infected never heard from anyone in the White House about the illness. They were replaced for the next party.
The latest data identified additional sequences in S:501 mutant variants from the UK, Denmark, Australia, & South Africa, but no additional countries.
(!This table does not distinguish variants & some countries listed haven't seen 501 in months!)
2/4
From the plot of variants frequency in sequences, per country, we can see that the 501Y variant (pink) is expanding in the UK (the last data point represents incomplete data & will likely change in future).
3/4
Seeing no new countries in sequences isn't at odds with media reports: our analysis is based only on sequences which are made available to scientists through GISAID. Countries can analyse their own sequences faster, so they may be detecting cases we do not have samples for.
4/4
by ti-amie From yesterday:
Dr Emma Hodcroft @firefoxx66
Is the new UK variant the same as the new South African variant (501Y.V2)?
No.
They both share the same mutation in spike: N501Y (N->Y at position 501). However, the 2 variants have arisen separately.
In the tree below, the UK variant is in green at the top. The SA variant is the one with large yellow circles nearer the bottom.
Though it's a bit hard to see in this tree, they are quite distant genetically: they have many mutations they do not share!
2/N
S:N501Y has occurred multiple times around the world. Not all of these have risen & become prominent. So the role of 501Y is probably more complex.
UK variant & SA variant both have many other mutations that are being investigated.
3/N
Both the UK & SA variants also sit on 'long branches'. This means they have more mutations (different in each) than we would expect. Both also have a higher number of mutations in spike.
Hard to interpret what this means, but another reasons scientists are investigating.
4/N
Where have we seen these variants so far?
For the UK variant:
In the UK, we see sequences from England, Wales (a little hard to see) and Scotland. None in Northern Ireland so far.
For the UK variant:
Outside of the UK, we see very small numbers of sequences in Denmark (a bit hard to see - hidden behind UK circle) & Australia. Their position on the tree indicates that they're likely exports from the UK.
Importantly!:
In Europe, the UK & Denmark are the most regular & prolific sequencers. So the variant could be elsewhere & not detected yet.
In Africa, same is true for South Africa.
More coordinated sequencing efforts regionally & globally would help us monitor variants
8/N
'm re-running the cluster builds now with data from yesterday. I'll post a link when they are done, though I don't expect much will change from the above pictures/links.
9/N
Are either/both more transmissible? I don't think we know for sure yet, but scientists in the UK seem to believe there are indicators of increased transmission in that variant.
Certainly, we should be extra cautious & each do our part to break transmission chains.
10/N
by ti-amie Part 3 of thread
Will it impact the vaccine? I don't think we know for sure yet. Hopefully not
The vaccine causes your body to recognise many parts of spike, so a few changes should not mean it stops working. However impact of more changes is less sure - scientists investigating this now.
11/N
Just to add: notifications exploding right now - I'll be missing a lot & can't respond to them all - sorry!
Will try to update this thread when I can, but will probably fall off from individual responses a bit.
12/N
Some vaccine information from
@KrutikaKuppalli from the ACIP (Advisory Committee on Immunization Practices - advises the CDC in the USA).
Dr.Krutika Kuppalli
@KrutikaKuppalli · Dec 19
Right now at #ACIP a question about how the @moderna vaccine may work against the new mutant strains of #COVID19 being identified such as those in the UK.
They are currently evaluating this but so far things appear okay and will do deep sequencing on breakthrough cases.
13/N
Very importantly - need to recognise incredible amounts of work on the new variant in South Africa (501Y.V2) by
@Tuliodna
&
@EduanWilkinson
at
@krisp_news
.
And a lot of hard work in the UK on that variant by scientists at
@CovidGenomicsUK
& SPI-M.
14/N
A new run of the S:N501 data is up now - with improved background sequencing to better show how the mutations have arisen independently!
UK variant at top in green. SA variant the blue in the middle - stemming from "20C" label.
by ti-amie I had to split the thread because there can only be 5 URL's per post.
by ponchi101
ti-amie wrote: ↑Sun Dec 20, 2020 11:55 pm
I had to split the thread because there can only be 5 URL's per post.
Can be easily changed. Let me know if you want that
by ti-amie This was an unusual thread so let's not tinker with things right now. If she always posts like this I'll PM you.
by MJ2004 Love the Doonesbury strip.
We just spent the last two days driving to my parents' place in Florida, even though my parents are staying in Maine until they get vaccinated. We weren't comfortable flying, which would have included two cars rides to and from the airport, time spent in the airport terminal (more dangerous than the flight itself), plus the obvious sitting next to strangers on the flight. People were masked in rest areas. We checked in/out of the hotel remotely and used keyless entry through our phone on the hotel door (cool feature). Packed most of our food with just one take-out stop at a restaurant.
We got to the land of Floriduh where masks are used much less. We were in the elevator with our luggage at my parents' condos (plan to take the stairs mostly) and of course a woman with no mask gets on with us.
Stay safe through the holidays everyone! Hopefully it's the final stretch before we are able to get vaccinated.
by ponchi101 Colombia going back to some restrictions. As of today, what they call "Pico y Cedula" (Peak & ID) goes back into effect. You can only shop on days matching your ID number (even numbers on even days, odds on odds). Xmas shopping and related activities made everybody go out, so the country is going back to high numbers of cases and deaths.
By now, only massive vaccination will control this. And that is hoping that none of the mutations can bypass the vaccinnation.
Enjoy Fla, MJ. Hope you have a view of the ocean.
by ti-amie toomas hendrik ilves
@IlvesToomas
Russian Scientist Who Worked on Coronavirus Vaccine Stabbed, Falls Out of Window
by ponchi101 Well, that's a change. I thought the standard Russian MO was for the people to fall from the window and LAND ON THE KNIFE.
They are getting better at this.
by Suliso 0.1% of US population has died from Covid-19 so far.
by ponchi101 It is one of those numbers that is puzzling. On the one hand, 0.1%. Very small. On the other, that is 350,000 people. A large cohort.
Today I received a mail from the skiing club I belong to in Colorado. Two members, elderly, have died of C19. The wife of one of them is in the ICU, but in stable conditions.
That little town (Pagosa Springs) is basically a retirement community. A large elderly population, which votes GOP. Then a large service sector (the stoners) that vote DEM. It would be interesting to see which group is suffering the most (the dems are also not that young. Lots of 60's hippies that found Nirvana in that mountain).
by ponchi101 Suliso's post got me curious. How many deaths are in the USA every year? The CDC keeps track. And for 2018, the numbers were (just the top 8):
So, with a little over one week to go for the year, C19 will end 2020 as the third leading cause of death (assuming numbers similar to 2018), combining for more deaths than accidents and respiratory disease put together.
by ti-amieThey Helped France Fight the Virus. Now France Is Fast-Tracking Their Citizenship.
Some 700 foreigners who were exposed to the coronavirus through their frontline work are being given expedited naturalization reviews.
By Constant Méheut
Dec. 22, 2020
PARIS — Nine months after its president declared “war” against the coronavirus, France announced Tuesday that it has fast-tracked hundreds of citizenship applications from foreign frontline workers who have distinguished themselves in the battle.
“Foreign workers gave their time and swung into action for all of us during the Covid crisis,” said Marlène Schiappa, France’s junior minister for citizenship. “It is now up to the Republic to take a step toward them.”
The beneficiaries include not just health care workers but also garbage collectors, housekeepers and cashiers, Ms. Schiappa said.
The fast-tracking measure is a notable departure for a country that has adopted increasingly tight immigration rules. Caught in the clog of paperwork, citizenship applications can take years to complete, and the number of naturalizations has been decreasing over the years.
Some 48,000 people acquired French nationality through naturalization last year, or about 18 percent fewer than in 2015, according to statistics from the National Institute of Statistics and Economic Studies.
The government initiated the measure in September, when France was bracing itself for a second wave of the pandemic. On Tuesday it announced that some 700 foreigners who were exposed to possible coronavirus infection through their work have been put on a fast track for naturalization since then.
Aziz Youssef, a Tunisian-born physiotherapist who migrated to France in 2014, said that obtaining citizenship by naturalization amounted to “an obstacle course.” He recalled first sending an application in late 2016 after graduating with a physiotherapy degree — and being given an appointment for a year later.
Mr. Youssef, who said that he had visited dozens of isolated patients during the first wave of the pandemic, had expected his application to be completed by 2022. But after learning about the government’s new exceptions for frontline workers, he checked in with the local authorities, who fast-tracked him. His penultimate interview took place in early December.
“Everything sped up very quickly,” Mr. Youssef said, adding that he viewed acceleration as “a form of recognition for the work that was done.”
The first coronavirus wave in France came close to breaking the country’s health care system — and frontline workers were at greater risks than most. So Ms. Schiappa asked regional officials to accelerate the citizenship applications of foreign workers who were among them.
“They actively participated in the national effort, with dedication and courage,” Ms. Schiappa wrote in a letter to regional authorities.
With more than 60,000 deaths caused by the coronavirus and close to 2.5 million coronavirus infections reported, France has paid a heavy toll in the pandemic. With infection rates failing to fall as quickly as predicted, the French government recently decided to delay the relaxation of some lockdown restrictions.
More than 70 applicants have obtained citizenship since September and 693 more are in the final stage of the process, the authorities said. Although their nationality has not been made public, beneficiaries mainly include health care and social workers, as well as shop employees and civil servants.
There are several different ways to gain citizenship in France: through marriage; by being born in France or to a French parent; and through naturalization. In this last case, the applicant must have lived in the country for at least five years — or two years for immigrants with a degree obtained in France — have stable resources and be considered integrated into French society.
In September, Ms. Schiappa also ordered officials to reduce the residency period in France required to obtain citizenship by naturalization to two years from the usual five in the case of “great services rendered.”
Didier Leschi, the director of the French Office of Immigration and Integration, said the fast-tracking measure was part of “a long tradition that can be traced back to the French Revolution, which is to grant citizenship to the benefactors of the country.”
But Mr. Leschi added that it partly broke with this tradition, which generally applied only to individual and exceptional cases. “Here, a collective effort was rewarded,” he said.
This was not the first time in recent years that France departed from its strict rules of naturalization to reward laudable actions. In September 2018, Mamoudou Gassama, a migrant from Mali, was made a French citizen after heroically rescuing a 4-year-old boy who was hanging from a balcony.
Mr. Youssef, the physiotherapist, said he was now waiting for his final interview, where he will be tested on his historical and cultural knowledge of France.
“This pandemic has revealed that France needs these people: doctors, surgeons, essential workers,” Mr. Youssef said.
by ponchi101 What a novel concept: grant citizenship to people that have risked their lives for your country.
I wonder what other country could use this idea. Uhm.... nope, I draw a blank.
by ti-amie Meanwhile back in the US...
Brandi Buchman @BBuchman_CNS
The unanimous consent request from Dems to vote on increasing direct payments to $2k failed on the House floor because GOP House Leader Kevin McCarthy needs to consent and he does not. @CourthouseNews
@DebDingell during the presser with Leader Hoyer lets loose and says of outgoing President Trump that he "doesn’t give a damn about people."
"He sowed more fear. He threw kerosene on a fire."
"Republicans blocked it, not Democrats," Dingell says of the push to increase stimulus checks from $600 to $2,000. "I’m merely to here to say on Christmas Eve we will come back on Monday."
The UC was blocked, the House can pass $2,000 but will McConnell take it?
Hoyer: We can only do in the House what we can do. We will have a new president and that president will give leadership.
Hoyer: "This president told R leaders he would sign this bill and then he gave his five-minute press conference."
On Monday, Hoyer will meet with Speaker Pelosi and leaders of Dem caucus and determine how to move forward.
Hoyer: "We're not going to let the government shut down and we're not going to let the American people down.
Hoyer, when fielding a question on whether it was a mistake to combine spending and the covid relief bill, he laughs lightly and says it was not but "perhaps the only mistake was believing the president would sign the bill."
Trump said he would not veto the bill explicitly. He said he wanted more. That's why Democrats are here today to get this done, Hoyer says, to "accommodate his perspective."
The MSM should really stop giving the GOP cover by saying "Congress"
by ti-amie CNN Breaking News @cnnbrk
Japan will ban entry to foreign nationals starting Monday through the end of January after several cases of the Covid-19 variant were recorded in the country, according to Japan's public broadcaster, NHK https://cnn.it/3hjMLHD
by ti-amieU.K. variant of coronavirus continues global spread, despite containment efforts
By
Miriam Berger
Dec. 26, 2020 at 12:12 p.m. EST
The highly transmissible variant of the novel coronavirus first detected in England had by Saturday been documented in several European countries, Japan, Australia and Lebanon, despite efforts to curb its spread through massive global disruptions in travel and movement.
Fears over the fast-spreading form of the virus that causes covid-19 come in sharp contrast to a wave of hope sweeping some countries and communities as vaccination programs begin to be rolled out. Scientists do not think that the British variant is more deadly or resistant to the current coronavirus vaccines.
The variant has also been detected in France, Denmark, Spain, Sweden, the Netherlands, Germany and Italy.
While the United States has not yet reported a case, experts say it is likely due to the nation’s very low rate of genetic sequencing of the virus to check for such changes, despite Americans leading the world in coronavirus infections and deaths.
Beginning Monday, the U.S. government will require all travelers flying in from Britain to show proof of a negative coronavirus test taken within 72 hours of the plane’s departure. Early in the pandemic, the United States banned travelers from China and the European Union, among others, though by that point the novel coronavirus had already been widely spreading undetected due to limited U.S. testing.
Japan on Saturday temporarily banned all foreign nationals except those with residency from entering the country starting Dec. 28 through the end of January. Japan reported its first case of the British variant on Friday amid a new surge of coronavirus cases in the capital, Tokyo. Japan said five patients detected with the variant had all traveled from the United Kingdom, from which Japan had curbed travel last week.
Countries across Europe and other continents began to block or restrict travelers from the U.K. last week in reaction to the variant’s outbreak. Some, like France, have since walked back near total border closures amid widespread disruptions in trade and travel.
France initially closed its border to all travelers from the United Kingdom on Sunday, but on Wednesday began allowing E.U. citizens to pass through. The border closure, however, led to a massive backlog in freight trucks, leading thousands of drivers stuck Christmas Day near the border waiting for coronavirus test results to be able to cross the English Channel back to France.
Elsewhere, hopes are tentatively rising. Hungary on Saturday became the first European Union member to begin vaccinations, a day ahead of France, Germany and Spain, among others, who will kick off vaccinating high-risk populations on Sunday.
Scientists, however, are additionally closely following news of another variant of the novel coronavirus first detected in South Africa that experts say also appears to be highly transmissible. British health officials have already documented cases of the South African variant in the United Kingdom.
by ti-amie Alissa Walker
Dec 25
Merry Christmas everyone! La Scala’s Beverly Hills location is tucking these invitations to an indoor New Year’s Eve dinner in their takeout bags: “Please keep this discreet, but tell all your friends.”
Molly Jong-FastHouse with garden
@MollyJongFast
There are zero ICU beds in Southern California.
by Deuce
ponchi101 wrote: ↑Wed Dec 23, 2020 3:30 pm
Suliso's post got me curious. How many deaths are in the USA every year? The CDC keeps track. And for 2018, the numbers were (just the top 8):
So, with a little over one week to go for the year, C19 will end 2020 as the third leading cause of death (assuming numbers similar to 2018), combining for more deaths than accidents and respiratory disease put together.
I wonder if they'll give COVID-19 their own separate category for 2020, or if they'll lump it in with 'influenza/pneumonia'.
The deaths by accident number seems very low to me for such a populated country.
I checked, and the number of deaths by accident for 2018 is correct. It makes up about 6% of all recorded deaths. In fact, it's a significant increase from 1999, where it was 97,860, and about 4% of all recorded deaths.
by ti-amie Anna Merlan @annamerlan
Another “secret” New Years Eve party in LA, referencing Prohibition, promising masks required (sure), rapid tests (notoriously unreliable) and hand sanitizer, which we all know makes it totally safe to be in a crowded space for as long as you want. Hope it’s worth it, partiers!
Miranda Yaver, PhD @mirandayaver
This is infuriating. We are at 0% ICU capacity in southern California. We have record hospitalizations. We're experiencing ~14,000 new coronavirus cases per day. Can people just drink at home for one goddamn New Year's instead of endangering communities further in this pandemic?
by ponchi101 Instant COVID antigen testing? Sounds like a coffee brand ("Instant Folgers!")
by ti-amie Maybe it's me but some one telling you to text "HELLOSUCKERS" to get on a list doesn't sound like something I would want to do. #justsaying
by ponchi101
ti-amie wrote: ↑Sun Dec 27, 2020 11:48 pm
Maybe it's me but some one telling you to text "HELLOSUCKERS" to get on a list doesn't sound like something I would want to do. #justsaying
If you are a sucker, yes you do
by Togtdyalttai
ti-amie wrote: ↑Sun Dec 27, 2020 11:48 pm
Maybe it's me but some one telling you to text "HELLOSUCKERS" to get on a list doesn't sound like something I would want to do. #justsaying
I mean, the place is called Spanky's after all.
by ti-amie amNewYork @amNewYork
Chile said on Tuesday it had recorded its first case of the British variant of coronavirus, prompting health authorities to reinstate a mandatory quarantine period for all visitors entering the South American nation from abroad.
by ti-amieFirst case of highly infectious coronavirus variant detected in Colorado
By Joel Achenbach, Ben Guarino, Lena H. Sun and Isaac Stanley-Becker
Dec. 29, 2020 at 4:40 p.m. EST
Colorado officials on Tuesday reported the first known case in the United States of a person infected with the coronavirus variant that has been circulating rapidly across much of the United Kingdom and has led to a lockdown of much of southern England. Scientists believe the variant is more transmissible but does not make people sicker.
The case involves a male in his 20s who is currently in isolation in Elbert County, about 50 miles southeast of Denver, and has no travel history, according to a tweet from the office of Gov. Jared Polis.
“The individual has no close contacts identified so far but public health officials are working to identify other potential cases and contacts through thorough contact tracing interviews,” the tweet said.
A federal scientist familiar with the investigation, speaking on background to provide context for the announcement, said the fact that the person had no known travel exposure — in contrast with most known cases in which the variant has been seen outside the United Kingdom — indicates that this is probably not an isolated case, but rather the variant is likely spreading person to person.
“And we can expect that it will be detected elsewhere,” the federal scientist said.
Researchers have now detected the more transmissible variant in viral samples in at least 17 countries outside the United Kingdom, including as far away as Australia and South Korea, as of Tuesday afternoon. Officials in Canada had previously said they identified two cases, the first in North America.
While the variant appears to spread more easily, it is not leading to higher rates of hospitalizations or deaths, according to a new report from Public Health England, a government agency. Nor is there any sign that people who were infected months ago with the coronavirus are more likely to be reinfected if exposed to the variant, according to the report.
Scientists also believe these mutations will not allow the virus to escape the immune response incited by vaccines.
“This is cause for concern but not alarm,” the federal scientist said of the arrival of the variant in the United States, noting that there is no evidence it causes more severe infection. But the scientist added that the United Kingdom variant, as well as one spreading rapidly in South Africa, “appear to be more transmissible, meaning they can move rapidly through a population of people. And this is one more reason to do everything you can to prevent infection and its spread.”
Officials in the United States have been signaling since last week that the variant was likely already present, but simply undetected.
“I’m not surprised,” Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said Tuesday. “I think we have to keep an eye on it, and we have to take it seriously. We obviously take any kind of mutation that might have a functional significance seriously. But I don’t think we know enough about it to make any definitive statements, except to follow it carefully and study it carefully.”
The variant has a higher attack rate, according to the UK report, which bolsters the hypothesis that the variant has outcompeted other versions of the coronavirus and is now the dominant variant across much of the United Kingdom. Among people known to have been exposed to someone already infected with the variant, 15.1 percent became infected. People exposed to someone infected with the non-variant version had a 9.8 percent infection rate.
That difference suggests the variant is more transmissible, though the health agency said more investigation is needed to bolster the hypothesis.
The working theory among many scientists is that the increased transmissibility of the variant, known as B.1.1.7, is driven by mutations that have altered the spike protein on the surface of the virus. The variant has 17 mutations — eight of which alter the spike protein
Precisely how those changes are leading to more infections is unknown. The virus may be binding more easily to receptor cells in the human body, or replicating more easily and driving higher viral loads, enhancing viral shedding by someone who is infected. Another possibility is that people are shedding virus for a longer period, upping the chances of passing along the virus.
“Preliminary evidence suggests that the new variant does not cause more severe disease or increased mortality,”said Susan Hopkins, a senior medical adviser to Public Health England, in a statement released Tuesday.
The newly published data echo the findings in a separate study published last week, based on modeling and hospitalization data — and not yet peer-reviewed — that estimated that the variant is 56 percent more transmissible but doesn’t appear to alter the lethality of the virus..
“The good news is that B117 does not seem to cause much more severe disease, and there’s no evidence that it is managing to evade the immune system, which means vaccines are expected to protect against it,” William Hanage, an epidemiologists at the Harvard T. H. Chan School of Public Health, said Tuesday after reviewing the new report. “The bad news is that B117 does appear to be much more transmissible.”
Research findings on coronavirus variants have been at times ambiguous, and scientists stress that they are still trying to tweeze reliable signals from noisy data. Several false alarms have been sounded about virus mutations in the past. A major challenge is discerning whether a virus variant is spreading rapidly because it has a competitive advantage based on its genetic and structural differences, or is simply lucky, having arrived early to a location or leveraged a few superspreader events to gain dominance.
But with the United Kingdom seeing a severe winter surge of infections, public officials are taking no chances and have effectively locked down southern England, including London. Other countries have banned travelers from the United Kingdom.
The United States, despite having the world’s highest number of documented infections, has a weak track record in publishing genomic sequences, the process that enables researchers to track changes in the virus. Most sequences have been published by academic or private research institutions. By contrast, the United Kingdom has a national health system with a robust surveillance system.
“The U.K. made the decision in the spring to do this. The U.S. has sequencing equipment and infrastructure. As with many things in this pandemic, it was not executed the way it should have been,” said Neville Sanjana, a geneticist at New York University.
“The UK is being punished for having information. No other country has any idea what viruses they have,” said Jeremy Luban, a virologist at the University of Massachusetts Medical School. “ The lack of virus sequencing and case tracking in the USA is a scandal.”
The novel coronavirus, SARS-C0V-2, mutates at a slow rate, and scientists do not think the genetic changes seen in the variant so far are sufficient to allow it to elude the vaccines now being administered to millions of people in many countries. But the coronavirus is a moving target and these mutations require surveillance.
Even without the mutations, the coronavirus has been and will continue to be highly contagious.
“The best way to stop infection, whatever the variant, is to stick to the rules — wash our hands, wear a face covering and keep our distance from others,” Hopkins said.
The new variant is being compared to a globe-saturating strain of the virus — known in shorthand as the “wild type” of the coronavirus — that is itself a mutant version of what originally was identified in Wuhan, China, a year ago.
All viruses mutate randomly and over time some of those mutations appear to confer some kind of advantage to the virus as in adapts to the human species. No mutation has been shown to make the virus more likely to be dreadly or cause a more severe illness.
But it appears that the coronavirus learned to spread more easily early in the pandemic. Every genomic sequence of newly infected people shows that the virus with a mutation known as D614G, which also affects the structure of the virus’s spike protein.
Francois Balloux, who directs the Genetics Institute at University College London, predicted on Twitter that it would take two more weeks of accumulating data to determine whether this new variant was indeed more transmissible.
Previously, Balloux and his colleagues combed through genome sequences, looking for evidence that common variants had increased transmissibility.
“We don’t see much,” he said, referring to a report published in Nature in November that found no signs of mutations that helped the virus to spread more easily. But he said that he “wouldn’t underestimate the evolutionary potential of SARS-Cov-2.”
by ti-amieWisconsin health-care worker ‘intentionally’ spoiled more than 500 coronavirus vaccine doses, hospital says
By
Andrea Salcedo and
Isaac Stanley-Becker
Dec. 31, 2020 at 3:15 p.m. EST
An employee at a hospital outside Milwaukee deliberately spoiled more than 500 doses of coronavirus vaccine by removing 57 vials from a pharmacy refrigerator, hospital officials announced Wednesday, as local police said they were investigating the incident with the help of federal authorities.
Initiating an internal review on Monday, hospital officials said they were initially “led to believe” the incident was caused by “inadvertent human error.” The vials were removed Friday and most were discarded Saturday, with only a few still safe to administer at Aurora Medical Center in Grafton, Wis., according to an earlier statement from the health system. Each vial has enough for 10 vaccinations but can sit at room temperature for only 12 hours.
Two days later, the employee acknowledged having “intentionally removed the vaccine from refrigeration,” the system, Aurora Health Care, said in a statement late Wednesday.
The employee, who has not been identified, was fired, Aurora Health said. Its statement did not address the worker’s motive but said “appropriate authorities” were promptly notified.
Wednesday night, police in Grafton, a village of about 12,000 that lies 20 miles north of Milwaukee, said they were investigating along with the FBI and the Food and Drug Administration. In a statement, the local police department said it had learned of the incident from security services at Aurora Health Care’s corporate office in Milwaukee. The system serves eastern Wisconsin and northern Illinois, and includes 15 hospitals and more than 150 clinics, according to its website.
Leonard Peace, an FBI spokesman in Milwaukee, would not comment on the Bureau’s involvement but said of the episode, “We’re aware of it.” The FDA was also aware, said a spokeswoman, Stephanie Caccomo, who similarly declined to address the existence of an investigation. She directed questions to the hospital.
Jeff Bahr, president of Aurora Health Care Medical Group, was scheduled to provide an update on the incident Thursday afternoon.
The tampering will delay inoculation for hundreds of people, Aurora Health officials said, in a state where 3,170 new cases were reported and 40 people died Wednesday of covid-19, the disease caused by the coronavirus, according to The Washington Post’s coronavirus tracker.
“We are more than disappointed that this individual’s actions will result in a delay of more than 500 people receiving the vaccine,” the health system said in a statement.
Tara C. Smith, an epidemiologist at Kent State University and an authority on antipathy toward vaccines, said the incident will prompt medical providers to reassess who has access to the shots, even among their own employees.
“Hopefully, this is a one-off, but I’m sure places will now have to think about whether those handling the vaccines are trusted, in addition to making sure supplies are under camera surveillance,” she said.
Security has been paramount in state planning, officials say. When Wisconsin began receiving vaccine shipments earlier this month, the health department did not disclose the eight regional hubs receiving the bulk of the materials.
Julie Willems Van Dijk, deputy secretary of Wisconsin’s Department of Health Services, said at a Dec. 14 news conference, “This is precious vaccine. We do not want to create any security risks.” She said the state had consulted with the Department of Homeland Security on the plans.
On Thursday, Health Secretary-designee Andrea Palm said her department has worked with Aurora Health officials as they “investigated the situation, reviewed their processes and implemented improvements.”
“It is disappointing that any covid-19 vaccine was wasted in Wisconsin,” she added in a statement to The Washington Post.
The Wisconsin incident comes as states continue to grapple with a bumpy rollout of the first doses of the Moderna and Pfizer-BioNTech vaccines, which were approved less than a month ago and prioritized for health-care workers and residents and staff of long-term care facilities. So far, distribution has lagged well behind federal projections, raising doubts about whether the outgoing administration will meet its already revised goal of 20 million vaccines distributed by the end of the year.
As of Wednesday, the Centers for Disease Control and Prevention said 12.4 million doses of the vaccine had been distributed across the United States, but only 2.6 million of those had been administered. (This means that just 1 in 125 Americans have received the first dose of the vaccine.) Trump administration officials have said these numbers lag behind the actual pace of vaccination, which they also vowed would accelerate starting next week.
The Moderna and Pfizer-BioNTech vaccines, the first two regimens to gain regulatory approval for emergency use, are two-shot protocols with intricate logistical requirements. Moderna’s vaccine doesn’t require subarctic temperatures, as does the Pfizer product, but it does need to be kept cold. It can be stored at freezer temperatures for six months, the company says, and kept at regular refrigerated conditions for 30 days. It can be maintained at room temperature for only 12 hours, though, and can’t be refrozen once thawed.
Complex storage requirements are among the reasons state officials are imploring providers to administer vaccine quickly once it is received. Wisconsin Gov. Tony Evers (D), taking to Twitter last week to celebrate the start of shipments of Moderna’s vaccine, said it marked “another step forward in fighting this pandemic.”
In its original statement on Monday, Aurora Health said it had successfully vaccinated about 17,000 people over the previous 12 days. Its initial review, it said, had found that the 57 vials were simply left out overnight by the employee after “temporarily being removed to access other items.”
The health system apologized, saying, “We are clearly disappointed and regret this happened.”
by ti-amieWisconsin hospital worker arrested for spoiled vaccine doses UPDATED
Last updated today at 4:28 pm
December 31, 2020
MADISON, Wis. (AP) -- Authorities have arrested a suburban Milwaukee pharmacist suspected of deliberately ruining 570 of doses of coronavirus vaccine by removing it from refrigeration for two nights.
The Grafton Police Department said the former Advocate Aurora Health pharmacist was arrested on suspicion of reckless endangerment, adulterating a prescription drug and criminal damage to property. All charges are felonies.
The department said in a news release Thursday that he is being held in Ozaukee County jail.
Police did not identify the pharmacist, saying he has not yet been formally charged.
Advocate Aurora Health Care Chief Medical Group Officer Jeff Bahr says the pharmacist deliberately removed 57 vials of the Moderna vaccine from refrigeration overnight on Dec. 24, returned them, then left them out again on the night of Dec. 25.
According to a press release from the Grafton Police Department, the pharmacist "knew the spoiled vaccinations would be useless and that people who received the vaccinations would think they had been vaccinated against the virus when in fact they were not."
That same press release indicates the monetary loss of the spoiled doses is between $8,000 and $11,000.
by ponchi101 He loses his license, right? To (expletive) begin with.
(And please, who did he vote for. Just to check if the stereotype is accurate).
by ti-amie
by ti-amie Meanwhile...
Sam Coates Sky @SamCoatesSky
A No10 spokesman said: ‘The spread of the new variant of COVID-19 has led to rapidly escalating case numbers across the country
‘The PM is clear that further steps must now be taken to arrest this rise and to protect the NHS and save lives.’
‘He will set those out this evening’
by ponchi101 My local update.
large sections of Bogota go back into quarantine starting tomorrow. My county is one. ICU beds occupancy are at 95%. The general idea is that the local Xmas tradition called "Novenas" (the Nines), in which people gather at night for religious ceremonies during the 9 days prior to Xmas led to the increase in cases. That, plus the "regular" partying. The major of Bogota declared a prohibition of alcohol sales starting on Dec 23rd through 27, prompting large numbers of people to stock up and celebrate parties at their houses.
The GOV will implement a web-based and app-based system to determine the timing for people to get the vaccine.
So, sort of back to April 2020. 2021, feelings-wise, has not rung in.
by ti-amieNew Variant Detected in New York Amid Growing Crisis Over Vaccine Rollout
The sluggish pace of vaccinations has been particularly striking in New York City, the onetime epicenter of the pandemic.
By Jesse McKinley, Luis Ferré-Sadurní and Emma G. Fitzsimmons
Jan. 4, 2021
Updated 4:28 p.m. ET
ALBANY, N.Y. — New York, the onetime center of the pandemic, faced a growing crisis on Monday over the lagging pace of coronavirus vaccinations, as deaths continue to rise in the second wave and Gov. Andrew M. Cuomo came under mounting pressure to overhaul the process.
The concern over vaccinations came as the first case of a more contagious variant of the virus was confirmed in the state. The 60-year-old man who tested positive was recovering, but Mr. Cuomo was urging rapid testing for anyone who might have come into contact with him at the jewelry store in Saratoga Springs where he worked.
The discovery of the new variant was just the latest complication for state health officials, who are overseeing a planned inoculation of some 20 million state residents.
The small number of vaccine recipients is particularly striking in New York City, where roughly 110,000 people — in a city of more than eight million — have received the first of two doses necessary to help prevent serious cases of the disease. That is about a quarter of the total number received by the city.
Mayor Bill de Blasio called on the Cuomo administration to allow the city to inoculate a broad array of essential workers and New Yorkers who are 75 and older. The vaccinations had been limited to some health care workers and those living and working at nursing homes; on Monday, many more health care providers were made eligible for the vaccine.
“There’s lots more we can do if we have both those categories approved,” Mr. de Blasio said at a news conference on Monday.
Shortly after the mayor spoke, Mr. Cuomo rejected any notion that his administration was at fault, asserting that the problem was a local issue, and urging Mr. de Blasio and other local leaders who oversee public hospital systems to take “personal responsibility” for their performance.
“They have to move the vaccine,” the governor said in Albany. “And they have to move the vaccine faster.”
The governor threatened to fine hospitals up to $100,000 — and redirect future vaccines to other hospitals — if they did not rapidly increase the pace of vaccination. He also named the slower-performing hospital systems in a slide show, something he said he did not do “to embarrass” them but to make sure they are “held accountable.”
“We want those vaccines in people’s arms,” Mr. Cuomo said, adding, “This is a very serious public health issue.”
But efforts to speed up vaccinations may prove to be at odds with the strenuous task of making sure to prioritize the right people.
In one possible example, the state has advised clinics and other facilities to rank each employee using a matrix that takes into account age, comorbidities, occupation and the section of the facility where the person works.
Mr. Cuomo said he would propose legislation that would impose criminal charges for facilities or health care providers that did not follow guidelines on who is eligible for the vaccine. “This vaccine can be like gold to some people,” the governor said.
Asked about whether his threat of fines for hospitals — already warned that they will face penalties if they break state mandates on who gets the vaccine — could be slowing down the process, Mr. Cuomo said no.
“I want to get needles in the arms and I want to get that done quickly as possible,” he said. “If there are some hospitals that are better at doing that, then they should be doing that.”
The governor estimated that about 300,000 people had received the vaccine in New York, but offered no single reason for the slow pace of vaccination. “There is no one cause,” he said, noting that he had spoken to dozens of hospitals about the issue.
He did suggest, however, that “management capacity and efficiency” were causing problems, saying there was a lack of “urgency” at some hospitals.
“It’s bureaucracy,” he said.
Mr. de Blasio acknowledged that the city’s rollout had been slow, blaming the logistical challenges of dealing with a new vaccine, and said the city took a cautious approach as it laid the groundwork for more widespread distribution.
“Now it’s time to sprint,” Mr. de Blasio said.
Avery Cohen, a spokeswoman for the mayor, said that Mr. de Blasio has stressed to the city’s public hospital system — NYC Health and Hospitals — that they should “get as many vaccines in arms as possible.” But she questioned the logic of Mr. Cuomo’s pledge to cut off hospitals that are not fast enough for his taste.
“Threatening to revoke the privilege of vaccination from the city’s public hospital system is punitive and unnecessary,” Ms. Cohen said.
Other elected officials in the city have been urging a more aggressive plan of attack, with round-the-clock operations. On Monday, the mayor seemed to agree, promising three new “vaccination hubs” would open on Sunday in Brooklyn, Queens and the Bronx, and pledging to offer shots of the vaccine seven days a week and 24 hours a day when possible. The city also hoped to double the number of locations offering vaccination to 250 sites by the end of the month.
The mayor repeated his pledge to reach a rate of 400,000 doses per week by the end of the month, with a goal of one million doses — safeguarding at least a half-million residents — by February.
Mr. de Blasio and Mr. Cuomo have long had a difficult relationship, but they have tried to show a united front in recent weeks as the state and city face a second wave of the virus. Mr. de Blasio was careful on Monday not to directly criticize Mr. Cuomo, but called on “the state” several times to alter its approach.
The mayor showed no such restraint when it came to the federal government, suggesting in a slide show that the “feds” needed to “PICK UP THE PACE” on distributing the vaccine.
Mr. Cuomo, a third-term Democrat, has touted his own response to the coronavirus crisis and the state’s vaccination plan in recent months, though statistics continue to bear troubling news: On Monday, more than 8,200 residents in the state were hospitalized with the coronavirus, levels not seen since early May, as deaths have topped 100 a day for several weeks. On Monday, the governor reported 170 deaths, the highest daily count since the dark days of the spring.
Over the past week, the state has seen more than 10,000 new cases per day, as the statewide rate of positive test results has also jumped alarmingly, even before an expected increase tied to holiday travel and gatherings. New York continues to be the hardest hit state in the nation, with more than 38,000 deaths.
Mr. Cuomo said on Monday that “there have been issues with the delivery of the vaccine,” laying that blame with federal officials whom he has regularly criticized for their handling of the crisis.
He said that the state would expedite delivery and injection of the vaccine to nursing homes — where thousands of New Yorkers have died — aiming to get 85 percent of residents vaccinated by the end of this week.
“The federal program has not worked as quickly as we would have liked,” Mr. Cuomo said.
Jesse McKinley is the Albany bureau chief. He was previously the San Francisco bureau chief, and a theater columnist and Broadway reporter for the Culture Desk. @jessemckinley
Luis Ferré-Sadurní covers New York State politics in Albany. He joined The Times in 2017 and previously wrote about housing for the Metro desk. He is originally from San Juan, Puerto Rico. @luisferre
Emma G. Fitzsimmons is the City Hall bureau chief, covering politics in New York City. She previously covered the transit beat and breaking news. @emmagf
by ti-amie To be fair no one gets along with Andrew and Bill isn't a walk in the park either so thatconversation, while often repeated, should be put aside.
by ponchi101 This happens so often, or at least in my industry. You set up so many regulations that eventually the system does not move.
If you are:
Over 60, or
Work at a hospital, or
Have some underlying condition
You get the vaccine. Make it simple.
by ti-amieThird national lockdown announced in England amid coronavirus surge driven by variant strain
By
Karla Adam,
Jennifer Hassan and
Ben Guarino
Jan. 4, 2021 at 6:06 p.m. EST
LONDON — Prime Minister Boris Johnson on Monday ordered a third national lockdown for England amid a surging coronavirus outbreak driven by a U.K. variant that appears to be more contagious and may have greater implications for children.
In a televised address to the nation on Monday evening, Johnson said the new variant was 50 percent to 70 percent more transmissible, spreading at a rate he called “frustrating and alarming.”
“With most of the country already under extreme measures, it’s clear that we need to do more together to bring this new variant under control while our vaccines are rolled out,” he said. “In England, we must, therefore, go into a national lockdown which is tough enough to contain this variant.”
Speaking on a visit to a hospital in London earlier in the day, Johnson said, “We have a new variant that is requiring extra-special vigilance.” The variant has spread to more than 30 countries.
The Monday announcement comes after a national lockdown in March and then a four-week one that began in November.
The government had been facing growing calls to impose further restrictions as coronavirus cases continue to rocket. On Monday, Britain recorded 58,784 new daily cases, the highest figure recorded here during the pandemic.
“Let me be candid with you: This virus is out of control,” London Mayor Sadiq Khan told LBC Radio earlier Monday. “We have more patients in hospital in London now with covid than anytime in March, April and May during the peak. Plus, we have the additional non-covid winter pressures.”
Britain has recorded more than 50,000 daily cases for seven days. The number of patients in London hospitals has more than doubled over the past two weeks. At least one London hospital has had to postpone urgent cancer surgeries this week because it is overwhelmed with covid patients.
Under the new lockdown, everyone in England will be asked to stay at home except in special circumstances. Schools and universities will close for in-class learning with immediate effect.
In his televised address, Johnson said, “I want to stress that the problem is not that schools are unsafe for children — children are still very unlikely to be severely affected by even the new variant of covid.
“The problem is that schools may nonetheless act as vectors for transmission, causing the virus to spread between households.”
The more contagious variant, which has spread to dozens of countries and has been detected in four U.S. states, may have had a disproportionate effect on people under 20 in the United Kingdom, according to a new report that has not gone through scientific peer-review.
When the study authors evaluated patients by age, they found a slightly higher proportion of new variant vs. non-variant cases in people younger than 20. The researchers’ observations cannot explain why. The difference they detected may have been circumstantial.
The fresh lockdown comes as Britain began rolling out the Oxford-AstraZeneca vaccine. Early Monday morning, Brian Pinker, 82, became the first person in the world to get a shot of the vaccine outside of clinical trials. The former maintenance manager rolled up his sleeve at a hospital in Oxford, where the vaccine was developed. “The vaccine means everything to me. To my mind, it’s the only way of getting back to normal life,” Pinker said afterward.
The government hopes that the Oxford-AstraZeneca vaccine, which is cheaper to produce and easier to transport than other vaccines that are being administered, will be a “game changer.” Nursing home residents, health-care workers and those over 80 are at the front of the line. Britain recently shifted its vaccine strategy so that it could inject as many people as possible, as quickly as possible, by allowing for 12 weeks between the first and second dose instead of the usual 21 days.
But inoculating an entire nation will take months, and the growing number of cases and hospitalizations has sparked alarm in Britain.
Scotland’s semiautonomous government also announced a new lockdown Monday for at least the rest of the month. Nicola Sturgeon, the first minister of Scotland, told the Scottish Parliament that starting Tuesday, there would be “a legal requirement to stay at home except for essential purposes. This is similar to the lockdown of March last year.”
She also said that students would move to remote learning for the rest of the month.
Sturgeon said that the “overall level of community transmission is simply too high” to keep schools open and that there was still “significant uncertainty about the impact of the new variant on transmission amongst young people.”
In England, schools will move to remote learning from Tuesday.
More than three-quarters of England was already at “Tier 4,” the highest level of restrictions.
Health Secretary Matt Hancock told the television program “Good Morning Britain” on Monday that Britain’s temporary “Nightingale hospitals,” built in weeks last year, were on “standby if needed.”
The National Health Service said in a statement that it was “working hard” to ready London’s flagship Nightingale hospital to treat patients “if necessary.” The London center will be used to rehabilitate people who are recovering from an emergency stay in a hospital and will not be used to treat patients who have covid-19, the statement said.
British media outlets have reported in recent days that the majority of the seven Nightingale hospitals had been dismantled or were not being used as cases began to climb in the country again — prompting many to question why.
ICU nurse Dave Carr told “Good Morning Britain” on Monday that the rise in infections was “breaking” exhausted NHS staff working in intensive care units in London that are full with patients, who are forced to share ventilators.
“The admissions keep coming in,” Carr said, adding that all available staff are already working at NHS hospitals and finding staff for the Nightingale facilities would be difficult. “It’s absolutely appalling planning,” he said of the government’s handling of the crisis.
Former health secretary Jeremy Hunt was among those on Monday urging the government to “close schools, borders, and ban all household mixing RIGHT AWAY.”
“To those arguing winter is always like this in the NHS: you are wrong,” he tweeted. “I faced four serious winter crises as Health Sec and the situation now is off-the-scale worse than any of those.”
by ti-amiePharmacist Accused of Tampering With Vaccine Was Conspiracy Theorist, Police Say
The police say a Wisconsin pharmacist believed the Moderna vaccine would harm people and tried to sabotage the effort to vaccinate frontline workers.
By Shaila Dewan and Kay Nolan
Jan. 4, 2021
Updated 6:33 p.m. ET
Police said Steven Brandenburg had twice removed a box of vials of the Moderna vaccine from the refrigerator for periods of 12 hours, rendering them “useless.”
Credit...Ozaukee County Sheriff's Office, via Associated Press
A pharmacist who was arrested on charges that he intentionally sabotaged more than 500 doses of the Covid-19 vaccine at a Wisconsin hospital was “an admitted conspiracy theorist” who believed the vaccine could harm people and “change their DNA,” according to the police in Grafton, Wis., where the man was employed.
The police said Steven Brandenburg, 46, who worked the night shift at the Aurora Medical Center in Grafton, Wis., had twice removed a box of vials of the Moderna vaccine from the refrigerator for periods of 12 hours, rendering them “useless.”
“Brandenburg admitted to doing this intentionally, knowing that it would diminish the effects of the vaccine,” the police said.
The attempt to destroy precious doses of the vaccine came over the holidays as the state worked to administer vaccines quickly to frontline health care workers. As of Saturday, the state had received 159,800 doses of vaccines and had administered 64,657, according to the Centers for Disease Control and Prevention. Although the Moderna product is sometimes described as a “genetic” vaccine, it does not alter a person’s genes in any way.
The vials, which contained 570 doses of vaccine and which prosecutors said were worth between $8,000 and $12,000, were discovered sitting out on Dec. 26. Five days later, Mr. Brandenburg was arrested on felony charges of reckless endangerment and property damage, though prosecutors on Monday said the charges could be dropped to a single misdemeanor if the vials, which have yet to be tested, are still usable.
The prosecutor, Adam Gerol, said that Mr. Brandenburg was “pretty cooperative and admitted to everything he’d done,” and that “he expressed that he was under great stress because of marital problems.” He said that according to co-workers, Mr. Brandenburg had brought a gun to work on two prior occasions.
Last month Mr. Brandenburg told his wife, who is in the process of divorcing him, that “the world is crashing down around us,” according to a motion she filed last week asking for sole custody of the couple’s two daughters, 4 and 6, after she learned he was under investigation in the incident at the hospital. She said she feared his reaction if he lost his job.
In her motion, Gretchen Brandenburg said that on Dec. 6, her husband picked up the children and dropped off a water purifier, a large bucket of powdered milk and two 30-day emergency buckets of food.
“He told me that if I didn’t understand by now that he is right and that the world is crashing down around us, I am in serious denial,” she said in an affidavit. “He continued to say that the government is planning cyberattacks and plans to shut down the power grid.”
She asked that his time with their children be supervised, saying he had made alarming remarks. The six-year-old had quoted him as saying, “This is not our home; heaven is our home,” and “All the bad angels and the devil are going to burn in the lake of fire forever,” she wrote.
“I was so concerned about my safety and the safety of our children that I left town for a period of time,” she wrote.
The Brandenburgs married in 2012, and Ms. Brandenburg filed for divorce last June. At a hearing in July, her lawyer testified that his client feared Mr. Brandenburg’s “temper” and said the parties have “vastly different views regarding parenting and views of the world.”
“My understanding is that the respondent is more aligned with the feeling of conspiracy theories,” the lawyer, Brian Herro, said. “He has theories about Covid-19. He believes the end of the world is coming. So my client would like him to be out.”
Mr. Brandenburg’s criminal defense lawyer, Jason Baltz, declined to comment. Mr. Herro did not immediately respond to a request for comment.
In an order signed Monday, the family court granted temporary sole custody to Ms. Brandenburg, finding that the children were in “imminent danger of physical or emotional harm.”
But the criminal court granted Mr. Brandenburg release on a promise to pay $10,000 if he did not show up for his next hearing, on Jan. 19. He was ordered to surrender any firearms; the prosecutor said the police had already confiscated some of his guns.
The Moderna vaccine must be kept frozen or refrigerated until it is used, though it does not require subarctic temperatures like the Pfizer vaccine does. The hospital has said that 57 people received injections of the compromised vaccine, but that Moderna had reassured officials that they would not harm the individuals who received them.
Hospital officials at first believed that the vials were left out inadvertently, but upon further investigation determined that the act had been intentional. They said the pharmacist was no longer employed.
In a July divorce hearing dealing with multiple issues, including whether Mr. Brandenburg should be required to move out of the family home, he talked about the pressure of his job, working from 9 p.m. to 7 a.m. “It’s not easy, especially with all of the other stress going on, in order to get enough sleep to function for work,” he said. “And if I make mistakes at work — I’m a hospital pharmacist at Grafton, right? — I’m responsible for life and death issues.”
The incident raised new fears of inadequate security for the vaccine. Last Thursday, in a video call with reporters, Jeff Bahr, the president of Aurora Health Care Medical Group, defended the hospital system’s protocols. “It’s become clear that this was a situation involving a bad actor, as opposed to a bad process,” he said.
The scarcity of supply has led some officials to store the vials at undisclosed locations, install security cameras and tracking systems or restrict access. Early in December, Interpol warned nations to prepare for attempts by organized crime rings to target vaccine supply chains. But most of the attention has focused on attempts to steal or divert the vaccine, not tamper with it.
Wisconsin experienced a surge of coronavirus cases in the fall, and at times has been one of the hardest-hit states in the nation relative to its population. Transmission has since slowed a bit, but the state is still reporting about 43 new cases a day for every 100,000 people. At least 5,264 Wisconsin residents have died.
Shaila Dewan is a national reporter and editor covering criminal justice issues including prosecution, policing and incarceration. @shailadewan
by Deuce The problem isn't so much the virus... the main problem, by far, is human beings.
Not just 'extremists' like the conspiracy theory pharmacist and those of his ilk, but also the people who somehow think that they can get away with not wearing masks or not being physically distant from others. We all know by now what to do and what to not do to greatly minimize the chances of contracting the virus. We've been hearing it for 9 months straight, over and over. But the lack of accurate foresight - and/or lack of concern for others - is incredible. These people - and there are millions of them, unfortunately - feel that, because the statistics show that they'll probably survive the virus, don't take proper precautions. They either don't think about or simply don't care about the fact that if they contract the virus, even if they are minimally affected by it themselves, they can pass it on to others who could die from it.
Yeah - the problem is definitely the human animal.
by ponchi101 Sure, but in this particular case, the problem with the human animal in this news is that this is more animal than human.
I wrote about it. This thing has defeated us. But, if on top of that, we have this kind of people sabotaging what is the only way to get rid of this virus, we can reach newer levels of despair. Which is outstanding after the four years we (America) has been through.
by ponchi101 Local update:
cars going doing the street with a PSA reminding people that the borough is under quarantine.
And therefore, (expletive) your rights. This is bigger than that.
(Which I agree).
by Suliso It's very hard to find any sustainable solution on this, but clearly assholes like the one above are not improving odds.
by ti-amie Kurt "Masks Save Lives" Eichenwald @kurteichenwald
Doctor in Illinois: A alarming number of teenagers are turning up at the hospital with brain swelling and heart damage during/post COVID infection. Also a huge spike in people showing up with new autoimmune diseases including type 1 diabetes likely incident to pancreatic damage.
by dryrunguy I apologize for being remiss in posting these of late. Here's the Situation Report for January 4, 2021.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 84.23 million cases and 1.84 million deaths as of 4:00am EST on January 5. Over the past 2 weeks, the WHO reported decreased global weekly incidence and mortality compared to the week of December 14, potentially a result of reporting delays over the 2 holiday weekends. The global cumulative incidence surpassed 80 million cases on December 29. From the first reported COVID-19 case, it took 177 days to reach 10 million cases. From there:
10 to 20 million- 44 days
20 to 30 million- 37 days
30 to 40 million- 31 days
40 to 50 million- 21 days
50 to 60 million- 17 days
60 to 70 million- 17 days
70 to 80 million- 16 days
The global cumulative mortality surpassed 1.75 million deaths on December 27. From the first reported death, it took 115 days to reach 250,000 deaths. From there:
250k to 500k- 56 days
500k to 750k- 46 days
750k to 1 million- 45 days
1 to 1.25 million- 40 days
1.25 to 1.5 million- 26 days
1.5 to 1.75 million- 23 days
On December 26, the US surpassed 330,000 cumulative COVID-19 deaths, which equates to approximately 1 death for every 1,000 people nationwide. The US is not the first country to reach this milestone, but it is certainly the largest in terms of population. To date, only 18 countries have reported per capita cumulative mortality greater than 1 death per 1,000 population. All but 2 of these countries are located in Europe, with the exceptions being Peru (1.15) and the US (1.07). More than half of these countries have populations less than 10 million, including 4 with fewer than 1 million people. San Marino—with a population of fewer than 34,000—is #1 globally, with 1.83 deaths per 1,000 population. Notably, Belgium (population 11.6 million) is close behind at 1.70. Slovenia is #3 with 1.37 deaths per million.
The trends in cumulative incidence among the European countries are very similar over the course of the pandemic, whereas Peru and the US exhibit different trajectories. In Europe, countries that were severely affected early in the pandemic have steep initial curves, which began to level off in May. The cumulative mortality curves for most of the European countries, regardless of whether they were severely affected during Europe’s “first wave,” were relatively flat over the summer before sharp increases starting in September-October, corresponding to Europe’s second wave. In contrast, Peru’s cumulative mortality curve increased steadily through approximately August, at the height of South America’s first wave, and has tapered off since that time. The United States’ initial sharp increase in March-April, during the initial COVID-19 surge, was less pronounced than many European countries; however, when Europe brought its COVID-19 epidemic over the summer under control, COVID-19 mortality in the US continued to grow steadily during its summer resurgence. US mortality rate then increased again in November, corresponding to the autumn/winter surge.
UNITED STATES
The US CDC reported 20.56 million total cases and 350,664 deaths. The US reported a new single-day record incidence of 284,554 new cases on January 3, becoming the first country to report more than 250,000 new cases in a single day. The US surpassed 20 million cumulative cases on January 2. From the first case reported in the US, it took 200 days to reach 5 million cases. From there:
5 million to 10 million- 92 days
10 million to 15 million- 29 days
15 million to 20 million- 24 days
The US surpassed 325,000 cumulative deaths on December 23 and 350,000 deaths on January 4. The 9 days to increase from 300,000 to 325,000 deaths matched the rate at the peak of the initial surge in March. Notably, the 12 days between 325,000 and 350,000 included 2 major holiday weekends, which likely delayed reporting to some extent. From the first US death, it took 55 days to reach 50,000 deaths. From there:
50k to 100k- 33 days
100k to 150k- 63 days
150k to 200k- 55 days
200k to 250k- 58 days
250k to 300k- 25 days
300k to 350k- 20 days
As a reminder, it may be difficult to track national-level epidemiological trends in the US over the coming weeks. Reporting delays over the Christmas and New Year’s holiday weekends, and associated catch-up reporting, could obscure epidemiological trends, including the effects of holiday travel and gatherings as far back as Thanksgiving.
While many of the metrics we track vary considerably over holiday weekends, hospitalizations tend to remain relatively consistent. Analysis reported by the COVID Tracking Project shows a 4.6% increase in hospitalizations for the last week of 2020, compared to the previous week. The number of nationwide hospitalizations does appear to be tapering off to some degree, but the US continues to set new records, now more than double the number of hospitalized COVID-19 patients reported at the height of the previous 2 peaks. Hospitalization trends vary by region, as the US epidemic shifts away from the Midwest, which was most severely affected in the earlier part of the autumn/winter surge. States in the South and West regions continue to report increasing hospitalizations, including new records in the South. Hospitalizations in the Midwest peaked in late November/early December and are now steadily decreasing, and Northeastern states appear to be approaching a second peak. While the raw totals vary widely by region, the per capita hospitalizations are actually relatively even, with all 4 regions falling between 310 and 410 hospitalizations per million population. In total, 6 states are reporting more than 500 hospitalizations per million population: Alabama (628), Arizona (659), California (560), Georgia (530), Nevada (632), and Tennessee (508). Only 2 states, Hawai’i (60) and Vermont (66), and Guam (68) are reporting fewer than 100 hospitalizations per million.
The Johns Hopkins CSSE dashboard reported 20.84 million US cases and 354,263 deaths as of 11:30am EST on January 5.
VACCINE AUTHORIZATIONS Considerable progress has been made over the past several weeks in terms of regulatory agencies authorizing the use of SARS-CoV-2 vaccines, including several new vaccines that had not previously been authorized for use anywhere. Following the US emergency authorization of the Moderna vaccine, Health Canada authorized the Moderna vaccine for use among the public. Canada is the second country to authorize the Moderna vaccine, and this is the second vaccine authorized for use in Canada. Additionally, the WHO issued its first Emergency Use Listing (EUL) for a SARS-CoV-2 vaccine for the Pfizer/BioNTech version. An EUL from the WHO can help expedite regulatory review and authorization in countries around the world, and it “enables UNICEF and the Pan-American Health Organization [PAHO] to procure the vaccine for distribution to countries in need.”
On December 30, the UK became the first country to issue an emergency authorization for the AstraZeneca/Oxford University vaccine, which was developed in the UK. This is the second vaccine authorized for use in the UK. India also authorized the use of the AstraZeneca/Oxford vaccine, which it is manufacturing domestically.
Additionally, India issued an emergency authorization for the vaccine developed by Bharat Biotech, an Indian pharmaceutical company, that appears to still be in the middle of Phase 3 clinical trials. Reportedly, the absence of publicly available Phase 3 trial data for the AstraZeneca/Oxford and Bharat Biotech vaccines and a lack of transparency regarding the conduct of those trials has prompted criticism from health experts in India, following the authorization of the two vaccines.
The European Medicines Agency (EMA) is reportedly assessing the Moderna vaccine for emergency use, but it has not yet finalized its recommendation. Additionally, an EMA official indicated that it could be another month or longer before it can evaluate and authorize the AstraZeneca/Oxford vaccine. A rolling review of the interim Phase 3 clinical trial data is underway, but AstraZeneca still needs to submit its request and provide additional data.
China issued a conditional approval for the vaccine developed by Sinopharm, a state-operated pharmaceutical company. China is not the first country to approve the vaccine, but this appears to be the first official authorization issued by the Chinese government. Egypt also reportedly authorized the use of the Sinopharm vaccine, and vaccination efforts are expected to begin later this month. Millions of doses of China’s Sinovac vaccine recently arrived in Indonesia; however, formal emergency authorization is still needed before vaccination efforts can begin. Unlike the Pfizer/BioNTech and Moderna vaccines, the final Phase 3 clinical trial data have not yet been published publicly for the AstraZeneca/Oxford, Bharat Biotech, and Sinopharm vaccines, and it appears that the Bharat Biotech vaccine is still undergoing Phase 3 trials.
US VACCINATION The rollout of the United States’ SARS-CoV-2 vaccination program has faced a number of challenges. While the federal government is responsible for procuring and distributing the vaccine, public health and healthcare in the US are largely controlled at the state level. According to US CDC data, more than 15 million total doses have been distributed nationwide; however, only 4.5 million (29.5%) have been reported as administered. This total includes 2.5 million doses distributed for use at long-term care facilities (LTCFs), of which only 365,000 (14.4%) have been administered. While distribution to states is relatively balanced nationwide, on a per capita basis, the speed at which states are administering the vaccines varies widely.
Delays in administering vaccines in several states have received significant media coverage. In Florida, for example, images and videos show older adults, many in wheelchairs, waiting in long lines to receive their vaccines, including some who waited outside overnight for the opportunity to be vaccinated. In Florida, local governments are responsible for implementing mass vaccination programs, including mechanisms to schedule appointments and allocate doses to appropriate populations, and differences in their approaches have impacted mass vaccination operations. States also vary in terms of who is eligible for vaccination, including who gets priority among the highest tier groups. In some states, such as New York, healthcare workers in primary care or outpatient settings were not among the initial priority for eligibility, but eligibility was expanded this week to include them. Many health professionals and experts have noted challenges that primary care clinicians are facing in terms of getting vaccinated, particularly considering their risk of exposure to patients with milder symptoms or who are seeking testing. Other states, such as Louisiana, are expanding beyond the federal Tier 1a recommendations to include all adults aged 70 years and older.
In some states, delays in administering the allocated vaccine doses have prompted stern responses from state officials. In Florida, Governor Ron DeSantis threatened to withhold future allotments from hospitals that do not increase the pace of their vaccinations. Similarly, New York Governor Andrew Cuomo indicated that he would hold back future doses and potentially impose substantial fines for hospitals that do not administer their allocated doses by the end of this week. One of the challenges affecting hospitals’ ability to administer their vaccines is opacity in the national allocation and delivery process. States may not know how many doses they will receive until days before the delivery arrives, so governments and hospitals may be unwilling to administer their entire inventory to ensure they have enough on hand to cover the second doses. Until state and local governments and health systems can gain confidence in the delivery volume and timeline, we could continue to observe lower vaccination rates in many locations.
EU VACCINATION European countries began initiating their mass vaccination efforts against SARS-CoV-2 on December 26. As of now, only the Pfizer/BioNTech vaccine is authorized for use in Europe; however, other vaccines are currently under evaluation by the European Medicines Agency (EMA), including ongoing assessments regarding emergency authorization for the Moderna vaccine, which has already been issued an Emergency Use Authorization (EUA) by the US FDA. As of today, EU countries have administered more than 900,000 doses of the vaccine, led by Germany, which has administered the first dose to nearly 317,000 individuals.
ISRAEL VACCINATION Israel appears to be leading all other countries in terms of its mass vaccination program. Since commencing vaccination operations on December 19, Israel has administered more than 1 million doses nationwide, covering more than 10% of its population. For comparison, the US has administered 4.56 million doses; however, on a per capita basis, Israel (14.14 doses per hundred population) is exceeding #2 Bahrain (3.62) by a factor of 4 and the UK (#3; 1.39) and US (#4; 1.38) by a factor of 10. Reportedly, Israel is administering more than 150,000 vaccinations per day. While this pace could enable Israel to cover 100% of its population (9 million) within 2 months, progress on administering the first doses will largely pause from January 10-31 to begin administering second doses. Israel is currently only using the Pfizer vaccine, but it expects to receive its first doses of the Moderna vaccine in March.
UK VACCINATION TIMING In an effort to increase the number of people with some degree of protection against SARS-CoV-2, the UK government announced that it is increasing the time between the first and second dose of SARS-CoV-2 vaccines to 4 months, for both the Pfizer/BioNTech and AstraZeneca vaccines. The policy will be implemented across all 4 UK countries based on advice from the UK’s Joint Committee on Vaccination and Immunisation (JCVI). This decision increases the time before individuals can be fully vaccinated against SARS-CoV-2; however, it allows the UK government to use its available vaccine doses to provide the first dose to more people, which can provide them with a lower degree of protection.
Some health experts, including multiple professional associations in the UK, have expressed opposition and concern about the decision, noting that the vaccines were not necessarily designed to be administered in this manner, and the clinical trials did not explicitly evaluate the degree or duration of protection conferred through partial vaccination. The concerns include a lower degree of protection from a single dose, waning immunity after 21 days, and the potential that partial immunity could contribute to the emergence of vaccine-resistant strains of the virus. The UK’s Chief Medical Officers defended the policy by citing the need to provide protection to as many people as possible, even if it is not the full degree of protection offered by the full vaccination. They argue that the first dose accounts for “the majority of the initial protection” and that the second dose contributes more to the duration of immunity. Notably, Pfizer issued a statement indicating that its clinical trials did not provide data on the level of protection conferred by the first dose beyond 21 days. The US FDA issued a statement yesterday indicating that the US would not follow the UK’s lead and would, instead, continue to administer the second vaccine doses at the “specified intervals,” 3 weeks for the Pfizer/BioNTech vaccine and 4 weeks for the Moderna vaccine.
VACCINE PHASE 3 CLINICAL TRIALS While a small selection of vaccines have gone through clinical trials and are conditionally approved for use, other vaccines are still under investigation and going through the clinical trials process. The vaccine candidate developed by Novavax recently entered Phase 3 clinical trials. The participants will be grouped into 2 cohorts, one aged 18-64 years and the other for individuals aged 65 years and older. The older cohort will form at least 25% of the intended 30,000 trial participants in the US and Mexico. The trial also aims for diversity among the participants, emphasizing the recruitment of racial and ethnic minorities that have been more severely affected by the pandemic, including Black, Latino/x, and Native American communities. The Novavax vaccine is a protein subunit vaccine and requires 2 doses administered 21 days apart.
The Kazakh Research Institute for Biological Safety Problems (RIBSP) also recently initiated Phase 3 clinical trials for its candidate vaccine, an inactivated vaccine that is also delivered in 2 doses administered 21 days apart. The Phase 3 trials will begin with 3,000 participants, but RIBSP is already scaling up production of the vaccine. According to information published by the US National Institutes of Health, the Phase 3 trials are expected to include only 3,000 participants (2,400 in the treatment arm), which is much smaller than the Phase 3 trials for other SARS-CoV-2 vaccine candidates. Additionally, a dedicated production facility is expected to be commissioned in March, which will reportedly be capable of manufacturing 60 million doses per year. Vaccinations could begin as early as March, but like other vaccines, this is contingent on demonstrating safety and efficacy in larger Phase 3 trials and obtaining the necessary regulatory authorization. Additionally, the candidate developed by India’s Zydus Cadila initiated Phase 3 clinical trials, which are expected to include 30,000 participants.
The results of the Phase 3 clinical trials for the Moderna vaccine were recently published in the New England Journal of Medicine. These data have already been published publicly, but they have now completed the peer review process. The Beijing Biological Products Institute has also announced preliminary Phase 3 clinical trial results for the Sinopharm candidate vaccine. According to the press release, the Sinopharm vaccine generated neutralizing antibody response in 99.52% of vaccines and demonstrated 79.34% efficacy. This is slightly lower than the 86% efficacy reported for the vaccine in an earlier trial in the United Arab Emirates, and no additional data were included in the statement.
OTHER VACCINATION NEWS Some early vaccine recipients reported allergic reactions after receiving the vaccine, but these types of reactions are not unique to the new SARS-CoV-2 vaccines. Four (4) vaccine recipients in Germany were reportedly admitted to the hospital after accidentally receiving 5 times the recommended dose for the Pfizer/BioNTech vaccine. The increased dose was accidentally administered to 8 individuals, and 4 were hospitalized for monitoring after experiencing flu-like symptoms. A pharmacist in Milwaukee, Wisconsin (US), was arrested for purposefully storing more than 500 vaccine doses unrefrigerated, which rendered them unusable. In West Virginia (US), 42 prospective vaccine recipients were mistakenly given an injection of the Regeneron antibody treatment instead of the SARS-CoV-2 vaccine. All of the affected individuals are expected to recover with no harmful effects. In New York, a major healthcare network is under investigation after violating the state’s directives by administering vaccinations to members of the general public rather than frontline healthcare workers and long-term care facility (LTCF) residents. The state fined the health system US$1 million for the violation.
NATIONAL SOCIAL DISTANCING & LOCKDOWN As countries around the world begin to implement SARS-CoV-2 vaccination programs or look ahead to future vaccination efforts, some are recognizing the need to strengthen social distancing and other COVID-19 containment measures in response to ongoing surges in transmission. Germany, which leads the EU in terms of vaccine doses administered, is reportedly considering an extension to its national “lockdown,” which is currently scheduled to end January 10. Germany is averaging nearly 18,000 new cases per day, which corresponds to more than 200 daily cases per million population. The UK is entering another period of “lockdown” as well, following the emergence of the B.1.1.7 variant and associated increases in incidence. New national Level 4 lockdowns are now in place in England, Scotland, and Wales, and Northern Ireland increased its national restrictions on December 26. South Africa also strengthened COVID-19 restrictions nationwide to Level 3 on December 29, which orders the closure of beaches and parks in hotspot areas, the closure of bars and pubs nationwide, and prohibits all alcohol sales, among other restrictions.
US ECONOMIC STIMULUS US President Donald Trump signed a US$900 billion COVID-19 economic stimulus package on December 27. He initially rejected the package and insisted that the Congress increase the individual payments from US$600 to US$2,000; however, after the House of Representatives passed a bill to increase the payments, the Senate did not vote on the bill. President Trump subsequently signed the original bill, but the delay caused a disruption in unemployment funding to millions of Americans that rely on this aid following the severe economic consequences of COVID-19.
Under the current bill, Americans enrolled in federal unemployment programs will receive a weekly US$300 unemployment supplement through mid-March. The stimulus package also includes funding for industries that have been severely affected by COVID-19. Additionally, US$82 billion will be allocated for educational resources, including both K-12 and colleges and universities. The package also includes US$285 billion in support for small businesses, including through the Paycheck Protection Program (PPP). Notably, the PPP will have stricter conditions for enrollment than previous stimulus packages, limiting eligibility to businesses with fewer than 300 employees that experienced at least a 25 percent drop in sales. Of that US$285 billion, US$12 billion is specifically set aside for minority-owned businesses. The airline industry will receive US$45 billion to continue to pay employees at a time when the travel and tourism industries continue to experience severe interruptions. Many billions are also set aside to support contact tracing, diagnostic testing, and vaccine distribution efforts.
SARS-CoV-2 VARIANTS Viral mutation is a common, expected process, although genetic changes often do not result in improvements or fitness advantages for the virus. The SARS-CoV-2 variants first identified in the UK and South Africa, however, do appear to have advantageous mutations in the spike protein, which allow the virus to more efficiently enter cells to begin the viral replication process. Emerging evidence indicates that these changes at the cellular and molecular level may result in increased transmissibility for these variants. Furthermore, these variants are emerging as the dominant strains of SARS-CoV-2 in the UK and South Africa, respectively. In response to news of the emerging variants, many countries have implemented travel restrictions for the UK, but the variant has already been identified in at least 37 countries, including the US.
Increased transmissibility of the SARS-CoV-2 variants poses serious problems to pandemic control efforts, especially among already burdened healthcare facilities. Preliminary studies indicate that the SARS-CoV-2 variants do not cause increased disease severity or case fatality; however, an increase in case loads substantially, further straining hospital systems. Social distancing measures—including mask use, physical distancing, and enhanced hygiene practices—will be critical to limit the spread of these new variants. Some scientists and health authorities have expressed concern over the possibility that existing vaccines and vaccine candidates may be less effective against the new variants, but preliminary studies have not found any indication current vaccines will be less effective in protecting against the UK variant. There are fewer studies on effectiveness against the South Africa variant, but research is ongoing. Notably, if current vaccines are determined to be less effective, BioNTech scientists have stated that they could make necessary changes in approximately 6 weeks.
by shtexas I think I managed to get my Mom a vaccine appointment. Saturday at the grocery pharmacy about 25 minutes north of me. Hope it happens. It has been quite an adventure trying to get one.
by ponchi101 Good for you, and specially for her. Keep us posted on how it goes, as I am, by now, ready to break into a lab, steal the frigging thing, and inject myself.
by shtexas
ponchi101 wrote: ↑Fri Jan 08, 2021 8:48 pm
Good for you, and specially for her. Keep us posted on how it goes, as I am, by now, ready to break into a lab, steal the frigging thing, and inject myself.
Once I am sure my Mom has had hers, I will go through it again for me. My pharmacist says I am eligible to take it now because of my high blood pressure. Plus, I think they are going to be in this eligibility group for a long time. Dallas County has been behind the curve. Not too surprising.
by JazzNU Sounds like they are ahead, not behind if they are giving out vaccines to people with pre-existing conditions. Most places have barely begun on first responders.
by shtexas
JazzNU wrote: ↑Fri Jan 08, 2021 11:02 pm
Sounds like they are ahead, not behind if they are giving out vaccines to people with pre-existing conditions. Most places have barely begun on first responders.
Maybe it just seems that way because the counties around Dallas are doing better.
by shtexas
shtexas wrote: ↑Fri Jan 08, 2021 7:56 pm
I think I managed to get my Mom a vaccine appointment. Saturday at the grocery pharmacy about 25 minutes north of me. Hope it happens. It has been quite an adventure trying to get one.
Well, it didn't happen. Despite a confirmation email and a reminder email, they claimed my Mom wasn't on the list. I was worried because the appointment was late in the day this would happen. They were out of shots. Why? Your guess is as good as mine. Back to the drawing board.
shtexas wrote: ↑Fri Jan 08, 2021 7:56 pm
I think I managed to get my Mom a vaccine appointment. Saturday at the grocery pharmacy about 25 minutes north of me. Hope it happens. It has been quite an adventure trying to get one.
Well, it didn't happen. Despite a confirmation email and a reminder email, they claimed my Mom wasn't on the list. I was worried because the appointment was late in the day this would happen. They were out of shots. Why? Your guess is as good as mine. Back to the drawing board.
I suggest you go to whomever is responsible for vaccines and present them with the confirmation E mail, the reminder E mail, a bill for the fuel your vehicle used to get to the vaccination site and back home, and an invoice for however much time you wasted in going there, calculated at slightly above minimum wage.
Vaccines for this virus are not something to take lightly.
by ti-amie I'm hearing from family sources about a superspreader event in Arizona that they heard about second hand. Anyone know about it?
by dryrunguy Sorry for the delay. Here is the Situation Report for January 7, 2021, I think. There's a lot here.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 86.75 million cases and 1.89 million deaths as of 11:45am EST on January 8.
Brazil, #2 globally in terms of cumulative mortality, surpassed 200,000 deaths, and India, #3 globally in terms of cumulative mortality, surpassed 150,000 deaths. The US remains #1 with 365,000 deaths, and #4 Mexico (131,000) is the only other country with more than 100,000 cumulative deaths.
To date, countries around the world have administered more than 17.5 million doses of SARS-CoV-2 vaccine. The majority of countries that have initiated vaccination efforts are in Europe and North America; however, a number of countries in Asia (China), the Eastern Mediterranean region (Bahrain, Israel, Kuwait, Oman, Saudi Arabia, UAE), and Central and South America (Argentina, Chile, Costa Rica) have begun vaccinating their populations as well. We are not aware of any ongoing vaccination efforts yet in Africa or Oceania.
At this point in time, national vaccination totals are not being updated at regular intervals, with some data dating back to December 28, which makes it difficult to form an accurate picture of the current state of vaccination efforts. Based on the most current data available, the US is #1 in terms of total doses administered (5.92 million), China is #2 (4.5 million; December 31), and Israel is #3 (1.69 million). Israel is also #1 globally in terms of per capita doses administered with 19.55 doses per hundred population, which is more than double the coverage in #2 UAE (9.52), more than 4 times #3 Bahrain (4.25), and more than 10 times the UK (1.91; January 3) and US (1.79).
UNITED STATES
The US CDC reported 21.26 million total cases and 359,849 deaths. We expect the US to surpass a cumulative total of 366,000 deaths in the next several days, which would correspond to 1,000 deaths per day for an entire year (2020 was a leap year). The first US death was not reported until February 29, however, so the actual timeline is closer to 10 months—corresponding to 1,170 deaths per day since the first reported US death.
Yesterday, the US reported 299,904 new cases, a new single-day record. This brings the average daily incidence to 228,003 new cases per day, surpassing the pre-holiday peak and setting a new record—a 27% increase over the holiday low of 179,791. The US also reported a new record high for single-day mortality*, with 3,844 new deaths. The US has reported 2 of the 3 highest daily mortality totals* over the past 2 days. The average daily mortality climbed to 2,664 deaths per day, which returns to the pre-holiday level—an increase of 21% over the holiday low of 2,200. It will potentially several more weeks before we begin to see the effects of holiday travel and gatherings.
*With the exception of April 15, when New York City reported more than 3,700 previously unreported probable deaths from the onset of its epidemic.
The US CDC reported 21.42 million vaccine doses distributed and 5.92 million doses administered (27.6%). These include 3.77 million doses distributed for use in long-term care facilities (LCTFs), of which 603,313 (16.0%) have been administered.
The Johns Hopkins CSSE dashboard reported 21.62 million US cases and 365,882 deaths as of 11:30am EST on January 8.
EMERGING VARIANTS Information and analyses continue to emerge about newly identified SARS-CoV-2 variants, most notably B.1.1.7 (first identified in the UK) and B.1.351 (first identified in South Africa). Both variants appear to be more transmissible than the variants that circulated earlier in the pandemic, including those that are still circulating widely in most places around the world, but research is ongoing to fully characterize them. Perhaps the biggest concern is the potential that these variants could be less susceptible to newly authorized vaccines or therapeutic drugs. Preliminary research (preprint), conducted by researchers at Pfizer and the University of Texas Medical Branch (UTMB), provides evidence that the Pfizer vaccine is efficacious against both the B.1.1.7 and B.1.351 variants. The study was conducted on blood specimens collected from vaccinated individuals, as opposed to data collected from clinical trials in humans, but it does provide initial confidence that the vaccine will remain a capable tool against the new variants.
Another study published recently (preprint) by researchers at the Fred Hutchinson Cancer Research Center (Seattle, Washington, US), analyzed the effects of various mutations on the virus’ susceptibility to antibody treatments. The researchers found that variants with the E484K mutation, such as the B.1.351 variant, “have greatly reduced susceptibility to neutralization by the...serum antibodies of some individuals.” In fact, they observed decreased neutralization on the order of 10-fold or greater for variants with this mutation. They believe this is a result of changes to the receptor binding domain, which stimulates the majority of the antibody response. Notably, the researchers found that the N501Y mutation present in the B.1.1.7 variant “is unlikely to greatly affect neutralization by most human sera,” an encouraging indication. Further research is needed to better characterize the effects of these and other emerging variants—including their effects on disease severity, transmissibility, and susceptibility to medical countermeasures —but these studies provide insight into the potential impact these variants can have on the COVID-19 pandemic.
VACCINE AUTHORIZATIONS On January 4, the Israeli Ministry of Health authorized the use of the Moderna vaccine, the first country to do so outside of North America. The Israeli MOH has reportedly secured 6 million doses of the vaccine, and the first deliveries were expected earlier this week. On January 6, the European Medicines Agency (EMA) recommended a conditional marketing authorization for Moderna’s SARS-CoV-2 vaccine. The European Commission issued the conditional authorization, making the Moderna vaccine the second vaccine authorized for use in the EU, after the Pfizer/BioNTech vaccine was authorized in December. The EU has purchased as many as 160 million doses of the Moderna vaccine, which are set to be delivered between now and September, adding to the 300 million doses of the Pfizer/BioNTech vaccine already ordered. Additionally, the EMA recommended an update to the Pfizer/BioNTech vaccine guidance “to clarify that each vial contains 6 doses of the vaccine.” The update recommends using “low dead-volume” syringes, which result in moderate improvements in vaccine wastage that can allow vaccinators to draw a full sixth dose from each vial, instead of 5. The EMA announcement notes that “standard syringes..may not [enable vaccinators] to extract a sixth dose.” Additionally, the European Commission reportedly offered Member States the opportunity to purchase as many as 300 million total additional doses, which could bring the total Pfizer/BioNTech allotment to 600 million across Europe. The combined 760 million doses could provide full vaccination for 380 million people, covering approximately 80% of Europe’s population.
VACCINE CLINICAL TRIALS According to multiple news media reports, Brazilian health officials announced that China’s Sinovac SARS-CoV-2 vaccine demonstrated 78% efficacy in Phase 3 clinical trials. With its COVID-19 epidemic largely contained, China coordinated with countries with more widespread transmission to conduct clinical trials. According to the US NIH clinical trial database, the Phase 3 trials in Brazil included 13,000 total participants, less than half the size of the study populations for the Pfizer/BioNTech and Moderna Phase 3 trials. Following these results, vaccine supplies have shipped around the world, waiting for its anticipated approval. Sinovac has already pledged 300 million doses to low- and middle-income countries, approximately half of the expected production capacity for 2020. Previously, researchers in Turkey announced that the Sinovac vaccine resulted in 91% efficacy in a clinical trial of 7,300 participants. To our knowledge, final Phase 3 data and analysis for the Sinovac vaccine has not yet been published publicly.
LOS ANGELES The burden of COVID-19 patient surge on hospitals and health systems can take many forms. While much of the coverage of these issues focuses on hospital beds, personnel, personal protective equipment, and ventilators, general medical supplies are also a major concern. In particular, oxygen supply is emerging as a constraint. Health experts previously forecast oxygen supply as a major concern in some parts of the world, and these concerns are now coming to fruition.
In response to the increased oxygen demand during the current COVID-19 surge, the Emergency Medical Services (EMS) Agency in Los Angeles, California (US) directed EMS personnel to only administer oxygen to patients with oxygen saturation below 90%. Many COVID-19 patients require supplemental oxygen therapy, and the increased use has resulted in a local shortage. The new directive aims to conserve the available oxygen supply for patients with the greatest need.
Additionally, EMS personnel in LA are directed to not transport cardiac arrest patients to hospitals if efforts to revive breathing or pulse in the field are not successful. Patients who can be resuscitated on site will still be transported to the hospital for treatment as usual. As we have covered previously, Los Angeles County hospitals are facing a major surge in COVID-19 patients, which has resulted in long lines for ambulances to drop off patients at the hospital, some lasting several hours, which is negatively impacting care for both COVID-19 and non-COVID-19 patients. The new policy aims to reduce the wait time for ambulances to drop off patients by not transporting patients who are unlikely to survive.
CLINICAL TRIAL PLACEBO GROUP VACCINATIONS One of the principal ethical challenges stemming from SARS-CoV-2 vaccine clinical trials is how to handle participants in the control group after vaccines are authorized for use. As a necessary part of randomized controlled trials, some participants receive the vaccine, and others receive a placebo. But now that authorized vaccines are available, it raises questions regarding when those who received the placebo can be eligible to receive the actual vaccination. The longer the control group goes unvaccinated, the more data researchers can collect to evaluate the vaccine’s safety and efficacy, particularly for determining its effect on mitigating infection and transmission risk; however, delaying vaccination for individuals who voluntarily placed themselves at risk to participate in the trial raises ethical concerns.
Negotiations between Pfizer, Moderna, and the US FDA have attempted to address this issue and balance the value of continued data collection against fairness to the trial participants. A recent agreement between Pfizer and the FDA will allow trial participants in the control group to be vaccinated by March 1, if they choose to do so, several months earlier than the original timeline. Moderna established a similar plan in December. Under the new plan, study participants can request to find out whether they received the vaccine or the placebo, and those who received the placebo will be immediately eligible to receive vaccine, even if they would not be eligible under the existing federal guidance.
DIABETES RISK A study published in The Lancet: Diabetes & Endocrinology evaluated the risk of COVID-19 disease and death among patients with diabetes. The researchers collected data on the entire population of Scotland, and focused on the country’s “first wave” of COVID-19 (March-July 2020). The researchers compared the cumulative COVID-19 mortality and the incidence of COVID-19 cases that required critical care among individuals with and without diabetes. The combined odds of requiring critical care or dying from COVID-19 (in or outside of a hospital) was significantly higher among individuals with diabetes (aOR=1.4). The odds of requiring critical care or dying was even higher for patients with Type 1 diabetes (aOR=2.4). Diabetes has been previously identified as a preexisting condition associated with elevated risk of severe COVID-19 disease and death, and this study provides further quantitative data to support that association.
The US CDC lists type 2 diabetes as a condition associated with increased risk and type 1 diabetes as a condition that “might be” associated with increased risk. Notably, this study identified higher risk of severe disease and death among individuals with type 1 diabetes than those with type 2 diabetes, but both were significantly associated with increased risk. Further study is needed to more fully characterize the effects of both types of diabetes on COVID-19 disease.
WHO INVESTIGATION The WHO has deployed a team to China to investigate the origin of the SARS-CoV-2 virus, but the team members are reportedly facing challenges entering the country. According to multiple news media reports, the Chinese government denied entry to the team because their visas had not yet been approved. Several team members had already started their travel when the WHO was notified of the delay in processing the visas, others had to delay their travel, and at least one team member was forced to return home. At his first press conference of 2021, WHO Director-General Dr. Tedros Adhanom Ghebreyesus expressed disappointment that China had not yet finalized the visas. He emphasized the importance of the mission and noted that he had been assured that Chinese officials were working to quickly resolve the issue. A spokesperson from China’s Ministry of Foreign Affairs reportedly indicated that the delay was the result of a “misunderstanding” and that Chinese officials were coordinating closely with the WHO to resolve the issue. The WHO investigation aims to determine the evolution of the SARS-CoV-2 virus, identify animal hosts, and understand the process and timeline by which the virus made the jump from animals to humans.
US VACCINATION Earlier this week, Nebraska (US) Governor Pete Ricketts stated that undocumented workers in meatpacking facilities would not be eligible to receive COVID-19 vaccines. The governor’s communication director reportedly attempted to clarify Governor Ricketts’ comments, indicating that citizens and legal residents would be prioritized over undocumented immigrants. A number of health and immigration policy experts and elected officials expressed opposition to Governor Ricketts’ policy, noting that many meatpacking facilities do employ undocumented immigrants, and that employees at these facilities are at risk for COVID-19, regardless of their immigration status.
Nebraska’s meatpacking industry is among the largest in the US, and 66% of its meatpacking workers are immigrants. According to data published by the Migrant Policy Institute, at least 14% of meatpacking workers are undocumented. In total, more than 52,000 COVID-19 cases nationwide have been reported among meatpacking workers, including 266 deaths. The Midwest Center for Investigative Reporting found that Nebraska reported the highest number of COVID-19 cases originating from meatpacking facilities of all US states, illustrating the risk to these workers. To date, 23 Nebraska meatpacking facilities have reported COVID-19 outbreaks, resulting in 5,267 cases and 22 deaths among meatpacking workers.
INDONESIAN VACCINATION The Indonesian Ulema Council, “Indonesia’s highest Islamic body,” announced that it determined China’s Sinovac SARS-CoV-2 vaccine to be halal, or “fit for consumption by Muslims.” The decision was made based on the Council’s deliberations on potential religious barriers to using the vaccine, including the inclusion of pork-derived gelatin commonly used as a stabilizer in vaccines. Similar concerns exist for members of the Jewish faith as well. Spokespersons for the manufacturers of multiple leading vaccines—including Pfizer, Moderna, and AstraZeneca—have indicated that no pork products are included in their SARS-CoV-2 vaccines.
Notably, the approval by one body is not necessarily universally accepted, but the Indonesian Ulema Council decision is a promising step in the complex effort to mitigate hesitancy surrounding the new SARS-CoV-2 vaccines. Conversations around the religious standing of vaccine candidates have created barriers in past vaccination campaigns, and it is important that these concerns are addressed fully when planning vaccination efforts. Reportedly, the vaccine is still being evaluated for authorization by Indonesia’s national regulatory authorities, which is required before vaccination efforts can begin.
ALLERGIC REACTIONS A study published in the US CDC’s MMWR provides detailed data on allergic reactions following receipt of the first dose of Pfizer/BioNTech SARS-CoV-2 vaccine. The Vaccine Adverse Event Reporting System (VAERS) reported 21 cases of anaphylaxis among a total of 1,893,360 first doses of the vaccine administered between December 14-23, 2020. The 21 cases represent a rate of 11.1 cases per million doses administered. Among the 21 reported anaphylactic reactions, 17 affected individuals had a documented history of allergies or allergic reactions, and 7 had a history of anaphylaxis. Of the cases, 71% occurred within 15 minutes of vaccination, and 18 were reported within 30 minutes. No deaths were reported among anaphylaxis patients. Since the study period, an additional 8 cases have been reported for a total of 29 cases of allergic reactions nationwide. In addition to anaphylaxis, 83 cases of nonanaphylaxis allergic reactions were reported in VAERS (87% documented as nonserious).
INDIA VACCINE The Serum Institute of India announced that it will first focus on supplying India with the Oxford University-AstraZeneca COVID-19 vaccine, approved January 3 for emergency use, before distributing to other countries. The Serum Institute is the world’s largest vaccine manufacturer by volume, and it has been contracted to produce 1 billion doses of SARS-CoV-2 vaccine. Serum Institute CEO Adar Poonawalla indicated that the first 100 million doses are being sold to the Indian government at a special price of 200 rupees (US$2.74) per dose, while the price for the private market will be 1,000 rupees (US$13.68). There is an existing contract with COVAX for 100 million doses each of the AstraZeneca-Oxford and Novavax vaccines, and Mr. Poonawalla says contract negotiations are ongoing to add another 300-400 million doses to that order; however, the export of vaccines for COVAX is not expected to begin until March or April 2021. He also indicated that the company plans to provide 200-300 million doses of the vaccine to COVAX by December 2021. The Financial Times reports that the Serum Institute expects to sell 2-3 million doses to private facilities for US$8 per dose after fulfilling its contract with the Indian government, but this has raised some concerns that the private sale of vaccine doses could shift access from those in the most need to those who can afford to purchase it.
IMMUNITY DURATION Researchers in California and New York (US) published findings from a study on the duration of immune memory response following SARS-CoV-2 infection. The study, published in Science, looked specifically at the role of B cells and CD4+ and CD8+ T cells, as opposed to the neutralizing antibodies analyzed in many other studies. While neutralizing antibodies are the key to preventing infection, immune memory, including B cells and T cells, is expected to play a larger role in preventing or mitigating the severity of disease. The study involved 188 participants who had recovered from SARS-CoV-2 infection—including “a range of asymptomatic, mild, moderate, and severe COVID-19 cases”—recruited in California and New York. Among the participants, 97% were symptomatic during their infection. Blood specimens were collected between 6 and 240 days after symptom onset, including 51 participants who provided multiple specimens over a period of several months.
The researchers observed an increase in the level of B cells corresponding to the SARS-CoV-2 spike protein over the period from 1 month after symptom onset to 6 months or longer. Conversely, the quantity of CD4+ and CD8+ T cells decreased over time, with a half-life of approximately 3-5 months. Additionally, B cells corresponding to the spike protein and the receptor binding domain (RBD) were significantly higher in hospitalized patients than in non-hospitalized patients. Conversely, CD8+ T cells were approximately the same in hospitalized and non-hospitalized patients, and CD4+ T cells were lower in hospitalized patients than in non-hospitalized patients (but not statistically significant). The researchers indicate that the temporal trends in the B and T cells are “consistent with the hypothesis” that the immune memory response is capable of “reduc[ing] COVID-19 disease severity.” While this is a relatively small study, it provides insight into the temporal dynamics of the human immune response to SARS-CoV-2 infection and the potential impact on lasting immunity.
ETHIOPIA A report by the UN Office for the Coordination of Humanitarian Affairs published an update on the humanitarian crisis in Ethiopia’s Tigray Region, describing the humanitarian situation as “dire.” Violence in the region has cut off hundreds of thousands of people from humanitarian aid, including several major cities. The Tigray Region is home to approximately 6 million people, and ongoing conflict has weakened the local health system. The report indicates that only 5 of the region’s 40 hospitals are physically accessible and that the spread of SARS-CoV-2 is a growing concern. Notably, COVID-19 surveillance has been interrupted for at least a month, and the humanitarian response has only been able to implement “limited prevention activities,” including the distribution of PPE and educational materials. The UN report that the displacement of refugees and overcrowded living conditions could be driving “massive community transmission.”
TOKYO Like many countries around the world, Japan is currently facing a major COVID-19 surge, its largest by a factor of 3. In response to increasing transmission in Tokyo, Japanese Prime Minister Yoshihide Suga declared a state of emergency for the city and strengthened COVID-19 restrictions. The state of emergency is currently scheduled to last for a month, through February 7. One of the primary measures is for the public to refrain from nonessential activities, particularly at night, and observe a requested 8pm curfew. The new measures also focus heavily on restaurants and bars, including requested restrictions on the hours they serve alcohol—i.e., not between 7pm and 11am. In order to promote compliance, some of the restrictions are tied to financial support for businesses as compensation for lost revenue, and the government is able to “name and shame” businesses that violate the measures.
by Suliso That day has come at last when all US states are on the red list (Vermont was the last struggler). Currently US is the 6th worst in the World, albeit there is probably no caching of UK and Ireland. Those two, particularly the latter, are on a true infection turbocharger probably due to the new variant. UK is one of the better countries in vaccination rate, though.
by ponchi101
dryrunguy wrote: ↑Sun Jan 10, 2021 5:55 am
Sorry for the delay. Here is the Situation Report for January 7, 2021, I think. There's a lot here.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 86.75 million cases and 1.89 million deaths as of 11:45am EST on January 8.
...
ALLERGIC REACTIONS A study published in the US CDC’s MMWR provides detailed data on allergic reactions following receipt of the first dose of Pfizer/BioNTech SARS-CoV-2 vaccine. The Vaccine Adverse Event Reporting System (VAERS) reported 21 cases of anaphylaxis among a total of 1,893,360 first doses of the vaccine administered between December 14-23, 2020. The 21 cases represent a rate of 11.1 cases per million doses administered. Among the 21 reported anaphylactic reactions, 17 affected individuals had a documented history of allergies or allergic reactions, and 7 had a history of anaphylaxis. Of the cases, 71% occurred within 15 minutes of vaccination, and 18 were reported within 30 minutes. No deaths were reported among anaphylaxis patients. Since the study period, an additional 8 cases have been reported for a total of 29 cases of allergic reactions nationwide. In addition to anaphylaxis, 83 cases of nonanaphylaxis allergic reactions were reported in VAERS (87% documented as nonserious).
...
Which is actually frigging great news. It is minute, specially with a vaccine that has been developed at such pace.
People with previous histories of allergies should be set aside, given the vaccine, and wait in the lobby for a little while. It would seem a like a possible and logical step.
Question, if anybody know. Do you have to be tested BEFORE the vaccine is administered? Because if you already have the virus it would make very little sense to apply the vaccine. An antigen test takes about 4 hours, so you could be tested in the morning and then get the shot in the afternoon (if you test negative). Otherwise, it might be one vaccine wasted.
by Suliso Not heard of that being the case. Probably not worth it due to additional complexity and possibly lower uptake of vaccines.
I have heard of lots of vaccines being wasted in NYC because they opened a vial, some people didn't show up and they couldn't find anyone from an eligible category within the few hours the vaccine is usable after being thawed. I find this ridiculous - just give it to anybody willing, even an 18 year old from a street. Anything is better than throwing away...
by ponchi101 That is truly absurd.
They are making the protocols too complex, just to make sure they "get it right". As you say, once a vaccine is ready, inject it in the next available arm.
Here they are talking about an app/website to tell people when they can get the vaccine. Not thinking that the most vulnerable population is the one that uses apps and websites the least: elderly people that may even not have access to a computer or truly use a smartphone with any dexterity.
by Suliso Found this somewhat technical article about how mRNA vaccine from BioNTech works. It's kind of biased towards people who understand IT better, but I understood it perfectly clearly as well. Perhaps some of you will find it illuminating too.
by ponchi101 To see if I got it. The vaccine produces mRNA that only codes for the SPIKES in the Sars V2 virus, not for the whole virus. And then the immune system learns to attack the spikes and anything with spikes, which means the virus primarily.
I had no idea that DNA printers existed. I will never cease to be amazed by what science can do.
by skatingfan
ponchi101 wrote: ↑Sun Jan 10, 2021 5:38 pm
To see if I got it. The vaccine produces mRNA that only codes for the SPIKES in the Sars V2 virus, not for the whole virus. And then the immune system learns to attack the spikes and anything with spikes, which means the virus primarily.
I had no idea that DNA printers existed. I will never cease to be amazed by what science can do.
I would add one thing - the spikes are important because they are the part of the virus that connects to our cells, and allows the virus to enter the cells. One of the reasons that the new variants of the virus are more infectious is because their spikes more easily line up with the ports on our cells.
by Suliso
ponchi101 wrote: ↑Sun Jan 10, 2021 5:38 pm
To see if I got it. The vaccine produces mRNA that only codes for the SPIKES in the Sars V2 virus, not for the whole virus. And then the immune system learns to attack the spikes and anything with spikes, which means the virus primarily.
I had no idea that DNA printers existed. I will never cease to be amazed by what science can do.
Indeed, this vaccine contains mRNA fragment which codes for the SPIKES protein of the actual virus. DNA copying is not that new anymore. Polymerase chain reaction (Karry Mullis, 1993 Nobel prize) is probably the initial key technology for that.
by Deuce
Suliso wrote: ↑Sun Jan 10, 2021 3:18 pm
I have heard of lots of vaccines being wasted in NYC because they opened a vial, some people didn't show up and they couldn't find anyone from an eligible category within the few hours the vaccine is usable after being thawed. I find this ridiculous - just give it to anybody willing, even an 18 year old from a street. Anything is better than throwing away...
by ponchi101 I did find a I AM SHOCKED CASABLANCA gif. But it is two big.
Wonder who grifted from that. I mean, of the kids and Jared.
by dryrunguy Sidebar: Something that is attracting a decent amount of local conversation here... Apparently, several reports indicate that vaccine candidates should abstain from consuming alcohol in the days leading up to and following the administration of COVID vaccination doses because alcohol lowers immunity and can significantly reduce vaccine effectiveness.
It's quite the topic of conversation around here. As you may know, rural Pennsylvania has astronomical rates of alcoholism, and for some, alcohol is far more important than preventing COVID.
Just mentioning it.
by Suliso Really? Instinctively that doesn't make much sense to me, would like to see some proper study proving it.
by Deuce
Suliso wrote: ↑Mon Jan 11, 2021 8:50 am
Really? Instinctively that doesn't make much sense to me, would like to see some proper study proving it.
Alcohol has been long thought to have a negative effect on the immune system.
Just dug these up quickly...
by Deuce It was one year ago today that the first official fatality of COVID-19 was recorded - a man in Wuhan, China.
And since then, the virus has spread as dramatically as it has rapidly, and grew quickly out of control all over the world.
It feels like we've been inhabiting a different planet for the past 10 months here.
What we had known as 'normal life' for the entirety of our respective existences seems like it happened a few lifetimes ago.
No-one could have imagined that what we're currently living would be our reality.
by ponchi101
Deuce wrote: ↑Mon Jan 11, 2021 10:49 am
It was one year ago today that the first official fatality of COVID-19 was recorded - a man in Wuhan, China.
And since then, the virus has spread as dramatically as it has rapidly, and grew quickly out of control all over the world.
It feels like we've been inhabiting a different planet for the past 10 months here.
What we had known as 'normal life' for the entirety of our respective existences seems like it happened a few lifetimes ago. No-one could have imagined that what we're currently living would be our reality.
I agree mostly with your post, except the bold part. After reading THE COMING PLAGUE, written in 1994, the immunology and viral experts of the world were clear that this was WHEN, not IF.
Remember that even "popular" culture foresaw this. Non-Fiction thrillers like Richard Preston's THE HOT ZONE, or films like Steven Soderbergh's CONTAGION made points about what could happen.
Were we warned? Debatable. Did this come completely out of nowhere? No. Some people saw it.
by Suliso A couple small things I'm wondering regarding vaccination...
- the first dose offers only partial protection. Suppose someone still gets ill two weeks after getting it. Does he/she gets the second dose anyway while they are ill?
- above it was described that few people got lucky and received the first dose of the vaccine well before "their time". But now what happens with the 2nd dose? Do they get that too in 3 weeks? Also what kind of proof of vaccination do people get in US?
by ponchi101
Suliso wrote: ↑Mon Jan 11, 2021 5:04 pm
A couple small things I'm wondering regarding vaccination...
- the first dose offers only partial protection. Suppose someone still gets ill two weeks after getting it. Does he/she gets the second dose anyway while they are ill?
- above it was described that few people got lucky and received the first dose of the vaccine well before "their time". But now what happens with the 2nd dose? Do they get that too in 3 weeks? Also what kind of proof of vaccination do people get in US?
Yes.
And one thing that I would like to see. People should get proof of vaccination that is visible to others, if they want it. I would not mind wearing a plastic bracelet for one year, showing I got my shot.
Your points are all spot-on. I wonder if the governments have thought about that.
by shtexas
Suliso wrote: ↑Mon Jan 11, 2021 5:04 pm
A couple small things I'm wondering regarding vaccination...
- the first dose offers only partial protection. Suppose someone still gets ill two weeks after getting it. Does he/she gets the second dose anyway while they are ill?
- above it was described that few people got lucky and received the first dose of the vaccine well before "their time". But now what happens with the 2nd dose? Do they get that too in 3 weeks? Also what kind of proof of vaccination do people get in US?
To the second point, the next appointment gets scheduled pretty much immediately. I know the grocery pharmacy near me will give you a number to call or weblink that you can use to schedule shot #2.
Suliso wrote: ↑Mon Jan 11, 2021 5:04 pm
A couple small things I'm wondering regarding vaccination...
- the first dose offers only partial protection. Suppose someone still gets ill two weeks after getting it. Does he/she gets the second dose anyway while they are ill?
- above it was described that few people got lucky and received the first dose of the vaccine well before "their time". But now what happens with the 2nd dose? Do they get that too in 3 weeks? Also what kind of proof of vaccination do people get in US?
Yes.
And one thing that I would like to see. People should get proof of vaccination that is visible to others, if they want it. I would not mind wearing a plastic bracelet for one year, showing I got my shot.
Your points are all spot-on. I wonder if the governments have thought about that.
The conservatives here would scream if they had to carry papers or wear a bracelet as proof.
by ponchi101 Oh, sure. I can see them screaming about their freedom and other nonsense. I was talking about myself; I would not mind wearing it as way of proof that I have taken it.
Maybe they can wear it wrapped around their gun. You know, open carry?
by Suliso I have a vaccination "passport" since I've been vaccinated as an adult against all kinds of tropical diseases few years ago. I assume my future covid vaccine will be added there as well. Not sure what percentage of people here or anywhere else do have such a thing.
by skatingfan
Suliso wrote: ↑Tue Jan 12, 2021 9:32 am
I have a vaccination "passport" since I've been vaccinated as an adult against all kinds of tropical diseases few years ago. I assume my future covid vaccine will be added there as well. Not sure what percentage of people here or anywhere else do have such a thing.
I had something similar when I was a kid, but it hasn't been updated since I was pretty young - my Mom probably still has it because she keeps everything.
by ponchi101 I have one too, which is basically mandatory for the industry. And for sure my vaccination will go there (I will request it). But I don't walk around with it, as it is too valuable a document for me. Would be in real trouble if I lost it.
The Yellow Fever vaccination document that is universal has space to fill in other vaccines, too.
I guess we are in agreement. Just wait and see if any government implements something.
by Suliso I think you'll need this or a similar document to fly internationally to many if not most destinations from fall 2021.
by shtexas After striking out at the grocery pharmacy, my Mom received an invitation from Dallas County (I had signed her up earlier) to sign up for an appointment at the County's hub at Fair Park (downtown Dallas) on Tuesday or Wednesday. I filled it out and chose Tuesday at 12:30 PM. We arrived at 12:25 PM and she had the shot in her arm by 12:38 PM. Talk about efficient. They did make her sit for a while to make sure there was no reaction. She returns February 9 for shot #2. Our County Judge Clay Jenkins (D) did an outstanding job. He set this whole thing up in one week.
by ponchi101 Great. Did you get your shot too? I saw in the news that people with co-morbidities under 65 can get the vaccine as a priority.
Not that I mind that I don't have any comorbidities, but that will mean that I am pretty much at the end of the line.
Down here: The Colombian GOV has acknowledged that legal residents will be treated in the same fashion as Colombian citizens. So the GF and I are in the list. Whenever that starts.
by dryrunguy The most recent Situation Report. It just keeps getting worse in the U.S.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 89.71 million cases and 1.94 million deaths as of 11:45am EST on January 12. Following 2 weeks of decreased global incidence and mortality, coinciding with holidays around the world, the WHO reported new record high weekly totals for both COVID-19 incidence and mortality. The WHO reported 4.95 million new cases last week, a nearly 20% increase over the previous week. The WHO also reported 85,653 deaths last week, an 11% increase over the previous week.
UNITED STATES
The US CDC reported 22.32 million total cases and 373,167 deaths. On January 8, the US reported 314,093 new cases, becoming the first country to surpass 300,000 new cases in a single day. To our knowledge, the US remains the only country to report more than 100,000 new cases in a single day. The US is now averaging 244,702 new cases per day, the highest daily incidence to date and nearly 1 million new cases every 4 days. The US reported a new record for single-day mortality* as well, with 4,180 deaths reported on January 7. The average daily mortality surpassed 3,000 deaths per day for the first time since the onset of the pandemic. The current average of 3,214 is 12.5% higher than the peak mortality during the United States’ initial surge, corresponding to nearly 10,000 deaths every 3 days.
*With the exception of April 15, when New York City reported more than 3,700 previously unreported probable deaths from the onset of its epidemic.
The US CDC reported 25.48 million vaccine doses distributed and 8.99 million doses administered (35.3%). These include 4.24 million doses distributed for use in long-term care facilities, of which 937,028 (22.1%) have been administered.
Distribution of SARS-CoV-2 vaccines continues to scale up nationwide, but the speed at which states are administering vaccinations varies widely. Among US states, all but 7 (and Washington DC) have received between 6,000 and 8,000 doses per 100,000 population from the federal government, illustrating that allocation has been largely consistent nationwide. Arkansas; Hawai’i; Maine; New Mexico; Vermont; Washington, DC; and West Virginia have received between 8,000 and 9,000 doses per 100,000 population, and Alaska has received 18,092 doses per 100,000 population, more than double the per capita total received by any other state.
While the per capita distribution is relatively consistent between states, vaccine administration is a much different story. Most US states have administered between 2,000 and 4,000 doses per 100,000 population. Among those states reporting higher vaccination coverage, Alaska (4,788); Maine (4,088); Vermont (4,128); Washington, DC (4,141); and West Virginia (5,376) are among those that have administered the most vaccine doses per capita. Connecticut is reporting 4,128 vaccines per 100,000 population, and North and South Dakota are reporting 5,100 and 5,451, respectively. On the other end of the spectrum, 9 states are reporting fewer than 2,000 vaccinations per 100,000 population, including Arkansas (1,355) and Georgia (1,346) with fewer than 1,500. Alabama (23.4%) and Arizona (24.5%) are also reporting fewer than 25% of doses administered. 10 states have administered more than half of their received doses. North and South Dakota are the top 2 states, with 72.6% and 70.0%, respectively.
The Johns Hopkins CSSE dashboard reported 22.71 million US cases and 378,457 deaths as of 1:30pm EST on January 12.
US VACCINATION
FEDERAL DISTRIBUTION
As vaccination efforts continue in the US, operational and policy challenges continue to emerge, some of which are slowing progress. One of the biggest issues with the US vaccination effort is the national distribution system. Under the current plan, the federal government is reserving approximately half of the available vaccine doses in order to ensure that enough supply is available to provide second doses to all vaccinees. In order to speed the United States’ COVID-19 vaccination progress, US President-Elect Joe Biden announced that he intends to release essentially all of the remaining federal inventory soon after taking office. The stated goal of administering 100 million vaccinations in the first 100 days of his term would be a tremendous achievement, particularly considering the US has administered fewer than 10 million doses in slightly less than a month. Efforts are ongoing to establish plans to provide states with additional information regarding future shipments that will enable vaccinators to improve scheduling and administration, but many challenges remain. Even if the federal government increases the distribution to states, there are still many barriers to increasing the pace of vaccination at the local level. Notably, the Biden Administration plan will not delay the second dose, like in some other countries. The aim is to increase the speed at which the first doses are administered and to provide increased transparency regarding the timing of future shipments to improve planning at the local level. Following the Biden Administration announcement, the US Department of Health and Human Services is expected to announce that the federal government will begin distributing the reserved vaccine doses prior to President-Elect Biden taking office.
SYRINGE VOLUME
As we covered previously, the European Medicines Agency (EMA) updated its guidance for the Pfizer/BioNTech vaccine to recommend the use of “low dead-volume” syringes in order to enable vaccinators to draw an extra, sixth dose from vaccine vials. Reports emerged early in the US vaccination effort that some Pfizer/BioNTech vials contained enough vaccine for a sixth (or sometimes seventh) dose; however, a report published by Politico indicates that some of the syringes distributed nationwide by Operation Warp Speed are not the kind that enable vaccinators to draw extra doses. The syringes are distributed along with the vaccine as part of “ancillary supply kits,” and federal officials are reportedly working on a solution to provide syringes with a smaller “dead-volume” that could increase the number of available doses. At 1 extra dose of vaccine per vial, the overall capacity could increase by 20%, which could translate to an extra 5 million doses, based on the current national distribution. A representative from the American Hospital Association indicated that the syringes included with the most recent distributions of the vaccine have a larger “dead-volume,” which is resulting in fewer doses of the vaccine compared to earlier shipments, posing challenges in terms of ensuring enough vaccine is available to provide individuals with the second dose. A representative for the American Pharmacists Association noted that the federal tracking system is based on the number of vials distributed, not the number of doses administered, so hospitals that receive the same number of vials may not have enough vaccine to provide everyone with a second dose, if they are not able to draw extra doses from each vial like they did previously.
MASS VACCINATION EVENTS
As vaccination efforts scale up nationwide, including expanded eligibility, state and local public health and healthcare officials are proceeding with plans to establish mass vaccination capacity. Some of these efforts are leveraging space available at large venues—such as stadiums, convention centers, and fairgrounds—which can provide space for many vaccinators that can process large crowds quickly. For example, Los Angeles, California, is converting Dodger Stadium from a mass testing site to administer vaccinations. California is reportedly also establishing mass vaccination sites at Disneyland Resort (Anaheim), Petco Park (San Diego), and CalExpo fairgrounds (Sacramento). In San Antonio, Texas, health officials began administering vaccinations at the Alamodome, where they expect to be able to vaccinate 30,000 people per week. With its regular season over, and most teams no longer playing, the NFL (football) is encouraging teams to make their stadiums available to serve as vaccination sites. While these large sites provide the space needed to administer vaccinations rapidly, many barriers still remain, including the logistics of transporting and storing vaccines and the need for additional personnel who are trained and qualified to administer vaccinations.
EMERGING VARIANTS Expanded sequencing and screening capacity and capabilities have helped identify several emerging variants of SARS-CoV-2 in the UK (B.1.1.7) and South Africa (B.1.351). More recently, similar variants were detected in Japan and Nigeria. The B.1.1.7 and B.1.351 variants have several mutations in the spike protein, which appear to confer increased transmissibility. The variant detected in Japan was first identified in 4 travelers from Brazil who arrived at Haneda Airport in Tokyo. The variant identified in Nigeria was first detected in the state of Osun, in specimens dating back to at least August 2020, and preliminary analysis indicates that it is “distantly different” from the B.1.1.7 and B.1.135 variants. Health authorities and researchers are investigating the particular characteristics of the new variants, including any potential effects on transmissibility, disease severity, and vaccine susceptibility.
Although the variants do not seem to cause increased morbidity or mortality, WHO Director-General Dr. Tedros Adhanom Ghebreyesus stated that the continued emergence of highly transmissible variants is “highly problematic.” While these variants may each exhibit similar mutations and characteristics, it appears that they have all emerged independently. The wide geographic distribution of emerging variants is concerning for control efforts, because the emergence and evolution of the virus, including the effects on the virus’ characteristics, are unpredictable. Continued and renewed efforts in genomic surveillance are necessary in order to monitor the geographic spread of existing variants and quickly identify the emergence of new ones.
VACCINATING RECOVERED INDIVIDUALS Since the onset of the pandemic, health experts and officials have studied the role of immunity conferred by natural infection. While reports of are relatively rare, the potential for reinfection does exist. In light of this risk, the US CDC emphasizes that individuals who were previously infected and recovered should still get vaccinated due to the “severe health risks” and uncertainty regarding the duration of natural immunity. Additionally, the degree of natural immunity “varies from person to person.” The duration of the immunity conferred by vaccination remains uncertain as well, but research is still ongoing via clinical trials. Depending on the duration of immunity following vaccination, it may be necessary for individuals to receive regular boosters to provide longer-term protection.
SHORTENED QUARANTINE In December 2020, the US CDC updated its COVID-19 quarantine guidance to offer several options that allow individuals to shorten their 14-day quarantine period following a known exposure to SARS-CoV-2. Specifically, individuals who are unable to quarantine for the full 14 days can end their quarantine after 10 days if they exhibit no symptoms or after 7 days if they test negative on Day 5 or later. The CDC’s MMWR published 2 recent studies that provide analysis of the transmission risk associated with shorter quarantine periods.
The first study was conducted by the US CDC COVID-19 Response Team and the COVID-19 Collegiate Athlete Testing Group, in collaboration with researchers from several US universities. The researchers evaluated SARS-CoV-2 testing data for 1,830 US college athletes who were quarantined and tested after exposure to known COVID-19 cases. Among these athletes, 458 (25%) tested positive at some point during their quarantine period, including 137 who never reported COVID-19 symptoms. Among 620 athletes with positive tests*, 303 (48.9%) had positive tests by Day 2 of quarantine and 453 (73.1%) by Day 5. For those who had a negative test on Day 5, the researchers estimate the risk of testing positive after that point to be 26.9%, including 14.2% after Day 7 and 4.7% after Day 10. Notably, however, 26 of the 29 athletes that tested positive on Days 11-14 were not tested at all prior to that point, so it is possible that they would have tested positive on earlier tests, had they been conducted.
*Including additional data from schools that only reported positive tests.
Officials from the Vermont (US) Department of Health issued recommendations for a shorter quarantine period in May 2020, 7 months before the US CDC update. The Vermont policy stated that individuals could conclude their quarantine period if they tested negative on or after Day 7, based on data indicating that approximately 75% of COVID-19 patients developed symptoms within 7 days of exposure. The researchers analyzed test results for 2,200 contacts of known COVID-19 cases who were tested on Days 7-10 after exposure, collected in May-November 2020. In total, 87 (4%) of these individuals tested positive on Days 7-10, including 24 (25%) who were asymptomatic at the time of testing. The researchers also present data on the results for subsequent testing for a subset of these individuals. Among those who initially tested negative, 262 were tested again within 7 days—154 initially tested on Day 7 and 108 initially tested on Days 8-10. None of those individuals tested positive on the second test, providing evidence that there is relatively low risk of becoming infectious after a negative test later in the quarantine period. This study included data from a small proportion of individuals who ended their quarantine early, but it does provide some evidence that the risk of becoming infectious late in the quarantine period is relatively low.
UK TRAVEL SCREENING & TESTING With the emergence of the B.1.1.7 variant of SARS-CoV-2, the UK has strengthened travel restrictions and increased testing volume. Many countries have implemented their own travel restrictions to decrease the number of travelers arriving from the UK, including some in response to the new variant. The UK, already struggling to keep up with increased incidence believed to be linked to the B.1.1.7 variant, has also implemented strict travel guidance to prevent the entry of other variants, including the B.1.351 variant. Anyone entering the UK by plane, boat, or train must now present a negative SARS-CoV-2 test, taken within 72 hours of departure, before they are permitted to enter the country. Travelers also must fill out a passenger locator form prior to their arrival in order to facilitate contact tracing efforts while they are in the UK. Failure to complete the passenger locator form could result in fines up to £500.
TRANSMISSION ON AIRCRAFT A study published in the US CDC’s Emerging Infectious Diseases journal describes in-flight transmission of SARS-CoV-2 among passengers on a flight from Dubai, UAE, to Auckland, New Zealand—with a stop in Kuala Lumpur, Malaysia. Upon arrival in New Zealand, all passengers were subjected to mandatory 14-day quarantine, with testing conducted at approximately Day 3 and Day 12. Testing identified 7 SARS-CoV-2 infections among the passengers, including 5 that tested negative prior to their departure. Genomic analysis of specimens collected from each passenger found that the viral genome in 6 of the 7 passengers was identical, with 1 mutation present in the seventh passenger. Combined with the timeline of symptoms and positive tests, this suggests that the infection was transmitted among the passengers, rather than from multiple sources prior to travel. While testing negative prior to travel will likely decrease the number of imported cases, by denying travel for those who are already infectious, negative tests only indicate the current state of infection and cannot detect individuals who will be infectious after that point. Travel screening can mitigate the risk of importing cases or transmission during travel, but it cannot prevent them.
HIGH-TITER CONVALESCENT PLASMA A study published in The New England Journal of Medicine, conducted on behalf of the Fundación INFANT–COVID-19 Group, evaluated convalescent plasma with a high IgG titer as a COVID-19 treatment. The randomized, double-blind, placebo-controlled trial included 160 patients in Argentina aged 75 years or older or aged 65-74 years with at least 1 pre-existing condition associated with elevated risk of severe COVID-19 disease and death. The convalescent plasma used in the treatment group included “antibody concentrations in the upper 28th percentile,” and the study participants were divided equally between the treatment and placebo groups (80 in each). The treatment group exhibited a 48% relative reduction in risk of severe respiratory disease compared to the placebo group—13 patients (16%) in the treatment group compared to 25 patients (31%) in the placebo group. Additionally, few patients in the treatment group died than in the placebo group, 2 (2%) compared to 4 (5%), but this result was not statistically significant. No adverse events were reported in either group.
LONG-TERM HEALTH EFFECTS Evidence continues to emerge on the many and varied long-term health effects of COVID-19. Research has already established correlation between COVID-19 disease and certain cardiac, respiratory, and neurological conditions, but it is still unclear for how long these “long COVID” symptoms may persist. A study published in The Lancet followed 1,733 recovered COVID-19 patients from Wuhan, China, who were initially recovered between January and May. Among these patients, 76% reported at least one symptom 6 months after their recovery, including muscle weakness or fatigue (63%), difficulty sleeping (26%), and hair loss (22%). Additionally, 23% of the participants reported anxiety or depression, and 27% reported persistent pain or discomfort. The odds of having persistent symptoms was statistically higher among participants with severe disease—i.e., requiring high-flow nasal cannula oxygen, non-invasive ventilation, or invasive mechanical ventilation—compared to patients who did not require any oxygen therapy (OR= 2.42). Data collection on “long COVID” patients must continue for the foreseeable future to track whether or when these symptoms resolve. The persistence of months- or years-long COVID-19 medical sequelae has significant implications for medical care and public health initiatives in the future, potentially long after the end of the pandemic.
DELIRIUM Mechanical ventilation has been previously associated with an increased risk of acute brain dysfunction, and a study published in Lancet: Respiratory Medicine investigated delirium and coma across critically ill COVID-19 patients. The study included 2,088 adult COVID-19 patients across 69 intensive care units (ICUs) across 14 countries. Patients with a history of mental health issues, neurological conditions, drug overdose, brain damage, blindness, and deafness were excluded. Within the cohort, 1,397 of patients were mechanically ventilated during the same day of ICU admission, and an additional 430 patients were mechanically ventilated at some other time during hospitalization. The researchers evaluated risk factors associated with coma or delirium within 21 days of ICU admission. Invasive mechanical ventilation and the use of restraints as well as the prescription of benzodiazepine (sedative), opioids, vasopressors, or antipsychotic medications were significantly associated with increased risk of delirium the following day. Notably, family visitation, whether in-person or virtual, was significantly associated with a lower risk of delirium (OR= 0.73). The researchers recommended that clinicians avoid continuous infusions of benzodiazepine and use alternative options for sedation. Authors also recommended that care providers arrange safe and appropriate family visitation, either in person or virtually.
mRNA VACCINE PLATFORM Following the success of the mRNA platform used in its SARS-CoV-2 vaccine, Moderna announced that it is expanding its mRNA vaccine development efforts. The 3 new programs will leverage the mRNA technology, successfully demonstrated to be effective in combating SARS-CoV-2, for other pathogens. Moderna will be expanding its research portfolio with 3 mRNA vaccine efforts for seasonal influenza, 2 for HIV, and 1 for Nipah virus, and it already has ongoing mRNA vaccine development efforts for a number of other pathogens. Beyond vaccines, Moderna is also expanding its mRNA research for therapeutics.
ponchi101 wrote: ↑Tue Jan 12, 2021 8:46 pm
Great. Did you get your shot too? I saw in the news that people with co-morbidities under 65 can get the vaccine as a priority.
Not that I mind that I don't have any comorbidities, but that will mean that I am pretty much at the end of the line.
Down here: The Colombian GOV has acknowledged that legal residents will be treated in the same fashion as Colombian citizens. So the GF and I are in the list. Whenever that starts.
They are doing 75+ only right now.
by ti-amie I'm glad to. hear about your mom shtexas. NY dropped the age to 65.
by Suliso
by Suliso I think these data from Israel are very important. About 50-60% reduction in covid infections in elderly patients 2-3 weeks after the FIRST shot (nothing after a week). This is from almost million patients (Pfizer clinical trials had ca 9,000 in that age group).
by ponchi101 Everything seems to be pointing to the vaccine being the sole solution. That article is very useful explaining why.
Hidden in there, also an interesting fact: EVERYBODY in Israel has a health provider, making it easier to gather stats and deliver the vaccine. A big plus for centralized health systems, as an argument to hold when you talk to those that oppose such schemes.
by atlpam In the meantime, international travel requires a negative Covid test within 72 hours of travel, but try and find someplace to get a test that will guarantee you will have your results within that time period.
by ponchi101 Here that is going well. My brother in law needed one to go back home (Peru) and we got a test on Saturday Jan 2nd, and he flew on Jan 3rd. And it seems there is a place really close by where you can get an antigen test in 4 hours.
Plus there is a company that gets you the test at the airport. But he did not want to risk it that close to departure.
by meganfernandez Keys and Murray have Covid. Keys won't go to Australia but Murray is hoping he can show up a little late.
Sandgren revealed that he tested positive in November and the Victoria govt had to review his medical file to ensure he was sufficiently recovered. They cleared him to travel to Australia.
by ti-amie I saw a tweet saying he tested positive four days ago. TA is saying their people call the positive the result of "virus shedding".
by ti-amie
by ponchi101 Just lets be honest and shut down international travel. The UK banning entry from other countries is truly ironic.
Shutdown, for one month, and then people with proof of vaccination can start. Vaccination and/or that already caught it.
by meganfernandez
ti-amie wrote: ↑Thu Jan 14, 2021 7:48 pm
I saw a tweet saying he tested positive four days ago. TA is saying their people call the positive the result of "virus shedding".
ti-amie wrote: ↑Thu Jan 14, 2021 7:48 pm
I saw a tweet saying he tested positive four days ago. TA is saying their people call the positive the result of "virus shedding".
ti-amie wrote: ↑Thu Jan 14, 2021 7:48 pm
I saw a tweet saying he tested positive four days ago. TA is saying their people call the positive the result of "virus shedding".
Sandrgen or Murray tested positive 4 days ago?
Murray. Sandgren had it in November.
Or, looks like Sandgren
From a NY Times article:
The American Tennys Sandgren, ranked No. 50, flew to Australia despite a recent positive test. He received special clearance after health officials determined that he was not infectious, because he showed no symptoms and had previously tested positive for the virus in November. “Some people who have recovered from Covid-19 and who are noninfectious can continue to shed the virus for several months,” the tournament said.
by ti-amieExperts warn of vaccine stumbles ‘out of the gate’ because Trump officials refused to consult with Biden team
Even as covid-19 cases continue to overwhelm hospitals, the Trump administration has balked at close communication with its successor.
By
Laurie McGinley,
Amy Goldstein,
Lena H. Sun and
Isaac Stanley-Becker
Jan. 14, 2021 at 7:39 p.m. EST
The last time a presidential transition began during a national emergency — in 2008 amid the Great Recession — the outgoing Bush administration set aside partisanship to work closely with incoming Obama officials about how to deal with the economic collapse.
“Everyone was completely responsive to any question,” said Lawrence Summers, director of the National Economic Council under President Barack Obama. “They talked to us about major decisions.”
That smooth handoff is in stark contrast to what is happening now as President-elect Joe Biden prepares to assume power during a double-barreled crisis involving a lethal virus and its economic fallout that experts say demands close cooperation. Instead, as the coronavirus overwhelms U.S. hospitals and kills more than 3,300 people a day on average, the Trump administration has balked at providing access to information and failed to consult with its successors, including about distributing the vaccines that offer the greatest hope of emerging from the pandemic.
For more than a month, the Biden team pressed to attend meetings that offered “real-time information on production and distribution of vaccine” — important details for the president-elect’s advisers debating ways to bring the pandemic under control, said a transition official, speaking on the condition of anonymity to discuss private interactions.
While health agencies’ career staff have been helpful, it was not until this week that Biden officials were allowed to attend meetings of Operation Warp Speed, the administration’s initiative to accelerate vaccine development and distribution. They were also not invited to the two Warp Speed sessions this weekend when Trump officials decided on sweeping changes to try to speed up the sluggish vaccine rollout. Nor were they briefed on those changes in advance.
While some of those policies mirrored Biden plans, others raised red flags among the president-elect’s advisers. One is a recommendation to offer vaccines immediately to tens of millions under 65 who have high-risk medical conditions — a change the Biden team fears could overwhelm state supply and already stressed sign-up systems, while creating unrealistic expectations for those eager to get inoculated.
Another new policy, involving the controversial question of whether to penalize slower-moving states, was supposed to take effect the week after Biden becomes president. State officials said they were uncertain about whether to take the new policy seriously or to brush it off because it seemed to lack support from the incoming administration.
But on Thursday, Connecticut Gov. Ned Lamont (D) tweeted that federal officials had notified the state that it would receive an additional 50,000 doses next week “as a reward for being among the fastest states” to get shots into arms. West Virginia, meanwhile, which is moving at the fastest clip based on Centers for Disease Control and Prevention data, did not get any additional doses, said Holli Nelson, a spokeswoman for the state’s National Guard. A Health and Human Services spokesperson did not immediately respond to a request for comment.
The Biden transition official also said it took the transition team several weeks to get access to Tiberius, a data system that would have helped officials understand earlier “where vaccine is going, which states are ordering, when it is moving.”
“Look, we are still prepared to meet our goal of 100 million shots in 100 days,” the official said, referring to a commitment Biden made in early December. “But it would have been a lot more helpful if we’d had access to real-time information.”
On Thursday afternoon, another senior Biden official described “uneven cooperation” from the Trump administration. He spoke on the condition of anonymity in advance of Biden’s speech Thursday night calling on Congress for an additional $400 billion to fight the pandemic, including $20 billion for a national vaccination program.
The lack of coordination has alarmed public health officials and experts on presidential transitions, especially as a more contagious virus variant first identified in Britain spreads across the United States and the CDC projects as many as 477,000 covid-19 deaths by Feb. 6.
The dearth of coordination “means we are stumbling out of the gate with the vaccine,” said Douglas Brinkley, a presidential historian at Rice University. “We are failing at a government level on distribution because there is no game plan. There is a chaotic Trump one and a learning-curve Biden one.”
The decision to urge states to immediately vaccinate a much larger pool of people — about 81 million between the ages of 16 and 64 with high-risk medical conditions — was “absolutely inappropriate,” said Michael Osterholm, a member of Biden’s covid-19 advisory board and director of the Center for Infectious Disease Research and Policy at the University of Minnesota.
“When you make a recommendation that … far exceeds the number of doses that are available for the foreseeable future, that’s not helpful,” Osterholm said. “It only creates confusion, frustration, and frankly, a lack of trust in the system.”
HHS Secretary Alex Azar and other Warp Speed officials said they made the decision to dramatically increase eligibility because too many doses are sitting in freezers and they have greater confidence in a reliable supply of vaccines.
A senior Trump official denied there was any effort to keep Biden in the dark about Warp Speed activities. The official, who spoke on the condition of anonymity to discuss internal deliberations said that while Biden officials have only recently been invited to Warp Speed meetings, they have been regularly briefed on what has been discussed.
The official said it was not appropriate for the Biden team to take part in making decisions because the United States has “one government at a time.” He added that when Biden becomes president, “they can change everything if they want.”
In a statement, an HHS spokesman said the agency “is committed to smooth, professional transition planning" and has been holding briefings with the Biden team as needed.
Tensions between incoming and outgoing administrations aren’t unusual — the post-election period between Democrat Harry S. Truman and Republican Dwight D. Eisenhower in the early 1950s was especially acrimonious, for example. But it’s hard to imagine a transition more fraught than this one, with a president raging against the election results as a deadly pandemic spreads out of control.
“It’s a very bad TV show that I would stop watching because it is so unbelievable,” said Howard Markel, a medical historian at the University of Michigan.
The transition initially was stalled when the General Services Administration, headed by a Trump appointee, refused to recognize Biden’s victory and provide funding to his transition team. The GSA administrator reversed course on Nov. 23. But even when Trump career officials were told they could talk to the Biden team, they were permitted to share only publicly available information, said an administration health official who spoke on the condition of anonymity to discuss internal matters. “After that, we could share nonpublic information, but it had to be cleared first.”
Even if the Trump team chose not to cooperate with Biden in some areas, there should have been a free flow of information on vaccines, said the Trump health official, who compares the current crisis to a war. “The pandemic should have been a DPZ — depoliticized zone,” he added.
Brinkley shared that view. “Operation Warp Speed should be deeply bipartisan,” with a constant exchange of information, he said. “The fact that has not been happening with Trump is because he’s called it a fraudulent election. Why would I give data to somebody who is a fake president-elect?”
Max Stier, president and CEO of the Partnership for Public Service and an expert on presidential transitions, described handoffs of power as a relay race in which runners have to pass the baton. “You run side by side as fast as possible so you can win,” he said. “You don’t want it to be a start-and-stop strategy, you want it to be a smooth handoff.”
“Because your decisions might only last for another week, there should be an alignment” with the incoming administration, he added.
Despite the challenges, Biden and his team have scooped up extensive information about coronavirus vaccine production and distribution from long-standing contacts in pharmaceutical companies and federal agencies. And they have gotten information through back channels from career staff working “off the clock” and using personal email accounts.
Jeffrey P. Koplan, a former director of the CDC, said it was “shocking” that members of the outgoing administration hadn’t involved Biden’s team in their decision-making.
“It’s not rocket science — it’s been done before,” said Koplan, who was head of the CDC under both Bill Clinton and George W. Bush.
There also was much more discussion and cooperation in prior transitions on a range of health issues, said Nicole Lurie, who is advising the Biden team, participated in the Obama transition and later served as Obama’s assistant secretary for preparedness and response at HHS.
“I knew the person who had been in the role before me, we had a period of overlap, and there was just a lot of information-sharing,” Lurie said. “It’s nowhere near as complicated as it is now.”
While the Bush-Obama handoff is often cited as a model, a well-functioning transition has been regarded by leaders of both parties as an important goal until very recently, according to former administration officials and historians.
Through most of the 20th century, outgoing and incoming presidents were occasionally antagonistic, such as in the transition between Herbert Hoover and Franklin D. Roosevelt in the early 1930s, Brinkley said. Yet even in those times, it was thought that “the crown jewel of American democracy is the smooth transition. You go out for political combat for two years” until the election, followed by a seamless transition, he said.
Partisanship intensified in the 1990s, he said. But even after the 2000 election, which was contested for more than a month before being decided by the Supreme Court, Bill Clinton’s staff provided the George W. Bush team with intelligence data on al-Qaeda and other terrorist groups. That occurred before it was clear that Bush — not Clinton’s vice president, Al Gore — would be the next president, Brinkley noted.
Recalling the drawn-out election battle, Summers, who in 2000 was Clinton’s outgoing treasury secretary, said, “We didn’t think what happened was fair or legitimate. But it didn’t occur to anyone to not concede, or to not work with the transition once the Supreme Court ruled.”
Said Brinkley: “It used to be seen as anti-American not to have a smooth transition.”
by Togtdyalttai California announced yesterday that it's allowing seniors 65+ to get the vaccine now. However, our counties aren't exactly stock full of vaccine. There's two places in San Diego that I know of which are giving out vaccine to people 65+, the grocery store Ralph's and UC San Diego. I tried to get an appointment at Ralph's for my mom (gracie on TAT1) but there's none to be had, and she's not a patient in UC San Diego's health system so I doubt she can get in. I have a feeling the situation won't change much in the near future.
by shtexas
Togtdyalttai wrote: ↑Fri Jan 15, 2021 4:24 am
California announced yesterday that it's allowing seniors 65+ to get the vaccine now. However, our counties aren't exactly stock full of vaccine. There's two places in San Diego that I know of which are giving out vaccine to people 65+, the grocery store Ralph's and UC San Diego. I tried to get an appointment at Ralph's for my mom (gracie on TAT1) but there's none to be had, and she's not a patient in UC San Diego's health system so I doubt she can get in. I have a feeling the situation won't change much in the near future.
Try UC San Diego anyway. See if you can open a patient portal for her and then request an appointment. One hospital system here is now allowing that.
by Liamvalid We're still in full lockdown in the UK, only essential stores that sell food allowed to open until the end of Feb. We are getting the vaccine rolled out pretty quickly though. My team at work have all been for their first dose (I was a volunteer for the Oxford vaccine last year and have just been unblinded-I did have the vaccine and not the placebo). I work for the NHS so am still working at the moment but with the weather being so crap i'm quite happy staying home on lockdown after work. Hope all you guys are safe and healthy
by Suliso We're moving to a stronger form of lockdown here in Switzerland from Monday, also till the end of February. No chance of me getting a vaccine anytime soon as I'm not in any kind of risk/preferred category. I'm a research scientist, but not directly involved in lab work anymore so I go to the office only once per week. My team working on site full time, though. So far lucky - no one I know has caught the virus in a bad way. Not that worried about myself, more about parents back in Latvia who're in their seventies now and not able to lock down completely either. And of course the life is really boring now, but I guess that's better than being ill...
by ponchi101 Strange news from back home (Venezuela).
A friend of the GF had a niece that gave a Bday party (I know, the story already starts with the wrong foot). The friend did not go because he thought it was irresponsible. So, as expected, somebody had the virus and spread it. The entire family had to be tested and went into quarantine.
To their surprise, three of the younger cousins showed they had had the virus a while back. None ever showed any symptoms. A reminder that a lot of people get it and are asymptomatic. This virus is insane.
Bogota is under curfew until Monday. Business to open again, but only some categories. I at the stage in which I want to get an antibody test just to see if by any chance I got it and was asymptomatic too. I am pretty good with flus and colds (seldom get them) so that chance is there.
by dryrunguy Here's the Situation Report released today. Mostly about incidence updates and international vaccination efforts. But while skimming it quickly, one paragraph really jumped out at me.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 91.49 million cases and 1.98 million deaths as of 7am EST on January 15.
Despite initial concerns about public health and healthcare infrastructure in many countries, the continent of Africa continues to represent a small fraction of the global daily COVID-19 incidence. But while many African countries have demonstrated prolonged success in terms of containing COVID-19, daily incidence and mortality in Africa have been increasing sharply since early December. Daily incidence has increased by nearly 150% and daily mortality has more than tripled since December 1.
As a whole, Africa’s daily incidence has increased 36% over the past 2 weeks, but this trend is not consistent across all countries. Much of the recent surge has been focused geographically in the southern part of the continent as well as the coastal portion of West Africa. In total, 23 countries have reported increases in daily incidence of more than 50% over the past 2 weeks. Excluding the island nations, all but 4 of these—Burundi, Chad, Sudan, and Tanzania—are located in the South or West regions of Africa. The countries reporting steady or declining daily incidence over the past 2 weeks are more evenly distributed geographically, with 12 of the 16 located in the East, Central, and North regions; 2 in the South region; and 2 in West Africa.
At the highest end of the scale, 11 countries in Africa have reported increases in daily incidence of more than 300% over the past 2 weeks, including São Tomé and Principe at 3,400% and Liberia at 1,533%. São Tomé and Principe is currently reporting only 12 new cases per day, and Liberia is reporting 14; however, the drastic proportionate increase over the past several weeks is certainly cause for increased attention. While it is actually near the middle of African countries in terms of the relative change in daily incidence, South Africa (46% biweekly increase) continues to represent the majority of the daily incidence in Africa. South Africa is currently reporting 18,031 new cases per day, approximately 56% of the continent’s daily total. In terms of total daily incidence, Tunisia is #2 (2,663; 37% biweekly increase) and Nigeria is #3 (1,363; 57% increase). On a per capita basis, Seychelles is #1 in Africa with 369 daily cases per million population (587% increase), followed by South Africa (304) and Tunisia (225). In total, 24 African countries are reporting fewer than 5 new daily cases per million population, including 10 with fewer than 2.
UNITED STATES
The US CDC reported 22.97 million total cases and 338,351 deaths. Since January 8, the average US daily incidence has hovered between 240-250,000 new cases per day, and it appears as though the daily incidence could be leveling off to some degree. Looking at the monthly average, which smooths out some of the effects of delayed holiday reporting, the US could be approaching a peak or plateau. That being said, it has been less than 3 full weeks since the Christmas holiday weekend and less than 2 weeks since the New Year’s holiday weekend, so we are likely not yet seeing the full effects of holiday travel and gatherings on the national scale.
On January 12 and 13, the US reported 4,131 and 4,096 deaths, respectively. These are the second and third highest daily totals to date*, and this is the first time since the onset of the pandemic that the US reported more than 4,000 deaths on consecutive days. The current average daily mortality (3,357 deaths per day) is 17.5% higher than the peak of the initial US surge in April, and the average mortality has remained higher than the initial peak for 6 consecutive days. The US reported 23,502 new COVID-19 deaths in the past week, which exceeds the estimated 22,000 seasonal influenza deaths for the entire US 2019-20 influenza season. If the US is, in fact, approaching a peak or plateau in terms of daily incidence, we can expect mortality to continue increasing for at least the next 2-3 weeks.
*With the exception of April 15, when New York City reported more than 3,700 previously unreported probable deaths from the onset of its epidemic.
The US CDC reported 30.63 million vaccine doses distributed and 11.15 million doses administered (36.4%), including 1.23 million administered in long-term care facilities (LTCFs). The CDC vaccine tracker now includes data on the total number of people who have received at least 1 dose (9.69 million) and those who have received 2 doses of the vaccine (1.34 million people). These data are also available at the state level. The CDC also added a breakdown of the administered doses by manufacturer, with 6.53 million doses of the Pfizer/BioNTech vaccine and 4.62 million doses of the Moderna vaccine.
The Johns Hopkins CSSE dashboard reported 23.36 million US cases and 389,581 deaths as of 12:30pm EST on January 15.
VACCINE TRIALS & AUTHORIZATION On January 12, the European Medicines Agency (EMA) received the conditional marketing application for AstraZeneca/Oxford University’s SARS-CoV-2 vaccine. A press release from the EMA indicated that the application “will proceed under an accelerated timeline,” with the EMA issuing its recommendation as early as January 29. The short timeline is possible as a result of the EMA’s rolling review process, which enabled EMA officials to evaluate interim Phase 3 clinical trial data as they became available.
Additional reports of clinical trial results for the vaccine candidate developed by Sinovac (China) continue to emerge. Researchers conducting Phase 3 clinical trials conducted in multiple countries have reported varying levels of efficacy over the past several weeks. Previously, researchers in Turkey reported 91%, Brazil reported 78% efficacy, and Indonesia reported 65%. Multiple news media reports indicate that, earlier this week, researchers from Brazil’s Butantan Institute released new efficacy analysis that is considerably lower than previous estimates. The newest results estimate the Sinovac to be 50.4% efficacious at preventing COVID-19 disease. While this is still above the generally accepted threshold for a successful vaccine, it is much lower than the estimates for other vaccines currently in use, and the inconsistency in the Sinovac trial results, coupled with relatively low value in the most recent results, has raised concerns. Notably, the individual clinical trials utilized their own study designs, so the efficacy estimates may not be directly comparable between trials. To our knowledge, neither the full datasets nor peer-reviewed analysis have been published for any of the Phase 3 trials of the Sinovac vaccine. Following the announcement, officials in Malaysia and Singapore reportedly indicated that more data would be required before finalizing existing purchase agreements.
Researchers conducting clinical trials for the Johnson & Johnson (J&J)/Janssen candidate SARS-CoV-2 vaccine published interim Phase 1/2a trial data in The New England Journal of Medicine (NEJM). The early-stage trials demonstrated that the J&J/Janssen vaccine generated neutralizing antibody response in 90% of participants after 29 days and in 100% after 57 days, and the vaccine exhibited an acceptable safety profile. This is encouraging news, but Phase 3 trial data will be important in terms of assessing the vaccine’s efficacy. The Phase 1/2a trials consisted of only 805 participants, but officials from J&J indicated that the results from much larger Phase 3 trials could be released by the end of January. In contrast to the vaccines already in use, the J&J/Janssen vaccine requires only a single dose, which could be an important tool in speeding vaccination efforts. A report published in The New York Times indicated that existing production capacity for the J&J/Janssen vaccine has not met the expected timeline, potentially 2 months behind schedule, which could slow its initial release once authorized for use.
INTERNATIONAL VACCINATION
EUROPE
Earlier this week, UK Prime Minister Boris Johnson announced that vaccination operations will be conducted around the clock. He also indicated that vaccine production and supply are the biggest barriers currently, as opposed to vaccine administration. Public Health England reported that more than a third of adults aged 80 years and older in England have received at least 1 dose of the SARS-CoV-2 vaccine.
In Spain, record snowfall across the central region of the country reportedly delayed vaccination distribution and operations. Approximately, 350,000 doses of the Pfizer/BioNTech vaccine arrived this week at airports across the country, but the inclement weather resulted in the doses destined for Madrid to be diverted to the northern city of Vitoria. A senior government health expert indicated that he expected the overall impact to be limited in terms of the total doses administered, but future plans will need to be adapted to increase efforts in the affected areas. According to the Ministry of Health, Spain has administered approximately 60% of its 1.13 million doses.
To aid vaccine rollout in Germany, mass vaccination sites are being established in sports venues and concert halls, with the aim of establishing national capacity to administer 300,000 doses per day. Many of these facilities remain empty, however, as long-term care facilities remain the priority. Like many other countries, Germany’s vaccination effort has experienced delays. In the first 2 weeks of the vaccination campaign, only 533,000 doses were administered, approximately 40% of the 1.3 million doses it received. Germany is expected to receive 5.3 million doses of the Pfizer/BioNTech vaccine by mid-February as well as another 2 million doses of the Moderna vaccine by the end of March. Additionally, Germany is in the process of establishing new production facilities and converting existing facilities to manufacture various SARS-CoV-2 vaccines, some of which could be operational in the coming weeks.
AFRICA
The African Vaccine Acquisition Task Team announced that it has provisionally secured access to 270 million doses for African countries, including 50 million that are expected to be available by June. The allotment will include doses from multiple manufacturers, including AstraZeneca (via the Serum Institute in India), Pfizer, and Johnson & Johnson. These efforts are intended to supplement the doses provided through COVAX, which may only be enough to cover frontline healthcare workers. Acquiring enough doses is a financial concern for many African countries, and the Africa CDC director has encouraged countries with surplus supply to donate to countries in need to supplement the efforts of COVAX and Gavi to support 92 low- and middle-income countries, more than half of which are in Africa.
South Africa reportedly expects to receive 1 million doses of the AstraZeneca/Oxford University vaccine in January, with another 500,000 doses in February, manufactured by India’s Serum Institute. This total is expected to cover approximately half of South Africa’s Phase 1 priority group, frontline healthcare workers (1.25 million). Phase 2 will expand eligibility to other essential workers, individuals living in congregate settings, adults aged 60 and older, and those with underlying health conditions. The AstraZeneca/Oxford vaccine is not currently authorized for use in South Africa, but regulatory officials will reportedly leverage the authorizations in other countries (e.g., UK, India) to permit the emergency use of an unregistered product. According to a report published in The Wall Street Journal, no vaccine manufacturers have yet filed applications for any kind of authorization; but this may not necessarily delay the vaccines’ availability for use in South Africa.
ASIA
Indonesia reportedly initiated its SARS-CoV-2 vaccination campaign after receiving shipments of China’s Sinovac vaccine. Indonesia will prioritize its frontline healthcare workforce (approximately 1.5 million people), largely due to high COVID-19 mortality among this group. Like other countries, Indonesia is facing challenges regarding vaccine hesitancy and opposition, including among healthcare workers, particularly in light of the recent Phase 3 clinical trial results from Brazil. Indonesian President Joko Widodo publicly received his vaccination this week in an effort to bolster community support. We have not identified a definitive list of priority groups for Indonesia, but new media outlets have reported multiple different strategies, including healthcare workers, older individuals, and younger individuals. Several news media reports indicate that social media “influencers” are among the highest priority groups. While many of these individuals are younger and at lower risk for severe COVID-19 disease and death, Indonesia hopes this approach can help build support for vaccination among the public and mitigate the effects of vaccine hesitancy and opposition.
China is also establishing large mass vaccination sites in an effort to scale up vaccine administration capacity. A recent surge in transmission—which has prompted regional “lockdowns,” including in Beijing—is a driver of the increased vaccination efforts. Concerns regarding the efficacy of Chinese-developed vaccines, as well as the lockdowns themselves, could be posing barriers to vaccination; however, analysis by Reuters indicates that China’s vaccination program is scaling up rapidly, surging from 1.5 million doses administered from July-November 2020 to 10 million doses as of January 13.
OCEANIA
Australia and New Zealand have both demonstrated the ability to effectively contain their respective COVID-19 epidemics. Considering their success in limiting transmission, both countries are reportedly delaying their vaccination campaigns until mid-to-late February. This extra time will allow health and regulatory officials to gather more information on the efficacy and safety of the various SARS-CoV-2 vaccines and vaccine candidates. Additionally, the delay will provide both countries an opportunity to better prepare their distribution plans.
In Australia, the government has announced that they plan to administer the Pfizer vaccine candidate to their highest priority groups and largely use the AstraZeneca/Oxford vaccine for the broader population. The rationale for this decision seems to be based on the anticipation that Australia will receive the Pfizer vaccine first, but that the AstraZeneca/Oxford vaccine will be manufactured domestically. The Australian first priority group includes, quarantine and border workers, frontline health care workers, and long-term care facility residents and workers, which could include approximately 700,000 people. The Australian government aims to vaccinate 80,000 people per week initially, with the goal of covering the entire country’s population by the end of 2021, using community partners like drug stores. In New Zealand, Prime Minister Jacinda Ardern announced plans to vaccinate the country’s entire population (5 million), largely in the second half of 2021. New Zealand could begin with border control personnel and first responders in the spring, and it will prioritize areas with ongoing COVID-19 outbreaks, including healthcare workers, household contacts, and the general public in affected areas. New Zealand has actually developed phased vaccination priority groups for 3 different scenarios, based on the level of community transmission.
US VACCINE PRIORITIZATION Last week, the incoming Biden Administration announced that it intends to make nearly all of the existing US SARS-CoV-2 vaccine inventory available to states, rather than the current plan of reserving vaccine to ensure availability for second doses. Following the release of the Biden Administration plan, US Secretary of Health and Human Services Alex Azar announced that the federal government will begin distributing the remaining reserve inventory to states even before President-Elect Biden takes office. Secretary Azar also recommended that states expand eligibility to all adults aged 65 and older as well as adults under the age of 65 with underlying health conditions that could put them at risk for severe COVID-19 disease or death. As part of this recommendation, the federal government will allocate doses to states based on their respective populations aged 65 and older. Secretary Azar argued that some states’ strict adherence to limited initial priority groups has slowed vaccinations and that the new policy would speed progress.
The sudden policy shift, with little warning and little financial or operational support for state and local officials responsible for implementing mass vaccination campaigns, has raised concerns among some experts. States are already conducting vaccination operations using their own priority groups—with substantial variation from state to state—some of which have caused confusion among the public regarding who is eligible or how to get vaccinated. Notably, this bulk expansion could include approximately 150 million adults nationwide, nearly half of the entire US population, all at once. Current production estimates project that the US could have 200 million doses available by the end of March; however, this is only enough to provide 2 doses for 100 million people, well short of the eligible population.
The new policy also deviates from the most recent guidance from the CDC’s Advisory Committee on Immunization Practices, which recommends expanding to adults aged 75 and older and essential workers in Phase 1b—approximately 49 million people. Under the ACIP plan, adults aged 65 and older and adults with underlying health conditions would be included in Phase 1c. The absence of essential workers (e.g., those who cannot work remotely) from the new HHS guidance could delay vaccination for those who are most likely to be exposed, many of whom are racial and ethnic minorities who have been disproportionately affected during the pandemic. The change to expand eligibility more broadly does align with comments from some experts, who argue that the complex eligibility requirements from ACIP were too difficult to implement and could slow vaccination progress, but this is not necessarily the only consideration in terms of establishing priority groups. At this point, it is unclear how states will respond to the new recommendations.
US CDC TRAVEL & TESTING REQUIREMENTS The US has implemented COVID-19-related travel advisories and restrictions for most countries around the world (including the US itself) for many months, but it recently updated screening and testing requirements for inbound travelers. The new policy, which takes effect on January 26, requires all airline passengers arriving from another country to have a negative SARS-CoV-2 test or documentation of prior infection before they are permitted to enter the US. The negative test must be administered within 3 days of the flight’s departure, and in order to document prior infection, travelers must provide both the test results and a written letter from a licensed healthcare provider that attests to the traveler’s recovery. The new order supersedes a similar order issued in December that applied only to travelers arriving from the UK. The order explicitly addresses the emerging B.1.1.7 variant, although not by the lineage nomenclature, which provides indication that the new travel restrictions aim to limit the introduction of new, more transmissible variants to the US.
The B.1.1.7 variant has already been detected in numerous US states, including in individuals with no recent international travel. In particular, the variant was recently identified in a patient in New York state, which prompted New York City Mayor Bill de Blasio to call for a complete ban on travel from the UK. Notably, prohibiting travel from other countries will not prevent the introduction to the US, particularly because it is already circulating to some degree among the general public. With the advance warning from the UK and other countries, it is critical to use any time gained by the new testing requirements to expand surveillance capacity capable of detecting the emerging variants (e.g., genomic sequencing) before the variant is widespread. Additionally, recommended public health measures—including enhanced hygiene, physical distancing, and mask use—will be important tools to mitigating community transmission and limiting the impact of emerging variants on the public’s health as vaccination efforts continue to scale up.
EMA CYBERATTACK In December, the European Medicines Agency (EMA) was the victim of a cyberattack that targeted communications and data related to its SARS-CoV-2 vaccine evaluation and authorization process. The EMA immediately initiated an investigation to determine the extent of the breach and to identify the perpetrators. On January 12, the EMA issued an update indicating that some of the documents accessed during the attack had been published publicly on the internet. In an update issued today, the EMA reported that some of the leaked documents were altered prior to their publication. Notably, the update states that some of these correspondence were “manipulated by the perpetrators...in a way which could undermine trust in vaccines.” These deliberate efforts to spread disinformation are highly concerning, particularly in light of concerns about the existing level of hesitancy and opposition to the new SARS-CoV-2 vaccines. The statement makes it clear that the EMA and EU countries have not compromised in any way regarding the safety and efficacy of the vaccines available in Europe. The EMA is coordinating with law enforcement officials, and the investigation is ongoing.
VACCINATION INCENTIVES As vaccine eligibility in the US expands beyond Phase 1a to include members of the broader public, some employers are evaluating options that aim to encourage employees to get vaccinated once they become eligible. As we have covered previously, there are growing concerns regarding the level of hesitancy and opposition to SARS-CoV-2 vaccination, in the US and around the world. In an effort to combat vaccine hesitancy and opposition, some businesses are offering incentives for those who get vaccinated. For example, a hospital system in Houston, Texas, is reportedly offering employees a US$500 bonus if they get vaccinated. Similarly, Dollar General, which operates a national chain of retail stores, is offering its employees 4 hours’ pay to enable them to get vaccinated. As opposed to a bonus-style payment, this effort aims to allow employees who earn hourly wages the ability to take time off of work in order to get vaccinated without negatively impacting their income. Some experts and elected officials have proposed similar programs that would pay all individuals who get vaccinated, but none have yet come to fruition, at least not in the US.
Some experts have raised concerns about these kinds of payments, noting that they could be viewed as efforts to coerce individuals because the vaccines are risky or dangerous, which can feed existing anxiety and concern in others. The use of financial incentives could “unfairly tak[e] advantage of those...who have lost jobs, experienced food and housing insecurity, or slipped into poverty during the pandemic” and who may then view vaccination as a necessity “in order to...purchase food or pay rent.” The prospect of financial payment or other incentives could also potentially lead some individuals to deliberately delay vaccination in hopes of future compensation.
Togtdyalttai wrote: ↑Fri Jan 15, 2021 4:24 am
California announced yesterday that it's allowing seniors 65+ to get the vaccine now. However, our counties aren't exactly stock full of vaccine. There's two places in San Diego that I know of which are giving out vaccine to people 65+, the grocery store Ralph's and UC San Diego. I tried to get an appointment at Ralph's for my mom (gracie on TAT1) but there's none to be had, and she's not a patient in UC San Diego's health system so I doubt she can get in. I have a feeling the situation won't change much in the near future.
Try UC San Diego anyway. See if you can open a patient portal for her and then request an appointment. One hospital system here is now allowing that.
UC San Diego doesn't allow you to make an appointment. They're only "inviting" people to come get a vaccine. Maybe I'm too skeptical, but it seems to me like it would be a great system to allow for rampant corruption.
by ti-amieVaccine reserve was already exhausted when Trump administration vowed to release it, dashing hopes of expanded access
States were anticipating a windfall after federal officials said they would stop holding back second doses. But the approach had already changed, and no stockpile exists.
by
Isaac Stanley-Becker and
Lena H. Sun
Jan. 15, 2021 at 1:06 p.m. EST
When Health and Human Services Secretary Alex Azar announced this week that the federal government would begin releasing coronavirus vaccine doses held in reserve for second shots, no such reserve existed, according to state and federal officials briefed on distribution plans. The Trump administration had already begun shipping out what was available beginning at the end of December, taking second doses directly off the manufacturing line.
Now, health officials across the country who had anticipated their extremely limited vaccine supply as much as doubling beginning next week are confronting the reality that their allocations will remain largely flat, dashing hopes of dramatically expanding access for millions of elderly people and those with high-risk medical conditions. Health officials in some cities and states were informed in recent days about the reality of the situation, while others are still in the dark.
Because both of the vaccines authorized for emergency use in the United States are two-dose regimens, the Trump administration’s initial policy was to hold back second doses to protect against the possibility of manufacturing disruptions. But that approach shifted in recent weeks, according to the officials, who spoke on the condition of anonymity because they were not authorized to discuss the matter.
These officials were told that Operation Warp Speed, which is overseeing the distribution of vaccines, stopped stockpiling second doses of the Pfizer-BioNTech vaccine at the end of last year. The last shots held in reserve of Moderna’s supply, meanwhile, began shipping out over the weekend.
The shift, in both cases, had to do with increased confidence in the supply chain, so that Operation Warp Speed leaders felt they could reliably anticipate the availability of doses for booster shots — required three weeks later in the case of the Pfizer-BioNTech product and four weeks later under Moderna’s protocol.
But it also meant there was no stockpile of second doses waiting to be shipped, as Trump administration officials suggested this week. Azar, at a Tuesday briefing, said, “Because we now have a consistent pace of production, we can now ship all of the doses that had been held in physical reserve.” He explained the decision as part of the “next phase” of the nation’s vaccination campaign.
Those in line for their second shots are expected to get them on schedule since states are still getting regular vaccine shipments. But state and local officials say they are angry and bewildered by the shifting directions and changing explanations of supply.
The health director in Oregon, Patrick M. Allen, was so disturbed that he wrote Azar on Thursday demanding an explanation. “Earlier today, we became concerned when we discovered there were no additional doses available for allocation,” he said in the letter, which was reviewed by The Washington Post.
On a call with Perna earlier the same day, Allen wrote, the four-star Army general had “informed us there is no reserve of doses, and we are already receiving the full allocation of vaccines.”
“If true, this is extremely disturbing, and puts our plans to expand eligibility at grave risk,” Allen added. “Those plans were made on the basis of reliance on your statement about “releasing the entire supply” you have in reserve. If this information is accurate, we will be unable to begin vaccinating our vulnerable seniors on Jan. 23, as planned.”
HHS spokesman Michael Pratt confirmed in an email that the final reserve of second doses had been released to states for order over the weekend but did not address Azar’s comments this week, saying only, “Operation Warp Speed has been monitoring manufacturing closely, and always intended to transition from holding second doses in reserve as manufacturing stabilizes and we gained confidence in the ability for a consistent flow of vaccines.”
He also said states have ordered only about 75 percent of what is available to them.
Azar’s comments followed a Jan. 8 announcement by President-elect Joe Biden’s transition team that his administration would move to release all available doses, rather than holding half in reserve for booster shots. Biden’s advisers said the move would be a way to accelerate distribution of the vaccine, which is in short supply across the country.
When Azar embraced the change four days later — after initially saying it was shortsighted and potentially unethical to put people at risk of missing their booster shots — he did not say the original policy had already been phased out, or that the stockpile had been exhausted. Signaling to states that they would soon see expanded supply, he also urged them to begin vaccinating adults 65 and older and those under 64 with a high-risk medical condition. Officials in some states embraced that directive, while others said suddenly putting hundreds of thousands of additional people at the front of the line would overwhelm their capacity.
In subsequent conversations with state and local authorities, federal officials sought to temper those instructions, said people who participated in the conversations. Gustave F. Perna, chief operating officer of Operation Warp Speed, spoke directly to officials in at least two of the jurisdictions receiving vaccine supply, explaining that allocations would not increase and that they did not have to broaden eligibility as they had previously been told, according to a health official who was not authorized to discuss the matter.
The revised instructions led additional jurisdictions to hold off on broadening their priority groups. One state health official noted that the updated eligibility guidance announced Tuesday did not appear on the website of the Centers for Disease Control and Prevention, even though it was stated as federal policy by Azar and by Robert R. Redfield, the CDC director, in their remarks earlier this week. Under the original recommendations, adults 65 and older and front-line essential workers were to comprise the second priority group, known as phase 1b, in line after medical workers and residents and staff of long-term care facilities.
But the issue of supply was most troubling to state health officials.
“States were shocked and surprised that they did not see an increase in their allocations, and when they asked for explanations, some of them were told there was not a large stockpile of second doses to draw from,” said an official working with numerous states on vaccination planning who spoke on the condition of anonymity to recount sensitive conversations. “They thought they were getting more doses and they planned for more doses and opened up to 65 and up, thinking they were getting more.”
In an email that reached some state officials on Friday morning, Christopher Sharpsten, an Operation Warp Speed director, called it a “false rumor” that “the federal government was holding back vaccine doses in warehouses to guarantee a second/booster dose.”
But it had been Azar who said Tuesday that “we are releasing the entire supply we have for order by states, rather than holding second doses in physical reserve.”
There was additional confusion. Another change Azar announced this week — making allocation of doses dependent on how quickly states administer them — would not take effect for two weeks, he said.
But Connecticut Gov. Ned Lamont (D) on Thursday tweeted that federal officials had notified the state that it would receive an additional 50,000 doses next week “as a reward for being among the fastest states” to get shots into arms. West Virginia, meanwhile, which is moving at the fastest clip based on CDC data, did not get any additional doses, said Holli Nelson, a spokeswoman for the state’s National Guard.
In a sign that the incentive structure may not be long-lived, a senior Biden transition official, speaking on the condition of anonymity to address ongoing deliberations, said this week the team did not look kindly on a system that “punishes states.”
by ti-amie Now we know why Tiny wouldn't share Covid info with the Biden transition team. There is no punishment too great for these people to be subjected to.
I wonder who the Wonder Boy sold it to and what his and Tiny's cut was.
Some are calling it incompetence. It's not that at all. It's criminals criming in plain sight.
by shtexas I went out to pick up some Chinese food and passed a Church with a packed parking lot. First, I shuddered thinking of all those people in one place. Then, I got angry. This is one of the reasons the numbers are rising.
by mmmm8
ponchi101 wrote: ↑Thu Jan 14, 2021 4:43 pm
Everything seems to be pointing to the vaccine being the sole solution. That article is very useful explaining why.
Hidden in there, also an interesting fact: EVERYBODY in Israel has a health provider, making it easier to gather stats and deliver the vaccine. A big plus for centralized health systems, as an argument to hold when you talk to those that oppose such schemes.
Those who oppose such schemes often oppose any centralized data gathering, and sometimes data
by patrick Local news said that Rebekah Jones was tested positive for Covid-19 today if I heard correctly. She is out on 2500 bond but do not know if any other conditions are attached.
by Togtdyalttai Whoever is responsible for this, we're already doing bad enough as a state in our vaccine rollout. Also, maybe it's not the worst thing that I couldn't get my mom an appointment yet.
California pauses Covid-19 shots from one lot of vaccine containing more than 330,000 doses
(CNN)Health officials in California are telling medical providers across the state not to administer doses from one lot of Moderna's coronavirus vaccine while they investigate possible severe allergic reactions last week in a number of people who got shots at a community vaccination clinic.
More than 330,000 doses from the lot were distributed to 287 providers across the state from January 5-12. Tens of thousands of doses may have already been administered, but the number of unused doses is unknown, according to Darrel Ng, a spokesperson for the California Department of Public Health.
CDPH said Sunday that fewer than 10 people at a clinic in San Diego who received Covid-19 shots from the lot required medical attention over the span of 24 hours. The state said it was not aware of anyone at any of the other 286 sites who had similar allergic reactions after receiving vaccine from the lot.
California's health department said it recommended pausing the entire lot, noting that there are not immediate replacement doses in addition to what had already been ordered.
"Out of an extreme abundance of caution and also recognizing the extremely limited supply of vaccine, we are recommending that providers use other available vaccine inventory," Dr. Erica Pan, California's state epidemiologist, said in the statement.
Moderna told CNN: "The company is fully cooperating with (the California Department of Public Health) in investigating these reported adverse events. Consistent with the statement from CDPH, at this point Moderna is unaware of comparable adverse events from other vaccination centers which may have administered vaccines from the same lot."
Dr. Paul Offit, director of the Vaccine Education Center at Children's Hospital of Philadelphia, said historically there is no such thing as a bad vaccine lot.
"The (US Food and Drug Administration) is generally so good at making sure that there is no lot-to-lot variation that you don't have a problem with so-called hot lots," he said.
State health officials didn't provide details on the symptoms associated with the allergic reactions but did provide a link to a US Centers for Disease Control and Prevention website about anaphylaxis -- a severe allergic reaction -- which can occur after getting a Covid-19 vaccine. Symptoms of anaphylaxis can include shortness of breath, low blood pressure, rapid heartbeat, dizziness and fainting. The CDC considers an allergic reaction to a Covid-19 vaccine to be severe if the person needs to be treated with epinephrine or must go to the hospital.
Offit, a top US vaccine expert who is a member of the FDA's vaccine advisory committee, said California's decision to hold back doses of vaccine carries its own risks, especially since allergic reactions can be monitored and treated and, in this case, they occurred at only one location.
"There are going to be people who either aren't getting this vaccine or aren't getting their second doses of vaccine, which then puts them at risk in a situation where we have a virus which is rapidly spreading in the country," Offit said. "There's going to be another probably roughly 100,000 people that die over the next couple of months, and among those people could be those who are not getting this vaccine because of quote-unquote 'an abundance of caution.'"
Thirty thousand doses from the lot were pulled from San Diego County's supply, according to the county. On Monday, Santa Clara County said in a statement that 21,800 doses from the lot had been allocated to the county, and that none of the doses had been administered.
California officials acknowledged the risk of a serious adverse reaction to the vaccine is small, noting that while less data exists for Moderna's vaccine, only approximately 1 in 100,000 people experience anaphylaxis with the similar Pfizer vaccine.
"The thing about anaphylaxis is although it is frightening to watch, it's easily identified, it's quickly identified, and it's easily treated with epinephrine," Offit said. "I don't see how taking this off the market is a conservative thing to do or exercising an abundance of caution. I think all it does is put people at risk unnecessarily." Vaccination sites are supposed to monitor people for side effects 15 minutes after they've been vaccinated. Sites are also required to have the means to treat a person for allergic reaction, if needed.
"None of the other places that used it had a problem. It was just one place. So do a careful examination of what was happening at that place," Offit added.
Officials said an investigation by the CDC, the US Food and Drug Administration, Moderna and the state is ongoing.
"We're not saying throw them away. We're not saying don't ever give them," Ng told CNN Monday, noting the state hopes to have an update this week.
California pauses Covid-19 shots from one lot of vaccine containing more than 330,000 doses
...
"There are going to be people who either aren't getting this vaccine or aren't getting their second doses of vaccine, which then puts them at risk in a situation where we have a virus which is rapidly spreading in the country," Offit said. "There's going to be another probably roughly 100,000 people that die over the next couple of months, and among those people could be those who are not getting this vaccine because of quote-unquote 'an abundance of caution.'"
Further up this topic (or maybe it was in TAT1.0' thread) this was talked about. If you are going to vaccinate 10 million people, the very next day you will have some of them dead, simply because of the stats. It is a huge number of people, and, currently, they are mostly elderly and people in high risk categories. So of course some of them will develop symptoms and reactions, which are not related to the vaccine.
You have to look at the overall numbers: do you let 10 people die because of some allergic reaction that may or may not be caused by the vaccine, or do you let 100K die because of the virus?
The lack of common sense is abysmal
I know. Personally, I could not care less as I have never suffered from any allergies. But it is a balance of your best chances. Take the vaccine, sit in the lobby if you have a history of allergies, and if you do have a reaction, get treated. Much better than ending up in the ventilator.
by shtexas Dallas is getting bad national press because the stats from the first few days of the vaccine roll-out at Fair Park (where I took my Mom) show it was the wealthier zip codes (North Dallas) that received the vaccine. The comments online are brutal because the articles make it sound like the vaccines were only available in North Dallas. But, Fair Park is not in North Dallas. The real problem is Dallas was not forthcoming with information on the vaccine. You had to go looking and know where and how to look. When I called pharmacies and the county, they were rude and not very informative. It was the internet and neighborhood communication apps that helped me. Many in South Dallas didn't have those resources, so they didn't know to come. This is like voting. You need to get boots on the ground to get the information out and get people signed up. It's a shame. I thought we were doing a good thing when they set the major hub up.
by JazzNU
ponchi101 wrote: ↑Tue Jan 19, 2021 2:29 pm
Further up this topic (or maybe it was in TAT1.0' thread) this was talked about. If you are going to vaccinate 10 million people, the very next day you will have some of them dead, simply because of the stats. It is a huge number of people, and, currently, they are mostly elderly and people in high risk categories. So of course some of them will develop symptoms and reactions, which are not related to the vaccine.
You have to look at the overall numbers: do you let 10 people die because of some allergic reaction that may or may not be caused by the vaccine, or do you let 100K die because of the virus?
The lack of common sense is abysmal
I know. Personally, I could not care less as I have never suffered from any allergies. But it is a balance of your best chances. Take the vaccine, sit in the lobby if you have a history of allergies, and if you do have a reaction, get treated. Much better than ending up in the ventilator.
Well I have a lengthy history of allergies almost since birth and an amazing (in a bad way) history of allergic reactions. And I can't wait to get the vaccine.
People are bugging. I read a story the other day and I think it was Dr. Ashish Jha who was talking about the vaccine warnings driving him a little bit crazy, because yes mention them, but don't focus them. That they've been underselling the vaccine and it's going to save your life and that should be the focus. I agree. I'll be taking it the moment I can. I absolutely might have an allergic reaction. Won't be the first or the last time. I'll get treated for the reaction as I always do if it's not something I can manage on my own. But honestly, Dr. Fauci mentioned this very early on in the discussion about the allergic reactions to the vaccine, most people like me who have allergic reactions to stuff, know how to deal with them on our own and he said, go to your appointment prepared to deal with an allergic reaction, be looking for it. Thanks for the warning. I will. Can't wait til my number is called.
by GlennHarman Ponchi is so right about the deaths after the vaccine. If we vaccinate thousands of people over the age of 80 who live in long-term-care facilities, a fair number of them will die soon after the vaccine. Of course, a fair number of them would have died during the same time without the vaccine. When one is doing a clinical trial on any treatment, this is the function of the control group when one is used. There are always "events" that will occur in both groups. You don't want a vaccine given 3 weeks ago to be blamed for a death in an automobile accident, as one sort of an extreme example.
Obviously, it is not good that those people are dying. But the risk of death from an allergic reaction should be very low, given the extensive trials that have been done. But that risk is precisely why people should "sit in the lobby...and if you do have a reaction, get treated." (quoting Ponchi)
by Suliso Israel has now reached 38% vaccination rate (first dose only). That means they must have mostly exhausted elderly and risk categories and are ready to start with general population. Of course all this is possible only because of their special deal with Pfizer.
by Suliso Purely statistically there is something else I'm wondering about. Very large percentage of fatalities (30-40%) have been from long term care facilities. Residents of such facilities statistically have only few more years of life left on average. Will we see significantly reduced death rates among elderly a year and two after the pandemic? Simply because a large percentage of most vulnerable will have died already in 2020 and 2021.
by ponchi101 You know it has been my main gripe about this pandemic: the lack of proper statistical analysis. The virus does not affect everybody in the same way. As you say, a large portion (perhaps even disproportionately large) of the deaths has come from those facilities you are talking about. People with underlying conditions and of a certain age. So yes, what you are saying will likely happen: the "strongest" of the elderly will see a reduction in death rates because the "weaker" ones will succumb to C19 in 2020/21.
I am also waiting for the total number of deaths worldwide in 2020 to be tallied. Generally, it should be about the same as 2019 PLUS 2 million from covid. If there is a large discrepancy, that will be an interesting study.
by ponchi101
Suliso wrote: ↑Fri Jan 22, 2021 12:52 pm
Israel has now reached 38% vaccination rate (first dose only). That means they must have mostly exhausted elderly and risk categories and are ready to start with general population. Of course all this is possible only because of their special deal with Pfizer.
Sorry. I missed that one. What special deal with Pfizer?
Meanwhile, here, the government is waiting to start in February. New roablock? They don't know if they have enough syringes for everybody. So they don't know when to start.
I mean, just START! Get the risk populations vaccinated. It is the typical mentality: trying to make it so perfect that then nothing gets done.
by Suliso
ponchi101 wrote: ↑Fri Jan 22, 2021 2:49 pmSorry. I missed that one. What special deal with Pfizer?
Meanwhile, here, the government is waiting to start in February. New roablock? They don't know if they have enough syringes for everybody. So they don't know when to start.
I mean, just START! Get the risk populations vaccinated. It is the typical mentality: trying to make it so perfect that then nothing gets done.
They get a preferential treatment in vaccine delivery in exchange for providing medical data exclusively to Pfizer and also they paid 50% more than others. Everyone in Israel will get this particular vaccine. From Pfizer's point of view they chose Israel as a testing ground (kind of phase IV trials) because of modest population (9 millions) and very centralized medical systems with everyone being insured and all data collected centrally.
by ti-amieDenmark is sequencing all coronavirus samples and has an alarming view of the U.K. variant
By
Michael Birnbaum and
Martin Selsoe Sorensen
Jan. 22, 2021 at 1:36 p.m. EST
Like a speeding car whose brake lines have been cut, the coronavirus variant first spotted in Britain is spreading at an alarming rate and isn’t responding to established ways of slowing the pandemic, according to Danish scientists who have one of the world’s best views into the new, more contagious strain.
Cases involving the variant are increasing 70 percent a week in Denmark, despite a strict lockdown, according to Denmark’s State Serum Institute, a government agency that tracks diseases and advises health policy.
“We’re losing some of the tools that we have to control the epidemic,” said Tyra Grove Krause, scientific director of the institute, which has begun sequencing every positive coronavirus test to check for mutations. By contrast, the United States is sequencing 0.3 percent of cases, ranking it 43rd in the world and leaving it largely blind to the variant’s spread.
British Prime Minister Boris Johnson suggested for the first time that the variant may be more deadly than previous strains of the coronavirus. Because it can spread more easily, it can also quickly overwhelm medical systems, turning previously survivable bouts with the virus into perilous ones if hospitals are full and medical care is limited.
Danish public health officials say that if it weren’t for their extensive monitoring, they would be feeling a false sense of confidence right now. Overall, new daily confirmed cases of the coronavirus in Denmark have been dropping for a month.
“Without this variant, we would be in really good shape,” said Camilla Holten Moller, the co-leader of the State Serum Institute group modeling the spread of the virus.
“If you just look at the reproduction number, you just wouldn’t see that it was in growth underneath at all,” she said.
But the British variant is spreading so quickly that Danish authorities project it will be the dominant strain of the virus in their country as early as mid-February.
That would put Denmark ahead of the United States, where the Centers for Disease Control and Prevention warned Friday that the U.K. variant, known as B.1.1.7, could be prevalent by March.
Danish officials say that as a result, daily coronavirus cases there could quadruple by the beginning of April. Charts from the public health institute project that in the worst-case contagion scenarios, even with a strict lockdown in effect, cases would skyrocket.
“This period is going to be a bit like a tsunami, in the way you stand on the beach and then suddenly you can see all the water retracts,” as cases drop, Krause said. “Afterward, you will have the tsunami coming in and overwhelming you.”
The first warning came to Krause on Dec. 14. British virus hunters had fingerprinted a new strain that appeared to be spreading wildly in pockets of their population. When they uploaded the genetic code to a public database of images, they saw that Danish researchers had posted matching mutations for three positive cases, meaning the more aggressive version of the virus had begun to move beyond Britain.
The variant had arrived in Denmark as early as Nov. 14, and it was already spreading inside its borders.
When the British variant was identified as a dangerous new risk, Denmark already had a fairly tight lockdown in place. But it shuttered primary schools, which had previously been open. It halved the number of people who may gather in public spaces to five. It banned nonessential international travel and imposed strict requirements that fresh arrivals into its borders produce negative test results that are less than 24 hours old.
Denmark has also launched a well-disciplined vaccination program, one of the fastest-running in Europe, although Britain and the United States had a head start because they approved the first vaccines earlier.
Even still, cases involving the U.K. variant are growing exponentially in Denmark. The latest British studies have estimated that the strain is 30 to 50 percent more contagious than its precursors. Danish officials crunching similar data slightly differently estimate that it is 36 percent more contagious in their country, although they say their numbers are still so small that the estimates may be inexact.
Worried Danish leaders have tried to explain to their citizens why they need to stay in lockdown, when overall metrics are good enough to suggest the country should have started to reopen weeks ago.
In a long Facebook post last week, Prime Minister Mette Frederiksen told people to imagine sitting in the top row of Copenhagen’s Parken Stadium, a soccer arena with a capacity of 38,000 people. A dripping tap is filling it up, one drop the first minute, two drops the second, four drops the third. At that rate, Frederiksen said, the park will be filled in 44 minutes. But it will seem almost empty for the first 42 minutes, she said.
“The point is that one only discovers that the water has risen when it is almost too late,” she wrote.
Danish officials say that at this stage, they are in a race to vaccinate as many people as possible before the British variant takes hold. Vaccinations will be the key to stemming the worst impact of its spread, they say. But the vaccines may not come fast enough: Under current plans, they only expect to be able to begin administering vaccinations at a large enough scale to bend down the curve of transmissions in April, and production delays this week from Pfizer may slow those plans even further.
Frederiksen joined several other European Union leaders at a virtual summit Thursday in urging that the European Medicines Agency, which approves vaccines across the 27-nation bloc, should speed up its processes. The agency is reviewing AstraZeneca’s vaccine for possible rollout in mid-February. The United States is still reviewing it, as well, but Britain granted emergency authorization last month.
Meanwhile, Copenhagen’s once-bustling bike lanes have fallen quiet as people work from home. Nonessential shops are closed. Preschools are one of the few sectors that remain open — and are a potential target for further tightening.
“It’s this strange silence before the war begins,” said Michael Dall, the chief medical officer at Odense University Hospital, the largest hospital in southern Denmark.
His hospital is opening new coronavirus wards and is confident there will be enough beds even for surging numbers of patients.
But he is fearful that infections among staff and their families could overwhelm his preparation efforts.
“If the mutation is massively more contagious, we’ll end up having even greater problems with the staff challenge,” he said.
Birnbaum reported from Riga, Latvia, and Selsoe Sorensen reported from Copenhagen.
by dryrunguy Today's Situation Report. I skimmed it very quickly, and a few things jumped out at me. I'll read it more carefully tonight.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 96.01 million cases and 2.08 million deaths as of 5am EST on January 22.
In our COVID-19 updates, we typically focus on epidemiological data, daily or cumulative, in countries or areas where the COVID-19 pandemic is more severe. This week, we will take a brief look at countries and territories that have had relative success in containing SARS-CoV-2.
The global average for per capita cumulative incidence is 12,507 cases per million population, and 106 of 190 countries and territories are reporting fewer per capita cases than that. In total, 31 countries and territories are reporting fewer than 500 cumulative cases per million population, and 15 are reporting fewer than 100. Among this short list are some notable examples that have received attention over the course of the pandemic regarding their success in containing transmission. New Zealand (#30; 472.0 cases per million) managed to interrupt domestic transmission, including a period of 100 days without a documented case of local transmission. China is #13 with 68.5 cases per million, despite facing the first major epidemic, which necessitated a full “lockdown” of more than 10 million people and the rapid construction of emergency hospitals in Wuhan to handle the severe patient surge. Taiwan (#9; 36.5) reported some of the earliest imported cases, but its government quickly implemented a response that included social distancing restrictions, testing and contact tracing programs, and quarantine and isolation for exposed and infected individuals in order to bring its epidemic under control. The top 4 countries—Vanuatu (3.3), Lao PDR (5.6), Tanzania (8.5), and Micronesia (8.7)—are all reporting fewer than 10 cumulative cases per million. The majority of countries reporting fewer than 500 cases per million are located in East, Central, and West Africa; Southeast Asia; and the Western Pacific, including a number of small island nations and territories. None are in Europe or North or South America, which have been impacted by the most severe surges or waves since early in the pandemic.
In terms of per capita cumulative mortality, the global average is 268.1 deaths per million population. In total, 110 countries and territories are reporting fewer per capita deaths than the global average. Of those, 45 are reporting fewer than 20 deaths per million population, including 13 countries with fewer than 5. There is considerable overlap between the lists for incidence and mortality. In fact, 38 countries and territories are among the top 50 in both lists. Much like the geographic distribution for cumulative incidence, most of the top countries/territories in terms of mortality are located in Africa, Southeast Asia, and the Western Pacific. Notably, however, there are also several countries from other regions, including Cuba (#39; 16.2) and St. Vincent and the Grenadines (#43; 18.0) in the Caribbean; Tajikistan (#30; 9.4),and Uzbekistan (#44; 18.5) in Central Asia; and Bhutan (#8; 1.3) and Sri Lanka (#35; 12.9) in Southern Asia. Burundi (0.2), Taiwan (0.3), Tanzania (0.4), and Vietnam (0.4) are all reporting fewer than 0.5 deaths per million.
Our World in Data reports that 55.58 million vaccine doses have been administered globally.
UNITED STATES
The US CDC reported 24.32 million total cases and 404,689 deaths. The US surpassed 400,000 cumulative deaths on January 19.
1 death to 50k- 55 days
50k to 100k- 33 days
100k to 150k- 63 days
150k to 200k- 55 days
200k to 250k- 58 days
250k to 300k- 25 days
300k to 350k- 20 days
350k to 400k- 16 days
On January 19, the US daily incidence fell below 200,000 new cases per day for the first time since January 1. At this pace, the US could surpass 25 million cumulative cases in the next 3-4 days. Following several days of depressed daily mortality over the Martin Luther King, Jr. Day holiday weekend, the US reported 4,383 new deaths yesterday, the highest single-day total to date*.
*With the exception of April 15, when New York City reported more than 3,700 previously unreported probable deaths from the onset of its epidemic.
The US CDC reported 37.96 million vaccine doses distributed and 17.55 million doses administered (46.2%), including 2.09 million administered in long-term care facilities (LTCFs). In total, 15.05 million people have received at least 1 dose of the vaccine, and 2.39 million have received both doses. The breakdown of doses by manufacturer remains relatively even, with slightly more Pfizer/BioNTech doses administered (9.82 million; 56%) than Moderna (7.72 million; 44%).
The Johns Hopkins CSSE dashboard reported 24.69 million US cases and 411,781 deaths as of 1:30pm EST on January 22.
US PRESIDENTIAL TRANSITION Almost immediately upon taking office, US President Joe Biden took action in the United States’ battle against COVID-19. On January 20, shortly after the President Biden's inauguration, the White House published its national COVID-19 response plan, which highlights priorities such as “listen[ing] to science,” increasing access to testing, bolstering the supply of personal protective equipment (PPE), providing support for schools and businesses, protecting high-risk individuals, and vaccination. The announcement was accompanied by a detailed, 200-page document that outlines goals and policies for a wide range of challenges facing the COVID-19 response.
President Biden also issued several executive orders shortly after taking office, which reversed the United States’ withdrawal from the WHO, established a COVID-19 Response Coordinator position in the White House, and mandated mask use by federal employees and in federal buildings. On January 21, his first full day in office, President Biden issued additional executive orders and directives to address specific aspects of the COVID-19 response, including to bolster the supply chain for critical supplies and equipment (eg, PPE, therapeutics, test kits, vaccines), including through the Defense Production Act; increase financial and operational support for state governments, including through the National Guard; enhance public health data collection and sharing; improve clinical care and expand access to novel therapeutics for COVID-19 patients; implement COVID-19 risk mitigation measures for domestic and international travel; protect worker health and safety; increase testing capacity and build a sustainable public health workforce; support schools and childcare; and promote equity in the COVID-19 response.
The US is also expected to commit funding for the WHO’s COVAX funding program, which will supply vaccines to low- and middle-income countries. President Biden also directed the Department of Education to extend the suspension of federal student loan repayments, reportedly through September 2021. Additionally, senior officials in the Biden Administration are working to develop their SARS-CoV-2 vaccine distribution plan, with the aim of achieving President Biden’s stated goal of 100 million vaccinations in 100 days.
US VACCINATION US States are struggling to maintain sufficient inventory to support their SARS-CoV-2 vaccination efforts, including multiple major cities that anticipate exhausting their supply in the coming days. In a press conference on January 20, New York Governor Andrew Cuomo said the state’s supply of SARS-CoV-2 vaccine for first doses would run out in 2-3 days. In New York City, tens of thousands of scheduled vaccination appointments were cancelled in order to ensure that sufficient reserve is available for second doses. Both New York State and New York City have scaled up vaccination capacity, but they are currently not able to maintain that pace due to supply limitations. There were concerns that San Francisco could exhaust its inventory by Thursday of this week due to limited incoming supply from the federal government and concerns about a lot of Moderna vaccines that caused those doses to be put on hold. California ultimately lifted the hold and released several thousand doses of the Moderna vaccine, which allowed vaccination efforts to continue. Officials in both New York and California have indicated that they are receiving fewer doses than in past weeks, despite expanded capacity and eligibility.
As we covered previously, Governor Cuomo appealed to Pfizer for the opportunity to purchase doses directly from the manufacturer, circumventing the federal government’s distribution system. Since then, several other states have raised the prospect of direct purchases, but the Biden Administration reportedly opposes the idea. A spokesperson for President Biden noted that a centralized national system is needed to “ensure states aren't competing against each other like they did with PPE, ventilators, and tests.” Biden Administration officials have repeatedly emphasized their intent to increase transparency and consistency in vaccine deliveries in order to facilitate longer-term planning at the state level.
EUROPE CONTROL MEASURES Several European countries have enacted new COVID-19 measures, including enhanced “lockdown” restrictions and updated mask guidance, in response to ongoing COVID-19 surges—including new records in some countries—and concerns about the increased transmissibility of emerging variants. One of the biggest efforts across Europe is a shift from cloth masks to medical-grade masks, which offer increased protection against SARS-CoV-2 transmission. Austria and Germany, for example, now require the use of medical-grade masks—including N95 or KN95 respirators or FFP2 surgical masks—on public transportation and some other public spaces (eg, retail stores, restaurants). Reportedly, France is considering a similar measure. In light of increased transmissibility of emerging SARS-CoV-2 variants, these policies hope to mitigate transmission risk through the use of more effective face coverings.
Some European countries are extending their current lockdown measures as well, including Germany (through February 14) and Austria (February 3). The Netherlands is implementing a nationwide curfew, the first of its kind since World War II. The curfew will be in effect from 9pm-4:30am, except for essential activities, and violators could face fines of €95 (US$115). In the UK, Home Secretary Priti Patel announced that fines will be issued starting next week for anyone attending house parties of more than 15 people. Fines will start at £800 (US$1,100) and double for each offence, up to a maximum of £6,400 (US$8,750)*. Existing fines of up to £10,000 for organizers of large gatherings (ie, more than 30 people) will remain in place.
*We have not been able to determine whether the fines will apply just to England or the entire UK.
EMERGING VARIANTS Many questions remain regarding the emergence of new SARS-CoV-2 variants around the world. One of the more prominent questions is whether certain mutations could affect vaccine efficacy. Last week, Dr. Ugur Sahin, co-founder and CEO of BioNTech, stated that he expected the Pfizer/BioNTech vaccine to be protective against the new variants. On January 19, Dr. Sahin and other researchers at BioNTech and Pfizer published (preprint) findings from a study that provides insight into preliminary data on the vaccine’s efficacy against new SARS-CoV-2 variants. The researchers utilized blood sera collected from 16 participants vaccinated in the Phase 1/2 clinical trials to evaluate the neutralizing capacity against the B.1.1.7 variant. The researchers found that the vaccine exhibited “no biologically significant difference in neutralization activity” between the B.1.1.7 variant and the reference strain. Research into the efficacy of existing vaccines against emerging variants continues, which will be critical to understanding the next phase of global vaccination efforts.
New evidence suggests that the B.1.351 variant may be less susceptible to antibody treatments, which also raises concerns about the potential for reduced vaccine efficacy. Researchers in South Africa, where the variant was first identified, published (preprint) findings from a study that evaluated the neutralizing capacity of blood sera collected from 21 COVID-19 patients who recovered after being hospitalized. The B.1.351 (or 501Y.V2) variant appeared to be less susceptible to the antibodies present in the sera specimens, which is cause for concern, considering that the production of such antibodies is the goal of most SARS-CoV-2 vaccines and candidates.
Additionally, analysis from South Africa’s National Health Laboratory Service (NHLS) identified more than 4,000 potential instances of reinfection in South Africa. To date, there have been relatively few documented cases of true reinfection with SARS-CoV-2, but this information raises questions regarding whether the emerging variant could increase that risk.Neutralizing antibodies generated during acute infection tend to provide some degree of protection against future infections, at least for a short period of time; however, if the neutralizing antibodies generate for one variant are less effective against new variants, recovered individuals may be more susceptible to reinfection. Further research is needed to definitively determine whether the 4,000 cases are true reinfections and to characterize any effects from the emerging variant.
The identification of emerging SARS-CoV-2 variants has prompted calls for expanded genomic surveillance globally to monitor for the emergence of novel variants as well as the spread of known variants. Ongoing genomic surveillance programs in South Africa and the UK played key roles in detecting 2 of the most prominent new variants, B.1.1.7 and B.1.351, which are believed to be driving regional surges in transmission. Without these real-time efforts, it is likely that new variants would go unnoticed, at least until their epidemiological effects become evident. Retrospective studies have started examining the timelines associated with the emergence and spread of different SARS-CoV-2 variants, illustrating the importance of active genomic surveillance activities. For example, a study published (preprint) this week by researchers at the University of Arizona (US) suggests that the B.1.1.7 variant was circulating in the US at least as early as November 2020, potentially as a result of multiple independent introductions. Continued sequencing of SARS-CoV-2 specimens in countries around the world is critical to understanding ongoing viral evolution, which can then inform effective public health response, including the development of effective medical countermeasures such as vaccines.
BAMLANIVIMAB Eli Lilly announced that its neutralizing antibody treatment bamlanivimab can reduce the risk of developing COVID-19 disease. In a press release on January 21, the company reported preliminary results from a study conducted among residents and staff at long-term care facilities. The randomized, placebo-controlled study, part of the BLAZE-2 trial effort, involved 965 total participants (299 residents and 666 staff). The researchers found that prophylactic use of bamlanivimab was associated with an 80% decrease in the risk of developing COVID-19 disease after 8 weeks. The full data have not yet been published publicly nor peer reviewed, but the company indicated that it intends to publish the data in the near future.
Eli Lilly’s Chief Scientific Officer, Dr. Daniel Skovronsky, stated that bamlanivimab is not a replacement for vaccines, but rather, it could be an option for emergency prophylaxis following known or suspected exposure. The drug could potentially mitigate the risk of disease when there may not be enough time for a vaccine to stimulate a sufficient immune response. Bamlanivimab previously received an Emergency Use Authorization (EUA) from the US FDA as a treatment for COVID-19, but not as a preventive measure.
ICU SURGE & MORTALITY Researchers in Indiana and California (US) published findings from a study on the association between patient surge in hospital intensive care units (ICUs) and COVID-19 mortality. The study, published in JAMA: Network Open, included data from more than 8,500 patients admitted to 88 Veterans Affairs hospitals across the US (March-August 2020). The researchers found that ICU patients treated during periods of high ICU patient surge were significantly more likely to die, even after discharge. Notably, patients treated in an ICU when demand—defined as the percent of the maximum ICU patient load—was greater than 75% were nearly twice as likely to die compared to patients treated when ICU demand was 25% or less (aHR=1.94).
The statistically significant results held up when stratified by date—March-May 2020 compared June-August 2020, when the patient surge was lower. During the June-August period, no patients were treated in ICUs with more than 75% of the beds filled, but those treated when the facility was at more than 75% of its maximum ICU usage still had nearly twice the risk of death than those treated at ICU demand of 25% or less (aHR=1.90). This illustrates the critical importance of mitigating community transmission and the subsequent impact on hospitals and health systems, even during times of relatively low levels of community transmission and ICU usage.
LONG COVID The UK’s Office of National Statistics (ONS) published data regarding the prevalence of symptoms associated with “long COVID” in patients who recovered from acute SARS-CoV-2 infection. The data indicate that approximately 20% of infected individuals exhibit symptoms for 5 weeks or longer, and 10% report symptoms for 12 weeks or longer. This corresponds to an estimated 186,000 individuals in England with symptoms lasting between 5 and 12 weeks. The findings are based on responses to the UK’s COVID-19 Infection Survey, which utilizes a nationally representative sample from across the UK, and efforts are ongoing to gather additional data, including on symptoms that persist longer than 12 weeks. A more detailed look at the available data shows that prevalence of long COVID symptoms* tends to increase with age, peaking in the 35-49 years (26.8%) and 50-69 years (26.1%) age groups, compared to the 2-11 years (12.9%) and 12-16 years (14.5%) age groups. Additionally, there appears to be a statistically significant increase in prevalence among women (23.6%) compared to men (20.7%). *Data displayed here refer to the presence of any symptom at 5 weeks, but the provided tables also include data on individual symptoms.
VACCINE CLINICAL TRIALS As more vaccines are authorized for use in countries around the world, it could pose challenges for conducting clinical trials for other vaccines. As we covered previously, there are ethical and practical challenges to keeping clinical trial participants “blinded” to knowing whether they received the candidate vaccine or the placebo, particularly once that particular product is ultimately authorized for use. Another problem is arising in trials for other candidate vaccines, as participants are starting to request that they be “unblinded” in order to determine if they want to get vaccinated with a product that is currently authorized for use. In one example, researchers conducting Phase 3 clinical trials for the Novavax vaccine are reporting that older participants are requesting to be unblinded after some US states expanded eligibility to adults aged 65 and older. Notably, the Novavax trials aim to include adults aged 65 and older as 25% of the study population, which could be a major challenge if adults in this age group are getting vaccinated using the Pfizer/BioNTech or Moderna products, and similar barriers could face any future clinical trials.
There are alternatives to randomized, blinded, placebo-controlled trials—considered to be the gold standard for clinical trials—but these, too, could be challenging for vaccine candidates. One option is a “non-inferiority” trial, which compares a new product to an existing product to determine if the new product performs on par with the existing one. Considering the high efficacy of both the Pfizer/BioNTech and Moderna vaccines, it could be difficult for new products to meet an acceptable threshold. Some of the new candidates, however, do have advantages over existing vaccines that could potentially outweigh shortcomings in terms of efficacy. The Johnson & Johnson (J&J)/Janssen vaccine, for example, would require only 1 dose, which could expand access and speed vaccination programs over 2-dose vaccines. And the Novavax vaccine is expected to be stable at normal refrigeration temperatures (eg, 2-8°C/35.6-46.4°F), as opposed to the freezing or ultra-cold temperatures required for other vaccines, which could make it easier to maintain a cold chain during distribution and longer-term storage, particularly in rural or resource-limited settings.
CHINA QUARANTINE China continues its response to an ongoing COVID-19 outbreak in Shijiazhuang, a city in the northern part of the country. Last week, the Chinese government imposed a “lockdown” on Shijiazhuang and Xingtai. The lockdown then expanded to include other cities across 11 regions in 3 provinces—including Langfang, which is located just south of Beijing. In total, the lockdowns now affect an estimated 22 million people. Additionally, the Chinese government is rapidly constructing a COVID-19 quarantine center outside Shijiazhuang that could house more than 4,000 individuals. The plan is for this facility to host close contacts of confirmed COVID-19 patients as a part of the country’s expansive COVID-19 contact tracing program. The Chinese government has expressed a sense of urgency to control the spread of the pandemic, particularly as the country prepares for increases in travel and large gatherings coinciding with the Lunar New Year in February.
PANDEMIC TREATY At a meeting of the WHO’s Executive Board this week, Director-General Dr. Tedros Adhanom Ghebreyesus expressed support for a recent proposal by the European Council to establish an “international treaty on pandemics.” The proposed treaty could address various aspects of pandemic preparedness, including risk assessment, coordinating research agendas and associated funding, information sharing and event reporting, and improving healthcare access and health system capacity. Notably, international agreements and programs already exist to address preparedness and response for health emergencies like pandemics, including the International Health Regulations (IHRs) and the Global Health Security Agenda (GHSA), and it is not immediately clear what the relationship would be between the proposed pandemic treaty and these existing efforts or how they might complement or overlap with each other. An independent panel of experts recently reported to the WHO Executive Board their findings on the effectiveness of the IHRs, including that the IHRs could be improved upon, but major changes are not necessary.
by ponchi101 How about this idea. This is not normal. We are in specially dangerous times. So: can we skip the final step for the Moderna vaccine (and J&J, and any other)? If somebody want to try it, after stage 2, let's go.
It is already 2 MM dead, and the new strain is more virulent. By now, the math is not that complicated: 1 month = 200K dead (the first couple of months last year were "slow", as the disease was spreading). And:
Unless you are an island (NZ, Australia, Singapore, South Korea, which is an island because it is separated from any other mainland by N. Korea), no lockdown has worked. It matters little if it is Europe, S. America, any given state in the USA. We are doing the proverbial Einstein definition: trying the same thing and expecting different results.
I am ready for Moderna. Better that than catching the new strain.
by Suliso Moderna is already approved in US and EU. I hear that AZ will be approved in Switzerland and EU within 2-3 weeks.
by Suliso However, it seems that Moderna production capacity is currently far below that of Pfizer. I really only hear about the latter currently being used in the West.
by Deuce Over the next 2 or 3 weeks, we'll be receiving more Moderna than Pfizer up here in Canada. We've had Moderna for at least 3 weeks now, I believe.
We'll be getting very little Pfizer over the next few weeks because Pfizer is 'restructuring' their plant in Belgium.
by Suliso I believe in Europe we ordered relatively little of Moderna. It's mostly Pfizer and AZ.
by Deuce We don't have AstraZeneca yet. There has been some talk about it - about how it will be better for the less populated more northern areas, because it doesn't need to be stored in extreme temperatures (they don't have the equipment to store vaccines in extreme freezers there). But, really, it isn't even being discussed yet in terms of a timeline to approve/receive it.
by ti-amie
by ti-amie
She left the bubble and realized that in the real world her reputation is, to put it nicely, in tatters.
by ponchi101 Indeed. An example of non-integrity.
by JazzNU I have always thought the criticism of Dr. Birx has been overly harsh, some of it clearly being about her being a woman, and she's been a convenient target of the public's ire for the botched handling of the pandemic even though she's essentially in the same situation as Dr. Fauci where speaking out against the President was difficult, but thought of as significantly different than him. I love Dr. Fauci, so this isn't about him. But it was always, and I do mean always, a mistake to think of Dr. Birx as being there to do the exact same thing as Dr. Fauci. She is military. An Army Colonel. She's up there wearing Hermes scarves and so people think she's just another doctor, but no, she's a military doctor. Whether you're a doctor or not, when you're military, you follow orders from the Commander in Chief, even if he's an ass, that's why we had that incredibly pitiful Lafayette Square debacle. And she's real military, training and career, not fake like Admiral Giroir, who deserves much more consternation and condemnation than he's gotten, who as far as I can tell, didn't earn an ounce of that esteemed title.
Now in addition to that, the majority of what she did, we didn't see. So while people are endlessly mad at her for not doing good for the people, she was the one who was advising the governors throughout the pandemic, who was giving information and guidance and signaling early warnings to state's about implementing stricter measures. Not all of them listened obviously, but she was doing this constantly. It wasn't for the public though, so that part of her role was largely ignored. But when governors spoke about who was the person they could reach for help, it was Dr. Birx. There was a story before about how she and her team travelled 25,000 miles around the country advising municipalities on implementing best practices. These sorts of things barely got media coverage whereas almost everything Fauci did to counteract bad information was highlighted.
I'm not saying she doesn't deserve criticism. She does. But she's in the same position as the others, doing her job under circumstances no one should have found themselves in. Could she have done more? Yes, but only to a certain extent to me in particular because of the military background. I don't think she's built because of that drilled in mindset to follow orders to go on the defensive and give interviews to any and every small non-news outlet like Fauci to counteract the nonsense coming from the White House after they tried to muzzle him and defend her reputation. It is very much not in the military mindset to take that strategy. She made things worse for herself by trying to put on too much of a show of being supportive of him, something Fauci never did. There was no need to pretend he was smart or provide cover for things that weren't going to blow back on her. She was not adept at handling him. But still, she is not all bad and I shudder to think how much worse off we'd be if she wasn't there. Because I think we can assume based on other actions, her position would've been filled by some Dr. Atlas type crackpot and isn't that just a frightening thought.
By all accounts, she's done a lot of great work for decades, especially working on the AIDS pandemic and the reason Obama appointed her in the first place. If you listen to doctors and researchers talk about her throughout the pandemic, they were always quick to point out that difficult position she found herself in, they didn't trash her the way the public does. Her reputation may be shot in the public, but it has never seemed like that was the case in the medical community, and I think they're much more willing to remember her entire career and not boil it all down to just this last year.
by ti-amie
by JazzNU
Suliso wrote: ↑Fri Jan 22, 2021 10:15 pm
However, it seems that Moderna production capacity is currently far below that of Pfizer. I really only hear about the latter currently being used in the West.
I wasn't sure what you meant by the West, possibly you're just referencing Europe. Pfizer and Moderna are being used at an almost comparable rate in the US now. The next one expected here is the Johnson & Johnson single dose vaccine. Fauci said he anticipates data within the next 2 weeks becoming public and then reviewed for emergency use.
The AstraZeneca one has been flagged here because there are questions on it's effectiveness in the elderly, it was apparently a group that either wasn't studied enough or at all in the trials and so there are questions. It's not expected to get approval for another couple of months last I heard.
by Suliso AstraZeneca likely to be approved in EU this week. We have hardly any Moderna here and without AZ we'll never get where we need to get. Nobody talking about Johnson & Johnson here, but hopefully they succeed as well.
by meganfernandez
Suliso wrote: ↑Mon Jan 25, 2021 7:37 pm
AstraZeneca likely to be approved in EU this week. We have hardly any Moderna here and without AZ we'll never get where we need to get. Nobody talking about Johnson & Johnson here, but hopefully they succeed as well.
Is vaccination underway in most European countries, and are they struggling with it as much as we are? Indiana, I must say, is doing a pretty good job. My mom just got vaccinated (she's a healthy 80). My husband, whose job takes him into hospitals every day, got it. You can volunteer at the sites and have a chance (a shot, haha) at getting an extra one at the end of the night.
Suliso wrote: ↑Mon Jan 25, 2021 7:37 pm
AstraZeneca likely to be approved in EU this week. We have hardly any Moderna here and without AZ we'll never get where we need to get. Nobody talking about Johnson & Johnson here, but hopefully they succeed as well.
Is vaccination underway in most European countries, and are they struggling with it as much as we are? Indiana, I must say, is doing a pretty good job. My mom just got vaccinated (she's a healthy 80). My husband, whose job takes him into hospitals every day, got it. You can volunteer at the sites and have a chance (a shot, haha) at getting an extra one at the end of the night.
It has started everywhere in EU, but we started late and it's going too slow... In Switzerland only 2% have been vaccinated and in Latvia it's not even 1%. UK is the only country which has done better than US, albeit I question their strategy of not giving the second dose at the time it has been prescribed.
by JazzNU So very concerned about that UK strategy diverging so far from the approach in the clinical trial. We've already had people here that have gotten covid after they've gotten the vaccine, some of them Congressmen and women. The public health officials I've seen talk about it have said, yes, it can happen because in the case of the one shot, they haven't been fully vaccinated, and in the case of two shots, it was too close to the second shot for them to develop the full immunity because it takes time to build up response fully in the body. But what's that mean for the UK strategy?
Suliso wrote: ↑Mon Jan 25, 2021 7:37 pm
AstraZeneca likely to be approved in EU this week. We have hardly any Moderna here and without AZ we'll never get where we need to get. Nobody talking about Johnson & Johnson here, but hopefully they succeed as well.
Is vaccination underway in most European countries, and are they struggling with it as much as we are? Indiana, I must say, is doing a pretty good job. My mom just got vaccinated (she's a healthy 80). My husband, whose job takes him into hospitals every day, got it. You can volunteer at the sites and have a chance (a shot, haha) at getting an extra one at the end of the night.
It has started everywhere in EU, but we started late and it's going too slow... In Switzerland only 2% have been vaccinated and in Latvia it's not even 1%. UK is the only country which has done better than US, albeit I question their strategy of not giving the second dose at the time it has been prescribed.
Are they waiting too long to give the second dose?
Here, anyone can get it actually. It's easy to jump the line. No one verifies if you actually qualify - they want needles in arms. Some people have done that. I don't judge... I've decided against it for myself because I don't need it urgently. I can wait.
by ti-amieFirst U.S. case of highly transmissible Brazil coronavirus variant identified in Minnesota
By
Joel Achenbach
Jan. 25, 2021 at 5:45 p.m. EST
Minnesota officials announced Monday they have identified a person infected with a highly transmissible variant of the coronavirus that has been spreading at alarming rates in recent weeks in Brazil. This is the first report in the United States of the so-called P.1 variant.
The Minnesota Department of Health said the case involved “a Minnesota resident with recent travel history to Brazil,” and the variant was detected through genomic sequencing of random blood samples. The person, a resident of the Twin Cities metro area, reported feeling sick the first week of January, and was tested Jan. 9.
“This isn’t surprising. It’s a very difficult development, but at the same time not unexpected,” Michael T. Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota and an adviser to President Biden’s coronavirus response team, said in an interview.
meganfernandez wrote: ↑Mon Jan 25, 2021 9:39 pm
Here, anyone can get it actually. It's easy to jump the line. No one verifies if you actually qualify - they want needles in arms. Some people have done that. I don't judge... I've decided against it for myself because I don't need it urgently. I can wait.
What?!?
To be clear, Megan must be talking about Indianapolis or Indiana, not the US. Anyone can absolutely not go get a vaccine or jump the line. It's not supposed to be happening in Indiana either according to their own guidelines. Truly messed up. I will judge harshly.
by ponchi101 Unfortunately, we do not have enough people from around the world to make a proper comparison.
Maybe we should start a poll. When will ALL OF US be vaccinated? Who will be the first? Who will be last? Because here, with already 45K+ people dead, the GOV is still talking about Feb 15th to start.
And you can bet they will be late.
by ti-amie I am not an anti-vaxxer. I have had all of the pneumonia shots, a booster shot for god knows what, and any and all shots seniors need to have. When It comes to this shot however, I am going to wait until my physical in March. Right now NYC is out of vaccine anyway.
ponchi101 wrote: ↑Tue Jan 26, 2021 1:24 am
Unfortunately, we do not have enough people from around the world to make a proper comparison.
Maybe we should start a poll. When will ALL OF US be vaccinated? Who will be the first? Who will be last? Because here, with already 45K+ people dead, the GOV is still talking about Feb 15th to start.
And you can bet they will be late.
I'm afraid you're likely to be last. As for the first probably one of our older members from US. I don't expect it for myself before July/August.
by Suliso Now I'm reading that AZ might not be approved for seniors (if at all) in EU. Data shows insufficient activity. The new mRNA technology will stand out even more if that is the case.
Just to illustrate my previous point about vaccines around here in Germany 1.78 million doses have been given including 1.76 million from Pfizer/BioNTech.
by Suliso There should be some kind of journalism prize for stupidity. Two large and seemingly respectable German newspapers printed a story claiming that AZ vaccine is less than 10% effective for people over 65. Sensational news except that the original document actually says that less than 10% of trial participants (8% to be exact) were 65+...
by ti-amie
Suliso wrote: ↑Tue Jan 26, 2021 6:24 pm
There should be some kind of journalism prize for stupidity. Two large and seemingly respectable German newspapers printed a story claiming that AZ vaccine is less than 10% effective for people over 65. Sensational news except that the original document actually says that less than 10% of trial participants (8% to be exact) were 65+...
There should be a censure of some kind when idiots spout off about science incorrectly.
by ti-amie
by ponchi101 A very respected person here in the country. Worked for almost every government since he came into public life.
by Suliso I used to post some covid statistics on TAT 1.0. Not as extensive this time, only the final mortality rate. Top 10 plus some notables excluding micro states. Note that 1000 means that 0.1% of the countries population has died from the disease in the last year or so.
Deaths per 1 million inhabitants
Belgium 1,791
Slovenia 1,638
UK 1,471
Czechia 1,457
Italy 1,431
Bosnia and Herzegovina 1,414
North Macedonia 1,350 USA 1,309
Bulgaria 1,284
Hungary 1,256
-------
Spain 1,215
Peru 1,200 (worst in SA)
Mexico 1,159
France 1,134
Sweden 1,110
Portugal 1,082 (currently the worst outbreak in EU)
Switzerland 1,059
Argentina 1,040
Brazil 1,026 (I suspect undercounting)
Colombia 1,018
Germany 648
Ireland 617
Latvia 601
Canada 511
Israel 491 (current leader in vaccinations)
Denmark 350
Finland 118
Norway 101 (best in continental Europe)
by Deuce
Suliso wrote: ↑Tue Jan 26, 2021 11:07 pm
I used to post some covid statistics on TAT 1.0. Not as extensive this time, only the final mortality rate. Top 10 plus some notables excluding micro states. Note that 1000 means that 0.1% of the countries population has died from the disease in the last year or so.
Deaths per 1 million inhabitants
Belgium 1,791
Slovenia 1,638
UK 1,471
Czechia 1,457
Italy 1,431
Bosnia and Herzegovina 1,414
North Macedonia 1,350 USA 1,309
Bulgaria 1,284
Hungary 1,256
-------
Spain 1,215
Peru 1,200 (worst in SA)
Mexico 1,159
France 1,134
Sweden 1,110
Portugal 1,082 (currently the worst outbreak in EU)
Switzerland 1,059
Argentina 1,040
Brazil 1,026 (I suspect undercounting)
Colombia 1,018
Germany 648
Ireland 617
Latvia 601
Canada 511
Israel 491 (current leader in vaccinations)
Denmark 350
Finland 118
Norway 101 (best in continental Europe)
Just to add further context...
Australia - deaths per 1 Million inhabitants: 36.
Australia is a 'modern' country with large cities. If they can handle the virus this well, why can't other modern countries with big cities?
They could have, had they taken the same approach as Australia has.
(Of course, Australia may go all to hell now that they've allowed the infected tennis population in...)
by Suliso Do special advantages of Australia and New Zealand really need to be spelled out? We're all smart enough to understand...
by JazzNU For the previous convo on vaccine by manufacturer, I was on the CDC website today looking at the numbers for different states and the current breakdown nationwide is:
13 million Pfizer
10.4 million Moderna
by dryrunguy The latest Situation Report.
::
...
ECONOMIC IMPACT & RECOVERY A report published this week by Oxfam International illustrates significant disparities in terms of the financial impact of the COVID-19 pandemic. The report—released to coincide with the annual World Economic Forum summit typically held in Davos, Switzerland—indicates that the “mega-rich” have already recovered financially from the pandemic, whereas the world’s poorest could take years or longer. Notably, the research suggests that COVID-19 could exacerbate economic inequalities in nearly every country on Earth. The 1,000 wealthiest people in the world, “mostly White male,” took approximately 9 months to recuperate financial losses, but those living in poverty are expected to take more than a decade to recover. The analysis also estimates that “the increase in the 10 richest billionaires’ wealth since the crisis began [more than US$500 billion] is more than enough to prevent anyone on Earth from falling into poverty because of the virus, and to pay for a COVID-19 vaccine for everyone.” Notably, women and racial and ethnic minorities are disproportionately affected by the global economic crisis. In addition to shorter-term and immediate financial struggles, many people around the world will face prolonged financial hardship stemming from the pandemic, compounding economic inequalities around the world.
Dry.
I AM SORRY. I thought I was replying to your post, and I clicked the EDIT button instead. I deleted your post.
I am super sorry. I am still sometimes lost here.
Can you re-post, please?
by ponchi101 About AUS and NZ. I said it: wealthy island nations that could isolate quickly, with low population densities, and separated from every body else. Plus, populations that could count on some social security network and not be forced to go out, having to choose between the chance of catching the virus or the certainty of going hungry.
by dryrunguy Here's the most recent Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 99.36 million cases and 2.14 million deaths as of 11am EST on January 26. The WHO reported decreasing global incidence for the second consecutive week, down to 4.10 million new cases last week, a 15.2% decrease from the previous week. But even with the recent decline, the average global daily incidence exceeds 575,000 new cases per day. At this pace, we expect the global cumulative incidence to surpass 100 million cases in the next 2 days. While daily incidence is decreasing, mortality continues to increase. The WHO reported 95,991 deaths last week, a new record and an increase of slightly more than 1% compared to the previous week.
Our World in Data reports that 55.58 million vaccine doses have been administered globally.
UNITED STATES
The US CDC reported 25.02 million total cases and 417,936 deaths. The US surpassed 25 million cumulative cases in yesterday’s update.
1 case to 5 million cases- 200 days
5 million to 10 million- 92 days
10 million to 15 million- 29 days
15 million to 20 million- 24 days
20 million to 25 million- 23 days
It is becoming more clear that the US has passed a peak in terms of daily incidence, and the current average is less than what it was prior to the Thanksgiving holiday weekend. In light of fluctuations in reporting over the winter holidays, it is difficult to determine when the daily incidence actually peaked; however, the peak in terms of reported incidence was 248,706 new cases per day on January 8. In addition to daily incidence, we are beginning to observe an associated decrease in hospitalizations at the national level.
This trend is evident at the regional and state levels as well. All 4 regions have reported decreasing daily incidence since approximately January 8-10, including a further decrease in the Midwest, which has reported a steady decline in daily incidence since mid-to-late November. According to data from the COVID Exit Strategy website, 28 states are reporting decreasing daily incidence over the past 2 weeks, including nearly every state stretching from the Midwest to the Pacific Northwest as well as several states in the South, Mid-Atlantic, and Northeast. According to data from The COVID Tracking Project, 45 states (plus Washington, DC) are reporting decreasing daily incidence over the past week, and 5 are holding steady (-10% to +10%). In fact, only Tennessee is reporting increased incidence over the past week, but at +7%, it still falls under the category of “Staying the Same.” Similarly, hospitalizations are decreasing in all 4 regions. Additionally, 33 states are reporting decreasing hospitalizations over the past week, and 15 (plus Washington, DC) are reporting steady hospitalizations (-10% to +10%)—compared to only 2 states reporting increases.
Looking at mortality at the regional level, COVID-19 deaths continue to decrease steadily in the Midwest, and the Northeast region appears to have recently passed a peak. The South and West regions may be at or approaching their own peaks, but holiday-related delays in reporting make it difficult to determine the longer-term trend in these regions. At the state level, 21 states (plus Washington, DC) are reporting decreasing daily mortality over the past week, compared to 11 with increasing mortality and 18 holding relatively steady (-10% to +10%).
The US has now administered more than half of the distributed vaccine doses. The US CDC reported 41.42 million vaccine doses distributed and 22.73 million doses administered (54.9%%), including 2.71 million administered in long-term care facilities (LTCFs). In total, 19.25 million people have received at least 1 dose of the vaccine, and 3.35 million have received both doses. The US is now averaging 1.13 million doses administered per day, an increase of 35% compared to this time last week. The breakdown of doses by manufacturer remains relatively even, with slightly more Pfizer/BioNTech doses administered (12.55 million; 55%) than Moderna (10.08 million; 45%).
The Johns Hopkins CSSE dashboard reported 25.34 million US cases and 422,583 deaths as of 1:30pm EST on January 26.
EMERGING VARIANTS & MORTALITY New evidence indicates the B.1.1.7 variant of concern (VOC) may be associated with increased mortality compared to other strains of SARS-CoV-2. At a press conference this week, Sir Patrick Vallance, the UK’s Government Chief Scientific Advisor, said that infection with the new variant may be associated with an increased risk of death, in addition to its increased transmissibility. He noted that the mortality risk could be on the order of 30-40% higher for some individuals, but he also said that further analysis is needed to better characterize this relationship. Analysis published by the UK’s New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) found that that mortality risk was significantly higher in individuals infected with the B.1.1.7 variant across multiple age groups, with increases ranging from 29% to 91% in multiple studies.
In response to the potential for increased mortality, UK Prime Minister Boris Johnson called for redoubled vigilance and adherence to COVID-19 prevention measures in order to protect the capacity of national healthcare system. Fortunately, current vaccine candidates still appear to be effective against the variant. The UK government will continue to drive toward its goal of vaccinating 15 million people by mid-February in order to protect the most vulnerable against infection by any variant of SARS-CoV-2.
In the US, Dr. Anthony Fauci acknowledged the NERVTAG results as highly concerning and in need of further study in the coming weeks. He emphasized that current vaccines still appear to be effective against existing VOCs, but adjustments can and will be made as needed. Dr. Fauci did note that monoclonal antibody treatments did appear to be significantly less effective against some VOCs compared to reference strains.
VACCINE DEVELOPMENT & EFFICACY On January 25, Merck announced that it “is discontinuing development of its SARS-CoV-2/COVID-19 vaccine candidates” as a result of poor performance during Phase 1 clinical trials. While Merck’s 2 candidates were well tolerated from a safety perspective, the immune response generated in the study participants was “inferior to those seen following natural infection and...for other SARS-CoV-2/COVID-19 vaccines.” The Merck vaccines were highly anticipated, as they used viral platforms that could replicate in the human body, which had the potential to confer longer-lasting immunity with a single dose.
Despite having already received authorization for the use of its SARS-CoV-2 vaccine in multiple countries, Moderna is already developing a booster to better protect against emerging variants. On January 25, Moderna announced preliminary results from a study assessing the current vaccine’s efficacy against emerging variants, including B.1.1.7 and B.1.351. Compared to reference strains, the vaccine did not exhibit any decrease in neutralizing antibody titers against the B.1.1.7 variant. Conversely, the vaccine exhibited a 6-fold reduction in neutralizing antibodies effective against the B.1.351 variant, which could indicate a lesser degree of protection or faster waning of immunity. A press release from the company indicated that while the immune response was lower, the vaccine did offer some protection. Considering that the immune response from the vaccine appears to be stronger than from natural infection, a moderate decrease in efficacy could still provide a meaningful degree of protection. In response to the concerning results, Moderna announced that it is in the process of developing a new booster that is tailored to provide increased protection against the B.1.351 variant. Additionally, Moderna is testing the effect of a second booster dose of the existing vaccine to determine any additional benefit in terms of protection against the B.1.351 variant. Considering that Moderna’s existing vaccine is already authorized for use in multiple countries, it is unclear what the regulatory review process would look like for a new booster or an additional booster dose.
AUSTRALIA VACCINE AUTHORIZATION On January 25, the Australian Therapeutic Goods Administration granted provisional authorization for the use of the Pfizer/BioNTech vaccine candidate. The provisional approval applies for use in individuals aged 16 years and older, and vaccinations are expected to begin in February. Australian Prime Minister Scott Morrison emphasized that the provisional approval is different from an emergency authorization and requires a more comprehensive review of the vaccine’s safety and efficacy, among the first such effort globally. The vaccine will be provided for free to all Australian citizens. According to the National Rollout Strategy, as many as 1.4 million doses will be distributed to “1a” priority groups, which include healthcare workers, long-term care facility staff and residents, and border and quarantine workers. The vaccine will initially be delivered to 50 priority vaccination sites during Phase 1a and then expanded to more than 1,000 sites nationwide. The initial vaccine hubs are concentrated in coastal areas, where the majority of the population resides. Few of the initial sites are located in Australia’s interior where many aboriginal communities reside. Australian authorities must set up cold storage facilities and train vaccinators in advance of beginning Phase 1a, and each batch will be tested before doses are administered.
VACCINE DONATIONS India has pledged to donate more than 4.5 million doses of the AstraZeneca vaccine, manufactured in India by the Serum Institute, to several neighboring countries. Deliveries have reportedly already arrived in Bangladesh, Bhutan, Maldives, Mauritius, Nepal, and Seychelles, and additional donations are expected for Afghanistan and Sri Lanka. India has already stockpiled 80 million doses of the AstraZeneca vaccine, and it is expected to manufacture an additional 50 million doses per month. In addition to India, China has donated vaccine to numerous countries, including Myanmar, Cambodia, Philippines, and Pakistan. Commentators have noted that these donations may be a strategic form of diplomacy that aims, in part, to increase political influence in the region and improve bilateral relations. In addition to donations, both India and China have also sold doses of vaccine to global partners.
US TRAVEL RESTRICTIONS Yesterday, US President Joe Biden issued travel restrictions for several countries that are currently experiencing increased COVID-19 incidence, including several emerging variants of SARS-CoV-2. The restrictions apply to individuals who traveled to Brazil, Ireland, South Africa, the UK, or any country in the EU (Schengen Area) in the 14 days prior to their arrival in the US. The restrictions existed previously for Brazil, Ireland, the UK, and the EU, but South Africa is new to the list. The presidential proclamation took effect today. Dr. Anthony Fauci described the restrictions as “very prudent,” particularly as new evidence indicates that these emerging variants may be associated with increased mortality risk. Exceptions to the new policy include US citizens, permanent residents, noncitizen nationals, certain immediate family members of permanent residents or citizens, individuals who fall under exceptions related to US national interests and individuals seeking asylum.
MEXICAN PRESIDENT On Sunday, Mexican President Andrés Manuel López Obrador announced that he tested positive for SARS-CoV-2. President Obrador described his symptoms as “mild,” but he is currently undergoing medical treatment. President Obrador will continue to isolate at home, and he has handed off responsibility for daily news conferences to Mexico’s Secretary of the Interior, Olga Sánchez Cordero. President Obrador had not yet been vaccinated against SARS-CoV-2.
RESTRICTIONS & PROTESTS For the past several days in the Netherlands, protests against stronger COVID-19 restrictions have turned violent. The Dutch government implemented new ”lockdown measures” on January 23, including a nighttime curfew from 8:30pm-4:30am, a travel advisory discouraging any travel out of the country, and a limit of 1 visitor per household per day. The curfew, in particular, drew opposition from the public. As we covered previously, the last time that the Netherlands implemented a nationwide curfew was during World War II. The large public protests turned violent on Sunday the 24, reportedly including a fire at a SARS-CoV-2 testing center. Since then, hundreds of protestors have been arrested, and several cities have imposed ordinances against entering the city center in order to suppress further riots. Prime Minister Mark Rutte condemned the riots, describing the events as instances of criminal violence rather than protests. The curfew and other new measures are scheduled to remain in place through February 9.
ECONOMIC IMPACT & RECOVERY A report published this week by Oxfam International illustrates significant disparities in terms of the financial impact of the COVID-19 pandemic. The report—released to coincide with the annual World Economic Forum summit typically held in Davos, Switzerland—indicates that the “mega-rich” have already recovered financially from the pandemic, whereas the world’s poorest could take years or longer. Notably, the research suggests that COVID-19 could exacerbate economic inequalities in nearly every country on Earth. The 1,000 wealthiest people in the world, “mostly White male,” took approximately 9 months to recuperate financial losses, but those living in poverty are expected to take more than a decade to recover. The analysis also estimates that “the increase in the 10 richest billionaires’ wealth since the crisis began [more than US$500 billion] is more than enough to prevent anyone on Earth from falling into poverty because of the virus, and to pay for a COVID-19 vaccine for everyone.” Notably, women and racial and ethnic minorities are disproportionately affected by the global economic crisis. In addition to shorter-term and immediate financial struggles, many people around the world will face prolonged financial hardship stemming from the pandemic, compounding economic inequalities around the world.
dryrunguy wrote: ↑Wed Jan 27, 2021 12:50 am
Here's the most recent Situation Report.
::
...
ECONOMIC IMPACT & RECOVERY A report published this week by Oxfam International illustrates significant disparities in terms of the financial impact of the COVID-19 pandemic. The report—released to coincide with the annual World Economic Forum summit typically held in Davos, Switzerland—indicates that the “mega-rich” have already recovered financially from the pandemic, whereas the world’s poorest could take years or longer. Notably, the research suggests that COVID-19 could exacerbate economic inequalities in nearly every country on Earth. The 1,000 wealthiest people in the world, “mostly White male,” took approximately 9 months to recuperate financial losses, but those living in poverty are expected to take more than a decade to recover. The analysis also estimates that “the increase in the 10 richest billionaires’ wealth since the crisis began [more than US$500 billion] is more than enough to prevent anyone on Earth from falling into poverty because of the virus, and to pay for a COVID-19 vaccine for everyone.” Notably, women and racial and ethnic minorities are disproportionately affected by the global economic crisis. In addition to shorter-term and immediate financial struggles, many people around the world will face prolonged financial hardship stemming from the pandemic, compounding economic inequalities around the world.
(ok, make sure you used the right buttons, you jerk...)
Ok, seriously here. I am really trying to NOT be a jerk. Did you strike out that section so we would not be depressed? I mean, you failed, but I want to know if you did it for protection (us).
That has to be the second most terrible aspect of this pandemic.
Time for a world tax (I dream out loud)
by dryrunguy LOL! I haven't even read the report yet. But when you struck through that text in your post, it struck through the text in my original post. I should be able to fix it, but I don't want anyone thinking I did that. LOL!
by Deuce
Suliso wrote: ↑Tue Jan 26, 2021 11:41 pm
Do special advantages of Australia and New Zealand really need to be spelled out? We're all smart enough to understand...
Sure, they're islands, but with air travel, that makes them as easily accessible as places like Canada and the U.S., as North America is quite different than Europe in terms of North American countries being larger and more independent of each other.
Here, the U.S./Canada land border has been closed since last March - but air travel between the countries has been allowed for some idiotic reason.
And therein lies the difference between how Australia has dealt with the virus and the manner in which most other countries have managed it. I think it has less to do with them being an island, and more to do with the way things have been managed.
Suliso wrote: ↑Tue Jan 26, 2021 11:41 pm
Do special advantages of Australia and New Zealand really need to be spelled out? We're all smart enough to understand...
Sure, they're islands, but with air travel, that makes them as easily accessible as places like Canada and the U.S., as North America is quite different than Europe in terms of North American countries being larger and more independent of each other. Here, the U.S./Canada land border has been closed since last March - but air travel between the countries has been allowed for some idiotic reason.
And therein lies the difference between how Australia has dealt with the virus and the manner in which most other countries have managed it. I think it has less to do with them being an island, and more to do with the way things have been managed.
Did you also consider thousands of lorries crossing the Canada/US border every day delivering food, factory spare parts etc? In Detroit area, for example, auto manufacturing on US side is highly integrated with just in time parts production on Canadian side. And then there is a road traffic to Alaska too. No such complications in Australia or NZ.
by atlpam My husband is scheduled for his 1st dose tomorrow. I think it will be at least May before I am eligible (phase 2). My son is in phase 1B (critical workforce - he's an Air Traffic Controller), but no word yet on when his group will be eligible (maybe March?) The scheduling is very hit or miss here in GA as you never really know when they will open up appts and every provider has a different scheduling process.
by ponchi101
Deuce wrote: ↑Wed Jan 27, 2021 2:52 am
Sure, they're islands, but with air travel, that makes them as easily accessible as places like Canada and the U.S., as North America is quite different than Europe in terms of North American countries being larger and more independent of each other.
Here, the U.S./Canada land border has been closed since last March - but air travel between the countries has been allowed for some idiotic reason.
And therein lies the difference between how Australia has dealt with the virus and the manner in which most other countries have managed it. I think it has less to do with them being an island, and more to do with the way things have been managed.
My theory is this. They are islands that did lock down very fast, and could do so. Other countries that have been successful have been Singapore (another island) and S. Korea, which is technically an island as their border with N. Korea is locked down. They also are affluent nations with large social security networks. What I said above: their population could afford a lock down and not have to worry about going hungry, which is what here in Colombia cannot be done.
Sure, they had proper a proper response, but that has been my gripe for quite a while. The income disparity between countries, which is reflected in that last terrible paragraph in Dry's report, makes it impossible for hundred of millions of people to really stop working. Bogota simply cannot remain locked down, as the small businesses (and Bogota is nothing more than small businesses) cannot afford more than one month or two of lock down. Their workers even less.
by ponchi101 BTW:
After one year of this, it seems that the Sweden experiment did not go well at all. Their death rate is huge in comparison to their three Scandinavian neighbors.
by Suliso
ponchi101 wrote: ↑Wed Jan 27, 2021 2:48 pm
BTW:
After one year of this, it seems that the Sweden experiment did not go well at all. Their death rate is huge in comparison to their three Scandinavian neighbors.
Yes, now it's quite clear. Nobody is talking about Sweden as an example in the press anymore. It's not the worst, but clearly in the bottom quarter or a third in EU.
by MJ2004 A frightening first-hand experience from a COVID survivor (an FT writer):
Covid and me: 10 days on life support
After a month in hospital, FT critic Tim Hayward reflects on his battle with coronavirus
I’d been under the weather for four days. Back then, in mid-November, the government’s pet message was the three symptoms of Covid-19: a persistent cough, loss of smell or taste, or a raised temperature. I had none of these, just the sort of chesty flu that hits me every autumn. My wife, Al, and my daughter, Liberty, both had bouts of something flu-like, so I followed orders. Then, on November 15, things suddenly got very weird, very quickly.
I woke feeling unusually short of breath. I’d bought, on the recommendation of a medical friend, a little gadget that measures SAT, the concentration of oxygen in the blood. My score was not out of the ordinary — above 94 — but something felt wrong nonetheless. Just after lunch, I called 111. I felt “out of it” and had an overpowering feeling that life would be a lot better if I could just take one decent full breath. The ambulance was outside in 15 minutes. Two reassuring medics stuck a mask on me, checked a few vital signs and said, “Yep . . . we’re seeing a lot of this . . . looks like Covid.”
Addenbrooke’s Hospital, in Cambridge, is a centre of excellence for all kinds of medicine. Everyone here knows people who work there and we live with a sense of reassurance. Even lying woozily in the back of an ambulance, it’s good to know you’re only a five-minute drive from the best minds, hands and equipment in the country. I remember someone introducing herself as a doctor from behind a mask, a visor, apron and gloves — over the next month, I’d get used to recognising people from a single strip, the bridge of the nose, tired eyes and a muffled voice. By 4pm, I was in a comfortable bed, waiting for the results of my first Covid test and “responding well” to oxygen therapy and Dexamethasone. But I wasn’t destined to get off that lightly — at 9 o’clock that night, they called Al to tell her I was being put on a ventilator.
Most people need to be knocked out to have a tube put down their throat but somehow, I’m told, I remained conscious, though I have no recollection of this at all. I’ve managed to piece together the timeline from a flurry of cheery text messages I sent, joking about the tubing and the huge bag full of brown gunge they drained from my lungs, relaying to worried family anything positive that any masked medic said. I’ve had to collate the text trail to tell this story because it’s all a merciful blank in my mind. One horrible recollection, though, remains very clear.
I am wheeled into a side room with four medics. One introduces himself as an anaesthetist; another, directly and with no hedging, tells me they’re “worried I’ll pull out the tubes” — they need to put me to sleep. There’s no debate . . . I guess that’s the point. But, like every other news junkie and doom scroller in the country, I know what this means. People who go into intensive care, who get anaesthetised and held on life support, don’t tend to have what the news euphemises as “good outcomes”. I’m hit with awful clarity that this is probably the most significant moment in my whole life. “It will just feel like going to sleep,” says the medic. True . . . but I have no idea whether I’ll wake up.
I have no religion. In fact, I remember thinking: “Well, if I don’t wake up, I won’t know anything about it.” Then they offered me my phone. I couldn’t raise Al on voice or text so, almost automatically, I thumbed on to Twitter . ..
“So this is hapimji@g In fuve mumutre they piu nr yo sleeo fky tn gayd”
Later a nurse tells me I’d become “a legend on the unit” — as I went under, they had to prise the phone from my fingers.
An anaesthetic is a cocktail. Some ingredients keep you “asleep”, others paralyse you so that you can’t roll about, dislodging the tubes, or choke. Back in November, every ICU patient still had an individual specialist nurse watching the monitors around the clock. Nourishment comes through a thin tube up your nose and goes out a catheter at the other end. To drain the constant build-up of toxic crap and to relieve the pressure of the other organs on your damaged lungs, you will probably be “proned” on 18-hour cycles — moved to a facedown position. It takes up to nine people to do it safely, keeping all the plumbing and wiring in place.
Most of the time, intensive care is there for people who’ve had massive surgery, traumatic injury or are near to death, and there’s a reason it’s not taken on lightly. It’s hard to imagine a more invasive assault on the body than paralysing it and taking over all its functions. My friend Binks is a specialist intensive care nurse who’s had way too much experience of it for her young years. As she puts it: “People don’t realise how intense intensive care is.”
I spent 10 days unconscious in the ICU, but that’s really the wrong word. The drugs, the unfamiliar sensory input, the physical treatment of my inactive body . . . “delirium” during and after ICU is an unsurprising side effect. Those days and a considerable period after were filled with dreams.
As soon as I could, I started writing them down. Thousands of words poured out, all of them ridiculous. I recalled 15 discrete dreams, each increasingly surreal. The earliest consist only of things I know or can imagine; later ones involve being injected, restrained, paralysed or frozen. The later dreams refer back to the earlier ones, creating a rigid narrative order. Scenarios include a road that can be driven only one way, a conspiracy of hippy aristocrats, Mossad, black helicopters and being kidnapped and pharmaceutically restrained with blue washing-liquid pods by the beautiful rebel daughter of Recep Tayyip Erdogan. I am to be appointed editor of the FT by MI6 — a proper delusion of grandeur. Men with rubber faces yell: “Do you know where you are?” and stuff things down my throat to the penetrating noises I will later recognise as the pings and beeps of my own monitoring equipment. Sounds quite amusing now, I know, but what’s scary is that I doubt I’ll ever forget any detail of the dreams. I’m not sure I’ll ever recover any of the real experience that they overlaid.
On the ninth day, they start reducing my sedation. I don’t immediately recover my own breathing and it’s another day before I come round. Someone yells: “Do you know where you are?” And I try to answer, “Scotland”. I don’t know who or where I am. I’m still delusional. The ICU nurse hooks up a FaceTime call with home in which, apparently, I croak, “Laptop, laptop!” through vocal cords wrecked by the tubes. They tell Al not to worry and that it’s not really me, but she’s terrified by my insane urgency. The next day, they arrange a call with my mother. She says I was so incoherent she was convinced I’d had a stroke.
Finally, I’m considered stable enough to be moved to a small Covid-19 ward that I share with two older men with dementia. They haven’t been in the ICU but their home circumstances mean they can’t look after themselves in isolation. During the days, nurses attend to us and our weird imaginings. At night, we’re woken every few hours to have all our vital signs taken. Drugs, confusion and sleep deprivation blend and I slip back, nightly, into my world of delusions. One of the men on the ward sleeps in a deep cot that seems to calm and partially restrain him. At night, I see the walls change to something imagined by Giger. The man cries out the same name over and over again and weeps inconsolably. I’m convinced by brief flashes, which show over the sides of the cot, that he’s wearing a Victorian nightgown. I dread the nights.
A new patient is brought into an empty bed. A little older than me, wiry as hell and with a collection of what may or may not be rightwing tattoos. He won’t understand that he can’t get up and roam the wards. When the nurses can, they talk him down and back to bed. On the second night, I wake to see him standing at the bottom of my bed, staring at me. I have an overpowering feeling that I don’t want to be mad any more. A couple of hours later, they wheel me into a new ward. The first thing I do is call home and demand my passport and a lift to the airport.
Over the next four days, the dreams subside and I begin to understand where I am and what’s going on. Ever-changing shifts of nurses, fully clad in PPE, come into the room to give patients food, administer medicine, change sheets and attend to those who can’t use the lavatory unaided. They are paragons of skill, concern and grace under pressure but there is, apparently, a limit to the time they can be exposed to us. In spite of their kindness and attentiveness, it doesn’t take many hours of mental clarity to begin to feel the sense of being locked up, like prisoners or dangerous animals. The staff, meanwhile, grow more pressured as the weeks pass. One morning, a nurse announces that they’re short-staffed and covering double shifts, so they only have time for “patient safety”. We must not use our call buttons if we can possibly avoid it and it may take them a while to respond.
The doctors, on their daily rounds, stop prefacing every interaction with “Do you know where you are?” While I was unconscious, one explains, I “sustained some neurological damage” — this is apparently not uncommon. My left foot is a bit numb, tests show my right arm to be mildly affected, but I have no movement at all in my right ankle and foot. No voluntary control, just very uncomfortable “pins and needles”. I have a “drop foot” that will require a brace to aid walking, a Zimmer frame while I learn to use it and, eventually, a walking stick.
In the early hours of the next morning, a nurse notices that my heart is beating at around 200BPM. In seconds, half a dozen masked medics appear. At the bottom of the bed is a big red-wheeled cabinet, with two paddles hanging off the side and “CRASH CART” in screamingly loud caps. Once they’ve explained that they won’t be shocking me, they hook up drugs and fluids, saying it’s probably a side effect of one of the many drugs they’ve used on me. Later, I’m put into a CT scanner where they discover I have a pulmonary embolism, a bloodclot in my lung. They won’t need to operate but instead inject me with “clot-buster” drugs daily. Later, I’ll be able to take these orally . . . for many months.
On December 15, I’m discharged with a big bag of pills and an assurance that community teams will be in touch to support my recovery. I was in Addenbrooke’s for 30 days. For about half that time, I was on oxygen; for 10 days, I was fully unconscious and on life support. For 30 days, I didn’t use most of my muscles and spent only minutes out of bed. I lost just over 14kg in weight, around two stone. I’d like to say it was all fat but, sadly, a lot of it is muscle.
My legs look like two bits of grey wool, my stomach is pleasingly flat, but so is my chest. I get exhausted after about 10 minutes of anything. My voice has lost its resonance and I’m cold all the time — no muscles working to generate heat, no fat to insulate. All of this, they tell me, is likely to come back with the physiotherapy. The “clot-busters” should get rid of my embolism, though I’ll have to take drugs for it daily, and take precautions to avoid any bleeding. If I nick myself with a kitchen knife, it may well need a tourniquet not a blue plaster.
One month on, with rest and daily physiotherapy, I’m building up strength and stamina, my voice is returning and I’m even beginning to get some limited movement in the “drop foot”. It’s likely I’ll always have to wear a brace and I have to sell my beloved stick-shift sports car. The month inside was the longest I’ve gone without alcohol since I was 16 and, as most of my life is now taken up with re-learning my sense of balance, I’m disinclined to do anything that might interfere with it. I doubt I’ll ever be teetotal but I have a chance to reassess my drinking . . . C’mon, you’ve got to look for the positives.
Unlike many who go through intensive care, I haven’t displayed symptoms of PTSD. Being asked to write this and being able to express it, is one of the reasons I can hope that I won’t. For a while, I was uncomfortable watching hospital footage on the news, but that seems to have passed. All the symptoms of actual Covid-19 are gone and I’m left with the injuries and impairments sustained in the process of saving my life — but, honestly, I’m just so bloody glad to be alive that it hardly matters.
I do struggle with survivor’s guilt. If I’d gone to sleep in ICU and not woken up, I’d have known nothing of it. My family, friends, the people the pandemic has taught us to call “loved ones”, had to confront the possibility of bereavement, unsure for days whether I was going to live or die in isolation, unable to say goodbye. Like the doctors and nurses in the hospital, I can’t speak for them, but I’m left with the feeling that they all had a worse ride than I did.
Since I was discharged, the situation in hospitals and community care has got significantly worse. I’m unbelievably lucky . . . Lucky to have lived and lucky enough to be in a position to contemplate six months “off work” to heal physically. I can’t begin to imagine how tough this is going to be for Covid-19 victims without that luck. But it’s the delirium that I still find most difficult to handle. Some people in the profession have warned that we’re unprepared for the mental health implications of the pandemic and I can’t disagree. I wasn’t expecting to spend two weeks palpably and certifiably insane. I didn’t “die” at any point in my treatment. I didn’t start drifting toward a great white light and have to be brought back by the jolt of the paddles, but — along with a stick and a brace to remind me of 2020 — I will always live with an experience of “madness”, and that is more difficult to come to terms with.
Tim Hayward is an FT contributing writer.
by Deuce
Suliso wrote: ↑Wed Jan 27, 2021 8:04 am
Did you also consider thousands of lorries crossing the Canada/US border every day delivering food, factory spare parts etc? In Detroit area, for example, auto manufacturing on US side is highly integrated with just in time parts production on Canadian side. And then there is a road traffic to Alaska too. No such complications in Australia or NZ.
ponchi101 wrote: ↑Wed Jan 27, 2021 2:44 pm
My theory is this. They are islands that did lock down very fast, and could do so. Other countries that have been successful have been Singapore (another island) and S. Korea, which is technically an island as their border with N. Korea is locked down. They also are affluent nations with large social security networks. What I said above: their population could afford a lock down and not have to worry about going hungry, which is what here in Colombia cannot be done.
Sure, they had proper a proper response, but that has been my gripe for quite a while. The income disparity between countries, which is reflected in that last terrible paragraph in Dry's report, makes it impossible for hundred of millions of people to really stop working. Bogota simply cannot remain locked down, as the small businesses (and Bogota is nothing more than small businesses) cannot afford more than one month or two of lock down. Their workers even less.
Granted. But comparing countries which are well off financially with those which are not financially well off is a game of apples and oranges.
When we get down to comparing apples with apples, even if the respective apples may be of slightly different varieties, I believe it is still a more valid comparison...
Canada is often viewed as being quite similar to Australia in that both countries have similar wealth, both countries possess a large land mass, both possess generously populated cities which are quite spread out from each other, and with lots of uninhabited land in between the cities. In terms of climate, Canada's winters are somewhat more harsh than are those of Australia - but that doesn't enter into this equation, because Australia was doing significantly better with the virus even before our Canadian winter set in (and we've had a comparatively mild winter thus far, at that).
Canada is not among the worst countries in terms of our management of the virus, but nor are we among the best. We're sort of somewhere in the middle. Australia is among the very best. And while some of that success can be attributed to the fact that they are an island, I believe that the majority of the discrepancy - by a significant amount - between Canada's results and those of Australia when it comes to management of the virus is due to the significantly different manners in which both countries have dealt with the virus situation.
Australia has been much more strict. I echo the words of several people on the front lines of this battle in saying that theirs is a recipe that other countries would do well to copy.
by ponchi101
MJ2004 wrote: ↑Wed Jan 27, 2021 6:11 pm
A frightening first-hand experience from a COVID survivor (an FT writer):
Covid and me: 10 days on life support
After a month in hospital, FT critic Tim Hayward reflects on his battle with coronavirus
...
Tim Hayward is an FT contributing writer.
Excellent piece.
by JazzNU My dad and his wife both got their first covid shots in South Carolina today. They got the Pfizer shots.
by JazzNU
Germany recommends AstraZeneca COVID-19 shot only for under 65s
BERLIN (Reuters) - AstraZeneca’s COVID-19 vaccine should only be given to people aged between 18 and 64, Germany’s vaccine committee said in a draft recommendation, a day ahead of a decision by European regulators on whether to approve the drugmaker’s shot.
“There are currently insufficient data available to assess the vaccine efficacy from 65 years of age,” the committee, also known as Stiko, said in a draft resolution made available by the German health ministry on Thursday.
“The AstraZeneca vaccine, unlike the mRNA vaccines, should only be offered to people aged 18-64 years at each stage,” it added.
Stiko’s assessment was based on the same trial data published by medical journal The Lancet on Dec 8.
The European Union approved a vaccine developed by Pfizer and its German partner BioNTech in late December, and gave the green light to a shot made by Moderna in early January.
AstraZeneca did not immediately respond to a request for comment.
On Monday, the drugmaker denied that its COVID-19 vaccine is not very effective for people over 65, after German media reports said officials fear the vaccine may not be approved in the European Union for use in the elderly.
The German health ministry said of the 341 people vaccinated in the group aged 65 and over, only one became infected with the coronavirus, meaning the expert vaccine panel had not been able to derive a statistically significant statement.
AstraZeneca Chief Executive Pascal Soriot said the company had less data than other drugmakers on the elderly because it started vaccinating older people later.
“But we have strong data showing very strong antibody production against the virus in the elderly, similar to what we see in younger people,” he told Die Welt newspaper in an interview earlier this week.
Germany is grappling with limited vaccine doses after Pfizer and AstraZeneca announced delays to deliveries in recent weeks, and Health Minister Jens Spahn warned the shortage would last well into April.
Spahn said there were younger age groups with existing conditions who were waiting to be vaccinated, adding the final recommendation on the use of the AstraZeneca shot would only come following EU approval.
As well as those aged over 80 and people living in senior citizens’ homes, Germany is prioritising front-line medical and care staff.
In late December, Britain became the first country to approve the coronavirus vaccine developed by Oxford University and AstraZeneca.
The government said it would not recommend one vaccine over another for different cohorts of the population, even though data on the AstraZeneca/Oxford shot’s efficacy in older people is currently limited.
It began rolling out the vaccine in January in a campaign that has targeted older people and seen more than 7 million given their first dose. Britain has also been using the vaccine developed by Pfizer and BioNTech.
Reporting by Caroline Copley; Additional reporting by Emma Thomasson and Ludwig Burger; Editing by Maria Sheahan and Alexandra Hudson
Germany recommends AstraZeneca COVID-19 shot only for under 65s
... The German health ministry said of the 341 people vaccinated in the group aged 65 and over, only one became infected with the coronavirus, meaning the expert vaccine panel had not been able to derive a statistically significant statement.
...
Reporting by Caroline Copley; Additional reporting by Emma Thomasson and Ludwig Burger; Editing by Maria Sheahan and Alexandra Hudson
So... what's the problem?
Sure, keep doing the statistical analysis. But I am confused.
by Suliso That's great for younger people. The oldies will get Pfizer instead.
by JazzNU
ponchi101 wrote: ↑Fri Jan 29, 2021 8:19 pm
So... what's the problem?
Sure, keep doing the statistical analysis. But I am confused.
Not from this article, but from previous reporting, it sounded as if there were too few participants in the over 65 group to reach a conclusion scientists were comfortable with.
I'd be super concerned with getting this one personally if you're in the upper section of the range if the full research review backs this up. So, I'm 60-64 and good to go? Am I still just as good when I turn 65 in May or ??? I don't get that.
by ti-amie Ask Jared.
Trump White House donated 8,700 ventilators to other nations. Officials now don’t know where many of them are, watchdog finds.
By
Yeganeh Torbati and
Lenny Bernstein
Jan. 29, 2021 at 1:42 p.m. EST
The Trump administration spent $200 million to send more than 8,700 ventilators to countries around the world last year, with no clear criteria for determining who should get them and no way to keep track of where many ended up, according to a new report from the Government Accountability Office.
The effort, driven by the Trump White House, was an unusual top-down initiative with little decision-making by experts at the U.S. Agency for International Development, which carried out the administration’s orders. Former president Donald Trump last year boasted about U.S. success in manufacturing the machines and declared the U.S. “the king of ventilators," promising donations to foreign countries.
Staff on the White House’s National Security Council communicated to the aid agency “U.S. government decisions regarding ventilator donations, including the recipient countries, quantities, and manufacturers,” the GAO found.
“These ventilators were not in State or AID’s strategic plan,” said David Gootnick, director of international affairs and trade at GAO. “They could not articulate for us the criteria they used for what ventilators went to what countries.”
The GAO was unable to identify how the Trump White House made its decisions on ventilator allocations, and White House officials did not respond to the watchdog’s questions, which came before President Biden took office last week. For instance, while Sri Lanka had just three new coronavirus cases per day when it received 200 ventilators, Bangladesh, which had 1,409 new cases, received just 100 of the machines, the report found.
Relatively wealthy recipients such as Italy and St. Kitts and Nevis also received ventilator donations, as did tiny island nations such as Nauru and Kiribati, which have yet to report a single coronavirus case.
ProPublica reported last year that the ventilator donation effort was marked by dysfunction and little clarity on how countries were chosen for the donations. The GAO’s findings largely confirmed that report and provided new details, finding that USAID ultimately spent $200 million to send 8,722 ventilators to 43 countries.
Throughout last year, USAID and White House officials frequently publicized the donations on social media, sharing pictures of large boxes plastered with USAID’s logo ready to be shipped out.
USAID and the State Department did not immediately respond to requests for comment, and a White House spokeswoman referred questions to them. The companies that manufactured the ventilators donated by USAID — Vyaire Medical, Zoll Medical and Medtronic — did not immediately respond. Chemonics, the development consulting firm that USAID paid to deliver the ventilators, confirmed its role in the ventilator deliveries and referred other questions to USAID.
“USAID-donated ventilators have equipped medical providers to deliver quality care that is saving lives around the world,” the agency said in a response to GAO’s findings, sent to the watchdog on Jan. 6.
The process revealed in the report runs counter to how foreign assistance usually works. Although officials at the White House may set priorities for foreign aid, Republican and Democratic administrations alike have generally left the details of the aid, how it is distributed, and on what basis it is allocated to experts within USAID, which has local missions around the world that work closely with their host countries to determine needs.
Ventilators are usually used in intensive care units to help the sickest pulmonary patients breathe. In the early days of the pandemic, a shortage of the devices became a symbol of how ill-prepared the United States was for this crisis, with Trump and New York Gov. Andrew Cuomo publicly arguing about the number New York hospitals would need.
Later, hospitals turned to alternatives for some patients and manufacturers churned out more of the devices, which are still widely employed for the most seriously ill covid-19 patients.
Global health experts say ventilator donations, while flashy and attention-getting, are often less useful than more basic health aid, such as simple oxygen delivery or protective personal equipment. Ventilator manuals often come in just a few major languages, and the machines require expert maintenance and operation — obstacles for stretched hospital staff in poor countries.
“I don’t think it’s at all just USAID,” said Rebecca Inglis, a physician specializing in intensive care who researches care for critically ill patients in places with few resources. “Donor organizations around the world have failed to realize that a ventilator is nothing without the people who can operate it safely and without the maintenance contracts.”
USAID said in its response to GAO that its ventilator donations included warranties, service plans, initial supplies of accessory equipment, and training.
“USAID’s investments in training are boosting the capacity of frontline workers to deliver quality care to patients in need in dozens of countries,” the agency said.
USAID also questioned whether the number of coronavirus cases is the best metric to judge the ventilator donations, given the pandemic is “not static.” The agency added that the Trump administration’s decisions on ventilator allocations were based “in part” on USAID data.
As of December, USAID and the State Department had very limited visibility into where the ventilators actually are, Gootnick said, making it difficult to know whether the aid it gave out is being used appropriately. In only 12 of 43 countries did the government have a fairly good idea where the ventilators are, he said.
USAID is now trying to figure out where the ventilators went, the report said.
While USAID rules typically require officials to monitor whether foreign aid efforts achieve their intended goals, agency officials told the GAO that it considers the ventilator donations exempt from some of those monitoring requirements.
The cost of donating the machines came out of several extra pots of money, totaling some $685 million, that Congress provided to the State Department and USAID last year to help combat the coronavirus pandemic globally, the GAO found.
In 21 of the 43 recipient countries, the cost of ventilator donations made up more than half of the extra covid-19 funding that USAID provided to those countries, the GAO found. In El Salvador, Paraguay, Egypt, and several other countries, the entire coronavirus aid budget was consumed by the ventilator donations.
“When I’m sitting there writing a budget for how a country should spend its covid money, you definitely wouldn’t dedicate that high a proportion to isolated procurement of mechanical ventilators,” Inglis said.
by JazzNU Testing out double masking at home today to see how I do, see which combo works best for me if any do. Anyone else double masking or planning to? I wasn't thinking much about it, feel comfortable and safe when I'm out, but there's been a lot of discussion about it this week. And the first case of the UK variant has been detected in my county, a person with no travel history, so thought it time for me to look into if I can manage it, see if it throws off my breathing too much or is workable.
by ponchi101 I had not thought about it. N95's are readily available everywhere here (heck, there are people on modified motorcycles riding the streets selling you a full kit with everything you need) so I don't know if I will go for double masking.
by Deuce I've been using KN95s - with a paper towel as a filter - pretty much since the outset. I don't believe I'll change from that.
Eye protection is interesting - in that we seem to hear about it in waves. We'll hear a significant amount about it for a week or so - with recommendations to wear a plastic visor or some sort of goggles or glasses... and then we'll hear nothing about it for a couple of months...
Strange.
by ti-amie I'm not sure about double masking. Fresh Direct has N95's available now. I hope they still do by my delivery date.
I have a shield for my face but I haven't used it yet.
by Suliso I have my company issued double cloth mask (5 pairs). Good enough, not going to change unless forced.
by JazzNU You guys are making me feel better about maybe forgoing the double mask for now. I wasn't all that comfortable in the first combo I tried, better in the 2nd and 3rd.I have the 3-ply disposable masks that are have been recommended by doctors and 5 cloth masks that I got back in the spring from different sellers on Etsy that are all 2 or 3 layers with room for a filter and I bought polyethylene foam sheets to use as filters. It's been working great and I'm comfortable in what I have. But the UK variant makes me wonder if it's enough. I can't really tell what they are and aren't doing there to know if I need to do better.
by dryrunguy Speaking of double masking, here's today's Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 101.05 million cases and 2.18 million deaths as of 1pm EST on January 29. The global cumulative incidence surpassed 100 million cases on January 28.
1 case to 20 million: 220 days
20 to 40 million: 68 days
40 to 60 million: 38 days
60 to 80 million: 32 days
80 to 100 million: 32 days
On January 23, the United Kingdom surpassed 100,000 cumulative deaths*, and Mexico surpassed 150,000 cumulative deaths on January 25. With these milestones in mind, we will take another look at national-level cumulative COVID-19 mortality data.
*Deaths within 28 days of a positive SARS-CoV-2 test.
In terms of total cumulative mortality, the UK (104,371) is currently #5 globally, and Mexico (155,145) is #4. The United States (427,626 deaths), Brazil (221,547), and India (154,010) represent the top 3. In total, 12 countries have reported more than 50,000 cumulative deaths, including 6 in Europe, 4 in the Americas, 1 Asia, and 1 in the Eastern Mediterranean region. Together, these 12 countries account for 70% of the total global deaths. A total of 133 countries and territories (of 179 total) have reported fewer than 5,000 cumulative deaths, including 91 with fewer than 1,000 and 38 with fewer than 100.
In terms of per capita mortality, there are 28 countries with more than 1,000 cumulative deaths per million population, which corresponds to more than 1 death for every 1,000 people. San Marino is #1 with 1,915, followed by #2 Belgium (1,810) and #3 Slovenia (1,658). The US is #10 with 1,309 deaths per million. Of these 28 countries, 21 are in Europe, and 7 are in the Americas. The global average is 279.63 cumulative deaths per million population. At the other end of the spectrum, 86 countries and territories have reported fewer than 100 deaths per million. Additionally, 30 countries and territories have reported fewer than 10 deaths per million, and 9 have reported fewer than 2.
Our World in Data reports that 86.14 million vaccine doses have been administered globally, a 50% increase since this time last week.
UNITED STATES
The US CDC reported 25.46 million total cases and 427,626 deaths. Daily incidence continues to decrease, down to 161,832, the lowest average since November 17* and 35% lower than the peak on January 8 (248,706).
*Excluding the week after Thanksgiving, during which the average was depressed due to delayed holiday reporting.
Yesterday, the US daily mortality returned to approximately 3,300 deaths per day. Overall, the daily mortality has remained relatively consistent for more than 2 weeks. Whether steady at approximately 3,300 or 3,100** deaths per day, the overall daily mortality has not fluctuated much from day to day since mid-January. Daily incidence continues to decrease, and it likely peaked somewhere between mid-December and mid-January—although difficult to determine exactly when due to fluctuations in reporting around the winter holidays. If this is the case, we expect to observe an associated decrease in daily mortality starting sometime in the next week or two.
**During the week following the Martin Luther King, Jr. Day holiday weekend, the average daily mortality dropped from approximately 3,300 to 3,100 deaths per day due to delayed reporting over the holiday weekend; however, even with this decrease, the daily mortality remained relatively constant until it increased again to 3,300.
The US CDC reported 48.39 million vaccine doses distributed and 26.19 million doses administered, including 3.10 million administered in long-term care facilities (LTCFs). The US has administered 54.1% of the distributed doses, which is actually a slight decrease from Monday’s update (54.9%). In total, 21.70 million people have received at least 1 dose of the vaccine, and 4.26 million have received both doses. The US is now averaging 1.24 million doses administered per day. The breakdown of doses by manufacturer remains relatively even, with slightly more Pfizer/BioNTech doses administered (14.36 million; 55%) than Moderna (11.74 million; 45%).
The Johns Hopkins CSSE dashboard reported 25.84 million US cases and 434,696 deaths as of 2:30pm EST on January 29.
US VACCINATION STRATEGY The US is continuing to adapt its SARS-CoV-2 vaccination strategy as the new presidential administration settles into office. Earlier this week, US President Joe Biden expressed confidence that the US will have enough supply to vaccinate 300 million individuals by the end of the summer. As part of this effort the federal government is negotiating the purchase of approximately more 200 million doses, 100 million each of the Pfizer/BioNTech and Moderna vaccines. Despite plans to scale up supply and distribution, the White House’s COVID-19 response team is calling for patience from the American people, noting that it will likely be months before everyone who would like a vaccine can get one. The administration is currently on track to meet its goal of vaccinating 100 million individuals in the first 100 days after President Biden took office.
Even with increased supply and distribution, a number of barriers remain to vaccinating the US population. Notably, the absence of a federal vaccine stockpile has led states to reserve half of their allocation to ensure enough supply for second doses, which is slowing vaccination efforts. Until states can have confidence in longer-term planning for vaccine deliveries, many will likely continue to reserve doses. Additionally, some of the world’s largest syringe manufacturers warn that the demand for specialized syringes—such as the low-dead volume syringes—may soon exceed production capacity. Without the low-dead volume syringes, vaccinators may not be able to draw extra doses from each vial, which could reduce the number of available doses by 17%. In an effort to support states’ vaccination operations, the Department of Defense is reportedly evaluating plans to use military personnel to supplement vaccinators. The plan could deploy military personnel domestically to assist in the logistics and vaccine administration at federal vaccination sites. FEMA intends to establish 100 vaccination sites nationwide in the coming months, but any deployment of active duty military personnel would require approval by state governments.
VACCINES & ALLERGIC REACTIONS The US CDC published new data on the incidence of allergic reactions following vaccination. The CDC reported 50 incidents of anaphylaxis after vaccination with the Pfizer product and 21 instances after receiving the Moderna vaccine, which corresponds to approximately 5 reactions per million doses for the Pfizer vaccine and 2.8 per million doses for the Moderna vaccine. Notably, the rate for the Pfizer vaccine is less than half what it was in late December (11.1 per million), although the rate for the Moderna vaccine increased slightly compared to the data reported through January 10 (2.5 per million). To date the CDC has reported no deaths due to an allergic reaction following vaccination.
EMERGING VARIANTS The recently discovered SARS-CoV-2 variants of concern continue to spread around the world. The B.1.351 variant was identified in South Carolina this week, the first time the variant has been reported in the US. The variant was identified in 2 patients with no known international travel history, and notably, there is “no known connection between these two cases.” This provides a good indication that the variant is already circulating in the community. The B.1.351 variant has already been identified in 30 countries, and has recently garnered attention due to its potential to reduce the effectiveness of SARS-CoV-2 vaccines.
The absence of large-scale genomic sequencing efforts in the US has left the country more vulnerable to the spread of these new SARS-CoV-2 variants, and many health experts have called for national programs to enhance domestic sequencing capabilities. Currently, approximately 3,000 specimens are sequenced each week, out of 1.4 million positive tests. These efforts are principally led by “a patchwork of academic, state and commercial laboratories” rather than a formal, centralized, and coordinated national system. Coverage by existing sequencing efforts varies widely by state, with some states reporting no sequencing data at all during the pandemic. Without proactive efforts to sequence specimens collected across the country, there is no effective way to identify the emergence or introduction of new variants or monitor their geographic spread.
ASTRAZENECA/OXFORD VACCINE After receiving the application for conditional authorization of the AstraZeneca/Oxford University vaccine on January 12, the European Medicines Agency (EMA) issued its recommendation today that the vaccine receive conditional marketing authorization in Europe. Prior to the EMA’s assessment, German officials called for the vaccine to be authorized only for adults under the age of 65, due to a dearth of efficacy data among older adults. German officials emphasized that there are no data suggesting that the vaccine is less efficacious in this age group, but rather, that the efficacy data are not sufficient to make a determination. The vaccine is already being administered in the UK, including to adults 65 years and older, and UK officials indicate that there is no evidence that the vaccine is less effective in older adults. German officials expected the EMA to include an age restriction in its recommendation, but the EMA recommendation did not include a maximum age limit.
In addition to concerns regarding the AstraZeneca/Oxford vaccine’s efficacy, AstraZeneca announced that production is lower than anticipated and that it will be unable to deliver the full order to the EU on time, potentially only 25% of the total doses by the end of March. The shortfall raised concerns that doses that should have been allocated to the EU were being sold to other countries. Officials from the European Commission have demanded AstraZeneca meet its commitment to the EU, even if it means diverting doses from the UK. Driven by the situation with AstraZeneca, the European Commission is implementing an “export transparency mechanism” for SARS-CoV-2 vaccines manufactured in the EU, which will require permission before exporting doses for sale. Humanitarian donations would not be affected. There are currently 2 facilities in the EU that are manufacturing the AstraZeneca/Oxford vaccine, but it remains to be seen how the new transparency measure would ultimately affect allocation of vaccine doses produced within the EU.
J&J/JANSSEN VACCINE Johnson & Johnson (J&J) announced interim efficacy data from the Phase 3 clinical trials of its SARS-CoV-2 vaccine candidate, developed in partnership with Janssen Pharmaceuticals. Overall, the vaccine demonstrated 66% efficacy in preventing moderate-to-severe COVID-19 disease across several trial locations: the US (72%), Latin America (66%), and South Africa (57%). The lower efficacy in Latin America and South Africa prompted concern about the vaccine’s protection against emerging variants, including B.1.351 which is circulating widely in South Africa. Notably, the J&J press release indicated that “nearly all cases of COVID-19 (95%) [in South Africa] were due to infection with...the B.1.351 lineage.” The vaccine demonstrated 85% efficacy in terms of preventing severe disease across all locations, regardless of the variant. Additionally, J&J noted that the vaccine “demonstrated complete protection against COVID-related hospitalization and death” after 28 days post-vaccination. The Phase 3 trials included nearly 44,000 participants across 8 countries on 3 continents. A study of the vaccine using 2 doses is still underway.
In contrast to the existing SARS-CoV-2 vaccines, the J&J/Janssen vaccine requires only a single dose, so while the efficacy is lower than for other products, it could provide benefit in terms of accelerating vaccination coverage. Additionally, it can be stored for up to 3 months at refrigerator temperature (ie, 35.6-46.4°F; 2-8°C). J&J intends to submit its application for Emergency Use Authorization (EUA) to the US FDA in “early February” with the goal of having supply available to distribute immediately. Even without efficacy in the 90%+ range, the J&J/Janssen is expected to be another valuable tool in combating COVID-19.
The results were published via press release, and to our knowledge, the trial data have not been published publicly or subjected to peer review; however, J&J committed to submitting “a comprehensive...data set” to a peer-reviewed journal in the near future.
NOVAVAX VACCINE Novavax issued a press release with preliminary Phase 2b and Phase 3 clinical trial results for its candidate SARS-CoV-2 vaccine. The vaccine demonstrated an overall efficacy of 89.3% in Phase 3 trials conducted in the UK. The UK trials included more than 15,000 participants, and of the 62 cases reported, 56 were in the placebo group, and 61 were mild or moderate cases. The only severe case was among the placebo group. Of 56 infections that were sequenced, 32 (57%) were due to the B.1.1.7 variant*. Further analysis indicates that the vaccine demonstrated 95.6% efficacy against the original strain and 85.6% against the B.1.1.7 variant.
*Described in the press release as the “UK variant strain,” which we presume to mean the B.1.1.7 variant, which was first reported in the UK.
Novavax also reported interim results from Phase 2b clinical trials in South Africa. Overall, the vaccine demonstrated 60% efficacy in preventing mild, moderate, or severe disease in HIV-negative participants (49.4% efficacy in HIV-positive participants). Sequencing data are available for 27 or 44 total cases, and 25 (92.6%) of the infections were due to the B.1.351 variant**.
**Described in the press release as “the triple mutant variant...widely circulating in South Africa,” which we presume to mean the B.1.351 variant, which was first reported in South Africa.
The underlying data for these results have not yet been published publicly or subjected to peer review, but Novavax intends to publish them via “prepublication servers” and submit them to a peer-reviewed journal. Additionally, Novavax is submitting data on a rolling basis to the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) in order to streamline the review process. In addition to these trials, further Phase 3 trials are ongoing in the US and Mexico, which have enrolled more than 16,000 of the target 30,000 participants. The timeline for completing the US-Mexico trials or submitting an EUA application to the US FDA remains uncertain.
Like existing SARS-CoV-2 vaccines, the Novavax candidate requires 2 doses, administered 21 days apart, although it can be stored for a prolonged period (6 months minimum) at refrigerator temperatures (ie, 35.6-46.4°F; 2-8°C)—and even 24 hours at room temperature—which will facilitate distribution and storage at the local level. While the vaccine appears to be less efficacious against the B.1.351 strain, Novavax is reportedly already developing a new version of the vaccine to better protect against the emerging variant.
DOUBLE MASKING The idea of “double masking”—ie, wearing 2 masks on top of one another rather than a single mask—has emerged over the past week or so in the US. The idea itself is not new, but it gained attention following recent comments by Dr. Anthony Fauci in support of wearing multiple masks. Dr. Fauci’s comments reference emerging SARS-CoV-2 variants that appear to be more transmissible than those circulating earlier in the pandemic, which could necessitate enhanced risk mitigation measures to sufficiently reduce transmission risk. Wearing an extra mask aims to provide additional layers of filtration for inhaled and exhaled air with the ultimate goal of further decreasing SARS-CoV-2 transmission risk.
Dr. Fauci stated that the benefit of double masking is “common sense,” but to our knowledge, the evidence supporting increased effectiveness is limited. Masks can vary considerably—including in terms of design, construction, materials, and fit—which make it difficult to accurately determine any increase in the effect of adding subsequent masks. Notably, the US CDC already recommends selecting a mask constructed with multiple layers. It is well established that face masks and coverings can reduce transmission risk, if used properly, and we continue to recommend following the CDC guidance regarding face coverings, particularly when appropriate physical distancing cannot be maintained. We will continue to monitor emerging evidence and guidance regarding double masking.
EUROPE CONTROL MEASURES Despite vaccination struggles, some countries in Europe are beginning to evaluate and implement steps to ease COVID-19 restrictions. England’s current national “lockdown” is scheduled to continue through March 8, and UK Prime Minister Boris Johnson indicated that in-person education will not resume before then, and the ultimate decision could hinge on vaccination progress. The UK aims to complete the first dose of vaccine for its highest-priority populations by February 15. England could begin phasing out the lockdown beginning the week of February 22, but nonessential shops, pubs, and restaurants are expected to remain closed into March. In addition to domestic restrictions, arriving international travelers from 22 hotspot countries, including South Africa and all of South America, will be required to quarantine for 10 days upon arrival, over concerns regarding highly transmissible emerging variants.
After 3 weeks of national “lockdown,” Cyprus will begin loosening restrictions in early February. Cyprus’ Minister of Health, Constantinos Ioannou, announced that the country would begin easing restrictions starting February 1. The efforts will reportedly begin with “hair and beauty salons,” followed by retail stores and elementary schools. Cyprus will maintain some restrictions, such as limits on large gatherings—including for religious services—and mandatory notification (via text message) before leaving one’s home, in order to mitigate the risk of increasing social activity too rapidly.
AFRICA The Africa CDC announced that it secured another 400 million doses of the AstraZeneca/Oxford vaccine, manufactured by India’s Serum Institute. This adds to the 270 million doses previously secured from Pfizer, AstraZeneca, and Johnson & Johnson (J&J). Countries in Africa are also expected to receive 600 million doses through the WHO’s COVAX initiative, which could ultimately provide enough vaccine to cover 2 doses for more than 600 million people—approximately half of the continent’s 1.2 billion people. A WHO spokesperson remarked that vaccinating 35% of Africa’s population by the end of 2021 is a “realistic assumption,” but many obstacles remain. In addition to vaccine supply and distribution, acceptance remains a problem in many countries, compounded by widespread misinformation. For example, Tanzanian President John Magufuli openly opposes the SARS-CoV-2 vaccines He has claimed that Tanzanians will be used as “guinea pigs,” and he has already declared COVID-19 to be eliminated in the country. Notably, Tanzania has not reported COVID-19 data since April 2020, when it reported only 509 cumulative cases.
While African countries struggle to secure enough doses of vaccine to protect their populations, many across the continent are also struggling with a surge of transmission and increased mortality. Dr. John Nkengasong, Director of the Africa CDC, noted that health systems in Africa are becoming overwhelmed by the current surge, which may be exacerbated by the emergence of highly transmissible variants, including B.1.351. To date, only 2 countries in sub-Saharan Africa—Mauritius and Seychelles—have commenced vaccination efforts. While many African nations managed to contain COVID-19 throughout 2020, the ongoing surge is a reminder that no country is safe from the pandemic, and without access to critical vaccine supply—which is largely limited to higher-income countries for now—fragile public health and healthcare systems in Africa could be at risk.
MANAUS, BRAZIL A study published in The Lancet analyzed the increased SARS-CoV-2 transmission in Manaus, Brazil, a region that had previously shown high levels of seroprevalence among its community members. A study conducted in October 2020 detected SARS-CoV-2 antibodies in samples from 76% of blood donors, which suggested that the region may have reached the threshold to provide some level of community immunity (ie, herd immunity). Despite the high seroprevalence, Manaus exhibited a large surge in COVID-19 cases and hospitalizations in January 2021.
The researchers present 4 possible explanations for the surprising surge in cases. First, the previous study could have overestimated the seroprevalence, which could have put the community below the herd immunity threshold. Second, immunity to SARS-CoV-2 conferred by earlier infection could have waned, resulting in re-infections. Third, the new infectious could be a result of emerging variants, including the P.1 variant first reported in the area, that are less susceptible to antibodies from prior infections. And finally, new SARS-CoV-2 lineages could simply be exhibiting much higher transmissibility, which could allow widespread community transmission even in areas with high existing seroprevalence. The researchers note that these theories are not mutually exclusive, and further study is needed to better characterize the factors driving the current resurgence. In particular, it is critical to investigate the potential that emerging variants could evade antibodies developed from infection with other strains, which could inform response activities in communities around the world.
MONOCLONAL ANTIBODIES Regeneron reported interim results from clinical trials for prophylactic use of its monoclonal antibody cocktail. The trial, conducted by researchers from the National Institute of Allergy and Infectious Diseases (NIAID), included 400 participants who were determined to be at high risk for infection due to living in the same household as a COVID-19 patient. In total, 186 participants received the antibody cocktail (casirivimab and imdevimab) prophylactically as a “passive vaccination,” and 223 received a placebo. Those in the treatment group exhibited a 100% reduction in the risk of symptomatic COVID-19 disease (0 out of 186) compared to the control group (8 out of 223) and a 50% reduction in the risk of infection, including asymptomatic—10/186 (5.4%) compared to 23/223 (10.3%). Additionally, infected individuals in the placebo group had nearly 100-fold higher peak viral loads than those in the treatment group.
This is a relatively small study population, but it provides evidence that there could be other options to provide protection beyond vaccines. The ability to administer monoclonal antibodies prophylactically could potentially be used to provide protection for exposed individuals who may not have time to develop immunity following a true vaccination. This study has not yet been subjected to peer review, and further study is needed to more fully characterize the prophylactic effect of the treatment.
OXYGEN SHORTAGE As we have covered previously, the evolving clinical treatment standards for COVID-19 patients are driving a shortage of oxygen, in the US and countries around the world. The use of high-flow oxygen, as opposed to mechanical ventilation, is placing strain on oxygen production and use capacity, which has resulted in efforts to mitigate the increase in use and identify solutions to bolster capacity. Dr. Eric Toner, from the Johns Hopkins Center for Health Security, published an overview of the challenges, lessons from existing efforts, and recommendations to combat shortages in the coming weeks and months, based on the experiences of clinicians and public health officials in California, Minnesota, and New York (US). High-flow oxygen uses 5-10 times the volume as a mechanical ventilator, and the increased flow, and associated decrease in temperature, is causing liquid oxygen vaporizers to freeze. Some facilities are using portable oxygen canisters to mitigate this risk, which is driving a subsequent shortage in canisters and regulators. And with the overall increase in demand, the larger supply network is struggling to provide necessary deliveries to healthcare facilities.
In order to mitigate these effects, hospitals and health systems are implementing a myriad of novel solutions. To reduce the risk of vaporizers freezing, some facilities are adding secondary supply lines, which can be connected to liquid oxygen tanks to divide the oxygen flow through additional vaporizers, or using warm water sprinkler systems to maintain vaporizer temperatures above freezing. The use of oxygen concentrators, as opposed to liquid oxygen tanks, can provide supplementary oxygen without the need for vaporizers. Additionally, lowering the oxygen saturation threshold for patients can reduce demand, and statewide coordination can help manage effective distribution of liquid oxygen and equipment to where it is needed most. Despite these efforts, solutions are still needed for a number of issues, including awareness of oxygen shortages and associated conservation efforts, cross-jurisdictional/interstate coordination regarding oxygen supply, transportation standards to facilitate deliveries, and manufacturing capacity for critical equipment (eg, regulators, vaporizers, cylinders).
by ponchi101 Quote:
In terms of per capita mortality, there are 28 countries with more than 1,000 cumulative deaths per million population, which corresponds to more than 1 death for every 1,000 people. San Marino is #1 with 1,915, followed by #2 Belgium (1,810) and #3 Slovenia (1,658). The US is #10 with 1,309 deaths per million. Of these 28 countries, 21 are in Europe, and 7 are in the Americas. The global average is 279.63 cumulative deaths per million population. At the other end of the spectrum, 86 countries and territories have reported fewer than 100 deaths per million. Additionally, 30 countries and territories have reported fewer than 10 deaths per million, and 9 have reported fewer than 2.
End quote.
Directly tied to population densities? PLUS older cohorts?
by Suliso I don't see a very good correlation with either population density or age. US is hardly densely populated there as Japan is. The best I can see is that the more isolated the country is from any neighbors the better it has been, but even then US is an exception.
by MJ2004 My parents just got vaccinated in Maine this morning, with the second dose scheduled in three weeks. My husband's mom was vaccinated in Massachusetts this morning as well (his dad was vaccinated two weeks ago at the VA). Glad to see progress on the elderly vaccination front. Woe to you if you don't know how to use the internet, though, or don't have someone to help you.
by Suliso
by Suliso There has been a limited progress in Switzerland lately. Covid positive patients in the hospital have fallen below 1,500 for the first time since mid October (peak was a bit shy of 4,000). If there were no new variants we'd feel a lot more comfortable.
by Togtdyalttai My mom got her first vaccine dose today. It took a bit of luck and a tip-off from a friend to get her the appointment, but we did it.
by JazzNU I don't know why I didn't think to mention this before on here, but just in case anyone is feeling uneasy about their getting the vaccine or their family getting it, I do know a good number of people who have gotten vaccines because my orbit includes healthcare workers. Everyone is doing good overall after getting both shots. Most of the people I know got the Pfizer vaccine since that what was issued first and went to the hospitals where they were administering it their employees, but I do know a few that have gotten the Moderna vaccine too.
For the Pfizer shot, everyone felt good after the first shot. Not a single report of any problems outside of soreness in their arm among my friends. But I do know of a friend of a friend who had some chills for a few hours after the first shot. However, several felt sick after getting their second shot. The sickness was minor overall and was mostly arm soreness, fatigue, and chills. A few others just in general felt sick. The chills that some had came without a temperature interestingly enough. No one I know experienced symptoms more than 3 days after the second shot. Most didn't have any symptoms after a day and a half or so. No one regrets getting the vaccine. They are grateful and feel the symptoms were very minor and nothing to complain about, more they were just reporting their experiences to give everyone an idea.
For the Moderna shot, so far so good. I don't know anyone who has gotten 2 Moderna shots just yet. No reports of feeling sick after the first shot. One friend had a decent amount of arm soreness, and another friend got a rash. The rash covered most of her upper arm. It started to clear up the next day and she's fine now. A doctor friend told her it wasn't concerning and she didn't need to seek additional treatment. I think someone who doesn't typically get rashes might be more alarmed than I would be at getting a rash such as this, because I saw it and said no biggie. But my friend was a bit freaked until our doctor friend talked her down. It'll be interesting to see if the second Moderna shot has similar reports of sickness as the second Pfizer shot.
Based on experiences thus far, it might be a good idea to plan ahead and either schedule a light day following getting the second shot or just take the day off if possible. I think this is fairly common from the trial data because the hospitals here planned ahead for this and staggered the schedule for vaccines in the departments so everyone wasn't feeling sick at the same time.
The vast majority of my friends referenced are white women ranging in age from about 35-65. There are a few black women in their 30s and 40s, one Puerto Rican woman in her 50s. And just a few guys, white in their 50s and 60s. YMMV, they test different races and ages during the trial for a reason, but like I said, so far so good across the board.
by ponchi101 Serious question, to everybody that feels like answering.
After you get the vaccine, what is your expected behavior? By that I mean, will you start going out on a regular basis (most likely still wearing a mask) to available locations if they are open? A movie theater, a restaurant, bar, etc?
As a society, we need to start re-activating our economy. Will you take a plane, go on vacation, become a bit more active both for your mental hygiene (man, am I running out of things to cook) and for the above mentioned economic recovery?
by Suliso I'll travel to Latvia to see my parents as soon as regulations allow AND they have gotten a vaccine (myself less important). I'm not much into bars or movie theaters, but would go to a restaurant from time to time. Even more importantly I would return to the office/lab most days.
by atlpam Once both my husband and I have been vaccinated, I will be willing to travel by air again (still masking, etc). I would love to be able to go visit my son since it's been over a year since I last saw him (other than FaceTime). Things like indoor dining will probably depend more on the trend in cases in our area as right now they are extremely high and the positivity rate on tests is still quite high as well.
by mmmm8 Given vaccinated people are still potential carriers of the virus, I don't think my behavior will change much (I've been maybe a bit less careful than some of you - we've flown and have gone to the gym - masked of course) but I'd certainly have less anxiety, especially on the subway and watching people with masks under their nose in stores and at the gym.
I would like to finally spend time indoors with my parents, but my parents aren't likely to get the vaccine for a long time still (both under 65 and my dad is immunocompromised because of a radiotherapy treatment, so they're afraid for him to get it) so that's not happening.
by Suliso Flying doesn't bother me too much to be honest. Have done it already during the pandemic and would do again if there was anywhere meaningful to fly to.
by Togtdyalttai I've been extremely cautious throughout the pandemic: the only times I go out are to work, where I stay in a private office except for restroom trips and warming up my lunch, and to the grocery store once every two weeks. In six weeks once my mom has immunity, I plan to be less cautious: talk to people in person at work, see friends outside of work, go to grocery stores more frequently, get take out from restaurants, and maybe go on a road trip. But I'm not going to fly or eat at a restaurant until I've been vaccinated at the earliest, and possibly not until positivity rates are down to around 1% and case numbers under 5/100,000.
by ti-amie‘It’s a mess’: Biden’s first 10 days dominated by vaccine mysteries
Biden’s team is still trying to locate upwards of 20 million vaccine doses that have been sent to states — a mystery that has hampered plans to speed up the national vaccination effort.
By TYLER PAGER, ADAM CANCRYN and JOANNE KENEN
01/30/2021 07:00 AM EST
Joe Biden promised he’d bring in a competent, tested team to run the pandemic response, set ambitious vaccination targets and impose strict public health guidelines.
His team arrived at the White House with a 200-page response plan ready to roll out. But instead, they have spent much of the last week trying to wrap their hands around the mushrooming crisis — a process officials acknowledge has been humbling, and triggered a concerted effort to temper expectations about how quickly they might get the nation back to normal.
After a week on the job, Biden’s team is still trying to locate upwards of 20 million vaccine doses that have been sent to states — a mystery that has hampered plans to speed up the national vaccination effort. They're searching for new ways to boost production of a vaccine stockpile that they've discovered is mostly empty. And they're nervously eyeing a series of new Covid-19 strains that threaten to derail the response.
“It’s the Mike Tyson quote: ‘Everybody’s got a plan until they get punched in the mouth,’” said one person with knowledge of the vaccine effort who’s not authorized to discuss the work. “They are planning. They are competent. It’s just the weight of everything when you sit down in that chair. It’s heavy.”
Biden officials leading the coronavirus response launched a series of regular briefings this week to keep the public informed on the state of the pandemic and government efforts to contain it and rush vaccines out to as many Americans as possible.
But the briefings were short on details. And behind the scenes, officials say, the team was still struggling to get a handle on basic information, liaise with the career government workers who have been running the response and build out a long-term strategy for bringing — and then keeping — the virus under control.
“One of the virtues of a well-run transition is that by the time you take the reins, you have developed some rapport and trust with the career people you’re working with,” the person familiar with the administration’s work said. The “courtship has been unnaturally short,” the person added.
“Nobody had a complete picture," said Julie Morita, a member of the Biden transition team and executive vice president at the Robert Wood Johnson Foundation. "The plans that were being made were being made with the assumption that more information would be available and be revealed once they got into the White House.”
It's a steep challenge that Biden officials said they'd been anticipating for weeks, amid a rocky transition period that left them scrambling to piece together vaccine distribution plans and coordinate with state health officials.
Yet in the days since taking over, the Covid response team has confronted a situation that officials described as far worse than expected — and that has prompted public assessments so dour they surprised some who had worked on the administration's former transition team.
On Tuesday, Biden warned that the "vaccine program is in worse shape than we anticipated or expected," echoing complaints from his chief of staff, Ron Klain, that a "plan didn't really exist."
Biden's Covid response team has since made a concerted effort not to heap blame on the Trump administration, one official said — even as their vague allusions to a worse-than-expected situation have prompted speculation about what specific problems they've encountered.
But people with knowledge of the response detailed fresh concerns that are centered largely on the federal government's vaccine supply. Biden's team is still trying to get a firm grasp on the whereabouts of more than 20 million doses of Covid-19 vaccine that the federal government bought and distributed to states but has yet to record as being administered to patients.
Only a small percentage of those unaccounted for doses — roughly 2 million, two officials said — is due to lags in data reporting, the Biden team believes. That would mean the rest of the crucial supply is boxed away in warehouses, sitting idle in freezers or floating elsewhere in the complex distribution pipeline that runs from the administration to individual states.
That’s a dilemma that predated the Biden team’s arrival, with Biden himself hammering the vaccine rollout’s first weeks under the Trump administration as a “dismal failure.”
Yet the response team underestimated at the outset how difficult it would be to fix.
The Biden transition had only received high-level briefings on the distribution effort in the runup to the inauguration on Jan. 20, a transition official said, and was largely kept out of detailed discussions about the on-the-ground operation. The team didn't get granular access to Tiberius — the central government system used for tracking vaccine distribution — until the transition's final days.
It was not until after Biden was sworn in that the Covid response team discovered the system was blinded to much of the route that vaccines traveled from the government's distribution hubs to people's arms.
Instead, once the vaccine shipments are delivered to the states, responsibility for tracking them has been left up to states’ individual public health systems. The administration then only gets an update once the doses are actually administered and an official record is submitted.
“I think they were really caught off guard by that,” said one adviser. “It’s a mess.”
Top Biden officials have stressed that the missing doses are spread out across the states, which remain largely responsible for getting them to the health providers charged with vaccinating the tens of millions of people waiting in line for shots.
But the Covid team has since had to spend hours on the phone with various state officials trying to manually track down the unused doses, a time-consuming task that's sapped resources and has yet to give officials a full picture of where exactly supplies are going.
They've also sought to persuade health providers to stop holding doses in reserve, a practice borne out of concerns people wouldn't be able to get the second shot of their two-dose regimen — but one that's no longer necessary and has only contributed to the confusion, according to two people with knowledge of the discussions.
On a call with White House officials Tuesday, Arkansas Republican Gov. Asa Hutchinson vented that some states are bearing the brunt of the blame for the uneven rollout because of those reserves — a nuance not reflected in the federal numbers, according to notes of the call obtained by POLITICO.
The complaint prompted a pledge from Centers for Disease Control and Prevention Director Rochelle Walensky to issue clearer guidance for how states should manage their allocated vaccines.
Illinois Democratic Gov. J.B. Pritzker later blamed a Trump administration program that designated pharmacies to distribute vaccines to long-term care facilities for “bringing our numbers way down” because of how slow it has been to get shots in arms.
The White House has since given states permission to seize unused doses from the pharmacy program and reallocate them elsewhere.
“There is no doubt they are doing a better job,” George Helmy, the chief of staff for New Jersey Democratic Gov. Phil Murphy, said about the Biden administration. “We have a true partner who is being transparent and collaborative.”
As they grapple with the immediate distribution issues, federal officials have also raced to build out detailed plans for eventually distributing the shots to broader populations beyond health care workers and older Americans — a project that people familiar with the effort say the Trump administration never even started on.
And though the Biden team had planned to boost the pace of vaccine manufacturing over time, some Biden officials said they were shocked to learn soon after Inauguration Day that there was little in the federal vaccine reserve — and that the companies producing the shots were nowhere near capable of churning out as many doses as the Trump administration had projected in the preceding months.
The Biden administration has since warned that supplies will remain limited until the summer, raising the possibility of ongoing shortages even as the nation's daily vaccination rate picks up.
The White House cheered promising data on a new single-dose vaccine from Johnson & Johnson on Friday. But production obstacles have dampened expectations for its immediate impact, with one federal official likening the anticipated early flow of shots to "a trickle."
That has turned the Covid team's first days into something closer to a triage operation than the more orderly rollout that the administration had hoped for, especially as much of the federal health department operates on a skeleton staff made up of career officials and a handful of early political appointees.
And though the Biden administration is still pressing ahead with building mass vaccination sites and long-planned preparations for the long-term response effort, officials said the time lost navigating this early set of difficulties has set back a response already likely to consume much of Biden's first year in office.
"This isn't over any time soon," said Craig Fugate, a former Obama administration FEMA administrator who worked on the transition. "There may not be a bright red line where when we cross that line we're done, we're finished and everything's going to be great."
by ti-amie See me, I'd have Jen Psaki come out and say "it's a s**t show people. We're trying to track down just what the he** they did but so far we can't find any records of anything. We're doing the best we can and will keep you informed."
That's why I'm not in politics. Because that is damn sure what the GOP would've done.
by ponchi101 Agree. There is a moment in which being diplomatic and measured means nothing.
I would go further: I would tell the press "make a team of five, and we will let you come in and see what we are dealing with. Yes, smartphones and all".
by JazzNU The long term care facility part is really interesting to hear. Because we have a ton of seniors in the state, plenty in LTC. Our county releases daily numbers and breaks out numbers in nursing facilities and prisons. I try to remember to check every day and I've been surprised to see fairly high LTC numbers and certainly no decrease and I've wondered why that is when they should be moving into the second shot phase at this point. We're not hearing much about healthcare workers getting sick, seems like it should've been the same case in the LTC by now.
by Deuce Perth, Australia - a city of 2 Million people - has gone into lockdown after 1 case - yes - ONE CASE - of COVID-19 was detected in the city.
Hey - if you're going to fight the virus, you might as well do it properly and completely.
Australia is among the most strict countries in terms of management of the virus. No-one can argue with their success so far.
See story below...
by dryrunguy To ponchi's question, I have been changed. I will be among the last to be vaccinated, but once I am, my behavior will not change much. No hugging, no shaking hands, no congregating... I am worried about the variants of today and the variants of the future. And the next pandemic is out there--just waiting for its next host that will give it the opportunity to replicate and mutate.
At some point, I will consider the idea of getting together in person with selective friends. But I will do it ONLY on my terms.
I realize this point of view is extreme. I know that. I want to see the future differently.
But like I said, I have been changed. Some would call it damaged.
There's a vaccine scandal in Philadelphia affecting over a million. It's barely a blip on the national news. The Villages has like 75,000 people living there, not a mystery why it's not getting national attention. Hopefully his grandmother gets a vaccine soon, but he's not thinking like a journalist, he's thinking like a grandson.
by ti-amie That ish in Philly is wild. How do you give a 22 year old with no background in health (or anything else) a contract like that?! He even took vaccine home to give to his girlfriend. The Twitterati are all over it.
At DeSantis Senior First plan, it will probably be 2023 before the regular population will get vaccinated at this pace.
by ponchi101 Message to self: Avoid the Covid topic on Mondays. It is too much...
by ti-amie Sorry ponchi.
New diabetes cases linked to covid-19
Researchers don’t understand exactly how the disease might trigger Type 1 or Type 2 diabetes, or whether the cases are temporary or permanent. But 14 percent of those with severe covid-19 developed a form of the disorder, one analysis found.
By Erin Blakemore
Feb. 1, 2021 at 1:15 p.m. EST
Mihail Zilbermint is used to treating diabetes — he heads a special team that cares for patients with the metabolic disorder at Suburban Hospital in Bethesda, Md. But as the hospital admitted increasing numbers of patients with covid-19, his caseload ballooned.
“Before, we used to manage maybe 18 patients per day,” he said. Now his team cares for as many as 30 daily.
Many of those patients had no prior history of diabetes. Some who developed elevated blood sugar while they had covid-19, the illness caused by the novel coronavirus, returned to normal by the time they left the hospital. Others went home with a diagnosis of full-blown diabetes. “We’ve definitely seen an uptick in patients who are newly diagnosed,” Zilbermint said.
Although covid-19 often attacks the lungs, it is increasingly associated with a range of problems including blood clots, neurological disorders, and kidney and heart damage. Researchers say new-onset diabetes may soon be added to those complications — both Type 1, in which people cannot make the insulin needed to regulate their blood sugar, and Type 2, in which they make too little insulin or become resistant to their insulin, causing their blood sugar levels to rise. But scientists do not know whether covid-19 might hasten already developing problems or actually cause them — or both.
As early as January 2020, doctors in Wuhan, China, noticed elevated blood sugar in patients with covid-19. Physicians in Italy, another early hot spot, wondered whether diabetes diagnoses might follow, given the long-observed association between viral infections and the onset of diabetes. That association was seen in past outbreaks of other coronavirus illnesses such as SARS.
A year after the pandemic began, the precise nature and scope of the covid-diabetes link remain a mystery. Many of those who develop diabetes during or after covid-19 have risk factors, such as obesity or a family history of the disease. Elevated blood glucose levels also are common among those taking dexamethasone, a steroid that is a front-line treatment for covid-19. But cases also have occurred in patients with no known risk factors or prior health concerns. And some cases develop months after the body has cleared the virus.
John Kunkel, a 47-year-old banking executive in Evening Shade, Ark., was one of the surprise cases. He was hospitalized with covid-19 in early July. During a follow-up visit with his doctor, he learned he had dangerously high blood glucose levels and was readmitted. Kunkel has since received a diagnosis of Type 2 diabetes.
“I had no preexisting health issues,” he said. “I was blown away. Why?”
Kunkel has had five emergency room visits and three hospital stays since getting covid-19. He recently lost his job because he was unable to return to work, given his continuing health problems. “Will you get your life back?” he asked. “Nobody knows.”
As many as 14.4 percent of people hospitalized with severe covid-19 developed diabetes, according to a global analysis published Nov. 27 in the journal Diabetes, Obesity and Metabolism. The international group of researchers sifted through reports of uncontrolled hyperglycemia, or high blood sugar, in more than 3,700 covid-19 patients across eight studies. While those diagnoses might be the result of a long-observed response to severe illness, or to treatment with steroids, the authors wrote, a direct effect from covid-19 “should also be considered.”
“I had no preexisting health issues,” he said. “I was blown away. Why?”
Concerns that covid-19 might be directly implicated also were supported, they said, by the exceptionally high doses of insulin that diabetes patients with severe covid-19 often require and the dangerous complications they develop.
Researchers do not understand exactly how covid-19 might trigger Type 1 or Type 2 diabetes, or whether the cases are temporary or permanent. But they are racing to find answers to these and other questions, including whether the novel coronavirus may have spawned an entirely new type of diabetes that might play out differently from the traditional forms of the disease.
Francesco Rubino, a diabetes surgery professor at King’s College London, is convinced there is an underlying connection between the diseases.
Over the summer, he and a group of other diabetes experts launched a global registry of patients with covid-19-related diabetes. After they spread the word with an editorial in the New England Journal of Medicine, more than 350 institutions from across the world responded, he said.
The database is accumulating patients — over 150 so far — although it will take months for researchers to sift through the data to draw any conclusions. “We really need to dig deeper,” Rubino said. “But it sounds like we do have a real problem with covid and diabetes.”
Some of the cases reported to his database do not fit the usual profile of Type 1 diabetes, in which the pancreas produces little or no insulin, or Type 2, in which people become insulin resistant, he said. Usually, a patient with one type of diabetes will experience specific complications; for instance, those with Type 1 may burn through their fat stores, or those with Type 2 may experience a syndrome that can involve severe dehydration and coma as the body pumps excess blood sugar into the urine. In some patients with covid-19, though, complications cross types.
“There’s a good chance that the mechanism of the diabetes isn’t typical,” Rubino said. “There could be a hybrid form. It’s concerning.”
Rubino is especially worried about reports of diabetes diagnoses after mild or asymptomatic coronavirus infections. As the number of novel coronavirus infections continues to rise, he said, “you could see a significant new volume of diabetes diagnoses.”
Diabetes already is increasing at an alarming rate in the United States. An estimated 34.2 million people, or 10.5 percent of the population, have the disorder, according to federal health data. And approximately 1 in 3 Americans, or 88 million people, have prediabetes, which indicates they are on a path to Type 2. If left uncontrolled, the disease can damage many parts of the body and is associated with serious complications including heart disease, stroke, blindness, kidney failure and nerve damage.
But whether those with diabetes that is newly diagnosed after covid-19 will have a lifelong problem is unclear. After the 2003 SARS pandemic, Chinese researchers tracked 39 patients with no history of diabetes who had developed acute diabetes within days of hospitalization with SARS. For all but six, blood sugar level had fallen by the time they were discharged, and only two still had diabetes after two years. The researchers also found evidence that the SARS virus might attack insulin-producing beta cells in the pancreas.
Beta cells play starring roles in both types of diabetes: The bodies of those with Type 1 attack and destroy the cells altogether, halting insulin production. Type 2 diabetics become resistant to the insulin they produce, so the beta cells make more and more, and eventually are worn out.
“If scientists could figure out how or if viral infection can damage beta cells, or what role viruses play in the development of the disease, it would be a real turning point,” said Katie Colbert Coate, a diabetes researcher and research instructor in medicine at Vanderbilt University Medical Center.
Though people with diabetes are no more susceptible to contracting covid-19 than those without, they are at much higher risk of severe complications or death once they do. In the early days of the pandemic, just over a third of those who died of covid-19 in British hospitals had preexisting cases of diabetes. Doctors in Wuhan also noticed that those with newly diagnosed diabetes were more likely to need intensive care than those who had diabetes before they contracted covid-19.
New diagnoses of diabetes in people with no classic risk factors also are scattered throughout case reports: A 37-year-old, previously healthy Chinese man who went to the hospital with a severe, and in some cases fatal, diabetes complication; a 19-year-old German who developed Type 1 diabetes five to seven weeks after a novel coronavirus infection but who lacked the antibodies commonly associated with the autoimmune disease.
Doctors at Children’s Hospital Los Angeles, meanwhile, noticed an increase in the number of Type 2 diagnoses in children, as well as a severe complication of diabetes. After some of them showed evidence of past coronavirus infections, Senta Georgia, an investigator in the hospital’s Saban Research Institute, began looking deeper. Her research, which repurposes tissue from primates used in vaccine tests, is undergoing peer review.
“Only with the scientific public square can we put all of this data out there, evaluate its strengths and weaknesses … until we really get the information we need,” Georgia said.
Such reports also have increased the sense of urgency for researchers like Coate, who dropped other work and began looking for keys to understanding the mechanism of the disease by examining how covid-19 might damage beta cells or other structures in the pancreas. She and others are asking whether certain covid symptoms predict whether a patient is vulnerable to diabetes and, most important, whether the disease’s onset is an effect of the immune response or a result of the virus directly attacking insulin-producing cells.
ACE2 receptor cells, the novel coronavirus’s entryway into the body, could provide one answer. When the spike proteins that surround the virus latch onto a host cell with an ACE2 receptor, they open up a cellular doorway that allows the virus to hijack the cell.
Strong evidence of ACE2 receptors on beta cells could confirm the long-standing suspicion that viruses trigger diabetes. But the research findings are inconclusive: Since the pancreas breaks down quickly after death, obtaining good samples from autopsied humans is difficult. And each study has its own limitations.
Last year, Cornell University researchers grew human pancreas cells and managed to infect them with SARS-CoV-2, as the novel coronavirus is technically known. They found ACE2 receptors on the cells, but the cells had been cultivated in a laboratory, not a human body.
Coate and her colleagues at Vanderbilt University were able to confirm the presence of ACE2 receptors in the physical structures of the pancreas, but their study focused on patients without covid-19 and found no evidence of the receptors on the insulin-producing beta cells. An Italian study did find the receptors in beta cells, but the donors did not have covid-19, either. Until receptors in pancreatic beta cells in tissue from covid-19 patients can be consistently confirmed by other researchers, the hunt for the mechanism underlying the diabetes-covid-19 connection continues. So does research on ways covid-19 might harm other parts of the endocrine system, which also might play a role in the disease mechanism.
For newly diagnosed patients such as nurse practitioner Tanisha Flowers, the answers can’t come soon enough.
Infected in April while working in a covid-19 ward in a Richmond hospital, the 40-year-old was diagnosed with diabetes in October. She now takes daily medications, watches her diet and is all too aware that she may be diabetic for life.
“I’m not myself anymore,” Flowers said. “No one knows what the lasting outcomes are.”
ti-amie wrote: ↑Mon Feb 01, 2021 9:48 pm New diabetes cases linked to covid-19
Researchers don’t understand exactly how the disease might trigger Type 1 or Type 2 diabetes, or whether the cases are temporary or permanent. But 14 percent of those with severe covid-19 developed a form of the disorder, one analysis found.
That is disturbingly high. It'd be interesting to see if that number remained steady with in-depth research.
Not sure why this doesn't mention it, but covid was thought of as a respiratory disease early on because of all the lung issues, but many are increasingly classifying it as a vascular disease. In that context, the sudden onset of diabetes makes a good deal more sense.
by MJ2004
JazzNU wrote:
ti-amie wrote: ↑Mon Feb 01, 2021 9:48 pm New diabetes cases linked to covid-19
Researchers don’t understand exactly how the disease might trigger Type 1 or Type 2 diabetes, or whether the cases are temporary or permanent. But 14 percent of those with severe covid-19 developed a form of the disorder, one analysis found.
That is disturbingly high. It'd be interesting to see if that number remained steady with in-depth research.
Not sure why this doesn't mention it, but covid was thought of as a respiratory disease early on because of all the lung issues, but many are increasingly classifying it as a vascular disease. In that context, the sudden onset of diabetes makes a good deal more sense.
Agree - 14% is disturbingly high.
I think that trying to think of it as a respiratory or a vascular disease is a mistake. It reminds me of autoimmune diseases where multiple parts of the body are attacked at once. It is causing severe inflammation and damage in many body organs simultaneously.
by ponchi101 Remember we are only one year into this. It took years to finally truly figure out what AIDS really was.
By the time this is over (if it is ever over) this thing will have mutated into some form of virus that we have not seen before.
And remember when I stupidly joked about Covid20 and Covid21? Well, P, you and your big mouth.
by mmmm8
MJ2004 wrote: ↑Mon Feb 01, 2021 10:53 pm
Agree - 14% is disturbingly high.
I think that trying to think of it as a respiratory or a vascular disease is a mistake. It reminds me of autoimmune diseases where multiple parts of the body are attacked at once. It is causing severe inflammation and damage in many body organs simultaneously.
This really seems to be the case.
by dryrunguy Here's the latest Situation Report. I was especially struck by the demographics of those already vaccinated in the U.S.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 102.94 million cases and 2.23 million deaths as of 11am EST on February 2. The weekly global incidence decreased for the third consecutive week, down to 3.63 million new cases. This is a decrease of nearly 15% compared to the previous week, and it is the lowest weekly total since late October. Weekly global mortality also decreased nearly 4% compared to the previous week, down to 93,803 deaths. Considering the reporting interruptions over the winter holidays, it is unclear exactly when the actual global incidence peaked; however, the decrease in mortality could be an early indication of a longer-term trend corresponding to decreases in incidence starting 2-4 weeks ago.
Our World in Data reports that 101.31 million vaccine doses have been administered globally, a 48% increase since this time last week.
UNITED STATES
The US CDC reported 26.03 million total cases and 439,955 deaths. The US is currently averaging 3,145 deaths per day, and it could surpass 450,000 cumulative deaths in the next 3-4 days.
National-level daily incidence continues to decrease, down from nearly 250,000 new cases in per day in mid-January to around 150,000. While the daily incidence continues to decrease, the current average is still more than double the peak of the summer surge. Daily mortality is also beginning to show signs of declining. The US has reported decreasing daily mortality for 5 consecutive days, down 5% since January 26. Additional data are needed to determine if this is an early indication of a longer-term trend, but a decrease spanning multiple days is an encouraging sign.
US Vaccination
The US CDC reported 49.94 million vaccine doses distributed and 32.22 million doses administered. The US has administered 64.5% of the distributed doses, which is an increase of more than 10 percentage points from Friday’s update (54.1%). In total, 26.02 million people (approximately 7.9% of the US population) have received at least 1 dose of the vaccine, and 5.93 million (1.8%) have received both doses. The US is now averaging 1.36 million doses administered per day, a 20% increase from the previous week. The breakdown of doses by manufacturer remains relatively even, with slightly more Pfizer/BioNTech doses administered (17.36 million; 54%) than Moderna (14.76 million; 46%).
The CDC moved data for vaccination at long-term care facilities (LTCF) to its own dashboard. A total of 3.75 million doses have been administered through the Federal Pharmacy Partnership for Long-term Care Program*, covering 3.14 million individuals with at least 1 dose and 594,857 with 2 doses. The dashboard breaks down the doses by those administered to LTCF residents and those administered to staff. Based on the available data, approximately 60% of the doses have gone to residents and 40% to staff.
*The dashboard only includes data for doses administered through the federal program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 26.35 million US cases and 444,336 deaths as of 1:30pm EST on February 2.
RUSSIAN VACCINE Sputnik V, Russia’s primary vaccine candidate, appears to be safe and effective in preventing symptomatic COVID-19, based on preliminary analysis of Phase 3 clinical trial data published in The Lancet. The clinical trials included nearly 20,000 participants, with 75% randomly assigned to receive the vaccine. The researchers identified 16 cases of COVID-19 among the treatment group (14,964 participants) and 62 cases among the placebo group (4,902), corresponding to an overall efficacy of 91.6% in terms of preventing COVID-19 disease, similar to the results for the Pfizer-BioNTech and Moderna vaccines. Notably, the vaccine also exhibited 91.8% efficacy among adults over the age of 60, and no moderate or severe cases of COVID-19 were reported among the vaccinated participants. No serious adverse events were determined to be associated with the vaccine.
The Sputnik V vaccine is administered in 2 doses, administered 21 days apart. It requires the temperature to be maintained at approximately 0°F (-18°C), with short-term storage at 36-46°F (2-8°C). In contrast, ultra-cold storage (approximately -80°F or -62°C) is required for the Pfizer-BioNTech vaccine.
The Russian government came under criticism in August 2020 after making the Sputnik V vaccine candidate available to the public before Phase 3 clinical trials were completed. More than a dozen other countries have already authorized the use of the Sputnik V vaccine.
US VACCINATION The US CDC COVID-19 Response Team published data from the early stages of SARS-CoV-2 vaccination efforts in the US. The first study, published in the CDC’s MMWR, described demographic characteristics among those vaccinated in the first month—December 14, 2020 to January 14, 2021. The researchers analyzed age, sex, and race/ethnicity data for nearly 13 million individuals who received at least 1 dose of the vaccine. The majority of those vaccinated were older adults, with 55% aged 50 years and older, including 13.4% aged 65-74 years and 15.6% aged 75 years and older. Additionally, 63% of those vaccinated were female.
Among 6.7 million individuals with race/ethnicity data, the majority (60.4%) were White*, compared to 11.5% Hispanic/Latinx, 5.4% Black*, 6.0% Asian*, and 2.3% American Indian, Alaskan Native, Native Hawaiian, or Other Pacific Islander* and 14.4% were listed as Multiple races/ethnicities or Other. The researchers indicate that the demographic distributions appear to largely reflect those of the earliest priority populations outlined by the CDC’s Advisory Committee on Immunization Practices, including LTCF residents and healthcare workers. Notably, however, the proportion of Black vaccinees was lower than would be expected considering the racial/ethnic distribution these priority groups.
*Non-Hispanic.
The second article, also published in the CDC’s MMWR, discussed vaccination coverage among LTCF residents and staff. The researchers evaluated data on nearly 1.3 million individuals vaccinated through the CDC Pharmacy Partnership for Long-Term Care Program from December 18, 2020 to January 17, 2021. Among these individuals, 713,909 were residents and 582,104 were facility staff. In total 12,702 facilities participated in the program, of which 11,460 (90.2%) conducted at least one on-site vaccination clinic. This effort provided at least 1 dose of the vaccine to an estimated 77.8% of residents at these facilities, but only 37.5% of staff. Due to a combination of factors—including age, underlying health conditions, and prolonged close contact in congregate settings—LTCF residents are at elevated risk for infection, severe disease, and death, so it is important to achieve high vaccination coverage at these facilities.
In addition to state and local governments, tribal nations are also scaling up vaccination efforts. The Navajo Nation, one of the most severely affected tribal nations during the US epidemic (29,860 cases), eased its weekend curfew in an effort to expand vaccination. The principal challenges are addressing vaccine hesitancy, particularly among older adults who are at elevated risk, and reaching individuals who live in rural areas that are unable or unwilling to travel to get vaccinated, especially during adverse winter weather conditions. Proactive effort by tribal leadership and health workers has driven substantial progress in terms of vaccination coverage. To date, Navajo Nation has administered at least 1 dose of SARS-CoV-2 vaccine to more than 20% of its population, higher coverage than any US state or territory.
VACCINATION PROTESTS Dodger Stadium in Los Angeles, California, is currently serving as one of the largest mass vaccination sites in the US, but protests by anti-vaccination groups caused the site to be temporarily shut down on Saturday when protesters blocked the entrance to the stadium. Fortunately, the disruption did not result in the cancellation of any appointments, but Governor Gavin Newsom emphasized that protests will not be deterred by protests. Protesters reportedly attempted to intimidate individuals waiting in line and spread misinformation about COVID-19 and the vaccine. New safety measures at Dodger Stadium will clearly delineate where protesters are permitted to be in order to prevent further disruptions to vaccination operations.
GERMANY On January 29, the European Commission issued a conditional marketing authorization (CMA) for the use of the AstraZeneca-Oxford University SARS-CoV-2 vaccine in adults aged 18 and older. While the announcement acknowledged that the clinical trials primarily included adults aged 18-55 years, the CMA did not include an upper age limit. In a decision stemming from a concern about insufficient efficacy data in older adults, Germany authorized the AstraZeneca-Oxford vaccine only for adults aged 18-64. Currently, vaccine eligibility in Germany is limited to residents and staff of long-term care facilities, adults aged 80 years and older, and frontline healthcare workers. Because the AstraZeneca-Oxford vaccine is not authorized for many high-risk individuals due to Germany’s age restrictions, Germany will reportedly review its eligible populations and prioritize use of that particular vaccine in younger healthcare workers and LTCF staff.
Germany has struggled with a slow start to its vaccination campaign, and Chancellor Angela Merkel reportedly met with state governors, EU leadership, and representatives from the pharmaceutical industry yesterday to identify mechanisms to speed progress toward national vaccination coverage. Following the meeting, Chancellor Merkel indicated that Germany still anticipates being able to vaccinate its entire population by September 2021, even if no additional vaccines are authorized for use.
Like many countries around the world, Germany recently instituted travel restrictions in response to emerging, highly transmissible SARS-CoV-2 variants. Notably, non-German citizens arriving from “areas of variant of concern”—currently Brazil, Eswatini, Ireland, Lesotho, Portugal, South Africa, and the UK—will not be permitted to enter the country, even with a recent negative SARS-CoV-2 test. Individuals who are eligible to enter—including German citizens and residents—and recent travel to “high incidence areas” or “virus variant areas” must provide proof of a negative test prior to entry, and all individuals with recent travel to “risk areas”—which covers most countries, including most in Europe—must be tested within 48 hours after arrival. All travelers arriving from places identified as at risk, high-incidence, or variant areas are required to self-quarantine for 10 days after they arrive. The quarantine can potentially be terminated after 5 days, with a negative test. The new restrictions are expected to remain in place through at least February 17.
DRC DRONE VACCINE DISTRIBUTION Drones have previously been used for the delivery of medical supplies, including vaccines, to areas that are remote or difficult to access. The Democratic Republic of the Congo (DRC) recently announced a partnership between VillageReach, Swoop Aero, and the DRC Ministry of Health—“Drones for Health”—will use drone to promote equitable access to healthcare for half a million people in remote communities of the Equateur province. In addition to standard medical supplies, the new program is expected to support SARS-CoV-2 vaccination efforts in the country. These drones will be used to deliver medicine and other supplies to 75 health facilities in the province.
REFUGEES & DISPLACED POPULATIONS Refugees are among the most vulnerable populations in the world, particularly in the midst of a pandemic. Being displaced from their homes and separated from community support systems, refugees and other displaced populations often live in congregate settings without access to clean water or proper sanitary equipment, which exacerbates risk of transmission and severe disease. Furthermore, displaced populations face significant barriers in terms of accessing healthcare, and medical organizations that work with these populations are often underfunded and overwhelmed. King Abdullah II Ibn Al Hussein of Jordan recently announced that the Jordanian government initiated vaccination operations for refugee population in the country. King Abdullah viewed it as part of Jordan’s “global responsibility” and “moral duty” to protect the most vulnerable from COVID-19. The UN Refugee Agency (UNHCR) applauded Jordan’s initiative to include displaced populations in its vaccination program and encouraged other countries to follow Jordan’s example.
In recognition of the disproportionate COVID-19 burden among immigrant populations, many of whom are racial and ethnic minorities, the US Department of Homeland Security (DHS) is committing resources to ensure equal access to SARS-CoV-2 vaccines for undocumented immigrants. A statement issued by DHS emphasized the “public health imperative” in ensuring access to vaccination, regardless of immigration status. While many undocumented immigrants are not refugees, they may face similar stigma and barriers to accessing public health and healthcare. As part of this effort, the Federal Emergency Management Agency will coordinate vaccination clinics that aim to reach “underserved and rural communities,” and federal immigration officials, including Immigration and Customs Enforcement and Customs and Border Protection, “will not conduct enforcement operations at or near vaccine distribution sites or clinics” in order to encourage participation by vulnerable individuals and communities.
PREGNANT WOMEN On January 26, the WHO updated its guidance on the Moderna SARS-CoV-2 vaccine to include pregnant women. Previously, the WHO recommended against vaccinating pregnant women unless they were at elevated risk, which conflicted with recommendations published by the US CDC. While the current iterations of both sets of guidelines do not explicitly recommend vaccinating pregnant women, both note that there is currently no evidence to suggest that the vaccine poses safety concerns for pregnant women.
A study published in JAMA: Pediatrics provides evidence that pregnant women may be able to pass IgG antibodies against SARS-CoV-2 to their fetus. The study involved 1,417 women who recently gave birth. Among 83 mothers with detectable SARS-CoV-2 antibodies, 72 (86.7%) transferred IgG antibodies to their fetus—as detected in the newborns’ cord blood. IgM antibodies were not detected in any cord blood specimens, and antibodies were not detected in any infants born to mothers without detectable antibodies. The concentration of antibodies in the cord blood was significantly correlated with the concentration in the mother, but the antibodies were successfully transferred by mothers who exhibited symptomatic disease and asymptomatic infection. The study did not explicitly evaluate the ability to transfer antibodies developed as a result of vaccination; however, the researchers indicate that the results align with similar studies on transplacental transfer of vaccine-conferred antibodies for other diseases. Further research is necessary to determine the recommended timing for vaccination of pregnant women in order to achieve sufficient transplacental transfer of SARS-CoV-2 antibodies to the fetus.
US ECONOMIC STIMULUS With the Democratic party now in control of the US House of Representatives, Senate, and White House, pressure is increasing to negotiate additional federal economic relief for the COVID-19 epidemic. US President Joe Biden announced his proposal for a new COVID-19 economic stimulus and recovery package, the American Rescue Plan, which includes US$1.9 trillion in funding. The package includes support for SARS-CoV-2 testing and vaccination efforts ($415 million) and small businesses ($440 million). It also includes $1 trillion in direct support for individuals and families, including another round of stimulus checks and increased and extended unemployment benefits. Additionally, the package includes broader provisions to increase the federal minimum wage and expand access to affordable childcare and healthcare.
While the Democratic party holds a majority in the Senate (with the tie-breaking vote from Vice President Kamala Harris), there are limited options available to pass a funding bill without some degree of Republican support. In hopes of stimulating bipartisan negotiations, 10 Republican Senators visited the White House to outline an alternate funding package, which totals $618 billion. The Republican proposal would include smaller and more targeted direct stimulus checks for individuals; maintain the current $300 federal supplemental unemployment benefits through June, as opposed to $400 through September in the White House plan; and reduce support for schools from $170 billion in the White House plan to $20 billion. The Republican plan would also eliminate funding to expand the national public health workforce; $350 billion in support to state, local, and tribal governments; subsidies for health insurance premiums; and the minimum wage increase. The initial meeting was reportedly productive, and there appears to be interest on both sides to continue negotiations.
As we have covered previously, the large-scale response efforts in many jurisdictions—including testing, surveillance, and vaccination—have posed major financial challenges to jurisdictions across the country. An investigation by STAT News found that senior US government officials under the Trump Administration “actively lobbied Congress to deny state governments any extra funding for the Covid-19 vaccine rollout.” STAT News reports that the primary point of contention reportedly dealt with the speed with which states were using previous federal funding allocations for COVID-19 response.
EMERGING VARIANTS As scientists continue to monitor emerging SARS-CoV-2 variants of concern (VOCs), researchers are identifying new mutations. Of particular concern is the E484K mutation, which consists of an amino acid change in the spike receptor binding domain of the SARS-CoV-2 virus. This change appears to result in increased binding strength of the spike protein to the ACE2 receptor, which is how the virus enters human cells. Notably, the E484K mutation appears to result in increased transmissibility and resistance to monoclonal antibody treatments. This mutation has been identified in several variants of SARS-CoV-2 in different geographic areas, including Brazil and the UK, and it appears to be increasing in prevalence, which suggests increased fitness compared to other mutations. The fact that this mutation has been independently acquired in multiple locations and variants indicates that the E484K changes in the spike gene are broadly advantageous to SARS-CoV-2 and may continue to arise in subsequent variants.
Aside from the E484K mutation, scientists monitoring the B.1.1.7 VOC also must track its prevalence and incidence among the population. Since whole genome sequencing to detect the Δ69-70 mutation is costly and time consuming, the UK’s NERVTAG expert group used existing laboratory PCR-based testing to track the variant. Specifically, the Δ69-70 mutation in the spike gene causes S gene target failure (SGTF) in the ThermoFisher TaqPath assay, resulting in a false negative PCR test from a known positive sample. By looking for SGTF in known positive samples (confirmed by other PCR assays), researchers can monitor the extent of the Δ69-70 mutation in the B.1.1.7 VOC without the need for time- and resource-intensive whole genome sequencing methods.
VACCINE DEVELOPMENT & TESTING Clover Biopharmaceuticals, a Chinese company developing a SARS-CoV-2 vaccine candidate, announced that it is moving forward with Phase 2/3 clinical trials for its candidate SARS-CoV-2 vaccine using an adjuvant manufactured by Dynavax, rather than one produced by GlaxoSmithKline (GSK). According to a press release from Clover, the two adjuvants induced similar immune response in Phase 1 clinical trials, but Clover selected the Dynavax adjuvant for its forthcoming Phase 2/3 clinical trials due to concerns about production capacity for the GSK product. Clover anticipates vaccine production capacity of “hundreds of millions of doses in 2021” and ultimately as high as 1 billion doses per year. Clover expects to have preliminary data available from the Phase 2/3 trials by the middle of 2021.
by shtexas I have seen a lot of Facebook comments claiming the vaccines are not FDA approved, may give you AIDS, and will change your DNA.
by ponchi101 Facebook has to be banned. It is getting to that point. If somebody were to quantify how much harm it does, it would be clear.
---0---
I am still not taking the Sputnik.
Here: vaccination to begin on Feb 20th. A five delay over the initial plan of Feb 15th.
I will get vaccinated by Jan 2022. You'll see.
by Suliso
ponchi101 wrote: ↑Tue Feb 02, 2021 9:12 pm
I will get vaccinated by Jan 2022. You'll see.
Optimist
by ti-amie
His Twitter bio:
Zach Buchanan @ZHBuchanan
Diamondbacks reporter for @TheAthleticAZ and prospect features for @TheAthleticMLB
. I watch a distressing amount of television.
by Suliso Just learned that in Latvia available vaccine will be distributed first to the usual priority groups and then the reminder via a monthly lottery (first dose, second appointment is automatic). Haven't heard such an approach anywhere else.
by Deuce
Suliso wrote: ↑Thu Feb 04, 2021 11:31 pm
Just learned that in Latvia available vaccine will be distributed first to the usual priority groups and then the reminder via a monthly lottery (first dose, second appointment is automatic). Haven't heard such an approach anywhere else.
How many tickets is each person permitted to have?
by ti-amie
by ponchi101 Solution:
Start vaccination. Vaccinate the people that want to get the vaccine. By September, when you will have sufficient people already vaccinated, pass a bill that allows insurance companies NOT TO PAY FOR YOUR TREATMENT if you refused the vaccine.
Other than that, they can so drop dead as far as I am concerned.
(Excluding seniors with cognitive impairment, who most likely will be vaccinated or not depending on their children's decisions)
by ti-amie
by dryrunguy The latest Situation Report. I only skimmed it, but saw something about a strike by health care workers in Myanmar.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 104.37 million cases and 2.27 million deaths as of 11am EST on February 5.
Our World in Data reports that 119.48 million vaccine doses have been administered globally, a 65% increase since this time last week.
According to data compiled by Our World in Data, at least 65 countries have initiated SARS-CoV-2 vaccination campaigns. The majority of these countries are in Europe and North America, although vaccination efforts are starting in Africa, South America, South and Southeast Asia, and the Eastern Mediterranean region. In terms of total doses administered, the US is #1 globally (35.2 million), followed by China (31.2 million), the UK (11.0 million), Israel (5.3 million), and India (5.0 million). In total, 15 countries have administered 1 million or more vaccine doses, and 42 have administered more than 100,000.
Because some individuals have only received the first dose while others have received both, it is difficult to determine the proportion of a country’s population with full coverage. The doses administered per capita, however, can provide insight into the progress toward full coverage. Full coverage with 2 doses would correspond to 200 doses per 100 population, so with that in mind, we can estimate the proportion of those doses that each country has administered so far. On a per capita basis, Israel is #1 globally with 61.7 doses administered per 100 population, which corresponds to approximately 30.8% of its way toward full coverage. The United Arab Emirates (UAE) is #2 with 34.8 doses per 100 population (19.5%), followed by Seychelles (37.7; 18.9%), the UK (16.2; 8.1%), and the US (10.6; 5.3%).
Broken down by continent, Asian countries have reported the most cumulative doses administered, with 49.77 million. Asia is followed by North America (36.98 million), Europe (28.44 million), South America (3.82 million), and Africa (390,160). In Asia (including the Eastern Mediterranean region), China represents the majority (64.2%) of the doses administered, which is not surprising, considering that it initiated vaccination months before most other countries. China is followed by Israel (10.7%), India (10.0%), the United Arab Emirates (7.7%), and Turkey (5.0%). The North American total is driven principally by the US, which is reporting more than 95% of the administered doses. Canada, Costa Rica, Mexico, and Panama have also started vaccinations. Similarly, Brazil is driving the South American total, with more than 80% of the administered doses. Brazil is followed by Argentina (11.6%) and Chile (7.6%). In Europe, the doses the UK accounts for slightly less than 40% of the total, followed by Germany (10.5%), Italy (8.2%), Spain (6.7%), and France (6.6%). Data are only available for 4 African countries—Algeria, Egypt, Morocco, and Seychelles. Morocco has reported approximately 90% of the doses administered, followed by Seychelles with 10%.
UNITED STATES
The US CDC reported 26.40 million total cases and 449,020 deaths. The daily incidence continues to fall, down to 134,523 new cases per day—a 46% decrease from the peak on January 8 (248,706). The daily mortality continues to decrease as well. The US is currently averaging 3,056 deaths per day, a decrease of 8% since January 26 (3,316). The US will almost certainly surpass 450,000 cumulative deaths in this afternoon’s update:
1 death to 50k- 55 days
50k to 100k- 33 days
100k to 150k- 63 days
150k to 200k- 55 days
200k to 250k- 58 days
250k to 300k- 25 days
300k to 350k- 20 days
350k to 400k- 16 days
400k to 450k- 16 days
US Vaccination Effort
The US CDC reported 57.49 million vaccine doses distributed and 35.20 million doses administered. The US has administered 61.2% of the distributed doses, which is a slight decrease from Tuesday (64.5%). In total, 27.91 million people (approximately 8.5% of the US population) have received at least 1 dose of the vaccine, and 6.93 million (2.1%) have received both doses. The average daily doses administered fell sharply over the past several days, down from a high of 1.4 million doses per day on January 30 to 892,946 on February 3, a decrease of 36%. The breakdown of doses by manufacturer remains relatively even, with slightly more Pfizer-BioNTech doses administered (18.84 million; 54%) than Moderna (16.26 million; 46%).
A total of 4.21 million doses have been administered at long-term care facilities (LTCFs) through the Federal Pharmacy Partnership for Long-term Care (LTC) Program*, including residents and staff. This covers 3.40 million individuals with at least 1 dose and 796,324 with 2 doses. Approximately 60% of the doses have gone to residents and 40% to staff.
*The dashboard only includes data for doses administered through the federal program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 26.72 million US cases and 456,900 deaths as of 1:30pm EST on February 5.
PANDEMIC FORECASTING In the White House’s National Strategy for the COVID-19 Response and Pandemic Preparedness, published in January, US President Joe Biden included the need for a National Center for Epidemic Forecasting and Outbreak Analytics “to modernize global early warning and trigger systems to prevent, detect, and respond to biological threats.” Under current systems, there are limited federal resources for epidemiological modeling, and independent disease modelers, including from academic institutions and private sector think tanks across the country, are often called upon to support the government’s preparedness and response efforts, typically as volunteers. Dr. Caitlin Rivers, from the Johns Hopkins Center for Health Security, and Dr. Dylan George, Vice President of In-Q-Tel, have advocated for this capacity for years, and the US government has finally heeded their call for action. President Biden directed federal agencies to develop plans to establish the center in an executive order issued on his second day in office.
The National Center for Epidemic Forecasting and Outbreak Analytics would provide a service similar to weather forecasting, except for endemic and epidemic diseases. COVID-19 will certainly not be the last major disease threat we face, and epidemiological and statistical analysis will be critical to rapidly identifying the emergence of outbreaks and epidemics and providing elected and health officials with the information needed to identify, implement, and adapt appropriate response activities. Funding under the proposed American Rescue Plan would support expanded testing and analytic capabilities during the COVID-19 response, including for genomic sequencing to address the threat of emerging variants, but longer-term investment is needed to embed the type of analytic capacity in the federal government, where it can inform national policy and response to epidemic events.
VACCINATION DOSE SCHEDULE & TRANSMISSION RISK
A study (preprint for The Lancet) of data from the Phase 3 clinical trials of the AstraZeneca-Oxford University vaccine evaluated vaccine efficacy after a single dose and for alternate timing for the booster dose. Notably, the UK adapted the timing for the booster dose from 4 weeks after the first dose—which is how the vaccine was designed to be administered and the timing used for clinical trials—to 12 weeks in an effort to provide the first dose to as many people as possible. This study assessed the vaccine’s efficacy in participants who received the 2 doses between 4 and 12 weeks apart.
The researchers found that the efficacy after the first dose did not wane in the first 12 weeks. A single dose of the vaccine was 76% efficacious in preventing symptomatic COVID-19 disease in the first 90 days after vaccination, although it was associated with a substantial decrease in efficacy with respect to preventing asymptomatic infection. Notably, however, the additional asymptomatic infections could potentially be among participants who would have otherwise developed COVID-19 symptoms. Additionally, the efficacy in preventing symptomatic disease was higher in participants who received the booster dose later than in those who received it earlier. Vaccine efficacy was 82.4% among participants who received their booster dose 12 weeks or longer after the first dose, compared to 54.9% in those who received their 2 doses less than 6 weeks apart. These results provide support for vaccination plans that delay the booster dose beyond the intended 4 weeks, considering that the immunity conferred after the first dose appears to be relatively stable over the first several months and the overall protection appears to increase with an increased time between the prime and booster doses.
The researchers also found that vaccination was associated with an overall reduced risk of infection—54.9% efficacy for 2 doses and 67% efficacy for 1 dose—which provides evidence that the vaccine could also provide protection against SARS-CoV-2 transmission. The role of SARS-CoV-2 vaccines in mitigating transmission risk remains uncertain, but these findings provide a promising indication that vaccination could reduce community spread of the virus, which would be a major tool to bring the pandemic under control.
J&J EUA SUBMISSION Yesterday, Johnson & Johnson (J&J) submitted an application to the US FDA for an Emergency Use Authorization (EUA) for its SARS-CoV-2 vaccine, developed in collaboration with Janssen Biotech. The US FDA announced that it will review the submission over the coming weeks, and it will convene a meeting of its Vaccines and Related Biological Products Advisory Committee (VRBPAC) on February 26 to discuss the vaccine’s safety and efficacy data. The FDA did not commit to a timeline for ruling on the EUA submission; however, it will “review the request as expeditiously as possible” following the VRBPAC meeting. As with the previous vaccines, the FDA intends to publish relevant data in the days prior to the VRBPAC meeting. J&J announced interim results from the Phase 3 clinical trials in a press release issued on January 29, but the full dataset or final analyses have not yet been released publicly or subjected to peer review. In addition to the US FDA, J&J intends to submit an application for a Conditional Marketing Authorisation (CMA) to the European Medicines Agency “in the coming weeks.”
J&J’s most recent press release indicates that it expects to be able to begin shipping vaccine doses “immediately following authorization.” The company expects to provide 100 million doses by mid-2021, but it did not indicate how much is currently available. Multiple news media reports indicate that the initial supply is expected to be relatively low. The J&J-Janssen vaccine utilizes a single dose, which provides an advantage over existing vaccines in terms of the potential to speed vaccination operations. And while the J&J-Janssen vaccine does require moderately low freezing temperatures (-4°F; -20°C) for long-term storage, it can be stored for up to 3 months at normal refrigeration temperatures (6°F–46°F; 2°-8°C), which could facilitate distribution and on-site storage at vaccination clinics.
COVAX VACCINE ALLOCATION On February 3, Gavi published interim SARS-CoV-2 vaccine allocation for the COVAX facility. The interim plan includes estimated quantities and timeline for vaccine distribution of the Pfizer-BioNTech and AstraZeneca-Oxford University vaccines to low- and middle-income countries eligible to receive doses through the COVAX effort. As we have covered previously, COVAX is a multilateral program to pool funding in an effort to help lower-income countries compete against wealthier countries in terms of purchasing doses of SARS-CoV-2 vaccines. In total, the interim plan estimates that 336 million doses of the AstraZeneca-Oxford vaccine and 1.2 million doses of the Pfizer-BioNTech vaccine will be distributed in the first half of 2021.
Due to the ultra-cold temperatures required for the Pfizer-BioNTech vaccine, those doses were only allocated to countries that requested early delivery of that vaccine and were determined to be capable of maintaining the cold chain. The available inventory was distributed relatively evenly across the eligible countries, with the aim of achieving full coverage for at least 3% of the population for each country in order to provide protection for the most vulnerable individuals (eg, healthcare workers). On average, the national allocations cover 3.3% of the countries' respective populations.
Of the 190 eligible countries, 145 are included in the earliest round of vaccine allocations, and delivery is expected to begin as early as late February and progress through the first half of 2021. The estimates aim to provide countries with an approximate quantity of doses in order to enable them to implement more concrete plans for national vaccine distribution and administration logistics and operations. The interim guidance notes that the AstraZeneca-Oxford vaccine has not yet received an Emergency Use Listing (EUL) from the WHO, but that evaluation process is in progress.
SARS-CoV-2 TRANSMISSION The scientific community is still uncovering the full picture of SARS-CoV-2 transmission dynamics. A study published in The Lancet: Infectious Diseases analyzed SARS-CoV-2 transmission among clusters in Catalonia, Spain, to understand the relationship between viral load and transmission risk. The researchers utilized participant data from a previous clinical trial, and they identified 314 COVID-19 patients that met their inclusion criteria. Among those patients, 282 had at least 1 contact (753 total contacts). The index patients infected 125 secondary cases, corresponding to a secondary attack rate of 17%. The researchers identified a statistically significant association between viral load in the index patients and the subsequent secondary attack rate. Among index patients with the lowest viral load, index patients exhibited a secondary attack rate of 12%, compared to 24% among the highest group. The researchers estimate that the odds of secondary transmission increase 30% for every log(10) increase in viral load. Additionally, the study found increased likelihood that secondary cases would develop COVID-19 symptoms associated with increased viral load in the index patients (aHR of 1.12 per log(10) increase in viral load). While further research is needed to more fully characterize the factors associated with transmission, this study provides evidence that the index patient’s viral load could be a major driver of secondary transmission risk and potentially disease severity in secondary cases.
An editorial published in Nature discusses the need to shift focus away from surface decontamination as a mechanism to reduce SARS-CoV-2 transmission risk. Multiple studies have found that transmission of SARS-CoV-2 via contaminated surfaces, or fomites, is relatively rare compared to respiratory transmission via droplets or aerosols. Despite the evidence supporting respiratory exposure as the overwhelming driver of community transmission, numerous public health entities, including the WHO and US CDC, continue to emphasize the importance of surface decontamination, which can cause confusion among the public regarding transmission risk and appropriate protective measures. Notably, surface decontamination efforts, while highly visible and easy to recognize, are costly and likely not effective means of reducing transmission risk. The editorial calls for increased focus on improving ventilation and air filtration capacity to reduce respiratory exposure. Additionally, proper physical distancing and face mask use remain key tools in mitigating exposure and transmission risk for individuals.
GSK-CUREVAC VACCINE CANDIDATE GlaxoSmithKline (GSK) announced a partnership with German biotech company CureVac to develop a new, multivalent SARS-CoV-2 vaccine and manufacture CureVac’s first generation vaccine candidate. The joint vaccine development effort aims to target emerging SARS-CoV-2 variants, with the goal of making a product available in 2022. Under the new agreement, GSK will also manufacture up to 100 million doses of CureVac’s existing vaccine candidate in 2021, which is currently in Phase 2b/3 clinical trials in Europe and Latin America. Interim data from the ongoing trials are expected sometime in the first quarter of 2021.
TAIWAN VACCINATION The Taiwanese government is preparing for its national SARS-CoV-2 vaccination effort, but the source of its doses remains uncertain. Like many countries, Taiwan is currently awaiting delivery for doses it purchased months ago from multiple sources. Taiwan has largely managed to contain COVID-19, but health officials are responding to its first outbreak in months. Notably, Taiwan did not report a single domestic case between April 2020 and January 2021. Multiple Taiwanese vaccine candidates are in clinical trials, but the most advanced have not yet completed Phase 2 trials. The Taiwanese government has taken multiple approaches to securing vaccines, including COVAX facility led by the WHO and Gavi. Reportedly, Taiwan is experiencing problems obtaining doses from Western countries, potentially as a result of opposition by the Chinese government. Taiwan’s Minister of Health has reportedly expressed opposition to importing SARS-CoV-2 vaccines developed in China, due in part to an existing policy that prohibits importing vaccines and other “biological products” from China. Additionally, there is some uncertainty regarding the vaccines’ efficacy and safety data.
Notably, the interim COVAX allocation plan published by Gavi indicates that 1.3 million doses of the AstraZeneca-Oxford vaccine will be allocated to non-UN member states, potentially including Taiwan; however, the final determination will not be made until after the WHO issues an Emergency Use Listing (EUL). There is resistance to import Chinese made vaccines due to policies the shipment of biological products from China. In an effort to contain the ongoing outbreak in the absence of a vaccine, Taiwan is placing as many as 5,000 at-risk individuals into quarantine.
MYANMAR PROTESTS Following Monday’s military coup d’etat in Myanmar, staff from more than 70 hospitals and medical departments across 30 towns have stopped work in protest. Protesting healthcare workers are wearing red ribbons, and the Myanmar Civil Disobedience Movement issued a statement on February 3 indicating that they will not work for the new military government. According to one doctor, many who volunteered to support the COVID-19 response did so were inspired by Aung San Suu Kyi, leader of Myanmar’s National League for Democracy, who was deposed during the coup. The protest by healthcare workers has raised concerns about Myanmar’s new vaccination campaign, which started in late January, just days before the coup.
EASTERN MEDITERRANEAN REGION Earlier this week, a number of countries in the Eastern Mediterranean region announced new COVID-19 restrictions. For the most part, the Eastern Mediterranean region has avoided high COVID-19 mortality experienced by countries in other parts of the world, but recent increases in daily incidence prompted concerns about another COVID-19 surge. In response to the increasing transmission, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates implemented new restrictions on gatherings, including in public and at events like weddings and funerals; the operations of businesses, including retail stores and shopping malls, restaurants and bars, gyms and fitness centers; and international travel. Additionally, Kuwait is prohibiting celebrations for its National Day holiday on February 25. The duration of the measures varies by country, ranging from 10 days to several weeks.
MIXING VACCINES Researchers in the UK are initiating a clinical trial to evaluate the efficacy of vaccination using doses from 2 different vaccines. Allowing (or potentially recommending) individuals to receive 1 dose each from 2 different vaccines could introduce flexibility into vaccination programs and potentially even increase the degree of protection from the vaccination. The UK government has allocated approximately £7 million (US$9.6 million) to fund the study, and early data could be available by this summer. The study aims to include more than 800 participants aged 50 years and older who have not yet been vaccinated.
The trial will initially involve the Pfizer-BioNTech and AstraZeneca-Oxford University vaccines. The vaccines utilize different technology, with the Pfizer-BioNTech vaccine using an mRNA platform and the AstraZeneca-Oxford vaccine using an adenovirus platform. The participants will be divided among 8 trial arms. Four (4) will be control groups, which will receive 2 doses of the same vaccine (2 groups per vaccine) either 4 or 12 weeks apart. The other 4 groups will trial the mixed doses, with 2 groups receiving the AstraZeneca-Oxford dose first followed by the Pfizer-BioNTech dose, administered either 4 or 12 weeks apart, and 2 groups receiving the doses in the opposite order (4 or 12 weeks apart). The UK announcement stated that additional combinations could be added later, as additional vaccines received authorization.
US PHARMACY VACCINATIONS On February 2, the White House announced that the US government will increase distribution of SARS-CoV-2 vaccine doses nationwide. The principal increase will be in the form of 1 million doses per week that will be distributed to approximately 6,500 retail pharmacies nationwide, including major chains such as CVS, Rite Aid, and Walgreens. The pharmacies will make vaccination available to eligible individuals free of charge, which will dramatically increase the number of locations in the community where individuals can get vaccinated. The plan aims to scale up the number of participating pharmacies to 40,000 locations across the country.
Notably, the allocation for pharmacies will be in addition to the doses already distributed to states, and the state allotment will also increase by 500,000 doses per week, up to 10.5 million doses per week nationally. The initial pharmacy locations were deliberately selected to improve equitable access for “socially vulnerable communities” that are at elevated risk for infection and severe disease, including racial and ethnic minorities. Many pharmacies are already supporting vaccination operations in collaboration with state and local governments, but the new program will distribute the doses directly to pharmacies.
EMERGING VARIANTS & TESTING The emergence of new SARS-CoV-2 variants, particularly those that appear to be more transmissible and/or could mitigate the efficacy of vaccines or therapeutics, and expanded access to vaccination are raising concerns regarding the accuracy of existing tests. A team of researchers from the Johns Hopkins Center for Health Security developed an overview of diagnostic testing accuracy for these new variants as well as an insight into the potential effects of vaccination on diagnostic and serological testing.
The molecular diagnostic tests widely in use for SARS-CoV-2 detect infections by targeting specific genetic sequences present in the virus. In fact, a specific type of failure for these tests—an S-gene (spike protein) target failure—was instrumental in first detecting the B.1.1.7 variant. Both the B.1.1.7 and 501Y.V2 (B.1.351) variants have mutations on the spike protein; however, most existing test kits target other sets of genes. The majority of tests are expected to remain effective in detecting infection with the new variants, and the US FDA has issued a warning for those tests that utilize genetic sequences for the spike protein. Most of the existing diagnostic tests are capable of detecting infection with the known emerging variants; however, their sensitivity could be affected for future variants, depending on the specific mutations involved.
Vaccination is not expected to result in positive diagnostic tests. While both of the vaccines currently authorized for use in the US—the products from Pfizer-BioNTech and Moderna—both include mRNA corresponding to the spike protein, the quantity of mRNA in each dose is very small, much less than is generated during SARS-CoV-2 infection, and it does not amplify like the virus would. As we noted above, most diagnostic tests target other portions of the SARS-CoV-2 genome, and in combination with low quantity of mRNA, it is unlikely that an individual would test positive due to the vaccine. On the other hand, serological tests after vaccination could yield either positive or negative results, depending on the test. Serological tests identify the presence of antibodies as an indication of prior infection; however, the specific antibodies vary by test. The Pfizer/BioNTech and Moderna vaccines generate antibodies against the spike protein, so only serological tests that target those antibodies would yield positive results after vaccination. Conversely, tests that target antibodies against other parts of the virus (eg, receptor binding domain) would not identify the antibodies induced by the vaccine or provide any indication if the vaccine successfully generated an immune response.
2020 OLYMPICS The International Olympic Committee (IOC), International Paralympic Committee (IPC), and the Tokyo 2020 Organising Committee published the first in a series of “playbooks” that will outline protective measures that will be put in place during the 2020 Olympic and Paralympic Games* in Tokyo, Japan—currently scheduled for July-August 2021. Each playbook will focus on a specific stakeholder group, including the international federations, press, broadcasters, and athletes and officials. The playbook for athletes and officials has not yet been published; however, multiple media reports indicate that there will be testing requirements for athletes, both before arrival and regularly during their stay, and athletes will be directed to return home after they are done competing. Additionally, there could be a prohibition on physical contact between athletes outside of competition.
*The 2020 Olympic and Paralympic Games will retain their 2020 designation, even though they will be held in 2021.
I have so, so much I could say about teachers these days. Or teacher's unions in particular. Not much of it positive, so I'll refrain from posting my true thoughts. But yeah, disappointed as I've almost always been in their corner.
Also, Dr. Wen being poached from MSNBC was real interesting.
by JazzNU
ponchi101 wrote: ↑Tue Feb 02, 2021 9:12 pm
I am still not taking the Sputnik.
Here: vaccination to begin on Feb 20th. A five delay over the initial plan of Feb 15th.
I will get vaccinated by Jan 2022. You'll see.
I know you've delayed your trip back here, but you have a residence in Colorado, right? You may be able to get the vaccine there if you're interested before January whenever you do come back. I don't know what the rules are for Colorado, but many places are allowing snowbirds to get their vaccines, they basically just want some version of residency. So something to consider and look into if you're interested.
by ponchi101 No. American residency does not work that way. I can only stay 4 months a year (maximum) or I become a FISCAL residence, i.e. I have to pay taxes on all income, generated IN or OUT of the States.
But I can never become a RESIDENT unless I start applying for that, but that means I have to rescind my current visa because I have shown interest in moving to the States, and therefore I can become an illegal alien. And, if I am rejected for a resident visa, I do not get my previous one because, again, I have shown I "want to move" to the States.
Lots of sense, right?
by JazzNU I didn't mean do you have residency, like as a legal status classification. I meant a residence, like a house or condo? You talk about a place in Colorado and it seems like it's the same place, so I wasn't sure if you owned or rented it.
Regardless, you come to the US legally. I'd check on Colorado rules. It varies from state to state, but Colorado is likely a place that is going to make allowances for those that are not just citizens and permanent residents.
by ti-amie
by Deuce ^^^^ People unclear on the concept of freedom.
You are free to contract COVID-19.
You are free to become ill from the virus.
You are free to die from the virus.
And, the most important freedom of all - you are free to infect others so that they become severely ill and/or die from the virus.
The Land of the Free, indeed...
Sigh.
by Deuce
ponchi101 wrote: ↑Sat Feb 06, 2021 12:44 am
No. American residency does not work that way. I can only stay 4 months a year (maximum) or I become a FISCAL residence, i.e. I have to pay taxes on all income, generated IN or OUT of the States.
But I can never become a RESIDENT unless I start applying for that, but that means I have to rescind my current visa because I have shown interest in moving to the States, and therefore I can become an illegal alien. And, if I am rejected for a resident visa, I do not get my previous one because, again, I have shown I "want to move" to the States.
Lots of sense, right?
^ In December, Canadians who winter in Florida were getting vaccinated (for free) in Florida. They didn't need to own property in the U.S. - just needed to be there and be within the age range that Florida was giving vaccines to, apparently. Canadians typically spend 3 to 4 months in Florida, during Canadian winters.
Then, after people (correctly) complained that these Canadians were taking U.S. vaccines out of the arms of Americans, they changed it so that only Canadians who own a residence in Florida are able to get vaccinated in Florida.
So, it sounds to me that if you own a residence in Colorado, and Colorado has similar rules to Florida, you might be able to get vaccinated. Assuming you can get to Colorado, what with all the various travel restrictions and all.
by ponchi101 Your last part is the key. I decided not to go this season, and missing my snow and my skis, because of the restrictions. I cannot get to CO in a non-stop or just one airport stop so I would have to stop somewhere (most likely Florida), quarantine for 14 days and then carry on.
Not worth it.
by Deuce You could stop in Florida, quarantine for 14 days, claim to be Canadian, and get vaccinated there .
You wouldn't even have to go all the way to Colorado!
by JazzNU
ponchi101 wrote: ↑Sat Feb 06, 2021 2:34 am
Your last part is the key. I decided not to go this season, and missing my snow and my skis, because of the restrictions. I cannot get to CO in a non-stop or just one airport stop so I would have to stop somewhere (most likely Florida), quarantine for 14 days and then carry on.
Not worth it.
Well I wasn't talking about getting one next week. But you mentioned next January and the Russian vaccine so I just thought I'd mention getting one here instead since you do come here often enough in case you hadn't considered that as a possibility. Those travel restrictions won't be there forever, so just something to keep in mind.
As for Canadians. Yes, like I said, snowbirds have been able to get vaccinated. Florida had an issue with vaccine tourism that is somewhat cracked down on, or so they say, I'm sure some of it is still going on. It's more of a free-for-all there than it is elsewhere. And it's not about owning property somewhere, that would be incredibly discriminatory that even Florida wouldn't be able to do that. But I think they are trying to make sure you're some version of a resident there, likely those who have addresses there because vacationers were going there with the intention of finding and getting a vaccine. It's not exactly breaking news, but Florida is not a well run state, so their approach to vaccine distribution has left a lot to be desired.
by ponchi101 Oh, sure. That could be a plan later on. Colombia will start vaccinating in about one more week, so I will see how things are going here. I think that I may go to Colorado in the fall (it is gorgeous that time of year) and I will likely go through Georgia (wanna visit my new grand-niece).
Colombia's plan is to vaccinate 125K/week as their target. If they can do that, that is almost 1MM/week, so maybe my paranoia will not come to fruition and I may get my shot before the end of the year.
But right now, the USA is not the most direct route. I will keep you idea in hand, though.
by Suliso No drastic changes in the last 10 days so this time I've added the new numbers for the same countries in red.
Suliso wrote: ↑Tue Jan 26, 2021 11:07 pm
I used to post some covid statistics on TAT 1.0. Not as extensive this time, only the final mortality rate. Top 10 plus some notables excluding micro states. Note that 1000 means that 0.1% of the countries population has died from the disease in the last year or so.
Deaths per 1 million inhabitants
Belgium 1,791 1838
Slovenia 1,638 1743
UK 1,471 1646
Czechia 1,457 1608
Italy 1,431 1506
Bosnia and Herzegovina 1,414 1461
North Macedonia 1,350 1400 USA 1,3091426 Portugal 1371
Bulgaria 1,284 1346
Hungary 1,256 1357
-------
Spain 1,215 1313
Peru 1,200 (worst in SA) 1267
Mexico 1,159 1278
France 1,134 1206
Sweden 1,110 1195
Portugal 1,082 (currently the worst outbreak in EU) now in the top 10
Switzerland 1,059 1105
Argentina 1,040 1081
Brazil 1,026 (I suspect undercounting) 1082
Colombia 1,018 1088
Germany 648 739
Ireland 617 739
Latvia 601 715
Canada 511 546
Israel 491 (current leader in vaccinations) 554
Denmark 350 382
Finland 118 124
Norway 101 (best in continental Europe) 107
by ti-amie Both Suliso and Dry are doing a great job keep us informed about what this pandemic is doing to the world. Thanks to you both.
by ti-amie
But hey way to go Iowa. Florida is a lost cause.
by ponchi101 On a personal note. The government of Bogota is setting up test sites across the city. I got tested (antigen) on Friday. Results uploaded to the web. I tested negative for the virus, meaning I have not caught the disease.
Now, please, that vaccine...
by ponchi101
ti-amie wrote: ↑Sun Feb 07, 2021 7:24 pm
Both Suliso and Dry are doing a great job keep us informed about what this pandemic is doing to the world. Thanks to you both.
Much more comprehensive than any news site I can think of. Thanks indeed to both.
by mmmm8
ponchi101 wrote: ↑Sun Feb 07, 2021 7:36 pm
On a personal note. The government of Bogota is setting up test sites across the city. I got tested (antigen) on Friday. Results uploaded to the web. I tested negative for the virus, meaning I have not caught the disease.
Now, please, that vaccine...
Mexico City have done this since November, seems to be convenient (I had to look into it for something) - haven't looked for any numbers in terms of whether it helped in the city.
by ponchi101 The only good thing that can come up from that is: people that test positive can go into quarantine (and the GOV will know who did, so fines are possible). And you know my peeve about lack of proper stats. This can help.
by ti-amie
by shtexas Waiting over 2 hours for my Mom's second shot. I am guessing at least 3 hours to go. We are off the streets and now driving up and down in a parking lot. It's ridiculous.
by shtexas
shtexas wrote: ↑Tue Feb 09, 2021 8:39 pm
Waiting over 2 hours for my Mom's second shot. I am guessing at least 3 hours to go. We are off the streets and now driving up and down in a parking lot. It's ridiculous.
Shot in arm at the 4 hr 15 minute mark.
by Suliso Doesn't smell like a good organization, but at least success.
by ponchi101 These are the kinds of things at which governments are not really good at. For them, private industry is better.
Want to get vaccinated? You walk in here and pay for the vaccines of 5 people not related to you, and in a risk group. You would see how a profit motive would have put that vaccine in several more millions by now.
by dryrunguy The most recent Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 106.13 million cases and 2.32 million deaths as of 11am EST on February 9. The global weekly incidence decreased for the fourth consecutive week, down to 3.12 million new cases last week, the lowest weekly total since mid-October. This is a 17.7% decrease from the previous week and a 38.2% decrease from the peak in reported incidence in early January. After holding relatively steady for the last 2 weeks of January, global weekly mortality decreased for the first time since mid-October*, a decline of 10% compared to the previous week. If this is indicative of a longer-term trend, it would correspond to approximately 3-4 weeks after the peak in global weekly incidence.
*With the exception of the weeks corresponding to the Christmas and New Year’s holidays.
Our World in Data reports that 134.65 million vaccine doses have been administered globally, a 31% increase compared to this time last week.
The Johns Hopkins Coronavirus Resource Center reported 27.11 million US cases and 465,648 deaths as of 12:30pm EST on February 9.
UNITED STATES
The US CDC reported 26.85 million total cases and 462,037 deaths. The US surpassed 450,000 cumulative deaths on February 4. Daily incidence in the US continues to decrease steadily, now down to 116,904 new cases per day. Since the peak on January 8 (248,607), the national average daily incidence is down by more than half; however, it is still nearly 75% higher than the previous peak (67,230 on July 22, 2020). The US is still #1 globally in terms of total daily incidence, and it is still reporting more than double the daily incidence in #2 Brazil (42,188).
The US reported 5,189 deaths on February 4. This is the second highest single day total reported by the US to date, following April 15, when New York City reported more than 3,700 previously unreported probable deaths from the onset of its epidemic. The February 4 spike was due to 1,507 deaths reported by Indiana, which caused the state’s cumulative total to jump 15.8%, from 10,091 to 11,637 deaths—and the per capita mortality to increase from 150 deaths per 100,000 to 173. These deaths caused the national daily average to jump from 3,056 to 3,227 deaths per day. The CDC is working with health officials from Indiana to determine the time frame corresponding to these deaths.
As the US daily incidence continues to decline, we want to take a closer look at US testing data to determine whether the decreasing daily incidence is a result of a true decrease in community transmission or a function of testing or reporting. To start, we will look at testing volume. US testing volume scaled up steadily from the onset of the pandemic through mid-July, around the peak of the summer 2020 surge, before declining in late summer. Testing increased again during the autumn 2020 surge and reached its highest peak in November. Testing volume has declined consistently since that time, with the exception of reporting fluctuations due to the Thanksgiving, Christmas, and New Year’s holiday weekends.
As we have covered previously, test positivity is one of the better measures of effective testing programs and sufficient volume. Test positivity in the US has varied widely over the course of the US epidemic. The peak national test positivity was more than 20% during the initial surge in the spring of 2020, when the supply of test kits was limited and testing was largely limited to symptomatic patients and/or those with relevant travel history. Test positivity fell as the initial surge receded and testing capacity scaled up, and it then climbed with the summer 2020 surge, up to approximately 10%. The minimum test positivity was approximately 5%, reported in mid-to-late September*, before it increased again in conjunction with the autumn 2020 surge. Test positivity peaked at 15.4% during the last week of December 2020, and it has decreased steadily over the past 4 weeks. The current test positivity is 9.7%, down from 11.2% the previous week. For reference, the cumulative national test positivity over the course of the US COVID-19 epidemic is 9.19%, and the current national average is quickly approaching this benchmark.
*The lowest preliminary values reported were 4.8% in 2020 Week 38 and Week 39; however, these were updated in the following weeks’ reports to 5.0% and 5.2%, respectively. The first reported weekly increase was from 5.3% to 5.4% during 2020 Week 41.
The combination of steadily declining daily incidence, testing volume, and test positivity provides a good indication that the overall declining trend in the US not an artifact of reporting or testing issues.
At the state level, the US CDC is currently reporting elevated test positivity (6% or higher) in 34 states, including 12 with 11% or higher, based on the average over the past 7 days. While this is still a concerning number of states above the 5% recommended threshold, many states are trending in the right direction. For comparison, the 30-day average test positivity is 6% or more for 41 states, including 23 reporting 11% or higher. The difference between the 30-day and 7-day averages indicates that numerous states are reporting decreasing test positivity over the past several weeks. In fact, 17 states have a lower 7-day average than 30-day average, and no states have a higher 7-day average. The COVID Exit Strategy website reports 15 states with test positivity greater than 15%, including 6 greater than 30%, and only 2 states with test positivity below 5% (Vermont and Hawai’i); however, 26 states are reporting decreasing test positivity over the past 2 weeks, including 8 of the 15 states currently reporting test positivity greater than 15%.
US Vaccination
The US CDC reported 59.31 million vaccine doses distributed and 42.42 million doses administered nationwide. The US has administered 71.5% of the distributed doses, an increase of more than 10 percentage points since Friday (61.2%). In total, 32.34 million people (nearly 10% of the entire US population) have received at least 1 dose of the vaccine, and 9.52 million (2.9%) have received both doses. The average daily doses administered is once again increasing, now up to a record high of 1.46 million doses per day.
A total of 4.95 million doses have been administered at long-term care facilities (LTCFs) through the Federal Pharmacy Partnership for Long-term Care (LTC) Program*, including residents and staff. This covers 3.78 million individuals with at least 1 dose and 1.15 million with 2 doses. Approximately 60% of the doses have gone to residents, and 40% to staff.
*The dashboard only includes data for doses administered through the federal program. It does not report data from West Virginia, which opted out of the program.
VACCINATION & VIRAL LOAD As vaccines continue to progress through clinical trials and vaccination efforts scale up in countries around the world, many questions remain about the efficacy of vaccines and vaccine candidates, particularly with respect to their ability to mitigate transmission risk. Researchers in Israel published (preprint) findings from a study on the viral load due to SARS-CoV-2 infection in vaccinated individuals. The researchers evaluated quantitative PCR results from individuals vaccinated with the Pfizer-BioNTech vaccine who subsequently tested positive for SARS-CoV-2 infection to determine any effect of vaccination on viral load. The study included specimens from nearly 3,000 patients in Israel collected December 23, 2020-January 5, 2021.
The researchers identified a significant decrease in the viral load in specimens collected 12 or more days after vaccination, corresponding to the expected “onset of early vaccine protection.” The researchers also compared the viral loads between vaccinated and unvaccinated individuals and identified a significant decrease in viral loads among the vaccinated individuals—12 days or longer after vaccination. In order to slow community transmission, a vaccine must be able to decrease the risk of infection in vaccinated individuals or decrease the transmissibility of vaccinated individuals. The viral loads in vaccinated patients indicates that they are still capable of being infected with SARS-CoV-2, but the risk of infection remains unclear. While this study does not assess transmissibility directly, it provides further evidence that the Pfizer-BioNTech vaccine can reduce the viral load, which could potentially contribute to reduced transmissibility.
VACCINATION EQUITY Inequity in vaccine access remains a major challenge in the US, and state and local health officials are working to mitigate equity issues as eligibility requirements expand. In many jurisdictions, efforts to administer vaccinations as quickly as possible have focused on populations that are more easily accessible, which in some instances, has resulted in lower vaccination coverage for high-risk groups, including racial and ethnic minorities, older adults, and lower-income communities. The location of vaccination sites and online scheduling systems can be barriers for many individuals, and health officials are combatting vaccine hesitancy in many communities. While some of these disparities may have been driven early on by the demographic characteristics of the earliest priority groups (eg, LCTF residents and staff, frontline healthcare workers), they have persisted as eligibility expands.
In New York City, the population is approximately 29% Latinx and 24% Black; however, these communities represent only 15% and 11% of the vaccinated population, respectively. The disparities increase with age as well, with Black individuals accounting for only 9% of vaccinees aged 65 years and older. New York City officials have identified major racial and ethnic disparities at some vaccination sites, which appear to be driven, in part, by individuals who live outside the community (eg, those who commute into the city for work). In order to mitigate these disparities, some vaccination sites will actively prioritize local residents for vaccination, and city health officials will begin reporting demographic data for vaccinations by ZIP code.
Researchers from The Working Group on Equity in COVID-19 Vaccination, CommuniVax, led by Dr. Monica Schoch-Spana at the Johns Hopkins Center for Health Security and Dr. Emily Brunson at the Department of Anthropology at Texas State University released their first report, part of an ongoing effort to promote equity in SARS-CoV-2 vaccination. The report focuses on state and local plans to engage Black, Indigenous, and People of Color (BIPOC) communities to support ongoing and future vaccination efforts, based on findings from a series of key informant interviews. The report outlines 5 key principles to facilitate effective engagement with racial and ethnic minority communities: Iteration, Involvement, Information, Investment, and Integration. Additionally, the researchers provide detailed descriptions of short- and long-term recommendations and tools to support state and local officials in their efforts to mitigate the disproportionate effects of the COVID-19 pandemic on these vulnerable communities.
SOUTH AFRICA VACCINATION In response to clinical trial data that indicate that the AstraZeneca-Oxford University SARS-CoV-2 vaccine exhibits low efficacy against the B.1.351 variant, South Africa announced that it is suspending vaccination efforts for that vaccine. The B.1.351 variant was first identified in South Africa in November 2020. Researchers from the Wits University Vaccines and Infectious Diseases Analytics (VIDA) Research Unit, which is conducting clinical trials for the vaccine in South Africa, found that the vaccine “provides minimal protection against mild-moderate COVID-19.” Notably, the researchers estimated the vaccine’s efficacy against the B.1.351 variant to be only 22%, based on a small study of approximately 2,000 participants. The study did not evaluate efficacy in preventing severe disease or death. South Africa will implement a new vaccination plan, which will aim, in part, to provide data needed to better characterize the vaccine’s efficacy against the B.1.351 variant. The data from this study have not yet been subjected to peer review, and further investigation is required.
EMERGING VARIANTS A study (preprint) by researchers in California (US) found that the prevalence of the B.1.1.7 variant of SARS-CoV-2 is rapidly increasing in the US. The researchers analyzed rates of S gene target failures (SGTFs) for PCR-based diagnostic tests and genomic sequencing to analyze the growth dynamics of the emerging and highly transmissible variant. SGTFs in specimens collected in the UK led to the initial detection of the B.1.1.7 variant, and they can serve as a proxy for the presence of the variant in clinical specimens.
Based on data from approximately 500,000 specimens collected from July 2020-January 2021, the researchers observed a slow but steady increase in the prevalence of SGTFs starting in October 2020, with a more rapid increase in January 2021—up from 0.8% in early January to 4.2% in late January. Based on the proportion of specimens with SGTFs, the researchers estimate the doubling time for the B.1.1.7 variant in the US to be approximately 10 days, which indicates increased transmissibility compared to the predominant strain. The genomic analysis of specimens collected in December 2020-January 2021 suggests that the variant was introduced to the US numerous times; however, most of the domestic transmission likely stems from “independent introductions into California...and Florida.” The researchers expect that the variant has been circulating in the US since November 2020.
US VACCINE PRODUCTION & DISTRIBUTION Shortly after taking office, US President Joe Biden indicated that he would utilize the Defense Production Act (DPA) to scale up production of critical supplies, including SARS-CoV-2 vaccines. In the February 5 White House COVID-19 response briefing, Tim Manning, the US government’s COVID-19 Supply Coordinator, announced that efforts are underway to give Pfizer “priority access” to critical supplies and equipment under the DPA in an effort to rapidly scale up production capacity. Some experts argue that the DPA is not sufficient to rapidly or meaningfully increase vaccine production capacity, because vaccine production processes are complex and require time to scale up. A senior official from Pfizer recently indicated that the company expects to shorten vaccine production time by half, which will significantly increase the overall production capacity. The improvements appear to stem from internal efforts to optimize the manufacturing process; however, improved availability of critical equipment and supplies could support further improvements to capacity.
Even as production capacity is scaling up, US states continue to struggle to implement vaccine administration operations at the local level. One of the principal challenges is uncertainty regarding the timing and quantity of vaccine deliveries. Without a clear idea of how many doses will arrive and when to expect them, hospitals, health departments, and other vaccinators are finding it difficult to schedule appointments, which is slowing vaccination progress. Reliable, longer-term delivery scheduling and tracking could provide state and local jurisdictions the confidence needed to schedule more appointments in advance or expand capacity at mass vaccination clinics; however, the existing process remains “opaque.” Eligibility is expanding in many states, and the demand for vaccination is easily exceeding the current supply. But even as efforts are ongoing to expand production capacity, it is likely that the supply will continue to fall short of demand for months to come.
ISRAEL VACCINATION Israel is conducting one of the most effective SARS-CoV-2 vaccination campaigns in the world. On a per capita basis, it currently ranks #2 in terms of daily doses administered (behind the UAE) and #1 in terms of cumulative doses—it is also #5 globally in terms of total cumulative doses, despite having a population of only 8.7 million. Israel has administered nearly 66 doses per 100 population, which corresponds to single-dose coverage for 66 percent of the population or full, 2-dose coverage for 33%.
It is unclear exactly how many individuals have received 1 or 2 doses of the vaccine, but of all countries, Israel is likely the closest to achieving coverage sufficient to make an impact on its COVID-19 epidemic. Israel’s daily incidence has decreased somewhat from its highest peak in mid-January; however, at more than 6,000 new cases per day, it remains equal to or higher than its previous peak in late September. While Israel may not yet be at the point of making an impact on the national scale, the effects of high coverage among the earliest priority groups are starting to become evident. A report published in Nature indicates that COVID-19 incidence among adults aged 60 years and older decreased 41% from January to February, including a 31% decrease in hospitalizations. For comparison, incidence and hospitalizations fell by only 12% and 5%, respectively, among younger adults over that time.
Israel’s COVID-19 response, including its vaccination efforts, has not been without challenges. Despite notable national progress toward vaccination coverage, a report published in New York magazine indicates that “until last week, [Israel] did not distribute vaccines to the Palestinian Authority, the semi-autonomous government of the West Bank,” illustrating disparities in vaccine access for the vulnerable minority population. Some human rights organizations argue that Israel is responsible for vaccinations in the Israeli-occupied territory and the “blockaded Gaza Strip,” but the Israeli government argues that Israeli citizens are its top priority.
WHO SARS-CoV-2 ORIGIN INVESTIGATION A WHO team of international experts visited China to further investigate the origins of the SARS-CoV-2 virus. The joint China-WHO investigation began on January 14, 2021, including investigations and site visits at several critical locations in Wuhan and other parts of China. At a press conference on February 9, the team presented their initial assessment. Perhaps most notably, the team concluded that a laboratory release of the virus was “extremely unlikely.” Rather, the investigation suggests that zoonotic transmission from an existing animal reservoir is much more likely. It will be very difficult, however, to determine the exact nature of the original spillover event.
Team leader Dr. Peter Ben Embarek stated that, while the understanding of the pandemic scenario did not change dramatically as a result of the investigations, the team’s research added important details to the story. The investigation was not able to identify a specific animal reservoir, but bats and pangolins remain the principal focus for future investigations. Dr. Marion Koopmans suggested that future investigations should include surrounding farmlands and farmers where human-bat or other human-animal interactions could facilitate the spillover of SARS-CoV-2 into humans. Another working theory is that the virus could have been introduced into humans via frozen food, such as the types of products sold at the Huanan seafood market, where one of the first clusters of cases was identified. This investigation alone was unlikely to pinpoint the exact origin of the COVID-19 pandemic, and further efforts over the coming years will continue to investigate potential sources and factors associated with the pandemic’s origin.
MASK MANDATES Although mask mandates and mask use have been sources of contention throughout the pandemic, including in the US, a study by the US CDC COVID-19 Response Team found that mask mandates are associated with decreased COVID-19 hospitalizations. This study analyzed COVID-19 data from 10 US states that instituted statewide mask mandates, implemented approximately from March through October 2020. The study included data collected by hospitals in the COVID-19–Associated Hospitalization Surveillance Network (COVID-NET) in California, Colorado, Connecticut, Maryland, Michigan, Minnesota, New Mexico, New York, Ohio, and Oregon.
The researchers found that states that implemented statewide mask mandates reported a significant decrease in COVID-19 hospitalization growth rates among adults aged 18-64 years. Within 2 weeks of implementing the mask mandate, hospitalization growth rates among adults aged 40-64 years decreased by nearly 3% compared to before the mandate. At 3 weeks or longer, the hospitalization growth rates decreased by 5.5% for adults aged 18-39 and 40-64 years. Hospitalization rates did not fall significantly for adults aged 65 years or older, but this group does face higher risk of severe COVID-19 disease. COVID-19 risk, including hospitalization, is the result of numerous factors, and it is not necessarily possible to determine causative associations; however, the correlation between statewide mask mandates and decreased COVID-19 hospitalizations provides further evidence of mask efficacy. Currently, 36 states, plus Puerto Rico, have statewide mask mandates in place, and states that do not have statewide mandates may have local requirements, such as at the city or country level.
VACCINE CERTIFICATES International vaccination certificates are already used to document travelers’ protection against some endemic diseases, such the “Yellow Card” for yellow fever vaccination. Some countries are beginning to investigate the possibility of a similar system for SARS-CoV-2 vaccination, which would allow travelers to enter a country without being subjected to testing or quarantine. The EU is reportedly evaluating a universal system for Member States, but individual countries are also creating their own certificates in the interim. Iceland was among the first to create its own certification system in January, and Poland is utilizing a digital QR code to document vaccination status. Denmark and Sweden reportedly plan to unveil vaccination certificates in June, and the UK is considering its own “vaccine passport,” which could be implemented this summer. Other countries, such as the US, have indicated interest in vaccine certificates but have not yet announced an anticipated timeline. The WHO has also been working with Estonia to create a universal digital vaccination certificate.
Suliso wrote: ↑Tue Feb 09, 2021 11:03 pm
Doesn't smell like a good organization, but at least success.
The sad thing is I will probably end up doing it 2 more times for myself.
Interesting note: Biden and the Feds have chosen Fair Park to expand services starting next week, turning it into a mega-site.
Can the Feds do it better, keeping in mind they are expanding the number of shots given per day to a site that can't handle the number they already are giving?
by Omess ^^^^ new avatar, I think you were one the few that kept the same one on TAT1.0
Sent from my iPhone using Tapatalk Pro
by shtexas
Omess wrote: ↑Thu Feb 11, 2021 7:10 am
^^^^ new avatar, I think you were one the few that kept the same one on TAT1.0
Sent from my iPhone using Tapatalk Pro
Yes. I did keep that same one for years. But, I started with a Barbara Schett avatar.
Wolverine was the first picture this site would accept as an avatar.
by Suliso Situation in Czechia:
The government has struggled to curb infections as more and more citizens ignore restrictions that have been in place on and off since March 2020.
Defying government-imposed closures, some pubs and restaurants as well as ski resorts have opened up for business.
A poll published on Wednesday showed widespread public scepticism about the pandemic, with fewer than half of Czechs saying they would stay at home if they showed the symptoms of Covid-19.
Some 45% said they thought the pandemic was just a “media bubble” and only 18% of respondents in the poll commissioned by the World Health Organization and a Czech medical society said the virus posed a high risk.
The above is from BBC updates. Czechia has the third highest covid death rate per population in EU.
by Suliso Situation is a bit similar in most of Eastern Europe because in our region there is a low trust in government (compared to the rest of EU not Venezuela). That's a cultural remnant from socialist times, the first instinct for most people is "government is lying and stealing".
by ponchi101
Suliso wrote: ↑Fri Feb 12, 2021 9:06 am
Situation is a bit similar in most of Eastern Europe because in our region there is a low trust in government (compared to the rest of EU not Venezuela). That's a cultural remnant from socialist times, the first instinctunderstanding for most people is "government is lying and stealing".
As we used to do in TAT1.0, corrected that for you.
When the people say the "government is lying and stealing", they are so seldom wrong.
by Suliso Some statistic from Switzerland (updated today)
Total cases: 540,727
Total hospitalizations: 22,694
Total fatalities: 9,030
Current daily cases (7 day average): 1,263 (-19% from a week before)
Current daily deaths (7 day average): 18.4 (-31%)
Currently in hospital: 1,086 (-15%)
Vaccination rate: 5.6% (482,243)
by JazzNU In the conversation of how Australia (and New Zealand) have been able to do so much better than other places. I'm not sure if anyone was listening to Darren Cahill the other night during I can't remember what match, but he was talking about how he had to quarantine to go back to Adelaide now that there were the cases in Melbourne.
Darren said that he had to stay home and apart from his family for that period of time. That he could go outside on his property, can't walk the dog up the street as long as he's alone, a question that Patrick asked about because it's something he did when he quarantined himself after testing positive. So if he's got no outdoor property, he's just SOL. And then he added, which I think is key, the police will come to check on him 3 to 5 times during his 14-day quarantine to make sure that he is staying home as he's supposed to. At least here in the US, the public resources aren't set up to handle checks like that for so many people. Could they have done this early on when case numbers were as low as they've been in Australia? Absolutely. And that may have been the thing that truly contained this here. But they aren't merely relying on people to "do the right thing" as has been suggested like Aussies are just so much more responsible than citizens of other countries. They might be somewhat more conscientious, but clearly it's not just that. They are enforcing the rules they put in place, and that is clearly making a big difference.
by dryrunguy The most recent Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 107.42 million cases and 2.36 million deaths as of 9am EST on February 12.
Approximately two-thirds of countries and territories worldwide are reporting decreasing trends in COVID-19 incidence. In total, 123 countries and territories (62.8%) are reporting a negative weekly growth rate—relative change in 1-week incidence compared to the previous week—compared to 73 with a positive growth rate over that time. 131 countries are reporting decreased incidence over the past 2 weeks (67.2%), compared to 64 with an increasing biweekly trend. Notably, 34 countries/territories are reporting decreases by half or more compared to 2 weeks ago, including 9 with decreases of 100% over the past 2 weeks (ie, currently averaging zero new cases per day). The largest biweekly increases are in Guinea-Bissau (+485%), Somalia (+473%), and Antigua and Barbuda (+436%), all of which exceed +400% over the past 2 weeks. In total, 28 countries are reporting biweekly increases of 50% or more, and only 11 with increases of 100% or more over that time. The overall global trend is a decrease of 24% over the past 2 weeks.
Countries and territories with decreasing daily incidence are spread across the globe, with several small pockets of increasing incidence. The areas with the highest concentration of countries/territories reporting positive biweekly growth rates are the northern part of Sub-Saharan Africa, including along the coast of West Africa and across Central Africa to Somalia; Southeast Europe; the Eastern Mediterranean region, including much of the Arabian Peninsula; and Southeast Asia, including Papua New Guinea.
Our World in Data reports that 160.07 million vaccine doses have been administered globally, a 28% increase compared to this time last week.
UNITED STATES
The US CDC reported 27.13 million total cases and 470,110 deaths. Daily incidence in the US continues its steady decline, now just slightly more than 100,000 new cases per day. Daily mortality continues to decrease as well, back down to slightly more than 3,000 deaths per day. We expect that to fall further in this afternoon’s update, as February 5 moves out of the 7-day window*. That being said, multiple reports indicate that Ohio may have inadvertently underreported COVID-19 deaths in November and December 2020. Ohio Governor Mike DeWine stated that Ohio underreported COVID-19 mortality by approximately 4,000 deaths over the past several months. An investigation into the mortality reporting is underway, and the deaths are expected to be included in official reports over the next several days. This would bring Ohio’s cumulative mortality from approximately 12,000 to 16,000, an increase of approximately one-third. This would also bring the cumulative national total to nearly 475,000 deaths, and depending on how the deaths are reported, it could artificially inflate the current daily average.
*On February 5, Indiana reported 1,507 new deaths, many of which were previously unreported deaths from earlier in its epidemic.
US Vaccination
The US CDC reported 68.29 million vaccine doses distributed and 46.39 million doses administered nationwide (67.9%). The CDC has added new data to its vaccination dashboard, including demographic data.
In total, 34.72 million people (10.5% of the entire US population) have received at least 1 dose of the vaccine, and 11.19 million (3.4%) have received both doses. The average daily doses administered is once again increasing, now up to a record high of 1.46 million doses per day*. The number of people receiving their second dose is increasing at nearly 550,000 per day*. The CDC is reporting slightly more Pfizer-BioNTech doses administered (24.25 million; 52%) than Moderna (22.04 million; 48%).
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 5.35 million doses have been administered at long-term care facilities (LTCFs) through the Federal Pharmacy Partnership for Long-term Care (LTC) Program*, including residents and staff. This covers 3.96 million individuals with at least 1 dose and 1.36 million with 2 doses. Approximately 59% of the doses have gone to residents, and 41% to staff.
*The dashboard only includes data for doses administered through the federal program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins Coronavirus Resource Center reported 27.41 million US cases and 476,183 deaths as of 12:30pm EST on February 12.
US SCHOOLS Last week, US CDC Director Dr. Rochelle Walensky stated that agency officials are finalizing recommendations regarding school reopening and that official guidance should be published soon. The guidance is expected to play a major role as state and local governments and school systems across the country continue to debate how to safely return students and teachers to the classroom. The issue has been fiercely debated, extending to courtrooms and picket lines. US President Joe Biden has indicated that he aims for most K-12 schools to reopen within his first 100 days in office. One of the biggest issues is how to prioritize teachers for vaccination and if or how to resume in-person classes before they can be vaccinated. Dr. Walensky recently stated that vaccinating teachers is not a prerequisite for resuming in-person classes. The CDC’s Advisory Committee on Immunization Practices (ACIP) includes teachers in its Tier 1b priority group, but Dr. Walensky indicated that schools can implement measures to mitigate transmission risk in the classroom until teachers can be vaccinated. In addition to teachers, there is also ongoing debate regarding the risk to students, most of whom are too young to be vaccinated against SARS-CoV-2.
Following protests in opposition to in-person learning in January, the Chicago Teachers Union approved an agreement with the nation’s third largest school district to resume in-person classes. With the agreement in place, Chicago avoids the risk of a teacher strike or lockout. While the agreement was approved by the union by a 2-1 margin, some are criticizing the terms as insufficient to protect teachers. Pre-kindergarten and special education classes will be among the first to return to in-person classes, followed by kindergarten through 8th grade returning for 2 days a week later this month or possibly in March. While in-person classes will resume, parents still have the option to continue remote/online learning for their students.
BRAZIL VACCINE PRODUCTION Brazil reportedly received its first shipment of the active pharmaceutical ingredients (APIs) necessary to manufacture the AstraZeneca-Oxford University SARS-CoV-2 vaccine. Vaccine production in Brazil will be conducted by the Oswaldo Cruz Foundation, commonly referred to as Fiocruz. Brazil expects to receive enough of the APIs in February to manufacture 15 million doses, and the government has purchased enough for 100 million total doses. While the vaccine was developed in the UK, a substantial portion of the APIs for the vaccine are produced by WuXi Biologics in China. According to a previous report by Reuters, Brazil struggled to navigate export procedures in China, which delayed the shipment of the APIs. While Brazil awaits domestic production capacity, it is utilizing the Chinese Sinovac vaccine in the early stages of its vaccination campaign. In addition to the Sinovac and AstraZeneca-Oxford vaccines, Pfizer submitted an application to regulatory authorities for the vaccine it developed in collaboration with BioNTech.
INDONESIA VACCINE AUTHORIZATION & PRIORITY GROUPS When Indonesia’s National Agency for Drug and Food Control (Badan POM) issued the Emergency Use Authorization (EUA) for China’s Sinovac vaccine, it only authorized the vaccine for use in adults aged 18-59 years. At the time, the clinical trial data available to Indonesian regulatory officials were not sufficient to determine the efficacy in adults aged 60 years and older. The age restriction drove Indonesia’s decisions regarding priority groups for vaccination, and eligibility was initially limited to healthcare workers, followed by other essential workers, aged 18-59. Without an EUA for adults aged 60 and older, Indonesia could not administer the vaccinations to older adults who are at elevated risk of severe disease and death.
Badan POM continued to monitor ongoing Phase 2 and 3 clinical trials in Brazil and China, and after evaluation of preliminary data from those trials, Indonesia determined that the vaccine demonstrated sufficient efficacy in older adults to warrant eliminating the upper age restriction. On February 5, Badan POM issued a new EUA that authorizes the vaccine for use in all adults aged 60 years and older. Following the announcement, the Indonesian MOH announced that eligibility would expand immediately to include all adults aged 60 and older. Indonesia began administering vaccinations to older adults on February 8, including doctors who were not previously eligible for vaccination due to their age.
RWANDA TRAVEL RESTRICTIONS RwandAir, Rwanda's national airline, announced a temporary restriction on flights to and from South Africa, Zambia, and Zimbabwe, beginning February 8. Restricted locations include Johannesburg and Cape Town, the 2 most populous cities in South Africa, as well as Lusaka and Harare, the capitals of Zambia and Zimbabwe, respectively. The Rwanda Biomedical Centre also published guidance and requirements for passengers, including a negative SARS-CoV-2 test within 72 hours of departure and additional testing upon arrival, conducted at the traveler’s expense (US$60). Travelers will be required to remain at a designated transit hotel until results of their arrival test are available. Travelers will be required to undergo a 7-day self-quarantine period, even with a negative test, and a final test will be available after the quarantine (free of charge).
UPDATED MASK USAGE RECOMMENDATIONS On February 10, the US CDC published updated guidance regarding ways to improve the efficacy of facemasks, which supplements existing mask guidance. The recommendations focus on 2 principal factors in how masks provide protection: fit and filtering ability. The CDC continues to recommend wearing a “mask [that] fits snugly against your face” and selecting masks that have multiple layers to filter respiratory droplets. The new guidance includes several additional recommendations and tips for improving both aspects of mask use.
Under the new guidance, the CDC now recommends selecting a mask with a “nose wire” that can be bent to mold the shape of your nose, which reduces the air that can escape around the top edge of the mask. The CDC also recommends using a “mask fitter or brace” on the outside of the mask to hold it more snugly to your face and provide a better seal around the edges. And finally, the CDC recommends adding layers of filtering material to your mask, including selecting a mask constructed of multiple layers of fabric or “double masking.” In the new guidance, double masking specifically refers to wearing a reusable cloth mask on top of a disposable mask (eg, medical, surgical mask). The CDC explicitly recommends against wearing multiple disposable masks or combining any kind of disposable or reusable mask with a respirator (eg, N95, KN95). The guidance also provides tips for determining whether your mask fits properly. The new guidance follows recent attention on double masking as a potential technique to reduce transmission risk in the face of emerging highly transmissible SARS-CoV-2 variants.
The updated guidance is based on findings from a study by the US CDC COVID-19 Response Team on improving the fit of facemasks. The researchers tested “double masking” and “knotting and tucking” to evaluate the extent to which they affected mask efficacy. Knotting and tucking refers to tying the straps/ear loops in a knot to bring the corners of the mask together and then tucking in the extra material “to minimize the side gaps.” One simulation compared the efficacy of double masking by comparing the combination of a cloth mask worn over a medical mask to each mask worn alone, and a second simulation compared various mask configurations, including double masking, to evaluate the effect of knotting and tucking. The simulations tested breathing and coughing and tested the effect for both exhalation and inhalation (ie, source and receiver, respectively). In the first experiment, the double masking configuration (unknotted) “blocked 92.5%” of cough particles, compared to 42% for the medical mask alone and 44.3% for the cloth mask alone. In the second experiment, when either the source (exhaling) or receiver (inhaling) utilized the double masking or knotted configuration (ie, only one of the two), the exposure to the receiver was reduced by approximately 82% and 63%, respectively. When either configuration was used on both the source and receiver, the receiver’s exposure was reduced by approximately 96%. A number of variables factor into the efficacy of these configurations, but this study provides evidence that these techniques can increase the level of protection for mask wearers. Notably, the new CDC mask guidance does not explicitly address knotting and tucking. See a quick tip from Sr. Scholar Caitlin Rivers to make your mask fit better.
UPDATED US VACCINATION GUIDANCE The US CDC published an update to its SARS-CoV-2 vaccination guidance. Most of the updates are relatively minor changes, including efforts to improve the reporting process for vaccine administration errors, clarifications on various contraindications, updated descriptions of injection-site reactions, and testing requirements for tuberculosis. The most notable update addresses quarantine requirements for vaccinated individuals after exposure to known COVID-19 cases. The new guidance largely eliminates quarantine recommendations for fully vaccinated individuals. Individuals who meet all of the following requirements do not need to quarantine after a known exposure:
Received all required doses of the vaccine (ie, 2 doses for a 2-dose vaccine; 1 dose for a single-dose vaccine)
Received their final doses 2 weeks or longer before the exposure
Are within 3 months of their final dose
Remain asymptomatic following the exposure
The guidance indicates that the timing associated with these requirements will be updated as additional information becomes available. Presumably, this will include extending the 3-month limit as new data are reported from clinical trials regarding the duration of immunity conferred by the vaccines. Notably, the CDC continues to emphasize that vaccination is not recommended as post-exposure prophylaxis and that eligible individuals with known exposure should wait until after the completion of their quarantine period to schedule their vaccination.
US VACCINE PRODUCTION Yesterday, US President Joe Biden announced that the US government finalized agreements to secure an additional 200 million doses of the Pfizer-BioNTech and Moderna vaccines, to be delivered by the end of July. He indicated that the total US procurement is now sufficient to fully vaccinate all Americans. At 300 million total doses, this should be enough to provide 2 doses to all US adults*. Dr. Anthony Fauci indicated that it could be “open season” for SARS-CoV-2 vaccination in America by April, with eligibility expanded beyond the initial high-priority groups.
*Currently, no SARS-CoV-2 vaccines are authorized for use in children.
While the federal government has procured enough doses, many barriers remain in terms of conducting nationwide mass vaccination operations. Distribution and logistics challenges continue to pose problems for state and local jurisdictions in terms of planning and scheduling, and many jurisdictions will likely face a shortage of the trained and qualified vaccinators that are critical to rapidly administering vaccinations to local populations. Additionally, it will be important to expand vaccination operations beyond those who will “readily seek” vaccination to ensure protection among those who may be hesitant or face barriers to accessing the vaccine. In addition to challenges to distributing and administering vaccinations domestically, many other countries have yet to access any doses, leaving most of the world vulnerable to COVID-19 as wealthier countries, principally in North America and Europe, scale up nationwide vaccination efforts. Without global protection through vaccination, COVID-19 will remain a threat everywhere.
COVID-19 DISPARITIES & EQUITY Research continues into the pandemic’s effects in exacerbating underlying and systemic disparities. The US national SARS-CoV-2 vaccination campaign is still in its early stages, but an investigation by STAT News already found that states with the largest gaps in wealth between counties are exhibiting similar gaps in vaccine coverage. For example, Connecticut has the largest disparity in median income at the country level of all US states. Early data indicate that vaccination coverage is 65% higher in the wealthiest counties than poorest.
COVID-19 has called attention to a broad scope of existing inequities in health and other sectors. One emerging issue that directly impacts COVID-19 patient care is the potential for pulse oximeters to be less accurate for patients of color. Pulse oximeters have emerged as an important tool in monitoring disease severity in COVID-19 patients, particularly those at risk of progressing from mild and moderate to severe disease. An editorial authored by several doctors at the University of Michigan, published in NEJM, presented a preliminary overview of data that shows significant disparities in the accuracy of pulse oximeters between Black and White patients. Based on data from nearly 50,000 blood oxygen saturation measurements, Black patients with pulse oximeter results in the normal range (92-96% oxygen saturation) were significantly more likely than White patients to have low oxygen saturation (<88%) when measured by arterial blood gas analysis. The study raised the attention of federal lawmakers, including several Senators who urged the US FDA to investigate racial and ethnic disparities in the accuracy of pulse oximeters and the requirements for testing their accuracy across a diverse set of study participants.
In an effort to combat inequities and disparities stemming from the pandemic, including in the vaccination plan, the White House announced the formation of a COVID-19 Health Equity Task Force. The task force will develop recommendations for addressing existing COVID-19 inequities and pathways to prevent such disproportionate impacts in the future. In addition to the task force’s 12 core members, leadership from 6 relevant federal government agencies will participate in and support the efforts: the Departments of Agriculture, Education, Health and Human Services, Housing and Urban Development, Justice, and Labor.
NORTHERN HEMISPHERE INFLUENZA SEASON Amid the COVID-19 pandemic, seasonal influenza rates are unusually low compared to historical data. Of the approximately 800,000 laboratory samples tested and reported to the US CDC since late September 2020, fewer than 1,500 were positive for seasonal influenza (0.2%). For comparison, that total was typically 25-30% at this point in the 2019-2020 influenza season. At this point in the season, there were nearly 100 times more cases last year than this year, even with approximately the same number of tests. Similar trends are also present for other respiratory viruses. Protective measures implemented for COVID-19, such as mask usage and social and physical distancing, may also be mitigating transmission risk for seasonal influenza. As we covered previously, the Southern Hemisphere also had a mild 2020 influenza season, which many believe was a direct result of COVID-19 risk mitigation measures.
GENOMIC SEQUENCING SURVEILLANCE The emergence of SARS-CoV-2 variants with the potential for increased transmissibility has provided the motivation necessary to rapidly scale up genomic sequencing capacity, in the US and elsewhere. Some members of the scientific community argue that existing capacity is available, at least in terms of having adequate hardware, technicians, and infrastructure; however, there is a lack of funding available to conduct this type of research, particularly on a scale needed to monitor the evolution of a national epidemic. In the global context, the US ranks #36 in terms of the proportion of specimens sequenced (0.36% of confirmed cases), compared to #1 Denmark, which has sequenced more than half.
In an article published in Science, the US CDC program officer responsible for the genomic surveillance efforts for emerging SARS-CoV-2 variants highlighted additional gaps in the system. Notably, linking samples and data from public health efforts to the sequencing technology is not necessarily a straightforward or direct process, and logistical solutions are necessary to enable the system to scale up the volume needed for COVID-19. The Biden Administration has called on the US Congress to authorize US$340 million dollars to support efforts to sequence 5% of all positive specimens. This number seems to be a middle ground, with some experts suggesting a loftier goal of 20%. Despite these efforts, there is still a sense that progress is moving too slowly. Mutation situation reports show that there are a number of notable SARS-CoV-2 variants of concern already circulating in the US, and public health and elected officials have a poor picture of the current prevalence of each of these variants. It is essential that the US and other countries develop better situational awareness of emerging variants, including the ability to rapidly detect those that emerge in the future.
MONOCLONAL ANTIBODY EUA On February 9, the US FDA issued an Emergency Use Authorization (EUA) for Eli Lilly’s monoclonal antibody cocktail of bamlanivimab and etesevimab as a treatment for COVID-19. The EUA specifically authorizes the treatment for “mild to moderate” COVID-19 in adults and pediatric patients aged 12 years and older who are “at high risk for progressing to severe” disease. Bamlaminivab was previously authorized for use under its own EUA. Under the new EUA, the two monoclonal antibodies are administered together in a single infusion, and the new EUA allows for infusion times as short as 16 minutes, which is less than a third of the time required for previous infusions. Like bamlanivimab by itself, the combination therapy can be administered as long as 10 days after symptom onset, but it is recommended to start treatment as soon as possible. The new EUA gives clinicians another outpatient option for treating individuals who are not ill enough to require hospitalization, which can reduce the burden on hospitals and health systems. According to a report from The New York Times, the FDA updated the EUA for bamlanivimab by itself to shorten its infusion time as well. The shortened infusion times are a result of feedback from clinicians, and the shorter time is expected to improve access and use of the treatments.
CARNIVAL & LUNAR NEW YEAR Major holidays and festivals around the world continue to face impacts from COVID-19 and associated protective measures. Carnival is an annual celebration that culminates with Fat Tuesday—the last day before Lent, observed by many Christian and Catholic denominations. It is a major festival in many locations around the world, perhaps most notably with the Carnival in Rio de Janeiro, Brazil, and Mardi Gras in New Orleans, Louisiana (US). This year, Fat Tuesday falls on February 16, but carnival celebrations have been scaled back considerably, including prohibitions on parades and mass gatherings in both Rio and New Orleans. In fact, the Sambadrome stadium in Rio is being utilized for mass vaccination operations this year instead of hosting some of Rio’s largest Carnival celebrations.
Today is the Lunar New Year, perhaps the most important holiday in China and celebrated in many other Asian nations. Last year’s Lunar New Year coincided with the earliest COVID-19 surge, which may have been driven, to some extent, by a high volume of international and regional travel associated with the holiday. Notably, many individuals who did travel last year found it difficult or impossible to return due to COVID-19 quarantines, “lockdowns,” and travel restrictions. This year, the Chinese government is encouraging individuals not to travel, reportedly including through “incentives” in the form of “gift baskets, activities and shopping discounts” to remain at home for the holiday. Despite the warnings, Chinese officials expect that hundreds of millions of people will travel over the course of the Lunar New Year season, which stretches to March. Those who do travel in China are required to provide documentation of a recent negative SARS-CoV-2 test, and some may face mandatory quarantine upon their arrival or return, depending on the destination.
TESTING TOOLKIT Researchers at the Johns Hopkins Center for Health Security, led by Dr. Gigi Gronvall, created the COVID-19 Testing Toolkit to provide information about SARS-CoV-2 test types, specific tests, and testing services, including how they work and what is known about their accuracy. SARS-CoV-2 testing has evolved rapidly over the course of the COVID-19 pandemic, as our understanding of SARS-CoV-2 improves and more tests enter the market. Testing is critical to identifying and monitoring the communities in which the virus is spreading as well as treating patients and informing good public health policies and operations during the pandemic. As more tests and test types become available, it is important to understand the purpose, capabilities, and limitations of these tests in order to select appropriate test types and test kits and accurately interpret the results. This toolkit provides a broad scope of information to support public health and healthcare decision-makers as well as the general public as they navigate an increasingly complex SARS-CoV-2 testing landscape.
dryrunguy wrote: ↑Fri Feb 12, 2021 7:50 pm
COVID-19 has called attention to a broad scope of existing inequities in health and other sectors. One emerging issue that directly impacts COVID-19 patient care is the potential for pulse oximeters to be less accurate for patients of color. Pulse oximeters have emerged as an important tool in monitoring disease severity in COVID-19 patients, particularly those at risk of progressing from mild and moderate to severe disease. An editorial authored by several doctors at the University of Michigan, published in NEJM, presented a preliminary overview of data that shows significant disparities in the accuracy of pulse oximeters between Black and White patients. Based on data from nearly 50,000 blood oxygen saturation measurements, Black patients with pulse oximeter results in the normal range (92-96% oxygen saturation) were significantly more likely than White patients to have low oxygen saturation (<88%) when measured by arterial blood gas analysis. The study raised the attention of federal lawmakers, including several Senators who urged the US FDA to investigate racial and ethnic disparities in the accuracy of pulse oximeters and the requirements for testing their accuracy across a diverse set of study participants.
WTH?!?
by Justme
JazzNU wrote:In the conversation of how Australia (and New Zealand) have been able to do so much better than other places. I'm not sure if anyone was listening to Darren Cahill the other night during I can't remember what match, but he was talking about how he had to quarantine to go back to Adelaide now that there were the cases in Melbourne.
Darren said that he had to stay home and apart from his family for that period of time. That he could go outside on his property, can't walk the dog up the street as long as he's alone, a question that Patrick asked about because it's something he did when he quarantined himself after testing positive. So if he's got no outdoor property, he's just SOL. And then he added, which I think is key, the police will come to check on him 3 to 5 times during his 14-day quarantine to make sure that he is staying home as he's supposed to. At least here in the US, the public resources aren't set up to handle checks like that for so many people. Could they have done this early on when case numbers were as low as they've been in Australia? Absolutely. And that may have been the thing that truly contained this here. But they aren't merely relying on people to "do the right thing" as has been suggested like Aussies are just so much more responsible than citizens of other countries. They might be somewhat more conscientious, but clearly it's not just that. They are enforcing the rules they put in place, and that is clearly making a big difference.
As an Australian I can quickly discuss my experiences.
Yes early on the government realised that they couldn’t rely on everyone to follow the rules. At the beginning of the pandemic, there were a lot of reports and instances where people were not quaranting after arriving back in Australia, I think it was up to 80% of people who were supposed to be quaranting were not at home or did not answer when the police checked on them. So all the states set up their own hotel quarantine programs. I would say the program has probably kept potentially many cases out of the community but we have had plenty of leaks as well.
They have definitely allocated a lot of police resources (and ADF) to quarantine programs and state checkpoints when borders have closed.
I would say general attitudes have also helped. There is a general feeling of everyone understanding the need to do their part and follow the rules to keep the numbers down and keep cases out of the community. I live in Melbourne and we had a strict 4 month lockdown during our second wave and it was interesting to see that people tended to monitor others and were willing to report them to the police if they thought they were breaking the rules.
by ponchi101 Somehow, the concept of American police checking whether people are really quarantining by knocking one people's homes brings some recent scenarios to mind, which did not end well.
Also. I am sure Australian police do not have to handle 15,000+ homicides a year.
by ti-amie
by JazzNU
'Unethical and unconscionable': Richer nations getting more COVID-19 vaccines than poorer
Megan Janetsky, USA TODAY
While images of people lined up for long-awaited COVID-19 vaccinations spurred hope in millions across the globe, they stirred up something else in Dr. Juan Jose Velez: frustration.
Velez runs the coronavirus ward in one of the biggest public hospitals in Colombia, a country with one of the highest death rates and coronavirus positivity rates in the world.
While more than 152 million COVID-19 vaccine doses have been administered globally, with roughly a third of those in the U.S., according to Bloomberg's vaccine tracker, Colombia is among a number of lower- to middle-income countries that still had not administered a single dose by mid-February.
“I think the greatest thing this has shown us is the lack of solidarity ... the fact that lots of countries have started vaccinating while many poorer countries haven't even started," Velez said.
This disparity is playing out across the world, and it’s one health experts have warned of since the onset of the pandemic: While richer countries rapidly vaccinate their populations and buy up doses, other nations are projected to not have wider access to the vaccine until late 2022 or 2023, according to the World Health Organization (WHO).
'On the brink of a catastrophic moral failure'
Though some efforts are being made to close that gap, WHO officials warn vaccine nationalism – where countries prioritize vaccination of their own citizens over the rest of the world – has put the world “on the brink of a catastrophic moral failure.”
In his hospital in Medellín, Colombia’s second-largest city, Velez said a refrigerator that would eventually carry COVID-19 vaccine vials had arrived, but it was still uncertain when he and other medical staff on the front lines would have access to their first shot. He said he lost count months ago of how many of his patients had died.
Dr. Salim Abdool Karim of South Africa was one of the first to warn of vaccine disparities.
When the pandemic began, he called for a “global public good.”
“The alternative is what we have now: which is countries scrambling, those with deep pockets going and outbidding others to get vaccines, and everyone is in a race to buy up vaccines,” said the infectious diseases epidemiologist, who has worked on HIV/AIDS and polio in Africa. “So middle-income countries, lower-income countries, they just fold their arms and say: 'What are we going to do? We don't have vaccines.'”
He told USA TODAY he’s concerned, but not shocked, at the inequality that has emerged.
President Joe Biden on Thursday announced a deal to purchase an additional 200 million coronavirus vaccine doses.
“We’ve now purchased enough vaccine supplies to vaccinate all Americans,” Biden said.
In addition to finalizing contracts with Pfizer and Moderna for 100 million more doses each that will be delivered by the end of July, Biden said 100 million other doses that were supposed to arrive in June will now be delivered in May.
“That’s a month faster,” Biden said. “That means lives will be saved.”
To fulfill his promise of administering 100 million vaccine shots in his first 100 days, Biden has taken steps both to increase production of vaccines and improve vaccination rates. Biden said Thursday that goal will be surpassed.
Despite high vaccination rates, disparities have also emerged within the U.S. People of color have suffered disproportionate rates of COVID-19 cases, hospitalizations and deaths as a result of longstanding systemic inequities and racism. A lack of data is further masking vaccination rollout transparency, health equity researchers say, and the data deficit is hurting those most vulnerable. So far, only 16 states are releasing vaccination counts by race and ethnicity, and the data is incomplete. Early findings show states that rank high on COVID-19 vulnerability indexes are falling behind on vaccinations.
In Britain, more than 12 million people have now had at least one dose of a coronavirus vaccine. Officials say they are on track to offer first doses to 15 million in the top-priority groups by Monday, and have set a target of vaccinating every adult in the country by the fall.
In Israel, vaccines were made available to all citizens over 16 last week.
It has delivered more than 3.5 million first doses of the Pfizer vaccine and at least 2.1 million second doses in a push to inoculate most of its population since late December. Tel Aviv also has started administering vaccines free of charge to the city’s foreign nationals, many of whom are undocumented asylum seekers.
While Israel's vaccination campaign has won praise internationally for its pace, WHO has also raised concerns that it does not include Palestinians in the occupied West Bank and the blockaded Gaza Strip.
In Africa, countries have counted lower rates of infections and COVID-19 deaths than South America – but the new variant that originated in South Africa has brought with it a worrying increase in infections.
“Vaccine hoarding will only prolong the ordeal and delay Africa's recovery,” Dr. Matshidiso Moeti, WHO regional director for Africa, said in a statement. “It is deeply unjust that the most vulnerable Africans are forced to wait for vaccines while lower-risk groups in rich countries are made safe.”
What about COVAX?
In April 2020, WHO launched the COVAX vaccination initiative with Gavi, the Vaccine Alliance, and the Coalition for Epidemic Preparedness Innovations, with a goal to distribute 2 billion doses before 2022. The aim is to ensure equitable distribution of vaccines to participating countries, regardless of income levels, and to distribute enough doses to allow countries to vaccinate 20% of their populations – largely health care workers and the elderly.
“That way, you avoid what in my view would be an unethical and unconscionable thing, which would be countries like the U.K. or the U.S. vaccinating low-risk young people (when) countries in Africa haven't even vaccinated their eldery,” Abdool Karim said.
“It would be completely unacceptable,” he said. Yet, he conceded, it’s probably going to happen. The world throwing its weight behind COVAX would be the best solution, he said.
Iran plans to import about 17 million doses of vaccine from COVAX and millions from other countries. But for now, it's using recently delivered Russian Sputnik V vaccines to inoculate health care professionals. Iranian media have reported that 2 million Russian vaccines will arrive in Iran in February and March.
Cambodia is set to get 7 million doses through the COVAX initiative. For now, China has donated 1 million doses of the Chinese-made Sinopharm vaccine, enough for half a million people, and the first shipment of 600,000 doses arrived in Cambodia on Feb. 7. Australia also announced a grant of $28 million to purchase 3 million doses.
WHO and global leaders have repeatedly urged richer countries to step up funding to COVAX to aid countries that have less capacity to buy doses. But those calls have been met with mixed success, said Dr. Felicia Knaul, a global health expert and economist.
Countries like Canada, which has done well to control the spread of the virus, has enough vaccines reserved to inoculate its population four times over. The United States, the United Kingdom, Australia, Chile, New Zealand and the European Union have also locked down more vaccines than their population counts. Yet Canada, New Zealand and Chile also elected to pull on COVAX for doses, as well, spurring criticism.
Global authorities said the move is a form of "double dipping" with vaccines – taking from a global aid scheme while also getting doses from private companies, which poorer nations may not be able to afford.
Canada’s international development minister defended the decision in an interview with CBC News in early February: “Our top priority is to ensure Canadians have access to vaccines. … Canada made the decision, as other countries have, to take on this first allocation, because we recognize how important it is that all Canadians have access to vaccines."
The European Union also recently came under fire when it announced export controls on vaccines produced in its territory, which could affect about 100 countries across the world.
“COVAX, ideally, could be enough. Let's put it this way: If all the world's governments stepped up to support COVAX ... it could be a strategy that could help to ensure equity in vaccine availability,” Knaul said. “There's going to be a lag in timing no matter what, but it could do an amazing amount to help poor countries get access more quickly and at better prices.”
Obstacles from infrastructure to mistrust
Lower- and middle-income countries also face greater challenges when vaccines do arrive.
Abdool Karim explained that many parts of Africa don’t have the medical infrastructure to distribute the shots.
Colombia is covered by large swaths of rurality and roadways that make it challenging to deliver basic medical services, let alone vials that require freezing temperatures.
While Colombia is considered a middle-income country and critics are fast to say a major cause of vaccination lags has also been government failure, it’s also one of the most unequal countries in the Western Hemisphere. Meanwhile, decades of conflict feeds an endemic distrust of government agencies that would have to distribute doses.
Clemencia Carabalí, a community leader in a remote nook of Cauca, Colombia, said she is “not that hopeful” vaccines will come.
“It’s always been difficult to access health services,” she said. “And for the vaccines to arrive to our land, that’s going to be really hard because of problems with intermediation and corruption. It’s possible that they’ll never arrive.”
Others, like Carlos Lopez, a director of a migrant shelter in Guatemala, said he has similar worries about migrant populations in the region because they often lack access to basic health services.
“The majority of migrants don't have any economic resources,” he said. “They're practically going to be the last to be taken into consideration.”
In such zones, Knaul said that ensuring citizens receive two doses will be challenging and that countries will need to play a balancing act in which vaccines they choose to distribute: weighing transportability, price, access, effectiveness and public trust.
In an encouraging sign for nations scrambling for the limited vaccine supply, a single shot of the AstraZeneca/Oxford University vaccine reduced transmission of the coronavirus by 67% and provided substantial protection against COVID-19 for at least three months, according to preliminary data from three trials unveiled earlier this month. Knaul and other experts said a single-dose vaccine could cut back significantly on logistical hurdles and concerns that many will get only half-vaccinated.
Johnson & Johnson also has developed a single-dose COVID vaccine.
'Until it is over for us all'
Despite worrying numbers, there have also been signs that point toward the gap closing.
Last week, UNICEF announced a deal with the Serum Institute of India that would create 1.1 billion doses of both the AstraZeneca and Novavax vaccines. The vaccines would cost $3 a dose and go to the poorest countries in the world.
UNICEF Executive Director Henrietta Fore said that the deal was just an initial agreement and that “more will follow.”
“For countries which have already initiated vaccination drives, and those yet to begin,” Fore said in a statement, “this information is a hopeful marker on the winding path out of a pandemic that will not be truly over, until it is over for us all.”
by ponchi101 Sorry but not sorry. This is our typical South American mentality. We invest almost zero in R&D, in all aspects. We decide to completely rely on the "developed" nations for our scientific and technical development, investing, again, nothing on those matters. And then, when it hits the fan, we play the "we are poor" card. Colombia not only is not able to produce a COVID vaccine; this country is unable to manufacture ANY vaccine because the government decided, almost a decade ago, to stop vaccine production in the country. It was "easier" to get all of the vaccines from the giant pharmaceutical companies abroad.
So now we expect the governments of the world to help us because "oh, we are poor". Sorry. Joe Biden is the president of the USA, not Colombia. Merkel has to look after Germany, Johnson after the UK. And it is not as if we are the only countries where the pandemic roams; it is worldwide.
This is typical:
“I think the greatest thing this has shown us is the lack of solidarity ... the fact that lots of countries have started vaccinating while many poorer countries haven't even started," Velez said.
Well, you want to start? Start developing scientific acumen within the country. Also, Pfizer ahs been talking about their vaccine for months now. The Colombian government secured NONE until very recently.
It is typical. We always play the victim's card. As if our internal running of our countries were the result of some developed nation's interference.
by Deuce Yes, richer countries also have more food, more shelter, and more of everything than poor countries do. That's nothing new - it's been this way forever.
It's the result of the human animal being inherently selfish. There are a few exceptions to this, of course - but not many among the rich.
There is more than enough money on this planet to feed, clothe, and house every person. The problem is, and always has been, that the money is very badly distributed.
And it's getting worse, not better. 'Famous' people - be they professional athletes, 'movie stars', musicians, etc. are being paid millions of dollars - far more than they could ever reasonably spend... while, at the same time on the same planet, their fellow human beings are starving to death because there is no money to feed them.
And the majority celebrate the rich and famous.
With these types of priorities, it is absolutely no surprise that the planet is a humanitarian mess.
by ponchi101 The numbers don't support that. I did not say that Colombia is a humanitarian mess. I was talking other issues.
The reality is that during the last 4 decades, the progress on all human areas have been verifiable. On average, as Pinker documents, over 100,000 people have been lifted from poverty every day during this stretch. Notice, for example, how we no longer hear of the famines that plagued Africa during the 70's and 80's.
My point is South America's refusal to accept responsibility in any case. But, with the exception of Venezuela and perhaps Argentina, all of South America is doing better than in the 70's. Only three clear cut dictatorships remain in the region (Cuba, Venezuela and perhaps Nicaragua).
But we still want the USA and the EU to solve a lot of our problems. That is what infuriates me.
by Deuce I was commenting on the post previous to yours, which stated that rich countries are getting more COVID-19 vaccines than are poor countries.
What I wrote stands. Completely.
When you've got people being given millions of dollars for throwing or catching a ball, or for pretending to be another person on TV, and you've got people starving to death on the same planet (and even in the same city in some cases), there is a humanitarian mess, and priorities are backwards.
by ponchi101 Colombia received their first vaccines yesterday. 50,000 doses, to go initially to front line workers. Next batch should be 125,000 next week.
Great hoopla and presidential speech to announce the whole thing.
BFD.
by ti-amie
10) If we let B117 spread further... it can acquire new further worse mutations that makes it evade immunity even more. Especially if exposed to immunocompromised people. Don’t let more mutations happen in Florida. Stop it now.
11) Fauci is warning about the new mutations too.
@GovRonDeSantis
- be a hero to America, not a Trump toady anymore. You don’t need him. Heed Fauci instead on this, if you don’t heed me.
12) Don’t let this be your legacy
@RonDeSantisFL
. Let it be that you’re a hero for stopping #B117. People will give you credit if you do,
@GovRonDeSantis
, I promise.
(...)
14) Some think I’m wasting my breath trying to convince
@GovRonDeSantis
. But fundamentally I hope
@RonDeSantisFL
can find it in his heart to care at least for his own political base of voters (elderly being infected), and his own political self interest that he might care.
15) When Germany Flag of Germany is concerned like this (with much less B117 than Florida), you know this is bad
@GovRonDeSantis
. Politically it is a no win situation if Florida is blamed for unleashing #B117 upon the state or rest of country.
by ponchi101 Is this ever going to end?
by ti-amie
ponchi101 wrote: ↑Tue Feb 16, 2021 7:24 pm
Is this ever going to end?
These are some of the tweets I didn't include.
Meanwhile in Florida...
by Suliso The new version is inevitable (about 20% in Switzerland already) so just need to vaccinate faster. Locking down even harder is not really feasible. Effects won't be as bad as the last wave because older people will already be protected by that time. Here government promises all at risk groups should be vaccinated with at least one shot by the end of the April and then it will be available to the general population. At that point kids who can't be vaccinated getting it is no big deal.
by skatingfan
ponchi101 wrote: ↑Tue Feb 16, 2021 7:24 pm
Is this ever going to end?
We have to remember that historically pandemics have lasted at least two years, and we're just about a year in, so it's entirely possible that we will be dealing with this for at least another year if not longer. The best hope we have is that the vaccine can knock down the virus spread enough that we can sort of resume normal life with some restrictions, like foreign travel.
by Suliso Some data about the current vaccination rates (top 10 and few notables). The data is for doses vs 100 inhabitants so full vaccination will be about 180 (2 doses, but minus children)
Israel 76.3 (30% population fully vaccinated)
Seychelles 56.9
UAE 51.4
UK 23.3
USA 15.8 (4% fully)
Bahrain 14.8
Serbia 14.0
Malta 11.7
Chile 11.2
Maldives 7.1
-----
Denmark 7.0
Poland 5.6
Switzerland 5.6
Spain 5.5
Italy 5.0
Germany 5.0
Sweden 4.5
Canada 3.3 (surprisingly lousy)
Argentina 1.4 ¨
Mexico 0.6
by dryrunguy The latest Situation Report. I read it very quickly. The new CDC guidance regarding schools is... confusing. But I thought the bit about vaccination success in tribal communities was a rare piece of good news.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 108.82 million cases and 2.40 million deaths as of 10:30am EST on February 16.
Both the global weekly incidence and mortality continue to decrease steadily. Weekly mortality has decreased by nearly half since the peak reported the week of January 4, 2020. The current weekly incidence is the lowest since mid-October 2020. Weekly mortality decreased for the second consecutive week, down nearly 25% from the high reported the week of January 25, 2021. At the regional level, only the Eastern Mediterranean Region is currently reporting increasing weekly incidence—up 7.5% compared to the previous week, following 3 consecutive weeks of decreasing incidence. Weekly mortality is decreasing in all WHO regions.
Our World in Data reports that 177.94 million vaccine doses have been administered globally, a 20% increase compared to this time last week. Vaccination efforts have been reported in at least 86 countries and territories.
UNITED STATES
NOTE: The US CDC did not update COVID-19 epidemiological or vaccination data yesterday due to the President’s Day holiday. The data below correspond to the most recent update on February 14.
The US CDC reported 27.42 million total cases and 482,536 deaths. Daily incidence in the US continues its steady decline, falling below 100,000 new cases per day for the first time since November 3, 2020.
On February 12, the US reported 5,520 new deaths. This is the second highest single-day total to date; however, the 3 highest single-day totals are the result of previously unreported deaths from a single state—New York (April 15, 2020), Indiana (February 4), and Ohio (February 12). As we covered previously, Ohio announced last week that it identified more than 4,000 previously unreported deaths, and it reported 721 deaths on February 11; 2,259 on February 12; and 1,204 on February 13.
The recent spikes in reported mortality make it difficult to get an accurate picture of the longer-term national trend. The mortality reported on February 11, however, could provide some insight. February 11 was the first day after the 7-day average window following February 4, and it was also the day prior to the largest report from Ohio. The average national daily mortality of 2,784 deaths per day on February 11 did include the first elevated report from Ohio, but it provides some indication that the true daily mortality is much lower than the current average of 3,136 deaths per day. This is the lowest daily mortality since January 6, prior to the estimated peak mortality in mid-to-late January, and it provides further evidence that daily mortality continues to decrease nationally.
US Vaccination
The US CDC reported 70.06 million vaccine doses distributed and 52.88 million doses administered nationwide (75.5%).
In total, 38.29 million people (approximately 11.6% of the entire US population) have received at least 1 dose of the vaccine, and 14.08 million (4.3%) have received both doses. The average daily doses administered continues to increase, now up to a record high of 1.50 million doses per day*. The number of people receiving their second dose is increasing at nearly 600,000 per day*. The breakdown of doses by manufacturer continues to shift toward the Moderna vaccine. The CDC is still reporting slightly more Pfizer-BioNTech doses administered (27.27 million; 52%) than Moderna (25.51 million; 48%), but the gap is closing.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 5.82 million doses have been administered at long-term care facilities (LTCFs)*, including residents and staff. This covers 4.16 million individuals with at least 1 dose and 1.64 million with 2 doses. Approximately 59% of the doses have gone to residents, and 41% to staff.
*The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
As the US SARS-CoV-2 vaccination effort continues, there remain substantial differences in terms of how efficiently states are administering their allotted doses. On a per capita basis, nationwide distribution remains relatively even. All by 9 states have received within 10%(+/-) of the median per capita doses distributed. Only Alaska has received more than 25% above the median, and no states have received less than 75% of the median. States vary widely, however, in terms of administration. By percent of doses administered, states range from 61.74% (Rhode Island) to 97.72% (West Virginia), with a median of 76.47%. In total, 36 states are within 10%(+/-) of the median in terms of percent of doses administered, a moderate decrease compared to the national distribution. Eight (8) states are reporting 60-70% of doses administered, 27 are reporting 70-80%, and 18 are reporting 80-90%. Three (3) states—New Mexico, North Dakota, and West Virginia—are reporting greater than 90%, which is more than 25% higher than the median. No states report less than 75% of the median.
States also vary widely in terms of how they are allocating doses between first and second vaccinations. In terms of the proportion of doses allocated for second vaccinations, states range from Delaware, with slightly more than one-fifth (21.35%), to West Virginia, the only state reporting more than one-third (35.92%). The median value is 27.33%. Approximately half of the states (26) are within 10%(+/-) of the median value. In total, 13 states are reporting 20-25%, 24 states are reporting 25-30%, and 12 states are reporting 30-35%. West Virginia is the only state reporting more than 35% and the only state reporting more than 25% higher than the median. No states are less than 75% of the median.
The Johns Hopkins Coronavirus Resource Center reported 27.71 million US cases and 486,572 deaths as of 12:30pm EST on February 16.
WHO VACCINE EMERGENCY USE LISTING The WHO issued Emergency Use Listings (EULs) for two versions of the AstraZeneca-Oxford University SARS-CoV-2 vaccine. The two versions are those produced directly by AstraZeneca-SKBio and those manufactured under the license to the Serum Institute in India. With the EUL in place, the AstraZeneca-Oxford vaccine can begin distribution through the COVAX facility, which will provide doses to low- and middle-income countries (LMICs) around the world, including nearly 340 million doses of the AstraZeneca-Oxford vaccine. The first COVAX distributions are expected later this month. Additionally, an EUL from the WHO can facilitate expedited regulatory authorization for the vaccine in many countries. This is the second EUL issued for a SARS-CoV-2 vaccine, following the Pfizer-BioNTech vaccine on December 31, 2020.
US SCHOOL GUIDANCE On February 12, the US CDC published updated guidance to support schools’ efforts to mitigate COVID-19 risk for in-person classes. The biggest update is a new “phased mitigation” strategy, which couples risk mitigation measures with the level of community transmission. The guidance emphasizes 5 key mitigation mechanisms—mask use, physical distancing, hand hygiene and respiratory etiquette, cleaning and sanitization, and surveillance and contact tracing—that are applicable across all levels of COVID-19 risk, but it also provides actionable information regarding how to implement those and other strategies at various levels of COVID-19 risk. The guidance also breaks down specific recommendations for elementary, middle, and high schools, and it includes guidance for extracurricular activities, including sports.
The updated guidance emphasizes that closing schools for in-person learning should be among the last measures taken to control local transmission. With that in mind, the guidance highlights some areas of flexibility in terms of the local community COVID-19 risk and what schools are capable of implementing. The guidance provides schools with recommendations regarding the minimum standards for conducting in-person classes for various levels of COVID-19 risk. For example, 6-foot physical distancing is recommended “to the greatest extent possible” for communities with low and moderate transmission; however, the CDC recommends mandatory 6-foot distancing for schools in substantial or high transmission areas. Schools that are unable to ensure the recommended physical distancing may need to reduce attendance and/or transition to hybrid or remote learning models, if community transmission is elevated. In addition to physical distancing, the guidance includes information on improving ventilation and implementing screening or testing programs for students and staff as well as additional risk mitigation measures if these programs cannot be implemented. Some view the guidance as a positive step toward supporting schools’ efforts to resume in-person learning, particularly the emphasis on closing schools as a last resort, whereas others argue that criteria for community transmission and testing are unrealistic and overly restrictive and that the guidance will ultimately keep schools closed longer.
Some aspects of the CDC’s previous school guidance remain in place, including the COVID-19 Mitigation Toolkit, Get Ready for In-Person Learning, Setting Up Your Classroom, and Teacher and Staff Checklists—all of which were published or updated in December 2020. The CDC also updated its Operating Schools During COVID-19 guidance on February 11, but there are no changes listed since December 31, 2020.
EMERGING VARIANTS Researchers from Switzerland and the US published (preprint) findings from a study of the emergence of new SARS-CoV-2 variants that include a specific mutation in the spike protein. Mutations at amino acid 677 affect the virus’ spike protein, which could potentially factor into the virus’ transmissibility or its susceptibility (or resistance) to antibodies, including those generated through vaccination. The researchers identified at least 7 distinct sub-lineages in the US that contain this mutation, all of which appear to have emerged in the US (ie, as opposed to imported from another country). These sub-lineages first appear in specimens sequenced at least as far back as August 2020, but it is unclear exactly when they first emerged. These sub-lineages already account for a substantial proportion of the documented SARS-CoV-2 genomes nationwide, but further research is needed to better characterize the effects of these mutations on transmissibility. Increased sequencing capacity is needed to improve surveillance for these and other emerging variants.
Researchers from the Johns Hopkins Center for Health Security—led by Dr. Caitlin Rivers and Lane Warmbrod and in collaboration with Dr. Matthew Frieman (University of Maryland) and Dr. Dylan George (In-Q-Tel)—published a report outlining recommendations to improve the United States’ ability to identify, monitor, and characterize emerging SARS-CoV-2 variants. Their principal recommendations address various aspects of containing and monitoring these variants. First, implementing policies to slow transmission can mitigate the risk of new variants emerging in the first place. In order to effectively monitor for the emergence of new variants, the US needs a national strategy for genomic surveillance, including resources necessary to implement it. At the local level, infections identified with variants of concern should be prioritized for contact tracing and other follow-up in order to effectively gather data regarding the variants’ performance compared to existing strains. And finally, coordination and resources are necessary to implement effective and efficient efforts to characterize the effects of specific mutations and the capabilities of emerging variants, including with respect to transmissibility, disease severity, and susceptibility to vaccines and therapeutics.
US TESTING CAPACITY A survey conducted by STAT News and The Harris Poll (February 5-7) indicates that SARS-CoV-2 testing capacity in the US is still not meeting demand. Among those who sought testing, 44% reported being unable to get tested*. Common complaints from the respondents who were unable to get tested included long wait times, distance to a testing site or lack of transportation, and uncertainty regarding where to get tested. Among those who had been tested at least once, the majority of testing (56%) occurred at drive-through or hospital-based testing sites, and most (69%) used nasopharyngeal swabs. The Biden Administration has acknowledged the ongoing nationwide shortage of test kits, and it is negotiating with the Congress to secure funding to purchase additional tests. Current plans include purchasing 8.5 million at-home rapid tests and scaling up production of the at-home kits to more than 60 million by this summer. At-home testing could potentially alleviate barriers due to test site location, transportation, and wait times by eliminating the need to find and travel to a testing site.
*31% sought testing and were able to be tested, 24% sought testing and could not get tested, and 45% did not seek testing.
An investigation conducted by The Wall Street Journal found that “at least 32 million of 142 million” rapid antigen tests distributed by the federal government to states remain unused. These tests were intended to support larger-scale screening efforts, including at schools and long-term care facilities, but logistical challenges for facilities implementing testing programs and reporting results has limited demand. The rapid tests were viewed by some as an important tool to ongoing screening programs that could be used to resume some activities (eg, in-person learning) and respond to outbreaks, but the low use is problematic. Many of the tests have a shelf life of 6 months, and millions of test kits delivered in autumn 2020 are approaching their expiration date.
US VACCINATION As US states continue to expand vaccination eligibility to larger portions of their populations and scale up vaccination capacity, some are limited by the available supply. As we noted in the Epi Update section above, at least half of all US states have administered more than 75% of the vaccine doses they have received from the federal government. Much of the remaining inventory at the state level is reserved for second doses. Some states have been forced to shut down various aspects of their vaccination programs, including large mass vaccination sites like Dodger Stadium in Los Angeles, California. Numerous local jurisdictions in the Atlanta, Georgia, area have also stopped scheduling new vaccination appointments due to insufficient supply. US President Joe Biden announced plans to bolster vaccine supply on February 2, but the increase to 10.5 million doses per week does not provide an increase over the current average of 1.5 million doses administered per day.
In addition to supply limitations, a massive winter storm that swept across much of the US is hindering vaccination efforts in many states. Shipments of doses to some areas have been delayed, and clinics and mass vaccination sites have closed in multiple states. In Texas, large-scale electrical outages have caused vaccine freezers to lose power, and health officials scrambling to administer doses of the vaccine before they go bad.
US TRIBAL VACCINATION Tribal nations in the US have been among the hardest hit by COVID-19 due to a variety of factors, including underlying health conditions, poverty, and limited access to healthcare services. Despite these challenges, evidence is emerging that many tribal nations are vaccinating their populations more efficiently than many other US communities. Among these success stories are the Cherokee and Navajo Nations, which are both reporting high rates of vaccination and high levels of interest in getting vaccinated. Notably, Navajo Nation reported that 47.7% of the population residing on tribal lands has received at least one dose of the vaccine. Both Nations credit culturally appropriate outreach and education efforts in the community as critical to the success of their vaccination efforts.
The ability of tribal nations to decide their own vaccination priorities also contributed to building greater confidence in the vaccine. For example, the Cherokee Nation chose to include their highly revered Cherokee language speakers and Cherokee National Treasures among its first priority groups. The decision signaled that tribal leaders were prioritizing Cherokee culture, and vaccinating respected tribal elders demonstrated to others that the vaccine is safe. The Navajo Nation is engaging in community outreach through a variety of fora, including radio broadcasts and frequent town halls, conducted both in English and the Navajo language. The apparent success of these efforts, exhibited by the high vaccine uptake and willingness to be vaccinated, underscore the importance of culturally relevant messaging and education in promoting SARS-CoV-2 vaccination.
MODERNA VACCINE DOSES The US FDA is reportedly considering allowing Moderna to increase the number of doses included in each vial of its SARS-CoV-2 vaccine. Moderna has been consulting with FDA officials to determine if it can increase the doses in each vial from 10 to 14 or 15. Moderna still needs to provide data to the FDA demonstrating that the increase in doses per vial would not compromise vaccine quality; however, increasing vial capacity by 40-50% could potentially increase the country’s overall COVID-19 vaccine supply by 20%. The associated modifications to Moderna’s production lines could be completed as early April. Filling and labeling the individual vials remains a major bottleneck in the vaccine manufacturing process, so increasing the volume of vaccine in each vial would substantially increase supply without adding time to the overall time to finish each vial. A substantial increase to the vaccine supply could have a major impact on vaccination operations, both in the US and around the world.
MASK EFFICACY A commentary published in JAMA by Dr. John T. Brooks and Dr. Jay C. Butler, two experts at the US CDC, provides an overview of the evidence supporting the use of facemasks during the COVID-19 pandemic. The researchers evaluate the existing body of evidence in support of universal masking, including results from contact tracing investigations, large surveys, and ecological studies that evaluate the effect of masking policies on COVID-19 incidence, including several that compare COVID-19 incidence before and after implementing a mask mandate. The authors draw a parallel between universal mask use and herd immunity, noting that increased mask use in a given community can increase the level of protection against SARS-CoV-2 transmission. Additionally, they argue that the specific type of mask used could be less important than the act of wearing the mask.
ISRAEL Israel continues to lead the world in terms of SARS-CoV-2 vaccination. Israeli Minister of Health Yuli Edelstein announced that 2.61 million individuals have received both doses of the vaccine, approximately 30% of Israel’s total population. With such a substantial portion of its population already vaccinated, Israel is among the first countries to begin evaluating the effect of vaccination on its COVID-19 epidemic. Israel’s largest healthcare provider—Health Maintenance Organization (HMO) Clalit, which covers more than half of Israel’s population—reported a 94% decrease in symptomatic COVID-19 cases among 600,000 individuals who received 2 doses of the Pfizer-BioNTech vaccine, compared to those who have not yet been vaccinated.
Despite its success, Israel still faces many challenges in terms of vaccine hesitancy. Like many countries, misinformation remains a major challenges during Israel’s COVID-19 epidemic, particularly with respect to SARS-CoV-2 vaccination. To combat misinformation, Israel’s Ministry of Health established a taskforce to find and remove misinformation on a wide range of social media sources, including in multiple languages. In further efforts to promote vaccination, Israel is reportedly considering measures to prohibit unvaccinated individuals from some public spaces, including museums or concerts. Israel is also implementing more creative measures to incentivize vaccination. At some mass vaccination centers, DJs play music in order to attract attention and draw in younger adults. Social media influencers have also been approached by the government to promote vaccination and disseminate information on the ongoing vaccination campaign.
NEW ZEALAND LOCKDOWN A cluster of COVID-19 cases in Auckland, New Zealand, has prompted new national “lockdown” measures. On February 14, the New Zealand Ministry of Health reported 3 cases in the same household. Case investigation efforts determined that several of the newly identified cases traveled to a nearby tourist attraction during the period when they could have been infectious, but it is not clear whether any of them were infectious at that time. All members of the household have been placed into isolation/quarantine. Genomic analysis from the cases indicates that the 3 individuals are infected with the B.1.1.7 variant of concern, but the analysis was unable to link the cases to any other known chains of transmission. To date, 109 close contacts have been identified and tested, and no additional cases have been linked to the cluster. The investigation is ongoing to identify the source of exposure.
Following the announcement, New Zealand implemented a Level 3 lockdown in Auckland and moved the rest of the country to Level 2 for a period of 72 hours to allow health officials time to investigate the cluster and assess the risk. The lockdown is currently scheduled to end at midnight on February 17. New Zealand health officials determined that several major events, including the America’s Cup (sailing) and the Big Gay Out festival could continue as scheduled, as long as event organizers implemented appropriate protective measures. The Big Gay Out festival reportedly did proceed as planned, but the America’s Cup postponed races scheduled for February 17 as a precaution.
by Suliso Perhaps we should revive the Science thread, but since it's about vaccines here will be good too. From time to time you hear folks, including some journalists, saying "why don't they just produce those mRNA vaccines faster, involve dozens of other companies, use defense production act etc." and so on. As I have a background in chemical R&D and manufacturing myself (nothing to do with vaccines) I was already pretty sure that those folks have no idea what they are talking about due to lack of any technical education.
Here are some very useful links explaining the process and why despite all the effort it's only as fast as it is and in fact is amazingly fast. I'm not copying it because then links and pictures are lost
Just to summarize mRNA vaccines are at the very pinnacle of capabilities of our biopharma industries, their equivalent of nanoscale chipmaking in terms of complexity of manufacturing and supply chain. Note that the entire supply chain and expertise is exclusively Western (not counting vials, syringes, gloves etc). That alone indicates how new all this is.
by ponchi101 Thanks Suliso. Very useful to understand the scope of the issue.
BTW: The Techno Babble thread is renamed SCIENCE and TECHNOBABBLE. No need to have two of those, as they are not terribly busy. Of course, feel free to post anything you want.
by Suliso
ponchi101 wrote: ↑Tue Feb 16, 2021 11:27 pm
BTW: The Techno Babble thread is renamed SCIENCE and TECHNOBABBLE. No need to have two of those, as they are not terribly busy. Of course, feel free to post anything you want.
Thanks, you're right. Didn't remember that thread, albeit in this case maybe more of us will find it here.
by Suliso I would also like to touch on a subject why exactly such high tech companies and production is currently found only in North America/Western Europe (could have been Japan as well, but they've abandoned this particular area). One reason is rather obvious - top level universities and highly qualified, well paid workforce. However, that's not the entirety of the picture and maybe not even the main part. It has to do with a long term funding by a venture capital. Look at the main two inventors (BioNTech and Moderna), both have existed for 10+ years, have spent billions of dollars AND have never had a product on the market. Even though there are rich people in SA or India too who could theoretically fund such an endeavor in practice they're more into quick profit as opposed to very risky long term bets.
by ti-amie I always said Andrew is not what he seems. For the most part he did well handling C19 in New York (he's no DeSantis) but this is no surprise.
dryrunguy wrote: ↑Fri Feb 12, 2021 7:50 pm
COVID-19 has called attention to a broad scope of existing inequities in health and other sectors. One emerging issue that directly impacts COVID-19 patient care is the potential for pulse oximeters to be less accurate for patients of color. Pulse oximeters have emerged as an important tool in monitoring disease severity in COVID-19 patients, particularly those at risk of progressing from mild and moderate to severe disease. An editorial authored by several doctors at the University of Michigan, published in NEJM, presented a preliminary overview of data that shows significant disparities in the accuracy of pulse oximeters between Black and White patients. Based on data from nearly 50,000 blood oxygen saturation measurements, Black patients with pulse oximeter results in the normal range (92-96% oxygen saturation) were significantly more likely than White patients to have low oxygen saturation (<88%) when measured by arterial blood gas analysis. The study raised the attention of federal lawmakers, including several Senators who urged the US FDA to investigate racial and ethnic disparities in the accuracy of pulse oximeters and the requirements for testing their accuracy across a diverse set of study participants.
WTH?!?
Like almost everything else in general medicine, these were developed for white men...
by mmmm8
ti-amie wrote: ↑Wed Feb 17, 2021 7:18 pm
I always said Andrew is not what he seems. For the most part he did well handling C19 in New York (he's no DeSantis) but this is no surprise.
I was wondering what will come out to bring his reputation down (not whether anything will come out). Can't do NY politics without a scandal!
by dryrunguy According to the CDC, life expectancy in the United States dropped by a full year during the first 6 months of 2020.
dryrunguy wrote: ↑Thu Feb 18, 2021 7:41 pm
According to the CDC, life expectancy in the United States dropped by a full year during the first 6 months of 2020.
by Suliso I guess I don't understand how exactly that number is calculated. Only ca 0.05% of US population died of covid during that time period. How can it have substracted an entire year?
by ponchi101 The only idea that comes to mind: the virus has indeed killed around 0.05% of the US population. But it killed disproportionately a large number of elderly. So, the number of elderly people alive by the end of 2020 was the cohort that was more affected by the virus. Since there are fewer elders, your life "expectancy" is now slightly less.
You mentioned this tangentially in one of your posts. In the next couple of years, the US (and maybe the whole world) will see fewer elder deaths because the deaths took place in 2020. So this life expectancy may rebound very quickly.
One idea.
Also. Reading the report tells you that these data are based on deaths for the first six months of 2020. Since most deaths took place in the second half, expect a further drop.
ti-amie wrote: ↑Wed Feb 17, 2021 7:18 pm
I always said Andrew is not what he seems. For the most part he did well handling C19 in New York (he's no DeSantis) but this is no surprise.
I was wondering what will come out to bring his reputation down (not whether anything will come out). Can't do NY politics without a scandal!
His long-winded Covid updates, while appreciated at the time, seemed like someone who was full of himself.
by dryrunguy
Suliso wrote: ↑Thu Feb 18, 2021 7:52 pm
I guess I don't understand how exactly that number is calculated. Only ca 0.05% of US population died of covid during that time period. How can it have substracted an entire year?
I would bet much of the decrease can be attributed to large numbers of deaths among middle-aged and "younger elderly" people of color (i.e., people advanced in years yet below the previous age for life expectancy). This age group was especially hard hit by COVID early on in the epidemic. Remember the early outbreak in New York City, Philadelphia, and some other urban centers? Large-scale deaths among people of color in their 40s, 50s, or 60s would bring down national life expectancy pretty quickly.
But that's just my theory based on early demographics of the pandemic.
by skatingfan
Suliso wrote: ↑Thu Feb 18, 2021 7:52 pm
I guess I don't understand how exactly that number is calculated. Only ca 0.05% of US population died of covid during that time period. How can it have substracted an entire year?
It's just an average of the age of people when they die - there was a significant increase in the number of deaths in that period (something like 15%) compared to previous years. Also, there was a significant increase in drug overdose deaths in that period as well, and those people tend be much younger than the average age of death, and so have a significantly higher impact on the average life expectancy.
Suliso wrote: ↑Thu Feb 18, 2021 7:52 pm
I guess I don't understand how exactly that number is calculated. Only ca 0.05% of US population died of covid during that time period. How can it have substracted an entire year?
It's just an average of the age of people when they die - there was a significant increase in the number of deaths in that period (something like 15%) compared to previous years. Also, there was a significant increase in drug overdose deaths in that period as well, and those people tend be much younger than the average age of death, and so have a significantly higher impact on the average life expectancy.
Because of COVID, we have completely lost track of the opioid/prescription drug overdose epidemic. Excellent point.
by Suliso We in Switzerland have gone under 1,000 covid patients in hospitals for the first time since mid November (peak of ca 3,800).
by ponchi101 Good news, Suliso. Good to hear (there are few of those).
---0---
Now that the vaccine is rolling out, and that some good news are coming (it seems the Pfizer vaccine is very good with only one dose), what are the plans for the recovery? By that I mean, when can we start behaving in more normal ways in order for the economies of the world to re-start?
Do we wear masks for at least one more year? (I don't see why not)
Do the Big Pharma companies already begin plans for future vaccines, as the original virus has mutated so much?
What will be the plans for international travel? What about that vaccine passport (I don't see a reason for not having it, in the same way that most of us travel with our yellow fever vaccination certificate)
When do the countries of the world get together to plan an early warning and detection system?
How deep must the investigation of the origins of the virus must be? Do we trust the Chinese GOVERNMENT with such a delicate issue?
How can we minimize this happening again?
by Suliso I think nothing big will happen before June. Here we plan to open nonessential shops and museums March 1st, restaurants outdoors and gyms from April 1st. For both if conditions don't worsen. Schools for younger children and hairdressers stayed open in Switzerland during wave two.
by dryrunguy The latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 109.59 million cases and 2.42 million deaths as of 10:00am EST on February 19.
As countries continue to scale up vaccination efforts, many are beginning to report data for both partially and fully vaccinated individuals. As we have covered previously, Israel is leading the world in terms of SARS-CoV-2 vaccination, with 48.8% of its population receiving at least 1 dose of the vaccine. Seychelles is #2, with 42.6%, followed by the UK countries—Wales (26.1%), Scotland (24.8%), England (24.6%), and Northern Ireland (22.6%). Bahrain (15.5%), the US (12.3%), and Chile (12.1%) are the only other countries reporting higher than 10% coverage with at least 1 dose. In total, 50 total countries are reporting 1-dose coverage greater than 1%. Of those countries that have commenced vaccinations, 51 are reporting the number of individuals who have been fully vaccinated, mostly in Europe and North America. Israel (33.0%) and Seychelles (19.8%) lead all countries in terms of the proportion of their populations with full coverage, and no other countries are reporting higher than 5%. The US (4.8%), Malta (4.2%), and Denmark (3.0%) round out the top 5. In total, 35 countries have reported full vaccination in more than 1% of their total population.
There are major differences in how countries are allocating their available supply to first and second doses, evident in the differences between partial and full vaccination coverage. Some countries are aggressively pursuing second doses for individuals who have already received their first dose, while others are focusing on broader coverage using the first dose. For example, Costa Rica (78.5%), Croatia (78.2%), Russia (76.8%), and Spain (70.0%) are all reporting full vaccination for 70% or more of individuals who received their first dose. In contrast, fewer than 10% of those who have received the first dose are fully vaccinated in the UK—England (3.6%), Northern Ireland (7.0%), Scotland (1.8%), and Wales (2.3%); Singapore (2.3%); and Chile (2.4%). While the UK and Chile have among the highest 1-dose coverage, they are among the lowest in terms of full vaccination coverage.
*These data address “fully vaccinated” from the perspective of the number of doses administered and not with respect to the time required after the last dose to develop the full immune response.
Our World in Data reports that 194.44 million vaccine doses have been administered globally, a 21% increase compared to this time last week. Vaccination efforts have been reported in at least 92 countries and territories.
UNITED STATES
The US CDC reports 27.67 million total cases and 489,067 deaths. Daily incidence in the US continues its steady decline, now down to 77,385 new cases per day—the lowest daily average since October 28, 2020. The daily mortality is currently 2,708 deaths per day, the lowest average since January 6, 2021; however, reporting irregularities due to previously unreported deaths and holiday delays are making it difficult to project the longer-term trajectory. While the actual 7-day average daily mortality is uncertain, we expect the US to surpass 500,000 cumulative deaths in the next several days.
US Vaccination
The US CDC reported 73.38 million vaccine doses distributed and 57.74 million doses administered nationwide (78.7%).
In total, 41.02 million people (approximately 12.4% of the entire US population) have received at least 1 dose of the vaccine, and 16.16 million (4.9%) have received both doses. The average daily doses administered continues to increase, now up to a record high of 1.54 million doses per day*, including 679,199 second doses per day*. The CDC is still reporting slightly more Pfizer-BioNTech doses administered (29.59 million; 51%) than Moderna (28.04 million; 49%), but the gap is closing.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 6.18 million doses have been administered at long-term care facilities (LTCFs)**, including residents and staff. This covers 4.31 million individuals with at least 1 dose and 1.84 million with 2 doses. Approximately 59% of the doses have gone to residents, and 41% to staff.
**The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 27.91 million US cases and 493,670 deaths as of 12:30pm EST on February 19.
VACCINE CLINICAL TRIALS The UK has approved plans for the world’s first SARS-CoV-2 human challenge trial, backed by £33.6 million (US$47 million) in government funding. The UK COVID Challenge trial is expected to begin sometime in the next month, pending final ethics review. It will include up to 90 healthy volunteers, aged 18-30 years old, who will be deliberately exposed to SARS-CoV-2 and monitored under controlled conditions. The first stage of the trial will aim to characterize “the smallest amount of virus needed to cause infection,” and future efforts will include patients who are vaccinated prior to exposure to assess vaccine efficacy. The trial will be a partnership between the UK government’s Vaccine Task Force, Imperial College London, the Royal Free London NHS Trust Foundation, and hVIVO, a company with experience in human viral challenge trials.
The University of Oxford announced that it will conduct a clinical trial for the AstraZeneca-Oxford vaccine in children. The Phase 2 clinical trial will take place across 3 study sites in England and include 300 participants aged 6-17 years. The placebo-controlled trial will administer the vaccine to as many as 240 participants, and the control group will receive a meningitis vaccine in order to stimulate a similar reaction (e.g., injection site soreness). Another team of researchers is also conducting a Phase 2/3 clinical trial for the Moderna vaccine. The Moderna trial aims to enroll 3,000 participants, and it will use a saline injection as its placebo. Now that several SARS-CoV-2 vaccines have demonstrated safety and efficacy in adults, children are an important population to evaluate in these next stages of clinical trials.
Researchers are also initiating clinical trials in other special populations, such as pregnant women. On February 18, Pfizer and BioNTech announced that the first participants were vaccinated in a “global Phase 2/3" clinical trial to evaluate the safety and efficacy of their SARS-CoV-2 vaccine in pregnant women. The study aims to include 4,000 participants (aged 18 years and older), and the vaccine will be administered between 24 and 34 weeks of gestation.
US VACCINE SUPPLY Following announcements from multiple US states that demand is outpacing federal supply of SARS-CoV-2 vaccine doses, the White House announced another increase in weekly distributions. The federal government will provide 13.5 million doses to state governments per week and 2 million weekly doses directly to pharmacies, compared to previous shipments of 10 million and 2 million doses per week, respectively. This brings the total national distribution to 15.5 million doses per week, which would enable 2.2 million doses to be administered per day nationwide. This corresponds to an increase of nearly 50% over the current average of 1.5 million doses administered per day.
HONG KONG AUTHORIZES SINOVAC VACCINE On February 18, the Hong Kong Secretary for Food and Health authorized the Sinovac SARS-CoV-2 vaccine for emergency use. The announcement followed recommendations from Hong Kong’s Advisory Panel on COVID-19 Vaccines. Reportedly, the efficacy data used in Hong Kong’s regulatory review showed 62% efficacy, which is higher than some other recent clinical results for the vaccine but lower than other vaccines authorized in other countries. The data have not been published, and some scientists have called on Sinovac to publicly release the clinical trial data. While Sinovac shared data with the advisory panel, critics argue that this does not meet the rigorous standard of a public peer review. Notably, a recent study conducted by Hong Kong University found that fewer than 30% of respondents would get vaccinated using the Sinovac vaccine due, in part, to concerns about its efficacy.
Hong Kong’s current agreement would supply 1 million doses of the vaccine to later this week, and vaccination is expected to start on February 26. Hong Kong established 5 priority groups for the earliest eligibility: (1) healthcare workers and “staff involved in anti-epidemic work,” (2) adults aged 60 years and older, (3) residents and staff at long-term care facilities, (4) essential workers, and (5) border control and workers at points of entry.
GLOBAL VACCINE ALLOCATION At least 92 countries and territories around the world have commenced SARS-CoV-2 vaccination campaigns. Several sizable gaps remain in vaccine access, most notably in Africa. In total, only 5 countries in Africa have reported vaccinations to date: Algeria, Egypt, Mauritius, Morocco, and Seychelles. In total African countries have reported 2.3 million cumulative vaccinations, the vast majority of which (97%) are in Morocco. Additionally, several African countries recently announced the delivery of their first vaccine doses or the start of vaccination campaigns. South Africa previously suspended its national vaccination program for the AstraZeneca-Oxford vaccine due to concerns regarding that vaccine’s efficacy against the B.1.351 variant, which was first identified in South Africa; however, it commenced vaccinations on February 17 using the Johnson & Johnson (J&J)-Janssen vaccine. Zimbabwe also commenced vaccinations this week, using Sinopharm vaccines from China. Sinopharm has also supplied doses to Egypt and Equatorial Guinea. Rwanda commenced its vaccination efforts as well, focusing initially on high-risk populations such as frontline healthcare workers. The Rwandan Ministry of Health announced the program on February 14.
In response to global disparities in SARS-CoV-2 vaccine access, particularly with respect to countries’ wealth, Mexican Minister of Foreign Affairs Marcelo Ebrard’s statement to the UN Security Council called for the “international community to guarantee fair, equitable and timely access” to the vaccine. Minister Ebrard’s statement noted that 10 countries have received 75% of the global vaccine supply and that more than 100 countries have not yet administered a single vaccination. Mexico has reportedly purchased 230 million doses of SARS-CoV-2 vaccines, across multiple manufacturers; however, its allotments have been limited relative to wealthier countries like China, the US, the UK, and many European countries. To date, Mexico has reported only 1.32 million doses administered, although more than 500,000 of those (43%) have been reported in the past 3 days. On a per capita basis, Mexico has administered only 1 dose per 100 people, compared to 17.4 in the US, 6.35 across Europe, and 2.8 in China.
As we reported previously, the COVAX facility published its anticipated vaccine allotments, which includes more than 88 million doses for 46 African countries and nearly 6.5 million doses for Mexico. The Emergency Use Listings recently issued by the WHO for the AstraZeneca-Oxford vaccine cover more than 99% of the 320 million doses in the first COVAX allotment and move COVAX one step closer to shipping the first doses.
EU VACCINE SUPPLY As supply continues to be a bottleneck in SARS-CoV-2 vaccination efforts, Pfizer and BioNTech are reportedly behind schedule in delivering vaccine to the EU, including approximately 10 million doses that were supposed to arrive in December. The missing Pfizer doses represent one-third of the anticipated supply, exacerbating the impact of delays in delivering the AstraZeneca-Oxford and Moderna vaccines. As a result of ongoing concerns regarding the availability of the AstraZeneca-Oxford vaccine, the European Commission reportedly finalized new contracts to purchase an additional 350 additional doses of the Pfizer-BioNTech and Moderna vaccines, scheduled to be delivered through the end of 2021. Recent agreements, including the February contract with Pfizer/BioNTech, include “anti-variant” clauses that would allow the bloc not to purchase vaccines that are not effective against emerging variants, and the EC reportedly hopes to add similar clauses to existing contracts. Additionally, the EU is funding almost US$300 million for efforts to combat variants, including at least €75 million (US$91 million) for expanded genomic sequencing capacity and the development of specialized tests for emerging variants and €150 million (US$182 million) for research and data sharing.
EMERGING VARIANTS A study published (preprint) by Harvard University examines the nasopharyngeal viral concentration in individuals infected with the B.1.1.7 SARS-CoV-2 variant. The researchers performed a series of PCR-based diagnostic tests over a series of weeks to evaluate temporal dynamics of the viral concentration for this variant of concern. The study included 65 total participants, including 7 infected with the B.1.1.7 variant. The researchers found that infection with the B.1.1.7 variant lasted significantly longer than for other variants, with a mean duration of infection of 13.3 days for the B.1.1.7 variant, compared to 8.2 days for non-B.1.1.7 variants. While the duration of infection was longer for the B.1.1.7 variant, the peak viral concentration was similar between B.1.1.7 and non-B.1.1.7 variants.
Even though the peak nasopharyngeal viral concentration is similar between the B.1.1.7 and non-B.1.1.7 variants, the longer duration of infection could potentially be a factor in the variant’s increased transmissibility. If individuals infected with the B.1.1.7 variant take longer to clear the virus from their system, their infectious period could potentially be longer as well, which could result in additional exposures compared to non-B.1.1.7 variants. Further investigation is necessary to better characterize the drivers of the increased transmissibility, but this study provides insight into potential mechanisms that contribute to the variant’s ability to spread more rapidly in the community.
US MORTALITY The US CDC published findings from analysis of US mortality data from January-June 2020, which indicates that the average life expectancy in the US decreased by 1 year compared to estimates from 2019. The analysis was conducted by the CDC’s National Center for Health Statistics, and the researchers evaluated all reported deaths from the first half of 2020*. The researchers estimate the overall life expectancy in the US for the first half of 2020 to be 77.8 years, a decrease from 78.8 years in 2019 and the lowest estimate since 2006. This is the largest single-year decline since World War II. The decrease was slightly greater in males than females—1.2 years compared to 0.9 years. The analysis also evaluated changes in life expectancy by racial and ethnic groups, a major concern due to the disproportionate burden of COVID-19 on racial and ethnic minorities. Life expectancy decreased by 0.8 years for the non-Hispanic White population, 1.9 years for the Hispanic population, and 2.7 years for the non-Hispanic Black population, illustrating “a worsening of racial and ethnic mortality disparities.”
Notably, these reported deaths include the initial COVID-19 surge, but they do not cover the autumn/winter 2020-21 surge, which exhibited a higher and more sustained mortality rate—exceeding 2,000 deaths per day since early December 2020 and 3,000 deaths per day from mid-January through mid-February 2021. One of the researchers indicated that the “majority of the decline” stemmed from the pandemic.
*The report indicates that the analysis is based on preliminary data and that some reports could be delayed by months.
JAPAN VACCINATION On February 17, Japan commenced its SARS-CoV-2 vaccination campaign, focusing initially on healthcare workers and older adults. Japan faced its largest surge in December 2020 and January 2021, but it delayed the start of its vaccination campaign after requiring domestic clinical trials of the Pfizer-BioNTech vaccine. Pfizer and BioNTech applied for emergency approval in Japan in December, but reportedly, Japan waited for preliminary data from a clinical trial of 160 Japanese participants in order to better assess safety in the Japanese population. Critics argue that the small sample size likely delayed the start of vaccination efforts while providing limited benefit. Review of the application for the AstraZeneca-Oxford is ongoing, and Moderna has not yet submitted an application in Japan. Japanese officials continue to express optimism that the delayed 2020 Summer Olympic Games will be held in 2021, and the national vaccination effort is likely a key step in achieving that goal.
TAIWAN VACCINE SUPPLY Taiwan’s Minister of Health and Welfare, Chen Shih-chung, announced that an agreement to purchase 5 million doses of the Pfizer-BioNTech SARS-CoV-2 vaccine is on hold. Reportedly, Taiwan was negotiating with BioNTech to purchase the vaccine, but “the company suddenly backed out.” Minister Chen indicated that the negotiations fell through as a result of “outside forces intervening,” but he did not elaborate further. Some have speculated that influence from the Chinese government is responsible for the delay, but Chinese officials deny involvement in the decision. BioNTech has not offered an explanation regarding the underlying factors in their decision.
BioNTech was coordinating with the Shanghai Fosun Pharmaceutical Group to manufacture SARS-CoV-2 vaccines for mainland China, Hong Kong, Macau, and Taiwan; however, Taiwanese pharmaceutical company TTY Biopharm was reportedly involved in negotiations directly between the Taiwanese government and BioNTech. Representatives from BioNTech stressed that the deal with Taiwan is only delayed and not withdrawn entirely. The response to the COVID-19 pandemic has further exacerbated the tense political relationship between Taiwan and China. Taiwan announced in late December that it secured approximately 20 million doses of SARS-CoV-2 vaccine, including 10 million from AstraZeneca, nearly 5 million from COVAX, and another 5 million from an impending contract, which is believed to be the suspended agreement with BioNTech.
VACCINE CEASEFIRE The UK government called for “local ceasefires across the globe” in order to enable governments and humanitarian aid organizations to implement SARS-CoV-2 vaccination efforts in conflict zones. UK Secretary of State for Foreign, Commonwealth, and Development Affairs Dominic Raab issued a statement at a meeting of the UN Security Council emphasizing the COVID-19 risk to more than 160 million people living in areas of ongoing armed conflict—“including in Yemen, South Sudan, Somalia and Ethiopia”—and highlighting the importance of conducting vaccination efforts in those areas. These “vaccine ceasefires” would not only provide direct benefit to vaccinated individuals, but it could also mitigate the risk of viral mutation and emerging variants. The UK also called for increased financial contributions to the COVAX facility, in order to increase the vaccine supply for low- and middle-income countries.
by Suliso Vaccination campaign in Israel is a success so far and clearly the vaccine is working very well (see here for lots of data: https://ourworldindata.org/vaccination-israel-impact). However, the social lockdown and all the other measures have been a failure with Israel still among the top 10 most infected places in the world. A serious issue is that vaccination rates are slowing down due to vaccine hesitancy among specific groups and young people. Epidemiologists say at least 70% full vaccination rates are needed, in Israel that's almost every adult because 25% are children too young to be vaccinated currently. It's very unlikely to be achieved in my opinion.
What if Countries That Excel at Vaccinations Still Don’t Achieve Herd Immunity?
TEL AVIV, Israel—In the race to herd immunity, Israel has three things that put it well ahead of other countries: a relatively small population, an ample supply of the COVID-19 vaccine, and a centralized health care system that coordinates the complicated logistics of distribution.
These advantages have put Israel at the top of the world vaccination chart, with over 30 percent of the population of 9.3 million having already received the required two doses. In the United States, by comparison, the number is about 4 percent.
But Israeli officials are finding out that the first stage of the vaccination campaign might be the easy part. They now face the daunting challenge of coaxing vaccine skeptics, younger Israelis, and members of more insular communities—chiefly ultra-Orthodox Jews and some Arab Israelis—to roll up their sleeves and get the shots. Without them, Israel is unlikely to defeat the coronavirus pandemic. The process has already been hampered by what many Israelis perceive as a politicizing of the vaccine campaign by Prime Minister Benjamin Netanyahu.
How Israel fares in this second stage will hold valuable lessons for other countries hoping to achieve herd immunity, a condition that many epidemiologists believe requires at least 70 percent of the population to have either been vaccinated or recovered from the disease. Failure to reach that number in Israel, with all its advantages, would bode ill for the rest of the world.
“Demand is for sure getting slower,” said Ido Hadari, head of vaccine promotion and government affairs at Maccabi Healthcare Services, Israel’s second-largest health care provider. “It’s like getting more than halfway to the top of the mountain: It doesn’t mean we aren’t going to have to sweat to get to the peak. And we are sweating.”
The Israeli rollout began early, driven in part by a doses-for-data agreement with Pfizer that would help the company study the impact of its own vaccine. Netanyahu received the inaugural injection in December 2020.
While the United States has struggled to get shots into arms as the public clamors for injections, Israeli health care providers conducted an orderly distribution. Within two months, the campaign helped ease the stress on hospitals by driving down the total number of patients in critical condition, and it lifted Israel out of its third lockdown. Around 90 percent of Israelis over the age of 60, the main target of the initial phase, have received at least a first dose,
But demand for the shots has dropped sharply in recent weeks. Television news programs have shown clips of empty vaccination centers. Though the vaccine is now available to all citizens over the age of 16, daily injections were down nearly 39 percent on Feb. 13 from the peak in January, according to the Israeli Health Ministry. (Israel has not included most Palestinians in the West Bank and Gaza Strip in its vaccination effort, though it is broadly recognized as the occupying power in these territories, drawing condemnation from rights groups).
“I’m scared to death,” said Etti Messika, a 58-year-old hairdresser in Tel Aviv—despite clinical data that shows very few people experience serious side effects. “I got all the vaccinations for my children, but I’m afraid there hasn’t been enough time or trials for this vaccine. I’m afraid they approved it just because of the pandemic.”
All told, Israel still needs to fully vaccinate another 2.7 million people, or 29 percent of the population. (Just under one-third of Israelis are not currently eligible to get the vaccine because they are too young.)
According to polling, many younger Israelis feel less vulnerable to COVID-19 and are taking a wait-and-see attitude. There also have been lower vaccination rates among Bedouin Arabs and ultra-Orthodox Jews, whom the government has a harder time reaching with public information campaigns. Israelis in rural blue-collar towns have responded in lower numbers as well.
Vaccine hesitancy persists even in some surprising places, including medical staff at some Israeli hospitals. As of Feb. 10, the staff vaccination rate ranged from 43 to 80 percent across major Israeli hospitals.
Channel 13 News conducted a poll this past December that found that one-quarter of Israeli adults would refuse to get vaccinated altogether or wait at least a year, according to chief international affairs correspondent Nadav Eyal, who oversaw the poll. Because Israel has a relatively young population, convincing vaccine skeptics to get the injection is critical to achieving herd immunity.
“If you calculate it, we need about … 75 to 80 percent vaccination level, but we’re not going to get it anyway because we have [a large population of] children here,” Eyal said. “It’s really important that everyone that can will get themselves vaccinated because of that.”
With the country embroiled in yet another election campaign these days—Israelis go to the polls March 23—the vaccination process has seeped into politics as well. Netanyahu has made appearances at vaccination centers and taken credit for the supply deal with Pfizer. A chatbot on Netanyahu’s Facebook page even encouraged visitors to share information about people who have not yet been vaccinated, prompting the social network to remove the post because it violated its privacy policy.
Netanyahu hopes the vaccines will help reopen Israel’s economy, boosting his reelection chances. In an interview this week on Israel’s 12 News, he said: “We are going to be the first ones to get out of this. … We are going to be the first in the world because of the millions of vaccines that we brought, and because of a fantastic health system that is distributing them.”
But the mixing of politics and the pandemic has helped fuel anti-vaccination conspiracy theories. It has also stoked some resistance to the vaccination campaign among Netanyahu’s political opponents on both the left and the right. Eli Avidar, a Knesset member from the ultranationalist Yisrael Beiteinu party and a prominent critic of the government’s pandemic policy, declared at a town hall meeting Saturday that he’s not getting vaccinated.
“It doesn’t suit me. It’s my decision. Every person has the liberty to make decisions about their body,” he said. “This isn’t North Korea.”
Nadav Davidovitch, a member of an expert team advising Israel’s government on COVID-19 and the head of Ben-Gurion University’s school of public health, said vaccines have become a vehicle to attack the government.
“It reflects the tensions within Israeli society—mistrust among minorities and political instability,” he said. “Some people think it’s a conspiracy because of the involvement of Netanyahu. I think it’s crazy, but I can understand.”
The misinformation circulates even as data based on Israeli vaccinations demonstrates broad effectiveness. A study of 1.2 million people released Sunday by Israel’s largest health care provider, Clalit Health Services, found a 94 percent decline in symptomatic COVID-19 infections and a 92 percent drop in serious illness among Israelis who had both doses of the Pfizer vaccine—a finding that corroborates the company’s clinical trials. Scientists at Israel’s Weizmann Institute found there’s been a 50 percent drop in deaths and a 48 percent drop in seriously ill patients among Israelis over age 60 since mid-January.
Some officials are offering incentives for people to get vaccinated, including a reduction in municipal taxes in one Tel Aviv suburb. In the ultra-Orthodox city Bnei Brak, local officials are distributing meals ahead of the Sabbath to people willing to get the shot. Mobile vaccination sites have been set up near popular nature reserves, in part to target young hikers.
Israel’s cabinet on Monday evening approved a “green passport” program restricting entry to gyms, cultural events, swimming pools, and hotels to people with vaccination certificates. Private companies might be allowed to restrict entry to their offices based on such certificates.
But such measures would surely face court challenges in Israel, and it’s not clear how they would hold up to scrutiny. Legal and public health officials say governments in Israel and elsewhere will have to strike a balance between individual rights and the overall national interest of defeating the pandemic.
“I’m against compulsion, but on the other hand, you can’t just give total freedom of choice,” like allowing individuals to smoke in public places, said Davidovitch of Ben-Gurion University’s school of public health.
“You can’t just look at individual freedoms and forget that someone who isn’t vaccinated is also infringing on other people’s freedom. So we have to do something that is proportionate. There is no simple answer.”
by Suliso Of course a solution would still be a mixture of older people getting a vaccine and many younger just getting mildly ill. Danger is that this could promote virus mutation...
by ponchi101 Eventually we will get to the stage of accepting this virus like something we have to live with. If people refuse to get the vaccine, there will always be a reservoir and the mutations you talk about.
Their freedoms. You know, the freedom to drive a car without brakes.
by ti-amieIt’s essential to understand why some health care workers are putting off vaccination
Early data on why health care workers are delaying the Covid-19 vaccine could help us end the pandemic sooner.
By Katherine Harmon Courage Updated Feb 19, 2021, 2:34pm EST
3 big reasons health care workers are putting off the vaccines
In addition to preventing infections, serious illness, and even death, vaccinating health care workers first provides an opportunity to gather a wealth of information we won’t be able to get from the general public. That’s because health care systems have the data not only on how many people were offered and got the vaccine, but also on their demographics.
It’s a diverse group: People working in health systems include not just nurses and doctors, but also those who move patients, work in food service, serve in administrative roles, and keep facilities clean and operational. And the people in these many roles span ages, races and ethnicities, educational attainment, income levels, and many other categories.
“In the United States, it’s our best shot at really understanding vaccine hesitancy and the populations we need to be considering for getting the most vaccine coverage,” says Whitney Robinson, an epidemiologist at the Gillings School of Public Health at the University of North Carolina.
From early trends, some key lessons about why some health care workers are putting off the vaccine are emerging.
1) Covid-19 vaccine hesitancy may not be the same as other vaccine hesitancy
The experts we spoke with noted that most of the health care workers who are reluctant to get the Covid-19 vaccine immediately are not necessarily refusing it indefinitely. Many nurses, Buttenheim said in early January, “are in a wait-and-see mode: ‘I wouldn’t mind if a few more million people got it before I did.’” Despite robust safety and efficacy data, they want to see more real-world proof first.
That’s a very different stance from people who refuse — or refuse for their children — vaccines that have been around and proven safe for decades. This means “you can’t necessarily just apply what we know about vaccine hesitancy for childhood vaccines and other vaccines,” Robinson says.
As the Yale study found, among those 15 percent of workers who said they were less likely to get a Covid-19 vaccine now, many wanted a year — or at least six months — of follow-up data on recipients. Only about 11 percent of these reluctant people said that nothing would make them comfortable getting it; and fewer than 1 percent of them said they were “anti-vaccine” overall. Still, as Vice reported, health care workers are vulnerable to both believing and disseminating the Covid-19 vaccine misinformation circulating via social media.
“Accounts with names like The Holistic Nurse are proclaiming that they won’t get vaccinated, and strongly implying their followers should do the same,” Vice’s Shayla Love and Anna Merlan write. “It’s a uniquely risky situation, where people claiming medical expertise are working to undermine trust in a vaccine, just as it becomes clear that a majority of the population worldwide will need to get it in order to keep us all safe.”
2) Covid-19 hesitancy among health care workers tends to follow education
The new February report found that, of workers in the health care field who had not received education beyond high school, 29 percent said they would not get the Covid-19 vaccine (and 22 percent said they would wait until most people they knew had been vaccinated) — compared to 9 percent (and 10 percent, respectively) of people who hold a graduate degree.
Similarly, of the 15 percent of adults in the Kaiser survey who said they would “definitely not” get a Covid-19 vaccine, more than half of those (53 percent) had a high school degree or less. On the flip side, those who reported they would get the vaccine “as soon as possible” were most likely to have at least a college degree.
These patterns track with reports from health systems so far. For example, groups getting the vaccine at higher rates also are those most likely to have among the highest education. Brita Roy, of the Yale School of Medicine, where she is also director of population health and co-author of the Yale NEJM Catalyst study, notes that by early January, about 90 percent of medical residents had chosen to get the vaccine right away, compared with about 20 to 25 percent for those working in environmental services, food service, and transportation (who are likely to have lower overall education attainment). These latter groups have since started signing up for the vaccine in larger numbers, with 45 percent of people in environmental services choosing to get the shot and 35 percent of those in food service. But a striking gap between uptake with those in higher-credentialed jobs remains.
3) There are historical reasons for health care workers of color to be skeptical about getting an early health intervention
About 40 percent of health care workers in the US are people of color. A deep history of institutionalized medical racism means that people of color have frequently been subjects of unethical experiments in the US, often sowing justified mistrust in the medical establishment. Unfortunately, due also to centuries of systemic racism, many of these groups have also been among those hardest hit by the pandemic.
“I want these populations that have been burdened so badly with Covid-19 to be prioritized” for the vaccine, Robinson says. But, she acknowledges that even that ethos could make people suspect. “That’s so unusual with how health care usually operates in the United States, people might have pause,” she says.
And while some workers who haven’t gotten a vaccine yet might be prompted to sign up through simple reminders or other behavioral nudges, overcoming mistrust due to systemic racism, “this is not a nudgeable problem,” Buttenheim says. “That set of concerns and history isn’t going to be solved by a ‘mythbusters’ fact sheet or another study. It’s about really frank conversations about what you need to feel comfortable about this vaccine.”
Another step in addressing this, she says, would also be for health and medical institutions to clearly communicate and own up to past wrongdoings and indicate their goals for equitable medical treatment now and in the future.
How to address vaccine hesitancy
The rate at which health care workers are declining or delaying Covid-19 vaccines is, to many experts, unfortunately not a surprise. “I’m on record banging my head against the wall for several months that we need to be prepared for this, to have a vaccine acceptance strategy,” says Saad Omer, an infectious disease professor at the Yale School of Medicine and director of the Yale Institute for Global Health.
Although some were optimistic that health care workers would have a particularly high uptake of the vaccine, Robinson was also skeptical. “Everybody saw this coming who works in this field,” she says. “This is one of my frustrations: We know things that we haven’t been acting on.”
And there is a vast amount of research on the best ways to help people feel more comfortable getting a vaccine in general, which we can borrow from to some extent for the new Covid-19 vaccines.
For starters, we know what not to do when approaching people who are reluctant to get a vaccine. “‘You’re wrong’ — that doesn’t tend to work,” Robinson notes. “It’s a delicate thing.” She has found that among the most effective techniques is understanding where people are coming from and what their hesitations are. Acknowledging the vaccines’ newness will likely be important in addressing people’s concerns — both in this first priority group and likely later ones, as well.
Also, giving people incentives — financial or otherwise — can actually discourage them from getting vaccinated, especially if they already have concerns about side effects.
Many health systems are already working hard to ramp up communications strategies with workers, provide peer-to-peer discussion opportunities, and even talking to their employees outside of work.
“Health care workers are also community members, so reaching them through social media and our local media outlets, as well as internal communications, has been key,” Mike Dacey, president and chief operations officer at Riverside Health System in Virginia (where they have now had about 66 percent uptake among workers), wrote to Vox in an email. “We are encouraging team members who are eligible to receive the vaccine to do so within their designated phase to best support the safety and health of our team and community.”
In a December JAMA op-ed, Buttenheim and her co-authors also suggested five behavior-based strategies for getting more people to get the Covid-19 vaccine:
Have community and public leaders endorse the vaccine
Frame vaccination as a “public act” that benefits others; maybe even hand out stickers
Make getting the vaccine free and easy
Give people early access to the vaccine — if they sign up early
Eventually make vaccination a requirement for entry, such as to schools, workplaces, and even restaurants, gyms, or airplanes
Other experts note that being transparent about any potential side effects, small and large, will help engender trust. For example, some people balked at a January 6 report from the CDC that noted several severe allergic reactions — anaphylaxis — following Covid-19 vaccinations, at a rate of about 11 per 1 million doses or about 0.001 percent of people who get the vaccine, and haven’t caused any deaths (unlike the virus itself). But these events would have been unlikely to surface in the trials of tens of thousands of people, which is why the government keeps careful record of all vaccines after they go to market.
Lesser side effects are also important to communicate clearly to improve trust and transparency now and in the future. “Planning to survey the population on mild side effects experience and share those data with our health care workers will also be useful for the community and [larger] population,” Brita Roy wrote to Vox in an email.
“The sooner we can get more people vaccinated, the sooner we can get back to some semblance of normal,” Buttenheim says. And we have to get a whole lot of people vaccinated. Director of the National Institute of Allergy and Infectious Diseases Anthony Fauci (after revising his public immunity estimations upward) says we’ll need 70 to 90 percent of people immune to the virus to squelch the pandemic.
For health care workers who refuse their first chance at a vaccine, getting back in line could be tricky. There’s no guarantee of when people will be able to get a vaccine if they wait past their designated phase — until more doses are available to the general public. And even more immediately, some states, including Connecticut, have been resupplying facilities based on the number of doses they were able to give the week before. So if uptake is chronically low, availability could dip, too.
That many health care workers are not refusing the vaccine outright and, instead, planning to wait and see provides some small glimmer of hope. Acceptance of the vaccine “is likely to grow as the social norm is established,” Omer says, with the result of more people getting it when they can.
For now, many advocate using the science and information we already have to meet people where they are, and help them feel comfortable getting the shot. “We just need to get ahead of it,” Robinson says. “So much of the response has been reactionary when it comes to Covid-19. I just hope we can break that cycle.”
by dryrunguy The latest Situation Report. I read it very quickly. Because of my work, I was particularly interested in the JAMA article on PTSD among survivors of severe COVID.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 111.42 million cases and 2.47 million deaths as of 9:00am EST on February 23. The global weekly incidence continues to decrease. The weekly total is fewer than 2.5 million cases for the first time since early October 2020 and less than half the weekly total of the peak in early January. Weekly mortality continues to decrease as well, down to 66,359 deaths last week. This is a decrease of nearly 20% compared to the previous week and an overall decrease of nearly one-third from the high in late January.
Our World in Data reports that 212.15 million vaccine doses have been administered globally, a 19% increase compared to this time last week. Vaccination efforts have been reported in at least 98 countries and territories.
UNITED STATES
The US CDC reported 27.94 million total cases and 497,415 deaths. Daily incidence continues to fall sharply in the US, now down to fewer than 65,000 new cases per day—the lowest average since October 23, 2020. This trend is evident across the country, with daily incidence decreasing rapidly in all 4 regions. Additionally, 40 states (plus Washington, DC) are reporting decreasing daily incidence over the past 2 weeks. Of the remaining states, 6 are holding relatively steady (-10% to +10% change), and only 4 are reporting increasing trends: Alaska (+108%), North Dakota (+46%), Rhode Island (+14%), and Wyoming (+117%).
As daily COVID-19 incidence and mortality continue to decrease in the US, so do hospitalizations. According to data compiled by the COVID Tracking Project, current hospitalizations nationwide are down to 55,403, a decrease of 58% from the peak on January 6. Notably, the current total is now below the previous peaks in April and July 2020. Similar to incidence and mortality, current COVID-19 hospitalizations are decreasing across all 4 regions of the country. The Midwest region peaked first, in late November/early December 2020, as it began to come down from its autumn/winter surge, and the Northeast, South, and West regions all peaked around January 6-12, 2021. Most US states are reporting fewer than 200 hospitalizations per million population, and no state is reporting more than 300. New York is reporting the most per capita hospitalizations, with 298 per million population, followed by Washington, DC, with 293. Compared to the previous week, 36 states are reporting decreasing hospitalizations, and 13 states (plus Washington, DC) are holding relatively steady (-10% to +10% change). Alaska (+11%) and Hawai’i (+35%) are the only 2 states reporting an increasing trend. Data compiled by the COVID Exit Strategy website show a different trend.
The official CDC data track the number of new hospitalizations per day (ie, as opposed to current hospitalizations). New hospitalizations peaked on January 6, with an average of 16,536 per day. Since then, new daily hospitalizations have declined steadily, down to 6,417—a decrease of more than 60% from the peak. The current average is more than 20% less than the previous week.
US Vaccination
The US CDC reported 75.21 million vaccine doses distributed and 64.18 million doses administered nationwide (85.3%).
In total, 44.14 million people (13.3% of the entire US population; 16.9% of the adult population) have received at least 1 dose of the vaccine, and 19.44 million (5.9%; 7.5%) have received both doses. The average daily doses administered decreased slightly to 1.46 million doses per day*, including 664,618 second doses per day*. These decreases could be a result of delays in vaccine distribution and administration stemming from severe winter weather affecting much of the country.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 6.58 million doses have been administered at long-term care facilities (LTCFs)**, including residents and staff. This covers 4.45 million individuals with at least 1 dose and 2.01 million with 2 doses. Approximately 59% of the doses have gone to residents, and 41% to staff.
**The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 28.20 million US cases and 501,117 deaths as of 12:30pm EST on February 23.
VACCINATION EFFICACY More evidence is emerging that vaccination campaigns are significantly reducing the risk of both severe COVID-19 disease and SARS-CoV-2 transmission. A study by Public Health England found that the risk COVID-19 disease among healthcare workers (HCWs) decreased by 65-72% after the first dose of the Pfizer-BioNTech vaccine, and more than 85% after the second dose. Additionally, the risk of infection decreased by 70% in HCWs who received one dose and 85% in those who received both doses. Similarly, data from Public Health Scotland indicates that hospitalization risk decreased 94% for individuals vaccinated with the AstraZeneca-Oxford vaccine and 85% for the Pfizer-BioNTech vaccine. In Israel, data from the Ministry of Health reportedly indicate that the Pfizer-BioNTech vaccine decreases the risk of infection by 89% and the risk of disease by 94%. Israel has fully vaccinated approximately 27-32% of the population using the Pfizer-BioNTech vaccine, and nearly 50% of the population has received at least one dose. This is some of the earliest evidence that demonstrates SARS-CoV-2 vaccines’ effect on transmission.
NOVAVAX CLINICAL TRIALS Novavax announced that it completed enrollment in Mexico and the US for the Phase 3 clinical trials for its candidate SARS-CoV-2 vaccine. Combined, the trials will include approximately 30,000 participants, many of whom are in “communities and demographic groups most impacted by the disease.” The researchers proactively sought a demographically diverse group of participants—including 20% Latinx, 13% African American, 6% Native American, 4% Asian American, and 13% aged 65 years and older—in order to test the vaccine in communities at elevated COVID-19 risk. Additionally, study sites were deliberately assigned to areas with elevated community transmission, with the aim of accelerating the timeline for obtaining the data needed to conduct the efficacy analysis.
Novavax is using a different vaccine technology than previously authorized SARS-CoV-2 vaccines. The Novavax vaccine is protein-based, and it contains recombinant nanoparticles constructed of synthetic SARS-CoV-2 spike proteins to generate the desired immune response. The vaccine also contains a proprietary adjuvant to boost the immune response. The Novavax vaccine requires 2 doses, administered 21 days apart.
COVAX DONATIONS In conjunction with the 2021 summit of the Group of Seven (G7) on February 19, the leaders of Canada, France, Germany, Italy, Japan, the UK, and the US issued a joint statement pledging improved international collaboration and support for the global COVID-19 response, including additional funding for the COVAX facility, which aims to provide SARS-CoV-2 vaccine for low- and middle-income countries (LMICs). Collectively, the G7 governments committed an additional US$4 billion to COVAX, bringing the total to US$7 billion from these 7 countries. The pledge includes US$2 billion from the US, with an additional US$2 billion in the future, contingent upon the other G7 countries fulfilling their commitments.
While the financial donations help to increase the doses COVAX can afford to purchase, it does not necessarily impact the current lack of accessibility for most countries eligible under COVAX. With countries like the US, the UK, and those in the European Union consuming the majority of available vaccine supply, most LMICs remain unable to access doses, even if they could afford to pay for them. WHO Director-General Dr. Tedros Adhanom Ghebreyesus called on high-income countries to make vaccine available to LMICs. He noted that “having the money doesn’t mean anything,” if there is no vaccine available to purchase. Unilateral arrangements directly with vaccine manufacturers to acquire additional doses are delaying access and reducing allocations for LMICs, including through programs like COVAX. Dr. Tedros called on high-income countries to consider the effect on COVAX before negotiating any new contracts to purchase additional doses. Notably, he emphasized that when high-income countries “undermine” the COVAX effort, they are not only increasing the risk for LMICs, they are also increasing their own risk, because areas that remain unvaccinated will allow continued transmission and mutation that could then spread internationally.
MENTAL HEALTH OF SURVIVORS Several recent articles have investigated mental health effects of the COVID-19 pandemic. One study conducted by researchers in Italy, published in JAMA: Psychiatry, evaluated post-traumatic stress disorder (PTSD) in survivors of severe COVID-19 disease. The study involved 381 patients who sought care through an emergency department. Trained psychiatrists diagnosed PTSD in these patients using a standardized Clinician-Administered PTSD Scale, based on the results of a psychiatric assessment. The researchers diagnosed PTSD in 115 (30%) of the participants as well as depressive episodes in 66 (17%) and generalized anxiety disorder in 27 (7%). The presence of persistent medical symptoms was among the factors significantly associated with PTSD diagnosis. While a relatively small sample size, this study provides evidence that severe COVID-19 disease could be associated with longer-term mental health issues in recovered patients. This illustrates the broad array of long-term health conditions that can stem from COVID-19.
US VACCINE SAFETY MONITORING Researchers from the US CDC COVID-19 Response Team and the US FDA published analysis of early SARS-CoV-2 vaccine safety monitoring from the US vaccination campaign. The study, published in the US CDC’s MMWR, reviewed safety monitoring data for the Pfizer-BioNTech and Moderna vaccines administered in the US from December 14, 2020, to January 13, 2021—accounting for approximately the first month of vaccinations for both products. During this period, 13.8 million doses of vaccine were administered, and there were 6,994 post-vaccination adverse events reported in the Vaccine Adverse Event Reporting System (VAERS). The most common symptoms were headache (22.4%), fatigue (16.5%), and dizziness (16.5%). Anaphylactic reactions were reported in approximately 4.5 out of every million vaccinations, which is similar to the rate expected for inactivated seasonal influenza vaccines. Adverse events were more likely to be reported after an individual’s second dose than their first dose.
Among the 6,994 total reports, 640 (9.2%) were considered to be serious adverse events, including 113 deaths (78 among residents of long-term care facilities). Notably, VAERS data include reports from “healthcare providers, vaccine manufacturers, and the public,” and further investigation is required in order to determine whether a reported adverse event was associated with the vaccine. Information collected from “death certificates, autopsy reports, medical records, and clinical descriptions from VAERS reports and health care providers” do not indicate that any of the deaths were caused by vaccination.
US ECONOMIC STIMULUS Yesterday, the White House announced changes to the federal Payment Protection Program (PPP), part of the United States’ COVID-19 economic relief efforts, that aim to better support small and minority-owned businesses. Starting this week, the PPP will institute a 2-week period dedicated to businesses that employ fewer than 20 employees, many of which have struggled to navigate the PPP application process, which will enable lenders to provide additional assistance to the smallest businesses. The PPP will also update how it determines financial support for independent contractors and self-employed individuals, many of whom received PPP loans as little as US$1 under previous iterations of the program. “Exclusionary restrictions” for businesses owned by individuals who committed non-fraud felonies or individuals who are delinquent in repaying federal student loans will be eliminated. Finally, the changes will correct inconsistencies to ensure eligibility for businesses owned by non-citizen legal US residents, including Green Card holders and individuals residing in the US under a visa. The PPP has distributed billions of dollars in support to small businesses, but critics have raised concerns that structural barriers have prevented funding from being allocated to those in the greatest need, including businesses owned by racial and ethnic minorities.
The US House of Representatives is expected to vote this week on the newest COVID-19 economic stimulus package. The bill—the American Rescue Plan, published on February 19—includes US$1.9 trillion in funding to support state and local COVID-19 response, including vaccination and schools; financial support for small businesses and extended unemployment benefits; and direct payments to individuals and families. Reportedly, efforts to negotiate a bipartisan funding package have largely stalled, and Democratic members of the Congress could use a budget reconciliation process to pass the bill without Republican support.
LONG COVID As more and more people recover from acute COVID-19 disease, clinicians and researchers are gathering additional information on the chronic effects of SARS-CoV-2, commonly referred to as “long COVID.” A study conducted in Israel, published in Clinical Microbiology and Infection, investigated chronic symptoms in recovered COVID-19 patients over a 6-month period. The study included 103 patients who recovered from mild COVID-19 illness, and investigators collected data on the onset and duration of a variety of symptoms. Fever was among the first symptoms to resolve, with a mean duration of 5.6 days, whereas fatigue (31.1 days), difficulty breathing (18.6), and changes to taste (18.6) and smell (23.5) tended to persist longer. Notably, nearly half of the participants reported chronic symptoms that persisted for 6 months, including 22% with ongoing fatigue, 15% with changes to taste and smell, and 8% with breathing difficulties. The onset of some of the chronic symptoms—such as fatigue, breathing difficulties, memory disorders, and hair loss—tended to be reported after the 6-week point, indicating that they were newly developed conditions in recovered patients rather than longer-term continuations of acute disease.
Increasing prevalence of long-term health effects from SARS-CoV-2 infection are raising concerns regarding how long-term care will be managed for patients with long COVID. Chronic health conditions such as fatigue, neurological disorders, and difficulty breathing can be debilitating for some patients, and advocates and elected officials have raised the possibility of classifying long COVID as a disability. Patients with severe chronic conditions following SARS-CoV-2 infection may be unable to return to work, or school or other activities, but they may not be eligible for Social Security Disability Insurance benefits. Some advocates have called on the US Social Security Administration to proactively issue guidance regarding how to handle COVID-19-related claims, in anticipation of increased need in the coming months and years for disability support for recovered patients, including financial support or accommodations or assistance in the workplace.
SCHOOL-BASED TRANSMISSION A study conducted by the University of Florida and the Florida Department of Health, published in JAMA, investigated the impact of student quarantine and testing protocols at K-12 schools in Alachua County, Florida. Data indicate that the COVID-19 incubation period in children is 6 to 7 days, shorter than the 4 to 5 days in adults. The county implemented 14-day self-quarantine for students exposed to known COVID-19 cases, and students were allowed to return to school early if they received a negative RT-PCR diagnostic test on Day 9 or later. The rationale for this program was that SARS-CoV-2 infection should be detectable by Day 9 and that students who tested negative could safely return to school the next day. Out of 799 students who received a negative test under this program, only 1 developed symptomatic disease after returning to school, and genomic data indicate that the student was actually infected through a different exposure than the one that prompted quarantine. The program to enable students to end their quarantine period early reduced the total number of missed school days by more than 30% without resulting in any additional transmission. This study provides evidence that schools can implement testing protocols to promote in-person learning while effectively mitigating transmission risk.
A study conducted by the US CDC COVID-19 Response Team and school and public health officials in Georgia, published in the CDC’s MMWR, found that half of school-associated cases initiated from teacher-to-teacher transmission and then spread from teachers to students. The researchers evaluated data from 24 days of in-person learning at elementary schools in a single school district, which included approximately 2,600 students and 700 staff. In total 9 clusters of cases were identified, involving 13 teachers, 32 students, and 18 additional instances of household transmission. Of the 31 school-associated cases, 15 were students who are believed to have been infected following transmission between teachers. Notably, all 9 of the school clusters “involved less than ideal physical distancing, and five involved inadequate mask use by students.” The “central” role of teachers in school-based transmission provides support for vaccinating teachers in order to mitigate transmission risk during in-person classes. Current US CDC guidance indicates that teachers need not be vaccinated before schools can reopen, but many teachers unions are calling for changes to existing guidance and policies that would prioritize teachers as essential workers in order to provide protection before resuming in-person learning.
TANZANIA On February 20, WHO Director-General Dr. Tedros Adhanom Ghebreyesus issued a statement urging the Tanzanian government to report COVID-19 data and implement COVID-19 control measures. He noted that numerous Tanzanians traveling to other countries have tested positive for SARS-CoV-2, which indicates that Tanzania's epidemic is not contained. Tanzanian President John Magufuli has repeatedly stated that Tanzania eliminated COVID-19 and opposed vaccination and other protective measures; however, recent reports of COVID-19 deaths, including several senior government officials, have called attention to the country’s ongoing epidemic. Tanzania has not reported COVID-19 data since May 2020, when it had 509 cumulative cases and 21 deaths. President Magufuli reportedly changed course to some degree, now encouraging Tanzanians to take appropriate precautions to protect against COVID-19, including mask use and proper hand hygiene.
INFODEMICS On February 19, the Johns Hopkins Center for Health Security, in collaboration with experts at the WHO, published a special feature on Infodemics and Health Security in the journal Health Security. As the COVID-19 pandemic unfolded, the quickly WHO recognized the critical need to combat mis- and disinformation. Following the first Global Infodemiology Conference in 2020, the WHO collaborated with partners across 5 disciplines to publish research and commentaries in 5 peer reviewed journals on topics related to misinformation and infodemic management during public health emergencies. The special feature in Health Security includes a series of articles that analyze infodemics in the midst of health emergencies and communication policies and practices to overcome a variety of misinformation challenges, particularly in the context of emerging and ongoing health emergencies. Additionally, the special feature includes commentaries that specifically address crisis and emergency risk communication during the COVID-19 pandemic.
by ponchi101 Overall, the news is getting better.
At this rate, I think it will be easier for me to travel to Colorado in the fall and get my vaccine IN THE USA (I will pay for it). Here in Colombia, the first 12,500 vaccines were applied and... who knows.
One more business gone under: the little mom & pop shop where I buy my tennis balls and overwraps. Went by it, gates closed. No sign of anything.
by mmmm8
ponchi101 wrote: ↑Tue Feb 23, 2021 10:53 pm
Overall, the news is getting better.
At this rate, I think it will be easier for me to travel to Colorado in the fall and get my vaccine IN THE USA (I will pay for it). Here in Colombia, the first 12,500 vaccines were applied and... who knows.
One more business gone under: the little mom & pop shop where I buy my tennis balls and overwraps. Went by it, gates closed. No sign of anything.
My semi-educated guess is that by the fall, it'll be cheaper and more convenient to get the vaccine privately in Bogota than in Colorado. Will have to wait to see if I'm wrong.
My semi-educated guess is that by the fall, it'll be cheaper and more convenient to get the vaccine privately in Bogota than in Colorado. Will have to wait to see if I'm wrong.
I hope you are right but I doubt it. The process here started last week with the 12,500 and then, nothing else. No progress, no news. It seems to have been truly poorly planned.
by dryrunguy This made today's NY Times morning newsletter. No one will be surprised. Headline: ‘V.I.P. Immunization’ for the Powerful and Their Cronies Rattles South America
by ponchi101 What surprises me is that some ministers actually resigned. That is very unusual down here. You don't resign until they find you in bed, with the underage son of the leader of a drug cartel, cocaine spread all over the yacht you bought with public funding. Until then, it is business as usual.
by MJ2004Africa will pay more for Russian Covid vaccine than ‘western’ jabs
Pricing undermines Moscow’s claim that it is supplying poor countries with cheaper vaccines
The African Union will pay three times more for Russia’s Sputnik V jab than it is paying for the Oxford/AstraZeneca and Novavax vaccines, according to people familiar with the procurement process.
The $9.75 price per dose for 300m shots of the Russian vaccine, developed by the state-run Gamaleya Institute, undermines Moscow’s argument that it is offering affordable jabs to countries priced out of deals with western pharmaceutical groups.
The deals struck by the AU, which is emerging as one of the world’s biggest vaccine buyers, provide a rare insight into how jab prices compare, a subject manufacturers have sought to keep out of the spotlight.
“Africa is a key market for Sputnik V,” said the Russian Direct Investment Fund, a Kremlin-run wealth fund overseeing Sputnik V’s foreign sales. “Our international price of just under $10 per dose is the same for all markets.”
Sputnik V recipients require two doses, meaning the cost per individual is just under $20.
RDIF has boasted that the Russian jab’s cost is “two times lower than that of other vaccines with similar efficacy rate”, and that its deals with poorer countries stand in contrast to other manufacturers that have prioritised wealthy nations.
Kirill Dmitriev, RDIF’s chief executive, told the Financial Times: “Countries really see, you know, tremendous double standards from some of the western nations who promised equal access and basically are just buying everything for themselves. And they see significant inequity in vaccine distribution to favour wealthy nations . . . It’s frankly unethical.”
However, the price of the Russian vaccine, which will not start arriving in Africa until May, compares with the $3 a dose the AU has agreed for the Oxford/AstraZeneca and Novavax jabs made by the Serum Institute of India, according to the people familiar with AU procurement.
The AU will pay $6.75 a dose for the BioNTech/Pfizer vaccine and $10 for Johnson & Johnson’s, a single-dose product. It is not purchasing any of Moderna’s two-shot inoculation, priced at $32 to $37 per dose.
In addition to 300m Sputnik V doses, the AU says it has acquired provisional orders for 670m doses of other jabs. It is buying vaccines on behalf of member states in order to supplement supplies from Covax, a facility backed by the World Health Organization that is providing vaccines for free to 92 countries, including many in Africa.
The AU declined to comment on pricing.
RDIF has said its vaccine’s 92 per cent efficacy, cost and ease of storage are “unique”. But scientists at the US Food and Drug Administration this week confirmed data showing that J&J’s jab — which can also be stored in a normal refrigerator — prevented severe or critical disease in 86 per cent of US participants and 82 per cent in South Africa where the 501.V2 variant was prevalent. Because only one shot of the J&J vaccine is required, at $10 it would be nearly half the price of Sputnik V.
The Oxford/AstraZeneca jab demonstrated efficacy of about 70 per cent in clinical trials, while the BioNTech/Pfizer product, which needs to be stored frozen, showed efficacy of 95 per cent.
African governments have been disappointed at the slow pace of vaccine arrivals and, in a few cases, have struck expensive side deals to secure early supplies. South Africa ordered 1.5m doses of the Oxford/AstraZeneca jab from SII at $5.25 a dose, though it later halted rollout after discovering that the shot might not prevent mild and moderate cases caused by the 501.V2 variant first discovered in the country.
This week, the first AstraZeneca vaccine supplied by Covax arrived in Africa when Ghana took delivery of 600,000 doses. Covax said it was paying $3 per dose of the jab, manufactured in India.
Covax had originally hoped to distribute 15m doses of vaccine to Africa this month, with a further 40m arriving in March, though that timetable appears to have slipped. It has promised to provide doses sufficient to inoculate at least 20 per cent of the population of qualifying countries by the end of the year.
David Malpass, president of the World Bank, said it was true that manufacturers were diverting supplies towards richer countries that were paying more. He called for less secrecy.
“We need transparency of their contracts with Covax and the doses that are available from Covax for developing countries,” he said. “Those will be key in getting the delivery schedules.”
African governments can access a $2bn vaccine facility provided by the Cairo-based African Export-Import Bank as well as funding from the World Bank.
China has supplied few doses to Africa so far, raising questions about possible Chinese supply constraints. Beijing this month donated 200,000 doses to Zimbabwe, a near-bankrupt country with which it has close but strained relations.
BioNTech said it would not comment on pricing, but emphasised that it had offered its vaccine to many low- and middle-income countries at cost. The company added that even high-income countries were getting a price that was “significantly discounted from normal benchmarks” during the pandemic.
- FT
by Suliso Astra Zeneca is supplying their vaccine at production/delivery cost only. Not the case with anyone else.
by Suliso Here in Switzerland I think we have reached a plateau point before the next wave. Death rate and number of people in the hospital is still falling moderately, but daily infections (about 1,000 per day country wide for 8.5 million people) is stable and the new variant is starting to dominate. We are opening back all the shops this Monday, let's see if any detrimental effect. I guess I'll wait few extra day before visiting my favorite bookstore.
by ponchi101 I just read that Germany have 1.4 million doses of AZ vaccines that are going unused.
How do I get myself to Frankfurt?
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 112.65 million cases and 2.50 million deaths as of 9:30am EST on February 26. The global cumulative mortality surpassed 2.5 million deaths today:
1 death to 500k- 171 days
500k to 1 million- 91 days
1 to 1.5 million- 66 days
1.5 to 2 million- 43 days
2 to 2.5 million- 41 days
With more than 110 million cases and 2.5 million deaths, case fatality ratios (CFRs) in most countries are reaching an equilibrium. The global average peaked at 7.2% in late April/early May 2020, and it is now settling around 2.2%. The CFRs at the continent level range from 1.7% in Asia to 2.9% in Oceania. The highest continental peak was in Europe in late April 2020, with 10% case fatality, and Asia (4.3% in late March 2020) and Oceania (3.1% in October/November 2020) have reported the lowest peaks. Notably, the CFRs in Africa, Europe, and North America have increased slightly since late 2020, although with a change of less than 0.5% over that period, and CFRs continue to decrease slowly in Asia, Oceania, and South America.
Case fatality ratios range widely between countries, from less than 1% to more than 25%. Of the 178 countries and territories with available CFR data, 38 are reporting 1% or less. Of these countries, most are reporting very few cumulative deaths; in fact, only 8 have reported more than 1,000 cumulative deaths—Israel (5,687), Serbia (4,398), Nepal (2,685), Belarus (1,948), Venezuela (1,334), UAE (1,182), Malaysia (1,100), and Kuwait (1,067). The median CFR is 1.8%, and most countries and territories are reporting between 1.1% and 2.6%. In total, 33 countries and territories are reporting CFRs of 3% or greater, including 6 countries with 5% or greater. Yemen is reporting the highest CFR, with 27.7%, but no other country or territory is greater than 10%. Among the 26 countries* with the highest CFR, most have reported fewer than 500,000 cumulative cases (the denominator when calculating CFR). Only Italy (2.87 million), Mexico (2.07 million), Iran (1.61 million), and Peru (1.30 million) have exceeded that total. For countries with lower cumulative incidence, any single death can have a larger effect on the CFR.
*3 countries are tied at #24 with 3.4%.
Most of the countries with elevated CFR are reporting relatively steady values over the past several months; however, some are reporting notable changes recently. Iran’s CFR remained relatively steady at approximately 5.7% from August to November 2020, but it has decreased since then, down to 3.7%. In Eswatini, the CFR was approximately 2% from August to late December 2020, and then it increased sharply in 2021 to 3.8%. Zimbabwe’s CFR declined slowly but steadily from 3.1% in September 2020 to 2.4% in January 2021 before increasing rapidly to more than 4%. Syria’s CFR has been increasing steadily since August 2020, up from 4% to 6.6%. Ecuador’s CFR has decreased steadily from a peak of 8.6% in May 2020; however, it reported more than 3,800 previously unreported deaths on September 7, which caused its CFR to jump from 5.7% to 9.6%. The CFR has continued its downward trend since then, down to 5.6%.
Our World in Data reports that 227.62 million vaccine doses have been administered globally, a 16% increase compared to this time last week. Vaccination efforts have been reported in at least 103 countries and territories. With vaccination efforts starting in Australia and New Zealand, vaccinations are now ongoing on all continents.
UNITED STATES
The US CDC reported 28.14 million total cases and 503,587 deaths. After steep declines since mid-January 2021, the average daily incidence increased for 2 consecutive days, up to 66,347 new cases per day. Daily mortality increased slightly as well, once again above 2,000 deaths per day. Some of these increases could be attributable to depressed or delayed reporting the previous week as a result of the President’s Day holiday and severe winter weather.
The US surpassed 500,000 cumulative deaths on February 23, less than 1 year from the first reported death on February 29, 2020. Despite reaching this tragic milestone, the daily mortality has decreased substantially over the past several weeks:
1 death to 50k- 55 days
50k to 100k- 33 days
100k to 150k- 63 days
150k to 200k- 55 days
200k to 250k- 58 days
250k to 300k- 25 days
300k to 350k- 20 days
350k to 400k- 16 days
400k to 450k- 16 days
450k to 500k- 19 days
US Vaccination
The US CDC reported 91.67 million vaccine doses distributed and 68.27 million doses administered nationwide (74.5%). This percentage is a notable decrease from the previous briefing (85.3%), and it appears to stem from a combination of increased supply and slowing vaccine administration, potentially a result of the ongoing effects of severe winter weather affecting much of the country.
In total, 46.07 million people (13.9% of the entire US population; 18.0% of the adult population) have received at least 1 dose of the vaccine, and 21.56 million (6.5%; 8.4%) have received both doses. The average daily doses administered continues to decrease, down from a peak of 1.64 million doses per day to 1.29 million, including 659,192 second doses per day*.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 6.82 million doses have been administered at long-term care facilities (LTCFs)**, including residents and staff. This covers 4.53 million individuals with at least 1 dose and 2.26 million with 2 doses. Approximately 59% of the doses have gone to residents, and 41% to staff.
**The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 28.42 million US cases and 508,806 deaths as of 12:30pm EST on February 26.
J&J-JANSSEN VACCINE EUA The US FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) will meet today to evaluate safety and efficacy data for the Johnson & Johnson (J&J)-Janssen Biotech SARS-CoV-2 vaccine candidate, the first single-dose vaccine to apply for an Emergency Use Authorization (EUA). Like with the previous VRBPAC meetings for the Pfizer-BioNTech and Moderna vaccines, detailed clinical trial data was made available in advance of the meeting, including briefing documents (and addendum) from Janssen and the FDA. To our knowledge this is the first time that detailed clinical trial data have been made public for the J&J-Janssen candidate. VRBPAC will submit its recommendations to the FDA, which will make the final determination regarding an EUA for the vaccine.
The briefing document from the FDA indicates that the vaccine demonstrated acceptable safety and efficacy profiles in the Phase 3 clinical trials. Overall, the vaccine demonstrated 66.1% efficacy in preventing moderate-to-severe COVID-19 disease, with 66 cases in the vaccine group compared to 193 in the control group, and it was 85.4% efficacious in preventing severe and critical disease. Notably, there were no deaths among vaccinated participants (compared to 7 in the control group), and there were no hospitalizations identified in the vaccine group after 28 days post-vaccination. In addition to assessing efficacy in preventing COVID-19 disease, the data also provide insight on the vaccine’s ability to prevent infection. Among a small portion of the participants—2,650 out of approximately 40,000 total—the vaccine reduced the risk of infection by 65.5%, demonstrating an effect in limiting transmission. The FDA’s analysis indicates that the efficacy could potentially be lower among older adults (e.g., ages 60 or 75 years and older), although additional data are needed.
With respect to emerging variants, the vaccine demonstrated 81.7% efficacy in preventing severe or critical COVID-19 disease and 64.0% efficacy in preventing moderate disease in the South Africa portion of the trial—where the B.1.351 variant represented 94.5% of the sequenced cases. The vaccine’s efficacy was not markedly lower in Brazil, where the P.2 variant is prominent. No cases were identified for the B.1.1.7 or P.1 variants.
As we have covered previously, the J&J-Janssen vaccine requires a single dose, rather than 2 doses spread over a period of weeks (or months in some countries). Additionally, the vaccine only requires refrigeration temperatures for medium-term storage and transportation. These characteristics could reduce operational and logistical challenges for large-scale vaccination operations, which could have a substantial impact on the speed at which vaccination programs can proceed. Notably, however, the current supply is limited, and it could be another month or longer before high-volume distribution can begin.
OCCUPATION TRANSMISSION RISK The UK government published a report on the infection risk associated with various occupations, based on data on COVID-19 cases in England from September 2020-January 2021. The analysis compared the likelihood of testing positive for SARS-CoV-2 during the study period for 25 standardized occupation categories. The occupation-specific risk ranged from 2.1% to 4.8%, with an overall risk of 3.9%. None of the individual occupation groups had a statistically significant difference from the overall average; however, some of the occupations with the highest risk showed a significant increase over those with the lowest risk. Occupation groups at the upper end include professions such as teachers, law enforcement and prison staff, childcare and home care, and secretarial professions. Occupation categories with lower infection risk include professions such as farmers and gardeners; scientists, engineers, and researchers; legal, social work, and news media; and textiles and printing services.
VARIANT-SPECIFIC VACCINES Vaccine efficacy against emerging SARS-CoV-2 variants is a growing concern, and vaccine manufacturers are already working to address specific variants of concern (VOCs). Pfizer and BioNTech announced that they are initiating clinical trials for a second booster dose (i.e., a third dose) of their vaccine to evaluate efficacy against emerging variants. Three doses could potentially provide additional protection by producing higher antibody titers. Pfizer and BioNTech are also developing an adapted version of the vaccine specifically to target new variants. Moderna also announced that it is conducting clinical trials for an updated version of their vaccine which will target the B.1.351 variant, following a study that found evidence of decreased neutralizing antibody titers against that variant. Moderna has shipped the variant-specific vaccine to the US NIH to evaluate 3 approaches: a single-variant booster dose, a multivalent booster dose, and a second booster dose (i.e., third total dose) of the original vaccine.
In anticipation of vaccines adapted for emerging variants, the US FDA released guidance this week regarding how EUAs will be evaluated for SARS-CoV-2 vaccines that target emerging variants. Most notably, the FDA indicated that it could accept data from smaller clinical trials, similar to those conducted for seasonal influenza vaccines. This could accelerate the review process for modified versions of vaccines that have already demonstrated acceptable safety and efficacy profiles.
COVAX VACCINE DISTRIBUTION This week, Ghana became the first country outside India to receive SARS-CoV-2 vaccines via the COVAX facility. The shipment of 600,000 doses of the AstraZeneca-Oxford vaccine arrived Wednesday as part of the effort to deliver at least 2 billion doses to low- and middle-income countries by the end of 2021. Another 504,000 doses arrived today in Cote d’Ivoire, and shipments will continue to other countries eligible under COVAX.
UNICEF is shipping syringes to COVAX countries to support future vaccination efforts. Over the next several weeks, UNICEF will distribute 14.5 million auto-disable syringes to more than 30 countries. The first shipments include 100,000 syringes for the Maldives, which are expected to arrive next Tuesday. Côte d'Ivoire and São Tomé and Príncipe are also among the earliest scheduled recipients. In total, UNICEF is expected to supply up to 1 billion syringes by the end of the year. Supply will be drawn from the UNICEF stockpiles in Dubai and Copenhagen that were established in 2020.
EU VACCINATION EU leaders met this week to discuss plans to accelerate vaccination efforts in the bloc, including efforts to alleviate production bottlenecks and delivery delays stemming from international travel restrictions. Reportedly, the discussions also included the possibility of issuing vaccination certificates in order to facilitate international travel. Many countries in Europe rely heavily on tourism—including Greece and Spain—which has been severely hindered throughout the pandemic, and they are eager to resume international travel before the summer tourist season. Discussions are ongoing regarding the extent to which these certificates could increase travel and any restrictions that could apply to individuals without a certificate. Media reports indicate that there could be a desire to develop a vaccination certificate for the EU before large US-based technology companies (e.g., Apple, Google) develop their own, in part due to concerns about data security and privacy.
The European CDC established a new Vaccine Tracker dashboard, alongside its weekly vaccine roll-out overview. As of today, 38.67 million doses have been distributed across EU/EEA countries, and 27.95 doses have been administered.
US VACCINE EQUITY The US continues to scale up vaccine distribution and administration nationwide, but many high-risk communities are still struggling to access the vaccine. The authority and responsibility for public health in the US exists at the state level, and states are taking a variety of approaches to rolling out vaccination programs. Even within the same region, or even in neighboring states, vaccine eligibility can vary widely. In some states, vaccines are still reserved for frontline healthcare workers and older adults, whereas others have expanded eligibility to other high-risk groups, including racial and ethnic minorities and those with underlying health conditions that put them at elevated risk for severe disease.
Younger individuals with underlying medical conditions are struggling in many states to access the vaccine. Some states are expanding eligibility to adults ages 64 and younger who have multiple high-risk comorbidities, while others require only one underlying health condition. Some states, including Connecticut and Nebraska, do not consider medical conditions at all and are relying solely on age to determine eligibility. And in some states, eligibility based on comorbidities can vary from county to county. Notably, the CDC's Advisory Committee on Immunization Practices (ACIP) includes individuals with high-risk comorbidities among its Phase 1c priority populations, alongside adults ages 65-74 years.
These inconsistencies are driving disparities in vaccination coverage and providing incentive for some individuals to cheat the system. California, for example, implemented a system to distribute access codes in racial and ethnic minority communities that enable individuals to schedule a vaccination appointment. The program aimed to facilitate access to the vaccine for those who might otherwise have difficulty obtaining an appointment. Some of the codes, however, have been circulated outside those communities and used by individuals in more affluent communities and some who are not yet eligible under California’s vaccination policy. California Governor Gavin Newsom indicated that the state is implementing changes to the access code program in an effort to ensure they are used by the intended communities, but critics have raised concerns that California’s vaccination program is inherently inequitable and called for larger-scale changes to promote equitable access for vulnerable communities.
US VACCINE SUPPLY Pfizer, Moderna, and Johnson & Johnson (J&J) committed to supply a total of 240 million doses to the US government by the end of March, with 220 million coming from Pfizer and Moderna and an additional 20 million from J&J (pending receipt of an EUA). Manufacturing these new vaccines at such a large scale is posing challenges, including in obtaining raw materials and optimizing manufacturing processes, but Pfizer and Moderna are working to increase supply.
As vaccine supply increases, the US CDC is increasing support for the general public to accelerate vaccine administration. This week, the CDC unveiled the VaccineFinder.org website, which provides US residents with updated information regarding local vaccine availability, including locations of local pharmacies, clinics, and health departments with available doses. For locations with vaccine in stock, individuals can also check appointment availability. The website is managed collaboratively by the CDC, Boston Children's Hospital, Harvard Medical School, and Castlight. Initially, the website included data on 29,000 locations nationwide, but it is expected to expand.
GLOBAL COVID-19 DATA PLATFORM An international team of epidemiologists launched a website to provide anonymized data on COVID-19 patients worldwide. The new site, Global.Health, was developed with support from Google and the Rockefeller Foundation. The website will include records for more than 5 million COVID-19 patients from 160 countries, with data ranging from patient demographics to travel history. Detailed data on COVID-19 patients has been difficult to obtain and compile since the onset of the pandemic. This data is critical to conducting the epidemiological analysis necessary to understand the effects of COVID-19. Previous efforts, including manual entry into a shared Google spreadsheet, quickly exceeded file size limitations, and the Global.Health effort aims to provide detailed open access to COVID-19 data on a much larger scale.
CRISIS STANDARDS OF CARE The Johns Hopkins Center for Health Security published its second report on COVID-19 crisis standards of care (CSC), in collaboration with New York City Health+Hospitals. This report focuses on lessons from New York City’s experience managing the early COVID-19 surge in April-June 2020. Based on discussions with frontline clinicians, hospital emergency management practitioners, and other experts from hospitals and public health agencies in New York City, the researchers identified a number of key themes and recommendations.
The study participants shared their experiences with developing and implementing CSC in the midst of an emergency; challenges with insufficient equipment, supplies, space, and personnel; the mental and physical toll of responding to multiple consecutive COVID-19 surges; and coordinating CSC and patient care between emergency medical services (EMS) and hospitals. The participants indicated that the effects on personnel were among the biggest challenges they faced, including the lasting mental health impact. The report also outlines a series of recommendations and issues for future consideration.
Established and consistent CSC, including a formal declaration from hospital or health system leadership, can help mitigate some of these burdens during a health emergency. This report is part of an ongoing effort to improve CSC during communicable disease emergencies.
by ponchi101 The mention of a "third dose" sounds like we will be going through periodic vaccination for several years, a la influenza. Could help in eradicating the virus, if that is possible.
by Suliso
ponchi101 wrote: ↑Fri Feb 26, 2021 6:57 pm
I just read that Germany have 1.4 million doses of AZ vaccines that are going unused.
How do I get myself to Frankfurt?
Germans are being stupid here... They registered this vaccine only for those under 65, but people under 65 are not being vaccinated yet (except medics). Additionally they praised superior performance of the local BioNTech vaccine so much that a large portion of population now consider AZ second rate product.
by atlpam hubby got Moderna dose 2 last night. Sleeping today with bad headache & ringing ears, but expect he'll be feeling better for the weekend. GA is adding K-12 teachers to this phase - guess the union lobbying was strong - by the time the teachers get their second doses, schools will be about to let out for the summer, so they probably could have waited their turn according to the original plan. It's been hard enough for people to get appointments as it is with the current group.
by JazzNU
ponchi101 wrote: ↑Thu Feb 25, 2021 6:04 pm
What surprises me is that some ministers actually resigned. That is very unusual down here. You don't resign until they find you in bed, with the underage son of the leader of a drug cartel, cocaine spread all over the yacht you bought with public funding. Until then, it is business as usual.
Off topic and maybe for the Random thread. But that's just so specific I kind of want details...
by JazzNU
atlpam wrote: ↑Fri Feb 26, 2021 8:03 pm
hubby got Moderna dose 2 last night. Sleeping today with bad headache & ringing ears, but expect he'll be feeling better for the weekend. GA is adding K-12 teachers to this phase - guess the union lobbying was strong - by the time the teachers get their second doses, schools will be about to let out for the summer, so they probably could have waited their turn according to the original plan. It's been hard enough for people to get appointments as it is with the current group.
Great to hear about your husband getting his second dosage. Sorry to hear he has some side effects, but yes, most say they are gone in a couple of days.
Is extending the school year into the summer being discussed down there? I've heard rumblings up here.
ponchi101 wrote: ↑Thu Feb 25, 2021 6:04 pm
What surprises me is that some ministers actually resigned. That is very unusual down here. You don't resign until they find you in bed, with the underage son of the leader of a drug cartel, cocaine spread all over the yacht you bought with public funding. Until then, it is business as usual.
Off topic and maybe for the Random thread. But that's just so specific I kind of want details...
Oh we definitely need receipts on this one ponchi.
by dryrunguy I assumed ponchi was being facetious and dramatic for effect. But if that's not the case, I want dirt. After all, it's Friday night. And to quote the great Olympia Dukakis, "If you can't say anything nice about anybody, come sit by me."
by ponchi101 My point being that here in L. America NOBODY resigns over points of morality.
Heck, they don't resign when their teenage daughter is found to have millions of dollars in cash in a bank safety deposit box, all still in the original plastic wraps that the US Treasury sends them out in. Why on earth should they resign simply for skipping line for a vaccine?
by JazzNU You've disappointed me @ponchi. I was gearing up to hear the salacious details of that scandal.
ponchi101 wrote: ↑Fri Feb 26, 2021 6:57 pm
I just read that Germany have 1.4 million doses of AZ vaccines that are going unused.
How do I get myself to Frankfurt?
Germans are being stupid here... They registered this vaccine only for those under 65, but people under 65 are not being vaccinated yet (except medics). Additionally they praised superior performance of the local BioNTech vaccine so much that a large portion of population now consider AZ second rate product.
The AstraZeneca vaccine was just approved here in Canada today. But some scientists are saying that was a mistake.
To me, the AstraZeneca vaccine IS a second rate product.
62% efficacy for AZ vs. over 90% for Pfizer/BioNtech and Moderna. Which would you choose?
Also, AZ has been shown to be less effective against the South African variant. And there are questions about its efficacy in older people.
On the other hand, it's more practical in that it can be stored at typical fridge temperatures, whereas the other two require significant freezing temperatures.
If AZ was the only one available, then sure, it beats the hell out of no vaccine. But if better options are available, I want the better option.
ponchi101 wrote: ↑Fri Feb 26, 2021 6:57 pm
I just read that Germany have 1.4 million doses of AZ vaccines that are going unused.
How do I get myself to Frankfurt?
Germans are being stupid here... They registered this vaccine only for those under 65, but people under 65 are not being vaccinated yet (except medics). Additionally they praised superior performance of the local BioNTech vaccine so much that a large portion of population now consider AZ second rate product.
The AstraZeneca vaccine was just approved here in Canada today. But some scientists are saying that was a mistake.
To me, the AstraZeneca vaccine IS a second rate product.
62% efficacy for AZ vs. over 90% for Pfizer/BioNtech and Moderna. Which would you choose?
Also, AZ has been shown to be less effective against the South African variant. And there are questions about its efficacy in older people.
On the other hand, it's more practical in that it can be stored at typical fridge temperatures, whereas the other two require significant freezing temperatures.
If AZ was the only one available, then sure, it beats the hell out of no vaccine. But if better options are available, I want the better option.
Yeah, J&J at least has the advantage that it's only one shot. AZ doesn't even have that. I know it's likely AZ is approved here sometime this spring, but I'd really have to think before getting it if there was the possibility of getting Pfizer or Moderna soon.
by Suliso Sure Pfizer a bit better than AZ, but it's good enough and in a situation this desperate we can't be too picky. If they don't want to use give it up to someone else. Danish PM already offered to take it all straight away. Seems to be working just fine in UK.
atlpam wrote: ↑Fri Feb 26, 2021 8:03 pm
hubby got Moderna dose 2 last night. Sleeping today with bad headache & ringing ears, but expect he'll be feeling better for the weekend. GA is adding K-12 teachers to this phase - guess the union lobbying was strong - by the time the teachers get their second doses, schools will be about to let out for the summer, so they probably could have waited their turn according to the original plan. It's been hard enough for people to get appointments as it is with the current group.
Great to hear about your husband getting his second dosage. Sorry to hear he has some side effects, but yes, most say they are gone in a couple of days.
Is extending the school year into the summer being discussed down there? I've heard rumblings up here.
I haven't heard anything about extending school, but I don't have a child in school anymore, so I might not be aware of any discussions.
by ponchi101 As Suliso says, it may be not as good but this is a public health crisis, not a personal one. The whole point is getting the virus under control. A proper policy would be to use it in lower risk groups, mainly the young and healthy. Keep vaccinating the entire world so that some bulkheads against further spread are set up. Later on, when the most vulnerable populations have been protected, return for your Pfizer/BioNTech/J&J shots and keep doing that for two or three years, until this is really under control.
By then who knows if we will have Covid22 and new vaccines may need to be out there but right now, it is a case of using anything and everything. Heck, if they say that wearing the vaccine vial on a string around your neck works, do it.
by JazzNU
Togtdyalttai wrote: ↑Sat Feb 27, 2021 3:52 am
Yeah, J&J at least has the advantage that it's only one shot. AZ doesn't even have that. I know it's likely AZ is approved here sometime this spring, but I'd really have to think before getting it if there was the possibility of getting Pfizer or Moderna soon.
J&J has more advantages than just one shot. But people are entirely too hung up on the Pfizer and Moderna numbers and are ignoring the rest, they just stop at the 90-95% and do not want to hear anything else even though it's greatly to their benefit to do so. Hopefully people get out of their own way on this, because if people start getting picky about the manufacturer shot they get, we will surely be stuck in this through most of 2022, but likely 2023.
by atlpam Best advice I saw was that your best option is the first one available to you.
by Deuce
atlpam wrote: ↑Sat Feb 27, 2021 6:00 pm
Best advice I saw was that your best option is the first one available to you.
I disagree.
If I'm assigned the AstraZeneca vaccine, I will do proper verification - and if it's possible for me to get the Moderna or Pfizer/BioNtech, I will choose the latter. If I have to wait longer for it, or pay for it, I will. Hell, I've been very careful with protecting myself (and others) thus far - if I have to do it for an extra few weeks, or even an extra few months, in order to get a more efficient vaccine, and thus gain more protection and freedom in the long run, I will.
There's a reason some scientists here are saying that it was a mistake for us to accept the AZ vaccine. They say that it lowers the standard of protection - because it does.
As far as giving it to 'low risk' groups - there are NO low risk groups with this virus. It has killed teenagers; it has killed people in their 20s and 30s... As long as no-one knows how the virus will affect each individual person - anything from no symptoms to death -, EVERYONE is in a high risk group.
Honestly, if I got the AZ shot, I don't see where my current behaviour would change, as I'd know that I'm only 62% protected... and perhaps not protected at all against the South African variant. Thanks, but no thanks.
by ponchi101 Of course it has killed teenagers, and people in their 20's and 30´s. In a population of millions of dead, you will find deaths in all cohorts.
It has killed 45 children under the age of 1, 648 kids in the 15-24 age group, 2,922 in the 25-34 group. 0.009%, 0.13% and 0.59%. (USA Data). Assuming that the AZ vaccine gives you a 65% protection, you can slash those numbers in half and safely assume new mortalities for those groups.
Get the AZ. Then, in September, get any other you want. They are not exclusive. And you are in the (I guess) 45-54 age group (21.251 deaths, 4.5%). Dropping that 4.5% to 2.76% is not trivial. Adding your medical history (any underlying conditions) gives you a better stat yet.
by Suliso It's likely even better than that. 65% is for protection against symptomatic illness, for a really severe one resulting in hospitalization about 85% reduction has been reported.
It's fine against the British variant too, South African one possibly eludes it but the latter is a far less common than the former.
by atlpam My point was if I can get AZ or J&J now vs. having to wait 3-6 more months for a “preferred” vaccine, what I can get now is better than no protection for another 3-6 months.
by dryrunguy Just an observation... This is the first time in my life I have seen people weigh the merits of different types of vaccines. In comparison, take the various vaccines for influenza. There are several of them, and influenza kills a lot of people (though not nearly as many as COVID). But I've never heard or seen people debate the merits of one type of flu vaccine versus another. I've never seen people ask (or heard that people had asked), "Which flu vaccine should I get?" People just get it. And I would bet the lay public doesn't even know there are different types of vaccines for influenza.
Another example... Do parents ask their pediatrician which of the measles/mumps/rubella combination vaccines their child should get? I don't think so.
It's curious.
by ti-amie
dryrunguy wrote: ↑Sun Feb 28, 2021 7:39 pm
Just an observation... This is the first time in my life I have seen people weigh the merits of different types of vaccines. In comparison, take the various vaccines for influenza. There are several of them, and influenza kills a lot of people (though not nearly as many as COVID). But I've never heard or seen people debate the merits of one type of flu vaccine versus another. I've never seen people ask (or heard that people had asked), "Which flu vaccine should I get?" People just get it. And I would bet the lay public doesn't even know there are different types of vaccines for influenza.
Another example... Do parents ask their pediatrician which of the measles/mumps/rubella combination vaccines their child should get? I don't think so.
It's curious.
You're right. It's never occurred to me to ask who made the vaccine I'm getting. Ever.
by ponchi101 People don't think about influenza the way we have been thinking about C19. Bet you the vast majority of people don't know how many people influenza kills every year.. Which is not trivial.
But yes, you are right.
by dryrunguy Just to be clear, I do not mean to suggest this is a negative development. Perhaps it's an encouraging development--as long as people aren't using these comparisons to make an overarching anti-vax argument.
So now let's ask another question... why? Why are we paying such close attention now? I would bet the answer is pretty simple. For most of us, this is our first pandemic (excluding HIV for those of us who are old enough). This marks the first time we have individually and collectively felt a strong sense of urgency to solve a widespread public health crisis (unlike HIV, which started out as a transmissible disease that in the early days was largely limited to a small population). With COVID, we have had a chance to observe the R&D process and read published data associated with individual vaccine candidates. We've never had that before. We've never needed that before.
I really think it's that simple. For most of us, this is our first pandemic.
::
Now, back to the original discussion. For purely logistical reasons--since I live in a remote, rural area that is a 70-mile round trip to and from medical care--I would greatly prefer a single-dose vaccine. But all of that will depend on whether my primary care provider will have access to single-dose vaccines.
If I get lucky and it turns out that someone in PA's public health structure recognizes how much smarter it would be in the public health interest for them to bring vaccines to Dry Run rather than make people in Dry Run come to them, I'll take whatever they give me. But I won't hold my breath waiting for that scenario to transpire.
by SulisoTanzania leader says prayer will cure Covid, as hospitals overflow
Experts fear policies of John Magufuli could undermine vaccine programme in Africa
Grieving relatives of Covid-19 victims, health experts and opposition politicians in Tanzania have accused President John Magufuli of causing thousands of deaths in the east African country and undermining the fight against the pandemic across the continent.
Magufuli has denied the local spread of Covid-19 in Tanzania, discouraged the mention of the disease by health workers, rejected most conventional measures in favour of prayer and said vaccines are dangerous, without offering any evidence.
Despite repeated requests by the World Health Organization, Tanzania has not published any statistics for Covid-19 cases since May, when it logged 509, and has no testing programme.
Experts fear that Magufuli’s policies will allow Tanzania to act as a source of infections and new variants, which could spread across Africa and beyond.
The WHO last week called on Tanzania to protect not only its own 58 million citizens but also neighbouring countries.
“This situation remains very concerning. Covid-19 is a serious disease that can cause severe illness and even death. National authorities everywhere must do all they can to protect people and save lives,” said Tedros Adhanom Ghebreyesus, the WHO’s director general.
Burial workers in Dar es Salaam, Tanzania’s biggest city, and on the semi-autonomous island of Zanzibar told the Observer they face unprecedented demand. Churches said priests are conducting more funeral services than “in living memory”.
Doctors said hospitals are overwhelmed, with an acute shortage of beds and oxygen.
“We have elderly patients coming in, showing every symptom that we’ve seen around the world but we cannot test … we are not allowed to even mention Covid-19. We have to call it pneumonia,” said one doctor, who requested anonymity for fear of punishment by employers and authorities.
Farida Saidi’s 82-year-old father died this month in a hospital in Dar es Salaam. His relatives were unable to find a bed in an intensive care unit because all were full.
“They said we could only keep him where he was and hope for the best. They called it pneumonia but said, ‘your father has the same condition that everybody is facing everywhere’,” Saidi said.
“Since January we have lost six family members. On my WhatsApp there are just messages and messages about people dying. They are all showing the same symptoms: struggling to breathe, fever, loss of sense of taste. It is desperate.”
Saidi said Magufuli’s policies had cost lives.
“I wouldn’t want anyone to watch their father die the way I did. It’s so wrong.”
Zitto Kabwe, leader of the opposition ACT-Wazalendo party, said that his party had called on its members to document and report all deaths due to suspected Covid-19 so that it could hold the government to account.
“We don’t have data. There is no testing, so it’s very difficult to cut transmission. Local media have been afraid even to mention Covid-19. We just see hospitals being full,” he said.
A second wave, fuelled by a more transmissible variant of the virus originating in South Africa, has pushed infections across the continent to 3.8 million, with more than 100,000 deaths. The total is thought to be a significant underestimate.
The extent of any outbreak in Tanzania is unclear, but South Africa, which has roughly the same population, has suffered almost 50,000 deaths from Covid-19, according to official statistics, and many more according to excess mortality figures.
Last month, Tanzania’s chief government spokesman, Hassan Abbasi, told Reuters that, while the country was not entirely coronavirus-free, it had “controlled” the disease.
“There are people intermingling with the global world. But we don’t have local transmissions. That is why you are seeing everything is open, universities, sports, arts, markets, and you have not heard someone has fallen down publicly,” Abbasi said.
A doctor at the coronavirus testing centre in Zanzibar said that more than 80 cases had been recorded on the island from mid-December to early January. “But we are not allowed to release the data,” said the doctor. “We keep it for future use.”
The rise in cases has led to mixed messaging from the government.
The Zanzibar health ministry last week issued a public announcement asking people to avoid gatherings and “rush to a nearby hospital for testing if you feel you have difficulties in breathing”.
But officials denied this was because of Covid-19, saying they wanted to encourage people to take precautions because the number of people suffering breathing difficulties is increasing.
A health ministry official, Mabula Mchembe, visited hospitals in Dar es Salaam and stressed that there were no coronavirus patients, just “rumours which may cause unnecessary panic”.
Vaccination programmes are now under way or planned in most African countries, but not Tanzania.
In late January, Magufuli, who won a second term in October in an election marred by violence and allegations of fraud, said prayers, steam inhalation or herbal remedies were better than “dangerous” foreign vaccines.
Faced with international pressure and after the deaths of a series of senior officials, there has been a change over the past two weeks.
Magufuli recently attributed the death of the head of the civil service to the “respiratory disease”, and official media have begun calling on Tanzanians to wear face masks and wash their hands.
“I can’t say there is any hope,” said Kabwe, the opposition leader. “It’s too late now, the spread at the community level is so widespread. “How many people need to die before the government accepts the obvious?”
With leaders like this what kind of help can one hope to provide?
by Deuce
ponchi101 wrote: ↑Sun Feb 28, 2021 2:52 pm
Of course it has killed teenagers, and people in their 20's and 30´s. In a population of millions of dead, you will find deaths in all cohorts.
It has killed 45 children under the age of 1, 648 kids in the 15-24 age group, 2,922 in the 25-34 group. 0.009%, 0.13% and 0.59%. (USA Data). Assuming that the AZ vaccine gives you a 65% protection, you can slash those numbers in half and safely assume new mortalities for those groups.
Get the AZ. Then, in September, get any other you want. They are not exclusive. And you are in the (I guess) 45-54 age group (21.251 deaths, 4.5%). Dropping that 4.5% to 2.76% is not trivial. Adding your medical history (any underlying conditions) gives you a better stat yet.
The problem with your scenario is that vaccines are not something you can walk into a Walmart anytime to purchase. I'm assuming that if I am assigned the AstraZeneca vaccine, and I accept it, I will not be able to dictate when I will get the Moderna or Pfizer/Biontech (or J&J if it is approved here) vaccine. I assume that determination and decision will be out of my hands. It may well be that once I get the AZ shots, I won't be permitted to get another vaccine for a year. This is yet to be determined - but I'm assuming it will be something along those lines.
Will the vaccine be available privately at some point on a per demand basis? I don't know when or if that will happen. Right now, it's being distributed only as part of our publicly funded universal healthcare.
Statistics, or 'odds', or percentages, mean nothing to me - for the simple reason that I have absolutely no idea how COVID-19 would affect ME. Therefore, I am assuming the worst, and not taking any unnecessary chances.
Everyone is in exactly the same situation of having no idea how the virus will affect them. So whether one is in in a 90 percentile group, or in a 2 percentile group is really irrelevant.
Each person can decide for him/her self how he/she deals with the circumstance. I've decided that I want the best protection available. To me, this is completely logical.
As for why people are being more selective about COVID-19 vaccines than about other vaccines... well, I think it's rather obvious that it's because A) COVID-19 kills 10 times more people than influenza, and we've all likely had influenza several times without any serious consequences, B) COVID-19 is very easily transmissible - and so protection from it is extremely important, and C) we have much more information about the efficacy, etc. of the COVID-19 vaccines than we have about other vaccines - the details of the COVID-19 vaccines are unavoidable - they're in our face every day.
I'm simply trying to make the best and most informed choice I can - if I am permitted to make that choice, which I feel everyone should be permitted to do.
by Togtdyalttai I am getting my first dose of the vaccine tomorrow. I feel slightly guilty because I'm not sure I agree with the policy that allows me to get it, but I'm happy to be getting it nonetheless.
The relevant part of the policy is that both formal and informal caregivers can qualify as health care workers for vaccine purposes. Given my mom's poor health of late and that I do more for her than I once did, I qualify as an informal caregiver. Her doctor wrote a letter to affirm this. The link to the policy is below.
Togtdyalttai wrote: ↑Mon Mar 01, 2021 1:11 am
I am getting my first dose of the vaccine tomorrow. I feel slightly guilty because I'm not sure I agree with the policy that allows me to get it, but I'm happy to be getting it nonetheless.
The relevant part of the policy is that both formal and informal caregivers can qualify as health care workers for vaccine purposes. Given my mom's poor health of late and that I do more for her than I once did, I qualify as an informal caregiver. Her doctor wrote a letter to affirm this. The link to the policy is below.
The relevant part of the policy is that both formal and informal caregivers can qualify as health care workers for vaccine purposes. Given my mom's poor health of late and that I do more for her than I once did, I qualify as an informal caregiver. Her doctor wrote a letter to affirm this. The link to the policy is below.
It seems reasonable to me, given what you state about your mom's health.
by Suliso I guess it's based on our personalities. Risks to me personally are unknown so I assume I'll be asymptomatic.
Mind you that doesn't mean I'm not taking all the basic precautions.
by atlpam My son received his first dose yesterday (phase 1B in his state - essential workforce). He has had several symptomatic friends that he did not have contact with (healthy 30 year olds), so he has not been taking precautions lightly. He has primarily only socialized with a co-worker for outdoor activities. I still think it will be at least May timeframe before I am eligible.
by ponchi101 Risk for the individual is different than risk for the society. The individual doesn't know what will happen to her, within the range of the disease. It will range from not catching the disease through all the stages of possible infection, including death.
Society does know what will happen. A percentage of people will not catch the disease, another will. The second group then is split into finer and finer groups: asymptomatic, symptomatic, mild, grave, etc. Society starts using Bayesian Stats then to fine tune its model. The leaders of such a society then have to use these figures to gauge their response, and cannot use anecdotal data to see how to handle it (or shouldn't).
That is the crux of any and all personal decisions. The guy that starts smoking at 17 does not know what will happen to him 50 years later. The insurance company knows very well what will happen to the 100,000 kids that started to smoke at the same age.
by ti-amie
by ponchi101 The tenth ring of hell. All for himself.
Too bad there it no such thing as divine justice,
by ti-amie Meanwhile at CPAC with apologies to Paul Simon
"And the people bowed and prayed to the golden god they made"
Opelka showed up today for his match vs Fuscovics with no mask. Fuscovics was masked.
by Deuce
ti-amie wrote: ↑Tue Mar 02, 2021 1:18 am
Meanwhile at CPAC with apologies to Paul Simon
"And the people bowed and prayed to the golden god they made"
Opelka showed up today for his match vs Fuscovics with no mask. Fuscovics was masked.
^ That should be in the 'C19 and Tennis' thread. Posting it here suggests a political motive for posting - which I think would be out of place if true.
Opelka is far from the only one. Over the past month, I've seen several players not wearing a mask either upon entering or upon exiting the court.
While each player should behave responsibly, it is ultimately up to the tournament officials to set the COVID-19 related rules for each tournament, and to enforce them. I agree that players should be wearing masks. I don't agree that one player - no matter who he/she is - should be singled out for it (and in a non-tennis thread, at that) when several other players have done the same thing.
by ti-amie Valid point re Opelka. Look into him a bit although he has scrubbed his social media.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 114.14 million cases and 2.54 million deaths as of 5:30am EST on March 2.
The global weekly incidence increased for the first time since the early January 2021. Last week, the global weekly incidence increased 6.6% compared to the previous week, up to 2.65 million new cases. Global weekly mortality continues to decline, down to 63,370 deaths, the lowest weekly total since the week of November 9, 2020.
Our World in Data reports that 249.26 million vaccine doses have been administered globally, a 17% increase compared to this time last week. The daily average increased to 5.18 million doses, 7% higher than this time last week. Vaccination efforts have been reported in at least 114 countries and territories.
UNITED STATES
The US CDC reported 28.41 million total cases and 511,839 deaths. The US reported 3,240 deaths on February 25, the highest single-day total in 2 weeks. This included 806 previously unreported deaths in Los Angeles County, California. Without these extra deaths, the mortality for February 25 would have been 2,434 deaths—on par with the previous day (2,407).
The daily incidence in the US has fallen considerably from its highest peak—249,303 new cases per day on January 11—but the current average (66,594) still remains equal to or greater than both of the previous 2 peaks (67,316 on July 23, 2020, and 31,936 on April 12, 2020).
The average daily mortality is currently 2,050 deaths per day, slightly less than the first peak in April 2020 (2,857*) but nearly double the peak in August 2020 (1,148). Mortality has also declined considerably over the past several weeks before leveling off in recent days. The decline in daily mortality is less marked than the decline in incidence; however, this difference could be due to lags in mortality data.
*This peak included April 15, when New York City reported more than 3,700 previously unreported probable deaths from the onset of its epidemic. Without these deaths, the peak average would have been closer to 2,300 deaths per day.
This week, we will look at the most severely affected states in terms of cumulative incidence and mortality and put them in the global context.
At the national level, the per capita cumulative incidence is 85,560 cases per million population, which ranks #8 globally*. In total, 31 US states are reporting higher per capita cumulative incidence than that. Notably, Utah (115,800) and Rhode Island (118,580) would each rank #3 globally, ahead of Czechia (115,795), and North Dakota (131,030) and South Dakota (127,080) would each rank #2 globally, ahead of Montenegro (121,458). Only Andorra (140,930) is reporting higher per capita cumulative incidence than all US states. Rhode Island was among the most severely affected states during the first US surge in spring 2020 and then experienced a much higher peak late during the autumn/winter 2020 surge. North and South Dakota were the most severely affected states during the early part of the autumn/winter surge, peaking at more than 1,600 daily cases per million population, higher than any of the top 10 countries in terms of per capita cumulative incidence.
The US ranks #10 globally* in terms of per capita cumulative mortality, with 1,540 deaths per million population. Five US states would each rank #1 globally, ahead of San Marino (2,180): New Jersey (2,610), Rhode Island (2,360), Massachusetts (2,320), Mississippi (2,240), and Arizona (2,190). Another 4 states would rank #2 globally: South Dakota (2,130), Connecticut (2,130), Louisiana (2,060), and Alabama (2,020). Additionally, New York City**—which reports data to the CDC separately from New York state—is reporting 3,500 cumulative deaths per million, 60% higher than San Marino. The high cumulative mortality in New York City, New Jersey, Rhode Island, and Massachusetts are driven largely by the severe impact of the initial surge, at a time when health systems were overwhelmed, especially in New York City, and little was known about effective clinical care for COVID-19 patients. Arizona was the most severely affected state during the summer surge, followed by a higher peak in the autumn/winter 2020 surge. Mississippi was also severely affected during the summer surge, but its daily mortality remained elevated through September and October before surging again in the autumn/winter.
*The Our World in Data website utilizes the Johns Hopkins CSSE COVID-19 dashboard as opposed to the official US CDC data, so the numbers do not match exactly.
**The COVID Tracking Project does not include separate data for New York City, so New York state is displayed.
US Vaccination
The US CDC reported 96.40 million vaccine doses distributed and 76.90 million doses administered nationwide (79.8%). In total, 50.73 million people (15.3% of the entire US population; 19.9% of the adult population) have received at least 1 dose of the vaccine, and 25.47 million (7.7%; 10.0%) have received both doses. The average daily doses administered is rebounding from its brief decrease, which was likely caused by severe winter weather and now stands at 1.42 million doses per day*. The breakdown of doses by manufacturer remains relatively steady, with slightly more Pfizer-BioNTech doses administered (39.26 million; 51%) than Moderna (37.52 million; 49%). No doses of the J&J-Janssen vaccine have been reported, but we expect the first of those doses to be reported this week.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 7.15 million doses have been administered at long-term care facilities (LTCFs)**, including residents and staff. This covers 4.65 million individuals with at least 1 dose and 2.47 million with 2 doses. Approximately 59% of the doses have gone to residents, and 41% to staff.
**The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-Term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 28.68 million US cases and 515,195 deaths as of 12:30pm EST on March 2.
J&J-JANSSEN VACCINE EUA On February 27, the US FDA issued an Emergency Use Authorization for the Johnson & Johnson (J&J)-Janssen Biotech SARS-CoV-2 vaccine. The EUA closely followed the review and recommendations by the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC). Additionally, the US CDC’s Advisory Committee on Immunization Practices recommended the vaccine for use in all adults aged 18 years and older. The ACIP recommendations were approved by CDC Director Dr. Rochelle Walensky on February 28.
Reportedly, the US government could begin shipping available inventory of the J&J-Janssen vaccine across the country early this week, with some deliveries arriving as early as today. The federal government currently has 3.9 million doses available, and it expects to receive “another 16 million doses...by the end of March.” Because only one dose is required, there will be no need to schedule follow-up appointments for booster doses or maintain stockpiles at the state and local level to cover second doses. Vaccinators will be able to administer all of the available J&J-Janssen doses, without needing to reserve any for booster vaccinations, which could further accelerate vaccination efforts. Additionally, the vaccine is stable at normal refrigerator temperatures and does not require on-site dilution.
Janssen Biotech’s briefing materials submitted for the VRBPAC review indicated that plans for future clinical trials for the vaccine include children under the age of 18, pregnant women and infants, and immunocompromised individuals (pages 34 and 93).
VACCINATION & TRANSMISSION RISK While multiple vaccines have demonstrated efficacy in terms of preventing COVID-19 disease, including severe disease and death, evidence is continuing to emerge regarding their ability to mitigate infection or transmission risk.
Last week, researchers from the University of Cambridge and Public Health England published (preprint) findings from a study on the efficacy of the Pfizer-BioNTech vaccine in preventing asymptomatic SARS-CoV-2 infection. The researchers evaluated PCR-based diagnostic test results for vaccinated and unvaccinated healthcare workers (HCWs) several weeks after the initiation of vaccination efforts. The researchers identified 26 positive results out of 3,252 total tests in unvaccinated healthcare workers (0.80%), compared to 13 positive tests out of 3,535 tests (0.37%) among HCWs vaccinated less than 12 days after their first dose and 4 out of 1,989 tests (0.20%) among HCWs who received their first dose 12 days or more before the test. This corresponds to a statistically significant decrease in infection risk among vaccinated HCWs. Viral loads in vaccinated HCWs tended to be lower than in unvaccinated HCWs, although these results were not statistically significant. While not a placebo-controlled and randomized clinical trial, this study does provide real-world evidence that the Pfizer-BioNTech vaccine could provide protection against infection.
A nationwide study conducted in Israel also found evidence of lower infection risk in individuals vaccinated with the Pfizer-BioNTech vaccine. The study, published in The New England Journal of Medicine (NEJM), included nearly 1.2 million participants, pairing nearly 600,000 vaccinated individuals to unvaccinated individuals (1:1 ratio) based on “demographic and clinical characteristics.” The researchers evaluated SARS-CoV-2 infection and COVID-19 disease during 2 periods: 14-20 days after the first dose and 7 or more days after the second dose. Between 14 and 20 days after the first dose, the vaccine demonstrated 46% efficacy in preventing SARS-CoV-2 infection. At Day 7 or later after the second dose, the vaccine efficacy was 92% in terms of preventing infection. The vaccine also demonstrated high efficacy (>90%) in preventing COVID-19 disease, including severe disease, at Day 7 or longer after the second dose. Like with the UK study, this provides real-world evidence that the Pfizer-BioNTech vaccine can mitigate infection risk.
CONVALESCENT PLASMA In a systematic review and meta-analysis published in JAMA, researchers evaluated treatment with convalescent plasma compared to standard of care or use of a placebo in randomized clinical trials (RCTs)—published through January 29, 2021. The researchers identified 10 total RCTs—4 published peer-reviewed studies and 6 unpublished studies—including a total of 11,782 COVID-19 patients. Overall, convalescent plasma did not significantly differ from placebo or standard of care for any of the major outcomes of interest: all-cause mortality, length of hospital stay, mechanical ventilation use, clinical improvement, clinical deterioration, and serious adverse events. The researchers noted that there was limited data available regarding clinical improvement, clinical deterioration, and serious adverse events in these studies.
POST-ACUTE SEQUELAE OF COVID-19 Last week, the US NIH announced a new initiative focused on learning more about COVID-19 patients who experience persistent symptoms or develop new symptoms after recovery from acute SARS-CoV-2 infection. Formerly known as “long COVID,” the condition is now being referred to as post-acute sequelae of SARS-CoV-2 infection (PASC). PASC can include fatigue, shortness of breath, “brain fog,” sleep disorders, fevers, gastrointestinal symptoms, anxiety, and/or depression. The NIH study will use US$1.15 billion in funding over 4 years to address PASC from multiple perspectives, including the underlying biological cause of PASC, the prevalence of PASC among those who recover from SARS-CoV-2 infection, and the risk factors for PASC, including the interaction between SARS-CoV-2 infection and pre-existing health conditions (e.g., cardiac and neurological disorders).
During the February 24 White House COVID-19 Press Briefing, White House Chief Medical Advisor and NIAID Director Dr. Anthony Fauci said the magnitude of the problem is not yet clear. But he cited a research letter published in JAMA: Network Open by researchers at the University of Washington (US), who found that approximately 30% of COVID-19 patients experienced persistent symptoms for up to 9 months following illness. That could correlate to more than 8 million Americans to date. According to a report by NBC News more than 80 specialized “post-COVID” clinics have been established across the US to provide support to individuals suffering from PASC and gather information to better understand the condition.
OXYGEN SHORTAGE Access to affordable and sustainable oxygen supplies has been a challenge, particularly in low- and middle-income countries (LMICs). These challenges have been exacerbated by the shift from mechanical ventilation to high-flow oxygen therapy for patients with severe disease. To address the shortages, the WHO’s Access to COVID Tools Accelerator (ACT-A) launched the COVID-19 Oxygen Emergency Taskforce. The taskforce falls under ACT-A’s therapeutics pillar, co-led by Unitaid and the Wellcome Trust. The taskforce estimates that US$90 million in immediate funding is needed to address oxygen shortages across 20 LMICs, and an estimated US$1.6 billion will be needed over the next 12 months. Unitaid and Wellcome committed a total of US$20 million for the effort.
Experts note that oxygen shortages are leading to unnecessary deaths in LMICs, with 500,000 patients in need of 1.1 million oxygen cylinders daily. Dr. Peter Piot, Director of the London School of Hygiene and Tropical Medicine, highlighted disparities in the availability of medical oxygen as “one of the defining health equities...of our age.” Notably, oxygen production capacity “met less than half the need” in sub-Saharan Africa. A number of countries are constructing oxygen production facilities in order to scale up production capacity; however, this process is taking time. According to a report by the Associated Press, many countries view oxygen production from the perspective of industrial uses, rather than medical. India is leveraging its existing industrial production capacity and repurposing industrial oxygen storage tanks for use at healthcare facilities.
GLOBAL VACCINE ACCESS & DISTRIBUTION Today, Gavi published updated information regarding the first round of COVAX allocations. The first allocation includes 237 million doses of the AstraZeneca-Oxford vaccine to 142 countries, with projected deliveries through May 2021. Additionally, the publication accounts for an “exceptional distribution” of 1.2 million doses of the Pfizer-BioNTech vaccine to countries that requested it and demonstrated the ability to manage the additional logistical requirements (e.g., ultra-cold freezer capacity).
COVAX began shipping vaccines last week, including 600,000 doses to Ghana and 504,000 doses to Côte d'Ivoire, and both of those countries began vaccinations on Monday. Today, the COVAX delivered 624,000 doses to Angola and 3.94 million doses to Nigeria, and on Monday, Colombia became the first of 36 COVAX countries in the Americas to receive the vaccine, with 117,000 doses of the Pfizer-BioNTech vaccine.
Even with the acceleration in vaccine distribution through COVAX, questions remain over how the world will achieve global vaccine equity. A recent report by The Economist Intelligence Unit estimates that some parts of South America, Africa, and Asia will not achieve widespread vaccination coverage until 2023. And many experts remain cautious that COVAX will hit its goal of delivering 1.8 billion vaccine doses in 2021, as funding and supply shortages persist.
Some governments and experts, including at the WHO, are calling for vaccine manufacturers to share technology, intellectual property, and data in order to expand production capacity. Sharing access to the information and technology necessary to produce the vaccines could be achieved in several ways. One option, supported by the WHO, is a “patent pool,” similar to the platforms used for HIV, tuberculosis, and hepatitis treatments. To date, no companies have offered to participate. Another proposal involves suspending intellectual property rights during the pandemic. This plan is opposed by vaccine developers, and it was rejected in the World Trade Organization by the US and European countries, despite support from at least 119 countries and the African Union.
Pharmaceutical companies argue that wealthier nations should donate more vaccine doses, including through COVAX. Some countries are doing that, including bilateral agreements with China, Russia, and India to obtain those nations’ locally developed and approved vaccines. India has launched a 49-nation “friendship program,” and China is shipping vaccine supplies across Africa nations, Turkey, and Afghanistan. As many as 50 countries have finalized agreements with Russia for its Sputnik V vaccine. WHO Director-General Dr. Tedros Adhanom Ghebreyesus has repeatedly warned against a focus on bilateral or selective vaccine supply deals, arguing that they could result in further inequities among lower-income countries. Instead, he continues to call for more investment in the COVAX facility. Even with the recent donations, including US$2 billion from the US, COVAX remains US$800 million short of its 2021 goals.
US COVID-19 PROTECTIVE MEASURES & RELIEF Despite warnings from White House and US CDC that emerging SARS-CoV-2 variants pose a growing risk, governors across the US are lifting and relaxing restrictions on businesses, schools, and social activities following substantial decreases in daily incidence over the past several weeks. Governors in several states, both Democrat and Republican, have announced efforts to remove or relax capacity limits on restaurants, reopen bars and performance venues, and end mask mandates. At a White House briefing on Friday, CDC Director Dr. Rochelle Walensky warned that the recent decline in COVID-19 incidence does not mean that the US can relax. Daily incidence is still at the same level as the peak of the summer 2020 surge.
Even with its calls for states to continue their mitigation efforts, the federal government continues efforts to support economic recovery. On Saturday, the US House of Representatives narrowly passed a US$1.9 trillion COVID relief bill, called the American Rescue Plan, which includes funding for vaccination programs, direct stimulus payments, expanded unemployment benefits, state and local governments, and schools as well as additional funding for the global response. The Senate is expected to vote on a similar bill in the near future, possibly as early as this week. If approved, the plan would represent the sixth round of federal aid during the COVID-19 epidemic. Speaking from the White House on Saturday, US President Joe Biden called for quick action from the Senate, saying that decisive action can help reinvigorate the US economy.
J&J-MERCK PARTNERSHIP Industry competitors Johnson & Johnson (J&J) and Merck & Co. are expected to announce that they will work together to manufacture the J&J-Janssen SARS-CoV-2 vaccine. Currently, there are only approximately 4 million doses available for distribution. J&J was supposed to produce 12 million doses by the end of February, but it fell behind schedule.
In order to augment production, the US government worked with the 2 pharmaceutical companies to establish a joint partnership to manufacture the vaccine. Merck will convert 2 of its manufacturing facilities to produce the new vaccine. Merck developed its own vaccine candidate, but it abandoned the effort after the candidate did not produce a sufficient immune response in early clinical trials.
Officials from J&J have indicated that the company is on track to produce an additional 16 million total doses by the end of March and more than 100 million total doses by the end of 2021. It is unclear whether those projected numbers factor in production at the Merck facilities.
NEW ZEALAND New Zealand has received praise for its aggressive, science-led response to its COVID-19 epidemic, but a recent outbreak in Auckland continues into its third week. New Zealand officials are conducting extensive contact tracing and surveillance efforts, including genomic sequencing for all detected cases. In response to recent cases linked to the outbreak that was first reported on February 14, the Auckland region has been moved back to Alert Level 3, which is scheduled to end on March 4. The rest of the country is at Alert Level 2.
Individuals in the Auckland region are expected to remain in their household bubbles outside of work or school obligations, and mask use and physical distancing are mandatory in public spaces. Additionally, the government implemented travel restrictions for the Auckland region. Public venues are directed to close, and gatherings are heavily restricted. In accordance with these restrictions, the first weekend of the 36th America’s Cup has been postponed.
by Suliso Texas is free at last! All covid restrictions including statewide mask mandate are to be lifted next week. It will be an interesting experiment for the rest of us. No way they'll reintroduce any restrictions ever.
by ponchi101 "Hey, you wanna be the guinea pig? Please, be our guest..."
(And to think this is the state were NASA has its Johnson Space Center)
by Deuce
Suliso wrote: ↑Tue Mar 02, 2021 10:32 pm
Texas is free at last! All covid restrictions including statewide mask mandate are to be lifted next week. It will be an interesting experiment for the rest of us. No way they'll reintroduce any restrictions ever.
Their philosophy is essentially 'Let's pretend that the virus is dead.'
They will discover that what they view as 'freedom' is the complete opposite.
I'm glad that Canada is a good distance from Texas - both geographically and ideologically.
by JazzNU Texas easing any and all restrictions isn't about covid. Politics 101. It's a mighty attempt to distract from the epic power and water (expletive) that has been unfolding since the deep freeze hit the South. This is as good as a distraction as Abbott can drum up.
by Suliso
JazzNU wrote: ↑Wed Mar 03, 2021 4:26 pm
Texas easing any and all restrictions isn't about covid. Politics 101. It's a mighty attempt to distract from the epic power and water (expletive) that has been unfolding since the deep freeze hit the South. This is as good as a distraction as Abbott can drum up.
Yes of course. I think none of us here would claim otherwise. This is the worst thing what Trump did last year - turn covid from a medical crisis to a political one. Once that happened Republicans have to oppose everything Democrats propose.
by JazzNU
dryrunguy wrote: ↑Sun Feb 28, 2021 7:39 pm
Just an observation... This is the first time in my life I have seen people weigh the merits of different types of vaccines. In comparison, take the various vaccines for influenza. There are several of them, and influenza kills a lot of people (though not nearly as many as COVID). But I've never heard or seen people debate the merits of one type of flu vaccine versus another. I've never seen people ask (or heard that people had asked), "Which flu vaccine should I get?" People just get it. And I would bet the lay public doesn't even know there are different types of vaccines for influenza.
Another example... Do parents ask their pediatrician which of the measles/mumps/rubella combination vaccines their child should get? I don't think so.
It's curious.
We're not usually paying close attention to the development and clinical trial phase either. I don't recall EUA panels being streamed and monitored by mainstream news , and I can't remember if we've ever even got news alerts that X vaccine has been approved. Maybe it happened with the flu vaccine and I just don't remember, but this is all highly unusual, so hard to draw comparisons. Not to mention, I don't think many of the vaccines we typically use are EUAs, think they go through the full review process. If technology was the same now as it was at the time of the polio or TB outbreaks, I think we'd have a much better comparison.
But also, it may not be a thing here, but it may be elsewhere. Last year in South Korea, there was an issue with the flu vaccine they gave out as part of their free inoculation program. But there was an option to pay a fee and choose the manufacturer which those who could afford it were doing because they had more confidence in it. And while I don't remember the one people were choosing, I remember they were requesting it specifically by name and knew the name of the one they didn't want that was free. And I could be wrong, but it didn't seem like this was a new approach in South Korea, it seemed like it was an existing framework for their free vaccination program.
by JazzNU FYI, Pennsylvania, which is doing absolutely terrible with the vaccine rollout, just announced a plan to vaccinate teachers and school staff with the J&J vaccine. The doses will go to the state, then the state will distribute them to the County Intermediate Units that oversee the various school districts and they will hold vaccination clinics. This is actually a great idea for once in administering the doses in this rollout. They hope to vaccinate everyone in the next 2 weeks and have most schools back in session by month's end.
Seems a bit optimistic to me, but it might happen. The first shipment of J&J is around 95k doses and due in this week, which is a bit under half the number who qualify in that group.
"Back in session" is relative here. Most school districts throughout the state have some form of in-person education already and I can't really imagine most teachers and parents approving of a full in-person schedule right now in the more populated regions. It's not like this does much for middle and high schoolers who can transmit the disease very effectively. But maybe they'll increase the number of in-person days in their hybrid plans.
Thought I'd mention this, as I wouldn't be surprised if other states develop similar plans.
by ponchi101 The process here has been nothing short of something that any administration that really had any sense of shame would resign over. A minimal number of vaccines, nowhere to be seen, and no reliable information on how this will work.
For all practical purposes, the vaccination program is non-existent.
by MJ2004Chinese and South African police seize fake Covid vaccines
Criminal gangs seek to capitalise on global demand for coronavirus jabs
Police in China and South Africa have seized thousands of doses of fake Covid-19 vaccines and made more than 80 arrests after uncovering a criminal network that was distributing counterfeit jabs, according to Interpol.
The export scam was found out after police in eastern China identified a network selling counterfeit inoculations. Officers raided a manufacturing premises and found more than 3,000 fake vaccines. More than 80 people were arrested.
Separately, South African police officers found 400 ampoules of fake vaccine, enough for about 2,400 doses, at a warehouse just outside Johannesburg. The officers also confiscated a large quantity of counterfeit masks and arrested three Chinese nationals and one Zambian.
The joint investigation was co-ordinated by Interpol’s illicit goods and global health programme, which has been working to prevent criminals from exploiting the disruption caused by the pandemic.
Jürgen Stock, Interpol’s secretary-general, warned that the discovery of this network represented “only the tip of the iceberg” of vaccine-related crime. The agency is tracking other reports of fake vaccine distribution and scam attempts targeting health bodies, such as nursing homes.
Interpol highlighted in December the growing risk that criminal gangs would seek to capitalise on the global demand for Covid-19 vaccines by either selling fake inoculations or stealing real ones. The agency said the pandemic had already triggered “unprecedented opportunistic and predatory criminal behaviour” and urged its 194 member countries to foster close co-operation between police and healthcare officials.
Research by the Financial Times has already exposed the boom in vaccines for sale on the dark web, with vendors offering “stealth delivery”, overnight shipping, and demanding payments in bitcoin. Experts said many of the shots advertised were either fake or would never be sent.
Security officials in the UK and the US have issued separate warnings that vaccine research is increasingly becoming an espionage target for hostile countries that might also seek to disrupt supply chains.
Last summer, Britain’s National Cyber Security Centre, a branch of GCHQ, said Russian state-backed hackers had targeted pharmaceutical companies and academic institutions involved in vaccine research in the UK, US and Canada. The US has accused China of hacking US healthcare and research institutions working on Covid-19 vaccines, treatments and testing.
Brigadier Vish Naidoo, national spokesperson for the South African police, welcomed Interpol’s co-ordination efforts in helping to apprehend “foreign nationals attempting to peddle fake vaccines to unsuspecting people” in his country. South Africa has so far administered only 70,500 doses, equivalent to 0.1 doses per 100 residents, according to the FT’s vaccine tracker.
A spokesperson for China’s ministry of public security said the Chinese government attached “great importance” to vaccine security.
“Chinese police are conducting a targeted campaign to prevent and crack down on crimes related to vaccines, proactively investigating and combating crimes related to vaccines in accordance with law,” the spokesperson said.
-FT
by ponchi101 Things that give you hope about the Human Species...
That's DeSantis for you. Manatee county commissioner picked two wealthy counties for the state rollout in the county. Also, included her and 4 others in getting the vaccaine. DeSantis got ripped for this and rightfully so.
JazzNU wrote: ↑Wed Mar 03, 2021 4:26 pm
Texas easing any and all restrictions isn't about covid. Politics 101. It's a mighty attempt to distract from the epic power and water (expletive) that has been unfolding since the deep freeze hit the South. This is as good as a distraction as Abbott can drum up.
Yes of course. I think none of us here would claim otherwise. This is the worst thing what Trump did last year - turn covid from a medical crisis to a political one. Once that happened Republicans have to oppose everything Democrats propose.
There is not one government on the planet - be it at a federal, state/provincial, or municipal level - which has not turned the COVID-19 virus situation into a political issue.
It's what politicians do.
by Liamvalid
ponchi101 wrote: ↑Wed Mar 03, 2021 11:29 pm
Things that give you hope about the Human Species...
My husband (who is Brazilian) has said that a nurse in Brazil has been arrested for faking injecting the vaccine into her patients, and selling that vaccine to people and administering it to them for a price
by ponchi101
Deuce wrote: ↑Thu Mar 04, 2021 7:14 am
...
There is not one government on the planet - be it at a federal, state/provincial, or municipal level - which has not turned the COVID-19 virus situation into a political issue.
It's what politicians do.
Sorry, not here. It has been mishandled and people are frustrated, but it has not become political. Everybody is aware of using masks and keeping distances.
I guess by making it political it was meant that DEMS and GOPS do not even believe in the same thing, simply because of their political association.
ponchi101 wrote: ↑Wed Mar 03, 2021 11:29 pm
Things that give you hope about the Human Species...
My husband (who is Brazilian) has said that a nurse in Brazil has been arrested for faking injecting the vaccine into her patients, and selling that vaccine to people and administering it to them for a price
Just WOW! I hope they throw the book at her. There was an asshole pharmacist who got caught earlier this year for doing something similar and he got off relatively lighter than he probably should have. There's a case for attempted murder to be made for what they did.
Deuce wrote: ↑Thu Mar 04, 2021 7:14 am
...
There is not one government on the planet - be it at a federal, state/provincial, or municipal level - which has not turned the COVID-19 virus situation into a political issue.
It's what politicians do.
Sorry, not here. It has been mishandled and people are frustrated, but it has not become political. Everybody is aware of using masks and keeping distances.
I guess by making it political it was meant that DEMS and GOPS do not even believe in the same thing, simply because of their political association.
What I mean is that every government on the planet, at every level, which faces some degree of competition for power is using the virus situation to manoeuvre and manipulate for what they view as being political gain; that their decisions relating to the virus are well calculated and are made with the priority being to do what they feel is best to get themselves re-elected.
It's the unfortunate nature of the political beast.
by JazzNU
EU, Italy stop AstraZeneca vaccine exports to Australia
By RAF CASERT
BRUSSELS (AP) — A shipment of over a quarter million AstraZeneca vaccines destined for Australia has been blocked from leaving the European Union, in the first use of an export control system instituted by the bloc to make sure big pharma companies would respect their contracts.
The move, affecting only a small number of vaccines, underscores a growing frustration within the 27-nation bloc about the slow rollout of its vaccine drive and the shortfall of promised vaccine deliveries, especially by Anglo-Swedish AstraZeneca.
The ban came at the behest of Italy, and the EU did not raise objections to the tougher line Rome has adopted in dealing with vaccine shortages in the bloc since a new government led by Mario Draghi came into power Feb 13.
Italy’s objections centered both on the general shortage of supplies in the EU and on “the delays in the supply of vaccines by AstraZeneca to the EU and Italy,” a foreign ministry statement said.
It said it also intervened because of the size of the shipment, more than 250,700 doses, that would go to Australia, which it did not consider a vulnerable nation.
Italy said it had informed the company on Tuesday. AstraZeneca refused to comment. The Financial Times first reported on the issue late Thursday.
Faced with shortages of doses during the early stages of the vaccine campaign that started in late December, the EU issued an export control system for COVID-19 vaccines in late January, forcing companies to respect their contractual obligations to the bloc before commercial exports can be approved.
The EU has been specifically angry with AstraZeneca because it is delivering far fewer doses to the bloc than it had promised. Of the initial order for 80 million doses to the EU in the first quarter, the company will be struggling to deliver just half that quantity.
There were rumors that the company was siphoning off from EU production plants to other nations, but CEO Pascal Soriot insisted that any shortfall was to be blamed on technical production issues only.
The EU has vaccinated only 8% percent of its population compared to over 30%, for example, in the United Kingdom. Australia is still very much at the start of its vaccination drive.
With such an action, the EU is caught in a bind. On the one hand, it is under intense pressure to ramp up the production of vaccines in the bloc while on the other hand it wants to remain an attractive hub for pharmaceutical giants and a fair trading partner to third countries.
The EU thought it had made perfect preparations for the rollout of vaccinations, heavily funding research and production capacity over the past year. With its 450 million people, the EU has signed deals for six different vaccines. In total, it has ordered up to 400 million doses of the AstraZeneca vaccine and sealed agreements with other companies for more than 2 billion shots.
It says that despite the current difficulties it is still convinced it can vaccinate 70% of the adult population by the end of summer.
___
Danica Kirka contributed from London, Colleen Barry from Milan.
by dryrunguy Of all the Situation Reports I have posted, this one may be the meatiest yet. Had I bolded and redded everything I thought was very interesting, pretty much the whole thing would be red and bold. The discussion of the variants is very intriguing. The new news out of Brazil is frightening. The discussion regarding vaccination equity is interesting.
And they don't waste any time. They lead off with how the COVID Tracking Project will stop "long-term monitoring and analysis of the US COVID-19 epidemic." Say what?!?!?
One helluva read.
::
FIRST, A THANK YOU The COVID Tracking Project is ending its long-term monitoring and analysis of the US COVID-19 epidemic. From early on in our own COVID-19 efforts, we have come to rely on their data, analysis, and figures in our briefings. Thank you to the COVID Tracking Project team for their hard work over the past year in helping provide data to track the pandemic.
EPI UPDATE The WHO COVID-19 Dashboard reports 115.29 million cases and 2.56 million deaths as of 10:00am EST on March 5.
As global attention on emerging variants continues to increase, this week we will look at global data on several of the prominent variants of concern (VOCs): B.1.1.7, B.1.351, and P.1. In many (if not most) countries, surveillance systems are not fully capturing the spread of emerging variants, but epidemiological data are increasing in many parts of the world. Unlike general COVID-19 incidence and mortality, which are tracked via countless official and unofficial databases and dashboards, obtaining quality data on emerging variants is more difficult. Efforts to track the geographic and community spread of these variants are growing, however.
While traditional diagnostic and serological testing are designed to generally identify current or past infection, genomic sequence data are often required to identify the specific variant causing the infection. Some traditional diagnostic tests do target specific sections of the viral genome that can vary between variants—such as the S-gene target failure (SGTF) in specimens infected with the B.1.1.7 for certain PCR-based tests—which can enable them to serve as a “proxy” for sequencing. The values reported below are certainly underestimates of the prevalence of these variants, and sequencing capacity varies considerably between and within countries.
The B.1.1.7 variant is the most geographically widespread of the 3 primary VOCs. In total, more than 121,000 sequences of the B.1.1.7 variant have been reported worldwide, and infections have been reported in at least 94 countries (84 with sequence data). The variant was first reported in the UK, and it was then detected throughout Western Europe and Australia. Canada, India, and the US were among the next countries to report the variant. More recently, several countries in South America, across Eastern Europe and the Eastern Mediterranean region, Southeast Asia, and Russia have reported cases. Several countries in Africa have also reported the variant. The UK still leads all countries in terms of the number of reported sequences, with more than 100,000 (nearly 90% of the global total). Notably, the proportion of sequenced specimens containing the B.1.1.7 variant is increasing on nearly every continent.
The B.1.351 variant appears to be much less pervasive than the B.1.1.7 variant, with only 2,515 total sequences globally across 48 countries (41 with sequence data). The variant first emerged in South Africa, followed by several other countries in Southern Africa and Australia. These countries were followed by Western Europe and then Canada, the US, Japan, and South Korea. While the relative proportion of B.1.1.7 in sequenced specimens is increasing, the B.1.351 appears to be remaining more consistent across most continents.
In total, 429 infections with the P.1 variant have been reported across 25 countries (19 with sequence data). The variant was first reported in Brazil, which has reported more than 60% of the global sequences to date. The variant has been reported in several other South American countries, Western Europe, Canada, the Faroe Islands, Japan, South Korea, Turkey, and the US. The relative proportion of the P.1 variant among sequenced specimens is relatively low outside of South America (approximately 20-40%); however, it appears to be increasing slowly in Europe.
In the US, the CDC is utilizing multiple surveillance systems and networks to gather genomic data from positive SARS-CoV-2 tests, including the SARS-CoV-2 Sequencing for Public Health Emergency Response, Epidemiology, and Surveillance (SPHERES) consortium and the National SARS-CoV-2 Strain Surveillance (NS3) system. The US has reported 2,672 infections of the B.1.1.7 variant across 46 states; Washington, DC; and Puerto Rico. Most of the cases involving the B.1.1.7 variant have been identified in Florida (642), Michigan (421), and California (250). Independent analysis by a private sector laboratory company, Helix, shows the highest incidence of the B.1.1.7 variant in Florida, California, Georgia, and Pennsylvania.
The US CDC has reported considerably fewer cases involving other VOCs, including 68 infections of the B.1.351 variant across 16 states and Washington, DC, and 13 infections with the P.1 variant across 7 states. These totals are certainly an underestimate of the total impact of these variants, as only a small portion of specimens undergo genomic sequencing or other genetic analysis. In fact, even the best-performing state, Wyoming, has only sequenced 3.5% of its positive specimens, and more than half of all US states have sequenced fewer than 0.5%. As discussed below, researchers and health officials in the US are identifying newly emerging variants as well, including the B.1.526 variant, first reported in New York, and the B.1.427/429 variants, first reported in California, but the US CDC is not yet reporting data on those variants.
In mid- February, Center experts published a report on policy recommendations to identify and manage variants of concern.
Global Vaccination
Our World in Data reports that 283.6 million vaccine doses have been administered globally, a 24% increase compared to this time last week. The daily average increased to 7.78 million doses, 64% higher than this time last week (up from 4.73 million doses). Vaccination efforts have been reported in at least 119 countries and territories.
UNITED STATES
The US CDC reported 28.58 million total cases and 517,224 deaths. The decline in daily incidence and mortality that persisted for the past several weeks appears to have leveled off to some degree. Daily incidence has remained between approximately 63-67,000 new cases per day since February 20, and daily mortality has hovered between approximately 1,900 and 2,100 deaths per day since February 19. Some of this trend could be the result of states catching up on reporting after recovering from severe winter weather, but it could be an early sign that the steep decline is coming to an end. Notably, both the daily incidence and mortality remain elevated, on par with or higher than the first 2 peaks.
US Vaccination
The US CDC surpassed 100 million vaccine doses distributed (109.9 million) and 80 million million doses administered (82.6 million) nationwide. In total, 54.0 million people (16.3% of the entire US population; 21.2% of the adult population) have received at least 1 dose of the vaccine, and 27.8 million (8.4%; 10.9%) have received both doses. The US set a new record high for daily doses administered, with 1.8 million doses per day*. The breakdown of doses by manufacturer remains relatively steady, with slightly more Pfizer-BioNTech doses (42.2 million) than Moderna (40.3) doses administered nationwide. No doses of the J&J-Janssen vaccine have been reported yet.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 7.3 million doses have been administered at long-term care facilities (LTCFs)**, including residents and staff. This covers 4.7 million individuals with at least 1 dose and 2.5 million with 2 doses.
**The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-Term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins Coronavirus Resource Center reported 28.83 million US cases and 520,518 deaths as of 11:30am EST on March 5.
EMERGING VARIANTS Novel SARS-CoV-2 variants, and associated surveillance data, continue to emerge around the world. Several high-profile variants—including B.1.1.7, B.1.351, and P.1—have gained attention due to concerns about their ability to transmit more efficiently, evade immune responses from therapeutics and vaccines, and increase disease severity. While the world focused on these variants, others continue to emerge, including in the US. Recently, researchers identified the B.1.526 variant in New York and the B.1.427 and B.1.429 variants in California.
The B.1.526 variant emerged in New York in November 2020, and 2 recent studies by researchers at the California Institute of Technology (Caltech) and Columbia University (New York)—both preprints—provide preliminary analysis of the variants’ characteristics relative to existing strains. The B.1.526 variant currently includes 2 versions of the virus, with one exhibiting the E484K mutation—found in the P.1 and B.1.351 variants—that helps the virus evade vaccine-induced immune response and the other exhibiting the S477N mutation that is believed to “affect how tightly the virus binds to human cells.”
The B.1.427 and B.1.429 variants were recently identified in California by researchers at the University of California, San Francisco (UCSF) and Cedars-Sinai Medical Center in Los Angeles. Early research on these variants* suggests that their transmissibility could be on par with the B.1.1.7 variant, which is quickly becoming the dominant variant in multiple countries. Reportedly, one study found that the variants were “40 percent more effective at infecting human cells than earlier variants.” Researchers also identified elevated viral loads in patients infected with the new variants, and they found evidence that the variants are better able to evade immune responses.
*To our knowledge, two studies on these emerging variants have not yet been published publicly.
Further study is needed to more fully characterize these new variants, but their emergence in the US illustrates the importance of containing transmission as vaccination efforts scale up. Vaccination is an important tool in bringing the pandemic under control, but it cannot be an excuse to prematurely relax risk mitigation measures or vigilance in adhering to existing guidance. Scaling up sequencing volume for SARS-CoV-2 specimens and facilitating collaboration and data sharing across disparate institutions will be key to generating a more comprehensive picture of genetic variations and evolution of SARS-CoV-2 in the US and around the world. Additionally, increasing the pace of global vaccination efforts, including through expanding international production of US- and European-developed vaccines, is critical to limiting transmission in countries around the world and mitigating the risk of future novel variants emerging.
GERMANY AUTHORIZES AZ-OXFORD VACCINE FOR ADULTS 65+ Germany’s national vaccine committee on Thursday formally recommended the AstraZeneca-Oxford SARS-CoV-2 vaccine for use in all adults, including those age 65 years and older. Germany initially withheld endorsement for older adults, citing a lack of data; however, recent real-world data from the UK and clinical studies show the vaccine is highly effective among older adults. While Health Minister Jens Spahn called the committee’s move “good news,” many Germans remain skeptical of the vaccine’s effectiveness. Germany’s decision to expand eligibility for the AstraZeneca-Oxford vaccine comes alongside similar announcements by Belgium, Denmark, France, and Sweden.
INDIAN VACCINE Bharat Biotech, developer of India’s SARS-CoV-2 vaccine, announced preliminary Phase 3 clinical trial results. The vaccine is already authorized for emergency use in India—issued on January 3, 2021, more than 2 months prior to release of the Phase 3 trial data. The trials included 25,800 participants (including more than 2,400 over the age of 60), half of whom received the vaccine. The vaccine demonstrated an overall efficacy of 81% in preventing COVID-19 disease (mild, moderate, or severe). The researchers have identified 130 total cases of COVID-19 among the participants, but the interim analysis is based on data from only the first 43 cases (36 among the control group and 7 among vaccinated participants). Like many of the existing SARS-CoV-2 vaccines, the results were announced via press release, and the full trial data have not yet been published publicly or been subjected to peer review. Bharat committed to publishing both the second interim analysis and final analysis via preprint servers and in peer-reviewed journals. Reportedly, many Indians have been hesitant to get vaccinated with the Bharat product until Phase 3 trial data were published.
Like many other SARS-CoV-2 vaccines, the Bharat vaccine requires 2 doses, but it does offer several advantages. The vaccine is stable at normal refrigerator temperatures (36-46°F; 2-8°C), and it can remain viable for 28 days after vials are opened, both of which can ease logistical and operational challenges for mass vaccination efforts. One notable difference from existing vaccines is that the Bharat vaccine utilizes an inactivated version of the SARS-CoV-2 virus, as opposed to mRNA or other viral platform to stimulate the immune response, similar to the vaccines developed by Sinopharm and Sinovac in China.
LONG-TERM EFFECTS IN CHILDREN A report from Kaiser Health News (KHN) discusses increases in pediatric cases of post-acute sequelae of SARS-CoV-2 infection (PASC)—commonly referred to as “long COVID-19.” Perhaps the most serious of these conditions is multisystem inflammatory syndrome in children (MIS-C), which has been reported in at least 2,060 children across the US, including 33 deaths (through March 1, 2021). Black and Hispanic/Latino children are disproportionately affected, representing 66% of the reported cases.
Children’s hospitals across the country are struggling to treat pediatric PASC patients, because so much remains unknown about the condition, particularly in children. Several facilities—including the University Hospitals Rainbow Babies & Children’s Hospital in Cleveland, Ohio—are establishing dedicated clinics to treat these patients and gather data to better characterize the long-term effects of SARS-CoV-2 in pediatric patients. KHN notes that disparities in US health coverage could potentially lead to large out-of-pocket costs specialize care, particularly because uncertainty surrounding the condition could necessitate a large number of tests and treatments.
With no available vaccine for children under age 16, and many school systems resuming in-person classes, in the US and around the world, it will be important to study the lasting effects of SARS-CoV-2 infection among children, including those with mild or asymptomatic infection in children.
US VACCINATION US President Joe Biden announced this week that the US has secured enough vaccine supply to vaccinate every US adult by the end of May, accelerating the previous timeline, which aimed to achieve that milestone by July. He also highlighted the ongoing efforts by FEMA to support vaccine distribution and collaborate with state governments to establish mass vaccination sites. Notably, President Biden urged all states to prioritize teachers, school staff, and childcare providers for vaccination as essential workers. He emphasized that existing CDC guidance can help schools mitigate COVID-19 risk and enable them to resume in-person classes even if teachers are not yet vaccinated, but he acknowledged that many educators have concerns. Currently, at least 30 states already prioritize teachers for vaccines, but President Biden aims to make that consistent across the country. He challenged states to administer at least 1 dose of the vaccine to every educator, school employee, and childcare provider by the end of March, and the US government intends to utilize federal vaccine distributions to pharmacies to further this effort.
GLOBAL VACCINE DISTRIBUTION Italy denied a request by AstraZeneca to export more than 250,000 doses of its SARS-CoV-2 vaccine, developed in collaboration with the University of Oxford, to Australia. According to a statement issued by the Italian Ministry of Foreign Affairs, Italy previously permitted the export of small quantities of the vaccine for research purposes; however, due to the quantity of vaccine in the recent request, Italy submitted a request to the European Commission (EC) to deny the export, which was approved by EC leadership. As part of its justification, Italy noted that Australia “is considered ‘non-vulnerable’” and that the large export would exacerbate ongoing shortages in Italy and the rest of the EU. This is the first time an EU country has blocked the export of a SARS-CoV-2 vaccine. Reportedly, Australia requested that the EC review its decision, but Australian officials emphasized that the blocked shipment would not have a major impact on its vaccination or COVID-19 control efforts. This incident highlights challenges in terms of ensuring equitable global access to SARS-CoV-2 vaccines, particularly for countries without domestic production capacity.
US VACCINE EQUITY & ACCESS State-level decisions regarding local distribution of SARS-CoV-2 vaccine doses have called attention to disparities in access between urban and rural areas. In some states, lawmakers and public health officials have raised concerns that too many vaccine doses are being distributed to urban centers and too few to rural areas. The vaccine supply in some urban areas is not sufficient to cover the large populations of healthcare workers who live there, which in turn, limits availability for other high-priority populations, such as older adults. In some instances, rural areas have already expanded eligibility to younger portions of the population, and older adults from urban areas who are unable to obtain a vaccination appointment locally are traveling to rural areas to get vaccinated.
According to a report from STAT News, a recent vaccination event in a rural, low-income area of Florida, where 60% of the population are Black and 25% Hispanic, most of the available doses were administered to individuals who lived elsewhere, including wealthier communities in West Palm Beach and Miami, many of whom were White. Even in wealthier communities, there are noticeable racial and ethnic disparities in terms of vaccination. For example, Black and Hispanic individuals make up nearly 40% of the population in Palm Beach County, but they have received less than 10% of the doses administered there.
Some experts and public health officials have expressed concern that the Johnson & Johnson (J&J)-Janssen vaccine could face challenges in terms of equitable distribution. Unlike the Moderna and Pfizer-BioNTech vaccines, the J&J-Janssen vaccine requires only one shot and can be stored for up to 3 months under normal refrigeration temperatures. Some experts have raised concerns that earmarking the J&J-Janssen vaccine for lower-income or rural communities could raise equity issues due to its lower reported efficacy relative to the other vaccines.
Dr. Marcella Nunez-Smith, head of the White House's COVID-19 Health Equity Task Force, acknowledged the vaccine’s advantages, but added its distribution "should be even across communities." Dr. Ruth Faden, Director of the Johns Hopkins Berman Institute of Bioethics, and Dr. Ruth Karron, Director of the Johns Hopkins Center for Immunization Research, emphasize that perceptions that certain communities are receiving an inferior vaccine could exacerbate existing vaccine hesitancy, particularly among lower-income and racial and ethnic communities. While the J&J-Janssen vaccine offers some logistical and operational advantages over other vaccines, it is essential to continue even distribution of all 3 vaccines.
BRAZIL Brazil is reporting its highest daily incidence and mortality to date, and health systems across the country are straining to handle the ongoing surge. Brazil is averaging more than 57,000 new cases and 1,300 deaths per day, an increase of 27% and 31%, respectively, over the past 2 weeks. On March 3, Brazil reported 1,910 deaths, its highest single-day total since the onset of the pandemic. According to a report by Fundação Oswaldo Cruz (FioCruz), the ICUs in 18 of 26 states are operating at over 80% capacity, and 9 of those are above 90% capacity, the most severe situation since the beginning of Brazil’s COVID-19 epidemic. Among the worst affected states are Rondônia and Rio Grande do Sul, where ICUs are operating at 97.5% and 97.2%, respectively. Additionally, the Federal District—home to Brazil’s capital city, Brasilia—is reporting ICUs at 96.45%. Vaccine rollout has been incredibly slow, with only 3% of the population receiving at least 1 dose of the vaccine and only 1% receiving both doses.
The combination of emerging variants, including the P.1 variant first identified in Brazil, and recent large-scale events such at Carnival are raising concerns about the potential for the emergence of new variants. Ongoing widespread community transmission will continue to provide the virus with an opportunity to mutate. Dr. Miguel Nicolelis, a epidemiologist and neuroscientist from Duke University (North Carolina, US) described the situation as “the largest open laboratory in the world for the virus to mutate.” Over the course of its epidemic, the Brazilian government has often been reluctant to impose risk mitigation measures, and the country is on track to surpass the US as the #1 country globally in terms of daily incidence in the coming days.
HUNGARY The Hungarian government announced tighter COVID-19 restrictions following in response to its ongoing COVID-19 surge. From March 8 to 22, non-essential businesses and services are suspended, restaurants will close for in-person dining, and in-person learning for kindergarten and primary school will be suspended until after spring break (April 7). Sporting events will continue, but no spectators will be permitted. These measures will be implemented in addition to existing restrictions, including an 8pm-5am curfew, mask mandate, and remote learning for high schools and universities. All measures will be enforced with fines or the closure of violating places. The new measures aim to curb transmission in time for the Easter holiday.
In an effort to expand vaccination coverage, Hungary decided to alter its vaccination plan to focus on ensuring as many people as possible receive the first dose of vaccine. Hungary will delay the interval between the first and second dose for both the Pfizer-BioNTech and AstraZeneca-Oxford vaccine. The second dose of the Pfizer-BioNTech vaccine will be administered at 35 days instead of 21, and the second dose for the AstraZeneca-Oxford vaccine will now be administered at 12 weeks.
COMMUNIVAX WEBINAR The Johns Hopkins Center for Health Security is hosting a webinar as part of the CommuniVax initiative to discuss recommendations from its first report on engaging communities of color to promote equity in SARS-CoV-2 vaccination. The combination of longstanding disparities and mistrust in government and the healthcare system among racial and ethnic minority communities and a disproportionate impact of COVID-19 pose significant challenges to ensuring equitable access to SARS-CoV-2 vaccination for those at elevated risk for infection and severe COVID-19 disease and death.
The webinar will include presentations by Dr. Monica Schoch-Spana from the Johns Hopkins Center for Health Security, Lois Privor-Dumm from the Johns Hopkins International Vaccine Access Center, Dr. Stephen B. Thomas from the Maryland Center for Health Equity, and Ysabel Duron from The Latino Cancer Institute, with Dr. Emily Brunson from Texas State University as moderator. The webinar will be held on Thursday, March 18 at 2pm EDT. Advance registration is required.
HEALTH SECURITY SPECIAL FEATURE: GENE DRIVES The Johns Hopkins Center for Health Security’s peer-reviewed journal, Health Security, is publishing a Special Feature devoted to regulation for gene drives and similar biotechnology in the US. Existing biotechnology frameworks may not adequately address emerging capabilities like gene drives. This Special Feature will focus on methods, programs, research, and policies that promote an optimal balance between developing and leveraging gene drive capabilities and effective oversight to mitigate the risk of misuse. Articles can be submitted for consideration though May 31, 2021.
by JazzNU I'm getting the fist shot of the vaccine this afternoon. Unexpected as I was thinking it would be April before they called my number. Scheduled it last night after receiving the notification. I've got a pre-existing condition that makes it more possible I wouldn't have a good outcome if I caught covid.
Pretty sure it will be the Moderna vaccine. I do have a lengthy history of allergic reactions, though they don't tend to be of the severe variety, so hoping for the best. Wish me luck!
by ti-amie Detroit's mayor refused the delivery of J&J vaccine to the surprise of a lot of people. The Mayor said it wasn't the best.
My doctor says the one to get is the Pfizer vaccine. Isn't J&J the company that knew for years its talcum powder causes cancer and said nothing but "oops" when they got caught?
by ponchi101
JazzNU wrote: ↑Fri Mar 05, 2021 8:19 pm
I'm getting the fist shot of the vaccine this afternoon. Unexpected as I was thinking it would be April before they called my number. Scheduled it last night after receiving the notification. I've got a pre-existing condition that makes it more possible I wouldn't have a good outcome if I caught covid.
Pretty sure it will be the Moderna vaccine. I do have a lengthy history of allergic reactions, though they don't tend to be of the severe variety, so hoping for the best. Wish me luck!
Keep us posted, I am sure it will go well
---0---
Brasil. The situation there is so dire that COLOMBIA CANCELLED the round-robin match between Brasil/Colombia (FIFA world cup) claiming that it could not guarantee the safety of the personnel HERE. Bolsanaro, in the meantime, went on national TV and stated that he saw no reasons to implement lockdowns and that everything was fine, that the epidemic (inside Brasil) was no issue at all, and therefore, in five minutes, claiming all for himself the mantle as the most lunatic leader of the world, now that Tiny is gone. Truly sick.
JazzNU wrote: ↑Fri Mar 05, 2021 8:19 pm
I'm getting the fist shot of the vaccine this afternoon. Unexpected as I was thinking it would be April before they called my number. Scheduled it last night after receiving the notification. I've got a pre-existing condition that makes it more possible I wouldn't have a good outcome if I caught covid.
Pretty sure it will be the Moderna vaccine. I do have a lengthy history of allergic reactions, though they don't tend to be of the severe variety, so hoping for the best. Wish me luck!
Keep us posted, I am sure it will go well
---0---
Brasil. The situation there is so dire that COLOMBIA CANCELLED the round-robin match between Brasil/Colombia (FIFA world cup) claiming that it could not guarantee the safety of the personnel HERE. Bolsanaro, in the meantime, went on national TV and stated that he saw no reasons to implement lockdowns and that everything was fine, that the epidemic (inside Brasil) was no issue at all, and therefore, in five minutes, claiming all for himself the mantle as the most lunatic leader of the world, now that Tiny is gone. Truly sick.
by shtexas
JazzNU wrote: ↑Fri Mar 05, 2021 8:19 pm
I'm getting the fist shot of the vaccine this afternoon. Unexpected as I was thinking it would be April before they called my number. Scheduled it last night after receiving the notification. I've got a pre-existing condition that makes it more possible I wouldn't have a good outcome if I caught covid.
Pretty sure it will be the Moderna vaccine. I do have a lengthy history of allergic reactions, though they don't tend to be of the severe variety, so hoping for the best. Wish me luck!
Got my first shot - Moderna - this afternoon as well. Stayed up several nights waiting for CVS to add appointments, and at 5:10 am Thursday, they opened at a store 20 minutes from me. Appointment was 3: 30. Had shot in my arm at 3:25. Plus, 2nd shot scheduled for same time 4/2.
by shtexas
ti-amie wrote: ↑Fri Mar 05, 2021 9:49 pm
Detroit's mayor refused the delivery of J&J vaccine to the surprise of a lot of people. The Mayor said it wasn't the best.
My doctor says the one to get is the Pfizer vaccine. Isn't J&J the company that knew for years its talcum powder causes cancer and said nothing but "oops" when they got caught?
The one to get is the one available to give you.
Detroit has a huge endangered demographic. They need to get shots in arms.
I got Moderna because that was what was available when a spot opened up. I would have taken J&J if that was the one available
by JazzNU I ended up getting the Pfizer much to my surprise. Recent local media attention with in-depth reports on Philly suburbs not getting an equitable amount of supply in line with their population resulted in a sudden increase in what the county got from the state from what I gather, and part of that must have included the Pfizer vaccine. Everything they've said, and the info on the site before this week referenced only the Moderna vaccine so I thought for sure that's what I was getting.
My county's site was very well run. Got the actual vaccine in under 15 minutes of arriving, after a few different checkpoints verifying identity. Most people stay for 15 minutes after getting the shot, they had me stay 30 minutes because of my allergy history. Didn't have any issues while I was there, and have been fine since. Shot was clean in and out, can't even see the entry point. I have very minor arm pain and discomfort. Though I will say, my doctors have told me in the past, I have a high threshold for pain, so it may be worse for someone else experiencing it. Nothing I'm not used to from the flu vaccine. Actually, I have had worse reactions to the flu vaccine depending on the year. My arm was heavy most of last night, but is considerably better this morning. I had a headache last night, could be related, but could've just been the start of a migraine. But took some medicine, which may have dulled some of the arm pain.
Feel very lucky to have gotten it already.
------
l would've taken any of the three. Doctors I know and trust, not to mention experts in the field, said all will protect me. I think people have focused on the initial numbers they heard on Johnson & Johnson and missed the overall picture. Unlike the Pfizer and Moderna vaccines, the J&J was tested when the variants were around, including conducting trials in both South Africa and Brazil among the two most worrisome variants to many. Tested in South Africa when their variant was dominant in over 90% of the cases. And still 100% protection against death and hospitalizations, which did occur in the placebo group. I said sign me up once I heard that, so I was always good with all of them. Definitely agree, at least in the US where verified ethical clinical trials were conducted, that the best vaccine is the one that is available to you.
by dryrunguy So glad everything went smoothly for you, Jazz.
by ti-amie I'm glad you're okay Jazz.
I'm looking to go in the next couple of weeks.
by ti-amie
by JazzNU
Single-shot COVID-19 vaccine is popular at vaccination sites
The first week of distribution eased worries that people might turn it down
By Nicole Wetsman
The messaging that all three authorized vaccines are good options appears to be sinking in around the country. When the first batch of single-dose Johnson & Johnson vaccines arrived in States this week, people were excited to take it.
In Connecticut, Hartford HealthCare let people decide which type of vaccine to sign up for, and the Johnson & Johnson shot was more popular than expected. People were also given the choice at a Miami vaccination site. One recipient told CNN that she picked Johnson & Johnson because it’s one dose; she’s afraid of needles and only wanted to do it once. A Minnesota couple told KTTC-TV that they were eager to get a vaccine that was only one dose.
That’s a big relief for experts who worried that the shot faced a communications problem. Even though the vaccine was just as good as the other two authorized vaccines at keeping people out of the hospital and alive, overall, its ability to prevent disease wasn’t quite as strong during the trials testing it. They thought there might be the (mostly unfounded) perception that the Johnson & Johnson vaccine wasn’t a good option.
“We have a vaccine now that has good efficacy that everyone is going to compare to the existing vaccines, and say it doesn’t look quite as good,” said Eric Rubin, a professor of immunology, during a meeting of the Food and Drug Administration’s vaccine advisory committee last week. Experts stressed that people should take whichever vaccine they’re offered first.
But despite those early concerns, people around the country seem eager to line up for the Johnson & Johnson shot. In addition to only requiring one dose — so people don’t have to take the time for two appointments — it can have fewer side effects than the gene-based Moderna and Pfizer / BioNTech products.
It’s hard to directly compare the Johnson & Johnson vaccine to the other vaccines. They were tested at different times and in different locations. The gene-based vaccines were tested before coronavirus variants that could make vaccines less effective were widespread. But all three vaccines are similar in one important way: they’re overwhelmingly effective at keeping people from developing severe cases of COVID-19 and out of the hospital. They’re also all more effective than the flu shot.
The single-dose formulation is also more convenient. “It’s a hassle having to take time off work,” Salome Ruperty told Spectrum News NY1 while lined up at a Johnson & Johnson vaccine site in New York City.
Some people may still turn down the Johnson & Johnson vaccine and seek out either the Moderna or Pfizer / BioNTech shots. But the early reports make it seem less likely that the doses will go unused.
Just under 4 million doses of the Johnson & Johnson vaccine were distributed to States this week. The company says it will have 20 million doses ready by the end of March and 100 million by June.
by MJ2004 I'd take any of the three options if it means getting it sooner. I'm on the "there's nothing special about me" list so I'm looking at waiting until June to vaccinated.
by JazzNU
Merck says study shows COVID-19 drug causes quick reduction in virus
(Reuters) - U.S. drugmaker Merck & Co Inc said on Saturday the experimental antiviral drug molnupiravir it is developing with Ridgeback Bio showed a quicker reduction in infectious virus in its phase 2a study among participants with early COVID-19.
“The secondary objective findings in this study, of a quicker decrease in infectious virus among individuals with early COVID-19 treated with molnupiravir, are promising,” said William Fischer, Associate Professor of Medicine at the University of North Carolina School of Medicine, in a statement from the companies.
The antiviral is being currently tested in a Phase 2/3 trial that is set to be completed in May.
Merck decided to focus on therapeutics after its two COVID-19 vaccines failed to generate desired immune responses, prompting it to abandon the program in January.
Reporting by Ann Maria Shibu in Bengaluru; Editing by Christian Schmollinger
Russia's COVID-19 death toll surpasses 200,000: Rosstat
MOSCOW (Reuters) - More than 200,000 Russians diagnosed with COVID-19 have died since the pandemic began last April, Russia’s Rosstat statistics agency said on Friday, more than double the widely cited figure used by the government’s coronavirus task force.
The figures from Rosstat suggest Russia has had the third most COVID-19 fatalities in the world, behind only the United States and Brazil.
Rosstat, which releases its figures infrequently and with a time lag, said it had recorded 200,432 deaths through January.
The government coronavirus task force’s tally, updated daily, had recorded 88,285 deaths as of Friday.
The authorities have said in the past that Rosstat’s figures are more complete, including data from autopsy reports not available for the daily tally.
Rosstat’s figure included 37,107 deaths in January, more than double the 16,064 deaths reported by the task force for the month.
Russian authorities imposed a lockdown during the first wave of the pandemic last year, but did not do so again in September when daily case numbers began to rise. Official tallies show cases falling in recent weeks and authorities have cautiously said the situation is improving.
On Friday, Moscow Mayor Sergei Sobyanin said that public transport cards for over 65s would be unblocked from Monday, although he urged people leaving their homes to visit vaccination centres.
“The situation with the pandemic is gradually improving. It is true that we are also seeing worrying signs coming from Brazil and other European countries,” he wrote on his website.
Russia has rolled out a mass vaccination campaign with its Sputnik-V vaccine, but so far only 5 million people have received a first shot, out of a population of 144 million.
Deputy Prime Minister Tatiana Golikova said deaths across the country had fallen by 21.7% in February, compared to January.
Russia reported 11,024 new cases on Friday, including 1,757 in Moscow, taking the total to 4,301,159 since the pandemic began.
Reporting by Gleb Stolyarov; Writing by Alexander Marrow; Editing by Tom Balmforth and Peter Graff
Coronavirus: Europe in vaccine race to save summer
By Kevin Connolly
BBC News, Brussels
Europe could be on the brink of a roaring twenties-style summer to remember, with budget airline flights packed and beachside bars brim-full of happy tourists.
Or, it faces another gloomy holiday season of travel restrictions, quarantine rules and a locked-down leisure industry.
In a few weeks from now we will know which it is to be - but the policy decisions which will shape the outcome are already being taken.
One big question is whether EU member states will be content to leave decision-making to the European Commission in Brussels - which has bungled the vaccine-buying programme - or simply take matters into their own hands.
Greece, for example, has already struck a deal to welcome tourists from Israel if they have a vaccine passport.
And Cyprus has said it will welcome British tourists from 1 May, as long as they have had two doses of any vaccine approved by the European Medicines Agency (EMA).
The Director-General of the Cyprus Hotels Association, Philokypros Roussonides, told the BBC: "We are really delighted with this development. It's going to be really effective and very good for airlines to schedule their flights. Cyprus is traditionally a very popular destination for British tourists."
Tourism jobs at stake
What is at stake here is not just the issue of whether wealthy northern Europeans get to enjoy a beer or an ice cream on the beach.
Tourism is big business, providing 27m jobs in Europe, and generating around 10% of the EU's GDP, when you take into account the other sectors which depend on it.
The economies of countries like Greece, Spain and Italy cannot recover until the tourist industry is reopened.
The GDP of the Balearic Islands - which include Majorca - fell by 27% last year. If a second summer season is lost to Covid-19 the consequences will be disastrous.
A tourism official in Majorca described the situation as "unsustainable" and said that if tourists were not allowed to return, many local business would disappear.
Saving the summer depends on two Europe-wide problems: getting people vaccinated and then agreeing rules about whether or not the right to travel should be linked to your vaccination status.
The chief economist of the Bank of Spain, Oscar Arce, told the Spanish newspaper El País: "If the vaccination levels are high in June, the tourist season will be saved. But if it's delayed to the end of the summer the economy will suffer a great deal. In those three months of radical uncertainty we have a lot at stake."
Slow vaccine rollout
So far at least the omens are not good.
By the end of this week only 4.96% of Belgians and 5.5% of Germans have had at least one vaccine dose.
The Politico news service produced a fascinating calculation this week, showing that if the vaccination rollout continues at the current rate, Belgium won't reach the threshold of protecting 70% of its population until July 2023.
The date calculated for Germany was September 2022.
That would suggest we should be asking about the holiday prospects for next year or the year after - not this July or August.
Now of course the Belgian and German governments - and the European Commission - would argue that the rollout is going to gather pace as supplies improve and new vaccines are approved. And so it might.
But what those figures show is that the vaccination programme so far in the EU has been a disaster. Less than 10% of the EU population has been vaccinated so far, against 31% in the UK and 52% in Israel.
The President of the European Commission, Ursula von der Leyen, admitted last month that the EU was "not where it wanted to be" on vaccinations. But German Finance Minister Olaf Scholz was widely reported to have summed things up more succinctly, telling a meeting that the EU rollout was a "total" horror show (using ruder word than "horror").
The slow vaccine rollout has been a political embarrassment for the European Commission, which took over responsibility from individual member states and then fell far behind other countries like the United States and Israel.
It cannot afford a second failure on vaccine passports, but so far the signs are not encouraging.
German Chancellor Angela Merkel has suggested that the technical work on the issue - what sort of information a passport should show and how it might be collected and stored - could be complete in three months.
But the problems with vaccine passports are political and ethical, rather than technical.
Mrs Merkel said it was not the EU's intention that only people with vaccine passports should be allowed to travel, adding "absolutely no political decisions have been made about that yet".
Discrimination fears
Some countries including France, where as many as 40% of adults may refuse a vaccination, are uncomfortable with creating rights for those who have had the jab - rights which are not available to those who have not.
Spain, desperate to get tourism moving again, has already said it won't restrict the right of entry to travellers who have been inoculated.
But if Chancellor Merkel is right, and freedom of movement is not restricted to those who have a vaccine passport, then travellers may feel there is no point in carrying one.
Huge political decisions are looming for Europe - freedom of movement is one of the founding principles of the EU.
If those decisions are going to help save this summer then the time to take them is already running short.
by dryrunguy Here's the latest Situation Report. My favorite part is the bit on Russian vaccine disinformation. Haven't I read this book before?
::
EPI UPDATE The WHO COVID-19 Dashboard reports 116.9 million cases and 2.6 million deaths as of 11:00am EST on March 9. The weekly global incidence remained steady from the previous week, with 2.70 million new cases. The weekly global mortality declined for the fifth consecutive week, down to 59,786 deaths—a 6.9% decrease from the previous week.
On March 7, Brazil surpassed the US as #1 globally in terms of total daily incidence. The US had held the #1 position since October 21, 2020, and it is still the only country to average more than 100,000; 150,000; and 200,000 new cases per day—it also fell just short of 250,000 at its highest peak (249,360 on January 11). Brazil is now reporting 66,381 new cases per day, and except for the weeks of Christmas and New Year’s, its daily incidence has increased steadily since early November 2020. Notably, Brazil’s daily incidence has increased 41% over the past 2 weeks, up from 46,921 new cases per day on February 22.
The WHO added cumulative vaccination data to its COVID-19 dashboard. In total, 268.2 million vaccine doses have been administered globally, including 156.3 million individuals with at least 1 dose. The dashboard does not yet include daily vaccinations.
Global Vaccination
Our World in Data reports that 312.2 million vaccine doses have been administered globally, an 18% increase compared to this time last week. The daily average fell slightly over the past week, from 7.2 million to 7.0 million doses (-4%). Vaccination efforts have been reported in at least 125 countries and territories.
UNITED STATES
The US CDC reported 28.81 million cumulative cases and 523,850 deaths. Daily incidence and mortality continue to decrease, but at a much slower rate than over the past several weeks. The US is averaging fewer than 60,000 new cases per day for the first time since October 20, 2020. The average mortality appears to have leveled off at slightly more than 1,700 deaths per day. As of March 4, the 806 previously unreported deaths in Los Angeles County, California, moved out of the 7-day window, which caused the average to decrease by nearly 200 deaths per day.
In addition to the overall national epidemiological trends, long-term care facilities (LTCFs) have also seen steady declines in COVID-19 incidence and mortality over the past several months, for both residents and staff. Due to the high risk of infection and severe disease, LTCFs were among the earliest priorities for SARS-CoV-2 vaccination. Through March 4, 2021, more than one-third of all US COVID-19 deaths* were among LTCF residents.
*Not including Arizona, which does not report LTCF COVID-19 deaths.
Since the start of the US vaccination effort in mid-December, weekly COVID-19 incidence and mortality has decreased substantially. At the peak (the week of December 20, 2020), the CDC reported 34,251 new cases among LTCF residents, and the weekly total has declined since then. During the week of February 28, 2021, the US reported only 1,474 new cases, a decrease of more than 95% from the peak. Similarly, the US reported 7,049 deaths among LTCF residents during the week of December 20, 2020, which fell to 1,350 the week of February 28, 2021—a decrease of more than 80%.
Beyond the residents, similar trends are evident in the LTCF staff population. At the peak (week of December 13, 2020), the US reported 29,181 new cases among LTCF staff. During the week of February 28, 2021, there were only 2,157 cases among LTCF staff, a decrease of 92% from the peak. The mortality data for LTCF staff is a little more difficult to analyze due to relatively low numbers and delayed holiday reporting, However, from the most recent peak of 63 deaths during the week of January 10, 2021, mortality fell to 26 deaths the week of February 28, 2021—a decrease of 58%.
For comparison, the national daily incidence and mortality have decreased by 77% and 49% since their peaks in mid-January 2021. The decline in weekly incidence and mortality among LTCF residents began in late December 2020, several weeks before the national epidemic peaked, and the weekly incidence peaked among LTCF staff at approximately the same time. The magnitude and timing of the COVID-19 decline in LTCF residents and staff provide evidence that the vaccination campaign is making a direct impact on this vulnerable population.
US Vaccination
The US CDC has distributed 116.4 million doses of SARS-CoV-2 vaccines and administered 92.1 million doses nationwide. In total, 60.0 million people (18.1% of the entire US population; 23.5% of the adult population) have received at least 1 dose of the vaccine, and 31.5 million (9.5%; 12.3%) have received both doses. The US continues to set new records for daily doses administered, up to 1.98 million doses per day*, including 815,748 individuals receiving their second dose. The breakdown of doses by manufacturer remains relatively steady, with slightly more Pfizer-BioNTech doses (46.8 million) than Moderna (44.9 million) administered nationwide. The CDC reported the first data for the J&J-Janssen vaccine, with 208,590 doses administered**.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
**As a 1-dose vaccine, all individuals receiving the J&J-Janssen vaccine are fully vaccinated.
The Indian Health Service (IHS) has administered 665,997 million doses, including 439,930 individuals with at least 1 dose (21.1% of the total population covered by IHS) and 219,925 individuals who have been fully vaccinated (10.6%). If IHS were a state, it would rank #9 nationally in terms of 1+ doses per capita and #13 for full vaccination per capita.
The Johns Hopkins CSSE dashboard reported 29.1 million US cases and 524,169 deaths as of 12:30pm EST on March 9.
VACCINE DISINFORMATION A spokesperson for the US Department of State’s Global Engagement Center discussed efforts by Russia to perpetuate disinformation about SARS-CoV-2 vaccines manufactured in the US. According to a report by The Wall Street Journal, the GEC identified 4 online media outlets that it believes serve as fronts for Russian intelligence agencies. These outlets have cooperated to share reports that emphasize the Pfizer-BioNTech and Moderna vaccines’ side effects, question their efficacy, and raise doubts about the accelerated development timeline. While the individual publications’ readership is small, social media platforms enable them to widely disseminate the disinformation. State Department officials did not elaborate on how the publications were controlled by Russian intelligence agencies, and the Russian government denies the allegations. An August 2020 GEC special report examined 7 disinformation proxy sites and organizations linked to the Russian government and their activities in amplifying information critical of the US and favorable to Russia, particularly related to COVID-19.
GUIDANCE FOR VACCINATED INDIVIDUALS The US CDC published guidance for individuals who have been fully vaccinated. The guidance defines fully vaccinated individuals as those who have received the full course of doses for their vaccine—i.e., 2 doses of a 2-dose vaccine or 1 dose of a single-dose vaccine—and at least 2 weeks having passed since receiving the final dose. The highly anticipated guidance provides information for vaccinated individuals regarding activities and precautions, including among other vaccinated individuals and unvaccinated individuals.
In public settings, vaccinated individuals are recommended to follow existing COVID-19 risk mitigation measures, including physical distancing (e.g., 6-foot separation) and mask use, because much of the public remains unvaccinated and still at risk for COVID-19. In private settings, fully vaccinated individuals can meet with other fully vaccinated individuals or with unvaccinated individuals from one other household without wearing masks or physically distancing, as long as all unvaccinated individuals are at low risk for severe disease. Gatherings of more than 2 households or gatherings with unvaccinated high-risk individuals should still employ COVID-19 prevention measures, such as mask use, physical distancing, enhanced hygiene, and meeting in a well-ventilated space. The CDC has not yet issued travel-related guidance for vaccinated individuals, and health officials continue to recommend against non-essential travel for everyone, regardless of vaccination status.
Vaccinated individuals do not need to quarantine or get tested if exposed to a known COVID-19 case, as long as they remain asymptomatic, with the exception of those living in congregate settings (e.g., long-term care facilities [LTCFs], correctional facilities). If a vaccinated individual does test positive or exhibit COVID-19 symptoms, s/he should self-isolate for 10 days.
In addition to the guidance itself, the CDC published information regarding the underlying evidence, including from animal studies, human clinical trials, and real-world data collected since the initiation of mass vaccination operations. The CDC emphasized that the guidance will continue to be updated as vaccination coverage increases, the epidemiological situation evolves, and researchers more fully characterize vaccine’s effectiveness, particularly with respect to the vaccines’ impact on transmission.
CANADA AUTHORIZES J&J-JANSSEN VACCINE On March 5, Health Canada authorized the J&J-Janssen SARS-CoV-2 vaccine for use in adults, making it the country’s fourth SARS-CoV-2 vaccine, along with the Pfizer-BioNTech, Moderna, and AstraZeneca-Oxford vaccines. Canada is the third country to authorize the J&J-Janssen vaccine for public use, following Bahrain and the US, and South Africa is reportedly administering it to healthcare workers as part of a Phase 3b clinical trial.
Vaccine deliveries to Canada have lagged behind many other countries, despite ordering more doses per capita than any other country. Canadian Prime Minister Justin Trudeau indicated that Pfizer has agreed to deliver 3.5 million doses to Canada in May, originally scheduled for this summer. Canada now expects to receive 36.5 million total doses by the end of June, enough to fully vaccinate nearly half of its population (38 million). To date, Canada has administered at least 1 dose to 3.6% of its population, including 1.4% who have been fully vaccinated.
J&J-Janssen has also submitted an application to the European Medicines Agency for conditional marketing authorization.
US COVID-19 STIMULUS On Saturday, the US Senate approved an updated version of the American Rescue Plan, the US$1.9 trillion COVID-19 economic relief package. The vote passed 50-49 (1 Senator absent), with all Democratic Senators voting in favor and no Republican support. The US House of Representatives is expected to vote on the new version of the bill tomorrow, and US President Joe Biden could potentially sign it this week. The Internal Revenue Service could begin distributing stimulus checks to qualified individuals as early as next week, based on the timeline for the previous round of stimulus checks.
The American Rescue Plan has gone through multiple iterations, and the current version includes US$1,400 stimulus checks for individuals earning US$75,000 or less and US$2,800 for married couples earning US$150,000 or less as well as their dependents. One notable change from previous stimulus packages is that individuals and married couples earning US$80,000 or US$160,000 or more, respectively, will not be eligible for the direct payments. The package also extends expanded federal unemployment benefits of US$300 per week through September 2021. Additionally, the federal child tax credit will temporarily increase by 50% or more per child, from US$2,000 to US$3,000 or US$3,600, depending on age. Additional funding will be allocated to support SARS-CoV-2 testing and sequencing capacity, state and local COVID-19 response activities, and small businesses.
COVID-19 THERAPEUTICS On March 2, the WHO published updated guidance for COVID-19 therapeutics. The guidance was published in The BMJ as part of an ongoing compendium of official WHO COVID-19 guidance. The WHO issued a strong recommendation against using hydroxychloroquine as COVID-19 prophylaxis. The guidance draws on results from 6 clinical trials with more than 6,000 participants, leading the WHO to conclude with “high evidence quality” that hydroxychloroquine has little or no effect in reducing the risk of COVID-19 incidence or SARS-CoV-2 infection compared, including “small or no effect” on death or hospitalization. Additionally, hydroxychloroquine has been associated with increased risk of adverse events severe enough to discontinue use of the drug.
The same day, the US NIH announced it halted a clinical trial evaluating the safety and effectiveness of SARS-CoV-2 convalescent plasma to treat emergency department COVID-19 patients with mild-to-moderate symptoms. An independent data and safety monitoring board (DSMB) concluded that while the treatment caused no harm, it was unlikely to provide any benefit to this group of patients. The DSMB recommended that NIH stop enrolling new patients for the study. According to a NIH press release, the Clinical Trial of COVID-19 Convalescent Plasma of Outpatients was being conducted at 47 hospital emergency departments across the US and had enrolled 511 of 900 intended participants.
A clinical trial conducted by researchers at the Centro de Estudios en Infectologia Pediatrica in Cali, Colombia, demonstrated that the antiparasitic drug ivermectin did not significantly shorten duration of COVID-19 symptoms among adults with mild disease. The study, published in JAMA, included nearly 400 total patients—200 randomly assigned to receive a 5-day course of ivermectin and 198 patients in the placebo group. Among the treatment group, the median time to symptom resolution was 10 days, compared to 12 days in the placebo group. Additionally, by Day 21, 82% of the treatment group had fully recovered, compared to 79% of the placebo group. Neither of these results were statistically significant, and the researchers concluded the findings do not support the use of ivermectin for the treatment of mild COVID-19 disease.
COVID-19 MORTALITY Researchers from the University of California, Irvine Medical Center (US) published findings in JAMA: Network Open from a study on outcomes of hospitalized COVID-19 patients early in the US epidemic. The study included data for nearly 200,000 COVID-19 patients from 555 hospitals across the US who were hospitalized from March 1-August 31, 2020. In-hospital mortality was strongly associated with age, with the case fatality ratio ranging from 1.4% for adults aged 18-29 years to 26.6% for adults aged 80 years and older. The researchers also analyzed the cost of care for these patients and found a median of US$10,520 for non-ICU patients and US$39,825 for those admitted to the ICU.
The overall in-hospital mortality was 13.6%, but the monthly average decreased significantly over time. In March 2020, the case fatality ratio was 22.1%, and it fell steadily to only 6.5% in August 2020. The elevated mortality early in the US epidemic illustrates the effect from both the intense patient surge on hospitals and limited initial understanding of clinical care best practices. Early in the US epidemic, the vast majority of cases were concentrated in a few major urban areas—including Boston, Detroit, New Orleans, and New York City—so while the overall national peak during the initial surge is similar to the summer 2020 peak and much lower than the fall/winter 2020 peak, the burden was concentrated in relatively few health systems, which threatened to overwhelm available resources. Additionally, many health systems faced shortages of critical equipment and supplies early in the US epidemic, including mechanical ventilators, which negatively affected patient care. As the epidemic spread across the country, the supply of critical equipment and supplies increased, and clinicians’ understanding of how to treat COVID-19 improved, the case fatality ratio decreased dramatically in hospitalized patients.
VACCINE DIPLOMACY Countries around the world continue to craft new partnerships with allies in an effort to secure adequate supply of SARS-CoV-2 vaccines for their domestic populations. Late last week, Israel, Austria, and Denmark established a joint fund for research and development and potential production of SARS-CoV-2 vaccines. The coalition aims to provide long-term stability for booster shots, in the event that emerging SARS-CoV-2 variants that reduce vaccine effectiveness become more widespread. Delays in distributing SARS-CoV-2 vaccines to EU member states may have played a role in Denmark and Austria seeking the partnership with Israel, particularly in light of the success of Israel’s national vaccination effort. Global health organizations have raised concerns over equitable global vaccine distribution during the COVID-19 pandemic, and multilateral efforts such as COVAX may not be sufficient to ensure sufficient access for lower-income countries.
Vaccine supplies and donations have been used as political tools in the past, and early vaccine distribution efforts during the COVID-19 pandemic appear to follow historical patterns and alliances. China and Russia have long been active players in the global vaccination space, fostering relationships with both neighboring and distant countries in an effort to distribute their domestically-produced vaccines. Some experts and news outlets have expressed concern that China and Russia may be overselling their vaccination resources, both in terms of efficacy and production capacity, in an effort to gain political support.
RUSSIAN VACCINE PRODUCTION Russia reportedly finalized an agreement to manufacture its Sputnik V SARS-CoV-2 vaccine in Italy. This would be the first time that the Russian vaccine would be manufactured in an EU country. The contract aims to produce 10 million doses of the vaccine in Italy by the end of 2021, leveraging the production capacity of an Italian subsidiary of Adienne, a Swiss pharmaceutical company. Italian Minister of Health Roberto Speranza indicated that he is open to introducing the Russian vaccine in Italy, but only after it receives approval from the European Medicines Agency (EMA). The EMA began a rolling review of the Sputnik V vaccine last week. Russia also announced that it is currently working on 20 additional production collaborations in Europe.
COVID-19 RISK MITIGATION The US CDC COVID-19 Response Team published findings from a study on the impact of state-level mask mandates and in-person dining restrictions on COVID-19 incidence and mortality. The study, published in the US CDC’s MMWR, evaluated county-level COVID-19 data from March 1-December 31, 2020, and compared counties in states that implemented mask mandates and restricted in-person dining to those in states without state-issued restrictions. To account for changes in state-level policies over the study period, the researchers evaluated COVID-19 incidence and mortality at multiple intervals following statewide changes—ranging from 1-20 days to 81-100 days after they took effect.
State-issued mask mandates were associated with significant decreases in both COVID-19 daily incidence and mortality. The daily incidence growth rate decreased 0.5% for Days 1-20, with the magnitude of the effect increasing over subsequent intervals, up to a 1.8% decrease for Days 81-100. The daily mortality growth rate decreased 0.7% for Days 1-20 and as high as 1.9% for Days 81-100. Similarly, lifting state-issued prohibitions on in-person dining was significantly associated with increased COVID-19 incidence and mortality, although not immediately after the policy change. The daily incidence growth rate increased by 0.9% for Days 41-60 and up to 1.1% for Days 81-100 after lifting the restrictions, and the daily mortality growth rate increased by 2.2% for Days 61-80 and 3.0% for Days 81-100. The researchers suggest that not all restaurants resumed in-person service immediately after state-level restrictions were lifted. Additionally, the public’s comfort with in-person dining may have been initially low and then increased over time following changes to state-level policy, which could potentially explain the limited effect on COVID-19 incidence and mortality soon after the changes.
dryrunguy wrote: ↑Tue Mar 09, 2021 9:09 pm
Here's the latest Situation Report. My favorite part is the bit on Russian vaccine disinformation. Haven't I read this book before?
And yet, the US Gov does not declare Russia an open enemy. It puzzles me, really.
Then again, I gather diplomats need job stability too.
by JazzNU Great news about the Indian Health Service. I hadn't heard any data on how they were doing with vaccinations.
by ponchi101 Down here.
It seems that the process is flowing better. I was talking to a friend and she tells me that there are batches of vaccines arriving daily. Not enough but the GOV has decided to do this via the health providers; as most people in Colombia have one, they are better used to dealing with vaccination programs.
Still, I may be slotted for Q4 this year. If that is the case, I gather by then the USA will be delivering on demand (walk in, pay for it, get it). In view that the anti-vaxxers are in full gear and that 70MM Americans will not believe in this, the USA may have a surplus. If so, I may decide to go to CO and get it. Most expensive vaccine ever but perhaps worth it.
by Suliso My parents in Latvia (72 and 75) might be getting their first dose either this Saturday or the next. If there are no delivery delays again...
by JazzNU
ponchi101 wrote: ↑Wed Mar 10, 2021 2:12 pm
Down here.
It seems that the process is flowing better. I was talking to a friend and she tells me that there are batches of vaccines arriving daily. Not enough but the GOV has decided to do this via the health providers; as most people in Colombia have one, they are better used to dealing with vaccination programs.
Still, I may be slotted for Q4 this year. If that is the case, I gather by then the USA will be delivering on demand (walk in, pay for it, get it). In view that the anti-vaxxers are in full gear and that 70MM Americans will not believe in this, the USA may have a surplus. If so, I may decide to go to CO and get it. Most expensive vaccine ever but perhaps worth it.
It will be slightly cheaper than you're thinking. Once you get here, you don't have to pay for it! But great to hear things are getting better there. I hope it picks up since Brazil is being all manners of reckless.
And don't let those 70 million fool you. There are definitely anti-vaxxers in that group. But a healthy portion are willing to knock over people on canes and in wheelchairs to get the vaccine immediately. They've been trying to get to any and every disadvantaged area that has been specifically targeted for rollout that they previously wouldn't step foot in if it means getting the vaccine early. I have legitimately seen people online giving instructions on "how to go to the ghetto to your vaccine." Where are you looking they ask someone else? No, no you can't look near your home they tell you. "When they say diverse, they mean the ghetto," you have to target X area to get one. Wish I was lying. It's the reason some cities have changed their criteria when targeting hard hit areas to specific zip codes on your ID rather than city residents as a whole.
ponchi101 wrote: ↑Wed Mar 10, 2021 2:12 pm
Down here.
It seems that the process is flowing better. I was talking to a friend and she tells me that there are batches of vaccines arriving daily. Not enough but the GOV has decided to do this via the health providers; as most people in Colombia have one, they are better used to dealing with vaccination programs.
Still, I may be slotted for Q4 this year. If that is the case, I gather by then the USA will be delivering on demand (walk in, pay for it, get it). In view that the anti-vaxxers are in full gear and that 70MM Americans will not believe in this, the USA may have a surplus. If so, I may decide to go to CO and get it. Most expensive vaccine ever but perhaps worth it.
It will be slightly cheaper than you're thinking. Once you get here, you don't have to pay for it! But great to hear things are getting better there. I hope it picks up since Brazil is being all manners of reckless.
And don't let those 70 million fool you. There are definitely anti-vaxxers in that group. But a healthy portion are willing to knock over people on canes and in wheelchairs to get the vaccine immediately. They've been trying to get to any and every disadvantaged area that has been specifically targeted for rollout that they previously wouldn't step foot in if it means getting the vaccine early. I have legitimately seen people online giving instructions on "how to go to the ghetto to your vaccine." Where are you looking they ask someone else? No, no you can't look near your home they tell you. "When they say diverse, they mean the ghetto," you have to target X area to get one. Wish I was lying. It's the reason some cities have changed their criteria when targeting hard hit areas to specific zip codes on your ID rather than city residents as a whole.
Jazz is correct; part of the issue is they set up mass sites in areas where people are higher risk, but the same population is also vaccine hesitant, so when the appointments go unclaimed, others travel to those areas to take a chance at jumping their spot in line.
by JazzNU The vaccine hesitant part has been overblown by the media to try to explain away the number. For the black community, at least. There are very few who wanted to go first for fear this was another guinea pig situation yet again. But after millions had taken it and there were very few issues, the hesitancy hasn't been a huge problem. I knew quite a few (I'm talking several dozens) who were hesitant about taking it in the summer and fall. I know only three who are still hesitant to take it now. And one of those three is getting vaccinated this week anyway (possibly because we may have threatened to bound and gag her and just take her to get it ourselves if she didn't go on her own - she is the very definition of high risk).
Different black doctors groups around the country have been trying to communicate to Public Health officials that the issue is not hesitancy anymore, but access. Almost every single vaccine registration that exists is online based, but not everyone has internet access. Bridging that gap is the biggest issue. Phone registrations have only recently been added to many county and state signup processes, they were non-existent at the start of this.
by Suliso Would it not be easier to go via family doctors? I assume most people, especially those on the older side, do have those.
by ti-amie
Suliso wrote: ↑Wed Mar 10, 2021 6:53 pm
Would it not be easier to go via family doctors? I assume most people, especially those on the older side, do have those.
This was my thought suliso until I found out doctors in private practice don't have it. I usually get my flu shot at Duane Reade but I'm hoping that private doctors will have access soon.
by JazzNU Private doctors would help. But plenty don't have that either, there are institutional issues here that go beyond covid. There are underserved populations that don't have as much access to doctors in their neighborhoods, have been discriminated against in healthcare settings and shy away from getting regular healthcare, and others that can't afford healthcare, so they don't necessarily have regular contact with a doctor.
I know there has been success using mobile units in many different areas. There's a program here in Philly that is spearheaded by a black doctors group. They work with church and community leaders to set up different vaccination sites in underserved communities. It's been very successful.
Private doctors have been advocating for a good 3 months to be one of the main places to get a vaccine. I haven't heard them making much progress in getting them yet. If I'm understanding the argument against it right, it would be too slow of a rollout if they went that route. That sites that can do hundreds or thousands per day are more efficient at getting us to herd immunity on the quickest timetable. I have no idea if that's true, but I understand how that might be possible.
by JazzNU Also, I should say. Private doctors can help with expediting the process many times right now, they just don't have the vaccine to administer themselves. My mom got her vaccine through her doctor technically. She had her appointment at maybe 10 AM with her doctor. He's part of a larger healthcare system with two major hospitals in the region and several health and diagnostic centers as well. Their larger hospital system does get vaccines from the state allocation, just not the individual doctors. Her doctor marked her as a very high risk (which she is, more than just her age) within their network system and asked that she get a vaccine soon. By 11 AM, she had an vaccination appointment invite in her email.
by atlpam Our governor is finally getting his act together with expansion of mass vaccination sites and expanded eligibility for those with high risk conditions as well as anyone over 55. I will be getting my 1st dose (Pfizer) on Monday.
by ti-amie
by Suliso The current top vaccine makers (Pfizer, Astra Zeneca, Johnson and Johnson, Moderna) have become household names. A friend was just invited for a final round of a job interview at AZ in a scientific position. If successful she'd move from Virginia to Gothenburg. Weird how these things happen entirely by Zoom these days. In my company as well, I wonder if the quality of our hires will be the same or higher/lower because of it.
What?!? I totally missed that that was even a possibility there. I know the vaccine rollout has been slow and they stopped that shipment from being sent to Australia, but I hadn't seen any mention of the current virus levels there.
I'm not sure if it's the same in Italy and Europe, but I'm pretty sure here there is too much laser focus on getting the vaccine and people are forgetting to make sure they don't have covid and aren't spreading it. I went for a covid test about two weeks ago and got a same-day appointment. That was just an impossibility in 2020 even when our infection rates were very low.
by atlpam
What?!? I totally missed that that was even a possibility there. I know the vaccine rollout has been slow and they stopped that shipment from being sent to Australia, but I hadn't seen any mention of the current virus levels there.
I'm not sure if it's the same in Italy and Europe, but I'm pretty sure here there is too much laser focus on getting the vaccine and people are forgetting to make sure they don't have covid and aren't spreading it. I went for a covid test about two weeks ago and got a same-day appointment. That was just an impossibility in 2020 even when our infection rates were very low.
When my husband inquired back in Jan for PCR testing prior to travel, no one would guarantee the results within 3 days due to volume. When he finally scheduled for earlier this week, they were providing results the same day. Numbers are down but probably in large part because people aren't getting tested.
by Suliso In my town they guarantee results in 24 h, usually much faster than that.
by Deuce
atlpam wrote: ↑Fri Mar 12, 2021 8:03 pm
Numbers are down but probably in large part because people aren't getting tested.
^ Indeed... this is the Trump approach - test less so that the number of positive cases decreases.
Too often, people look only at the quoted numbers, and not the circumstances behind those numbers. It happens here - and I suspect it occurs pretty much everywhere - that everyone is happy that the number of positive cases is down significantly from, say, 10 days previous... and the government is all proud... and no-one checks to see that they're testing 20,000 fewer people now than they were 10 days ago.
The government knows that fewer people were tested, of course, but they don't include the number of tests when they release the number of positive cases - they try to keep that hidden as much as they can.
by Suliso That's why you look at positivity rate which at least here is also widely reported. Right now ours is 5% which is not great, but also not terrible.
by Deuce Yes - and I do. I'm just saying that governments (at least over here) should be more transparent and give all the relevant information, rather than give only selective information and make people search for the circumstances behind those numbers via some third party.
by shtexas My brother insists he is going to the Rangers home opener. He says he will just double mask. I said you need at least one shot under you. He said with work, I can't just get off and wait at a place, etc. I set my alarm for 5 am this morning, refreshed my screen for just over an hour and got him set up. First shot Monday at 6:15 pm at CVS. He gets off work at 5:30. The CVS is maybe 15 minutes from him. Plenty of time.
by ponchi101
shtexas wrote: ↑Fri Mar 12, 2021 9:15 pm
My brother insists he is going to the Rangers home opener. He says he will just double mask. I said you need at least one shot under you. He said with work, I can't just get off and wait at a place, etc. I set my alarm for 5 am this morning, refreshed my screen for just over an hour and got him set up. First shot Monday at 6:15 pm at CVS. He gets off work at 5:30. The CVS is maybe 15 minutes from him. Plenty of time.
As always, because I was speed reading, I thought: "Oh no, Shtexas shot his brother!!!". Then I got it.
(Good for you )
by MJ2004 Our campus unexpectedly shut down this week because there were almost one hundred cases amongst students over the past two weeks.
This is a dangerous time with people feeling more at ease because of the vaccine, without actually having been vaccinated.
by ti-amie
by dryrunguy Today's Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 118.1 million cases and 2.6 million deaths as of 5:00am EST on March 12.
March 10 marked the 1-year anniversary of the WHO designating COVID-19 as a pandemic.
Global Vaccination
The WHO reported 300.0 million vaccine doses administered globally, including 180.7 million individuals with at least 1 dose. The dashboard does not yet include daily vaccinations.
Our World in Data reports that 335.4 million vaccine doses have been administered globally, a 17% increase compared to this time last week. While the daily average is still depressed compared to the previous week, down from 8.1 million to 7.1 million doses per day (-12%), the overall trend continues to increase. At least 129 countries and territories are reporting national vaccination data.
Israel continues to lead the world in most metrics related to SARS-CoV-2 vaccination, but other countries are reporting increasing vaccination volume and coverage. Cumulatively, Israel has administered 106 doses per 100 population. Israel is followed by Seychelles (89) and the UAE (65) as the only 3 countries reporting more than 50 doses per 100 population. In total, 9 countries are reporting more than 25 cumulative doses per 100 population. On a daily basis, Chile is now #1 globally with 1.4 daily doses administered per 100 population, followed by Maldives (1.3), San Marino (1.2), and Israel (1.0) as the only countries reporting 1 or more daily doses per 100 population. A total of 12 countries are administering more than 0.5 doses per 100 population per day.
As vaccination efforts expand, the data on vaccination coverage is increasing as well. Seychelles is currently #1 globally in terms of the proportion of the population that has received at least 1 dose of the SARS-CoV-2 vaccine, with 61.5%. Israel is #2, with 59.0% of its population, followed by the UAE (35.2%)* and the UK (34.0%). In total, 14 countries have reported 1-dose coverage of 10% or greater. In terms of full vaccination coverage, Israel leads all other countries by nearly double. Israel is reporting 47.0% of its population receiving 2 doses of the SARS-CoV-2 vaccine**, followed by Seychelles (27.0%) and the UAE (22.1%). Only 8 countries are reporting full vaccination coverage greater than 5%.
*The UAE has only reported data on January 10 and February 23.
**Israel is using the Pfizer-BioNTech and Moderna vaccines, both of which require 2 doses.
As COVAX continues its first allocation of SARS-CoV-2 vaccines to eligible low- and middle-income countries (LMICs) around the world, more and more countries are initiating SARS-CoV-2 vaccination efforts. With the exception of India, COVAX commenced its global vaccine distribution effort on February 24, with the first shipment arriving in Ghana. At that time, 106 countries and territories were reporting vaccinations administered. Currently, 129 countries and territories are reporting ongoing vaccination efforts. Of the 21 new countries since February 24, 19 are included in the initial COVAX allocation. A number of other countries eligible under COVAX had initiated small vaccination efforts prior to that date as well, and many of those countries have scaled up their vaccination efforts since receiving their first COVAX deliveries.
With the exception of a 1-day spike in doses on February 9, the global average for daily vaccinations remained between approximately 4.6 million and 4.9 million doses per day from January 31 to February 24. The current global average is 7.1 million doses per day, an increase of nearly 50% over a period of 2 weeks. Countries that initiated vaccination efforts prior February 24, including some COVAX countries, continue to increase their daily capacity; however, there is a noticeable change in the global trend around the time that COVAX began to distribute doses.
UNITED STATES
The US CDC reported 29.1 million cumulative cases and 527,726 deaths. Daily incidence and mortality continue to decrease, but at a slower rate than over the past several weeks. Daily mortality is down to 1,484 deaths per day, falling below 1,500 for the first time since November 30, 2020. While the current daily mortality is less than half of the peak on January 13, 2021 (3,378), it is still nearly 30% higher than the summer 2020 peak (1,147).
US Vaccination
The US CDC has distributed 131.1 million doses of SARS-CoV-2 vaccines and administered 98.2 million doses nationwide. In total, 64.1 million people (19.3% of the entire US population; 25.1% of the adult population) have received at least 1 dose of the vaccine, and 33.9 million (10.2%; 13.3%) are fully vaccinated. Among adults aged 65 years and older, 62.4% have received at least 1 dose and 32.2% are fully vaccinated.
The US surpassed 2 million doses administered per day but fell slightly below that benchmark in the most current average (1.99 million)*, including 733,733 individuals receiving their second dose. The breakdown of doses by manufacturer remains relatively steady, with slightly more Pfizer-BioNTech doses (49.7 million) than Moderna (47.7 million) administered nationwide, followed by J&J-Janssen (638,469)**.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
**As a 1-dose vaccine, all individuals receiving the J&J-Janssen vaccine are fully vaccinated.
A total of 7.5 million doses have been administered at long-term care facilities (LTCFs)***, including residents and staff. This covers 4.8 million individuals with at least 1 dose and 2.7 million with 2 doses.
***The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-Term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins CSSE dashboard reported 29.3 million US cases and 531,276 deaths as of 12:30pm EST on March 12.
EU AUTHORIZES J&J-JANSSEN VACCINE On March 11, the European Commission issued a conditional marketing authorization for the J&J-Janssen SARS-CoV-2, based on the recommendation of the European Medicines Agency (EMA). This is the fourth vaccine available in the EU, but the first 1-dose vaccine authorized in Europe. The EMA indicated that the full risk management plan and clinical data will be available in the coming days. J&J is expected to deliver 200 million doses to the EU by the end of June 2021. That contract also allows EU member states to purchase an additional 200 million doses.
COMPARING VACCINES As more data become available from Phase 3 clinical vaccine trials, it is natural to compare vaccines’ performance characteristics against each other. For example, the Mayor of Detroit, Michigan, reportedly declined a shipment of the J&J-Janssen vaccine in favor of prioritizing the Pfizer-BioNTech and Moderna vaccines. But unlike many products that have well-established standards and metrics, the clinical trials for each vaccine were designed and implemented independently, which makes direct comparison difficult. The focus on specific efficacy numbers between trials may not provide the whole picture. The relatively small numbers of severe cases and deaths in the clinical trials for all of the vaccines so far make it more difficult to evaluate their efficacy in preventing more severe forms of COVID-19, as a single case could result in major changes to the efficacy estimates.
Health officials and experts continue to emphasize the importance of vaccination, regardless of which vaccine is available: “The best vaccine is the one that’s in your arm.” This does not mean that the vaccines are identical in terms of their performance, but regardless of whether one specific vaccine is slightly more efficacious than another, any of them will provide more protection—and a high degree of protection—than no vaccine at all. And beyond the direct effect to the vaccinated individual, evidence continues to emerge that vaccination reduces the risk of infection, which could contribute to broader community protection in the form of herd immunity.
GLOBAL VACCINE ACCESS Approximately 190 countries, including 64 high-income countries, have joined the COVAX effort, which aims to distribute SARS-CoV-2 vaccines equitably to low- and middle-income countries. Many higher-income countries have made their own arrangements directly with vaccine manufacturers, including some that have secured access to considerably more doses than needed to fully vaccinate their population. In fact, 11 countries have secured enough supply to vaccinate 2.9 billion people beyond their own populations, including the US and Canada. Even as vaccine production continues to scale up, access remains largely limited to higher-income countries, posing significant questions regarding global equity and potential barriers to bringing the pandemic under control.
Several countries, such as France and Norway, already have committed to sharing their vaccine supply with other countries in the midst of their own vaccination efforts. The US has indicated it will share excess supply, but not until all Americans are vaccinated. Reportedly, Mexico requested the US share some of its current vaccine inventory, and after the request was denied, it negotiated an agreement with multiple Chinese manufacturers—including Sinovac, CanSino Biologics, and Sinopharm—to supplement its supply. But while some higher-income countries appear to be reserving much of the available supply, some LMICs are supporting their neighbors. For example, Chile donated 40,000 doses of its Sinovac vaccine supply to Ecuador and Paraguay, even though it qualifies to receive doses under COVAX.
While the US has indicated it does not intend to share its existing supply of authorized vaccines right away, the federal government reportedly has tens of millions of doses of the AstraZeneca-Oxford vaccine that it is currently unable to use. The AstraZeneca-Oxford vaccine is not yet authorized for use in the US, but it is in a number of other countries. According to multiple news media reports, there are ongoing discussions in the US government, including with AstraZeneca, regarding whether these doses can and should be donated to other countries. Officials from AstraZeneca reportedly requested the US government “loan” doses for distribution in Europe, where the company is behind schedule in fulfilling purchase agreements. Because the vaccine was developed with support from funding issued under the Defense Production Act, the doses manufactured in the US require presidential authorization before being exported.
ASTRAZENECA-OXFORD VACCINE & BLOOD CLOTTING Several countries across Europe have partially or fully suspended the use of the AstraZeneca-Oxford SARS-CoV-2 vaccine following reports of blood clotting (thromboembolic) in some vaccinated adults, including multiple deaths. The European Medicines Agency (EMA) is investigating the reports. Austria, Bulgaria, Estonia, Lithuania, Luxembourg, Latvia, and Italy have suspended the use of at least some batches of the AstraZeneca-Oxford vaccine. Additionally, Denmark, as well as non-EU members Iceland and Norway, completely suspended use of the vaccine for at least 2 weeks as EMA and national regulatory agencies conduct their investigations.
On March 11, the EMA issued a statement indicating that the available evidence does not suggest a link between vaccination and the thrombolytic conditions, noting that they are not listed as a side effect of the vaccine. As of March 10, 30 cases of thromboembolic events had been reported among nearly 5 million people vaccinated with the AstraZeneca-Oxford vaccine. The EMA’s safety committee urged countries to continue AstraZeneca-Oxford vaccination campaigns, as “the vaccine’s benefits continue to outweigh its risks.” A spokesperson for AstraZeneca emphasized that patient safety was the company’s highest priority and that peer-reviewed clinical trial data demonstrate that the vaccine is generally well tolerated.
US VACCINE EQUITY As access to SARS-CoV-2 vaccines continues to grow in the US, states are struggling with equitable distribution. Nationwide, there is a consistent pattern of disparities in vaccine coverage of racial and ethnic minority communities, particularly relative to their disproportionate burden of COVID-19 incidence and mortality. In Alabama, NPR reports that some local officials have accused the state of not distributing vaccines to Black-majority communities because of an unsubstantiated fear that the doses will go unused because of a lack of interest in getting vaccinated. In Michigan, state officials are engaged in a partisan battle over the use of the US CDC's Social Vulnerability Index—used to distribute aid following natural disasters based on economic and demographic factors—to help guide its vaccine distribution. Elected officials in some White-majority parts of the state have expressed concern that distribution based on the index has prevented older residents in their communities from accessing the vaccine, leaving them at elevated risk for severe disease and death.
But some states, like Colorado, are moving their focus to equitable distribution, with the intent to reach racial and ethnic minorities and rural residents who typically have less access to health care. Colorado plans to send 40% of its doses to local public health agencies and safety net clinics and 15% to “equity clinics,” which are located in underserved areas; provide services in multiple languages; and provide additional information on other services, such as food banks and rental assistance. California made a similar
shift this week, announcing that 40% of its vaccine allocation would be directed to 446 communities that fall in the bottom quartile of the state’s Healthy Places Index. These communities represent approximately 40% of the state’s COVID-19 cases and deaths.
BRAZIL Brazil is experiencing a deadly surge of COVID-19 incidence, with hospital ICUs nearing or exceeding capacity and daily mortality reaching record highs. While many nations are experiencing decreasing incidence and mortality, Brazil is facing its worst surge, averaging nearly 70,000 cases per day. Brazil reported a record number of COVID-19 deaths on March 10 (2,286) and surpassed the US as #1 globally in terms of daily mortality.
According to a study by the Oswaldo Cruz Foundation (Fiocruz), more transmissible and lethal SARS-CoV-2 variants of concern are now dominant in at least 6 Brazilian states, including Amazonas, where the P.1 variant first emerged. Because the virus continues to spread rapidly within the country, researchers are warning Brazil is now home to potentially hundreds of new variants, increasing the possibility of an even more dangerous variant emerging and spreading globally. President Bolsonaro continues to adamantly oppose COVID-19 risk mitigation measures, leaving state and local governments to implement their own restrictions. Some experts have also blamed President Bolsonaro for not securing more vaccine doses. With less than 2% of the population fully vaccinated, Brazil must implement more rigorous risk mitigation measures in order to bring its epidemic under control.
LONG-TERM CARE FACILITY GUIDANCE On March 10, the Centers for Medicare & Medicaid Services announced updated visitation guidance for long-term care facilities (LTCFs), developed in collaboration with the US CDC. The guidance allows for increased indoor visitation for all residents, regardless of the vaccination status of the visitor or the resident. The guidance lists 3 conditions that would limit visitation for: (1) unvaccinated residents, if the local test positivity exceeds 10% and less than 70% of facility residents are fully vaccinated; (2) residents with confirmed SARS-CoV-2 infection, regardless of vaccination status; and (3) residents who are in quarantine following a known exposure, regardless of vaccination status. While indoor visits are allowed, outdoor visits are preferred. These changes come among a continued decrease in daily COVID-19 incidence across much of the country and an increase in vaccination coverage at LTCFs.
VACCINE DISTRUST & HESITANCY In Pakistan, the legacy of fake vaccination programs conducted by the US Central Intelligence Agency (CIA)—such as the program used to locate Osama bin Laden in 2011—is reportedly contributing to vaccine distrust during the pandemic. Mistrust of vaccinators in Pakistan, stemming in part from these operations, has impacted polio eradication efforts, and it threatens to hinder SARS-CoV-2 vaccination efforts. In addition to the potential effect on vaccination coverage, vaccinators and other health workers could face risks of violence due to concerns they support intelligence services. According to an investigation by Vice, there may be more willingness among Pakistanis to accept Chinese or Russian vaccines than those developed in Europe or the US.
In Ukraine, vaccine hesitancy is reportedly stemming from concerns that government corruption and incompetence led to the distribution of ineffective or dangerous vaccines. Additionally, misinformation spread by politicians is negatively affecting perceptions of SARS-CoV-2 vaccine safety and efficacy. A nationwide survey conducted by the Kyiv International Institute of Sociology estimated that 60% of the population is unwilling to get vaccinated. Ukraine received 500,000 doses of the AstraZeneca-Oxford vaccine in late February, but it has administered fewer than 40,000 doses nationwide.
In the US, a poll conducted by Monmouth University found that 24% of respondents do not intend to get vaccinated, and another 21% indicated that they will wait for others to get vaccinated before making a decision. A majority of respondents either already received the vaccine (16%) or intend to get vaccinated when they become eligible (38%). Vaccine hesitancy among people of color declined from 22% in January 2021 to 14% in the most recent poll. There remains a stark divide along political divisions, with 36% of Republican respondents indicating that they do not intend to get vaccinated, compared to 6% among Democrat respondents.
US VACCINE SUPPLY & COVID-19 RELIEF BILL On March 11, US President Joe Biden addressed the nation and outlined the next phase of the US COVID-19 response. He expressed hope that the US can return to some semblance of normalcy by July 4th (Independence Day). Notably, President Biden indicated that he is directing all states, territories, and tribes to expand eligibility for SARS-CoV-2 vaccines to all adults by May 1. Earlier in the day, he signed the American Rescue Plan, a US$1.9 trillion bill that provides funding for vaccine distribution, stimulus checks, expanded unemployment benefits and child tax credits, SARS-CoV-2 testing, schools, and state and local governments. Additionally, the federal government plans to purchase another 100 million doses of the J&J-Janssen vaccine, which would bring the US total to 800 million doses ordered from 3 manufacturers, more than enough to fully vaccinate the entire US population. The federal distribution of the Pfizer-BioNTech and Moderna vaccines to state governments and pharmacies will increase to more than 20 million doses per week.
VACCINE EFFICACY Pfizer issued a press release that discusses effectiveness data from Israel’s vaccination program. Based on data collected from January 17-March 6, 2021, the Pfizer-BioNTech vaccine was at least 97% effective in preventing symptomatic COVID-19 cases, hospitalizations, and deaths. Furthermore, the vaccine demonstrated 94% effective in preventing asymptomatic SARS-CoV-2 infections. Notably, the data were collected at a time when the B.1.1.7 variant was the dominant circulating strain in Israel, providing further evidence that the Pfizer-BioNTech vaccine remains effective against this variant.
Novavax reported the final efficacy analysis from Phase 3 clinical trials in the UK for its vaccine candidate. The Phase 3 trials included more than 15,000 participants, including 27% over the age of 65. The vaccine demonstrated 96.4% efficacy against any COVID-19 disease caused by the original SARS-CoV-2 strain and 86.3% efficacy against the B.1.1.7 variant. Additionally, the vaccine completed Phase 2b clinical trials in South Africa, demonstrating 55.4% efficacy among HIV-negative participants in an area where the B.1.351 variant is dominant. While efficacy against the B.1.351 variant was lower, the Novavax candidate was 100% efficacious in preventing severe COVID-19 disease, including hospitalization and death, across both the Phase 3 and 2b trials. To our knowledge, the full clinical trial data has not been published publicly or subjected to peer review.
35 Million people fully vaccinated - that's essentially the entire population over here (Canada).
And 100 Million doses given...
Meanwhile, only 2.5 Million doses have been given here, and only about 6% of our population has received at least one dose.
Of course, we've managed the virus better than the U.S. did, and so haven't had nearly as many positive cases, or deaths, per capita as the U.S. has had.
But still...
VACCINE DISTRUST & HESITANCY In Pakistan, the legacy of fake vaccination programs conducted by the US Central Intelligence Agency (CIA)—such as the program used to locate Osama bin Laden in 2011—is reportedly contributing to vaccine distrust during the pandemic. Mistrust of vaccinators in Pakistan, stemming in part from these operations, has impacted polio eradication efforts, and it threatens to hinder SARS-CoV-2 vaccination efforts. In addition to the potential effect on vaccination coverage, vaccinators and other health workers could face risks of violence due to concerns they support intelligence services. According to an investigation by Vice, there may be more willingness among Pakistanis to accept Chinese or Russian vaccines than those developed in Europe or the US.
Yikes!
by ti-amie Why are they always shocked when no one comes to their aid?
by JazzNU
by Deuce
ti-amie wrote: ↑Sat Mar 13, 2021 7:43 pm
Why are they always shocked when no one comes to their aid?
^ The woman was obviously being stupid and arrogant, and was clearly in the wrong.
But the cop used excessive force. Other than her not wearing a mask, she was no threat to him, or to anyone else physically. Apart from the possibility of the virus exiting from her mouth, no-one in the vicinity was in any physical danger from her. She was moving toward the door when he pushed her to the ground. What he did was entirely unnecessary.
Another example of a cop abusing his authority - because he knew he could get away with it. Until cops face real consequences for this type of thing, it will continue.
by JazzNU No, that's the textbook definition of resisting arrest. There was no excessive force used. There is no abuse of authority. Letting her walk out after deciding he was placing her under arrest would've been special treatment. Not arresting or charging her because she was no longer causing harm to others even though she had already broken the law, would also have been special treatment.
by Deuce (Removed expletive)
I have no idea what you were watching, but in the video that I watched, he was asking her to go outside, and only threatened to arrest her if she didn't go. She wasn't resisting arrest when he tackled her, because she wasn't under arrest. After a minute or so of stupid arguing, she was headed toward the door. And it looked like he simply decided she wasn't moving fast enough, or he got upset with what she was saying, so he tackled her.
That makes him an idiot in my book.
The police always use "Resisting arrest" as an excuse for their excessive and unnecessary violence. George Floyd was "resisting arrest"... sigh...
Again - she was no physical threat to anyone. She had no weapon. She was headed toward the exit. The only reason for a cop to tackle someone is if they are a physical threat. Other than that, maybe very lightly guide the person toward the door...
The bottom line is that cops who are power hungry or who are too stupid to talk out a peaceful resolution resort to unnecessary physical violence (under the false claim of 'resisting arrest'). It happens several times every day, sadly.
And, by the way, to ME, it matters not what nationality or colour a person is - I despise when police abuse their authority - period.
by Suliso That woman clearly needed to be charged BUT tackling of anyone by the police is an absolute no go in my opinion unless there is a damn good reason (I mean really good not imaginary) to think that the person is armed AND dangerous. US police is way too violent with non violent offenders.
by ti-amie I applaud the actions of the police officer. He was firm, told her what her options were, and she was still in his face. I think she was expecting the other customers to come to her defense and was left to her own devices which, to me, was to provoke the policeman. People have been tasered, shot and/or arrested for half of what she did.
It's ironic that the people who were screaming "blue lives matter" are now out to try and provoke and as we saw on 1/6 harm officers.
by Deuce
ti-amie wrote: ↑Sat Mar 13, 2021 11:24 pm
I applaud the actions of the police officer. He was firm, told her what her options were, and she was still in his face. I think she was expecting the other customers to come to her defense and was left to her own devices which, to me, was to provoke the policeman. People have been tasered, shot and/or arrested for half of what she did.
So... cops reacting violently to provocation is ok in your book? I thought cops were supposed to be above that. Sigh...
The cop was brought in to the situation because the woman wasn't wearing the required mask and refused to leave the establishment. Fine. His job is then to get her to leave the place. He was trying to do that. Fine. Once she is outside, the cop can rationally assess the situation, talk with others, and decide whether to charge her or not.
She was arguing stupid nonsense with him - which he should expect. After about a minute of this stupid arguing, she was headed toward the door - to leave the establishment, which was the goal. At this point, everything is fine and under control. Then he decides to jump on her.
Just because you don't like someone, or because they are being belligerent, or arrogant, or stupid, does not give anyone - including cops - the right to tackle the person.
Again - the only reason for police to use physical force is when there is a physical threat to them or to people in the vicinity. Police are not allowed to use physical violence just because they don't like someone, or just because someone is rude, or because they don't like the way that the person is behaving. Isn't this exactly what the entire 'Black LIves Matter' protests against the police have been about?!?!
I have no doubt that if the woman in this video were black, not too many people would say that what the cop did was justified.
Welcome to America and its ever-changing double standards.
Again - she was headed toward the door when he tackled her. That's assault.
Sigh...
by mmmm8
Suliso wrote: ↑Fri Mar 12, 2021 7:43 pm
The current top vaccine makers (Pfizer, Astra Zeneca, Johnson and Johnson, Moderna) have become household names. A friend was just invited for a final round of a job interview at AZ in a scientific position. If successful she'd move from Virginia to Gothenburg. Weird how these things happen entirely by Zoom these days. In my company as well, I wonder if the quality of our hires will be the same or higher/lower because of it.
A friend of mine (formerly from the tennis media!) has just a couple months ago started at AZ. Her background is scientific but the job I think is in project management, and likely related to the vaccine rollout. She's based in the DC area, I think her office is in Maryland.
As a side note, I really liked Gothenburg. A bit small, but very laid-back city.
by dryrunguy At some point, the New York Times opened its Primal Scream Line for mothers feeling overwhelmed by their children due to the impacts of COVID. There are lots of interesting data in this piece, too. This was published back in early February.
by ponchi101 Wow. This ties up to the brief topic we had a while back regarding parenting. Not for everybody, as the effort is so herculean.
I know that if I had kids I would be under heavy sedation, either clinically or by Jose Cuervo. No work, no income, no immediate solution. That would put me over the edge. It ties up to the rescue plan the GOP voted against. One has to wonder how many people simply are facing at a bank account that reads "Balance = $0.00", and that have kids. I truly would not know how to deal with something like that.
by ti-amie
by JazzNU I think that's over 10 countries now. But there's no evidence of it not being safe. The incidence of the blood clots is not statistically significant.
There is a Russian misinformation campaign to undermine confidence in Western vaccines and you've got to wonder if they are succeeding at least somewhat.
by ponchi101 Again: you are vaccinating millions of people, mostly elderly and people with previous conditions. Of course you are going to have people coming with "reactions" that are not related to the vaccine.
But: when you have a population that rejects science as an explanation, this is expected.
Give me the AZ vaccine. I'll take it.
by Deuce Well, I won't take the AstraZeneca. Because no-one knows when we'll be able to take the next vaccine after we get the 2 doses of AZ.
We might have to wait a full year to get the next shot... So, during that year, I want to have the best vaccine available in my body - the one with the highest efficacy, and one where no significant side-effects are suspected, and which hasn't been pulled by several countries. This is only logical.
ponchi101 wrote: ↑Mon Mar 15, 2021 3:02 am
Again: you are vaccinating millions of people, mostly elderly and people with previous conditions. Of course you are going to have people coming with "reactions" that are not related to the vaccine.
But: when you have a population that rejects science as an explanation, this is expected.
Give me the AZ vaccine. I'll take it.
I'm not rejecting science in saying I don't want the AZ shot... on the contrary - I'm saying that I want the best science available.
Yes, millions of people are being vaccinated - with 5 or 6 different vaccines. But only one of those vaccines is potentially causing problems; only one of those vaccines is being pulled from use by a growing number of countries.
So I want one of the vaccines that isn't suspected of possibly causing problems, and isn't being pulled by various countries. Again - I view this as being perfectly logical.
As well, in addition to the mentioned problems, the AZ has a lower efficacy rate for preventing the virus than do the other vaccines available to me.
All of this combined makes it an easy and obvious choice.
by ponchi101 The sample of people with "issues" for the AZ vaccine is not significant.
So the countries that are pulling the vaccine off are not looking at the data properly. It is exactly what I am saying: you are vaccinating an elderly population, by the millions. Of course some people are going to wake up the next day with some medical issues; by definition, they are a population more susceptible to having those.
YOU can decide which vaccine to get or not. The Governments cannot look at YOU, or for that matter, any other anecdotal data. They have to look at the population as a whole in order to make proper public policy.
by Deuce Obviously the (growing number of) countries who are pulling the AZ vaccine from use believe that there is a possible problem. Maybe it's a big conspiracy... and maybe not. There may or may not be an actual problem with the AZ vaccine - hopefully an honest investigation will reveal the answer. But as long as other options are available, I think it's only logical to choose one of the vaccines which is not being investigated for possible problems - and this is true for individuals as well as for countries.
Obviously, the growing number of countries who have pulled the AZ vaccine agree with this.
I'm not saying that the AZ vaccine causes blood clots. And I'm not saying that it doesn't. Because I don't know. But what I do know is that none of the other vaccines are suspected of possibly causing blood clots.
Essentially, it's a matter of 'better safe than sorry'.
Also, I had decided I don't want the AZ vaccine before any mention of the blood clots. My decision was made based on the lower efficacy of the AZ vs. the others. Again - if I have a choice between 62% efficacy and 94% efficacy, I'll take the 94% - especially with something that involves the potential for serious illness or death.
I use this approach with less important things, too - if I have a choice between tennis shoes which will last me 3 months and tennis shoes which will last me one year, all other elements being equal, I'll choose the shoes that will last me one year.
by dryrunguy Here's the most recent Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 119.8 million cases and 2.7 million deaths as of 5am EDT on March 16. Global weekly incidence increased for the second time in 3 weeks*, up to 3.0 million new cases. This represents a 10.4% increase over the previous week. Global weekly mortality continues to decline for the seventh consecutive week. Mortality fell to 59,031 deaths, a 3.33% decrease from the previous week.
*The weekly incidence last week remained essentially consistent with the previous week (-0.15% change).
Global Vaccination
The WHO reported 325.6 million vaccine doses administered globally, including 190.7 million individuals with at least 1 dose. The dashboard does not yet include daily or weekly vaccinations.
Our World in Data reports that 381.3 million vaccine doses have been administered globally, a 22% increase compared to this time last week. The daily average is approaching 10 million doses per day. The current average of 9.7 million doses per day is a 37% increase compared to a week ago. At least 133 countries and territories are reporting national vaccination data.
UNITED STATES
The US CDC reported 29.3 million cumulative cases and 532,355 deaths. After several weeks of steady decline, the national daily incidence appears to have leveled off to some degree. The current 7-day window includes March 8, when Missouri reported more than 81,000 previously unreported cases, so the current average is still artificially inflated. We expect the actual average is closer to 55,000 new cases per day. This would indicate that daily incidence is still decreasing, but more slowly than it was previously. Daily mortality continues to decrease steadily, down to 1,212 deaths per day—the lowest average since November 15, 2020.
US Vaccination
The US CDC surpassed 100 million SARS-CoV-2 vaccine doses administered on March 9. In total, the US has distributed 135.8 million doses of SARS-CoV-2 vaccines and administered 109.1 million doses nationwide. This includes 71.1 million people (21.4% of the entire US population; 27.5% of the adult population) who have received at least 1 dose of the vaccine, and 38.3 million (11.5%; 14.8%) who are fully vaccinated. Among adults aged 65 years and older, 64.1% have received at least 1 dose and 35.9% are fully vaccinated.
The US once again surpassed 2 million doses administered per day*, including 829,356 individuals fully vaccinated (i.e., second dose of a 2-dose vaccine or a single dose of a 1-dose vaccine). Broken down by manufacturer, both the Pfizer-BioNTech and Moderna vaccines surpassed 50 million cumulative doses, and the J&J-Janssen vaccine is approaching 1.5 million doses**.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
**As a 1-dose vaccine, all individuals receiving the J&J-Janssen vaccine are fully vaccinated.
As the US SARS-CoV-2 vaccination program continues to scale up, vaccination administration and coverage are becoming more even between states. Currently, the median state-level doses delivered is 41,289 doses per 100,000 population, and most states are within approximately 5% of that total. In terms of doses administered, the median state-level total is 34,066 doses per 100,000 population. The variation is only slightly larger for administered doses, with most states falling within 7-8% of that total.
With respect to distributed doses, only Utah (35,715) has received less than 90% of the median value. With respect to doses administered, only Alabama (26,644), Georgia (26,278), and Tennessee (28,589) are reporting less than 85% of the median. Notably, South Dakota and Alaska have received 26.1% and 56.4% more than the median value, respectively. Both states are also among the top 3 in terms of doses administered, with Alaska at #1 (35.3% more than the mean), New Mexico at #2 (+33.4%), and South Dakota (+25.6%). Similarly, the median proportion of doses administered—i.e., out of the number of doses received—is 82.4%, and most states fall between 78.5-85.9%. In total, 5 states have administered more than 90% of their received doses, including Washington state at #1 with 94.3%. At the other end of the spectrum, Alabama (68.1%) is the only state to administer fewer than 70% of its doses.
Looking at actual vaccination coverage (i.e., the proportion of the population that has been vaccinated), most states are within 6-8% of the median values. With respect to individuals who have received at least 1 dose of the vaccine, the median coverage is 22.2% of the total state population. Most states fall between approximately 20.5-24%. Eight states are reporting greater than 25% coverage for at least 1 dose, including New Mexico (29.3%), Alaska (28.1%), and South Dakota (27.6%). Ten states are reporting less than 20% coverage, including Tennessee (18.5%), Alabama (17.4%), and Georgia (15.9%). Trends in full vaccination coverage are fairly similar. The median coverage is 12.3%, and most states fall between approximately 11.25% and 13%. Alaska (18.1%), New Mexico (16.9%), and South Dakota (15.6%) are the only 3 states reporting full vaccination coverage greater than 15%, and Texas (9.9%), Tennessee (9.8%), Georgia (9.8%), and Utah (8.3%) are the only states reporting less than 10% coverage.
With respect to older adults, states are reporting wider variation in terms of vaccination coverage. Looking specifically at full vaccination for adults aged 65 years and older, the median coverage is 36.3%, and most states fall between approximately 32.5-41.5%. At the upper end, 2 states have fully vaccinated more than half of their older adult population: Alaska (55.6%) and Indiana (50.1%). At the other end of the spectrum, Oregon (21.8%) and Rhode Island (21.4%) are the only 2 states that have fully vaccinated less than a quarter of their older adult population.
ASTRAZENECA-OXFORD VACCINE & BLOOD CLOTTING Multiple countries in Europe—including Germany, Italy, France, Spain, the Netherlands, Norway, Iceland, Ireland, Denmark, Bulgaria, Sweden, and Latvia—have temporarily suspended use of the AstraZeneca-Oxford SARS-CoV-2 vaccine due to reports of blood clots occurring in a small number of vaccinated individuals. The suspensions are creating additional challenges for vaccination campaigns across Europe, as the region faces a third surge. AstraZeneca has reported 15 events of deep vein thrombosis and 22 events of pulmonary embolism in vaccinated individuals as of March 8.
The European Medicines Agency (EMA) and the WHO will meet today to review data on the vaccine and blood clotting. The EMA then plans to hold a meeting on March 18 to discuss the findings of their investigation and announce any resulting recommendations. A WHO spokesperson noted the agency thus far has not received reports of blood clotting events outside of Europe. In a press release on March 14, AstraZeneca said a review of data from 17 million vaccine recipients in Europe and the UK demonstrated “no evidence of an increased risk of pulmonary embolism, deep vein thrombosis (DVT) or thrombocytopenia, in any defined age group, gender, batch or in any particular country.” As the EMA and the WHO investigate the reports, the agencies continue to advise there is no evidence the AstraZeneca-Oxford vaccine has caused the blood clotting events and that the benefits of the vaccine outweigh the potential risks of adverse events.
GLOBAL VACCINE ACCESS & PRODUCTION US President Joe Biden is under increasing pressure to share the nation’s SARS-CoV-2 vaccine supply with other countries. On Friday, President Biden met virtually with the leaders of Japan, India, and Australia—members of the Quadrilateral Security Dialogue, an alliance to address mutual concerns about China—and agreed to work together to increase production of SARS-CoV-2 vaccines in India to bolster the Indo-Pacific region’s supply. The summit committed to supplying at least 1 billion vaccine doses to the region by the end of 2022. Though not the focus of the agreement, the leaders hope these efforts will challenge China’s growing influence in the region and other parts of the world, as China’s ability to produce millions of vaccine doses and ship them to low- and middle-income countries has offered it advantages in terms of strengthening diplomatic and economic relations.
ITALY LOCKDOWN Italy is reinstating lockdown measures in order to curb Europe’s potential third wave of COVID-19. The measures came into effect on March 15 and are set to last through April 6, spanning the upcoming Easter holiday weekend. Unlike previous national lockdowns, not all areas of the country will be subject to the same measures, based on their risk level. Italy’s regions are broken down into 4 levels—red, orange, yellow, and white—with red being the highest level of risk and white being the lowest level of risk. Red zone regions will be subject to the most restrictive lockdown measures, including stay-at-home orders (except for essential work or shopping), closure of non-essential businesses, and suspension of indoor and outdoor activities. Additionally, Italy is strengthening measures in yellow and orange zones to include restrictions previously designated for the next higher level.
Approximately half of Italy’s regions are currently in the red zone, including Rome, Milan, and Venice. The risk classifications are subject to regular review, but areas with more than 250 weekly cases per 100,000 population will be classified automatically as a red zone. Additionally, all regions will be subject to red zone measures over the Easter weekend, April 3-5, in order to limit travel and family gatherings during the holiday. The nationwide mask mandate remains in effect, as well as a national curfew from 10pm-5am.
Italy is not the only European country attempting to stave off a third wave. Germany’s daily incidence appears to be rising, and hospitals in Hungary are mobilizing surge capacity to combat a COVID-19 patient surge.
COMBATING VACCINE HESITANCY As we have covered previously, vaccine hesitancy remains a major challenge during the COVID-19 pandemic. Existing hesitancy toward routine immunizations is compounded by skepticism regarding the pace of research, development, and testing for the novel SARS-CoV-2 vaccines as well as apathy and concerns regarding inequitable access. In an effort to combat vaccine hesitancy in the US, the White House is reportedly implementing a nationwide public relations campaign with the hope of influencing both those who are opposed to SARS-CoV-2 vaccination and those who remain uncertain whether they should get vaccinated.
According to a report by STAT News, the US$1.5 billion effort will target younger individuals, who may not view themselves as being at risk for COVID-19; racial and ethnic minorities, who may face barriers to accessing the vaccine and mistrust of government; and those on the conservative end of the political spectrum, who may not view COVID-19 as a threat or may oppose the Biden Administration on political grounds. While the program will be initiated at the federal level, the plan includes a significant focus on supporting local community outreach efforts. And while much of the initiative’s funding comes from the most recent COVID-19 funding package, the White House already has pledged an additional US$500 million from other sources for education and outreach programs, including those aimed at racial and ethnic minorities and other underserved communities.
FACEBOOK VACCINE ACCESS & VACCINE HESITANCY Beyond outreach and education efforts by national, state, and local governments and community organizations, social media platforms also are beginning to recognize their role in combating vaccine hesitancy. On March 15, Facebook announced plans for a global campaign to support SARS-CoV-2 vaccination. The company will now add labels and links to official information (eg, from the WHO) on Facebook and Instagram posts discussing SARS-CoV-2 vaccination. In addition to providing updated, factual information about the vaccines, Facebook’s Covid Information Center will add a tool to help individuals schedule vaccination appointments. Facebook also is partnering with national governments to support communication efforts via WhatsApp, including official notifications to inform individuals they are eligible to schedule vaccination appointments.
Facebook is also conducting internal research on the spread of vaccine hesitancy and misinformation via its various social media platforms. The research includes an examination of both vaccine hesitancy-related content as well as the social networks through which misinformation spreads. Preliminary analysis found that only a small portion of the users and networks on Facebook platforms engage in the majority of vaccine hesitancy content. In fact, 10 of 638 “population segments” analyzed contained half of all vaccine hesitancy content, and in the most prominent segment, only 111 users were responsible for half of the vaccine hesitancy content—out of more than 3 billion users worldwide. In partnership with Carnegie Mellon University and the University of Maryland, Facebook is providing data and analysis of SARS-CoV-2 vaccine hesitancy trends that can support government efforts to implement effective outreach campaigns.
J&J-JANSSEN VACCINE WHO EMERGENCY USE LISTING On March 12, the WHO issued an emergency use listing for the J&J-Janssen SARS-CoV-2 vaccine. The WHO made the designation only one day after the European Commission authorized the vaccine, with WHO and outside evaluators using an “abbreviated assessment” based on the review by the European Medicines Agency (EMA). In addition to the EMA review, the WHO considered quality, safety, and efficacy data and suitability requirements for low- and middle-income countries, including cold chain storage and risk management plans. The J&J-Janssen vaccine is the first single-dose vaccine to receive emergency use listing by the WHO, which should help facilitate vaccination campaigns in many countries, according to the agency. The WHO also has listed the Pfizer-BioNTech and AstraZeneca-Oxford vaccines for emergency use.
US SECOND-DOSE VACCINATION COVERAGE Researchers from the US CDC COVID-19 Response Team published findings from a study on the proportion of vaccinees who received their first dose of a SARS-CoV-2 vaccine that went on to receive their second dose. The study, published in the US CDC’s MMWR, included 2 analyses based on data from more than 40.5 million first doses of the Pfizer-BioNTech and Moderna vaccines administered December 14, 2020-February 14, 2021. Current guidance recommends that Pfizer-BioNTech vaccine recipients receive their second dose 21 days after their first dose and that Moderna recipients receive their second dose 28 days after their first dose. However, individuals may receive their second dose up to 42 days after their first dose for either vaccine, if a delay is unavoidable. Among vaccinees who received their first dose, 88% received the second dose within the recommended timeframe, and 8.6% had not received the second dose but had not yet reached Day 42. Among all individuals who received both doses, 95.6% completed the vaccination series within the allowable time.
The researchers noted differences among jurisdictions and demographic groups and recommended that public health officials identify and address challenges to receiving a second dose to ensure equitable distribution. Some of their recommendations include scheduling an appointment for a second dose at the time of first-dose administration, rescheduling any cancelled vaccination clinics, and sending appointment reminders to first-dose recipients.
US CDC CHILDCARE GUIDANCE Following its issuance of updated COVID-19 guidance for schools, the US CDC published revised recommendations for childcare programs. The new guidance, published on March 12, includes updates regarding mask use for younger children, cohorting and staggering children’s schedules, communal spaces and playgrounds, and ventilation. The guidance is intended for a broad range of childcare settings, including dedicated childcare facilities, pre-kindergarten and Head Start programs, and home-based services, and it includes specific guidance for children with disabilities or special needs as well as individuals, including staff, at elevated risk for severe disease and death. In addition to the guidance itself, the CDC discusses evolving evidence regarding SARS-CoV-2 transmission risk in childcare settings and COVID-19 disease risk in children.
The new guidance increases the emphasis on mask use by all children 2 years and older, except when eating or sleeping, and reinforces consistent and proper use by children. The new guidance reiterates that mask use should be used in combination with proper physical distancing, not as a substitution. The guidance also discusses vaccination for childcare staff, noting that childcare workers are covered in the federal Phase 1b vaccination priority group guidance as essential workers as well as the recent Department of Health and Human Services directive to states to expand eligibility to educators. The guidance also reiterates that COVID-19 risk mitigation measures need to remain in place even after childcare personnel are vaccinated.
COMMUNIVAX WEBINAR The Johns Hopkins Center for Health Security is hosting a webinar as part of the CommuniVax initiative to discuss recommendations from its first report on engaging communities of color to promote equity in SARS-CoV-2 vaccination. The webinar will include presentations by Dr. Monica Schoch-Spana from the Johns Hopkins Center for Health Security, Lois Privor-Dumm from the Johns Hopkins International Vaccine Access Center, Dr. Stephen B. Thomas from the Maryland Center for Health Equity, and Ysabel Duron from The Latino Cancer Institute, with Dr. Emily Brunson from Texas State University as moderator. The webinar will be held on Thursday, March 18 at 2pm EDT. Advance registration is required.
atlpam wrote: ↑Tue Mar 16, 2021 8:10 pm
Got my first Pfizer dose yesterday!
I believe you mean your pfirst Pfizer...
When you received that pfirst shot, did you automatically get an appointment for your 2nd shot?
by dryrunguy Well, I can't NOT share this gem.
by ti-amie
dryrunguy wrote: ↑Wed Mar 17, 2021 12:17 am
Well, I can't NOT share this gem.
I literally spit my food out.
by dryrunguy From beginning to end, that was one of the best Golden Girls episodes ever.
by the Moz
dryrunguy wrote: ↑Wed Mar 17, 2021 12:43 am
From beginning to end, that was one of the best Golden Girls episodes ever.
Oh Frieda Claxton. Bless her!
by ti-amie
(...)
by dryrunguy From the very beginning of this pandemic, I worried about Brazil. That wasn't an irrational fear in itself. But the degree to which I worried about Brazil OVER other countries and regions of the world was completely irrational.
I know it's a crazy thing to even hope for, but I hope Bolsanaro suffers miserably for his dereliction of duty.
I'm going back and forth every 5 minutes over whether or not the cumulative nature of complete and utter inaction in Brazil potentially DOES fall into the category of a genocide. I bristle when I see that word. But when it's all said and done, genocides do not necessarily need to involve armies and guns. (I still haven't ruled out that may be precisely what happened in the United States in 2020.)
by ti-amie If Brazilians are calling it a genocide I'll go with what they're saying.
Was the same thing attempted here? I don't think it's out of the realm of possibility.
by ponchi101 I would prefer a different word. Genocide has a specific connotation which, if we extend it, may start losing meaning and purpose.
I do not deny that Bolsanaro is guilty of a major crime. I just don't want to compare this with Rwanda, Armenia and the current genocides in China and, recently, Myanmar.
by dryrunguy
ti-amie wrote: ↑Wed Mar 17, 2021 3:31 am
If Brazilians are calling it a genocide I'll go with what they're saying.
Was the same thing attempted here? I don't think it's out of the realm of possibility.
I am pretty sure I alluded to it at least once before--almost certainly on the old board.
But I never thought it was a coincidence that people of color in the United States were being disproportionately affected by COVID, from the very beginning of the pandemic, both in terms of COVID morbidity but especially in COVID mortality, and the policy stances that were taken by the previous administration. Even as COVID moved into poor white rural areas, it is quite conceivable the previous administration saw the demographic shift as simply expanding into another disposable population--even if we're talking about their voting base--because the rural white population in the United States is overwhelmingly older (Social Security, Medicare, Medicaid) and poor (Medicaid, food stamps, welfare, unemployment, etc.).
To be clear, I'm not saying I am convinced of it. I'm only saying I cannot rule it out. And I won't be at all surprised if someone squeals in a tell-all book (which may or may not be believable) or as federal documents/emails are made public.
But if we had a global pandemic that disproportionately affected millionaires or billionaires, we'd be all over it.
atlpam wrote: ↑Tue Mar 16, 2021 8:10 pm
Got my first Pfizer dose yesterday!
I believe you mean your pfirst Pfizer...
When you received that pfirst shot, did you automatically get an appointment for your 2nd shot?
I did not, but they said I will receive an email in 2 weeks with a link to schedule my 2nd dose.
A friend went to the same vaccination site a week or so ahead of me, so she should be receiving her email soon if the process is working.
When my son got his first dose, they did schedule the second at that time.
by Deuce
atlpam wrote: ↑Wed Mar 17, 2021 3:40 pm
I did not, but they said I will receive an email in 2 weeks with a link to schedule my 2nd dose.
A friend went to the same vaccination site a week or so ahead of me, so she should be receiving her email soon if the process is working.
When my son got his first dose, they did schedule the second at that time.
So your son got vaccinated before you did?
Is he a front line worker of some sort? Or is the vaccine priority not at all done by age where your son is?
atlpam wrote: ↑Wed Mar 17, 2021 3:40 pm
I did not, but they said I will receive an email in 2 weeks with a link to schedule my 2nd dose.
A friend went to the same vaccination site a week or so ahead of me, so she should be receiving her email soon if the process is working.
When my son got his first dose, they did schedule the second at that time.
So your son got vaccinated before you did?
Is he a front line worker of some sort? Or is the vaccine priority not at all done by age where your son is?
Yes, he is in an essential worker category - he's an air traffic controller.
by ponchi101 It is starting to happen.
Received a possible call for a job, which I will not get*, and one of the conditions is "Covid Vaccinated".
I believe a bit too early to "demand" that you have the vaccine. It is still not like I can go to the local health provider, stand in line and get it.
Off Topic
* Won't get it because I know the company (Repsol) and they always do the same: they go out on a tender because it is in their manuals, but then they stick to their 5-6 Spaniards which are the only ones they hire. Don't have a problem with that except that they are not honest and people have to work to present the bid. Guess it keeps them in their jobs.
by Deuce
ponchi101 wrote: ↑Thu Mar 18, 2021 2:23 pm
It is starting to happen.
Received a possible call for a job, which I will not get*, and one of the conditions is "Covid Vaccinated".
I believe a bit too early to "demand" that you have the vaccine. It is still not like I can go to the local health provider, stand in line and get it.
Given that several million people worldwide have been vaccinated now, I think it's fair that any company ask that applicants for a job be vaccinated. That's a pretty large pool from which to select.
It may not seem fair to those who've not yet been vaccinated... but such is life. There are plenty of other conditions for getting jobs, or for every day life - not everyone is given the same opportunity... only people with a valid driver's licence are permitted to drive, for example.
From the employer's perspective, it makes sense. If they have a choice between a vaccinated person and a non vaccinated person, they'll choose the vaccinated person in order to create a safer workplace. That's less trouble and less costly than testing the employees every 3 days.
Makes sense to me.
by ponchi101 It rules out almost all personnel in South America and Africa. We all are under 70 and, by job description, without underlying conditions, by and large.
Guess that since it affects me directly, my myopia increases.
by Suliso Depending on when the job is supposed to start it rules out almost everyone from EU too.
by JazzNU
Experts: Virus surge in Europe a cautionary tale for US
By JOHN SEEWER and CARLA K. JOHNSON
Optimism is spreading in the U.S. as COVID-19 deaths plummet and states ease restrictions and open vaccinations to younger adults. But across Europe, dread is setting in with another wave of infections that is closing schools and cafes and bringing new lockdowns.
The pandemic’s diverging paths on the two continents can be linked in part to the much more successful vaccine rollout in the U.S. and the spread of more contagious variants in Europe.
Health experts in the U.S., though, say what’s happening in Europe should serve as a warning against ignoring social distancing or dropping other safeguards too early.
“Each of these countries has had nadirs like we are having now, and each took an upward trend after they disregarded known mitigation strategies,” said Dr. Rochelle Walensky, director of the U.S. Centers for Disease Control and Prevention. “They simply took their eye off the ball.”
The result has been a sharp spike in new infections and hospitalizations in several European countries over the past few weeks.
Poland’s rate of new COVID-19 cases has more than doubled since February, straining its health care system and leading to a three-week nationwide lockdown announced Wednesday for shopping malls, theaters, galleries and sports centers.
Italy closed most of its classrooms at the beginning of this week and expanded areas where restaurants and cafes can do only takeout or delivery. The country’s health experts say they’re seeing an increasing number of patients who are middle-aged and younger.
In France, officials imposed weekend lockdowns around the French Riviera in the south and the English Channel in the north, and are preparing new restrictions for the Paris region and perhaps beyond to be announced Thursday.
COVID-19 patients occupy 100% of standard intensive care hospital beds in the area surrounding the nation’s capital.
“If we don’t do anything, we’re heading toward catastrophe,” Remi Salomon, a top official in the Paris public hospital authority, told BFM television.
Serbia announced a nationwide lockdown for the rest of the week, closing all nonessential shops and businesses. The country of 7 million people reported more than 5,000 new cases on Tuesday, its highest number in months.
The trends are far more encouraging in the U.S., which has recorded about 537,000 deaths overall, more than any other country.
Deaths per day in the U.S. have plunged to an average of just under 1,300, down from a high of about 3,400 two months ago. New cases are running at about 55,000 per day on average after peaking at more than a quarter-million per day in early January.
An empty hallway and a row of unused face shields inside the closed COVID-19 ICU unit at Mission Hospital in Mission Viejo, California, tell the story of the improved outlook in the U.S.
The wing was teeming with the patients at the beginning of the year.
“It gives me goosebumps. It’s really just surreal because, you know, a month and a half ago, our unit was full of super, super sick COVID patients, many of which didn’t survive,” said ICU nurse Christina Anderson.
The European Union’s overall vaccination efforts lag far behind those of Britain and the U.S because of shortages and other hurdles. Roughly 1 in every 5 people in the U.S. has received at least one dose, while in most of the European countries, it’s fewer than 1 of every 10.
In another troubling turn, many European countries — including Germany, France, Spain and Italy — have suspended use of AstraZeneca’s COVID-19 vaccine over reports of dangerous blood clots in a small number of recipients, though regulators say there is no evidence the shot is to blame.
European nations haven’t vaccinated quickly enough to stay ahead of the more contagious variants, said Dr. Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security in Baltimore, Maryland. Those variants are also taking hold in the U.S.
“Vaccination with no speed limit, 24/7, that’s what’s going to protect us from what’s happening in Europe,” Adalja said.
He believes it is too early for states to drop mask mandates but OK to allow restaurants and other places to increase capacity gradually.
“You don’t have to do what Texas did,” Adalja said. “You can increase capacity while keeping the masks in place.”
Texas and a few other states have lifted their statewide mask requirements or plan to do so soon, while governors in more than half the states have moved to ease other restrictions in the coming weeks for restaurants, gyms and movie theaters.
Disneyland in Southern California announced it will reopen with limited crowds at the end of April for the first time since the start of the pandemic. And airlines have had their best weeks since the crisis began and say more people are booking flights for spring and summer.
Amelia Fowler, among a stream of people getting their shots Wednesday at Medgar Evers College in New York City, is looking forward to grocery shopping and returning to a normal routine in her acting job after a dark year.
“It was just literally terror: terror going out of the house, terror going down the street, terror dealing with other people, and the terror has been removed,” she said.
Yusuf Lamont, who got his second dose, worries the threat is not over, saying, “It’s not a time to just start whipping masks off and dancing around.”
“There’s a false sense of security with numbers going down and people getting vaccinated. It’s like, ‘Oh, it’s safe to go do whatever.’ No. It’s a big country. There’s 330 million people,” he said.
Josh Michaud, associate director of global health policy with the Kaiser Family Foundation in Washington, said the optimism in the U.S. should come with caution.
Europe’s “rapid relaxation of distancing requirements in a lot of places, combined with populations letting their guard down as they look ahead to the light at the end of the long pandemic tunnel, helped set the stage for the current surges,” he said.
The lesson for the the U.S., he said, is to keep vaccinating those at risk as fast as possible, keep an eye on variants, and “keep slow and steady with the easing of social distancing requirements.”
___
Associated Press video journalist Eugene Garcia in California, reporter Thalia Beaty in New York and AP reporters across Europe contributed to this report.
by ponchi101 @Suliso. April 24th, you must arrive with your Covic vaccination in Philadelphia (port of call) and then proceed to 6 days quarantine, before boarding the vessel. Prior to boarding, you STILL need to take a Covid test, maximum 72 hours before that, to get clearance. I suspect that they are just asking for impossible requirements so then they can claim they need to hire their buddies because "nobody else could comply with the requirements".
You know, you have a donkey, your company wants a horse, so you ask for a winged pink unicorn that poops marshmallows and when nobody qualifies, you tell your company "we have to go with the donkey".
by JazzNU Posted the above article in particular because it mentions some lockdowns in Europe I hadn't heard about before, such as Poland, Serbia, and the French Riviera.
by ponchi101 Thanks. So maybe I can be the donkey.
Fun fact too (and sorry to hijack the thread, as this should be in the JOBS TOPIC): the actual job is in Guyana. In normal times, I would be the closest possible techie for this. Now... ha ha ha
by JazzNU
Covid: Paris lockdown as France fears 'third wave'
The French capital Paris is set to go into a month-long Covid lockdown as the country fears a third wave.
Another 15 departments in the country will also be placed under the same measures from midnight on Friday.
These measures will not be as strict as the previous lockdown, Prime Minister Jean Castex said, with people allowed to exercise outdoors.
France has recorded more than 35,000 new infections within the past 24 hours.
Mr Castex said a "third wave" of infections in the country was looking increasingly likely.
The situation in Paris is particularly worrying with 1,200 people in intensive care there, more than at the peak of the second wave in November, Health Minister Olivier Veran said.
Under the new measures, non-essential businesses will be forced to close but schools will remain open. People will be allowed to exercise outdoors within 10km (6 miles) of their home and are not allowed to travel to other parts of the country unless they have a valid reason. Those in the affected areas will have to fill out a form to explain why they have left their homes.
France's nationwide curfew will remain in place. However, it will begin an hour later at 19:00 (18:00 GMT), taking into account the longer hours of daylight.
Fears of a third wave come as the French government faces criticism for its slow vaccine rollout.
From Friday, France will resume vaccinating using the AstraZeneca jab following the EMA's announcement that it was fit for use. Mr Castex said he would be getting the vaccine straight away to prove that it was okay.
France had suspended the jab after a number of cases in Europe of blood clots developing after the vaccine was administered. A survey conducted just as the suspension was announced found that only 20% of the French have confidence in AstraZeneca.
by ti-amie I think the US is rushing to open up. Not just in the South and West but right here in NYC, which has its own variant.
I'm very worried.
by JazzNU Yes, they are opening up more here too. More attendance, increased capacity, etc. The good news is that ours doesn't take effect for another couple of weeks, but I'd prefer it be pushed til the end of April. We're not doing well enough with vaccinations to rush it to me. The region is down to a 5% positivity rate, so I'm hoping that paired with the vaccinations will be enough to hold off a resurgence. But it's all very concerning.
by patrick
ti-amie wrote: ↑Fri Mar 19, 2021 3:19 am
I think the US is rushing to open up. Not just in the South and West but right here in NYC, which has its own variant.
I'm very worried.
With Spring break happening, DeSantis is all smiles as revenue is coming. Beaches are crowded and hotels are 90% booked. With DeSantis being slow in opening up vaccine to people below 60, Orange County(Orlando) will lower age to 40. Will be interesting to hear what DeSantis will say. DeSantis said next week age to be lowered to 55 and predicts that vaccines will be available to all in April.
by dryrunguy Here's the latest Situation Report. I was intrigued by the section on how incarcerated individuals are lower on the priority list for vaccination. I guess I hadn't thought about it before.
This B.1.1.7 variant is scary.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 121.5 million cases and 2.7 million deaths as of 11am EDT on March 19.
Many countries in central and eastern Europe are exhibiting what could be the early signs of a “third wave” of COVID-19. Looking at the relative change in daily incidence, most European countries were still combating the autumn 2020 surge in November 2020 and then turned a corner in December 2020 and January 2021. By late February/early March 2021, however, incidence in many European countries began to increase again. Unlike the period between Europe’s first and second waves—during which many European countries maintained low levels of transmission over a period of months—the most recent decline barely fell below half of the autumn 2020 peak, and only briefly, before increasing again.
Not all European countries are exhibiting increasing daily incidence, but many are. A number of countries that are experiencing a surge exhibit a similar epidemic trajectory. These countries tend to peak between early November and early December, followed by a steady decline into 2021 and then a surge beginning in early-to-mid February 2021. A number of European countries exhibit this trend, including Austria, Bosnia and Herzegovina, Bulgaria, Greece, North Macedonia, Romania, Serbia, and Ukraine. In some of these instances, the current surge is quickly approaching the peak of the autumn 2020 surge, which accounted for the most severe portion of the pandemic in many European countries.
In terms of total daily incidence, a number of larger European countries stand out. France’s daily incidence has steadily increased since it came down from its autumn 2020 surge in early December 2020, while the surges in other countries started closer to mid-February 2021. In Hungary, for example, the daily incidence increased from approximately 1,500 new cases per day in mid-February to more than 7,700, an increase of more than 400%. In Poland, the daily incidence has more than tripled since mid-February, up from approximately 5,400 new cases per day on February 13 to more than 17,000 (and still increasing steadily). Italy’s daily incidence nearly doubled over the past month, although it appears to be tapering off to some degree.
Looking at the per capita daily incidence, it is evident that smaller countries are facing similar surges. Estonia never really came down from its autumn/winter 2020 surge. Rather, it plateaued in late December 2020 and then surged again starting in early February. At its low in October 2020, Estonia reported 28 new cases per day, which increased to approximately 600 in late 2020/early 2021 and then increased again to more than 1,400 new cases per day currently. Czechia is battling its third COVID-19 spike since October, the most recent of which started in early-to-mid February. Each spike peaked at approximately 12-13,000 new cases per day, and the current spike appears to be starting to decline.
At this point, the major drivers of the ongoing surge remain uncertain. It is likely a combination of a number of factors, including geographic and community spread of emerging variants that exhibit increased transmissibility, and increased social interaction due to relaxing COVID-19 restrictions that were put into place following the autumn 2020 surge. European countries continue to scale up vaccination efforts, but many experts and government officials have noted the slow distribution process across the continent, which is negatively impacting governments’ ability to increase vaccination coverage. At this point, it appears that many European countries have not yet achieved sufficient vaccination coverage to begin containing their respective epidemics, and it will be critical to both increase vaccine supply and vaccination capacity and maintain necessary protective measures over the coming months, particularly as many European countries look ahead to the summer tourist season.
Global Vaccination
The WHO reported 364.2 million vaccine doses administered globally, including 207.8 million individuals with at least 1 dose. The dashboard does not yet include daily or weekly vaccinations.
Our World in Data reports that 409.8 million vaccine doses have been administered globally, a 21% increase compared to this time last week. The daily average surpassed 10 million doses per day. The current average of 10.3 million doses per day is a 40% increase compared to a week ago. At least 143 countries and territories are reporting national vaccination data.
UNITED STATES
The US CDC reported 29.4 million cumulative cases and 535,217 deaths. Daily incidence continues to level off, although it may still be decreasing slowly. After falling from nearly 250,000 new cases per day to fewer than 64,000 between January 11 and February 22, the national average has decreased just 9,998 new cases per day since then. The current daily decline of 435 fewer new cases per day since February 22 is approximately one-tenth of what it was previously (4,420 fewer new cases per day). Daily mortality continues to decrease as well, but it may have passed an inflection point and appears to be starting to taper off slightly. On March 16, the average daily mortality fell below the peak of the summer 2020 surge.
US Vaccination
The US CDC reported 151.1 million SARS-CoV-2 vaccine doses distributed and 115.7 million doses administered. This includes 75.5 million people (22.7% of the entire US population; 29.2% of the adult population) who have received at least 1 dose of the vaccine, and 41.0 million (12.3%; 15.9%) who are fully vaccinated. Among adults aged 65 years and older, nearly two-thirds (66.3%) have received at least 1 dose and 38.6% are fully vaccinated.
The average doses administered* appears to be leveling off at approximately 2.2 million doses per day, including 902,781 individuals fully vaccinated (ie, second dose of a 2-dose vaccine or a single dose of a 1-dose vaccine). In terms of full vaccination, 20.5 million individuals have received the Pfizer-BioNTech vaccine, 19.4 million have received the Moderna vaccine, and 2.0 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 7.6 million doses have been administered at long-term care facilities (LTCFs)**, including residents and staff. This covers 4.8 million individuals with at least 1 dose and 2.8 million with 2 doses. Vaccination progress at LTCFs has slowed considerably, as the available vaccine supply is shifting toward lower-tier priority groups and the broader public.
**The dashboard only includes data for doses administered through the Federal Pharmacy Partnership for Long-Term Care (LTC) Program. It does not report data from West Virginia, which opted out of the program.
The Johns Hopkins Coronavirus Resource Center is reporting 29.7 million cumulative cases and 539,868 deaths as of 12:30pm EDT on March 19.
ASTRAZENECA-OXFORD VACCINE IN EUROPE After a number of countries paused vaccination efforts using the AstraZeneca-Oxford SARS-CoV-2 vaccine, health experts raised concerns that these decisions were not consistent with the available scientific evidence. While countries in Europe were the first to suspend their vaccinations, some countries in Africa reportedly took similar measures. Following reports of several instances of blood clotting conditions in recently vaccinated individuals, the European Medicines Agency (EMA) initiated a study of the available evidence to assess any safety issues with the vaccine.
On March 18, the EMA issued a statement regarding its preliminary findings. The analysis found no association between the vaccine and increased risk of blood clots (thromboembolic events), and there was no evidence that the clotting events were associated with a specific batch of the vaccine. The EMA did identify a potential association between the vaccine and “very rare cases of blood clots associated with thrombocytopenia, i.e. low levels of blood platelets...including rare cases of clots in the vessels draining blood from the brain (CVST),” but further analysis is needed. The EMA reviewed data from 7 cases of individuals with multiple blood clots and 18 cases of CVST out of approximately 20 million vaccinated individuals. It emphasized that COVID-19, itself, is associated with potentially fatal blood clotting conditions and that the benefits of vaccination outweigh the risk of adverse events.
The WHO also issued a statement on the vaccine, emphasizing that the vaccine “will not reduce illness or deaths from other causes” and that thromboembolic events “occur frequently.” Following its own analysis, Africa CDC issued a recommendation that all African Union countries continue vaccination efforts using the AstraZeneca-Oxford vaccine. At least a dozen European countries have reportedly resumed use of the vaccine this week. But even as countries resume use of the vaccine, health experts are concerned “the damage is done” and that decisions to suspend the use of the vaccine will have lasting effects on public confidence in the vaccine.
While other countries were curtailing their use of the AstraZeneca-Oxford vaccine, Canada announced it is expanding its use in older adults. Previously, Canada’s National Advisory Committee on Immunization (NACI) did not recommend the vaccine for adults over the age of 65 due to insufficient evidence, but it issued the update based on real-world data from ongoing vaccination efforts.
US LOANS ASTRAZENECA-OXFORD VACCINE The US government is finalizing plans to ship millions of doses of its available AstraZeneca-Oxford SARS-CoV-2 vaccine supply to Mexico and Canada. During a March 18 press conference, White House Press Secretary Jen Psaki said the US has 7 million available doses and plans to send 2.5 million doses to Mexico and 1.5 million doses to Canada. She noted that the shipments would amount to a loan, with the US expected to receive doses of the same or a different vaccine in the future, and that the US government’s first priority remains vaccinating the US population. The US has faced increasing pressure to share its supply of vaccines with other countries, particularly the AstraZeneca-Oxford vaccine, which is not yet authorized for use in the US. Ms. Psaki said the White House continues to engage in conversations regarding requests from other countries, but providing the vaccine to US neighbors to the north and south is in the country’s best interest. The plan could be finalized as soon as today.
GLOBAL VACCINE PRODUCTION On March 17, a group of Democratic members of the US House of Representatives urged President Joe Biden to support an emergency temporary waiver of some World Trade Organization (WTO) Trade-Related Aspects of Intellectual Property Rights (TRIPS) rules, which they argue would increase global production of vaccines, treatments, and diagnostic tests for SARS-CoV-2. At issue is a joint India-South Africa proposal to the WTO TRIPS Council that would provide a temporary intellectual property waiver for equipment, drugs, and vaccines related to the COVID-19 pandemic. While the proposal is supported by more than 50 low- and middle-income countries (LMICs), Western nations have blocked the proposal 8 times, the latest on March 10. Proposals need a consensus of at least 164 countries to pass. The TRIPS Council is scheduled to meet again June 8-9, when the proposal could be addressed again.
Though the idea to issue intellectual property waivers seems simple and is supported by multiple international organizations—including Oxfam, Médecins Sans Frontières (MSF), and the WHO—some experts and pharmaceutical companies argue the benefits of the move are not clear-cut. The Pharmaceutical Research and Manufacturers of America (PhRMA) says there is no evidence that waivers would increase vaccine production or access. In fact, some experts believe waiving intellectual property rights could backfire and cause some companies to disengage from global access efforts. Instead, some experts suggest that voluntary licensing agreements, under which vaccine developers can enter into manufacturing contracts with generic producers, could be a solution. They emphasize that cooperation and smart incentives, and not the elimination of intellectual property rights, is the best route to increasing production and access to COVID-19 medical products.
MODERNA VACCINE CLINICAL TRIALS Moderna announced that it administered the first doses of its SARS-CoV-2 vaccine to pediatric participants in a Phase 2/3 clinical trial. The study will include 6,750 children aged 6 months to less than 12 years enrolled at sites in the US and Canada. The study will begin by evaluating multiple vaccine doses, including 3 different doses (25μg, 50μg, and 100μg) in children under 2 years old and 2 different doses (50μg or 100μg) for children 2 years and older. Interim analysis will determine which doses will be used in the larger study.
Moderna also announced it commenced a Phase 1 clinical trial for its “next generation” SARS-CoV-2 vaccine. The new vaccine candidate utilizes an mRNA platform, like Moderna’s existing vaccine, but it aims to be stable at normal refrigerator temperatures rather than freezer temperatures like the current vaccine. Moderna intends to conduct future clinical trials to evaluate the new candidate’s efficacy as both a standalone vaccine and as a booster for its existing vaccine. Moderna also started a Phase 2 clinical trial of a modified version of its existing vaccine that aims to serve as a booster dose to increase efficacy against the B.1.351 variant. The trial includes 3 arms testing multiple formulations of the new candidate, including 20 µg and 50 µg doses of the variant-specific booster candidate and a multivalent booster candidate, which contains mRNA for “ancestral strains” and the B.1.351 variant.
VACCINE EFFICACY ON EMERGING VARIANTS Researchers in South Africa—in collaboration with researchers in the UK, including from AstraZeneca and the University of Oxford—published findings from a study of the AstraZeneca-Oxford vaccine’s efficacy against the B.1.351 variant. The study, published in The New England Journal of Medicine (NEJM), was a randomized, placebo-controlled clinical trial, and it included nearly 1,500 participants aged 18-65 years who had not been previously infected in the primary analysis. The study enrolled participants from June-November 2020.
The vaccine exhibited an overall efficacy of 21.9% against any COVID-19 disease, with 19 cases among 750 vaccinees compared to 23 cases among 717 participants in the control group; however, the efficacy results did not demonstrate a statistically significant benefit. There were no cases of severe disease or death in either group. Of 41 cases with sequencing data available, 39 (95.1%) were caused by the B.1.351 variant, suggesting the vaccine efficacy against this variant to be 10.4%, but again, the results did not demonstrate a statistically significant level of protection. In contrast, the researchers also looked at data from before the B.1.351 variant was widespread in South Africa. Using cases detected on October 31, 2020 or earlier as a “proxy for non-B.1.351 variant” infection, they estimated an efficacy of 75.4%.
While further analysis is needed to more fully characterize the efficacy of all available vaccines against emerging variants, this study provides further evidence that variants of concern (VOCs), like B.1.351, could pose significant challenges in terms of containing COVID-19 through vaccination. Efforts are ongoing to update the AstraZeneca-Oxford and other vaccines to provide better protection against emerging variants.
EMERGING VARIANTS On March 16, the US CDC updated its information on emerging SARS-CoV-2 variants. The CDC introduced classifications for emerging variants: Variants of Interest, Variants of Concern, Variants of High Consequence. Variants of Interest have “genetic markers” that could potentially affect transmissibility, disease severity, or susceptibility to vaccines or therapeutics, whereas Variants of Concern include those for which there is existing evidence of increased transmissibility, disease severity, or reduced susceptibility. Variants of High Consequence are limited to variants with clear evidence of reduced effectiveness for risk mitigation measures or medical countermeasures (MCMs). The CDC has classified 3 variants—B.1.526, B.1.525, and P.2—as Variants of Interest and 5 variants—B.1.1.7, P.1, B.1.531, B.1.427, and B.1.429—as Variants of Concern. Notably, the previous CDC guidance, prior to its tiered classification system, included only B.1.1.7, P.1, and B.1.351 as Variants of Concern, and the 2 new additions are variants that were first identified in California. There are currently no Variants of High Consequence.
Two recently published studies found evidence of increased mortality linked to the B.1.1.7 variant. The first study, published in Nature, included data from 2.2 million positive SARS-CoV-2 tests in England from November 2020 to February 2021, including nearly 17,500 deaths. The researchers estimate an increase in mortality of approximately 60% associated with the B.1.1.7 variant (adjusted hazard ratio=1.61). The second study, published in The BMJ, matched nearly 55,000 pairs of participants in the UK to compare the mortality of the B.1.1.7 variant against others. The researchers paired participants based on the ability of the TaqPath diagnostic assay to detect the spike protein gene as a proxy for B.1.1.7 infection to ensure each pair included one and only one B.1.1.7 infection. These researchers also estimated an increase in mortality of approximately 60% associated with the B.1.1.7 variant (adjusted hazard ratio=1.64). The researchers note that this change represents an increase in deaths from 2.5 to 4.1 per 1,000 detected cases.
INTERNATIONAL TRAVEL GUIDANCE On March 18, WHO officials announced they are working on the development of a “smart vaccination certificate” for people who have received a SARS-CoV-2 vaccine. WHO Regional Director for Europe Dr. Hans Kluge emphasized that this effort is simply a method of documenting vaccination status and not a “vaccine passport.” The vaccination certificate should not be mandatory for international travel. There still remains a global shortage of vaccines, which would put travelers from some countries at a disadvantage if it were mandatory, and the duration of vaccine-induced immunity is still highly uncertain, which poses a technical barrier for a mandatory vaccine passport. In a WHO webinar on international travel during the COVID-19 pandemic, a representative of the WHO Smart Vaccination Certificate Working Group said the group intends to solicit public comment to inform its discussions starting today.
The WHO’s distinction on vaccine certificates versus passports came one day after the European Commission (EC) proposed delivering free “Digital Green Certificates” that would allow EU residents to travel freely within the bloc. The certificates would be made available to those who have been vaccinated as well as those who test negative for the virus or have recovered from natural infection. Some countries have expressed opposition to the plan, considering many individuals have not yet been able to access the vaccine, but the EC noted that vaccination would not be mandatory for EU citizens to travel between EU countries. The plan is set to be discussed next week at a summit of EU leaders. A WHO official noted the agency is looking into the details of the EC plan.
In the US, Senior Advisor for the White House COVID Response Team, Andy Slavitt, suggested that the government should not be involved in verifying individuals’ vaccination status nor in issuing certification. Though Americans will need a way to document vaccination, Slavitt indicated that the process should be private, secure, free, available digitally and on paper, and available in multiple languages.
GLOBAL COVID-19 MORTALITY Analysis published by Think Global Health puts global COVID-19 mortality in the context of other major causes of death. To date, the WHO has reported more than 2.6 million cumulative COVID-19 deaths worldwide, including 1.8 million in 2020. Since the onset of the pandemic, COVID-19 has accounted for 4.4% of all reported deaths globally, making it the fourth leading cause of death over that period, following ischemic heart disease (15.5%), stroke (11.1%), and chronic obstructive pulmonary disease (COPD; 5.6%). Notably, COVID-19 was the leading cause of death in some parts of the world, including nationally in France, Mexico, Spain, and the UK as well as half of the countries in South America and some US states. The proportion of deaths due to COVID-19 varies widely by region. Not surprisingly, the Americas, led by the US and Brazil, has the highest proportion of deaths due to COVID-19 (13.0%), followed by Europe (9.3%). The Eastern Mediterranean region (3.0%), Southeast Asia (2.3%), Africa (0.8%), and the Western Pacific region (0.2%) are all below the global average. Notably, COVID-19 was outside of the top 50 or top 100 causes of death in most countries in Africa, south and southeast Asia, and Oceania. Overall, COVID-19 was the 24th leading cause of death in Africa.
US VACCINE ELIGIBILITY AND ACCESS Due to variability across US states in both demographics and vaccine allocation strategy, some states are beginning to move into different phases of their SARS-CoV-2 vaccine rollout. Earlier this week, Mississippi joined Alaska as the second state to open COVID-19 vaccination to all adults ages 16 and older, having reached target thresholds for higher priority groups. US President Joe Biden has called for all states to open vaccination to all adult residents by May 1, as vaccine supply and administration continue to ramp up. Some states, like Ohio, Indiana, and Wisconsin, are opening their vaccination eligibility to larger groups of adults, with specific requirements varying among states. Other states are announcing wider eligibility standards for the coming weeks or months.
Despite these promising announcements, challenges persist around availability of appointments and equitable vaccine access. In a report published in the US CDC’s MMWR, the US CDC COVID-19 Response Team examined county-level vaccination coverage based on the CDC’s Social Vulnerability Index (SVI) score, which uses 15 socioeconomic, demographic, and other indicators “to help local officials identify communities that may need support before, during, or after disasters.” The researchers found that SARS-CoV-2 vaccination coverage was lower in high vulnerability counties than in low vulnerability counties, with an overall difference of 1.94 percentage points. The largest coverage disparities were associated with socioeconomic disparities, with vaccination coverage 2.5 percentage points higher in low vulnerability counties than high vulnerability counties. The researchers called for increased attention to achieving equity in vaccine administration.
At a more granular level, advocates continue to question why incarcerated individuals are lower on the priority list for SARS-CoV-2 vaccination. Some argue that prisons should be considered as long-term care facilities (LTCFs), just like nursing homes, due to the elevated risk of transmission and elevated rates of underlying health conditions associated with higher risk of severe disease and death. According to a report by STAT News, 19 states do not plan to administer SARS-CoV-2 vaccines to incarcerated populations until they finish with the broader public. The high COVID-19 risk for incarcerated populations and risk of community outbreaks originating in correctional facilities underlie the need for vaccination prioritization.
US CDC SCHOOL PHYSICAL DISTANCING GUIDANCE The US CDC published updated guidance for physical distancing in K-12 classrooms, which reduces the recommended physical distancing in some settings from 6 feet to 3 feet. Earlier this week, Chief Medical Advisor to the President Dr. Anthony Fauci and CDC Director Dr. Rochelle Walensky indicated that the CDC was considering the change, based on evolving evidence about transmission risk in school settings and notable challenges facing schools in terms of maintaining 6-foot separation for students and staff. The changes were based in part on the findings from several studies published in today’s MMWR, which provide further evidence regarding SARS-CoV-2 transmission dynamics in school settings. In addition to physical distancing, the new guidance includes updates regarding improved ventilation, physical barriers, and other aspects of COVID-19 mitigation in schools.
The updated guidance indicates that elementary schools can reduce physical distancing to 3 feet as long as mask use is universal, regardless of the level of community transmission. For middle and high schools, in classrooms where mask use is universal, the CDC recommends 3-foot separation in schools where community transmission is low, moderate, or substantial. For middle and high schools in areas where community transmission is high, the CDC recommends 6-foot separation if cohorting—ie, keeping the same groups of students together throughout the day to reduce mixing with other groups—is not possible. Schools in high-transmission areas that are able to implement cohorting strategies can operate using 3-foot distancing.
The CDC continues to recommend 6-foot physical distancing between adults, in common areas (eg, lobbies, auditoriums), when masks cannot be worn (eg, when eating), and during activities that involve “increased exhalation” (eg, singing, band practice/performance, sports practice/competition). Reducing the recommended physical distancing separation to 3 feet aims to make it easier for schools to resume in-person classes while continuing to mitigate transmission risk.
patrick wrote: ↑Fri Mar 19, 2021 9:56 am
With Spring break happening, DeSantis is all smiles as revenue is coming. Beaches are crowded and hotels are 90% booked. With DeSantis being slow in opening up vaccine to people below 60, Orange County(Orlando) will lower age to 40. Will be interesting to hear what DeSantis will say. DeSantis said next week age to be lowered to 55 and predicts that vaccines will be available to all in April.
Yeah, I thought about you when I saw those many, many Spring Break photos and videos. Looks wild down there especially in the Miami area from what I've seen.
by ponchi101 From the report:
"The EMA reviewed data from 7 cases of individuals with multiple blood clots and 18 cases of CVST out of approximately 20 million vaccinated individuals. It emphasized that COVID-19, itself, is associated with potentially fatal blood clotting conditions and that the benefits of vaccination outweigh the risk of adverse events."
25 total people "suffered" side effects (if they were really due to the vaccine).
Is the math needed? AITA?
by ti-amie I'm jus' gonna leave this here...
by ponchi101 To the tune of James Brown's "I feel good".
I literally cracked.
by ti-amie
P1
by Suliso What may save you, but not us is high vaccination rates in US. The most vulnerable are already protected. Most countries in EU are going up already or at a plateau. Again UK probably in the best position due to high vaccination rates.
by Suliso By the way it's (expletive) that EU low vaccination rates compared to US/UK are because of slowness of signing contracts. The real reason is that US/UK keep all vaccines produced in their countries to themselves there as EU does not. If they did Canada would have 0% vaccination rate right now as they have no capability of making their own and Israel success story wouldn't have happened either for the same reason. Maybe we should have been more greedy...
by ti-amie
by Deuce
Suliso wrote: ↑Sat Mar 20, 2021 10:04 am
By the way it's (expletive) that EU low vaccination rates compared to US/UK are because of slowness of signing contracts. The real reason is that US/UK keep all vaccines produced in their countries to themselves there as EU does not. If they did Canada would have 0% vaccination rate right now as they have no capability of making their own and Israel success story wouldn't have happened either for the same reason. Maybe we should have been more greedy...
I have heard that the U.S. currently has significantly more doses than they need to vaccinate the entire population, including the 2 doses where required. And they won't share. If true, this is indeed mighty greedy.
I don't know if the same is true of the U.K.
The U.S. has just agreed to LEND a tiny portion of their overstock to Mexico and Canada (2 Million and 1 Million doses of AstraZeneca, respectively)...
by ti-amie
by ti-amie
by ti-amie
by ti-amie
by ti-amie This is awful and also shows why you can't condemn an entire state because of a few loonies (the jury is out on Florida though)
by JazzNU
Saudi Arabia, UAE expand COVID-19 vaccination drive
DUBAI (Reuters) - Saudi Arabia and neighbouring United Arab Emirates said on Sunday health authorities have expanded COVID-19 vaccinations to all citizens and residents aged 16 and above as Gulf states race to bring the virus under control.
Riyadh said the health ministry will start inoculating its population aged 16 and above with Pfizer vaccines, while its citizens and residents aged of 18 and above will have Astrazeneca shots.
It did not provide further details.
The government said on Saturday around 3 million vaccines had been distributed across 500 vaccination centres.
The UAE, the region’s commercial and tourism hub and a global travel centre, has set a blistering pace for its vaccine rollout to keep its economy open for business. It ranks second globally behind Israel for doses per 100 people.
The Emirati health ministry urged its citizens and residents aged 16 and over to register for COVID-19 vaccinations, a statement published on state media late on Saturday said. The move, it said, comes after nearly 73% of elderly Emiratis, residents and those with chronic diseases have been vaccinated.
The country is providing four types of vaccine free of charge.
The UAE’s daily COVID-19 cases surged to nearly 4,000 in late January from about 600 in September after Dubai opened its doors to visitors during the peak winter tourism season.
The rate has fallen after authorities tightened restrictions at public venues but stopped short of imposing new lockdowns. Some restrictions have since been eased but mask-wearing in public and social distancing are still required.
The UAE, which does not give a breakdown for each of its seven emirates, registered 2,013 new infections on Saturday to take its total tally to 438,638 with 1,433 deaths.
Reporting by Ghaida Ghantous; Editing by David Goodman and David Evans
Third dose of Sinopharm coronavirus vaccine needed for some in UAE after low immune response
by Paul Schemm
DUBAI — A "very small number" of people in the United Arab Emirates are being invited to receive a third shot of the Sinopharm coronavirus vaccine after antibody tests indicated they did not have a sufficient immune response following two doses of the Chinese-made vaccine, its distributor confirmed Sunday.
There have also been reports out of China of people being initially unresponsive to the vaccine and requiring additional doses.
Walid Zaher, the chief researcher for G42 Healthcare, which distributes the Sinopharm vaccine in the UAE, told Dubai Eye radio that a study was underway to give some people third doses.
“When some people are found to be not really responsive to the vaccines, which is expected with all vaccines, there was an initiative to approach these people and give them a third shot of the Sinopharm vaccine, which has shown, within the context of the study, to boost their immunity,” he said.
Zaher said anyone with low levels of antibodies after a test could ask their doctor to contact health authorities and an appointment would be made for them to have another dose, but generally it’s the officials that approach the person.
He likened the third shot to a flu booster shot and said the amount of people who need it is a “very small number.” The need for a third shot was first mentioned March 10 to the National newspaper by the spokeswoman for the country’s health sector, Farida al-Hosani.
Doctors told the Wall Street Journal there were cases of people with little or no antibody response after two doses of Sinopharm.
The revelations could raise doubts about the effectiveness of the vaccine, which is being widely used around the world as countries scramble to inoculate their populations. Many of the more effective Western-made vaccines have been snapped up by wealthier nations.
The Sinopharm vaccine has a self-reported efficacy rate of 79 percent, which global health experts say is more than adequate, but its data has not been publicly released. In addition to the UAE, the vaccine has been purchased by countries such as Egypt, Cambodia, Senegal and Peru.
In China, over the weekend, medical authorities also announced that a clinical pathologist had become infected with the coronavirus despite being vaccinated weeks earlier. They did not specify which vaccine she had used, but her facility is known to administer the Sinopharm one.
“Perhaps she needs to get a third shot as the two doses of inactivated vaccine had failed to create enough antibodies in her,” Gao Fu, director of the Chinese Center for Disease Control and Prevention, told state broadcaster China Central Television on Saturday. “Or she is one of the few who happen to be unresponsive to the vaccine.”
The UAE has distinguished itself with an aggressive vaccination program that initially used Sinopharm, which conducted Phase 3 trials in the country, and was later expanded to include Pfizer-BioNTech, AstraZeneca and Russia’s Sputnik V.
Nearly 73 percent of the elderly population and 56 percent of all adults have received at least one vaccine dose, authorities said Saturday.
As of Sunday, everyone in the country is eligible for a vaccine, authorities said, after restricting injections for the past six weeks to those with special needs.
The UAE has the second-highest national vaccination rate in the region after Israel, with more than 7 million doses given to a population of 9 million. The vaccine is free to all citizens and residents.
The UAE saw an explosion of new coronavirus infections in January after tourists from all over the world flocked to Dubai, which had marketed itself as a restriction-free holiday destination.
The number of new daily cases quadrupled to nearly 4,000 in January and only now has dropped down to about 2,000 new cases a day.
by Suliso In Israel 81% of adults have received at least one dose of vaccine and 71% have been fully vaccinated. All of them with Pfizer vaccine.
With most adults vaccinated, Israel’s large inoculation centers start to close
As pace slows, Tel Aviv shuts major sites; focus shifts to smaller communities as health providers run mobile units in various places with low rates of vaccination
With the vast majority of Israelis age 16 and up already vaccinated or recovered from COVID-19, big vaccination centers in the country’s main cities have started to close as the focus shifts to smaller, mobile stations in smaller communities.
More than 5.1 million of Israel’s 9.3 million population have received at least one vaccine dose, and over 4.5 million have gotten both shots.
With at least 3 million others unable to get inoculated since they are under the age of 16, the vaccination pace has slowed down dramatically since those who want to get vaccinated have mostly already done so.
A massive vaccination center at Tel Aviv’s Rabin Square has been taken down, with works on a planned light rail planned to begin there next month, the Globes business daily reported.
The huge tent complex run by the municipality along with the city’s Ichilov hospital has been used by the Maccabi and Meuhedet health providers to inoculate many thousands of residents.
Another big center at a stadium in northern Tel Aviv is also being closed down, as sports events are slowly returning. It wasn’t immediately clear what would be done with the large vaccination centers set up in Jerusalem. Health providers will now give vaccines in some of their existing clinics.
In addition, health providers and the Magen David Adom ambulance service have shifted their focus to small, mobile vaccination centers in different places every day, with focus on communities where immunization rates are relatively low, particularly in predominantly Arab locales.
Those who have recovered from COVID-19 at least three months ago can also get a (single) vaccine dose.
Officials have said vaccination of kids under the age of 16 could possibly begin in the summer, if trials show the shots are safe for them.
by JazzNU Just curious. Is there a European country that you think would have agreed to share data with Pfizer the way that Israel has? I'm rather amazed at that aspect.
But I'm also shocked at countries like the UK taking the manufacturer's word for their research. We've got so many class actions here because you can't trust what they tell you, we've been down that road before. There are people here who won't take the Johnson & Johnson vaccine for love or money. I'm sure you're thinking it's because of the efficacy numbers, but no, it's because J&J's talcum powder sickened or killed their sister, cousin, or friend.
by Suliso Remember that the particular vaccine was discovered at Oxford. Trust in their own premier university is probably high. At least in Switzerland we don't seem to have such an adversarial relationship with our own pharma industry. In Basel in particular they employ close to 30k people and pay very well.
Not sure about data sharing, but also health systems tend not to be as centralized as the one in Israel. UK perhaps, but I think Pfizer preferred a smaller country.
by ti-amie
by dryrunguy Here's the latest Situation Report. Lots of interesting stuff here--way too much to highlight. And yes, the spring break rioters got a mention.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 123.4 million cases and 2.7 million deaths as of 11am EDT on March 23. The global weekly incidence increased for the fourth consecutive week, up to 3.3 million new cases (7.9% more than the previous week). After 6 consecutive weeks of decreases, the global mortality increased last week as well, up to 60,414 global deaths (2.5% more than the previous week). If this is the beginning of a longer-term trend, it would correspond to a 4-week lag behind the global weekly incidence, consistent with the pattern exhibited throughout the pandemic.
Global Vaccination
The WHO reported 398.0 million vaccine doses administered globally, including 226.0 million individuals with at least 1 dose. The dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports that 458.1 million cumulative vaccine doses have been administered globally, a 19% increase compared to this time last week. The daily average continues to increase, up to 10.6 million doses per day (+6% compared to the previous week). At least 146 countries and territories are reporting national vaccination data.
UNITED STATES
The US CDC reported 29.7 million cumulative cases and 539,517 deaths. Daily incidence continues to level off at approximately 53-54,000 new cases per day. While this is an 80% decrease from the peak in January 2021, it is only 20% less than the peak during the summer 2020 surge. Daily mortality is beginning to taper off as well. The CDC has reported an average of approximately 1,000-1,050 deaths per day over the past 5 days.
On March 19, the CDC reassigned more than 80,000 previously unreported cases in Missouri (reported on March 8) to the correct dates. The correction caused the average daily incidence for January 11, 2021, to exceed 250,000 new cases per day, making the US the only country to surpass that benchmark to date. The US was also the first, and remains the only, country to surpass 100k, 150k, and 200k new cases per day.
While the national-level trends are leveling off, a number of states are reporting increasing daily incidence*. These states are mostly distributed across the Midwest and Northeast regions, but case counts in Idaho, Maryland, and West Virginia are also increasing. Perhaps the largest resurgence is in Michigan, which has reported increasing trends since February 22. After peaking in early December 2020, Michigan’s daily incidence decreased by 90% before rebounding. Michigan’s daily incidence has nearly tripled since February 22—currently 2,997 new cases per day—and it appears to still be accelerating.
*In an effort to be consistent with respect to the timing of the most recent data, we are using official data reported to the CDC. The data published on the state COVID-19 websites referenced in this section may vary.
New Jersey’s autumn/winter surge peaked in early January and then leveled off briefly from February 19-February 26 before increasing again. Unlike many states, New Jersey’s daily incidence only declined 50%—from approximately 6,000 new cases per day** to 3,000—before rebounding. New Jersey is now reporting 3,980 new cases per day, higher than its first peak in April 2020, and increasing steadily. Maine’s epidemic also rebounded almost immediately after its autumn/winter surge, falling 80% from January 14 to February 22—624 to 131 new cases per day—before increasing immediately back up to 206, a 50% rebound.
**With the exception of the week following January 7 and 8, when New Jersey reported 23,925 and zero new cases, respectively, which resulted in aberrations in the average values.
The current surge in several states started more recently. After coming down from the peak of its autumn/winter 2020 surge, Maryland’s daily incidence began to increase again relatively quickly. Maryland’s lull lasted from approximately February 20-March 7, and its average daily incidence has increased nearly 25% since then, up to 949 new cases per day. Idaho (312), Massachusetts (1,566), and West Virginia (336) followed similar trajectories, with small bumps following their autumn/winter surges—approximately February 22-March 8***—and then a steady increase in daily incidence of approximately 25% or more. In Minnesota, the daily incidence held relatively steady for most of February at approximately 775-800 new cases per day, but it also started to surge on March 8. Minnesota is currently reporting 1,118 new cases per day, approximately 40% higher than in February. In New Hampshire, the decline in daily incidence leveled off at 200-220 new cases per day from March 5-10 before climbing back up to 275, a 25-35% increase and still rising. Pennsylvania is just beginning to exhibit increasing daily incidence, up from 2,473 new cases per day on March 13 to 2,949 on March 21 (+19%).
***The President’s Day holiday was February 15, so weekly averages in the following week were artificially depressed due to reporting delays and interruptions.
Following the decline in daily incidence in the wake of the autumn/winter 2020 surge and expanding vaccination efforts, many states are relaxing or eliminating COVID-19 restrictions. Most of the country has not yet been vaccinated, however, and there is evidence of increasing prevalence of emerging variants, both of which could increase COVID-19 risk. It will be critical to monitor the epidemiological trends in these and other states over the next several weeks in order to mitigate the risk of another surge.
US Vaccination
The US CDC reported 156.7 million SARS-CoV-2 vaccine doses distributed and 126.5 million doses administered. This includes 82.8 million people (24.9% of the entire US population; 32.0% of the adult population) who have received at least 1 dose of the vaccine and 44.9 million (13.5%; 17.4%) who are fully vaccinated. Among adults aged 65 years and older, 69.2% have received at least 1 dose and 42.5% are fully vaccinated.
The average doses administered* continues to level off at approximately 2.3 million doses per day, including 901,311 individuals fully vaccinated (i.e., second dose of a 2-dose vaccine or a single dose of a 1-dose vaccine). In terms of full vaccination, 22.2 million individuals have received the Pfizer-BioNTech vaccine, 20.3 million have received the Moderna vaccine, and 2.4 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 29.9 million cumulative cases and 543,057 deaths as of 11:30am EDT on March 23.
ASTRAZENECA-OXFORD VACCINE PHASE 3 TRIAL AstraZeneca announced preliminary results from a Phase 3 clinical trial for its SARS-CoV-2 vaccine, developed in collaboration with the University of Oxford. The trial included more than 32,000 participants in Chile, Peru, and the US, including 21,583 who received at least one dose of the vaccine. The press release reports an overall efficacy of 79% against any COVID-19 disease among all age groups and 80% efficacy for adults aged 65 years and older. Additionally, the press release describes 100% efficacy against severe disease and hospitalization. AstraZeneca explicitly noted that an independent review of the safety data “found no increased risk of thrombosis or events characterised by thrombosis” associated with the vaccine. Previous analysis of data from trials in Brazil, South Africa, and the UK estimated the overall efficacy to be 60%.
AstraZeneca has not yet published the full clinical trial data—including the number of severe cases and hospitalizations among the placebo group nor data pertaining to emerging variants—and the results have not yet been subjected to peer review. The press release indicates AstraZeneca is continuing to analyze the trial data to prepare a final analysis for submission to the US FDA. The AstraZeneca-Oxford vaccine has received a conditional marketing authorization in the EU and similar emergency use authorizations in a number of other countries as well as an emergency use listing from the WHO, but it has not been granted an Emergency Use Authorization from the US FDA. Similar to the J&J-Janssen vaccine, the AstraZeneca-Oxford vaccine does not require freezer (or ultra-cold freezer) temperatures for storage and transportation, which reduces logistical and operational barriers to mass vaccination efforts.
Today, the US National Institute of Allergy and Infectious Diseases (NIAID) issued a statement that called into question the vaccine’s efficacy estimate. The statement indicated the Data Safety Monitoring Board (DSMB) that oversaw the clinical trials had concerns regarding the efficacy reported in the press release. In particular, the DSMB expressed concern that “outdated information” was included in the calculation, “which may have provided an incomplete view of the efficacy data.” No further details were provided, but the NIAID called on AstraZeneca to work with the DSMB to identify and correct any issues. In response, AstraZeneca stated the preliminary results were based on a “pre-specified interim analysis” of a subset of data collected through February 17. AstraZeneca indicated that it is validating its statistical analysis and engaging with the DSMB, with the goal of publishing the primary results in the next 48 hours.
ASTRAZENECA-OXFORD VACCINE HESITANCY AstraZeneca’s announcement of results from Phase 3 clinical trials, combined with statements last week from the European Medicines Agency (EMA) and WHO supporting the AstraZeneca-Oxford vaccine’s safety, appeared poised to provide a boost in confidence in the vaccine, but questions regarding the accuracy of the trial’s efficacy analysis threaten to further erode public trust and interest. While the most recent issues may be more of an issue with AstraZeneca’s communications than the vaccine itself, the misstep could taint the public’s impression of the vaccine. In fact, Chief Medical Advisor to the President Dr. Anthony Fauci described the issue as an “unforced error” by AstraZeneca that could have an unfortunate negative effect on the public’s perception of what is “very likely a very good vaccine.”
Recent surveys conducted in several European countries found a substantial portion of the population still believes the vaccine is unsafe. Notably, 61% of French respondents indicated that they felt the vaccine is unsafe, up 18% compared to results from February. Similarly, 55%, 52%, and 43% of German, Spanish, and Italian respondents, respectively, expressed concern about the vaccine’s safety. In Spain and Italy, the new totals are 27 percentage points higher than in February. The UK—where the vaccine was originally developed—was the only country to express confidence in the vaccine, with nearly 75% believing the vaccine is safe.
In addition to challenges of public perception, the AstraZeneca-Oxford vaccine finds itself in the middle of a battle between the EU and the UK regarding access. Reportedly, the European Commission continues to evaluate a “ban” on exporting doses of the vaccine manufactured in the EU in order to direct those doses to meet contractual commitments to EU countries before allowing them to be delivered outside the bloc, including to the UK. Reportedly, the EU has received only one-third of its doses of the AstraZeneca-Oxford vaccine, and the UK has been able to vaccinate approximately 40% of its population, compared to less than 12% across the EU. Officials from AstraZeneca noted that the UK contracts were signed before the EU contracts, which likely factors into the company’s allocations.
PASC/LONG COVID Researchers from the COMEBAC Study Group published data in JAMA from a cohort study describing 4-month outcomes for patients who were hospitalized with COVID-19 in Paris. Among 478 participants contacted by telephone, 244 patients (51%) reported they were experiencing at least 1 new symptom 4 months post-hospitalization. The most common complaints were fatigue (31%), cognitive impairment (21%), and dyspnea (ie, difficulty breathing; 16%). In addition, 63% of 171 patients assessed at follow-up ambulatory visits had abnormal lung CT scans, although the researchers note that lasting severe pulmonary impacts are not uncommon among COVID-19 survivors. The researchers emphasize their data is limited by the lack of a control group and pre-COVID baseline data.
Another study published in The Annals of Clinical and Translational Neurology by researchers from Northwestern University describes the experiences of patients treated at the university’s specialized clinic for patients experiencing COVID-19-related neurological symptoms. The study included 100 patients from 21 states (50 testing positive for SARS-CoV-2 but non-hospitalized, and 50 testing negative for SARS-CoV-2; average age of 43) who were treated between May and November 2020. The most frequently reported neurologic manifestations included “brain fog” (81%), headache (68%), numbness/tingling (60%), dysgeusia (altered taste; 59%), anosmia (loss of smell; 55%), and myalgias (55%). The researchers note that only anosmia was significantly more frequent in patients who tested positive than those who tested negative (74% vs 36%) and that positive patients performed worse in attention and working memory cognitive tasks when compared to a demographic‐matched US population.
Several experts are calling for media outlets to be cautious in their reporting of so-called “long COVID,” collectively referred to as Post-Acute Sequelae of SARS-CoV-2 infection (PASC). They note some patients who describe long-lasting symptoms of COVID-19—including gastrointestinal symptoms, “brain fog,” severe fatigue, hair loss, and headaches—never tested positive for SARS-CoV-2. They also emphasize these symptoms are associated with many conditions and are common in the general population, especially among individuals experiencing social and emotional distress. But the experts also call for more study on the potential long-term impacts of SARS-CoV-2 infection, but they caution against “getting ahead of the evidence.” As we reported previously, the US National Institutes of Health in February launched a US$1.15 million initiative to study the potential long-term health impacts of COVID-19.
SPRING BREAK US colleges and university students typically visit popular warm-weather destinations for spring break for a vacation from classes. This year, the combination of the timing of spring break, unusually discounted prices on accommodations and travel, and efforts to ease COVID-19 restrictions in Florida have made officials concerned that mass gatherings could lead to local and national spikes in transmission. On Saturday, tens of thousands of spring breakers converged on Miami Beach, leading city officials to declare a state of emergency for 3 days, including a curfew imposed from 8pm-6am for all non-essential travel and operations. Traffic also was shut down in certain areas, and indoor and outdoor dining establishments in high-traffic areas were ordered to cease operations starting at 7pm through the duration of curfew.
Local law enforcement have made more than 160 arrests in the past week related to gatherings—often citing lack of proper mask use, overcrowding, violence, or damage to local property. Law enforcement officials fired pepper spray-filled balls to break up crowds, among other measures. On March 21, city officials extended some emergency measures for an additional 3 weeks, including traffic restrictions and curfews, although city residents, hotel guests, and local employees are exempt.
NEW ZEALAND CONSIDERS “TRAVEL BUBBLE” New Zealand’s COVID-19 control strategy has received praise as one of the most effective in the world. Neighboring Australia has shown similar effectiveness in controlling COVID-19, prompting the two countries to consider creating a COVID-19 bubble for air travel. The so-called “trans-Tasman travel bubble” would allow travelers to skip 14-day quarantine measures. Ideally, the travel bubble would consist of shared protocols, detailed plans for isolation facilities, and contact tracing; however, plans for the travel network have not been finalized.New Zealand Prime Minister Jacinda Ardern postponed an announcement for a definitive launch date until April 6.
A study by New Zealand public health officials, published in the US CDC’s Emerging Infectious Diseases (EID) journal, outlines an outbreak investigation in September 2020 originating from an international flight from India to New Zealand. At least 6 passengers tested positive in the managed quarantine and isolation facility or following the completion of their 14-day quarantine. Using genomic analysis and standard contact tracing, the authors hypothesized that transmission occurred during the quarantine period, including between individuals with no direct contact. The case investigators demonstrated that SARS-CoV-2 transmission on international flights can be successfully traced and managed, which will be critical if travelers in the bubble can forgo the quarantine period.
GLOBAL VACCINE COORDINATION Earlier this month, COVAX shipped some of their first COVID-19 vaccine doses to almost 30 different countries. An editorial in The Lancet and a letter in The BMJ raised the idea of appointing a Global Vaccine Coordinator, who would lead an international effort for the equitable distribution of vaccines. The authors argue that clear leadership and oversight are needed to organize what has become largely a piecemeal vaccination effort, with nations, NGOs, and the private sector working independently or bilaterally. While a centralized global champion or body could provide high-level coordination for global vaccine allocation and distribution, it would be a major challenge to ensure they have the authority necessary to compel national governments and private sector companies to participate.
MATERNAL AND NEWBORN IMMUNITY Previously published research has already provided evidence that seropositive pregnant mothers can transfer SARS-CoV-2 antibodies to their fetus via the placenta, based on IgG antibodies detected in umbilical cord blood. Now, pre-prints and new publications are supporting the notion that this phenomenon also may be true in vaccinated pregnant women, with SARS-CoV-2-specific antibodies present in both breast milk and cord blood.
A prospective cohort study (preprint) investigated the effects of COVID-19 mRNA vaccination on pregnant and lactating women, including immunogenicity, reactogenicity, and presence of vaccine-generated antibodies in umbilical cord blood and breast milk samples. The researchers found that vaccine-generated antibodies were present across all samples of umbilical cord sera and breast milk, when compared with baseline samples. The effect was also dose dependent, with detectable SARS-CoV-2-specific IgG increasing in cord blood and breast milk after administration of the second dose. Researchers from Florida Atlantic University (US) published a case report in BMC: Pediatrics documenting the first known presence of vaccine-induced SARS-CoV-2 IgG antibodies in cord blood. The antibodies were detected in the cord blood for an infant born to a mother who received the first dose of the Moderna vaccine 3 weeks before delivery.
SEROPREVALENCE AND IMMUNITY IN WUHAN In a study published in The Lancet, Chinese researchers estimate the burden of SARS-CoV-2 infection during the initial COVID-19 outbreak in Wuhan, China. They performed a cross-sectional analysis of seropositivity for SARS-CoV-2 antibodies in 9,702 individuals who reported living in Wuhan during December 2019. Initial blood specimens were collected in April 2020, and subsequent specimens were collected in June and October 2020. The researchers estimate a seroprevalence of 6.92% in their study population. Notably, 82% who were seropositive were asymptomatic during the study period.
In an associated commentary, experts from the University of Melbourne (Australia) point out that this seroprevalence estimate would equate to more than 622,000 COVID-19 cases during the initial outbreak if applied to the entire Wuhan population, far more cases than were reported in April 2020 (50,333 as of April 17). The commentary authors hypothesize that the discrepancy could be due to high levels of asymptomatic infection and transmission or potentially underreporting, which could also be impacted by high proportions of asymptomatic infections. Of the 6.92% of seropositive participants, approximately 39.8% were positive for neutralizing antibodies at the baseline visit in April 2020, and this value persisted throughout the study period, which provides evidence of protective immunity conferred through natural infection. With less than half of this population showing protective immunity, the authors underscore the importance of mass vaccination campaigns to prevent future infections and reinfections.
REINFECTION RISK Researchers in Denmark found that natural infection confers lasting immunity against SARS-CoV-2, but to a lesser degree in older adults. The study, published in The Lancet, included data from more than 500,000 individuals during Denmark’s first surge, including 11,068 who tested positive. Among those who tested positive, 72 tested positive again at least 90 days later, compared to 16,819 who tested negative. This corresponds to 80.5% protection against reinfection. A secondary cohort analysis of more than 2.4 million individuals found similar overall results (78.8% protection), but lower protection (47.1%) in adults aged 65 years and older.
A study by researchers at the Cleveland Clinic (Ohio, US), published in Clinical Infectious Diseases, found similar levels of protection. The study included test data from more than 150,000 patients tested prior to August 30, 2020, including 8,845 who tested positive. Among the positive patients, 1,278 were retested at least 90 days later, and the researchers identified 63 possible reinfections (31 symptomatic). The researchers estimate 81.8% protection against reinfection.
Both studies acknowledge that PCR tests can be positive for prolonged periods of time following the resolution of acute infection, due to persistent fragments of SARS-CoV-2 RNA, but these studies provide further evidence regarding the degree of protection conferred by natural infection and help characterize the risk of reinfection.
COVID-19 TESTING TOOLKIT WEBINAR The Johns Hopkins Center for Health Security is launching a new informational webinar series on SARS-CoV-2 testing strategies and best practices from selected organizational leaders. This webinar series will be hosted as part of the Center’s new COVID-19 Testing Toolkit, which aims to provide essential information for all organizations seeking to engage in SARS-CoV-2 testing.
This first webinar, held on March 24 at 11am EDT, will feature a conversation with Ginkgo Bioworks on how they launched their innovative SARS-CoV-2 testing service, Concentric by Ginkgo, and their efforts to pilot the program in schools. The panelists will discuss the importance of testing to mitigate COVID-19 risk as schools resume in-person classes as well as the role of biotechnology in countering future outbreaks and pandemics. Register for the webinar here.
Suliso wrote: ↑Tue Mar 23, 2021 5:02 pm
Remember that the particular vaccine was discovered at Oxford. Trust in their own premier university is probably high. At least in Switzerland we don't seem to have such an adversarial relationship with our own pharma industry. In Basel in particular they employ close to 30k people and pay very well.
Not sure about data sharing, but also health systems tend not to be as centralized as the one in Israel. UK perhaps, but I think Pfizer preferred a smaller country.
Interesting. Pharma pays excellent here and probably has millions of workers, but that doesn't translate into trust. Interesting that it does in Switzerland. But they are absolutely considered a great place to work overall. Very coveted positions. We have a large pharma presence locally. It's not adversarial on the that level, more like the actions of the company as a whole are remembered. Like J&J. Like Purdue Pharma.
Suliso wrote: ↑Tue Mar 23, 2021 5:02 pm
Remember that the particular vaccine was discovered at Oxford. Trust in their own premier university is probably high. At least in Switzerland we don't seem to have such an adversarial relationship with our own pharma industry. In Basel in particular they employ close to 30k people and pay very well.
Not sure about data sharing, but also health systems tend not to be as centralized as the one in Israel. UK perhaps, but I think Pfizer preferred a smaller country.
Interesting. Pharma pays excellent here and probably has millions of workers, but that doesn't translate into trust. Interesting that it does in Switzerland. But they are absolutely considered a great place to work overall. Very coveted positions. We have a large pharma presence locally. It's not adversarial on the that level, more like the actions of the company as a whole are remembered. Like J&J. Like Purdue Pharma.
I'm probably a bit biased here being a chemist and close to pharma industry myself. All I could really say is that I haven't noticed any significant mistrust in mainstream media or talking with friends. It helps that we haven't had a company like Purdue Pharma here... As for J&J they have a small R&D center in Switzerland (not Basel).
by ponchi101 The mistrust in all large companies and industries is a very American phenomenon. The famous "they", as in "they know what we are doing" and "they don't tells us everything" is something that I have only heard in America. In S. America, we don't trust the governments because of their corruption, but we don't go full coocoo believing they have ulterior motives. In S. America, we know they are there to steal, but they do so just by grabbing public funding; they do not start elaborate schemes to make a profit.
by JazzNU
ponchi101 wrote: ↑Tue Mar 23, 2021 8:04 pm
The mistrust in all large companies and industries is a very American phenomenon. The famous "they", as in "they know what we are doing" and "they don't tells us everything" is something that I have only heard in America. In S. America, we don't trust the governments because of their corruption, but we don't go full coocoo believing they have ulterior motives. In S. America, we know they are there to steal, but they do so just by grabbing public funding; they do not start elaborate schemes to make a profit.
Do you have the same level of lies and scandal though? Genuinely asking, I'm not sure. I'd assume you have cigarette company lies. Do you have the Enron, Madoff, Savings and Loan, J&J, Purdue, Monsanto, etc., etc. repeatedly happening as well? Or just the corrupt government and that's the root of the scandal almost always?
by mmmm8 Re: data privacy: The EU has very strict data protection laws (GDPR is the main one). I work with employee data and, in practice, there's a bit more slack than you'd expect, and I think anonymized data could be collected, but overally probably not to the extent of Israel.
Re: pharma mistrust. Jazz, I think in LATAM, Eastern Europe, Africa, many places in Asia, mistrust in ALL institutions is so high that corruption is assumed to be happening as a matter of fact. That saves one from picking out specific industries. But then, like ponchi said, the corruption is usually simple (steal state budget money, bribe someone to give you a government contract) rather than complex and inhumane but kind of legal (i.e. create addictive drugs and semi-legally coax doctors in prescribing them, publish accurate but biased research papers, etc.)
by mmmm8
mmmm8 wrote: ↑Tue Mar 23, 2021 9:01 pm
Re: pharma mistrust. Jazz, I think in LATAM, Eastern Europe, Africa, many places in Asia, mistrust in ALL institutions is so high that corruption is assumed to be happening as a matter of fact. That saves one from picking out specific industries. But then, like ponchi said, the corruption is usually simple (steal state budget money, bribe someone to give you a government contract) rather than complex and inhumane but kind of legal (i.e. create addictive drugs and semi-legally coax doctors in prescribing them, publish accurate but biased research papers, etc.)
As an example, think of the Oderbrecht scandal that had been bringing down politicians in Latin America for almost 7 years... at the root, simple bribery and money laundering:
by Suliso In Switzerland scandals usually derive from shady banking industry (not as much as 30 years ago), tax avoidance of rich foreigners etc. Government not so corrupt here and individual large companies rarely singled out. Few exceptions like Nestle or Glencore, but it's generally for what they did abroad not locally. In Latvia it's more or less like 4m8 is describing only to lesser severity than in LATAM.
by JazzNU
dryrunguy wrote: ↑Tue Mar 23, 2021 5:47 pm
On March 19, the CDC reassigned more than 80,000 previously unreported cases in Missouri (reported on March 8) to the correct dates. The correction caused the average daily incidence for January 11, 2021, to exceed 250,000 new cases per day, making the US the only country to surpass that benchmark to date. The US was also the first, and remains the only, country to surpass 100k, 150k, and 200k new cases per day.
While the national-level trends are leveling off, a number of states are reporting increasing daily incidence*. These states are mostly distributed across the Midwest and Northeast regions, but case counts in Idaho, Maryland, and West Virginia are also increasing. Perhaps the largest resurgence is in Michigan, which has reported increasing trends since February 22. After peaking in early December 2020, Michigan’s daily incidence decreased by 90% before rebounding. Michigan’s daily incidence has nearly tripled since February 22—currently 2,997 new cases per day—and it appears to still be accelerating.
So, so proud to be an American. Sheesh.
For the Mid-Atlantic and Northeast, I've been in touch with family and friends in most Northeastern states and they've seeing what I am here in PA. The warm weather two weeks ago doomed us. People came out in droves during that time and were thrilled about it. The Jeannie is out of the bottle and our only hope is to vaccinate as quick as possible. People were certainly out before and doing too much, but there's been a noticeable uptick since the warm weather hit and it getting cold again on and off hasn't mattered. Warmer weather will continue. Daylight Savings took effect. It's done, these people refuse to stay home at this point. I'm not looking for a monsoon or anything, but possibly April showers will help us out a bit. I have little hope for anything else curbing activity. And knowing Chicago like I do, I'd suspect this is also the major challenge there.
by Suliso It's not harmless to gather in large crowds outside, but I was reading somewhere that it's up to 20x more likely to be infected with the same size crowd indoors. So warmer weather is actually helpful as we also saw last summer.
Do you have the same level of lies and scandal though? Genuinely asking, I'm not sure. I'd assume you have cigarette company lies. Do you have the Enron, Madoff, Savings and Loan, J&J, Purdue, Monsanto, etc., etc. repeatedly happening as well? Or just the corrupt government and that's the root of the scandal almost always?
M8 gives a very good explanation. We don't have a local Monsanto hiding data that some of their chemicals will make your eyeballs explode because, simply, we don't have a local Monsanto. Just an example, of course. We do have pyramid schemes and Ponzi schemes, but that is "normal" corruption to us. In Argentina they have seen 7 or 9 "Corralitos", the government freezing assets and accounts which then, by the time the freeze is over, are worthless. Traditional stuff.
We don't have Purdue & Oxycotin corruption because we don't have a Purdue.
In short, we are simply people. One of our simple politicians will accept a simple bribe from a simple mega-conglomerate to drain an entire endangered eco-system and then he will be found in Panama, a few simple millions in his account, partying with a simple 19 year old ex-miss Someplace. Simple stuff.
by JazzNU
Suliso wrote: ↑Tue Mar 23, 2021 10:46 pm
It's not harmless to gather in large crowds outside, but I was reading somewhere that it's up to 20x more likely to be infected with the same size crowd indoors. So warmer weather is actually helpful as we also saw last summer.
Oh sure. If only I was merely talking about meeting outside. The warm weather just makes people get out of the house, they don't necessarily congregate outside. For instance, in Philly, Southern and Northern NJ, the indoor restaurant reservations are almost as full as the outdoor ones at this point.
by ti-amie No one has made a gif of Bugs sawing Texas off the map of the US.
It was Texas where they tried to run a Biden campaign bus off the road.
by mmmm8
ti-amie wrote: ↑Wed Mar 24, 2021 12:18 am
No one has made a gif of Bugs sawing Texas off the map of the US.
It was Texas where they tried to run a Biden campaign bus off the road.
I'm not sure Mexico wants it back, Florida has the convenience of floating out into the ocean.
I always love the Texas secessionist/exceptionalism sentiment ("The Lone Star State"). They have already tried being a country! It lasted less than 10 years.
ti-amie wrote: ↑Wed Mar 24, 2021 12:18 am
No one has made a gif of Bugs sawing Texas off the map of the US.
It was Texas where they tried to run a Biden campaign bus off the road.
I'm not sure Mexico wants it back, Florida has the convenience of floating out into the ocean.
I always love the Texas secessionist/exceptionalism sentiment ("The Lone Star State"). They have already tried being a country! It lasted less than 10 years.
I didn't know that. Txs.
by JazzNU
ti-amie wrote: ↑Wed Mar 24, 2021 12:18 am
No one has made a gif of Bugs sawing Texas off the map of the US.
It was Texas where they tried to run a Biden campaign bus off the road.
Oh they made it. Just doesn't get used as often as Florida even though it should be used more than it is. The Florida one is also just better as I think this is a manipulation of that one.
by Deuce This seems to be AstraZeneca responding to desperate times with desperate measures...
'It wasn't completely accurate': Fauci criticizes AstraZeneca's COVID-shot disclosure, calling it an 'unforced error'
by ti-amie I got my first Pfizer shot yesterday. I was feverish and tired last night but they tell you about that and to take Tylenol for those symptoms. I got it at the Duane Reade (Walgreens) yesterday morning. It's the one where we do all of our pharmacy business. My second shot is scheduled for mid April. No long line and they get you in and out as quickly as possible. The advantage of getting it there was that I could do some in person shopping during the 15 minute wait after the shot, something I haven't done in a very long time.
by dryrunguy There is no link to this as it was in the body of this morning's NY Times e-newsletter. But this is an analysis of U.S. media coverage of COVID compared to coverage globally. Not surprising. These figures are probably fairly consistent with how we have talked about it here (i.e., positive discussion versus negative discussion).
::
Good morning. The U.S. media is offering a different picture of Covid-19 from science journals or the international media, a study finds.
Is bad news the only kind?
Bruce Sacerdote, an economics professor at Dartmouth College, noticed something last year about the Covid-19 television coverage that he was watching on CNN and PBS. It almost always seemed negative, regardless of what was he seeing in the data or hearing from scientists he knew.
When Covid cases were rising in the U.S., the news coverage emphasized the increase. When cases were falling, the coverage instead focused on those places where cases were rising. And when vaccine research began showing positive results, the coverage downplayed it, as far as Sacerdote could tell.
But he was not sure whether his perception was correct. To check, he began working with two other researchers, building a database of Covid coverage from every major network, CNN, Fox News, Politico, The New York Times and hundreds of other sources, in the U.S. and overseas. The researchers then analyzed it with a social-science technique that classifies language as positive, neutral or negative.
The results showed that Sacerdote’s instinct had been right — and not just because the pandemic has been mostly a grim story.
The U.S. media is an outlier
The coverage by U.S. publications with a national audience has been much more negative than coverage by any other source that the researchers analyzed, including scientific journals, major international publications and regional U.S. media. “The most well-read U.S. media are outliers in terms of their negativity,” Molly Cook, a co-author of the study, told me.
About 87 percent of Covid coverage in national U.S. media last year was negative. The share was 51 percent in international media, 53 percent in U.S. regional media and 64 percent in scientific journals.
Notably, the coverage was negative in both U.S. media outlets with liberal audiences (like MSNBC) and those with conservative audiences (like Fox News).
Sacerdote is careful to emphasize that he does not think journalists usually report falsehoods. The issue is which facts they emphasize. Still, the new study — which the National Bureau of Economic Research has published as a working paper, titled, “Why is all Covid-19 news bad news?” — calls for some self-reflection from those of us in the media.
If we’re constantly telling a negative story, we are not giving our audience the most accurate portrait of reality. We are shading it. We are doing a good job telling you why Covid cases are rising in some places and how the vaccines are imperfect — but not such a good job explaining why cases are falling elsewhere or how the vaccines save lives. Perhaps most important, we are not being clear about which Covid developments are truly alarming.
As Ranjan Sehgal, another co-author, told me, “The media is painting a picture that is a little bit different from what the scientists are saying.”
Why the bad-news bias?
The researchers say they are not sure what explains their findings, but they do have a leading contender: The U.S. media is giving the audience what it wants.
When the researchers examined which stories were the most read or the most shared on Facebook, they tended to be the most negative stories. To put it another way, the stories that people choose to read skew even more negative than the stories that media organizations choose to publish. “Human beings, particularly consumers of major media, like negativity in their stories,” Sacerdote said. “We think the major media are responding to consumer demand.”
That idea is consistent with the patterns in the data, Sacerdote added: It makes sense that national publications have better instincts about reaching a large audience than, say, science journals. And overseas, some of the most influential English-language media organizations — like the BBC — have long received government funding, potentially making them less focused on consumer demand.
All of that sounds plausible to me, but I don’t think it is the full explanation. I have worked in media for nearly three decades, and I think you might be surprised by how little time journalists spend talking about audience size. We care about it, obviously, but most journalists I know care much more about other factors, like doing work that has an impact.
In the modern era of journalism — dating roughly to the Vietnam War and Watergate — we tend to equate impact with asking tough questions and exposing problems. There are some good reasons for that. We are inundated by politicians, business executives, movie stars and others trying to portray themselves in the best light. Our job is to cut through the self-promotion and find the truth. If we don’t tell you the bad news, you may never hear it.
Sometimes, though, our healthy skepticism can turn into reflexive cynicism, and we end up telling something less than the complete story. I am grateful to Sacerdote, Cook and Sehgal for doing to us journalists what we normally do to others — holding up a mirror to our work and giving us a chance to do better.
by ponchi101 Why the bad news bias? Because that is the modern model of news. Bad news keep you nervous and on the edge, which makes you come back for more news, in hope that the news will be "not bad". When that does not happen, you come back for more.
Also, the pandemic must have been a panacea for news outlets. People stuck at home, with nothing else to do but mortify over the pandemic. Get the remote and flagellate yourself with more bad news.
I recommend "How to watch TV News" by Neil Postman. Written in the 1990's, and still very much up to date.
by JazzNU This also isn't an apples to apples comparison. You tell me when last spring and early summer there was good news to be had? Was it all the cases, all the illness, all the job losses, all the food lines, all the hospitalizations, or all the death? The good news of the vaccine actually being truly viable didn't come til November, no way could that overshadow the previous 9 months of news coverage. The US had more cases and deaths than anyone, so stands to reason the bad news would be more common here. They point out that when cases were falling, they highlighted places that were rising. Huh? It is well known that different regions of the US had different spikes at different times. Was the news supposed to ignore what was happening in Arizona, Florida, and Texas just because things had improved in the Northeast and the Midwest? And unless there's been a change, we're also the only industrialized country that didn't pay people to stay home adding to the unemployment and food lines. Other places curbed their outbreaks in a way that the US never did. They weren't sure whether to call what happened in the late summer and fall the "second wave" because most scientists agreed, we never truly got out of the first one.
There's a lot to criticize the US about, but I'm not sure this is one that needs a light shined on it. The news was keeping you informed. It was unfortunate but true that bad news was all we had for months on end in 2020.
by ti-amie When you had the former guy screaming about something that was killing thousands every day and other uninformed people echoing his words it was left up to the news organizations (Fox is not one of them in my opinion) to publicize just how bad it was. Maddow did a great job of this, tracking the disease as it moved outside of the North East and into the very places where people were denying the deadliness of the disease and how bad it was in their states.
by Deuce
ponchi101 wrote: ↑Wed Mar 24, 2021 5:50 pm
Why the bad news bias? Because that is the modern model of news. Bad news keep you nervous and on the edge, which makes you come back for more news, in hope that the news will be "not bad". When that does not happen, you come back for more.
Also, the pandemic must have been a panacea for news outlets. People stuck at home, with nothing else to do but mortify over the pandemic. Get the remote and flagellate yourself with more bad news.
I recommend "How to watch TV News" by Neil Postman. Written in the 1990's, and still very much up to date.
Indeed. Bad news also keeps people in fear - and this makes it easier for governments to keep the population under a certain control.
As for the media - of course they love this kind of thing. It used to be that they would wait in great anticipation for something like a plane crash. But they could only milk that coverage for a week or two. This virus has given them non-stop material for a full year - with really no signs of letting up.
Neil Postman was a genius. It would be very difficult to find a more insightful person.
I have several of his books, including the one you mention, and I don't recall ever disagreeing with anything written in any of them.
by ti-amie
by ti-amie
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
Editor’s Note: Our COVID-19 Situation Report team is taking a short break next week; we will not send updates on Tuesday, March 30 nor Friday, April 2. We’ll be back on Tuesday, April 6 with our curated analysis of the latest COVID-19 news and research.
Thanks to our wonderful team who pulls these together: Alyson Browett, Amanda Kobokovich, Margaret Miller, Christina Potter, Caitlin Rivers, Matthew Shearer, Marc Trotochaud, and Rachel Vahey.
EPI UPDATE The WHO COVID-19 Dashboard reports 124.9 million cases and 2.7 million deaths as of 12:00am EDT on March 26.
As global-level epidemiological trends indicate another COVID-19 surge, the epidemics in Brazil and India are driving a major portion of the global increase in daily incidence and mortality. Brazil’s current surge began in mid-November 2020, and its incidence has increased relatively steadily since then. It experienced brief decreases in daily incidence in early January and early-to-mid February 2021, but not enough to affect the overall trajectory. Conversely, India’s current surge began in late February 2021, but it is accelerating more rapidly. Brazil is currently #1 globally in terms of daily incidence, with more than 77,000 new cases per day. With more than 47,000 new cases per day, India is currently #3 globally; however, it could surpass the US (~59,000) as #2 in the coming days if it continues on its current trajectory. The global daily incidence was at a relative low on February 20, with 358,550 new cases per day, and since that time, daily incidence has increased by nearly 50% to 528,854—a difference of 170,304 cases. Notably, Brazil and India account for 38% of the global increase over that time (65,081 combined cases).
Brazil has reported more than 500,000 new cases each of the past 2 weeks, its 2 highest weekly totals to date. Brazil reported its highest single-day total on March 25, surpassing 100,000 new cases for the first time since the onset of the pandemic. Brazil’s daily incidence has increased 11% over the past 2 weeks and 50% over the past 4 weeks. On March 9, Brazil surpassed the US as #1 globally in terms of daily mortality, and its trend continues to increase sharply. With more than 2,300 deaths per day, Brazil is currently reporting more than a quarter of the global daily COVID-19 mortality. Last week, Brazil reported 15,650 deaths, its highest weekly total to date and 22% more than its previous record the week before. On March 23, Brazil reported 3,251 deaths, its highest single-day total. Brazil’s daily COVID-19 mortality has increased 34% over the past 2 weeks and doubled over the past 4 weeks.
While India’s current surge started much more recently, it is exhibiting a much sharper increase in daily incidence. India’s daily incidence has increased 146% over the past 2 weeks, and it has more than tripled since the beginning of March. On this trajectory, it will surpass the US as #2 globally in the next several days. India’s national records in terms of daily incidence remain from its peak in mid-September 2020 (93,198 new cases per day), but its epidemic currently is accelerating proportionately faster than at any time since May 2020, when the daily incidence was still fewer than 4,000 new cases per day. From its low on February 11, India is already 44% of the way back to its previous peak. India’s daily mortality is beginning to increase as well. Notably, the increase in mortality started on March 9, approximately 3 weeks after the daily incidence began to increase (February 16), consistent with the pattern exhibited throughout the pandemic. Since March 9, India’s daily mortality has more than doubled, from 102 deaths per day to 225—and is still accelerating. In fact, the current relative increase in mortality is India’s highest since June 2020.
India and Brazil are both in the top 5 globally in terms of total vaccine doses administered per day. Brazil is currently administering more than 500,000 doses per day, #5 globally, and India is #2 with 2.3 million. Both countries also are in the top 5 in terms of total cumulative doses administered—India at #3 (55.5 million doses) and Brazil at #5 (16.6 million). Both countries have very large populations, however, and they rank much lower in terms of the per capita daily and cumulative doses administered. With such large populations, even the large number of doses administered does not necessarily translate to high vaccination coverage. Brazil reports that 6.0% of its population has received at least 1 dose and 1.8% is fully vaccinated. In India, 3.4% of the population has received at least 1 dose and 0.6% is fully vaccinated. Both countries are far behind some other countries in terms of vaccination coverage, including Israel, the US, and the UK. For reference, the global average is 3.7% with at least 1 dose and 1.4% fully vaccinated, and many countries have not yet started vaccination efforts or have only recently started.
Global Vaccination
The WHO reported 456.8 million vaccine doses administered globally as of March 24, including 256.1 million individuals with at least 1 dose. The dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports that more than half a billion doses have been administered globally (508.2 million), a 23% increase compared to this time last week. The global cumulative total continues to increase at a rate of approximately 20% per week. The daily average continues to increase, up to 13.7 million doses per day (+29% compared to the previous week). At least 145 countries and territories are reporting vaccination data.
UNITED STATES
The US CDC reported 29.8 million cumulative cases and 542,584 deaths. Daily incidence has increased slightly over the past 5 days, up from 53,501 new cases per day to 57,249 (+7%). It is too early to determine if this is the beginning of a longer-term trend, but this is the highest daily incidence since March 7. Daily mortality continues to level off, hovering at slightly more than 1,000 deaths per day for more than a week.
US Vaccination
The US CDC reported 173.5 million SARS-CoV-2 vaccine doses distributed and 133.3 million doses administered. With 87.3 million individuals receiving at least 1 dose of the vaccine, more than a quarter of the entire US population (26.3%) and a third of all adults (33.7%) have been at least partially vaccinated. Of those, 47.4 million (14.3% of the total population; 18.3% of adults) are fully vaccinated. Among adults aged 65 years and older, 71.0% have received at least 1 dose and 44.8% are fully vaccinated.
The average daily doses administered* decreased slightly to 2.2 million doses per day, including 823,570 individuals fully vaccinated (ie, second dose of a 2-dose vaccine or a single dose of a 1-dose vaccine). In terms of full vaccination, 23.6 million individuals have received the Pfizer-BioNTech vaccine, 21.1 million have received the Moderna vaccine, and 2.7 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 30.1 million cumulative cases and 546,915 deaths as of 12:15am EDT on March 26.
ASTRAZENECA-OXFORD VACCINE PHASE 3 RESULTS Following questions about reported Phase 3 clinical trial efficacy data, AstraZeneca issued a press release containing updated results for its SARS-CoV-2 vaccine, developed in collaboration with the University of Oxford. The updated analysis estimates an overall efficacy of 76% against any symptomatic COVID-19 disease, slightly less that the 79% announced in the original press release. The updated analysis included an additional 49 symptomatic cases, bringing the total to 190 out of more than 32,000 participants, and an additional 14 possible or probable cases were identified, though they have not yet been adjudicated. Additionally, AstraZeneca reported 85% efficacy in adults aged 65 years and older and 100% efficacy against hospitalization and death. Notably, the new press release indicates there were 8 cases of severe COVID-19 disease among the placebo group. AstraZeneca noted that these figures “will be the basis for a regulatory submission [to the US FDA] in the coming weeks.” The clinical trial data have not yet been published publicly nor subjected to peer review.
EU VACCINE EXPORTS The European Union continues to weigh options that will limit the export of regionally produced COVID-19 vaccinations. The governing body this week proposed emergency legislation that would curb the number of vaccine exports over the next six weeks. AstraZeneca is in line to be most heavily impacted by these new rules. The company has been in conflict with the EU since the manufacturer reduced the number of COVID-19 vaccines they planned to deliver earlier this year. The EU’s original contract with AstraZeneca aimed to deliver 300 million vaccine doses by the end of June, but the company has since cut this target by two-thirds. While some EU leaders acknowledge the negative implications that curbing vaccine distribution will have on global vaccination targets, others are steadfast in their opinion that vaccine production companies work to meet earlier agreements. The EU has stressed that this new legislation will not be a blanket ban on regional exports and that there will be measures put in place to allow for flexibility of vaccine exports internationally.
PFIZER-BIONTECH VACCINE TRIALS IN CHILDREN Pfizer and BioNTech announced they are beginning a Phase 1/2/3 clinical trial evaluating their SARS-CoV-2 vaccine in children under the age of 12. Results from the trial are expected later this year, and depending on data, will support an application to the US FDA for emergency use authorization (EUA) this autumn, a company spokesperson noted. The companies finished enrolling a study of the vaccine among children ages 12-15 in January. The FDA already granted an EUA for use of the Pfizer-BioNTech vaccine among people ages 16 and older. The new trial intends to enroll 144 children in the first phase, which is aimed at identifying the preferred dosing level for 3 age groups—participants ≥5 to <12 years, ≥2 to <5 years, and ≥6 months to <2 years of age. Phase 2/3 will evaluate the safety, tolerability, and immunogenicity in each age group at the selected dose level from Phase 1, when compared with patients in a placebo arm. After 6 months, the trial will be unblinded and offer the vaccine to all participants. The trial is expected to enroll a total of 4,500 children in the US and UK.
The news follows announcements last week from Moderna that it began enrolling for a Phase 2/3 trial testing its SARS-CoV-2 vaccine, which is authorized for adults ages 18 and older, among children ages 6 months to less than 12 years. AstraZeneca last month began testing its vaccine in children 6 months and older, and Johnson & Johnson-Janssen has plans to extend its trials of its vaccine among younger children. Though children appear to be at lower risk of contracting SARS-CoV-2 compared with adults, the American Academy of Pediatrics estimates they account for 13% of US COVID-19 cases. Children comprise 23% of the US population, so vaccinating the younger population is critical to achieving herd immunity, according to experts. Vaccinating children also will help lower their and teachers’ risk of disease as they return to school buildings.
EMERGING VARIANTS & VACCINES In a letter published in the New England Journal of Medicine, infectious disease experts from South Africa provide an overview of emerging COVID-19 variants, including those that have become the dominant strain in several countries, and evaluate the implications for vaccine efficacy, transmissibility, and disease severity. The authors highlight the B.1.1.7 strain, first identified in the UK; B.1.351 (501Y.V2), first identified in South Africa; and P.1 (B.1.1.28.1), first reported in Brazil, and note the need for continued genomic surveillance to manage variants.
A group led by researchers from the London School of Hygiene and Tropical Health report on case fatality risk of the B.1.1.7 variant in an Eurosurveillance article. Noting the strain is now dominant in the UK and increasing in prevalence across Europe, the authors evaluated the case fatality risk of the variant in England from November 2020-January 2021. Infection with the variant of concern (VOC) was consistently associated with an increased hazard of death, and once adjusted for comorbidities and demographics, the researchers found a two-thirds higher hazard ratio in the VOC group (1.67 HR, 95% CI: 1.34-2.09).
The B.1.351 (501Y.V2) variant, now the dominant strain in South Africa, elicits cross-reactive neutralizing antibodies that may provoke an immune response capable of fending off multiple variants. In a preprint study published in bioRxiv, South African researchers describe how sera from B.1.351-infected patients showed robust binding and neutralizing activity against variants from the first wave of infections in South Africa as well as against the P.1 variant. The cross-reactive responses of sera from B.1.351-infected patients suggests the broad specificity potential of a vaccine designed with the that variant’s sequence. Moderna is conducting a Phase I clinical trial of its mRNA-1273.351 vaccine, which encodes for a protein specific to the B.1.351 variant. Other developers are expected to follow suit.
The B.1.1.7 variant has been identified for the first time in household pets. In a preprint study published in bioRxiv, veterinarians from a specialty veterinary clinic located in the southeast of England describe the first cases of B.1.1.7 infection among 8 cats and 3 dogs, all of which required veterinary visits due to new-onset symptoms, including lethargy, loss of appetite, rapid breathing, and severe cardiac abnormalities. All of the owners had tested positive for SARS-CoV-2 prior to their pets developing symptoms. In another report, researchers from Texas A&M University, as part of an ongoing research project funded by the US CDC, describe a cat and dog from the same household infected with the B.1.1.7 variant but showing no symptoms at the time of initial testing. Their owner was diagnosed with the B.1.1.7 variant only two days prior to the pets’ tests. The report notes both pets later developed symptoms, including sneezing, that resolved after one month. The researchers say these cases raise questions regarding the risk companion animals may play in the COVID-19 pandemic, particularly given the enhanced infectivity and transmissibility of the B.1.1.7 variant, and encourage additional research.
GERMANY EASTER SHUTDOWN On March 22, Germany announced highly restrictive COVID-19 “emergency brake” measures that were scheduled to be in effect through April 18, including additional restrictions over the Easter holiday weekend. However, German Chancellor Angela Merkel reversed that decision on March 24. Chancellor Merkel noted that the plan was finalized too close to the start date and that too many questions remained regarding how to implement the restrictions. The original plan included “quiet days” on April 1 and April 3, the Thursday before and Saturday of Easter weekend, during which non-essential businesses would be closed and gatherings would be limited to individual households plus one additional individual, up to 5 total individuals. Additionally, the restrictions would have limited gatherings in churches and other religious services. Combined with the existing national holiday dates on Friday and Monday, the restrictions would have resulted in a 5-day national shutdown over Easter weekend. Germany’s daily incidence has more than doubled since its low on February 14, including a 69% increase over the past 2 weeks.
On March 25, Germany announced a reinstatement of vaccination efforts using the AstraZeneca-Oxford vaccine. Germany resumed use of the vaccine following safety analysis by the European Medicines Agency (EMA) and Germany’s Paul Ehrlich Institute (PEI). Vaccination with this vaccine was paused on March 15 over concerns regarding the possible associated risk of blood clots (thromboembolic events) following vaccination.
US EVICTION MORATORIUM The US government is weighing an extension of a federal policy prohibiting landlords from evicting tenants who have fallen behind on paying rent during the COVID-19 pandemic. The extension, which would impact an estimated 10 million families, could run through at least July. Without an extension, the ban is set to expire at the end of this month. The recently passed stimulus bill, known as the American Rescue Plan, included more than $40 billion to help homeowners and renters behind on their mortgage and rent payments. However, due to implementation delays, many people have not yet received the assistance, putting pressure on the government to extend the ban. According to a survey by the Census Bureau released last week, nearly 1 in 5 renters say they are behind on payments, with people of color bearing a majority of the hardship. According to the Washington Post, some officials at the US CDC, which implements the policy, have expressed concern over the agency overseeing the ban, saying it was implemented in a way no one thought possible. Biden administration officials largely have been silent on the extension and have not named another agency that could steward the policy.
COVID-19 WAVES IN AFRICA In a report published online in The Lancet, researchers led by the Africa CDC detail the first and second waves of SARS-CoV-2 infections across the African continent from February 2020 to December 2020. Using epidemiological, testing, and mitigation strategy data reported by African Union (AU) member states, the group conducted descriptive analyses for cumulative and weekly incidence rates, case fatality ratios (CFRs), tests per case ratios, growth rates, and public health and social measures in place. Their analysis showed the continent experienced a more aggressive second wave of infections compared to the first. In July 2020, at the peak of the first wave, the continent’s mean daily number of new cases was 18,273, with that number rising to a mean of 23,790 daily new cases by the end of December 2020, representing a 30% increase. Nine of 55 AU member states accounted for 82.6% of reported cases as of December 2020, and eighteen countries reported CFRs greater than the global CFR of 2.2%. By April 15, 2020, 96% of 50 AU countries had five or more stringent public health and social measures in place, but that number decreased to 36 (72%) countries as of December 31, 2020, despite an increasing number of cases.
Dr. John Nkengasong, Director of the Africa CDC and one of the study’s authors, said the increase in cases likely was due to several factors, including lower adherence to public health mitigation strategies like mask wearing and physical distancing as well as a growing prevalence of more infectious SARS-CoV-2 variants. In a statement to CNN, he called on countries to improve testing capacity, strengthen their public health campaigns, and recognize the importance of balancing mitigation strategies with economic needs. Dr. Nkengasong also called for a scale-up of vaccine distribution throughout the continent, warning some countries are beginning to see the start of a third wave.
CUBAN VACCINES Cuba announced that one of its five SARS-CoV-2 vaccine candidates, Soberana 2, has had promising preliminary results and is entering a Phase 3 trial involving 44,000 people. This is the first SARS-CoV-2 vaccine developed in Latin America to enter the final phase of testing. A second Cuban vaccine candidate, named Abdala, has entered Phase 3 testing. Several Cuban experts shared that the country could produce enough vaccinations for its entire population by the end of the summer, assuming the vaccine candidate proves successful in the last phase of clinical trials. This is a major development for Cuba, which has not yet purchased foreign-produced vaccines nor attempted to acquire vaccines through the COVAX initiative. By May, Cuba plans to administer one of its experimental vaccines to 1.7 million people, nearly the entire population of the capital, Havana. The country already has begun vaccinating the city’s frontline workers. Havana is experiencing its worst outbreak since the beginning of the pandemic, according to local authorities.
US GOVERNMENT PATENT A group of public health advocates and academics is urging the US NIH to negotiate with Moderna to create patent licensing terms that would help speed the production and reduce the price of its SARS-CoV-2 vaccine for use in low- and middle-income countries (LMICs). At issue is a key patent owned by the US government that applies to the spike protein molecule necessary for Moderna’s vaccine to elicit a human immune response against the virus. The group, led by PrEP4All, claims the patent is being used by 5 different vaccine manufacturers, although only one, BioNTech, has paid to obtain a license. Historically, the US government has been reluctant to exert its patent rights over private sector partners. However, the US government filed a lawsuit in 2019 against the pharmaceutical company Gilead over a patent used in the HIV treatment and prevention medications Truvada and Descovy. That lawsuit is pending. Some patent lawyers and public health experts say similar lawsuits over the SARS-CoV-2 patent are possible unless other companies negotiate licensing agreements with the government.
SINOPHARM VACCINE Reports are emerging from the United Arab Emirates (UAE) that some individuals vaccinated with the Sinopharm vaccine from China may require a third dose. Some individuals have not developed sufficient immune response following their second dose, and they may benefit from a third dose to stimulate the appropriate antibody response. The UAE reportedly has implemented a program to reach out to individuals with low antibody response and offer them an additional booster. It is unclear what proportion of vaccinees are affected or the degree to which they benefit from a third dose, but it is not necessarily rare for individuals to not respond to vaccines against other pathogens. China has distributed its vaccines, including the Sinopharm vaccine, to numerous other countries; however, Phase 3 clinical trial data for these vaccines have not yet been published publicly. Sinopharm has reported efficacy of 79%. The UAE issued an emergency authorization for the Sinopharm vaccine in September 2020, prior to the completion of a Phase 3 clinical trial conducted there.
COMBATING MISINFORMATION The COVID-19 pandemic has illustrated that health-related misinformation and disinformation can dangerously undermine responses to public health crises. To address this issue, the Johns Hopkins Center for Health Security published the National Priorities to Combat Misinformation and Disinformation for COVID-19 and Future Public Health Threats. The report provides an overview of mis- and disinformation challenges during the pandemic—including contradictory messaging and active subversion, increased mistrust in science, and the politicization of public health measures—and ongoing efforts to counter them. The report also presents a series of recommendations targeted at a broad range of stakeholders, including media companies, government officials, and the public. The report also calls for a national strategy, under the purview of the National Security Council (NSC), to coordinate government activities and policies to counter mis- and disinformation and to develop evidence-based guidelines and recommendations for nonpartisan oversight of these challenges.
PANDEMIC PREPAREDNESS On Tuesday, March 30 at 11am EDT, Anita Cicero, JD, Deputy Director of the Johns Hopkins Center for Health Security, will moderate a webinar for the Capitol Hill Steering Committee on Pandemic Preparedness and Health Security, titled “Strengthening the Supply Chain for US Pandemic Response: Strategies for Stockpiling, Surge Capacity, and Distribution.” The webinar will examine supply challenges in the ongoing COVID-19 pandemic, vulnerabilities exposed by the pandemic, and emerging lessons from both the private and public sectors that can inform new policies and practices that enhance US preparedness for future pandemics. The non-partisan Steering Committee is sponsored and managed by the Johns Hopkins Center for Health Security. Register for the webinar here.
by Deuce The world has been getting increasingly vaccinated over the past few months.
Despite that, cases of COVID-19 are rising more and more rapidly in many - maybe most - countries.
This isn't how it was 'supposed' to happen.
At this point, in the race between the variants and the vaccines, the variants are winning.
Everyone seemed sure that 2021 would be significantly better than 2020 was.
It's looking now like that may not be the case.
by Suliso Vaccination rates, except in 3-5 countries, are still very low.
by ponchi101 Down here, we went to our local health provider to see how my GF could get registered for the vaccine. Just a few elderly people were in line.
The GOV has decided this: they import the vaccine but then hand them over to the health providers, all of which have good vaccination programs and are better equipped to handle that process. But the bottleneck is still the quantity: the amount of doses available is laughable. So no real progress is being done.
I was able to register us both on the website which simple gave me a reply: "You will be contacted when your turn is set". One interesting "detail": the registration has to be validated via CAPTCHA, and when I did so, the question is IN ENGLISH. Wonder how many people will not be able to answer.
Cuban vaccine. Venezuela will start getting it too, as part of an exchange. I am starting to really worry about my family there. Heck, I do not even trust Cuban RUMS, much less a vaccine.
by Suliso Which vaccine is Colombia getting even in small amounts? Astrazeneca?
by ponchi101 Both Chinese and Pfizer/BioNTech. But I really can't tell you the percentages.
We already had the first news of big shots skipping the line. You know, we are who we are. Those are getting Pfizer.
by Deuce
Suliso wrote: ↑Fri Mar 26, 2021 9:25 pm
Vaccination rates, except in 3-5 countries, are still very low.
Low rates of vaccination is still considerably higher than no vaccinations, which is obviously what we had prior to people first being vaccinated.
My point is that the rate of infections is increasing at the same rate as before the vaccinations. Here in Canada, we have a little over 10% of the population who have received at least one dose. That's a significant proportion. Yet our rates of infection are rising and will presumably soon be at the same level as they were prior to anyone being vaccinated. The infection rates are already higher now than they were at certain times in 2020.
Some major European countries are having to lock down again, despite vaccinations...
It doesn't look good to my eyes.
It's going to get worse than people thought before it gets better - and is going to take considerably longer to get better than people thought when the vaccines began.
by Suliso Actually 10% is virtually nothing as far as population protection is concerned. Obviously very good for those 10% mostly old people who're now unlikely to die. If you don't believe me you can play around with math yourself. Take R number of 1.2 (means 10 sick people will infect 12 new ones) and just 10% probability of these 10 encountering a vaccinated person...
To show any serious statistical effect at least 30% should have had the first dose, for a serious protection 60-70% (including children). Only Israel has reached the latter, perhaps UK and parts of US the former.
by Suliso Just for clarity I should add - if 80% of 70+ population is vaccinated but nobody else you would expect lower fatalities since that is the most vulnerable segment but not really have any effect on the overall spread. That's assuming vaccine is incredibly effective, if it's not then vastly higher spread might compensate protection.
by Deuce Vaccines are not supposed to protect only against severe symptoms and death, they are also supposed to protect against being infected. If 10% of a population have been vaccinated, one would expect that approximately 10% less of the population should become infected. But we're seeing more people being infected, not less. I assume this is due to the variants being more easily transmitted.
I agree that obviously the more people who are vaccinated, the more that a city, country, etc. will be protected.
But, again, my point is that virtually everyone was saying that once we get the vaccines rolling out, the number of infections will begin to slowly but surely decrease. And instead, the number of infections is increasing. Many countries are well into a third - or fourth - wave now, and these third/forth waves have begun months after vaccinations began.
I didn't hear this being predicted by anyone.
Most 'experts' are saying now that it is literally a race between the vaccines and the variants. That is, the number of people being vaccinated vs. the number of people being infected with a variant. And in many countries, the variants are winning.
by ti-amie If anyone is watching the Andreescu/Martincova match and watched the Sloane Stephens/Amanda Anisimova matches taking place in Florida you'd get a good idea of why things are how they are. The coaches of Stephens and Andreescu just stopped wearing their masks during their players matches.
It's so frustrating.
by Suliso
Deuce wrote: ↑Fri Mar 26, 2021 10:46 pm
Vaccines are not supposed to protect only against severe symptoms and death, they are also supposed to protect against being infected. If 10% of a population have been vaccinated, one would expect that approximately 10% less of the population should become infected. But we're seeing more people being infected, not less. I assume this is due to the variants being more easily transmitted.
Yes, but at any given time vast majority of us are NOT infected. Imagine a virus walking on a street in Toronto with a virus gun and shooting people on random, 10% of these people have body armor (vaccine) and thus maybe hurt but not so badly unless there is a lucky shot (correlates to vaccine effectiveness). Now imagine that the old version has 10 bullets, with 10% protected 9 people will be hit. The new variant is more virulent and gets 15 bullets, - despite 10% protection 13 people will be hit. Now add another complexion - virus only has 30 min to do all the shooting. If the street is very crowded (zero social distancing) very easy to get his 13 targets, now if street is nearly deserted (masks, good social distancing) he'll not get all 13 targets before time is over.
Let me know if I what I wrote makes sense. I understand statistics myself to some extent, but explaining without graphs or formulas tough...
by Suliso Menwhile Zverev lost to Ruusuvuori. Color me surprised...
by Deuce
ti-amie wrote: ↑Fri Mar 26, 2021 10:52 pm
If anyone is watching the Andreescu/Martincova match and watched the Sloane Stephens/Amanda Anisimova matches taking place in Florida you'd get a good idea of why things are how they are. The coaches of Stephens and Andreescu just stopped wearing their masks during their players matches.
It's so frustrating.
Yes - the people in Sloane's camp seemed to be taking turns throughout the match as to who would take the mask off. There were 3 of them, and there always seemed to be a different one who had the mask off at different times.
It's obviously hot and humid, which makes wearing a mask more uncomfortable... but still - if you're going to be sitting together for an extended period of time, keep the mask on. Otherwise, just sit 10 feet apart from each other.
I do wonder, though, why anyone sitting alone in an outdoor match - with no-one within 20 feet of them - keeps the mask on. I've seen that too. Bizarre.
Deuce wrote: ↑Fri Mar 26, 2021 10:46 pm
Vaccines are not supposed to protect only against severe symptoms and death, they are also supposed to protect against being infected. If 10% of a population have been vaccinated, one would expect that approximately 10% less of the population should become infected. But we're seeing more people being infected, not less. I assume this is due to the variants being more easily transmitted.
Yes, but at any given time vast majority of us are NOT infected. Imagine a virus walking on a street in Toronto with a virus gun and shooting people on random, 10% of these people have body armor (vaccine) and thus maybe hurt but not so badly unless there is a lucky shot (correlates to vaccine effectiveness). Now imagine that the old version has 10 bullets, with 10% protected 9 people will be hit. The new variant is more virulent and gets 15 bullets, - despite 10% protection 13 people will be hit. Now add another complexion - virus only has 30 min to do all the shooting. If the street is very crowded (zero social distancing) very easy to get his 13 targets, now if street is nearly deserted (masks, good social distancing) he'll not get all 13 targets before time is over.
Let me know if I what I wrote makes sense. I understand statistics myself to some extent, but explaining without graphs or formulas tough...
Yeah - I get what you're saying. I even understand it . But I didn't hear this being predicted, except after it had already begun.
I suppose the joker in the equation is the variants being more transmissible, and thus overriding (for now, at least) the effect of vaccine protection. I don't mean that the variants are still infecting those who've been vaccinated (which may or may not be the case - only time will tell on that), but that, as in your shooting explanation, the vaccine isn't protecting as many people as the variants are infecting, relatively speaking.
by Suliso
Deuce wrote: ↑Fri Mar 26, 2021 11:11 pm
Yeah - I get what you're saying. I even understand it . But I didn't hear this being predicted, except after it had already begun.
I suppose the joker in the equation is the variants being more transmissible, and thus overriding (for now, at least) the effect of vaccine protection. I don't mean that the variants are still infecting those who've been vaccinated (which may or may not be the case - only time will tell on that), but that, as in your shooting explanation, the vaccine isn't protecting as many people as the variants are infecting, relatively speaking.
Yes!!! That's exactly my point.
As for predicting these things a lot has to do with poor understanding of exponential growth by decision makers and also many doctors. The confusion also arose because we eventually had two epidemics going on at the same time - old variant which was declining (mostly due to social distancing but also vaccines) and the new one which is expanding. While the new one was only 20% or less data was obscured, particularly if no genetic analysis took place.
Watch the animation below for exponential growth
by Suliso Maybe an even better graph - the red line is a standard linear growth. An example would be you filling your bathtub at a constant x l/min. The green line is an exponential growth. That relates to things like nuclear explosions, population growth, compounding interest and also unfortunately viral infections.
by ti-amie
Suliso wrote: ↑Fri Mar 26, 2021 11:03 pm
Menwhile Zverev lost to Ruusuvuori. Color me surprised...
That makes two of us.
by atlpam I think a big part of the issue in the US is that the younger population is now taking more risk because they feel like they don't need to worry about protecting the older vaccinated population anymore. When I look at the Georgia trends, the cases are ticking back up in the 30-59 group, but the 7-day average for over 60 is still trending down. I'm hopeful that now that the state has opened vaccine eligibility to everyone 16 and over that our overall %vaccinated will start to reverse the upward case trend. I for one will still be limiting my socializing to primarily outdoor activities. I am looking forward to having some friends over for dinner once we are all vaccinated.
by ti-amie Sorry but I don't trust this one bit. I'll carry my little white card thank you very much.
NY Launches Vaccine Passport For Use At Venues, But Privacy Expert Urges You To Read The Fine Print
BY DAVID CRUZ
MARCH 27, 2021 1:25 P.M.
As a way of helping stadiums and concert halls reopen safer, faster and at greater capacity, the state has rolled out a smartphone app that confirms whether someone has received a COVID vaccine or recent negative test for the coronavirus. But one expert contends that the platform's privacy policy fails to outline how secure the app really is.
"It's really just high-tech hydroxychloroquine," Albert Fox Cahn, an attorney and founder of Surveillance Technology Oversight Project—an advocacy group ensuring privacy rights are upheld—said of the "Excelsior Passport" app.
The app officially launched Friday following a trial run involving thousands of New Yorkers testing the program. The Excelsior Passport is the first of its kind to be rolled out in United States and allows specific sites that administer COVID vaccines or test for the coronavirus to upload the data to the app.
The app, produced by IBM in partnership with the state, functions similar to a virtual airline boarding pass. Activating the passport produces a secure QR code that can then be shown and scanned by a participating business or venue using a companion app to confirm someone has been vaccinated or recently tested negative for the virus. A pass can also be printed and shown at the door. The state said other types of proof can be used at the door as a way of "reducing any barriers to usage."
So far, big venues such as Madison Square Garden in Manhattan have announced they will begin using the technology over the next few weeks, with owner James Dolan saying the app is "critical to New York's recovery." Users who don't have a smartphone can also bring physical documentation from a healthcare provider showing they either received a vaccine or tested negative for the coronavirus.
The hope is to decrease virus transmission in large venues and even allow them to operate at greater capacity as the state's reopening moves along. In a statement, Governor Andrew Cuomo said Excelsior will allow "more sectors of the economy to reopen safely and keeping personal information secure."
The state is opening the use of the Excelsior Passport to smaller venues in the arts and entertainment business beginning April 2nd. The roll out of the app comes just weeks after the state announced that baseball stadiums can start the seasons with limited numbers of fans in the stands beginning April 1st. Venues that do use the technology will be allowed to open at greater capacity. Those that don't will continue to face more stringent capacity restrictions.
IBM and the state insist user data will be kept confidential thanks to the use of blockchain technology, which records public data that can then be safely stored in a variety of database. But Cahn told Gothamist/WNYC that the fine print does not explicitly state how the data is tracked or safeguarded.
"I have more detailed technical documentation about the privacy impact of nearly every app on my phone than I do for this health pass," Cahn said. "IBM and the governor are using lots of buzzwords, but they're not explaining their cryptographic model. They're not explaining the security, implementation. And on top of it, the past itself is incredibly revealing, disclosing not only people's health status, and name but their date of birth."
Cahn said there are no guarantees listed on the terms of service determining whether the information won't be accessed by police departments or the Immigration or Customs Enforcement agency.
Cahn specifically pointed to the application's terms and services, which he said "have absolutely nothing to do with this type of app" and don't specifically cite the type of blockchain technology—including public, private, consortium, or hybrid–IBM utilizes.
"I know that it's very easy for this to come off as sort of alarmist or as over the top," Cahn said. "But, no, usually when I'm pushing back against these apps, I'm pushing back on the periphery; I'm making mild critiques. This is just like, my jaw hit the floor when I read how poorly this policy was written."
Cahn also criticized the state's use of a system requiring a smartphone, which he said creates a new form of "digital segregation" since it would exclude the millions of New Yorkers who lack a smartphone.
Cuomo's office did not immediately respond to a request for comment.
by ponchi101 Sorry, but: the MILLIONS of New Yorkers that lack a smartphone? Is that correct? NYC is a town with MILLIONS of tech-troglodytes?
I want my little white card too. Actually, I will tell them to paste the sticker of my vaccine on my yellow fever vaccination card, which has my other vaccines too.
by ti-amie
ponchi101 wrote: ↑Sat Mar 27, 2021 5:57 pm
Sorry, but: the MILLIONS of New Yorkers that lack a smartphone? Is that correct? NYC is a town with MILLIONS of tech-troglodytes?
I want my little white card too. Actually, I will tell them to paste the sticker of my vaccine on my yellow fever vaccination card, which has my other vaccines too.
There are many NY'ers who are on special programs for disadvantaged people who do not have smart phones. In the Before Time I used to see this a lot when I took the bus to church.
If MSG is going for it I expect the USO will do the same. And that would be an existential crisis for me.
by ti-amie
by ti-amie My daughter's inlaw's hold a family Zoom chat once a week. I jump in from time to time. They're pushing very hard to have everyone together on Mother's Day at either my daughters mother-in-law or at her sister's new place in New Jersey.
I noticed that when you say you have gotten either your first or second shot the next question is "which one". The preference seems to be for Pfizer. I think it's safe to say that in this part of the world it's considered the gold standard.
by Suliso Better than Moderna? They seem functionally indistinguishable to me.
by JazzNU Most people I know ask which one, but there isn't a gold standard in my circles, just curiosity and sometimes questions about how things went in terms of side effects. But nothing further than that.
I haven't changed Mother's Day plans. I made an outdoor dinner reservation and everyone is on board with that as the safest option. I've thought about making a backup indoor reservation in case it is pouring, but the place I made the reservation at has a great outdoor area that is covered, so I think it'll still work.
by JazzNU
ti-amie wrote: ↑Sat Mar 27, 2021 5:59 pm
There are many NY'ers who are on special programs for disadvantaged people who do not have smart phones. In the Before Time I used to see this a lot when I took the bus to church.
There's also many low income who are on subsidized plans with limited data and minutes. If say, they need to verify vaccination on the 20th of the month? Might be dicey. Pretty common to run out of your small allotted amounts.
by ponchi101 Sure. It is a huge city, which I understand is 8MM people strong at the very lower possible count. But THE MILLIONS? That is where I am wondering. Of course you must have the one guy in NYC that has no phone, smart or dumb, no WiFi, no PC and still pays cash for everything, after withdrawing his money by cashing a check. But THE MILLIONS seems a bit too much.
I can assure you there are not MILLIONS of people in Bogota without a smartphone.
by JazzNU So I think it likely is millions. It's been a several years since I've seen figures and maybe it's improved. But the issue is the smartphone vs, dumb phone. I think it's something like 90% who might have a cell phone. But more like 70-75% who have a smartphone. If those are around the right numbers are correct it would mean millions. The other issue is going to be age. There's a few million in NY that are over age of 65, and the older you are, the less likely you are to own a smartphone.
by ponchi101 Ok. I am surprised. It has been a while since I have seen somebody with a dumb phone here in Bogota. Even the old people have smartphones. They don't know how to use them, but they have them. They have grandchildren to teach them, I guess.
by Deuce When I meet someone who doesn't have a cell phone (let alone a 'smart' one), I admire them. A good friend of mine got his first cell phone just 2 years ago.
My ultimate wish is to meet a woman who has no cell phone, and go to and live in the woods, just her and I.
Oh... and she'll have to kind of like me, too...
Any 'vaccination certificate' on a smart phone can be copied/duplicated - I would think very easily by 'hackers' - to produce - and sell - fraudulent certificates which would serve the same purpose as the legitimate ones.
The same for any physical vaccination certificate card.
How long will it be before someone proposes inserting a microchip somewhere under a person's skin as a certificate of vaccination? And even that would eventually be able to be fraudulently duplicated.
As I've said before - the virus isn't the main problem... the main problem is the human animal.
by ponchi101 Why would you want a fraudulent vaccination certificate? If you are anti-vaxx, you wear that as a badge of honor. You are not and will not be vaccinated, and you will say that proudly. If you believe in vaccination, you really want to be vaccinated, not carry a fake certificate. There is no profit motive to buy a vaccine certificate if the vaccine is available and relatively cheap.
by JazzNU
ponchi101 wrote: ↑Sat Mar 27, 2021 9:56 pm
Ok. I am surprised. It has been a while since I have seen somebody with a dumb phone here in Bogota. Even the old people have smartphones. They don't know how to use them, but they have them. They have grandchildren to teach them, I guess.
Now, I can never tell if you'll be able to view a site or not, but hopefully you're able to see this. Most of the cell carriers continue to have dumb phones. They started to get rid of them a few years ago, but there was pushback to keep several options available. Popular choices for seniors and kids. There appears to be a comfort in using them for the seniors with not a lot of extra stuff on them, and for the kids, a security measure as well as a parenting decision many times.
ponchi101 wrote: ↑Sat Mar 27, 2021 10:11 pm
Why would you want a fraudulent vaccination certificate? If you are anti-vaxx, you wear that as a badge of honor. You are not and will not be vaccinated, and you will say that proudly. If you believe in vaccination, you really want to be vaccinated, not carry a fake certificate. There is no profit motive to buy a vaccine certificate if the vaccine is available and relatively cheap.
Umm... if you don't want to be vaccinated, but you do want to attend basketball games, or concerts, or to fly in an airplane, etc...
As such, I would think there would be a significant market for fraudulent certificates.
by ti-amie
by ponchi101 Superb animation but: my understanding is that that is the mechanism that EVERY virus uses to replicate itself. Hijacking your cells' replication functions to multiply.
Are there other types of viruses? Too lazy right now to go look in my library.
by mmmm8 Re: Smartphones.
I don't know if it's millions who in fact have no cell phones or a "dumb" phone only, but another factor is that to get a smartphone plan from a provider, which gives it to you at a discount and a "loan" (i.e. you don't pay for the phone outright), you often need credit history and maybe proof of income and a lot of New Yorkers are recent immigrants or unemployed/don't have credit history, or are children. For them, the smartphones may be registered to relatives or otherwise not tracked, so I would guess that group accounts for some of the "millions"
by Deuce
ponchi101 wrote: ↑Sun Mar 28, 2021 3:19 pm
Superb animation but: my understanding is that that is the mechanism that EVERY virus uses to replicate itself. Hijacking your cells' replication functions to multiply.
Are there other types of viruses? Too lazy right now to go look in my library.
So... you have a library of viruses that you're just waiting to unleash on the world?!!?
by dryrunguy Sidebar: According to this morning's NY Times e-newsletter, roughly 125 people in Brazil are dying every HOUR due to COVID--and those are just the ones we know about.
by ti-amie
dryrunguy wrote: ↑Sun Mar 28, 2021 10:12 pm
Sidebar: According to this morning's NY Times e-newsletter, roughly 125 people in Brazil are dying every HOUR due to COVID--and those are just the ones we know about.
The numbers out of Brazil have always been suspect as you know dry. The same with the numbers out of India. There are many, many people in both countries who are not being tested or monitored.
by Suliso What I hear anecdotally from my Indian friends is that everything seems normal and not too many people affected. Brazil at least right now is completely different.
by ti-amie
Suliso wrote: ↑Sun Mar 28, 2021 10:27 pm
What I hear anecdotally from my Indian friends is that everything seems normal and not too many people affected. Brazil at least right now is completely different.
Maybe ask them about the tribal areas of their country suliso.
Suliso wrote: ↑Sun Mar 28, 2021 10:27 pm
What I hear anecdotally from my Indian friends is that everything seems normal and not too many people affected. Brazil at least right now is completely different.
Maybe ask them about the tribal areas of their country suliso.
They are upper middle class folks from Mumbai and Bangalore. Would know nothing about tribal areas...
Suliso wrote: ↑Sun Mar 28, 2021 10:27 pm
What I hear anecdotally from my Indian friends is that everything seems normal and not too many people affected. Brazil at least right now is completely different.
Maybe ask them about the tribal areas of their country suliso.
They are upper middle class folks from Mumbai and Bangalore. Would know nothing about tribal areas...
by JazzNU
mmmm8 wrote: ↑Sun Mar 28, 2021 9:31 pm
Re: Smartphones.
I don't know if it's millions who in fact have no cell phones or a "dumb" phone only, but another factor is that to get a smartphone plan from a provider, which gives it to you at a discount and a "loan" (i.e. you don't pay for the phone outright), you often need credit history and maybe proof of income and a lot of New Yorkers are recent immigrants or unemployed/don't have credit history, or are children. For them, the smartphones may be registered to relatives or otherwise not tracked, so I would guess that group accounts for some of the "millions"
This is no longer the case though. Prepaid phones which don't require any credit check being readily available counteracts that previous large barrier to having a cell phone of some kind. They don't need to be registered and can be bought with cash, hence the name burner phones.
mmmm8 wrote: ↑Sun Mar 28, 2021 9:31 pm
Re: Smartphones.
I don't know if it's millions who in fact have no cell phones or a "dumb" phone only, but another factor is that to get a smartphone plan from a provider, which gives it to you at a discount and a "loan" (i.e. you don't pay for the phone outright), you often need credit history and maybe proof of income and a lot of New Yorkers are recent immigrants or unemployed/don't have credit history, or are children. For them, the smartphones may be registered to relatives or otherwise not tracked, so I would guess that group accounts for some of the "millions"
This is no longer the case though. Prepaid phones which don't require any credit check being readily available counteracts that previous large barrier to having a cell phone of some kind. They don't need to be registered and can be bought with cash, hence the name burner phones.
But those are mostly not smartphones or very low model smartphones and not what people not looking to hide their identity are after. Case in point, my partner doesn't have a US credit history but there was a Black Friday deal we found where Verizon (my provider) was giving away the latest iPhone at a net negative cost (we got back ~$50 above the phone retail price) for new customers (he probably wouldn't have qualified for financing) OR if I added a new line, so we did that and now his phone is in my name.
by ti-amie
by JazzNU
mmmm8 wrote: ↑Mon Mar 29, 2021 12:11 pm
But those are mostly not smartphones or very low model smartphones and not what people not looking to hide their identity are after. Case in point, my partner doesn't have a US credit history but there was a Black Friday deal we found where Verizon (my provider) was giving away the latest iPhone at a net negative cost (we got back ~$50 above the phone retail price) for new customers (he probably wouldn't have qualified for financing) OR if I added a new line, so we did that and now his phone is in my name.
I mentioned burner phones because they are just a well known way to refer to them in pop culture in case people weren't sure of the phones I was talking about, not because this is an instance where people are concerned about their identity. But the point remains.
Prepaid phones and plans are all over the place and many users may not get the latest and greatest iPhone, but it's not just the worst smartphones on the market either. It all comes down to what you want to spend. When you're talking about Verizon, AT&T, T-Mobile? That's different. They are known as mostly postpaid carriers. But their have prepaid carriers either as part of their business now or one of their partners and those carriers run on their networks. Cricket, Boost Mobile, Metro PCS, TracPhone, etc. are where you need to go for prepaid plans that do not require credit checks.
You don't have to take my word for it, you can see the kind of smartphones you can get on those sites. And there are in-store options for this as well. Walmart, for instance, is a big seller of prepaid phones and plans or pay as you go minutes. This segment of the cell phone market is significant, I don't remember the more recent estimates, but know it passed 50 million awhile ago.
And now I know why "impending doom" was trending on Twitter. I refused to click on it as I just didn't need whatever bad news it was in the middle of my day. Very sad, but I saw those air travel numbers of late, so not surprising.
by Suliso Getting a prepaid Sim card in US on your smartphone bought elsewhere is no problem either. It takes 20 min max and nothing needs to be financed nor there need to be a credit history. So if someone only a week in the country could do it there should be no issue for locals either. Obviously assuming you've got a bit of money.
by ti-amie
Andy Slavitt @aslavitt46
But 1,000 Americans are still dying every day.
We must wear a mask through the final stretch until millions more complete their vaccinations.
by dryrunguy Anxious to see how that pledge of being able to get a vaccine within 5 minutes of my home will work here--or if I'll be part of that outlying 10%.
by Suliso Probably the closest pharmacy or doctor's practice which might not be 5 min.
by MJ2004 Honestly it’s been a year and people are just burned out. Combine that with expectations of the vaccine, the knowledge that grandparents are now protected, and spring weather, and people going to be taking risks they shouldn’t.
by JazzNU
‘Real world’ study by CDC shows Pfizer and Moderna vaccines were 90% effective
By Helen Branswell
A new study suggests the messenger RNA vaccines produced by Moderna and the Pfizer-BioNTech partnership appeared to be 90% effective in preventing Covid-19 infection in a real-world setting.
The study was released Monday in Morbidity and Mortality Weekly Report, an online journal published by the Centers for Disease Control and Prevention.
The study followed nearly 4,000 health care workers, first responders, and other essential workers in eight U.S. locations as the first Covid vaccines were rolled out starting in December. Participants were tested weekly to look for all cases of Covid infection, even asymptomatic ones.
In the period from Dec. 14, 2020, to March 13, 2021, nearly 75% of the workers in the cohort received at least one dose of one of the mRNA vaccines. Both are given in a two-dose schedule.
Related: What to make of the AstraZeneca vaccine data — and the surrounding controversy
There were 161 Covid infections in the unvaccinated workers, compared with 16 in workers who had received only one dose by the time of their infection and only three infections in people who had received both doses and were two weeks out from their second dose. The vaccine effectiveness following two doses was 90% — roughly in line with the 95% and 94% that the Pfizer and Moderna vaccines showed, respectively, in the clinical trials that supported their emergency use authorizations.
The study was not conducted in such a way as to allow the researchers to estimate effectiveness measures for each of the vaccines.
The study suggested that even the first dose of vaccine was 80% effective at preventing infection, starting from two weeks after receipt of that dose. That estimate, however, only applies to the brief period until the second dose was administered. The study was not designed to test how well the vaccine works if an individual does not receive the second dose.
The majority of infections — 58% — detected in the study were found because participants were tested weekly to look for infections; 42% of the infections were identified when study participants were tested after developing symptoms. Most of the people who tested positive in the study had some Covid-related symptoms, though 10.7% had none. Only 23% of the people who became infected needed medical care and only two were hospitalized. There were no Covid deaths in the study.
by ponchi101 I know it sounds very expensive but if the USA starts vaccination in that scale, I may consider going over to get the vaccine. If I have work by then, for sure.
by Deuce More problems for the troubled AstraZeneca vaccine...
MJ2004 wrote: ↑Mon Mar 29, 2021 8:40 pm
Honestly it’s been a year and people are just burned out. Combine that with expectations of the vaccine, the knowledge that grandparents are now protected, and spring weather, and people going to be taking risks they shouldn’t.
Yup. I got my first, but surely not my last, party invite for the summer yesterday, this one is for a wedding. This is not a couple that needs in any way to get married any time this year even. And not the first wedding for either. Planned to marry in 2020, they are apparently done waiting. Doesn't seem to matter that the pandemic isn't over, 100+ person wedding is on order for July. I think "safe enough" is going to be good enough for a large majority going forward and that's a risky approach when we are nowhere near herd immunity.
I have a cousin that should be in a bigger rush to get married. And so he is. Next week at City Hall. Outdoor dinner celebration with immediate family. Big wedding reception on hold til 2022. The much more reasoned and mature approach imho.
MJ2004 wrote: ↑Mon Mar 29, 2021 8:40 pm
Honestly it’s been a year and people are just burned out. Combine that with expectations of the vaccine, the knowledge that grandparents are now protected, and spring weather, and people going to be taking risks they shouldn’t.
Yup. I got my first, but surely not my last, party invite for the summer yesterday, this one is for a wedding. This is not a couple that needs in any way to get married any time this year even. And not the first wedding for either. Planned to marry in 2020, they are apparently done waiting. Doesn't seem to matter that the pandemic isn't over, 100+ person wedding is on order for July. I think "safe enough" is going to be good enough for a large majority going forward and that's a risky approach when we are nowhere near herd immunity.
I have a cousin that should be in a bigger rush to get married. And so he is. Next week at City Hall. Outdoor dinner celebration with immediate family. Big wedding reception on hold til 2022. The much more reasoned and mature approach imho.
My daughter got married in November of 2020. There were a total of 8 people at her mother-in-law's house, immediate family of her and her husband. A tent was erected in the back yard and food was catered. The officiant was there virtually. We had a wonderful time.
I applaud what your cousin is doing. Small weddings are not sad.
by Deuce
ti-amie wrote: ↑Mon Mar 29, 2021 10:39 pm
My daughter got married in November of 2020. There were a total of 8 people at her mother-in-law's house, immediate family of her and her husband. A tent was erected in the back yard and food was catered. The officiant was there virtually. We had a wonderful time.
I thought nothing was to be erected before the honeymoon...
ti-amie wrote: ↑Mon Mar 29, 2021 10:39 pm
My daughter got married in November of 2020. There were a total of 8 people at her mother-in-law's house, immediate family of her and her husband. A tent was erected in the back yard and food was catered. The officiant was there virtually. We had a wonderful time.
I thought nothing was to be erected before the honeymoon...
Ok... that's my childish comment for the week...
.
by ponchi101
Deuce wrote: ↑Mon Mar 29, 2021 10:46 pm
...
I thought nothing was to be erected before the honeymoon...
Ok... that's my childish comment for the week...
.
Timer is on. You have 6 days...
by dryrunguy I talk to a friend of mine in Barinas, Venezuela every Sunday night. Last week, he had told me that his sister was very ill, so when I talked to him last night, I asked for an update. It turns out her appendix actually burst, and they barely got her to the hospital in time. But she's okay.
While he was in the hospital (he should NOT have been allowed to be in the hospital), he snapped a few photographs of people on gurneys in the hallways. I won't share them because he should not have taken the pictures (patient privacy). But he said every hallway he saw in the hospital was full of sick people on gurneys. Every hallway. And he said they were all or almost all COVID cases. (I don't know how he would know that.)
But if that's true, or even partially to true, the images were beyond alarming and heartbreaking. And he said public perception is to blame Brazil. I'm not quite following that. No one from Brazil is going to Venezuela, right?
by ponchi101 Oh my god. Venezuelans blaming a different country for their own problems. How (expletive) unusual.
The outbreak in the country is very severe. And no, it is not coming from Brasil. The gov't has been completely inept at vaccination, both in getting any or distributing it. By now the sole possible vaccines are the Russian or Chinese.
And nobody here in this forum needs geography lessons but Venezuela and Brasil share a border, made of the most impenetrable forest in the world.
by dryrunguy
ponchi101 wrote: ↑Tue Mar 30, 2021 2:32 am
Oh my god. Venezuelans blaming a different country for their own problems. How (expletive) unusual.
The outbreak in the country is very severe. And no, it is not coming from Brasil. The gov't has been completely inept at vaccination, both in getting any or distributing it. By now the sole possible vaccines are the Russian or Chinese.
And nobody here in this forum needs geography lessons but Venezuela and Brasil share a border, made of the most impenetrable forest in the world.
It was a baffling and depressing conversation, ponchi. On multiple fronts. I was glad I was able to cut it a little shorter than usual because my meetings started at 8 a.m. this morning.
by ti-amie
by ti-amieBrazil is rocked by political turmoil as pandemic outlook darkens
By Heloísa Traiano and
Terrence McCoy
March 30, 2021 at 5:26 p.m. EDT
RIO DE JANEIRO — Six cabinet members are out. The military’s top leaders are also gone. And it’s only Tuesday.
First came the Monday morning exit of Brazil’s foreign minister, a right-wing ideologue blamed for failing to secure enough coronavirus vaccines. Then the defense minister was gone. Then the justice minister was replaced. Tuesday morning brought still more tumult: the departures of the navy, army and air force chiefs.
The exits have sent political shock waves across Latin America’s largest country, precipitating the most politically uncertain moment of President Jair Bolsonaro’s two-year-plus tenure. Brazil must now face what public health analysts say could be the darkest weeks of the pandemic with a raft of new officials and an incoherent national strategy.
The sudden moves — some expected, others not — suggested mounting political desperation in the presidential palace. Health systems have collapsed. Some 2,600 people are dying of the coronavirus every day. And Brazilians are increasingly looking to blame the failures of the pandemic on Bolsonaro, who has never appeared more vulnerable. Earlier this month, the leader of the congress implied the president may face impeachment.
“These are defensive actions,” said Ricardo Ismael, a political scientist at the Catholic Pontifical University in Rio de Janeiro. “There is a fragility to him.”
That impression has only deepened since the return to the scene of Bolsonaro’s greatest political rival, former president Luiz Inácio Lula da Silva, out of prison and now cleared by the supreme court to run in the 2022 presidential election. If Bolsonaro is to have any shot at maintaining power, quieting calls for impeachment and eventually winning reelection, he has to start making changes, analysts said.
“He’s feeling the heat,” said Matias Spektor, an associate professor of international relations at Fundação Getúlio Vargas in São Paulo. “He knows things will get worse in the next months, and he needs to prepare for that and get ready for the next election.”
Bolsonaro has somewhat moderated his messaging on the virus, which he earlier dismissed as little more than an annoyance Brazilians had to work around. Long a mask skeptic, he began wearing one. He also embraced vaccines, which he previously fretted could turn people into alligators. He dismissed his health minister, a military general, and replaced him with a cardiologist. And finally, he booted the foreign minister, the right-wing hard-liner castigated by the powerful center bloc of congress for not wrangling enough vaccines from foreign powers.
Those moves were expected. Then came ones that weren’t.
Bolsonaro replaced the justice minister with a close family ally. Then he sacked the defense minister, Fernando Azevedo e Silva, who had taken the virus more seriously and had reportedly chafed under the president’s leadership. Bolsonaro, a former army captain, has repeatedly said the military was on his side in political disputes. Earlier this month, he called it “my military.”
Azevedo e Silva disagreed — and was gone by the end of Monday.
“During this time, I preserved the Armed Forces as institutions of state,” Azevedo e Silva wrote in his departure statement. “I leave in the certainty of a mission accomplished.”
On Tuesday morning, the three top commanders of the armed forces — who had joined Azevedo e Silva in a November statement reinforcing the separation of military and politics — also announced they were leaving. It’s unclear whether they resigned or were forced out.
In a country that spent decades under a military dictatorship — and is now led by a president who has frequently lamented its collapse — the departure of the top military officials has caused widespread consternation and fanned fears about Bolsonaro’s authoritarian impulses.
“He has the idea that, as soon as he was elected, he is the state,” said Carlos Melo, a professor at São Paulo University’s Insper education and research school. “That the institutions are subordinate to him and not to the state.”
Politicians and former allies across the country echoed the concerns about the strength of Brazilian democracy.
“Bolsonaro is increasingly similar to Chávez and Maduro,” said Rodrigo Maia, a former congressional president, referring to past and current Venezuelan presidents. “An authoritarian will always be an authoritarian.”
by ponchi101 Well, similar to Maduro or Chavez... other than he is from the EXTREME RIGHT and our primates claim to be from the LEFT...
Another country that has no excuse to be where it is. Or be what it is.
by mmmm8 I take that prediction that you'd be able to get vaccinated in Colombia for $ before you could get vaccinted in the US back, ponchi... It's really ramping up here (across states).
Today, New York opened it up to those 30+ (all except children eligible from April 6)... getting the first dose Thursday!
by ponchi101 The sole problem would be traveling. Air tickets have really gone up. Two round trip tickets for the GF and I will be around $1500, when it was around $700 BOG-MIA before the pandemic.
But if I get a job we are on that flight the next day. The buffoons here are unable to get this going. A trickle of vaccines are coming into the country and the pace is very slow.
I was afraid this was coming. I think they've done well to avoid school closures in large part compared to most other Western countries. Hopefully the mass vaccination centers they are opening now will also start to make a difference.
And I'm not sure this will have any bearing on it or not. But I thought most flew into Nice when traveling to Monte Carlo. And, the Monte Carlo Masters starts in just over a week...
And I'm not sure this will have any bearing on it or not. But I thought most flew into Nice when traveling to Monte Carlo. And, the Monte Carlo Masters starts in just over a week...
Rafa can get on his yacht and sail there. Everybody else, you are right.
by Suliso Exceptions will be made... By the way Thiem is out.
by Suliso All the countries around us are in one kind of lockdown or another. Not in Switzerland - all shops and schools are open for now.
We're going to southern Switzerland over Easter for few days. Not planning to meet anyone, just hiking in the hills.
by Deuce It just keeps getting better and better...
Sigh indeed.
It seems to me that this should be something in which private industry could do better than government. Make it socialist/capitalist: you want the vaccine and can pay for it? Fine. You pay for yours, and for three more people (not family) in line.
Of course, nothing that would assist in this contamination issue, but it can't be that not even the EU can get this thing going smoothly.
@Suliso: good for your folks. I bet that will make you feel better too. I am really worried about my mom being in Vennieland, where nothing works.
by Suliso
ponchi101 wrote: ↑Thu Apr 01, 2021 3:24 pm
@Suliso: good for your folks. I bet that will make you feel better too. I am really worried about my mom being in Vennieland, where nothing works.
Definitely. Particularly since I can't convince mom that inviting people regularly to garden parties not the safest thing to do right now. At least neither of them are antivaxxers. Hope you can arrange something for your mom eventually.
by ti-amie
by ponchi101 My GF's sister in law, currently in Miami as a visitor, got her vaccine. One friend of her (my GF) who just turned 55 got his shot. More stories like that are all around.
The US is doing better than almost everybody else. Perhaps Israel and others are ahead but, all in all, Biden is delivering.
by Suliso A friend of mine in Virginia got hers. She's only 35 and have no risk factors.
by Togtdyalttai I got my second dose of Moderna yesterday, and I'm home from work with a fever today. That said, even a few more days like this would still be worth it to get the immunity from the vaccine.
by ponchi101 Get better soon. Hope it is only temporary and you will be up and ready by tomorrow.
by ti-amie
Togtdyalttai wrote: ↑Thu Apr 01, 2021 11:09 pm
I got my second dose of Moderna yesterday, and I'm home from work with a fever today. That said, even a few more days like this would still be worth it to get the immunity from the vaccine.
Feel better!
by mmmm8 So, obviously it's better than no vaccine, but I'm a little worried about the large percent of vaccines being J&J, with its lower efficacy. People are going to stop using precautions after vaccination, so, while J&J may be reliable to stop serious illness it's not necessarily going to stop the proliferation of the virus and, as we know, this thing mutates very effectively.
Not sure there's much to be done but if I weren't in dire need, for example, I would choose to hold out longer until more Pfizer/Moderna were available. I would probably prefer AZ to J&J too.
---
Got my first shot of Moderna yesterday, though so not an issue for me personally (shot itself was painless, sore arm and I got super sleepy for a couple hours about 6 hours after the inoculation).
by mmmm8
Togtdyalttai wrote: ↑Thu Apr 01, 2021 11:09 pm
I got my second dose of Moderna yesterday, and I'm home from work with a fever today. That said, even a few more days like this would still be worth it to get the immunity from the vaccine.
Feel better - congrats!
by Suliso Is that really so that AZ is better than JJ? I was under impression of opposite being the case...
by mmmm8
Suliso wrote: ↑Fri Apr 02, 2021 2:12 pm
Is that really so that AZ is better than JJ? I was under impression of opposite being the case...
AZ seems to have higher risks but efficacy is 76% (100% vs severe disease) while J&J is 66% (85% against severe disease). I think there are different results in different regions and age groups but these are the main overall stats
by Suliso Maybe one can combine. Start with JJ and then give Pfizer or Moderna as a booster 4 weeks later.
by ponchi101 This might end up being like a influenza vaccination regime. Once a year, you need your shot. There still is no evidence of for how long will this protect you. So maybe yes, start with J&J, then a boost, then regular vaccinations for a few years until we can drive the virus away. If that is possible at all.
by mmmm8
Suliso wrote: ↑Fri Apr 02, 2021 2:57 pm
Maybe one can combine. Start with JJ and then give Pfizer or Moderna as a booster 4 weeks later.
mmmm8 wrote: ↑Fri Apr 02, 2021 2:48 pm
AZ seems to have higher risks but efficacy is 76% (100% vs severe disease) while J&J is 66% (85% against severe disease). I think there are different results in different regions and age groups but these are the main overall stats
You should post what you are reading. I haven't read anything that actually references the trial data where J&J isn't 100% against hospitalizations and death. Severe disease is this context doesn't include being hospitalized with the virus. And unlike the other approved vaccines, it ran trials where the most concerning variants are and while those variants were dominant and that was still the case. And they had hospitalizations and death in the placebo group.
Also, the AZ vaccine had concerning results against the South African variant to the point that the trial was suspended there and use of the vaccine were halted as they study that variant more.
If you're seeing something else legitimate, you should post it.
National mission: Chile hits 1 million COVID cases, slams doors
SANTIAGO (Reuters) -Chile closed its borders and tightened an already strict lockdown further on Thursday to slow the spread of the coronavirus and stop the influx of contagious new variants as cases climbed past 1 million despite one of the world’s fastest vaccination rates.
The dramatic move came as hospitals warned they were close to saturation with middle-aged and younger victims of the disease as cases have spiked in recent weeks following the Southern Hemisphere summer holidays.
Chile struck early deals with vaccine makers Pfizer and Sinovac, and has already vaccinated more than 35% of its population, ranking it third in the world for inoculations per capita, according to a Reuters tally.
But a second wave hit before the country could reach a goal of herd immunity by July.
On Thursday, the country reported 7,830 cases of the virus, its highest single-day tally, adding up to a total of 1,003,406 infections, since the pandemic began in March 2020.
The caseload has prompted Chile to delay elections due on April 11 and resulted in accusations by health experts that the government allowed the triumph of its vaccination program to muddy its message, resulting in citizens dropping their guard - a claim angrily rejected by Health Minister Enrique Paris.
Movement restrictions have been swiftly ramped up, with more than 80% of the country of 19 million people now in lockdown to ease pressure on near-saturated urgent care wards.
On Thursday, Officials said they would close the South American country’s border for a month beginning on Monday to both Chileans and foreign residents, with exceptions only in emergencies. No foreign tourists will be allowed to enter - the first time it has taken the extreme measure since the early days of the pandemic in March 2020.
Authorities also ratcheted up restrictions on movement inside Chile, banning purchase or delivery of non-essential goods like toys, clothes or electronics, including from supermarkets, limiting circulation permits to a small group of essential workers - primarily supermarket and medical staff - and restricting authorizations for people to leave their homes.
Previous measures which granted a large number of companies “essential work” status and their staff permission to move around, and permits allowing citizens to take a trip during the summer holidays, have been blamed by medical experts for contributing to the spike in cases.
Locals also trade anecdotes and the media carries stories about people misusing permits to variously attend parties, go to beach houses and on fishing trips.
Government spokesman Jaime Bellolio implored all Chileans to take the rules seriously.
“It is now when we can save lives, when we need to take extreme care,” he said. “This is a national mission, each of us has a duty within our family group and those close to us to stress the urgency of being responsible now, today. Tomorrow may be too late.”
The vaccination program has resulted in a tailing off of hospital admissions among people in their 60s and 70s, but they have been replaced by a growing number of people in their 40s and 50s, health ministry figures show.
To date, just over 100 of the more contagious variants of the virus such as P1, which originated in Brazil, have been detected in Chile, but intensive care unit doctors say they could be behind the changing face of their patients.
Carlos Romero, head of the intensive care unit at the University of Chile’s clinical hospital in Santiago, told Reuters he was seeing patients in their 30s without pre-existing conditions die of COVID-19.
He said restricting movement was critical until more was known about the variants and the power of vaccines to quell them.
“If young people are more active, they are also more exposed,” he said.
Reporting by Dave Sherwood and Aislinn Laing; Editing by Franklin Paul and Jonathan Oatis
by Togtdyalttai Thank you all for your concern. I'm back to normal today, which seems to be pretty much in line with other people who have had reactions like I did.
by Deuce
Suliso wrote: ↑Fri Apr 02, 2021 2:57 pm
Maybe one can combine. Start with JJ and then give Pfizer or Moderna as a booster 4 weeks later.
ponchi101 wrote: ↑Fri Apr 02, 2021 3:50 pm
This might end up being like a influenza vaccination regime. Once a year, you need your shot. There still is no evidence of for how long will this protect you. So maybe yes, start with J&J, then a boost, then regular vaccinations for a few years until we can drive the virus away. If that is possible at all.
I would strongly advise against getting doses of 2 different vaccines at this time. Not until it has been proven to be both safe and effective to do so.
by JazzNU
Togtdyalttai wrote: ↑Fri Apr 02, 2021 6:57 pm
Thank you all for your concern. I'm back to normal today, which seems to be pretty much in line with other people who have had reactions like I did.
That's awesome @Tog. So glad you're feeling better. I hope your mom is doing good as well.
by atlpam Getting my second Pfizer dose on Tuesday. Prepared to feel lousy on Wed.
by ponchi101 But you will be fine AND PROTECTED on Thursday Keep us posted.
by ti-amie
Demonstrators take part in a protest against Brazilian President Jair Bolsonaro and his handling of the coronavirus outbreak in Brasilia on Tuesday. (Ueslei Marcelino/Reuters)
Opinion: Which world leader has the worst pandemic record? The competition is fierce.
Opinion by
Frida Ghitis
Contributing columnist
March 30, 2021 at 2:57 p.m. EDT
A catastrophic pandemic and a calamitous presidency combined to give the United States the world’s worst pandemic death toll. That was essentially confirmed by Deborah Birx, President Donald Trump’s coronavirus task force coordinator, who told CNN that most deaths in the United States could have been prevented.
And yet — cold comfort — Trump might not have been the worst leader of the pandemic. Others arguably botched the crisis even worse than Trump did, and the list tells you a lot about the state of global governance.
It’s hard to top the response of Nicaragua’s near-eternal President Daniel Ortega and his wife, who responded to news of a pandemic by calling people into the streets for a festive parade they called “Love in the Time of Covid-19” — a perversely fitting allusion to the work of Gabriel García Márquez, whose novels seamlessly blend fact and hallucination. The reckless move horrified human rights activists and scientists alike.
Hard to top it is, but not impossible. There’s Jair Bolsonaro, president of Brazil, where the health-care system stands on the verge of collapse, and the unchecked spread of the virus has spawned variants now threatening other struggling countries.
Bolsonaro has echoed Trump’s claims about hydroxychloroquine, squandering emergency pandemic funds on the useless treatment. He has fired health ministers for refusing to go along with his covid-19 denial and claimed that Brazilians might be immune to the “little flu” because they swim in sewage and nothing happens to them. Bolsonaro, who himself became infected, called on Brazilians to protest antivirus measures and joined them in the streets. Few people wore masks, and he gleefully shook hands — sometimes after coughing into his own.
As the pandemic explodes across Brazil, with thousands dying every day, he recently told Brazilians to “stop whining” about it.
Another president who caught the virus while playing it down is Mexico’s Andrés Manuel López Obrador. Early on, he advised Mexicans to “live life as usual.” Even after he became infected, he rejected requests to wear a mask. He says he will wear one when corruption is eradicated in Mexico, a distant prospect. As in the United States, mask-wearing became highly politicized, a development that contributed to the climbing death toll.
This weekend, Mexican authorities quietly released a report showing the real count is 60 percent higher than the official figure, putting Mexico neck and neck with Brazil for the world’s second-highest pandemic death toll, behind the United States.
Coincidence? Populism seems to be a comorbidity in a pandemic, raising its deadly toll.
Then there are the dictators, like Belarus’s Alexander Lukashenko, who described the pandemic as nothing more than a “psychosis” and prescribed vodka and saunas to prevent it. Lukashenko, who has faced months of mass protests after a disputed election last summer, has blocked common-sense measures to slow down the virus at almost every turn.
Yet many Belarusians have resisted his negligent approach — just as many have pushed back against his dictatorship. Ignoring his calamitous advice, individuals practiced social distancing, held crowdfunding campaigns to buy supplies for hospitals and, in the end, have probably helped to keep the virus and the death toll in Belarus from spiraling out of control.
In Turkmenistan, another post-Soviet dictatorship, the government has set a new low for denial by banning mask-wearing and any discussion of the pandemic. The use of the word “coronavirus” has reportedly been outlawed in media or health information materials. Turkmenistan still claims it hasn’t had any coronavirus cases, a claim no one believes.
In Cambodia, where Prime Minister Hun Sen has held power since 1985 (making him one of the world’s longest-ruling heads of government), the first move was denial. He welcomed cruise ship passengers shunned by other countries for fear of the pandemic. Gradually, his response turned to repression, banning criticism and arresting those who complained, then using the emergency to tighten the regime’s grip.
In Africa, yet another authoritarian populist, President John Magufuli of Tanzania, also dismissed talk of a global emergency. He told people not to bother with masks or vaccines, claiming that three days of prayer eradicated the virus in Tanzania. To make his point, he claimed to have submitted samples of pawpaw fruit and said they came back positive, ridiculing scientists.
Magufuli died this month. Authorities say he died from heart complications, but members of the opposition say they have it on good authority that he died of covid-19.
It’s impossible to cover all the outrages by populist demagogues and assorted tyrants. (Apologies if I left out one you found particularly offensive.) Every world leader made mistakes, but there’s something uniquely malignant about the manipulations and deceptions of the most outrageous players.
It is sometimes hard to suppress a chuckle when watching the antics of these buffoons. Yet the sense of absurdity is quickly stifled by the realization that their actions have likely contributed to the deaths of hundreds of thousands around the world — perhaps more.
As for Trump, these other leaders remind us that he wasn’t alone in his mishandling of the pandemic. He has a lot of competition for the title of worst pandemic president. But he’s still a contender.
by ti-amie I still think the former guy is the worst because if the United States had come from the beginning used every power it has to try and protect its citizens none of these clowns would've been able to pretend this "hoax" was a "psychosis" and tell the citizens of their countries to ignore the virus.
by ponchi101 Whether other people like it or not, the USA stills sets the pace in many aspect. When the person in charge of the USA says something, a lot of people listen.
So maybe not the worst, but the clearest example.
by Deuce
ponchi101 wrote: ↑Sat Apr 03, 2021 3:06 pm
But you will be fine AND PROTECTED on Thursday Keep us posted.
We have to remember that it takes 2 or 3 weeks for the vaccine to produce the protection..
by ponchi101 I did not go to Colorado this year because of COVID. I felt it was not a responsible thing to do.
But, idiot that I am, I just went on-line to check vaccine availability for my GF and me in my little town up there. We are both eligible and we could get an appointment for, for example, tomorrow.
Man, I just want to catch a break lately. Just one.
ponchi101 wrote: ↑Sat Apr 03, 2021 3:06 pm
But you will be fine AND PROTECTED on Thursday Keep us posted.
We have to remember that it takes 2 or 3 weeks for the vaccine to produce the protection..
Yes, another 2 weeks for full protection, but I already have about 70% protection from the first dose.
by atlpam So the hubby had to get a ferry back to the mainland to return to the US after closing out his father’s estate on Vancouver Island. The ferry had to turn back to remove an unruly passenger who refused to wear a mask or stay in his car. Apparently he was going to an anti-mask rally.
by ponchi101 I hope that person gets charged for time and money wasted due to his behavior.
These people should be given like their own country. See how long it takes for them to descend into savagery.
by atlpam
ponchi101 wrote: ↑Sun Apr 04, 2021 4:02 pm
I hope that person gets charged for time and money wasted due to his behavior.
These people should be given like their own country. See how long it takes for them to descend into savagery.
There were plain closed police on board and the man was taken off in handcuffs. Hubby talked to the neighbor to his Dad’s house who saw it on the news; she didn’t know that was the ferry my hubby was on.
by JazzNU
atlpam wrote: ↑Sun Apr 04, 2021 3:56 pm
So the hubby had to get a ferry back to the mainland to return to the US after closing out his father’s estate on Vancouver Island. The ferry had to turn back to remove an unruly passenger who refused to wear a mask or stay in his car. Apparently he was going to an anti-mask rally.
This is wild. Thanks for sharing. You see these things on the news sometimes, but I don't know anyone who has witness these crazies in person.
And sorry to hear about your family's loss. I hope your husband is doing okay.
mmmm8 wrote: ↑Fri Apr 02, 2021 2:48 pm
AZ seems to have higher risks but efficacy is 76% (100% vs severe disease) while J&J is 66% (85% against severe disease). I think there are different results in different regions and age groups but these are the main overall stats
You should post what you are reading. I haven't read anything that actually references the trial data where J&J isn't 100% against hospitalizations and death. Severe disease is this context doesn't include being hospitalized with the virus. And unlike the other approved vaccines, it ran trials where the most concerning variants are and while those variants were dominant and that was still the case. And they had hospitalizations and death in the placebo group.
Also, the AZ vaccine had concerning results against the South African variant to the point that the trial was suspended there and use of the vaccine were halted as they study that variant more.
If you're seeing something else legitimate, you should post it.
[DELETED URLS FROM YOUR POST BECAUSE OF THE LINK LIMIT)
Sorry for the late response but work and life get in the way - which is why I didn't post sources in the first place. Maybe I should have, but this isn't a news site, we are not always going to have the footnotes ready.
The materials I saw had "severe illness" for not only J&J but Pfizer and Moderna.
Conscious that there is no apples-to-apples comparison because of the timing of the testing, but there have been reports that "real world" current research supports the fact that Pfizer and Moderna are 90% effective, although doesn't provide data for each of the two. https://www.healthline.com/health-news/ ... ld-setting
atlpam wrote: ↑Sun Apr 04, 2021 3:56 pm
So the hubby had to get a ferry back to the mainland to return to the US after closing out his father’s estate on Vancouver Island. The ferry had to turn back to remove an unruly passenger who refused to wear a mask or stay in his car. Apparently he was going to an anti-mask rally.
This is wild. Thanks for sharing. You see these things on the news sometimes, but I don't know anyone who has witness these crazies in person.
And sorry to hear about your family's loss. I hope your husband is doing okay.
Thanks Jazz - My father-in-law passed 3 years ago. Family was taking the time to sort through what was in the house prior to selling, but with Covid, no one had been able to travel there since all the family is in the US. They got a contract on the house, so as executor my husband had to go finish clearing out the house. Bittersweet as the home had a fabulous view, but it wasn't financially feasible for the family to hold on to it.
Scheduling the trip was a nightmare - he changed his reservations at least 5 or 6 times. Finally ended up flying to Seattle & renting a car to drive across the border & take a ferry to the island so he could go directly to the house to quarantine instead of a hotel. He was fully immunized prior to travel. He had to take 3 Covid PCR tests - 1 prior to travel, 1 when he crossed the border into Canada, and 1 after 10 days of quarantine. He had to stay in his car on the ferry. I think International travel is still a ways off for us.
by JazzNU My 99-year old great aunt finally got her covid vaccine today! In NYC, she's been eligible since very early on, but the city didn't send mobile units to senior apartments like hers early on, only to the senior centers and they aren't considered a nursing home. So she could get one, but she had to leave her building. We all decided that wasn't a necessary risk to take given her fragile health. So had to wait for them to send out mobile units like this where she could get it administered in her apartment or at least in her building and that finally happened today.
She got the J&J. She is deathly afraid of needles. The look on her face (her aide sent us photos) getting the shot is heartbreaking, she looks petrified, so I'm very happy she won't have to get a second shot.
by ti-amie I guess no one ever told him huh? Either that or he's never traveled outside of the country.
by ponchi101 The same way everybody in the world feels when we are required to have a Yellow Fever vaccine before we can enter ANY country in Africa or many in South America. Perfectly normal.
by mmmm8
ponchi101 wrote: ↑Mon Apr 05, 2021 8:47 pm
The same way everybody in the world feels when we are required to have a Yellow Fever vaccine before we can enter ANY country in Africa or many in South America. Perfectly normal.
It's almost like vaccines are for your own protection...
by JazzNU
ti-amie wrote: ↑Mon Apr 05, 2021 8:41 pm
I guess no one ever told him huh? Either that or he's never traveled outside of the country.
He could've never left the state of California, this is egregious. Who the heck ever heard of a Internal Medicine doctor that doesn't know and hasn't signed off on immunization records for their patients to travel or attend school or go to camp or wherever else? Outside of pediatricians, that's the #1 doctor that signs those forms. If he's still board certified, a hearing needs to be called to put that certification into question. And if he sits on any medical school's boards, they need to ditch him quickly if they didn't in 2020 when they should have. His mind is cracked.
by ti-amie I actually never heard of him until today but it seems like as usual I'm out of the loop.
by ti-amie
by JazzNU
ti-amie wrote: ↑Tue Apr 06, 2021 12:41 am
I actually never heard of him until today but it seems like as usual I'm out of the loop.
The height of his fame was in the late 90s as the co-host of the MTV show Loveline with Adam Carolla, really a call-in radio show turned into a TV show giving out relationship advice. I never understood their or the show's popularity, though Drew was easier to take than Adam's abrasive personality by a mile. The last few years are not what people expected out of Dr. Drew at all. Adam, on the other hand, is partly why I've never fully warmed up to Jimmy Kimmel like others have.
by atlpam Received my second dose this morning. Very few cars at the state mass vaccination site - no wait. Sign as you entered said no appointment necessary. Just shows how low the demand is once you leave the Atlanta metro area and enter rural GA. Anyone 16 and over is eligible.
by ponchi101 Georgia is looking like the place to go for a vaccine. I will keep it mind.
Hope this time you will have no side-effects or feel not 100%, atlpam
by dryrunguy The Situation Report is back. Lots to report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 131.3 million cases and 2.9 million deaths as of 6:00am EDT on April 6. Global weekly incidence and mortality continue to increase. The weekly total of 4.0 million new cases is the highest incidence since mid-January 2021, and 71,387 deaths is the highest weekly mortality since early February 2021.
India surpassed both Brazil and the US to become #1 globally in terms of total daily incidence. India is reporting 84,313 new cases per day, more than 7.5 times its most recent low on February 11 (11,145). For comparison, India’s current surge started 53 days ago, while a similar increase took 83 days during its previous surge. India’s daily incidence is only 9.5% below its record peak in September 2020 (93,199) and shows little sign of slowing. On this trajectory, India will surpass its previous peak in the next several days. The US surpassed Brazil as #2, but the two countries are reporting essentially equal daily incidence—64,662 in the US and 62,855 in Brazil. Brazil’s daily incidence has decreased sharply since its peak on March 27, down from 77,129 new cases per day—an 18.5% decrease. Combined, India, Brazil, and the US represent more than 35% of the global daily incidence.
In terms of total daily mortality, Brazil reported a new national record high of 3,117 deaths per day on April 1, nearly triple its average on February 22 (1,053) and 9% fewer deaths than the United States’ peak in January (3,428). Brazil’s daily mortality fell sharply to 2,698 over the past several days, but the rapid turnaround makes it difficult to determine the longer-term trajectory. India’s daily mortality also is accelerating, up from fewer than 100 deaths per day on March 8 to 490.
Global Vaccination
The WHO reported 604.0 million vaccine doses administered globally as of April 6, including 315.0 million individuals with at least 1 dose. The dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports 677.8 million doses administered globally. The global cumulative total continues to increase at a rate of approximately 20% per week. The daily average appears to have leveled off at approximately 16 million doses per day. At least 161 countries and territories are reporting vaccination data.
UNITED STATES
The US CDC reported 30.5 million cumulative cases and 554,064 deaths.
The US surpassed 30 million cumulative cases on March 27:
1 case to 5 million cases- 200 days
5 million to 10 million- 92 days
10 million to 15 million- 29 days
15 million to 20 million- 24 days
20 million to 25 million- 24 days
25 million to 30 million- 62 days
The US surpassed 550,000 cumulative deaths on April 1:
1 death to 50k- 55 days
50k to 100k- 33 days
100k to 150k- 63 days
150k to 200k- 55 days
200k to 250k- 58 days
250k to 300k- 25 days
300k to 350k- 20 days
350k to 400k- 16 days
400k to 450k- 16 days
450k to 500k- 19 days
500k to 550k- 37 days
National-level data continue to indicate the start of a fourth COVID-19 surge, and more states are beginning to show the early signs as well. According to analysis published by Data USA, 29 states (and Puerto Rico) are reporting increasing daily COVID-19 incidence over the past 2 weeks (>+5%). Among these states, 16 are reporting increases of more than 20% over that period, including 5 with more than 30%: Michigan (+61.5%), Nebraska (+59.3%), Alaska (+45.0%), Maine (+31.4%), and Washington (+31.1%). Puerto Rico is reporting an increase of 61.1% over the past 2 weeks. There are concentrations of these states across the country, including all of New England, most of the Midwest and West Coast regions, and several states in the Southeast and Mid-Atlantic regions as well as Alaska and Hawai’i.
Michigan continues to exhibit among the most concerning trends, currently reporting daily incidence nearly 6.5 times its most recent low in late February. On a per capita basis, Michigan is reporting 67.3 daily cases per 100k population, the highest in the country and 40% higher than #2, New Jersey (47.9). Michigan is quickly approaching its record high daily incidence (8,344 new cases per day), set in early December 2020. Michigan’s current surge started in late February/early March, and its daily mortality appears to be starting to increase as well, up from 11 deaths per day on March 29 to 15 on April 4. It is too early to determine if this is the start of a longer-term trend, but the timing is consistent with a lag of 4 weeks behind the daily incidence trend. According to CDC data, Michigan is the only state reporting test positivity greater than 10%, and the Johns Hopkins Coronavirus Resource Center is reporting Michigan’s test positivity at 16.4% over the past week and increasing.
US Vaccination
The US surpassed 200 million SARS-CoV-2 vaccine doses distributed, and the US has administered 167.2 million doses. The US is currently administering 2.77 million doses per day*, including 1.24 million people fully vaccinated.
More than 100 million individuals have received at least 1 dose of the vaccine, equivalent to nearly one-third of the entire US population and more than 40% of all adults. Of those, 62.4 million (18.8% of the total population; 23.2% of adults) are fully vaccinated. More than 75% of adults aged 65 years and older have received at least 1 dose, and more than half are fully vaccinated.
In terms of full vaccination, 31.1 million individuals have received the Pfizer-BioNTech vaccine, 27.1 million have received the Moderna vaccine, and 4.2 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 30.8 million cumulative cases and 555,638 deaths as of 10:15am EDT on April 6.
SARS-COV-2 ORIGIN On March 30, the WHO published a report on its investigation into the origin of SARS-CoV-2. While it is nearly impossible to definitively identify the exact source of the COVID-19 pandemic, the report describes information collected during the WHO team’s visit to China in January and February 2021. The investigators considered a broad scope of evidence, including epidemiological data, genomic analysis of SARS-CoV-2 specimens, environmental sampling from animal markets and laboratories, and interviews with health officials and laboratory researchers.
The report outlines the evidence for 4 potential scenarios: (1) zoonotic transmission direct from an animal reservoir to humans, (2) zoonotic transmission via an intermediate host, (3) transmission to humans via cold/food chain products, and (4) laboratory accident. The investigators indicated that spillover from animals to humans via an intermediate host was the most likely scenario, and a laboratory accident was determined to be “extremely unlikely.” Based on a review of potential cases of COVID-19 from October and November 2019 (identified retrospectively), before the first cases were reported in Wuhan, the researchers determined that it is unlikely the virus was spreading in the community prior to December 2019.
Because the report does not provide clear-cut answers regarding the pandemic’s origin, experts around the world continue to espouse a range of theories and speculation, including that the virus escaped containment in a laboratory in Wuhan. WHO Director-General Dr. Tedros Adhanom Ghebreyesus commented that the investigation was not “extensive enough” and that further research is necessary to more fully characterize the circumstances surrounding the emergence of SARS-CoV-2. Notably, the report outlines future areas for study, focusing largely on zoonotic transmission rather than the laboratory-escape scenario; however, Dr. Tedros emphasized that “all hypotheses are open.”
The report has been described as a “compromise” between the international and Chinese members of the WHO-sponsored team, a fact seized upon by some in their critiques of the team’s findings. The terms of the agreement between China and the WHO outlined a collaborative effort, as opposed to an independent, external investigation. In particular, some experts are calling attention to a lack of transparency by Chinese officials and researchers, and the close professional relationship between some of the WHO team members and the Wuhan Institute of Virology.
J&J TO SUPPLY AFRICAN UNION On March 29, J&J-Janssen announced a new purchase agreement with the African Vaccine Acquisition Trust (AVAT) to provide up to 400 million doses of its single-shot SARS-CoV-2 vaccine to the African Union’s 55 member states. Up to 220 million doses will be available with delivery beginning in the third quarter of 2021, and potential for the AVAT to order an additional 180 million doses through 2022. Within member states, availability of the vaccine will be subject to authorization or approval by national regulatory agencies. This agreement is in addition to an agreement with Gavi, the Vaccine Alliance to support the COVAX vaccine facility. J&J-Janssen and Gavi expect to finalize an advance purchase agreement that would provide up to 500 million vaccine doses to COVAX in 2022. Many African nations are participating in COVAX.
VACCINE EFFECTIVENESS On April 2, a team of researchers led by the US CDC COVID-19 Response Team published interim estimates of a prospective cohort study describing the effectiveness of the two-dose Pfizer-BioNTech and Moderna SARS-CoV-2 mRNA vaccines among healthcare and other frontline workers. The report, published in the CDC’s Morbidity and Mortality Weekly Report (MMWR), describes data collected from December 14, 2020 to March 13, 2021, through the HEROES-RECOVER network of 8 US sites. Overall, 3,950 frontline workers (i.e., those who routinely are within 3 feet of other individuals as part of their occupation) with no prior laboratory documentation of SARS-CoV-2 infection were included in the analysis. Participants were actively monitored for COVID-19 symptoms and self-collected weekly nasal swabs which were tested for SARS-CoV-2 infection.
Among the 3,950 participants, 2,479 (62.8%) received both recommended vaccine doses and 477 (12.1%) received only one dose of vaccine during the 13-week study period. For the duration of observation, there were 78,902 person-days followed for fully vaccinated individuals (two weeks or more post-second dose), 41,856 person-days of observation for partially vaccinated individuals (two weeks or more after first dose through receipt of second dose) and 116,657 person-days of observation for unvaccinated individuals (no doses received). 161 infections were identified among the unvaccinated group (1.38 infections per 1,000 person-days), 8 infections were identified among the partially vaccinated group (≥14 days after first dose and before second dose; 0.19 infections per 1,000 person-days), and 3 infections were identified among the fully vaccinated group (≥14 days after second dose; 0.04 infections per 1,000 person-days). The researchers note that the 13 days following participants’ first or second dose when immune status was indeterminate (67,483 person-days) were not included in analysis, but 33 infections were identified during that period of observation.
The unadjusted vaccine effectiveness for the partially immunized group was 82% (95% CI: 62-91) and 91% for the fully immunized group (95% CI: 73-97). The adjusted vaccine effectiveness for the partially immunized group was 80% (95% CI: 59-90) and 90% for the fully immunized group (95% CI: 68-97). Notably, a majority of infections were symptomatic with common COVID-19-associated symptoms (87.3%), but only two hospitalizations occurred and no deaths occurred. In light of these findings, the CDC encourages vaccinated individuals to continue taking public health precautions to prevent infection and transmission.
ASTRAZENECA-OXFORD VACCINE AGE RESTRICTIONS As countries continue to evaluate the risk of blood clots associated with the AstraZeneca-Oxford SARS-CoV-2 vaccine, some are implementing age restrictions for that product. Canada’s National Advisory Committee on Immunization (NACI) issued updated guidance recommending the vaccine not be used in individuals under the age of 55 while it conducts further investigation into the risk of vaccine-induced prothrombotic immune thrombocytopenia (VIPT). NACI notes that VIPT cases reported thus far “have been primarily in women under the age of 55 years” who received the AstraZeneca-Oxford vaccine, but the exact frequency has not yet been confirmed. Canada is receiving sufficient supply of other vaccines, so the decision to restrict the use of the AstraZeneca-Oxford vaccine to older adults should not adversely impact vaccination progress.
Similarly, Germany suspended the use of the vaccine in individuals under the age of 60. Germany’s Standing Committee on Vaccination (STIKO) also indicated it will finalize its guidance for younger adults who already received the first dose of the AstraZeneca-Oxford vaccine by the end of April. Notably, Germany is administering the second dose of the vaccine at 12 weeks, so the first round of second doses are not scheduled to be administered until May since first doses began to be administered at the beginning of February.
SARS-COV-2 VACCINE PEDIATRIC TRIALS On March 31, Pfizer-BioNTech announced findings from a Phase 3 clinical trial of its SARS-CoV-2 vaccine among adolescents ages 12-15 with or without evidence of previous infection. No symptomatic COVID-19 cases were identified in the vaccinated group (n=1,131), and 18 symptomatic COVID-19 cases were identified in the placebo group (n=1,129), translating to 100% vaccine efficacy among vaccinated participants. Vaccinated participants demonstrated strong immunogenicity one month after their second dose, and the vaccine was well-tolerated. Both immunogenicity and side effects were consistent with results seen in previous trials among participants 16 to 25 years of age.
Pfizer-BioNTech plans to submit amendments to the US FDA and the European Medicines Agency for use of the vaccine among individuals 12 and older under the current US Emergency Use Authorization and EU Conditional Marketing Authorization, respectively. Currently, the Pfizer-BioNTech COVID-19 vaccine is authorized for individuals ages 16 years and older. Depending on regulatory authorization, adolescents could begin to receive vaccinations soon, possibly before the beginning of next academic year. The companies also plan to submit the data for peer-reviewed publication.
Pfizer-BioNTech also provided an update on the ongoing SARS-CoV-2 vaccine Phase 1/2/3 study among children ages 6 months to 11 years. Children in the trial are grouped by age: 5 to 11 years, 2 to 5 years and 6 months to 2 years. Dosing has begun in the oldest cohort, with the 2- to 5-year-old cohort to commence next.
J&J-Janssen on April 2 announced it began vaccinating participants ages 12 to 17 in an ongoing Phase 2a trial that has been testing safety, reactogenicity and immunogenicity of one- and two-dose schedules with participants ages 18-55 years and 65 years and older since September 2020. Adolescents will be included in a step-wise approach, with participants ages 16-17 years included first before expanding to younger adolescents. Moderna is conducting clinical trials for its vaccine among adolescents 12 up to 18 years old and among children 6 months to 12 years old.
US CDC TRAVEL GUIDANCE On April 2, the US CDC released new domestic and international travel recommendations for individuals who are fully vaccinated. Fully vaccinated individuals are defined as people who have received all recommended doses of SARS-CoV-2 vaccine (i.e., two doses of Pfizer-BioNTech or Moderna vaccines or one dose of J&J-Janssen vaccine) and two weeks have passed since their final dose.
CDC guidance now states that fully vaccinated people “can travel safely within the United States” and “are less likely to get and spread COVID-19” while traveling internationally. Regarding domestic travel, fully vaccinated individuals are encouraged to continue following public health guidance such as masking, physical distancing, and increased handwashing or hand sanitizer use. Under the guidance, fully vaccinated domestic travelers do not have to self-quarantine or get tested pre- or post-travel unless their destination requires it.
Compared with domestic travel, CDC guidance notes that international travel is inherently riskier due to the possibility of becoming infected with and spreading new SARS-CoV-2 variants. Accordingly, all air passengers traveling to the US are required to show proof of a negative SARS-CoV-2 test within three days of travel or documentation of COVID-19 disease and recovery in the past three months prior to boarding their flight to a US destination. Additionally, fully vaccinated international travelers are encouraged to get tested 3-5 days after arriving in the US, follow advice for domestic travel, and adhere to local and state guidance. These new changes in travel guidance, based on studies showing the real world effectiveness of vaccination, are expected to bring some relief to individuals who have missed travel as well as a struggling travel industry. However, CDC Director Dr. Rochelle Walensky urged caution, advocating that individuals avoid travel due to rising case numbers in the US.
US COVID-19 MORTALITY Researchers from the US National Center for Health Statistics on March 31 published a report in the US CDC’s Morbidity and Mortality Weekly Report describing the leading causes of US deaths in 2020. The authors analyzed provisional mortality data from the CDC’s National Vital Statistics System, ranking causes of mortality and contextualizing COVID-19 mortality trends with available demographic and medical data. Based on the provisional data, the estimated age-adjusted death rate in the US increased from 715.2 deaths per 100,000 in 2019 to 828.7 deaths per 100,000 in 2020 (+15.9%). COVID-19 was an underlying or contributing cause of death for 11.3% (377,883) of deaths in 2020; approximately 9% of COVID-19-associated deaths had an underlying cause of death that was not COVID-19. The top 3 leading underlying causes of death in 2020 were heart disease (690,882), cancer (598,932), and COVID-19 (345,323), with the next 7 leading underlying causes of mortality being unintentional injury, stroke, chronic lower respiratory disease, Alzheimer disease, diabetes, influenza and pneumonia, and kidney disease. Previously, suicide was the 10th leading underlying cause of death in the United States but was displaced from the list in 2020 due to mortality from the COVID-19 pandemic.
FDA AUTHORIZES SERIAL SCREENING TESTS On March 31, the US FDA authorized several SARS-CoV-2 tests under a recently developed streamlined pathway for test developers to gain emergency use authorization for testing tools. The FDA authorized 3 over-the-counter, at-home SARS-CoV-2 tests for serial screening of individuals who are asymptomatic and have not had a known or suspected recent exposure to COVID-19; a point-of-care (POC) test for use without a prescription; and another POC test for use with a prescription. The FDA previously had authorized these tests for symptomatic individuals. Regulators and experts hope the availability of these tests will increase access to testing, aiding pandemic responses particularly in schools, workplaces, communities, and others that plan to establish screening programs.
J&J-JANSSEN VACCINE DOSES RUINED A mistake at a vaccine manufacturing facility in Maryland (US) resulted in the loss of millions of doses of J&J-Janssen’s SARS-CoV-2 vaccine. A facility operated by Emergent Biosolutions was producing both the J&J-Janssen and AstraZeneca-Oxford vaccines and “accidentally conflated the ingredients,” resulting in the loss of an entire lot of 15 million doses of the J&J-Janssen vaccine. The error was identified through routine quality control processes before the doses were shipped. The facility had not yet received authorization to begin shipping any vaccine doses, and the incident does not affect any vaccine that was already distributed. Following the incident, the US government reportedly facilitated J&J to take over operations at the facility, and production of the AstraZeneca-Oxford vaccine has been moved to another facility. While the wasted doses were scheduled to be allocated to the US, the federal government does not anticipate major delays to national vaccination efforts.
FEMA COVID-19 FUNERAL COSTS The US Federal Emergency Management Agency (FEMA) announced it will provide financial support to offset the cost of funeral services for COVID-19 victims. The financial support is available for individuals who died in the US from COVID-19 (documented on the death certificate) after January 20, 2020, and while applicants must be US citizens or residents, there is no citizenship or residency requirement for the deceased individuals. FEMA is offering up to US$9,000 per funeral, and applicants can submit requests for multiple COVID-19 victims, up to US$35,500 per application. Among its many roles, FEMA supports disaster relief, and this effort will help mitigate the financial burden on the families of COVID-19 victims. Some of the funding for this program was allocated in the December 2020 federal COVID-19 relief package, which provided US$2 billion to FEMA to cover funeral costs for COVID-19 victims in 2020.
by ponchi101 But the pace in the USA is slowing down. That has to be taken as good news.
by atlpam Feeling pretty good after dose 2. Slight headache and sore arm - paid special attention to my hydration yesterday, as recommended when they gave me the shot.
by ponchi101 Good to hear that, atlpam.
Down here: News continue to get worse. We will go back into full city quarantine these weekend. But, even worse, the city mayor has announced that the plan for 2021 is to vaccinate the population OVER 70. So, if the USA really opens up vaccination to all people starting April 19th, I gather I will be on a plane the week after that.
Here, again, political wisdom has taken over. The GOVT has approved for private industry to import vaccines, but THEY CANNOT CHARGE FOR THEM. The socialist streak in our continent remains strong. A plan such as: you pay for your vaccine AND the vaccine of three others, not related people. Nah, too avant-garde. Only Ponchi's imagination at work.
In the meantime, the official unemployment figure in the country is 17.6%. And that does not include the informal economy, which of course is hard to measure.
by ti-amie The "informal economy". I like that expression.
by Suliso At least you aren't in Brazil, ponchi...
Informal economy is where majority work in poor countries.
by ponchi101 It is an accepted term in all L. American countries. Mostly street vendors, but with the advent of WhatsApp and a lot of internet tools that sector is also increasing. Of course, the whole thing is to avoid paying taxes and simply because the a lot of people have no access to any kind of credit so they can't open a small shop or set up a workshop.
by Suliso It's a common term in India as well. Refers to anyone who works for cash only. Street vendors, small farmers, day labourers etc. About 80% of workforce and 50% of gdp id informal. I'd expect less in SA.
by JazzNU
ponchi101 wrote: ↑Wed Apr 07, 2021 4:05 pm
Down here: News continue to get worse. We will go back into full city quarantine these weekend. But, even worse, the city mayor has announced that the plan for 2021 is to vaccinate the population OVER 70. So, if the USA really opens up vaccination to all people starting April 19th, I gather I will be on a plane the week after that.
We haven't mentioned it a ton, but vaccinations are widely open now in many states. Not uncommon now to know people in their 30s and 40s with no pre-existing conditions starting to get vaccinated now. April 19th and May 1st are more formalities and really apply more to the over 16 crowd as a whole for a national goal even though distribution is state by state. More groups in almost all states were added in the last 2 weeks, a few more this week, and more groups next week. There are some states already doing 16 and older. a few like Nevada moved in that direction probably 3 weeks ago. Point being, I think you and your girlfriend would qualify now in most states. Colorado is already allowing 16 and over. Let me know if you want me to check somewhere specifically if you're having trouble finding information. Getting an appointment can still prove to be a wait, but in terms of eligibility, it's fairly open already.
by ponchi101 Thanks, JazzNu. I am thinking either GA or FL, as it is a cheap flight (two of us) and we have family in both places. Right now, getting to CO (my place) will cost me over $1000 each, and I simply can't afford it at the moment.
I am being able to check the Kroger/City Market websites and they usually have easy registration. My little town (Pagosa Springs) has openings for TOMORROW, and that would be nice (if possible) because I can say with a straight face that I "live" there, as I have a place.
The GF is having some dental work done, so we have to wait for that to finish. Then I will make up my mind but she is pretty adamant on going. Her brother had it and he is still suffering some side effects so she is weary that the genetics will affect her (if she catches the bug).
Will post you. And anyway, going to NYC or PA means bankruptcy for me. You know, NYC shopping and my GF are no strangers...
by atlpam
ponchi101 wrote: ↑Wed Apr 07, 2021 9:43 pm
Thanks, JazzNu. I am thinking either GA or FL, as it is a cheap flight (two of us) and we have family in both places. Right now, getting to CO (my place) will cost me over $1000 each, and I simply can't afford it at the moment.
I am being able to check the Kroger/City Market websites and they usually have easy registration. My little town (Pagosa Springs) has openings for TOMORROW, and that would be nice (if possible) because I can say with a straight face that I "live" there, as I have a place.
The GF is having some dental work done, so we have to wait for that to finish. Then I will make up my mind but she is pretty adamant on going. Her brother had it and he is still suffering some side effects so she is weary that the genetics will affect her (if she catches the bug).
Will post you. And anyway, going to NYC or PA means bankruptcy for me. You know, NYC shopping and my GF are no strangers...
I expect you would have no problem in GA. Most of the state mass vaccination sites in the Southern part of the state are not requiring appointments (but you can make them if you want to be assured of a spot). There is also a large federal site set up at Mercedes Benz Stadium.
by dryrunguy For me, it's frustrating to be eligible to receive the vaccine but not to have any vaccine available within 50 miles. I figured this would be the problem.
by dave g
dryrunguy wrote: ↑Thu Apr 08, 2021 5:27 pm
For me, it's frustrating to be eligible to receive the vaccine but not to have any vaccine available within 50 miles. I figured this would be the problem.
I have to drive 60 to get mine on Sunday, but I am not surprised by that.
by Suliso Why is that the case? Small towns don't have?
by dave g
Suliso wrote: ↑Thu Apr 08, 2021 6:26 pm
Why is that the case? Small towns don't have?
My town is so small that no longer actually has a doctor. There is a clinic with a tele-medicine capability. The nearest hospital is 30 miles away. But I went with the state sign-up list and they are having a large vaccination effort in the nearest real city, which is 60 miles away.
by Suliso Ok, but then you're used to driving that long for a doctor or dentist appointment anyway.
by atlpam It really depends on the state's distribution & registration systems. Sometimes it can be difficult to find a site nearby that has appointments available, or you have to check/call a dozen different places because there's not a centralized system. I chose to drive 60 miles away because it was easier process to get an appointment. Not that many doctors offices have access to the vaccines. There's typically wider access through the big pharmacy chains.
by JazzNU
dryrunguy wrote: ↑Thu Apr 08, 2021 5:27 pm
For me, it's frustrating to be eligible to receive the vaccine but not to have any vaccine available within 50 miles. I figured this would be the problem.
Where are you looking? I saw some in Chambersburg and Shippensburg. That's closer than 50 miles to you I think. Want me to send you info?
dryrunguy wrote: ↑Thu Apr 08, 2021 5:27 pm
For me, it's frustrating to be eligible to receive the vaccine but not to have any vaccine available within 50 miles. I figured this would be the problem.
Where are you looking? I saw some in Chambersburg and Shippensburg. That's closer than 50 miles to you I think. Want me to send you info?
I was looking at pa.gov. Yes, Shippensburg and Chambersburg are each 35 miles from me. So if you have a better source, that would be great. Many thanks in advance. I was hoping to not have to go that route, but if I must, I must.
by MJ2004 I'm still not eligible. I expect to the be last person on this board who's in the U.S. to get it. MA has been f***ing this up from the start.
by JazzNU
MJ2004 wrote: ↑Thu Apr 08, 2021 9:20 pm
I'm still not eligible. I expect to the be last person on this board who's in the U.S. to get it. MA has been f***ing this up from the start.
Sorry MJ. Hopefully you're pre-registered wherever MA allows and they'll work through the list quicker than you're thinking.
by dryrunguy Here's the latest Situation Report. There's A LOT here...
::
EPI UPDATE The WHO COVID-19 Dashboard reports 133.1 million cases and 2.9 million deaths as of 6:00am EDT on April 9.
The global attention on vaccination progress has largely focused on China, Israel, the US, and Europe. Among the first to initiate large-scale mass vaccination efforts, these countries have made more progress than most; however, vaccination has commenced in most countries around the world, and today, we will take a closer look at the progress made elsewhere*.
In terms of the continent-level breakdown, Asian countries account for more than half of the daily total doses administered globally, followed by North America, Europe, South America, Africa, and Oceania. On a per capita basis, the global average is currently 0.21 daily doses administered per 100 people. North America (0.62), Europe (0.29), and South America (0.27) are higher than the global average, and Asia (0.20), Oceania (0.09), and Africa (0.02) are reporting less than the average.
Excepting the US, Brazil (25.0 million) is reporting the most cumulative doses administered in the Americas, and Chile (11.4 million) and Mexico (10.6 million) are the only other countries reporting more than 10 million doses. Most countries are reporting fewer than 1 million doses. On a per capita basis, Chile is #1 in the Americas, with 60 doses per 100 population, followed by the US (52), Uruguay (28), Antigua and Barbuda (27), and Dominica (25). Most countries are reporting fewer than 10 doses per 100 population. After the US, Brazil is leading the Americas in terms of total daily doses administered, with more than 700,000 doses per day. Mexico (342,160), Canada (193,674), and Argentina (106,885) are the only other countries reporting more than 100,000 doses per day. Approximately half of the countries in the Americas are reporting fewer than 10,000 doses per day. Uruguay (0.98 daily doses per 100 population) is reporting more daily doses per capita than the US (0.91), followed by Chile with 0.68. Canada is the only other country reporting more than 0.5.
Compared with other continents, limited data are available for Africa**, as many countries have not yet commenced vaccination efforts or reported vaccination data. In terms of cumulative doses administered, Morocco is leading the continent with 8.5 million doses, more than 8 times #2 Nigeria (nearly 1 million). Ghana (599,128), Rwanda (348,926), Kenya (340,121), Senegal (326,910), and South Africa (283,629) have also reported more than 200,000 cumulative doses. Notably, Nigeria commenced vaccination operations more recently than a number of African countries, but its progress accelerated quickly compared to others. On a per capita basis, Seychelles is #1 in Africa with more than 1 dose administered per person (106 per 100 population), followed by Morocco (23 per 100). No other African countries are reporting more than 5 doses per 100. Most countries that have reported data are at fewer than 1, with many reporting fewer than 0.5 doses per 100. Morocco (58,968 doses per day), Nigeria (44,891), and Kenya (25,479) are reporting the highest total daily doses administered. Zimbabwe is the only other country reporting more than 10,000 doses per day, and most countries are reporting fewer than 5,000 doses per day.
Asia and Oceania span multiple WHO regions, so we will provide a brief look at the Eastern Mediterranean, Southeast Asia, and Western Pacific regions individually. In the Eastern Mediterranean region**, the UAE is #1 in terms of cumulative total doses administered, with 8.9 million, followed by Saudi Arabia (5.8 million). All other countries are reporting 1 million or fewer doses. On a per capita basis, only the UAE (90), Bahrain (53), and Qatar (35) are reporting more than 20 doses per 100 population. In terms of daily progress, Saudi Arabia (168,367) and the UAE (71,181) are the only 2 countries reporting more than 30,000 doses per day, and most are reporting fewer than 15,000.
In Southeast Asia, India is #1 and rapidly approaching 100 million cumulative doses, more than 7 times the doses administered in #2 Indonesia (14.1 million). South Korea is the only other country to report more than 1 million doses administered. On a per capita basis, Bhutan (61 doses per 100 population) and Maldives (52) are #1 and #2, respectively, with India in a distant #3 (7). India is also #1 in terms of daily doses administered. With more than 3.5 million, it is reporting nearly 14 times the daily doses in #2 Indonesia (263,637). All other countries are reporting fewer than 50,000 doses per day. And finally, in the Western Pacific***, China is far and away #1 in terms of cumulative total doses administered, with more than 150 million, although it commenced vaccination efforts well before other countries. Singapore is #2 with 1.7 million. On a per capita basis, Singapore (29), Mongolia (18), and China (11) are the only 3 countries reporting more than 10 doses per 100 population. China is also #1 in terms of daily doses administered, with more than 4 million doses per day. Japan (62,499) and Cambodia (57,059) are #2 and #3, respectively, and several countries are reporting 25-40,000 doses per day.
*For the purpose of this analysis, we will limit our scope to WHO Member States. The WHO COVID-19 Dashboard does not break down vaccinations in terms of individual countries or by vaccination status (i.e., partial or full), so we will rely on data published by Our World in Data, which principally draws from national-level reporting.
**We included Djibouti, Egypt, Libya, Morocco, Somalia, Sudan, and Tunisia, in Africa, even though they are in the WHO’s Eastern Mediterranean Region.
***Our World in Data is missing data available for some WPRO countries, particularly small island nations.
Global Vaccination
The WHO reported 669.2 million vaccine doses administered globally as of April 9, including 361.1 million individuals with at least 1 dose. The dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports 733.6 million doses administered globally. The global cumulative total continues to increase at a rate of approximately 20% per week. The daily average appears to have leveled off at approximately 16 million doses per day. At least 171 countries and territories are reporting vaccination data.
UNITED STATES
The US CDC reported 30.7 million cumulative cases and 556,106 deaths. The recent increase in daily incidence appears to have leveled off to some degree, at approximately 63-64,000 new cases per day, although this could be a function of delayed reporting over the Easter holiday weekend. Daily mortality continues to decrease, now down to 710 deaths per day, the lowest average since October 2020. Daily mortality is approaching the low between the first and second surges (671 on October 6, 2020).
On April 7, Oklahoma reported approximately 1,300 previously unreported cases and 1,800 deaths. The previously unreported cases were a result of a technical error with the state’s electronic laboratory reporting system, and they occurred between December 2020 and March 2021. The deaths were a result of a discrepancy in the state’s reporting to the CDC. Oklahoma state officials are working to resolve the reporting issue, but there may be additional previously unreported deaths over the coming weeks.
US Vaccination
The US has distributed nearly 230 million doses of SARS-CoV-2 vaccine and administered nearly 175 million doses. The US is currently administering 2.8 million doses per day*, including 1.3 million people fully vaccinated.
A total of 112 million individuals have received at least 1 dose of the vaccine, equivalent to approximately one-third of the entire US population and 43% of all adults. Of those, 66.2 million (20% of the total population; 26% of adults) are fully vaccinated. Among adults aged 65 years and older, 77% have received at least 1 dose, and 58% are fully vaccinated.
In terms of full vaccination, 32.8 million individuals have received the Pfizer-BioNTech vaccine, 28.5 million have received the Moderna vaccine, and 4.9 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 31.0 million cumulative cases and 560,152 deaths as of 10:15am EDT on April 6.
ASTRAZENECA-OXFORD VACCINE & BLOOD CLOTS Now several weeks after the initial reports of blood clots in a handful of individuals who were recently vaccinated with the AstraZeneca-Oxford vaccine in Europe, countries are still struggling to determine the best approach to using the vaccine. On April 7, the European Medicines Agency (EMA) released preliminary findings from its analysis of blood clotting events associated with the vaccine. The EMA’s Pharmacovigilance Risk Assessment Committee (PRAC) analyzed data from 86 total cases of thrombosis following vaccination, including 18 deaths, and determined that blood clotting should be listed as a “very rare” adverse event for the AstraZeneca-Oxford vaccine—approximately 1 case per 100,000 people. Notably, the 86 cases occurred out of approximately 25 million people who have received one or more doses of the vaccine. The clotting events occur more frequently in women under the age of 60 and typically occur within 2 weeks of vaccination, but additional risk factors have not yet been characterized. The EMA explicitly noted that the “overall benefits of the vaccine in preventing COVID-19 outweigh the risks of side effects.” The PRAC called for further investigation of blood clotting following vaccination in order to more fully characterize risk factors and overall risk. AstraZeneca is working with British and European regulators to list thromboembolic events as an extremely rare but potential adverse event.
Evaluations by multiple other national regulatory authorities are ongoing, and in addition to Canada and Germany, several other countries restricted the use of the AstraZeneca-Oxford vaccine in younger adults. Australia’s Technical Advisory Group on Immunisation reported the blood clotting risk as 4-6 cases per million people, and it recommended largely restricting use of the vaccine to adults aged 50 years and older. Adults under the age of 50 who have already received the first dose and have not exhibited serious adverse events can receive the second dose.
The UK’s Joint Committee on Vaccination and Immunisation recommended a much younger age, setting its cutoff at 30 years. The UK’s Medicines and Healthcare Products Regulatory Agency found a slightly lower risk than the EMA at 1 case per 250,000 vaccinations. The UK guidance notes that there are no reports of blood clotting following the second dose, so anyone who has already received the first dose of the vaccine should continue with their second dose, regardless of age. For younger adults, Australia and the UK both recommend alternate vaccines that are already authorized for use. The Philippines and South Korea also suspended the vaccine’s use among people under age 60, and France, Italy, and the Netherlands all set minimum ages for the vaccine this week, following the release of the EMA’s findings.
Additionally, the African Union suspended plans to purchase the AstraZeneca-Oxford vaccine, citing concerns over shortages of supply from India. Dr. John Nkengasong, Director of the Africa CDC, said AU member states will receive the AstraZeneca-Oxford vaccine through the COVAX facility, while the AU focuses on purchasing J&J-Janssen’s single-shot vaccine. Dr. Nkengasong stressed the decision had “nothing to do” with the blood-clot concerns and noted the Africa CDC continues to recommend the AstraZeneca-Oxford vaccine.
VACCINATION CERTIFICATES Some experts and government officials have proposed vaccine certificates or passports as a means to resume “normal” pre-pandemic activities, but there have been mixed responses over the idea. Israel has implemented a “Green Pass” to those who have received two vaccine doses more than a week prior or have recovered from COVID-19 with presumed immunity to allow them access to gyms, hotels, and theaters. Applicants’ status is proven either with a hardcopy of their vaccination certificate or digitally through a health ministry app that is linked to the person’s medical file. China and the European Union also have expressed support for vaccine passports, with both planning to move forward with implementation. Although originally opposed to the idea, EU leaders are working toward approving and implementing a “digital green pass” program, which is expected to take three months to establish.
Despite growing support among some nations, not all are onboard. The American Civil Liberties Union previously expressed concern that vaccine passports would exacerbate racial and economic disparities. Some US Republicans have shown disapproval of vaccine passports, including Florida Governor Ron DeSantis, who promised an executive order barring the state from participating in any vaccination credentialing efforts. Texas Governor Greg Abbott, also opposed to requirements to show proof of vaccination, issued an executive order on April 5 saying government agencies, private businesses, and institutions that receive state funding cannot require people to show proof that they have been vaccinated on the grounds that vaccination status is private health information.
White House Coronavirus Response Coordinator Jeff Zients has said there will not be a federally mandated vaccination credentialing system and has promised more information in the coming weeks. US officials say they are struggling with several challenges in devising recommendations, including data privacy and health-care equity. Several international and US efforts are underway to provide guidance, including those by the WHO Smart Vaccination Certificate Working Group, the Vaccination Credential Initiative, and the US Federal Health IT Coordinating Council.
PANDEMIC TREATY On March 30, leaders from more than 2 dozen countries, the EU, and the WHO published a call for an international treaty for pandemic preparedness that they argue would “build a more robust international health architecture that will protect future generations.” Citing COVID-19 as the biggest global challenge since World War II, the leaders acknowledged the “pandemic has been a stark and painful reminder that nobody is safe until everyone is safe.” The main goals of the treaty would be to foster international cooperation on information sharing and research and to strengthen national, regional, and global resilience for future pandemics, including the production and distribution of public health tools, such s diagnostics, vaccines, medicines, and personal protective equipment. European Council President Charles Michel first proposed the idea of a pandemic treaty at the UN General Assembly in December.
According to WHO Director-General Dr. Tedros Adhanom Ghebreyesus, the treaty would fill gaps exposed by the COVID-19 pandemic by strengthening the implementation of the agency’s International Health Regulations (IHR) and providing a framework for pandemic preparedness cooperation. However, some experts warn that without more authority to independently verify official state reports, the WHO would continue to struggle in its efforts to alert the world of potential threats in a timely and transparent manner. The IHR, in its current form, has been in place since 2005; however, many countries have not fully implemented “core health system capacities” required under the IHR and technical and financial assistance from wealthier to lower-income countries remains lacking in many areas, so it is unclear if or how a new treaty could fill those gaps. Formal negotiations of the proposed treaty have not begun, but Dr. Tedros said discussions could begin in May at the World Health Assembly. He added that all Member States should be involved in drafting the treaty, which would be grounded in the WHO constitution and include “the principles of health for all and no discrimination.”
EMERGING VARIANTS During the April 7 White House COVID-19 Response Team briefing, US CDC Director Dr. Rochelle Walensky said that 52 jurisdictions were reporting SARS-CoV-2 variants of concern and that the B.1.1.7 variant is now the most common lineage circulating in the US. A study published on March 30 in the journal Cell suggests the B.1.1.7 strain is 40-50% more transmissible than other known variants. The researchers note the strain is more transmissible among younger populations and can lead to more severe disease, although there is no evidence the strain can evade currently available SARS-CoV-2 vaccines. Dr. Walensky urged the public to continue mitigation strategies, including mask use, physical distancing, and avoiding large gatherings, especially among younger individuals. Michigan has seen the sharpest rise in new cases among US states over the past week, and surveillance data indicate that approximately 70% of the state’s new cases are due to the B.1.1.7 strain.
Researchers from Stanford University (US) identified at least 5 cases of a “double mutant” SARS-CoV-2 strain in the San Francisco area that was originally detected in Maharashtra, India. The variant contains 2 key mutations, E484Q and L452R, that have been found separately in other variants. US regional variants, including the B.1.526 strain that first appeared in New York City in November 2020, are believed to be driving an increase in community transmission in several Northeastern states.
US VACCINE ELIGIBILITY & DISTRIBUTION On April 6, US President Biden announced that all US adults will be eligible to receive a SARS-CoV-2 vaccine on April 19, two weeks earlier than his previous deadline for states. Biden noted the US government is on track to meet its new goal of administering 200 million doses in its first 100 days, and approximately 80% of K-12 teachers in the US have received at least one vaccine dose. Many states have accelerated their eligibility timelines, with some already ahead of Biden’s new April 19 goal.
Michigan is experiencing a surge of new daily cases near its all time peak in December, with state officials and scientists urging the federal government to send additional vaccine doses. However, federal officials said they plan to maintain vaccine-allocation strategies based on population, not new COVID-19 cases. Michigan Governor Gretchen Whitmer first requested additional doses and a shift away from population-based allocation to instead target hard-hit areas of the country on March 30, but White House Coronavirus Response Coordinator Jeff Zients rebuffed the request, saying the administration is not inclined to change its system at this time.
MANDATORY VACCINATION Discourse continues over the potential implementation of SARS-CoV-2 vaccination mandates for various institutions and workplaces before their return to normal operating procedures. Several universities have implemented policies requiring students to be fully vaccinated if they wish to attend in-person classes this fall. The rationale behind these decisions comes from data suggesting college campuses might be a significant contributor to local SARS-CoV-2 transmission due to factors such as congregant living and travel from various geographic regions. Of the at least 8 universities who have announced this plan, all will allow for religious and medical exemptions. The CDC has offered guidance for SARS-CoV-2 vaccination policies in the workplace, but there are no discussions of a national vaccine mandate.
“BRIDGING” TRIALS India, one of the world’s largest vaccine manufacturers, is facing a new challenge after the Drug Controller General of India (DCGI) implemented requirements for foreign companies and domestic companies working with foreign partners to perform “bridging trials” before the agency will consider authorizing any vaccines first tested abroad. In other words, DCGI is requiring any vaccine that completed Phase 3 trials outside of the country to undergo bridging trials, or local clinical trials, before being considered for authorization. The rationale behind the bridging trials is to see whether vaccine candidates are able to provide similar results when applied to specific in-country factors.
COVID-19 & NEUROLOGICAL CONDITIONS A study published in The Lancet Psychiatry estimates that more than one-third of COVID-19 survivors experienced neurological symptoms within 6 months of their infection. Researchers at the University of Oxford (UK) evaluated medical record data for nearly 250,000 COVID-19 patients and found that 33.62% were diagnosed with a neurological or psychiatric condition in the 6 months following their infection, including 12.84% for whom this was their first such diagnosis. The proportion increased among those who were admitted to an intensive care/treatment unit (ICU/ITU), up to 46.42% and 25.79%, respectively. The most common conditions included anxiety disorders (17.39%), mood disorders (13.66%), substance use disorder (6.58%), insomnia (5.42%), nerve disorders (2.85%), and ischemic stroke (2.10%). The study breaks down each condition by disease severity.
The researchers also compared the cohort against patients who were diagnosed with influenza and other respiratory diseases and found that COVID-19 patients were at significantly higher risk of neurological and psychiatric conditions following infection. Many neurological and mental health conditions are underdiagnosed in the broader population, so it difficult to definitively link these conditions to COVID-19, but the evidence indicating the elevated incidence compared to patients with other respiratory diseases provides further indication that SARS-CoV-2 can have lasting effects long after the acute stage of infection or disease.
SCHOOL TESTING WEBINAR The Johns Hopkins Center for Health Security is hosting a webinar on April 13 (2pm EDT) to discuss lessons from K-12 testing programs in Delaware (US). A panel of experts will discuss school-based testing strategies and best practices as well as the importance of testing to ensure schools can effectively mitigate COVID-19 risk and resume in-person learning. The panelists will also provide insights into Becton Dickinson's SARS-CoV-2 testing capabilities, including training and education efforts.
The panelists include Dr. Adam Zerda, Director of Strategy and Public Affairs at Becton Dickinson; Dr. Richard Pescatore, Delaware’s Chief Physician and Associate State Medical Director; and Andrew Lux, Director of Application Management and Implementations for Healthcare IT Leaders, and the panel will be moderated by the Center for Health Security’s Dr. Gigi Gronvall. This webinar is part of a series hosted by the Center’s COVID-19 Testing Toolkit program, which provides essential information for organizations seeking to engage in SARS-CoV-2 testing. You can register for the webinar here.
dryrunguy wrote: ↑Fri Apr 09, 2021 5:55 pm
COVID-19 & NEUROLOGICAL CONDITIONS A study published in The Lancet Psychiatry estimates that more than one-third of COVID-19 survivors experienced neurological symptoms within 6 months of their infection. Researchers at the University of Oxford (UK) evaluated medical record data for nearly 250,000 COVID-19 patients and found that 33.62% were diagnosed with a neurological or psychiatric condition in the 6 months following their infection, including 12.84% for whom this was their first such diagnosis. The proportion increased among those who were admitted to an intensive care/treatment unit (ICU/ITU), up to 46.42% and 25.79%, respectively. The most common conditions included anxiety disorders (17.39%), mood disorders (13.66%), substance use disorder (6.58%), insomnia (5.42%), nerve disorders (2.85%), and ischemic stroke (2.10%). The study breaks down each condition by disease severity.
The researchers also compared the cohort against patients who were diagnosed with influenza and other respiratory diseases and found that COVID-19 patients were at significantly higher risk of neurological and psychiatric conditions following infection. Many neurological and mental health conditions are underdiagnosed in the broader population, so it difficult to definitively link these conditions to COVID-19, but the evidence indicating the elevated incidence compared to patients with other respiratory diseases provides further indication that SARS-CoV-2 can have lasting effects long after the acute stage of infection or disease.
This is disturbing especially since here in the US information like this is not given adequate media attention.
by ti-amie Also here in the good ol' US of A...
by ti-amie They're asking for the contracts to be rewritten but what if countries turn around and do what India is doing re "bridge testing"? If only the previous guy and his staff had cared about this even as a potential situation vaccine distribution could face.
by JazzNU
ti-amie wrote: ↑Fri Apr 09, 2021 6:05 pm
This is disturbing especially since here in the US information like this is not given adequate media attention.
That bird app that many think has no value, had this story on my sidebar for the last 3 days. There's certainly downsides to it, but I get considerably more news about things I wouldn't hear about by using it.
ti-amie wrote: ↑Fri Apr 09, 2021 6:05 pm
This is disturbing especially since here in the US information like this is not given adequate media attention.
That bird app that many think has no value, had this story on my sidebar for the last 3 days. There's certainly downsides to it, but I get considerably more news about things I wouldn't hear about by using it.
Yep. I saw it awhile before posting it here. Complain about the bird app all you want but it's what you make it. If you don't know how to start set up an account and follow someone you like and then see who they follow. That's how I started.
by mmmm8
MJ2004 wrote: ↑Thu Apr 08, 2021 9:20 pm
I'm still not eligible. I expect to the be last person on this board who's in the U.S. to get it. MA has been f***ing this up from the start.
I think you'd mentioned having celiac disease/intolerance, doesn't that qualify as a relevant co-morbidity (auto-immune condition)? I know my friend with a similar food-related auto-immune issue was able to get vaccinated, although in NY (also, no one checks for medical proof of the co-morbidity).
by MJ2004 Nope. Doesn’t count.
Sent from my iPhone using Tapatalk
by atlpam New Hampshire is opening vaccines to out-of-state visitors.
by Deuce
atlpam wrote: ↑Sat Apr 10, 2021 9:09 pm
New Hampshire is opening vaccines to out-of-state visitors.
^ And only 2650 miles from Bogota!
Go for it, ponchi!
atlpam wrote: ↑Sat Apr 10, 2021 9:09 pm
New Hampshire is opening vaccines to out-of-state visitors.
Day trip to Nashua?
by ti-amieMany of Michigan’s Thumb residents are done with COVID-19 pandemic, even as virus rages like ‘wildfire’
Updated Apr 10, 4:51 PM; Posted Apr 10, 9:15 AM
Sandusky, population 2,500, is the county seat of Sanilac County, 40 miles north of Port Huron and in the heart of the Thumb, a region known for its expansive Lake Huron shorelines, its rolling farmlands and its friendly small towns.
In recent weeks, it’s also become known for its coronavirus rates.
On Friday, five of the nation’s top 15 counties in per-capita coronavirus cases were in Michigan’s Thumb -- St. Clair, Huron, Sanilac, Tuscola and Lapeer.
Collectively, the five counties have reported 3,167 new cases of COVID-19 reported in the past seven days, a per capita daily rate of 1,216 cases per million residents -- six times the national average and eight times the benchmark for the state’s highest risk level of 150 cases per million residents.
The region also has an eye-popping 32% positivity rate as a seven-day on coronavirus diagnostic tests, more than six times the level considered safe.
“These communities are literally on fire,” said Dr. Mark Hamed, public medical director for Lapeer, Huron, Sanilac and Tuscola counties.
Ask the region’s health experts for the reasons behind the spike, they point to multiple factors.
Compared to the rest of Michigan, the Thumb was less impacted by previous surges, which meant fewer people had natural immunity coming into the spring. The area appears to be hard-hit by the new B.1.1.7. variant which is much more contagious and also more lethal. Restrictions implemented in November have been eased, increasing social interactions.
And fanning the flames is widespread resistance among local residents to coronavirus mitigation strategies such as masking and avoiding indoor gatherings, said Bryant Wilke, Sanilac County public health director.
“There’s been a defiance towards masks,” Wilke said, “and I think it was because it got so political at the beginning of the pandemic. People said, ‘We don’t trust this. We never had to do it before,’ even through its been proven that it is a protective factor. People haven’t gotten over the hump to say, ‘We need to do this,’ and now we’re seeing the causation of not doing it and that’s the skyrocketing numbers in cases.
“I compare us to a potential wildfire,” Wilke said. “You’ve got fuel out there and the virus hadn’t hit us that bad yet. Now it’s hitting us and we’re dealing with the U.K. variant, and it’s just moving through the population rapidly.”
At the same time, Thumb residents -- like many in Michigan -- are thoroughly sick of more than a year of various coronavirus restrictions. They are ready to move on, whether the pandemic is over or not.
“We’re just f----- done with it,” Heberling said.
At the beginning of the pandemic, Tank said, people were “scared enough about the virus” to pay attention to emergency orders issued by the state.
But people have moved beyond that now, he said. “They’ve had it.”
Joseph Schlichting, 29-year-old who grew up in Sanilac County and moved back just before the pandemic, He said he’s not surprised that the Thumb has become an epicenter for coronavirus.
“Some people who took the restrictions seriously saw the numbers go down, so they stopped working with the restrictions,” he said. “But I think there’s a large group of people who just never followed the rules from Day 1.
“It’s been kind of eye-opening to see people that you’ve known all your life, people you would think would take this kind of risks seriously or take precautions seriously, but they don’t or seem to just flat out think it’s a lie.”
The politics of COVID
Hamed has long worried that the Thumb is vulnerable because of residents’ disdain for coronavirus restrictions.
Still, good luck and geographic isolation meant the Thumb wasn’t hit as hard as other parts of Michigan in 2020.
“I think that allowed people to discount how serious this is,” Hamed said.
But as COVID-19 numbers came down statewide in January, the numbers dropped less in the Thumb.
“So we were still at a higher level, higher than average,” Hamed said. “Than gradually as the variants became more predominant, combined with the behaviors on mask use and distancing,” the numbers took off.
“We kind of saw this coming,” he said.
Fueling the attitude around the pandemic are the region’s political leanings. In the November election, 72% of voters in Sanilac County cast their ballots for Donald Trump, one of the highest percentages in the state. In the five-county Thumb region, it was 67%.
Trump’s popularity in the region certainly didn’t help with public health messaging around COVID-19, considering the former president’s skepticism of the masks and the seriousness of the pandemic in general, Hamed said.
“It created mixed messages that muddied the waters for a lot of rural Michigan” where Trump is revered, Hamed said.
No question, echoes of Trump’s talking points about the pandemic are apparent in talking to his supporters about the pandemic. That said, the rhetoric of conservatives has shifted over time. A year ago, some were suggesting the pandemic was a hoax, something no more harmful than seasonal flu. Today, skeptics are less likely to offer that argument.
“I definitely don’t think it’s a hoax,” Tank said. “I do think the virus is real. I know people who have had it. I know people who have gotten very sick from it. My father got it, and he was very sick. My brother, who’s a couple years younger than me, relatively healthy guy in his 30s, had it quite bad.”
But Tank is among those who question whether the mitigation strategies have made any difference.
“We all just need to live our lives,” he said. “My opinion is that you’ve either had coronavirus or you’re going to get it.”
He points to states such as Florida that have far less restrictions than Michigan and currently lower caseloads. In his reading on the topic, he said, it appears that coronavirus particles are too small to be contained by cloth masks. He’s highly skeptical that indoor dining contributes to coronavirus transmission rates. The vaccine “makes him a little nervous” and he questions whether it really works.
Tank said he greatly resents what he feels is government overreach. He sees Gov. Gretchen Whitmer as “extremely power hungry” who is just using the pandemic as an excuse to be an authoritative leader. He especially doesn’t trust government officials after a November election that Tank is convinced was stolen from Trump.
Another thing that’s fueled his skepticism, he said, is the changing advisories from the federal Centers for Disease Control.
“One day, a mask is great, and the next day, it’s not great. One day, you should be six feet apart. The next day, it’s three feet,” he said. “They’re just all over the map. So when the people who are supposed to be the professionals are so unclear, that kind of leaves enough doubt in my mind to where I’m just going do what I feel is best for me and my family.
“We’re strong. We’re healthy. We take care of ourselves and do the proper things that I think prevents us from getting sick,” he said.
That fact that more than a year after the pandemic started, the state is still under emergency orders proves to Tank that experts really don’t know what they’re doing.
“It started out as two weeks to flatten the curve and here we are, 13 months later,” he said.
Like Tank, Heberling said that he doesn’t question whether the virus is real. But he does think the pandemic has been grossly mismanaged.
On a mirror in Heberling’s barbershop is a sticker that reads “MI COVID POW.”
He’s scornful of lockdowns and mask use, saying keeping people indoors and masked has hurt their immune systems. “You need fresh air in your lungs every day,” he said. And people “are constantly touching their masks, so they’re transporting bacteria to the next thing they touch.”
Heberling also thinks the United States has ignored medications such as hydroxychloroquine and ivermectin as coronavirus treatments. “I think there are medications out there if used early on could have greatly decreased the number of cases,” he said.
Hamed is clearly frustrated by the misinformation being passed around.
Because COVID-19 is a new disease, the science is evolving and advisories have changed as experts have learned more, he said. But it’s clear by now that masking reduces transmission rates, as do other mitigation strategies such as a restrictions on indoor dining. Researchers have yet to come up with medications that can prevent coronavirus. The vaccines have proven to be highly safe and effective.
As for the emphasis on individual liberty, “that’s fine when the individual decisions affect you and only you,” Hamed said. But when battling a highly contagious, lethal disease, “you have to be mindful of others. When it involves decisions that impact others around you -- your employees, your colleagues, your family members -- that changes the dynamics entirely.”
A sense of urgency
But even as people such as Tank and Heberling say they’re done with governmental attempts to address the pandemic, the medical professionals on the frontline in the Thumb see a deepening crisis.
A big concern is that COVID-19 variants seem to be spreading infection more rapidly and causing more serious illness.
“Anecdotally, we’re seeing people are getting sick from teenagers to 50-year-olds in age brackets where they didn’t get that sick before,” Wilke said. “Now they’re getting sick and we’re seeing more hospitalizations.”
In his daily conversations with the county’s communicable disease nurse, Wilke said, she’s reporting that increase in contagion.
“At the beginning of the pandemic, one or two people in the family may have gotten COVID,” Wilke said. “Now we’re seeing the entire family get it, because it’s so contagious.”
His contagious disease nurse also is reporting that some people are catching COVID for the second time, Wilke said.
Current trends upend the idea that communities simply need strategies to protect the elderly and those with serious health conditions, Hamed said. “The fact is, we’re seeing a lot of otherwise healthy people get very sick. So it’s no longer just about protecting the vulnerable.”
Hamed said he also worries about the strain on hospital resources, for both COVID and non-COVID patients. At one point this week, he said, it took five hours for the emergency department at the small Sandusky hospital to find an inpatient bed for a patient “because every one of our local hospitals that accept patients was absolutely full.”
“So this is a reality that we need to accept, Hamed said. “It’s affecting us all. It really is.”
Wilke said that he’s convinced the road out of this current surge is through vaccinations, and he’s trying to vaccinate as many Sanilac County residents as fast as he can.
But there’s resistance on that front, too: 31% of adults in Sanilac County and 33% in the five-county Thumb region have gotten at least one vaccine dose so far compared to a state average of 39%.
Heberling, the Sandusky barber, is among those suspicious of COVID-19 vaccines.
“It’s not a vaccine that’s been proven. It’s basically in test form now,” he said. “I know very few people who have gotten the vaccine. I bet 80% of people in this community won’t get it.”
Wilke acknowledges that many are hesitant to get the vaccine. But he also sees that hesitance eroding. He pointed to the Sanilac County Sheriff’s Office. During the first vaccine clinic for the department, “about 10 deputies come through. The next time, another 10 signed up. And then another 10 the next time,” he said. “So it takes a little time for people to get used to the idea.”
Initially, “there was quite a bit of hesitance,” Hamed said. “We’re seeing less now. I think the reasons are twofold: I think people are seeing others getting vaccines without developing weird side effects, and people also are seeing others get very sick with this illness.”
At the vaccination clinic
It’s a hopeful sign, Wilke said, that he had no trouble filling up the schedule for several mass vaccination clinics being held in Sanilac County this past week.
Jennifer Gierman, a stay-at-home mother, was among those at a vaccination clinic Tuesday,.
“I’m pretty excited” about getting her first shot of the Moderna vaccine, said Gierman, who is 49.
Gierman said she’s taken the pandemic much more seriously than many others in the Thumb. “I haven’t seen my mom or dad since Christmas,” she said. “My daughter calls me COVID mom because there’s friends where she’s very close to them and we don’t allow them in the house.”
It’s dismaying to see the dismissive attitude that many have adopted about the pandemic, she said.
“I don’t feel like wearing a mask is a political thing. I think it’s a respect thing,” she said. “Yet here you get looks for wearing a mask.
“And like at school, my younger daughter said that in the beginning, the school was good about enforcing the masks but kids push the limits and by the end of the day they’re wearing them as chin diapers,” Gierman said. “For sure, teenagers are going to push boundaries no matter what. But they also mimic what they see at home and in the community.”
Even at this point, with community people getting sick and hospitalized, she said, “people still don’t take seriously. I don’t know what it takes to convince them.”
Hamed is more optimistic.
“We’re getting hit hard right now, and I think behaviors definitely will change,” he said. Thumb residents “care a lot about each other. When their neighbors are sick, when they’re hospitalized, that’s a motivator right there. These are small communities and they all know each other.
“What we’re doing right now is focusing on prevention, treatment and education. We think having reliable information from reliable sources can be key to combatting misinformation,” Hamed said. “I think people are going to come out of this knowing that the information they heard from the people who downplayed it was absolutely false.
“People accuse us of trying to feed a narrative, trying to fix a narrative,” Hamed said. “That’s no narrative to fix. Let’s save lives.”
Imagine what life would be like today if at the height of the polio pandemic, people decided they didn't want to get vaccinated because they thought they knew more about the vaccines than the scientists who made them.
by JazzNU ^^ How very Michigan that article is. As someone who went to college in the Midwest and experienced Michiganders who broke out their hand as part of their introduction to explain where they were from and no one from outside of the state knowing what the heck they were doing, I thought I'd include a rough map to explain why they are referring to "the thumb." Michigan can kind of sort of fit on a hand. So they know where to identify themselves to one another throughout the state. Everyone knows where Detroit is, not so many may know where Holland is, for example, so it seemingly simplifies things. Very common within the state according to Michigan friends. To me and many others, very uncommon outside of the state to know anything about this.
Can't find a more descriptive photo, but gives an idea at least.
by ponchi101 Even after I get my vaccine I will wear my mask, will avoid large crowds (although I hope I will be able to patronize establishments so that I can do my part for the economy), will continue with proper hygiene and, if it is needed, will get any and all booster shots that may come in the future.
But if you do not want to get vaccinated or decide you are getting the homeopathic (or some other ridiculous idea) remedy, please, go ahead. I really will not cry if evolution takes your hand.
If entire swaths of "educated" populations are wiped out with a remedy at hand, so be it. It is not as if we are an endangered species.
by ti-amie
by JazzNU Alright then. The apparently "not going to be cancelled" 2020 Olympics start in just over 3 months...
by Suliso Large and rich country, but rather weak pharma sector (except Takeda) with zero domestic vaccine manufacturing capacity. Combine that with over conservative approach and here we are.
by Suliso
by Suliso The above is super important. All the theater about disinfecting surfaces is irrelevant, catching it on the beach very unlikely as well. Any kind of gathering indoor is risky. Where unavoidable solution is masks AND ventilation by keeping windows open as much as possible. Restricting the number of people helps too, but keeping distance is irrelevant. I suspect public transport is an issue too. In a train from which I write this post there are no openable windows...
by Deuce ^ ^
I think it's rare to see trains whose windows open. While this is certainly problematic within this pandemic, it's to be expected.
Here, we have new city buses with windows that don't open. Because, just before the pandemic hit, they decided to order several buses that have air conditioning.
Now, you can have BOTH air conditioning in buses AND windows that open. But they ordered the ones with windows that don't open. Stupid.
Even more stupid is the fact that they are using these buses whose windows don't open. There is no need to use them - they have plenty of other, older buses without air conditioning whose windows open - and they're in fine condition. But they want to show off the new air conditioned buses - even at the cost of having little to no proper ventilation in the midst of a year-long pandemic which has killed over 20,000 people in this country.
I somehow doubt I'm alone in preferring to be uncomfortably hot while being significantly more safe from COVID-9 than to be comfortably cool in air conditioning while I contract the virus...
by ponchi101 European/Canadian public transportation style should not be a problem. It will be a problem in L. America, Africa and places like Central Asia and India. Here, the problem is not A/C or no A/C, or opening windows. All buses have opening windows because non have A/C, but the issue is that a 30 people bus will be crammed with 50+. No such thing as BUS LOAD LIMIT or anything like that.
The only place where I have seen buses with empty seats at normal business hours is Buenos Aires. Other than that, it is "sardine can" style.
by ponchi101 6 cases of blood clots appear to be related to the J&J vaccine, so the "abundance of caution" clause kicks into effect. The FDA is pausing the use of the vaccine. I wonder how many million doses of the vaccine have already been applied.
Down here, we are hearing that the government is administering the Pfizer/BionTech to people in the health areas but for the rest of the population they are applying the Chinese vaccine (Sinovac). Which pretty much seals the deal that I will travel to the USA to get my shots.
by Suliso Chinese officials recently admitted that their vaccines are barely 50% effective.
Wouldn't wind be a factor, though? And a larger area for disbursement/dilution?
by ponchi101
Suliso wrote: ↑Tue Apr 13, 2021 2:49 pm
Chinese officials recently admitted that their vaccines are barely 50% effective.
We saw that which is one more reason why we are not taking it. The health provider I am registered with explains that they are handing out 4 types: Pf-BT, AZ, Jansen or Sinovac, but you do not get to chose which vaccine you will get. I sincerely will not accept the Sinovac if I get there and that is what they are about to give me, so that makes it at a minimum a 25% chance of getting that one. At 50% effectiveness I think it may have a little beneficial impact as a public health tool, but at the individual level it makes no sense. Therefore, Georgia here I come.
The situation is a bit more interesting. There are several stories doing the rounds that the US Govt is voiding your visa if you travel their to get vaccinated. Of course, my GF has several friends that have had their shots there and ICE and the FBI have not arrested them, so it seems it is simply a bit of South American paranoia.
Meanwhile, in Venezuela, where there are NO vaccines, a small black-market is developing. Some people are peddling vaccines at $500/shot. Of course, there is no guarantee that you are getting an actual vaccine or they are just injecting you a vial of distilled water.
Sometimes being a Venezuelan is truly a shameful thing.
by Suliso Yes, exactly. Wind quickly blows the aerosol away and dilutes it below infectious level. Hence outdoors infections unlikely except in particular crowded situations (dense outdoor market, choir singing, crowds at a football match etc).
by JazzNU
Suliso wrote: ↑Tue Apr 13, 2021 2:49 pm
Chinese officials recently admitted that their vaccines are barely 50% effective.
What?!? Is this tied to the vaccines being administered in the UAE? I know they found little immune response in some and suggested those patients comes in for a third dosage. But I only heard about it in UAE though. Do you know if it's the 2nd or 3rd doses that are registering the 50% efficacy?
Also, not sure how many vaccines China has, but last I read, China was set to supply Japan with vaccines for Olympic athletes.
Suliso wrote: ↑Tue Apr 13, 2021 2:49 pm
Chinese officials recently admitted that their vaccines are barely 50% effective.
What?!? Is this tied to the vaccines being administered in the UAE? I know they found little immune response in some and suggested those patients comes in for a third dosage. But I only heard about it in UAE though. Do you know if it's the 2nd or 3rd doses that are registering the 50% efficacy?
Also, not sure how many vaccines China has, but last I read, China was set to supply Japan with vaccines for Olympic athletes.
Not clear which specific Chinese vaccine (I think there are five) this is about or maybe all. In Brazil it has been measured as barely over 50%.
by Suliso I don't think we can trust either Chinese or Russian vaccines fully. Their data have not been review by trustworthy medical authorities not under their government control.
by ti-amie These Tweets are easy to understand for me, a layperson.
ponchi101 wrote: ↑Tue Apr 13, 2021 2:37 pm
6 cases of blood clots appear to be related to the J&J vaccine, so the "abundance of caution" clause kicks into effect. The FDA is pausing the use of the vaccine. I wonder how many million doses of the vaccine have already been applied.
Down here, we are hearing that the government is administering the Pfizer/BionTech to people in the health areas but for the rest of the population they are applying the Chinese vaccine (Sinovac). Which pretty much seals the deal that I will travel to the USA to get my shots.
More than 6.8 million doses of J&J given in US as of Monday (per FDA)
by ponchi101 6 cases of blood clots in a population of 6+ million.
Here's. My. Arm.
This is extremely poor risk management, and very simple math to understand. If the vaccine gives you a 1/1,000,000 chance of blood clots, that is still extremely better than NOT getting a vaccine and getting the virus.
I really don't understand why this so hard to understand.
by Deuce
Suliso wrote: ↑Tue Apr 13, 2021 3:29 pm
Yes, exactly. Wind quickly blows the aerosol away and dilutes it below infectious level. Hence outdoors infections unlikely except in particular crowded situations (dense outdoor market, choir singing, crowds at a football match etc).
And yet, I can no longer play OUTDOOR SINGLES tennis here without wearing a mask!
I’m all in favour of being careful - and I’ve been very, very careful with the virus... but this is completely insane.
Also, doubles (masked) is only allowed with people from the same household... but doubles lessons (masked) are allowed with people from different households!
And you can sit outside with 7 other people (from different houses) with no masks, as long as you’re 2 metres apart... but you have to wear a mask playing singles tennis when you’re 30 metres apart.
It makes no sense at all. Absolutely None.
Rational thinking has gone out the window as politicians manipulate and manoeuvre, trying desperately to show people "Look - we're trying to protect you - aren't we wonderful?! Vote for us!".
Sigh...
by ponchi101 Bogota's major ordered all tennis and golf clubs to be closed for the weekend, because of the risk.
Soccer fields? No problems.
It can be that they are not trying to get votes. They may actually be that dumb.
by ti-amie
by dryrunguy
ponchi101 wrote: ↑Tue Apr 13, 2021 7:10 pm
6 cases of blood clots in a population of 6+ million.
Here's. My. Arm.
This is extremely poor risk management, and very simple math to understand. If the vaccine gives you a 1/1,000,000 chance of blood clots, that is still extremely better than NOT getting a vaccine and getting the virus.
I really don't understand why this so hard to understand.
If only mass shootings were vaccine-related blood clots...
by mmmm8
dryrunguy wrote: ↑Wed Apr 14, 2021 2:40 pm
If only mass shootings were vaccine-related blood clots...
If only women's birth-control-related blood clots were vaccine-related blood clots.
by Deuce It's no longer illegal for us to play singles tennis outside without wearing a mask. That mandate lasted barely 24 hours. It was obviously entirely ridiculous (insane, actually), and the government repealed it as soon as they became aware that the rest of the world was laughing at them.
by atlpam
Deuce wrote: ↑Thu Apr 15, 2021 2:09 am
It's no longer illegal for us to play singles tennis outside without wearing a mask. That mandate lasted barely 24 hours. It was obviously entirely ridiculous (insane, actually), and the government repealed it as soon as they became aware that the rest of the world was laughing at them.
In my husband's league tennis, they substituted a 10 pt tiebreak for a 3rd set due to Covid - not sure how a 3rd set adds any more risk than the 2 you already played - just another stupid & inconsistent rule.
by ponchi101 Germany rejecting 10MM doses of the J&J vaccine. Smart.
Random headline I read (paraphrasing): "man has stroke six hours after receiving vaccine".
I wonder how many people had a car accident on their way back home when returning from their vaccination. It must have been the vaccine too.
by Suliso EU might be able to vaccinate itself entirely with mRNA vaccines alone even if it takes a couple months more. No such luxury globally.
by JazzNU
ponchi101 wrote: ↑Thu Apr 15, 2021 2:03 pm
Germany rejecting 10MM doses of the J&J vaccine. Smart.
Random headline I read (paraphrasing): "man has stroke six hours after receiving vaccine".
I wonder how many people had a car accident on their way back home when returning from their vaccination. It must have been the vaccine too.
Not sure why they are at the point of rejecting. Doctors here have been on the news explaining the pause in more depth. In addition to making sure they have an effective treatment plan for this type of blood cot since the standard one is contraindicated, they need to educate doctors around the country on what to look for to identify this as a potential issue and how to treat a patient that is presenting symptoms. This is not presenting at the vaccination sites like allergic reactions were, but a week or two later, so primary care and ER doctors are the most likely doctors that will need to diagnose patients. Also, one of the research doctors said this approach will likely lead to identifying a few more cases, and commonalities can be determined to see if there's a specific group that shouldn't be taking the J&J.
Makes sense to me. Hopefully it will make sense to others and stop the panic. Having a one-shot vaccine is going to be key in this race, there are a few populations where two doses is truly just not feasible. And last I checked, Germany does have some of them.
by Suliso Just random from Twitter
by dryrunguy Here's the latest Situation Report. Haven't read it.
EPI UPDATE The WHO COVID-19 Dashboard reports 138.4 million cases and 3.0 million deaths as of 5:15am EDT on April 16.
On April 13, India surpassed 150,000 new cases per day, and on April 14, it reported more than 200,000 new cases in a single day for the first time. India’s COVID-19 epidemic appears to still be accelerating. In fact, its average daily incidence is increasing at approximately 10,000 more new cases each day. If it continues on this trajectory, India could surpass 200,000 new cases per day in the next 2-3 days. India is only the second country to surpass 150,000 new cases per day, after the US; however, due to the size of its population, India remains well below the United States’ peak on a per capita basis. Turkey’s current COVID-19 surge is twice as high as its previous peak (December 2020), and it continues to move toward the US (#2) and Brazil (#3) in terms of total daily incidence.
As countries increase vaccination coverage, governments and experts are beginning to look for evidence of the vaccines’ effect on national COVID-19 epidemics. It remains unclear exactly what degree of coverage is necessary to make a noticeable impact on community transmission—or how that might depend on the current level of community transmission—so there is no clear target in place. It is likely that the vaccines will begin to slow community transmission before countries achieve the coverage necessary for herd immunity—ie, the level of immunity that will contain most outbreaks in the absence of other interventions (eg, mask use, physical distancing)—particularly in areas where COVID-19 restrictions remain in place. This week, we will look at COVID-19 incidence trends in countries with the highest vaccination coverage*.
Israel and Seychelles remain the top 2 countries in terms of SARS-CoV-2 vaccination coverage. Israel is #1 globally in terms of full vaccination coverage, with 57.3% of its population, and Seychelles is #2 with 46.7%. The ranks are reversed for partial vaccination (ie, at least 1 dose), with Seychelles at #1 (67.4%) and Israel at #2 (61.7%). Israel and Seychelles have made considerably more progress than the rest of the top 20 countries. In terms of full vaccination, the remaining countries range from Chile with 26.8% to Czechia with 7.7%. For partial vaccination, the UK is #3 with 47.8%, and Morocco is #20 with 12.3%.
Among these 20 countries, 9 are reporting increasing incidence over the past 2 weeks. Turkey is reporting the largest biweekly change, with daily incidence up 78.9% compared to 2 weeks ago. Bahrain (34.1%), Singapore (28.6%), and Morocco (24.3%) are all reporting increases of more than 20% over that period. Notably, Bahrain and Turkey are facing ongoing surges, while Singapore and Morocco are reporting consistently low daily incidence. While Turkey’s full vaccination coverage is still relatively low (9.2%), Bahrain’s coverage ranks #4 globally, with more than one-quarter of its population fully vaccinated. But even this level of coverage does not appear to be sufficient to contain Bahrain’s epidemic, although it appears to be leveling off to some degree over the past several days. Other countries among this group that are exhibiting clear increases in daily incidence include Chile, Denmark, Switzerland, and the US.
Each country’s epidemiologic situation is different, so it may not be possible to draw any direct conclusions solely based on vaccination coverage and incidence for each individual country, but perhaps grouping countries by coverage could allow us to identify relevant trends. Among the top 20 countries, 7 are reporting full vaccination coverage of less than 10%. Three (3) of these countries—Czechia, Iceland, and Romania—are reporting decreasing daily incidence, while the other 4—Denmark, Singapore, Switzerland, and Turkey—are reporting increasing trends. Five (5) countries are reporting 10-20% coverage. Among these countries, only Morocco is reporting increasing daily incidence, while Hungary, Malta, Serbia, and the UK are all decreasing. In fact, the UK’s epidemic has been declining from its highest peak since early January 2020, when its vaccination coverage was less than 1%. Another 6 countries are reporting 20-30% full vaccination coverage. This group is split evenly, with 3 countries reporting decreasing daily incidence—Monaco, San Marino, and the UAE—and 3 reporting increasing trends—Bahrain, Chile, and the US. The top tier includes just 2 countries: Israel and Seychelles, both with coverage greater than 40%. Israel’s epidemic has been declining since mid-January, when its vaccination coverage was less than 4%. Seychelles’ epidemic trends are more difficult to discern, but its monthly average does appear to show an overall decline from its largest peak.
Looking at just the top countries in terms of partial coverage, there is not much additional evidence of vaccination related trends. In terms of daily incidence, Chile’s epidemic has been steadily growing since late 2020, despite 40% of the population with at least 1 dose. Maldives and Malta are reporting decreases from their highest peak, which both occurred within the past month. The UAE is reporting a relatively steady decline from its highest peak, and the United States’ daily incidence has increased steadily over the past several weeks, despite increasing vaccination coverage. Bhutan has reported essentially zero daily incidence since late January, so it is difficult to identify any meaningful trend.
Clearly, we are not yet to the point at which we can draw definitive conclusions regarding the effect of national vaccination efforts on containing COVID-19. The clinical trials have demonstrated high efficacy at the individual level for many of the vaccines currently in use**, but it is more difficult to observe their effects on the population level. While countries like Israel and the UK are reporting consistent and long-term declines in daily incidence, the trends began well before vaccination coverage was at a meaningful level. It could be possible, however, that the current coverage is high enough to help keep low-level transmission suppressed. A number of other countries near the top in terms of vaccination coverage are reporting ongoing COVID-19 surges, including some that are setting new national records. Some of these countries are quite large, and regional differences in vaccination coverage and SARS-CoV-2 community transmission could be masked in national-level data. It is likely that the countries demonstrating success in terms of containing their respective COVID-19 epidemics are utilizing a combination of COVID-19 restrictions (eg, physical distancing, mask use) and vaccination. Without sufficient vaccination coverage to contain community transmission by itself, COVID-19 risk mitigation measures are still needed in the near term to drive down transmission until vaccination coverage is high enough.
*Not all countries that are reporting COVID-19 incidence data are reporting the number of partially (ie, at least 1 dose) or fully vaccinated individuals. We limited our analysis to the top 20 countries with available data for fully vaccinated individuals.
**Several vaccines do not yet have publicly available Phase 3 clinical trial data.
Global Vaccination
The WHO reported 751 million vaccine doses administered globally as of April 16, including 422 million individuals with at least 1 dose. The WHO dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports 860 million doses administered globally. The global cumulative total continues to increase at a rate of approximately 18% per week. The daily average surpassed 18 million doses per day briefly before falling slightly to 17.5 million doses per day. At least 176 countries and territories* are reporting vaccination data.
*Out of 191 reporting COVID-19 incidence data.
UNITED STATES
The US CDC reported 31.2 million cumulative cases and 561,356 deaths. Daily incidence continues to increase, up more than 30% from the recent low on March 19. Daily mortality also has increased over the past several days, up from 642 deaths per day on April 7 to 712 on April 14, an 11% increase over that period. The timing of the most recent low in daily mortality coincides with the Easter holiday weekend, so that could be due, in part, to delayed holiday reporting.
US Vaccination
The US has distributed 255 million doses of SARS-CoV-2 vaccine and administered 198 million doses. Daily doses administered* has leveled off at approximately 3 million, including 1.6 million people fully vaccinated.
A total of 126 million individuals have received at least 1 dose of the vaccine, equivalent to 38% of the entire US population and 48% of all adults. Of those, 78 million (24% of the total population; 30% of adults) are fully vaccinated. Among adults aged 65 years and older, 80% have received at least 1 dose, and 64% are fully vaccinated. In terms of full vaccination, 38 million individuals have received the Pfizer-BioNTech vaccine, 32 million have received the Moderna vaccine, and 7.7 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 31.5 million cumulative cases and 565,318 deaths as of 10:15am EDT on April 16.
J&J-JANSSEN VACCINE & BLOOD CLOTTING On April 14, the US CDC’s Advisory Committee on Immunization Practices (ACIP) met to discuss data on blood clotting events—specifically, cerebral venous sinus thrombosis (CVST) with thrombocytopenia—in individuals who recently received the J&J-Janssen SARS-CoV-2 vaccine. ACIP was expected to vote on any updated recommendations in the meeting; however, committee members determined that additional data are needed before deciding on next steps. Reportedly, ACIP aims to hold a follow-up meeting in the next 7-10 days to avoid unnecessary delays in resuming the vaccine’s use. Some of the ACIP members acknowledged that continuing or extending the pause could have negative downstream effects on vaccination efforts, both in the US and around the world.
The US CDC’s recommendation to pause the vaccine’s use remains in place, and the CDC published updated information regarding the blood-clotting events, including symptoms and treatment recommendations. In addition to providing time to assess whether an increased risk of thrombosis is associated with the J&J-Janssen vaccine, it also enables the CDC to disseminate treatment guidance for clinicians, including via the Health Alert Network to public health and healthcare systems nationwide, as these blood clots must be treated differently than many others. Some health experts criticized ACIP for postponing their recommendations, but the CDC, including ACIP, and US FDA are grappling to balance transparency and oversight to ensure vaccine safety with the risk of COVID-19 and the potential effects on vaccine confidence in the J&J-Janssen vaccine specifically, other vaccines utilizing similar vaccine platforms, and SARS-CoV-2 vaccines as a whole.
“BREAKTHROUGH” INFECTIONS During an April 15 hearing of the US House Select Subcommittee on the Coronavirus Crisis, US CDC Director Dr. Rochelle Walensky discussed the agency’s investigation into “breakthrough” infections—ie, infections in individuals who are fully vaccinated against SARS-CoV-2. According to Dr. Walensky, the CDC has identified approximately 5,800 such infections, out of 77 million fully vaccinated individuals*. Among these infections, 396 required hospitalization and 74 died. As has been the case from the beginning of the pandemic, it is more difficult to detect asymptomatic infections. The CDC noted that 29% of the infections detected were asymptomatic, but it is likely that there are more undetected infections. Dr. Walensky did not identify any patterns related to vaccinees’ demographic characteristics or specific vaccines. More than 40% of the infections were among adults aged 60 years and older, but this is not unexpected, considering that adults aged 65 years and older represent 44% of fully vaccinated individuals. The low number of hospitalizations and deaths is encouraging. No vaccine is 100% effective, and this is the first data reported by the CDC on breakthrough infections. The CDC is continuing to monitor vaccine effectiveness, including genomic sequencing to evaluate the effects of emerging variants, and it expects to begin publishing official data starting next week.
*At the time of the report.
VACCINE THIRD DOSE Pfizer CEO Albert Bourla recently said people likely will need to get a third dose of the company’s SARS-CoV-2 vaccine within 12 months of completing their vaccinations. He speculated that annual vaccinations might be required but more research needs to be completed to confirm his predictions. Bourla’s comments were made on April 1 at a CVS Health event but were released April 15. That same day at a US House Select Subcommittee on the Coronavirus Crisis hearing, Chief Science Officer of the White House COVID-19 Response Team Dr. David Kessler noted the emergence of variants of concern will challenge available vaccines’ effectiveness, probably requiring booster shots. However, Dr. Kessler also stated additional research is needed to understand timing and necessity.
RACIAL & ETHNIC DISPARITIES Researchers from the CDC COVID-19 Response Team and colleagues on April 12 posted 2 early release studies in the CDC’s Morbidity and Mortality Weekly Report that further investigate and validate previous findings on racial and ethnic disparities in COVID-19 hospitalizations and emergency room visits. The studies, published in today’s MMWR, provide more data on longstanding systemic inequities in the US health system, which researchers hope will be used to prioritize care for disportionately affected communities moving forward. Additionally, the CDC has launched a Racism and Health page on its Minority Health and Health Equity site, accompanied by a commentary by CDC Director Dr. Rochelle Walensky, to promote education and discussion around racism and health.
In one study, researchers evaluated disparities in COVID-19 hospitalizations by US region from March-December 2020. Age-adjusted COVID-19 proportionate hospitalization ratios (aPHRs) were calculated from administrative discharge data and found that the cumulative aPHR was highest (range 2.7-3.9) among Hispanic and Latino patients across the four US census regions. Disparities were largest from May to July in 2020, and while they became less pronounced through the end of the year, they remained in all regions by December 2020. The other study used National Syndromic Surveillance Program data to evaluate emergency department visits in 13 states from October-December 2020. According to the data, when compared with White persons, Hispanic and American Indian or Alaska Native persons experienced 1.7 times the rate of emergency department visits during the study period and Black persons experienced 1.4 times the rate.
VACCINE ACCESS FOR IMMIGRANTS According to the US government, every person in the country can receive a SARS-CoV-2 vaccination regardless of immigration status. However, the registration process varies among states and clinics, with some requesting proof of residency, official identification, or insurance card. Because of these policies, often expressed in English, immigrants have been discouraged or turned away from pharmacies and other places offering vaccines, exacerbating racial and ethnic divides in vaccination access. A recent analysis by the Kaiser Family Foundation showed only about one-quarter of state websites explicitly note that undocumented immigrants are eligible for vaccinations and that getting a vaccine will not negatively impact immigration status. Advocates insist reaching immigrant populations requires holding vaccine clinics in places they trust, including churches, cultural centers, and advocacy organizations. Some experts have called on the US CDC to issue clear guidance noting that lack of documentation should not be a reason to deny a person vaccination.
US AND GAVI HOST COVAX EVENT The US government and Gavi, the Vaccine Alliance, on April 15 hosted the “One World Protected” event to take stock of global progress toward equitable access to SARS-CoV-2 vaccines and launch a campaign seeking to raise an additional US$2 billion for such efforts through the COVAX facility. The funding will be allocated to the facility’s Advance Market Commitment (AMC), which expects to use the additional funding to reach 30%, instead of 20%, of target populations in 92 lower-income countries this year. At the event, a variety of countries, private sector partners, and foundations announced new pledges totaling nearly US$400 million. In addition to new funding pledges, the first commitments to vaccine dose sharing were announced. New Zealand said it will donate more than 1.6 million doses of SARS-CoV-2 vaccines to COVAX, with a focus on the Pacific region. At the virtual event, US Secretary of State Antony Blinken called on nations to support vaccine manufacturing but did not propose specific policies nor address the issue of surplus vaccine supply in the US.
A paper from Duke University published on April 15 estimates the US will have at least 300 million excess vaccine doses by the end of July and argues US leadership is “imperative” to achieve equitable global access. The paper proposes a 3-part US-led effort to increase and leverage funding through COVAX to improve vaccine access; undertake bilateral and multilateral actions to provide excess doses to countries in need; and increase manufacturing and distribution capacities. Another proposal from the Center for Strategic & International Studies’ (CSIS) Global Health Policy Center lays out a 4-part US diplomatic strategy for shrinking the global vaccine access gap. The CSIS plan focuses on the US helping to bring greater predictability, transparency, and investment partnerships to the vaccine marketplace; expand global supply through various funding, sharing, and manufacturing efforts; build local capacity for vaccine manufacturing, distribution, and administration; and boost demand for and confidence in SARS-CoV-2 vaccines worldwide. On April 14, the People’s Vaccine Alliance released an open letter signed by more than 100 former heads of state and Nobel laureates calling on the US government to support a waiver of intellectual property rights for SARS-CoV-2 vaccines to help expand global vaccine manufacturing.
MERCK ANTIVIRAL TRIALS Merck announced April 15 that it will end a clinical trial of its antiviral molnupiravir in hospitalized COVID-19 patients but will continue testing the treatment among outpatients with the disease. Additionally, Merck said it is discontinuing development of MK-7110 for the treatment of hospitalized COVID-19 patients. In a statement, the company said it plans to focus its pandemic efforts on advancing molnupiravir and manufacturing J&J-Janssen’s SARS-CoV-2 vaccine.
B.1.1.7 CLINICAL DATA In an article published April 12 in The Lancet Infectious Diseases, researchers from University College London and colleagues outline new clinical data of patients who contracted the B.1.1.7 SARS-CoV-2 variant. The study used a cohort design to assess if individuals hospitalized with B.1.1.7 infection experienced with worse disease outcomes. Researchers sequenced and analyzed samples positive for SARS-CoV-2 from patients admitted to two British hospitals between November 9, 2020 and December 20, 2020, and used the WHO’s ordinal scale for severe disease as their outcome measure. The final set of study participants included 198 patients who contracted the B.1.1.7 SARS-CoV-2 variant and 143 who contracted a non-B.1.1.7 variant. The research team found no evidence for a higher risk of severe disease among those who had contracted the variant in both adjusted and unadjusted models. The researchers did see that patients with the B.1.1.7 variants presented with higher viral load levels than their non-B.1.1.7 counterparts, implying that those with the B.1.1.7 variant could be more infectious. While this research presents valuable findings, additional research will continue to be compiled to further analyze the relationship between emerging SARS-CoV-2 variants and disease outcomes.
DISEASE SEVERITY IN CHILDREN Researchers from the US CDC and US Public Health Service published a cohort study in JAMA Network Open estimating adjusted associations between demographic and clinical characteristics and severe COVID-19 among hospitalized pediatric patients using data from more than 20,000 patients ages 18 or younger. Of the 20,714 patients included in the study, 10,950 were female (52.9%), 11,153 were aged 12-18 years (53.8%), 8,148 were Hispanic (39.3%), and 5,054 were non-Hispanic Black individuals (24.4%). Additionally, 6,047 had one or more chronic conditions (29.2%). Among the cohort of 2,430 patients who were hospitalized for COVID-19 (11.7%), nearly one-third of those (756, 31.1%) experienced severe COVID-19. An increased association of severe COVID-19 was seen in patients with one or more chronic conditions versus those with none (AOR 3.27) and in male versus female patients (AOR 1.52). An increased association with severe COVID-19 was also seen in the 2-5 year and 5-11 year age groups when compared to the 12-18 year group (AOR 1.53 for both).
BRAZIL Brazil continues to struggle with increased COVID-19 activity across the country. Earlier this week, the health secretary of Sao Paulo warned that a diminishing supply of critical therapeutics needed to treat COVID-19 patients has put the state’s medical system on the verge of collapse. On April 14, Science published a paper from a group of researchers taking a closer look at the spread of SARS-CoV-2 through the country’s different geographic regions. The group concludes that there is no singular explanation for the virus’s spread across the country, rather a set of reinforcing factors have led to devastating health outcomes. These factors include the country’s expansive size, large gaps in equity of resources, the density of urban populations, the political response to the pandemic, and a lack of early detection. The researchers warn that without improved risk mitigation strategies, the current surge in cases and deaths and the circulation of variants of concern will further increase the country’s COVID-19 burden.
AUSTRALIA TRAVEL RESTRICTIONS Under Australia’s COVID-19 travel restrictions, Australian citizens do not necessarily have the right to return home, ostensibly “stranding” tens of thousands of Australians overseas. The UN Human Rights Commission (UNHRC) is scheduled to hear a case filed by 2 such individuals, who argue that Australia is violating the International Covenant on Civil and Political Rights by not allowing them to return. Both individuals reportedly already have been vaccinated and are willing to undergo the mandatory quarantine period. Australia currently has a quota for returning Australians, due in part to limitations on space available for mandatory quarantine. While the UNHRC has agreed to hear the case, Australia has 8 months to respond, indicating there may not be resolution anytime soon.
Reportedly, Australia is considering steps to ease its international travel restrictions, including allowing vaccinated individuals to travel overseas, although they may still be required to undergo quarantine upon their return. On April 19, Australia and New Zealand are scheduled to officially implement a “travel bubble,” which will allow travelers to move relatively freely between the 2 countries. Travelers will still be required to wear masks during their flights; however, if they show proof of a negative SARS-CoV-2 test or vaccination, they will not be required to undergo quarantine upon their arrival.
MASK-WEARING POLICIES In a paper published April 14 in PLOS ONE, researchers from the Boston University School of Public Health examine mask-wearing policies and adherence in association with COVID-19 case rates across the United States. The research team collected data on mask wearing and physical distance policies, mask adherence, COVID-19 cases, and demographics from publicly available resources. According to the data, none of the 8 states with at least 75% reported mask adherence experienced a high COVID-19 rate. However, states with the lowest levels of reported mask adherence were most likely to have high COVID-19 rates in the subsequent month, independent of mask policy or demographic factors. The researchers conclude that their findings reinforce the importance of mask-wearing policies, and adherence to such policies, in association with reduced COVID-19 incidence.
dryrunguy wrote: ↑Fri Apr 16, 2021 6:56 pm
Here's the latest Situation Report. Haven't read it.
...
“BREAKTHROUGH” INFECTIONS During an April 15 hearing of the US House Select Subcommittee on the Coronavirus Crisis, US CDC Director Dr. Rochelle Walensky discussed the agency’s investigation into “breakthrough” infections—ie, infections in individuals who are fully vaccinated against SARS-CoV-2. According to Dr. Walensky, the CDC has identified approximately 5,800 such infections, out of 77 million fully vaccinated individuals*. Among these infections, 396 required hospitalization and 74 died. As has been the case from the beginning of the pandemic, it is more difficult to detect asymptomatic infections. The CDC noted that 29% of the infections detected were asymptomatic, but it is likely that there are more undetected infections. Dr. Walensky did not identify any patterns related to vaccinees’ demographic characteristics or specific vaccines. More than 40% of the infections were among adults aged 60 years and older, but this is not unexpected, considering that adults aged 65 years and older represent 44% of fully vaccinated individuals. The low number of hospitalizations and deaths is encouraging. No vaccine is 100% effective, and this is the first data reported by the CDC on breakthrough infections. The CDC is continuing to monitor vaccine effectiveness, including genomic sequencing to evaluate the effects of emerging variants, and it expects to begin publishing official data starting next week.
...
VACCINE THIRD DOSE Pfizer CEO Albert Bourla recently said people likely will need to get a third dose of the company’s SARS-CoV-2 vaccine within 12 months of completing their vaccinations. He speculated that annual vaccinations might be required but more research needs to be completed to confirm his predictions. Bourla’s comments were made on April 1 at a CVS Health event but were released April 15. That same day at a US House Select Subcommittee on the Coronavirus Crisis hearing, Chief Science Officer of the White House COVID-19 Response Team Dr. David Kessler noted the emergence of variants of concern will challenge available vaccines’ effectiveness, probably requiring booster shots. However, Dr. Kessler also stated additional research is needed to understand timing and necessity.
74 people have died out of 77 million vaccinated. The math seems simple.
And a third shot: sure, let's do that. See if we can get rid of this thing in a couple of years.
by mmmm8 I mean, we knew efficacy was in the low-mid 90%... This actually suggests efficacy is 99.993%, although I'm sure this percentage will go down a bit as time passes.
by JazzNU
Suliso wrote: ↑Fri Apr 16, 2021 6:46 pm
Just random from Twitter
From Twitter, but originally posted to Instagram. Also, we're doomed from covid or something else because people are freaking idiots.
by ponchi101
mmmm8 wrote: ↑Fri Apr 16, 2021 8:43 pm
I mean, we knew efficacy was in the low-mid 90%... This actually suggests efficacy is 99.993%, although I'm sure this percentage will go down a bit as time passes.
Not necessarily. The bulk of the people vaccinated are elderly. If we start vaccinating young people soon, they will even improve this figure.
What I read about this is that this virus is eradicable. If we get the majority of people to get vaccinated, AND we go a couple of rounds (booster shots) at this rate of vaccination the virus could be wiped out, barring mutations.
by Suliso
From NYT
by Suliso Is the vaccine freely available for everyone in all states in US from tomorrow as was promised?
by dave g
Suliso wrote: ↑Sun Apr 18, 2021 12:04 pm
Is the vaccine freely available for everyone in all states in US from tomorrow as was promised?
In my area, that started about 2 weeks ago.
by ponchi101 My niece, in GA, had her second shot on Thursday. She asked specifically about our situation and was told that all we would need to do would be show our passports, as a form of ID. They told her they have plenty of vaccines and she reports that, the whole time she was there (she is highly allergic to everything, so she was kept the extra 1/2 hour) there were some people but nothing like a crowd.
Only "issue": they have MODERNA, which calls for a second shot at 28 days. So the stay would have to be long.
In Colorado, all our friends have bene vaccinated, even their children. So it seems Uncle joe delivered on his promise.
by MJ2004 I'm happy to report that I just got my appointment for ten days from now, for Pfizer 1.
by atlpam
ponchi101 wrote: ↑Sun Apr 18, 2021 3:51 pm
My niece, in GA, had her second shot on Thursday. She asked specifically about our situation and was told that all we would need to do would be show our passports, as a form of ID. They told her they have plenty of vaccines and she reports that, the whole time she was there (she is highly allergic to everything, so she was kept the extra 1/2 hour) there were some people but nothing like a crowd.
Only "issue": they have MODERNA, which calls for a second shot at 28 days. So the stay would have to be long.
In Colorado, all our friends have bene vaccinated, even their children. So it seems Uncle joe delivered on his promise.
The state mass vaccination sites in Georgia having been giving Pfizer.
by ponchi101 She did go to a private health provider, as she works in a University and that is her supplier.
When I finally decide to go I will look into the state sites. Specially one that has J&J, if possible.
by ti-amie This really is a thing. Ask someone which vaccine they got and if they got Pfizer the nose goes in the air and an expression of moral superiority appears on their face before they even answer you.
by ti-amie I get my second Pfizer shot on Tuesday April 20.
by Togtdyalttai
ti-amie wrote: ↑Sun Apr 18, 2021 8:43 pm
This really is a thing. Ask someone which vaccine they got and if they got Pfizer the nose goes in the air and an expression of moral superiority appears on their face before they even answer you.
I can't believe that exists. I would have happily gotten Pfizer (or J&J for that matter), but a small part of me is happy to have gotten Moderna because it's a small company, as opposed to a pharma giant.
by atlpam Lots of anecdotal info around side effects being worse with Moderna, but from people I know, there hasn’t been much difference. My husband had Moderna; I had Pfizer. We didn’t choose - it was what was available when/where we were able to schedule.
by JazzNU
ponchi101 wrote: ↑Sun Apr 18, 2021 3:51 pm
My niece, in GA, had her second shot on Thursday. She asked specifically about our situation and was told that all we would need to do would be show our passports, as a form of ID.
That's great, looser than other places that I know of. Early on, I have a friend of a friend who flew here to get their vaccine from another state. Took their parents electricity bill and their passport and were able to get the vaccine. But they needed something with an address on it.
by JazzNU
atlpam wrote: ↑Mon Apr 19, 2021 12:34 am
Lots of anecdotal info around side effects being worse with Moderna, but from people I know, there hasn’t been much difference. My husband had Moderna; I had Pfizer. We didn’t choose - it was what was available when/where we were able to schedule.
Though not apples to apples, Moderna is over 3x as strong as Pfizer, so not surprising that the side effects may be a bit more frequent or severe. Only time will tell if there's an advantage of it being stronger dosage, such as the Moderna potentially giving a longer window of protection than the Pfizer.
Personally, from what I've seen in the news and on social media, I've never seen so much whining about mild symptoms that disappear in 2 days in my life. You'd think people were at the hospital getting pumped full of IV medicine for the amount you hear about these side effects yet every story ends with "I was feeling fine after a few days."
by dryrunguy There's also this weird "pity brag" thing happening. "Yes, I did the socially responsible thing and got the vaccine, but oh, the suffering, the suffering!"
That said, the complaining has been frequent enough that the two people living in this house are already planning to get their vaccines at separate times--just in case one or both of us is laid up, at least we will be laid up at different times. And one of us will be able to keep things going (feeding critters, cooking, laundry, etc.) on the other's behalf for a day or two if necessary.
by atlpam I took the day off after my second dose (because I could), but the headache and low fever I experienced would not have prevented me from working from home that day. A good friend's daughter ran a pretty high fever after her second Moderna. It was good that she had decided to spend the night with her Mom rather than being alone at her apartment, so scheduling at separate times, just in case, probably makes sense.
by Suliso It seems to be very individual. A friend in Virginia (35, no health risks) got her first dose (Moderna) few weeks ago and reported virtually no side effects at all and went back to work the same day.
by atlpam
Suliso wrote: ↑Mon Apr 19, 2021 5:23 pm
It seems to be very individual. A friend in Virginia (35, no health risks) got her first dose (Moderna) few weeks ago and reported virtually no side effects at all and went back to work the same day.
Most people have no effects to the first dose. The side effects are usually associated with the second dose. I went hiking after my first dose
by JazzNU Yeah, I don't think there's any rhyme or reason to who has side effects and who doesn't. My sister and brother-in-law are not high risk like I am and both of them were laid up and running fevers while I barely had much more than some extended arm pain and headaches (that could be completely unrelated since I have migraines).
I think staggering the vaccines are a great idea for those that can. Not everyone is able to since, for instance, they might need to take off work at the same time, or traveling the distance to get the vaccine needs to be done at once, especially since it requires two trips. But if you can, yeah, it's a great idea as is taking the next day off when possible.
by JazzNU
by JazzNU Kiwis and Aussies can now travel back and forth. No testing or proof of vaccination required.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 141.5 million cases and 3.0 million deaths as of 4:30am EDT on April 20. Global weekly incidence and mortality continue to increase. Last week, the WHO reported a new record high for weekly incidence, with 5.23 million new cases, a 14% increase over the previous week. Weekly incidence has increased for 8 consecutive weeks, and it appears to be accelerating. Global weekly mortality has increased for 5 consecutive weeks, up to 83,021 deaths, a 7.6% increase over the previous week and the highest weekly total since early February.
The global surge is largely driven by the epidemic in India, which continues to set new national records. On April 17, India became the second country to exceed 200,000 new cases per day, after the US. India is currently reporting 233,074 new cases per day, and its epidemic continues to accelerate. If it continues on this trajectory, India could surpass 250,000 new cases per day and set a new global record in the next 1-2 days. India set its national single-day incidence record on April 18, with 273,802 new cases before falling slightly to 259,167. India is #2 globally in terms of total daily mortality, with 1,353 deaths per day, and still accelerating rapidly. India is reporting fewer than half the daily mortality of #1 Brazil (2,866), but on this trajectory, it could close that gap quickly.
Turkey continues to exhibit a concerning surge as well. At 60,003 new cases per day, Turkey is now within 11% of the US (#2; 67,122) in terms of total daily incidence. Turkey’s COVID-19 surge appears as though it could be starting to level off, but it could potentially approach Brazil or the US in the near future.
Global Vaccination
The WHO reported 843 million vaccine doses administered globally as of April 20, including 450 million individuals with at least 1 dose. The WHO dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports 920 million doses administered globally. The global cumulative total continues to increase at a rate of approximately 18% per week. The daily average has declined for 5 consecutive days, down from 18.6 million doses per day on April 14 to 15.6 million on April 19. At least 185 countries and territories* are reporting vaccination data.
*Out of 191 reporting COVID-19 incidence data.
UNITED STATES
The US CDC reported 31.5 million cumulative cases and 564,292 deaths. Daily incidence has decreased slightly over the past several days—down from 69,953 new cases per day on April 13 to 66,747 on April 18. The daily incidence is still elevated compared to several weeks ago. Daily mortality is slightly elevated compared to last week, but it has held relatively steady at approximately 700 deaths per day since April 12, approximately equal to the low reported immediately prior to the autumn/winter 2020 surge.
Michigan appears to have passed a peak in terms of daily incidence, but some inconsistencies in its recent reporting make it difficult to determine if this is the beginning of a longer-term trend. Michigan does not typically report COVID-19 data to the CDC on Sundays (or holidays), but last week—on Sunday, April 11—it reported 4,837 new cases.
US Vaccination
The US has distributed 265 million doses of SARS-CoV-2 vaccine and administered 211 million doses. Daily doses administered* remains steady at approximately 3 million, including 1.6 million people fully vaccinated.
More than half of all adults have received at least one dose of SARS-CoV-2 vaccine, and one-third are fully vaccinated. A total of 132 million individuals have received at least 1 dose of the vaccine, equivalent to 40% of the entire US population and 51% of all adults. Of those, 85 million (26% of the total population; 33% of adults) are fully vaccinated. Among adults aged 65 years and older, 80% have received at least 1 dose, and 65% are fully vaccinated. In terms of full vaccination, 42 million individuals have received the Pfizer-BioNTech vaccine, 35 million have received the Moderna vaccine, and 7.9 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
In light of the US surpassing 50% coverage in terms of adults with at least 1 dose of SARS-CoV-2 vaccine, we will look at the partial coverage (i.e., 1 or more doses) at the state level**. New Hampshire stands out among all states, leading in terms of partial coverage among both all adults and adults aged 65 and older. In fact, New Hampshire is reporting at least 1 dose for 99.9% of its older adults. And its 71.2% partial coverage among all adults is nearly 10 percentage points higher than #2 New Mexico (61.5%). New Hampshire’s success is likely a factor in the state’s decision to open vaccination to non-residents starting April 19, the same day that the few remaining US states expanded eligibility to everyone aged 16 years and older.
Four other states are reporting partial coverage greater than 60% among all adults: New Mexico (61.2%), Connecticut (61.2%), Maine (60.3%), and Massachusetts (60.2%). The median is slightly higher than 50%, and most states fall between approximately 46% and 54%. Alabama (38.7%) and Mississippi (38.2%) are the only states reporting less than 40% partial coverage among all adults. Impressively, the median coverage among adults aged 65 years and older is nearly 80%, with most states falling between 75-85%. In addition to New Hampshire, Vermont (93.6%) is reporting partial coverage greater than 90% among older adults. Hawai’i (69.3%) and West Virginia (69.5%) are the only 2 states reporting less than 70% coverage among older adults.
Most of the states that fall in the top and bottom 10 in both partial and full coverage. In fact, 7 states appear in the top 10 of both lists, and 8 appear in the bottom 10 of both lists. However, Hawai’i ranks #25 for partial coverage among all adults (50.1%), but it falls all the way to #50 among adults aged 65 years and older (69.3%). Kansas falls from #9 in terms of partial coverage among older adults (86.5%) to #21 among all adults (52.5%). Both New Mexico and New Jersey rank in the top 10 for all adults but fall 12 places for older adults. New Mexico ranks #2 in terms coverage among all adults (61.5%) and #14 (84.3%) among older adults, and New Jersey falls from #6 among all adults (58.8%) to #18 for older adults (82.3%).
**By state of residence, even if individuals received the vaccination in another state.
ROUTES OF TRANSMISSION Scientific evidence increasingly supports the theory that the primary mode of SARS-CoV-2 transmission is through airborne infectious aerosols passed from person-to-person, according to some researchers. In three separate pieces published last week, experts outlined reasoning and evidence supporting SARS-CoV-2 transmission from both near-field and far-field aerosols. In a commentary published April 15 in The Lancet, researchers from the UK, US, and Canada present 10 reasons backing airborne transmission. In another piece published online in JAMA on April 16, experts from Harvard University and the University of Michigan describe the rationale for improving air circulation and filtration in indoor spaces to reduce far-field transmission of SARS-CoV-2 and other respiratory infectious diseases. While noting that airborne viral particles are a significant route of SARS-CoV-2 transmission and calling for improved air ventilation in indoor spaces, experts from the UK, US, and China in an editorial published April 14 in The BMJ also underline the significance of mask quality and fit.
These pieces appeal to the public health community to take action to help improve indoor air quality, ventilation, and filtration, through policy and structural changes, particularly in healthcare, work, and educational settings. Such efforts could help reduce the number of COVID-19 cases as well as other airborne infectious diseases. The commentaries could be viewed as rebuttal to a systematic review funded by the WHO and published last month that says there is inconclusive evidence for airborne transmission. On April 19, a US CDC official said during a telephone briefing that the CDC has determined the risk of SARS-CoV-2 transmission via surfaces is low and secondary to transmission through direct contact with droplets and aerosolized particles. In light of the evidence, the CDC has updated its guidance for cleaning and disinfecting surfaces in community settings.
EMERGING VARIANT RESPONSE FUNDING The US government on April 16 announced it will invest US$1.7 billion from the American Rescue Plan to help states and local jurisdictions detect, monitor, and mitigate emerging variants of SARS-CoV-2. A White House fact sheet says that an essential component of these efforts is increasing genomic sequencing, especially in states experiencing surges of cases. According to the US CDC, the B.1.1.7 variant is now the dominant strain in the US, and several states have seen recent increases in cases due to the variant. The US government is committing US$1 billion of the total allocation to the CDC, states, and localities to bolster surveillance. Of the remaining funds, US$400 million will help create 6 new Centers of Excellence in Genomic Sequencing across the nation. These centers will work in partnership with state health departments and academic institutions to develop new concepts, methods, and technologies for genomic surveillance tools. Additionally, US$300 million will go toward developing and supporting a National Bioinformatics Infrastructure to help scientists track the spread of diseases and allow for improved decision-making. The fact sheet outlines funding distribution by state, noting the first tranche will be distributed in May with a second tranche expected to be invested over the next several years.
INDIA & BANGLADESH The city of Delhi, India initiated a weeklong lockdown on April 19 in an effort to stem a severe surge in cases. On Sunday, the city reported a record single-day case count, with 24,642 cases. As a result of the increasing number of cases, city hospitals have reported near-full ICU capacity and critical shortages of oxygen and drugs. Crematoriums also report being overburdened. During the lockdown, casual gatherings will be prohibited and non-essential businesses will be ordered to close, although essential services will be allowed to remain open. Weddings and funerals will be allowed to continue, albeit with capacity restrictions. Sporting events without spectators will be permitted to continue. Public transport will be reduced to 50% seating capacity. The city lockdown is scheduled to lift the morning of April 26. Various factors may be fueling this rise in cases in India, including recent mass gatherings, as well as a new variant of interest, B.1.617. In addition to the restrictions in Delhi, new mitigation measures have been implemented in localities in the states of Uttar Pradesh and Maharashtra.
Bangladesh enacted a similar but more restrictive lockdown on April 5, with the closure of shops and offices and the cessation of domestic transportation and international flights. Citizens have been asked not to leave their residences from 6pm-6am. Restrictions were expected to lift on April 22, but they have been extended an additional week. Several senior government officials indicated that the extended lockdown will be enforced more strictly, which could further exacerbate financial impacts on lower-income individuals. Reportedly, the government is considering easing some of the restrictions before the Eid holiday.
BREAKTHROUGH INFECTIONS With vaccination rates continuing to climb in the United States, many who are vaccinated are beginning to engage in more activities that could increase their exposure to SARS-CoV-2 infection. While the vaccines available under US FDA Emergency Use Authorizations are effective, there is still a chance that vaccinated persons can become infected with SARS-CoV-2. These “breakthrough” infections are considered rare events, with the CDC on April 19 reporting fewer than 6,000 cases out of 84 million vaccinated persons. The agency continues to monitor reports of breakthrough cases and launched a website with information for public health departments and laboratories to investigate and report such cases. The agency is monitoring the age, sex, type of vaccine, and underlying conditions from breakthrough cases, but no pattern among cases has been identified. When possible, monitoring also includes genomic sequencing to identify which virus lineage caused the infection.
US VACCINE ELIGIBILITY As of April 19, all US states have expanded COVID-19 vaccine eligibility to include all individuals aged 16 years and older, meeting the goal set by the US government to expand vaccine eligibility to all adults by April 19. Hawai’i, Massachusetts, New Jersey, Oregon, Rhode Island, and Vermont were the last states to meet the deadline yesterday.
AT-HOME TEST KITS On April 19, Abbott announced that its BinaxNOW rapid antigen at-home test kit is available for purchase in the US. The test is available without a prescription and provides results in approximately 15 minutes. Initially, the test kits will be available through national chain pharmacies, including CVS, Walgreens, and Walmart. At less than US$25 per kit—which includes 2 tests—they are likely still too expensive for routine daily testing. Over-the-counter (i.e., non-prescription) test kits provide a widely accessible at-home test that can be kept on hand or potentially obtained quickly for a variety of purposes, such as after an exposure to a known COVID-19 case or prior to travel. Abbott’s announcement indicates that it aims to produce “tens of millions” of tests per month, with the potential to increase capacity beyond that point, if necessary. The test kit received an Emergency Use Authorization from the US FDA in March 2021 for use in both symptomatic and asymptomatic individuals as young as 2 years old.
VACCINE DISINFORMATION Researchers are launching projects to catalogue and counteract misinformation and disinformation about SARS-CoV-2 vaccines on social media, as well as collect data on how that information spreads and influences vaccination uptake. One research consortium, called the Virality Project and started by experts from multiple US academic institutions, is using strategies learned during the 2020 US presidential election to help social media platforms counter vaccine mis- and disinformation. Earlier this year, Facebook and Twitter announced new policies aimed at stemming the spread of misinformation. The companies will remove offending posts and shut down accounts that perpetually post false information about vaccines. However, social media platforms increasingly are running up against “gray area misinformation,” or posts that do not contain explicitly false information but present only select facts that drive commentary meant to further misleading narratives. A researcher from the nonprofit First Draft News alleged that many of the same people who pushed misleading information via social media during the 2020 election also are peddling misinformation about vaccines and the COVID-19 pandemic.
US EXCESS DEATHS Researchers at the US CDC’s National Center for Health Statistics published a brief overview of excess deaths in the US since the start of the US COVID-19 epidemic. The study, published in the US CDC’s MMWR, analyzed mortality data from the National Vital Statistics System (NVSS), corresponding to deaths from 2013 through February 2021. Between January 26, 2020—the date of the first reported COVID-19 death in the US—through February 27, 2021, the researchers estimate 545,600-660,200 excess deaths above what would be expected during that period based on historical data. During that time, approximately 75-88% of the excess deaths were directly attributable to COVID-19, leaving 63,700-162,400 additional excess deaths. These additional deaths could potentially be directly attributable to COVID-19 (i.e., undiagnosed victims), or they could result from the downstream effects of the pandemic beyond the disease itself, including “disruptions in health care access or utilization.”
US FDA REVOKES BAMLANIVIMAB EUA On April 16, the US FDA terminated the Emergency Use Authorization for Eli Lilly’s investigational monoclonal antibody bamlanivimab as a treatment for COVID-19. Specifically, the agency terminated the EUA that authorized bamlanivimab as a treatment “when administered alone”*. Analysis of available clinical data found a “sustained increase of SARS-CoV-2 viral variants that are resistant” to the drug and “increased risk for treatment failure.” Bamlanivimab remains authorized for use in combination with etesevimab, another of Eli Lilly’s monoclonal antibodies. Notably, the FDA’s decision came at the request of Eli Lilly, but a press release from the company indicates that it does not currently intend to request the withdrawal of emergency authorization for bamlanivimab as a standalone treatment in any other country.
*Emphasis in original source.
TRIAL EXAMINING REPURPOSED DRUGS The US NIH on April 19 announced it is launching a large randomized, placebo-controlled clinical trial to test whether several existing prescription and over-the-counter medications can help resolve mild-to-moderate symptoms among people with COVID-19. The Phase 3 trial, part of the Accelerating COVID 19 Therapeutic Interventions and Vaccines (ACTIV) public-private partnership, will explore up to 7 drugs approved by the US FDA for other conditions, a strategy called drug repurposing. According to the Washington Post, which quotes anonymous sources, several of the drugs under consideration for the trial include the antiparasitic ivermectin, the antidepressant fluvoxamine, and the acid-controller famotidine, the generic name for Pepcid. At least one study published in the March 4 JAMA showed that early administration of ivermectin did not significantly shorten the time to symptom resolution among nearly 400 adults with mild COVID-19 randomized to take ivermectin or placebo. As for fluvoxamine, 2 small studies, one published in JAMA and the other in Open Forum Infectious Diseases, showed the serotonin reuptake inhibitor helped reduce disease progression among those who took the drug compared with people who took a placebo or refused the drug. At least 3 other clinical trials are currently recruiting to test fluvoxamine, according to ClinicalTrials.gov, and a recent episode of 60 Minutes highlighted the drug’s potential as a COVID-19 treatment.
SUBUNIT VACCINE On April 19, Nature published an early-version manuscript describing research into a subunit SARS-CoV-2 vaccine that researchers hope will provide protective immunity against the virus. Subunit vaccines are widely used and highly effective against several infectious diseases. Researchers from various US-based institutions and the pharmaceutical company GSK showed positive results that a SARS-CoV-2 spike receptor binding domain on a protein nanoparticle (RBD-NP) can offer protection against the virus in non-human primates. The researchers evaluated 5 different adjuvants, showing variation in efficacy against SARS-Cov-2 variants and wild-type virus. With these promising results of an adjuvanted RBD-NP vaccine candidate among primates, the authors report the vaccine will move to Phase 1/2 human trials. A successful adjuvanted subunit vaccine potentially could help fill vaccination gaps in younger and older populations, as other such vaccines historically have good safety profiles in these groups.
by ponchi101 Not only I never had an album of his, I really can't recall ever hearing a single song from this man.
One thing that is impressive of these people (the Tiny acolytes) is their use of the phrase, or a variation of the phrase, "nobody knows ...". This idiot says "nobody knows what is in the vaccine". Heck, a simple search will let you find out everything about the vaccine.
I can't be graceful with this guy. I hope covid takes out his vocal cords, so he won't be able to speak any more nonsense.
by MJ2004 Many years ago when I was still on FB, I unfriended an old friend because she posted a video of this a**. Haven't heard from her since. Don't regret it.
by ti-amie
by JazzNU Poor India. Was genuinely hoping no country would ever come close to passing any of the US' pitiful covid milestones. Double mutant variant is no joke.
by Suliso Yes, but there was also a lot of arrogance both from the government and population in general which led to this. We are special, more used to microbes and pollution etc., pandemic almost over so lets open everything and have hundreds of thousands gather for religious ceremonies. Well, not so special after all...
by Suliso It's very likely that Brazil will pass US fatality numbers as well without even considering all the undercounting...
by ti-amie
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 144.1 million cases and 3.1 million deaths worldwide as of 5:45am EDT on April 23.
On April 21, India surpassed 250,000 new cases per day and set a new global record for total daily incidence. India is currently reporting 281,683 new cases per day and still increasing rapidly. On this trajectory, India could surpass 300,000 new cases per day in the next 1-2 days. On April 21, India became only the second country to report more than 300,000 new cases in a single day, after the US. India has reported more than 300,000 new cases on 2 consecutive days, including a record high 332,921 new cases on April 22.
The global daily incidence is already setting new records, and daily mortality is on track to surpass its previous high as well. While the global trends in daily incidence are largely driven by India’s ongoing surge, this is slightly less the case for mortality. Currently, South America accounts for nearly one-third of the global daily mortality, more than any other continent; however, it appears to have leveled off over the past week or so. Asia recently surpassed Europe as #2 globally, and both are reporting essentially equal daily mortality—each accounting for more than a quarter of the global total. Asia’s daily mortality is accelerating rapidly, up by more than 400% since mid-March—driven largely by India—and it could surpass South America as #1 in the coming days. Europe’s daily mortality remains slightly elevated from its most recent low in mid-March, but it has declined over the past several days. Daily mortality in Africa and North America steadily decreased from late January through mid-April; however, both are reporting increases over the past 2 weeks. Oceania averaged fewer than 1 death per day from October 2020 through mid-March 2021, and while its daily mortality is increasing, it is still fewer than 3 deaths per day.
In terms of total daily mortality, Brazil remains #1 globally, with 2,580 deaths per day, but it has decreased steadily since April 12. Brazil’s daily mortality has fluctuated around 2,700-3,000 deaths per day since late March, but this is the largest and longest decline during that period. India is #2 globally, with 1,802 deaths per day and increasing rapidly. On this trajectory, India could surpass Brazil as #1 in the coming days. Daily mortality in the US (#3; 698) and Mexico (#5; 409) have decreased steadily from their highs in mid-to-late January, but both appear to be leveling off. Poland (#4; 506), Colombia (#6; 397), Peru (#7; 399), and Iran (#8; 365) are all reporting steadily increasing trends over the past several weeks. Ukraine (#10; 379) also reported increases over the past several weeks, but it appears to be leveling off. Russia’s daily mortality (#9; 380) has held relatively steady since December 2020.
On a per capita basis, the top countries are all in Europe and South America. In fact, among the top 20 countries in terms of per capita daily mortality, 15 are in Europe, and 5 are in South America. Hungary is #1 globally, with 21.9 daily deaths per million population. Bosnia and Herzegovina (20.1) is the only other country reporting more than 20 daily deaths per million population. At #3, Uruguay (17.9) is the highest ranked South American country. All other countries in the top 10 are reporting more than 10 daily deaths per million, more than 6 times the global average (1.6). The European countries largely exhibit a similar trend. Their daily mortality peaked in December 2020, followed by a steady decline through January/February 2020 and then another steep increase. Most of these countries appear to be at or near another peak, and as noted above, the overall European daily mortality is beginning to decline. Similarly, the South American countries are reporting similar trends. With the exception of Uruguay, the South American countries reported surges with peaks between July and September 2020—Uruguay did not exhibit a major surge in 2020. Brazil and Uruguay reported increasing trends starting in late 2020, and in January 2021 for Peru. All 4 countries began exhibiting a sharp increase in daily mortality between early and late March, and all have far surpassed their previous peaks.
Global Vaccination
The WHO reported 900 million vaccine doses administered globally, including 491 million individuals with at least 1 dose. The WHO dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reports 973 million doses administered globally. This is 13% more than this time last week, slightly lower than the previous growth rate of approximately 18% per week. After 6 consecutive days of declining averages, the daily doses administered rebounded slightly over the past 2 days to 15.6 million. At least 189 countries and territories* are reporting vaccination data.
*Out of 191 reporting COVID-19 incidence data.
UNITED STATES
The US CDC reported 31.7 million cumulative cases and 566,494 deaths. Daily incidence has decreased slightly over the past several days—down from 69,878 new cases per day on April 13 to 62,595 on April 21. The daily incidence fell below the summer 2020 peak, but it is still elevated compared to several weeks ago. Daily mortality continues to hold relatively steady at approximately 700 deaths per day (since April 12), which is approximately equal to the low reported immediately prior to the autumn/winter 2020 surge.
US Vaccination
The US has distributed 282 million doses of SARS-CoV-2 vaccine and administered 219 million doses. Daily doses administered* has decreased over the past several days, down from a high of 3.2 million (April 11) to 2.8 million. The fully vaccinated population is increasing by 1.4 million people per day.
A total of 136 million individuals have received at least 1 dose of the vaccine, equivalent to 41% of the entire US population and 52% of all adults. Of those, 89 million (27% of the total population; 34% of adults) are fully vaccinated. Progress among older adults has slowed considerably. Among adults aged 65 years and older, 81% have received at least 1 dose, and 66% are fully vaccinated. In terms of full vaccination, 44 million individuals have received the Pfizer-BioNTech vaccine, 37 million have received the Moderna vaccine, and 8.0 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 31.9 million cumulative cases and 570,357 deaths as of 9:15am EDT on April 23.
INDIA COVID-19 OXYGEN SHORTAGE As India faces the world’s most severe COVID-19 epidemic, setting new records in terms of daily incidence and mortality, India’s health system is unable to manage the patient surge, and its health system may be nearing collapse. One critical problem is a severe nationwide shortage of oxygen. As we have covered previously, high-flow oxygen therapy has become a key component of COVID-19 patient care, and hospitals in areas with ongoing surges may be unable to produce or procure sufficient supply. Reportedly, hospitals are exhausting their supply or are down to minutes or hours of oxygen on hand, which is contributing to COVID-19 patient deaths, and hospitals are competing against each other to obtain limited resources.
This week, the High Court of Delhi held an emergency hearing to address a complaint filed by one Delhi hospital system alleging that India’s national government was not doing enough to ensure adequate oxygen supply. In response, a representative of the national government indicated that relevant agencies already had made plans to provide 480 metric tons of oxygen to Delhi. Regardless, the court ordered the national government to “ensure strict compliance” with that allocation plan and threatened “criminal action” in the event of non-compliance. Following the original hearing, several additional hospitals filed similar pleas. The court also chastised the government for not prioritizing hospitals over industrial uses to ensure adequate supply. Following the hearing, India’s national government reportedly put oxygen tankers on express trains to transport it to areas of need, and India’s Supreme Court directed the national government to submit its COVID-19 response plans, including for oxygen supply and vaccination.
US TRAVEL ADVISORIES The US Department of State updated its travel advisories, resulting in nearly 80% of countries falling under the “Do Not Travel” category. Previously, the State Department issued Level 4 (Do Not Travel) guidance for only 34 countries, but the recent additions bring the total to more than 150. Among the Level 4 category countries are Austria, Brazil, France, India, Italy, Mexico, Russia, and the UK. The department said the additions were made "to better reflect CDC's science-based Travel Health Notices" as well as to consider the logistics of testing availability and other travel restrictions for US travelers. The department also noted it is continuing to monitor COVID-19 data across the globe and will regularly update destination-specific advice as conditions evolve.
US PUBLIC HEALTH FUNDING US public health officials fear that once the COVID-19 pandemic ends so will state and federal public health emergency funding, pushing them back to patching together budgets from a variety of sources to provide basic, necessary services to their communities. According to the Trust for America’s Health, funding for the Public Health Emergency Preparedness cooperative agreement—which provides critical federal funding to state, local, and territorial public health departments—dropped by about half between fiscal years 2003 and 2021. Since 2010, spending for state public health departments dropped by 16% per capita and spending for local health departments has fallen by 18%, a KHN/Associated Press (AP) analysis published in July 2020 showed. These decreases led to the loss of at least 38,000 public health jobs at the state and local levels between 2008 and 2019. Compounding the problem, at least 248 state and local public health department leaders resigned, retired, or were fired during the COVID-19 pandemic, between April 1, 2020, and March 31, 2021. Experts warn this is the largest exodus of public health leaders in US history.
Years of underfunding have not only impacted staffing as public health departments’ infrastructures are suffering too, with antiquated computer, data collection, and communication systems. Several US Senators have introduced the Public Health Infrastructure Saves Lives Act, which would eventually provide $4.5 billion annually in core public health funding. But in the meantime, some state legislatures have proposed measures to weaken or remove public health powers, according to a KHN/AP investigation from December 2020. If public health departments continue to operate under a boom-or-bust cycle, experts warn they will be forced to operate at a deficit during the current pandemic and be incapable of properly preparing for the next public health disaster.
GLOBAL VACCINE ACCESS On April 22, the New York Times published an opinion piece by WHO Director-General Dr. Tedros Adhanom Ghebreyesus, who called the inequity in global SARS-CoV-2 vaccine distribution “unacceptable.” According to Dr. Tedros, of more than 890 million vaccine doses administered globally, more than 81% have been given in high- and upper-middle-income countries, with low-income nations only receiving 0.3%. To address the problem, Dr. Tedros urged countries and companies that control the global supply of vaccines to share financial support, share extra vaccine doses with the COVAX Facility, and support the massive scale-up of vaccine production and distribution. In order to achieve the latter, he proposed companies use voluntary licensing with technology transfer; share licenses through the COVID-19 Technology Access Pool, started by the WHO last year; or waive intellectual property rights on COVID-19 products, an option that South Africa and India have proposed repeatedly at the World Trade Organization. Dr. Tedros’s commentary echoed calls to action he made last week during an UN Economic and Social Council (ECOSOC) special ministerial meeting titled “A Vaccine for All.” During his opening remarks at the meeting, Dr. Tedros said, “Vaccine equity is the challenge of our time. And we are failing.” Experts warn that the longer it takes to reach vaccine equity worldwide, the longer the pandemic will continue and the higher the risk of variants emerging to which the currently available vaccines provide diminished protection.
HEALTH WORKER STRESS According to a Washington Post-Kaiser Family Foundation poll, approximately 3 in 10 healthcare workers have considered leaving their profession during the COVID-19 pandemic, with those feelings fueled by burnout, trauma, and disillusionment. The poll of 1,327 US frontline healthcare workers, conducted between February 11 and March 7, showed more than half of respondents said they are burned out and about 6 in 10 said pandemic stress has negatively impacted their mental health. Respondents cited a lack of equipment to protect themselves or treat patients, guilt and trauma over patient deaths, or frustration with governments and some in the public for refusing to enforce or take basic risk mitigation precautions. Some noted the pandemic exposed and magnified how ill-equipped the nation’s health system is to deal with public health emergencies. Experts warn the US was facing a shortage of doctors and nurses prior to the pandemic and additional losses to staffing could further harm US health care by making it more expensive, less accessible, and lower in quality.
Healthcare workers’ responses also highlight the importance of addressing mental health to prevent post-traumatic stress, anxiety, depression, substance use, or suicide. Because many healthcare workers suffer in silence, implementing accessible mental health programs becomes even more important. Still, 76% of respondents said they feel “hopeful,” and two-thirds said they remain “optimistic” about going to work. Nearly 6 in 10 said they anticipate the COVID-19 pandemic in the US will be controlled enough by early 2022 or later so people can resume normal life, while nearly half said they hope normal life can resume by mid-fall or sooner—including 5% who believed life can safely resume now.
UK CHALLENGE TRIALS A research team at the University of Oxford (UK) have announced the start of a human challenge trial that will look at what type of immune response is necessary to prevent SARS-CoV-2 reinfection and how the immune system responds during reinfection. The study is designed to include two phases. During the first phase, researchers will determine the lowest dose of SARS-CoV-2 needed to cause active but asymptomatic or low-symptom infection in 50% of participants who have fully recovered from a previous natural infection. In the second phase, scheduled to begin this summer, researchers plan to inject all participants with the “optimal” dose determined in phase one. Notably, the study will use the original strain of the virus. In February, the UK became the first country to approve human challenge trials for SARS-CoV-2, in which volunteers are deliberately exposed to the virus. Some researchers cite the positive impact these controlled trials can have on scientific understanding, while critics question the ethical and practical nature of the method.
NURSING HOME OUTBREAKS Health officials in Kentucky and experts at the US CDC published a case study of an outbreak at a long-term care facility (LTCF) initiated by an unvaccinated employee. At the facility, 90% of the residents and 53% of the staff received 2 doses of SARS-CoV-2 vaccine. Routine testing identified the outbreak, which began in an unvaccinated and symptomatic healthcare worker. Ultimately, the outbreak involved 46 total cases, including 26 residents and 20 facility personnel. Notably, 18 of the residents and 4 personnel received their second dose of the vaccine more than 14 days before the outbreak. Three (3) residents died, including 2 who were unvaccinated.
The risk of infection among unvaccinated residents was 3 times higher than among vaccinated residents. Similarly, the risk among unvaccinated personnel was 4 times higher than among vaccinated personnel. For this outbreak, the vaccine’s effectiveness against SARS-CoV-2 infection was estimated to be 66% among residents and 76% among employees, and the effectiveness against symptomatic COVID-19 disease was 86.5% among residents and 87% among employees. This is in line with the expected effectiveness based on clinical trial efficacy data. The authors conclude that low vaccination coverage among employees at LTCFs could facilitate introduction of SARS-CoV-2, which could result in outbreaks, even among resident populations with high vaccination coverage. While the authorized SARS-CoV-2 vaccines are highly effective*, COVID-19 risk remains, particularly among individuals at elevated risk for exposure and severe disease. Even as vaccination coverage increases, it is critical to maintain COVID-19 risk mitigation measures until sufficient community protection is in place to bring the pandemic under control.
*For those vaccines with publicly available Phase 3 clinical trial data.
VACCINATION & PREGNANCY The New England Journal of Medicine on April 21 published a study of preliminary findings of mRNA SARS-CoV-2 vaccine safety among pregnant people. Researchers from the CDC’s V-safe COVID-19 Pregnancy Registry Team used data from the agency’s V-safe surveillance system, the V-safe pregnancy registry, and the Vaccine Adverse Event Reporting System (VAERS). A total of 35,691 V-safe participants aged 16 to 54 years identified as pregnant. Among those people, injection site pain was reported more frequently than among the nonpregnant population, but headache, muscle aches, chills, and fever were reported less frequently. Of 221 pregnancy-related adverse events reported to the VAERS, the most frequently reported was spontaneous abortion (46 cases). The researchers note that although not directly comparable, the proportions of adverse pregnancy and neonatal outcomes (eg, fetal loss, preterm birth, small size for gestational age, congenital anomalies, and neonatal death) among vaccinated persons who had completed pregnancy were similar to incidences reported in studies of pregnant people conducted prior to the COVID-19 pandemic. The preliminary findings did not show obvious safety signals for pregnant persons receiving mRNA SARS-CoV-2 vaccines, but the researchers noted the need for continued monitoring. The American Society for Reproductive Medicine has encouraged everyone, including pregnant persons and those seeking to become pregnant, to receive a SARS-CoV-2 vaccination.
EMERGENCY DEPARTMENT VISITS The CDC’s Morbidity and Mortality Weekly Report (MMWR) on April 16 published updated data on changes to emergency department (ED) visits during the COVID-19 pandemic. Previously, researchers with the CDC COVID-19 Response Team and colleagues published data collected from the National Syndromic Surveillance Program (NSSP) showing ED visits declined 42% between March 29-April 25, 2020, following the national emergency declaration on March 13, 2020. Although the number of ED visits increased by July 2020, they remained below pre-pandemic levels. The updated data show ED visits were 25% lower during December 2020-January 2021 when compared with the same months from a year prior. The researchers note the reasons for ED visits have changed during the pandemic period when compared to those during the pre-pandemic period, with more people seeking care for mental and behavioral health-related concerns, especially pediatric patients. The researchers emphasize that, although smaller in total number, the increased proportion of visits due to mental and behavioral health complaints in both adult and pediatric groups is a sign of concern and call for public health measures to provide health messaging and resources for managing related symptoms. The impact of COVID-19 on mental health is well noted, and the CDC provides some resources on managing stress during the pandemic.
COUNTERFEIT VACCINES & VACCINATION CARDS Pfizer announced that counterfeit vaccines were seized in Mexico and Poland. Reportedly, approximately 80 people received the counterfeit vaccine in Mexico, at a cost of US$1,000 each—but so far, none of the recipients have reported any physical harm. In Poland, the doses were seized before they could be administered, and the vials are believed to contain an “anti-wrinkle treatment.” Laboratory analysis confirmed that the products contained in the vials were not the Pfizer-BioNTech vaccine. With high demand and limited supply for the SARS-CoV-2 vaccines, these incidents highlight the risk of criminals distributing counterfeit products for profit. Some of these products are being sold online, and Pfizer emphasized that no legitimate SARS-CoV-2 vaccines are sold online. Pharmaceutical companies and law enforcement agencies around the world are collaborating to quickly identify counterfeit vaccines and intervene.
As countries, businesses, schools, and other organizations evaluate options regarding mandatory vaccination, counterfeit vaccination cards also are a growing problem. Individuals who elect not to get vaccinated are seeking counterfeit vaccination cards to serve as documentation for a vaccination that they never received. There also are reports of individuals falsifying documentation of the first dose in order to jump ahead in the queue. Some of the counterfeit cards are truly counterfeit, and others are blank versions of the official vaccination cards, such as those reportedly sold online by a pharmacist in Chicago (US). The US FBI issued a warning about the counterfeit vaccination cards, emphasizing that making or purchasing the cards or filling in a blank card with false information are all illegal. The FBI encouraged the continued use of COVID-19 risk mitigation measures (eg, mask use, physical distancing) to mitigate the risk posed by counterfeit vaccination cards. The National Association of Attorneys General issued a statement calling on social media and e-commerce companies to take immediate action to prevent the sale of fraudulent vaccination cards. Some experts have criticized the use of paper forms to document vaccination status, as opposed to digital documentation, due to the ease of counterfeiting them. Reportedly, the US CDC originally intended to use digital certificates, but technical problems and delays prevented the implementation of a nationwide system in time to begin vaccination efforts.
TOKYO OLYMPICS With only 3 months until the start of the rescheduled Summer Olympics in Japan, Prime Minister Yoshihide Suga today implemented a third state of emergency order for Tokyo and 3 western prefectures—Osaka, Kyoto, and Hyogo. The order, set to last through May 11, is intended to prevent people from traveling and gathering in public spaces during Japan’s “Golden Week” holidays that run from late April through the first week in May. Prime Minister Suga expressed concern over the spread of a SARS-CoV-2 variant, saying more stringent measures are needed to curb the number of new cases. Under the state of emergency, bars, department stores, malls, theme parks, theaters, and museums in the 4 prefectures are ordered to close. Restaurants that do not serve alcohol and public transportation are being asked to close early, and universities should return to online classes, although grade schools will remain open. International Olympic Committee President Thomas Bach is scheduled to visit Japan on May 17-18 to greet the Olympic torch relay in Hiroshima. Bach said the new state of emergency is not related to his planned visit, and an official with the Japan Olympic organizing committee said there is no discussion of cancelling the event, scheduled to begin on July 23.
RECRUITING FOR VACCINATION STUDY The Johns Hopkins COVID-19 Vaccine Risk Uptake study is recruiting in-home healthcare providers to participate in focus groups to discuss motivation, hesitancy, and situational factors that impact awareness, acceptability, and access to vaccines. Interviews will be conducted in focus groups remotely (via Zoom) and will last approximately 90 minutes. If you are interested in participating, or know someone who may be, please contact Jennifer McKneely at (571) 228-1680 or Jennifer.McKneely@jhuapl.edu. Additional information is available here.
by ti-amie Thanks again dry. When I got my second shot Tuesday the person checking me in said to keep the card in a safe place because they're going to become very important.
Fake cards is why mitigation efforts have to continue.
by JazzNU
ti-amie wrote: ↑Fri Apr 23, 2021 9:43 pm
Thanks again dry. When I got my second shot Tuesday the person checking me in said to keep the card in a safe place because they're going to become very important.
Some people are getting their cards laminated. I opted not to do that because of the likelihood we'll need a 3rd or booster shot and I want access to the card to add that next shot. So I got clear vaccine card holders, you slip the card in and there's a closure, but you can still pull it out later on if you need to.
If you go this route, just be aware that CDC cards come in at least two sizes. The petite size will fit into any of the advertised 4x3 holders you can find (Etsy and Amazon have loads of them), but the bigger size, it's a much tighter fit. You might be able to fit it with a little maneuvering (basically slightly bending the top to slip it in, it fits cleanly, but it's a seriously tight fit that way). The only other option I've found thus far s 2 inches larger, so unnecessarily bigger for carrying around all the time, and that is a clear passport holder (go with 4x6).
I didn't touch my vaccine card for the month in between appointments, just stayed in my wallet the entire time. And it definitely was looking less than pristine come the second vaccine appointment. You definitely need something to keep it safe.
by ponchi101 I am scanning that baby, printing it in high quality paper, laminate the scan and keep the original in a zip lock, in my safe.
Of course, if I ever get vaccinated, that is.
by JazzNU I should also add - laminate, holder, etc - that should be in addition to a photo. Keep a photo, front and back, on your phone for easy access. Especially important if you lose it apparently and also especially important if your vaccine provider doesn't provide an electronic record of your vaccine.
by Deuce Why don't they simply implant a microchip in every vaccinated person's earlobe?
That wouldn't get stolen... and no-one would lose it (unless they become a disturbed and obsessed artist).
by ponchi101 Oh, that would certainly not bother the Q-Anon people, and the billions of other paranoids, one bit
(And I am a paranoid, so I should know )
by dryrunguy A microchip would be The Mark of the Beast.
by Suliso Heard from my Indian friends that Modi's government has basically said any vaccination is now up to States and they can manufacture or import whatever they want. He's not going to do anything. This will go great...
by Suliso A friend's brother, an engineer living in Bangalore, is saying that everything has been closed down except stores of a company connected to government. Difficult life now, nowhere to go except for food and only working online...
ti-amie wrote: ↑Fri Apr 23, 2021 9:43 pm
Thanks again dry. When I got my second shot Tuesday the person checking me in said to keep the card in a safe place because they're going to become very important.
Some people are getting their cards laminated. I opted not to do that because of the likelihood we'll need a 3rd or booster shot and I want access to the card to add that next shot. So I got clear vaccine card holders, you slip the card in and there's a closure, but you can still pull it out later on if you need to.
If you go this route, just be aware that CDC cards come in at least two sizes. The petite size will fit into any of the advertised 4x3 holders you can find (Etsy and Amazon have loads of them), but the bigger size, it's a much tighter fit. You might be able to fit it with a little maneuvering (basically slightly bending the top to slip it in, it fits cleanly, but it's a seriously tight fit that way). The only other option I've found thus far s 2 inches larger, so unnecessarily bigger for carrying around all the time, and that is a clear passport holder (go with 4x6).
Finally, all those variously-sized tennis media credentials with holders I've kept for bragging rights will come in handy.
Some people are getting their cards laminated. I opted not to do that because of the likelihood we'll need a 3rd or booster shot and I want access to the card to add that next shot. So I got clear vaccine card holders, you slip the card in and there's a closure, but you can still pull it out later on if you need to.
If you go this route, just be aware that CDC cards come in at least two sizes. The petite size will fit into any of the advertised 4x3 holders you can find (Etsy and Amazon have loads of them), but the bigger size, it's a much tighter fit. You might be able to fit it with a little maneuvering (basically slightly bending the top to slip it in, it fits cleanly, but it's a seriously tight fit that way). The only other option I've found thus far s 2 inches larger, so unnecessarily bigger for carrying around all the time, and that is a clear passport holder (go with 4x6).
Finally, all those variously-sized tennis media credentials with holders I've kept for bragging rights will come in handy.
[/quote]
If I go to GA I will send you a self-stamped envelope for you to send me one (if you have so many).
Actually, not a bad idea. Carry it like a badge.
by ti-amie
I'm not going to post that gif. I'm not.
by Deuce ^ The fact that they sold $1 million worth of this stuff does not speak well for the capacity of human intelligence.
Then again... it seems that their claim of it being a cure for COVID-19, cancer, autism, etc. may very well be correct, technically.
Ingestion of enough of this stuff will kill you - which effectively eliminates the COVID-19, cancer, autism, etc. within you.
by ponchi101 A bit of an extreme solution, but you are right.
Also, give them a Darwin award. It would be well deserved.
by atlpam
Deuce wrote: ↑Sun Apr 25, 2021 8:09 pm
^ The fact that they sold $1 million worth of this stuff does not speak well for the capacity of human intelligence.
Then again... it seems that their claim of it being a cure for COVID-19, cancer, autism, etc. may very well be correct, technically.
Ingestion of enough of this stuff will kill you - which effectively eliminates the COVID-19, cancer, autism, etc. within you.
My thoughts exactly!
by Suliso I'd like to see data from few extra days but seems like vaccines are starting to show a major effect in US. It also makes sense, same happened in Israel once they reached 40-50% with at least one dose + all those who have had it recently.
by ti-amie
by Suliso Those patents should be waived, but I don't see how that would help India in a medium (half a year) term. They already produce AZ and couldn't product Pfizer/BioNtech or Moderna patents or no patents.
by ti-amie While funeral pyres burn in India here in the country with the most and best access to vaccines there is this stupidity.
A private school in Miami, citing false claims, bars vaccinated teachers from contact with students.
By Patricia Mazzei
April 26, 2021, 4:10 p.m. ET
A private school in the fashionable Design District of Miami sent its faculty and staff a letter last week about getting vaccinated against Covid-19. But unlike institutions that have encouraged and even facilitated vaccination for teachers, the school, Centner Academy, did the opposite: One of its co-founders, Leila Centner, informed employees “with a very heavy heart” that if they chose to get a shot, they would have to stay away from students.
In an example of how misinformation threatens the nation’s effort to vaccinate enough Americans to get the coronavirus under control, Ms. Centner, who has frequently shared anti-vaccine posts on Facebook, claimed in the letter that “reports have surfaced recently of non-vaccinated people being negatively impacted by interacting with people who have been vaccinated.”
“Even among our own population, we have at least three women with menstrual cycles impacted after having spent time with a vaccinated person,” she wrote, repeating a false claim that vaccinated people can somehow pass the vaccine to others and thereby affect their reproductive systems. (They can do neither.)
In the letter, Ms. Centner gave employees three options:
Inform the school if they had already been vaccinated, so they could be kept physically distanced from students;
Let the school know if they get the vaccine before the end of the school year, “as we cannot allow recently vaccinated people to be near our students until more information is known”;
Wait until the school year is over to get vaccinated.
Teachers who get the vaccine over the summer will not be allowed to return, the letter said, until clinical trials on the vaccine are completed, and then only “if a position is still available at that time” — effectively making teachers’ employment contingent on avoiding the vaccine.
Leila Centner at an event in Miami in 2019.
Credit...Romain Maurice/Getty Images for Haute Living
Ms. Centner required the faculty and staff to fill out a “confidential” form revealing whether they had received a vaccine — and if so, which one and how many doses — or planned to get vaccinated. The form requires employees to “acknowledge the School will take legal measures needed to protect the students if it is determined that I have not answered these questions accurately.”
Ms. Centner directed questions about the matter to her publicist, who said in a statement that the school’s top priority throughout the pandemic has been to keep students safe. The statement repeated false claims that vaccinated people “may be transmitting something from their bodies” leading to adverse reproductive issues among women.
“We are not 100 percent sure the Covid injections are safe and there are too many unknown variables for us to feel comfortable at this current time,” the statement said.
The Food and Drug Administration, the Centers for Disease Control and Prevention, the World Health Organization and many other authorities have concluded that the coronavirus vaccines now in emergency use in the United States are safe and effective.
The Centner Academy opened in 2019 for students in prekindergarten through eighth grade, promoting itself as a “happiness school” focused on children’s mindfulness and emotional intelligence. The school prominently advertises on its website support for “medical freedom from mandated vaccines.”
Ms. Centner founded the school with her husband, David Centner, a technology and electronic highway tolling entrepreneur. Each has donated heavily to the Republican Party and the Trump re-election campaign, while giving much smaller sums to local Democrats.
In February, the Centners welcomed a special guest to speak to students: Robert F. Kennedy Jr., the prominent antivaccine activist. (Mr. Kennedy was suspended from Instagram a few days later for promoting Covid-19 vaccine misinformation.) This month, the school hosted a Zoom talk with Dr. Lawrence Palevsky, a New York pediatrician frequently cited by anti-vaccination activists.
by ponchi101 I am on the other side. I have too much.
by dryrunguy Here's the latest Situation Reports. Lots of things to note.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 147.5 million cases and 3.1 million deaths worldwide as of 10:00am EDT on April 27. The WHO reported a new record high last week in terms of weekly incidence, with nearly 5.7 million new cases. Weekly incidence increased for the ninth consecutive week. Global weekly mortality increased for the sixth consecutive week, up to 87,733 deaths—the highest weekly total since the first week of February.
India continues to set new global records in terms of daily incidence. On April 24, India became the first country to surpass 300,000 new cases per day, and its daily incidence continues to increase rapidly. India is currently reporting more than 330,000 new cases per day, and if it continues on this trajectory, it could surpass 350,000 new cases per day in the next 2-3 days. The rate of increase appears to have slowed slightly over the past several days, but it is not yet clear whether this is an early sign of a longer-term trend. India also became the first country to report more than 350,000 new cases in a single day on April 25.
Turkey’s daily incidence peaked on April 20, with 60,266 new cases per day. Turkey approached Brazil (#3) and the US (#2)—both of which continue to report decreasing daily incidence—but it did not surpass either country before declining for 6 consecutive days. The epidemics in Argentina, Colombia, Germany, and Iran also appeared to level off over the past several days. France’s and Italy’s epidemics are declining as well.
Global Vaccination
The WHO reported 961 million vaccine doses administered globally, including more than 500 million individuals with at least 1 dose. The WHO dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
According to Our World in Data, the global cumulative total doses administered surpassed 1 billion doses. This is 13% more than this time last week, slightly lower than the previous growth rate of approximately 18% per week. After 6 days of declining averages, the daily doses administered rebounded slightly over the past 6 days, back up to 16.6 million.
UNITED STATES
The US CDC reported 31.9 million cumulative cases and 569,272 deaths. Both daily incidence and mortality are decreasing in the US. Daily incidence is down to 54,405 new cases per day, a 22% decrease from the most recent peak on April 13 (69,878). Daily mortality fell to 661 deaths per day, which is still essentially equal to the low that preceded the autumn/winter 2020 surge (662).
US Vaccination
The US has distributed 291 million doses of SARS-CoV-2 vaccine and administered 231 million doses. Daily doses administered* continue to decrease, down from a high of 3.2 million (April 11) to 2.6 million. Approximately 1.4 million people are achieving fully vaccinated status per day.
A total of 141 million individuals have received at least 1 dose of the vaccine, equivalent to 43% of the entire US population and 54% of all adults. Of those, 96 million (29% of the total population; 37% of adults) are fully vaccinated. Among adults aged 65 years and older, progress has largely stalled at 82% with at least 1 dose and 68% fully vaccinated. In terms of full vaccination, 48 million individuals have received the Pfizer-BioNTech vaccine, 40 million have received the Moderna vaccine, and 8.0 million have received the J&J-Janssen vaccine.
As of April 19, all US states expanded vaccination eligibility to all individuals aged 16 years and older, but the pace of vaccinations is beginning to taper off. Since the national high of 3.2 million doses per day on April 11, the daily average has steadily decreased by more than 20%, down to 2.4 million*. Even with everyone aged 16 years and older now eligible and with sufficient supply, progress toward herd immunity will slow considerably over the coming weeks for a variety of reasons. Some reasons include vaccine opposition and hesitancy, barriers to accessing the vaccine, and dwindling unvaccinated population. In light of the slowing pace, we will look at state-level trends in daily vaccine administration.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The majority of states reported their peak doses administered around the time they expanded eligibility to everyone aged 16 years and older or shortly thereafter. More than half of US states (27) reported peaks between 3 days before and 11 days after they expanded to full eligibility. Three states—New Mexico (44 days before), Oklahoma (32 before), and South Dakota (39 before)—reported peaks more than 4 weeks before they expanded eligibility to all individuals aged 16 years and older. If you remove short, temporary reporting spikes for these states, however, their peaks would be in early April, near or shortly after they expanded eligibility. Three (3) states reported peaks at least 3 weeks after they expanded eligibility: Alaska (+35 days), Florida (+25), and Utah (+26). All 3 states reported peaks in early-to-mid April, similar to many other states, but they expanded eligibility much earlier than most states. Alaska was the first state to expand eligibility to everyone aged 16 years and older (March 9), and Florida (March 25) and Utah (March 24) were among the first 6 states to do so.
In total, 9 states reported their peak daily doses administered by the end of March; however, none of these states appear to have exhibited a definitive early peak. Notably, reporting aberrations could account for nearly half of these states. As noted above, the peaks in New Mexico (February 25), Oklahoma (February 25), and South Dakota (February 25) appear to be due to reporting fluctuations, and Louisiana (March 13) exhibited a similar brief spike. The true peaks for these states were actually in early April. Additionally, Arizona’s peak was on March 31, just before April, and Idaho’s average held relatively steady between March 24 and April 13. Iowa (March 13), Mississippi (March 4), and North Carolina (March 18) all reported early peaks, followed by a slight decrease and then a second peak in April that was nearly as high, before finally beginning to decline steadily.
Only 3 states reported their record high in the past week: California (April 20), Hawai’i (April 26), and Maryland (April 24). California and Hawai’i were among the last states to expand to full eligibility (April 15 and 19, respectively). The peak in Hawai’i could be a function of a spike in reported doses on April 20, but the trend does appear to still be increasing overall. More than half of all states (28) reported their peak daily doses administered within the past 2 weeks.
A total of 6 states are currently reporting increasing daily doses administered over the past week**. Pennsylvania reported its highest peak on April 16, but its overall trend appears to still be increasing. As noted above, Hawai’i reported a sharp spike in doses administered on April 20, which puts its weekly average far above the previous week; however, it still appears to be exhibiting an increasing trend since that jump. While Idaho and Wyoming are reporting increases compared to last week, they both appear to be exhibiting an overall decline in daily doses administered—although it is a little difficult to be certain due to fluctuations in the weekly average. Rhode Island and Minnesota appear to be near their respective peaks, but they have not begun to exhibit a clear decline. Massachusetts also could still be approaching its peak, but it is difficult to determine the longer-term trend. The remaining states generally appear to be past their peak and either holding relatively steady or declining. Nine (9) states are holding steady (including Massachusetts), and 35 are reporting decreasing trends**.
**Increasing means at least a 5% increase compared to this time last week, holding steady is less than a 5% increase or decrease, and decreasing means 5% or greater decrease.
The Johns Hopkins Coronavirus Resource Center is reporting 32.1 million cumulative cases and 572,794 deaths as of 11:15am EDT on April 27.
INDIA India is experiencing the world’s largest COVID-19 surge, with more than 350,000 new cases per day. Experts fear the true number of cases could be substantially higher, with cases underreported for reasons including a variety in case-reporting infrastructures and lack of testing. Under the already strained health care system, hospitals are unable to take new patients and many grieving families have been forced to forgo regular funeral ceremonies for mass cremations, painting a devastating picture of the reality on the ground. India’s government has left decisions about non-pharmaceutical interventions such as physical distancing or mask wearing up to individual states, with many citizens lamenting a lack of proper government direction and dearth of resources, including diagnostics, hospital bed space, and oxygen. While some volunteers, dubbed “COVID Warriors,” are developing databases to connect people to resources, hospitals, and supplies, others are turning to the black market in a last-ditch effort to save their loved ones. In response to international pressure and rising calls for action, the US government on April 25 announced intentions to provide supplies and support to India, and lifted previous bans on the export of raw materials, diagnostic kits, and equipment. Additionally, USAID and the US CDC are deploying a “strike team” of staffers to India to work with local governments and organizations to address the surge in cases.
US DONATING ASTRAZENECA-OXFORD VACCINE The US government announced on April 26 it intends to share up to 60 million doses of the AstraZeneca-Oxford SARS-CoV-2 vaccine with other nations, greatly expanding its previous announcement to share about 4 million doses of the vaccine with Mexico and Canada. The US FDA has not yet authorized the AstraZeneca-Oxford for emergency use, although it is widely available in other countries. White House Coronavirus Response Coordinator Jeffrey Zients said about 10 million doses of the vaccine are undergoing a safety and quality review, which is expected to be complete in the next several weeks. An additional 50 million doses are in various production stages and could be available to ship in May and June after FDA review. White House officials said they are in the planning phase and do not yet know which countries will receive the donated doses. The announcement followed a conversation between US President Joe Biden and India Prime Minister Narendra Modi, whose country currently is facing the world’s largest surge in COVID-19 cases. The US government has come under increasing pressure to do more to address the pandemic abroad, and the announcement marks a shift in the government’s willingness to commit to vaccine donations.
VACCINE INTELLECTUAL PROPERTY US Trade Representative Katherine Tai on April 26 met virtually with executives of Pfizer and AstraZeneca to discuss increasing access to and production of SARS-CoV-2 vaccines during the COVID-19 pandemic. The meetings follow delivery to the White House of a petition signed by more than 2 million people urging the US government to support a proposal at the World Trade Organization to temporarily waive the intellectual property (IP) rights of pharmaceutical companies to allow low- and middle-income countries (LMICs) to more easily produce SARS-CoV-2 vaccines. India and South Africa, with support from more than 100 LMICs, repeatedly have proposed the waiver to the WTO’s Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS), but their efforts have failed amid pushback from the pharmaceutical industry and several wealthy nations, including the US. Industry lobbyists have increased their efforts to oppose a waiver, with some warning a loosening of patents could expose new technologies to exploitation by China and Russia. However, US trade officials have acknowledged steps need to be taken to increase global vaccine production, as gaps in access could undermine US progress toward ending the COVID-19 pandemic. Tai’s meetings with the pharmaceutical executives reflect the USTR’s engagement in efforts to increase access to vaccines and support her statements at a recent WTO meeting that the divide in access is “completely unacceptable.”
J&J-JANSSEN VACCINE & BLOOD CLOTS The US CDC and US FDA on April 23 recommended resuming use of the J&J-Janssen SARS-CoV-2 vaccine following a temporary pause. The agencies issued a pause on April 13 due to reports of rare but potentially serious blood-clotting events among 6 vaccine recipients, out of nearly 7 million recipients at the time. The FDA has amended the vaccine’s Emergency Use Authorization to mention the potential for clotting issues and will add warnings on fact sheets for providers and vaccinees specifically mentioning blood clots occurring with low platelets. The CDC’s Advisory Committee on Immunization Practices (ACIP) also recommended the continued use of the vaccine after a meeting on Friday, saying their review of data shows that the J&J-Janssen vaccine’s “known and potential benefits outweigh its known and potential risks.” The committee emphasized that nearly all reported cases of the adverse event occurred among women younger than age 50, that those women should be aware of the rare but increased risk, and that there are other SARS-CoV-2 vaccine options. Some experts are warning the pause might have caused more harm than good, with more than 10 million doses of the single-shot vaccine now waiting to be administered. According to a Washington Post-ABC poll, only 22% of respondents who are not yet vaccinated said they are willing to receive the J&J-Janssen vaccine. This unwillingness of the public to use the vaccine could negatively impact US vaccination efforts, especially in rural areas, prisons, and among homebound or transient populations, where the single-dose shot provided convenience.
On April 20, the European Medicines Agency (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) issued a statement recommending a warning about unusual blood clots with low blood platelets be added to the label of the J&J-Janssen vaccine but maintained these events should be listed as very rare. Like the US agencies, the European regulator emphasized that the vaccine’s benefits in preventing COVID-19 outweigh the risks of adverse events. On April 23, the EMA Committee for Medicinal Products for Human Use (CHMP) addressed concerns over blood-clotting events associated with the AstraZeneca-Oxford SARS-CoV-2 vaccine, saying people who have received a first dose should move forward to receive a second dose between 4 and 12 weeks after their initial shot. As we previously reported, the same rare type of blood clots with low platelet counts have been identified among some people who received that vaccine, which uses a viral vector platform similar to the J&J-Janssen vaccine.
US CDC RECOMMENDS VACCINATION FOR PREGNANT WOMEN Following the publication of preliminary findings detailing the effectiveness of SARS-CoV-2 mRNA vaccines in pregnant persons in the April 21 New England Journal of Medicine, US CDC Director Dr. Rochelle Walensky said during a briefing on April 23 that the agency recommends all pregnant persons receive a vaccine. Dr. Walensky noted that no safety concerns arose for pregnant persons vaccinated during their third trimester nor for their infants, although the study did not include the J&J-Janssen vaccine. Experts have taken special interest in the effect of vaccinations in pregnant persons, and a study published on April 22 in JAMA Pediatrics shows they are at a higher risk for complications due to COVID-19. The research, which described the experiences of 2,130 pregnant persons in 18 countries, concluded that the risks of COVID-19-related morbidity and mortality among pregnant people and their infants are greater than previously thought, underscoring the importance of vaccination for pregnant people.
BRAZIL REJECTS RUSSIAN VACCINE Brazil’s national health surveillance agency Anvisa has rejected importation of Russia’s Sputnik V vaccine, citing a lack of consistency in the vaccine’s efficacy and safety data. The decision was made following a unanimous vote from Anvisa’s 5 board directors, each of whom expressed doubts about the vaccine candidate’s benefits and concerns over the potential risk of harmful adverse events. Ana Carolina Moreira Marino Araújo, advisor for the Directorate of Authorization and Registration at Anvisa, stated the agency’s inspectors were denied access to key manufacturing facilities in Russia and found faults in areas they were able to inspect. Russian officials pushed back against the decision, alleging it was politically rather than scientifically motivated. The Gamaleya National Research Center of Epidemiology and Microbiology, which developed the Sputnik V vaccine, maintains the vaccine’s efficacy to be 97.6% in preventing symptomatic COVID-19 disease. Several of Brazil’s state governments have contracts to receive millions of Sputnik V doses once it is cleared for importation. Despite pushback, Anvisa has stood behind its decision, even amid circulation of the P.1 SARS-COV-2 variant, saying other SARS-CoV-2 vaccines are approved for use in Brazil.
SECOND DOSES According to new US CDC data reported by multiple news media outlets, nearly 8% of people who received their first dose of the Pfizer-BioNTech or Moderna SARS-CoV-2 vaccines have not received their second dose. That is more than double the rate seen in the early part of vaccination campaigns, from December 2020 to February 2021. The CDC’s new data cover missed doses through April 9, including those who received a first Moderna dose by March 7 or a first Pfizer-BioNTech dose by March 14. Reasons for the lapses in dosing vary, ranging from a lack of supply, fears of side effects, or feelings among vaccine recipients that one dose provides sufficient protection, especially as vaccine administration becomes more widespread. But the increasing number of people missing or foregoing a second dose is fueling concern among state public health officials, some of whom are implementing reminder services and allocating doses to be used specifically for people who are overdue for their second shot. Data from clinical trials and real-world follow-up studies show that a single dose triggers a weaker immune response than two doses, potentially leaving those one-dose recipients more susceptible to infection.
Brazil is facing similar concerns, with 1.5 million people missing appointments for their second dose, according to the Ministry of Health. In a technical note issued April 26, the agency urged people to receive their second dose even if the recommended timing target had passed. Some experts cited concerns over real-world data from Chile, showing the Sinovac SARS-CoV-2 vaccine, which accounts for about 80% of Brazil's vaccination program, is only 16% effective after one shot. The Ministry of Health said it is planning a national media campaign to improve communication surrounding the importance of getting the second dose.
EU LAWSUIT AGAINST ASTRAZENECA The European Commission (EC), the EU’s executive branch, announced a lawsuit against AstraZeneca alleging the company has failed to meet its contractual agreements for vaccine delivery. The lawsuit claims AstraZeneca has failed to deliver hundreds of millions of vaccine doses in a timely manner, according to an advanced purchase agreement. AstraZeneca previously stated it would only be able to provide about 100 million out of 300 million promised vaccine doses by the end of June. EC representatives also allege AstraZeneca has not developed an adequate strategy to combat delivery delays. In response to the lawsuit, AstraZeneca said in a statement that it is on course to fulfill its commitments to the EU for the end of this month and noted that its vaccine made up 97% of the vaccine doses provided through the COVAX facility. The lawsuit follows a dispute resolution mechanism launched by the EC in March that was intended to internally settle existing disputes between the two entities. Regardless of the outcome, the fact remains that the EU has fewer than anticipated doses of SARS-CoV-2 vaccines to distribute among its Member States. To fill in some of these gaps, EC President Ursula von der Leyen announced a new contract with Pfizer-BioNTech last week for 1.8 billion doses of its vaccine over the 2021-2023 period.
LONG-TERM EFFECTS Research continues to better characterize the long-term health effects of SARS-CoV-2 infection, formally referred to as post-acute sequelae of SARS-CoV-2 infection (PASC) and commonly referred to as “long COVID.” Researchers from St. Louis, Missouri (US), published an analysis of morbidity and mortality risk in the 6 months following infection. The study, published in Nature, included data from more than 73,000 COVID-19 patients treated in the US Department of Veterans Affairs health system and compared them with nearly 5 million non-COVID-19 patients within the system. The researchers found that mortality risk among COVID-19 patients beyond the first 30 days of illness was nearly 60% higher, corresponding to 8.39 excess deaths per 1,000 individuals at the 6-month point. The excess deaths among hospitalized COVID-19 patients was even higher (28.79).
The researchers also observed a statistically significant increase in outpatient care and use of certain treatment drugs, including opioid and non-opioid pain medications, among COVID-19 patients. The use of beta blockers and opioid analgesics was nearly 10 times higher among COVID-19 patients when compared with non-COVID-19 patients. The study presents detailed results for more than 75 conditions and medications associated with COVID-19. Notably, many of the statistically significant results remained when compared against seasonal influenza patients. This appears to be the largest study of its kind to evaluate the long-term health effects of SARS-CoV-2 infection.
HOMELESSNESS & VACCINATION As the US moves toward increased SARS-CoV-2 vaccine coverage among a majority of adults, current vaccination efforts aim to address at-risk and vulnerable populations, such as persons experiencing homelessness. Public health officials are facing vaccine refusal and hesitancy among the entire US population, but they face additional policy and logistical challenges—such as the added complexity of a multi-dose regimen—when creating outreach plans for persons experiencing homelessness. Reaching adequate coverage among this population will require joint task forces, community-level outreach, information and education campaigns geared at addressing vaccine willingness, and establishing mobile vaccination teams to meet residents where they are. For example, the City of San Francisco implemented mobile teams to serve homebound adults and people living in congregate facilities. Community members and non-profit organizations are collaborating to provide food and other incentives at vaccination events to increase accessibility and awareness of the SARS-CoV-2 vaccine.
by ponchi101 Oh, yeah, EU. This is the best moment to sue a large pharmaceutical company, just when you need people to have confidence in what they do. Not myopic at all.
---0---
GF and I went to get our INFLUENZA vaccines today. But, as our lucky streak continues, we were told that, as there have been no studies of how the INF vaccine interacts with the COVID vaccine, if we got our flu shots we would have to wait at least 60 days before being eligible for the COVID one.
Since we "know" we will not die of INF, we bailed.
AITA?
by Deuce
ponchi101 wrote: ↑Tue Apr 27, 2021 9:03 pm
Oh, yeah, EU. This is the best moment to sue a large pharmaceutical company, just when you need people to have confidence in what they do. Not myopic at all.
---0---
GF and I went to get our INFLUENZE vaccines today. But, as our lucky streak continues, we were told that, as there have been no studies of how the INF vaccine interacts with the COVID vaccine, if we got our flu shots we would have to wait at least 60 days before being eligible for the COVID one.
Since we "know" we will not die of INF, we bailed.
AITA?
I don't know what the situation is like in Colombia, but here in Canada, they said there was no 'flu season' this past winter - for the first time in a long, long time. This is because COVID-19 kept people apart from each other.
So I wonder if the flu shot is necessary at all in these times. If there's no 'flu season', there's nothing to protect oneself against.
The flu season here is during the winter. Most people think that it's the cold weather that brings on the flu - but it's not that at all, of course... not directly, at least. The flu is most active in the winter because that's the time of year that people are inside together (in non-pandemic times) - and thus transmission occurs more readily.
by ponchi101 Situation in Colombia is pretty bleak. ICU's are all either at 100% or close to it, in the major cities. People can't remain without work anymore and the number of people in the street begging is increasing and, a bit scary, these people are getting aggressive.
Nothing good.
by JazzNU
ponchi101 wrote: ↑Tue Apr 27, 2021 9:03 pm
GF and I went to get our INFLUENZA vaccines today. But, as our lucky streak continues, we were told that, as there have been no studies of how the INF vaccine interacts with the COVID vaccine, if we got our flu shots we would have to wait at least 60 days before being eligible for the COVID one.
Since we "know" we will not die of INF, we bailed.
AITA?
Well here, they ask questions to make certain you haven't had a vaccine of any kind 2 weeks before getting your covid vaccine. So, unless you've got a different kind of flu vaccine there, you'd be good to go in terms of your plans to come to Georgia to get vaccinated.
ponchi101 wrote: ↑Tue Apr 27, 2021 9:03 pm
GF and I went to get our INFLUENZA vaccines today. But, as our lucky streak continues, we were told that, as there have been no studies of how the INF vaccine interacts with the COVID vaccine, if we got our flu shots we would have to wait at least 60 days before being eligible for the COVID one.
Since we "know" we will not die of INF, we bailed.
AITA?
Well here, they ask questions to make certain you haven't had a vaccine of any kind 2 weeks before getting your covid vaccine. So, unless you've got a different kind of flu vaccine there, you'd be good to go in terms of your plans to come to Georgia to get vaccinated.
Yes, 2 weeks is the recommended wait between vaccines. I had to consider this when I opted to get my Shingles vaccine. I got the first in late Jan before I was eligible for the covid vaccine. Since there's a 2-6 month window to get the second, I'm waiting until June, so I will have almost 2 months since my Covid vaccine. Personally I would want at least 4 weeks in between to not confuse any potential side effects.
ponchi101 wrote: ↑Tue Apr 27, 2021 9:03 pm
GF and I went to get our INFLUENZA vaccines today. But, as our lucky streak continues, we were told that, as there have been no studies of how the INF vaccine interacts with the COVID vaccine, if we got our flu shots we would have to wait at least 60 days before being eligible for the COVID one.
Since we "know" we will not die of INF, we bailed.
AITA?
Well here, they ask questions to make certain you haven't had a vaccine of any kind 2 weeks before getting your covid vaccine. So, unless you've got a different kind of flu vaccine there, you'd be good to go in terms of your plans to come to Georgia to get vaccinated.
Yes, 2 weeks is the recommended wait between vaccines. I had to consider this when I opted to get my Shingles vaccine. I got the first in late Jan before I was eligible for the covid vaccine. Since there's a 2-6 month window to get the second, I'm waiting until June, so I will have almost 2 months since my Covid vaccine. Personally I would want at least 4 weeks in between to not confuse any potential side effects.
My sister had to wait to get her first shot because she'd just taken her first shingles vaccine shot. Now that you can walk in here in NYC she's going next week I think
by ti-amie
This is why I will continue to wear masks in public. The only solution would be for an official card or - gasp - a vaccine passport.
by Suliso I have a paper vaccine passport. Doesn't seem that hard to fake a Covid vaccine entry there if one is so inclined. They're talking about it being available online and being verifiable, but that will be maybe in the summer. I wonder what kind of documents US travelers will need for coming here (to be allowed soon).
Anyway someone cheating is inevitable, those things will never be as secure as actual passports. Would cost way too much.
by ti-amie
Suliso wrote: ↑Thu Apr 29, 2021 9:29 pm
I have a vaccine passport of the same format as shown below. Doesn't seem that hard to fake a Covid vaccine entry there if one is so inclined. They're talking about it being available online and being verifiable, but that will be maybe in the summer. I wonder what kind of documents US travelers will need for coming here (to be allowed soon).
We had yellow cards just like that when we were kids that our pediatricians filled out and had to be provided to schools when you registered. I think they're going to have to step up from that.
by Suliso It would be convenient to add covid mark to all the other vaccines I have had in recent years, but indeed maybe they'll have to do a more secure version.
by ponchi101 The only system that I know off is here in Colombia, where they peel the label of the vaccine off the vial and paste it back in your vaccine passport/card.
I have a "passport" that was issued by a vaccinations center in Bolivia. Totally non-official but helpful to keep all vaccines straight. The ones from Colombia are stapled there.
My understanding is that modern passports have a chip to store info (mine does). I wonder how difficult can it be to develop some software to include "COVID = DATE()" and set it to NULL (no vaccine) or a date (when you got it).
by ti-amie
by JazzNU I wholeheartedly agree with Joe's assessment of himself. And as a diehard Newsradio fan, I take no pleasure in it.
That is basically where our ex-governor and medicare fraud expert wants to do. (By the way, our current governor wants the fed money to allocate it for businesses)
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 150.1 million cases and 3.2 million deaths worldwide as of 8:45am EDT on April 30. From the first reported COVID-19 case, it took 90 days to reach 1 million cases and 177 days to reach 10 million cases:
1 case to 25 million- 240 days
25 to 50 million- 69 days
50 to 75 million- 41 days
75 to 100 million- 40 days
100 to 125 million- 57 days
125 to 150 million- 35 days
India surpassed 200,000 cumulative COVID-19 deaths on April 28, and Brazil surpassed 400,000 deaths on April 29. Brazil remains #2 globally, with 401,186 deaths, and India is #4 with 208,330. The US is #1 (575,194), and Mexico is #3 (216,447). At its current pace, however, India could surpass Mexico in the next several days. Additionally, India surpassed 350,000 new cases per day on April 29, the only country to surpass this milestone. With 357,040 new cases per day, India currently accounts for more than 40% of the global daily incidence and nearly 6 times the daily incidence in any other country. It does appear as though India may have passed an inflection point, as the increase in daily incidence has tapered off to some degree over the past several days.
In addition to India, several other countries in and near the WHO’s South-East Asia Region (SEARO) are exhibiting concerning COVID-19 incidence trends. Including India, 7 of the 11 SEARO countries are exhibiting biweekly increases greater than 100%. These countries’ respective epidemics are considerably smaller than India’s, which is allowing them to be overlooked; however, the proportionate increases are concerning indications that they could be facing severe impacts in the very near future. In addition to the SEARO region, nearby Afghanistan, Cambodia, and Laos also are battling substantial surges. The surges in these countries—most of which either border India or are located within approximately 1,000 miles (1,600 km)—started around the same time or shortly after India’s. If these countries continue on this trajectory, they could face similar impacts on their health systems as we have observed in India as well as associated increases in COVID-19 mortality. These countries should be monitored closely.
Nepal’s COVID-19 biweekly incidence increased by more than 600% compared to 2 weeks ago. After peaking at more than 3,800 new cases per day in October 2020, Nepal brought its COVID-19 epidemic under control, down to 71 new cases per day in mid-March 2021. Nepal’s epidemic began a sharp surge in early April, and it is already back up to more than 3,600 new cases per day and still increasing rapidly. The current surges in Thailand and Bhutan began in late March/early April as well, but their increases have not been quite as sharp as Nepal’s. Thailand is currently reporting more than 2,200 new cases per day, more than double its previous peak, and still increasing rapidly. Bhutan is only reporting 10-12 new cases per day, but this is at least a 20-fold increase since late March.
The surges in Sri Lanka and Maldives started several weeks later, in mid-to-late April. In Sri Lanka, the daily incidence increased from a recent low of 215 new cases per day on April 17 to more than 1,100. Sri Lanka is currently reporting nearly 25% more daily cases than its previous highest peak, and its epidemic continues to accelerate rapidly. Maldives is also setting new national records. Its current daily incidence climbed from 84 new cases per day to 327, 75% higher than its previous highest peak and still increasing rapidly.
Timor-Leste is the most remote SEARO country relative to India, and its surge started in early March, around the same time as India’s. Timor’s daily incidence increased from fewer than 0.5 new cases per day to nearly 90. The daily incidence fell sharply from 88 to 76 new cases per day on April 29, but it is too early to determine if this is the start of a longer-term trend.
Outside the SEARO region, nearby Afghanistan, Cambodia, and Laos also are facing surges that raise concern. Cambodia and Laos are in the WHO’s Western Pacific Region, but they border Thailand and are located approximately 1,000 miles (1,600 km) or less from India. Laos is the #1 country globally in terms of the relative increase in biweekly incidence, up more than 15,000% compared to 2 weeks ago. From the onset of the pandemic through April 20, Laos reported more than 5 cases in a single day only once and only 60 cumulative cases; however, it has reported more than 600 new cases since then. Laos currently is averaging more than 80 new cases per day and increasing rapidly. In the context of larger countries and epidemics, Laos’ epidemic is small, but its rapid acceleration is particularly concerning. Cambodia reported fewer than 1 new case per day as recently as mid-February, before a smaller surge. Since early April, however, its daily incidence has surged sharply, up from 53 new cases per day to more than 650—a 12-fold increase in less than a month. Afghanistan is in the WHO’s Eastern Mediterranean Region, but it is located approximately 125-250 miles (200-400 km) from India. Afghanistan’s current surge began in mid-to-late March, and its daily incidence has increased from fewer than 20 new cases per day to 181, and still increasing. The current daily incidence is approaching Afghanistan’s previous peak (217 on November 24, 2020), but it is still well below its highest peak (759 on June 5, 2020). Afghanistan’s epidemic is accelerating at a much slower rate than many of the other countries discussed here.
Global Vaccination
The WHO reported 1.0 billion vaccine doses administered globally, including 546 million individuals with at least 1 dose. The WHO dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reported 1.1 billion cumulative doses administered globally. The global total continues to increase at 13% per week. After a brief decline, the daily doses administered rebounded to the previous record high of 18.7 million doses per day. Our World in Data estimates that there are 262 million people worldwide who are fully vaccinated, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.0 million cumulative cases and 571,297 deaths. Both daily incidence and mortality continue to decrease. Daily incidence is down to 52,528 new cases per day, the lowest average since October 12, 2020. The CDC reported an average of 626 and 628 deaths per day, respectively, over the past 2 days, which are the lowest daily mortality averages since June 27, 2020*. Notably, national test positivity is decreasing as well, down from 5.43% on April 12 to 4.47% on April 27**, which is an encouraging sign.
*Excepting the reports immediately following the 2020 Independence Day holiday.
**Test positivity data not published for April 28.
US Vaccination
The US has distributed more than 300 million doses of SARS-CoV-2 vaccine and administered 237 million doses. Daily doses administered* continues to decrease, down from a high of 3.2 million (April 11) to 2.5 million. Approximately 1.4 million people are achieving fully vaccinated status per day.
A total of 144 million individuals have received at least 1 dose of the vaccine, equivalent to 43% of the entire US population and 55% of all adults. Of those, nearly 100 million (99.7 million) are fully vaccinated, which corresponds to 30% of the total population and 38% of adults. Among adults aged 65 years and older, progress has largely stalled at 82% with at least 1 dose and 68% fully vaccinated. In terms of full vaccination, 50 million individuals have received the Pfizer-BioNTech vaccine, 41 million have received the Moderna vaccine, and 8.1 million have received the J&J-Janssen vaccine.
The Johns Hopkins Coronavirus Resource Center is reporting 32.3 million cumulative cases and 575,213 deaths in the U.S. as of 10:15am EDT on April 30.
UPDATED US CDC GUIDANCE On April 27, the US CDC issued updated guidance on COVID-19 protective measures, with the changes focusing largely on vaccinated individuals and outdoor activities. The new guidance accounts for a variety of factors, including increasing vaccination coverage, declining community transmission, and evolving evidence regarding transmission risk factors. The CDC’s overhauled webpage on “Choosing Safer Activities” provides a consolidated overview of the changes, including differences between vaccinated and unvaccinated individuals across a broad scope of activities. Notably, the new guidance indicates that fully vaccinated individuals can participate in a number of outdoor activities without wearing a mask, including exercise, small gatherings with vaccinated and unvaccinated individuals, and dining at restaurants. Mask use is still recommended for vaccinated individuals, however, for large outdoor gatherings (eg, concerts, sporting events) and indoor settings, including restaurants and bars, movie theaters, gyms and fitness centers, and places of worship.
Recognizing the relatively low risk of transmission in most outdoor settings, the CDC no longer recommends mask use for unvaccinated individuals in general outdoor settings (eg, walking or exercising) or for small gatherings with vaccinated individuals. Unvaccinated individuals are encouraged to wear masks in small gatherings with other unvaccinated individuals and in higher-risk settings, including indoor and outdoor dining at restaurants and bars, large indoor and outdoor gatherings, and other indoor settings. The CDC guidance emphasizes that many of these higher-risk settings are “less safe” or “least safe” for unvaccinated individuals, even with mask use.
The CDC also issued updated guidance this week for international travelers, including removing the requirements for a negative SARS-CoV-2 test before departing the US* and mandatory quarantine upon arrival in the US for fully vaccinated individuals**. Testing remains mandatory for all air travelers before departing on a flight to the US. Last week, the CDC issued new COVID-19 guidance for youth and summer camps, including updates regarding vaccination, physical distancing, screening and testing, and ventilation.
*Unless required by the destination country.
**Notably, the guidance explicitly specifies vaccines authorized for use by the US FDA or WHO.
EUROPEAN TRAVEL After restrictions on nonessential travel over the past year, fully vaccinated Americans will be allowed to travel to the EU this summer. European Commission President Ursula von der Leyen said in an interview Sunday with the New York Times that as long as visitors have been vaccinated with a product authorized by the European Medicines Agency (EMA), they will be permitted to enter all 27 member countries. The 3 vaccines authorized by the US FDA also are authorized by the EMA: Moderna, Pfizer-BioNTech, and J&J-Janssen. A specific date has not been announced to lift restrictions, but President von der Leyen noted that policies are in flux based on vaccination rates, the “epidemiological situation,” and vaccination certificates. Individual EU countries will be allowed to enact stricter regulations than the EU as a whole when travel resumes to the region.
INDIA VACCINE SUPPLIES India’s record-breaking COVID-19 surge is impacting the country’s ability to supply SARS-CoV-2 vaccine doses domestically and abroad. India is the world’s leading producer of vaccines, but it is struggling to produce and distribute enough vaccines for its population of 1.4 billion. As a result, India Prime Minister Narendra Modi recently suspended exports of nearly all 2.4 million doses of the AstraZeneca-Oxford vaccine produced daily by the Serum Institute of India, in effect stopping supply of the vaccine to the COVAX facility. This has raised alarms in Africa, which relies on COVAX for its vaccine doses. Africa CDC officials called the anticipated delay in supplies “devastating” and urged other nations to step in to fill the gaps. In an unexpected move, the Democratic Republic of Congo is returning 1.3 million vaccine doses to COVAX, saying it will be unable to administer them before they expire due to difficulties in distribution and vaccine refusal. The vaccines will now go to nations who can use them more quickly.
Additionally, many global health experts and others worldwide are insisting the US and other nations support a proposal at the World Trade Organization (WTO) by India and South Africa to temporarily waive some trade and intellectual property rules to help low- and middle-income countries (LMICs) fill the gaps. Even if the temporary waiver goes through at the WTO, which is set to hold its next General Council meeting on May 5, production and distribution challenges will remain. But experts contend these constraints could be overcome with more global cooperation and funding. In an April 28 address to the US Congress, US President Joe Biden focused his comments on the COVID-19 pandemic’s impacts on the US population and economy and did not mention global cooperation on vaccines. However, US government officials insist several proposals are being considered to pressure companies to share information on vaccines or boost US vaccine production for export. The White House also on April 28 published a fact sheet outlining its plans to help India with emergency assistance.
US-MADE VACCINE SHIPPED TO MEXICO This week Pfizer shipped US-made doses of its SARS-CoV-2 vaccine produced with BioNTech to Mexico, marking the first time the pharmaceutical company has delivered abroad from US facilities following the expiration of US government restrictions on vaccine exports. Pfizer is Mexico’s largest supplier of SARS-CoV-2 vaccines, having shipped more than 10 million doses so far. Pfizer expects to be making up to 25 million vaccine doses each week in the US by mid-year, more than it needs to meet US commitments. With agreements to supply more than 1 billion doses to countries worldwide, the company plans to continue shipping extra US-made vaccine doses abroad, as well as from production facilities in Belgium.
VACCINE EFFECTIVENESS An early release article published April 28 in the US CDC’s Morbidity and Mortality Weekly Report details the effectiveness of the Pfizer-BioNTech and Moderna vaccines in preventing COVID-19-related hospitalizations among a population at higher risk of the disease. Data from 24 hospitals in 14 states were collected from January to March 2021 for adults ages 65 years and older who were hospitalized for COVID-19-like illnesses to gauge the effectiveness of the two vaccines via partial or full vaccination. The adjusted vaccine effectiveness for full vaccination against COVID-19-associated hospitalization was estimated to be 94% (95% CI: 49-99%), and 64% (95% CI: 28-82%) for partial vaccination. The real-world findings confirm those from clinical trials, highlighting the importance of vaccinating older populations to reduce the risk of COVID-19-associated hospitalizations and potentially leading to reductions in post-COVID conditions and deaths.
SECOND DOSES The US government has directed pharmacies to expand access for second-dose vaccinations to include those who may have received their first dose elsewhere. The move follows reports that millions are skipping their second dose, sometimes due to supply challenges or access issues. The directive is aimed largely at college students, many of whom received their first dose on or near their campuses but will be returning home before becoming eligible for their second dose. Pharmacies participating in the federal vaccine distribution program will waive any residency requirements to allow people easier access to receive a second dose.
VACCINATION & RACIAL/ETHNIC DISPARITIES Preventing disparities in vaccine uptake among racial and ethnic groups in the US will be critical to mitigating disproportionate impacts of COVID-19 among people of color. According to US CDC data as of April 29, race/ethnicity data were available for 55% of people with at least one dose of vaccine and 58% of those fully vaccinated, with 64% and 67% of those, respectively, identifying as white. The Kaiser Family Foundation (KFF) also monitors this data, comparing it to localized health outcomes of race/ethnicity groups during the pandemic. According to KFF, Black and Hispanic populations have received smaller shares of vaccine doses compared to their shares of COVID-19 burden (cases and deaths) and their shares of total population in most states. According to experts, a complex set of reasons has led to these disparities in vaccine coverage, but access remains a leading issue. Across the US, vaccination sites’ locations, registration processes, time requirements to register and receive a vaccine, and transportation play predominant roles in vaccination coverage. Public health officials are encouraging the establishment of vaccination sites in communities with the lowest vaccination rates and with easier appointment scheduling, including walk-in clinics.
VACCINATION INCENTIVES With the number of daily SARS-CoV-2 vaccines administered in the US declining, public health entities and companies are getting creative, implementing various incentives to encourage more people to be vaccinated. Examples include offers of free donuts, beer, and even marijuana in states where it is legal; chances to win vehicles, airline tickets, or other large items; time off from work; or cash for people who give others rides to vaccination sites. Officials say the incentives are necessary to reach people who have yet to be vaccinated due to hesitancy, difficulties making appointments, or obstacles to accessing sites. According to one survey, more than two-thirds of respondents would get vaccinated in exchange for a financial incentive. However, some critics say the incentives could perpetuate individual unhealthy behaviors while promoting public health efforts. And some experts are calling for more strict interventions, urging some employers—including health systems and academic institutions—to make vaccination mandatory for employees.
TURKEY Earlier this week, Turkish President Tayyip Erdoğan announced a nearly 3-week lockdown in response to a sharp rise in COVID-19 cases and deaths across the country. The measure, which is being described as a “full lockdown,” went into effect on the evening of April 29 and will remain active until the early morning of May 17. The lockdown order requires residents to stay at home, with exceptions for essential functions such as grocery shopping, and mandates individuals receive permission before conducting inter-city travel. Notably, some businesses and industries are exempt from the shutdown, and lawmakers, healthcare workers, law enforcement officers, and tourists also are exempt from the stay-at-home order. The lockdown will encompass the final weeks of Ramadan, including Eid al-Fitr, a holiday traditionally marked by social gatherings across the country. Some families departed city centers for coastal vacation homes before the lockdown’s initiation, causing crowding in bus terminals and airports and along the nation’s highways.
ROUTINE TESTING STRATEGIES Researchers from the UK developed a model to evaluate the ability of routine asymptomatic PCR-based testing to detect SARS-CoV-2 infection. The study, published in BMC Medicine, utilized data from a study of repeated, self-administered testing of healthcare workers to estimate probability that twice-weekly testing would identify infected, asymptomatic individuals. Notably, individuals who were infected within several days of testing may not have sufficient virus present to result in a positive test. The researchers evaluated both the probability that a symptomatic case would be detected before the onset of symptoms and the probability that an asymptomatic infection would be detected within 7 days of infection, including test turnaround time, for various testing frequencies.
Assuming a 1-day test turnaround time, the researchers estimate that testing every 4 days would have a 76% probability of detecting an asymptomatic infection within 7 days, but increasing the frequency to every 2 days would increase that probability to 95%. Not surprisingly, increased test turnaround time decreased the probability of timely detection for both symptomatic and asymptomatic infections. The researchers note that as the frequency of testing increases, burden on laboratories increases, which can slow the turnaround time. It may be necessary to balance increased testing frequency against the associated increase in testing volume and slower turnaround times. As organizations—including health systems, businesses, and schools—consider routine testing programs, this study can provide insight into the appropriate frequency to mitigate transmission risk.
by ponchi101 As we are well into a full year of the pandemic, I remembered something that we talked about last year. India's count is obviously faulty and it is an undercount; however, I have not seen the STATS for TOTAL number of deaths in 2020 as opposed to 2019. If a non-significant increase, after COVID has been factored in, is what we can see, then the world-wide counts are accurate. But if we can see that there is an increase in total deaths, and this increase is beyond numbers that can be explainable, then we know that C19 has been even deadlier than what the numbers report.
Some people may have died of C19 and classified with some other cause of death (pneumonia). Specially, if we can see that there is a statistically valid increase in elderly deaths, which are not explained by other known causes, we could see how serious this has been.
Not that we do not know how serious it is, but it may be even more.
by ti-amie
by ti-amie
by ti-amie
by ti-amie
by Suliso Why not just vaccinate every participant? By June there will be a huge excess of doses in US, they could donate (or sell) for this cause. It's not an absolute protection true, but would make the whole endeavor much safer for sure.
by ti-amie
by JazzNU
by ti-amie
by ti-amie
by Suliso It's the right thing to do, symbolically if not otherwise. However I fail to see how this will increase vaccine supply in the short and medium (1-2 years) term. There should be regional vaccines manufacturers (Brazil, South Africa, Japan, Middle East etc), but it will take a long time to set this up. Factories are not there and people need to be trained and educated, logistics supply chains established and so on.
By the way read that India's Serum Institute is going to move some production to UK because of unfriendly Indian government. Prices government demands there are barely covering production costs not allowing any investment or expansion.
by dryrunguy I forgot to post the latest Situation Report distributed yesterday. Sorry. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 153 million cases and 3.2 million deaths worldwide as of 5:00am EDT on May 4. The global weekly incidence remained relatively consistent from the previous week at 5.7 million new cases, a decrease of 0.6%. Global weekly mortality increased for the seventh consecutive week, up to 93,253 deaths. This is the highest weekly total since late January 2021 and the fourth highest weekly total to date.
The COVID-19 epidemic in India continues to worsen, setting new global records for total daily incidence. India is currently reporting an average of 378,092 new cases per day. On April 30, India became the first country to report more than 400,000 new cases in a single day, but this was followed by 3 consecutive days of decreasing reports. India has reported more than 300,000 cases for 13 consecutive days, and it is currently reporting nearly 6.5 times the daily incidence in any other country and 47% of the global daily incidence.
Global Vaccination
The WHO reported 1.05 billion doses of SARS-CoV-2 vaccines administered globally, including 564 million individuals with at least 1 dose. The WHO dashboard does not yet include data for daily or weekly vaccinations or fully vaccinated individuals.
Our World in Data reported 1.2 billion cumulative doses administered globally, and the global total continues to increase at 13% per week. The daily doses administered decreased over the past 2 days, down from a high of 20.6 million doses per day on May 1 to 18.7 million. Our World in Data estimates that there are 280 million people worldwide who are fully vaccinated, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.2 million cumulative cases and 574,220 deaths. Both daily incidence and mortality continue to decrease. Daily incidence is down to 48,164 new cases per day, the lowest average since October 8, 2020. Daily mortality leveled off over the past several days, at approximately 625-650 deaths per day.
US Vaccination
The US has distributed 313 million doses of SARS-CoV-2 vaccine and administered 247 million doses. Daily doses administered* continues to decrease, down from a high of 3.3 million (April 11) to 2.3 million. Approximately 1.3 million people are achieving fully vaccinated status per day.
A total of 148 million individuals have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 44% of the entire US population and 56% of all adults. Of those, 106 million are fully vaccinated, which corresponds to 32% of the total population and 41% of adults. Among adults aged 65 years and older, progress has largely stalled at 83% with at least 1 dose and 70% fully vaccinated. In terms of full vaccination, 54 million individuals have received the Pfizer-BioNTech vaccine, 44 million have received the Moderna vaccine, and 8.3 million have received the J&J-Janssen vaccine.
As daily vaccinations continue to decline in the US, the impact is not distributed equally between first and second doses**. At the national level, the total doses administered has decreased from a high of 3.26 million doses per day on April 11 to 2.30 million on April 28, a 29% decline over that period. In terms of full vaccination**, the average fell 24% from the peak on April 12—1.77 million doses per day to 1.35 million. In contrast, the average for first doses decreased by half from its peak on April 11—from 1.93 million doses per day down to 965,421. The steep decline in first doses is being masked in the overall national data due to the continued progress by those obtaining their second dose. As we reach 3-4 weeks past the peak in first doses—when those individuals will receive their second doses—we can expect a sharper decline in the number of fully vaccinated individuals each day.
Vaccinations in long-term care facilities (LTCFs) illustrate the time lag between trends in first and full vaccination, but the magnitude of the changes align more closely than we are currently seeing in the overall national data. The overall national LTCF average decreased from a peak of 164,790 doses per day on February 6 to 34,095 on March 6—corresponding to an 80% decrease, or 2.9% per day over that period. In terms of first doses, the daily average began to peak in mid-January. The peak in fully vaccinated individuals started around February 7, nearly 4 weeks later, although the peak lasted only a few days. Following the peak, daily first doses declined 87% between January 31 and March 4, corresponding to 2.7% per day. In terms of full vaccination, the average decreased 84% from February 12 to March 15, also 2.7% per day.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
**The CDC only reports vaccination data for first doses and fully vaccinated individuals. It does not distinguish between fully vaccinated individuals who received 2 doses of the Pfizer-BioNTech or Moderna vaccines and those who received a single dose of the J&J-Janssen vaccine.
US VACCINE HESITANCY A complex combination of challenges faces ongoing vaccination efforts, including barriers to accessing vaccination, vaccine hesitancy, and denialism. Notably, a recent survey conducted by the Kaiser Family Foundation observed declining vaccine hesitancy from December 2020 through March 2021. Overall vaccine hesitancy and opposition—those who would “wait and see,” get vaccinated “only if required,” or “definitely not” get vaccinated—decreased from 64% to 37%. Notably, “wait and see” responses fell from 39% to 17% over that period, indicating increased confidence among those who were uncertain. These data were collected prior to the temporary suspension of the J&J-Janssen vaccine. With vaccine supply now exceeding demand, it is critical to identify and implement effective mechanisms to engage individuals and populations that have not yet been vaccinated. Some people in higher risk professions—including law enforcement, long-term care facility personnel, and healthcare workers in rural areas—as well as in certain rural communities, have lower vaccination coverage. It is also important to continue public education efforts regarding the benefits and timing of second doses to ensure vaccinated individuals develop full protection.
PEDIATRIC VACCINES The US FDA is expected to authorize the Pfizer-BioNTech SARS-CoV-2 vaccine for adolescents ages 12 to 15 late this week or early next week, according to an anonymous federal official. An amendment to the vaccine’s existing Emergency Use Authorization would open the US vaccination campaign to millions more people, reaching a younger population key to raising levels of immunity. If authorization is granted, the US CDC’s Advisory Committee on Immunization Practices (ACIP) would meet soon after to review data and make recommendations for the vaccine’s use among adolescents. According to data from Pfizer released at the end of March, a clinical trial involving 2,260 participants aged 12 to 15 showed the vaccine was well-tolerated and 100% efficacious. The Pfizer-BioNTech vaccine is currently authorized for people ages 16 and older. The companies are conducting clinical trials using the vaccine in people as young as 6 months old. BioNTech Chief Executive Ugur Sahin last week told German magazine Spiegel that the company expects first results in July for the group ages 5 to 12 and in September for the youngest age group. He also said the company will soon submit an application to European regulators to expand the vaccine’s use to adolescents there.
US VACCINE WASTAGE US CDC data suggest two national pharmacy chains are responsible for the majority of wasted SARS-CoV-2 vaccine doses, according to a KHN analysis. Overall, waste has been minimal, with the agency recording 182,874 wasted doses as of late March, out of approximately 189.5 million doses delivered and 147.6 million doses administered at that time. Of those wasted doses, CVS was responsible for about 50% and Walgreens for 21%, a greater total percentage than waste reported by US states, territories, and federal agencies combined*. The Pfizer-BioNTech vaccine accounted for nearly 60% of the wasted doses, possibly because it was the first to be rolled out in December 2020 and initially required storage at ultracold temperatures. CVS said “nearly all” of its reported vaccine waste happened in 2020 during early efforts to administer the vaccines to residents and employees of long-term care facilities. Walgreens did not specify what percentage of doses were wasted during those early efforts. KHN noted that while understanding vaccine waste is important to identify bottlenecks in distribution efforts, reporting has been inconsistent among US states and territories, and the CDC continues to have limited knowledge about how many doses are wasted, where the waste is occurring, and who is responsible. Public health experts warn that vaccine waste could increase in the coming weeks as efforts shift to administer doses among harder-to-reach populations, as perhaps the biggest reason for waste is people not showing up for their shot once a vial is opened.
*CDC data include reporting from 35 states, 17 pharmacies, and three other federal agencies through March 29, likely resulting in underreported waste.
VACCINE INTELLECTUAL PROPERTY U.S. Trade Representative Katherine Tai is expected this week to begin talks at the World Trade Organization (WTO) about efforts to more widely distribute, license, and share SARS-CoV-2 vaccines among countries in need. The White House has been under pressure from lawmakers and others to join an effort to temporarily waive intellectual property (IP) rights on vaccines to facilitate the manufacture of generic versions in low- and middle-income countries. On Sunday during an appearance on NBC News' "Meet the Press," US Senator Bernie Sanders said the US has a “moral responsibility” to help other nations and called efforts to slow the pandemic in “our own self interest.” He called on pharmaceutical companies and the WTO to waive intellectual property rights on vaccines and for the US to donate excess vaccine doses. Surges of COVID-19 cases in India and several other nations are driving what appears to be an increased willingness by the US to consider the issue of IP waivers.
Experts estimate around 11 billion doses are required to immunize 70% of the world’s population with 2-dose vaccines. To date, around 8.6 billion doses have been ordered, but 6 billion of those are earmarked for high- and upper-income countries. Pharmaceutical companies continue to oppose IP waivers, maintaining they can produce 10 billion vaccine doses this year under the existing IP system. However, some say that number is unattainable. Other critics say IP waivers alone will not help boost vaccine supplies because other drugmakers might not have the personnel, technology, and manufacturing techniques necessary to produce the newer mRNA vaccines. Instead, they encourage pharmaceutical companies to expand their own output, partnering with and licensing their technologies to other companies to support manufacturing expansions.
Another option could be laws passed at the national level. For example, Brazil’s Senate last week passed a bill that would suspend patent protections for SARS-CoV-2 vaccines, diagnostics, and medications during the pandemic. It remains unclear if the country’s lower house of Congress will support the bill. Brazil President Jair Bolsonaro, while facing mounting pressure from public health officials to increase vaccinations, does not support patent waivers.
INDIA The world continues to watch the grave situation in India, which last week became the first country to report more than 400,000 new COVID-19 cases in one day and continues to record more than 3,000 deaths per day. Experts warn these numbers are underestimates of the true impact of the pandemic in the country.
Prime Minister Narendra Modi has reached out to other nations for assistance, with the US and UK pledging to send supplies. Last week, the US sent a cargo plane full of oxygen cylinders, rapid diagnostic tests, and 100,000 N95 masks to assist India’s efforts, and the UK is planning to send an additional 1,000 ventilators to the country as well as offering technical assistance in the form of an expert advisory group. Over the weekend, US White House Chief of Staff Ron Klain said the US government is looking into ways to distribute more SARS-CoV-2 vaccines to India. Late last month, Prime Minister Modi discussed with US President Joe Biden lifting intellectual property rights for the vaccines, an issue expected to be discussed this week at a World Trade Organization meeting. Domestic and international health experts are urging Prime Minister Modi to implement a nationwide lockdown to ameliorate the impacts of the current surge. After reviewing India’s situation, the US government on April 30 imposed a travel ban for individuals coming from India, with exceptions for U.S. citizens. The Australian government has implemented similar policies, asking even their citizens to remain in India.
Critics point out the current surge is in stark contrast to the February comments by Prime Minister Modi’s party, the BJP, which declared defeat of COVID-19. They also admonish the government for exporting vaccines to bolster international standing at the expense of its own vaccination rates—less than 2% of the nation’s 940 million adults have been fully vaccinated—and continuing to allow mass religious gatherings and political rallies. Some health experts are decrying the lack of coordinated response, overcrowded cremation grounds, and neglected health system that has left many impoverished and without care for years.
MODERNA VACCINE & COVAX On May 3, Gavi, the Vaccine Alliance announced that it finalized an advance purchase agreement with Moderna for 500 million doses of its SARS-CoV-2 vaccine to be distributed through the COVAX facility. The agreement will start with 34 million doses in the fourth quarter of 2021, with the remaining doses delivered in 2022. The WHO issued an Emergency Use Listing (EUL) for the Moderna vaccine on April 30, the fourth SARS-CoV-2 vaccine to receive an EUL*. The EUL will facilitate many countries’ efforts to “expedite their own regulatory approval” for the vaccine, and it enables the vaccine to be distributed by COVAX. Additionally, Moderna announced that it is scaling up its production capacity at its Massachusetts (US) facility, with the goal of increasing output by 50% by early 2022, and it revised its 2021 production forecast from 800 million to 1 billion doses. Moderna also is increasing production capacity across its partner facilities, which could increase global production capacity to 3 billion doses per year in 2022.
*The WHO has issued 5 EULs, but 2 of them apply to the AstraZeneca-Oxford vaccine.
COVID-19: VASCULAR DISEASE The spike protein of SARS-CoV-2 helps the virus latch onto and invade healthy cells. It also plays a key role in damaging vascular endothelial cells, according to a study published in Circulation Research. The findings show COVID-19 is a vascular disease and provide a clear link to disease processes that lead to blood clots and stroke, researchers from the Salk Institute and colleagues said. Notably, this is the first research to show the spike protein causes damage on its own, without viral replication. The researchers hope the findings can lead to more effective therapies to interrupt the spike protein’s mechanisms for damaging cells.
INCARCERATED POPULATIONS & VACCINATION As we have covered previously, incarcerated populations are at elevated risk for both SARS-CoV-2 infection and severe COVID-19 disease and death. But as vaccination efforts expand in the US, it is unclear when or how people who are incarcerated will be vaccinated, particularly considering that many states did not include these populations as a priority for vaccination. A commentary published in the New England Journal of Medicine calls for increased attention and priority for vaccinating these populations as well as decarceration to mitigate COVID-19 risk. The authors assert that while vaccination is critical to protecting incarcerated individuals, it may not necessarily be enough. Incarcerated populations are at increased risk for transmission—approximately 5.5 times the risk of infection compared to the general public—and even a high-efficacy vaccine, such as those available for SARS-CoV-2, may not provide sufficient protection to contain outbreaks. In order to effectively contain COVID-19 in incarcerated populations, the authors call for increased decarceration efforts in combination with vaccination. Decarceration could include releasing individuals who do not pose public safety risks, increasing the use of home confinement, reducing the use of pretrial detention, and increasing the use of noncarceral alternatives for individuals whose alleged offenses do not represent “ongoing threats to public safety.”
OLYMPICS The 2020 Summer Olympic Games in Tokyo, Japan, have been surrounded with controversy, but also with innovation, as their start date rapidly approaches in July. With the prospect of tens of thousands of Olympic athletes and team members entering the country, the Japanese public has expressed concerns over holding the Games. A recent public opinion poll showed that 80% of the Japanese public wanted the Games to be either postponed or canceled, as the country undergoes a renewed surge in COVID-19 cases and an increase in COVID-19-related deaths. On April 23, the Japanese government declared its third state of emergency for the Tokyo region. Hospitals and ICU beds are at some of their highest occupancy levels in months. With this backdrop, many are skeptical about the ability of the International Olympic Committee (IOC) to ensure the safety of athletes and the surrounding community.
While some experts argue that it is possible to hold mass gathering events during COVID-19 by following strict precautions, it is unclear whether the Games will be able to meet these requirements. Underlining the public’s reluctance to host the Games, a call from Tokyo Olympic organizers for the Japanese Nursing Association to recruit 500 nurses to volunteer at the event was met with harsh rebukes by Japanese nurses who say they already are desperately needed in their own hospitals and healthcare facilities. Apart from volunteer medical personnel, the corps of 78,000 Olympic volunteers is concerned that they will not be able to enforce safety measures to the levels needed or that they themselves could transmit SARS-CoV-2 to the athletes within the Olympic bubble. While athletes and other Olympic staff will be ordered to remain within the Olympic bubble and undergo daily testing, volunteers must pass in and out of the bubble daily and might not be subject to tests. The IOC remains undecided about whether to allow Japanese spectators into the Games, but a decision is expected to be made in June.
by MJ2004US backs plan to suspend Covid vaccine patents during pandemic
Move to rip up intellectual property rights prompts sell-off in jab maker shares
The US has backed a temporary suspension of intellectual property rights for Covid-19 vaccines in a move likely to enrage the pharmaceutical industry, which strongly opposes a so-called waiver.
Joe Biden’s top trade adviser Katherine Tai said that while the US administration “believes strongly” in IP protections, it would support a waiver of those rules for vaccines.
“This is a global health crisis, and the extraordinary circumstances of the Covid-19 pandemic call for extraordinary measures,” Tai said in a statement.
Shares of the major coronavirus vaccine companies were hit by the announcement on Wednesday. Moderna, BioNTech and Novavax’s shares fell by between 5 and 7 per cent in New York trading, while Pfizer’s stock price fell by almost 1 per cent before recovering.
The companies did not immediately respond to request for comment.
A measure to allow countries to temporarily override patent rights for pandemic-related medical products was proposed at the World Trade Organization by India and South Africa in October, and has since been backed by almost 60 countries.
Donald Trump’s administration firmly opposed the waiver at the WTO, along with the UK, EU and Switzerland, but Tai had rattled US pharmaceutical companies by putting that position under review.
Tai said the US would “actively participate” in text-based negotiations at the WTO, but that those negotiations would take time given the consensus-based nature of the institution and the complexity of the issues involved.
“As our vaccine supply for the American people is secured, the administration will continue to ramp up its efforts — working with the private sector and all possible partners — to expand vaccine manufacturing and distribution,” Tai said.
“It will also work to increase the raw materials needed to produce those vaccines,” she added.
Tai and her staff have in recent weeks discussed the WTO’s IP rules with the chief executives of pharma companies and vaccine makers, trade unions, advocacy groups and Seth Berkley, chief executive of the UN-backed vaccine alliance Gavi.
In a speech to a WTO meeting on vaccine equity earlier this month, Tai said that both the government and the private sector would need to do their part to “live up to” the “spirit” of the Trade-Related Aspects of Intellectual Property Rights (Trips) agreement, which was born out of the HIV crisis.
Gregg Gonsalves, assistant professor of epidemiology at the Yale School of Public Health, welcomed the announcement on Wednesday as “a start”.
He added: “We need the writing of the text of this waiver to be transparent and public. But as we have always said we need tech transfer now and the US to use the $16bn already appropriated in the American Rescue Plan to lay the groundwork for international and domestic scale-up of manufacturing. There is no going back.”
Earlier this week, Anthony Fauci, the president’s chief medical adviser, said he was “agnostic” on the question of whether there should be a waiver, but warned of the political implications of backing such a move.
He said: “Going back and forth, consuming time and lawyers in a legal argument about waivers — that is not the endgame. People are dying around the world and we have to get vaccines into their arms in the fastest and most efficient way possible.”
His comments provoked a backlash from Biden’s liberal supporters however, especially when he was questioned by the journalist Mehdi Hasan on his online television show.
Saikat Chakrabati, president of the leftwing think-tank New Consensus, responded to Fauci’s comments in a tweet: “Waiving Covid patents is in no way mutually exclusive with giving vaccine doses to countries now.”
He added: “You don’t get the privilege of being ‘agnostic’ when you are the chief medical adviser to the president. There is no such thing as agnostic. Agnostic means doing the status quo, which is itself a decision.”
-FT
by mmmm8
ponchi101 wrote: ↑Tue Apr 27, 2021 9:03 pm
Oh, yeah, EU. This is the best moment to sue a large pharmaceutical company, just when you need people to have confidence in what they do. Not myopic at all.
---0---
GF and I went to get our INFLUENZA vaccines today. But, as our lucky streak continues, we were told that, as there have been no studies of how the INF vaccine interacts with the COVID vaccine, if we got our flu shots we would have to wait at least 60 days before being eligible for the COVID one.
Since we "know" we will not die of INF, we bailed.
AITA?
Here as well, one of the pre-requisite to getting the vaccne is to not have had any other vaccine, including flu shots recently. Through all the screenings I'd gone through to get the two shots, most asked if I'd had other vaccines withing 14 days and one asked 30 days
by MJ2004 A largely symbolic effort?
Moderna CEO ‘didn’t lose sleep’ over US backing of patent waiver
Chief of vaccine maker says relaxing protections ‘will not help’ boost Covid jab supplies
The chief executive of Moderna said he “didn’t lose a minute of sleep” following the US government’s decision to support the suspension of Covid-19 vaccine patents, a move that stunned the pharmaceutical industry.
The Biden administration said on Wednesday it would support the temporary waiver of the patents, a step that had been opposed by many in the industry who said suspending intellectual property rights for the jabs set a dangerous precedent and risked halting innovation in the sector.
But Stéphane Bancel, Moderna’s chief executive, said he believed “it doesn’t change anything for Moderna,” during a call with analysts on Thursday to discuss the company’s first-quarter results.
He argued that there were not enough production sites or skilled workers to be able to rapidly increase the supply of mRNA vaccines such as Moderna’s, and that focusing efforts on expanding manufacturing within companies that already had the technology and knowledge was the fastest and most effective way to supply the world with mRNA jabs.
“There is no idle mRNA manufacturing capacity in the world. This is a new technology, you cannot go hire people who know how to make mRNA — those people don’t exist,” Bancel said.
He added that the patent waiver “will not help supply more mRNA vaccines to the world any faster in 2021 and 2022”, the most crucial period of the pandemic.
“If you were to start today, you’re going to have to start by hiring people. Those vaccines don’t fall from the sky,” Bancel told the FT US Pharma and Biotech Summit later on Thursday. “There is no mRNA industry . . . When we hire people that come from traditional pharma, we have to train them in the art of mRNA.”
The Moderna and BioNTech/Pfizer jabs are made with mRNA, a sequence of genetic code that instructs the body’s immune system to fight infection. The technology had never before been used in a vaccine. By contrast, the Johnson & Johnson and Oxford/AstraZeneca shots use an adenovirus to deliver the vaccine into the body.
Morgan Stanley analysts said they “do not see significant practical implications” from the IP waiver, since they believed the World Trade Organization had no power to force Moderna to teach other manufacturers how to make the vaccine, “suggesting no change to the status quo”.
Moderna’s shares fell 10 per cent on Thursday, despite reporting its first-ever quarterly profit, but had recovered by midday to trade about 2 per cent lower.
The company sold $1.7bn worth of Covid vaccines in the first three months of the year, and said it would apply to US health agencies for full approval of its jab this month.
The drugmaker said total revenues surged to $1.9bn in the first quarter as it sold 102m doses of its two-dose shot. It reported net income of $1.2bn compared with a loss of $124m in the same period a year ago.
Moderna also said results from its phase 2/3 vaccine trial on children aged 12 to 17 showed 96 per cent efficacy. The trial on 3,235 participants elicited no serious side effects, it said.
The trial results came as countries sought to expand their vaccine programmes to younger age groups. The BioNTech/Pfizer vaccine was authorised for use on 12 to 15-year-olds in Canada on Wednesday, the first country to approve a coronavirus jab for children.
Moderna is likely to benefit from the need for booster shots to tackle emerging variants of coronavirus in the years to come and Bancel emphasised the demand from governments for boosters. The drugmaker has expanded its capacity to manufacture up to 3bn vaccine doses in 2022.
A new variant has already fuelled a disastrous wave of the virus in India, which has registered more than 20m cases, pushing health systems to the brink of collapse.
The company said that a single 50mg booster shot in people who were already vaccinated had proved to be effective against the original virus and the variants first detected in South Africa and Brazil.
Bancel told the FT that governments that had bought doses of adenovirus-based vaccines were looking to use mRNA vaccines for boosters because mRNA jabs had proved to be more effective.
Moderna said it had so far signed vaccine contracts worth an expected $19.2bn in total revenues for 2021 and that it expected to deliver up to 250m doses in the second quarter.
Switzerland on Thursday became the latest country to order booster shots from Moderna, signing up for 7m doses in 2022 and an option for an additional 7m doses to be delivered by at least the first quarter of 2023.
-FT
by Suliso
MJ2004 wrote: ↑Thu May 06, 2021 5:04 pm
A largely symbolic effort?
He argued that there were not enough production sites or skilled workers to be able to rapidly increase the supply of mRNA vaccines such as Moderna’s, and that focusing efforts on expanding manufacturing within companies that already had the technology and knowledge was the fastest and most effective way to supply the world with mRNA jabs.
“There is no idle mRNA manufacturing capacity in the world. This is a new technology, you cannot go hire people who know how to make mRNA — those people don’t exist,” Bancel said.
He added that the patent waiver “will not help supply more mRNA vaccines to the world any faster in 2021 and 2022”, the most crucial period of the pandemic.
Of course, isn't that obvious to absolutely everyone familiar with a pharmaceutical and chemical industry? I've been writing the same here for some time...
Of course, isn't that obvious to absolutely everyone familiar with a pharmaceutical and chemical industry? I've been writing the same here for some time...
A forum with 200 members, of which only 25 show up with any frequency.
We are informed of these issues thanks to you. I had to explain to one lady here at my building that the vaccine was an mRNA vaccine, as she thought it was the old fashion way of "weakened" viruses. Of course, mRNA went over her head. Then she wondered what was so hard of making more of these vaccines. I tried again.
Try to explain this to a "Intelligent Design" follower. It is not easy science.
by Suliso
ponchi101 wrote: ↑Thu May 06, 2021 6:28 pm
A forum with 200 members, of which only 25 show up with any frequency.
We are informed of these issues thanks to you. I had to explain to one lady here at my building that the vaccine was an mRNA vaccine, as she thought it was the old fashion way of "weakened" viruses. Of course, mRNA went over her head. Then she wondered what was so hard of making more of these vaccines. I tried again.
Try to explain this to a "Intelligent Design" follower. It is not easy science.
I know... I'm not pointing fingers at anyone in our community anyway. It's more of a general pet peeve of mine. People don't want to spend any time understanding how the world works and what unintended consequences this or that decision might have.
In this particular case pharma companies are a solution not a problem. Fundamental science is mostly done in academia, but they don't manufacture anything nor they should. Applied research and manufacturing expertise is needed to make high complexity products and that is best done by private companies. Lots of people involved (not just CEO's with crazy salaries) and most of them can't afford to work for free. There are plenty of problems in the industry including overcharging for drugs, overprescription and so on, however vaccines are cheap for what they do. 50$ for two doses of the most expensive, about 5$ for a cheaper but not as effective.
What Western governments ought to do is help subsidise this cost for those countries where even this is too much, also pay for extra doctors and distribution networks. In the more medium term incentivize vaccine production regionally by capable pharma partners (for sure there ought to be a big producer in Latin America).
Lastly if it were so easy to make lots of money out of covid vaccines most pharma giants would. In reality only three companies, one large (Pfizer) and two small (BioNTech and Moderna) are profiting in a serious way. The latter two, the real inventors, would go out of business if they couldn't. As for AZ they're selling for no profit and probably now regret being involved since all they've gotten in return is damaged reputation.
What Western governments ought to do is help subsidise this cost for those countries where even this is too much, also pay for extra doctors and distribution networks. In the more medium term incentivize vaccine production regionally by capable pharma partners (for sure there ought to be a big producer in Latin America).
...
I know I am extreme in this position, but L. America simply could not care less about science, so, as far as I am concerned, we can go to hell in that aspect. Western govts could try to subsidize our vaccine production facilities and rest assured, that money would go into some fat cat's pockets. Remember I said this: Colombia has ZERO vaccine production capabilities, not for C19 but for any kind of vaccine because years ago the GOVT decided to drop all support for that sector of health care. All vaccines are purchased from abroad because, I suspect, some people make money from the imports.
So now we are screwed. And this country asked for it.
by ti-amie The sad thing is you can't ignore these idiots because their lies spread so quickly on social media.
by dryrunguy Yet again, I forgot to share the most recent Situation Report distributed on Friday. So it's probably a little out of date. I haven't read it myself, yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 156 million cases and 3.2 million deaths worldwide as of 5:30am EDT on May 7.
India continues to set new global records in terms of total daily incidence. It is currently reporting a 7-day average of nearly 390,000 new cases per day, and it could surpass 400,000 in the next several days. India has reported more than 400,000 new cases on each of the past 2 days, including a new global record of 414,188 on May 6. Among the top 10 countries globally, India is the only one currently reporting increasing daily incidence.
As India’s COVID-19 epidemic continues to surge, Asia is the #1 continent globally in terms of total daily incidence. Countries in Asia are reporting more than 4 times the daily incidence as any other continent. South America and Europe are #2 and #3, respectively, reporting nearly the same daily incidence. North America is reporting slightly more than half of the daily cases in Europe and South America. Countries in Africa and Oceania continue to largely contain their respective COVID-19 epidemics, with approximately 8,500 new cases per day in Africa and 100 in Oceania. On a per capita basis, Asia (107 daily cases per million population) is sitting right at the global average (102). It is not surprising that the global average aligns closely with Asia, considering that the continent represents approximately 60% of both the global population and the current global daily incidence. North America is reporting similar per capita daily incidence, with 104. At 269 daily cases per million, South America’s per capita daily incidence is more than 150% higher than the global average, followed by Europe, with 146 daily cases per million. As with total daily incidence, Africa and Oceania are reporting much lower per capita totals—only 6.4 and 2.6, respectively.
In terms of total cumulative incidence, Europe is still #1 globally, with more than 45 million cases. Asia (42 million) surpassed North America (38 million) on April 26 to become #2, and if it continues on this trajectory, it will soon overtake Europe. South America is #4, with 25 million cases. The epidemics in Europe and North America are both tapering off, while Asia’s and South America’s are still accelerating. There have been 4.6 million cases in Africa and fewer than 45,000 in Oceania. Notably, there are 6 individual countries—the US, India, Brazil, France, Turkey, and Russia—that have each reported more cumulative cases than the whole of Africa. On a per capita basis, North America (#1), Europe (#2), and South America (#3) have all reported 3 times the cumulative global average or more. Asia is #4, but it has reported less than half the global per capita average. Africa has reported 17% of the global average, and Oceania is at 5%.
Global Vaccination
The WHO reported 1.17 billion doses of SARS-CoV-2 vaccines administered globally, including 597 million individuals with at least 1 dose. Our World in Data reported 1.24 billion cumulative doses administered globally. This is an increase of 11% over the previous week, slightly less than the 13% weekly increases exhibited over the previous several weeks. The daily doses administered continues to decrease, down from a high of 20.6 million doses per day on May 1 to 17.4 million—a 16% decrease in just a week. Our World in Data estimates that there are 298 million people worldwide who are fully vaccinated, although reporting is less complete than for other data.
Of the 191 countries and territories reporting COVID-19 incidence data, 125 are reporting data on the number of people who are fully vaccinated. These predominantly represent Europe, North and South America, and South and Southeast Asia. Data are missing for numerous countries in Africa and the Caribbean, Central Asia, and Eastern Mediterranean regions. Other notable countries missing data include Australia and China. In terms of the proportion of the population that is fully vaccinated, Seychelles (61%) has surpassed Israel (59%) as #1 globally. These are the only 2 countries reporting more than 50% coverage. The UAE (39%) is #3, followed by Chile (37%) and Bahrain (33%) to round out the top 5. By region, 5 of the top 10 countries are in Europe, 2 are in the Eastern Mediterranean, and 2 are in the Americas. Seychelles is the only country in Africa. Among the reporting countries, the median coverage is 6.8%, and most countries fall between 1.4% and 13.0%.
UNITED STATES
The US CDC reported 32.4 million cumulative cases and 576,238 deaths. Daily incidence continues to decrease, down to 45,816 new cases per day, the lowest average since October 7, 2020. Daily mortality has increased over the past week or so, up from a recent low of 631 deaths per day on April 27 to 674 on May 4—a 7% increase over that period—before decreasing to 656 on May 5. Over the course of the US epidemic, trends in daily mortality have generally lagged 3-4 weeks behind trends in daily incidence; however, since early April, the trends appear to be slightly disconnected. For example, following the brief surge in daily incidence from mid-March to mid-April, we did not observe a similar surge in mortality, as we would have expected based on historical trends. We will continue to monitor these trends over the coming weeks.
US Vaccination
The US has distributed 325 million doses of SARS-CoV-2 vaccine and administered 252 million doses. Daily doses administered* continues to decrease, down from a high of 3.3 million (April 11) to 2.1 million. Approximately 1.3 million people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 149 million individuals have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 45% of the entire US population and 57% of all adults. Of those, 109 million are fully vaccinated, which corresponds to 33% of the total population and 42% of adults. Among adults aged 65 years and older, progress has largely stalled at 83% with at least 1 dose and 70% fully vaccinated. In terms of full vaccination, 56 million individuals have received the Pfizer-BioNTech vaccine, 45 million have received the Moderna vaccine, and 8.6 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 32.6 million cumulative cases and 580,076 deaths in the US as of 10:15am EDT on May 7.
VACCINE INTELLECTUAL PROPERTY In an historic move, the US government on May 5 announced its support for temporarily waiving intellectual property (IP) rights for SARS-CoV-2 vaccines, vowing to actively participate in negotiations at the World Trade Organization (WTO) on a proposal aimed at increasing vaccine production to reach low- and middle-income countries (LMICs). The administrations of former US presidents have supported patent protections, so the move represents a major shift in US policy and shocked many on both sides of the issue. In a statement, US Trade Representative Katherine Tai said the US government “believes strongly in intellectual property protections,” but its support of a waiver is “in service of ending this pandemic” and will bolster the government’s goal “to get as many safe and effective vaccines to as many people as fast as possible.” US support of a waiver does not mean the measure will pass, as the WTO requires unanimous consent to approve any proposal. The leaders of some countries, including Germany, continue to express opposition, although sentiment appears to be shifting, with Canada and the European Commission voicing support for discussions after initially opposing the proposal. WTO Director-General Ngozi Okonjo-Iweala welcomed the US government’s willingness to participate in negotiations on the body’s Trade-Related Aspects of Intellectual Property Rights (TRIPS) agreement. India and South Africa, which have presented the waiver proposal 10 times previously, signaled they will revise the plan prior to another discussion later this month and a formal meeting of the TRIPS Council scheduled for June 8-9.
Even if WTO members adopt the proposal, an increase in vaccine production is not guaranteed. Experts note that several steps need to happen in order for countries to be able to produce generic versions of the vaccines safely and effectively. If IP rights are waived, countries would have to remove any national-level policies hindering generic production; pharmaceutical companies and manufacturers would need to transfer technologies and know-how; massive investments in manufacturing capacity would need to occur; and finally, plans to equitably distribute the vaccines would need to be developed and implemented.
Essentially, waiving IP rights might provide the recipe for vaccines, but having a recipe does not mean the end result will be successful without properly trained workers, raw ingredients, equipment, supplies, knowledge, and funding. And without full support from the pharmaceutical industry, whose lobbying organization opposed the US’s move, the issue could become wrapped up in litigation, preventing any of the next steps from happening, some experts warn. IP rights are simply one obstacle to increasing SARS-CoV-2 vaccine supply. Reportedly, Moderna in October 2020 vowed it would not enforce any of its Covid-19-related patents during the pandemic, but it’s unclear whether anyone has reproduced the company’s vaccine, underlining the difficulties in boosting global manufacturing capacity.
PFIZER-BIONTECH VACCINE EUA & FULL APPROVAL APPLICATION Following reports that the US FDA is expected to soon issue an Emergency Use Authorization (EUA) for the Pfizer-BioNTech SARS-CoV-2 vaccine in children aged 12-15 years, new reports are emerging that Pfizer is expected to apply for an EUA for younger children as well as full approval in adults. During a quarterly earnings call this week, Pfizer officials indicated that the company intends to apply for an EUA for children aged 2-11 years in September. Pfizer also anticipates applying for full FDA approval for the vaccine in individuals aged 16-65 years later this month. Full approval could facilitate businesses, schools, and other organizations mandating vaccination, but the extent to which this will happen remains uncertain. Pfizer’s chief scientific officer discussed the potential for a third dose of the company’s vaccine, suggesting populations at higher risk of COVID-19 disease or complications, including the elderly or those with chronic medical conditions, should be the first to receive any authorized booster shots, although that recommendation would be made by the US CDC. At least one study supports the theory that neutralizing antibodies following vaccination might not develop as robustly or could wane more quickly among older populations (>80 years old).
In addition to the FDA applications, Pfizer expects to have clinical trial safety data for pregnant people available by August. The vaccine’s current EUA does not explicitly omit pregnant people, but initial clinical trials were not designed to collect data on that population. Currently available clinical trial data do not indicate any safety concerns for pregnant people or their infants. Existing CDC guidance states that pregnant people can receive a SARS-CoV-2 vaccine, noting they are at elevated risk for severe COVID-19 disease and death and that the disease might put them “at increased risk of adverse pregnancy outcomes, such as preterm birth.”
On May 5, Canada became the first country to authorize the use of a SARS-CoV-2 vaccine in children. Health Canada authorized the Pfizer-BioNTech vaccine for use in children aged 12-15 years.
INDIA With India continuing to set devastating milestones during its 8-week-long second pandemic wave, the country’s Supreme Court on May 5 ordered the government to provide more medical oxygen to hospitals in New Delhi, after 12 COVID-19 patients died when a hospital ran out of oxygen. The government, under pressure to more quickly distribute supplies coming from other countries, agreed to increase the capital city’s medical oxygen supply from 490 tons per day to 730 tons per day. The Supreme Court also reportedly urged the government to prepare for a third wave of outbreak, and the nation’s principal scientific adviser also warned of an “inevitable” third wave, although he did not discuss timing. Assistance from other nations continues to pour into the country, with Pfizer and partners this week offering to supply more than US$70 million worth of medicines, including steroids, anticoagulants, and antibiotics. Though the government opened the nation’s vaccine program to all adults on May 1, supply shortages are hindering progress, exacerbating concerns among experts that the current surge will continue unabated without increased implementation of lockdowns at the state or federal levels.
India’s outbreak now is spilling over to neighboring countries, like Nepal, which is logging record numbers of new daily cases. The national positivity rate is reported to be 47%, with rates even higher in some areas.
THAILAND Thailand is struggling with a third wave of COVID-19, reporting more than 2,000 new cases a day recently. More than half of the 78,855 cases recorded by the Centre for COVID-19 Situation Administration have been confirmed since April 1. The latest surge is reported to have begun in bars and nightclubs in Bangkok and spread to the Klong Toey area, where about 100,000 people live in a 1 square mile area. Healthcare workers in the area are working to vaccinate up to 3,000 people a day to curb the virus’s spread. Nearly 2% of Thailand’s nearly 70 million people have received at least one dose of vaccine. Following reports that the more than 2.5 million foreigners from other countries who live in Thailand would be last in line to receive vaccinations, the director-general of Thailand’s Department of Disease Control on May 6 clarified that foreigners and diplomats will have the same criteria as Thais in order to receive a vaccine. Thailand has authorized SARS-CoV-2 vaccines from J&J-Janssen, AstraZeneca-Oxford, and China’s Sinopharm, but only the latter 2 are currently being administered.
WHO PANDEMIC INTELLIGENCE HUB The World Health Organization and Germany will establish a new hub for pandemic and epidemic intelligence, data, surveillance, and analytics innovation. Called the WHO Hub for Pandemic and Epidemic Intelligence, the global platform will be based in Berlin and incorporate partners from around the world to collaborate, share data, and develop tools that countries can use to prepare, detect, and respond to pandemic and epidemic threats. The hub was created as part of WHO Health Emergencies Programme to increase data availability, develop tools and models for risk assessment, and monitor disease control measures worldwide. The hub also will provide public health experts and policymakers with relevant information to support their work and aid in the rapid decision making process that is critical for prevention and response to public health emergencies. Germany has provided start-up costs for the hub, but efforts to collect additional funding are ongoing.
VACCINES & VARIANTS OF CONCERN The emergence of SARS-CoV-2 variants, particularly those that exhibit increased transmissibility or disease severity, are causing concern regarding the efficacy of existing vaccines, which were developed based on earlier strains of the virus. Recent data provide further evidence that existing vaccines do provide protection against some variants of concern (VOCs), including real-world data from mass vaccination campaigns. A study published in The Lancet utilized data from more than 4.7 million individuals in Israel who were fully vaccinated using the Pfizer-BioNTech vaccine. Overall, the vaccine showed 95.3% effectiveness against infection among people who were fully vaccinated, defined in the study as 7 days or longer after the second dose. Among a subset of nearly 8,500 specimens with the spike gene target failure (SGTF), which is used to identify B.1.1.7 infections, the vaccine demonstrated 94.5% effectiveness against infection for fully vaccinated individuals. Data from 74,000 fully vaccinated individuals in Qatar, published in the New England Journal of Medicine, demonstrate 89.5% effectiveness for the Pfizer-BioNTech vaccine against infection with the B.1.1.7 variant—at 14 or more days after the second dose—but only 75.0% against the B.1.351 variant. Notably, the vaccine demonstrated 100% effectiveness against “severe, critical, or fatal disease” for both variants.
To increase protection against VOCs, some manufacturers are developing and evaluating booster doses. Moderna published, via press release, positive preliminary results from a Phase 2 clinical trial. The trial involves administering a third dose to fully vaccinated individuals, approximately 6-8 months after their second dose, using either the existing vaccine or a variant-specific version. The researchers identified increased neutralizing antibody response against the B.1.351 variant for both versions of the third dose, with higher antibody titers for the variant-specific version. Moderna also is testing a third option, a 50/50 multivalent mix of the standard and variant-specific vaccines. Moderna committed to publishing the full data via a peer-reviewed journal once the completion of the multivalent arm of the trial.
Novavax, developer of another mRNA-based SARS-CoV-2 vaccine, published preliminary findings from its Phase 2 clinical trial in NEJM. The study demonstrated 60.1% efficacy against symptomatic COVID-19 among adult participants who were HIV-negative and seronegative for SARS-CoV-2. Overall, among HIV-negative and medically stable HIV-positive participants, the vaccine demonstrated 49.4% efficacy. Notably, the study was conducted in South Africa, and the B.1.351 variant represented 93% of the sequenced specimens. In post hoc analysis, the vaccine demonstrated 51% efficacy against the variant. As Novavax proceeds with Phase 3 clinical trials, it will include up to 3,000 children aged 12-17 years.
IMPACT OF VACCINATION COVERAGE Researchers at several US universities and the Johns Hopkins Center for Health Security adapted a model to project the impact of various timelines and levels of vaccination coverage on COVID-19 incidence and mortality as well as medical costs and productivity losses. The researchers modeled several scenarios, ranging from 10-90% national vaccination coverage and 180-360 days to achieve that coverage, including sensitivity analysis using 50-90% vaccine efficacy to account for varying degrees of real-world vaccine effectiveness. They estimate that even small increases in vaccination coverage could have a major impact in terms of decreasing cumulative incidence and mortality as well as mitigating financial and economic effects. For example, an increase of 1% coverage—in the 40-50% range and on a 270-day timeline—could avert 1.5 million cases and 6,660 deaths and save more than US$600 million in medical costs and US$1.3 billion in productivity losses. Similarly, accelerating the timeline has major effects. Shortening the time to 180 days (ie, by the end of the summer) could prevent 5.8 million cases and more than 25,000 deaths. A shortened timeline also could mitigate US$3.5 billion in medical costs and US$4.3 billion in productivity losses. While the model cannot precisely predict the effects of changes in vaccination coverage or timeline, it illustrates that even minor improvements can have substantial longer-term benefits.
US VACCINATION GOALS & MESSAGING States across the US are preparing for a long SARS-CoV-2 vaccination process, as the demand for vaccines wanes in many regions. Reports show the number of daily vaccinations administered has already fallen by 40% from an earlier peak set in April, as the number of those with interest in getting the vaccine as quickly as allowed dwindles. Earlier this week, the US government set a new goal for COVID-19 vaccinations, aiming to reach 70% of the country’s adult population with at least one dose by July 4th. The government also announced new flexibilities for distributing vaccines to participating agencies and pharmacies in an effort to better match demand and supply. Public health organizations working on vaccine uptake support the focus on a flexible vaccine supply as well as the US government’s signal of greater investment into outreach to help reach underserved communities. Community-based organizations have a more robust understanding of community-specific concerns around the COVID-19 vaccination process and can help identify trusted messengers who may be better positioned to relay vaccine information. Community officials say the government’s increased focus on local efforts will help address current barriers to vaccination, including a lack of materials in different languages, difficulties in scheduling and traveling to appointments, and vaccine hesitancy.
AUSTRALIA & NZ TRAVEL BUBBLE Less than 3 weeks after New Zealand and Australia implemented a “travel bubble” allowing residents from each country to travel to the other without having to enter a mandatory quarantine period, New Zealand officials on May 6 announced a temporary pause to the plan. The lead of New Zealand’s COVID-19 response, Chris Hipkins, announced a 48-hour suspension of flights from New South Wales, the region that is home to Sydney, where officials are investigating the source of 2 COVID-19 cases. The pause on travel does not restrict flights leaving New Zealand headed to Australia.
VACCINE DONATION FOR OLYMPIC DELEGATIONS On May 6, Pfizer and BioNTech announced they will donate SARS-CoV-2 vaccines to all Olympic and Paralympic delegations planning to attend the rescheduled 2020 Summer Olympic Games in Tokyo, Japan. The announcement, welcomed by the International Olympic Committee (IOC), comes as many countries are struggling to obtain enough vaccine doses for their populations. Even Japan is grappling with low vaccination rates, trailing behind many of its economic counterparts, with only 1-2% of its population fully vaccinated. Today, Prime Minister Yoshihide Suga pledged to speed up vaccinations to Japan’s older populations, setting a daily target of 1 million shots and aiming to have the nation’s 36 million elderly fully vaccinated by the end of July. Polling shows that most Japanese favor cancelling or postponing the Olympic Games, and social and political tensions are increasing throughout the country. Prime Minister Suga also announced an extension and expansion of a third state of emergency declaration for Tokyo and several other areas through May 31. He maintained the Olympics can be held safely and securely, despite public sentiment.
by mmmm8 Ponchi/anyone - Can confirm both in residency is no longer required in New York City to get vaccinated, just show up with any official ID. Some Colombian colleagues have traveled here for vaccines. (Another one is travelling to MIami).
by ti-amie
by dryrunguy Here's the latest Situation Report. The paragraph on mental health is interesting though not one bit surprising.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 159 million cases and 3.3 million deaths worldwide as of 4:45am EDT on May 11. The global weekly incidence declined for the first time since early-to-mid February, a decrease of 5% compared to the previous week. Global weekly mortality decreased as well—the first time since early March—down 4% from the previous week. Notably, the weekly incidence decreased in every region with the exception of South-East Asia, and weekly mortality decreased except in South-East Asia and the Western Pacific.
It appears that India’s second COVID-19 wave is peaking. On May 7, India’s average daily incidence decreased for the first time since mid-February, and it decreased for the past 2 days, down to 387,098 new cases per day. Unless India’s daily incidence decreases dramatically, however, we expect it to surpass 25 million cumulative cases in the next 5-6 days. India has reported 249,992 cumulative deaths, and we expect it to pass 250,000 in its next report. Additionally, India reported more than 4,000 deaths on both May 7 and 8. To our knowledge, India is only the third country, after the US and Brazil, to report more than 4,000 deaths in a single day. India’s daily mortality continues to increase, but it appears it may have passed an inflection point over the past week. Based on historical trends, we expect daily mortality to peak in the next 3-4 weeks.
Global Vaccination
The WHO reported 1.21 billion doses of SARS-CoV-2 vaccines administered globally, including 606 million individuals with at least 1 dose. Our World in Data reported 1.32 billion cumulative doses administered globally. This is an increase of 12% over the previous week, slightly less than the 13% weekly increases over the previous several weeks. After a week of declining daily doses administered, the trend is once again increasing, back up to 19.6 million—5% less than the record high (20.67 million on May 1). Our World in Data estimates that there are 319 million people worldwide who are fully vaccinated, corresponding to approximately 4% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.5 million cumulative cases and 578,945 deaths. Daily incidence continues to decrease, down to 38,678 new cases per day, the lowest average since September 16, 2020. On May 9, the US reported just 24,080 new cases, the lowest single-day incidence since June 17, 2020 (23,984). In the period between the first and second surges in the US, the lowest average daily incidence was 34,666 new cases per day. If the US continues on its current trajectory, daily incidence could soon fall below that number. Daily mortality is declining slowly, down to 608 deaths per day. With the exception of holiday reporting anomalies, this is the lowest average since April 2, 2020, early in the first surge.
The CDC categorizes states by Level of Community Transmission—Low, Moderate, Substantial, and High—based on the current average per capita weekly incidence and test positivity. The 4 categories for weekly incidence are 0-9.99, 10-49.99, 50-99.99, and 100 or more new cases per 100,000 population, and the categories for test positivity are 0-4.99%, 5-7.99%, 8-9.99%, and 10% or higher*. If the categories for a given state differ between the 2 metrics, the CDC classifies the state at the higher of the 2 categories. Overall, the CDC classifies the national epidemic as Substantial community transmission, with 81.6 weekly cases per 100,000 population and test positivity of 4.09%. In total, 9 states are classified as Moderate transmission, 27 (and Washington, DC) are Substantial, and 14 are High. No states are classified as Low. Unlike earlier in the US epidemic, there does not appear to be a strong geographic correlation.
*The CDC only reports state-level test positivity as 0-5% and 6-10%, so it is unclear exactly which category states fall into for that part of the assessment.
Alabama is reporting the lowest per capita weekly incidence, but at 29.5 weekly cases per 100,000, it is still well above the Low category threshold. Alabama is the only state in the Moderate category currently reporting 6-10% test positivity, so while we can infer that it is less than 8% because of the Moderate classification, it would also need to bring that down below 5% before it could achieve the Low classification. Notably, only 10 total states are reporting test positivity of 6-10%, and none are reporting higher than that. Three states in the High category—Indiana (105.0), North Carolina (105.4), and North Dakota (100.1)—are reporting fewer than 110 weekly cases per 100,000, so they could potentially transition in the near future. Among the 27 states currently classified as Substantial, 7 (and Washington, DC) are reporting fewer than 60 weekly cases per 100,000, including Texas and Washington, DC, that are within 10% of the Moderate category threshold. A
US Vaccination
The US has distributed 330 million doses of SARS-CoV-2 vaccine and administered 262 million. Daily doses administered* continues to decrease, down from a high of 3.3 million on April 11 to 2.0 million. Approximately 1.3 million people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 152 million individuals have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 46% of the entire US population and 58% of all adults. Of those, 116 million are fully vaccinated, which corresponds to 35% of the total population and 44% of adults. Among adults aged 65 years and older, progress has largely stalled at 84% with at least 1 dose and 72% fully vaccinated. In terms of full vaccination, 60 million individuals have received the Pfizer-BioNTech vaccine, 47 million have received the Moderna vaccine, and 9.0 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
PFIZER-BIONTECH EUA FOR ADOLESCENTS The US FDA on May 10 expanded the Emergency Use Authorization (EUA) for the Pfizer-BioNTech SARS-CoV-2 vaccine to include adolescents ages 12 to 15, making it the first such vaccine available to children under age 16 in the US. The amendment to the original EUA is based on Phase 3 clinical trial results showing the vaccine is safe and effective among that age group. The US CDC Advisory Committee on Immunization Practices will meet on May 12 to review the data on use among 12- to 15-year olds and is expected to recommend the vaccine be used in this age group. Pfizer-BioNTech are testing the vaccine among children aged 2 to 11 and plan to include children aged 6 months to 2 years in the coming weeks. Moderna and J&J-Janssen also are testing their vaccines in children.
On May 7, Pfizer-BioNTech announced they have begun a Biologics License Application with the FDA for full regulatory approval of their SARS-CoV-2 vaccine for individuals ages 16 years and older. The companies will submit data to support the application on a rolling basis, with a goal of achieving full approval in the coming months.
US CDC TRANSMISSION GUIDANCE On May 7, the US CDC issued a Scientific Brief on SARS-CoV-2 transmission and updated its associated guidance. Notably, the brief describes respiratory fluid as existing along a “spectrum of sizes,” rather than distinguishing between droplets and aerosols. The CDC emphasizes the role that the volume of exposure plays in transmission risk, including the “concentration of virus in the air” and its viability. The guidance notes that transmission risk is the greatest at close proximity to infectious individuals and that the concentration of virus generally “decreases with increasing distance.” The agency concluded certain conditions can increase the risk of infection at longer distances, including enclosed spaces with inadequate ventilation, increased exhalation rates (e.g., when exercising or singing), and prolonged exposure (e.g., more than 15 minutes). The brief emphasizes that exhaled viruses in the air—whether via inhalation or contact with mucous membranes like the eyes, nose, or mouth—remains the greatest transmission risk, and while fomites do pose some risk, they are not a substantial driver of transmission.
The updated guidance does not explicitly distinguish between droplet (i.e., via small respiratory droplets at close distance) and airborne transmission (i.e., via aerosolized respiratory fluid that can remain aloft for longer periods of time and travel longer distances). Previous iterations of the guidance included separate sections for droplet and airborne transmission, describing droplet transmission as more likely than airborne. The new guidance removes any mention of aerosols and airborne transmission entirely. Instead, the CDC discusses them together, as “droplets and very small particles.” Additionally, the CDC removed the term “close contact” and shifted the focus to the type of exposure—i.e., inhalation, splashes/sprays to mucous membranes, and touching mucous membranes. While the update is viewed by many as an improvement, some critics are still calling on the CDC to more explicitly address the risk of aerosol/airborne transmission, particularly for prolonged exposure in indoor spaces.
WHO EUL FOR SINOPHARM VACCINE On May 7, the WHO issued an Emergency Use Listing (EUL) for the Sinopharm vaccine for use among adults 18 years and older, the sixth SARS-CoV-2 vaccine to receive an EUL. The vaccine—an inactivated vaccine administered in 2 doses given 3-4 weeks apart—is produced by Beijing Bio-Institute of Biological Products Company Ltd., a subsidiary of China National Biotec Group. The WHO noted the listing of the vaccine included on-site inspections of the production facility. The designation facilitates many countries’ efforts to speed their own regulatory approval of the vaccine and is a prerequisite for the vaccine to be distributed by the COVAX facility. The vaccine’s storage requirements make it well-suited for use in low-income countries, according to the WHO, and its vials will be the first to include a small sticker that changes color when exposed to heat, allowing healthcare workers to know whether the vaccine is safe to use.
According to the WHO’s Strategic Advisory Group of Experts on Immunization (SAGE), more than 65 million doses of the Sinopharm vaccine have been administered worldwide in the 45 countries/jurisdictions with existing authorizations, with an estimated 79% efficacy at preventing symptomatic COVID-19 among adults ages 18-59. However, SAGE experts did not estimate the vaccine’s efficacy among people ages 60 and older. The Sinopharm vaccine reportedly is the first-ever Chinese-produced vaccine to receive WHO emergency authorization, although the agency next week is expected to consider another Chinese SARS-CoV-2 vaccine from the company Sinovac.
ASTRAZENECA-OXFORD VACCINE British officials have recommended that people under 40 be given options other than the AstraZeneca-Oxford SARS-CoV-2 vaccine when available, due to a small risk of blood clots. According to data analysis from the UK Medicines and Healthcare Products Regulatory Agency (MHRA), the risk of these rare adverse events is slightly higher among younger age groups compared to older adults, and there are no known risk factors for the blood clotting events. In an update to guidance released on April 7 recommending individuals under age 30 be offered an alternative to the AstraZeneca-Oxford vaccine when possible and only where no substantial delay or barrier in access to vaccination would arise, the UK’s Joint Committee on Vaccination and Immunisation on May 7 expanded that guidance to adults ages 30-39 who are not at increased risk of COVID-19 complications. MHRA Chief Executive June Raine stressed the benefits of the AstraZeneca-Oxford vaccine continue to outweigh the risks for the vast majority of people. UK public health officials hope to vaccinate the entire adult population by the end of July.
NOVAVAX EUA APPLICATION In quarterly earnings results announced May 10, US-based pharmaceutical company Novavax indicated it does not plan to file for US FDA Emergency Use Authorization for its SARS-CoV-2 vaccine until July at the earliest but expects to have the application process complete in the US, UK, and Europe by the third quarter of 2021. The company could announce safety and efficacy data on the vaccine this month, although manufacturing delays have impacted clinical trial progress. Novavax CEO Stanley Erck said the company hopes to have production slowdowns resolved by the fourth quarter, with plans to produce up to 3 billion doses worldwide next year with partner Serum Institute of India. However, the Serum Institute, the world’s largest vaccine maker, has been unable to deliver on its promises of vaccine production for several companies, including AstraZeneca, which has served the company a legal notice over the delays. These delivery delays are heavily impacting supply to the COVAX facility, which is committed to delivering 2 billion doses of SARS-CoV-2 vaccine to low- and middle-income countries in 2021. On May 6, Gavi, the Vaccine Alliance, one of the co-leaders of COVAX, signed an advance purchase agreement with Novavax for 350 million doses of its vaccine to begin delivery in the third quarter. However, with the Serum Institute saying it has “temporarily deferred” some of its delivery commitments and offering refunds for at least one bilateral purchase agreement, it remains to be seen whether the companies can deliver on their obligations.
SOUTH ASIA India’s second wave remains the most severe COVID-19 situation in the world, although it does appear to be peaking. Amid continued calls on Prime Minister Narendra Modi to reinstitute a nationwide “lockdown,” including from White House Chief Medical Advisor Dr. Anthony Fauci, some states are implementing their own restrictions. Reportedly, approximately half of India’s states have implemented a full “lockdown,” and the rest have implemented varying degrees of restrictions.
Neighboring Nepal also is facing its largest COVID-19 surge on a similar trajectory to India’s. Notably, Nepal’s daily incidence has surged from 500 new cases per day on April 16 to more than 8,600 on May 10, a 17-fold increase in less than 4 weeks. Much like India, Nepal’s health system is struggling to manage the wave, so much so that the Ministry of Health issued a statement indicating that it was “losing control of the situation.” Perhaps the most concerning aspect of the current surge is Nepal’s high test positivity. Since mid-March, test positivity surged from 2% to 45%, which indicates that testing is not sufficient to fully capture the scope of the epidemic and that the reported incidence likely is well below the actual total.
Bangladesh, another of India’s neighbors, recently detected its first cases of COVID-19 caused by an emerging SARS-CoV-2 variant first reported in India. The B.1.617 variant is characterized by 3 mutations that are believed to confer increased transmissibility and resistance to existing vaccines. On May 10, the WHO announced that it classified B.1.617 as a variant of concern, although the US CDC still classifies it as a variant of interest. Some preliminary research (preprint) provides some evidence that the B.1.617 variant exhibits “reduced neutralization” to existing vaccines, but further study is needed to more fully characterize the variant’s attributes.
MORTALITY DUE TO COVID-19 As we have covered previously, limitations in public health surveillance and reporting can result in an undercount of COVID-19 deaths. The Institute for Health Metrics and Evaluation recently shifted its modeling approach to use total mortality due to COVID-19, as opposed to official COVID-19 mortality reports. The new approach accounts for historical seasonal fluctuations as well as temporal and geographic variations in testing capacity and reporting. It also takes into account the early months of the pandemic, when a higher proportion of deaths or cases were uncounted, and because of the disproportionate impact on long-term care facilities, COVID-19-related deaths among older individuals may have been overlooked. Additionally, the model aims to estimate the proportion of excess deaths that are due directly to COVID-19 by accounting for changes in historical trends during the pandemic. In order to do this, IHME researchers consider 6 drivers of all-cause mortality that relate to the pandemic and physical distancing requirements, including increases in mortality due to the reduced utilization of healthcare services for non-COVID-19 conditions, increases in deaths due to mental health disorders and drug use, decreases in reported deaths due to cardiovascular and respiratory diseases and accidental injury, and fewer deaths due to other respiratory illnesses, especially influenza. The new IHME model estimates more than 900,000 total COVID-19 deaths in the US, more than 50% higher than official figures. The estimates for some countries—including Azerbaijan, Belarus, Japan, and Kazakhstan—are more than 10 times the reported total. On a global scale, the model estimates nearly 7 million total COVID-19 deaths, more than double the 3.24 million deaths reported at the time of publication.
MENTAL HEALTH Mental health experts are concerned over potential long-term ramifications of the COVID-19 pandemic on the psychosocial health of people worldwide. For some, prolonged feelings of anxiety or depression, a lack of social connection, job uncertainty, or food insecurity during the pandemic are unlikely to dissipate with the loosening of social restrictions. A disproportionate impact could be seen in some individuals, including LGBTQ+ people or those who experience violence at home, as well as Black, Latinx, and Indigenous communities more heavily affected by the pandemic. Another notable population of interest is children, whose formative years have been upended by the pandemic, resulting in familial socioeconomic stress, delays in learning, and an increase in mental health issues. In the US, pediatric hospitals are reporting higher proportions of emergency department visits for mental health conditions during the COVID-19 pandemic. Although the US$1.9 trillion American Rescue Plan earmarks US$3.5 billion in block grants for states and organizations to address mental health in communities and the workforce, experts warn the funding might not be sufficient to bolster already under-resourced mental health care in the country.
COVID SOLIDARITY TRIAL The WHO Solidarity clinical trial, launched in 2020 to test various medical interventions for COVID-19 disease, is beginning a randomized controlled trial of three immune regulating drugs that have shown promise in smaller studies. These three drugs—infliximab, imatinib, and artesunate—were selected for their abilities to dampen inflammatory immune responses, preliminary positive efficacy against severe COVID-19, and widespread global availability. The Solidarity trial previously evaluated remdesivir, hydroxychloroquine, lopinavir/ritonavir, and interferon, with all having little to no effect in managing patients hospitalized with COVID-19. In addition to the Solidarity trial, another large international study called REMAP-CAP is exploring various ways to control immune responses in COVID-19 patients. Taken together, researchers hope the trials will identify more treatments to provide additional support to hospitalized COVID-19 patients.
MOUNT EVEREST China is implementing strict measures to prevent new COVID-19 cases on the Tibetan side of Mount Everest, known as Mount Qomolangma in China. The peak of the world’s highest mountain straddles the border of China and Nepal at 29,032 feet above sea level, with climbers able to approach from either the northern Tibetan side or southern Nepalese slope. China banned foreign mountaineers last year due to the pandemic, but it has issued 21 expedition permits this year for nationals to attempt to reach the summit from the Tibetan side. To prevent commingling of climbers from each side who reach the small peak on the same day, China plans to establish a “line of separation” near the border as part of its “zero contact strategy,” according to state media. Details of how this will be accomplished are not yet known. Additionally, the China Tibet Mountaineering Association has set up a checkpoint 300 meters from the Tibetan base camp to test anyone with a permit to enter. Nepal is experiencing a surge in COVID-19 cases, and cases have been detected in the main Nepalese base camp. Last week, Nepalese officials reportedly confirmed 18 COVID-19 cases at the base camp, but anecdotal reports say the number could be nearly double. The Nepal Mountaineering Association has asked climbers and their Sherpa guides to return spent oxygen canisters instead of abandoning them on the mountainside so they can be refilled to help alleviate oxygen shortages.
MENTAL HEALTH Mental health experts are concerned over potential long-term ramifications of the COVID-19 pandemic on the psychosocial health of people worldwide. For some, prolonged feelings of anxiety or depression, a lack of social connection, job uncertainty, or food insecurity during the pandemic are unlikely to dissipate with the loosening of social restrictions. A disproportionate impact could be seen in some individuals, including LGBTQ+ people or those who experience violence at home, as well as Black, Latinx, and Indigenous communities more heavily affected by the pandemic. Another notable population of interest is children, whose formative years have been upended by the pandemic, resulting in familial socioeconomic stress, delays in learning, and an increase in mental health issues. In the US, pediatric hospitals are reporting higher proportions of emergency department visits for mental health conditions during the COVID-19 pandemic. Although the US$1.9 trillion American Rescue Plan earmarks US$3.5 billion in block grants for states and organizations to address mental health in communities and the workforce, experts warn the funding might not be sufficient to bolster already under-resourced mental health care in the country.
Due to IT issues my daughter had to go into her office to upgrade her laptop. Everyone had to make an appointment and there were restrictions on how many of them could be there at one time.
I would've said she was coping with the situation despite some hiccups (she is a very social person. Me? I go out when I have to - basic introvert personality). She made her walk through Central Park, took some wonderful nature shots, and went to Starbucks. On her way home she texted that she was so happy.
There are going to be major issues. Gang bangers aren't the only ones who are stressed out.
by atlpam Even being vaccinated, I am still stressed about being in a public indoor space. I hiked with some vaccinated friends last weekend and we decided to have lunch/beer after our hike. It just so happened to coincide with the removal of all spacing restrictions on restaurants & mask use in our state. (We didn't realize that until we were seated). Not long after ordering, one of my friends overheard 2 people at a nearby table discussing one of them thinking she might have Covid and the other telling her where to go for testing. As they had already taken our order, we were fortunate to be able to move to an outdoor table. Otherwise I would have just paid & left. Vaccinated or not, I don't need to put myself at risk because other people are stupid.
by mmmm8
atlpam wrote: ↑Tue May 11, 2021 8:14 pm
Even being vaccinated, I am still stressed about being in a public indoor space. I hiked with some vaccinated friends last weekend and we decided to have lunch/beer after our hike. It just so happened to coincide with the removal of all spacing restrictions on restaurants & mask use in our state. (We didn't realize that until we were seated). Not long after ordering, one of my friends overheard 2 people at a nearby table discussing one of them thinking she might have Covid and the other telling her where to go for testing. As they had already taken our order, we were fortunate to be able to move to an outdoor table. Otherwise I would have just paid & left. Vaccinated or not, I don't need to put myself at risk because other people are stupid.
Now that I'm vaccinated and am feeling safer, I've reached out to some friends about meeting up. It's appalling how many of them haven't gotten vaccinated. No objection to it, just taking their sweet time setting appointments (when you can now make one right before walking in in most locations!)
by ti-amie My daughter had to be masked entering her office building today.
I'm not going anywhere unmasked specifically because of situations like the one @atlpam mentioned.
by Suliso Maybe I'm weird, but I don't feel particularly unsafe even though I'm not vaccinated yet (not possible yet here, hopefully in June). Certainly not when hiking with a friend or two, but also not really when taking a train to work (masked).
by atlpam I don't have any issues when hiking or walking outside - that's been my main stress relieving activity throughout this mess.
The indoor dining still makes me nervous because I don't trust the behavior of the people around me. No issue with grocery stores or similar establishments where the businesses are still requiring masks.
by dmforever
atlpam wrote: ↑Tue May 11, 2021 9:01 pm
I don't have any issues when hiking or walking outside - that's been my main stress relieving activity throughout this mess.
The indoor dining still makes me nervous because I don't trust the behavior of the people around me. No issue with grocery stores or similar establishments where the businesses are still requiring masks.
I ate indoors for the first time last weekend. My dining partner and I had both been vaccinated. Our table was definitely 6 feet from another table. They took people's temperature before letting them in the restaurant, which was at maybe 40% capacity. The door was open. And you had to wear a mask unless you were eating. The wait staff and cooks were masked. I think a lot of it boils down to particular situations.
Kevin
by atlpam Agree, due to removed restrictions, in the restaurant I went to, no one wore masks, separation between tables was back to pre-pandemic layouts.
by Suliso Six feet really makes no difference at all given what we now know about how the virus spreads, same about wearing masks only intermittently. Simply having less people around does decrease odds and of course being vaccinated decrease them vastly. Speaking about indoor places here.
by Suliso For US in particular I think it also matters a lot in which state you are. Those of you in Vermont (62%) or New Hampshire (58%) could already be reaching semi heard immunity there as if you live in Mississippi (32%) you're nowhere close.
by Suliso As for us we're at 25% (at least one dose) and increasing at a rate of about 4% population per week. I think I can start expecting an appointment when we reach 35%.
by Deuce
Suliso wrote: ↑Tue May 11, 2021 10:17 pm
Six feet really makes no difference at all given what we now know about how the virus spreads, same about wearing masks only intermittently.
This article/study agrees.
Frightening stuff, and definitely worth reading...
by ponchi101 Totally on the money, but if the guideline had been 60 feet, you basically could only have one person per ambience anywhere in the world.
The only way my GF and I can be 60 feet apart at our place is if I open the window panes and I stand in the garden, while she stands at the door of our apartment.
Pretty good study. No wonder all these measures have had so little success.
by Suliso It's not all hopeless. Good ventilation helps a lot.
by ponchi101 Agree. I said that last year. Negative pressure systems should have been engineered during these 15 months of pandemic. Extract systems installed. This is not going away just yet.
In places like Colombia, where we don't have to deal with extreme temperatures, fans moving the air out could have helped.
---0---
True story. I have my GF to vouch for me. Last year, as this started, I thought of designing an app. Voluntary reporting by people with symptoms, so you could track where you were and if people that had later declared themselves with symptoms or the disease could report themselves. Geolocation could help you make a map. I contacted my GF's cousin, who is very good at programming. She never even replied.
Today we found out that the COL GOV has issued an app that does that, and works with Bluetooth signals, and you are close to somebody with symptoms it will warn you (why somebody with self-reported symptoms would be out is another matter).
So: If PONCHI101 could think of it, it was not that hard. Really.
We need more ideas on how to deal with this, until the vaccines are everywhere.
by Deuce
Suliso wrote: ↑Wed May 12, 2021 1:53 am
It's not all hopeless. Good ventilation helps a lot.
But, for various reasons, good ventilation is not always feasible, unfortunately.
by Deuce I received my first Moderna vaccine yesterday. From the outset, I felt that everyone should be able to choose which vaccine they want - some will take the first one available, regardless of what it is - and that's fine. Others - like me - prefer to do some research and make an educated decision on which vaccine to get. I simply figure that if a foreign material is going to be injected into MY body, I should have the right to decide which it will be - everyone should have that right.
So my goal was to work it so that I had a choice. And I did.
My first option was AstraZeneca - that was available to me about a month ago. I chose not to get it for various reasons... firstly, because both of my parents had a (different) form of blood cancer. In my Mom, it produced too many platelets, which increases the risk of the blood clotting. In my Dad, it robbed his blood of enough platelets.
As well, I don't like some of the things that AstraZeneca has done - playing with the numbers to make it appear that it had a greater efficacy than it actually had (and Dr. Fauci admonished them for doing that)... and changing the name of the vaccine in Europe - as of the end of March, 2021, the AstraZeneca vaccine is called Vaxzevria in most of Europe. This is nothing short of deliberate deception, trying to fool people into thinking that it's not AstraZeneca - because of the bad press they've been getting about the blood clots. I did not want a vaccine from a company whose ethics were this degree of shady. (As a related aside, 3 provinces - thus far - here in Canada have stopped giving AstraZeneca as a first dose.)
Although it's not really public information, my 'research' showed me where the Pfizer and where the Moderna vaccines were being given in my area. I made an appointment to get the Pfizer - simply because a Pfizer appointment was available before a Moderna one. I had also left my name at a pharmacy close to me that I knew had Moderna. They called me just after I had made the Pfizer appointment to offer me an appointment that was 3 days after my other appointment. I said 'OK'. I was surprised that I could have 2 different appointments at 2 different locations - but I did.
I cancelled the Pfizer appointment when I got a rare chance to play pickleball on the same day and time as the appointment (I cancelled the appointment in plenty of time for it to be filled by someone else - and it was filled within 10 minutes of my cancellation).
I had a plan going in to get my Moderna shot: I was going to ask if I could please have the shot in my rear end - just to see what kind of reaction it would provoke (it is a rather large muscle, is it not? - so it's likely feasible). But I forgot that, for some reason, when I got there. Instead, as the nurse was preparing to vaccinate me, I said "Just give me one dose, please." She was puzzled. Then I told her about an article I read the other day that told of a nurse in Italy being distracted and injecting a complete vial - 6 doses - into a woman.
Story here...
I asked the nurse if I could have an empty vial - as a souvenir of these crazy times. She said she cannot give me one, as they go back to Moderna, who re-use them. I doubt very much that they're re-used - I hope they are, as it means much less garbage - but it's highly unlikely.
by mmmm8 Why do you think it's unlikely they're reused? There are severe shortages in manufacturing everything needed for the vaccine supply and glass isn't as cheap or quick as plastic.
I imagine the main reason to no give out the vials is to avoid people having samples to manufacture fake vaccines or use the remaining biological materials in some sort of unauthorized research.
by atlpam
Deuce wrote: ↑Thu May 13, 2021 5:21 am
I received my first Moderna vaccine yesterday. From the outset, I felt that everyone should be able to choose which vaccine they want - some will take the first one available, regardless of what it is - and that's fine. Others - like me - prefer to do some research and make an educated decision on which vaccine to get. I simply figure that if a foreign material is going to be injected into MY body, I should have the right to decide which it will be - everyone should have that right.
So my goal was to work it so that I had a choice. And I did.
My first option was AstraZeneca - that was available to me about a month ago. I chose not to get it for various reasons... firstly, because both of my parents had a (different) form of blood cancer. In my Mom, it produced too many platelets, which increases the risk of the blood clotting. In my Dad, it robbed his blood of enough platelets.
Based on your family history, totally understand your reluctance to get AZ. Congratulations on getting your first dose!
I asked the nurse if I could have an empty vial - as a souvenir of these crazy times. She said she cannot give me one, as they go back to Moderna, who re-use them. I doubt very much that they're re-used - I hope they are, as it means much less garbage - but it's highly unlikely.
mmmm8 wrote: ↑Thu May 13, 2021 11:11 am
Why do you think it's unlikely they're reused? There are severe shortages in manufacturing everything needed for the vaccine supply and glass isn't as cheap or quick as plastic.
I imagine the main reason to no give out the vials is to avoid people having samples to manufacture fake vaccines or use the remaining biological materials in some sort of unauthorized research.
Suliso would be our guide here but most likely they are chemical grade glass, and that is not cheap. Re-cycling would be a very wise investment. I remember that one time I was thinking about replacing all my glassware in my house with chemical beakers (I think they are lovely) and the prices were outrageous. So I would believe the nurse. M's reasoning also holds.
I booked my flight to Atlanta for May 25th. My niece will book me a J&J vaccine, if possible for the same day of our arrival. We will stay 21 days in case we can't get the J&J and will opt for PF/BionTech. She tells me Moderna is completely available in the area.
Here? Chinese Sinopharm. Sorry, I pass.
mmmm8 wrote: ↑Thu May 13, 2021 11:11 am
Why do you think it's unlikely they're reused? There are severe shortages in manufacturing everything needed for the vaccine supply and glass isn't as cheap or quick as plastic.
I imagine the main reason to no give out the vials is to avoid people having samples to manufacture fake vaccines or use the remaining biological materials in some sort of unauthorized research.
Suliso would be our guide here but most likely they are chemical grade glass, and that is not cheap. Re-cycling would be a very wise investment. I remember that one time I was thinking about replacing all my glassware in my house with chemical beakers (I think they are lovely) and the prices were outrageous. So I would believe the nurse. M's reasoning also holds.
I don't know about recycling, but those vials are definitely made of a special type of borosilicate glass similar to chemistry lab glassware. Corning has developed a Valor glass brand for this purpose which is similar to ultra tough glass used on cell phone screens. German company Schott is also a major manufacturer probably using similarly reinforced product. I remember seeing somewhere that you can drop those vials from a third floor height on a concrete floor without breaking them.
As for the cost of beakers (flasks are more expensive) it shouldn't be too expensive, something like 10-50$ per piece depending on size.
by ponchi101 I wanted beakers for drinking glasses. A set of 6 250ML, and 6 500 ML. It was well into the $300 range (I was in Venezuela, where of course everything like this is imported).
Just for vanity glasses, that was too much.
by Suliso
ponchi101 wrote: ↑Thu May 13, 2021 3:06 pm
I wanted beakers for drinking glasses. A set of 6 250ML, and 6 500 ML. It was well into the $300 range (I was in Venezuela, where of course everything like this is imported.
Just for vanity glasses, that was too much.
That sounds expensive albeit you wanted many and rather big. By the way beakers larger than 50 ml are rarely used in the lab these days. Not sure I even have any above 250 ml. Instead we use Erlenmeyer flasks. A large one (1 l) pictured below you can order in Switzerland for ca 15 $, small ones would be 8-10 $.
by Deuce
mmmm8 wrote: ↑Thu May 13, 2021 11:11 am
I imagine the main reason to no give out the vials is to avoid people having samples to manufacture fake vaccines or use the remaining biological materials in some sort of unauthorized research.
I understand that - but I was asking for one vial, not several dozen.
mmmm8 wrote: ↑Thu May 13, 2021 11:11 am
Why do you think it's unlikely they're reused? There are severe shortages in manufacturing everything needed for the vaccine supply and glass isn't as cheap or quick as plastic.
For one: "The two largest issues in process development are sterility and degradants. Reusing old vials fails both of these fronts. After injecting the contents of a vial drug product residue is left behind that can become infested with bacteria. This would need to be cleaned out of the vial, and go through an intense sterilization cycle then be tested. Even after this you would have to verify that there were no trace degradants left behind in the process, as a large portion of pharmaceutical degradants are heat catalyzed the sterilization would induce a worst-case scenario that could provide dangerous levels of degradants that are tightly controlled in the drug. And then after all of that you have to prove vial integrity, and show that the wear and tear on the vial didn’t increase the likelihood of extractables, leachables, and elemental impurities getting transferred into your product.
The FDA maintains tight controls on container closures for a reason, when you overlook small aspects of these controls people are at risk of injury and illness."
by Suliso They might be recycling the glass for making new vials.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 161 million cumulative cases and 3.3 million deaths worldwide as of 6:15am EDT on May 14.
Despite concerns early in the pandemic, African countries have largely managed to contain their respective COVID-19 epidemics, and the continent as a whole has fared better than most others. In terms of total cumulative incidence, South Africa has remained #1 in Africa since March 2020, and its 1.6 million cases ranks #21 globally. Morocco (514,432) and Tunisia (324,103) are a distant #2 and #3 in Africa, respectively, with fewer than one-third the cases reported in South Africa. Only 9 African countries have reported more than 100,000 cumulative cases. In fact, more countries have reported fewer than 10,000 cases (16) than have reported more than 50,000 (14). On a per capita basis, Seychelles is #1 in Africa, with 93,390 cumulative cases per million population. Notably, even with the world’s highest vaccination coverage, Seychelles’ cumulative incidence has more than tripled since early March—from 2,688 cases on March 1 to 9,184 on May 13—its largest surge to date. Cabo Verde (48,614 cases per million population) is #2 in Africa, followed by Tunisia, South Africa, and Libya clumped together at #3-5 (~26-27,000). Botswana (20,854) is the only other African country reporting higher than the global average (20,584). The average across the continent is only 3,474 cases per million population, approximately one-sixth the global average.
As noted above, Seychelles is facing a severe surge, despite its high vaccination coverage. It is currently reporting more than 4,000 daily cases per million population. This ranks #1 globally, and it is more than 8.5 times the per capita daily incidence in Cabo Verde (478; #2 in Africa, #5 globally). Tunisia (94.4) is the only other Africa country reporting higher than the global average (93.6). Notably, the global average is 15 times higher than the continent average (6.2). In terms of total daily incidence, South Africa (2,126 new cases per day) is once again #1, surpassing Tunisia on May 6. On May 13, Egypt (1,158) surpassed Tunisia (1,116) as #2 in Africa. Ethiopia (594) is the only other country reporting more than 500 new cases per day, and all but 13 countries are reporting fewer than 100. Additionally, only 12 countries across the continent are exhibiting growth rates of more than +10% over the past 2 weeks, and all but 14 have negative growth rates over that period.
Overall, African nations have performed better than many expected in terms of limiting the spread of COVID-19. As vaccine production and distribution continue to scale up, it remains critical to ensure global access and increase vaccination coverage in order to provide protection before epidemics have an opportunity to surge, which could threaten many countries’ limited health system capacity and vulnerable infrastructure.
*We included Djibouti, Egypt, Libya, Morocco, Somalia, Sudan, and Tunisia, in Africa, even though they are in the WHO’s Eastern Mediterranean Region.
Global Vaccination
The WHO reported 1.26 billion doses of SARS-CoV-2 vaccines administered globally, including 637 million individuals with at least 1 dose. Our World in Data reported 1.40 billion cumulative doses administered globally, an increase of 13% over the previous week. After a week of declining daily doses administered, the trend increased once again, up to a new record of 22.6 million doses on May 12. Our World in Data estimates that there are 341 million people worldwide who are fully vaccinated, corresponding to approximately 4.4% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.6 million cumulative cases and 580,837 deaths. The United States’ daily incidence (35,442 new cases per day) is at its lowest since mid-September 2020, during the lowest point between the second and third surges. The lowest average during that period was 34,096 new cases per day on September 13, and the US could drop below that number in the coming days. The daily mortality—586 deaths per day on May 11 and 591 on May 12—is at its lowest point since April 1, 2020, early in the country’s first surge.
US Vaccination
The US has distributed 339 million doses of SARS-CoV-2 vaccine and administered 267 million. Daily doses administered* continues to decrease, down from a high of 3.3 million on April 11 to 1.8 million. Approximately 1.3 million people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 155 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 47% of the entire US population and 59% of all adults. Of those, 119 million are fully vaccinated, which corresponds to 36% of the total population and 46% of adults. Among adults aged 65 years and older, progress has largely stalled at 84% with at least 1 dose and 72% fully vaccinated. The CDC added data for individuals aged 12 years and older to its vaccination dashboard, and in total—including individuals aged 16 and 17 who were previously eligible—2.5 million adolescents have received at least 1 dose, and 1.3 million are fully vaccinated. In terms of full vaccination, 61 million individuals have received the Pfizer-BioNTech vaccine, 48 million have received the Moderna vaccine, and 9.3 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 32.9 million cumulative cases and 584,510 deaths in the US as of 10:15am EDT on May 14.
CDC RECOMMENDS PFIZER-BIONTECH VACCINE FOR ADOLESCENTS On May 12, the US CDC’s Advisory Committee on Immunization Practices (ACIP) met to discuss SARS-CoV-2 vaccine recommendations, following the US FDA’s decision to expand the Emergency Use Authorization (EUA) for Pfizer-BioNTech’s vaccine to include adolescents aged 12-15 years. After receiving briefings on relevant safety and efficacy data from recent clinical trials, ACIP members voted unanimously—14-0; 1 recusal by a member who conducted SARS-CoV-2 vaccine clinical trials—to recommend the vaccine’s use for 12-15-year-olds. Later that day, CDC Director Dr. Rochelle Walensky issued a statement announcing that the CDC updated its vaccination guidance to recommend the Pfizer-BioNTech vaccine for children aged 12-15 years. The CDC’s decision makes the vaccine immediately available to children in that age group at all vaccination sites nationwide that offer the Pfizer-BioNTech vaccine. While children tend to experience milder disease than adults, several committee members noted the 127 COVID-19-related deaths among adolescents from January-April 2021 would have placed COVID-19 among the top 10 causes of death for that age group in 2019.
J&J-JANSSEN VACCINE & BLOOD CLOTTING The US CDC has confirmed 28 cases of a rare blood clotting disorder among adults who received the J&J-Janssen SARS-CoV-2 vaccine, all of whom were vaccinated prior to an 11-day pause of the vaccine’s use that began on April 13. During a presentation to the agency’s Advisory Committee on Immunization Practices (ACIP) on May 12, Dr. Tom Shimabukuro, deputy director of the immunization safety office at the CDC, said current evidence “suggests a plausible causal association” between the vaccine and the extremely rare post-vaccination occurrence of thrombosis with thrombocytopenia syndrome (TTS), characterized by a blood clot in combination with low levels of blood platelets. Of the cases, 22 were female and 6 were male, with a median age of 40 (18-59). Most of the cases occurred among women ages 18-49 years old. The median time from vaccination to the onset of symptoms was 9 days (3-15 days), and 19 of the 28 cases experienced cerebral venous sinus thrombosis (CVST). Dr. Shimabukuro noted that 3 of the patients died, 4 remained in the hospital as of May 7, 2 have been moved to post-acute care facilities, and the remaining 19 have been discharged.
The ACIP concluded the benefits of the J&J-Janssen vaccine continue to outweigh the risks, as the single-shot vaccine is useful among some populations. At least 2 committee members expressed concern with continuing the vaccine’s use without some stipulations. One suggested allowing the vaccine’s use only among people over age 60, who appear to be at less risk of TTS, while another proposed obtaining written informed consent from women under age 60 to ensure they are aware of possible risks. Although the ACIP did not adopt either suggestion, states and localities could implement their own guidance. While the blood clotting events associated with the J&J-Janssen vaccine appear to be similar to reports of rare events following administration of the AstraZeneca-Oxford vaccine in Europe, the CDC stressed that TTS does not appear to be associated with the mRNA vaccines from Pfizer-BioNTech and Moderna available in the US. The ACIP assured it would continue its enhanced monitoring of the CDC’s Vaccine Adverse Event Reporting System (VAERS) and conduct surveillance in other vaccine safety systems, as well as underlined its commitment to open and transparent communication about vaccine safety with the public.
EMERGING VARIANTS OF CONCERN In this week’s WHO epidemiological update, the WHO designated the B.1.617 variant as a variant of concern (VOC). The WHO Virus Evolution Working Group has determined that viruses within the B.1.617 lineage, which contains three sublineages, to be VOCs because they appear to be more transmissible, less responsive to some treatments, and less susceptible to antibody neutralization. Additionally, animal models show the B.1.617 variant may cause more severe disease. As of May 11, more than 4,500 sequences were added to the GISAID database and assigned to B.1.617 from 44 countries in all six WHO regions. At least 5 additional countries have reported detection of the variant. The B.1.617 variant was first reported last year in India and is possibly contributing to the current surge of COVID-19 cases and deaths there. Additional research is needed and ongoing to confirm characteristics of the variant, which is now the dominant strain in India.
INDEPENDENT PANEL ON PANDEMIC PREPAREDNESS According to a report by the WHO-sanctioned Independent Panel on Pandemic Preparedness, the COVID-19 pandemic was a “preventable disaster” and the world needs a new system of pandemic preparedness. Calling global preparedness for and response to the pandemic “inconsistent,” “under-funded,” “slow,” and “meek,” the 15-member panel examined the current pandemic but focused largely on efforts moving forward. The report recommends 7 action items to ensure COVID-19 is the last pandemic. Among the key recommendations are elevating pandemic preparedness to the highest levels of political leadership, including the adoption of a Pandemic Framework Convention; improving global surveillance and alert systems; strengthening the authority and financial-backing of the WHO; and investing in preparedness activities now to prevent future crises. The panel likened the COVID-19 pandemic to a “Chernobyl moment” for the gravity of its threat to global health and security. They urged world leaders and heads of international and regional organizations to “urgently accept their responsibility to transform the way in which the world prepares for and responds to global health threats,” asking, “If not now, then when?”
US MASK GUIDANCE On May 13, the US CDC updated its guidance for fully vaccinated individuals, which eliminates previous recommendations regarding physical distancing and mask use, including indoors. The update closely follows comments earlier this week by White House Chief Medical Advisor Dr. Anthony Fauci, who stated that fully vaccinated individuals do not need to wear a mask, except in densely crowded environments, based on a “growing body of evidence” regarding the low risk of infection and transmission for fully vaccinated individuals. The CDC’s updated guidance for fully vaccinated individuals now indicates they no longer need to wear masks or practice physical distancing in most settings. Notable exceptions include higher-risk environments, including “planes, buses, trains, and other forms of public transportation” and “correctional facilities and homeless shelters,” as well as anywhere that masks are mandated by tribal, state, or local governments or in businesses or workplaces that have their own mandates. The guidance applies to individuals who received their final vaccine dose at least 2 weeks prior.
In response to the shift in CDC guidance, some states immediately removed their mask mandates, but others are taking a more cautious approach. CDC Director Dr. Rochelle Walensky and US President Joe Biden acknowledged that some individuals may find it difficult to remove their masks in public, after wearing them for more than a year, and emphasized that individuals should make the transition when they are comfortable. Speaker of the US House of Representatives Nancy Pelosi indicated she would maintain the mask mandate until vaccination coverage increases among House members. Some mandates may remain in place due to concerns about elevated risk of community transmission in some areas or concerns about the inability to accurately identify individuals who have been vaccinated.
TAIWAN Local governments in Taiwan’s capital city of Taipei and some northern counties have announced business closures in response to 29 new domestic COVID-19 cases reported on May 14, the highest single-day figure since the pandemic began. More than half (16) have been linked to teahouses in Taipei. Health officials have not yet identified the source of infection for 7 of the cases, raising concerns of community spread. Additionally, Taiwan CDC announced 5 imported cases in arriving travelers. The previous day, Taiwan reported 13 domestic cases and 12 imported cases.
In Taipei, officials ordered the indefinite closure of bars, internet cafes, gaming and entertainment venues, including hostess clubs and teahouses, and public sport centers starting Saturday morning. The measures go beyond national guidance set by the central government, which said Taiwan will remain, for now, in Level 2: Local Cases of Unknown Sources. Under Level 2, hospitals and long-term care facilities (LTCFs) will allow only 1 individual to accompany or visit a patient or resident, with some exceptions. Taiwan Premier Su Tseng-chang took to Facebook to emphasize the importance of the next 2 weeks in controlling the outbreak, saying the alert level will not be upgraded “for the time being.” If there are 3 community clusters reported within a week or 10 locally transmitted cases from an unknown source in 1 day, Taiwan will enter Level 3. Officials are urging people to remain home, wear masks in public, and seek testing if they have been exposed to a known case or experience symptoms. Since the beginning of the pandemic, Taiwan has recorded only 1,290 cumulative COVID-19 cases, with the majority of those detected among travelers.
EID AL-FITR RESTRICTIONS Muslims around the world this week celebrated Eid al-Fitr with subdued festivities for a second year in a row, amid conflict in some regions and restrictions due to the COVID-19 pandemic. The end of the holy month of Ramadan usually is marked by millions traveling to social gatherings to pray and spend time with loved ones. The WHO’s Eastern Mediterranean Regional Office (EMRO) published guidance for safe practices during the holiday, urging people to avoid large gatherings and practice individual behaviors like wearing masks, washing hands, and getting vaccinated, when possible. Many countries with large Muslim populations—including Pakistan, India, Malaysia, and Singapore—took their own actions to prevent large social gatherings during the holiday, implementing limits on crowd sizes and temporary closures of some mosques and shops. In Bangladesh, thousands traveled from the capital of Dhaka to join their families in rural villages despite a national lockdown and road checkpoints. Some experts fear the holiday travel will lead to an increase in COVID-19 cases in the country, which is struggling to obtain sufficient vaccine supplies and concerned over the recent detection of cases due to the B.1.617 variant from India.
ENGLAND/WALES COVID-19 APP A manuscript published online May 12 by the journal Nature provides evidence for the epidemiological impact of a UK National Health Service (NHS) COVID-19 mobile phone app for England and Wales. From its launch in September 2020 through the end of December 2020, the app was used regularly by approximately 16.5 million people (28% of the total population) and sent approximately 1.7 million exposure notifications (4.4 per index case that consented to contact tracing). The estimated fraction of app-notified individuals subsequently showing symptoms and testing positive (the secondary attack rate, SAR) was 6.0%, comparable to the SAR for manually traced close contacts. Using a modeling approach, researchers estimated that 284,000 cases were prevented by the app (108,000 to 450,000), while statistical analysis estimated the number to be even higher at 594,000 (317,000 to 914,000). The researchers projected roughly one case was averted for each case that consented to notification of their contacts through the app. For every percentage point increase in users, the number of new cases could be reduced by 0.8% (modeling) and 2.3% (statistical analysis), according to the researchers, who recommended the continued development and deployment of similar apps, especially in populations where vaccination is ongoing.
GERMANY RELAXES TRAVEL RESTRICTIONS Germany has relaxed travel restrictions for travelers who have been vaccinated or recovered from COVID-19. Such travelers will not have to be tested for SARS-CoV-2 or quarantine when entering the country, unless they are traveling from an area where variants of concern are prevalent. Additionally, non-vaccinated people will be allowed to end their quarantine early if they test negative. Health Minister Jens Spahn said the country expects to implement a digital immunity certificate by the end of June, to aid in validating vaccination status for travelers. The country hopes the app will be compatible with the vaccination certification system in development by the European Union, which also is expected to roll out by the end of June. Notably, the European Parliament has said that the EU certificate should not be used as a vaccine passport and that countries will not be obligated to implement the certificate.
US PUBLIC HEALTH WORKFORCE The White House announced a program to invest US$7.4 billion to reinforce the public health workforce, drawing from the US$1.9 trillion American Rescue Plan that was signed into law in March. Many experts attribute the US’s struggle to combat the COVID-19 pandemic, in part, to decades of chronic underfunding for public health infrastructure. Of the new funding, US$4.4 billion will support state and local health departments in hiring personnel to address shortcomings in critical capabilities, including contact tracing and case investigations, as well as school nurses to facilitate resuming in-person classes. Additionally, some of the funds will be dedicated to expanding the CDC Epidemic Intelligence Service (EIS) and establishing a Public Health AmeriCorps program. The remainder, US$3 billion, will allow the CDC to establish a federal grant program to support state and local governments’ efforts to “expand, train, and modernize the public health workforce for the future.”
SARS-COV-2 ORIGIN A group of scientists published a letter in Science asking the international scientific community to further investigate the origins of SARS-CoV-2. The group recognized the effort organized by the World Health Assembly and the WHO that occurred in May of 2020, suggesting that there was not enough evidence presented to thoroughly investigate the theory that the origins of SARS-CoV-2 stemmed from an accidental release. The group emphasized the importance of determining the pandemic’s origins, calling for a “proper” investigation that is “transparent, objective, data-driven, inclusive of broad expertise, subject to independent oversight, and responsibly managed to minimize the impact of conflicts of interest.” The group also noted recent anti-Asian sentiment in some countries and recognized the efforts of Chinese citizens who shared information about the emerging disease with the world, “often at great personal cost.”
CONSUMER GOODS PRICES The US Consumer Price Index rose in April, up 4.2% from a year ago, the sharpest increase since 2008. The rise in prices has some economists worried, suggesting that the rebounding of an economy depressed by the COVID-19 pandemic may sustain these higher prices on everything from fuel to groceries. US Federal Reserve Chair Jerome Powell has expressed his opinion that the price increases will be transient, representing supply chain hiccups and an increased willingness among Americans to travel after a prolonged period of COVID-19 restrictions. It will take time to see which trends last as the global economy begins to recover from the COVID-19 pandemic.
They had received the J&J vaccine more than 2 weeks prior to testing positive. Only one of the eight has shown symptoms.
Though vaccinated persons can still contract the virus, it is considered quite odd that the virus broke through the vaccine in EIGHT vaccinated persons from the same group of people.
by ponchi101 Buried in the article: that maybe the J&J vaccine should also be a two-shots vaccine.
Very interesting.
by ti-amie
Now we know your alias Ponchi!
by ponchi101 Damn...
by Deuce Allowing vaccinated people to not wear a mask makes no sense at this point.
If you go to a grocery store, for example, do you really think they're going to check everyone for confirmation of vaccination?
Not to mention many other locations.
So you'll have all of these 'ani-vaxers' walking around without masks.
Not good.
by atlpam If a business still requires a mask, it doesn’t matter if you are vaccinated or not. You wear the mask or don’t patronize that business. Unfortunately the “honor” system doesn’t work since the anti-maskers will just claim they are vaccinated and no one can ask for proof. Why they think it’s an incentive for those on the fence to get vaccinated is beyond me. It just gives them a free pass not to wear a mask.
by Suliso I've been talking about the dire need for strong regional vaccine manufacturing in the context of this pandemic (too late really), but more importantly any subsequent ones. Found the article below about challenges and opportunities in Africa which would probably be the hardest nut to crack. I personally think it's not going to happen without a major help (finance and technology) from developed countries, but it's worth trying. South Africa would be the obvious location in the Sub-Saharan Africa and perhaps Morocco in the north.
I've only copied few paragraphs here and encourage those of you who're interested to read the whole thing.
Africa needs vaccines. What would it take to make them here?
Vaccines: it’s safe to say that no one living today has ever thought quite so much about these invaluable substances. Rollouts of COVID-19 vaccines are well underway in some countries, especially those with large domestic manufacturing capacity. Many African countries have received their initial shipments from the COVAX facility1 and from bilateral deals, in some cases months earlier than in previous pandemics such as H1N1, but on the whole Africa has struggled to secure timely access to adequate supplies. Africa relies heavily on vaccine imports: the continent imports almost 99 percent of its routine vaccines today. The COVID-19 pandemic has revived a long-standing question in African and global circles: What would it take for Africa to manufacture its own vaccines?
....
Despite the presence of a few players, vaccine manufacturing in Africa is still nascent, especially in the upstream segments of the value chain, such as antigen production (Exhibit 2). Building on valuable recent research,7 we looked deeper at the current capabilities of Africa’s vaccine manufacturers across products, value-chain steps, and the key dimensions that have the potential to swing business-case assessments.
(click for a graph)
Only a handful of companies manufacture the drug substance, typically at small scale, which results in relatively high production costs. Fill-and-finish and package-and-label capacity is better established—for example, in South Africa, Egypt, and Senegal; more than ten products are currently filled on the continent. In comparison, Asia and Western Europe each have more than ten established, large-scale vaccine manufacturers, many of which operate across the full value chain, including the higher value-adding steps, and produce high-quality products at low cost. While there is potential to expand the capacities of today’s African manufacturers, much of the sector’s expansion will likely also come from greenfield investments that carefully consider technological and process innovations and structural realities.
....
Five keys to vaccine manufacturing
The dynamics of supply and demand are subject to myriad influences, as are production costs. But there is another set of factors that is entirely within Africa’s power to fix. Our review of the literature and interviews with leaders in the field suggest that five barriers constrain the industry’s growth today: lack of a clear agenda or coordination across efforts, restricted access to finance, weak regulatory environments, challenging demand dynamics, and limited local talent. For each, we explore the actions that may be needed to get past these obstacles.
by Suliso Another article, this time from Nature, about the same topic. This time I only post an picture which really tells you all you need to know. Just fill and finish is not going to do and of course the scale needs to be large (min 20 million doses per year).
I picked articles on Africa because the situation is the most dire there, however strong regional manufacturing needs to be established also in South America and certain parts of Asia. Even some rich countries (Japan) lack adequate capability.
I think this is the best way of dealing better with future pandemics. Merely releasing patents doesn't really do anything. If there were strong local manufacturers technology could be easily licensed to them from the original developers which will always be in the richest countries.
by ponchi101 Thanks for those.
You know I wrote about Colombia's idea, ten years ago, to stop all local production of all vaccines. That has come to hurt them bad now.
Even if these industries need to be subsidized, all countries need to have some sort of vaccine production capability. This pandemic has proven it. Or, as you say, have some regional hubs run by the surrounding countries.
by Suliso Probably not all countries, that's not sustainable production wise. I'd argue for regional hubs with at least one for every 100-200 million inhabitants. In South America could be say Colombia for the northern part, Argentina or Chile for the south and Brazil for itself since it's so big. Of course that's just a guess, would need to look closely at capability of the local industry already, talent pool, safety etc.
Completely off topic: a friend asked yesterday why is it that all the important cities in Colombia are in the mountains and not on the coast as one would normally expect? I imagine you have an intelligent answer to that.
by ponchi101 Colombia. That is not completely accurate. Bogota and Medellin are certainly the largest cities and are both in mountains, but they are not the only ones. Cali is a bit below, at about 1,000 Mts. The coastal cities are also important: Cartagena, Santa Marta and Barranquilla are important ports.
But the reason is simple, sort of like in Switzerland: the important cities are in the mountains because almost the entire country is mountainous. If you look at the map, it is crisscrossed by mountain ranges. So either you have a city on a mountain, or you have it in a valley because it has mountains on either side.
Bogota is on a mountain, but in itself, it is built on the valley of two smaller ranges. As a city, it is flat.
Last idea: the valleys in Bogota, Medellin and Cali are very fertile. When the Spaniards conquered and found the cities, these were ideal places. Good soil, and rivers running through them. Perfect conditions for agriculture.
by Suliso Very mountainous indeed but still the capital and the biggest city could have been on the coast, couldn't it? Come to think of it Costa Rica is similar - so much space on the coast, but the only densely populated area is high up. There must be some kind of historical reason. So I kind of favor your soil hypothesis.
As for Switzerland all the major cities we do have are located at near the lowest points of the country. I don't think there are any serious cities above 1,000 m in Europe.
by ponchi101 I believe it was the soil. Caracas is also like that. Many of our boroughs are named after the plantations that were there before urbanization. My mom lives in "El Cafetal" (the coffee plantation), which is near "Los Naranjos" (the orange grove). And then other sectors are named after the forests that were there: Los Caobos (a local tree), Los Ruices (another) and so forth.
Soil and water. No cities without those conditions (specially a river with fresh water) were built before modern times (Las Vegas, Dubai, etc).
As for your example in Switzerland: you guys have the issue of snow. Not a great idea to build a city where you will be snowed in for months of the year. Or outright die of exposure. No such issue here.
by Suliso In the ancient past vast majority of cities were built at confluence of some kind of trade routes (sea, river, near mountain crossing etc) and trade routes in those days were mostly water based. A notable exception are some Italian cities which were founded deliberately as military veteran colonies at the crossroads of Roman roads.
by ti-amie
I agree with Dr Wen on this. Fauci has been working trying to clarify what the new guidelines mean but I think that horse, for some people, is long gone.
by ponchi101 In CONTAGION (the movie) the vaccines came with a band that you could strap on your wrist to verify you had the vaccine.
C'mon, it can't be that hard. The people that took the vaccine certainly won't mind, the antivaxxers are out on their own.
by ti-amie
ponchi101 wrote: ↑Sun May 16, 2021 11:53 pm
In CONTAGION (the movie) the vaccines came with a band that you could strap on your wrist to verify you had the vaccine.
C'mon, it can't be that hard. The people that took the vaccine certainly won't mind, the antivaxxers are out on their own.
I just heard a report on the local all news station that was about companies are concerned about how to guarantee a safe work environment since there is no real way - at this time - of telling who is vaccinated and who is not.
There is a Mass I've been watching on Sunday mornings during the pandemic. The Rector, in his remarks before the start said, and I'm paraphrasing, that despite what the CDC or the government says they have no way of knowing who is vaccinated and who is not. He went on to say that masking will continue to be mandatory inside the Basilica. I've been retired for awhile but why can't companies do the same thing?
ponchi101 wrote: ↑Sun May 16, 2021 11:53 pm
In CONTAGION (the movie) the vaccines came with a band that you could strap on your wrist to verify you had the vaccine.
C'mon, it can't be that hard. The people that took the vaccine certainly won't mind, the antivaxxers are out on their own.
I just heard a report on the local all news station that was about companies are concerned about how to guarantee a safe work environment since there is no real way - at this time - of telling who is vaccinated and who is not.
There is a Mass I've been watching on Sunday mornings during the pandemic. The Rector, in his remarks before the start said, and I'm paraphrasing, that despite what the CDC or the government says they have no way of knowing who is vaccinated and who is not. He went on to say that masking will continue to be mandatory inside the Basilica. I've been retired for awhile but why can't companies do the same thing?
Companies can do the same thing (at least private ones). When the governor here removed all the restrictions, it was still noted that businesses were free to continue requiring masks and/or continue with capacity restrictions as they see fit. For example, my town has outdoor concerts on a green. When restrictions were in place, they were creating distanced spaces and only taking reservations for 500 people. After guidance on low risk for outdoor activities, they are still requiring reservations but now allowing 2500 people (total capacity is 5000). Based on the state guidelines, they could go full capacity, but they are continuing to be more cautious.
by MJ2004 The university I work for just announced that students will be required to be vaccinated, and that staff are “strongly advised” to get the vaccine.
by Suliso How will you verify? I hear some states are refusing to provide any documents.
by SulisoHow can more covid-19 vaccines be made available?
The nuts and bolts of scaling up production matter more than intellectual property
Biomedicine has never seen anything like it. This time last year, no company had ever made a vaccine against sars-cov-2, the virus that causes covid 19, on an industrial scale. By the middle of this April a billion doses had been delivered. According to Airfinity, a data provider, a second billion doses are expected by June 1st. On current estimates the world’s pharmaceutical companies look set to provide 10.9bn doses over the course of 2021.
So far this effort has increased the world’s capacity for producing vaccines of all sorts by a factor of three to four. “It’s insane,” says Tim Gardner, the boss of Riffyn, a biotechnology startup focused on speeding up drug-production processes. “It’s an incredible success.”
At the same time many parts of the world have no smooth-running avenues of supply. The Covid-19 Vaccines Global Access Facility (covax), a vaccine-sharing scheme designed to provide supplies to low- and middle-income countries, has so far distributed only 59m doses. Most of the most vulnerable unvaccinated people look unlikely to be vaccinated soon. This is both inequitable and inefficient; it will increase the death toll and prolong the pandemic, increasing both economic losses and the odds of new variants of concern.
A recent report from the oecd, a club of mostly rich countries, made the case for continued government investment in vaccine-production capacity, putting the idea into the context of long-term strategies such as “co-ordinated approaches to the sharing of intellectual property and technology transfer”.
It is the sharing of intellectual property, not increased investment, which has drawn the most attention. Since last October, South Africa and India have been arguing for an arrangement whereby the World Trade Organisation no longer obliges countries to protect patents, industrial designs, copyright and trade secrets which apply to covid-19 vaccines, therapeutics and diagnostics. America, Britain, the European Union and Switzerland—home, between them, to most of the world’s big drugmakers—opposed the waiver. But on May 5th President Joe Biden broke ranks. Katherine Tai, the us trade representative, said that the administration would support proposals to waive intellectual property protections for covid-19 vaccines, winning the administration plaudits from over 100 countries which support the waiver as well as from people at home who think drug companies inherently villainous.
If such a waiver is agreed on, it will not be soon. Proponents take that in their stride: better to arrive at the end of the year with a waiver agreement close to hand and no need to use it, goes one argument, than still to be facing a global crisis of unmanageable proportions but with a diplomatic mountain to climb. That may be so. But the world’s need to create new production facilities, and ideally to work the various capabilities it has already developed even harder, will not wait. And intellectual-property rights are far from the most pressing, or most restrictive, constraint.
Billion wise, trillion foolish
The increase in capacity seen over the past year was brought about in large part because of government interventions, most notably Operation Warp Speed in America and the activities of the Vaccine Taskforce in Britain, which guaranteed payments and drove the expansion of supply chains.
These efforts splashed around a lot of money which, if none of the vaccines had worked, would have been lost. But with the benefit of hindsight it is now hard not to wish they had been more generous still. In March Science, a journal, published estimates from a group of economists of the total global economic loss that would have been avoided if enough money to produce vaccines for the entire world had been provided up front, rather than enough for most of the rich world. They calculated that if the world had put in place a vaccine-production infrastructure capable of pumping out some 1.2bn doses per month by January 2021, it would have saved the global economy almost $5trn (see chart).
Eric Budish of the Chicago Booth School of Business, one of the model’s authors, explains the situation using a plumbing metaphor: it is faster to lay down a wider-bore pipe at the start of a project than to expand a narrow one later. The rich world succeeded in producing effective vaccines remarkably quickly in quantities broadly sufficient to its needs: an extraordinary achievement. But the capacity of the system it built in order to do so created constraints that the rest of the world must now live with. That was a choice, not destiny.
by Suliso But if the best time to invest was last year, the second best is now. Three distinct types of vaccine—based on mrna, on dna packaged inside an adenovirus, and on inactivated sars-cov-2 particles—have been widely authorised for use, if in most cases and places only on an emergency basis. Companies that play a role in relevant supply chains are able to invest with an assuredness about what is to come that they could not have had last year. Thermo Fisher, an American firm which sells a range of scientific and pharmaceutical supplies, having seen “mrna confidence increase on the demand side”, is spending $60m on a facility in Texas that will produce more of the nucleotide building blocks from which mrna vaccines are assembled.
The mrna vaccines made by Pfizer/BioNTech and Moderna are, in general, those which Western customers are most excited about seeing scaled up. Moderna is ramping up production around the world; it recently announced that it will make 3bn doses next year. On May 10th BioNTech said it plans to create a factory with an annual capacity of several hundred million doses in Singapore. The firm is in discussion with other countries about further production sites. A joint venture with Fosun Pharma, a Chinese firm, could make up to 1bn doses a year. A number of African countries are known to be keen on bringing the technology to the continent.
Unfortunately for the vulnerable people at growing risk around the world none of this will be quick. Stéphane Bancel, the boss of Moderna, says that it takes six to nine months at a minimum to add significant capacity, which means there is no way to increase capacity this year beyond what is already planned. Even when a company has a site ready to take mrna manufacturing equipment, machines have to be ordered, built, shipped and installed, a reliable supply of raw materials has to be arranged and people have to be hired, trained and brought up to speed on the processes involved.
Pollyanna, meet Polanyi
Building up the requisite knowledge in the new teams is the hardest task. The problem, says Rob Carlson, a veteran biotechnology investor, is that that knowledge is not stored in a format that is easy to copy between facilities. Each vaccine is produced according to a “recipe” which lists the settings for all of the things in a production facility that can be changed from job to job: every dial on every machine, timings, temperatures, masses, volumes and concentrations. Such a recipe may run to hundreds of pages. And it will still typically be incomplete; tacit knowledge matters, too, and it is for the most part lodged in the minds of very busy people.
Under pandemic conditions accessing what those people know will be complicated by the fact that they may well be on the edge of burnout. Mr Bancel says his team “has been working hard for a year, seven days a week…we are not even finished doing all the tech transfer to deliver the billion for this year.” Every day he worries that he is pushing them too close to their breaking point.
The non-mrna Western firms have been working just as hard at transferring their technology. AstraZeneca made global production of its adenovirus vaccine a particular focus; the tech transfer of Oxford University vaccine taken forward by AstraZeneca to one British production site took about seven months, says Sandy Douglas, the Oxford professor who managed the transfer. Novavax has taken the better part of a year to transfer the insect-cell-based manufacturing system for its not-yet approved protein-subunit vaccine to the Serum Institute of India (sii), a huge and very experienced vaccine-maker. Stan Erck, the company’s ceo, says it is repeating the process in the Czech Republic, Korea, Japan and America.
All told, pharma firms have made 280 partnership contracts covering the production of covid-19 vaccines, says Thomas Cueni, head of the International Federation of Pharmaceutical Manufacturers and Associations, a trade group. About three-quarters of those deals involve technology transfer. He adds that the firms that are doing well in terms of meeting production targets tend to have relatively few production sites, pointing to the benefits centralisation offers attempts to scale up.
Biobags and bottlenecks
Despite all this activity, though, some companies which could be making vaccines are not. Teva Pharmaceutical Industries, an established Israeli generic-medicine maker, has failed to reach a co-production deal with any covid-19-vaccine-maker. At the end of April it said it had stopped trying. Incepta, a Bangladeshi firm with the capacity to fill and finish hundreds of millions of vaccine vials a year, has also complained that it has been unable to interest producers in its services.
Given the constraints on expansion, it is vital that the supply chains on which current production rests be kept in fine fettle. “The number one priority today must be to do everything that we can to ramp up raw materials and get them to the production centres,” says the European Federation of Pharmaceutical Industries and Associations, a trade group. Unfortunately, production has been slowed at various facilities by insufficient supplies of biobags (the containers in which vaccines are often made), tubing, filters and growth media for cells. Novavax’s lines in both Britain and India have been hit by shortages, at times coming to a halt; the company’s production plans have been set back significantly.
On April 16th the trouble with the Indian line led to a remarkable tweet. Adar Poonawalla, the head of sii, begged President Biden—“Respected @potus”—“to lift the embargo of raw material exports out of the U.S. so that vaccine production can ramp up”. At issue was America’s Defence Production Act (dpa), which grants the president broad industrial-mobilisation powers. The government is using the dpa to prioritise domestic firms’ orders for material and equipment used in vaccine production over those flooding in from other countries. Overseas producers who depend on American equipment or materials are feeling the pinch.
The sii said difficulties in getting materials from America were putting an AstraZeneca line at risk, as well as the Novavax one; between them they have a capacity of 160m-170m doses a month. On April 26th Tim Manning, the White House’s supply co-ordinator for covid-19, defended the use of the dpa, saying it is not a “de facto ban” on export and does not create supply shortages. But Biovac, a South African vaccine-maker, told Reuters that its American supplier of biobags was explicitly blaming the dpa for a 14 month backlog on biobag deliveries. Last year a number of big pharma firms started re-creating supply chains outside America to serve international customers. The sii Novavax line is still running at a fraction of its full capacity.
Disruptions to supply chains, whether down to the dpa or other factors, are a source of deep frustration. “Why on earth is production at the Serum Institute being delayed because it can’t get enough culture media?” asks Dr Douglas. “It’s madness! Is it because the company that makes culture media has a shortage of its own? If so let’s fix that.” Such problems have a worrying tendency to amplify themselves; when companies have concerns about supply chains they stockpile supplies, stressing the chains even more. The fact that some of the equipment needed for vaccine-making also plays a part in the production of considerably higher-margin products such as cancer treatments further complicates the situation, breeding suspicion.
Despite the supply difficulties, Airfinity says that current roll-out forecasts suggest that the America, Britain, Canada, the eu and Japan will have enough doses for their entire adult populations between the summer of 2021 and January 2022. But middle- and low-income countries are at risk. Donors have committed money to covax, but it has not been getting the vaccines it is meant to buy. Bruce Aylward, senior adviser to the director general at the World Health Organisation (who), says covax hopes to have the j&j adenovirus vaccine by June but “who knows, it is at risk for a million reasons so maybe June, maybe July, maybe August”. Of the 40m doses that Pfizer has promised, he says, it has delivered only 960,000. There was, though, some good news for covax on May 7th, when Sinopharm’s vaccine was given emergency-use authorisation by the who. This means that the vaccine, one of two inactivated-virus formulations being made in bulk by China, can now be distributed through covax.
Some countries have promised to donate doses to covax, but the volumes are small. Spain and New Zealand, the most generous, have pledged 1.6m and 7.5m doses respectively. The organisation has so far dealt with just 100,000 donated doses, provided by France and dispatched to Mauritania, says Dr Aylward. Rasmus Bech Hansen, boss of Airfinity, says he hears that the large purchase orders made by some governments may be resold rather than donated. The possibility of donations could be further dampened by a perceived need for booster shots as new variants spread.
Fail better
Bottlenecks in supply and hold-ups in distribution have led to calls for a fresh round of state investment. Public Citizen, an American consumer-advocacy group, says that with $25bn the Biomedical Advanced Research and Development Authority, a part of America’s Department of Health which comes up with solutions to health emergencies, could scale up vaccine production enough to cut years off the tail of the pandemic. The money would be spent on stimulating production all the way along the supply chain, on technology transfer and on the construction of new facilities around the world. All of those people that The Economist spoke to who work in the existing vaccine-supply chain agreed that this was one sure-fire way to boost vaccine output yet further. The second-best time will always be now.
"In Dallas County, there have been 506 “breakthrough” cases of COVID-19 in people who have been fully vaccinated, or about six cases for every 10,000 fully vaccinated residents. Eighty-two of those breakthrough patients were hospitalized, and seven died."
How do you throw out these numbers without telling us how many cases there were without the vaccine, what that percentage is, how many were hospitalized, and how many died?
Just saying what they wrote gives people the impression the vaccine is not working. If they gave all the numbers, I am sure the difference between the vaccinated and the unvaccinated will be significant.
by atlpam Just curious, in all the reports of golfer Jordan Spieth having Covid, they never mention vaccination status.
Are we only publicizing breakthrough cases for those who were vaccinated and not publicizing cases that could have been avoided through vaccination?
by dryrunguy Here's the latest Situation Report. Haven't read it. I have been distracted by Eurovision.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 163 million cumulative cases and 3.4 million deaths worldwide as of 5:45am EDT on May 18. As India’s current COVID-19 surge peaked and began to decline, global weekly incidence decreased for the second consecutive week, down more than 12% compared to the previous week. Global weekly mortality also declined for the second consecutive week, down nearly 5% from the previous week. Notably, the global trend in mortality is not lagging incidence by 3-4 weeks, as we have observed previously during the pandemic. It is not immediately apparent why this is the case, and it warrants monitoring over the coming weeks.
India’s daily incidence continues to decrease sharply from its peak on May 8 (391,282 new cases per day). Notably, the rate of decrease since the peak appears to be even sharper than the steep increase prior to the peak. The current daily incidence is 319,497 new cases per day, representing a 18% decrease over the past 9 days. India’s test positivity is also decreasing sharply, down from a peak of 22.7% on May 8 to 18.9% on May 15*, a 17% decrease over that period. While India’s test positivity remains elevated, which suggests that the official reports continue to undercount the true daily incidence, the decreasing trend provides an indication that testing volume is beginning to catch up to the scale of community transmission.
*The most recent data available for India.
Global Vaccination
The WHO reported 1.26 billion doses of SARS-CoV-2 vaccines administered globally, including 637 million individuals with at least 1 dose, but these data have not been updated since May 12. Our World in Data reported 1.50 billion cumulative doses administered globally, an increase of 13% over the previous week. Daily doses administered continues to increase, up to a new record of 24.7 million doses per day. Our World in Data estimates there are 360 million people worldwide who are fully vaccinated, corresponding to approximately 4.6% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.8 million cumulative cases and 583,074 deaths. On May 16, the US reported 17,724 new cases, the first day with fewer than 20,000 new cases since June 15, 2020, and the lowest single-day total since June 7, 2020. On May 14, the United States’ per capita daily incidence fell below 10 daily cases per 100,000 population for the first time since early in the country’s second surge. The current daily incidence (30,211 new cases per day) is the lowest since June 23, 2020. Between the first and second surges, the lowest average daily incidence was 19,817 new cases per day (June 1, 2020), the only day below 20,000 since March 2020. If the US continues on its current trajectory, it could fall below that number in the next week or so. At 545 deaths per day, the current daily mortality is at its lowest point since April 1, 2020, which was less than 1 month after the first COVID-19 death was reported in the US.
Daily incidence and mortality continue a prolonged decline, first from the largest peak in January 2021 and again following the minor surge that peaked in mid-April. Testing volume similarly decreased over that time. At the national level, test positivity peaked at nearly 15% in early January 2021, the highest point since the initial surge in early 2020, when testing capacity was extremely limited and eligibility was focused on symptomatic patients. From there, both testing volume and positivity decreased substantially through mid-March 2021, as the US recovered from its winter surge. Testing volume increased only slightly during the March-April surge, but test positivity increased over that period, from 4% to nearly 5.5%. Test positivity decreased steadily after that peak, and on May 16, the CDC reported the lowest average since it started tracking it on March 1, 2020 (3.32%).
In total, 10 states are reporting test positivity* of more than 5%. Of these states, only Montana is reporting an increasing trend, up from 3.52% on March 28 to 5.17% on May 15. Most of these states—including Florida (5.58%), Michigan (6.36%), Nebraska (5.89%), Oregon (5.02%), South Dakota (6.94%), Tennessee (5.18%), and West Virginia (5.97%)—have reported declines in test positivity since mid-to-late April, and if they continue on their respective current trajectories, they could fall below 5% in the near future. Indiana’s test positivity (5.18%) increased after its most recent surge and has hovered around 4.5-5.5% since then. Alabama (5.44%) has largely hovered around 5.25-6% since mid-March.
The majority of states are reporting steady declines in test positivity over the past several weeks, particularly since the peak of the most recent surge in mid-April. Massachusetts is reporting the lowest test positivity, at 1.03% and still decreasing. New Mexico and Utah have reported steadily increasing test positivity since late March/early April. New Mexico’s average is up from a low of 1.93% to 2.66% in its more recent report on May 5, and Utah’s average has increased from 3.73% on April 4 to 4.6%. Louisiana (3.61%) is reporting a slight increase over the past several weeks, up from 2.62% on May 1. Arizona is exhibiting a similar trend, but on a longer timeline. Arizona’s test positivity has increased slowly from a low of 3.58% on March 24 to 4.95% on May 12, before falling slightly to 4.69%. The overall decreasing trends, including a number of states that are setting or approaching new record lows, is an encouraging indication that testing volume is reaching and sustaining at a level that can accurately capture the scale of community transmission.
*Data not available for May 16; the values reported here correspond to the most recent data available for each state, most of which are from May 15.
US Vaccination
The US has distributed 345 million doses of SARS-CoV-2 vaccine and administered 274 million. Daily doses administered* continues to decrease steadily, down from a high of 3.3 million on April 11 to 1.6 million. Approximately 1.1 million people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 158 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 48% of the entire US population and 60% of all adults. Of those, 124 million are fully vaccinated, which corresponds to 37% of the total population and 47% of adults. Among adults aged 65 years and older, progress has largely stalled at 85% with at least 1 dose and 73% fully vaccinated. Among individuals aged 12-17 years—including individuals aged 16 and 17 who were previously eligible—3.3 million have received at least 1 dose, and 1.6 million are fully vaccinated. In terms of full vaccination, 64 million individuals have received the Pfizer-BioNTech vaccine, 50 million have received the Moderna vaccine, and 9.6 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
US CDC MASK GUIDANCE Following the US CDC’s announcement of updated mask guidance on May 14, federal health officials have spent the past several days “defending” the updated guidance. Numerous accounts describe the new guidance that eliminated recommendations for mask use and physical distancing for fully vaccinated individuals in most situations as “surprising” or “startling.” Reportedly, the CDC did not brief state and local health officials on the changes prior to the announcement, which resulted in many being caught off guard by the new guidance. Numerous states and businesses removed or relaxed mask mandates in response to the change, some with little or no advance notice. The sudden change has caused confusion among the public, state and local health and elected officials, and schools and businesses, particularly regarding whether (and how) to maintain mandates for unvaccinated individuals while allowing vaccinated individuals to go maskless.
Some experts applauded the change, but others expressed concern about both the policy’s content and its rollout. While many felt guidance has evolved too slowly, the CDC is now being criticized for overcorrecting and moving too quickly. Some are concerned that the change—and subsequent end of mandates—will encourage individuals to forego COVID-19 protective measures, such as mask use, even if they are not yet vaccinated, which could increase the risk for individuals who are not yet fully protected. Some argue that the guidance is based, at least in part, on the assumption that anyone who wants to get vaccinated is already fully protected. Notably, some states only expanded eligibility to everyone aged 16 years and older in late April, adolescents aged 12-15 have only been eligible since May 12, children under the age of 12 are still not eligible at all, and millions of individuals with compromised immune systems either cannot be vaccinated or may only obtain partial protection. National Nurses United, the country’s largest nurses union, issued a statement opposing the new guidance, emphasizing concern about ongoing elevated daily incidence, increasing prevalence of variants of concern, risk to healthcare workers and patients, and the disproportionate impact on historically underserved Black, Hispanic/Latino, and Indigenous populations.
CDC Director Dr. Rochelle Walensky emphasized that the risk of infection and transmission for vaccinated individuals is very low and that the changes stem from evolving data. She also encouraged “individual assessment of...risk” and stressed unvaccinated individuals should continue practicing physical distancing and mask use. White House Chief Medical Advisor Dr. Anthony Fauci acknowledged that additional clarification on the new guidance likely would be published in the coming weeks.
US VACCINE ACCESS As vaccination progress in the US slows, health officials are increasing efforts to understand and mitigate the remaining barriers, particularly in undervaccinated populations. Much attention has been given to vaccine hesitancy, particularly in the context of historical examples of unethical medical practices in communities of color, the lasting effects of systemic racism, and political divisions. However, vaccine hesitancy may be less of an issue among some communities than barriers to accessing the vaccine.
The declining trend in daily doses administered, particularly in the context of increasing supply, could signal waning demand, but evidence shows that interest remains high. In fact, recent data from the US Census Bureau indicates that more than 40% of adult Americans who have not yet been vaccinated are interested in doing so, which is more than those who do not intend to get vaccinated (37.8%; 21.6% remain unsure). Many individuals are finding it difficult to make time to get vaccinated, particularly lower-income individuals who do not have the benefit of paid time off to get vaccinated and who may be working multiple jobs to provide for their families.
Looking ahead, there appears to be a shift away from large-scale, centralized mass vaccination sites and toward smaller efforts that disperse vaccination sites throughout communities. Vaccination availability at national and regional chain pharmacies and drug stores has increased access in many communities, but including primary care offices and mobile programs to reach people at home or other convenient locations can further increase accessibility. In addition to making vaccination more convenient, community-based efforts also can make vaccination more comfortable by involving vaccinators or advocates who have established relationships in the community.
US VACCINE DONATIONS On May 17, US President Joe Biden announced the US government will send an additional 20 million SARS-CoV-2 vaccine doses abroad. Previously, the US government announced a donation of 60 million doses of the AstraZeneca-Oxford vaccine as soon as they are reviewed by the US FDA, and Monday’s announcement adds at least 20 million doses of vaccines already authorized in the US. The government also previously committed to providing about 4 million doses of vaccine to Canada and Mexico, although in the form of a loan. According to a White House fact sheet, the government will continue to donate vaccines from its excess supply as it receives delivery of that supply. US government officials are expected to announce in the coming days how they are deciding where to send vaccines.
The US has come under increasing pressure to play a larger role in global vaccination efforts, as countries in South Asia and South America struggle with outbreaks. Additionally, US diplomats and other experts are pressing the US to move more quickly in helping to distribute vaccines to counter efforts by China and Russia, over concerns that those countries are using their homegrown vaccines as political collateral. The US government explicitly states it “will not use its vaccines to secure favors from other countries.” US diplomats in South Asia, the Middle East, and Africa say they received urgent requests from officials in their host countries for COVID-19 assistance. On Monday, President Biden committed to working with the international community, including the COVAX facility and G7 leaders, to play a significant role in helping to slow the pandemic’s global toll.
TRACKING VARIANTS GLOBALLY Researchers and health officials are tracking the emergence of several variants of concern (VOCs), including B.1.1.7, B.1.351, P.1, and the B.1.617 variant that appears to be driving the surge in India. Because emerging variants may behave differently, which can affect the effectiveness of protective measures (e.g., physical and social distancing, vaccines), it is critical to quickly identify and characterize new variants and to identify their origin.
One of the principal challenges in identifying and tracing VOCs back to their origin is genomic sequencing capacity at the global and national levels. Countries vary widely in terms of the proportion of COVID-19 cases that they can sequence, and even higher-income countries like the US have struggled to scale up this capacity in the midst of the pandemic. Health officials also are monitoring the geographic spread of VOCs, such as possible expansion of the B.1.617 from India to neighboring countries, including Sri Lanka and Nepal. The national sequencing capacity in many countries would be limited under ideal circumstances, but restricted travel during the pandemic is further stressing available resources by delaying the delivery of supplies, such as the reagents necessary for genomic sequencing. A number of organizations are supporting efforts to expand laboratory capacity to monitor emerging variants, including the Coalition for Epidemic Preparedness Innovations, which is expanding its laboratory network to provide better global surveillance coverage for emerging variants—from 8 laboratories to 10—with a focus on assessing vaccine efficacy against VOCs, part of a US$17.5 million effort.
VACCINATION TIMING When rolling out its vaccination program at the end of 2020, the UK made a bold and controversial decision to recommend a longer interval between SARS-CoV-2 vaccine doses to extend its limited supply and maximize the number of people who would at least be partially protected from hospitalization and death. Now a study (preprint) published May 17 by medRxiv shows delaying the second dose of the Pfizer-BioNTech SARS-CoV-2 vaccine to 12 weeks instead of 3 weeks produced a much stronger antibody response among older adults. Researchers from the University of Birmingham and Public Health England found that delaying the second shot of the mRNA vaccine produced peak antibody responses 3.5-fold higher among people aged 80-99 years who had no evidence of previous infection when compared with those who received the vaccine after the recommended 3-week interval. Cellular immune responses were 3.6-fold lower among those in the 12-week group but that did not impact antibody level decline over 9 weeks post-final vaccination. The researchers noted the extended interval has the potential to enhance and extend humoral immunity among older individuals, although further research is needed to assess long-term immunity and clinical protection. This data—as well as data from a predictive modeling study from US researchers published in The BMJ showing delaying mRNA vaccine second doses could reduce deaths, hospitalizations, and infections among people aged 65 and older if certain conditions are met—could inform other countries’ vaccination efforts and recommendations.
PFIZER-BIONTECH VACCINE STORAGE The European Medicines Agency Committee for Medicinal Products for Human Use (CHMP) updated its recommendation regarding the storage of the Pfizer-BioNTech SARS-CoV-2 vaccine. The new guidance extends the duration that thawed but unopened/undiluted vials of the vaccine can be stored at normal refrigerator temperatures (2-8°C; ~36-46°F) from 5 days to 31 days. This change will facilitate vaccination efforts, particularly those conducted outside of healthcare facilities, by reducing the dependence on ultra-cold freezers. The CHMP approved the change based on an assessment of “additional stability study data” submitted by BioNTech. The US FDA previously extended the storage period for frozen vials at regular freezer temperature to 2 weeks, but it has not extended storage for thawed vials. The US FDA guidance continues to limit the storage of thawed vials at refrigerator temperatures to 5 days.
INDIA India’s cumulative COVID-19 caseload passed 25 million today, as Cyclone Tauktae hit the western states of Gujarat and Maharashtra, complicating pandemic response efforts in those already hard-hit states. Although India recently reported a decline in new COVID-19 cases, the number of daily deaths remains above 4,000, and health experts estimate the true burden of COVID-19 in the country to be much higher due to poor testing availability, fear and stigma of getting tested, and limited health service capacity especially in rural areas. In Mumbai, the number of new cases has dropped precipitously, and New Delhi is beginning to see shrinking caseloads, with some experts attributing the declines to strict and tightly enforced lockdowns. Others lament the lack of adequate preparedness and government-facilitated response, especially given India’s size, population density, and social structure.
In a comment published online May 14 by The Lancet, a group of clinicians, public health professionals, and scientists working in India or with collaborators in the country endorsed the national action plan put forth by The Lancet COVID-19 Commission India Task Force and outlined 8 steps for the international community to help ameliorate the crisis in India, including expanding healthcare capacity, scaling up mass vaccination and testing, and stepping in to ensure the global supply chains of medications produced in India is not interrupted.
SINGAPORE With the number of new COVID-19 cases rising in Singapore, health officials are expressing concern over unknown chains of community transmission, and the government has tightened measures meant to control the virus’s spread. Increased restrictions on travel and in-person activities—such as restaurant dining and limitations on social gatherings—began on May 16 and will run through June 13. The number of new cases without a link to an identified case has more than doubled over the previous week. Overall, 71 new cases have been identified in the last week, up from 48 the previous week, with a cluster linked to Changi Airport. Singapore’s increase in cases and move to tighten restrictions is hindering its ability to meet criteria to open an “air travel bubble” with Hong Kong, which was expected to open on May 26. Officials plan to reevaluate the launch of the travel bubble no earlier than June 13.
UK EASING RESTRICTIONS The United Kingdom moved this week into their third of 4 phases to lift COVID-19 restrictions. In this phase, pubs and restaurants are allowed to serve customers indoors, museums and movie theaters can open, and more people from separate households can gather. Additionally, travel restrictions have been somewhat eased, with destination countries classified as “red,” “amber,” or “green” depending on each country’s situation. The different color classifications also outline various requirements for quarantine following travel. Supporting the easing of restrictions is the UK’s strong vaccination program, which has delivered a first dose to nearly 70% of its population. However, the proportion of the population fully vaccinated remains closer to 36%.
While the vaccines appear to be contributing to decreasing COVID-19 cases overall, the UK government is concerned with the spread of the B.1.617.2 variant that was first identified in India. Current evidence suggests that the B.1.617.2 variant may be even more transmissible than the B.1.1.7 variant but current evidence suggests it does not cause more severe disease. Still, the UK has pledged to speed up its vaccinations in order to remain abreast of the variant’s spread. It is hoped that the B.1.617.2 variant will not disrupt further relaxations of COVID-19 restrictions or, in a worse case, cause the country to reinstate stricter measures.
GLOBAL EXCESS MORTALITY On May 14, The Economist published statistical modeling that estimates 7-13 million people have died worldwide as a result of the COVID-19 pandemic, approximately 2-4 times the deaths reported in the official WHO data. The model is based on 121 indicators and modeled excess mortality in more than 200 countries. They used a machine learning approach to identify relationships between the various indicators and excess mortality in countries that report it and then used those relationships to project excess mortality at the national level for all of the included countries.
The model estimates 10 million excess deaths (95% CI: 7.1-12.7 million) globally. Notably, excess deaths include those directly attributable to COVID-19 as well as those due to downstream effects of the pandemic. The Economist researchers assert that the most severe impact of excess mortality is in low- and middle-income countries, where SARS-CoV-2 testing is less widespread, which could result in the underreporting of COVID-19 cases and deaths. In India, the researchers estimate that 20,000 people are dying each day, 5 times the 4,000 deaths per day reported in India’s official COVID-19 data. Some countries—including Australia, New Zealand, and Norway—actually have negative excess mortality (ie, fewer deaths than expected based on historical data). These countries have faced relatively mild COVID-19 epidemics, and the decreased mortality could be a result of COVID-19 measures (eg, physical distancing, mask use) on other causes of deaths, such as seasonal influenza.
Notably, the researchers estimate that on a per capita basis, the impact of COVID-19 has been worse in higher-income countries. They posit that this could be driven by differences in population age. Because older individuals are at elevated risk for severe COVID-19 disease and death, countries with older populations—which tend to be higher-income countries—may have elevated COVID-19 mortality, while lower-income countries with younger populations may have higher incidence but lower mortality.
COVID-19 “LONG HAULER” REGISTRIES Long-term symptoms following recovery from acute SARS-CoV-2 infection continue to be described for a nontrivial portion of the population. Commonly described symptoms of so-called “long COVID-19,” also known as Post-Acute Sequelae SARS-CoV-2 infection (PASC), include brain fog, trouble breathing, and fatigue. To gain insight into lasting COVID-19 symptoms, some US state and federal lawmakers are pushing to create COVID-19 registries to track such cases. These registries could be modeled on the registry created to track chronic illnesses among those exposed to toxins during the September 11, 2000, World Trade Center attacks. New York state lawmakers have drafted legislation for a registry based on this model. Through these voluntary registries, researchers will be able to analyze possible patterns within the data to target potential treatments. Already, some studies are underway to evaluate the effect of vaccination on improving “long COVID-19” symptoms. One survey indicated improvement of lasting symptoms in just over half of 812 people surveyed following their first vaccine dose. The data also showed mRNA vaccines appear to have a greater effect on symptom improvement compared to other types of vaccines.
“COVID HEART” According to a case-control study published in JACC: Cardiovascular Imaging, SARS-CoV-2 infection does not impact the heart more than other viral illnesses. The issue of “COVID-19 Heart” was first introduced into mainstream media early in the pandemic, when some researchers expressed concern over the potential impact of SARS-CoV-2 infection on cardiovascular health. Results from this recent study, which examined 74 seropositive healthcare workers 6 months post-infection and 75 seronegative matched control subjects, showed no differences between cardiac structure, function, tissue or biomarkers. Some experts say data from this study, along with information from several others, should be sufficient evidence to show COVID-19 does not cause cardiac problems. Though COVID-19 can result in some cardiac issues, like other viral diseases, science communication in the future must do a better job of explaining the scientific review process, methodology, and study implications, experts maintain.
by ponchi101 The Global Excess Mortality numbers go along with what we have been saying here since the beginning. There is no way that the death numbers are accurate, with so many "smaller" countries unable to report properly. I doubt the numbers from Ecuador or Venezuela can be believed, for example.
Side note. An article I read yesterday claims that at the rate Venezuela is vaccinating people, the country will reach full vaccination in 10 years.
by ti-amie
by Suliso Argentina has now overtaken Brazil as the worst affected country in South America (per population).
by ponchi101
Suliso wrote: ↑Thu May 20, 2021 12:12 pm
Argentina has now overtaken Brazil as the worst affected country in South America (per population).
They have a good percentage of vaccination with Sputnik V vaccines, so they can be taken as a model for that one.
It is simple: the economic collapse of the country is accelerating quickly. Inflation is at 50%, people need to go out to work and make a living. It is spiraling again into 1980's economic failure. I wish Drop would be around a but more often so he could tell us.
---0---
WaPo photos: I did not even need to go to the essay to know that the main shot of the two people crossing the river was between Colombia and Venezuela.
---0---
India. Now they are dealing with something called "black fungus". True bad luck.
And guess who is being proposed for a job in India, which he will take in a second as his other option right now is a 9-5, rat-race, sit-in-your-cubicle position for 20% of his usual salary?
by ti-amie This is worrying.
Eric Feigl-Ding @DrEricDing
Epidemiologist & Health Economist. Health Policy & Social Justice. Senior Fellow, FAS. Former 16 yrs
@Harvard. @JohnsHopkins& @HarvardEPI alum.
After 15 million doses of J&J vaccines earlier ruined by Emergent’s factory, it’s further revealed >100 mil doses are on hold as FDA checks for possible contamination. Emergent has long troubling record—but Trump WH awarded big contract anyway.#COVID19
2) In more than three hours of testimony before a House subcommittee, the chief executive, Robert G. Kramer, calmly acknowledged unsanitary conditions, including mold and peeling paint, at the Baltimore plant.
3) He conceded that Johnson & Johnson — not Emergent — had discovered contaminated doses, and he fended off aggressive questions about his stock sales and hundreds of thousands of dollars in bonuses for top company executives.
4) Emergent’s Baltimore plant was forced to halt operations a month ago after contamination spoiled the equivalent of 15 million doses. He said he took “very seriously” a report by federal regulators that revealed manufacturing deficiencies & accepted “full responsibility.”
5) Mr. Kramer’s appearance before the House Select Subcommittee on the Coronavirus Crisis, offered the public its first glimpse of the men who run Emergent, a politically connected federal contractor that dominates a niche market in biodefense preparedness.
6) Testifying virtually, Mr. Kramer was joined by the firm’s founder and executive chairman, Fuad El-Hibri, who over the past two decades has expanded Emergent from a small biotech outfit into a company with $1.5 billion in annual revenues.
7) Executive compensation documents made public show that the company’s board praised Mr. El-Hibri, who cashed in stock shares and options worth more than $42 million last year, for “leveraging his critical relationships with key customers, Congress and other stakeholders.”
8) Among those members of Congress is Representative Steve Scalise of Louisiana, the No. 2 House Republican. Federal campaign records show that since 2018, Mr. El-Hibri and his wife have donated more than $150,000 to groups affiliated with Mr. Scalise.
9) Mr. Kramer’s estimate of 100 million doses on hold added 30 million to the number of Johnson & Johnson doses that are effectively quarantined because of regulatory concerns about contamination.
10) Federal officials had previously estimated that the equivalent of about 70 million doses — most of that destined for domestic use — could not be released, pending tests for purity.
11) House Democrats began their inquiry into Emergent after The New York Times documented months of problems at the Baltimore plant, including failure to properly disinfect equipment and to protect against viral and bacterial contamination.
12) Hours before the hearing, committee released confidential audits that cited repeated violations of manufacturing standards. A top federal manufacturing expert echoed those concerns in a June 2020 report, warning that Emergent lacked trained staff and adequate quality control.
13) Mr. Kramer initially testified that contamination of the Johnson & Johnson doses “was identified through our quality control procedures and checks and balances.” But under questioning, he acknowledged that a Johnson & Johnson lab in the Netherlands had picked up the problem.
14) Johnson & Johnson hired Emergent to produce its vaccine and, at the insistence of the Biden administration, is now asserting greater control over the plant.
15) The government awarded Emergent a $628 mil contract last year. Among other things, lawmakers are looking into whether @emergentbiosolu leveraged its contacts with a top Trump official, Dr. Robert Kadlec, to win that contract and whether officials ignored known deficiencies.
16) Emergent is skilled at working Washington. Its board is stocked with former government officials, and Senate lobbying disclosures show that the company has spent an average of $3 million a year on lobbying over the past decade.
17) Democrats pressed Kramer & El-Hibri about contacts with Dr. Kadlec, who had consulted for Emergent. Emergent agreed to pay him $120,000 annually 2012-2015, and that he recommended that Emergent be given a “priority rating” so that the contract could be approved speedily.
18) The government has so far paid Emergent $271 million, even though American regulators have yet to clear a single dose of vaccine produced at the Baltimore plan
19) A Times investigation found that Emergent has exercised outsize influence over the Strategic National Stockpile, the nation’s emergency medical reserve; in some years, Emergent’s anthrax vaccine has accounted for as much as half the stockpile’s budget.
20) The investigation found that some federal officials felt the company was gouging taxpayers — an issue that also came up at Wednesday’s hearing when @RepMaloney, demanded to know how much it cost to make the vaccine and what it sold for. Mr. El-Hibri promised info later.
• • •
ponchi101 wrote: ↑Thu May 20, 2021 2:16 pm
India. Now they are dealing with something called "black fungus". True bad luck.
And guess who is being proposed for a job in India, which he will take in a second as his other option right now is a 9-5, rat-race, sit-in-your-cubicle position for 20% of his usual salary?
If you get vaccinated (with Pfizer/Moderna), you should be ok in India. I've been talking to colleagues there pretty much daily (about COVID) and while it's really bad - about 15% of our team there have been sick at any one time over the past weeks and many with milder symptoms are working from home while ill - if you have money and aren't needing to be hospitalized, the situation is tenable, the larger businesses there have been adapting. This isn't to minimize the depth of the crisis there for the wider population, just a comment on your potential health and safety.
by Suliso Your colleagues have been "lucky". My company also has a site in India and currently almost 30% of employees are off work. Either sick themselves or as close contacts to someone. True about vaccines - according to the latest news mRNA vaccines are 80%+ effective against all known variants so far.
by ponchi101 Going to GA on Tuesday (red eye flight). Should be in Macon by 3PM. Undecided between PF/Bio, MOD or J&J: And after that post by Dry, even more. J&J allows me to be ready to go to work ASAP. PF/Bion seems safer.
So, I will be vaccinated. And I have really made it clear to the possible contractor that I will do anything to get that India job, but there might be no job at all. The situation there is dire.
by ptmcmahon Pfizer shot one for me today.
by Suliso
ponchi101 wrote: ↑Thu May 20, 2021 7:23 pm
So, I will be vaccinated. And I have really made it clear to the possible contractor that I will do anything to get that India job, but there might be no job at all. The situation there is dire.
Good luck with the job! I wasn't aware there is any oil or gas in India...
by mmmm8
ponchi101 wrote: ↑Thu May 20, 2021 7:23 pm
Going to GA on Tuesday (red eye flight). Should be in Macon by 3PM. Undecided between PF/Bio, MOD or J&J: And after that post by Dry, even more. J&J allows me to be ready to go to work ASAP. PF/Bion seems safer.
So, I will be vaccinated. And I have really made it clear to the possible contractor that I will do anything to get that India job, but there might be no job at all. The situation there is dire.
So, to me, the choice is simple. Just with one shot of Pfizer/Moderna, you get somewhere between 52 and 89% protection, likely 70-80%. With J&J you get nearly the same protection but no second shot to get even more protection. Take Pfizer/Moderna and then get the second shot when you can. As we discusse, UK/Canada are allowing 3-4 months between the two shots.
ponchi101 wrote: ↑Thu May 20, 2021 7:23 pm
So, I will be vaccinated. And I have really made it clear to the possible contractor that I will do anything to get that India job, but there might be no job at all. The situation there is dire.
Good luck with the job! I wasn't aware there is any oil or gas in India...
There is oil and gas everywhere in the world. In 2019, if you remember, I was in Albania, not totally famous for its oil production. Yet they pump a bit over 100,000 barrels a day, which are very useful for internal consumption.
Heck, I am in a very long list for a possible job in Switzerland. The whole point of oil is that, if the economics work out, the technology to pump it out is by now very well known. And, as we have discussing, even in countries that are moving to alternative energies, there are still cars to fill up.
by MJ2004 Got Pfizer shot 2 yesterday, just a bit of arm soreness. Otherwise feel fine.
At this point in the U.S., any adult who doesn't have the shot is because they don't want it. I have an otherwise very rational co-worker who isn't getting the shot because she fears miscarriage. Mind you, she is NOT pregnant. Those anti-vax rumors are killer. Quite literally. I heard a response on NPR to that particular rumor, the doctor being interviewed saying "there is no biological pathway by which that could happen", i.e. that future miscarriages could occur due to the vaccine. Sigh...
by Suliso Covid prevalence is much reduced in USA, but hardly completely gone. Still about 30k new infections per day and 500-700 deaths. In absolute numbers that's still good for #3-4 on the global list.
by ptmcmahon
MJ2004 wrote: ↑Fri May 21, 2021 2:56 am
Got Pfizer shot 2 yesterday, just a bit of arm soreness. Otherwise feel fine.
At this point in the U.S., any adult who doesn't have the shot is because they don't want it. I have an otherwise very rational co-worker who isn't getting the shot because she fears miscarriage. Mind you, she is NOT pregnant. Those anti-vax rumors are killer. Quite literally. I heard a response on NPR to that particular rumor, the doctor being interviewed saying "there is no biological pathway by which that could happen", i.e. that future miscarriages could occur due to the vaccine. Sigh...
Likewise, shot 1 just gave me a little arm soreness, no more than any other shot. Still feel fine today otherwise.
In our province they opened 25-29 yesterday for booking..so getting close to "all" adults able to book soon.
by ponchi101 I was able to book my shots for Tuesday 25th. And of course, I did not do it sooner because I am not there. At a Kroger, basically no questions asked (other than regular forms items like "Am I feeling well?"). In theory, I will get Pfizer.
by ptmcmahon
MJ2004 wrote: ↑Fri May 21, 2021 2:56 am
Got Pfizer shot 2 yesterday, just a bit of arm soreness. Otherwise feel fine.
At this point in the U.S., any adult who doesn't have the shot is because they don't want it. I have an otherwise very rational co-worker who isn't getting the shot because she fears miscarriage. Mind you, she is NOT pregnant. Those anti-vax rumors are killer. Quite literally. I heard a response on NPR to that particular rumor, the doctor being interviewed saying "there is no biological pathway by which that could happen", i.e. that future miscarriages could occur due to the vaccine. Sigh...
Further to that point... after being "behind" for a long tine...
Canada now has a higher % of people with first dose than US now.
by mmmm8
Suliso wrote: ↑Thu May 20, 2021 7:20 pm
Your colleagues have been "lucky". My company also has a site in India and currently almost 30% of employees are off work. Either sick themselves or as close contacts to someone. True about vaccines - according to the latest news mRNA vaccines are 80%+ effective against all known variants so far.
Yeah, obviously "lucky" a relative term, we did lose a colleague (she was only 36!). I think it depends a lot on location (some Indian states doing better than others) and also on whether one can stay at home. All our colleagues are working from home. Does your company have any manufacturng/agricultural sites that have been in person?
by atlpam Canada has had much more severe lockdowns & penalties, so it's not surprising that there is a lot of pent up demand to be vaccinated and have more freedom. Also with a much larger population, it's expected it would take longer for the US to reach the same % level. I wonder how long before a trip from Vermont to Quebec will be a possibility.
by MJ2004India and Pfizer hit impasse over vaccine indemnity demand
NEW DELHI/NEW YORK, May 21 (Reuters) - Pfizer and the Indian government are at loggerheads over a demand by the U.S. drugmaker for legal protection from any claims linked to the use of its COVID-19 vaccine in one of the world's biggest markets, two sources told Reuters.
India has not given any manufacturer of a COVID-19 vaccine indemnity against the costs of compensation for any severe side effects, which is a condition Pfizer has obtained in many countries where its shots have already been widely rolled out, including Britain and the United States.
"The whole problem with Pfizer is the indemnity bond. Why should we sign it?" an Indian government source with direct knowledge of the matter told Reuters.
"If something happens, a patient dies, we will not be able to question them (Pfizer). If somebody challenges in a court of law, the central government will be responsible for everything, not the company," the source added.
Pfizer declined to comment, citing ongoing discussions with the government. India's health ministry did not reply to Reuters requests for comment on Friday.
The second source said Pfizer has been consistent in its position on indemnity and is not planning to change its approach for a deal with India.
Both sources declined to be named as they were not authorised to talk to the media.
India, which is facing a shortage of shots as coronavirus cases soar, pledged last month to fast-track approvals for overseas vaccine makers including Pfizer, Moderna and Johnson and Johnson.
However, none have since sought permission from India's drug regulator to sell their vaccine in the country, which has a population of 1.35 billion.
The second source said the other issue being discussed between Pfizer and New Delhi was the Indian government's insistence on a local trial for any vaccine approval. The source added that Pfizer cannot finalize terms of a supply agreement, including indemnity, if the vaccine is not first authorized for use in India.
Pfizer withdrew its application for emergency use authorisation for the vaccine developed with Germany's BioNTech in February after India insisted on such a trial.
But three other shots on sale in India, developed by AstraZeneca, Russia's Sputnik V and Bharat Biotech in collaboration with state-run Indian Council of Medical Research, have completed the small-scale safety trials.
Albert Bourla, Pfizer's chief executive said on May 4 that he was hopeful that the government would change its policy of local trials and that a path to delivering the drugmaker's shots in India could be found.
A third source told Reuters that India's foreign minister would visit the United States this month or in early June to try and address Pfizer's concerns and ease exports of vaccine raw materials to India.
The Indian foreign ministry did not immediately respond to a request for comment. (Reporting by Neha Arora and Carl O'Donnell; Additional reporting by Rupam Jain; Editing by Krishna N. Das and Alexander Smith)
Suliso wrote: ↑Thu May 20, 2021 7:20 pm
Your colleagues have been "lucky". My company also has a site in India and currently almost 30% of employees are off work. Either sick themselves or as close contacts to someone. True about vaccines - according to the latest news mRNA vaccines are 80%+ effective against all known variants so far.
Yeah, obviously "lucky" a relative term, we did lose a colleague (she was only 36!). I think it depends a lot on location (some Indian states doing better than others) and also on whether one can stay at home. All our colleagues are working from home. Does your company have any manufacturng/agricultural sites that have been in person?
We have R&D site with 95% of people working in the lab or directly overseeing those who do. So no chance of widespread home office.
by Suliso I'll probably be the last on this board to get my first vaccine dose...
by ponchi101 It's looking that way.
I decided to go to the USA because here they are using solely Sinovax, and even if they were to call me tomorrow I am very hesitant about that one. Plus, of course, I have not received any confirmation of when will my turn be, as I am in population 3.
India.
Are they dense? Do the understand the concept of EMERGENCY? You are going to test the vaccine which, for all practical purposes is being tested daily on the US population?
Politicians can be deadly with increasing frequency.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 165 million cumulative cases and 3.4 million deaths worldwide as of 4:45am EDT on May 21.
Following a brief decrease, India’s daily mortality is once again increasing, setting new global records. On May 18, India reported 4,529 deaths, surpassing the previous record for single-day mortality (US: 4,475 deaths on January 12, 2021). With 4,150 deaths per day on May 18, India also holds the global record for average daily mortality. India is the only country to report an average of more than 4,000 deaths per day, and it has hovered around 4,100 deaths per day for the past several days.
On Tuesday, we looked at state-level test positivity in the US, and in light of numerous ongoing surges in countries around the world, we will take a similar look at some national trends in test positivity. Of the top 20 countries* globally, 10 are in Central and South America (including 5 of the top 7), plus Trinidad and Tobago and the Dominican Republic in the Caribbean; 4 are in Africa; and 3 are in Asia. Ukraine is the only country in Europe. Notably, 13 of these countries are reporting test positivity of more than 20%, including 5 with more than 30%: Nepal (44.2%), Paraguay (36.9%), Maldives (31.3%), Argentina (30.6%), and Ecuador (30.6%).
*Oman would be in the top 20, based on its most recent report, but it has not updated its test positivity data since July 2020.
Fortunately, fewer than half of these countries are reporting increasing trends in daily incidence. In terms of the relative biweekly change, 9 are reporting positive values, 7 of which are greater than +10% and 4 of which are greater than +50%. Maldives is reporting the largest biweekly increase, with +177%, followed by Trinidad and Tobago (+94%), the Dominican Republic (+89%), and Nepal (+57%). The high test positivity in these countries could result in substantial underreporting of COVID-19 incidence, which is particularly concerning in light of their increasing trends. Maldives may be the most concerning country on this list. In addition to having the largest biweekly increase, it is also reporting the world’s highest per capita daily incidence. At more than 2,500 daily cases per million population, Maldives is reporting more than 2.5 times the per capita incidence of the next closest country in this group (Uruguay; 906). Notably, while Nepal’s overall biweekly trend is positive, it does appear to have passed a peak and is now declining.
While their relative biweekly increases do not necessarily reflect it, several other countries also are reporting concerning increases in daily incidence. Following approximately 2 weeks of decreasing trends, both Uruguay and Argentina are reporting increasing daily incidence. In fact, Argentina has already surpassed its previous peak, and Uruguay could soon do so as well, if it continues on its current trajectory. Additionally, Bolivia’s daily incidence has increased steadily since late March, briefly surpassing its previous record on May 17. Paraguay’s epidemic has exhibited a protracted but slow increase since early February, and it is currently reporting near its record high, set on April 23.
Notably, most of the countries with high test positivity are reporting decreasing daily incidence, including 4 that have decreased by more than one-third over the past 2 weeks: Madagascar (-49%), Tunisia (-36%), the Democratic Republic of Congo (-35%), and Ecuador (-33%).
Several countries with biweekly increases in daily incidence also are reporting increasing test positivity, which signals that testing capacity is falling further behind as the surges worsen. The Dominican Republic reported a steady decline in test positivity in early 2021; however, it recently reported a considerable increase, from 11.4% on May 10 to 15.3% on May 15 (its most recent report), an increase of more than one-third over only a few days. After a prolonged decline from late January to April, Bolivia’s test positivity has increased from a low of 9.5% on April 17 to nearly 25% on May 17 before falling slightly to 22.3%. Trinidad and Tobago’s test positivity accelerated consistently from 1% in late February to a high of 38.2% on May 10 before falling sharply to 20.2% on May 11 (its most recent report). Maldives also reported a concerning accelerating trend, up from 3.2% on April 16 to 30.9% on May 19, slightly more than a month later. While Nepal’s test positivity increased from less than 2% in early March to a peak of more than 45% on May 13, it has declined steadily in the few days since then. In contrast to other countries discussed here, this is an encouraging indication that its testing capacity is beginning to move in the right direction during its ongoing surge, even though test positivity remains elevated.
Global Vaccination
The WHO reported 1.42 billion doses of SARS-CoV-2 vaccines administered globally as of May 20, including 666 million individuals with at least 1 dose. Our World in Data reported 1.59 billion cumulative doses administered globally. The global cumulative total continues to increase at approximately 13% per week. Daily doses administered continue to increase, up to a new record of 26.0 million doses per day. Our World in Data estimates there are 376 million people worldwide who are fully vaccinated, corresponding to approximately 4.8% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.9 million cumulative cases and 584,975 deaths. The current average daily incidence—27,788 new cases per day—is the lowest since June 18, 2020. The average daily COVID-19 mortality fell below 500 deaths per day for the first time since March 31, 2020.
US Vaccination
The US has distributed 352 million doses of SARS-CoV-2 vaccines and administered 279 million. After more than a month of decline, the daily doses administered* increased slightly on May 15 to 1.6 million doses per day. Approximately 1.0 million people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 160 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 48% of the entire US population. Among adults, 61% have received at least 1 dose, and 4.1 million adolescents aged 12-17 years have received at least 1 dose. A total of 127 million people are fully vaccinated, which corresponds to 38% of the total population. Among adults, 48% are fully vaccinated, and 1.8 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 85% with at least 1 dose and 73% fully vaccinated. In terms of full vaccination, 65 million individuals have received the Pfizer-BioNTech vaccine, 51 million have received the Moderna vaccine, and 9.8 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 33.1 million cumulative cases and 588,559 deaths in the US as of 10:15am EDT on May 21.
BRAZIL PEDIATRIC MORTALITY Since early in the pandemic, it was clear that older adults were at elevated risk for severe COVID-19 disease and death. In contrast, Brazil’s epidemic is exhibiting elevated mortality among children and infants. A report by The New York Times describes some of the factors that could be contributing to increased pediatric mortality. Since the onset of the pandemic, Brazil has reported at least 832 deaths among children aged 5 years and younger, which likely is a “substantial undercount.” In fact, researchers at the University of São Paulo estimate that the actual total is closer to 2,200, including more than 1,600 infants younger than 1 year. For comparison, the US has reported only 139 deaths among children aged 4 years and younger. While the age range is slightly smaller than in Brazil’s tally, the US has a population approximately 50% larger than Brazil’s.
Myriad factors could be contributing to Brazil’s high pediatric mortality. The P.1 variant that is circulating widely in Brazil has been linked to increased disease severity and mortality among pregnant women as well as elevated risks of stillbirth or premature delivery. A lack of testing leads to untimely or inadequate access to health care for children with COVID-19, and poor and overwhelmed health systems also could result in increased mortality among this population. Underlying health conditions—some related to poverty and food insecurity—can exacerbate the risk of severe disease in children, but Brazil’s pediatric COVID-19 mortality also is elevated in otherwise healthy children. Further study is needed to better characterize the factors influencing elevated mortality among children and infants in Brazil.
COVAX MANUFACTURING TASK FORCE The COVAX facility is struggling to reach its goal of providing 2 billion doses of SARS-CoV-2 vaccines to low- and middle-income countries (LMICs) by the end of this year. So far, COVAX has delivered just over 68 million doses, or 3.4% of its goal. Experts maintain the 3 primary obstacles preventing COVAX from reaching its goal include a lack of funding, vaccine supply constraints, and a lack of willingness from some countries to share vaccine doses. But they also argue all of these problems are solvable. WHO Regional Director for Africa Dr. Matshidiso Moeti on Thursday appealed to rich nations to share their surplus vaccine doses, commending France for shipping jabs to Mauritania and the US for pledging to donate 80 million of its excess doses. Yet more needs to be done, as the world continues to stumble in ramping up manufacturing of vaccines that were developed with record speed.
In an effort to address bottlenecks in the supply of vaccine raw materials and trade barriers impacting the supply chain, the co-leads of COVAX—the Coalition for Epidemic Preparedness Innovations (CEPI), WHO, Gavi, and UNICEF, working in partnership with the Bill & Melinda Gates Foundation, International Federation of Pharmaceutical Manufacturers and Associations (IFPMA), Developing Countries Vaccine Manufacturers Network (DCVMN), and Biotechnology Innovation Organization (BIO)—announced the launch of the “COVAX Manufacturing Task Force.” The Task Force plans to engage additional partners within the clinical development, manufacturing, and regulatory sectors, as well as governments, regional entities, and other institutions, to address short-, medium-, and long-term objectives that aim to alleviate shortages of raw and single-use materials, speed delivery of such materials, and encourage cooperation among manufacturers.
EMERGENT VACCINE PRODUCTION FACILITY On May 19, the US House of Representatives Select Subcommittee on the Coronavirus Crisis held a hearing as part of an investigation into Emergent BioSolutions’ failures to address manufacturing problems at its Baltimore, MD, (US) plant that led to the contamination and subsequent destruction of 15 million doses of the J&J-Janssen SARS-CoV-2 vaccine made at the facility. The hearing comes 1 month after the US government put J&J in charge of the plant following revelations that Emergent, under federal contract to make key materials for J&J-Janssen and AstraZeneca-Oxford vaccines, cross-contaminated ingredients for the different jabs.
At the hearing, Emergent executives testified for more than 3 hours about manufacturing deficiencies and disclosed for the first time that more than 100 million doses of the J&J-Janssen vaccine are on hold and under review by the US FDA, 30 million more than previously recognized. Emergent CEO Robert G. Kramer acknowledged that it was J&J, not Emergent, that first discovered the contaminated doses. The subcommittee also released a preliminary report outlining details about unaddressed issues at the Emergent plant, including unsanitary conditions, mold, poor employee training, and insufficient attention paid to operating protocols. In 2020, the federal government awarded Emergent a $628 million contract to produce SARS-CoV-2 vaccines, and so far has paid $271 million. However, the FDA has yet to clear for use a single dose of vaccine produced at the plant. The FDA published a report in April stating the Baltimore facility was unsuitable to produce vaccine doses, and Emergent agreed to pause production of materials until issues identified in the report are resolved.
EU TRAVEL The European Council on May 20 adopted updated recommendations for non-essential travel into the region, a move that could increase the number of foreign travelers able to enter the EU. The bloc has had many restrictions on the movement of travelers during the COVID-19 pandemic, with this new policy marking a turning point for pandemic policies. The plan would grant anyone vaccinated with an EU-approved COVID-19 vaccine permission to travel, greatly increasing the potential for tourism. This rule could open up travel to an increasing number of foreign individuals but would restrict those who received Russian- or Chinese-made vaccines, none of which are authorized in the EU. Bloc leadership has shared that countries may still implement more restrictive guidance if they choose, but they are urging member states to move toward more open borders as larger percentages of adults receive SARS-CoV-2 vaccines. The recommendations allow for an “emergency brake mechanism,” under which member countries can adopt urgent, temporary travel restrictions if a variant of concern or interest is detected.
MODERNA VACCINE PRODUCTION In an effort to further scale up SARS-CoV-2 vaccine production capacity, the Swiss government is supporting efforts to hire temporary personnel to staff a facility operated by the Lonza Group. The Lonza facility in Visp, Switzerland, manufactures ingredients that are needed to produce Moderna’s SARS-CoV-2 vaccines, and Lonza recently added 3 new production lines to meet the ongoing demand. Reportedly, Lonza was struggling to find qualified personnel to operate the production lines, but the Swiss government was able to identify 75 personnel with the required expertise from within government agencies as well as academic institutions. Lonza anticipates further efforts to increase production capacity, up to 600 million doses per year. Lonza will require additional personnel in the future, as the current temporary employees are not a long-term solution.
INDIA VACCINATIONS At the beginning of May, India expanded eligibility for SARS-CoV-2 vaccinations to its entire adult population. The country has faced an incredibly challenging surge in new COVID-19 cases, increasing the urgency to vaccinate its population. However, access to vaccines is being hindered by the current outbreak, lockdowns, cost, and production backlogs. The government recently estimated it would be able to produce 1.46 billion doses of the authorized AstraZeneca-Oxford, Sputnik V, and Covaxin vaccines between the months of August and December, but lower-than-expected production estimates reported to Reuters fall short of the government’s goal. In a further setback, the Indian government and Pfizer have reached an impasse over the company’s demand for indemnity against any claims related to its vaccine. In addition to questions over vaccine supply, the influence of mis- and disinformation surrounding COVID-19 and vaccines is hampering willingness among some to be vaccinated, particularly those in rural areas. It is reasonable to expect that the severity of the ongoing outbreak, and other events like Cyclone Tauktae, have negatively impacted the country’s vaccination efforts, but it will be troublesome if a high prevalence of vaccine hesitancy impedes vaccination rates as more doses become available.
CHINA VACCINE DONATIONS China on May 20 said it has donated or sold at “favorable prices” its homegrown vaccines to nearly 40 African countries, describing its actions as purely altruistic. The announcement is the latest example of how geopolitics is intensifying global moves on what is being called vaccine diplomacy. A day before, the 15-member UN Security Council unanimously approved a presidential statement calling for the accelerated availability of SARS-CoV-2 vaccines for Africa and expressing concern that the continent has received only about 2% of all doses administered worldwide. Also at the Security Council meeting, organized by China, which holds the body’s rotating presidency for May, member states heard from Africa Union Commission Chair Moussa Faki Mahamat, who said vaccine access is the biggest challenge Africa faces, amid increasing numbers of COVID-19 cases and related deaths. The same day, the US government said it will prioritize sending excess vaccine doses to Latin America over concerns that China is using vaccine donations to the region to influence nations there to drop diplomatic recognition of Taiwan. Both Paraguay and Honduras have signaled they might switch ties from the US to China, which claims Taiwan as its territory, in order to gain access to Chinese vaccine supplies. Chinese and Taiwanese officials have accused one another of politicizing pandemic responses, accusations both sides deny.
AFRICA R&D FUNDING Global health experts affiliated with academic, medical, and nonprofit institutions in Africa, the UK, and the US published an open letter to African political and research leaders, calling on them to expand funding and support for research and development capacity on the continent. In 2006, African Union member countries pledged to allocate at least 1% of their GDP to research and development; however, by 2019, the average across the continent remained below 0.5% of GDP—compared with 1.7% globally. The authors emphasized that the COVID-19 pandemic should serve as a wake-up call and inspire investments to avert future health emergencies. They argue that a “glaring lack of leadership” at the national level is driving “the chronic lack of government investment—and regard—for science,” both for COVID-19 and the broader scope of infectious diseases. The absence of political priority has driven an “overreliance on international funding” across Africa, and as COVID-19 forced countries to focus inward, international funding support dwindled. The group previously penned a letter published in Nature Medicine that called on international funders of science and development in Africa to recognize power imbalances, include more Africa-based programs in their investments, and more equitably distribute funding.
PFIZER-BIONTECH VACCINE STORAGE The US FDA extended the storage period at refrigeration temperatures for the Pfizer-BioNTech SARS-CoV-2 vaccine. The FDA now permits the vaccine to be stored at refrigerator temperatures—2-8°C (35-46°F)—for as long as 1 month. The change applies only to thawed but undiluted vials. Previously, FDA guidance limited refrigerator storage to only 5 days. Earlier this week, the European Medicines Agency (EMA) announced a similar change. Increasing the time that the vaccine can be stored outside of ultra-cold temperatures will ease logistical and operational burdens for this vaccine and can increase the radius of vaccination efforts from centralized ultra-cold freezers.
IMMUNE RESPONSE The human immune system’s production of antibodies is important to fend off infection with SARS-CoV-2, but more evidence is emerging that the production of autoantibodies—which can target a person’s tissues and organs and interfere with other immune system proteins meant to fight infections—can cause more severe or longer-lasting disease in some COVID-19 patients. In a study published in Nature, Yale University researchers detail how these so-called “rogue autoantibodies” interact with nearly 3,000 human proteins using a novel technology called Rapid Extracellular Antigen Profiling (REAP). The researchers underscored the importance of SARS-CoV-2 vaccination to lower the risk of infection, as autoantibody production was seen in even mild COVID-19 cases, having the potential to cause long-term health consequences. The team’s findings could lead to treatment or prevention strategies for SARS-CoV-2, and the new REAP technology already is being used to identify specific antibody responses for other conditions, including autoimmune diseases, cancer, and neurological illnesses.
VACCINE LOTTERIES In an effort to promote vaccinations, some US states are turning to lotteries to increase interest. In contrast to lotteries to allocate scarce vaccines—such as those proposed and opposed during the pandemic response—these vaccine lotteries are offering the chance for cash payments and other prizes, and eligibility is limited to vaccinated individuals. Under Ohio’s Vax-A-Million lottery, the state government is awarding US$1 million to 1 lucky adult vaccinee each week for 5 weeks. Additionally, the state will award a full 4-year scholarship to 5 vaccinated adolescents aged 12-17 years. Notably, Ohio reported increasing vaccination rates following the program’s announcement—a weekly increase of more than 50%—a potential indication that the program is increasing interest in vaccination. In a similar program, New York state will distribute “scratch-off” lottery tickets to individuals who get vaccinated at some state-run clinics. New York’s “Vax and Scratch” tickets offer a 1-in-9 chance of a prize, ranging from US$20 to US$5 million. Maryland also announced its own vaccine lottery, VaxCash, which will award a total of US$2 million through 40 daily drawings for US$40,000 each and a final grand prize drawing on July 4 worth US$400,000.
OLYMPICS As the 2020 Summer Olympic and Paralympic Games in Tokyo, Japan, rapidly approach, many questions remain regarding the status of the games. According to multiple news media reports, there is growing opposition to the Tokyo Olympics—including among the public, Japan’s health system, and other experts—in light of ongoing struggles to contain the country’s COVID-19 epidemic. Earlier this month, an online petition to cancel the Tokyo Olympics reportedly received approximately 50,000 signatures within the first 24 hours. Recent polling data estimate that 60-80% of the Japanese public oppose hosting the Olympics this summer. The Tokyo Medical Practitioners’ Association recently called on senior Tokyo and Japanese elected officials—including Prime Minister Yoshihide Suga, Tokyo Governor Yuriko Koike, and Olympic Minister Tamayo Marukawa—to cancel the games. Some high-profile athletes also are questioning the safety of holding the Olympics this year.
On May 19, the International Olympic Committee (IOC) provided an update on the situation, emphasizing that it intends to move forward as planned. The IOC statement indicated that the 2020 Summer Olympics have now moved into the final “operational delivery” phase of preparations and that the IOC and Japanese government will “move forward at full speed” to ensure that the Olympics can be hosted in a safe manner, both for the athletes and the Tokyo community. Additionally, the IOC committed to providing additional support for the medical community, including at the Olympic Village and event venues, but it is unclear exactly what that will entail.
Suliso wrote: ↑Fri May 21, 2021 5:17 pm
I'll probably be the last on this board to get my first vaccine dose...
I'm still waiting - no vaccine appoints anywhere in Eastern Ontario until mid June.
by Suliso The effectiveness of Pfizer and AZ vaccines against the Indian variant is almost the same as against the British one after two doses, but significantly less after only one. Moderna was not studied, but given it's similarity to Pfizer likely the same.
by ponchi101 If the virus mutates this fast we will need "boosters" or totally new variations for years to come.
No big news there, I know, but if the rest of the world does not speed up their vaccination, then this is a losing fight. Herd immunity will never be achieved.
by Suliso I think it's been obvious for a while that there won't be a global herd immunity. There isn't one against flu either.
by ponchi101 Correct me here. Global herd immunity for influenza COULD be achieved were it not for the fact that the family of HxNx viruses mutate so fast. We need new vaccines every year because of that.
My understanding is that the HxNx viruses, once you catch them, can trigger immunity for long periods, but only for the specific variant. Since they mutate in less than a year, ergo we need the new vaccines.
Covid would be the same, but first we would need to stop this "initial" wave of contagion.
by MJ2004 Today's FT Big Read covers this very topic:
Vaccines versus variants: Will the world ever reach herd immunity?
New strains and persistent hesitancy to take jabs are complicating government plans to reopen economies
In Ohio, anyone getting a Covid vaccine could win one of five lottery prizes of $1m. New Jersey residents getting the jab are being offered free beers. One site in New York boasted an even more unlikely incentive: a courtesy marijuana joint.
Since the start of the year, America has successfully ramped up its vaccine campaign so that more than 160m people have had at least one shot so far — already meeting the target President Joe Biden had set for July 4.
But if children are included, that is still less than half of the population and in some parts of the country the take-up of vaccines has started to slow. As a result, states and businesses are turning to unorthodox incentives to try to persuade the vaccine hesitant to have a jab.
The UK, one of the other countries with a relatively advanced vaccine programme, is facing some similar problems. Even though hesitancy has fallen as vaccines have been rolled out, take-up is uneven: the majority of the 23 people in hospital in Bolton, north-west England, where the highly transmissible variant first found in India is spreading, had been eligible for vaccination. Only five had been vaccinated.
When the news broke at the end of last year that coronavirus vaccines could be more than 90 per cent effective, it seemed to usher in the prospect of eradicating the disease.
But over the past couple of months, those heady hopes have given way to a more complicated reality. For governments, the appearance of new variants and the persistent hesitancy over vaccines are causing problems for their plans to reopen economies and bring some normality back to life.
For the scientists tracking the pandemic, they have called into question the idea that societies will ever achieve herd immunity, even when there is an abundant supply of vaccines. Herd immunity is the concept that an infectious disease can be eradicated once a sufficient threshold of immunity has been reached — either through already having had the infection or through vaccination. Once that level is passed, so the theory goes, transmission of the virus slows rapidly and it eventually fizzles out.
At the start of the pandemic, some scientists hoped the threshold could be as low as 60 per cent. For most of the last year, Peter Hale, executive director of the Foundation for Vaccine Research in Washington DC, says US health agencies have informally set herd immunity at about 75 per cent.
The trial results for the messenger ribonucleic acid (mRNA) vaccines developed by BioNTech/Pfizer and Moderna seemed to hold the prospect of getting over that hurdle, he says. But given that the B.1.1.7 “UK” variant, which is now dominant in the US, is more transmissible than the strains prevalent in the country last year, the threshold for herd immunity may now be closer to 80 per cent, he says.
In the UK, the potential spread of the Indian variant, which is thought to be even more transmissible, further complicates the country’s calculations about herd immunity.
The result is that if the vaccine-hesitant cannot be persuaded to change their minds and if new variants of the virus continue to spread, many countries will struggle to stamp out Covid-19. Instead, they will remain vulnerable to surges that could require new restrictions.
Lauren Ancel Meyers, director of the University of Texas Covid-19 modelling consortium, says estimates of the proportion of the population that would need to be vaccinated to achieve herd immunity range from 60 to 80 per cent.
“I would not say that herd immunity is out of the question,” she says. “But I would say that herd immunity is pretty unlikely in the foreseeable future, in most communities and in most cities in the US and across the world.”
Viral and human behaviour
The estimates about herd immunity vary so widely because they depend on two unpredictable factors: how the virus behaves and how humans behave. Scientists do not know the extent to which new variants will make the virus more transmissible, nor how many people will get the vaccine.
Natalie Dean, a biostatistician at the University of Florida, says the calculations can often be crude, assuming we are “gas particles bouncing around”, rather than humans with different patterns of contact, with some potential superspreaders.
Throwing vaccines into the mix creates more variables. In the Seychelles, the virus has burst back on to the island despite a high level of vaccination. Some researchers believe this could be because it was relying on a shot from Chinese pharma company Sinopharm, which some studies have shown may be about 50 per cent effective, despite reporting a better efficacy rate in its clinical trial.
Researchers also do not know how effective the shots are at preventing transmission, although early studies suggest they do limit the ability of vaccinated people to pass along the virus. It is also not clear if they will stand up to variants that emerge in the future.
Scientists prefer to think about herd immunity as a cumulative process, rather than a finish line to cross. John Edmunds, a professor at the London School of Hygiene and Tropical Medicine, says it is not an “on-off switch”. The higher the level of immunity in a population, the more it will slow the virus down, he says.
“Eventually, there will be such high levels of immunity in the population that the virus will struggle to spread even without any social restrictions. We are still quite a long way from this point, unfortunately,” he says.
If an area achieves true herd immunity, even cases introduced from outside will fail to spread. Jonathan Ball, a professor of virology at the University of Nottingham, gives measles as an example where we only see outbreaks when the local immunity drops below a certain threshold.
“If you have a small amount of infected people every year coming into the UK with measles, but most of the population is immunised, it simply won’t take off,” he says.
Paul Hunter, professor of medicine at the University of East Anglia, sees “a lot of misunderstanding about what herd immunity means, even among medical people. They confuse reduced transmission through vaccination with true herd immunity.”
Hunter doubts whether herd immunity for the Sars-Cov-2 virus can be achieved with any of the current jabs, given levels of hesitancy and incomplete protection provided by even the best vaccines, which is likely to wane over time.
“For me there are two reasons why misusing the term ‘herd immunity’ may be damaging,” he says. “The first is that some individuals may think wrongly that they don’t need to be vaccinated because they are protected by everyone around them who has been vaccinated. The second is that people are using herd immunity as an argument for relaxing social distancing restrictions too quickly.”
If — as now — large swaths of the world remain unvaccinated, travel between regions risks setting off new outbreaks in areas where vaccine uptake has been erratic and importing variants that can evade vaccination.
“Cities can serve as reservoirs where the virus can continue to thrive and continue to evolve, and we would very likely see variants emerging and spreading around the globe,” Meyers says.
Entrenched resistance
In the US, public health experts believe incentives like free beer — or making vaccination a condition of employment or going to school — may lure the “vaccine indifferent” to get a jab. Jennifer Reich, author of Calling the Shots: Why Parents Reject Vaccines, says the first priority will be encouraging these people who are not intentionally opposed to vaccines, but nor are they motivated to seek one out.
But after this category, it gets trickier. There are several groups of people who are vaccine-hesitant, sceptical or even entrenched anti-vaxxers. In the US, they range from Trump supporters who have long played down the severity of the pandemic, to more nonconformist leftwingers who scorn anything “unnatural”.
Vaccine resistance is not limited to the US. A survey of 14 countries found about six in 10 people were willing to take a vaccine, with France, Singapore and Japan among the least willing, according to the Imperial and YouGov poll between November and February.
More recently, concerns about a rare side-effect from the Oxford/AstraZeneca vaccine have hit confidence: after the shot was suspended in March, the number of people who perceived it was safe dropped substantially in France, Germany, Italy and Spain, according to YouGov.
Across the western world, minority ethnic groups are often more sceptical of the vaccine after a history of scarring experiences with the medical establishment.
In the US, black and Hispanic adults have been the most likely to say that they will “wait and see” before they get vaccinated themselves, according to data from the Kaiser Family Foundation. Income also has an influence: knowing someone who has been vaccinated is an important factor in people’s acceptance, and earlier in the year, households earning over $90,000 were almost twice as likely to know people who had been vaccinated than those with incomes of less than $40,000.
Vaccine hesitancy is falling in the UK but it is still significant in the black, Asian and minority ethnic populations. Some 66 per cent of white people say they would take the vaccine when invited, compared with 55 per cent of black respondents, in an April survey by the Vaccine Confidence Project.
Recent headlines about side-effects — even if they are very rare — have weighed on vaccine acceptance. Alex De Figueiredo, a research fellow at a project run at the London School of Hygiene and Tropical Medicine, says the most common reasons for being unsure about whether to vaccinate were overall safety concerns and the rare blood clotting side-effect in the AstraZeneca vaccine in particular. But he adds that having a choice in vaccines increases confidence, so the UK’s decision to allow under-40s a choice of shot should boost uptake.
Even without concerns about side effects that regulators say are more prevalent in the young, there may be a higher degree of hesitancy in this group because they are less likely to become seriously ill. “The challenge of that right now is that we have inadvertently communicated to young people that they might not really have to worry about this,” Reich says.
Part of the problem may be that Covid-19 vaccines have been sold for their benefits to individuals, rather than as a collective good, she adds. Young people, more likely to be asymptomatic carriers, may have a higher probability of infecting others.
The BioNTech/Pfizer vaccine is now approved in the US for children over 12, giving the potential of vaccinating more of the population. However, experts expect many parents to be hesitant because they will see it as an more of an individual risk/benefit calculation and know far fewer children have become seriously ill with Covid-19.
“We’re already facing the battle among adults and I think we may be facing an even greater battle when it comes to vaccinating children,” says Meyers.
Populations in developing countries tend to be more convinced of the benefits of vaccination, so when they receive more supplies their citizens may be more likely to take it. A pre-pandemic survey of 149 countries from 2015 to 2019 published in the medical journal The Lancet found respondents in Africa, Latin America and many parts of Asia were more likely to believe that vaccines were safe and effective. There are exceptions, including Brazil, where a vaccine-sceptical leader has led to greater reluctance among some of the population.
Dr Kate O’Brien, the World Health Organization’s director of immunisation, vaccines and biologicals, says there has been some hesitancy influenced by the regulatory and policy decisions in Europe, but overall there was no “significant stepping back” from the desire to have the vaccine in countries receiving shots from the WHO programme Covax.
People in low and middle income countries “know how horrible infectious diseases can be”, says Ball. Though the debate continues over how to increase supplies to the developing world, he adds that “it is ironic that people who can’t get access to vaccines are the ones most likely to take them.”
- Hannah Kuchler and Clive Cookson
by ti-amie
Dr Kate O’Brien, the World Health Organization’s director of immunisation, vaccines and biologicals, says there has been some hesitancy influenced by the regulatory and policy decisions in Europe, but overall there was no “significant stepping back” from the desire to have the vaccine in countries receiving shots from the WHO programme Covax.
People in low and middle income countries “know how horrible infectious diseases can be”, says Ball. Though the debate continues over how to increase supplies to the developing world, he adds that “it is ironic that people who can’t get access to vaccines are the ones most likely to take them.”
Meanwhile the only reason anyone can argue vaccines aren't needed is because of the success of the polio vaccine followed by those against measles, mumps and rubella. They don't know a world where these diseases ran rampant and caused disabilities as well as deaths. Most of the anti vaxxers were vaccinated as children by parents who did know what the alternative was.
It's been said that African countries that had to deal with ebola had already created infrastructure to support anti pandemic methods especially in West Africa. Where ebola didn't hit is where the problems are on that continent.
by ponchi101 I was in Niger, at the local market in Niamey. A person, so disfigured by one type of pox (I couldn't tell which one) approached me for some alms.
It was an image that I wish I could share with anti-vaxxers. The level of facial injuries (all I could see, of course) was devastating. And I was the sole person that paid attention, as for the people there, this was "normal".
by ti-amie Sadly the only way to post this is using the tweets. The author doesn't allow @threadreaderapp to consolidate them.
p1
by ti-amie P 2
by ti-amie P3
Pwn All The Things
@pwnallthethings
Replying to
@pwnallthethings
and
@thedailybeast
That's not to say it's impossible for the Wuhan lab theory to be right. Maybe it is. Maybe it isn't. But this reporting is garbage, and has more red flags than a Chinese National Day parade.
by Deuce Over the past week or so, I have seen a major golf tournament in the U.S. where there were thousands of unmasked fans with no physical distancing at all... Major League Baseball games in the U.S. where there are thousands of unmasked fans with no physical distancing at all... NHL hockey games in the U.S. with thousands of fans - indoors - with no physical distancing at all...
Watching these sporting events, I see no difference between their environment now and the environment of these sporting events 2 (or 20) years ago, before the pandemic.
Again, this is all in various states in the U.S., which not very long ago was among the worst countries on the planet in terms of positive COVID-19 cases, as well as deaths.
So... has the U.S. simply gone completely insane in pretending that COVID-19 no longer exists... or have I missed something along the way?
Please don't tell me that all of these fans at all of these venues are fully vaccinated - because there is no way in hell that I will believe you.
by mmmm8 I have tickets to a baseball game and they stopped requiring a negative COVID test last week (we are vaccinated, otherwise I would consider not going, a test was required when the tickets were purchased). It is at 20% capacity only, though.
But they will be checking temperatures! (which does nothing)
by mmmm8
mmmm8 wrote: ↑Mon May 24, 2021 11:19 am
I have tickets to a baseball game and they stopped requiring a negative COVID test last week (we are vaccinated, otherwise I would consider not going, a test was required when the tickets were purchased). It is at 20% capacity only, though.
But they will be checking temperatures! (which does nothing)
Actually, just looked into this and they're creating full capacity sections for vaccinated people, as authorized by the authorities.
by ponchi101 I will be able to report as of tomorrow, but my niece in GA tells me that the situation is back to normal completely. Indoor dining, people gathering, etc.
Which is the reason the USA is still reporting 500 deaths/day, I guess. The vaccinated population is what keeps the number from going up.
But it is as you say, Deuce. This is insane. The pandemic is far from over. Go to the park, sure, but wear that mask. Just a few more months. It is not much to ask.
by Suliso What will change in couple more months? US has already reached 80% of those who are willing to get vaccinated. A pity that it's only 39% as of now in GA (54% in NY, 65% in MA)
by Drop-shot In response to Ti's debunking post, I read an article that laid out various points of the investigation. And while I too read it as a whole with skepticism there were some points that do leave room for doubt:
- the spike molecule being so adept at targeting human cells and having a specific aminoacid not found in other coronavirus
- the missing host between bats and humans. For all previous pandemics and zoonotic viruses this link was found rather quickly. Think swine, bird and MERS. Yet here we are, almost a year and a half and still nothing.
- the single jump from animal to humans. The rule is for there to be numerous cases (various jumps). For a very up-to-date example, google H5N8 and you will see articles warning about a possible new bird flu since there have already been various jumps, not a single one place/one moment a la Wuhan.
Trying to keep the reasoning as scientific as possible, I will grant the different theories different probabilities of being true, but will discard none (within the bounds of logic) until one has been proven to be the correct one.
by atlpam
ponchi101 wrote: ↑Mon May 24, 2021 2:12 pm
I will be able to report as of tomorrow, but my niece in GA tells me that the situation is back to normal completely. Indoor dining, people gathering, etc.
Which is the reason the USA is still reporting 500 deaths/day, I guess. The vaccinated population is what keeps the number from going up.
But it is as you say, Deuce. This is insane. The pandemic is far from over. Go to the park, sure, but wear that mask. Just a few more months. It is not much to ask.
GA is definitely treating the situation as normal, although how people are acting varies by where you go. I went to Target over the weekend and even though there is no longer a mask requirement, most people inside the store were still wearing masks (including me). Similar for restaurants we have been to - except for one I went to after hiking, most places I have been still require/request masks inside when not at your table. It is probably highly dependent on the patrons of the establishment complying without a firm requirement in place.
by ponchi101
Suliso wrote: ↑Mon May 24, 2021 2:45 pm
What will change in couple more months? US has already reached 80% of those who are willing to get vaccinated. A pity that it's only 39% as of now in GA (54% in NY, 65% in MA)
Indeed. I should have been more clear and say that IF people were to continue a thorough vaccination program, it would be just a couple of months.
But as you point out, the USA is far from that.
by JazzNU
ponchi101 wrote: ↑Mon May 24, 2021 2:12 pm
I will be able to report as of tomorrow, but my niece in GA tells me that the situation is back to normal completely. Indoor dining, people gathering, etc.
Which is the reason the USA is still reporting 500 deaths/day, I guess. The vaccinated population is what keeps the number from going up.
But it is as you say, Deuce. This is insane. The pandemic is far from over. Go to the park, sure, but wear that mask. Just a few more months. It is not much to ask.
That's the situation in most of the country. In the Northeast, the West, and some of the Midwest masks are still worn more often and at times it's a requirement but almost nowhere outdoors as of mostly last week in almost all states. In the South, it was either never a requirement or dropped quite a while ago and yes, life is super duper normal there. Indoor dining has returned to normal in most places as well. You're gonna want to prepare yourself for what you're about to see if you haven't already. I'm guessing it may be a shock because I've seen the gradual change and it's still a shock for me to see it.
by ti-amie Brad Gilbert was raging about the galleries at the golf event yesterday. they were unmasked and there was no distancing.
by JazzNU By the way, I went to an eye exam last week and the optometrist asked if I wanted to take off my mask after asking if I was vaccinated. I wasn't expecting the question, so after a moment's hesitation, I told him he could if he wanted, but I'd keep mine on despite being fully vaccinated. So he said he'd keep his on as well.
Now, should I be more okay with people now that I'm fully vaccinated? Yes, I know this, but it's a process to get over the last year and my comfortability with basically strangers is going to be real gradual getting comfortable with them again.
And I can tell you I was THRILLED with my decision to keep my mask on, because when he was examining my eyes with one of the manual instruments and his face was a centimeter away from my face? I may have actually had a legitimate freak out had we not had our masks on. Like I wasn't thinking that far ahead in the least, but I should have. So, just if you're going into a setting with strangers or casual acquaintances and you're thinking of ditching the mask since you're vaccinated, I highly suggest thinking through the entire visit.
by Suliso It's been a long time since I've been to a restaurant (not counting take away) in Switzerland. Late September, I think. Terraces are now open again and indoors might be in few weeks. I probably wait till I'm actually vaccinated, though.
by JazzNU
ti-amie wrote: ↑Mon May 24, 2021 7:13 pm
Brad Gilbert was raging about the galleries at the golf event yesterday. they were unmasked and there was no distancing.
It was about as rowdy as it's ever been at a golf tournament.
A bit more unnerving than plenty of other sporting events held thus far to me, because they were more on top of each other than many other events. And given this was in South Carolina with plenty of fans from there and nearby states, it's hard to get your mind to a place where you think the majority of the people even had one dose, let alone fully vaccinated.
by Suliso Golf is outside, NBA playoff games with a full house are likely to be more dangerous.
by JazzNU
Suliso wrote: ↑Mon May 24, 2021 7:43 pm
Golf is outside, NBA playoff games with a full house are likely to be more dangerous.
I doubt it. If you go by just outdoor vs. indoor, then sure. But the details of most NBA teams' rules and ticketing approach make their setup far from dangerous. PGA has next to nothing in place and so outdoors is great, but those people were on top of each other. And regardless of what perception is when you watch an NBA playoff game on TV, there haven't been any full houses as of yet, a few teams will be moving towards that in another week or two.
by Suliso That doesn't look good... Outdoors vs indoors can trump a lot, but on the other hand if you're literally screaming in each others face maybe not.
As for NBA I'm reading Dallas will have 12,000 people attending when the series go back to Texas in later this week.
by Deuce
mmmm8 wrote: ↑Mon May 24, 2021 11:19 am
I have tickets to a baseball game and they stopped requiring a negative COVID test last week (we are vaccinated, otherwise I would consider not going, a test was required when the tickets were purchased). It is at 20% capacity only, though.
^ You need to test negative to purchase tickets... I don't know how that works if purchasing the tickets online - but even so, is there anything stopping you from purchasing the tickets with a negative test, then giving the tickets to someone else?
Or from contracting the virus a week after you purchased the tickets, but still before the date of the game?
JazzNU wrote: ↑Mon May 24, 2021 7:19 pm
By the way, I went to an eye exam last week and the optometrist asked if I wanted to take off my mask after asking if I was vaccinated. I wasn't expecting the question, so after a moment's hesitation, I told him he could if he wanted, but I'd keep mine on despite being fully vaccinated. So he said he'd keep his on as well.
Now, should I be more okay with people now that I'm fully vaccinated? Yes, I know this, but it's a process to get over the last year and my comfortability with basically strangers is going to be real gradual getting comfortable with them again.
And I can tell you I was THRILLED with my decision to keep my mask on, because when he was examining my eyes with one of the manual instruments and his face was a centimeter away from my face? I may have actually had a legitimate freak out had we not had our masks on. Like I wasn't thinking that far ahead in the least, but I should have. So, just if you're going into a setting with strangers or casual acquaintances and you're thinking of ditching the mask since you're vaccinated, I highly suggest thinking through the entire visit.
^ I agree...
But if the optometrist/dentist/doctor/hairdresser, etc. simply take people's word as to whether they are vaccinated or not - and the client also simply takes the word of the optometrist/dentist/doctor/hair dresser, etc., then it's all basically a crapshoot. Unless the two people know each other fairly well, and trust each other, if they merely say that they're vaccinated, it's essentially meaningless.
As one late nighte talk show host said last week in answer to the question "How can you tell which people are fully vaccinated, and which people are not?" - "Easy - the fully vaccinated people are the ones who are still wearing their masks!"
Suliso wrote: ↑Mon May 24, 2021 7:43 pm
Golf is outside, NBA playoff games with a full house are likely to be more dangerous.
^ I would say that people being very close together outside - so that there is very little space between people for the air to scatter or dilute the virus particles - is just as dangerous as people sitting side by side at an indoor NBA game.
I haven't watched any basketball games, but I have watched hockey games in the past week in the U.S. where the seats are filled as they normally were before the pandemic - no masks, no physical distancing. They may only allow the arena to be 20% full - but if everyone is together, as I've seen, that defeats the entire purpose of allowing only 20% of capacity. The whole point of restricting capacity to a certain percentage is so that people from different households can have some space between them all!!
Here in Canada, hockey games are still completely without fans. Montreal is talking about possibly allowing 2500 fans next week (capacity is 22,000). I hope they don't do it.
by JazzNU There is space between ticketing groups at most NBA and NHL games. That will be the case for some places in general, for other places for another week or two before capacities percentages are raised or lifted entirely. Sometimes it is hard to tell on TV, people are not as close as they seem. For the most part right now, if you see a section where people look like they are very, very close together, that's going to be the one of the vaccinated seating sections of the arena, which is typically allowed to have full or near full capacity. Proof of vaccination along with ID required upon entry. And I have friends and friends of friends who have been, they do check and turn you away if you don't have it. My brother-in-law's friend had a photo of the front but not the back of the vaccine card and that wasn't enough.
Tickets are operating differently in large part. Mostly contactless. Mobile wallets and apps used for additional verification and screenings. You don't need to test negative to purchase tickets, you need to test negative to attend. Testing and screenings are done in close proximity to the game, not the time of purchase. And resell is not as traditional as before, many times you must resell your entire pod of tickets to another same sized group in the designated marketplace.
by Deuce Sounds like what is commonly referred to as being a 'logistical nightmare'. It's very likely that several 'infiltrators' (people who are either not fully vaccinated and/or who have not tested negative) have gotten around or through the screening, and will continue to. Anti-maskers and anti-vaxxers revel in trying to circumvent rules like this - and you can be sure that some of them are succeeding.
mmmm8 wrote: ↑Mon May 24, 2021 11:19 am
I have tickets to a baseball game and they stopped requiring a negative COVID test last week (we are vaccinated, otherwise I would consider not going, a test was required when the tickets were purchased). It is at 20% capacity only, though.
^ You need to test negative to purchase tickets... I don't know how that works if purchasing the tickets online - but even so, is there anything stopping you from purchasing the tickets with a negative test, then giving the tickets to someone else?
Or from contracting the virus a week after you purchased the tickets, but still before the date of the game?
I was confused then just realized you misunderstood my post. At the time I purchased the tickets, a negative test was required to ATTEND Yankees games. But now, they are not requiring tests anymore, so it won't be required at the time of the actual game I bought tickets to. The game is in early June.
No test was required to purchase, that wouldn't make sense.
And yet another reason to doubt the "natural" theory is the accelerated mutation rate. The flu virus has been mentioned abundantly as one that mutates annually but you can cover that with the booster shots. How many mutations has COVID had in a year? Seems much more than normal, even to the extent that some of the vaccines are not effective against some strains (Astrazeneca - South Africa strain)
Again, they're all perfectly valid questions and observations that need answering. If this were a horse race, Lab-Virus is catching up to Natural Theory though the latter maintains a healthy lead... for now
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 167 million cumulative cases and 3.5 million deaths worldwide as of 4:45am EDT on May 25. Global weekly incidence and mortality continue to decline, both for the third consecutive week. The weekly incidence decreased 14% from the previous week, and weekly mortality decreased by 2%.
Global Vaccination
The WHO reported 1.49 billion doses of SARS-CoV-2 vaccines administered globally as of May 24, and 700 million individuals have received at least 1 dose. Our World in Data reported 1.70 billion cumulative doses administered globally. The global cumulative total continues to increase at approximately 13% per week. Daily doses administered continue to increase, up to a new record of 28.4 million doses per day on May 22 before falling slightly to 28.1 million. The global increase is largely driven by Asia, which, in turn, is largely driven by China. Our World in Data estimates there are 395 million people worldwide who are fully vaccinated, corresponding to approximately 5.1% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 32.9 million cumulative cases and 587,342 deaths. Daily incidence continues to decline, to the lowest levels since early in the pandemic. The current average daily incidence—22,877 new cases per day—is the lowest since June 14, 2020. The lowest daily incidence between the United States’ first and second surge was 20,733 on June 1, 2020, and the US could fall below that average in the coming days, if it continues on this trajectory. After falling below 500 deaths per day on May 20, daily mortality increased slightly, up to 508 on May 22 before falling back to 500.
US Vaccination
The US has distributed 357 million doses of SARS-CoV-2 vaccines and administered 287 million. After more than a month of decline, the daily doses administered* has increased for 5 consecutive days, back up to 1.7 million doses per day. The increase over the past several days is due to an increase in the number of first doses administered—up from 554,890 individuals per day on May 12 to 882,463 on May 19, an increase of nearly 60% over that period. Approximately 953,000 people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12. If this level of interest is sustained from the first to the second dose, we could expect to see an increase in the number of fully vaccinated individuals each day starting in the next 2-3 weeks, once second doses are administered.
A total of 164 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 49% of the entire US population. Among adults, 62% have received at least 1 dose, and 5.2 million adolescents aged 12-17 years have received at least 1 dose. A total of 131 million people are fully vaccinated, which corresponds to 39% of the total population. Among adults, 50% are fully vaccinated, and 2.0 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 85% with at least 1 dose and 74% fully vaccinated. In terms of full vaccination, 67 million individuals have received the Pfizer-BioNTech vaccine, 53 million have received the Moderna vaccine, and 10.2 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
Following updated guidance from the US CDC regarding recommendations for fully vaccinated individuals, US states are moving forward with efforts to relax or remove COVID-19 restrictions. However, US states vary widely in terms of vaccination coverage, and increased social interaction among unvaccinated individuals could increase risk of community transmission. The full vaccination coverage in states at the top of the rankings is nearly double the coverage in states at the bottom, ranging from 26.5% to 52.7%. There are 4 states currently reporting full coverage greater than 50%—Vermont (52.7%), Connecticut (51.6%), Maine (51.9%), and Massachusetts (50.5%)—and Rhode Island is nearly there with 49.9%. At the other end of the spectrum, there are 6 states reporting 31% or lower, including 2 with less than 30%—Mississippi (26.5%) and Alabama (28.7%). The median full vaccination coverage is 39%, and most states fall between approximately 34-44%.
There are some notable regional disparities as well. The top 6 states in terms of full vaccination coverage are all in the Northeast region. Conversely, the South represents the bottom 6 states and 9 of the bottom 12. Maryland (#9) is the highest-ranking state from the South, although it is among the northernmost states in the region, bordering the Northeast region. New Hampshire is the lowest-ranking state from the Northeast region, although at #22, it is still among the top half of all states. It is also #4 in terms of partial vaccination coverage. The states from the West and Midwest regions are largely scattered throughout the middle of the rankings. While the West represents 3 of the bottom 10 states—Idaho (#42), Utah (#43), and Wyoming (#44)—it also accounts for 2 of the top 10—Hawai’i (#7) and New Mexico (#8).
G20 BACKS VACCINE VOLUNTARY LICENSING On May 21, G20 leaders adopted a declaration pledging to bridge gaps in responses to the COVID-19 pandemic and to support voluntary licensing and technology transfers in order to boost vaccine production. Some view the Rome Declaration, adopted at the conclusion of a special summit on the COVID-19 pandemic hosted by Italy and the European Union's Executive Commission, as a snub to recent international discussions about waiving intellectual property rights for certain COVID-19 vaccines. Instead, G20 leaders reaffirmed their support for patent pooling through the WHO’s ACT-Accelerator, allowing pharmaceutical companies more flexibility in deciding what information to share. While the leaders supported technology pooling, they did not commit to additional financial resources for the scheme, which remains $19 billion short of its goal. Additionally, there are no commitments in the declaration to share vaccine stockpiles with low- and middle-income countries, although it does mention the COVAX facility as a means to do so. The Rome Declaration also lists 16 guiding principles for responding to the current pandemic and preparing for the next.
WORLD HEALTH ASSEMBLY The 74th World Health Assembly opened on May 24 with a focus on ending the COVID-19 pandemic and preparing for the next one. The meeting of the WHO’s decision-making body, this year held virtually, will run through June 1. In his opening remarks, WHO Director-General Dr. Tedros Adhanom Ghebreyesus paid tribute to the more than 100,000 healthcare workers who lost their lives fighting the COVID-19 pandemic on the front lines and called on member states to urgently invest in their health and care workers. Dr. Tedros also warned that no country is “out of the woods” in the pandemic, despite their vaccination rates, saying the pandemic will not end until transmission is controlled in every nation. He urged wealthier countries to help reach a goal of vaccinating at least 10% of the population of every country by September, and a “drive to December” to reach at least 30% by the end of the year.
In a video message, UN Secretary-General António Guterres laid out a 3-part plan to end the pandemic, calling on nations to more equitably distribute vaccines, diagnostics, and treatments; boost domestic primary health care and universal health coverage; and commit to transforming existing pandemic warning systems, with the WHO at the center of any global preparedness strategy. Member states are expected to receive 3 pandemic-related reports during the meeting, including one from the Independent Panel for Pandemic Preparedness and Response, an independent review of the WHO's Health Emergencies Programme, and a review of how the International Health Regulations have performed during the pandemic.
NOVAVAX VACCINE PHASE 3 TRIAL RESULTS Last week, US pharmaceutical company Novavax posted complete results from a Phase 3 clinical trial testing its 2-dose recombinant protein SARS-CoV-2 vaccine candidate to the preprint server medRxiv, after releasing initial results in March. According to the results of the randomized, double-blind, placebo-controlled study conducted in the United Kingdom, the vaccine, NVX-CoV2373, was 89.7% (95% CI, 80.2-94.6) effective in preventing COVID-19, with no hospitalizations or deaths reported, with post hoc analysis showing efficacies of 96.4% (73.8-99.5) and 86.3% (71.3-93.5) against the original strain and B.1.1.7 variant, respectively. According to some reports, Novavax is expected to apply for emergency authorization in the US in the coming weeks. Notably, the company has never brought a product to market. If it receives authorization, the company has pledged to provide 100 million doses to the US later this year and has promised 1.1 billion doses to COVAX for distribution in low- and middle-income countries. Indian vaccine maker Serum Institute is contracted to make most of the 1.1 billion doses, but backlogs there have Novavax seeking other options. Novavax recently reaffirmed its relationship with the South Korea Ministry of Health and Welfare and SK Bioscience Co. Ltd. to manufacture NVX-CoV2373 and explore expansion of the partnership, having previously entered into a licensing agreement with SK Bioscience to produce 40 million doses of its vaccine candidate.
Additionally, Novavax announced its participation in a mix-and-match clinical trial testing the potential of 7 SARS-CoV-2 vaccines as booster doses for vaccines from different manufacturers among people who are already fully vaccinated. The company also noted the UK National Health Service, Vaccines Task Force, and National Institute for Health Research are working to ensure participants in the Phase 3 clinical trial who received NVX-CoV2373 are entered into the NHS App, which helps vaccinees prove their vaccination status when traveling.
MODERNA VACCINE ADOLESCENT CLINICAL TRIAL Moderna announced this week that their SARS-CoV-2 vaccine trial in adolescents, TeenCOVE, has reached its primary endpoint. More than 3,700 adolescents aged 12 to less than 18 years old were enrolled in the trial. No cases of COVID-19 were recorded in vaccine recipients following two doses of the Moderna vaccine. With these results indicating an efficacy of 100% 14 days after both doses, Moderna also found approximately 93% efficacy following one dose of the vaccine. The company plans to send the trial data to regulators in early June. Moderna would be the second SARS-CoV-2 vaccine to be authorized for use in adolescents in the US, following Pfizer-BioNTech’s authorization earlier in May. Both Moderna and Pfizer-BioNTech are investigating vaccine safety and efficacy in children aged 6 months to 11 years, but those results are not expected for some time due to the need to adjust dosing amounts.
AFRICA COVID-19 MORTALITY People in Africa who become critically ill with COVID-19 are more likely to die than people in other parts of the world, according to a study based on data from 64 hospitals in 10 countries collected between May and December 2020 and published in The Lancet. Among 3,077 critically ill patients admitted to the hospitals—located in Egypt, Ethiopia, Ghana, Kenya, Libya, Malawi, Mozambique, Niger, Nigeria, and South Africa—48.2% died within 30 days, compared with a global average of 31.5%, according to the study. The majority of patients were men (61%), and the overall cohort had an average age of 56 and few underlying conditions. People with pre-existing conditions had the highest risk of poor outcomes. Having chronic kidney disease or HIV/AIDS nearly doubled the risk of death, chronic liver disease more than tripled the risk of death, and diabetes also was associated with poor survival.
Notably, being male was not associated with increased mortality, an unexpected result, according to the African COVID-19 Critical Care Outcomes Study researchers. They noted this could be due to women having less access to care or biases in care when critically ill. Overall, the researchers posited scarce critical care resources and under-resourced facilities could have played a role in the deaths, as well as an apparent failure to use available resources and medical interventions. The researchers highlighted limitations to their study, including that the observations occurred primarily at university-affiliated, government-funded, and tertiary hospitals, so outcomes could be worse in lower-level, less-resourced hospitals across the continent. Another analysis published in The Lancet found that Africa’s second COVID-19 wave was more severe than the first. Taken together, these studies underscore the importance of improved epidemiological surveillance on the continent.
RESPIRATORY STATUS & MORTALITY RISK Researchers from the University of Washington and Rush University Medical Center (Illinois; US) found that respiratory symptoms may not be an accurate predictor of COVID-19 mortality risk. The presence of respiratory symptoms—such as coughing, wheezing, or difficulty breathing—may not necessarily correlate with respiratory compromise. Clinical measurements such as blood oxygen saturation and respiratory rate can provide a more objective assessment of respiratory compromise. The researchers evaluated data from more than 1,000 hospitalized COVID-19 patients and assessed COVID-19 mortality risk associated with both respiratory symptoms as well as oxygen saturation and respiratory rate.
The researchers found that blood oxygen saturation of 91% or lower was significantly associated with increased risk of COVID-19 mortality (compared to 92% or higher), ranging from 1.8 times the risk for 89-91% to 4.0 for less than 80%. Increased respiratory rate was also significantly associated with increased mortality. The risk of death was 1.9 times higher among individuals with respiratory rates of 23-24 breaths per minute (compared to 20 or fewer). Individuals with more than 32 breaths per minute were 3.2 times as likely to die. In contrast, the presence of respiratory symptoms or fever were not significantly associated with increased COVID-19 mortality.
LONG-TERM EFFECTS IN CHILDREN Most children with COVID-19 who develop a rare but potentially severe condition known as multisystem inflammatory syndrome in children (MIS-C) experience symptom alleviation within 6 months, according to a small study published May 24 in The Lancet Child & Adolescent Health. Researchers followed 46 children initially admitted with COVID-19-related MIS-C—also known as pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2—to Great Ormond Street Hospital (London; UK) between April 4 and September 1, 2020. Six months after discharge from the hospital, only 1 child still had systemic inflammation, 2 had heart abnormalities, and 6 had gastrointestinal symptoms. Eighteen of the children continued to have diminished exercise tolerance and 15 were experiencing emotional difficulties. The researchers emphasized that longer-term follow-up studies are needed to better characterize the natural history of MIS-C among children with COVID-19.
US COVID-19 EPIDEMIC IN UNVACCINATED INDIVIDUALS A report from The Washington Post breaks down national and state populations into vaccinated and unvaccinated individuals by assuming that all vaccinated individuals are fully immune and removes them from the population. While this is not necessarily the case, we expect this to be a reasonable approximation due to the low risk of breakthrough infection—and even lower risk for severe disease and death. With just the unvaccinated portion of the population remaining, the report estimates the per capita COVID-19 daily incidence, hospitalization, and mortality among unvaccinated individuals.
While the overall daily incidence is declining across the country, the Washington Post analysis says that COVID-19 “is spreading as fast among the unvaccinated as it did during the winter surge.” There are just fewer susceptible individuals due to vaccination. Similar trends are apparent for both hospitalizations and mortality. While nearly half of the US population has received at least 1 dose and nearly 40% are fully vaccinated, unvaccinated individuals remain at risk, and vaccination coverage is not yet sufficient to provide protection to the unvaccinated portion of the population. Vaccination coverage varies widely by state, and states with lower coverage still have substantial populations remaining to facilitate community transmission if effective protective measures are not in place.
CLINICAL TRIAL LANDSCAPE Since the beginning of the pandemic, many studies testing potential COVID-19 therapies have been too small to gather meaningful data or did not include a control arm. Researchers in Europe and the US are working to launch large-scale, randomized clinical trials of multiple drugs to evaluate whether they work to help people with COVID-19 are more likely to survivor or recover more quickly. The WHO is relaunching its multi-arm Solidarity trial to look at repurposed drugs meant to prevent immune system overreaction in COVID-19 patients, and the REMAP-CAP study is ongoing in Europe. In the US, the NIH-sponsored Accelerating COVID-19 Therapies and Vaccines (ACTIV) program is set to begin enrolling patients in ACTIV-6, a master protocol that will evaluate at least 4 different oral medications already approved to treat other diseases among people with mild to moderate COVID-19 who are not hospitalized. These trials are all designed to examine several treatment options simultaneously and efficiently, with built-in flexibilities and pooled control groups. The FDA recently released new guidance for these types of master protocols. One potential obstacle for these larger studies is enrolling sufficient numbers of patients, as some places are experiencing sustained declines in new COVID-19 cases.
SARS-COV-2 ORIGINS Many questions remain regarding the origin of the SARS-CoV-2 virus. An article in the The Wall Street Journal (WSJ) says that 3 illnesses among personnel who worked at the Wuhan Institute of Virology (WIV; China) in November 2019 are linked to the COVID-19 pandemic. Reportedly, the individuals’ symptoms were consistent with COVID-19; however, COVID-19 shares many common symptoms with other diseases, including seasonal influenza. The illnesses were previously listed in a fact sheet issued by the US Department of State, but the WSJ article indicates that additional details—including the number of cases and the timing of the illnesses—are contained in an “undisclosed U.S. intelligence report.” The WSJ article acknowledges that some government officials familiar with the intelligence report question the “supporting evidence for the assessment,” and to our knowledge, the report’s contents have not been released publicly. In a separate article, WSJ also investigated a potential link between illnesses at a Chinese mine in 2012 and the emergence of SARS-CoV-2 in 2019.
As we have covered previously, it will be difficult to definitively determine the original source of SARS-CoV-2, whether from a natural spillover event, laboratory accident, or other events. Continued discussions about the possibility of a laboratory release has fueled calls for further investigations into activities at WIV. A previous investigation led by the WHO determined that the likelihood of the pandemic originating from a laboratory release to be “extremely low,” but in the absence of definitive evidence of another source, it is nearly impossible to rule it out. Rigorous, transparent, and independent investigations are an important step to understanding the origins of the pandemic, but myriad technical, practical, and political barriers remain that could impede these efforts.
OLYMPICS With the 2020 Summer Olympic Games scheduled to begin in July, Japan continues to combat one of its largest COVID-19 surges. Officials from hospitals in Osaka, Japan’s second largest city, are warning that the medical system could be on the verge of collapse. Some experts and health officials worry that the influx of tens of thousands of Olympic participants will further strain the already overburdened health system and potentially introduce new variants of concern into the population. The Japanese government recently opened 2 mass vaccination centers following Prime Minister Yoshihide Suga’s pledge to vaccinate the country’s entire elderly population of 36 million citizens by the end of July. Still, vaccination levels remain extremely low, with only around 2% of the population fully vaccinated.
In response to Japan’s ongoing surge, the US Department of State recently upgraded its travel advisory from a Level 3 (Reconsider Travel) to Level 4 (Do Not Travel). The US CDC also stated that even vaccinated travelers could be at risk of contracting and spreading SARS-CoV-2 due to the circulation of variants of concern. Notably, international spectators will not be permitted to attend the Olympics, but it is unclear if or how the Level 4 travel advisory could impact athletes’ travel from the US or other nations that consider US guidance.
by ti-amie A very sobering look at the effect of WhatsApp especially in countries where there is distrust of media. Or people simply want to believe (although Mulder has seemingly been proven right).
When misinformation comes for the family WhatsApp
As my grandfather’s health deteriorated in India, my family turned to fake news.
By MEGHNA RAO
Meghna Rao is a writer and editor from Queens.
25 MAY 2021
Last July, my 80-year-old grandfather woke up in the middle of the night, unable to recognize any of the people in his small apartment in central Bangalore — not my aunt, not my uncle, not even my grandmother, his wife of sixty years.
My mother and I were helpless in Queens. Covid-19 cases were on their first ascent in India; we couldn’t risk traveling from New York to be by his side. For solace, we turned to our family WhatsApp group, a jumble of aunts, uncles, and cousins spread across India, the Middle East, and the U.S. — most of whom I have only met once or twice as a child.
Each night, we would go to bed hopeful, but in the morning, the news would be the same. My grandfather still had no recollection of who he was surrounded by, where he was, or why he was there. Finally, on his sixth day in a stupor, my aunt decided to drive him to the hospital. The doctors were as confused as we were. He hadn’t had a stroke or a head injury. It was as if a thief had robbed him of his memory and left without a trace.
Eventually, a doctor suggested a Covid-19 test. When the results came out positive, the doctors concluded that my grandfather was suffering from an extreme version of “brain fog.” My uncle shared the news with my mother, who called me. Yes, it was Covid-19, but we were lucky that he had none of the other symptoms. He could still breathe.
My family WhatsApp group panicked. In the summer of 2020, most members lived in countries where Covid-19 was still something that happened to other people: migrant laborers, health professionals, and domestic workers who couldn’t afford to take time off. These were all sad stories, but they were many degrees away.
My uncle, who works as a dentist in Brunei, proposed a solution on the family chat. An Indian student had purportedly found a remedy to Covid-19 by mixing black pepper powder, honey, and ginger juice. If ingested for five days straight, the tonic would rid any person of the virus.
“PLEASE CIRCULATE,” the message demanded. WhatsApp tagged it as a viral message that had been “forwarded many times.” My uncle received many emojis of brown clapping hands in return.
My grandfather, the traditional head of the household, had seemed invincible. He was born in Mangalore shortly after India’s independence, and had moved from country to country, spending decades learning Arabic and working as a secretary in a hospital in Abu Dhabi. By sixty, he had perfected a New York accent and taken a job as a clerk for a small NGO in Queens. We knew death would come for him some day, but we didn’t think it would be like this –– not from the virus that hopped from person to person like a hitman.
But the forwards grew worse, morphing in tone. My family, mostly Hindu and upper-caste, gravitated towards content that confirmed their beliefs. The virus was spread by meat-eaters, one message said. Upper-caste vegetarian diets would never have led to this.
The messages mutated from pseudo-scientific to xenophobic and bigoted. An aunt who lives on the outskirts of Bangalore forwarded a WhatsApp message listing a series of distances from Wuhan to Beijing, Milan, New York, and Iran, as if to claim that the virus had been an inside job. “All business areas of China are safe,” the message read. “Something is fishy.”
They were grasping at anything to explain my grandfather’s sudden case. The truth was far more mundane. My uncle left the house weekly to visit a dialysis center. My aunt, who works as a lawyer, had continued to meet with her clients. My grandfather interacted with both of them, unable to isolate in the cramped, city-center apartment. But it was far easier to drown in incendiary messages than to admit these things.
WhatsApp, with just over a reported half a billion users in the country, is India’s most popular messaging platform. During the pandemic, the app has become a stand-in for the country’s broken infrastructure. These days, as Covid-19 cases spread like wildfire, groups message day and night to organize extra oxygen tanks, connect people with ventilators, and source hospital beds. Others raise funds for the many Indians who can’t afford to make ends meet in quarantine. Businesses that shut their physical stores have turned to the platform to sell their goods and stay afloat.
But its ubiquity and myriad uses are also why misinformation on Whatsapp can be so potent. The messages I’ve been forwarded rarely link to reported articles. Few in India trust the news — misinformation easily masquerades as the truth. Though often touted as the world’s largest democracy, India recently ranked 142 out of 180 in the World Press Freedom Index. That’s the worst India has ranked since the organization began indexing the country in 2013. The report cited factors like police violence against reporters, attacks by those in disagreement with reported work, and corruption. Just in 2020, six journalists in India were killed.
Misinformation is not a new problem for WhatsApp, which launched in India in 2010. Some trace the roots of misinformatio’s spread to the 2014 prime minister campaign, when Narendra Modi’s Bharatiya Janata Party (BJP) went up against the dynastic Congress party. The BJP, which is the political arm of fringe Hindu extremist group Rashtriya Swayamsevak Sangh (RSS), used WhatsApp as a means to push messages that furthered their agenda.
“We should be capable of delivering any message we want to the public, whether sweet or sour, true or fake,” BJP president Amit Shah said to a crowd in 2018, endorsing fake news as a means to spread an ideology and to influence and convert believers.
While misinformation can seem like a harmless game online, it has devastating repercussions in India. And the problem is not new. One of the first recorded cases of WhatsApp-linked violence in India was in 2017, when a mob killed seven people after widespread rumors of strangers abducting children.
Since then, the problem has only grown, expanding with the pandemic. In April 2020, a series of messages went viral about a Muslim missionary group that had gathered in Delhi despite the lockdown. In response, a young Muslim man was beaten, and assaulted with threats that he would be doused with fuel and set on fire.
Although the doctors had diagnosed my grandfather with Covid-19, they didn’t have a cure for his memory loss. Days into his hospitalization, he remained confused, and pandemic numbers continued to increase. An uncle who lives in a small, coastal town in Karnataka sent a lengthy message to my family group quoting an article by “Joseph Hope, editor-in-chief of The New York Times.” Hope praised Modi’s strategic management of India, painting him as a mastermind who would steer the country into the 21st century.
Neither the article — nor its supposed author — exist, but WhatsApp only flagged that the message has been “forwarded many times.”
Facebook, WhatsApp parent company, has poured money into India. In 2020, it invested $5.7 billion for a 9.9% stake into Reliance Jio, the Indian internet company that spearheaded the plummeting data prices that helped much of the country get online. Compared with the size of this investment, its attempts at fixing misinformation seem paltry. Most attempts have been small-scale product changes: It’s impossible to share messages with multiple groups if they have been forwarded more than five times, and hovering over messages reveals a small magnifying glass to cross-reference them on search engines.
To be sure, misinformation is not entirely WhatsApp’s burden to bear. WhatsApp is just a platform, and these behaviors unfold in other places, like ShareChat and YouTube. And there are many villains in this game. A new, draconian rule in India could force WhatsApp to break its encryption and make messages traceable. If WhatsApp is forced to comply, the company might be required to hire Indian officials to make decisions on what messages should be removed.
Facebook has also granted research awards to study the nature of misinformation, and created WhatsApp accounts like one for the World Health Organization, where messaging brings up a list of auto-generated options for news, vaccine updates, and health topics.
And yet, false messages continue to thrive on the platform.
After his 11th day of confusion, my grandfather woke up and asked where he was. Then, he asked for my grandmother. After that, he wanted his phone. The doctors filed papers to send him home; they had no time to observe him. Case numbers were growing and the hospital was running out of beds. Memory loss was mild compared to what they were seeing.
Our family rejoiced. For a few days, things returned to normal. The WhatsApp group was celebratory, peppered with news of upcoming vaccines and local heroes helping their communities. My grandfather called my mother over WhatsApp and asked her to distribute sweets to everyone he knew in Queens. He would foot the bill. My mother and I laughed at the suggestion. It was a strangely flamboyant gesture for a man I otherwise knew to be stoic.
But my grandfather grew stranger by the day. Sometimes, his clarity would be punctuated with lapses in memory. Then, on a phone call, with conviction, he shared with me the plot against India. Modi had built a strong country, he explained, and Covid-19 death numbers had been fudged to make the country seem poor and weak.
I was surprised to hear him repeat this textbook talking point of Internet conspiracy theorists. Unlike many others around him, my grandfather had been browsing the internet for decades. His issue wasn’t news literacy. In the 2000s, over an AOL connection in Queens, my grandfather was reading a range of international publications and forming his own opinions. He was one of the first people I had known to purchase a cellphone. He kept up with the technology’s evolution, downloading apps when they became available, and teaching himself how to change language settings on his phone so he could read things in Kannada.
But this new person was unrecognizable. Like many other Indians, his main portal into the internet had become Facebook and WhatsApp. His viewpoints morphed into a hodgepodge of viral WhatsApp messages.
As I watched him change, I couldn’t help but accept the obvious conclusion: Facebook does not care to fix its misinformation problem. Instead, it only wants to keep people glued to the platform.
My grandfather’s cognitive abilities have now deteriorated, and the brief spell of clarity he returned to over the summer has passed. He often experiences “sundowning,” where he spirals into a deep confusion each evening. He’s off WhatsApp now, less focused on the material and the political, his brain set on some far-out horizon.
There is little space to mourn where he has gone. Cases of Covid-19 have again ascended, this time steeper and quicker than before. The intensity of each new story eclipses the last.
Just in the past month, my grandmother’s cousin’s body was found dead and cold in her home in Kundapura; a friend’s uncle was transported to the pyres by his daughter-in-law in the back of a rickshaw. Another friend lost her father, her husband, and her son in three days, leaving her with no one to earn money for the home.
After my uncle lost his childhood neighbor to the virus, he sent a message to the family group. The message had a tag that it had been forwarded multiple times, and claimed to have been written by a woman who had traveled several times over the past year, and hadn’t gotten the virus.
“One reason why I could prevent Corona is , I apply coconut oil in the nose 4 times a day,” the message read. I can’t imagine how many times that must have been forwarded.
My family turns to WhatsApp for answers, and WhatsApp continues to fail them
Suliso wrote: ↑Mon May 24, 2021 7:43 pm
Golf is outside, NBA playoff games with a full house are likely to be more dangerous.
I doubt it. If you go by just outdoor vs. indoor, then sure. But the details of most NBA teams' rules and ticketing approach make their setup far from dangerous. PGA has next to nothing in place and so outdoors is great, but those people were on top of each other. And regardless of what perception is when you watch an NBA playoff game on TV, there haven't been any full houses as of yet, a few teams will be moving towards that in another week or two.
by ti-amie Good on your government. I don't know what the rush is here. My complex just said masks are not required outside but are required inside buildings. Go figure.
by atlpam Risk of exposure outside is extremely low unless you're in some heavily crowded area. Personally I've found it very easy to spend time outdoors throughout the pandemic since it's typically easy to maintain distance from others. Outdoor activity has been my saving grace during this time as outdoor walks are how I relieve stress.
by dryrunguy The latest Situation Report. Haven't read it yet. Please note they will be on hiatus next week.
::
Editor’s Note: Our COVID-19 Situation Report team is taking a break next week. We will be back on Tuesday, June 8, with our curated analysis of the latest COVID-19 news and research.
Thanks to our wonderful team who pulls these together: Alyson Browett, Natasha Kaushal, Amanda Kobokovich, Margaret Miller, Christina Potter, Dr. Caitlin Rivers, Matthew Shearer, Marc Trotochaud, and Rachel Vahey.
SCHOOL VENTILATION Many K-12 schools in the US do not have good ventilation, a longstanding problem with negative effects far beyond COVID-19. The Johns Hopkins Center for Health Security published a new report, School Ventilation: A Vital Tool to Reduce COVID-19 Spread, to present findings and recommendations regarding school ventilation in the context of COVID-19. The analysis is based on interviews with more than 30 subject matter experts and current scientific evidence and guidance. Ventilation improvements may be perceived as a complicated and expensive investment, but these upgrades can actually be cost-effective compared to enhanced cleaning and disinfection. As new and potentially more transmissible SARS-CoV-2 variants continue to emerge, improvements in indoor air quality are important for reducing transmission risk, and federal COVID-19 funding could provide the resources to make necessary improvements in K-12 schools, particularly as many schools plan to resume in-person classes before the next school year starts in the fall.
EPI UPDATE The WHO COVID-19 Dashboard reports 169 million cumulative cases and 3.5 million deaths worldwide as of 8:00am EDT on May 28.
While much of the world’s attention has been on the surging COVID-19 epidemics in India and nearby countries, the ongoing surges in South America have remained comparatively under the radar. In terms of per capita daily incidence, South America represents 5 of the top 10 countries globally—Uruguay (#4), Argentina (#5), Paraguay (#7), Colombia (#8), and Suriname (#10)—as well as Chile at #11, Brazil at #12, and Bolivia at #16. Additionally, nearby Costa Rica (#6) and Trinidad and Tobago (#9) also are in the top 10. Most of these countries are setting new national records or are near their highest peak. The daily incidence in some countries—including Bolivia, Paraguay, and Suriname—has increased steadily since at least early April. Others—such as Argentina, Brazil, Chile, and Colombia—reported peaks or plateaus in mid-to-late April before increasing again in early-to-mid May. All 8 of the South American countries listed above are reporting increasing trends in daily incidence over the past 2 weeks, including Bolivia (+59.4%) and Suriname (+89.7%) with biweekly increases greater than 50%.
In terms of per capita daily mortality, South America represents 7 of the top 10 countries globally, including the top 3: Paraguay (#1), Uruguay (#2), and Argentina (#3). Additionally, Bolivia is #11, Guyana is #18, and Chile is #19. Nearby Trinidad and Tobago (#5) and Costa Rica (#16) also are among the top countries globally. Notably, Bolivia (+128%) and Suriname (+170%) are reporting biweekly increases in daily mortality greater than 100%.
Of the 8 South American countries reporting test positivity data, only Chile (11.0%) and Peru (15.4%*) are reporting less than 20%. Paraguay (36.9%), Argentina (32.6%), Colombia (29.2%), and Ecuador (29.2%) are all reporting higher than 25%, well above the 5% target. Notably, South America accounts for 6 of the top 12 countries globally: #2 Paraguay, #4 Argentina, #7 Colombia, #9 Ecuador, #11 Uruguay, and #12 Bolivia.
*Peru’s most recent data are from April 26, 2021.
Following a report of 8.6 million doses of SARS-CoV-2 vaccine administered on May 25, South America’s average jumped up similar to Asia and North America, at approximately 0.45 daily doses per 100 population—up from 0.23 on May 24—although it will likely decrease once May 25 moves out of the 7-day average window. At the national level, Uruguay is the highest-ranked South American country in terms of per capita daily doses administered, ranking #18 with 0.88 daily doses per 100 population. In terms of total daily doses administered, Brazil is #1 in South America and #4 globally with 1.33 million doses per day. Concerningly, Venezuela is reporting fewer than 2,000 doses per day, which equates to fewer than 0.01 daily doses per 100 population—or fewer than 1 dose per 10,000 population. Venezuela reportedly did not officially join the COVAX effort in April 2021, and it has received a limited number of vaccine doses from China and Russia.
On a cumulative basis, South America ranks #3 globally, with approximately 8.9% of the total population fully vaccinated and 17.7% with at least 1 dose. At the national level, Chile (53%) is #11 globally in terms of coverage with at least 1 dose, and Uruguay (49%) is #17, right behind the US (50%). In terms of full vaccination coverage, Chile (41%) ranks #6 globally, just ahead of the US (40%), and Uruguay (29%) ranks #16.
Global Vaccination
The WHO reported 1.55 billion doses of SARS-CoV-2 vaccines administered globally as of May 26, and 736 million individuals have received at least 1 dose. Our World in Data reported 1.81 billion cumulative doses administered globally, and the global cumulative total continues to increase at 13% per week. Daily doses administered continue to increase, up to a new record of 31.0 million doses per day on May 26 before falling slightly to 30.4 million. Our World in Data estimates there are 413 million people worldwide who are fully vaccinated, corresponding to approximately 5.3% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.0 million cumulative cases and 589,547 deaths. Daily incidence continues to decline, to the lowest levels since early in the pandemic. The current average daily incidence—21,627 new cases per day—is the lowest since June 4, 2020. The lowest daily incidence between the United States’ first and second surge was 20,733 on June 1, 2020, and the US could fall below that average in the coming days, if it continues on this trajectory. Daily mortality continues to decline as well, down to 437 deaths per day, the lowest average since March 31, 2020, early in the United States’ initial surge.
US Vaccination
The US has distributed 361 million doses of SARS-CoV-2 vaccines and administered 291 million. After a brief increase, the daily doses administered* is once again decreasing, down to 1.5 million doses per day, the lowest average since February 23. Approximately 843,000 people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 166 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 50% of the entire US population. Among adults, 62% have received at least 1 dose, and 5.8 million adolescents aged 12-17 years have received at least 1 dose. A total of 133 million people are fully vaccinated, which corresponds to 40% of the total population. Among adults, 51% are fully vaccinated, and 2.1 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 86% with at least 1 dose and 74% fully vaccinated. In terms of full vaccination, 68 million individuals have received the Pfizer-BioNTech vaccine, 54 million have received the Moderna vaccine, and 10.4 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 33.2 million cumulative cases and 593,314 deaths in the US as of 10:15am EDT on May 28.
SINOPHARM VACCINE PHASE 3 CLINICAL TRIALS Researchers from China and several Eastern Mediterranean countries published Phase 3 clinical trial efficacy data for 2 SARS-CoV-2 vaccines developed by Sinopharm (China). While the WHO issued an Emergency Use Listing (EUL) to one of the Sinopharm vaccines several weeks ago and the vaccines are in use in multiple countries, to our knowledge, this is the first time that the Phase 3 trial data have been published publicly. Additionally, this is the first efficacy data available for an inactivated virus vaccine—to date, the others have utilized mRNA or viral vector platforms. The data, published in JAMA, presented interim analysis from clinical trials conducted in Bahrain and the UAE involving more than 40,000 adult participants with no known history of COVID-19. Nearly 27,000 participants received one of 2 vaccines (2 doses each, 21 days apart).
The vaccine authorized by the WHO (designated HB02) demonstrated 78.1% efficacy against laboratory-confirmed, symptomatic COVID-19 at least 14 days following the second dose, and the other vaccine (designated WIV04) demonstrated 72.8% efficacy. In December, Sinopharm announced a preliminary efficacy estimate of 79% via press release and an updated estimate of 72.5% in February 2021. The study did not evaluate efficacy against asymptomatic infection, and there were only 2 severe cases (both in the placebo group), which was not sufficient to support efficacy analysis against severe disease. Additionally, efficacy was not assessed against specific variants of concern (VOCs; eg, B.1.1.7, B.1.351, P.1), as their prevalence was not high enough in the trial locations to provide sufficient data. The trials included only 612 participants aged 60 years and older, so additional data is required to allow efficacy analysis in older adults—or other high-risk groups. Both vaccines demonstrated an acceptable safety profile. Additional data from clinical trials in Jordan and Egypt will be included in the final analysis.
SARS-COV-2 ORIGIN INVESTIGATION US President Joe Biden announced on May 26 that he has asked the US Intelligence Community to redouble its efforts to investigate the origins of SARS-CoV-2 and report back to him in 90 days. As we covered previously this week, the Wall Street Journal reported on an “undisclosed US intelligence report” that there is some evidence to support a theory that the virus originated at the Wuhan Institute of Virology (WIV; China) in November 2019. According to intelligence officials, there remains a bulk of information needing additional computer analysis, and the US government’s announcement of a reinvigorated investigation could bring allies to mine their own intelligence data for new information to determine whether an accidental laboratory leak led to the COVID-19 pandemic. A previous investigation led by the WHO determined that the likelihood of the pandemic originating from a laboratory release to be “extremely low,” but in the absence of definitive evidence of another source, it is nearly impossible to rule it out. A source familiar with the call for a revived investigation said the US government was prompted in part because China refused to fully cooperate with the original WHO-led query. US officials cautioned there is no proof the virus originated in a Chinese lab.
The US announcement brought counter accusations from the Chinese government, with one official reigniting an unsubstantiated theory blaming the US for releasing the virus from an Army research facility. Perhaps more notably, researchers around the world raised concern over the volatility of the debate, warning the tone could harm efforts to investigate the virus’s origin but also hinder cooperation during upcoming high-level discussions about pandemic preparedness. Others worry the rhetoric is fueling online bullying of scientists and anti-Asian harassment in the US. While knowing the origin of SARS-CoV-2 could help prevent future disease outbreaks, it is feared that political posturing will continue to impede investigations and transparency.
BREAKTHROUGH INFECTIONS The US CDC COVID-19 Vaccine Breakthrough Case Investigations Team published analysis of breakthrough infections reported through April 30. The study, published in the US CDC’s MMWR, includes 10,262 breakthrough infections from 46 states. From preliminary data, 27% of breakthrough cases were asymptomatic, 10% were hospitalized, and 2% died. Of the hospitalized cases, 29% were asymptomatic or hospitalized for a reason other than COVID-19. Sequence data were available for only 5% (555 cases) of cases, 64% of which identified variants of concern: B.1.1.7 (56%), B.1.429 (25%), B.1.427 (8%), P.1 (8%), and B.1.351 (4%). The University of Washington Virology Lab (UWVL) also found variants of concern to be responsible for breakthrough infections. They sequenced 20 vaccination breakthrough infections from UW Medicine and found that all 20 cases were classified as variants of concern. Of the variants, B.1.1.7 represented 40%, B.1.429 40%, B.1.427 10%, B.1.351 5%, and P.1 5%. Compared to the control group, the frequency of VOC breakthroughs increased 1.47 fold. During that same time interval, 68% of Washington state cases sequenced at UWVL consisted of variants of concern.
As of May 1, the CDC is no longer investigating all vaccine breakthrough infections, instead focusing only on hospitalized and fatal cases. Vaccine effectiveness studies will continue, but only in limited populations.
IMMUNITY DURATION Two new studies shed light on questions surrounding the longevity of SARS-CoV-2 immunity following infection or vaccination. In one study, published May 24 as an unedited manuscript in Nature, researchers from the University of Washington Medical School (Missouri; US) examined COVID-19-convalescent individuals for evidence of long-lived bone marrow plasma cells (BMPCs), a persistent and essential source of protective antibodies. Among 77 individuals who had recovered from mild COVID-19, the researchers found that serum anti-SARS-CoV-2-spike antibodies decayed significantly 4 months after infection with a continued, more gradual delay for at least 7 more months. Among 18 patients from whom bone marrow aspirates were obtained, spike-specific BMPCs persisted 7-8 months post infection, suggesting that they were part of a dormant, long-lived compartment. The research team concluded that previous SARS-CoV-2 infection resulting in mild symptoms led to a robust antibody response, showing potential for these immune factors to persist months after infection.
In another study, published in bioRxiv (preprint), researchers from Rockefeller University (New York; US) report on a cohort of 63 COVID-19-convalescent individuals assessed at 1.3, 6.2, and 12 months after infection, 41% of whom also received mRNA vaccines. In individuals who were not vaccinated, neutralizing activity and a specific type of memory B cells remained relatively stable from 6 to 12 months. Notably, vaccination increased all components of the humoral response and resulted in serum neutralizing activities against variants of concern that are comparable to or greater than neutralizing activity against the original SARS-CoV-2 strain achieved by vaccination of naïve individuals. The data suggest that immunity among recovered COVID-19 patients likely will be very long lasting, and those who receive mRNA vaccines should produce enough antibodies and memory B cells to provide protection against circulating SARS-CoV-2 variants. The researchers speculate this is evidence to consider boosters for non-convalescent but vaccinated individuals as new variants of concern emerge.
VACCINE EFFICACY IN RECOVERED CASES A group of researchers from Italy, the UK, and the US have called for updating vaccination guidance to recommend a single dose of mRNA-based SARS-CoV-2 vaccines for individuals who have recovered from SARS-CoV-2 infection. The commentary, published in The Lancet, cites several recent studies that provide evidence that a single dose of these vaccines in individuals who were previously infected with SARS-CoV-2 stimulates a similar or better protective immune response than in naïve individuals after their second dose. Essentially, the first dose would act like the booster dose in individuals who have recovered from SARS-CoV-2 infection. The authors acknowledge that these were small studies; however, they argue that eliminating the second dose for these individuals would allow additional doses to be distributed to areas of need and expand the reach of the existing limited vaccine supply. This could increase the number of vaccinated individuals without sacrificing protection for recovered individuals. If this strategy were applied globally, it potentially could save nearly 170 million doses (ie, at 1 dose per reported case), which would be sufficient to fully vaccinate an additional 85 million people.
UK INCREASE IN VARIANT CASES A software error in the UK government’s test and trace system might have contributed to the spread of the B.1.617.2 variant in the country, with reported cases of that variant rising more than 160% over the week ending May 19. Case numbers of the variant, first detected in India, rose from 1,313 to 3,424, according to data from Public Health England. The agency has designated another variant, known as VUI-21MAY-01 or AV.1, as a “variant under investigation,” with 49 cases detected across the country. Several localities that experienced an increase in B.1.617.2 cases did not have access to full data on positive test results in their areas between April 17 and May 17, meaning 734 positive tests went unreported to local authorities, who in turn could not conduct contact tracing. Officials say the issue has been resolved, and they are working to contain the outbreaks.
INDIA This week, India became the third country to record more than 300,000 COVID-19 deaths, although the true death toll is likely much higher. In the coastal areas of West Bengal and Odisha states, officials evacuated about 1.5 million people to cyclone shelters ahead of Cyclone Yaas, which made landfall May 26, complicating efforts to contain SARS-CoV-2 amid the country’s devastating second wave. Although officials appealed for evacuees to double-mask and maintain physical distance, experts worry evacuation efforts never took the pandemic into account, instead focusing on rescuing as many people as possible in a short time span.
Meanwhile, Indian officials have recorded nearly 9,000 cases of mucormycosis, the so-called black fungus, primarily among people with COVID-19 or those who have recovered. The increase in cases of the usually rare fungal infection is raising fears that it could impact COVID-19 patients more severely than others, as it spreads through the respiratory tract and is especially harmful to those with weakened immune systems and underlying conditions. Health officials say the disease is more prevalent in rural areas and smaller cities, where unqualified doctors are improperly treating COVID-19 patients with steroids, which increasingly is associated with contracting mucormycosis. Some experts speculate unsanitary conditions, including the use of improperly or non-sanitized oxygen cylinders or ventilators, could be contributing to the outbreak, although others argue unsanitary conditions in many hospitals existed prior to the pandemic.
OXYGEN SHORTAGES As India continues to struggle amid a surge in COVID-19 cases, experts warn other nations are reporting record increases over the last few weeks. Countries from Argentina to Nepal are experiencing record surges, while inequity in vaccine distribution continues. Like India, these countries face oxygen shortages amid increasing demand, according to an analysis by the Bureau of Investigative Journalism. The report—based on data provided by Every Breath Counts Coalition, PATH, and the Clinton Health Access Initiative (CHAI), as well as global vaccination data—determined 19 countries are most at risk of elevated death rates from oxygen shortages. Those countries—including Argentina, Colombia, Iran, Nepal, the Philippines, Malaysia, Thailand, Pakistan, Costa Rica, and South Africa—need more than 50,000 cubic meters a day for COVID-19 patients. The report notes that in nearly all of the countries, less than 1% of the population has received one dose of vaccine, underscoring the need to quickly distribute and administer vaccines in low- and middle-income countries (LMICs).
AUSTRALIA In response to an ongoing COVID-19 outbreak, Victoria, Australia is entering its fourth “lockdown.” The state government is implementing COVIDSafe “circuit breaker” restrictions for a period of 7 days due to concerns that contact tracing efforts are not able to keep up with community transmission. Like previous lockdown periods, individuals are directed to remain at home, except for essential activities, including grocery shopping, health care (including SARS-CoV-2 vaccination), authorized work or study, and exercise. Additionally, several other Australian states have implemented travel restrictions, including mandatory quarantine, for travelers from Victoria. Reportedly, case investigations of 26 recent infections have identified approximately 10,000 contacts who may be at risk of exposure at more than 150 locations across the state.
PROPOSED LIMITS ON PUBLIC HEALTH AUTHORITY The Network for Public Health Law and the National Association of County and City Health Officials (NACCHO) published a report on the risks posed by new and pending legislation to limit public health authority in US localities, including during public health emergencies. In response to executive and public health orders issued at the state and local levels during the US COVID-19 response, a number of state legislatures have passed or are actively considering bills to “limit severely the legal authority of public health agencies to protect the public from serious illness, injury, and death.” The report provides an overview of the history of public authority in the US and outlines current efforts to “undermine the authority of public health agencies.” Current efforts to limit local public health authority attempt to shift power away from local public health agencies and toward either other local entities or to the state level.
Additional efforts are targeting executive authority of governors in favor of state legislatures, and others aim to eliminate the authority to implement specific public health interventions, including mask mandates, business closures, and quarantine. While these efforts are arising from the COVID-19 experience, they could have far-reaching impacts on other public health threats. In addition to impacting routine disease control efforts or non-emergency outbreak responses, they could remove decision-making authority from public health and medical experts and place it in the hands of elected officials, who may not possess the necessary expertise. The report also concludes that some of these efforts could exacerbate racial and ethnic disparities during the ongoing pandemic response.
RURAL HOSPITAL CLOSURES For decades, a variety of issues have put US rural hospitals in a fragile position, challenges amplified by the COVID-19 pandemic. According to research by the University of North Carolina at Chapel Hill, a record 19 rural hospitals shuttered in 2020 amid the pandemic, more than in any other year. For people with COVID-19, or those with suspected SARS-CoV-2 infection, these closures and crowding at other rural facilities are creating obstacles and delays for people seeking care and testing. A new STAT analysis shows that communities containing hospitals that closed experienced disproportionate COVID-19 deaths, 37% higher in counties where hospitals shut than in their states overall. In most rural counties—those with fewer than 50,000 residents and at least 50 miles from a major city—death rates were two-thirds higher than in their states. The closures are clustered across the South and Southeast, erecting another barrier to care for largely Black communities. Although several rural hospital closures were avoided last year due to US government support, experts fear more are on the horizon once short-term funding dries up. These closures are impacting care for primarily lower-income populations with declining health and forcing those who lose healthcare jobs to leave the areas. Experts fear the worst is yet to come, with rural hospital closures having impacts far beyond COVID-19 patients.
PARENTAL CONSENT FOR TEENS Young people across the US have taken to social media sites to promote SARS-CoV-2 vaccination among their peers. While many parents have lept at the opportunity to vaccinate their teenagers, there are some who are resisting the idea, with parents’ willingness to vaccinate their children usually aligning with their own intentions. According to data collected in April through the KFF COVID-19 Vaccine Monitor, 3 in 10 parents of children ages 12-15 say they will get their child vaccinated, 25% say they will wait a while to see how the vaccine is working, 18% plan to get their child vaccinated if their school requires it, and nearly 25% say they will definitely not get their child vaccinated. Parental consent is needed in most states, except for in North Carolina, where all teenagers can receive vaccinations without parental permission; in Tennessee and Alabama, where those 14 and older do not need consent; and in Oregon, where parental approval is not required for teens 15 and older. Public health experts maintain that vaccinating the US teen population is critically important for completely returning to in-person schooling and for the economy.
SOTROVIMAB EUA The US FDA issued an Emergency Use Authorization (EUA) for a new monoclonal antibody treatment for COVID-19. The drug, sotrovimab, was developed by Vir Biotechnology and GlaxoSmithKline (GSK) to target the SARS-CoV-2 spike protein. The FDA authorized the use of sotrovimab in COVID-19 patients aged 12 years and older who are at high risk for progressing to severe disease, including adults aged 65 years and older and those with underlying medical conditions. The treatment is currently undergoing rolling review by the European Medicines Agency (EMA). On May 21, the EMA’s Committee for Medicinal Products for Human Use (CHMP) recommended issuing a Conditional Marketing Authorization, but to our knowledge, the European Commission has not yet issued the authorization.
VACCINE EFFICACY AGAINST EMERGING VARIANTS In a study published in the New England Journal of Medicine, US pharmaceutical company Novavax reported its SARS-CoV-2 vaccine had an acceptable safety profile and exhibited strong neutralizing antibody responses in a Phase 2a-b clinical trial in South Africa. The study included 2,682 baseline seronegative participants, of which 94% were HIV-negative. Symptomatic COVID-19 was observed in 15 participants in the vaccine group and 29 in the placebo group, most of which were categorized as mild to moderate cases with the exception of one severe case in the placebo group. Vaccine efficacy in the HIV-negative group was 60.1% and 49.4% regardless of HIV status, which meets the efficacy criteria for primary Phase 2b evaluation. Researchers sequenced 41 isolates from the symptomatic cases, of which 38 (92.7%) were the B.1.351 variant. In a post hoc analysis, the vaccine’s efficacy against the B.1.351 variant was 51.0% in the HIV-negative group and 43.0% in the combined HIV-negative and HIV-positive population.
by ponchi101 I was only able to read the title until the pay-wall kicked in. I am far from that. My sister in law has several friends that have done it, from Venezuela (Dest Miami). Some people in Colombia too. So it is not unusual, for middle class and those that can afford it.
Plus, remember, Colombia is vaccinating with Sinopharm. Sorry, not for me.
by JazzNU
ponchi101 wrote: ↑Mon May 31, 2021 1:01 am
I was only able to read the title until the pay-wall kicked in.
‘Like a Dream’: Latin Americans Head to U.S. for Covid Shots
Frustrated with the lagging pace of vaccinations at home, well-off Latin Americans have been flying north for a shot — and feeling guilty about those left behind.
By Ernesto Londoño, Daniel Politi and Santi Carneri
RIO DE JANEIRO — Florencia Gonzalez Alzaga, a photographer from Buenos Aires, hatched her plan to fly to the United States for a coronavirus vaccine after the subject came up in her Zoom book club.
Juan Pablo Bojacá, an Instagram influencer from Colombia who specializes in frugal travel, urged his 137,000 followers to give it a try, posting a step-by-step video guide that showed him clearing passport control in Miami.
José Acevedo, a real estate agent in Paraguay, was stunned by how easy the whole thing was in Las Vegas.
Frustrated with the lagging pace of vaccine campaigns at home and seeing a surplus of doses in the United States — where tens of millions of Americans have opted not to get inoculated — wealthy and middle-class Latin Americans with American tourist visas have been flocking to the United States in recent weeks to score a Covid-19 shot.
“It’s like a dream,” said Ms. Gonzalez, who got her shot in Miami in April.
The access has proved a bonanza for the privileged in countries where the virus continues to take a brutal toll — even if many, including those who are benefiting, struggle with the fact that vaccine tourism exacerbates the inequality that has worsened the pandemic’s toll.
Sean Simons, a spokesman for the ONE Campaign, which works to eradicate disease and poverty, said vaccine travel could have serious unintended consequences, and urged nations with vaccine surpluses to funnel them instead through a World Health Organization vaccine distribution system known as Covax.
“Millionaires and billionaires traveling across continents or oceans to get a vaccine, usually twice, means greater exposure, higher likelihood of variants spreading and access only for the most elite,” he said.
The Biden administration said this month that it would give 80 million vaccine doses by the end of June to countries that are scrambling to vaccinate their people.
Still, as success stories of Latin Americans getting their jabs are shared on social media posts and by word of mouth, and local officials in New York and Alaska actively encourage vaccination tourism, the cost of airfare on several routes has skyrocketed as thousands make plans to head north.
Travel agencies in the region have begun selling vaccination packages, including multicountry itineraries for Brazilians, who must spend two weeks in a third country before being allowed to enter the United States.
José Carlos Brunetti, the vice president of Maral Turismo, a travel agency in Paraguay’s capital, Asunción, said these trips had been a godsend for his industry after a dismal year.
“The frenzy to travel to the United States to try to get vaccinated began in March,” he said. “Now we’re seeing exponential growth in the number of passengers and flights.”
Broadly, foreigners who enter on a tourist visa are allowed to seek medical care in the United States.
While the State Department conducts security background checks on foreigners applying for visas, officials said it did not screen for people who are visiting explicitly to get a vaccine, and there appears to be no federal government guidance for foreigners coming to the United States for that purpose.
Once in the country, officials said, it is up to states, local communities and individual health care providers to decide whether to give the vaccine without proof of American residency.
Prominent politicians in Latin America have been among those who have flown to the United States for a shot.
César Acuña promised as a presidential candidate in Peru earlier this year that he intended to be “the last” in his country to get a shot. But after losing at the polls, he said there was no point in keeping that promise.
“Remember I’m 68 years old; I’m a vulnerable person,” he said in a radio interview.
Mauricio Macri, the former president of Argentina, vowed in February that he would not “be vaccinated until the last Argentine in a high-risk group and all essential workers have.” Despite having imposed a series of strict quarantine measures since last year, Argentina is facing a widespread epidemic that experts believe is being fueled in part by a highly contagious variant first detected in Brazil.
Despite his vow on waiting to get vaccinated, Mr. Marci wrote in a post on Facebook this month that he had received the Johnson & Johnson single-shot vaccination in Miami after realizing that “vaccines are being applied everywhere, from beaches to malls and even at pharmacies.”
Among 12 Latin Americans who traveled to the United States for vaccines and were interviewed for this article, several expressed feeling conflicted. Some who declined to speak on the record said they felt guilty about getting vaccines while compatriots who are more vulnerable to the disease remain exposed.
Ms. Gonzalez, the Argentine photographer, said her plan had been conceived after members of her online book club began talking more about their fears related to the pandemic than about the books they were reading.
“We started talking about it and figured: Why shouldn’t we go to Miami and get vaccinated?” she said. “From one week to the next we bought the tickets.”
Ms. Gonzalez said she had been able to easily book a vaccine appointment the day after arriving in Miami on April 1. The Johnson & Johnson shot she received at a Salvation Army center there was the end of an agonizing period of isolation that reminded her of her cancer treatment seven years ago.
She was surprised by how few questions the people at the vaccination site asked. “They wanted to vaccinate people,” she said. “They were excited to be vaccinating.”
The early wave of Argentine vaccine travelers who returned home with American vaccine certificates drove a sharp rise in the cost of airfare, said Santiago Torre Walsh, who runs a popular travel blog, Sir Chandler.
Travelers were initially reluctant to acknowledge the purpose of their trip, he said.
“Now that’s changed,” he said. “People seem more willing to talk about it openly, and that in turn motivates other people to do it as well.”
That’s what Mr. Bojacá, the Colombian Instagram influencer, did. The video of his vaccination journey, posted on Instagram, includes a surreptitiously recorded scene in which an American passport control officer asked who he was visiting. He and a travel companion said they were visiting friends.
“The guy didn’t even ask what we came here to do,” Mr. Bojacá marveled in a subsequent scene in the video. “I had practiced like 80 times how to say ‘vaccines’ in English.”
While the stream of vaccine travelers from countries like Colombia, Peru, Argentina and Mexico has been growing for months, Brazilians have faced a unique challenge.
The United States currently bars most people who have spent time in Brazil from boarding flights to American cities, unless they have spent two weeks in a country that is not subject to coronavirus travel restrictions. Returning American citizens and permanent residents are still allowed to enter the United States.
Andrea Schver, the owner of Venice Turismo, a travel agency based in São Paulo, said the ban had not been insurmountable for wealthy customers, who are increasingly willing to spend several thousand dollars to secure a shot. In April she sold packages that included a two-week layover in places like Cancún or a Caribbean island. Just in the first 18 days of May, she arranged trips for more than 40 passengers, she said.
Clients include a television personality who will start recording a new show soon and other wealthy Brazilians who are used to taking extravagant vacations each year, she said.
“These are families who travel all year long, and they’ve been grounded for the past year with money to spare,” she said, noting that almost all clients had purchased business-class tickets. “These aren’t people who are going to look for bargains.”
Mr. Acevedo, the real estate agent in Paraguay, said he had come to see his vaccine trip as a worthwhile investment and possibly a lifesaving step, because being overweight puts him at higher risk.
“I can’t stop working, producing, and my work entails contact with many people,” he said.
He reasoned that by securing an American vaccine, he is easing the burden on the Paraguayan government.
“Part of this is not taking up a dose from people who need them more,” he said.
Ernesto Londoño reported from Rio de Janeiro, Daniel Politi from Buenos Aires and Santi Carneri from Asunción, Paraguay. Lis Moriconi contributed reporting from Rio de Janeiro and Lara Jakes from Washington.
ponchi101 wrote: ↑Mon May 31, 2021 1:01 am
I was only able to read the title until the pay-wall kicked in. I am far from that. My sister in law has several friends that have done it, from Venezuela (Dest Miami). Some people in Colombia too. So it is not unusual, for middle class and those that can afford it.
Plus, remember, Colombia is vaccinating with Sinopharm. Sorry, not for me.
Are you staying in the U.S. for the 3 weeks until your second shot, or have you returned home, and will go back for the second dose?
If you don't want to divulge that information, I understand - you can even delete this post if you wish.
by mmmm8
ponchi101 wrote: ↑Mon May 31, 2021 1:01 am
I was only able to read the title until the pay-wall kicked in. I am far from that. My sister in law has several friends that have done it, from Venezuela (Dest Miami). Some people in Colombia too. So it is not unusual, for middle class and those that can afford it.
Plus, remember, Colombia is vaccinating with Sinopharm. Sorry, not for me.
Yup, 2 of my Colombian colleagues have come and friends who live in Mexico (but are American). My SO's Venezuelan family aren't bothering (which is stupid because they can afford it and his aunt died from COVID) except his sister and brother-in-law who would like to but can't because they live in Brazil and the US won't let them in...
by ponchi101
Deuce wrote: ↑Mon May 31, 2021 2:49 am
...
Are you staying in the U.S. for the 3 weeks until your second shot, or have you returned home, and will go back for the second dose?
If you don't want to divulge that information, I understand - you can even delete this post if you wish.
I can put my paranoia on hold for a while
I am staying with my family. My sister in law and my niece live in Macon, and they can use a hand repairing stuff and things at their homes. Also, my niece had a premature baby back in November so we are visiting and getting to know the baby, who is doing wonderfully.
Cheaper for me to stay here for a few weeks than fly back and forth. Round trip tickets are, at the cheapest fare, about $600, times two (my GF is with me). I can eat a lot with that much money.
by Suliso Have you all been paying attention to the fact that covid lab leak theory MIGHT be true after all? That would be monumental...
Also a lot of credit to a particularly sceptical colleague of mine (a scientist, but not inefctologist) who was laughing a year ago and saying "of course it's a lab leak".
by mmmm8
Suliso wrote: ↑Tue Jun 01, 2021 5:37 pm
Have you all been paying attention to the fact that covid lab leak theory MIGHT be true after all? That would be monumental...
Also a lot of credit to a particularly sceptical colleague of mine (a scientist, but not inefctologist) who was laughing a year ago and saying "of course it's a lab leak".
Always seemed like the most plausible theory (but an accidental leak, what I didn't buy is that it was malicious)
by Suliso I don't think malicious is claimed, albeit telling a difference between accidental and malicious by a single scientist would be impossible.
Lesson for all - don't dismiss information because you don't like the messenger.
by skatingfan
Suliso wrote: ↑Tue Jun 01, 2021 5:48 pm
I don't think malicious is claimed, albeit telling a difference between accidental and malicious by a single scientist would be impossible.
Lesson for all - don't dismiss information because you don't like the messenger.
The problem was that a year ago there was no information just a theory that was used to attack Asian-Americans, and the messenger had the authority to investigate the theory but whether it was true or not has never been important to that particular individual.
Suliso wrote: ↑Tue Jun 01, 2021 5:48 pm
I don't think malicious is claimed, albeit telling a difference between accidental and malicious by a single scientist would be impossible.
Lesson for all - don't dismiss information because you don't like the messenger.
The problem was that a year ago there was no information just a theory that was used to attack Asian-Americans, and the messenger had the authority to investigate the theory but whether it was true or not has never been important to that particular individual.
I know, but we shouldn't have dismissed it merely because you know who was pedling it. Actually I also never fully dismissed it because that would involve trusting Chinese (the state not private citizens).
Sometimes even horrible people are right.
by ponchi101 Remember that what we were being mostly skeptical about was that it was a Lab virus, but that it was designed and released on purpose.
Which, we were saying, would make no sense because if the Chinese Govt would release a virus to hurt the rest of the world, releasing it inside its borders would be really dumb.
Other than that, as you say, this news would be monumental.
by Drop-shot
Suliso wrote: ↑Tue Jun 01, 2021 5:37 pm
Have you all been paying attention to the fact that covid lab leak theory MIGHT be true after all? That would be monumental...
Also a lot of credit to a particularly sceptical colleague of mine (a scientist, but not inefctologist) who was laughing a year ago and saying "of course it's a lab leak".
Have you read my last posts in this thread? Hellooooo
by Suliso Sorry, drop-shot. Forgot that you already mentioned it. Maybe doubly convincing now
by Suliso Peru has updated their covid fatality rate to 1/200 people, the worst in the world. Peru's growth rate is ca 1.1% per year so the disease has almost halved it.
by ponchi101 Colombia has increased its rate of vaccination during the last week considerably. A friend, younger than I, got vaccinated yesterday with Pfizer.
So basically, I just wasted a considerable chunk of money to fly here and get vaccinated. So far, the story of my year: try to do the sensible thing, have it blow up in my face.
I frequently wonder how come I am not an alcoholic.
(Good for Colombia, one must admit)
by Suliso Don't be too sad ponchi. You got an vacation out of it and a reason to visit relatives.
by ponchi101 I know. I am really trying to look at it that way. That is a plus.
But I really spent some money that right now I have not a lot of. I already cut down the gym and the tennis back home and, unless some works comes my way soon, those activities are out of any planning anytime soon
by JazzNU
ponchi101 wrote: ↑Wed Jun 02, 2021 1:19 pm
Colombia has increased its rate of vaccination during the last week considerably. A friend, younger than I, got vaccinated yesterday with Pfizer.
So basically, I just wasted a considerable chunk of money to fly here and get vaccinated. So far, the story of my year: try to do the sensible thing, have it blow up in my face.
I frequently wonder how come I am not an alcoholic.
(Good for Colombia, one must admit)
Well you said you might have had to get Sinovac if you went to where you would get the vaccine at home, that you couldn't guarantee the one you'd get, that they wouldn't let you choose, so probably still the better plan to ensure you got the one you're most confident in.
Another plus - Much less likely to catch covid here before you're fully vaccinated. When I read about the Copa America plan that is just begging to be a super spreader event for the continent I thought really good you're not there right now, you can get fully vaccinated before returning to that well thought out plan they've got.
by Suliso Just a reminder that not every vaccine is the same and it does matter which one you take.
Early adopters of Chinese vaccines see case surges; China plows ahead anyway
China is now giving 20 million doses a day despite low efficacy.
Despite a sluggish start, China is now vaccinating its people against COVID-19 at an impressive clip, currently averaging nearly 20 million doses administered per day. As of Friday, the country had given more than 720 million vaccinations since mid-December, with nearly 400 million of those were given in May alone.
The dramatic ramp up comes at an awkward time, however. Early adopters of China’s vaccines have seen dramatic surges in COVID-19 cases—despite high vaccination rates—and are now backing away from the country’s offerings.
In Bahrain, for instance, officials are now offering high-risk people who have already received two doses of China’s Sinopharm vaccine a third vaccine dose—but one made by Pfizer-BioNTech. The apparent vote of no confidence by officials is striking: Bahrain was one of the first countries to back and rollout Sinopharm’s vaccine, and it has had a highly successful vaccination campaign. Nearly 58 percent of the Persian Gulf country has received at least one dose of a vaccine, and most of the vaccines given in Bahrain are from Sinopharm. But the country is now seeing its worst wave of COVID-19 yet and the government has recently issued a two-week lockdown to try to get transmission under control.
The Seychelles went through a similar struggle. The archipelago saw a dramatic spike in cases in mid-May, despite having around 70 percent of its population vaccinated with at least one dose. Like Bahrain, the Seychelles had largely relied on the Sinopharm vaccine.
Dubai, which has also relied on Sinopharm’s vaccine, is now quietly offering residents who have been fully vaccinated with the Sinopharm vaccine the opportunity to get re-vaccinated with the Pfizer-BioNTech vaccine, according to the Wall Street Journal.
Efficacy "not high"
In a study published on May 26 in JAMA, Sinopharm researchers reported results suggesting that their inactivated virus vaccine was up to 78 percent effective against symptomatic COVID-19 cases. But the study was done mainly in young, healthy men, and the results were not conclusive regarding whether the vaccine was effective against severe disease or asymptomatic cases.
Unpublished data out of Serbia suggested that some people given the vaccine may not produce antibodies to fight off the pandemic coronavirus three months after vaccination, according to reporting by the Wall Street Journal. “The Sinopharm vaccine is not immunogenic enough, and it appears that its impact is especially low on elderly recipients,” said Olgica Djurkovic-Djakovic, of the University of Belgrade, who led the unpublished study and shared the findings with the Journal.
In April, the head of China’s Centers for Disease Control and Prevention, George Gao, seemed to acknowledge this potential problem. “The efficacy of the existing vaccines is not high,” he said at a conference, discussing the country’s vaccines. Last month, Beijing reportedly began planning to offer third doses of the country’s vaccines to try to boost protection.
Still, last month the World Health Organization granted an emergency use listing (EUL) for Sinopharm's COVID-19 vaccine, paving its way for global use. Just on Tuesday, the WHO granted an EUL to China’s Sinovac vaccine. Like Sinopharm’s vaccine, Sinovac's vaccine is an inactivated virus vaccine, and the two appear to have similar track records. Both Chile and Uruguay rolled Sinovac’s vaccine into their mass vaccination campaigns and have seen subsequent spikes in cases.
by dryrunguy Dolphins got the J&J vaccine yesterday. He drove himself back home, was a little wobbly, but he got along just fine and maintained his usual activities though the afternoon and evening.
And then this morning happened. He had a pounding headache all morning and it is just now starting to go away. But the thing is that he routinely has headaches, since his body is so mucked up, so I can't certainly attribute it to the vaccine--even though this one, from my standpoint as an observer, looked and "felt" worse than usual.
I'm planning to get my dose Tuesday afternoon. I'm glad we stuck to the plan to get vaccines at different times.
by Suliso Get the Pfizer one dry if you can choose. From everything I hear the side effects are the lowest and efficiency the highest for that one.
by ti-amie I'm so sorry for Dolphins. I hope he'll be better by later today.
by dryrunguy
Suliso wrote: ↑Sat Jun 05, 2021 4:15 pm
Get the Pfizer one dry if you can choose. From everything I hear the side effects are the lowest and efficiency the highest for that one.
I cannot overstate what a pain in the keester it would be to give up roughly 6 hours over 2 days to get 2 doses. I agree with what you said, but when you're 35-40 minutes from a vaccination site, the single dose is really attractive--even if you're compromising on potential side effects and efficacy. We talked about it at length and ultimately decided, all things considered, J&J was good enough. It probably sounds like silly reasoning, especially given the lengths to which ponchi has gone to get the vaccine, but...
by ti-amie Suliso's post about what is happening with the vaccine ponchi traveled to avoid is sobering. I'm glad he made the trip to Georgia.
by Deuce This is potentially interesting...
(But I don't recommend anyone wait for it - it's much better to go get a current vaccine NOW...)
by dryrunguy The Situation Report is back. Here's the latest. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 173.2 million cumulative cases and 3.7 million deaths worldwide as of 6:00am EDT on June 8. Global weekly incidence and mortality continue to decline. The weekly incidence as of May 31 decreased 15.43% from the previous week, and weekly mortality decreased by 8.33%. Data are showing potentially steep declines for the week ending June 7, although data remain incomplete.
Global Vaccination
The WHO reported 1.9 billion doses of SARS-CoV-2 vaccines administered globally as of June 5, and 800 million individuals have received at least 1 dose. Our World in Data reported 2.18 billion cumulative doses administered globally, and the global cumulative total continues to increase at 12% per week. Daily doses administered have begun to decrease, to 34.5 million doses per day, down from a record of 35.9 million doses per day on June 5. Our World in Data estimates there are 467 million people worldwide who are fully vaccinated, corresponding to approximately 6% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.2 million cumulative cases and 594,802 deaths. Daily incidence and mortality continue to decline, to the lowest levels since early in the pandemic. The current average daily incidence—13,276 new cases per day—is the lowest since March 27, 2020, early in the United States’ initial surge. On May 31, the US reported fewer than 10,000 new cases in a single day for the first time since March 21, 2020. With 378 deaths per day, the United States’ daily mortality is the lowest since March 29, 2020. Additionally, the US continues to report new record values for test positivity, now down to 2.11%.
As the US reaches daily incidence levels not reported since the earliest days of its COVID-19 epidemic, we will take a brief look at trends in daily incidence at the state and regional levels. At the regional level, current trends are relatively similar across the country. All regions are currently reporting decreasing trends in daily incidence. On a per capita basis, Regions 7 (central), 8 (mountain west), and 9 (west coast) faced the most severe winter 2020 surges, but Regions 7 and 9 reported minimal surges in spring 2021. Regions 4 (southeast) and 6 (south central) also reported relatively small spring 2021 surges. On a per capita basis, the largest spring 2021 surges were in Regions 1 (northeast), 2 (New York/New Jersey), and 5 (midwest).
While there was considerable variation in terms of the timing and magnitude of the regional peaks in winter 2020 and spring 2021, all regions are currently reporting similar per capita daily incidence and decreasing trends. Regions 8 (8.1 daily cases per 100,000 population) and 10 (northwest; 7.1) are currently reporting the highest per capita daily incidence, and Regions 1 (2.3) and 9 (2.4) are reporting the lowest. Most of the remaining regions fall between approximately 3.0-4.5 daily cases per 100,000 population. For context, most regions were reporting between 60 and 100 daily cases per 100,000 population during their autumn/winter 2020 peak.
Notably, multiple sources indicate that most US states are reporting decreasing or steady trends in daily incidence. The Johns Hopkins Coronavirus Resource Center identifies only 6 states (plus Washington, DC) with notable increasing trends over the past 2 weeks: Alabama, Idaho, Louisiana, Montana, Nevada, and Wyoming. The Reuters COVID-19 Tracker reports that 40 states are reporting decreasing trends over the past 2 weeks, and the other 10 (plus Washington, DC) are reporting steady trends over that period. Analysis by The New York Times shows state-level biweekly trends in daily incidence range from -5% to -81%, with no states reporting increasing trends over that period.
According to US CDC data, the state-level per capita daily incidence ranges from Vermont with 1.0 daily case per 100,000 population to Colorado with 9.9. Wyoming (9.3) and Florida (9.1) are the only other states reporting more than 9 daily cases per 100,000. South Dakota (1.3), California (1.6), Nebraska (1.6), New Hampshire (1.6), Connecticut (1.75), Michigan (1.8), and Maryland (1.8) are other states reporting fewer than 2.0 daily cases per 100,000. Most states fall between approximately 3.1 and 6.2. As a whole, the US is reporting 4.0 daily cases per 100,000. But even with this wide variation between states, all are currently reporting a small fraction of their highest peak.
US Vaccination
The US has distributed 371.5 million doses of SARS-CoV-2 vaccines and administered 302.8 million. After a brief increase, the daily doses administered* is once again decreasing, down to 828,634 doses per day as of June 2, the lowest average since January 11. Approximately 469,294 people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 171 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 51.6% of the entire US population. Among adults, 63.7% have received at least 1 dose, and 6.8 million adolescents aged 12-17 years have received at least 1 dose. A total of 139.7 million people are fully vaccinated, which corresponds to 42.1% of the total population. Among adults, 53% are fully vaccinated, and 3 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 86.4% with at least 1 dose and 75.6% fully vaccinated. In terms of full vaccination, 72 million individuals have received the Pfizer-BioNTech vaccine, 56.6 million have received the Moderna vaccine, and 11 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
WHO VARIANT NAMING CONVENTION For months, experts have recognized the challenge of effectively communicating about variants of concern (VOCs) and called for a simplified naming convention. On May 31, the WHO unveiled a new system that will assign Greek letters to VOCs and variants of interest (VOIs) as a more convenient label. While many VOCs have been colloquially labeled using their place of origin (e.g., Brazil, India, South Africa, UK), the use of locations is inconsistent with existing WHO guidelines for naming diseases and pathogens. The use of locations, events, peoples, or other characteristics contributes to stigmatization of affected individuals, locations, and cultures. The use of Greek letters for SARS-CoV-2 variants shortens the nomenclature into a convenient shorthand without risking associated stigma.
The WHO has updated its list of VOCs, with Greek letters assigned to the first 4 VOCs—Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2)—as well as 6 VOIs. The existing scientific VOC/VOI labels will continue to be used in some settings, as they “convey important scientific information,” but the Greek letters will be used broadly in public communications. While the new method aims to simplify communications, it is not without limitations. Perhaps most notably, it is not immediately clear what will happen if more than 24 VOCs/VOIs are identified. Additionally, the new naming convention does not appear to apply to variants that are not designated as VOCs/VOIs, and it is unclear whether variants will retain their Greek letter if they are ultimately removed from these lists.
US GLOBAL VACCINE DONATION As part of the US pledge to donate 80 million doses of SARS-CoV-2 vaccines by the end of June, US President Joe Biden on June 3 announced an immediate donation of 25 million doses to low- and middle-income countries. About 75%, or 19 million doses, will go to the COVAX initiative, through which approximately 5 million doses will go to Africa, 7 million to South and Southeast Asia, and 6 million to Latin America and the Caribbean. The vaccine donation to COVAX represents nearly one-third of the total vaccine doses the initiative has supplied to date. The other 6 million doses will be donated bilaterally to countries in need, those experiencing surges, immediate neighbors, and other countries that have requested US assistance, including India, the West Bank and Gaza, Canada, Mexico, Egypt, Iraq, and the Republic of Korea. The total 80 million doses are expected to come from 4 manufacturers: Pfizer-BioNTech, Moderna, J&J-Janssen, and AstraZeneca-Oxford, the last of which has not yet received emergency authorization in the US.
According to White House COVID-19 Response Coordinator Jeffrey Zients, the US also lifted the Defense Production Act’s “priority rating” for 3 vaccine manufacturers—AstraZeneca, Novavax, and Sanofi—that do not have vaccines authorized in the US. This means US producers of vaccine materials and ingredients do not have to prioritize orders from those companies, potentially clearing the way for more materials to be shipped to overseas vaccine manufacturers. Zients acknowledged that the US pledge to provide 80 million doses by the end of June will not be sufficient to end the pandemic but represents a significant step toward that goal. He promised the US government will continue to work among its own agencies and with other countries, including the G7, to end the pandemic.
GLOBAL VACCINE ACCESS Amid alarming global disparities in SARS-CoV-2 vaccine access, more than 230 former government leaders and prominent figures are calling upon leaders of G7 countries to pay the majority of the US$66 billion required to vaccinate people in low-income countries. The letter, released ahead of a 3-day G7 summit hosted by the UK that begins June 11, argues that such an investment is affordable, vital to stopping the spread of new SARS-CoV-2 variants, and “the best insurance policy in the world.” The letter—signed by former Prime Ministers Gordon Brown and Tony Blair, former UN Secretary-General Ban Ki-moon, and 15 former African leaders—calls on G7 countries to lead the way on sharing vaccine doses, voluntary licensing agreements, and temporary patent waivers to enable vaccine manufacturing to begin on every continent. The signatories expressed dismay over the failure of global cooperation in 2020, but conveyed hope that 2021 could usher in a new age. In another open letter published on June 7, global health experts laid out an action plan for the G7 to quickly and fairly distribute vaccine doses.
UK Prime Minister Boris Johnson on June 5 called for leaders of the G7 to commit to vaccinating the world by the end of 2022 amid mounting pressure for the UK to take the lead in sharing vaccine doses. Leaders of the International Monetary Fund, WHO, World Bank, and World Trade Organization are calling on the G7 to prevent a “two-track pandemic,” with richer countries having access to vaccines and poorer ones being left behind. The leaders endorsed an IMF proposal published in May that supports the ongoing work of WHO, its partners in the Access to COVID-19 Tools Accelerator initiative, and its global vaccine access programme COVAX, and includes a goal to vaccinate at least 40 percent of the population in all countries by the end of 2021 and at least 60 percent by the first half of 2022. On June 2, the COVAX initiative received nearly US$2.4 billion in pledges during a virtual summit hosted by Japan, which pledged US$800 million. The initiative has raised a total of US$9.6 billion, with a goal of providing 1.8 billion vaccine doses to lower-income countries and economies in 2021 and early 2022. So far, COVAX has shipped more than 81 million COVID-19 vaccines to 129 participants.
WHO VALIDATES SINOVAC VACCINE On June 1, the WHO validated the Sinovac-CoronaVac SARS-CoV-2 vaccine for emergency use. The vaccine, produced by the Beijing-based pharmaceutical company Sinovac, is an inactivated vaccine that has storage requirements that make it suitable for low-resource settings. As such, the WHO recommends the vaccine for use in adults aged 18 and older, as a 2-dose regimen spaced 2-4 weeks apart. WHO noted that vaccine efficacy data show the vaccine prevented symptomatic disease in 51% of those vaccinated and prevented severe disease and hospitalization among 100% of those studied.
On June 4, China granted emergency authorization for the Sinovac-CoronaVac vaccine’s use for children and adolescents ages 3 to 17. Sinovac also announced results (unpublished) from a Phase 2 study showing a third booster shot of the vaccine resulted in up to a 20-fold increase in antibody production after 2 weeks. However, the company cautioned that more research needs to be completed to determine the timing and dose of a third shot.
VACCINE MIX & MATCH Canada’s National Advisory Committee on Immunization is allowing patients to choose a different shot for their second dose following an initial AstraZeneca-Oxford dose. Some studies suggest this mixing of doses may provide additional protection against emerging variants by triggering a stronger immune response. In one small study published by medRxiv (preprint), German researchers examined reactogenicity, antibody response, and T-cell reactivity among 26 people ages 25-46 who received the AstraZeneca-Oxford vaccine followed by the Pfizer-BioNTech vaccine 8 weeks later. The researchers concluded the heterologous vaccination regimen was at least as protective as a 2-dose regimen of the same vaccine, but they cautioned more research is needed. Another clinical trial involving 673 people in Spain showed similar results. If data continue to support safe and effective mixing of vaccines, the strategy could provide countries with solutions to some supply challenges.
VARIANTS OF CONCERN In the UK, evidence is growing that the delta variant of SARS-CoV-2 (B.1.617.2, VOC21APR-02) first identified in India is more transmissible and more capable of immune escape when compared with the previously dominant Alpha variant (B.1.1.7), even in vaccinated individuals. The delta variant is now dominant in the UK, with the number of new cases recorded daily rising slowly. According to a report from Public Health England, there is some suspicion that the delta variant may be associated with an increased risk of hospitalization. UK health officials are evaluating data on the delta variant to determine whether the country will lift lockdown restrictions by June 21 as planned.
Last week, researchers reported in The Lancet that the Pfizer-BioNTech SARS-CoV-2 vaccine elicited a weaker antibody response to the delta variant than to the original wildtype virus, especially among older populations. The data raise the likelihood of a booster shot being needed for some people, although the scientists cautioned that more data are needed to know whether the vaccine would be any less effective at preventing severe disease, hospitalization, or death.
US CONTACT TRACING A recent study published in JAMA details the contact tracing efforts of 14 local health departments between June 2020 and October 2020. Contact tracers had difficulty reaching individuals with laboratory-confirmed COVID-19, and many that were reached by phone did not report any contacts. Researchers estimate that approximately 66% of recent contacts were not identified through contact tracing efforts. With this many contacts unidentified, researchers conclude that contact tracing efforts at these locations were minimally helpful in controlling community transmission of SARS-CoV-2. However, contacts that were named by individuals with confirmed disease were able to be reached at much higher rates; approximately 71% of named contacts were successfully reached by health departments. High levels of transmission, antiquated contact tracing systems, low numbers of available contact tracers, and public unfamiliarity or lack of trust in the contact tracing process all contributed to low success rates of contact identification. Uptake of digital contact tracing tools allowed public health staff to focus their efforts on targeted outreach and alleviated some of the burden.
ADOLESCENT HOSPITALIZATIONS US CDC Director Dr. Rochelle Walensky on June 4 urged parents to vaccinate their eligible children against SARS-CoV-2 and follow prevention measures for the disease, citing new data from a CDC study showing increased hospitalization rates in spring 2021 for adolescents with COVID-19. Researchers used data from the Coronavirus Disease 2019-Associated Hospitalization Surveillance Network to examine demographic and clinical characteristics and hospitalization rates of adolescents aged 12-17 years who were admitted to hospitals between March 1, 2020 and April 24, 2021. Among 204 adolescents who were likely hospitalized primarily for COVID-19 during January 1-March 31, 2021, 31.4% were admitted to an intensive care unit, and 4.9% required invasive mechanical ventilation. There were no COVID-19-associated deaths. Of the 204 adolescents, 52% were female, 31% were Latino, and 36% were Black. About 70% of the 204 adolescents had at least one underlying medical condition, with the most common being obesity. But nearly 30% had no underlying condition, reinforcing that even healthy adolescents are at risk of severe COVID-19-related disease.
Between March 1, 2020 and April 24, 2021, weekly adolescent hospitalization rates peaked at 2.1 per 100,000 in early January 2021, declined to 0.6 in mid-March 2021, and then rose to 1.3 in April 2021. The cumulative COVID-19 hospitalization rates for the adolescents from October 1, 2020, through April 24, 2021, were 2.5 to 3 times higher than recent seasonal influenza-associated hospitalization rates. Notably, some experts raised concern over the researchers’ use of data only through April 24, despite the availability of data through the end of May, which show another decrease in the 3-week average, down to 0.9 per 100,000.
The FDA’s Center for Biologics Evaluation and Research on June 10 will convene a virtual meeting of the Vaccines and Related Biological Products Advisory Committee to discuss the data needed to support an Emergency Use Authorization and Biologics License Application for SARS-CoV-2 vaccines intended for use in children younger than 12 years old. The committee will not discuss individual products during this meeting.
GLOBAL SUPPLY CHAIN Before COVID-19, global businesses had evolved to run efficiently with minimal stockpiling of necessary materials, instead leveraging their smaller overhead to produce a wider array of products. Relying on Just In Time manufacturing, parts and materials are delivered to manufacturers as they are needed rather than being stored in large quantities. While this practice has boosted global industry, the practice could not be adapted rapidly enough to handle the demands put on the supply chain by the COVID-19 pandemic. Everything from obtaining raw materials to delivering products to the end user came under acute stress as manufacturers struggled to keep up with changing pressures.
A recent policy paper from the Center for Global Development analyzes global supply trends in 2020 and highlights key lessons. Among these is the interplay between political and market powers to influence global supply and movement of goods. While market forces have a large influence on product movement, political powers played a significant role during the pandemic to procure medicines and other medical supplies. Policy recommendations from the paper include increasing redundancy in the global supply chain and localizing production of critical materials for medicines. Although the worst of supply shortages appears to have mostly resolved, the cascading supply chain effects could have a lasting impact. Certainly, the world has witnessed supply chain fragility in the face of a global crisis, and realized more work must be done to better secure its resources.
I would add that Ryan Gosling giggling gif but that would be overkill no?
by ponchi101 If it weren't because we need to be informed, I would delete that post. The level of insanity is beyond description.
by ti-amie
ponchi101 wrote: ↑Wed Jun 09, 2021 7:53 pm
If it weren't because we need to be informed, I would delete that post. The level of insanity is beyond description.
It's been around since yesterday and I wasn't going to post it for the same reason ponchi. When I saw that the second person is supposed to be a nurse I changed my mind. The only thing worse is Gohmert asking if moving the earth and the moon would fix climate change.
by JazzNU For the first time this week, I walked into 2 places (grocery store and Panera) and some of the people weren't wearing masks. That's allowed by those companies and the state if you're vaccinated. But it was a bit of a shock to just see full faces of people outside of a restaurant. Nothing changed in the last week in terms of mandates or allowances, so I didn't get the memo that this was the week when we'd start doing that.
Also, bit of a surprise at who wasn't wearing a mask - all of them were senior citizens.
Is everyone else having the same experiences? And I guess I'm really asking those who live in areas where everywhere they went people wore masks.
by Deuce The important question is: Was anyone checking for documented confirmation that people are fully vaccinated before allowing them to come in without a mask?
And, if so, how strict/accurate was that screening process?
Like proof that you are the person that the vaccine 'certificate' refers to, for example...
If all those elements were not in place, then it's no different than not checking anyone or anything at all.
.
by ponchi101 Reporting from Georgia: I would say 1/3 of people at the supermarket are not wearing masks. Nobody checks at the entrance.
by Deuce Wow.
So it's basically a free-for-all in many parts of the U.S., then?
Pandemic - what's a pandemic?
This is not just very sad... but also very dangerous.
And incredibly stupid.
by ponchi101 The numbers, for all categories (new infections, positivity, deaths) keep falling in the country. People can see that.
It is obvious that vaccination is the way to go; in that, we all agree. The disagreement may be how long to carry on the other measures.
Being 1/2 vaccinated, I am still wearing my mask, which I plan to do for, at a minimum, 6 months. That's me.
by Jeff from TX
Deuce wrote: ↑Thu Jun 10, 2021 12:08 am
Wow.
So it's basically a free-for-all in many parts of the U.S., then?
Pandemic - what's a pandemic?
This is not just very sad... but also very dangerous.
And incredibly stupid.
Unfortunately, much of the United States is, apparently, incredibly stupid. Hate to say it, but there it is.
by Togtdyalttai I'm not going to argue that no one should be wearing a mask in a grocery store in Georgia, where just over 40% have gotten even one vaccine dose. I'm also not going to say that the two are equivalent: surely not wearing a mask when you should is orders of magnitude worse. But this does go the other way too. I don't understand why so many people still wear masks when they're walking alone outside here. As of a week ago, 81.7% of people in my zip code had at least one dose.
by Deuce It's one thing to say that FULLY vaccinated people don't have to wear a mask in public indoor places (stores, etc.). Personally, I will continue to wear a mask after I get my 2nd dose... but if some FULLY vaccinated people don't wear a mask, it's not a huge issue to me.
Where it goes completely wrong, however, is to have this policy of FULLY vaccinated people not having to wear a mask, and then NOT VERIFYING if people are FULLY vaccinated or not. This is downright insane.
It's like saying that only people who've purchased tickets to Centre Court may enter to watch the match - and having NO-ONE there to verify that people have tickets.
Actually, it's significantly worse than that, because of the very real health risks involved.
As for people walking alone outside wearing a mask... yes, I've seen that here, too. Doesn't make much sense, and it's hard to understand. The only thing I've come up with is that they are coming from or going to more than one store, and are just too lazy to make the huge effort of putting the mask on and/or taking it off... So they just put it on and take it off once.
Yesterday, I saw a young woman of about 20 years old sitting completely alone on a bench (outside) waiting for a bus on a hot, sunny day. She had a mask on. You still must wear a mask on public transport (and in all stores) here - so she was ready to get on the bus. But I saw her sitting there for at least 15 minutes - alone, outside, and masked.
by Suliso Some people maybe have psychological scars and are afraid still. I don't wear a mask outdoors as I think it makes no sense, but if someone wants to it doesn't bother me.
by MJ2004 Now that I'm vaccinated I've stopped wearing a mask outside but I'm still more comfortable wearing it indoors.
That's in contrast with our state requirements - they've basically opened up almost everything indoors to be mask-free (excluding public transportation). Businesses can still require them on their own, but most aren't.
We have a high vaccination rate and cases are running extremely low in MA (dropped to 100 per day) so I guess that's why most people feel comfortable no longer wearing masks. I'd feel more comfortable waiting until we have no deaths per day (still about 5-10 per day).
by mmmm8
JazzNU wrote: ↑Wed Jun 09, 2021 9:08 pm
For the first time this week, I walked into 2 places (grocery store and Panera) and some of the people weren't wearing masks. That's allowed by those companies and the state if you're vaccinated. But it was a bit of a shock to just see full faces of people outside of a restaurant. Nothing changed in the last week in terms of mandates or allowances, so I didn't get the memo that this was the week when we'd start doing that.
Also, bit of a surprise at who wasn't wearing a mask - all of them were senior citizens.
Is everyone else having the same experiences? And I guess I'm really asking those who live in areas where everywhere they went people wore masks.
Businesses here (including in my workplace) have made it optional if you are vaccinated (honor system).
Yesterday, I took off my mask at the gym and it felt very weird (became optional too).
I've definitely seen unmasked people walk into businesses this week even if the mask sign is still up for everyone.
by mmmm8 BTW, the other day, there was some sort of group of 20-25 high schoolers on a trip going into Starbucks(100% not local to New York City, you can tell by... the lack of diversity). None were wearing masks. They were definitely under 16 and since most states have allowed 12+ vaccinations only recently, very doubtful they were vaccinated...
by JazzNU
Togtdyalttai wrote: ↑Thu Jun 10, 2021 4:13 am
I'm not going to argue that no one should be wearing a mask in a grocery store in Georgia, where just over 40% have gotten even one vaccine dose. I'm also not going to say that the two are equivalent: surely not wearing a mask when you should is orders of magnitude worse. But this does go the other way too. I don't understand why so many people still wear masks when they're walking alone outside here. As of a week ago, 81.7% of people in my zip code had at least one dose.
That's very interesting. Outside mask wearing has dropped to very low levels here. Probably 1 in 20 I'll see outside might wear one, but that's about it and certainly not when they are alone. Surprised to hear you're still seeing that so often.
Though I should add the caveat that my county is among the highest vaccinated in the state and cases have dropped significantly, less than 2% positivity rate, and averaging less than 20 cases a day in a county of 830k. Personally, I've been waiting for the increased vaccination rates plus the significant drop in positivity rate to even consider ditching the mask, so I'm very happy the time has arrived.
That being said, I'm pretty uncomfortable with the idea of not wearing a mask in an establishment where the employees (most not making a ton of money) are still wearing masks and I have yet to see that happen, so until it seems like that's a personal choice for them, I'm likely to keep wearing one for the time being as I don't want them feeling uncomfortable where they work. I'd be more than willing to keep wearing a mask while shopping if the employees were allowed to ditch the masks. Me wearing it for 30 minutes versus them wearing one for 8 hours is just not remotely comparable.
by Suliso Yahooo! Finally got my vaccine appointment, for this Sunday afternoon.
Where as before we saw exponential growth currently in Switzerland exponential decay. It's still a bit more than in US (two week incidence 84 per 100k), but nothing like it used to be and positivity rate is low (2.3%). We start returning to office a bit more from next week.
by ponchi101 Apparently we were a bit too pessimistic about our vaccinations. Colombia is also progressing so, again, my trip to the USA made it the most expensive vaccines in the world. You are getting it soon. If the manufacturers can keep up the pace or even increase production, the rest of the world may start catching up with the USA/EU.
After 18 months of terrible news, a bit of optimism may be due. It looks as if this virus can be defeated. Now, set up the proper virus detection systems to avoid another pandemic, which is simply waiting out there. Whatever the cost, it will be drops in a barrel compared to what this pandemic has cost the world.
by ti-amie
by dmforever
Togtdyalttai wrote: ↑Thu Jun 10, 2021 4:13 am
I'm not going to argue that no one should be wearing a mask in a grocery store in Georgia, where just over 40% have gotten even one vaccine dose. I'm also not going to say that the two are equivalent: surely not wearing a mask when you should is orders of magnitude worse. But this does go the other way too. I don't understand why so many people still wear masks when they're walking alone outside here. As of a week ago, 81.7% of people in my zip code had at least one dose.
Just to offer another perspective, I got my second vaccination months ago, but I still wear a mask when I go out for the following reasons:
1. It makes other people feel more comfortable with me. They don't have to worry if I'm an anti vaxxer or not.
2. It doesn't really bother me that much, so why not?
3. There is still a very small chance that I could still get sick.
In SF most people are masked when you go out, and even in restaurants they ask you to wear a mask inside when you aren't eating.
Kevin
by Deuce Right now, I would caution very, very strongly against optimism in 'defeating' this virus to any degree...
During the 1st wave, many people were saying that if there is a 2nd wave, it would not be as bad as the first. The 2nd wave was worse than the first.
During the 2nd wave, many people were saying that if there is a 3rd wave, it would not be as bad as the 2nd. The 3rd wave was worse than the 2nd, largely due to the variants.
Now many people are saying (and behaving as if) we have control over this virus. I don't believe that for a second.
Apart from the virus being able to mutate in unpredictable ways - with some of the mutations being more transmissible and even more dangerous -, feeling that we've won the battle now also results in many people completely letting their guard down and living life as they lived it before this virus existed - as is being seen in many parts of the U.S. now.
It's WAY, WAY too early to think that way.
While I'm seeing thousands of maskless fans crammed together into indoor NHL hockey games in the U.S., I'm seeing far more empty seats than full ones at the OUTDOOR Roland Garros venue - and the relatively few occupied seats are mostly apart from each other, and contain fans wearing masks.
France is doing it right. The U.S. is not.
by Suliso Difference is that we all are vaccinated now. That's a big deal.
by Deuce My point is that this virus is unpredictable. And part of that unpredictability is that it may be able to evade the current vaccine protections (as is currently being hypothesized about the Delta variant).
It's far, far too early in the game to believe that we've won this battle.
by Suliso One could believe or not, but soon time to relax most rules. I think in Switzerland there will be no more restrictions by August. Except probably masks in public transport.
by Deuce I think that is setting up for a rude awakening.
New variants which evade current vaccine protection could pop up at any time.
Particularly in parts of the world that have a cold winter, where people congregate inside much more, it would be much wiser to be safe than to be sorry. That goes for government restrictions as well as individual precautions.
by Suliso
Deuce wrote: ↑Thu Jun 10, 2021 7:59 pm
I think that is setting up for a rude awakening.
New variants which evade current vaccine protection could pop up at any time.
Particularly in parts of the world that have a cold winter, where people congregate inside much more, it would be much wiser to be safe than to be sorry. That goes for government restrictions as well as individual precautions.
And your advice would be? These restrictions are not sustainable forever. Even Swiss government will eventually run out of money supporting people who can't work.
by Deuce My advice would be to be much more cautious than the U.S. is being right now.
Wearing masks, avoiding close contact with others, working from home whenever possible, etc.
If it's a choice between the protecting the economy and protecting people from severe illness and death due to the virus, I'll choose saving lives.
The human tendency is to be arrogant with these things. As in 'Oh, we've got this virus under control'. Such arrogance has a price.s
People are pretending that the virus is under control so that they can do unimportant, trivial things like go to movies and hockey games and have parties. People are very spoiled today. This virus should be a wake-up call to all of us, and remind us of what is truly important in life.
by ti-amie The Delta variant is worrying. I wear my mask outdoors and if not at home indoors as well.
by Suliso For me and you it's just a party, for lots of others it's a job which feeds their family...
by JazzNU
Suliso wrote: ↑Thu Jun 10, 2021 7:55 pm
One could believe or not, but soon time to relax most rules. I think in Switzerland there will be no more restrictions by August. Except probably masks in public transport.
That's mostly what's going on in many places here. Public transport, schools, and medical offices and hospitals are the main places that will likely continue to require masks. But we've had many states of varying vaccination levels loosen restrictions in the last two or so months and have seen consistent sharp decline in cases, hospitalizations, and deaths almost everywhere despite people socializing in person more and more often. There's plenty of reason for optimism of how much difference the vaccine makes even when we aren't at traditional herd immunity levels. In most respects, it's the best case scenario we were all hoping for.
by Deuce
Suliso wrote: ↑Thu Jun 10, 2021 8:17 pm
For me and you it's just a party, for lots of others it's a job which feeds their family...
... and ends up killing people.
Not justifiable in my eyes.
In the U.S., people are behaving like if they stand up to the virus and/or ignore it, the virus will back down and admit defeat. They are treating the virus as if it’s a bully, and can be defeated in the same manner.
Not so.
by Suliso I should have my vaccine certificate valid by August 1st. Looking forward to a vacation somewhere, just need to think where exactly.
by ponchi101 I said "a bit of optimism". We all are in agreement that this is not over.
We all agree that proper measures should still be in place.
But we also talked about this last year. What would happen if a vaccine would never be developed? Locked in forever?
One consequence from the vaccine, at least for me. Colombia's turmoil is directly related to the economy. So, the vaccine will be an indirect reason why Colombia will veer to the left in 2022.
We said it too. Staying locked in also carried consequences.
by dryrunguy I had a Teams meeting with a few colleagues today at 3 p.m. The most important person needed in the meeting (she's leading the proposal) showed up 5 minutes late--and didn't quite seem like her usual self. Halfway through our discussion, she burst into tears.
It turned out she had just received word that her cousin (from the American Indian side of her family) had just died from COVID. She has lost several family members from that side of the family to COVID.
I told her this meeting could wait. But she wanted to continue because she felt like she "needed the distraction"...
So, yeah... It's not behind us yet.
by Suliso This is what happens when you trust Chinese vaccines not approved anywhere in the West... Somehow this stupid BBC article fails to mention that!
Covid-19 pandemic: Chile capital locks down despite mass vaccination
Chile has announced a lockdown in the capital Santiago amid rising Covid cases, despite nearly 60% of the country being fully vaccinated.
More than eight million residents living in and around the capital now must stay at home from Saturday.
On Thursday, Chile reported 7,716 new daily cases, with the vast majority of infections being among those who had not been fully vaccinated.
Intensive care beds are nearing full capacity, health officials warn.
Jose Luis Espinoza, the president of Chile's National Federation of Nursing Association, says his members are "on the verge of collapse", Reuters reports.
About 58% of the country's 17.5 million people have been fully vaccinated, and as many as 75% have received at least one vaccine dose.
But critics have accused the government of getting caught up in triumphalism over the vaccine rollout and of having loosened coronavirus restrictions too fast.
Chile's borders had been closed from March to November 2020. But after a strict lockdown had driven infections down, the decision was taken to reopen them.
Chileans were also given special holiday permits to travel more freely around the country during the southern hemisphere summer holidays.
Restaurants, shops, and holiday resorts were opened up to kickstart the faltering economy.
Chile has had nearly 1.5 million infections since the pandemic began, with more than 30,000 Covid-related deaths, according to America's Johns Hopkins university.
Suliso wrote: ↑Fri Jun 11, 2021 10:25 am
This is what happens when you trust Chinese vaccines not approved anywhere in the West... Somehow this stupid BBC article fails to mention that!
Covid-19 pandemic: Chile capital locks down despite mass vaccination
That is what scares me about Colombia. Although we are getting some Pfizer now, the bulk of the vaccination has been with Chinese vaccines. So, in reality the population is barely protected, and the group most at risk are the elderly that were vaccinated earlier with Sinovax and Sinopharm.
Then, yesterday my GF got a tweet about some Pfizer vaccines about to expire because the logistics could not get them into arms.
And people then wonder why I so totally dislike my countries. We are such a mess.
by Suliso I'm afraid most of those people will need to be revaccinated with better working vaccines. Not sure if there is any real difference between the two Chinese vaccines.
by JazzNU
Suliso wrote: ↑Fri Jun 11, 2021 10:25 am
This is what happens when you trust Chinese vaccines not approved anywhere in the West... Somehow this stupid BBC article fails to mention that!
Insane not to mention the Chinese vaccines. At the end of the article there's a related story on Chile vaccination success and in mid-April at least, 93% of the vaccines given in Chile were Sinovac (also called CoronaVac apparently). So, I'm definitely questioning why there is no mention in the article you posted.
by mmmm8 I'm curious if Argentina doing a little better (not by much) is related to using more of the Sputnik vaccine or some other factor.
Things are getting really bad in Russia again (and there is lots of anecdotal evidence from Russian doctors of the virus growing more resistant to treatment). But it's not because of the quality of the vaccines but because of very low rates of vaccination.
by Suliso Nobody truly knows how good are Russian vaccines either. Anecdotally better than Chinese, but only anecdotally...
by mmmm8
Suliso wrote: ↑Fri Jun 11, 2021 9:25 pm
Nobody truly knows how good are Russian vaccines either. Anecdotally better than Chinese, but only anecdotally...
That's why I'm curious about Argentina.
They've just started local production of it in Argentina as well, so presumably in a couple months we'll get even more data on it from outside Russia
by ti-amieFDA has decided at least 60 million doses of Johnson & Johnson’s coronavirus vaccine must be be discarded; 10 million can be released
The doses underwent a safety review after J&J shots were contaminated with AstraZeneca’s vaccine, prompting a plant shutdown
By
Laurie McGinley, Christopher Rowland and Isaac Stanley-Becker
June 11, 2021 at 3:45 p.m. EDT
The Food and Drug Administration has decided at least 60 million doses of Johnson & Johnson’s coronavirus vaccine made at the problem-plagued Emergent BioSolutions plant must be discarded, according to an individual familiar with the situation.
The agency, after an extensive safety review, also is releasing 10 million doses for use, according to the individual and a statement released by the agency on Friday. The statement said “several other batches are not suitable for use, but additional batches are still under review.”
The 60 million doses that must be discarded are in addition to the 15 million already thrown out that were contaminated by the AstraZeneca vaccine at the plant earlier this year, according to the knowledgeable person who spoke on the condition of anonymity because the individual was not authorized to discuss details. The person said the 60 million doses were made before and after the 15 million previously discarded and that the agency could not determine whether they were safe to use.
The decision about the 60 million doses being discarded was first reported by the New York Times.
The 10 million doses being released are expected to be sent overseas as part of President Biden’s effort to share vaccines with other nations. Millions of other doses that were made at the plant are still under review. The FDA has not yet authorized the facility to resume production of the single-shot Johnson & Johnson vaccine.
Peter Marks, director of the agency’s Center for Biologics Evaluation and Research, said in the statement, “These actions followed an extensive review of records, including the production history of the facility and the testing performed to evaluate the quality of the product. This review has been taking place while Emergent BioSolutions prepares to resume manufacturing operations with corrective actions to ensure compliance with the FDA’s current good manufacturing practice requirements.”
Europe’s drug regulator said Friday that batches of Johnson & Johnson’s coronavirus vaccine made for the region about the time when contamination issues were revealed at a U.S. manufacturing site would, as a precaution, not be used, according to Reuters.
South Africa’s Aspen Pharmacare, which was performing finish and fill of Johnson & Johnson vaccine, also was waiting for word on which of its doses would be cleared for use and which might have to be discarded, according to a local media report.
“This may pose another huge blow to African vaccine distribution,” said Zain Rizvi, law and policy researcher at the advocacy group Public Citizen.
The decision brings Johnson & Johnson closer to a resolution over a crisis that has frozen domestic production and distribution of its vaccine for months.
“Today’s decisions represent progress in our continued efforts to make a difference in this pandemic on a global scale, and we appreciate the close collaboration with the FDA and global health authorities,” Kathy Wengel, Johnson & Johnson’s executive vice president and chief global supply chain officer, said in a statement released by the company.
The company’s statement confirmed two batches of vaccine had been authorized for release. It did not address the question of the shots that were earmarked for disposal. Emergent also did not address the discarded doses. It said in a brief emailed statement it was pleased about the release of some doses but did not confirm the amount.
U.S. officials learned in April that up to 15 million doses of the Johnson & Johnson vaccine had been contaminated with the vaccine developed by Oxford and AstraZeneca, which was also being made at the facility. Federal authorities halted plant operations and directed Johnson & Johnson to assume a larger role in fixing the plant’s problems and managing it.
(...)
The panel also released an Emergent report saying a harmless virus from the AstraZeneca vaccine that is used to trigger immunity against the coronavirus was detected in a large batch of the Johnson & Johnson vaccine. The cross-contamination was detected by Johnson & Johnson on March 5 in a batch of vaccine manufactured between Jan. 19 and Feb. 21.
Emergent officials said the most likely route of contamination was during preparation of a growth medium for the Johnson & Johnson vaccine, which came into contact with the “waste path” from an area used to make the AstraZeneca vaccine.
During a hearing of the House subcommittee, Emergent officials were attacked for taking huge bonuses at the same time the factory failed to produce any vaccine that could be used in the United States or elsewhere.
Emergent’s CEO, Robert Kramer, told the House Oversight select subcommittee in testimony May 19 that Emergent has retained an independent quality oversight firm to monitor its performance. He said the company has performed cleaning, disinfection and repairs throughout the facility; improved waste-handling procedures; and boosted training for workers at the site.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 174.4 million cumulative cases and 3.8 million deaths worldwide as of 7:30am EDT on June 11.
Global Vaccination
The WHO reported 2.2 billion doses of SARS-CoV-2 vaccines administered globally as of June 11, and 874 million individuals have received at least 1 dose. Our World in Data reported 2.30 billion cumulative doses administered globally, an increase of 12% compared to this time last week. After a week-long decline, global daily doses administered rebounded slightly to 34.4 million doses per day, down from a record of 36.0 million doses per day on June 5. Our World in Data estimates there are 488 million people worldwide who are fully vaccinated, corresponding to approximately 6.3% of the global population, although reporting is less complete than for other data.
The recent decline in global average daily doses administered is driven largely by a sharp decline in Asia and, to a lesser degree, a steady decline in North America over the past several weeks. Asia’s recent decline is largely a result of the trend in China, where the average daily doses administered fell by more than 15% from June 5 to June 9 before rebounding slightly. After a steady 6-week decline from its April peak, India’s daily average began increasing again in late May. It appears that India could potentially surpass its previous peak if it continues on its current trajectory, but there is still a considerable gap to its current record. Similarly, the trend in North America is driven largely by the steady decline in the US, down by two-thirds compared to its peak on April 13. Longer-term increases in Canada, the Dominican Republic, Mexico, and other countries in the region are making up for some of the decline in the US.
With the exception of North America, all continents are reporting steadily increasing or accelerating trends in daily vaccinations. While Asia’s daily average decreased over the past week, it is still more than 5.5 times higher than it was in mid-March and double where it was in mid-May. Notably, Oceania is now reporting an average daily per capita vaccination rate that is nearly on par with North America and slightly below the global average. Daily vaccinations continue to increase slowly in Africa as well. As a whole, Africa remains well behind the other continents on a per capita basis, but it appears that its collective daily vaccination trend may be starting to accelerate. On a per capita basis, Europe is reporting the highest daily average, and its peak on June 7 was only 11% less than North America’s record high in mid-April.
At the national level, China is easily #1 globally in terms of total daily doses administered. Despite its decline over the past week, China’s 17.4 million doses per day is more than 5.5 times the average in #2 India (3.13 million). At #3, the US (1.14 million) is the only other country reporting more than 1 million doses per day. Among the top 10 countries, 4 countries are in Asia, 4 are in Europe, and 2 are in the Americas.
On a per capita basis, the Dominican Republic is #1 globally with 1.6 daily doses per 100 population, and Fiji is #2 with 1.4. Notably, China (1.2) is #3 globally, despite having the world’s largest population. In fact, China accounts for approximately 18.5% of the global population but more than half of the daily global vaccinations. South Korea also is in the top 10 for both total and per capita daily doses administered, and its daily average has increased by a factor of 7.5 since mid-May. Among the top 10 countries in terms of per capita daily doses administered, 5 are in Europe, 2 are in Asia, 2 are in the Americas, and Fiji represents Oceania. All countries in the top 10 are reporting more than 1 daily dose per 100 population, more than double the global average (0.44).
Among African countries, Morocco (189,216 doses per day) is reporting the highest total average, and Mauritius is reporting the highest per capita average (0.54 daily doses per 100 population). In Oceania, Australia is reporting the highest total daily doses administered, with 120,710 doses per day.
UNITED STATES
The US CDC reported 33.2 million cumulative cases and 596,059 deaths. After steady declines since mid-April, the United States’ daily incidence increased slightly on June 7-8. Notably, however, states have reported nearly 12,500 previously unreported cases over the past week—including more than 1,000 on June 3; more than 2,500 on June 8; and more than 7,500 on June 9—which is contributing to an artificially elevated average. Additionally, delayed reporting over the Memorial Day holiday weekend is likely contributing to elevated reports as states caught up. A similar effect can be observed in daily mortality. Daily mortality quickly climbed from a low of 321 deaths per day on June 4 to 366 on June 7—the first day that the Memorial Day holiday weekend moved outside the 7-day window—an increase of 14% over that period. We expect both daily incidence and mortality to continue decreasing once reporting fully returns to normal, but we will monitor these trends closely.
US Vaccination
The US has distributed 372.8 million doses of SARS-CoV-2 vaccines and administered 305.7 million. Similar to daily incidence and mortality, the average daily vaccine doses administered* increased slightly over the past several days, likely stemming from delayed reporting over the Memorial Day holiday weekend. The US is averaging 867,109 doses per day, and 535,221 people are achieving fully vaccinated status per day, down from a high of 1.8 million per day on April 12.
A total of 172 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 51.9% of the entire US population. Among adults, 64.0% have received at least 1 dose, and 7.3 million adolescents aged 12-17 years have received at least 1 dose. A total of 141.6 million people are fully vaccinated, which corresponds to 42.6% of the total population. Among adults, 53.4% are fully vaccinated, and 3.6 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 86.5% with at least 1 dose and 75.8% fully vaccinated. In terms of full vaccination, 73 million individuals have received the Pfizer-BioNTech vaccine, 57 million have received the Moderna vaccine, and 11 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
The Johns Hopkins Coronavirus Resource Center is reporting 33.4 million cumulative cases and 598,756 deaths in the US as of 10:30am EDT on June 11.
mRNA VACCINES & RISK REDUCTION US CDC researchers last week published a study in medRxiv (preprint) showing 2-dose mRNA vaccines, specifically those from Pfizer-BioNTech and Moderna, are highly effective among working-age adults in preventing SARS-CoV-2 infections when administered in real-world conditions. Additionally, the vaccines lessened viral load, febrile symptoms, and illness duration among those vaccinated participants who became ill with COVID-19. Initial findings from the study, called HEROES-RECOVER, were released in March, with the latest findings based on 3,975 healthcare personnel, first responders, and other essential and frontline workers who self-collected nasal swabs for 17 consecutive weeks from December 13, 2020 to April 10, 2021.
Once fully vaccinated, participants’ risk of SARS-CoV-2 infection was reduced by 91%, and the risk among those with partial vaccination was reduced by 81%. Only 16 of the 204 people who became infected had been vaccinated. Participants who were fully or partially vaccinated were more likely to have milder and shorter illness when compared with those who were unvaccinated, with some having asymptomatic infection. Those participants who were fully or partially vaccinated and experienced infections also had 40% less detectable viral load, were 66% less likely to test positive for the virus for more than 1 week, and experienced 6 fewer days of viral shedding when compared with those who were unvaccinated. The study adds to the growing body of real-world evidence that US FDA-authorized mRNA vaccines are effective at preventing SARS-CoV-2 infection, according to the CDC.
VARIANTS OF CONCERN & VACCINATION The emergence of the SARS-CoV-2 Delta variant (B.1.617.2) has prompted health officials worldwide to encourage people to become fully vaccinated to help lower the risk of infection and severe disease. The Delta variant appears to be more transmissible than the wild type virus and other SARS-CoV-2 variants, shows some ability to escape immune detection in individuals after vaccination or initial infection, and could cause more severe disease, although more research is needed to confirm the latter. In the UK, the Delta variant is associated with more than 60% of infections and is causing surges of COVID-19 in some parts of England. In the US, the variant is responsible for more than 6% of infections sequenced by researchers. At a White House briefing on June 8, White House Chief Medical Advisor Dr. Anthony Fauci noted the variant has been detected in 60 countries and, in the UK, is impacting younger populations aged 12- to 20-years-old. Dr. Fauci also discussed vaccine effectiveness against the Delta variant, saying 2 doses of the Pfizer-BioNTech and AstraZeneca-Oxford vaccines appear to be significantly more effective than 1 dose in preventing infection or severe disease caused by the variant, and urged everyone to be vaccinated.
In a study published in Nature on June 9 as an accelerated article preview, researchers reported the J&J-Janssen vaccine offers “strong protection against symptomatic” cases of COVID-19 caused by the wild type SARS-CoV-2 virus, as well as the Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Epsilon (B.1.427 and B.1.429) variants. The small study, which examined the immune responses of 20 volunteers between the ages of 18 and 55, found fewer neutralizing antibodies against the Beta and Gamma variants when compared to the original wild type virus. However, the non-neutralizing antibody and T-cell immune responses remained largely preserved in these individuals, making up for a lack of neutralizing antibodies when challenged by variants. These findings reiterate the importance of full vaccination in protecting against all known SARS-CoV-2 variants.
VACCINE PASSPORTS The use of vaccination “passports” continues to expand in Europe. This week, Germany unveiled CovPass, a digital vaccination card that individuals can save on their mobile phones. CovPass is compatible with the EU’s Digital COVID Certificate, which will document vaccination status, negative test results, or prior SARS-CoV-2 infection for individuals across the European bloc starting July 1, 2021. Jens Spahn, Germany’s Federal Minister of Health, indicated that CovPass is expected to be fully implemented by the end of June, which would support international travel during Europe’s summer tourism season. In addition to travel, the digital vaccination documentation can be used at businesses, museums, and other venues that require vaccination. Individuals can upload their vaccination status into the CovPass smartphone application by scanning a QR code provided after vaccination, and the app can then display the QR code wherever it is required. Vaccinated individuals will still be able to use the printed vaccination certificate, if they elect or are unable to use the digital version.
As vaccination coverage increases, many countries are allowing travelers to provide documentation of full vaccination status instead of negative SARS-CoV-2 test results upon arrival. The International Air Transport Association (IATA) already has documented instances of counterfeit vaccination documents in multiple countries, but it appears that the responsibility for verifying these documents is largely falling on airlines. Reportedly, airlines are calling for increased use of digital documentation, which is more difficult to counterfeit than paper copies, and it reduces the burden on airline personnel, who do not necessarily have the expertise necessary to identify fraudulent documentation.
US TRAVEL ADVISORIES On June 8, the US updated its COVID-19 travel advisories for several dozen countries. Notably, the Department of State lowered 58 countries from Level 4 (Do Not Travel) to Level 3 (Reconsider Travel) and lowered another 27 countries to either Level 1 (Exercise Normal Precautions) or Level 2 (Exercise Increased Caution). Additionally, the CDC issued updates for more than 120 countries and territories. The CDC’s Level 4 category (Very High COVID-19 Activity) fell from 140 countries and territories to 61, and the number of countries in the Level 1 category (Low COVID-19 Activity) jumped from 30 to 56. The changes reflect both a continuing decrease in COVID-19 burden in many countries around the world and growing evidence of the protection conferred by SARS-CoV-2 vaccines, in the US and elsewhere. The changes also aim to differentiate countries “with severe outbreak situations from countries with sustained, but controlled” transmission.
The CDC continues to recommend that individuals are fully vaccinated before traveling to other countries. Additionally, all unvaccinated individuals should avoid travel to Level 3 (High COVID-19 Activity) countries, and unvaccinated individuals who are at elevated risk for severe COVID-19 disease should avoid nonessential travel to Level 2 (Moderate COVID-19 Activity) countries.
VACCINE DONATIONS TO TAIWAN Last week, Taiwan received a donation of 1.24 million doses of the AstraZeneca vaccine from Japan to aid in its vaccination campaign. Taiwan is facing challenges in acquiring vaccines, with Taiwan President Tsai Ing-wen repeatedly turning down offers from China after expressing concerns about the Chinese vaccines’ safety. Taiwan also has accused China of trying to block its vaccine purchases internationally. China regards Taiwan as part of its territory. On June 6, 3 US Senators stopped in Taiwan for a 3-hour visit, expressing bipartisan US support for the island and pledging the US government will donate 750,000 vaccine doses to reduce its severe vaccine shortage. Notably, the Senators’ visit could have implications of its own on US-China relations, as the delegation arrived in a US Air Force C-17 Globemaster III freighter, a primary strategic lift aircraft for the military. Some speculated that the optics of a military aircraft capable of transporting troops and tactical cargo on a Taiwanese runway could rouse a response from Chinese officials.
Approximately 3.25% of Taiwan’s 23.5 million people have received at least one dose of vaccine. Through COVAX, Taiwan has signed contracts for 4.76 million doses as well as 10 million doses of the AstraZeneca vaccine, and 5.05 million of the Moderna vaccine. Delivery delays are expected for the AstraZeneca vaccine produced in Thailand over distribution concerns in Southeast Asia. Taiwan also is pursuing development of its own vaccines; Medigen Vaccine Biologics said it will apply for Emergency Use Authorization locally following the release of phase 2 vaccine trial results and plans to apply to the European Medicines Agency (EMA) and other international health authorities to start large-scale phase 3 trials. Taiwan also is engaged in early stage discussions to produce vaccines for US companies. Additionally, Germany reportedly is assisting Taiwan in talks with Pfizer-BioNTech to supply the island with the company’s vaccine.
CHINA LOCKDOWN Officials in Guangzhou, the capital of the southern province of Guangdong, China, this week instituted strict lockdowns impacting more than 180,000 residents after a new SARS-CoV-2 outbreak, blamed on the Delta variant, was detected among people who ate at several restaurants in the city’s Liwan district. Officials said each infected person has passed the virus along to more people than in any other previous outbreak in the country. As of June 11, officials reported 2 imported COVID-19 cases and 9 indigenous cases in Guangdong, with nearly the city’s entire population of 18.7 million people undergoing testing earlier this week. China continues to rely on several core principles of prevention strategies, including tight lockdowns, widespread testing, limits on movement, and 2-week or longer government-supervised quarantines for people arriving from other countries. The strict travel restrictions are expected by many to remain in place through at least February, when Beijing will host the Winter Olympics.
Chinese leaders are urging people to get vaccinated, with an average of nearly 20 million people getting vaccinated daily. As of June 8, the nation has administered more than 794 million doses to its population of 1.4 billion, according to the government. The majority of the vaccinations are using 2 Chinese-produced vaccines, Sinovac’s Coronavac and the Sinopharm vaccine, both of which have received Emergency Use Listings (EUL) from the WHO. In clinical trials, the Sinovac vaccine showed it prevented symptomatic disease in 51% of those vaccinated and prevented severe COVID-19 and hospitalization in 100% of the studied population. The Sinopharm vaccine’s efficacy for preventing symptomatic and hospitalized disease was estimated to be 79% for all age groups combined. However, with the spread of the Delta variant in Guangzhou, some are raising questions about the effectiveness of China’s vaccines, as that variant has proven capable of vaccine escape in other countries.
VACCINES IN AFRICA WHO Director-General Dr. Tedros Adhanom Ghebreyesus said on June 7 he hopes that some SARS-CoV-2 vaccine manufacturing sites in Africa will be close to commencing production by the end of 2021. Senegal reportedly is among the potential sites, under an agreement with Belgian biotech group Univercells. Last month, the EU announced an investment of €1 billion (US$1.2 billion) for manufacturing and access to vaccines, medicines, and health technologies in Africa. The leading candidates for regional manufacturing hubs are Senegal, South Africa, Rwanda, Morocco, and Egypt. In South Africa, Aspen Pharmacare is already producing the J&J-Janssen vaccine locally, and the Biovac Institute is working with the French and German governments and pharmaceutical companies to establish production capacity of 30 million doses annually.
A report by The Wall Street Journal indicates that government officials in South Africa seized 2,400 doses of counterfeit SARS-CoV-2 vaccines. The problem of counterfeit vaccines is certainly not limited to African nations, but the limited supply available to most countries could drive increased demand, fueling a market for fraudulent products. Previously, fraudulent doses have been confiscated in Mexico, Poland, China, and other countries. Networks and markets for counterfeit medications already exist in many low- and middle-income countries (LMICs), which could facilitate the distribution of fake SARS-CoV-2 vaccines. In fact, the WHO estimates that 10% of all medical products in LMICs are “either substandard or falsified.” In response to an increased risk of counterfeit vaccines, Kenyan officials suspended the importation of SARS-CoV-2 vaccines by private companies in order to provide more control and oversight. To date, there are no known instances of fraudulent vaccines being administered at any government vaccination sites, and national governments are collaborating with Interpol to continue combating the threat.
INDIA VACCINATION POLICIES India’s federal government announced this week it would begin to play a larger role in the administration of SARS-CoV-2 vaccinations across the country. The change comes amid public backlash at the low rates of domestic vaccine administration, especially amid the country’s worst COVID-19 surge. As of June 10, more than 46 million people in India, or 3.4% of the population, are fully vaccinated. India has set an ambitious goal to vaccinate 900 million adults by the end of 2021 and provide cost structures that enable people from all economic backgrounds to receive a vaccine. The Indian government also reversed its original plan to have states and the private sector lead the charge to vaccinate those between the ages of 18 and 44, announcing the federal government will provide free vaccines to any adult starting later this month. Under the new directive, the federal government will send 75% of vaccines procured directly from manufacturers to states at no cost. The remaining 25% of vaccines will be available for sale to the private sector, which can resell the vaccines through private clinics or hospitals. This is a change from previous allocations, which sent 50% of vaccines to the federal government and the other 50% to states and the private sector. The hope is that the new policy, which will go into effect on June 21, will increase vaccine coverage across the country, aiding in the government’s response to the ongoing COVID-19 surge.
PEDIATRIC VACCINE CLINICAL TRIALS Pfizer announced this week it will expand its SARS-CoV-2 vaccine clinical trials to include children aged 5 to 11 years, with testing among younger age groups to begin in the coming weeks. The vaccine being used is the same as that authorized for use among adolescents and adults ages 12 and older, but it will be administered as lower doses based on age group. The phase 2/3 trial is expected to enroll as many as 4,500 participants across the US, Finland, Poland, and Spain. The company said it expects to have safety and immune response data for children aged 5-11 years in September, with data for children as young as 2 expected shortly after. Data for children aged 6 months to 2 years is expected to be available in October or November, according to company officials.
PEDIATRIC LONG COVID/PASC The risk factors, clinical presentation, and recovery timeline for post-acute sequelae of COVID-19 (PASC), colloquially referred to as “long COVID,” largely remain a mystery, even 1.5 years into the COVID-19 pandemic. Most of the attention remains on adult PASC patients, and relatively little data are available for children who experience longer-term effects of SARS-CoV-2 infection. Estimates for the prevalence of PASC among adults who recover from acute SARS-CoV-2 infection range from 1-in-10 to 1-in-3 patients, but a dearth of data on pediatric PASC patients makes it more difficult to estimate the burden in that population. Several small studies suggest that approximately 7-20% of pediatric SARS-CoV-2 infections could result in longer-term physical and mental health effects.
There remains considerable uncertainty regarding the risk factors for PASC in both adults and children, and the focus on adults—in terms of both testing and clinical care—and relatively milder COVID-19 disease among children during the pandemic could make it difficult to identify children who are at risk of PASC. Additionally, pediatric PASC patients tend to have more normal test results, including blood tests, EKGs, and imagery (eg, CT scan), despite experiencing PASC symptoms. It may also be more difficult for children to explain symptoms such as “brain fog” to parents, guardians, or clinicians, and the longer-term impacts of PASC on physical and mental development may not be fully evident for years later. Similar long-term effects have been documented in children who recover from other diseases, such as Lyme disease or mononucleosis, but it likely will take dedicated research efforts over many years to fully characterize PASC in pediatric patients.
ROUTINE CHILDHOOD IMMUNIZATIONS A study published today in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) examines the impact of the COVID-19 pandemic on the administration of certain routine childhood and adolescent vaccines. Researchers examined data from 10 US jurisdictions with robust vaccination reporting systems, comparing the number of vaccine doses administered between March-September 2020 with the same time period in both 2019 and 2018. The research team split the time frame into two distinct periods of March-May and June-September to account for areas implementing and then lifting stay-at-home orders. The researchers found that administration of routine pediatric and adolescent vaccines lagged significantly in the first time period (March-May) when compared to past years. Though the researchers noted a rebound in the second time period (June-September), it was not significant enough to make up for the lack of vaccine administration during the first period. The CDC expressed concern that this gap in vaccine coverage could lead to an increased risk of disease outbreaks in schools when many children return to in-person learning this fall, and the agency encouraged health care providers to consider providing missed vaccines at the same time as administering SARS-CoV-2 vaccines in an effort to catch up. The CDC previously advised a 2-week break between administering a SARS-CoV-2 vaccine and other vaccines but reversed that guidance late last month.
BAMLANIVIMAB Results from a phase 3 clinical trial published in JAMA found that the preventive administration of the monoclonal antibody (mAb) treatment bamlanivimab as a monotherapy reduced the incidence of SARS-CoV-2 infection among residents and staff at skilled nursing home facilities with at least 1 confirmed index case. The randomized, double-blind, single-dose trial enrolled residents and staff at 74 skilled nursing and assisted living facilities across 11 states with at least one confirmed COVID-19 case, for a total of 1,175 participants for the duration of the trial between August and November 2020. Within 7 days of a confirmed SARS-CoV-2 case at a facility, participants were screened for enrollment, tested for SARS-CoV-2 infection, and randomly assigned and dosed with 4,200 mg of intravenous bamlanivimab or placebo (saline) if eligible. Bamlanivimab significantly reduced the incidence of COVID-19 in the prevention population compared with placebo (8.5% vs 15.2%; odds ratio, 0.43 [95% CI, 0.28-0.68]; P < .001). Five (5) deaths attributed to COVID-19 occurred during the trial period, all of whom were in the placebo group. Notably, the US FDA in April 2021 rescinded its Emergency Use Authorization (EUA) for bamlanivimab as a monotherapy because of resistance of SARS-CoV-2 variants to the drug. However, the mAb treatment is still permitted to be used as a treatment in combination with another monoclonal antibody, etesevimab.
by ti-amie I was watching a baseball game between the Chicago Cubs and St Louis Cardinals. It was played in Chicago in front of a full house and there was not a mask in sight.
by JazzNU I think in another week or so, pretty sure wearing a mask around here will make it seem like I'm not vaccinated.
by ponchi101
dryrunguy wrote: ↑Fri Jun 11, 2021 10:34 pm
As vaccination coverage increases, many countries are allowing travelers to provide documentation of full vaccination status instead of negative SARS-CoV-2 test results upon arrival. The International Air Transport Association (IATA) already has documented instances of counterfeit vaccination documents in multiple countries, but it appears that the responsibility for verifying these documents is largely falling on airlines. Reportedly, airlines are calling for increased use of digital documentation, which is more difficult to counterfeit than paper copies, and it reduces the burden on airline personnel, who do not necessarily have the expertise necessary to identify fraudulent documentation.
Well, Deuce was right. There are enough douchebags in this planet to do something as idiotic as this.
dryrunguy wrote: ↑Fri Jun 11, 2021 10:34 pm
As vaccination coverage increases, many countries are allowing travelers to provide documentation of full vaccination status instead of negative SARS-CoV-2 test results upon arrival. The International Air Transport Association (IATA) already has documented instances of counterfeit vaccination documents in multiple countries, but it appears that the responsibility for verifying these documents is largely falling on airlines. Reportedly, airlines are calling for increased use of digital documentation, which is more difficult to counterfeit than paper copies, and it reduces the burden on airline personnel, who do not necessarily have the expertise necessary to identify fraudulent documentation.
Well, Deuce was right. There are enough douchebags in this planet to do something as idiotic as this.
That was NID my friend. They busted someone who worked in a hospital for stealing hundreds of blank cards.
dryrunguy wrote: ↑Fri Jun 11, 2021 10:34 pm
As vaccination coverage increases, many countries are allowing travelers to provide documentation of full vaccination status instead of negative SARS-CoV-2 test results upon arrival. The International Air Transport Association (IATA) already has documented instances of counterfeit vaccination documents in multiple countries, but it appears that the responsibility for verifying these documents is largely falling on airlines. Reportedly, airlines are calling for increased use of digital documentation, which is more difficult to counterfeit than paper copies, and it reduces the burden on airline personnel, who do not necessarily have the expertise necessary to identify fraudulent documentation.
Well, Deuce was right. There are enough douchebags in this planet to do something as idiotic as this.
Never underestimate the capacity of a large proportion of humans to do bad and self-serving things.
Uh... I mean...
by ti-amie
You simply can't fix ignorant. I say ignorant because she simply may not know what she is saying is garbage. When she said the Nuremberg trials were the beginning of the Holocaust you can only sa she is ignorant.
by Suliso Isn't this similar to the old Reductio ad Hitlerum? That is all mutual accusations and comparisons escalate until you get compared to Hitler and Nazis as stand in for pure evil.
by Drop-shot Russian ambassador in Buenos Aires flatly states that they want to build nuclear reactors in Argentina in return for the vaccines. Business as always on both ends. The people and science be damned.
by ponchi101 Russian nuclear reactors. Nothing wrong with that technology. Not. One. Bit.
---0---
2nd dose in the left arm. No signs of anything. Back home, I understood how my friend was able to get a Pfizer vaccine: I had forgotten he has three underlying conditions: diabetes, High Blood pressure, and two stones of extra weight. I would still be waiting and scheduled for late in the summer.
by ti-amie The anti vaxxers have been busy it seems...
COVID-19
·
This morning
Christian Eriksen was not vaccinated against COVID-19 before his cardiac arrest, says Inter Milan director
The Danish midfielder suffered a cardiac arrest while representing his country at EURO 2020. His condition is now stable, and representatives from his current club, Inter Milan, say that he had not contracted COVID-19 and was not vaccinated.
Photo via @FoxSportsBrasil
by ti-amie
by ti-amie
The Washington Post
@washingtonpost
The broader slowdown in vaccinations may be a sign that the U.S. cannot vaccinate its way to safety from new virus variants, said Neha Agarwal, associate director of diagnostics at PATH, a global health equity nonprofit. http://wapo.st/3gnWNsk
by JazzNU
ponchi101 wrote: ↑Mon Jun 14, 2021 3:40 pm
2nd dose in the left arm. No signs of anything. Back home, I understood how my friend was able to get a Pfizer vaccine: I had forgotten he has three underlying conditions: diabetes, High Blood pressure, and two stones of extra weight. I would still be waiting and scheduled for late in the summer.
That 3 weeks went by fast. Happy to hear you got your second shot. I think it's great you travelled to get the shot and didn't delay. The Delta variant is damn scary and I hope I'm wrong, but seems that by late summer, that might be the dominant or second dominant strain in many more countries than it is the case right now.
by Suliso By the way even the Delta variant is 3-4x less virulent than measles (most potent pathogenic virus known). So if we're particularly unlucky there is still a room for worse variants.
by JazzNU
by MJ2004 Re. Eriksen, because no athlete ever dropped from a heart condition pre-Covid.
by Suliso About Novavax: just sell it to other countries. It would be stupid for US to buy that one too and EU doesn't truly need it either. Latin America does.
by JazzNU Novavax Vaccine - Though we may have 3 vaccine options in the US, many have felt for months that Novavax was an important option that needed to be available in the US. Different technology than the others, and thought to be a good candidate for boosters and for those that can't take the other 3 because of pre-existing conditions. Easier to be made and scale up, so a good candidate for global distribution. Also, the anti-vaxxers and skeptics have appeared to be less resistant to this vaccine and it helps that it had less side effects. Meaning, this is potentially the vaccine that could get us to herd immunity levels in the US in addition to the rest. So, not sure why NYT and any other outlets would downplay this important announcement. Novavax took a really long time getting here, they were originally supposed to be here in the early Spring I think, their numbers were looking promising in the winter and it was thought their application was coming in a matter of weeks back then.
by JazzNU
Suliso wrote: ↑Mon Jun 14, 2021 8:11 pm
About Novavax: just sell it to other countries. It would be stupid for US to buy that one too and EU doesn't truly need it either. Latin America does.
Already purchased. They are similar to Moderna were the US helped to fund the vaccine's development, so more than a billion dollars has already been put into this.
by Suliso Now is the time to share with other countries in a major way. Otherwise who knows what kind of variants will arrive later on. As for antivaxxers I can't believe they won't come up with a reason not to use this one either.
by atlpam Meanwhile, a family member of mine who chose not to be vaccinated has come down with Covid.
by JazzNU The US is sharing in a major way.
Not all those not getting the vaccine yet are crazy anti-vaxxers FYI. Some are skeptical of the rushed vaccine. Some are unsure of the newer technology, and are much more open to a traditional vaccine. There's a lot of bad info about how the MRNA vaccine is going to alter your DNA. In addition to J&J's side effects being worrisome to many, they are just coming out of something that makes people justifiability skeptical of them as a company. Novavax doesn't have those hurdles, so that's why it is thought to be a good candidate that more will be willing to take.
No matter how it may seem given the attention paid to them, we don't have a decent percentage of people who would rather homeschool their kids than given them the vaccinations required by their school district to enroll them. That is a very, very small percentage. I don't think anyone is spending time on convincing that group to get vaccinated. It's the ones whose kids have their MMR, TB, tetanus, meningitis shots, etc already that public health officials are trying to communicate the vaccine safety to the most.
by JazzNU
atlpam wrote: ↑Mon Jun 14, 2021 9:05 pm
Meanwhile, a family member of mine who chose not to be vaccinated has come down with Covid.
So sorry to hear that. I hope they are doing okay.
by Suliso I don't think they are all crazy antivaxxers either. Judging from Latvia it's mostly people who don't give a *** and think they have a strong immunity and don't need no bloody vaccine. Some still believe that covid just a different kind of flue, some others would take if offered on a silver platter but can't be bothered to actually register. Real crazies are indeed not that many.
From company website: NVX-CoV2373 contains a full-length, prefusion spike protein made using Novavax’ recombinant nanoparticle technology and the company’s proprietary saponin-based Matrix-M™ adjuvant. The purified protein is encoded by the genetic sequence of the SARS-CoV-2 spike (S) protein and is produced in insect cells.
I wonder what kind of craziness true antivaxxers and demagogues will derive from this. They have more imagination than I do...
by ponchi101 Recombinant will be assumed to be combining DNA's with other things.
Nanoparticle technology = Bill Gates/Elon Musk micro-chips implanted to work with space based Chinese lasers.
And I am not one of them. You are right, they will derive something outlandish.
by ti-amie
atlpam wrote: ↑Mon Jun 14, 2021 9:05 pm
Meanwhile, a family member of mine who chose not to be vaccinated has come down with Covid.
Sorry to hear this Pam.
by ti-amie
by Deuce After a slow start to vaccination, this is mostly good stuff about Canada... but 2nd doses are lagging behind.
I, myself, received my 1st dose about a month ago, and am not eligible for my 2nd dose until the 2nd week of July. In addition to that, I got Moderna at a pharmacy, and no pharmacies are taking appointments right now here for 1st or 2nd doses because they don’t have any Moderna on hand. So I have to wait just to make an appointment for July. There should be some Moderna coming in by the beginning of next week, though...
by Suliso I got my first dose Sunday and are scheluded for the second a month later. Lots of vaccine around now and we're only 10% behind US numbers now and catching up rapidly.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 176 million cumulative cases and 3.8 million deaths worldwide as of 5:30am EDT on June 15. The WHO reported declining weekly global incidence and mortality for the sixth consecutive week. The weekly incidence last week decreased 12.6% from the previous week, and it is the lowest weekly total since mid-February. If the global trend continues on this trajectory, the weekly incidence next week will reach the lowest value since October 2020. Global weekly mortality fell nearly 2% from the previous week. Most of the continuing decline is a result of trends in the WHO’s Southeast Asia and Europe regions.
Global Vaccination
The WHO reported 2.2 billion doses of SARS-CoV-2 vaccines administered globally as of June 14, and 914 million individuals have received at least 1 dose. Our World in Data reported 2.42 billion cumulative doses administered globally, an increase of 10% compared to this time last week. The global daily doses administered has exhibited an overall decline since its peak on June 4, down from a high of 35.8 million doses per day to 32.6 million. Our World in Data estimates there are 733 million people worldwide who are fully vaccinated, corresponding to approximately 9.4% of the global population, although reporting is less complete than for other data. On June 10, China reported its cumulative number of fully vaccinated individuals for the first time*, 223 million, causing the global total to jump from 484 million on June 9 to 713 million on June 10 and the global coverage to jump from 6.2% to 9.2%
*June 10 is the only report from China currently included in the OWID database.
UNITED STATES
The US CDC reported 33.3 million cumulative COVID-19 cases and 597,343 deaths. The cumulative incidence in the US accounts for approximately 10% of the entire US population. After briefly leveling off following the Memorial Day holiday weekend, daily incidence is once again decreasing. The current average (12,223 new cases per day) is the lowest since March 26, 2020. Daily mortality is once again decreasing as well, after a brief bump following Memorial Day. At 331 deaths per day, the daily mortality is at its lowest point since March 28, 2020.
US Vaccination
The US has distributed 374 million doses of SARS-CoV-2 vaccines and administered 311 million. Similar to daily incidence and mortality, the average daily vaccine doses administered* is once again declining, as routine reporting resumes following the Memorial Day holiday. The US is averaging 978,023 doses per day, and 653,441 people are achieving fully vaccinated status per day.
A total of 174 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 52.5% of the entire US population. Among adults, 64.5% have received at least 1 dose, and 7.7 million adolescents aged 12-17 years have received at least 1 dose. A total of 145 million people are fully vaccinated, which corresponds to 43.7% of the total population. Among adults, 54.4% are fully vaccinated, and 4.1 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 86.8% with at least 1 dose and 76.4% fully vaccinated. In terms of full vaccination, 75 million individuals have received the Pfizer-BioNTech vaccine, 58 million have received the Moderna vaccine, and 11 million have received the J&J-Janssen vaccine.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
On May 25, we compared state-level vaccination coverage and observed notable differences between states as well as some regional trends. At that time, the states at the top of the list were reporting full vaccination coverage that was nearly double the coverage in states at the bottom. This week, we will update that analysis to see if the differences have increased or decreased over the past several weeks. On May 25, 3 states were reporting full vaccination coverage of 50% or greater, which has since increased to 11. Previously, 6 states reported 31% or lower; today, only 2 states are reporting less than 31% (and only 1 with less than 30%). The median value for full coverage increased from 39% (interquartile range [IQR]: ~34-44%) to 43%, with most states currently reporting between approximately 37-49%. The lower bound of the IQR increased 3 percentage points (pp), but the upper bound increased by 5pp, illustrating that the states with the highest coverage are increasing their advantage over the lower states.
Since May 25, the disparities in coverage at the state level have increased, with the top states now reporting more than double the partial and full coverage as the bottom states. Previously, full coverage ranged from 26.5% in Mississippi to 52.7% in Vermont—not quite double. Today, Vermont and Mississippi retain their respective ranks, but at 61.9%, Vermont is now reporting more than double Mississippi’s 28.1% coverage. Vermont’s full coverage increased by 9.2pp since May 25, while Mississippi’s only increased 1.6pp over that period. In terms of partial coverage, Vermont is again #1 nationally, with 72.4% of the population receiving at least 1 dose, and it is reporting more than double the 34.9% coverage in Mississippi.
States’ rankings for full vaccination coverage continue to largely align with their rankings for partial coverage. In fact, only 7 states have rankings that differ by more than 5 places between the 2 lists. Minnesota ranks 6 places higher in terms of full vaccination than partial, jumping from #20 to #14. The remaining 5 states rank lower for full vaccination. Hawai’i and Illinois both fall 9 places. Hawai’i drops from #3 to #12, and Illinois from #16 to #25. Pennsylvania and Utah both fall 8 places, #9 to #17 and #34 to #42, respectively. California falls 7 places, from #12 to #19, and Arizona falls 6 places, from #28 to #34.
In terms of full vaccination, the Northeast region continues to represent most of the states reporting the highest coverage, including all of the top 7 states and 8 of the top 10. Most states in the South region continue to report among the lowest coverage, representing the bottom 3 states as well as 9 of the bottom 12. Of the states in the South region, Maryland (#8; 52.0%), Virginia (#15; 48.4%), and Delaware (#20; 46.3%) are reporting the highest coverage, and interestingly, all 3 are located on or near the Northeast region border. The Midwest and West regions are spread more evenly throughout the rankings. The West has more variation—spanning #9 Washington (as well as #11-13) to #47 Wyoming (as well as #42-43). Conversely, Midwestern states are largely clumped in the middle—with all 12 states falling between #14 Minnesota and #38 Missouri.
As we have reported over the past several weeks, vaccination among adults aged 65 years and older has largely stalled at the national level, with the full coverage holding relatively steady at 76.4% and partial coverage at 86.8%. As with coverage among the entire population, we can observe marked differences at the state level in terms of coverage among older adults, although the magnitude of the differences are generally smaller, due in part to the overall higher coverage across all states. Full vaccination coverage among older adults ranges from Utah with 60.5% to Vermont with 92.7%. In total, 17 states are reporting greater than 80% coverage among older adults, and only 7 are reporting less than 70%. The median coverage is 77.6%, and most states fall between approximately 72-82%. In terms of the relative difference, Vermont is reporting 1.5 times the lowest coverage among older adults (ie, 92.7% compared to 60.5% in Utah), but it is reporting 2.2 times the lowest coverage among the entire population (61.9% compared to 28.1% in Mississippi).
The Johns Hopkins Coronavirus Resource Center is reporting 33.5 million cumulative cases and 599,950 deaths in the US as of 10:30am EDT on June 15.
NOVAVAX VACCINE Novavax on June 14 reported preliminary efficacy data for its investigational SARS-CoV-2 vaccine. Based on data from a phase 3 clinical trial involving nearly 30,000 participants, the vaccine’s overall efficacy is estimated to be greater than 90% in preventing moderate and severe COVID-19 disease. The vaccine also demonstrated 93% efficacy against variants of concern/interest (VOCs/VOIs) and 100% efficacy against non-VOC/VOI variants. This places the Novavax vaccine on par with currently authorized vaccines. Like most other SARS-CoV-2 vaccines, the Novavax vaccine is a 2-dose regimen, but it uses a much different platform. The Novavax vaccine uses nanoparticles composed of synthetic SARS-CoV-2 spike proteins to mimic the surface of a SARS-CoV-2 viral particle and stimulate an immune response. The press release did not present the full clinical trial data, but Novavax committed to publishing its full analysis via preprint servers and in a peer-reviewed manuscript.
Reportedly, Novavax may apply for an Emergency Use Authorization (EUA) from the US FDA in the third quarter of this year; however, with multiple existing EUAs for SARS-CoV-2 vaccines, the FDA may direct Novavax to instead apply for full licensure. Novavax is also evaluating options for international authorization, including in the UK, the EU, India, and South Korea. Novavax has partnered with international manufacturers, such as the Serum Institute in India and SK Biosciences in South Korea, and agreed to supply 1.1 billion doses to low-and middle-income countries. In an effort to close the gap in global vaccine access, Novavax expects to produce 100 million doses by the end of the third quarter 2021 and 150 million doses by the end of the year. The Novavax vaccine can be stored in standard refrigerators, reducing logistical challenges for distribution and administration, which could provide an advantage, particularly in low-resource settings. In conjunction with international vaccination efforts, researchers expect that Novavax shots, due to their unique formula, may be particularly useful as boosters in the future.
DELTA VARIANT As countries around the world continue to expand vaccination efforts, there is growing concern that the Delta variant of concern (B.1.617.2; VOC) could cause significant problems before many countries can achieve sufficient vaccination coverage. The Delta variant is the most recent VOC designated by the WHO and US CDC. Reportedly, the current COVID-19 surge in southeastern China is being driven by the Delta variant, and other countries are adapting COVID-19 restrictions in order to mitigate the risk from this VOC. Emerging evidence indicates that the Delta variant poses an elevated risk for severe disease compared to others, and it is believed that the variant is largely responsible for India’s largest surge, which peaked in early May. The Delta variant also represents an increasing proportion of COVID-19 cases in the US—up to 6%, compared to 1% only a month ago—and the UK at 91% of new cases. In response to increasing prevalence of the Delta variant, the UK is extending existing COVID-19 restrictions for another 4 weeks—shifting the expected date from June 21 to July 19—which will allow for accelerated vaccination efforts before taking further steps to ease restrictions.
Emerging data indicate that existing vaccines, including the Pfizer-BioNTech and AstraZeneca-Oxford vaccines, are effective in preventing severe disease and hospitalization. Analysis published by Public Health England, based on real-world cases, indicates that the vaccines are 96% and 92% effective in preventing hospitalization, respectively, which is on par with the protection conferred against the Alpha variant (B.1.1.7). Notably, however, several countries that are using vaccines developed in China have reported increased “breakthrough” infections, potentially stemming from increased circulation of the Delta variant, including Seychelles and Mongolia. Dr. Scott Gottlieb, former US FDA Commissioner, expects that full vaccination will provide high levels of protection against the Delta variant.
G7 SUMMIT COMMITMENTS Recognizing that the world’s interconnectedness means the “COVID-19 pandemic is not under control anywhere until the disease is under control everywhere,” G7 leaders agreed to a collective goal of ending the pandemic in 2022 at the end of its 3-day summit in England.
In the Carbis Bay Declaration, G7 leaders committed to sharing at least 870 million SARS-CoV-2 vaccine doses directly with low- and middle-income countries over the next year, aiming to deliver at least half by the end of 2021, primarily through the COVAX facility. The leaders also highlighted financial commitments made to the Access to Covid-19 Tools Accelerator (ACT-A) and COVAX since the beginning of the pandemic, which, when taken together with vaccine donations, equate to more than 2 billion vaccine doses. Prior to the summit, US President Joe Biden and British Prime Minister Boris Johnson announced donations of 500 million and 100 million vaccines, respectively. Canada is expected to pledge up to 100 million doses, and other G7 nations likely will follow suit.
Additionally, the declaration addresses access to and production of COVID-19-related tools by expressing support for voluntary licensing, technology transfers, tiered pricing, and not-for-profit global and regional production capabilities, with an emphasis on Africa, although it does not address patent waivers for such products. The leaders committed to continuing to strengthen the WHO by supporting its leadership role in the global health system; boosting SARS-CoV-2 global surveillance and genomic sequencing, pledging to sequence at least 10% of all new cases and sharing that information in existing databases; and urging the World Bank and other multilateral development banks to speed their financial support, especially to ACT-A and its partners, including the Global Fund and Unitaid.
The meeting of G7 leaders was anticipated to be a landmark summit with war-footing levels of commitment to end the COVID-19 pandemic, but many experts, NGOs, and health advocates expressed disappointment that the nations did not commit to a more detailed plan. WHO leadership and health campaigners welcomed the vaccine donations, but some called the summit an “historic missed opportunity” and a “failure,” criticizing leaders’ commitments, which fall far short of the at least 11 billion doses needed to vaccinate the world’s population. UN Secretary-General António Guterres called on G7 nations to do more than pledge vaccine doses, saying a global vaccination plan based in logic and delivered with a sense of urgency would better help vaccinate people in LMICs and prevent new and potentially more dangerous SARS-CoV-2 variants from developing.
MANDATORY VACCINATIONS A federal judge in Texas on June 12 dismissed a lawsuit brought by 117 employees of Houston Methodist Hospital challenging the hospital’s SARS-CoV-2 vaccine requirement. In a 5-page ruling, US District Judge Lynn Hughes upheld the vaccination mandate, underlining that the requirement broke no federal law and criticizing the plaintiff’s arguments as false, irrelevant, and reprehensible. Houston Methodist is among the first hospital systems in the country to mandate its employees receive a SARS-CoV-2 vaccine, and the decision marks an early test for how similar employer-mandated vaccine policies may fare in the courts. Notably, the US Equal Employment Opportunity Commission earlier this year issued guidance for employers wishing to require vaccines for on-site workers. Houston Methodist welcomed the judge’s decision, and a lawyer for the plaintiffs said the employees would appeal the ruling.
SARS-COV-2 ORIGINS With continued international attention on the origins of SARS-CoV-2, the G7 in its June 13 Carbis Bay Declaration called for the WHO to convene “a timely, transparent, expert-led, and science-based” Phase 2 COVID-19 Origins study, including investigations in China. While the scientific community continues to investigate the origins of SARS-CoV-2, conclusively determining the source of any new human virus remains elusive. Frequently, this line of scientific inquiry can point only to a group of possible viral ancestors, and pinpointing the exact virus requires an enormous database of samples, collection of which takes time, rigor, and some luck.
A group of researchers on June 9 published data on 411 bat samples collected from China’s Yunnan province between May 2019 and November 2020, identifying 24 full-length coronavirus genomes, including 4 novel viruses related to SARS-CoV-2. The researchers note the study highlights the significant diversity of bat coronaviruses at the local level, underscoring the difficulties in attempting to identify a single-source viral origin of the COVID-19 pandemic. The debate over whether SARS-CoV-2 escaped a Chinese laboratory or even originated in the country continues to fuel geopolitical discussion over China’s role in the pandemic, including its potential involvement in cover-ups, and could impact China’s global status over the long term, depending upon investigational findings. Researchers note that future pandemic preparedness hinges on scientists’ ability to conduct epidemiological surveillance and understand viral emergence through well-funded inquiry.
REBOUND OF RESPIRATORY VIRUSES Masking has been a vital component in the global public health response to the COVID-19 pandemic. However, as many US states achieve higher levels of vaccination, several state and local governments are relaxing mask measures, a consequence of which is a resurgence of common respiratory viruses. Cases of seasonal cold and respiratory syncytial virus (RSV) have made a comeback in states that have relaxed masking policies. Still, incidence of these seasonal respiratory viruses was markedly lower over the past year than in previous years, reinforcing the efficacy of masks in protecting against a broad spectrum of respiratory infections, not only SARS-CoV-2. For comparison, the CDC reported 1 pediatric death due to influenza in 2020 compared to 199 in 2019. Experts hope that some continuation of public health precautions will help keep these numbers lower than in previous years, especially as children return to in-person learning in the fall. Some parents are encouraging their children to continue wearing masks at school, even following SARS-CoV-2 vaccination, as a way to minimize colds among their families.
VACCINATION ADVERSE EVENTS A higher-than-expected number of people under age 30, especially young men, have experienced heart inflammation, also called myocarditis or pericarditis, following their second dose of SARS-CoV-2 mRNA vaccine, including the Pfizer-BioNTech and Moderna vaccines. According to data from the US CDC, 226 confirmed cases of heart inflammation among people 30 or younger were reported to the U.S. Vaccine Adverse Event Reporting System as of May 31, compared with an expected 10 to 102 cases for that age range based on background incidence among the US population. Of those cases, most occurred among men and most have recovered fully from their symptoms. The CDC said it is continuing to investigate the cases and has not concluded there is a causal relationship between the vaccines and cases of heart inflammation. The agency is scheduled to hold a meeting of its Advisory Committee on Immunization Practices on June 18 to evaluate myocarditis or pericarditis following mRNA vaccination and assess the benefit-risk balance.
J&J-JANSSEN VACCINE PRODUCTION J&J-Janssen’s 1-dose SARS-CoV-2 vaccine has hit another obstacle in its rollout and manufacturing efforts in the US. Federal regulators recently informed J&J that 60 million doses of its vaccine are unusable due to possible contamination during the manufacturing process. According to sources familiar with the situation, the US FDA is expected to allow the use of around 10 million doses, distributed with a warning that regulators cannot guarantee the vaccine was produced following good manufacturing practices. The doses were made at an Emergent Biosolutions facility in Baltimore, Maryland, which already has documented several manufacturing problems. Previously, regulators found that workers at the plant contaminated around 15 million doses of the J&J-Janssen vaccine with one of the components of the AstraZeneca-Oxford vaccine, which also is produced at the facility. Following this incident, Emergent Biosolutions was stripped of its authority to operate the plant, and J&J was placed in charge of manufacturing its own vaccine at the facility. The repercussions of these problems are ongoing, as the US plans to export millions of doses of the J&J-Janssen vaccine to bolster international vaccination administration. Canada recently rejected a shipment of 300,000 J&J-Janssen vaccine doses following a safety review. These doses had been held since April following the initial contamination event.
SARS-COV-2 ARRIVAL IN THE US Researchers from the All of Us initiative today published findings (Clinical Infectious Diseases) from a SARS-CoV-2 serological study conducted in early 2020. The study included more than 24,000 participants from across all 50 US states (part of existing All of Us research efforts), who provided specimens from January 2-March 18, 2020. The researchers identified 9 seropositive participants, including 7 who provided specimens prior to the first confirmed case in their state. The first 12 cases of COVID-19 in the US all had recent travel to China or had close contact with travelers, and the earliest reported symptom onset was January 14, 2020. The study provides further support for the idea that SARS-CoV-2 was circulating in the community prior to the first reported cases. Early testing strategies that restricted eligibility to individuals with recent travel history to high-risk areas (e.g., China)—as well as emphasis on early travel restrictions to prevent the introduction of COVID-19—likely hindered early disease surveillance and response activities in the US.
US SUPPLY CHAIN Although the COVID-19 pandemic remains far from over, some are calling on the US to evaluate structural vulnerabilities in the nation’s supply chain, particularly for medical supplies including personal protective equipment (PPE). In the early stages of the pandemic in the US, hospitals and other healthcare facilities were forced to ration vital PPE and bid for additional supplies at prices far above market value. Federal efforts to distribute PPE from the Strategic National Stockpile also were fraught with miscalculations, resulting in unequal and inequitable distribution. Writing in a STAT News opinion piece, U.S. Major General (retired) John Wharton, who most recently served as commanding general of the US Army Research, Development and Engineering Command at Aberdeen Proving Ground, proposes measures to help prevent similar disparities in future public health emergencies. First, the US federal government should create and fund a monitoring and dissemination network for PPE, medicines, and other medical supplies. Second, the US should increase domestic manufacturing of PPE and medical supplies to decrease reliance on overseas manufacturing capabilities. The ability to monitor, manufacture, and distribute PPE and other vital medical supplies when and where they are needed will better prepare the US against future stresses to its supply chain system.
by ponchi101 Got my second dose on Monday (I posted), and then flew home yesterday. A very tiring day, and last night I feel I got a side effect: I was really freezing (Bogota is cold but not that cold) and then I got a fever. Feel fine this morning and if that is the sole side effect, no issues. But kind of odd, I think.
---0---
Packed plane. Everybody wearing a mask, and the Colombian govt is requesting a PCR test, which I had. Plus, I was all giggly for them to ask for my vaccination card.
Nothing. They did not ask me for anything. Kind of sloppy, if my opinion is asked.
---0---
Wake up this morning, catching up with news. The Yahoo feed has one story: "Covid patients in the USA have one thing in common". I click the article, wondering what the condition is: Diabetes? Obesity? They are left handed? They eat at Burger King, not McDonalds? Nope. The one thing in common for covid patients is: they are not vaccinated.
Talk about a non-news.
by MJ2004
ponchi101 wrote: ↑Wed Jun 16, 2021 2:50 pmThey are left handed?
Hey now, I'm left-handed. No need to draw us into it.
I saw the click-bait article too and had the same reaction. Non-news.
by atlpam
ponchi101 wrote: ↑Wed Jun 16, 2021 2:50 pm
Got my second dose on Monday (I posted), and then flew home yesterday. A very tiring day, and last night I feel I got a side effect: I was really freezing (Bogota is cold but not that cold) and then I got a fever. Feel fine this morning and if that is the sole side effect, no issues. But kind of odd, I think.
---0---
Packed plane. Everybody wearing a mask, and the Colombian govt is requesting a PCR test, which I had. Plus, I was all giggly for them to ask for my vaccination card.
Nothing. They did not ask me for anything. Kind of sloppy, if my opinion is asked.
---0---
Wake up this morning, catching up with news. The Yahoo feed has one story: "Covid patients in the USA have one thing in common". I click the article, wondering what the condition is: Diabetes? Obesity? They are left handed? They eat at Burger King, not McDonalds? Nope. The one thing in common for covid patients is: they are not vaccinated.
Talk about a non-news.
That is a typical reaction to the second dose. Mine was similar - a low fever for a few hours a little over 24 hours after the second dose.
by ti-amie I was out and about today in my neighborhood. Almost everyone I saw with two exceptions was masked.
by ponchi101 Vaccinated and masked. Two years of that and this thing can be defeated.
But those other people...
by ti-amie
by ti-amie
by ponchi101 Here.
After the massive protests of last month, the expected wave of cases is upon us. Daily deaths are at about 600+, cases are at about 12,000.
Several not verified cases of people that were vaccinated and are in ICU's. Vaccinated with Chinese brands.
Government has opened vaccination to all that simply show up at the vaccination site. But the sites are at random. Rumor is it that the GOVT simply has decided that better vaccinate people this way than lose those precious but hard to keep properly refrigerated Pfizer vaccines.
by ti-amie
by ti-amie
by ti-amie
by JazzNU Even though the US did stick with the 2-dose approach because that's what the clinical trials supported. There were a decent number public health and doctors panicking earlier this year and pushing for a change to this approach, so we potentially could've been in the same tough spot.
This Delta variant may well get us to herd immunity. The more stories come out about the difference between one shot and two, the more likely those one dose people rush back in for their second even though it's a couple of months later than it was originally scheduled.
We're gonna get a boost in the next two months anyway because of students, especially college students getting them as required by their universities to return to campus. But thinking the boost will be higher than I thought. A decent number of schools were trying to punt and wait for full FDA approval to go through, and they may not be able to pretend that's soon enough anymore.
by Deuce The head coach of the Montreal Canadiens NHL hockey team has tested positive for COVID-19.
Some medical professionals are saying that it is conceivable that he could have contracted the virus during one of the two games played in Las Vegas, as, with 18,000 UNMASKED fans in the indoor arena, and no verification of negative testing or vaccinated status having been done among the fans upon entering the arena, the air inside the arena could have contained enough contaminated particles (aerosols) to infect someone.
The possibility of him having been contaminated during the games was raised because of the timing of the positive test, as well as that the team was restricted to the arena and the hotel while in Vegas.
Of course, it's unlikely that it can ever be determined exactly how he contracted the virus - but several medical professionals are saying that the above is a possible scenario.
This would seem to confirm, then, that parts of the U.S. are completely crazy in lifting essentially all protections and behaving as if the virus no longer exists.
by ti-amie
Deuce wrote: ↑Fri Jun 18, 2021 10:51 pm
The head coach of the Montreal Canadiens NHL hockey team has tested positive for COVID-19.
Some medical professionals are saying that it is conceivable that he could have contracted the virus during one of the two games played in Las Vegas, as, with 18,000 UNMASKED fans in the indoor arena, and no verification of negative testing or vaccinated status having been done among the fans upon entering the arena, the air inside the arena could have contained enough contaminated particles (aerosols) to infect someone.
The possibility of him having been contaminated during the games was raised because of the timing of the positive test, as well as that the team was restricted to the arena and the hotel while in Vegas.
Of course, it's unlikely that it can ever be determined exactly how he contracted the virus - but several medical professionals are saying that the above is a possible scenario.
This would seem to confirm, then, that parts of the U.S. are completely crazy in lifting essentially all protections and behaving as if the virus no longer exists.
...not
by Suliso Is it known whether the coach was fully vaccinated?
by ti-amie
Suliso wrote: ↑Fri Jun 18, 2021 11:55 pm
Is it known whether the coach was fully vaccinated?
He got the second shot but he hadn't made it to two weeks after to get out and about.
by Deuce
Suliso wrote: ↑Fri Jun 18, 2021 11:55 pm
Is it known whether the coach was fully vaccinated?
Yes - he was fully vaccinated... BUT he received his 2nd dose of the vaccine only 8 days ago, and it takes 14 to 21 days after vaccination for the vaccine to be fully effective.
I've not seen anywhere where it identifies which 'brand' of vaccine he received.
by Suliso My city is currently the best in Switzerland in vaccination against covid. As of Friday 32% of all population has been fully vaccinated and another 15% (including myself) have received the first dose. For comparison the worst region is 21+18% and Zurich, the most populous district, is 26+19%.
by ponchi101 Even though that is good news, serious question here: isn't Switzerland a pharmaceutical powerhouse? You should be able to produce enough vaccines to cover all your population (quick Google tells me Switzerland is a bit under 9MM). Or do we go back to the fact that the technology needed for this vaccine is very high?
by Suliso
ponchi101 wrote: ↑Sat Jun 19, 2021 2:03 pm
Even though that is good news, serious question here: isn't Switzerland a pharmaceutical powerhouse? You should be able to produce enough vaccines to cover all your population (quick Google tells me Switzerland is a bit under 9MM). Or do we go back to the fact that the technology needed for this vaccine is very high?
We'll cover all the population, it just takes some time. We don't have any home developed vaccines, but Moderna is mostly manufactured in Switzerland for the European market. Currently about 60% of doses used is this vaccine the rest being German manufactured Pfizer/BioNTech.
Local authorities are really going by the book here. Only the two most efficient vaccines used and the second dose comes exactly like prescribed (3 weeks for Pfizer, 4 for Moderna). I think in the longer run this will be better than all the experiments UK undertook. The vaccine has been available to all age groups for about six weeks now.
We'll cover all the population, it just takes some time. We don't have any home developed vaccines, but Moderna is mostly manufactured in Switzerland for the European market. Currently about 60% of doses used is this vaccine the rest being German manufactured Pfizer/BioNTech.
Local authorities are really going by the book here. Only the two most efficient vaccines used and the second dose comes exactly like prescribed (3 weeks for Pfizer, 4 for Moderna). I think in the longer run this will be better than all the experiments UK undertook. The vaccine has been available to all age groups for about six weeks now.
The Swiss going by the book? Get out of here!!!
by Togtdyalttai I went to a grocery store today for the first time since CA's restrictions loosened. The percentage of people wearing masks has declined noticeably, from nearly 100 to just above 50 by my estimation. Probably not a big deal because cases are at around 2/100,000/day and there's 84% with at least one shot, 67% fully vaccinated, but it was different to see.
by Suliso Below is the current vaccination situation in Switzerland by age groups. Dark green is two doses and light green only one.
by ponchi101 Meanwhile, at the other end of efficiency and proper management of this pandemic, Brasil has hit 500K deaths.
by Suliso
ponchi101 wrote: ↑Sun Jun 20, 2021 4:29 pm
Meanwhile, at the other end of efficiency and proper management of this pandemic, Brasil has hit 500K deaths.
Is that including estimation of all the unofficial deaths? I believe the "leader" is currently India with 2-2.5 million deaths.
by ponchi101 Well, we know that the real tallies are not accurate. The number I read was the official one, from the Brazilian government, so it could be anywhere from 1/2 the real number to even more distorted figures.
India we know has no idea of how many people have died.
by Deuce If any of you are hesitating about getting vaccinated - or are not planning to get vaccinated... I strongly suggest that you read this...
by ponchi101 People that are not vaccinated nor plan to be are at BAT.COM; Babble About Tennis.
They sort of don't like us.
(MJ and I talked about that article. Somehow, it did not surprise us)
by ti-amie
by mmmm8 Then there's the part where he thinks Guantanamo is "an island we own."
by ponchi101 That's his view of the world. You own or not stuff. Of course, he can extend it to people. You do not hire, work with, employ, or contract people. You own them.
by ponchi101 I remember last year, when the pandemic was gaining speed, that Suliso was joking (in good nature) that I had traded hell (the USA) for a hot place (Colombia), as I was stranded there.
A small situation report for Colombia, which just reached 100K deaths, with only 1/9th the USA population.
Current daily deaths: 590 +/- ‘Everything is collapsing’: Colombia battles third Covid wave amid unrest
by dryrunguy I finally got vaccinated today (J&J). I know this is going to sound silly, but I cried the whole time and for a few minutes after. Those tears were entirely about a profound sense of relief. Roughly 16 months of constant fear was immediately lifted off my shoulders. I had no idea it was going to be an emotional experience. No idea at all.
by JazzNU
dryrunguy wrote: ↑Tue Jun 22, 2021 5:25 pm
I finally got vaccinated today (J&J). I know this is going to sound silly, but I cried the whole time and for a few minutes after. Those tears were entirely about a profound sense of relief. Roughly 16 months of constant fear was immediately lifted off my shoulders. I had no idea it was going to be an emotional experience. No idea at all.
Congrats @dry. Agree that it is an emotional experience.
by dryrunguy Here's the latest Situation Report. Lots of interesting stuff here. Stopped in Sheetz to get dolphins a coffee after his surgery this morning (outpatient). There were about 20 people inside. I was the only one wearing a mask.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 178 million cumulative cases and 3.9 million deaths worldwide as of 7:00am EDT on June 22. Global weekly incidence and mortality decreased for the seventh consecutive week. Global incidence fell by 5.5% compared to the previous week, and mortality decreased by 11.75%.
On June 19, Brazil surpassed 500,000 cumulative COVID-19 deaths, the second country to do so after the US. If it continues on this trajectory, Brazil could surpass the US as #1 globally in terms of cumulative mortality, but it is still approximately 100,000 deaths behind. Brazil remains #3 globally in terms of cumulative incidence; however, the US and India are both reporting declining daily incidence, whereas Brazil’s epidemic continues to accelerate. Over the past several days, Brazil surpassed India as #1 globally in terms of both daily incidence (June 17) and daily mortality (June 20).
Global Vaccination
The WHO reported 2.4 billion doses of SARS-CoV-2 vaccines administered globally as of June 21, and 983 million individuals have received at least 1 dose. Our World in Data is reporting 2.66 billion cumulative doses administered globally, an increase of 11% compared to this time last week. The global daily doses administered is once again increasing, largely driven by trends in Asia, up to a new record high of 39.8 million doses per day. Our World in Data estimates there are 782 million people worldwide who are fully vaccinated, slightly more than 10% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.4 million cumulative COVID-19 cases and 599,354 deaths. We expect the US to officially surpass 600,000 cumulative deaths in this afternoon’s or tomorrow’s update.
The rate of decline in the United States’ COVID-19 incidence is beginning to taper off. This was inevitable as the US appears to be entering the “long tail” of its COVID-19 epidemic, but there is some concern that the slowing progress could be a function of increasing prevalence of the Delta variant of concern (B.1.617.2; VOC). The US CDC publishes genomic sequencing data, both at the national and regional levels, and this week, we will analyze trends in VOCs, including Delta, that could potentially impact COVID-19 incidence. Official data are available through May 22 and are updated every 2 weeks; however, the CDC also displays its “Nowcast” projections for the next 2-week period, through June 5. The CDC’s SARS-CoV-2 genomic surveillance represents a relatively small fraction of reported cases, so the prevalence values are weighted estimates that account for “non-random sampling of sequencing data over time and across states.”
From February 28 through May 22, the proportion of sequences corresponding to the Alpha variant (B.1.1.7) increased significantly, from 26.6% to 69.5%, becoming the dominant variant over that period. The prevalence of the Gamma variant (P.1) also increased, from 0.5% to 8.4%, the #2 variant in the US as of May 22. The proportion of sequences corresponding to the Delta variant (B.1.617.2) increased slowly from February 27 through May 22 (0.0% to 2.7%); however, it jumps to 9.9% in the CDC’s Nowcast projection for May 23-June 5, which would make it the #3 variant nationwide. If this jump is indicative of a longer-term increasing trend, the Delta variant could quickly become the dominant variant in the US. The Nowcast projection also shows another, smaller jump for the Gamma variant, from 8.4% up to 11.6%. The projected prevalence of the Alpha variant fell slightly to 65.5%, and all other variants are projected to represent fewer than 5% of new cases nationwide.
At the regional level, the Alpha variant remains the dominant strain in all 10 HHS regions as of May 22, but the Nowcast projection potentially signals major changes in the coming weeks. For the period ending May 22, the Alpha variant prevalence ranges from 51.7% in Region 1 (New England) to 76.6% in Region 7 (Central), and it is more than 70% in most regions. Interestingly, Region 7 also represents the highest Delta variant prevalence, with 7.3%. Region 3 (Mid-Atlantic) has the lowest Delta variant prevalence, with only 1.4%. In the Nowcast projection for May 23-June 5, the Alpha variant still represents more than 50% sequences in all but 1 region, with only Region 2 (New Jersey/New York) projected to be 49.7%. The projected prevalence is 50.4% in Region 1 (New England), which could indicate that the Alpha variant prevalence could soon drop below 50% in a second region. The Gamma variant is #2 in Region 1 (17.5%), and the Delta variant is #2 in Region 2 (17.7%). The Gamma variant is also currently #2 in several other regions: 6 (South Central), 7 (Central), 8 (Mountain), and 9 (West Coast). The largest increases in the projected Delta variant prevalence are in Regions 7 (Central) and 8 (Mountain), with increases of 16.2 percentage points (pp) and 19.4pp, respectively. The Gamma variant is also projected to make substantial jumps in several regions, including Region 9 (+7.2pp), Region 1 (+6.3pp), and Region 10 (Pacific Northwest; +5.3pp).
In light of inconsistencies in reporting due to the Memorial Day holiday weekend (May 29-31), it is difficult to get a clear understanding of the current trends in daily incidence. The United States’ daily incidence is at its lowest point since early in the initial surge in March 2020, and while it has exhibited a relatively consistent overall decline since mid-April, it appears that the decline could be leveling off to some degree. Prior to the Memorial Day holiday weekend, the relative biweekly change was -35%, indicating a substantial decline. Reporting delays over the holiday contributed to further declines over the next 1.5-2 weeks, which brought the relative change down to a low of -44% on June 10. Since then, it increased to -24%, still indicating a decline, but to a lesser degree than before Memorial Day.
Notably, the new federal Juneteenth holiday weekend (June 18-20) could result in further disruptions to reporting, as will the upcoming Independence Day holiday weekend (July 3-5). Juneteenth (June 19) was only officially designated as a federal holiday last week, and with little advance notice, it is unclear to what extent state and local health departments across the country were closed on Friday, June 18, in observance of the holiday. With these 3 holidays in rapid succession, it could be difficult to identify longer-term trends in SARS-CoV-2 transmission, which could potentially mask impacts from VOCs, including the Delta variant, through the middle of July.
US Vaccination
The US surpassed 150 million fully vaccinated individuals on June 21. The US has distributed 379 million doses of SARS-CoV-2 vaccines and administered 319 million. The daily vaccine doses administered* continues to decline steadily, down from a high of 3.4 million doses per day on April 11 to 855,986 on June 16. The US is averaging 581,391 new fully vaccinated individuals per day.
*The US CDC does not provide a 7-day average for the most recent 5 days due to anticipated reporting delays for vaccine administration. This estimate is the most current value provided.
A total of 177 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 53.4% of the entire US population. Among adults, 65.4% have received at least 1 dose, and 8.4 million adolescents aged 12-17 years have received at least 1 dose. A total of 150 million individuals are fully vaccinated, which corresponds to 45.2% of the total population. Among adults, 55.9% are fully vaccinated, and 5.8 million adolescents aged 12-17 years are fully vaccinated. Progress has largely stalled among adults aged 65 years and older: 87.3% with at least 1 dose and 77.1% fully vaccinated. In terms of full vaccination, 79 million individuals have received the Pfizer-BioNTech vaccine, 59 million have received the Moderna vaccine, and 12 million have received the J&J-Janssen vaccine.
CUREVAC VACCINE CLINICAL TRIAL On June 16, CureVac announced preliminary efficacy results from a Phase 2b/3 clinical trial of its candidate SARS-CoV-2 vaccine. CureVac is based in Germany, but the studies included approximately 40,000 participants from across 10 countries in Europe and Latin America. The vaccine demonstrated an overall efficacy of 47% against any COVID-19 disease severity, falling short of the 50% threshold established early in the pandemic.
While the CureVac candidate vaccine uses an mRNA platform similar to those used in the Pfizer-BioNTech and Moderna vaccines, the estimated efficacy is much lower, approximately half of what was observed in those vaccines’ Phase 3 clinical trials. The exact cause for the lower efficacy is unclear; however, there are some potential factors that could contribute to the disparity. First, the CureVac clinical trials were conducted at a time when variants of concern (VOCs) are more prevalent around the world, and lower efficacy against these variants would impact the overall estimate. Additionally, the CureVac product uses a much smaller dose than other mRNA vaccines—12μg compared to 30μg or 100μg in the Pfizer-BioNTech and Moderna vaccines, respectively—which could potentially limit the magnitude of the immune response. One researcher who led one of the trials in Germany indicated that the lower efficacy is “very likely due to the dose.” The mRNA used in CureVac’s vaccine was slightly different from those in other vaccines, and it did not allow for higher doses due to increased risk of adverse events.
*125 of 134 total cases have genomic sequence data available for the interim analysis.
The CureVac press release indicates that final analysis is still underway, and the company will assess potential regulatory options once that is complete. While the vaccine’s performance may be viewed as disappointing compared to similar products already authorized for use, this example illustrates the extreme difficulties in developing novel vaccines, particularly on an accelerated timeline, and it should serve as a reminder of how fortunate we are that multiple of the early vaccine candidates successfully demonstrated such high efficacy.
DELTA VARIANT OF CONCERN Experts predict the highly transmissible Delta variant of concern, also known as B.1.617.2, will become the dominant strain in the US in the near future. As select states roll back pandemic guidelines and restrictions on social gatherings, the number of Delta variant cases has roughly doubled every two weeks in the US, raising concerns among experts over the potential for breakthrough infections and localized outbreaks. US CDC Director Dr. Rochelle Walensky warned that transmission of the variant coupled with stagnating vaccination rates in some states could allow the variant to mutate enough to evade protection offered by the vaccines. Dr. Walensky and other experts continue to urge the public to get fully vaccinated, while others note an alarming trend in some states: people skipping their second dose. According to one study (preprint), 2-dose effectiveness of the Pfizer-BioNTech vaccine was 87.9% with the Delta variant, but only 33.5% after 1 dose.
According to data from the CDC and the US Department of Health and Human Services, 5 states—Alabama, Arkansas, Missouri, Oklahoma and Utah—have experienced increases of 37% or more in their 7-day daily case averages over the last two weeks. Notably, the vaccination rates in those 5 states are lower than the national average. Currently, 45.7% of the US population has been fully vaccinated. States with higher vaccination rates, including Vermont, Hawaii, and Massachusetts, have achieved levels of population immunity that could be more successful at keeping the Delta variant at bay.
Internationally, COVID-19 cases attributable to the Delta variant are rising sharply in parts of Indonesia, including the capital Jakarta, which has seen an increase in the number of severe cases among younger adults. In Europe, experts are closely watching spikes in SARS-CoV-2 cases driven by the Delta variant. Officials in the UK and Portugal have reimplemented or held off on lifting lockdown measures due to an increasing number of cases, and experts in France, Germany, and Spain are monitoring clusters of Delta cases. The greater transmissibility and disease severity of the Delta variant could cause outbreaks to grow more serious more quickly than surges caused by previous variants.
GLOBAL COLLABORATION On June 21, the WHO and its COVAX partners announced they are working with a South African consortium to establish the African continent’s first COVID-19 mRNA vaccine technology transfer hub, aimed at scaling up SARS-CoV-2 vaccine production. Over the coming weeks, the partners—including Biovac, Afrigen Biologics and Vaccines, a network of universities, and the Africa CDC—will negotiate details with the government of South Africa and other stakeholders. The hub is expected to provide training and knowledge transfers on mRNA technologies that would allow manufacturers in low- and middle-income countries to produce the vaccines locally. However, the hub still needs to secure licensing agreements with vaccine manufacturers, notably Pfizer-BioNTech and Moderna, according to WHO officials, who noted those discussions are underway. Manufacturing at the South African hub is expected to begin in 9-12 months. South Africa President Cyril Ramaphosa praised the hub’s launch, calling it a historic step in the right direction, but he urged continued discussions on an intellectual property waiver under the World Trade Organization’s Agreement on Trade-Related Aspects of Intellectual Property Rights, or TRIPS.
At the conclusion of this past weekend’s Summit for Vaccine Internationalism, led by countries from the global south, national health officials committed to openly collaborate on SARS-CoV-2 vaccine technologies, pool manufacturing capacity for vaccines and other medical supplies, and provide regulatory capacity support. Cuba and Mexico pledged to offer open licenses for their domestically developed vaccines, and Venezuela proposed creating a technology transfer platform similar to the WHO’s COVID-19 Technology Access Pool. While the COVID-10 pandemic has spurred remarkable and rapid collaboration among a variety of partners, some researchers are expressing concern that the benefits of collaboration could be hindered by geopolitical tensions and are not always shared equally. Additionally, global health experts continue to call for more robust efforts to increase access to and production of vaccines in low and middle income countries, underlining the mantra that the pandemic will not end until it’s under control in every country.
SOUTH AMERICA COVID-19 is surging across South America, which accounts for only 5% of the world’s population but 25% of the pandemic's death toll. Collectively, the region’s death rate per capita is 8 times the world’s rate. Nearly 1 million people have died of COVID-19 across 12 countries in South America, and the region holds 7 of the 10 countries worldwide with the highest daily death rates per capita.
In Brazil, tens of thousands of protestors took to the streets of cities nationwide on Saturday, with demonstrators blaming Brazil President Jair Bolsonaro for dismissing the seriousness of the pandemic. The Brazilian Senate is investigating President Bolsonaro’s handling of the nation’s pandemic response, including accusations he purposefully delayed vaccination efforts. Brazil passed 500,000 COVID-19-related deaths this past weekend, second only to the US and India, where the official death toll is 389,302 but is estimated to be up to 4.2 million. Nearly 18 million people have been infected with SARS-CoV-2 in Brazil, and the country is experiencing a daily average of nearly 73,500 new cases and around 2,000 deaths. Only 11.5% of residents are fully vaccinated. Notably, Brazil’s outbreak is being fueled by the Gamma variant, also known as P.1, which was first identified in the country’s Amazon region. The Oswaldo Cruz Foundation (Fiocruz), part of the nation’s Ministry of Health, warned the situation is “critical” and the onset of winter could result in even more infections.
PHILIPPINES VACCINATION According to multiple news media reports, Philippines President Rodrigo Duterte recently indicated that he could begin arresting individuals who refuse SARS-CoV-2 vaccination. President Duterte is known for “brash rhetoric,” but he has demonstrated the willingness to take extreme measures to combat other threats, such as his “war” on drugs. The extent to which President Duterte can or will implement efforts to mandate vaccinations remains unclear. In comments earlier this week, he indicated that he would direct local government officials to compile lists of individuals who refuse vaccination. Mandatory vaccination policies pose a number of practical and ethical challenges, and many experts argue that they may not necessarily be the best option for increasing vaccination coverage, particularly from the perspective of establishing trust in the government and response. The Philippines has administered at least 1 dose of SARS-CoV-2 vaccine to approximately 5.7% of its population, and nearly 2% are fully vaccinated.
LONG COVID/PASC Studies are ongoing to improve our understanding of the longer-term physical and mental health effects of SARS-CoV-2 infection. Previous studies have documented cardiovascular, respiratory, and neurological symptoms that can persist for months after recovery from SARS-CoV-2 infection, including in individuals who experienced mild or asymptomatic COVID-19 disease. A study conducted by FAIR Health investigated private health insurance claims associated with “Long-Haul COVID.” The study included nearly 2 million COVID-19 patients and looked for the presence of COVID-19-related symptoms 30 days or longer after recovery from acute COVID-19 disease. The researchers found that 23.2% of COVID-19 patients reported at least 1 symptom 30 days or longer after recovery. The prevalence of persistent symptoms was higher among patients with severe COVID-19, but persistent symptoms also were present in patients who were asymptomatic or mildly symptomatic during the acute stage of their infection. Additionally, patients of all ages were affected by longer-term health effects, including children.
Researchers in the UK found that COVID-19 could be associated with the loss of brain tissue after recovery, even among individuals with mild COVID-19 disease. The study (preprint) utilized brain scans taken as part of an ongoing Biobank study. The researchers compared scans taken before infection and after recovery for 394 COVID-19 patients, and compared them with 388 healthy control participants. The study documented loss of grey matter brain tissue in recovered COVID-19 patients, compared to the controls. The effects were observable in multiple parts of the brain, including areas that could potentially increase the risk of Alzheimer’s disease or dementia later in life. The researchers also compared hospitalized and non-hospitalized COVID-19 patients. There was potential evidence of an association between disease severity and brain tissue loss, but it was not statistically significant. Notably, there were only 15 hospitalized patients included in the study, which limited the available data. The availability of brain imagery from before the pandemic provided the researchers with an opportunity to directly observe changes in brain tissue in individuals who were later infected with SARS-CoV-2.
MONOCLONAL ANTIBODY TREATMENT Regeneron’s monoclonal antibody (mAb) combination treatment appears to reduce deaths in COVID-19 patients who are unable to mount their own antibody response, according to RECOVERY trial preliminary results. In the clinical trial, 24% of patients given a combination of two monoclonal antibodies (casirivimab and imdevimab) died, compared with 30% of patients given standard care (rate ratio 0.80; 95% CI 0.70–0.91; p=0.001). The study also saw a reduction in the median length of hospital stays for those given the treatment compared to the control group. Patients receiving Regeneron’s treatment also were significantly less likely to require mechanical ventilation.
While mAbs have been available for use during the majority of the pandemic, their relative effectiveness in decreasing deaths or improving clinical markers has been debated. Previous studies have shown that some patients greatly improve following mAb infusion while others show no improvement at all. The US government had previously purchased 1.5 million doses of the combination therapy after it received emergency use authorization from the FDA, but those doses have widely gone unused. With the availability of antibody tests, hospitals can now test COVID-19 patients for evidence of an antibody response, or lack thereof. In those patients with no discernible antibody response, the REGEN-COV could be a potentially life saving intervention. However, the therapy’s high price (around $1,400 per treatment) likely will inhibit greater uptake in high-income countries and could be cost-prohibitive in developing countries.
MODERNA VACCINE The US government recently signed an agreement to purchase 200 million more doses of the Moderna vaccine, including an option to buy experimental doses in development. The US order brings the nation's total number of Moderna doses purchased to 500 million. Moderna thus far has provided 217 million doses to the US and is expanding its manufacturing capacity to fulfill this contract and others in the future. Moderna has added two new production lines to its plant in Boston, Massachusetts. These and other additions will increase its manufacturing capacity by 50% by the end of 2022. Moderna is currently developing booster shots and other experimental vaccines aimed at targeting newer SARS-CoV-2 variants.
US CDC CRUISE SHIP REGULATION A federal judge on June 18 ruled the US CDC cannot enforce its COVID-19 conditional sailing orders—under which cruise lines were required to implement a phased approach to testing and other safety measures before they could start sailing—that were intended to prevent the spread of SARS-CoV-2 on Florida-based cruise ships. Florida challenged the CDC rules in April, arguing they were obstructing the cruise industry’s operations and causing the state to lose hundreds of millions of dollars. In his ruling, US District Court Judge Steven D. Merryday sided with the state, issuing a preliminary injunction to begin on July 18, when the conditional sailing order will exist only as non-binding guidelines. Judge Merryday wrote in the 124-page decision, “In a word, never has CDC implemented measures as extensive, disabling, and exclusive as those under review in this action.” The ruling orders both parties to return to mediation to work out a final solution, efforts that have previously failed; however, the CDC could appeal the decision. On June 16, the CDC lowered its risk level guidance from Level 4 “Very High” to Level 3 “High” for cruise ship passengers who are not fully vaccinated.
SUMMER OLYMPICS & WORLD CUP The 2020 Summer Olympic Games are slated to proceed in Tokyo despite rising concerns over Japanese vaccination rates and the nation’s current burden of COVID-19 cases. Olympic organizers announced some local fans will be allowed at events under strict rules, including mask wearing, no cheering, and returning directly home. Stadiums and other venues will be limited to 50% capacity or up to 10,000 domestic fans, whichever is less. Spectators will be allowed only if no state of emergency is in effect, and the rules could change as vaccinations increase or if a surge is predicted. Japan is advancing efforts to improve national vaccination rates, with 33 million inoculations to date and 7.7% of the population fully vaccinated.
As the international community looks to future sporting events, Qatar has stated that only vaccinated fans will be allowed at the 2022 World Cup, posing a substantial barrier for players and fans from many low- and middle-income countries who have yet to be vaccinated. Qatar is in the process of securing 1 million SARS-CoV-2 vaccine doses in case global efforts lag. FIFA President Gianni Infantino said the November 2022 matches are expected to be held in full stadiums. Qatar has fully vaccinated 45% of its population to date.
ponchi101 wrote: ↑Tue Jun 22, 2021 3:04 pm
That's his view of the world. You own or not stuff. Of course, he can extend it to people. You do not hire, work with, employ, or contract people. You own them.
It's also just not an island
by Deuce How could vaccines which were not proven to be effective be approved for use?
by ponchi101 Serious here. Have you ever worked with or for the Chinese? Their mentality is not the same as "ours". If the boss says he want THIS by THAT time, he gets THIS by THAT time. By that I mean, the boss will not be told the truth, he will be told what he wants to hear. Otherwise, he sacks you.
And if later on he gets in trouble, he will flatly blame you for it and sack you again.
It is a very different cultural approach.
by Suliso I haven't worked with Chinese, but I have worked with Indians. Not the same thing, but also the blame percolates down to the lowest rung and the boss is always right.
by Deuce
ponchi101 wrote: ↑Wed Jun 23, 2021 5:09 pm
Serious here. Have you ever worked with or for the Chinese? Their mentality is not the same as "ours". If the boss says he want THIS by THAT time, he gets THIS by THAT time. By that I mean, the boss will not be told the truth, he will be told what he wants to hear. Otherwise, he sacks you.
And if later on he gets in trouble, he will flatly blame you for it and sack you again.
It is a very different cultural approach.
I know East Asians (Japanese, Chinese, Koreans, etc.) to be exceptionally disciplined, efficient, and hard workers.
A shoddy vaccine doesn't figure into that equation.
Also, your theory doesn't explain how other countries could approve an inefficient vaccine, thus putting their populations at risk.
by ti-amieRed and blue America are evolving into vulnerable and safe America
By
Philip Bump
National correspondent
June 23, 2021 at 2:24 p.m. EDT
As it turns out, polling on Americans’ willingness to be vaccinated against the coronavirus was accurate from the outset.
In January, before the vaccine was widely available, Monmouth University polling found that 56 percent of Americans planned to get vaccinated as soon as possible or had already received at least one shot (At that point, of course, few had). Another 19 percent indicated that they would wait and see how the rollout went, and about a quarter said they were unlikely to get it at any point.
Over the next five months, Monmouth polling found exactly what you’d expect. The percentage of people who’d gotten the vaccine or said they planned to went up and the percent saying they would wait and see went down. The percentage who said they likely wouldn’t get a dose also remained steady, with about a quarter of Americans sticking by that position even now.
There’s been a lot of analysis of this pattern, repeated looks at who isn’t getting the vaccine and why. That analysis, too, has been fairly consistent. For example, it remains the case that Democrats are far more likely to say they have gotten the vaccine than are Republicans. Democrats are also a lot less likely to say they don’t plan to get it at all.
In Monmouth’s June poll, released on Wednesday, there’s an interesting additional divide. Those who have children in their homes are much more likely to say they likely won’t get a dose of the vaccine. Exactly why isn’t clear.
The partisan reticence to get vaccinated shows up in the actual vaccine numbers. Washington Post analysis of data from the Centers for Disease Control and Prevention shows an obvious correlation between 2020 presidential vote and vaccinations. Each dot below represents one state, color-coded depending how wide the margin in favor of President Biden or Donald Trump was last year. The state that preferred Biden in 2020 that has the lowest rate of vaccinations is Georgia.
That color-coding is useful when we then overlap vaccination rates with the change in new infections in each state since the beginning of the month. There are eight states that have seen an increase in their 7-day average of new infections since June 1; seven of them preferred Trump in 2020. The exception is Nevada.
More importantly, the states with the highest vaccination rates are also those that have seen the biggest drops in new cases. There are states with relatively low vaccination rates that have seen substantial drops in new cases; South Carolina, for example, has the tenth-lowest vaccination rate but has seen one of the largest drops in new infections.
Overall, though, the states that voted most heavily Democratic last year are more likely to have higher vaccination rates and bigger drops in their infection totals than states that voted heavily for Trump.
Last summer, the country saw a surge in states like Florida, Arizona and Texas. It’s possible that the seasonal heat contributed to that increase, given the need to head to air-conditioned spaces where the virus could more easily be transmitted. The same could happen this summer even as the so-called delta variant of the virus, a much more contagious iteration, is making up a larger percentage of new coronavirus infections. Even before autumn and winter, when infections have been more rampant, there are dangers.
Those are lessened if people take precautions against infection. Which brings us to another component of that Monmouth poll. Since January, when infections were rampant, the percentage of Americans saying they’re very or somewhat concerned about themselves or their family getting vaccinated has fallen from 79 percent to 42 percent.
But on this question, too, there’s an important divide. Those who’ve been vaccinated are about as likely to express concern about a family member becoming seriously ill from the virus as they are to not being very worried about it. Among those who haven’t been vaccinated, though, there is far less concern.
The gap is even wider on a particularly salient question: How concerned are you about a new surge in cases? Among those best protected against the virus — and, therefore, least likely to spread it — nearly three-quarters worry about a new surge. Among those least protected and most likely to be infected during such a surge, 85 percent express little to no concern about it happening.
by ponchi101 I did not postulate a theory. You were asking how come some countries were using a vaccine that was not completely tested.
If you work with the Japanese, once they give you their word you can forget about the issue. It will be done.
No experience with Koreans.
But in the Chinese culture, if the boss wants something he will be told that that something is ready and done, regardless of the truth. Therefore, if Xi Jinping demanded a vaccine for Covid, within a certain span of time, the column of bureaucracy in between would work to ensure that Xi's demands were met, and would tell him so, even if the vaccine was either not properly tested or was properly tested but the results, as they seem to be, were not what was expected.
Why would Chile use the Chinese vaccine? Easy. Chile is a well run and efficient bureaucracy FOR A SOUTH AMERICAN COUNTRY*. What the GOVT wanted to do was to do something, anything, that would look as if they were in control. And the only vaccine readily available was the Chinese, so they went with that, trusting the Chinese claims that it would work well. Here in Colombia, with nothing going well, the GOVT accepted Chinese vaccines too, simply because of pressure to appear to be in control and because politically you do not go on public and do a NaziPonchi "The Chinese will lie to us and we do not trust their vaccine". Most likely, both Colombia and Chile trusted the Chinese, a major superpower, and now they face the consequences.
Mongolia will not deny a Chinese vaccine for obvious reasons and the Seychelles won't either, the second because it was available and cheap.
Off Topic
* Which makes it comparable. Like the rest of S. America, our governments would be classified as shoddy, corrupt and inefficient by any other developed country's scale, like, for example, Canada
by ti-amie
by ti-amieInside the extraordinary effort to save Trump from covid-19
By
Damian Paletta
and
Yasmeen Abutaleb
June 24, 2021 at 8:13 a.m. EDT
This article is adapted from “Nightmare Scenario: Inside the Trump Administration’s Response to the Pandemic That Changed History,” which will be published June 29 by HarperCollins.
Health and Human Services Secretary Alex Azar’s phone rang with an urgent request: Could he help someone at the White House obtain an experimental coronavirus treatment, known as a monoclonal antibody?
If Azar could get the drug, what would the White House need to do to make that happen? Azar thought for a moment. It was Oct. 1, 2020, and the drug was still in clinical trials. The Food and Drug Administration would have to make a “compassionate use” exception for its use since it was not yet available to the public. Only about 10 people so far had used it outside of those trials. Azar said of course he would help.
Azar wasn’t told who the drug was for but would later connect the dots. The patient was one of President Donald Trump’s closest advisers: Hope Hicks.
A short time later, FDA Commissioner Stephen Hahn received a request from a top White House official for a separate case, this time with even greater urgency: Could he get the FDA to sign off on a compassionate-use authorization for a monoclonal antibody right away? There is a standard process that doctors use to apply to the FDA for unapproved drugs on behalf of patients dealing with life-threatening illnesses who have exhausted all other options, and agency scientists review it. The difference was that most people don’t call the commissioner directly.
The White House wanted Hahn to say yes within hours. Hahn, who still did not know who the application was for, consulted career officials. The FDA needs to go by the book, the officials insisted. Hahn relayed the message back to the White House. They kept pressing him to effectively cut corners. No, we can’t do that, Hahn told them several times. We’re talking about someone’s life. We have to actually examine the application to make sure we’re doing it safely.
When Hahn later learned the effort was on behalf of the president, he was stunned. For God’s sake, he thought, it’s the president who’s sick, and you want us to bend the rules? Trump was in the highest-risk category for severe disease from covid-19 — at 74, he rarely exercised and was considered medically obese. He was the type of patient with whom you would want to take every possible precaution. As it did with all compassionate-use applications, the FDA made a decision within 24 hours. Agency officials scrambled to figure out which company’s monoclonal antibody would be most appropriate given the clinical information they had, and selected the one from Regeneron, known simply as Regen-Cov.
A five-day stretch in October 2020 — from the moment White House officials began an extraordinary effort to get Trump lifesaving drugs to the day the president returned to the White House from the hospital — marked a dramatic turning point in the nation’s flailing coronavirus response. Trump’s brush with severe illness and the prospect of death caught the White House so unprepared that they had not even briefed Vice President Mike Pence’s team on a plan to swear him in if Trump became incapacitated.
Trump’s medical advisers hoped his bout with the coronavirus, which was far more serious than acknowledged at the time, would inspire him to take the virus seriously. Perhaps now, they thought, he would encourage Americans to wear masks and put his health and medical officials front and center in the response. Instead, Trump emerged from the experience triumphant and ever more defiant. He urged people not to be afraid of the virus or let it dominate their lives, disregarding that he had had access to health care and treatments unavailable to other Americans.
It was, several advisers said, the last chance to turn the response around. And once the opportunity passed, it was the point of no return.
...On Saturday, Sept. 26, he had hosted a party with scores of maskless attendees to announce Amy Coney Barrett as his pick for Supreme Court justice. The celebrations had continued indoors, where most people remained maskless. By that time, the virus was surging again, but Trump’s contempt for face coverings had turned into unofficial White House policy. He actually asked aides who wore them in his presence to take them off. If someone was going to do a news conference with him, he made clear that he or she was not to wear a mask by his side.
The day after the Supreme Court celebration, Trump had also hosted military families at the White House. At Trump’s insistence, few were wearing masks, but they were packed in a little too tight for his comfort. He wasn’t worried about others getting sick, but he did fret about his own vulnerability and complained to his staff afterward. Why were they letting people get so close to him? Meeting with the Gold Star families was sad and moving, he said, but added, “If these guys had covid, I’m going to get it because they were all over me.” He told his staff that they needed to do a better job of protecting him.
Two days after that, he flew to Cleveland for the first presidential debate against his Democratic challenger, Joe Biden. Trump was erratic that whole evening, and he seemed to deteriorate as the night went on. The pundits’ verdicts were brutal.
Almost 48 hours later, Trump became terribly ill. Hours after his tweet announcing he and first lady Melania Trump had coronavirus infections, the president began a rapid spiral downward. His fever spiked, and his blood oxygen level fell below 94 percent, at one point dipping into the 80s. Sean Conley, the White House physician, attended the president at his bedside. Trump was given oxygen in an effort to stabilize him.
The doctors gave Trump an eight-gram dose of two monoclonal antibodies through an intravenous tube. That experimental treatment was what had required the FDA’s sign-off. He was also given a first dose of the antiviral drug remdesivir, also by IV. That drug was authorized for use but still hard to get for many patients because it was in short supply.
Typically, doctors space out treatments to measure a patient’s response. Some drugs, such as monoclonal antibodies, are most effective if they’re administered early in the course of an infection. Others, such as remdesivir, are most effective when they’re given later, after a patient has become critically ill. But Trump’s doctors threw everything they could at the virus all at once. His condition appeared to stabilize somewhat as the day wore on, but his doctors, still fearing he might need to go on a ventilator, decided to move him to the hospital. It was too risky at that point to stay at the White House.
Many White House officials and even his closest aides were kept in the dark about his condition. But after they woke up to the news — many of them were asleep when Trump tweeted at nearly 1 a.m. on Friday that he had the virus — Cabinet officials and aides lined up at the White House to get tested. A large number had met with him the previous week to brief him about various issues or had traveled with him to the debate.
It was unclear even to Trump’s closest aides just how sick he was. Was he mildly ill, as he and Conley were saying, or was he sicker than they all knew? Trump was supposed to join a call with nursing home representatives later that day as part of his official calendar. Officials had been scheduled to do it in person from the White House, but that morning they were informed the call would be done remotely. Trump’s aides insisted that he would still be on it.
As one aide waited in line for a coronavirus test, she saw Conley sprint out of his office with a panicked look. That’s strange, the aide thought. An hour or two later, officials were informed that Pence would be joining the nursing homes call. Trump couldn’t make it.
(...)
Throughout Trump’s time in the hospital, his doctors consulted with the medical experts on the White House coronavirus task force whom the president had long ago discarded. They talked to Hahn, National Institute of Allergy and Infectious Diseases Director Anthony S. Fauci and Centers for Disease Control and Prevention Director Robert Redfield, seeking input about his treatment.
Trump and his aides had ignored numerous warnings from the task force doctors that they were putting themselves and everyone in the West Wing at risk by their cavalier behavior. Over the past eight months, Trump had come dangerously close to the virus a number of times. Those repeated escapes had made the White House more careless, constantly tempting fate. Deborah Birx, the White House coronavirus task force coordinator, and Redfield wrote to top aides after every White House outbreak, warning them that 1600 Pennsylvania Avenue was not safe. Birx took her concerns to Pence directly. This is dangerous, she told him. If White House staff can’t or won’t wear masks, they need to be more than 10 feet away from one another. This is just too risky.
Their warnings had gone unheeded, and now some would pay a price. Trump hadn’t wanted to go to the hospital, but his aides had spelled out the choice: He could go to the hospital Friday, while he could still walk on his own, or he could wait until later, when the cameras could capture him in a wheelchair or gurney. There would be no hiding his condition then.
At least two of those who were briefed on Trump’s medical condition that weekend said he was gravely ill and feared that he wouldn’t make it out of Walter Reed. People close to Trump’s chief of staff, Mark Meadows, said he was consumed with fear that Trump might die.
It was unclear if one of the medications, or their combination, helped, but by Saturday afternoon Trump’s condition began improving. One of the people familiar with Trump’s medical information was convinced the monoclonal antibodies were responsible for the president’s quick recovery.
(...)
Redfield spent the weekend Trump was sick praying. He prayed the president would recover. He prayed that he would emerge from the experience with a newfound appreciation for the seriousness of the threat. And he prayed that Trump would tell Americans they should listen to public health advisers before it was too late. The virus had begun a violent resurgence. Redfield, Fauci, Birx and others felt they had limited time to persuade people to behave differently if they were going to avoid a massive wave of death.
There were few signs that weekend that Trump would have a change of heart. It had already been a battle to get him to agree to go to Walter Reed in the first place. Now, he was badgering Conley and others to let him go home early. Redfield heard Trump was insisting on being discharged and called Conley on the phone. The president can’t go home this early, Redfield advised the doctor. He was a high-risk patient, and there were no guarantees that he wouldn’t backslide or experience some complication. (Many covid-19 patients seemed to be on an upswing and then quickly deteriorated.) Trump needed to stay in the hospital until that risk had passed. Conley agreed but said the president had made up his mind and couldn’t be convinced otherwise.
(...)
Just as the country had been watching a few days before, many people tuned in again as Trump took Marine One back to the White House’s South Lawn on Monday night. They saw him step out in a navy suit, white shirt and blue-striped tie, with a medical mask on his face. He walked along the grass before climbing the steps to the Truman Balcony.
But Trump didn’t go inside. It was a moment of political theater too good to pass up — as suffused with triumph as his trip Friday had been humbling. He turned from the center of the balcony and looked back toward Marine One and the television cameras. It was clear that he was breathing heavily from the long walk and the climb up the flight of stairs.
Redfield was watching on television from home. He was praying as Trump went up the steps. Praying that he would reach the Truman Balcony and show some humility. That he would remind people that anyone could be susceptible to the coronavirus — even the president, the first lady and their son. That he would tell them how they could protect themselves and their loved ones.
But Trump didn’t waver. Facing the cameras from the balcony, he used his right hand to unhook the mask loop from his right ear, then raised his left hand to pull the mask off his face. He was heavily made up, his face more orange tinted than in the photos from the hospital. The helicopter’s rotors were still spinning. He put the mask into his right pocket, as if he was discarding it once and for all, then raised both hands in a thumbs-up. He was still probably contagious, standing there for all the world to see. He made a military salute as the helicopter departed the South Lawn, and then strode into the White House, passing staffers on his way and failing to protect them from the virus particles emitted from his nose and mouth.
Right then, Redfield knew it was over. Trump showed in that moment that he hadn’t changed at all. The pandemic response wasn’t going to change, either.
by ponchi101 So the big macs are not doing it.
The diet cokes are not doing it.
The lack of exercise and the obesity are not doing it.
And Covid could not do it.
It is going to take a meteor striking Mar-A-Lago. Nothing less.
by JazzNU
ponchi101 wrote: ↑Thu Jun 24, 2021 7:24 pm
So the big macs are not doing it.
The diet cokes are not doing it.
The lack of exercise and the obesity are not doing it.
And Covid could not do it.
It is going to take a meteor striking Mar-A-Lago. Nothing less.
Much less can do it. Much, much less. Use your imagination. So many potential gifs to illustrate I couldn't choose.
by Suliso Because they started much slower, but if you analyze carefully those graphs you'll see that the slope in the last 2-3 months is much steeper than in US. That means EU is catching up fast now and will overtake US for the 1st dose by July 14th and for the second about a month later. US has already reached almost everyone who wants to be vaccinated. The final numbers depend on the proportion of hard antivaxxers in both areas.
Nice graph. I remain shocked about the 1st dose vs. 2nd dose for the UK.
In terms of comparisons as we keep going further, the EU is one thing against the US. But these comparisons of UK and Canada are really ridiculous to me. Choose a state or two, but it's so misleading to pretend like vaccinating less than 40 million is comparable to 320 million when you're just using percentages.
by Suliso They deliberately extended the time advised by manufacturers. In general in the early stages of vaccination the gap is large and stays large while the process is accelerating. Once it comes closer to the end the gap necessarily shrinks. Also large share of AZ vaccine (now only in UK) does it too since the advised gap is 9 weeks instead of 3 or 4.
by Deuce Still undecided about getting the vaccine?
Know anyone who is undecided about, or resisting, vaccination?
by dryrunguy Here's the latest Situation Report. Haven't read it yet. But I saw that they led with some dismaying news about transmissions in Africa.
::
Starting next week, we will shift to 1 detailed epidemiological analysis each week. We will continue to publish 2 situation reports per week, including the high-level epi data, but the in-depth epi analysis will only be included on Fridays.
EPI UPDATE The WHO COVID-19 Dashboard reports 180 million cumulative cases and 3.9 million deaths worldwide as of 4:30am EDT on June 25.
While African countries have largely contained their respective COVID-19 epidemics, the continent as a whole has exhibited a substantial increase in daily incidence since mid-May. Africa’s daily incidence has more than tripled since its most recent low on May 17, increasing from 7,849 new cases per day to 26,250. If it continues on this trajectory, Africa could soon surpass its highest peak (32,750). On a per capita basis, the only continent reporting fewer daily cases is Oceania, but if it continues on this trajectory, Africa’s per capita daily incidence could potentially reach the same range as Asia, Europe, and North America. Previously, Africa has briefly exhibited higher per capita daily incidence than Asia, but it has not really been close to Europe or North America until now. In terms of total daily incidence, Africa surpassed North America on June 22. The last time Africa reported higher total daily incidence than any continent other than Oceania was July 2020, when the peak of Africa’s first wave briefly exceeded Europe’s low between its first and second waves.
Many countries in sub-Saharan Africa are reporting substantial increases in daily incidence. In fact, at least 14 countries are reporting relative biweekly changes of +100% or higher, mostly in Central, Eastern, and Southern Africa. Notably, the biweekly change is +1,363% in Lesotho; +791% in South Sudan; +694% in Rwanda; and +649% in Zimbabwe. In West Africa, Gambia, Liberia, and Sierra Leone are reporting biweekly increases of more than 300%. Namibia and South Africa are exhibiting the longest surges, starting in early May (or possibly mid-April for South Africa), with daily incidence increasing by a factor of 13 and 10, respectively, since that time. Zambia’s surge began closer to mid-May, and its daily incidence is now more than 50 times higher than it was at that time—up from fewer than 50 new cases per day to more than 2,500. The remaining countries’ surges began around early June. Fortunately, most of these countries are still reporting fewer than 100 new cases per day, and the large relative changes are principally a factor of very low daily incidence at the start of the surge—in some instances, fewer than 10 new cases per day. But Zambia’s surge illustrates the risk that even epidemics that were once largely contained can accelerate rapidly to substantial levels of community transmission.
South Africa, the most severely affected country in Africa, is combating its third wave and quickly approaching its highest peak. Namibia and Zambia have already set new records for daily incidence. Analysis from Reuters indicates that Sierra Leone, Rwanda, and Zambia are all reporting record-high daily incidence, and the Democratic Republic of the Congo and Namibia are currently reporting at least 90% of their highest peak.
Looking globally, Africa continues to stand out as having among the lowest vaccination coverage, illustrating the critical importance of providing international support and increasing access to vaccine doses. Only 10 countries in Africa are reporting 1+ dose coverage greater than 5%, and only Mauritius and Seychelles are reporting greater than 30%. In terms of full vaccination, only 13 countries are reporting greater than 1% coverage, but data are not available for many countries. As a whole, Africa’s 1+ dose vaccination coverage is 2.6%, 14 percentage points below Oceania and approximately one-tenth the global average (22.6%). Similar trends are evident with respect to full vaccination.
Most countries in Africa have limited genomic sequencing data available, which limits the ability to understand changes in prevalence for emerging SARS-CoV-2 variants. South Africa is one of the few countries with enough sequence data available to provide some indication of these changes. There, the Beta variant (B.1.351) became the dominant strain over the course of 2020 and has remained dominant through the first half 2021. The Delta variant began to emerge in late April, and its prevalence appears to be increasing rapidly. Alpha variant (B.1.1.7) prevalence began to increase around the same time, but the Gamma variant (P.1) does not represent a meaningful proportion of new cases. The extent to which the Delta variant is driving the ongoing surges in Africa remains uncertain, but similar associations have been observed in other parts of the world.
Global Vaccination
The WHO reported 2.6 billion doses of SARS-CoV-2 vaccines administered globally as of June 24, and 1.03 billion individuals have received at least 1 dose. After a period of steady increase, the global daily doses administered decreased slightly from the record high of 41.6 million doses per day on June 23 to 41.2 million yesterday. Our World in Data estimates there are 806 million people worldwide who are fully vaccinated, corresponding to 10.3% of the global population, although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.4 million cumulative COVID-19 cases and 600,442 deaths. The US surpassed 600,000 cumulative deaths on June 22, the first country to do so:
1 death to 100k*- 84 days
100k to 200k- 113 days
200k to 300k- 86 days
300k to 400k- 33 days
400k to 500k- 33 days
500k to 600k- 130 days
*From February 29, 2020, the date of the first reported COVID-19 death in the US. Since then, health officials have identified more than 200 COVID-19 deaths that occurred prior to that date.
The CDC updated its SARS-CoV-2 genomic surveillance data, adding official data for May 23-June 5 and projections for June 6-19. Including the new projection period, the Delta variant (B.1.617.2) prevalence has increased from less than 1% to 20.6% over a period of 8 weeks, more than doubling in every 2-week period. Based on the current projection, the Delta variant is now the #2 variant nationwide. Gamma variant (P.1) prevalence also continues to increase steadily, now up to 16.4% of new cases. While still technically dominant based on the estimated prevalence, Alpha variant (B.1.1.7) prevalence has noticeably decreased over the past 2 reporting periods, down from a high of 70% to 52.2% in the June 6-19 projection. Combined, the Alpha, Gamma, and Delta variants account for more than 90% of all new cases in the US. These genomic data provide further evidence that the Delta variant is poised to become the dominant variant in the US over the coming weeks. In fact, the projection indicates that Delta is already the dominant variant in HHS Regions 7 (Central; 47.5%) and 8 (Mountain; 46.4%).
US Vaccination
The US has distributed 379 million doses of SARS-CoV-2 vaccines and administered 321 million. A total of 178 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 53.7% of the entire US population. Among adults, 65.7% have received at least 1 dose, and 8.5 million adolescents aged 12-17 years have received at least 1 dose. A total of 151 million individuals are fully vaccinated, which corresponds to 45.6% of the total population. Among adults, 56.2% are fully vaccinated, and 6.0 million adolescents aged 12-17 years are fully vaccinated.
mRNA VACCINES & MYOCARDITIS/PERICARDITIS The US CDC’s Advisory Committee on Immunization Practices (ACIP) is meeting this week as part of ongoing evaluation of SARS-CoV-2 vaccine safety and efficacy data. A major portion of this week’s meeting addressed emerging data regarding the risk of myocarditis and pericarditis—inflammation of the heart muscle and lining around the heart, respectively—following vaccination. Researchers presented data collected from several systems the CDC uses to monitor for adverse events after vaccination.
The data indicate there is a “likely association” between the mRNA-based SARS-CoV-2 vaccines, from Pfizer-BioNTech and Moderna, and elevated risk of myocarditis and pericarditis in adolescents and younger adults, although the risk appears to be very low. The rates of myocarditis/pericarditis are higher in males than females, and the conditions are more common after the second dose of the vaccine. The analysis estimates the overall rate of myocarditis/pericarditis to be 12.6 cases per million second doses of the vaccines in individuals aged 12-39 years old. The conditions tend to present within approximately 5 days, and while most of the affected individuals were hospitalized, symptoms were generally mild and most recovered quickly. To our knowledge, neither condition has resulted in death among recently vaccinated individuals.
Importantly, the available data indicate that the benefits of vaccination still far outweigh the risks of myocarditis/pericarditis. Even for males aged 12-17 years—the group with the lowest COVID-19 risk and highest myocarditis/pericarditis risk—risk and benefit calculations* estimate that 1 million second doses of the mRNA vaccines would prevent 5,700 COVID-19 cases, 215 hospitalizations, and 2 deaths, compared to 56-69 cases of myocarditis/pericarditis. A group of prominent public health and healthcare organizations—including HHS, CDC, and the American Academy of Pediatrics—issued a statement emphasizing the rarity of myocarditis/pericarditis following vaccination and encouraging all eligible individuals to get vaccinated. The US FDA is expected to update associated information for the mRNA vaccines, and the CDC continues to recommend SARS-CoV-2 vaccination to all eligible age groups.
*Calculated over a 120-day period.
US VACCINATION COVERAGE White House Coronavirus Response Coordinator Jeff Zients said the US will not reach US President Joe Biden’s goal of 70% of adults receiving at least 1 dose of SARS-CoV-2 vaccine by July 4. With the expectation now being that the US will fall slightly short of that benchmark, the White House issued a new goal of at least 1 dose of vaccine to 70% of adults aged 27 years and older by July 4. Currently, 150 million people are fully vaccinated, and Mr. Zients said that the US is expected to reach 160 million by mid-July.
As we have discussed previously, there are some regional disparities in terms of vaccination coverage in the US. In particular, several states in the South and West regions are lagging behind in their vaccination campaigns. Fewer than 40% of adults in Alabama, Mississippi, Louisiana, Idaho, and Wyoming have received at least 1 dose. Though Missouri is reporting 44% of adults receiving at least one dose, health officials are concerned about several counties in the south and north of the state reporting well below that rate, with one county reporting only 13% vaccination coverage. There is concern that lagging interest in vaccination among younger adults could provide a large enough unprotected population to continue fueling COVID-19 surges. At one hospital in Springfield, Missouri, nearly two-thirds of COVID-19 patients in the ICU last weekend were under 40 years old. In Missouri, Arkansas, and Utah, COVID-19 hospital admissions have increased more than 30% since the beginning of June. The Mayo Clinic’s ”hot spot” map shows Missouri as one of only 2 states reporting more than 10 daily cases per 100,000 population—the other being Nevada. The states reporting between 5 and 10 are largely located in the Southeast and Western portions of the country.
As the prevalence of variants of concern (VOCs) increases, including the Delta variant, vaccination remains a critical tool for containing community transmission and protecting against severe disease and death. Analysis from the Associated Press found that “breakthrough” infections accounted for only 0.1% of US COVID-19 cases in May, and only 0.8% of the 18,000 COVID-19 deaths were among fully vaccinated individuals. Previously, Dr. Andy Slavitt—former White House COVID-19 advisor—estimated that 98-99% of COVID-19 deaths are among unvaccinated individuals.
DELTA VARIANT The Delta variant (B.1.617.2) currently accounts for an estimated 20% of new COVID-19 cases in the US and likely will become the dominant strain in a matter of weeks, according to White House Chief Medical Advisor Dr. Anthony Fauci, who also noted the variant as the United States’ greatest threat in dealing with COVID-19. The European CDC (ECDC) Threat Assessment for the Delta variant projects that the variant will be responsible for 90% of cases by the end of August. Russia has already reached that threshold, where 90% of new cases in Moscow are being attributed to the Delta variant. This variant of concern (VOC) has been reported in 85 countries, is 40-60% more transmissible than Alpha (B.1.1.7), and may be associated with a higher risk of hospitalization.
According to a Public Health England study, a single dose of either the Pfizer or AstraZeneca vaccines reduced a person’s risk of developing COVID-19 symptoms caused by the Delta variant by 33%, compared to 50% for the Alpha variant. A second dose of AstraZeneca brought protection to 60% (66% for Alpha), and a second dose of Pfizer increased protection to 88% (90% for Alpha). A Scottish study found an increased likelihood of hospitalization among patients infected with the Delta variant, nearly double the risk for the Alpha variant. Additionally, that study showed that among fully vaccinated individuals, Pfizer’s vaccine provided 79% protection against the Delta variant, while it offered 92% against the Alpha variant. Vaccination with the AstraZeneca vaccine showed substantial but reduced results among those fully vaccinated, with 60% efficacy against the Delta variant and 73% protection against the Alpha variant. These studies underline the importance of vaccination as a tool to reduce hospitalizations and disease severity among COVID-19 patients.
CUBAN VACCINES Cuban health authorities on June 21 released new data on the nation’s home-grown Abdala SARS-CoV-2 vaccine, showing efficacy on par with several existing vaccines. As noted in previous updates, Cuba had foregone outside assistance when it came to vaccine imports, choosing to hold off and vaccinate its population with the 3-dose Abdala vaccine. The country began vaccinations in May, prior to the completion of studies examining the vaccine’s efficacy, in parts of the country where SARS-CoV-2 was spreading quickly. New results from the manufacturer’s Phase 3 trial suggest that this early vaccination initiative may have paid off. Abdala showed 92.28% efficacy among individuals who received all three doses. Following the announcement of these results, study organizers shared they would be opening the study codes of the Phase 3 clinical trial to vaccinate all participants who received the placebo.
Cuban health officials also announced that a second vaccine candidate, Sovereign 02, boasted 62% efficacy following its two-dose schedule. These are encouraging results, especially given the epidemiological backdrop of Cuba’s COVID-19 outbreak. Cuba is in the midst of a peak of COVID-19 cases, reporting a record-high 7-day average of new cases of about 1,625. The rate of people who have been vaccinated continues to increase alongside this change in the country’s epidemiological situation, with just over 20% of the population having received at least one dose of a COVID-19 vaccine. Hopefully, recent clinical trial results will spur vaccination rates to counter increased disease activity.
CHINESE VACCINE EFFECTIVENESS Several countries that mostly relied on the Chinese Sinopharma and Sinovac Biotech vaccines are currently facing large outbreaks. Despite high vaccination coverage, Seychelles, Bahrain, Chile, and Mongolia have all reported their highest daily incidence since mid-May*, all after reaching 50% coverage with at least 1 dose. In March, Seychelles was one of the world’s most vaccinated countries, with approximately 57% of its vaccinations using the Sinopharm vaccine. Between 50-68% of the population has been fully vaccinated in these countries, compared to 45% in the US, raising some questions regarding the effectiveness of the vaccines.
*Chile’s peak on June 8 was within 30 new cases per day (0.04%) of its highest peak.
Breakthrough infections are certainly possible, as no vaccine is 100% effective, but lower efficacy for the 2 Chinese-made vaccines and the role of emerging variants could be driving the increases in daily incidence in these countries. The Sinopharm vaccine’s efficacy rate is estimated to be 78.1%, and the Sinovac vaccine’s is 51%. In comparison, the Pfizer-BioNTech and Moderna vaccines have over 90% efficacy, AstraZeneca-Oxford is at 63%, and J&J-Janssen has 85%. Bahrain has now begun offering booster shots of the Pfizer-BioNTech vaccine to those who originally received the Sinopharm vaccine, which accounts for about 60% of the doses administered there. More than 95 countries have received doses of the Chinese-produced vaccines.
AFRICA Africa is facing a rapidly increasing third surge, with the number of new COVID-19 cases rising for 5 consecutive weeks since the beginning of this wave on May 3. At the current rate of infection, the third surge will surpass the previous one by early July, with at least 12 nations experiencing case increases. Experts are citing the spread of the Delta variant (B.1.617.2) as one factor influencing this latest surge, with 14 nations across the continent reporting cases of the variant. In Kisumu, Kenya, health officials say Delta is driving an upswing in cases, particularly among young people, and have expressed fear that a wave of infections like that seen in India in April and May could be on the horizon. Weak adherence to public health measures, including an increase in social gatherings and movement, also is contributing to a rise in infections. Many hospitals are overwhelmed, and a shortage of oxygen on the continent is hindering patient care for those who do find beds.
Only about 1.1% of the continent’s population is fully vaccinated. According to WHO Regional Director for Africa Dr. Matshidiso Moeti, the continent needs an additional 215 million vaccine doses to fully vaccinate 10% of its population, and about 700 million doses to reach 30% of the population by the end of the year. Eighteen (18) countries have used 80% of their doses received through COVAX, with 8 of those having exhausted their supplies, and another 29 nations having used more than 50% of their doses. Just under 1.5% of the 2.7 billion vaccine doses administered globally have been administered in Africa. Many health experts were confused by how African countries initially kept COVID-19 at arm’s length, and if this surge proves as devastating as India’s latest, a collective failure of the international community to adequately support the continent could be to blame.
AUSTRALIA The Australian government has run a highly effective COVID-19 response, with efforts to close borders and enforce physical distancing rules limiting the cumulative number of COVID-19 cases to just over 30,300. The country has seen only two spikes of COVID-19 incidence, with the latter tapering off around the end of September 2020. Roughly 11% of Australia’s cumulative COVID-19 cases have come since the beginning of October 2020, representing a slow burn of new cases. These new cases have come in small outbreaks, forcing the Australian government to enact stricter public health measures intermittently. Notably, a recent outbreak in Queensland of nine cases is being attributed to the Delta SARS-CoV-2 variant. Health officials have expanded mandates on mask wearing, citing concerns of the Delta variant’s heightened transmissibility. A separate and larger COVID-19 outbreak of the Delta variant is ongoing in Sydney, leading the city to implement stricter public health measures to limit the spread of the virus. The Australian government has raised concerns over the longevity of its response measures in light of these recent clusters of new cases. Nearly 25% of the country’s adults have received one dose of vaccine, but less than 5% are fully vaccinated. The low vaccination rates have led some to question whether the nation is prioritizing contact tracing and testing over vaccination, while some experts blame shortfalls in expected vaccine shipments for lagging rates.
ISRAEL Israel reinstated its indoor mask mandate today, less than 2 weeks since the mandate was dropped on June 15. Public Health Director Dr. Sharon Alroy-Preis said the Ministry of Health previously determined the mask mandate should be reintroduced if Israel records a daily average of 100 new COVID-19 cases over one week. As of June 24, the rolling 7-day average of confirmed cases was 99.57, with daily incidence rising, according to Our World In Data. Israel’s coronavirus czar Dr. Nachman Ash announced the country recorded 227 new cases on June 24, though he said he does not feel the nation is entering a fourth surge. Dr. Alroy-Preis blamed a lack of adherence to mandatory quarantine rules for travelers from high-risk countries for the introduction of the Delta variant into the country, one of the causes of the latest outbreak, and she called on the government to more strongly enforce the rules. Israel is one of the world’s most vaccinated countries, but the Delta variant is driving new cases among unvaccinated children and vaccinated individuals, who account for as much as 50% of new cases. However, there is not yet enough data to conclude the vaccines’ effectiveness against the Delta variant, according to Dr. Alroy-Preis. Prime Minister Naftali Bennett, who took office last week, announced the government will reestablish its coronavirus cabinet to assist in future decisions related to the pandemic.
Most countries in Africa have limited genomic sequencing data available, which limits the ability to understand changes in prevalence for emerging SARS-CoV-2 variants. South Africa is one of the few countries with enough sequence data available to provide some indication of these changes. There, the Beta variant (B.1.351) became the dominant strain over the course of 2020 and has remained dominant through the first half 2021. The Delta variant began to emerge in late April, and its prevalence appears to be increasing rapidly. Alpha variant (B.1.1.7) prevalence began to increase around the same time, but the Gamma variant (P.1) does not represent a meaningful proportion of new cases. The extent to which the Delta variant is driving the ongoing surges in Africa remains uncertain, but similar associations have been observed in other parts of the world.
I wonder if this situation is different in countries that were hit hard by Ebola a few years ago. Many of those countries were able to react quickly to the threat of C19 because of what they had to do to fight ebola. I wish they'd separate the data for the countries/regions of the African continent like they do for other continents.
ISRAEL Israel reinstated its indoor mask mandate today, less than 2 weeks since the mandate was dropped on June 15. Public Health Director Dr. Sharon Alroy-Preis said the Ministry of Health previously determined the mask mandate should be reintroduced if Israel records a daily average of 100 new COVID-19 cases over one week. As of June 24, the rolling 7-day average of confirmed cases was 99.57, with daily incidence rising, according to Our World In Data. Israel’s coronavirus czar Dr. Nachman Ash announced the country recorded 227 new cases on June 24, though he said he does not feel the nation is entering a fourth surge. Dr. Alroy-Preis blamed a lack of adherence to mandatory quarantine rules for travelers from high-risk countries for the introduction of the Delta variant into the country, one of the causes of the latest outbreak, and she called on the government to more strongly enforce the rules. Israel is one of the world’s most vaccinated countries, but the Delta variant is driving new cases among unvaccinated children and vaccinated individuals, who account for as much as 50% of new cases. However, there is not yet enough data to conclude the vaccines’ effectiveness against the Delta variant, according to Dr. Alroy-Preis. Prime Minister Naftali Bennett, who took office last week, announced the government will reestablish its coronavirus cabinet to assist in future decisions related to the pandemic.
This is very interesting. I believe that travelers could be to blame for the spike. But also, have we found out yet if the Palestinians were able to get vaccinated? Because for a long time at least, Israel was not giving them anywhere near the number of vaccines that Israelis were getting, which shouldn't be a surprise to anyone paying attention.
This is very interesting. I believe that travelers could be to blame for the spike. But also, have we found out yet if the Palestinians were able to get vaccinated? Because for a long time at least, Israel was not giving them anywhere near the number of vaccines that Israelis were getting, which shouldn't be a surprise to anyone paying attention.
This is very interesting. I believe that travelers could be to blame for the spike. But also, have we found out yet if the Palestinians were able to get vaccinated? Because for a long time at least, Israel was not giving them anywhere near the number of vaccines that Israelis were getting, which shouldn't be a surprise to anyone paying attention.
But so few people do.
Actually, at least here, more people were paying attention with their eyes wide open than they ever have in the past on this topic, which was encouraging. Not live changing unfortunately, but baby steps.
by ti-amie
by ti-amie
by ti-amie
by dryrunguy Let's try this again. Here's the latest Situation Report. Of particular note, the surge across Africa continues to get worse (but I couldn't get the data table to open, so I don't know where in Africa). We still have no idea what the long-term mental health sequalae associated with COVID will be, but it doesn't look good. And life expectancy for Hispanics and Blacks continues to drop due to COVID. There's more...
::
EPI UPDATE The WHO COVID-19 Dashboard reports 181 million cumulative cases and 3.9 million deaths worldwide as of 7:00am EDT on June 29. After 7 consecutive weeks of declining weekly incidence, the WHO reported an increase of 2.2% compared to the previous week. Weekly incidence increased 10% in Europe, 13% in the Eastern Mediterranean Region, and 34% in Africa. Based on WHO data, the African Region reported its highest weekly total to date. Weekly global mortality decreased for the eighth consecutive week. Global weekly mortality fell by 10% from the previous week, reaching its lowest total since early November 2020.
Global Vaccination
The WHO reported 2.66 billion doses of SARS-CoV-2 vaccines administered globally as of June 28, and 1.07 billion individuals have received at least 1 dose. Analysis from Our World in Data shows that the global daily doses administered reached a new record high of 41.3 million doses per day on June 27 before falling slightly yesterday. The trend continues to be largely driven by vaccination efforts in Asia. Our World in Data estimates that there are 1.8 billion vaccinated individuals (1+ dose) worldwide (23.8% of the global population). There are an estimated 834 million who are fully vaccinated (10.7% of the global population), although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.5 million cumulative COVID-19 cases and 601,506 deaths.
US Vaccination
The US has distributed 381 million doses of SARS-CoV-2 vaccines and administered 324 million, and it is administering approximately 614,000 doses per day. A total of 180 million individuals in the US have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 54.1% of the entire US population. Among adults, 66.1% have received at least 1 dose as well as 8.8 million adolescents aged 12-17. A total of 154 million individuals are fully vaccinated, which corresponds to 46.3% of the total population. Among adults, 57.0% are fully vaccinated, and 6.5 million adolescents aged 12-17 years are fully vaccinated.
VACCINE MIX & MATCH Researchers have posited that mixing multiple different vaccines (e.g., mRNA, viral vector) could yield improved immune response and ease the impact of supply shortages for specific products without sacrificing efficacy. Researchers in the UK, led by a team from the University of Oxford published results from a study that administered 1 dose each of the Pfizer-BioNTech and AstraZeneca-Oxford vaccines. The study, published in The Lancet (preprint), evaluated safety and efficacy data for 830 participants aged 50 years and older, divided into 8 groups. Half of the participants received the 2 doses of either the Pfizer-BioNTech (BNT/BNT) or AstraZeneca-Oxford (ChAd/ChAd) vaccine, administered 28 or 84 days apart. The other half received 1 dose of each vaccine, with half receiving the Pfizer-BioNTech and then AstraZeneca-Oxford (BNT/ChAd) and vice versa (ChAd/BNT) for the other group—also administered either 28 or 84 days apart. This article describes the results for only the participants who received the doses 28 days apart.
The researchers found that the anti-spike IgG levels following the ChAd/BNT regimen were non-inferior to the standard ChAd/ChAd regimen, but the immune response from the BNT/ChAd regimen was not as strong as for the BNT/BNT regimen. While the IgG response in the BNT/ChAd group fell short of the BNT/BNT group, the antibody levels were approximately 5 times higher than the ChAd/ChAd group. The researchers anticipate that the advantage among the groups that received BNT first will decrease in the groups who received the booster dose at 84 days, as the AstraZeneca-Oxford vaccine has been shown to generate an increased immune response with the later booster dose.
No serious adverse events were attributed to vaccination in any study group. This study evaluated only the IgG antibody response and did not estimate efficacy.
VACCINE PROTECTION DURATION One of the major limitations of the accelerated vaccine trial and regulatory review process for SARS-CoV-2 vaccines is that the duration of immunity remains uncertain. A study by researchers at several academic medical centers in the US, published in Nature, found evidence that immunity conferred by the Pfizer-BioNTech vaccine could potentially persist for years. The study included 41 fully vaccinated participants, including 8 who were previously infected with SARS-CoV-2, and blood and lymph node samples were collected before the second dose and up to 15 weeks after the first dose.
The researchers found that the vaccine results in the formation of “germinal centers” in lymph nodes, which serve as a “boot camp” where B cells—the cells that produce antibodies—can evolve to improve their function and recognize a variety of viral genetic sequences. This evolution provides the immune system with increased ability to recognize and respond to emerging variants. The germinal centers in study participants were still “highly active” at 15 weeks, much longer than germinal centers formed following seasonal influenza vaccination. While the study did not explicitly evaluate the Moderna vaccine, the researchers extrapolate their results broadly to mRNA-based vaccines. The researchers did not test the J&J-Janssen vaccine, which is a viral vector vaccine that only requires 1 dose, and it is unclear if that vaccine would generate a similar germinal center response in the absence of a booster dose.
It remains unclear exactly how long the germinal center activity continues for SARS-CoV-2 vaccines, but this initial evidence suggests that vaccine-conferred immunity may not wane as quickly as some have feared. If overall immunity remains high, it could mitigate the need for routine boosters, and if boosters are needed at all, they may be designed to combat specific variants as opposed to waning immunity.
COVID IMPACT ON US LIFE EXPECTANCY As we have covered previously, the morbidity and mortality associated with COVID-19 have resulted in decreased life expectancy* in the US, although the exact degree remains uncertain. Research recently provides evidence that these effects have disproportionately affected racial and ethnic minority populations.
*The underlying assumptions and methods used to estimate life expectancy can make it difficult to interpret the results, and alternative methods can yield markedly different estimates.
One study, published in The BMJ, estimates that life expectancy in the US fell 1.87 years between 2018 and 2020 (78.74 to 76.87 years)**, compared with an average of 0.22 years of life lost in 16 other high-income countries. Compared to peer countries—including the UK, Israel, France, Denmark, Switzerland, and South Korea—the US life expectancy was 1.88 years lower in 2010, and the gap increased to 3.05 years by 2018. Based on the 2020 estimates, the gap widened again to 4.69 years. The researchers also found disproportionate decreases among racial and ethnic minorities in the US. From 2018 to 2020, the decrease in life expectancy among Hispanic populations (3.25 years) was 2.4 times the decrease among non-Hispanic White populations (1.36 years), and the decrease among non-Hispanic Black populations (3.88 years) was 2.9 times higher. The reductions in life expectancy among Hispanic and non-Hispanic Black populations in the US were 18 and 15 times the average change in peer countries, respectively.
**Data from 2019 not included due to a dearth of available life table data in many countries. Estimates were generated manually for 2020 based on age-specific mortality data.
The authors of a study published in JAMA Network Open provide updated estimates to previous estimates of decreasing life expectancy in the US. The researchers estimated US life expectancy at birth from February 1-October 3, 2020, including more than 380,000 COVID-19 deaths. Race/ethnicity data was available for more than 99% of these deaths. The updated analysis estimates that COVID-19 reduced the overall 2020 US life expectancy by 1.31 years, from 78.74 years to 77.43 years. The Latino population had the largest decline (3.03 years), followed by the Black population (1.90 years). These declines were 3.2 and 2.0 times as large as the estimated decline among the White population (0.94), respectively. The researchers expect that COVID-19 deaths through April 2021 will continue to negatively impact US life expectancy, and Black and Latino communities likely will continue to face disproportionate impacts.
MENTAL HEALTH The COVID-19 pandemic has impacted the mental health of the general public, health care workers, and other frontline workers. To assess the pandemic’s mental health effects on public health workers, researchers from the CDC and colleagues collected data through an anonymous online survey conducted March 29-April 16, 2021. According to the results, 53% of 26,174 respondents employed by state, tribal, local, and territorial public health departments reported having at least one mental health symptom of depression, anxiety, post-traumatic stress disorder (PTSD), or suicidal ideation in the 2 weeks prior to completing the survey. The highest prevalences were reported among younger respondents, and transgender or nonbinary respondents, and the severity of symptoms increased as the proportion of time spent on COVID-19-related activities and time spent at work increased. Among respondents, the prevalence of reported PTSD symptoms were 10-20% higher than previously reported among healthcare workers, frontline workers, and the general public.
Equally alarming is the impact on the mental health of Americans of all ages. Emergency departments are witnessing an increasing proportion of patients with mental health crises, with more people visiting emergency rooms seeking help for overdoses and suicide attempts. These increases in adverse mental health symptoms are taxing already stressed healthcare systems, placing further pressure on frontline workers, and causing increased absenteeism, high turnover, lower productivity, and lower morale. Some experts warn that the true mental health impacts of the pandemic might not be known for years.
WHO MASKING GUIDANCE The WHO recently urged people fully vaccinated for SARS-CoV-2 to continue to wear masks in public, physically distance, and practice other COVID-19 prevention strategies in light of the rapidly spreading Delta variant of concern (B.1.617.2; VOC). The Delta variant, which has been identified in as many as 85 countries, is highly infectious and may be more likely to cause severe disease when compared with other SARS-CoV-2 variants. WHO Senior Advisor Dr. Bruce Aylward encouraged people who are vaccinated to continue to take precautions to avoid becoming part of a transmission chain. Even in countries with relatively high vaccination rates, including the UK and Israel, the Delta variant is causing an uptick in cases.
In the US, Delta variant prevalence has doubled over the last 2 weeks, and the variant is estimated to be responsible for 1 in 5 COVID-19 cases. US President Joe Biden on June 24 called the VOC a “serious concern,” warning those Americans who are not yet vaccinated are most at risk. The US CDC in May told fully vaccinated Americans they no longer need to wear masks indoors or physically distance themselves from other vaccinated individuals, and a CDC spokesperson gave no indication the current guidance will change. Some health experts encouraged US communities to tailor their masking guidance based on local vaccination and infection rates. However, various local recommendations could add confusion for some Americans who already cite questions over national guidance.
VACCINE PASSPORTS Travelers within the US have been required to wear masks on certain domestic modes of transportation since the implementation of a White House Executive Order issued in January. Now, a group of Republican US Senators have introduced a resolution urging the CDC to lift masking requirements for people using public transportation. The CDC requirements have been in place since February 1, and the US Transportation Security Administration in April extended the orders to be enforced through September 13.
But with no way to verify whether people have been vaccinated, making it safer for them to unmask, some health experts are calling on the US government to do more to encourage and promote the use of SARS-CoV-2 vaccine mandates and passports. So far, the White House has largely avoided the topics, saying private companies should decide whether to implement passport requirements or mandates. Recently, at least 153 employees of Houston Methodist were terminated or resigned after a federal judge dismissed a lawsuit brought by workers of the health system, one of the first in the nation to impose a vaccine mandate. Many Republican governors have banned mandates or passports in their states, saying that vaccination is a personal choice. Some employers may be waiting for SARS-CoV-2 vaccines to receive full US FDA approval before implementing vaccination mandates. Both Pfizer-BioNTech and Moderna have applied for full approval, and the FDA is expected to make decisions later this summer or in early fall.
VACCINATING US HOMELESS POPULATIONS Although vaccinating persons experiencing homelessness is challenging in terms of outreach and education, about half of US states prioritize people living in homeless shelters in their vaccination plans, according to the Kaiser Family Foundation. Persons experiencing homelessness are less likely to seek medical care and lack access to adequate transportation, information, and personal protective equipment, placing them at greater risk of adverse health outcomes, including for COVID-19. The US Department of Housing and Urban Development estimates that 580,000 people were homeless during its January 2020 point-in-time survey.
In Nashville, Tennessee, the city’s Metro Public Health Department collaborated with local organizations and partners to improve access to SARS-CoV-2 vaccination for all persons experiencing homelessness through community-based events and outreach. According to Metro Health, the city has vaccinated at least 60% of its population experiencing homelessness, higher than the rate among the general public. Similarly, non-profit groups and partner organizations in Phoenix, Arizona, are coordinating vaccination drives and establishing mobile clinics in an effort to meet people where they are.
EUA FOR ACTEMRA The US FDA last week issued Emergency Use Authorization (EUA) for Roche’s Actemra/RoActemra (tocilizumab), already approved to treat moderate-to-severe rheumatoid arthritis. While healthcare providers have been offering the intravenous Interleukin-6 (IL-6) receptor antagonist to hospitalized COVID-19 patients on a compassionate care basis, the EUA will help expand the drug’s use to more patients who might benefit. Under the EUA, Actemra/RoActemra can be used in hospitalized adults and children (2 years of age and older) who are receiving systemic corticosteroids and require supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation. In clinical trials, Actemra/RoActemra, in conjunction with corticosteroid treatment, reduced the risk of death through 28 days of follow-up, shortened the length of hospital stays, and reduced the need for mechanical ventilation. The FDA’s decision was informed by 4 clinical trials, particularly data from the RECOVERY and EMPACTA trials. Though Actemra/RoActemra is not authorized for outpatient use, the EUA adds another treatment to healthcare providers' toolkits to treat hospitalized COVID-19 patients.
AUSTRALIA The rapid global spread of the Delta variant of concern (B.1.617.2; VOC) has prompted renewed calls for lockdowns and other public health measures in countries worldwide. In Australia, which has had relative success in controlling the spread of SARS-CoV-2 within its borders, several major cities have reimposed lockdowns in response to a spike in COVID-19 cases caused by the Delta variant. These outbreaks have renewed questions over the dangers posed by strict hotel quarantines, which are the source of most community-spread cases, and the nation’s stuttering vaccination campaign, which has reached only 4.8% of adults, one of the lowest vaccination rates among high-income countries. Australia Prime Minister Scott Morrison met with state and territory leaders this week, agreeing to new measures to keep ahead of the Delta variant’s spread, as well as a no-fault indemnity plan for doctors administering SARS-CoV-2 vaccines. That plan effectively allows anyone under age 40 to receive the AstraZeneca-Oxford vaccine if they ask for it. Currently, the AstraZeneca-Oxford vaccine is recommended only for Australians over age 60 due to an increased risk of blood clots in younger individuals. That guidance has placed additional pressure on supplies of the Pfizer-BioNTech vaccine, which must be imported and is the only vaccine available for younger adults. Officials hope a return to stricter public health measures and a widening of vaccine access will help to control outbreaks as they arise.
OLYMPICS With less than 1 month before the 2020 Summer Olympic Games Opening Ceremony in Tokyo, a rise in daily COVID-19 cases in the country is prompting fears of another wave of infections and concerns over how Olympic organizers and Japanese authorities plan to host a safe event. This week, border control measures were put under a spotlight after an Ugandan Olympic team member tested positive for SARS-CoV-2 on June 26 upon arrival at the airport. While the team member was quarantined, officials allowed the rest of the team to proceed to the training center, where a second team member tested positive. Both team members tested positive for the Delta variant of SARS-CoV-2 (B.1.617.2), raising alarms over the variant’s increased transmissibility. On June 28, Japanese Prime Minister Yoshihide Suga pledged to strengthen border health controls in advance of more Olympic teams’ arrivals, but some health officials said the cases highlight how easily the controls can be breached. The government also has stepped up vaccination efforts, with the country last week administering more than 1 million doses a day. Still, only 11% of the population is fully vaccinated, and some wonder whether the accelerated pace will be enough to make a difference before the Olympic Games begin.
A recent poll showed that about 86% of those surveyed are concerned there will be an increase in COVID-19 cases following the Olympics, which are set to begin on July 23. Given the ongoing spread of the Delta variant and growing concern among the Japanese population, Japanese Emperor Naruhito gave a rare and unexpected remark of concerns over Japan hosting the Olympics. Though Emperor Naruhito does hold political power to stop the Olympics from proceeding, he is widely respected in Japan, and his comments put extra scrutiny on Olympics organizers to take as much care as possible.
by ponchi101 The MENTAL HEALTH section is very interesting. I would like to ask: are people in danger of mental health issues DUE to the pandemic (i.e. front line workers and jobs that expose you to it) and/or are they in danger of mental health issues due to collateral developments due to the pandemic (i.e. unemployment, loved ones that are more exposed, etc).
I don't know if they will be the same but, for example, unemployment will not go away after the pandemic is over. Many jobs will not come back.
by Suliso On a flip side lots of people have done well financially during the pandemic. Savings rates are sky high in many countries.
by ponchi101 Rolls Royce had their best year ever (2020)
The number of millionaires around the world increased.
Yet...
L. America has gone to hell.
And unemployment is very high in many countries.
I can't reconcile both things. Can't.
by Suliso I've not seen lots of suffering in Switzerland to be honest. I can't complain myself either, except for not being able to travel to see family for far longer than I'd prefer. Wish I could say I can afford a Rolls Royce
by ponchi101 A few days ago, I went to the supermarket, protected by my foreign-based vaccine (and wearing all my PPE). As I was coming back, I was surprised to hear a woman's voice singing Bizet's CARMEN (Habanera). I kept walking towards where the music was coming and came across a group of 4 trained musicians, on the street. They had set up a loudspeaker and where singing there, the ubiquitous pot for alms in the center.
My mental health issue is seeing so many people like this on the street. Coupled with the influx of Venezuelans that are spilling over the border because of the situation back home, I simply can't walk to the market without seeing 5-6 of such groups. I know that it is not only due to the pandemic (S. America has its systemic problems that were there prior to C19) but it is getting to be too much.
by ti-amie The late Bob Marley has a lyric that goes "a hungry man is an angry man". This was the first thing that came into my head when I read your post Ponchi. I hope not.
by mmmm8
ponchi101 wrote: ↑Tue Jun 29, 2021 10:15 pm
The MENTAL HEALTH section is very interesting. I would like to ask: are people in danger of mental health issues DUE to the pandemic (i.e. front line workers and jobs that expose you to it) and/or are they in danger of mental health issues due to collateral developments due to the pandemic (i.e. unemployment, loved ones that are more exposed, etc).
I don't know if they will be the same but, for example, unemployment will not go away after the pandemic is over. Many jobs will not come back.
It's both of the above and more, some of which is here to stay (people stuck together in small apartments having relationship issues, isolation, work stress from longer hours and/or balancing work and childcare, etc.)
by dryrunguy Yeah, the mental health sequalae associated with COVID are pretty complex. And it goes much deeper than the people who are miffed that they haven't been able to do all the things they want to do, which causes the sadz. That does not constitute a mental health crisis, though you wouldn't know that by some of the people you see going on and on about how their "rights" are being trampled on, blah blah blah...
Of course, you have the grief associated with the loss of loved ones.
Some literature has been published about the impact of isolation on young girls. Other studies have focused on video games among boys.
Then we have the psychiatric and neurological complications of long COVID.
Some of it MUST be related to economic distress.
Cancer diagnoses are shooting through the roof because people stopped going to doctors or having screenings because of COVID.
The opioid crisis is no better than it was; if anything, it's worse. And that crisis continues to be exacerbated in states and regions with increased access to firearms (economic distress fits here, too).
It goes on and on.
::
Suliso posted something earlier that piqued my attention, and I've read the same thing about some folks in the U.S. So I'll ask:
Who the hell are these people who have accumulated significant financial savings during COVID? I'm not talking about the uber-rich. I'm talking about ordinary folks. I keep hearing about all these people who are anxious to spend their surplus savings accumulated during COVID on vacations, etc.... Who ARE these people? I can't name a single person I know who would fall into this category. I am a 2%er, and I'm not even close to falling into this category. So, if not me, then who?
by Suliso Me for example. My income has risen about 10% since the pandemic began, but spending has plunged. I'm nowhere near the upper 2% by income in my country, the upper 20% possibly.
by mmmm8
dryrunguy wrote: ↑Wed Jun 30, 2021 4:43 am
Suliso posted something earlier that piqued my attention, and I've read the same thing about some folks in the U.S. So I'll ask:
Who the hell are these people who have accumulated significant financial savings during COVID? I'm not talking about the uber-rich. I'm talking about ordinary folks. I keep hearing about all these people who are anxious to spend their surplus savings accumulated during COVID on vacations, etc.... Who ARE these people? I can't name a single person I know who would fall into this category. I am a 2%er, and I'm not even close to falling into this category. So, if not me, then who?
There are a few potential cases:
- People who saved on commuting/gas, expenses (going out, social activities, gym memberships, etc.) by working from home. I would say that applies to me; on average, my spending went down. I put the savings towards debt, so no pondering of what to do with the money.
- People who had more time while working from home or were furloughed/laid off and started actively investing/day trading (while surely a miniscule portion, I actually know quite a few of such people) and got lucky/were good at it.
- In related, people who invested a bit of money when the market crashed last spring and then watched it grow.
- Self-employed people whose operating costs were reduced in an online environment (i.e. tutors, psychologists, consultants, etc.)
by ponchi101 I would say it would be more general. IF you kept your job, you were certainly able to save.
by Suliso
ponchi101 wrote: ↑Wed Jun 30, 2021 1:54 pm
I would say it would be more general. IF you kept your job, you were certainly able to save.
Exactly. I used to spend ca 20% of post tax income on various entertainment (eating out, events, lots of travel etc). For the last year 80% of that has gone to savings/investment instead. Fortunately I didn't have any debt before the pandemic.
by JazzNU
dryrunguy wrote: ↑Wed Jun 30, 2021 4:43 am
Suliso posted something earlier that piqued my attention, and I've read the same thing about some folks in the U.S. So I'll ask:
Who the hell are these people who have accumulated significant financial savings during COVID?
I think @mmmm8 captured almost everything I was thinking, but I'll add to it a bit.
Clothes. How much have you honestly been shopping for clothes in the last 18 months? I've gotten some new yoga pants and loungewear that double as my "work clothes" and not much else because who the **** am I trying to impress or look presentable for right now?
And for women in particular, at least in my group of family and friends - spending much, much less on accessories and makeup - not many designer bags, shoes, sunglasses, earrings, and most kinds of makeup being bought in the last year and that alone could save hundreds but more likely thousands for many. Why would you spend on this stuff when you've got nowhere to go? Ride out with what you've got and maybe buy something new this summer or fall.
For example, I found a gently used designer bag of a version I used to own for like $50 on Poshmark that I used for most of the pandemic when one of the straps on my last purse was starting to fail. Not the norm for me because it doesn't show as well, but no biggie in the last year. My sister bought a couple of nice necklaces so she can look good from the neck up on Zoom, but next to nothing else in terms of an accessory.
Also, for a period of time, you couldn't spend to get your hair, nails, or feet done even if you wanted to. Easily hundreds saved right there alone for so many. Looking decent for women can be expensive.
The people I've been seeing during the pandemic, they know and love me and will put up with whatever kind of mess I might look like on a given day.
by Suliso Obviously the key to all this is as ponchi said - job not affected by the pandemic and also no one close got seriously ill.
by ti-amie I hate reading these stories of covidiocy.
by Suliso Died as a free man
by ti-amie
Suliso wrote: ↑Thu Jul 01, 2021 9:11 pm
Died as a free man
by JazzNU I'm so confused by those that get it, are sick to the point of being hospitalized and still downplaying the disease. If you know anyone that's gotten covid to the point of being hospitalized, if they are lucky enough to be alive, they will tell you, there is no mistaking the two.
Also, these people that say it's the flu. I'd like them to name even 3 people they personally know who have been hospitalized by the flu or die from it. You typically have to know healthcare professionals to know that many, and even then, not many can name someone who has died from flu complications.
by ponchi101
JazzNU wrote: ↑Thu Jul 01, 2021 10:22 pm
I'm so confused by those that get it, are sick to the point of being hospitalized and still downplaying the disease. If you know anyone that's gotten covid to the point of being hospitalized, if they are lucky enough to be alive, they will tell you, there is no mistaking the two.
Also, these people that say it's the flu. I'd like them to name even 3 people they personally know who have been hospitalized by the flu or die from it. You typically have to know healthcare professionals to know that many, and even then, not many can name someone who has died from flu complications.
(Cognitive dissonance)3
(the people you talk about)
by Deuce I hate to rain on the American 're-opening everything as if the pandemic is finished' parade, but...
(Actually, I don't hate to rain on this parade, as more information like this may well save some lives...)
by ponchi101 I wish we were that relevant.
The 25 people that come to this forum have all been vaccinated or plan to. Our lives are saved, except for that news of the Gulf of Mexico being on fire
(Putting you on. txs for the link)
by dryrunguy A sidebar that is somewhat related to my previous post here.
A few weeks ago, my company had an All Hands Meeting (virtually, of course). The last topic discussed was current plans for returning staff to headquarters. It will happen in phases. Executive leadership, HR, contracts, and project management personnel go back first. Then additional staff. Many staff like me will continue to work remotely (but there will be many more staff working remotely than before COVID).
When asked if staff will be required to vaccinated before they can return to the office, our president said, "At this time, there are no plans to require staff to be vaccinated."
I have debated that corporate policy back and forth in my head ever since. I was also struck by a statement made by a colleague of mine this past Monday during our Business Development staff meeting. She said, and I paraphrase: "I'll never sit in a conference room again."
::
I expect that courts will eventually decide this, at least to some degree, but I'll ask you all the question: Can or should companies require staff to be vaccinated before returning to work? I'm not asking how we FEEL about it. I'm asking about the LEGALITY of it. I ask because the first thought that popped into my head when I read about the firefighters at the fallen condo building was, "How the hell do we have first responders who are NOT vaccinated?"
by ponchi101 Yes. That is the entire base of a democracy. While individual freedoms are paramount for a democracy, some public issues will trump those freedoms. The vaccines have proven to be effective and innocuous as far as creating side effects. Therefore, in this case the needs of the many (the society) trump the needs of the few (the individual).
There is no difference here than the requirements set in almost all democracies regarding vaccinations of small children prior to go to school.
There is a moment in which the answers are not "well, let's split this down the middle". Sometimes, one side is simply right and the other simply wrong. That is the case right now. If you do not want to be vaccinated, then you are admitting to be outside of society. So go.
by ti-amie Yes. All you need is one of the unvaxxed to cause a major breakout. Imagine the lawsuits that would follow.
Your coworker is 100% correct too. Never say never they say but in this case I would say never too.
by ti-amie
by ti-amie
by ti-amieChris Whitty suggests guidelines for use of masks after 19 July
England’s medical chief gives three situations in which it would be important to wear face covering
Prof Chris Whitty, England’s chief medical officer, has set out three simple personal guidelines for when to continue wearing face masks after the Covid restrictions have been lifted.
Boris Johnson and Whitty were asked at Monday’s Downing Street press conference what circumstances they would still use face coverings after 19 July.
Johnson said he wanted to move away from “government diktat”. But then Whitty offered a three-part rule of thumb for continuing to wear a mask: in crowded indoor spaces; when required to by an authority; or to make someone else feel comfortable.
He said these situations were all particularly important at a time when “the epidemic is significant and rising”.
Whitty said: “The first is in any situation is indoors and crowded, or indoors with close proximity to other people. And that is because masks help protect other people.”
He added: “The second situation is if I was required to by any competent authority … And the third reason is if someone else was uncomfortable if I did not wear a mask – as a point of common courtesy.”
The chief scientist, Sir Patrick Vallance, endorsed the approach. He added: “Masks are most effective at preventing somebody else catching the disease from you, and they have some effect to prevent you catching it.”
He also played down fears that the upcoming European Championship semi-final at Wembley would be a super-spreading event. Vallance said: “It’s very often not the big outdoor environments, it’s the indoor environments with crowded spaces that become the risk of spreading, and that’s where most super-spreading events have occurred.”
Whitty’s three rules of thumb for continued mask wearing come after several cabinet ministers, including Robert Jenrick and George Eustice, have indicated they will not be wearing masks after restrictions are lifted.
Johnson said his own mask wearing “will depend on the circumstances”. He said: “What we’re trying to do is move from universal government diktat, to rely on people’s personal responsibility.
“Clearly there’s a big difference between travelling on a crowded tube train and sitting late at night in a virtually empty carriage on the main railway line. So what we want to do is for people to exercise their personal responsibility, but to remember the value of face coverings both in protecting themselves, and others.”
dryrunguy wrote: ↑Sun Jul 04, 2021 4:22 pm
I expect that courts will eventually decide this, at least to some degree, but I'll ask you all the question: Can or should companies require staff to be vaccinated before returning to work? I'm not asking how we FEEL about it. I'm asking about the LEGALITY of it. I ask because the first thought that popped into my head when I read about the firefighters at the fallen condo building was, "How the hell do we have first responders who are NOT vaccinated?"
Legally they are good to go. EEOC has been perfectly clear that employers can require vaccinations. Lawsuits have been brought in multiple places. A big one in Texas was dismissed in favor of the employer.
Personally, I can tell you the hospital my mom worked at has required the flu vaccine for the last 8 years or so. They put out announcement after announcement they'd be required, they held clinics on site to administer them, gave warning after warning after warning that they'd need to get them or be fired. Some people didn't take it seriously and were surprised when they got that pink slip. No one was given a pass without a signed medical or religious exemption in line with customary ADA regulations.
If you think about this it makes sense though. Many employers require a tetanus shot and other immunizations upon hiring and haven't faced any blowback, they check when they are doing the onboarding health screening. Again at my mom's hospital, it's strange that there were a few dozens didn't take it seriously since they already required current tetanus, MMR, and a few others before they added the flu on. People really seem to have a brain cramp where previous vaccinations they've had for decades are concerned and newer ones it seems.
A good deal of employers are holding off on requiring the covid vaccine while it is under an EUA and waiting for the full review. Many are apparently set to require Pfizer or Moderna the moment whichever gets the earliest full approval. Now those same employers that are currently scared to make the hard call now may abandon that plan as the Delta variant spreads. And as @ti said, there will be fallout, and they don't want to deal with any of it, especially it leading to vaccinated employees giving it to their kids, which is the most at risk group by a mile.
In terms of firefighters - their vaccination rates haven't been great, lower than almost all other essential workers, at
least that was the case a couple of months ago.
by Deuce And... directly from the 'You can't make this stuff up' file...
She was protesting against the holding of the Olympics during the pandemic, and with only 14% of Japanese people fully vaccinated.
I applaud her - though her chosen method was neither very practical nor effective.
by ti-amie
by Suliso We in Switzerland reached the lowest point about 2 weeks ago. Now it's going up again (+63% from a week ago). I think this is inevitable (in US too), the question is how much protection will be provided to the most vulnerable population. Here, for example, full vaccination rate for 70+ is 81%. Vaccination for that group is almost over (remaining don't want to), for other age groups still ongoing strongly.
by dryrunguy Of all people, the Governor of West Virginia summed it up best recently. As quoted in this morning's NY Times e-newsletter, anyone who is not vaccinated has willingly entered "the death lottery"...
by JazzNU
dryrunguy wrote: ↑Wed Jul 07, 2021 7:23 pm
Of all people, the Governor of West Virginia summed it up best recently. As quoted in this morning's NY Times e-newsletter, anyone who is not vaccinated has willingly entered "the death lottery"...
Of all people indeed. The man is damn near a caricature.
by ti-amie
by dryrunguy And I'm perplexed by Mitch McConnell, totally perplexed.
by Suliso
dryrunguy wrote: ↑Thu Jul 08, 2021 10:29 pm
And I'm perplexed by Mitch McConnell, totally perplexed.
You should meet for an afternoon tea and be perplexed together.
Pfizer to seek FDA authorization for booster of COVID-19 vaccine
BY PETER SULLIVAN
Pfizer and BioNTech announced Thursday that they plan to seek authorization from the Food and Drug Administration (FDA) for a third dose of their COVID-19 vaccine, saying it would provide even stronger protection.
In a statement released Thursday afternoon, the companies said they have seen "encouraging data" from an ongoing trial of the booster shot, adding that it provides levels of neutralizing antibodies five to 10 times higher, when administered six months after the second dose. The companies plan to submit data "in the coming weeks."
It will be up to U.S. regulators — the FDA and the Centers for Disease Control and Prevention — whether to recommend a third dose.
Some experts have cautioned that vaccine makers have a financial incentive to develop booster shots and for the government to invest in more doses.
U.S. health officials have thus far said it is not clear whether a booster shot is needed.
Anthony Fauci, the government's top infectious diseases expert, reiterated earlier Thursday that two shots of the Pfizer and Moderna vaccines are protective even against the delta variant.
However, Pfizer pointed to data from Israel.
"As seen in real world data released from the Israel Ministry of Health, vaccine efficacy in preventing both infection and symptomatic disease has declined six months post-vaccination, although efficacy in preventing serious illnesses remains high," Pfizer said.
"Based on the totality of the data they have to date, Pfizer and BioNTech believe that a third dose may be beneficial within 6 to 12 months following the second dose to maintain highest levels of protection," the companies said.
Pfizer also said that it is preparing to begin clinical trials in August of a modified vaccine specifically targeted at the delta variant, in case it is needed. The company said, though, that a third dose of the original vaccine could be a better course.
After Pfizer's announcement, the FDA and the CDC released a joint statement on Thursday night downplaying the need for a booster shot.
"Americans who have been fully vaccinated do not need a booster shot at this time," the agencies said, while adding that they are engaged in a "science-based, rigorous process," to determine if one will be needed.
The agencies again stressed that the current vaccine regimens are effective. "People who are fully vaccinated are protected from severe disease and death, including from the variants currently circulating in the country such as Delta," the agencies said.
by Suliso Not something I had thought about before... I guess getting ill, but not dead, really is a necessity in childhood.
New Zealand children falling ill in high numbers due to Covid ‘immunity debt’
Doctors say children haven’t been exposed to range of bugs due to lockdowns, distancing and sanitiser and their immune systems are suffering
New Zealand hospitals are experiencing the payoff of “immunity debt” created by Covid-19 lockdowns, with wards flooded by babies with a potentially-deadly respiratory virus, doctors have warned.
Wellington has 46 children currently hospitalised for respiratory illnesses including respiratory syncytial virus, or RSV. A number are infants, and many are on oxygen. Other hospitals are also experiencing a rise in cases that are straining their resources – with some delaying surgeries or converting playrooms into clinical space.
RSV is a common respiratory illness. In adults, it generally only produces very mild symptoms – but it can make young children extremely ill, or even be fatal. The size and seriousness of New Zealand’s outbreak is likely being fed by what some paediatric doctors have called an “immunity debt” – where people don’t develop immunity to other viruses suppressed by Covid lockdowns, causing cases to explode down the line.
Epidemiologist and public health professor Michael Baker used the metaphor of forest brushfires: if a year or two have passed without fire, there is more fuel on the ground to feed the flames. When a fire finally comes, it burns much more fiercely. “What we’re seeing now is we’ve accumulated a whole lot of susceptible children that have missed out on exposure – so now they’re seeing it for the first time,” Baker said.
The “immunity debt” phenomenon occurs because measures like lockdowns, hand-washing, social distancing and masks are not only effective at controlling Covid-19. They also suppress the spread of other illnesses that transmit in a similar way, including the flu, common cold, and lesser-known respiratory illnesses like RSA. In New Zealand, lockdowns last winter led to a 99.9% reduction in flu cases and a 98% reduction in RSV - and near-eliminated the spike of excess deaths New Zealand usually experiences during winter.
“This positive collateral effect in the short term is welcome, as it prevents additional overload of the healthcare system,” a collective of French doctors wrote in a May 2021 study of immunity debt. But in the long term, it can create problems of its own: if bacterial and viral infections aren’t circulating among children, they don’t develop immunity, which leads to larger outbreaks down the line.
“The lack of immune stimulation… induced an “immunity debt” which could have negative consequences when the pandemic is under control and [public health intervientions] are lifted,” the doctors wrote. “The longer these periods of ‘viral or bacterial low-exposure’ are, the greater the likelihood of future epidemics.”
New Zealand has reported nearly 1,000 RSV cases in the past five weeks, according to the Institute of Environmental Science and Research. The usual average is 1,743 over the full 29-week winter season. Australia is also experiencing a surge, with overcrowded Victoria hospitals also hit by unusually high rates of RSV.
Peaks like the current outbreak don’t necessarily mean the country will have more RSV cases overall, Baker says – it may just be that all the cases are grouped together, instead of spread out over several years. But even that can cause major problems. “If you get a big peak it can overwhelm your health system, or put real pressure on it, which we’re seeing with RSV,” Baker said.
The current outbreak is already stretching New Zealand’s hospitals. At Middlemore hospital in Auckland, a playroom has been converted into a clinical space with 11 special care baby cots. Health boards in Auckland and Canterbury have postponed surgeries to divert resources into children’s wards. A number of hospitals have asked children under 12 not to visit, to try to avoid spreading the virus. John Tait, chief medical officer for the Wellington area’s district health boards said the region had 46 children hospitalised, including two in intensive care. Those numbers were “continually changing as patients are discharged and others admitted,” he said.
Usually, people experience near-universal exposure to RSV as children, Baker said, with most exposed in their first year of life.
“If you remove that exposure for a period then you will have a bigger cohort of unexposed children, and therefore – as you can see we have happening at the moment – it can sustain a much bigger outbreak when they are eventually exposed to the virus.”
While RSV is a common cause of winter hospitalisation of children, elderly people and people with suppressed immune systems are also vulnerable. New Zealand’s director-general of health, Dr Ashley Bloomfield, said he was “certainly concerned about the sharp surge in RSV cases”.
“We had very little RSV last year,” he said. “There’s some speculation that [the current outbreak] may be partly exacerbated by the fact we didn’t have any last year and so there is a bigger pool of children who are susceptible to it.”
by Deuce ^ Interesting angle on the collateral damage of trying to avoid the COVID-19 virus. ^
by Suliso Vaccination situation in Switzerland by age groups as of today. We have no serious regional differences.
by ponchi101 My grandniece, the one born very prematurely, is in the hospital with RSV. She is in the NICU, because of her history (born at 5 months, 3 weeks). She is fine, and will be back home tomorrow, but the doctor told my niece that there is an outbreak of the disease around the USA.
I was recently wondering if the newer generations are so protected that their immune systems are not being "trained" to handle viruses and other diseases. I always joke "heck, we used to drink water from the garden hose, and our first kiss was with a dog".
I know, me and my bad jokes.
by JazzNU
ponchi101 wrote: ↑Fri Jul 09, 2021 5:02 pm
My grandniece, the one born very prematurely, is in the hospital with RSV. She is in the NICU, because of her history (born at 5 months, 3 weeks). She is fine, and will be back home tomorrow, but the doctor told my niece that there is an outbreak of the disease around the USA.
I was recently wondering if the newer generations are so protected that their immune systems are not being "trained" to handle viruses and other diseases. I always joke "heck, we used to drink water from the garden hose, and our first kiss was with a dog".
I know, me and my bad jokes.
Happy to hear your grandniece will be fine and back home soon.
Don't get me started on newer generations and protections. I'm not old and the change has been dramatic in the last two decades, nothing resembling how I grew up. I think we can start with food. If you never or very rarely eat anything from an animal, my guess is yeah, you're cutting off exposure to build up immunity. I laugh at every commercial of an athlete promoting some new nut milk. We'll be getting them during the Olympics again I'm sure. What did you drink day after day for years on end as a toddler, child, and teenager is my question? Those bones aren't built with nut milk is my guess.
by Deuce Some myths never die... sigh...
I haven't drunk milk from an animal in 40 years, and I've never broken a bone in my life (and I've been, and am, much more physically active than most people).
I haven't consumed any animal products in those 40 years, and am more fit and healthy than the vast majority of people my age.
Again - humans are the only species who voluntarily drink milk from another species. Cow's milk is naturally meant for baby cows, quite obviously, just as human mother's milk is naturally meant for human babies.
by ti-amie Being vegan can be very expensive and many can't afford to live that lifestyle even if they want to. Of course now you get sticker shock every time you shop for food.
There are other sources of calcium though. Do you take a lot of supplements?
by Suliso Humans are natural predators too if you want to go all natural. Our bodies are meant to metabolize animal products there as say a cow can't do it.
by Deuce
ti-amie wrote: ↑Fri Jul 09, 2021 7:08 pm
Being vegan can be very expensive and many can't afford to live that lifestyle even if they want to. Of course now you get sticker shock every time you shop for food.
There are other sources of calcium though. Do you take a lot of supplements?
Being vegan is considerably less expensive than being a meat eater.
It's only expensive if you go for the fancy, newfangled (and mostly fraudulent) stuff. If you eat simply - fruits, vegetables, various pasta, rice, quinoa, etc., it's considerably less expensive than is buying meat. That being vegan is expensive is another myth - likely begun by the meat and dairy industries...
Suliso wrote: ↑Fri Jul 09, 2021 7:09 pm
Humans are natural predators too if you want to go all natural. Our bodies are meant to metabolize animal products there as say a cow can't do it.
I don't see anything natural in the manner in which animal foods are produced today. Factory farms and slaughterhouses, having to pasteurize milk, etc. are as unnatural as can be - so the argument that eating animal products is part of the natural process is easily dismissed today. And that's not even mentioning the very inherent cruelty and suffering of the animals in those places.
“One farmer says to me, 'You cannot live on vegetable food solely, for it furnishes nothing to make bones with;' and so he religiously devotes a part of his day to supplying his system with the raw material of bones; walking all the while he talks behind his oxen, which, with vegetable-made bones, jerk him and his lumbering plow along in spite of every obstacle.” ~ Henry Thoreau.
by dryrunguy Here's the latest Situation Report. NOT GOOD.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 185 million cumulative cases and 4.0 million deaths worldwide as of 4:30am EDT on July 9. On July 8, the global cumulative mortality surpassed 4 million deaths:
1 death to 1 million- 251 days
1 to 2 million- 114 days
2 to 3 million- 89 days
3 to 4 million- 89 days
Global weekly incidence increased for the second consecutive week, up 3.8% from the previous week. Global weekly mortality, however, continues to decrease down to its lowest point since late October 2020—a decrease of 6.5% compared to the previous week.
Analysis by Reuters indicates that 19 countries* are currently reporting a daily incidence that is 90% or greater of their highest peak. While these countries represent nearly all of the WHO regions—with the exception of Europe—they tend to be clustered in smaller regional areas. In the Americas, there are 3 countries in Central America and the Caribbean. Cuba, Honduras, and Guatemala are all currently reporting their record high daily incidence to date. In Africa, Tunisia (at its peak) is the only country in the northern region, but there are 5 countries in sub-Saharan Africa. Liberia, Mozambique, South Africa, and Zimbabwe are all reporting record highs, and Rwanda is at 99% of its record. In the Eastern Mediterranean region, Iraq and Kuwait are both reporting 97% of their record highs. The South-East Asia region accounts for a third of the countries globally that are currently exceeding 90% of their highest peak, stretching from Bangladesh to Indonesia. Bangladesh, Indonesia, Myanmar, Thailand, and Vietnam are all at their highest peak. Additionally, Malaysia is at 92% of its record high, and Cambodia is at 92%. Fiji (at its peak) is the only country in the Western Pacific region.
*In addition to WHO countries, Reuters lists the British Virgin Islands at 91% of its highest peak.
Among these countries, most epidemics are continuing to accelerate. In fact, all 19 countries are reporting positive relative changes over the past 2 weeks, and Liberia (-34%) is the only country reporting a negative trend over the past week. Notably, the daily incidence has more than doubled over the past 2 weeks in nearly half of these countries, including Fiji (+201%), Zimbabwe (+276%), Mozambique (+375%), and Myanmar (+403%). The surges in most of these countries began between mid-May and mid-June, although a few are exhibiting long-term increasing trends. It appears that most of the countries with longer-term increases—including Cambodia, Guatemala, Honduras, Iraq, and Malaysia—reported relative peaks in April or May and then declined slightly before their current surges. A number of these countries were reporting fewer than 100 new cases per day as recently as late June, with some as low as single-digits in the weeks and months prior. But as we have discussed previously, even countries with low daily incidence can be at risk for rapidly accelerating epidemics if transmission is not contained. Currently, Liberia is the only one of these countries reporting fewer than 100 new cases per day, and Cambodia, Fiji, and Rwanda are the only other countries reporting fewer than 1,000.
Global Vaccination
The WHO reported 3.03 billion doses of SARS-CoV-2 vaccines administered globally as of July 8. The WHO reports a total of 1.23 billion individuals received at least 1 dose and 552 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered is falling rapidly from the record high of 43.1 million doses per day on June 27, now down to 31 million. The trend continues to be largely driven by vaccination efforts in Asia, which is, in turn, driven by China. Our World in Data estimates that there are 1.94 billion vaccinated individuals worldwide (1+ dose; 24.8% of the global population). There are an estimated 923 million who are fully vaccinated (11.8% of the global population), although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.6 million cumulative COVID-19 cases and 603,958 deaths. Daily incidence has increased over the past several weeks, up from a low of 11,281 new cases per day on June 20 to 14,884 on July 7, an increase of 32% over that period—including an increase of 16% over the past week. Daily mortality continues to decline, although it increased slightly on July 7. It is likely that reporting delays over the Independence Day holiday weekend are impacting the incidence and mortality figures; however, some states have transitioned from daily to weekly reporting, so the degree of impact may differ compared to earlier in the pandemic.
The CDC published updated genomic surveillance data, including Nowcast projections for June 20-July 3. In the most current official data, the Delta variant (B.1.617.2) reached 30.4% of new cases for June 6-19. The Delta variant remains #2 behind the Alpha variant (B.1.1.7; 44.2%); however, its relative proportion continues to increase rapidly, tripling from the previous 2-week period (10.1%). In the CDC’s projection, Delta is not only the dominant variant, but it accounts for more than half of all new cases in the June 20-July 3 period (51.7%). The prevalence of the Alpha variant continues to decrease steadily, down from a high of 69.9% for April 25-May 8 to 28.7% in the Nowcast projection. The Gamma variant (P.1) is now beginning to decrease slowly as well, down from a high of 11.1% for May 23-June 5 to 8.9% in the projection period. At the regional level, Delta variant prevalence is projected to exceed 50% in 5 of the 10 HHS regions, including 74.3% in Region 8 (Mountain) and 80.7% in Region 7 (Central).
US Vaccination
The US has administered 332 million cumulative doses of SARS-CoV-2 vaccines, and it is administering approximately 484,000 doses per day. A total of 183 million individuals in the US have received at least 1 dose, equivalent to 55.2% of the entire US population. Among adults, 67.3% have received at least 1 dose as well as 9.4 million adolescents aged 12-17. A total of 158 million individuals are fully vaccinated, which corresponds to 47.7% of the total population. Among adults, 58.5% are fully vaccinated, and 7.2 million adolescents aged 12-17 years are fully vaccinated.
MIX & MATCH VACCINES This week, Germany became one of the first countries to strongly recommend that anyone who received the AstraZeneca-Oxford vaccine for their first dose should receive a dose of either the Pfizer-BioNTech or Moderna vaccines for their second dose. The German Standing Committee on Vaccination (STIKO) said those who received a first dose of the AstraZeneca-Oxford vaccine "should get an mRNA vaccine as their second dose, regardless of their age." Canada's National Advisory Committee on Immunization made a less strongly worded recommendation last month when it said "an mRNA vaccine is now preferred as the second dose for individuals who have received a first dose of AstraZeneca/COVISHIELD vaccine." Leaders of both countries have set an example for vaccine mixing, as German Chancellor Angela Merkel and Canada Prime Minister Justin Trudeau received the AstraZeneca-Oxford vaccine for their first dose, followed by a second dose of Moderna. The European Medicines Agency (EMA) has not yet made a definitive recommendation on mixing SARS-CoV-2 vaccines.
In addition to a study recently published in The Lancet that demonstrated sufficient immune response following mixed doses of the AstraZeneca-Oxford and Pfizer-BioNTech vaccines, 2 German studies (both preprint) reported similar findings. The first study included 340 healthcare workers and found similar immune responses among participants who received 2 doses of the Pfizer-BioNTech vaccine and those who received a prime dose of the AstraZeneca-Oxford vaccine followed by a booster dose of the Pfizer-BioNTech vaccine. The second study included 216 participants who received either 2 doses of the AstraZeneca-Oxford vaccine, 2 doses of the Pfizer-BioNTech or Moderna vaccines, or a prime dose of AstraZeneca-Oxford followed by a booster dose of one of the mRNA vaccines. The immune responses in the heterologous group were similar to those who received 2 doses of the mRNA vaccines and better than those who received 2 doses of the AstraZeneca-Oxford vaccine. While these studies are small and evaluate immune response rather than vaccine efficacy against infection or disease, they do provide further evidence that using an mRNA vaccine as the second dose can stimulate sufficient immune response and potentially even improve on 2 doses of the AstraZeneca-Oxford vaccine.
DELTA VARIANT VACCINE EFFICACY Researchers continue to evaluate how well available SARS-CoV-2 vaccines protect against the Delta variant (B.1.617.2), which is driving outbreaks in both vaccinated and unvaccinated communities in several countries and is now the dominant variant in the US. To date, studies show the most widely used shots offer strong protection against severe disease and hospitalization, although protection may be reduced for infection. On July 5, Israel’s Ministry of Health released results of a study examining the effectiveness of the Pfizer-BioNTech vaccine against all circulating variants, including Delta, for the past month beginning June 6. The ministry noted a “marked decline” in the vaccine’s effectiveness in preventing infection (64%) and symptomatic illness (64%). While this rate is lower than the vaccine’s effectiveness prior to circulation of the Delta variant in Israel (95%), and lower than other studies from Britain (88%), Scotland (79%), and Canada (87%), the Israeli study maintained the vaccine was 93% effective in preventing serious illness and hospitalization. Israeli officials cautioned that the study data are preliminary, based on highly localized outbreaks, and potentially had other methodological weaknesses. A Pfizer spokesperson declined to comment specifically on Israel’s data but confirmed other research shows its vaccine is effective against all variants, including Delta, although at a reduced rate.
Pfizer-BioNTech on July 8 announced it plans to seek authorization in the US and Europe for a third booster dose of its vaccine based on “encouraging data.” However, some experts contend there is no indication for a booster or third dose of an mRNA vaccine, and the US FDA and US CDC published a joint statement saying people who have been fully vaccinated do not need a booster shot at this time. The agencies said they will continue to monitor ongoing studies and are “prepared for booster doses if and when the science demonstrates that they are needed.” Pfizer-BioNTech also announced they plan to begin trials as early as next month of a vaccine targeted specifically at Delta, although it is not clear whether this shot would be intended as a booster or an additional, separate vaccination.
As we previously reported, vaccine efficacy is reduced following 1 dose of mRNA or viral vector vaccine versus the full 2-dose schedule. On July 8, researchers from France published a peer-reviewed report in Nature showing a single shot of a 2-dose vaccine (Pfizer-BioNTech or AstraZeneca-Oxford) “barely” offered protection against the Delta variant. Notably, J&J-Janssen recently announced preliminary data demonstrating its single-shot SARS-CoV-2 vaccine generates a strong immune response against all highly prevalent variants for at least 8 months, including Delta. Little is known about the effectiveness of the Chinese-produced vaccines from Sinopharm and Sinovac Biotech Ltd. against Delta, although the companies say they are studying variants. Research and real-world data consistently show that people who are unvaccinated or not fully vaccinated remain at an increased risk of infection and more severe disease, underlining the importance of fully vaccinating as many people as possible, particularly in the face of Delta and other emerging variants of interest and concern.
CUBAN VACCINES Cuban pharmaceutical company BioCubaFarma announced preliminary efficacy estimates for a second candidate SARS-CoV-2 vaccine. The company issued a press release indicating a regimen of its 2-dose Soberana 02 vaccine plus a booster of Soberana Plus demonstrated 91.2% efficacy against symptomatic COVID-19 over a 56-day period in a Phase 3 clinical trial. According to the press release, the trial was conducted in 8 municipalities in the capital of Havana, but it does not provide further details, including the number of participants. A clinical trial of the same vaccine regimen is already underway in children and adolescents. In June, BioCubaFarma announced that another vaccine candidate, Abdala (also a 3-dose regimen), demonstrated 92.3% efficacy in a Phase 3 trial. To our knowledge, the full trial data have not yet been released publicly nor subjected to peer review, but efficacy estimates greater than 90% would put both of Cuba’s vaccines in the same category as others in wider use around the world, including the Pfizer-BioNTech, Moderna, and Sputnik V vaccines. Cuba has a well-established vaccine development sector, which produces approximately 80% of its vaccines as well as some for export.
VACCINE EFFICACY IN IMMUNOSUPPRESSED POPULATIONS The Coalition for Epidemic Preparedness Innovations (CEPI) announced it will co-fund a study to assess immune response to SARS-CoV-2 vaccines in patients aged 18 or older who are immunocompromised or who take immunosuppressive medications following an organ transplant. CEPI will provide $3.1 million alongside $3.6 million in funding from several Norwegian health organizations, including Oslo University Hospital, which will lead the trial. Large trials of vaccine efficacy in immunosuppressed populations have been limited, despite this subpopulation having an increased risk of developing severe COVID-19. The study aims to recruit at least 6,000 patients and 10,000 healthy participants who have received 2 doses of vaccines that are included in the Norwegian National Corona Immunization Program (currently Pfizer-BioNTech and Moderna). The primary goal of the trial is to assess the level of adaptive immune responses in these populations. Participants in the intervention arm of the study who have low or no immune response to vaccination will be offered a booster dose and monitored. Researchers also plan to evaluate the effect of immunosuppressive medications on immune response to vaccination and associated demographic and immunologic indicators.
VACCINATION & HEART INFLAMMATION The US CDC’s Advisory Committee on Immunization Practices (ACIP) on July 7 published an update on the use of mRNA SARS-CoV-2 vaccines following its review of reports of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the thin tissue surrounding the heart) among some vaccine recipients. ACIP concluded that the benefits of vaccination (prevention of COVID-19 disease and associated hospitalization and death) outweigh the risks (expected myocarditis after vaccination) in all populations for which vaccination is currently recommended. However, the committee noted the balance of benefits and risks vary by age and sex because myocarditis cases occurred predominantly among males less than 30 years old and the risk of complications from COVID-19 increase with age. For every 1 million second doses of mRNA vaccine administered to males ages 12-29 years, 11,000 COVID-19 cases, 560 hospitalizations, 138 ICU admissions, and 6 deaths due to COVID-19 could be prevented, compared with 39-47 expected myocarditis cases after SARS-CoV-2 vaccination. Among older males aged ≥30 years, the benefits increase, with 15,300 COVID-19 cases, 4,598 hospitalizations, 1,242 ICU admissions, and 700 deaths potentially prevented, compared with 3-4 expected myocarditis cases. The authors note their analysis did not include the possible benefit of preventing longer-term COVID-19 symptoms nor multisystem inflammatory syndrome in children (MIS-C). ACIP emphasized the importance of informing providers and families about the benefits and risks of vaccination, including myocarditis, and monitoring for adverse events following vaccination.
Notably, the American Heart Association (AHA) on the same day published a scientific statement on the diagnosis and management of myocarditis in children in the journal Circulation. Though the statement was developed prior to the COVID-19 pandemic, the recommendations could be useful for healthcare providers in identifying and treating myocarditis/pericarditis among young people following SARS-CoV-2 vaccination or infection, as there currently is no standard treatment for either condition. With no alternatives to mRNA vaccines for adolescents available for the foreseeable future, no deaths or severe outcomes from myocarditis/pericarditis reported at the time of ACIP’s meeting, and about one-third of US COVID-19 cases occurring in people ages 12-29 in May 2021—many unvaccinated—most experts agree with the committee’s conclusion to continue recommending vaccination for all people aged 12 and older. Questions remain about whether reports of myocarditis/pericarditis among younger populations will impact vaccination rates, but many experts point out that potential future risks, posed by the Delta variant (B.1.617.2) or another possibly more virulent strain, should prompt parents to vaccinate their children in order to protect them and those around them.
REDUCING VACCINE DOSE As vaccination efforts continue to scale up in most countries, production capacity is still “woefully inadequate” to meet the global demand. Some experts are beginning to speculate whether reducing the dose volume could increase the number of available doses without sacrificing protection. This concept, referred to as “fractionation,” has been implemented in the past for other vaccines, such as yellow fever, polio, and meningococcal conjugate vaccines. In these instances, existing research provided evidence that smaller doses still provided sufficient protection; however, that is not necessarily the case for SARS-CoV-2 vaccines. Because the vaccines are so new—and research to this point has focused principally on establishing safety and efficacy profiles to support regulatory authorization—the necessary data simply are not available to demonstrate efficacy for smaller doses. Small studies early in the development process compared several dose options against each other, but these largely focused on safety rather than efficacy. There have not yet been dedicated efforts to determine the minimum dose required to provide protection.
There is limited evidence that smaller doses of some existing vaccines could stimulate sufficient immune responses, but not enough to provide robust, reliable efficacy estimates. Additionally, it could be argued that the nature of the pandemic demands different calculus in terms of evaluating benefit. Smaller doses of the vaccine might provide less protection at the individual level, but increasing the number of vaccinated individuals could provide a net benefit at the population level. Beyond the technical questions, implementing fractionation at this point in the pandemic—ie, after many higher-income countries have already vaccinated substantial portions of their respective populations—could pose ethical and political challenges, considering that much of the future supply will be allocated to low- and middle-income countries.
COVID-19 THERAPEUTICS The WHO recently updated its living guideline for the use of COVID-19 therapeutics with a strong recommendation to use interleukin-6 (IL-6) receptor blockers, including both tocilizumab and sarilumab, in patients with severe COVID-19 disease. IL-6 is an inflammatory cytokine that is activated as part of the immune response, but can be over-activated during SARS-CoV-2 infection and contribute to more severe disease. The WHO’s decision followed the publication of a meta-analysis on IL-6 blockers by its Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. The meta-analysis included review of 27 randomized clinical trials using IL-6 receptor antagonists in 10,930 patients. Overall, the REACT study found that 28-day all-cause mortality was lower in patients who received IL-6 receptor antagonists than in those who did not. It is important to note, however, that the improvement in all-cause mortality was only seen when co-administered with corticosteroids. Thus, the updated WHO recommendation specifies that patients meeting criteria for severe and critical COVID-19 disease should be treated with both IL-6 receptor antagonists and corticosteroids.
BIOMARKERS Throughout the pandemic, scientists have been studying why some people are more susceptible than others to severe COVID-19 disease and what genetic factors might play into this heightened susceptibility. This week, a group of researchers with the COVID-19 Host Genetics Initiative published a study in Nature that identifies 13 genome-wide significant loci that are associated with increased risk of SARS-CoV-2 infection and with severe COVID-19 disease outcomes. The identified loci (locations of genes along chromosomes) previously have been correlated with lung function and inflammatory disorders. Understanding genetic predisposition to poor outcomes from SARS-CoV-2 infection is especially important for the development of medical countermeasures. Other studies have identified human biomarkers associated with severe COVID-19 disease whose genetic expression can be modified using existing drugs in a hospital setting. The ACE-2 receptor and associated ACE2 gene were identified early on as one such marker.
Beyond treatment of COVID-19 patients, scientists also are investigating biomarkers of successful responses to SARS-CoV-2 vaccines. Researchers at the University of Oxford who developed the AstraZeneca-Oxford vaccine are investigating the ability of their vaccine to induce high levels of neutralizing antibodies in recipients. When researchers compared vaccinated individuals who were fully protected to cases of “breakthrough infections” among other vaccinated individuals, high levels of neutralizing antibodies were correlated with better protection. Although neutralizing antibodies may not be an appropriate marker of vaccine success in other platforms, future vaccines with similar profiles to the AstraZeneca-Oxford vaccine may be able to accelerate their development if they can demonstrate high levels of this biomarker.
UK SUMMER COVID-19 PLAN On July 5, the UK announced its “Summer 2021” COVID-19 response plan, which will move the country to Step 4 of its recovery and eliminate many existing restrictions later this month. The changes are scheduled to take effect July 19, and the final decision will be made on July 12, based on updated epidemiological and other data. The decision will eliminate “all remaining limits on social contact,” including on public and private gatherings at businesses, restaurants, pubs, and other venues. Additionally, all mandates regarding mask use and physical distancing will be removed, although local health authorities can implement targeted measures in response to COVID-19 outbreaks. Beyond the social distancing-related protections, the UK also will eliminate requirements to self-quarantine after known exposure to a COVID-19 case for fully vaccinated individuals and those under the age of 18. Schools will no longer keep students in “bubbles,” and they will no longer be required to conduct contact tracing for identified cases, “which will help to minimise the number of children isolating.” The existing national testing and contact tracing program will remain in effect through the winter.
The UK plan notes that there is “a sufficiently high proportion of the population vaccinated” and that “the country can learn to live with COVID-19” without the existing restrictions. The UK reports national vaccination coverage among adults as 87% for at least 1 dose and 65% for full vaccination. Notably, UK Secretary of State for Health Sajid Javid reportedly acknowledged that removing the restrictions could result in the daily incidence exceeding 100,000 new cases per day, nearly 4 times the current average and more than 50% higher than the UK’s current record (59,829 new cases per day on January 9, 2021). The UK is currently facing its second-largest surge, which has been widely attributed to a rapid increase in the prevalence of the Delta variant (B.1.617.2). In the current surge, the UK’s daily incidence increased by a factor of 12 since mid-May, even with the existing restrictions in place.
As countries like the UK ease COVID-19 restrictions, the WHO continues to emphasize that the pandemic is far from over and urge governments to maintain effective protections. In response to the UK’s plan, more than 4,000 clinicians and other experts signed an open letter published in The Lancet, referring to the plan as “mass infection” and a “dangerous and unethical experiment” and highlighting the increased risk to children, most of whom are still not eligible for vaccination.
FIJI Fiji reported a record daily high in new COVID-19 cases on July 7, with 636 cases in 24 hours. Government officials attributed the recent outbreak to a case of the Delta variant that escaped the country’s isolation facility. Of the 39 deaths that have been reported throughout the pandemic, 37 deaths have occurred since the latest outbreak began. This newest surge is straining Fiji’s health system, where its largest hospital is now exclusively treating COVID-19 patients and its mortuary is at full capacity. Over 1,000 patients have been sent home to quarantine and recover, as medical facilities have no space. A makeshift clinic is reportedly being established, utilizing a sports arena outside the capital of Suva. The Ministry of Health has suspended all pregnancy services in and around Suva until July 26, and the ministry no longer will test residents in their homes. While no nationwide lockdown is in place, police have arrested 48 people for failure to follow local mask ordinances or limits on social gatherings. About 36% of Fiji’s population has been partially vaccinated, and just over 6% have been fully vaccinated.
OLYMPICS Two weeks from today, Tokyo will kick off its scaled-back 2020 Summer Olympic Games amid another state of emergency. The Japanese government imposed a fourth state of emergency in the Tokyo metropolitan area that will begin on July 12 and extend until August 22, through the entire Olympic Games. Olympic organizers also decided against allowing any spectators into the games, with some exceptions for events taking place in areas outside of Tokyo that are not under a state of emergency. Further changes to the Olympics programming include cancelling the Olympic torch relay through Tokyo. Athletes and other team members also must abide by strict quarantine and testing measures in order to participate. These heightened measures follow weeks of concern over rising numbers of COVID-19 cases, public opposition to the games, and consultation with experts. However, with the number of new COVID-19 cases on the upswing and vaccination rates unable to keep pace, many public health experts fear these efforts may not be enough to prevent another pandemic wave in Japan.
COMMUNIVAX The Johns Hopkins Center for Health Security is hosting the next in its series of CommuniVax webinars on July 15 at noon EDT. The webinar follows the publication of CommuniVax’s second report—The Public’s Role in COVID-19 Vaccination—and it will focus on “a new strategy for the COVID-19 vaccination campaign,” informed by input from racial and ethnic minority communities. The CommuniVax project aims to address racial and ethnic disparities in vaccination, particularly in the context of the COVID-19 pandemic. The webinar will feature presentations by and discussions with speakers representing a broad spectrum of US academic institutions and non-governmental organizations, moderated by Dr. Emily Brunson (Texas State University) and Dr. Monica Schoch-Spana (Johns Hopkins Center for Health Security). Additional information and registration is available here.
by JazzNU Really surprised to see no mention of Russia in the WHO report. Daily covid deaths steadily increasing in recent weeks and hitting records in recent days.
by ponchi101 Down here. The country is open, virus be damned.
I took my citizenship exam today (flunked it) and in the invitation e-mail I was told that I needed to register with a local C19 tracking APP, which I would need to show at town hall. Nothing. They made me wash my hands and that was it. Everybody is wearing a mask and any and all vaccines are being delivered. The process is faulty, but the government has decided that any vaccine available will be used on whomever asks for it. Slowly, it is being done. There are NO anti-vaxxers here, so the issue is getting more doses. Sure, numbers are still high, but it will be the way it will work.
But...
back "home", my mom and sister received their first dose of Sputnik V three weeks ago. They were scheduled for their second dosed on Wednesday and today, and, well, they don't have any left. They will be called. With the country not having any money (and refusing American vaccines, while here the government is accepting any and all that Uncle Joe is sending) they are finding out how generous the Russian govt really is.
by Suliso Is it difficult to obtain Colombian citizenship compared to say American or Spanish if you have lived legally there for some time? At least the language is not a problem for you.
by ponchi101 Very difficult. The exam today.
I received a mail telling me I would be tested on the constitution (178 pages long), history and geography. But they give you no books to read (or a list), no indications of what they will ask for. Nothing.
So I crammed on the constitution, the history and national geography. On the history I went back to all the crap about our independence (it is similar to Venezuela's) and geography I learned all 32 states and their capitals. Learned the national anthem, poured over the current cabinet.
So, what did they ask me about:
name 5 municipalities of the state we are in.
3 really obscure historical figures (Colombian pioneer of neurosciences, inventor of the malaria vaccine, and the name of an obscure lady from the independence movement).
Nothing about the constitution.
5 states, write down their capitals.
5 longest rivers in the country, in order (I remembered the 1st one, the others I did not know the order).
Nothing about the anthem, or the 150 years of wars this country has been waging.
So the exam is basically set up to flunk you. So yes, the language is the same, but that was about it.
And, BTW. The exams and processes are all in Spanish. You do not speak the language? Mala suerte, idiota.
(bad luck, buddy).
by JazzNU How many times are you allowed to take it? Is it a problem for your resident status that you didn't pass?
by Suliso Well, I hope you do get it eventually. Will make traveling and working easier for you, I assume. As funny as it is to say it about a Colombian passport...
by ponchi101
JazzNU wrote: ↑Fri Jul 09, 2021 11:20 pm
How many times are you allowed to take it? Is it a problem for your resident status that you didn't pass?
No, no problem at all. You can take it as many times as possible, but it takes 6 months for a new date. So kind of a drag.
Suliso wrote: ↑Fri Jul 09, 2021 11:32 pm
Well, I hope you do get it eventually. Will make traveling and working easier for you, I assume. As funny as it is to say it about a Colombian passport...
The sole reason for doing this. Getting a Venezuelan passport is right now somewhere in between miraculous and impossible. I guess it will have to be next year.
by Suliso Pills against stupid are not through the clinical trials yet.
In other news got my second vaccine yesterday. Feel fine only kind of sleepy at 10 am.
by ponchi101 Good for you, Suliso.
My understanding is that the main problem with the pills against stupidity is that the people that will take them are not stupid, and the people that will not take them are. Sort of a placebo effect for people that know about the placebo effect.
About the two dead Covid skeptics. Please do not post any more of those because, when I fail to feel any sort of sorrow or pity for them, it reminds me of what a lousy human being I am. Instead of "gee, that is sad", my initial train of thought is "Damn, Darwin keeps getting proven right". And the worst part is that I feel no shame in not feeling sorry at all.
Off Topic
And of course I am joking. Post anything you want about idiots that have a vaccine readily available and decide to gamble with their lives.
by Suliso Covid infections up 100% the last seven days. Driven mostly by 20-40 year olds. Number of people in a hospital (88) still low, but we'll see in a week or two.
Only 21% of 20-29 year olds are fully vaccinated...
by ti-amie
by ti-amie
ponchi101 wrote: ↑Mon Jul 12, 2021 2:48 pm
Good for you, Suliso.
My understanding is that the main problem with the pills against stupidity is that the people that will take them are not stupid, and the people that will not take them are. Sort of a placebo effect for people that know about the placebo effect.
About the two dead Covid skeptics. Please do not post any more of those because, when I fail to feel any sort of sorrow or pity for them, it reminds me of what a lousy human being I am. Instead of "gee, that is sad", my initial train of thought is "Damn, Darwin keeps getting proven right". And the worst part is that I feel no shame in not feeling sorry at all.
Off Topic
And of course I am joking. Post anything you want about idiots that have a vaccine readily available and decide to gamble with their lives.
Ponchi a lot of people on the Bird App agree with you. I think they should post them because while many do not use that app they may have people in their circle who do and word will get around. Maybe that will help save a few lives that would otherwise be lost. I don't know.
This was making the rounds yesterday. It's a bit harsh but makes the point.
by atlpam
ponchi101 wrote: ↑Mon Jul 12, 2021 2:48 pm
Good for you, Suliso.
My understanding is that the main problem with the pills against stupidity is that the people that will take them are not stupid, and the people that will not take them are. Sort of a placebo effect for people that know about the placebo effect.
About the two dead Covid skeptics. Please do not post any more of those because, when I fail to feel any sort of sorrow or pity for them, it reminds me of what a lousy human being I am. Instead of "gee, that is sad", my initial train of thought is "Damn, Darwin keeps getting proven right". And the worst part is that I feel no shame in not feeling sorry at all.
Off Topic
And of course I am joking. Post anything you want about idiots that have a vaccine readily available and decide to gamble with their lives.
The struggle is real ponchi - especially when it involves your family and all you want to say is why the heck didn't you get vaccinated. Instead you have to hold your tongue until after they recover (which fortunately my family members did - a co-worker was not so fortunate). Obviously I'm sad they are sick and want them to get better, but it's tough to be sympathetic when they didn't take the precautions available to them.
by ponchi101 Must be that since I am here in Colombia, and our problem is that there are not enough vaccines yet, I am truly puzzled by these people. I have only one friend that believes the virus and the response are lies (he believes Fauci is a hoax, as if Fauci were making any money out of this) and therefore, reading about these people is amazing to me.
Sorry to sound callous, but honestly, these news leave me perplexed, not feeling any sorrow for the people in them.
by Suliso Ponchi, it's still early days in Colombia. You'll arrive at your vaccine deniers too hopefully sooner than later. In Switzerland about 25% of adults intend not to take the vaccine no matter what. In Latvia it's even more.
Mind you they're not all conspiracy theory believers. Lots of younger people simply think that they are young and strong and need no stinking vaccine.
by ponchi101 No, really, not here. I have yet to find anybody, or read any news, about people not planning on getting the vaccine. The young ones are not rushing to get it for the reasons you mention, but when they get their place in line, they will.
Remember that Colombia is one of those countries where you need vaccination to go to school. My GF has a friend, one of the vegan/ant-vaxxer/holistic medicine believers that moved here from Vennieland and was trying to get her children into school, without vaccination. My GF told her it was impossible, so she should just simply vaccinate her children (young kids when they moved here from Venezuela, so they had never gone to school back there). She said she would not, my GF said "good luck".
She had her children vaccinated. All schools simply pointed at the law.
If the U.S.A. simply wants to get rid of some vaccines, send them here. The Govt will take all they can.
by Suliso I believe childhood vaccines are mandatory here as well, but these ones are seen completely differently. It would be amazing if you could really achieve 90%+ coverage for adults. I don't think any European country will manage to get that high. Israel has done really well, but not reached that magical number either.
by Deuce Some much needed perspective on greed, and vaccine equity...
by dryrunguy Here is the latest Situation Report. I'm telling you, our overdeveloped sense of entitlement to being entertained (see Netherlands) will get us all killed.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 187 million cumulative cases and 4.04 million deaths worldwide as of 8:30am EDT on July 13. Global weekly incidence increased for the third consecutive week, up nearly 10% from the previous week. After 9 consecutive weeks of decline, global weekly mortality increased 3.4% compared to the previous week. The increase in weekly mortality follows 2 weeks behind the trend in weekly incidence, and while the timing is slightly earlier than the 3-4 weeks we have observed over the course of the pandemic, it is still relatively consistent with what we would expect.
Global Vaccination
The WHO reported 3.33 billion doses of SARS-CoV-2 vaccines administered globally as of July 13. The WHO reports a total of 1.28 billion individuals received at least 1 dose and 590 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered continues to decline rapidly from the record high of 43.1 million doses per day on June 27, now down to 29.2 million. Vaccinations are decreasing in Asia and North America, leveling off in Europe and Africa, and increasing in Oceania and South America. Our World in Data estimates that there are 1.98 billion vaccinated individuals worldwide (1+ dose; 25.4% of the global population). There are an estimated 957 million who are fully vaccinated (12.3% of the global population), although reporting is less complete than for other data.
UNITED STATES
The US CDC reported 33.7 million cumulative COVID-19 cases and 604,710 deaths. The US reported 17,753 new cases per day on July 9—a 55% increase from the low of 11,455 new cases per day on June 20—before decreasing to 15,497 on July 11. Daily mortality also “peaked” on July 9—increasing from 150 on July 6 to 167 (+11%)—before falling slightly to 156 on July 11. These fluctuations could still be a result of delayed reporting over the US Independence Day holiday weekend. Reporting should return to normal by later this week, but it could be another week before we have a clearer picture of the longer-term trends.
US Vaccination
The US has administered 335 million cumulative doses of SARS-CoV-2 vaccines, and it is administering approximately 421,000 doses per day, the lowest average since January 1. A total of 184 million individuals in the US have received at least 1 dose, equivalent to 55.5% of the entire US population. Among adults, 67.7% have received at least 1 dose as well as 9.6 million adolescents aged 12-17 years. A total of 159 million individuals are fully vaccinated, which corresponds to 48.0% of the total population. Approximately 58.9% of adults are fully vaccinated, as well as 7.4 million adolescents aged 12-17 years.
US CDC SCHOOL & CHILD CARE GUIDANCE On July 9 the US CDC released updated guidance for COVID-19 prevention in K-12 schools, prioritizing a return to in-person learning for students this fall and highlighting the importance of vaccinating as many eligible children as possible. So far, 1 in 3 adolescents ages 12 to 17 have been vaccinated, a number experts are hoping will increase over the coming months. Overall, the CDC recommends school districts tailor their recommendations to local laws and epidemiological situations, tightening or relaxing layered prevention strategies such as mask wearing and physical distancing based on local transmission rates. Some experts criticized the agency for leaving so many decisions up to local officials, saying more specific guidance would be helpful. Others, including officials with the country’s two major teachers’ unions, praised the guidance, calling it “grounded in both science and common sense.” With nearly all of the nation’s school districts set to open this fall, the CDC updated its guidance based on progress in the national vaccination campaign.
In alignment with its national recommendations for the general public, the CDC said masking could be optional for vaccinated students and school staff but unvaccinated students ages 2 and older and staff should use masks when indoors, especially when physical distancing cannot be maintained. Masks are not needed for outdoor activities such as recess or extracurricular activities, unless people are in a crowded situation, such as in the stands at a football game. The recommendation for physical distancing for students was decreased from 6 feet to 3 feet. The guidance notes that if distancing inhibits in-person learning, layering multiple other prevention strategies can be substituted. All school staff should maintain a 6-foot distance from students when possible. If the number of cases in a community begins to rise, if vaccination rates are low, or if schools cannot determine who has been vaccinated, school districts could opt for universal masking if local and state laws allow.
The CDC encouraged schools to promote vaccination among students and staff, including offering vaccinations on-site, providing sick leave for employees to get vaccinated, and excusing student absences for vaccinations. In addition, the agency said schools should support those who want to wear masks even if they are vaccinated. Schools should also consider layering other prevention strategies, including regular screening testing, improving ventilation, promoting good hand hygiene, staying home when sick, contact tracing with isolation or quarantine, and cleaning and disinfection. Cohorting, or keeping students and staff in small groups throughout the day, might be useful in some cases to limit contact, but the practice should not replace other prevention strategies nor mix vaccinated and unvaccinated individuals, the agency said. The CDC also released updated guidance for early care and education and childcare programs. With the more transmissible Delta variant now dominant in the US, it remains to be seen how local jurisdictions will enforce the CDC’s guidance in areas of low vaccination coverage, where cases and hospitalizations are already rising.
VACCINES & GUILLAIN-BARRÉ SYNDROME The US FDA announced that it is including a warning regarding the risk of Guillain-Barré syndrome (GBS), a rare but potentially serious autoimmune neurological condition, associated with the J&J-Janssen SARS-CoV-2 vaccine. To date, there have been approximately 100 preliminary reports of GBS among 12.8 million recipients of the J&J-Janssen vaccine, but additional data are required in order to establish a causal relationship. Most of the cases have been identified within 2 weeks of vaccination, and mostly among men aged 50 years and older. Regulatory officials have not identified a similar trend associated with the Pfizer-BioNTech or Moderna vaccines. However, the FDA's update comes only days after the European Medicines Agency's Pharmacovigilance Risk Assessment Committee recommended including a warning to raise awareness among healthcare professionals and people taking the AstraZeneca-Oxford vaccine of GBS cases reported following vaccination. Both the J&J-Janssen and AstraZeneca-Oxford vaccines are adenovirus vector vaccines.
While rare in terms of the frequency of cases, GBS is a known risk associated with viral infections and other vaccines. The FDA includes warnings regarding GBS risk for several common vaccines, including both the nasal mist and injection versions of the seasonal influenza vaccine and the DTaP (diphtheria, tetanus, and pertussis) vaccine. Prior research has also found elevated risk of GBS following seasonal influenza infections, which is orders of magnitude higher than from the vaccine.
On average, approximately 3,000-6,000 cases of GBS are reported annually in the US. One previous COVID-19 study involving more than 70,000 COVID-19 patients in Spain estimated the GBS risk following infection to be 0.15%, which is approximately 1,500 GBS cases per million SARS-CoV-2 infections. One previous study on GBS and seasonal influenza found the GBS risk to be approximately 1 case per million seasonal influenza vaccinations and 18 cases per million cases of seasonal influenza. Like with other adverse events identified following SARS-CoV-2 vaccination, experts emphasize that the benefits far outweigh the risks.
FULL VACCINE APPROVAL With 3 SARS-CoV-2 vaccines authorized for emergency use by the US FDA, attention is shifting toward the process for these vaccines to receive full regulatory approval. The FDA is facing pressure, including from some high-profile experts, to move quickly with the full approvals in order to encourage individuals to get vaccinated, but some experts are pushing back on the idea that the Emergency Use Authorization is discouraging Americans from getting vaccinated and that the impression that the FDA hastily issued full approval for one or more vaccines could pose the risk of harming its credibility. FDA officials have commented that the agency is moving as quickly as practicable, and the sheer volume of vaccinations administered already are providing a wealth of data for regulatory officials, which could shorten the timeline to some degree.
VACCINE DOSE STRETCHING In an effort to accelerate the pace of global immunization, scientists are exploring whether administering a quarter of the standard dose of the Moderna SARS-CoV-2 vaccine could provide lasting immunity to more people. Similar dose-stretching strategies have been employed in the past, including with yellow fever vaccinations in Africa and South America, but no similar approach has been tried for COVID-19 despite slow vaccination rollouts in low- and middle-income countries and evolving variants of concern. To evaluate whether 2 25 microgram doses, versus the authorized 2 100 microgram doses, could elicit lasting neutralizing antibodies, researchers analyzed blood samples from 35 individuals involved in the original trial of the Moderna vaccine. In a preprint study published last week in medRxiv, the researchers report that nearly all the participants had neutralizing antibodies and various types of T cells 6 months after vaccination. The antibody and T cell levels were similar to people who had recovered from COVID-19. According to a preprint modeling study conducted by researchers from Harvard University and colleagues, vaccine dose-stretching could accelerate global vaccination efforts, helping to prevent more COVID-19 cases and related deaths than current strategies. Another trial testing lower doses of the Pfizer-BioNTech vaccine in people ages 18-55 is ongoing in Belgium.
VACCINE BOOSTER According to multiple news media reports, representatives from Pfizer met with scientists and regulatory officials from the US government this week to present information regarding the need for booster doses of its SARS-CoV-2 vaccine (developed in collaboration with BioNTech). Notably, the meeting took place privately, as opposed to other recent presentations of key vaccine safety and efficacy data that took place at public meetings of the US CDC’s Advisory Committee on Immunization Practices or the US FDA’s Vaccines and Related Biological Products Advisory Committee. Reportedly, this meeting aimed to review preliminary data and initiate discussions, as opposed to present formal arguments or make any decisions regarding the booster doses. Pfizer is expected to submit data on clinical trial participants’ immune responses following a third dose of its vaccine to the FDA in the coming weeks; however, decisions regarding guidance on booster doses likely will depend heavily on CDC data regarding breakthrough infection risk.
WHO Director-General Dr. Tedros Adhanom Ghebreyesus recently issued a statement calling for a continued focus on increasing vaccination coverage globally, rather than using much-needed doses for boosters in countries that already have high vaccination coverage. Vaccine supply has not yet met the global demand, and many countries continue to struggle to access doses for their populations. Dr. Tedros emphasized that there are divergent COVID-19 trends, with low- and middle-income countries with low coverage facing severe surges while wealthier, vaccinated countries fare better. Dr. Soumya Swaminathan, the WHO’s Chief Scientist, noted that adding a third dose of the vaccine in just 11 high- and upper-middle-income countries could require an additional 800 million doses—enough to fully vaccinate 400 million people—that are badly needed in many countries.
Despite the WHO’s call to avoid extra doses, Israel on June 12 became the first country to offer a third dose of the Pfizer-BioNTech vaccine to immunocompromised individuals. Israel Health Minister Nitzan Horowitz did not explain how the decision to offer the booster shots was reached before authorization by any major regulators, and he indicated the ministry is evaluating whether to extend the offer to the entire population.
SENEGAL VACCINE PRODUCTION On July 9, the Republic of Senegal announced it will begin construction of a vaccine manufacturing facility at the Institut Pasteur in Dakar later this year, with support from the EU, US, and World Bank. The effort aims to produce 25 million doses of SARS-CoV-2 vaccines per month by the end of 2022, as well as manufacture vaccines for other diseases to reduce Africa's reliance on imported doses. The construction is supported by nearly €30 million (US$35 million) from Germany, France, and the EU, and the facility is expected to be finished within 18 months from the start of construction.
Africa currently relies on importation for 99% of its vaccine needs. The COVID-19 pandemic has confirmed the need for local vaccine production, with less than 3% of the continent’s population vaccinated (1+ dose) and less than 1.5% fully vaccinated. During the pandemic, African countries have relied on the COVAX facility and bilateral agreements in order to obtain access to SARS-CoV-2 vaccines. COVAX anticipates delivering a total of 520 million doses of vaccine to African countries by the end of 2021 and 850 million by March 2022. That target would supply enough vaccine doses to achieve about 30% coverage in each eligible African country.
NETHERLANDS Dutch Prime Minister Mark Rutte apologized on July 12 for what he said was “poor judgment” in loosening COVID-19 restrictions, as the country’s number of new cases rose to its highest levels of the year. Despite warnings from health experts that a nearly complete reopening was premature, the Dutch government allowed bars, nightclubs, and festivals to reopen beginning on June 26 following a marked decrease in cases. Although around two-thirds of the population have at least one vaccine dose, the lifting of restrictions in combination with the circulation of the Delta variant clearly had a rapid impact on virus transmission, as the 7-day average of COVID-19 cases increased by 572% this week compared with last week. Cases are surging particularly among the young adult population, who briefly were able to take advantage of reopened nightlife. The government moved 7 regions into the highest “very serious” risk level and 10 others into the second highest “serious” risk level. Last week, almost all of the regions were within the lowest two risk levels of “vigilant” and “worrisome.” The renewed control measures went into effect on July 10 and are set to last through August 14.
AIR HANDLING A new CDC MMWR report explores safety precautions that can be taken indoors to reduce transmission of SARS-CoV-2. In particular, the combination of portable high efficiency particulate air (HEPA) cleaners with universal masking policies appears to be very effective in preventing transmission between people in close-contact indoor environments. Previous studies have shown that HEPA air cleaners, portable or built-in, can greatly reduce aerosol transmission in indoor environments. For the MMWR report, CDC researchers simulated a conference room presentation scenario by using respiratory simulators to mimic a person with COVID-19 as well as other, uninfected persons. When 2 portable HEPA air handlers were used alone, aerosol exposure was reduced by up to 65%. When masks were worn by all simulated participants without air cleaning, the aerosol exposure was reduced by 72%. However, when both air cleaning and masks were employed as mitigation measures, the aerosol exposure was reduced by up to 90%. According to the experiment, the HEPA air cleaners were most effective when placed close to the simulated infected participant. The researchers conclude that portable HEPA air cleaners and masking in combination are viable options to prevent aerosolized SARS-CoV-2 transmission, especially in environments without HVAC systems or other built-in air cleaning technology.
US IMMIGRATION DETENTION CENTERS Public health officials warn of infectious disease transmission risk at high-density facilities, and immigration detention centers are no exception. With relatively few detainees vaccinated for SARS-CoV-2 and the total number of detainees increasing to pre-pandemic levels, US Immigration and Customs Enforcement (ICE) is reporting outbreaks and surges in new COVID-19 cases. According to a New York Times analysis of ICE data, more than 7,500 COVID-19 cases have been reported among detainees since April, accounting for more than 40% of the total reported cases in ICE facilities since the pandemic began. Experts who have visited detention centers report low adherence to public health interventions like mask wearing and physical distancing among detainees and ICE staff members. According to an ICE spokesperson, all new detainees are tested and quarantined for 14 days upon arrival. As of May, the agency’s data show only 20% of detainees received at least 1 dose of vaccine while in custody. Sharon Dolovich, a law professor and director of UCLA’s COVID Behind Bars Data Project, said COVID-19 outbreaks would remain high among detained individuals until ICE prioritizes vaccinations. As the Delta variant takes hold in regions with low vaccination rates, public health officials warn against further outbreaks among vulnerable detainees and the potential for the development of other variants.
NETHERLANDS Dutch Prime Minister Mark Rutte apologized on July 12 for what he said was “poor judgment” in loosening COVID-19 restrictions, as the country’s number of new cases rose to its highest levels of the year. Despite warnings from health experts that a nearly complete reopening was premature, the Dutch government allowed bars, nightclubs, and festivals to reopen beginning on June 26 following a marked decrease in cases. Although around two-thirds of the population have at least one vaccine dose, the lifting of restrictions in combination with the circulation of the Delta variant clearly had a rapid impact on virus transmission, as the 7-day average of COVID-19 cases increased by 572% this week compared with last week. Cases are surging particularly among the young adult population, who briefly were able to take advantage of reopened nightlife. The government moved 7 regions into the highest “very serious” risk level and 10 others into the second highest “serious” risk level. Last week, almost all of the regions were within the lowest two risk levels of “vigilant” and “worrisome.” The renewed control measures went into effect on July 10 and are set to last through August 14.
Sadly I think the US will be heading in this direction shortly. Cuomo has already said he will not reinstate a lockdown so I don't know what is going to happen here.
Thanks for posting the report dry.
by atlpam
dryrunguy wrote: ↑Tue Jul 13, 2021 6:19 pm
US IMMIGRATION DETENTION CENTERS Public health officials warn of infectious disease transmission risk at high-density facilities, and immigration detention centers are no exception. With relatively few detainees vaccinated for SARS-CoV-2 and the total number of detainees increasing to pre-pandemic levels, US Immigration and Customs Enforcement (ICE) is reporting outbreaks and surges in new COVID-19 cases. According to a New York Times analysis of ICE data, more than 7,500 COVID-19 cases have been reported among detainees since April, accounting for more than 40% of the total reported cases in ICE facilities since the pandemic began. Experts who have visited detention centers report low adherence to public health interventions like mask wearing and physical distancing among detainees and ICE staff members. According to an ICE spokesperson, all new detainees are tested and quarantined for 14 days upon arrival. As of May, the agency’s data show only 20% of detainees received at least 1 dose of vaccine while in custody. Sharon Dolovich, a law professor and director of UCLA’s COVID Behind Bars Data Project, said COVID-19 outbreaks would remain high among detained individuals until ICE prioritizes vaccinations. As the Delta variant takes hold in regions with low vaccination rates, public health officials warn against further outbreaks among vulnerable detainees and the potential for the development of other variants.
I don't understand why they don't just require anyone at a US immigration detention center to be vaccinated. You come across the border, you get a jab. When they say only 20% received a dose, is it that they're offering and getting no takers? It seems like this shouldn't be a choice.
by JazzNU
ti-amie wrote: ↑Tue Jul 13, 2021 6:58 pm
Sadly I think the US will be heading in this direction shortly. Cuomo has already said he will not reinstate a lockdown so I don't know what is going to happen here.
Difference here is that the health officials made the majority of the calls on re-opening, i.e. CDC changed the guidelines for vaccinated after a significant amount of data gave them the confidence to do so and there was a domino effect of restrictions loosening around the country.
Doesn't mean we won't have a spike, but places like the UK and Netherlands, you have the health officials putting out statements in opposition to their leaders trying to get them to follow their advice, and while that's the case in some states, in particular in the South and Missouri, that's not what has been happening largely in the US.
And so far, their recommendations and timing of their decisions seems accurate, so hoping for the best and not assuming we will be headed in that direction.
by JazzNU
atlpam wrote: ↑Tue Jul 13, 2021 7:22 pm
I don't understand why they don't just require anyone at a US immigration detention center to be vaccinated. You come across the border, you get a jab. When they say only 20% received a dose, is it that they're offering and getting no takers? It seems like this shouldn't be a choice.
I get what you're saying. But I understand. US History. Can of worms.
by ti-amie
by MJ2004 I have two family members in Spain, both who are very conservative politically, who refuse to get vaccinated. Trump pov transferred to the VOX party.
by dmforever In the movie Outbreak (it resurged in popularity when the pandemic started), they got a lot of things right. It was kind of amazing especially since usually Hollywood doesn't even care enough to try to get things right. What they didn't get right, because who could have ever imagined it, is that so many people would politicize science and getting a vaccination. It's just so unfathomable.
Kevin
by ponchi101 Sort of attached to the demonization of Big Pharma. The people that I know that are into the "holistic approach" to medicine simply believe that every, and it is every, medicine produced by pharmaceutical companies has ulterior motives. It cures one symptom, creates two more.
So this pandemic was fertile ground for these ideas. My friend here, completely submerged into all things things "natural", believes that the C19 virus was developed so that Big Pharma could sell more PCR tests, so the masterminds created the pandemic. The fact that such a plan, if true, has backfired terribly simply escapes scrutiny.
by Suliso Tell her that having six kids before age 35 with half dying in childhood is super natural as well.
by ponchi101
Suliso wrote: ↑Wed Jul 14, 2021 3:29 pm
Tell her that having six kids before age 35 with half dying in childhood is super natural as well.
It's a "he", with a BS in Aeronautical Engineering from UCLA.
He firmly believes in magic, too. I never understood...
by Suliso What kind of magic? Harry Potter type?
by ponchi101 Things like:
He lost his wallet in NYC. He finds out a bit later, when he tries to pay for something. His GF is going crazy; they are now with no credit cards or cash, only hers (smaller limits). They have no idea what happened, but they go back to the hotel, where his wallet is waiting for him. Somebody found it on the street and brought it to his hotel.
Magic.
I say: "Did you have your room key (nowadays invariably a card) in it?"
"Yes".
"The person only had to bring it back to the hotel, where you would be identified. The card told him what hotel you were in".
"In NYC? Where everybody is so rude? NO WAY!"
"People are not rude in NYC. The vast majority of people in the world are good. Since you lost it early in the day (most likely it fell from his backpack) you must have lost it close to the hotel. Maybe the person found it in the same block, because most likely you lost it when you were going out and indeed putting it inside your back pack".
"And he did not steal the money? NO WAY!"
"People are good, N. Would you steal money from a found wallet? No. And most people are like that".
No, no, no. It was magic. It was the power of his mind, because he always has a positive outlook of the world.
I bet you know the type.
by ti-amie
by ti-amie
by ti-amie I'm not sure if this is fear mongering or based in fact. It's the second time I've seen 1,000,000 deaths projected.
by ti-amie I'm also seeing this sentiment now.
From NYT comments on this article:
Delta Variant Widens Gulf Between ‘Two Americas’: Vaccinated and Unvaccinated
Data from overseas, particularly Britain, suggest the spread of the virus will set vaccinated and unvaccinated communities on very different paths. https://www.nytimes.com/2021/07/14/heal ... k-usa.html
H. Clark
Long Island, NY
The U.S. should build a database of all citizens unwilling to be vaccinated, and share those names with insurance carriers, Medicare and Medicaid. Anyone who refuses to be inoculated against Covid-19 who becomes ill with the virus will not be eligible for medical coverage, and that includes all care and/or hospitalization. Good luck with the $698,552.91 bill from your local hospital. And that’s if you live.
And of course...
B
CA
I don’t understand personal choice of hen (sic) it comes to vaccinations. Insurance companies should be able to make covid treatment an uncovered medical expense if the person has no medically necessary reason to not take the vaccine. I refuse to subsidize these people.
1 REPLY
D
DecliningSociety
Baltimore
What if the COVID patient had not planned on getting COVID? I guess we should also let people choose not to subsidize unplanned pregnancy?
by dmforever
ponchi101 wrote: ↑Wed Jul 14, 2021 4:47 pm
Things like:
He lost his wallet in NYC. He finds out a bit later, when he tries to pay for something. His GF is going crazy; they are now with no credit cards or cash, only hers (smaller limits). They have no idea what happened, but they go back to the hotel, where his wallet is waiting for him. Somebody found it on the street and brought it to his hotel.
Magic.
I say: "Did you have your room key (nowadays invariably a card) in it?"
"Yes".
"The person only had to bring it back to the hotel, where you would be identified. The card told him what hotel you were in".
"In NYC? Where everybody is so rude? NO WAY!"
"People are not rude in NYC. The vast majority of people in the world are good. Since you lost it early in the day (most likely it fell from his backpack) you must have lost it close to the hotel. Maybe the person found it in the same block, because most likely you lost it when you were going out and indeed putting it inside your back pack".
"And he did not steal the money? NO WAY!"
"People are good, N. Would you steal money from a found wallet? No. And most people are like that".
No, no, no. It was magic. It was the power of his mind, because he always has a positive outlook of the world.
I bet you know the type.
Aeronautical engineering? Can you please tell me which planes he helped design so I can stay off them?
Kevin
by ponchi101
ti-amie wrote: ↑Wed Jul 14, 2021 7:06 pm
I'm also seeing this sentiment now.
From NYT comments on this article:
Delta Variant Widens Gulf Between ‘Two Americas’: Vaccinated and Unvaccinated
Data from overseas, particularly Britain, suggest the spread of the virus will set vaccinated and unvaccinated communities on very different paths. https://www.nytimes.com/2021/07/14/heal ... k-usa.html
H. Clark
Long Island, NY
The U.S. should build a database of all citizens unwilling to be vaccinated, and share those names with insurance carriers, Medicare and Medicaid. Anyone who refuses to be inoculated against Covid-19 who becomes ill with the virus will not be eligible for medical coverage, and that includes all care and/or hospitalization. Good luck with the $698,552.91 bill from your local hospital. And that’s if you live.
And of course...
...
That was MY IDEA!!!!! I wrote that in TAT1.0!!!!
I hate it when I get plagiarized...
Aeronautical engineering? Can you please tell me which planes he helped design so I can stay off them?
Kevin
He was very fond of the de Havilland Comet
He went back to Venezuela after that and, of course, never got involved in aviation.
And he is not a dumb guy. Very successful. But it is the one thing with these creeds: they fall down the hole and never, ever look back.
ti-amie wrote: ↑Wed Jul 14, 2021 7:06 pm
I'm also seeing this sentiment now.
From NYT comments on this article:
Delta Variant Widens Gulf Between ‘Two Americas’: Vaccinated and Unvaccinated
Data from overseas, particularly Britain, suggest the spread of the virus will set vaccinated and unvaccinated communities on very different paths. https://www.nytimes.com/2021/07/14/heal ... k-usa.html
H. Clark
Long Island, NY
The U.S. should build a database of all citizens unwilling to be vaccinated, and share those names with insurance carriers, Medicare and Medicaid. Anyone who refuses to be inoculated against Covid-19 who becomes ill with the virus will not be eligible for medical coverage, and that includes all care and/or hospitalization. Good luck with the $698,552.91 bill from your local hospital. And that’s if you live.
And of course...
...
That was MY IDEA!!!!! I wrote that in TAT1.0!!!!
I hate it when I get plagiarized...
I remembered seeing it here first. Don't be mad just do the dance.
The only thing is idiots will start making the argument that Person A didn't intend to get C19 and compare it to coverage for medical procedures like abortion after an unintended pregnancy. Maybe that's why it hasn't been done?
by Deuce In Japan (you know, the country which is insisting on the Olympics going ahead), COVID-19 rates are currently increasing more rapidly than they have in many months.
COVID-19 rates are also increasing significantly in 45 U.S. states.
No-one can say they weren't warned about lifting protections like the mask mandate...
Sigh...
by ponchi101 Argentina reached 100K deaths, with a population of 45MM. Translated to the USA population of 360MM (my approximation), that would be 800,000 deaths.
They have relied on Sputnik V, AZ and Chinese Sinopharm for their vaccination program.
by ti-amie
by JazzNU Cases were always going to increase this week and next. It's naive to have thought otherwise. Without the delta variant, we'd still have gotten a spike. No sense is shown by the masses when celebrating the 4th, and that goes for pre-pandemic as well. Fools are going out regardless, we had a spike last year too when none of the major variants were talked about.
Staten Island really showing everyone, huh? Nothing like proving your point from a hospital bed. Still not sure what the point is besides stupidity.
by ti-amie Staten Island is the most Republican borough. Make of that what you will.
by ti-amie Sometimes you have to let the dangerous people speak for themselves. I really think all of them are vaccinated and I don't think they believe any of the crap they say. I hesitate to call them stupid because they know what they're doing.
by JazzNU
ti-amie wrote: ↑Thu Jul 15, 2021 7:34 pm
Staten Island is the most Republican borough. Make of that what you will.
Oh I know. I'd think twice before calling emergency services right now. It'd need to be dire.
by dryrunguy Here's the latest Situation Report. Highlights include:
Indonesia is the new infection epicenter in Asia
A discussion of "breakthrough infections"
The Wuhan lab
Don't Fauci my Florida
Tennessee
Opioid overdoses skyrocketed in 2020 primarily due to COVID and severely reduced access to treatment
::
EPI UPDATE The WHO COVID-19 Dashboard reports 188 million cumulative cases and 4.06 million deaths worldwide as of 4:30am EDT on July 16.
Global Vaccination
The WHO reported 3.40 billion doses of SARS-CoV-2 vaccines administered globally as of July 15, including 1.31 billion individuals who have received at least 1 dose and 620 million who are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered continues to decline rapidly from the record high of 43.3 million doses per day on June 27, now down to 29.0 million. Daily vaccinations are decreasing steadily in Asia and North America, leveling off in Europe and Africa, and increasing in Oceania and South America. Our World in Data estimates that there are 2.02 billion vaccinated individuals worldwide (1+ dose; 25.9% of the global population). There are an estimated 988 million who are fully vaccinated (12.7% of the global population), although reporting is less complete than for other data.
UNITED STATES
The US CDC is reporting 33.8 million cumulative COVID-19 cases and 605,905 deaths. The US is averaging 26,306 new cases per day, more than double the low of 11,472 on June 20. Superficially, the epi curve over the past several weeks closely resembles the early stages of previous US surges. Daily mortality has increased over the past several days as well, up to 211 deaths per day from a low of 154 on July 11—a 37% increase over the past 4 days. If this is the beginning of a longer term increasing trend in daily mortality, it would correspond to a lag of 3 weeks behind the trend in daily incidence, which is consistent with trends we have observed over the course of the pandemic. Analysis from the New York Times indicates that all 50 states are exhibiting increasing daily COVID-19 incidence over the past 2 weeks, including 22 (plus Washington, DC and Puerto Rico) that have doubled or more over that period.
As the US continues to exhibit early signs of a COVID-19 surge, increasing daily incidence in some states is calling attention to disparities in vaccination coverage. This week, we will take a closer look at recent trends in incidence and vaccination coverage at the state level.
Among the 10 states with the lowest per capita weekly incidence, 7 are in the top 10 in terms of 1+ dose vaccination, and 7 are in the top 10 in terms of full vaccination. While the majority of states with lower weekly incidence also are reporting higher vaccination coverage, there are some notable exceptions. Michigan is currently reporting the lowest per capita weekly incidence (9.2 weekly cases per 100,000 population), but it ranks #24 in terms of 1+ dose coverage (52.2%) and #23 for full coverage (48.1%). Similarly, South Dakota is reporting the third lowest incidence, but it is #28 (51.3%) and #26 (46.2%) for partial and full vaccination coverage, respectively.
Among the 10 states with the highest per capita weekly incidence, 4 are reporting among the bottom 10 in terms of both partial and full vaccination coverage—Mississippi, Wyoming, Louisiana, and Arkansas—and Oklahoma ranks just outside the bottom 10 for partial coverage (#39) but ranks #41 for full coverage. Like with the states reporting lower incidence, there are exceptions here as well. Notably, Florida is #21 (55.2%) and #25 (47.3%) in terms of partial and full vaccination coverage, respectively, but it is reporting the third-highest per capita weekly incidence (183.2).
Analysis from the New York Times—which draws from official CDC and state data—provides the relative change in daily incidence over the past 2 weeks. Among those states in the top 10 largest changes, 4 are among the bottom 10 states in terms of vaccination coverage—Tennessee (+373%), Alabama (+194%), Louisiana (+185%), and Oklahoma (+155%). Notably, however, this list also includes Vermont (+211%) and Massachusetts (+208%), which are #1 and #2, respectively, in terms of full vaccination coverage. The low daily incidence in these 2 states results in large relative changes for even small increases in total daily incidence.
There appears to be an association between recent COVID-19 incidence trends and vaccination coverage at the state level, although on the surface, it is not quite as clear as might be expected. Additionally, the increased effect from full vaccination coverage is not quite as strong as we anticipated, and more detailed analysis is needed to better characterize the differences between partial and full vaccination. It is important to remember, however, that vaccination coverage and SARS-CoV-2 transmission are not distributed evenly across states, and community-level vaccination coverage is likely a better measure of protection. Pockets of lower vaccination coverage can provide ideal conditions for transmission, particularly in the absence of other protective measures, which have been largely lifted across the country.
US Vaccination
The US has administered 336 million cumulative doses of SARS-CoV-2 vaccines, and it is administering approximately 421,000 doses per day, holding relatively steady over the past several days. A total of 185 million individuals in the US have received at least 1 dose, equivalent to 55.8% of the entire US population. Among adults, 67.9% have received at least 1 dose as well as 9.7 million adolescents aged 12-17 years. A total of 160 million individuals are fully vaccinated, which corresponds to 48.3% of the total population. Approximately 59.2% of adults are fully vaccinated as well as 7.6 million adolescents aged 12-17 years.
INDONESIA The more transmissible Delta variant of SARS-CoV-2 is driving a steep increase in COVID-19 cases in Indonesia, the world’s fourth most populous country. Indonesian officials reported a record 56,757 new cases on July 15, with a 7-day average of 44,145, putting the nation ahead of India and Brazil and making it the pandemic epicenter in Asia. The test positivity rate is 29.3%, suggesting the number of infected people likely is much higher. Results from a survey published July 10 indicate that nearly half (44.5%) of Jakarta’s approximately 10.6 million residents may have acquired SARS-CoV-2 by the end of March. Nevertheless, the daily number of new cases recorded in the archipelago country has risen 10-fold since then. Hospitals across the country are at or nearing capacity, family members are buying up scarce oxygen supplies for home use, and gravediggers are working day and night. On July 3, the islands of Bali and Java entered an Emergency Community Activity Restriction (PPKM) in an effort to stem new infections, with President Joko Widodo urging residents to “remain calm and alert.” The government is working to increase the number of available hospital beds; provide treatments for 210,000 COVID-19 asymptomatic patients or those with loss of smell, fever, or cough; import additional oxygen supplies; and distribute rice and other food to fulfill a presidential order stating “that no one should go hungry.”
The government also is increasing vaccination efforts, implementing programs for junior high and high school students and door-to-door vaccinations. Indonesia has relied primarily on the Chinese-produced Sinovac SARS-CoV-2 vaccine for its national vaccination rollout, but some experts have raised concerns over that vaccine’s effectiveness against the Delta variant. In total, Indonesia has received nearly 138 million doses of the Sinovac, AstraZeneca-Oxford, and Moderna vaccines, enough to fully vaccinate 69 million people but far short of its goal of reaching 181 million by March 2022. On July 15, the Indonesian FDA (BPOM) authorized the Pfizer-BioNTech vaccine, and the country is set to receive 50 million doses. Only about 15% of the country’s population has received at least one dose of vaccine, with approximately 6% fully vaccinated. Coordinating Minister for Maritime Affairs and Investment Luhut Binsar Pandjaitan expressed hope that the government’s efforts would quickly begin to realize results, but it remains to be seen how the country will fare over the coming weeks.
SARS-COV-2 ORIGIN WHO Director-General Dr. Tedros Adhanom Ghebreyesus on July 15 said there had been a “premature push” to rule out the theory that SARS-CoV-2 escaped a Chinese laboratory and asked China to be more transparent and cooperative with investigators trying to determine the origins of the COVID-19 pandemic. Dr. Tedros’s remarks stray from the agency’s own report that concluded a laboratory leak was “extremely unlikely.” As we previously reported, most experts agree that SARS-CoV-2 was not man made nor genetically modified, and there is no empirical evidence suggesting the virus accidentally or intentionally escaped a laboratory setting. Nevertheless, the issue has become entangled in politics, with China arguing that attempts to link the pandemic’s origins to a lab are politically motivated and encouraging future attempts to search for the virus’s origin continue in other countries. In remarks to the media, Dr. Tedros renewed calls for China to share information about a government lab in Wuhan, the city where SARS-CoV-2 was first identified, saying, “If we get full information, we can exclude (the lab theory).”
US SURGE Following months of decline, the number of new daily COVID-19 cases is rising again in the US, more than doubling over the past 3 weeks. The increase in cases likely is being driven by the highly transmissible SARS-CoV-2 Delta variant, low vaccination rates in some regions, a loosening of prevention measures, and gatherings over the Independence Day holiday. Nationwide, 55.8% of the population has received one dose of vaccine and 48.3% is fully vaccinated. However, the 5 states with the largest 2-week rise in cases per capita all had vaccination initiation rates lower than the national rate: Missouri (45.7%); Arkansas (43.4%); Nevada (51.4%); Louisiana (39.5%); and Utah (50.5%).
US NIH Director Dr. Francis Collins expressed concern about the increase in cases in Missouri, where the Delta variant is spreading rapidly. The state is reporting a 7-day average of nearly 1,800 new cases each day, compared with about 400 at the beginning of June. In Los Angeles County, California, the Delta variant also is driving an increased number of cases. In response, the county is reinstating its indoor mask mandate for all residents regardless of vaccination status beginning July 17. Almost all of the county’s COVID-19 cases and related hospitalizations and deaths are among unvaccinated individuals. In contrast, Florida Gov. Ron DeSantis’s reelection campaign team this week unveiled new merchandise reading “Don’t Fauci My Florida,” at the same time the state is experiencing some of the greatest increases in new infections, COVID-19-related deaths, and hospitalizations per capita in the country.
BREAKTHROUGH INFECTIONS In order to understand the effectiveness of vaccination efforts, health officials are monitoring for signs of “breakthrough” infections—ie, infections in fully vaccinated individuals—which provide insight regarding both the degree of protection provided by the vaccines as well as risk factors that could affect that protection. But in order to effectively utilize these data, health officials must determine (1) what qualifies as a breakthrough infection and (2) whether they should treat all breakthrough infections equally. As we covered previously, clinical trials for SARS-CoV-2 vaccines utilized different metrics to estimate efficacy, and depending on whether you look at SARS-CoV-2 infection, symptomatic COVID-19 disease, or severe disease or death, vaccine efficacy can vary widely. An article published in The Atlantic takes a similar look at breakthrough infections.
From a strict epidemiological perspective, taken by the US CDC, any SARS-CoV-2 infection in a fully vaccinated individual is technically a breakthrough infection; however, breakthrough infections are not “synonymous with vaccine failure.” Breakthrough infections encompass a broad scope of disease severity, ranging from asymptomatic infections to severe disease and, in some instances, death. But the fraction of breakthrough infections that result in severe disease is extremely small, which is exactly what the clinical trial data illustrate. While the authorized vaccines’ efficacy against symptomatic COVID-19 disease is 90% or higher, the efficacy against severe disease is nearly 100%. Symptomatic breakthrough infections are not unexpected—nor are severe cases—but the vaccines have demonstrated their ability to drive that risk to nearly zero. In fact, the CDC has reported only 3,554 hospitalized breakthrough cases and 733 deaths out of more than 157 million fully vaccinated individuals*. Ultimately, the goal of vaccination is to prevent severe disease and death, and any additional benefit in terms of mitigating infection or transmission is a bonus. Based on the available data, it is clear that the SARS-CoV-2 vaccines are excelling, and they will remain a critical tool in preventing serious disease and death around the world as vaccination efforts continue.
*Through July 6; excluding asymptomatic individuals and those whose hospitalization or death was a result of other conditions.
J&J-JANSSEN VACCINE IMMUNITY DURATION Researchers from Janssen Vaccines and Prevention and Beth Israel Deaconess Medical Center conducted an 8-month Phase 1/2a clinical trial to assess the duration of immunity following vaccination with the J&J-Janssen SARS-CoV-2 vaccine (Ad26.COV2.S) and published interim results in the New England Journal of Medicine. The study consisted of 20 participants who received 1 or 2 doses of the vaccine and 5 who received a placebo. The researchers evaluated antibody and T-cell responses 8 months after the first dose—which corresponds to 6 months after the second dose for those who received 2 doses.
Antibody responses remained relatively stable over the study period and were detectable in all 20 vaccinated participants. The median neutralizing antibody titer decreased by a factor of 1.8 between the peak response on Day 71 and the end of the study, a relatively minimal difference over that period. In addition to the wild-type strain of the virus, the researchers also tested for antibodies against several variants of concern/interest (VOCs/VOIs), including Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2). The immune response to the VOCs/VOIs tended to be substantially lower early after vaccination (Day 29), but while the overall antibody response decreased slightly, the neutralizing antibody titers against the variants increased over time. By the end of the study period, the antibody response against the VOCs/VOIs reached levels comparable to those against the wild type strain, regardless of whether participants received 1 or 2 doses. This demonstrates both that the J&J-Janssen vaccine maintains sufficient protection over a prolonged period of time and stimulates increasing protection against emerging variants, even without a booster dose.
DELTA VARIANT TRANSMISSION In a report posted on the Virological discussion forum, researchers compared data from quarantined patients in a 2021 outbreak of the SARS-CoV-2 Delta variant (B.1.617.2) in mainland China to those of a 2020 outbreak caused by the 19A/19B genetic strains. Between May 21, 2021 and June 18, 2021, 167 cases of Delta were reported, all of which could be epidemiologically or genetically traced back to the index case. The time interval from exposure to first PCR positive test in the 2020 outbreak was 6 days, compared with 4 days in the 2021 outbreak. On the day of first detection, the relative viral loads of the Delta variant infections were 1,260 times higher than the 19A/19B strains infections, suggesting a higher within-host growth rate of Delta and a higher degree of infectiousness in the early days of infection. The researchers also note that this higher degree of viral replication for Delta likely results in an increased risk of viral mutation during outbreaks, underlining the need to quickly identify and quarantine people who have been exposed in outbreaks.
PEDIATRIC VACCINE CLINICAL TRIALS A recent study published in the New England Journal of Medicine reports that the Pfizer-BioNTech vaccine (BNT162b2) produced a greater immune response in 12-to-15-year-old participants than in young adults aged 16 to 25 and was highly effective against COVID-19 with a favorable safety profile. The ongoing multinational, placebo-controlled, observer-blinded trial randomly assigned 2,260 participants in a 1:1 ratio to receive two injections, 21 days apart, of 30 μg of vaccine (1,131 participants) or placebo (1,129 participants). There were no serious vaccine-related adverse events but some mild-to-moderate primary complaints, including injection site pain (79-86% of participants), fatigue (60-66%), and headache (55-65%). Among participants with no evidence of previous SARS-CoV-2 infection, no cases of COVID-19 with onset of 7 days or more after the second dose occurred in the vaccine group, while 16 cases were reported in the placebo group, resulting in an observed efficacy level of 100% (95% confidence interval [CI], 75.3 to 100). After dose 1 and before dose 2, there were 3 cases of COVID-19 in the vaccine group, and 12 cases in the placebo group (vaccine efficacy, 75%; 95% CI, 7.6 to 95.5). The Pfizer-BioNTech vaccine currently is the only SARS-CoV-2 vaccine authorized for younger individuals aged 12 and older.
SUMMER CAMPS & SCHOOLS In what some experts fear could be a forecast for the upcoming school year, recent COVID-19 outbreaks at summer camps have occurred in several US states. Camps in Illinois, Texas, Kansas, Florida, Utah, and Missouri have reported outbreaks among children and staff, with some leading to transmission in the wider community. Many of the camps did not require masking or physical distancing, and, from what we can ascertain, a majority of the cases were among unvaccinated campers and staff. Other camps—including 225 overnight and thousands of day camps run by local YMCAs—have been operating at slightly reduced capacity, requiring masks indoors, and taking other precautions, and have recorded only a few COVID-19 cases. Experts agree that vaccination is the best way to reduce the risk of COVID-19, but no SARS-CoV-2 vaccine is authorized for children under age 12. Until a vaccine is authorized for that population, the US CDC in updated guidance highlighted masking, physical distancing, improved ventilation, screening and testing, and other layered prevention measures for students and staff as schools resume in-person learning this fall.
TENNESSEE VACCINATIONS This week, the Tennessee (US) Department of Health suspended all adolescent vaccine outreach, including for SARS-CoV-2, stating the conversation surrounding the issue is “polarized” and highlighting the cessation as an opportunity to evaluate its messaging. In Tennessee, minors as young as 14 years are able to be vaccinated without parental consent under the state’s “Mature Minor Doctrine.” Notably, Tennessee lags behind most other states in SARS-CoV-2 vaccination coverage, ranking #43 with only 38% of its total population fully vaccinated.
Tennessee’s Health Commissioner, Dr. Lisa Piercey, reportedly directed health officials to stop sending second-dose reminders to teenagers and end all SARS-CoV-2 vaccine events on school property. But the effort expands beyond SARS-CoV-2 vaccines, including terminating outreach regarding routine vaccinations, including the HPV vaccine, as well as “pre-planning” for influenza vaccination events at schools. Additionally, health officials were directed not to acknowledge August as National Immunization Awareness Month. The decision is believed to be in response to a mid-June legislative hearing, during which several state lawmakers accused the health department of attempting to circumvent parents’ vaccine decisions and pressuring minors to get vaccinated. Reportedly, the hearing also included discussions about dissolving the health department entirely. Health department leaders are scheduled to appear again before the same group of lawmakers on July 21 for additional questioning.
On July 12, the Tennessee Department of Health reportedly fired Dr. Michelle Fiscus, the state’s Medical Director of Vaccine-Preventable and Infectious Diseases, without explanation. Dr. Fiscus published a 1,200-word letter in response to her dismissal, noting that she and other health officials have felt pressure as COVID-19 vaccinations have increasingly become politicized. The American Academy of Pediatrics issued a statement in support of Dr. Fiscus. Also on July 12, several experts published a commentary in JAMA Pediatrics arguing that teenagers should be allowed to decide for themselves whether to get vaccinated. US CDC Director Dr. Rochelle Walensky called Tennessee’s decision to halt vaccine outreach to teens “incredibly disturbing,” and the CDC has warned that pandemic-related disruptions to routine childhood vaccinations continue, which could lead to outbreaks of certain illnesses. These events help illustrate the risks of resource diversions and political divisions stemming from the COVID-19 pandemic spilling into broader public health efforts.
NATIVE AMERICAN VACCINATION Thanks to targeted efforts and historic levels of investment, US indigenous peoples have the highest vaccination rates in the country. Currently, the CDC COVID Data Tracker estimates that approximately 46.3% of American Indians/Alaska Natives (AI/AN) have received at least one dose of a SARS-CoV-2 vaccine, compared with 34.1% of the non-Hispanic white population and 26.5% of the Black population. According to the US Indian Health Service (IHS), AI/AN persons have infection rates up to 3.5 times higher than white persons and are 4 times more likely to be hospitalized. Given these grim statistics, the IHS, along with many non-affiliated indigenous health organizations, undertook massive campaigns to educate, vaccinate, and bring necessary supplies to US indigenous populations. A common rallying point to encourage people to get vaccinated is the sense of responsibility to one’s community and tribe, and the importance of preserving culture in the face of the pandemic. A report by the Urban Indian Health Institute recommends that vaccination campaigns center their efforts on tribal cultural values in order to encourage even more AI/AN persons to receive their doses.
DRUG OVERDOSE DEATHS According to provisional data released by the US CDC this week, more than 93,000 people died of a drug overdose in 2020, a nearly 30% increase over the number of overdose deaths in 2019. This estimate is the highest number of overdose deaths ever recorded and the largest percent increase since 1999. Public health agencies continue to fight the opioid epidemic, declared a public health emergency by the US government in 2017, but health departments were overwhelmed by the demands put on them during the COVID-19 pandemic. As a result, non-COVID-19 programs suffered. In addition, pandemic control measures such as lockdowns and stoppages of in-person treatment groups facilitated an environment that exacerbated conditions for those with substance use disorders. The combination of isolation and increasing barriers to treatment appear to have resulted in the staggering increase in overdose numbers for 2020. Preliminary estimates for 2021 do not show much improvement, although Congress did allocate an additional $1.5 billion this year to address the opioid epidemic in the context of COVID-19. Other useful federal measures include allowing patients enrolled in methadone clinics to take doses home with them and the use of federal funds to buy supplies for needle exchange programs, including rapid test strips that can detect fentanyl in drugs. The federal government also eased regulations to facilitate access to care through telemedicine services for people in treatment.
COMMUNIVAX REPORT As the US SARS-CoV-2 vaccination campaign continues, it is critical that vaccines are delivered fairly and equitably—to ensure everyone has access. CommuniVax, a coalition to strengthen the community’s involvement in an equitable vaccination rollout, this week released a new report, “Carrying Equity in COVID-19 Vaccination Forward: Guidance Informed by Communities of Color.” The report provides specific guidance on adapting SARS-CoV-2 vaccination efforts to achieve greater vaccine coverage in underserved populations, and through this, to develop sustainable, locally appropriate mechanisms to advance equity in health. The report provides 5 overarching policy and practice recommendations, across 2 focus areas: urgently providing vaccines for Black and Latino/Hispanic communities and putting in place essential changes to provide a more robust public health system moving forward.
by Suliso Here is the overall situation in Switzerland as of today. The red line indicates infections since March 1st and the violet number of people in hospital. Above red numbers average daily infections and the green are fully and once vaccinated (total 53%).
by ti-amie
by ti-amie
by Suliso Australia was the envy of many last year, but now they have really painted themselves in the corner with their zero covid strategy. It will never be zero abroad so now what?
by ponchi101 We also talked about it in TAT1.0. The strategy of locking up had limitations, and they are showing now. For example, we also talked about what would happen if we had never found a vaccine. How long could the world go on like that.
We had several models. The Aussie model was simply delaying; what is happening now was the expected outcome. The Swedish model was accepting it and braving a storm of infections and death, waiting for herd immunity. It did not go well.
But we would be in one of those scenarios if the vaccines had not been found in such record time.
by Suliso By the way the ultimate outcome in Sweden not really that bad. Currently #20 in Europe by covid deaths/million. Clearly worse than their immediate neighbors, but about average in the greater region. Better than USA too in case anyone is wondering and all that without any lock downs, school closures etc.
by ponchi101 I remember you were finding some very good info at TAt1.0, with the maps and lists/rankings for countries. Do you still have access to those?
by ti-amie
by Suliso
ponchi101 wrote: ↑Sat Jul 17, 2021 4:24 pm
I remember you were finding some very good info at TAt1.0, with the maps and lists/rankings for countries. Do you still have access to those?
Sure, just been too lazy to analyze.
by ponchi101 About France.
Yes, democracy does not equal you can be irresponsible. You don't get to drive without your seatbelt in a democracy. You don't smoke in a theater. And really, you should not walk around the streets, possibly carrying a deadly virus, when there is a vaccine.
And that is the country of Liberte, Egalite et Fraternite.
by ti-amie
by JazzNU That's a very simplistic view of things and only a claim she can make 2 months after the fact, so it clearly can't be just that. And also, though I like Lena, she's one of the ones who has been waiting to say "I told you so" since they changed the guidelines and I guess this is close enough.
The lifting of the mask guidelines for vaccinated people by the states, not the CDC since they have no power to do that, was also an incentive to get the vaccine. Because for a good stretch there, there was a "why should I get vaccinated if I still have to wear a mask?" question circulating loudly by many and it was disincentivizing getting the vaccine. The honor system rarely works and certainly doesn't in this context, but this is too simplistic and painting things too broadly especially because the change in guidelines also incentivized getting the vaccine.
by ti-amie Macron telling the French to fish or cut bait worked there. If President Biden did that here there'd be riots.
I never saw things working any other way than what Dr. Wen is saying. There are too many yahoos and knuckleheads out here to think relaxing mask requirements was going to make them do what they've been resisting for so long.
You may be right about the intent but that was a pipe dream.
by Suliso From Economist:
Anti-covid vax sentiment on the right, by contrast, is fuelled by the country’s deepest divisions and the conservative entrepreneurs, in media and politics, who aggravate them. It explains why America’s vaccination rate has slowed in recent weeks, despite the availability of vaccines, an uptick in infections and deaths, and the fact that a third of adults have not received a first dose. Surveys suggest this large minority is overwhelmingly Republican. It represents half the party’s voters, predictably dominated by its most pessimistic and conspiracy-prone groups, white evangelicals and rural folk: the Trumpian base.
The problem looks even worse—politically, economically and health-wise—where such voters are concentrated. Vaccination rates are lowest wherever Donald Trump romped to victory last November. In Tennessee, where he won 61% of the vote, 43% have had a first dose. In Ohio, a more divided state with a pragmatic governor in Mike DeWine, it is a slightly more hopeful 48%. But in the most conservative Ohioan counties, the rate plummets. In Holmes County where the former president won 83% of the vote, 15% of people have had a first dose. The chances of succumbing to the virus in such places is correspondingly high; 99% of America’s recent covid-19 fatalities had not been vaccinated.
The highlighted part is a surprise to me. I wouldn't have guessed it would be THAT low.
by ponchi101 But the numbers match. If Tiny won with 83% of the vote, that leaves 17% that did not vote for him. Take the 2% that always think it is smart to vote for a looney candidate, it leaves you the 15% that are vaccinated.
Oversimplified, of course, but the numbers are too close to not, at least, give it some attention.
JazzNU wrote: ↑Sat Jul 17, 2021 9:36 pm
That's a very simplistic view of things and only a claim she can make 2 months after the fact, so it clearly can't be just that. And also, though I like Lena, she's one of the ones who has been waiting to say "I told you so" since they changed the guidelines and I guess this is close enough.
The lifting of the mask guidelines for vaccinated people by the states, not the CDC since they have no power to do that, was also an incentive to get the vaccine. Because for a good stretch there, there was a "why should I get vaccinated if I still have to wear a mask?" question circulating loudly by many and it was disincentivizing getting the vaccine. The honor system rarely works and certainly doesn't in this context, but this is too simplistic and painting things too broadly especially because the change in guidelines also incentivized getting the vaccine.
Whether it's simplistic or not, it is an extremely accurate account of what occurred. And it was 100% predictable for anyone with an even partially functioning brain - so the level of intelligence of the people at the CDC must absolutely be questioned... Well, actually, there is no question - it should just be strongly criticized.
I don't know if the CDC actually ordered the removal of the mask mandate, but it did definitely issue a statement which said that vaccinated people need not wear masks in indoor public places - idiotically counting on everyone to be honest about it. This level of complete stupidity was obviously very dangerous - and very predictably so - and it should not go unpunished.
by Suliso At some stage restrictions will need to be removed anyway so why not now? Conventional wisdom says you keep them until you reach maximum vaccination level, but in USA maximum is reached already. Those Trumpers will not vaccinate themselves no matter what. Thus it would be logical to now relax and let them get immunity via disease. I see no other long term solution. Do you?
by Deuce
Suliso wrote: ↑Sun Jul 18, 2021 8:11 am
At some stage restrictions will need to be removed anyway so why not now? Conventional wisdom says you keep them until you reach maximum vaccination level, but in USA maximum is reached already. Those Trumpers will not vaccinate themselves no matter what. Thus it would be logical to now relax and let them get immunity via disease. I see no other long term solution. Do you?
With the high number of unvaccinated people, plus the current variants, and the unknown number and severity and resistance to vaccines of variants still to come, it is far too early to even think of long term solutions now.
The problem with the human animal is that it thoroughly lacks patience (and common sense). People want a universal cure yesterday (so that they can get back to doing tremendously important things like going to movie theatres and getting their hair done) - and so, as no such universal cure exists yet (because we are still very early in the overall timetable of a pandemic) - because there is no universal cure, people are simply pretending there is one.
Doing what the U.S. has done - which is, essentially, to pretend that the pandemic is over - is completely asinine, and shows the impulsivity and impatience of a 2 year old child.
by Suliso So what's your long term solution? Let's set long term at 5 years.
by Deuce I just said that it's far too early to find a long term solution.
There are still too many variables and unknowns.
And as I also just said, people are far too impatient. People have been conditioned to expect instant results and instant solutions to everything. But that's a fool's path.
And people are too egotistical, as well. People cannot admit that they don't know something. So they pretend. And that's dangerous.
by Suliso I strongly disagree. 1 1/2 years into the pandemic is by no means too early to think how we're going to deal with this in a medium and long term.
by Suliso I was just thinking what kind of big stick could US federal government wield to force Trumpers to vaccinate. It's a bit limited due to federal nature, but there are still some things. The most effective might be no flying (no exceptions) if you're not doubly vaccinated by September 1st. Dishonorable discharge from army/navy at the same date. The squeeze states by not giving aid to those who don't get their vaccination rate up to 80% adults.
Of course there will be riots, but let them riot...
by ponchi101 All of those "unimportant" things that people do FEED other people.
We had that conversation before. In countries with good social security, people can stay without a job longer because they have the support of the government. In the USA, the government can go and issue $3 Trillion in debt and deliver stimulus checks to the vast majority of the population and the economy goes on. Try to do that in South America and see how your economy burns overnight.
Glenn left this forum (actually TAT1.0) because when Drop and I explained that people in Colombia and Argentina simply could not remain locked in, not because they needed to be entertained but because they needed work, he found our opinions irresponsible. But the reality is that, worldwide, the service sector of the economy is far larger than the production sector, and that means people interacting with people. I have already stated that my mental health problem here in Colombia is walking to the frigging supermarket and running into 10-12 groups of people begging for alms. Or running into the professional musicians that take over a corner and stand there, singing and playing their music because the restaurant where they used to work went bankrupt. You go tell them that the restaurant and entertainment sector should remain closed until not one single person has Covid, which will be in 5 years, if we re lucky.
The role of governments is to make plans. Short, mid and long term. We, a small community, have zero power on what happens, but plans need to be made. What will happen if the percentage of purposely-non-vaccinated people remains at 40% is something every government should look into, because a reservoir of 40% means that the virus stays here for good, and will mutate accordingly. So ideas like what Suliso says need to be considered at government level:
After such a date, you don't get to fly, and I would extend that to using trains.
Companies have the right to terminate you if you refuse vaccination.
Children have to be vaccinated to attend school.
You purposely did not get vaccinated and your landed in an ICU? Your insurance is not responsible.
The pandemic is not over, that is clear. But life is not over either and a global plan to vaccinate and see if we can stop the virus is needed. Here in Colombia, everything is opening again but now we have the other side of the vicious circle: businesses are empty because, after 18 months of shutdown, the number of people WITH NO JOBS is so high we can't go and patronize a restaurant, or a theater, or a bar. I hate to use myself as an example but I had to stop playing tennis because I see no future employment, in the short or medium term. That means my tennis pro is not seeing my $30/session, twice a week. My car is under cover because my insurance lapsed, and I can use public transport fine, but that means the small place where I buy my insurance missed one payment. It cascades, on and on.
Us, the responsible ones, need to see what will the governments will do with the lunatics that feel that vaccination and wearing masks is useless. Because that percentage can bring everybody down, when they remain the incubation pool for variant Epsilon, Gamma and the others.
by ti-amie Los Angeles is shutting down again. The unvaxxed will mix with the vaxxed while Delta variant rages uncontrolled. This doesn't bode well.
by JazzNU
ti-amie wrote: ↑Sun Jul 18, 2021 6:12 pm
Los Angeles is shutting down again. The unvaxxed will mix with the vaxxed while Delta variant rages uncontrolled. This doesn't bode well.
Where are you reading that LA is shutting down? They re-instituted the mask mandate in the county, but I haven't seen anything about a shutdown.
ti-amie wrote: ↑Sun Jul 18, 2021 6:12 pm
Los Angeles is shutting down again. The unvaxxed will mix with the vaxxed while Delta variant rages uncontrolled. This doesn't bode well.
Where are you reading that LA is shutting down? They re-instituted the mask mandate in the county, but I haven't seen anything about a shutdown.
I rechecked and you are right. It's just the mask mandate for now.
by dryrunguy First, ponchi, I want to thank you for your thoughts, particularly as it relates to the harsh realities facing those in the majority world. Their options are severely restricted. Widespread access to a high-quality vaccine is probably the only thing that can save them--at least until the next pandemic hits.
::
Second, as for the U.S., I guess I have come to accept day-to-day life as something fairly similar to defensive driving. I can be a safe and conscientious driver, but I have no control over the person driving drunk, the person texting while driving, the dumb kid flexing his testosterone at 90 mph, or the elderly person whose eyes aren't so great anymore. When you drive, you have to look for any sign of trouble around you.
We CAN open up here in the United States, but each of us has to live defensively.
What burns me, though, is that these dingbats who scream "liberty" and "freedom" (two words that have completely lost their meaning since they've been completely adulterated) are the very same people who want to govern reproduction and whether LGBTQ folks should be allowed to marry or adopt children, etc. These idiots have completely ruined EVERYTHING. And they render any kind of legitimate, long-term plan nothing more than wasted ink.
by ti-amie
by Deuce
Suliso wrote: ↑Sun Jul 18, 2021 9:40 am
I strongly disagree. 1 1/2 years into the pandemic is by no means too early to think how we're going to deal with this in a medium and long term.
And I strongly disagree with your position on this. 1 1/2 years is a blip in life - even in the average duration of a human life. The problem, as I previously mentioned, is that people have been conditioned to expect instant results (and solutions) to everything. There is no speed of internet that is fast enough for people today - they always want faster and faster... That is but one example. Instant results; instant gratification - that's what people are expecting in everything, because technology - upon which people are increasingly dependent - provides those instant results.
The obvious problem is that, the faster things are done, the less properly they are done much of the time. The U.S. has fallen into this trap with the virus.
But this COVID-19 situation is not a video game. It's real life. Real people are really dying. Real people are really becoming really ill for really long periods. Real families are really being torn apart. So to pretend that the virus is under control - or that it has disappeared - just because we want it to be is as extremely irresponsible as it is extremely dangerous. As I've said previously - the U.S. is treating the virus as if it's merely an annoying bully, and expecting it to go away if it is ignored - like bullies usually do.
Human beings are also incredibly addicted to convenience. But convenience has a price - and most people are not willing to accept that. They want to have their cake and eat it, too.
And the ever-present ego problem I mentioned previously of not being able to accept that they don't know something - and so pretending to know, instead, which is dangerous.
In the end, I am saying the same thing that thousands of doctors and other medical professionals have been, and are, saying - because I trust their knowledge and experience and concern, and because, upon my personal analysis of the situation, even without any medical degrees, I reach the same conclusion as they. Take your argument that 1 1/2 years is long enough to be inconvenienced, and that 1 1/2 years is plenty of time to start taking control of the virus - take that argument to the medical professionals, and see how they respond.
Ponchi: As for my claim that people want too much of the unimportant stuff like the luxury of going to movie theatres and getting their hair done (which are absolutely luxuries in the midst of a pandemic) - I stand by my statement. I was, and am, commenting on the situation in the U.S. - where the appetite for entertainment is out of control. It is also out of control in other parts of the world. Even Dry wrote in a post last week that people's appetite for entertainment is going to end up killing them. I've been saying that for a couple of decades now, at least - in global terms. Like many things, it's a question of supply and demand. And as long as the demand to be perpetually entertained exists, we will be headed toward disaster. The 'economy' may well be 'healthy' as we ride that road straight to hell - but the destination is inevitable.
“How well-behaved are cows! When they approach me reclining in the shade, from curiosity, or to receive a whisp of grass, or to share the shade - they do not intrude. Their company is acceptable, for they can endure the longest pause; they have not got to be entertained.” ~ Henry Thoreau
by Suliso I'd win a Nobel prize before I convince you of even a tiniest thing on any topic you're not already convinced off. So whatever and let's agree to disagree.
by Deuce I can say exactly the same in the reverse direction. And that's fine.
I put experience (when available) and considerable thought into my positions and perspectives - they are not obtained flippantly, or due to a popular consensus. As a result, if I have a position/perspective on something, I believe in it. And so, yes, it is usually difficult for someone to change my position.
I don't believe the ultimate objective should necessarily be to change the other person's position, but rather to engage in discussion. If two positions oppose each other, that's ok. If everyone possessed the same position on everything, half the things that get done would not get done. It's even possible to learn something from the other's position without changing one's own position.
by ti-amie Re the Bubonic Plague:
How many people died because of the Black Death?
In Europe, it is thought that around 50 million people died as a result of the Black Death over the course of three or four years. The population was reduced from some 80 million to 30 million. It killed at least 60 per cent of the population in rural and urban areas. In fact, in some places such as a village on an estate in Cambridgeshire manorial rolls attest that 70 per cent of its tenants died in a matter of months in 1349, and the city of Florence tax records drawn up shortly before and after the Black Death suggest that its toll may have been about the same in 1348.
Some communities such as Quob in Hampshire were wiped out; many rural communities went into decline (and were in time deserted). We know that some populations survived, but medieval people had no such knowledge – all they believed was that everyone would certainly die.
The plague skipped over or barely touched some European villages, and may not have infected at all vast regions (such as ones in northern German-speaking lands). Given the state of record-keeping and preservation, we will probably never be able to estimate the Black Death’s European toll with any precision.
Hesitant Man Just Waiting To Observe Long-Term Effects Of Vaccine Over Next Several Eons
CORVALLIS, OR—Stressing that he was hesitant to get one until more evidence came to light, local man Jeff Bryan told reporters Monday that he was just waiting to observe the long-term effects of the Covid-19 vaccine over the next several eons. “Look, I get that people are saying it’s safe right now, but I think I’d rather wait another billion years or so to really get a sense of the potential consequences,” said Bryan, adding that he understood Covid was a pressing problem but didn’t see the issue of waiting until the fall of 202120201021 C.E. or so to decide whether to take the vaccine. “Sure, doctors are saying there’s no side effects now, but what about in 2.5 billion years? Frankly, I think anything under a few hundred million years is just too soon to know what this thing’s gonna do. Don’t get me wrong, I’m not a strict anti-vaxxer or anything like that, but I think it’s reasonable to ask what effects the vaccines will have on our children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children’s children.” Bryan added his hesitancy was also due to such a small number of overall vaccine recipients, which made their own experiences more anecdotal and less reliable as data, adding that he’d feel more comfortable after hearing how the vaccine affected a larger sample size of around 100 billion people.
by dryrunguy Here's the latest Situation Report. There's a lot to digest. What stood out to me was the weekend vandalism of vaccination sites in France, the Olympics (what the hell are these people thinking?), HIV and COVID, and new long COVID studies.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 191 million cumulative cases and 4.10 million deaths worldwide as of 6:00am EDT on July 20. Global weekly incidence increased for the fourth consecutive week, up 11.6% from the previous week and the highest weekly total since the week of May 24. Weekly global mortality increased for the second consecutive week, but the weekly increase was only 1.1% compared to the previous week.
Weekly incidence decreased in Africa for the first time since mid-May. Overall, the Americas are holding relatively steady over the past several weeks; however, reported cases in South America are declining, while reported cases in North America are increasing—both starting in late June. Case counts in other WHO regions are increasing as of late June.
Global Vaccination
The WHO reported 3.44 billion doses of SARS-CoV-2 vaccines administered globally as of July 19. The WHO reports a total of 1.35 billion individuals have received at least 1 dose, and 637 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered leveled off over the past week, now hovering at slightly more than 30 million doses per day. Vaccinations leveled off in Asia as well. Europe’s daily vaccinations are beginning to decline, down 11% over the past 2 weeks, and North America continues to decline steadily. Vaccination trends in Africa are increasing slightly, with daily vaccinations up 25% since the beginning of July. Trends in South America continue to increase steadily, and daily vaccinations leveled off in Oceania (with a slight decline) over the past week or so. Our World in Data estimates that there are 2.06 billion vaccinated individuals worldwide (1+ dose; 26.5% of the global population) and 1.02 billion who are fully vaccinated (13.1% of the global population).
UNITED STATES
The US CDC reported 33.9 million cumulative COVID-19 cases and 606,618 deaths. The US reported 29,578 new cases on July 16—more than 2.5 times higher than the low on June 18 (11,457)—before falling slightly on July 18 (26,011). Daily mortality also peaked on July 16, increasing from a low of 159 deaths per day on July 11 to 234 (+47%) before falling slightly to 218.
We have observed a similar trend over the past several weeks, with data reported early in the week indicating a slight decrease in the average daily incidence and mortality from Friday to Sunday. The trend disappears, however, after several days, which indicates that it is likely an artifact of reporting, potentially due to states shifting from daily to weekly reports to the CDC. This shift in reporting could complicate efforts to maintain an accurate understanding of the US COVID-19 epidemic in real time, particularly at a time when the country is facing the early stages of another surge. The most recent several days’ worth of COVID-19 data may no longer be a reliable representation of the current state of the US epidemic.
US Vaccination
The US has administered 338 million cumulative doses of SARS-CoV-2 vaccines. After reaching a low of approximately 425,000 doses per day on July 9 (the lowest average since January 2), daily vaccinations increased slightly over the next several days, up to 447,583*. A total of 186 million individuals in the US have received at least 1 dose, equivalent to 56.1% of the entire US population. Among adults, 68.3% have received at least 1 dose as well as 10.0 million adolescents aged 12-17 years. A total of 161 million individuals are fully vaccinated, which corresponds to 48.6% of the total population. Approximately 59.5% of adults are fully vaccinated, as well as 7.8 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current value provided here corresponds to 5 days ago.
CHILDHOOD IMMUNIZATIONS DISRUPTED The COVID-19 pandemic has disrupted routine immunizations for millions of children worldwide. According to data from WHO and UNICEF published July 15, 23 million children missed out on routine immunizations in 2020 due to the pandemic, with up to 17 million children not receiving a single vaccine in 2020. This lapse in routine vaccinations, the greatest since 2009, risks resulting in outbreaks of measles, polio, meningitis, or other vaccine-preventable diseases. Not only are these outbreaks dangerous to children and their communities, but they could burden health systems and reverse decades of progress in closing the global gap in vaccinations. Countries with the greatest increase in the number of children not receiving their first dose of diphtheria-tetanus-pertussis combined vaccine (DTP-1) include India, Pakistan, and Indonesia, all of which have come under strain during the pandemic. A recent study published in The Lancet examined the impact of the pandemic on childhood vaccine coverage and highlighted the need to strengthen health systems, surveillance systems, and targeted outreach programs in order to reach children who have missed routine immunizations. As countries begin to loosen COVID-19 restrictions, experts highlight the very real possibility of seeing increased transmission and outbreaks of vaccine-preventable pathogens.
PRIORITY REVIEW OF PFIZER-BIONTECH VACCINE Pfizer-BioNTech on July 16 announced the US FDA granted priority review status for the Biologics License Application for their 2-dose SARS-CoV-2 mRNA vaccine. An FDA official reportedly said a decision on whether to grant full approval for the vaccine’s use in people ages 16 and older will come soon, possibly within the next 2 months. The FDA must make its decision by January under the priority review. Pfizer-BioNTech completed their application in May and expects to apply for full approval for people ages 12 to 15 when data are available. Moderna has begun its application to the FDA for full approval of its 2-dose SARS-CoV-2 vaccine, and J&J-Janssen also is expected to seek full approval of its 1-dose vaccine. Full approval of a vaccine could impact US vaccination coverage by prompting vaccine mandates for some schools, businesses, or the US military, and by swaying some who are reluctant because of safety concerns to undergo vaccination.
VACCINE DISINFORMATION On July 15, US Surgeon General Dr. Vivek Murthy warned of the threat of health misinformation. As we covered previously, misinformation on a wide variety of topics has had a substantial negative effect on COVID-19 response and risk mitigation activities, including vaccination. Dr. Murthy emphasized that “health misinformation is an urgent threat to public health” and that it puts “American lives...at risk.” Notably, the announcement explicitly highlighted the role of social media platforms in spreading misinformation, and Dr. Murthy called on social media companies to take action in countering this ongoing threat. In a report published in March, the Center for Countering Digital Hate found that approximately two-thirds of all anti-vaccine misinformation found on social media platforms originates with one of 12 individuals. While some accounts operated by these individuals have been removed from social media platforms, many remain active. Dr. Murthy also called on the American public to refrain from sharing questionable information via their social media networks. Combating the far-reaching network that supports the spread of misinformation will require a “whole-of-society effort.” The health advisory outlines key principles for promoting accurate information, including identifying trusted voices in the community and longer-term investments in “media, science, digital, data, and health literacy.”
UK “FREEDOM DAY” England marked “Freedom Day” on July 19, with the government lifting all but a few COVID-19 restrictions amid a 41% surge in new cases over the past week. Prime Minister Boris Johnson defended his decision to open from his country residence, where he is isolating after coming into contact with UK Health Secretary Sajid Javid, who on Saturday said he tested positive for COVID-19 and is showing mild symptoms. The move into phase 4 of the country’s reopening plan removes limits on social gatherings and events, the need for physical distancing, and mask requirements except on public transportation.
Many experts see England's move to reopen as a major gamble, with more than 1,200 scientists signing a letter published in The Lancet calling the plan “dangerous and premature,” highlighting the likely negative impacts on children’s health and education, and warning the strategy “provides fertile ground for the emergence of vaccine-resistant variants.” Others say the reopening risks a massive wave of infections and will test the resilience of the nation’s health care system and the effectiveness of vaccines. Nearly 70% of the adult population is fully vaccinated, with 87.9% having received at least one dose.
On July 19, the country’s Joint Committee on Vaccination and Immunisation advised against the mass vaccination of all children and teenagers, instead opting to offer doses only to children between 12 and 15 who are at increased risk of serious COVID-19 disease—including those with "severe neurodisabilities, Down’s syndrome, immunosuppression, and multiple or severe learning disabilities"—and children and young people aged 12 to 17 who live with an immunocompromised person.
Also on July 19, the US CDC raised its UK Risk Assessment Level for COVID-19 to “Level 4: COVID-19 Very High,” prompting the US Department of State to raise its travel advisory level for the UK from “Level 3: Reconsider Travel” to “Level 4: Do Not Travel.” Notably, though the travel advisory is for the whole of the UK, the lifting of restrictions only impacts England, as Scotland, Wales, and Northern Ireland continue to make their own policies on COVID-19 restrictions.
FRANCE VACCINATIONS In an effort to control the surging Delta variant (B.1.617.2), French President Emmanuel Macron announced that proof of SARS-CoV-2 vaccination or a recent negative COVID-19 test must soon be provided to enter certain public venues or transportation. Beginning in August, a “green pass” will be required for anyone over the age of 12 to enter a cinema, theater, museum, theme park, or cultural center, and anyone entering venues like cafés, restaurants, shopping centers, or public transit must show the pass. Additionally, vaccination will be mandatory for anyone working in healthcare facilities and retirement homes, or assisting with elderly or other vulnerable people. Those employers and employees who do not comply could face sanctions or fines. The digital vaccine green pass will serve as a certification of vaccination and regulate entry to venues via a QR code specific to each person.
France has fully vaccinated 40% of its population, and the new restrictions on the unvaccinated are spurring people to get vaccinated. Immediately following Macron’s announcement, online French medical platform Doctolib received a record of more than 900,000 visits as people rushed to book their first vaccine dose. However, opponents of the requirement have taken to the streets in protest, citing government overreach. Several vaccination sites were vandalized over the weekend. Although polls suggest two-thirds of the population support the new measures, some claim the pass is too ambitious, may not clear institutional hurdles, and will infringe on personal freedoms. Health officials continue to fine tune the details of the health pass, and parliament is set to vote on the legislation.
OLYMPIC ATHLETES COVID-19 CASES With only days to go before the start of the 2020 Summer Olympic Games in Tokyo, Japan, reports of COVID-19 cases among Olympic athletes and other residents of the Olympic Village are clouding the already delayed event. Olympic organizers said at least 71 people have tested positive, including athletes, team officials, volunteers, contractors, and a “games-concerned personnel.” Two athletes and a video analyst with the South African soccer team tested positive in the Olympic Village despite receiving 2 negative tests within 4 days of traveling to Tokyo. Eight members of the UK delegation are in isolation after exposure to SARS-CoV-2 from an infected individual on their flight to Japan. At least 2 members of the US delegation are in isolation after an alternate for the US Women’s Gymnastics Team tested positive. Additionally, US tennis star Cori “Coco” Gauff on July 18 announced she will not compete in the Olympics after testing positive. Despite unprecedented measures to control COVID-19 during the Olympics, including daily testing and required masking when not training, competing, eating, or sleeping, the growing number of cases is raising questions over how well outbreaks can be controlled. At a press conference today, the head of the 2020 Tokyo Olympics organizing committee did not rule out a last-minute cancellation of the event.
HAJJ Historically, the annual Muslim pilgrimage to Mecca draws millions of visitors from around the world. Last year, Saudi Arabia limited visitors to only 1,000 pilgrims, but for the ongoing Hajj (July 17-22), the government is permitting a total of 60,000 visitors, limited to Saudi residents who are fully vaccinated, aged 18-65 years, and have no chronic health conditions. While this is considerably more people than were permitted in 2020, it is still far fewer than the more than 2 million who typically attend Hajj.
In order to reduce risk, the Saudi Ministry of Hajj and Umrah implemented additional restrictions and protective measures. Upon arrival, pilgrims are assigned to groups of 20, with no mixing between groups. Individuals are assigned specific dates and times to visit the Grand Mosque, where 6,000 individuals are permitted to enter every 3 hours. Facilities at the Grand Mosque undergo sterilization between each session. Despite the additional protective measures, including the vaccination requirement, the US CDC still has a Level 3 Travel Warning in place (Avoid Nonessential Travel) for the Hajj, due in part to the risk of SARS-CoV-2 transmission associated with mass gatherings.
VACCINE EQUITY The global inequities in access to SARS-CoV-2 vaccines are worsening, with wealthy nations continuing to stockpile instead of share unused doses and lacking a viable, well-funded global plan to reach poorer nations. For some nations dependent upon vaccine imports, the shipments have only recently begun, more than 1.5 years into the pandemic. COVAX has delivered only 135.5 million doses to 136 countries, and with little funding to purchase additional doses, the facility is left to depend upon donations from countries. Last week, COVAX launched an international marketplace to help address supply chain challenges hampering global vaccination efforts. The platform hopes to match vaccine producers with suppliers of vital components—such as bioreactor bags, biologic ingredients, or vials—who might have unused products needing to be reallocated.
Additionally, leaders of countries in the Asia-Pacific Economic Cooperation (APEC) trade group on July 16 pledged to expand their global sharing and manufacturing of SARS-CoV-2 vaccines, including encouraging voluntary transfer of technologies. However, they offered no specific details about how this expansion would be accomplished. Following the virtual meeting, New Zealand Prime Minister Jacinda Ardern, whose country serves as the current APEC host, said, “Our discussions moved us beyond vaccine nationalism. Now we are focusing on all aspects of contributing to the global vaccination effort—making vaccines, sharing vaccines, and using vaccines.”
HIV INFECTION HIV infection is a significant comorbidity for both severe or critical COVID-19 at hospital admission and in-hospital mortality, according to a WHO report released last week. The report described clinical surveillance data from 37 countries in Asia, Europe, Africa, and South America, and found that the risk of developing severe or fatal COVID-19 was 30% greater for people living with HIV compared with people without HIV, and 23.1% of all people living with HIV who were hospitalized with COVID-19 died. Other underlying conditions such as diabetes and hypertension increased the risk further, especially among men living with HIV over the age of 65 years.
In sub-Saharan Africa, home to two-thirds of people living with HIV, less than 3% of the population had received one dose of vaccine by July 2021, according to the UNAIDS Global AIDS Update 2021, also released last week. COVID-19 lockdowns and restrictions have disrupted HIV testing, referrals to care, and HIV treatment initiation and continuation. In some places, these disruptions bred ingenuity, with the emergence of new models of differentiated service delivery starting in communities worldwide, often guided by patients and advocates themselves. Health officials and organizations are detailing these efforts during the International AIDS Society Conference on HIV Science, which began July 18 in Berlin, Germany, and calling for continued flexibility to meet people’s lifestyles beyond the COVID-19 pandemic.
LONG COVID/PASC Researchers continue efforts to understand and treat post-acute sequelae of SARS-CoV-2 infection (PASC), commonly referred to as “long COVID.” PASC is a constellation of long-lasting symptoms following an initial infection with SARS-CoV-2 that can affect individuals regardless of the presence or severity of the acute COVID-19 symptoms. The UK announced it will provide £20 million (US$27.17 million) to support 15 clinical trials examining the diagnosis, treatments, and care of the condition. The studies will test existing drugs as therapies, look at the use of MRI scans for diagnosing organ damage, assess the possible role of overactive or impaired immune systems, and evaluate the impact of obesity among people with long COVID-19, among other objectives. The UK government previously allocated £100 million (US$36 million) for support services for people with long COVID-19, establishing 80 such services so far.
At least 4 new studies examining long COVID-19 recently were published. The first study, published in The Lancet’s journal EClinicalMedicine and the largest-ever international study on long COVID-19, identified more than 200 symptoms of the condition and prompted researchers—all of whom have had or are still living with long COVID—to call for the creation of a national screening program in the UK for anyone who suspects they have the condition. The second study, published in the Journal of the Royal Society of Medicine, found that people who experience 5 or more COVID-19 symptoms in the first week of infection are significantly more likely than people with fewer symptoms to develop long COVID-19. A third study, published in JAMA, found a low prevalence of long-term COVID-19 symptoms among a randomly selected cohort of children who were assessed at least 6 months after being tested for SARS-CoV-2. A fourth study, published in PLOS ONE, found that 26% of adult COVID-19 patients did not fully recover within 6-8 months after diagnosis, with 55% experiencing fatigue, 25% breathlessness, and 26% symptoms of depression. The researchers highlighted the need for accessible care for individuals experiencing long COVID-19 symptoms.
SUPER ANTIBODY In a study published July 14 in Nature, researchers describe a newly discovered “super antibody” capable of protecting against SARS-CoV-2 and a group of related coronaviruses, called sarbecoviruses. The antibody, named S2H97, is believed to work by attaching to a section of the ACE2 receptor binding motif on the virus spike protein that is only exposed when a sarbecovirus is attempting to enter a cell. S2H97 was able to prevent the spread of multiple sarbecoviruses between cells in a lab, and the antibody also protected hamsters from infection with SARS-CoV-2 isolated from the initial Wuhan, China, outbreak. Researchers further described the antibody as a pan-sarbecovirus due to its broad efficacy across the sarbecovirus subgenus. The description of a usually hidden antibody binding region in the ACE2 RBM is important because it could be used as a target for future vaccines and therapeutics. Additionally, a pan-sarbecovirus vaccine could be used to prevent outbreaks from as-of-yet-undiscovered members of the Coronaviridae family of viruses.
by MJ2004 I can't differentiate that Onion article from reality.
by ti-amie
by Jeff from TX
MJ2004 wrote: ↑Tue Jul 20, 2021 10:13 pm
I can't differentiate that Onion article from reality.
I agree - I just had a brief interaction with a person on Facebook who had this to say:
What's the point of getting this vaccine when there's already a 95 percent chance of survival, and it won't prevent you from catching Covid or spreading it?
My reply:
Virtually no vaccine can guarantee 100% immunity to the disease they are designed to protect. You mention that there is a 95% chance of of survival. What this fails to also address is that for many people, they survive, but that doesn't mean that they fully recover. If you choose not to get vaccinated, that is your choice, but please do not discuss this as if there are only 2 consequences - death and full recovery. Vaccination has been highly effective at mitigated the worst effects (besides death) from COVID.
His answer:
I will discuss it. The bottom line is that there really hasn't been enough research on the vaccine and here they are telling us we are better off with the vaccine. With all the evidence I've seen we aren't.
I'm can't really provide the research, because he wouldn't probably believe it anyway.
MJ2004 wrote: ↑Tue Jul 20, 2021 10:13 pm
I can't differentiate that Onion article from reality.
I agree - I just had a brief interaction with a person on Facebook who had this to say:
What's the point of getting this vaccine when there's already a 95 percent chance of survival, and it won't prevent you from catching Covid or spreading it?
My reply:
Virtually no vaccine can guarantee 100% immunity to the disease they are designed to protect. You mention that there is a 95% chance of of survival. What this fails to also address is that for many people, they survive, but that doesn't mean that they fully recover. If you choose not to get vaccinated, that is your choice, but please do not discuss this as if there are only 2 consequences - death and full recovery. Vaccination has been highly effective at mitigated the worst effects (besides death) from COVID.
His answer:
I will discuss it. The bottom line is that there really hasn't been enough research on the vaccine and here they are telling us we are better off with the vaccine. With all the evidence I've seen we aren't.
I'm can't really provide the research, because he wouldn't probably believe it anyway.
One other result of being vaccinated, of course, is that vaccinated people are less likely to pass the virus on to others. And the effect of the virus on others is, of course, unpredictable, as well.
Therefore, if you don't think you need to protect yourself from the virus by getting vaccinated, at least get vaccinated to protect other people. Who knows - you may even love some of them.
MJ2004 wrote: ↑Tue Jul 20, 2021 10:13 pm
I can't differentiate that Onion article from reality.
I agree - I just had a brief interaction with a person on Facebook who had this to say:
What's the point of getting this vaccine when there's already a 95 percent chance of survival, and it won't prevent you from catching Covid or spreading it?
My reply:
Virtually no vaccine can guarantee 100% immunity to the disease they are designed to protect. You mention that there is a 95% chance of of survival. What this fails to also address is that for many people, they survive, but that doesn't mean that they fully recover. If you choose not to get vaccinated, that is your choice, but please do not discuss this as if there are only 2 consequences - death and full recovery. Vaccination has been highly effective at mitigated the worst effects (besides death) from COVID.
His answer:
I will discuss it. The bottom line is that there really hasn't been enough research on the vaccine and here they are telling us we are better off with the vaccine. With all the evidence I've seen we aren't.
I'm can't really provide the research, because he wouldn't probably believe it anyway.
One other result of being vaccinated, of course, is that vaccinated people are less likely to pass the virus on to others. And the effect of the virus on others is, of course, unpredictable, as well.
Therefore, if you don't think you need to protect yourself from the virus by getting vaccinated, at least get vaccinated to protect other people. Who knows - you may even love some of them.
True - I just didn't have the energy to try to get into a long debate/education session
by MJ2004‘A form of brainwashing’: why Trump voters are refusing to have a vaccine
Pace of inoculations in the US is starkly correlated with politics
In downtown Little Rock, a chorus echoes around the room at Willy D’s Rock & Roll Piano Bar as groups of friends clutching beers and each other sing along to the soul hit “Stand By Me”.
Yet far from standing together, the capital of Arkansas is deeply divided over how to deal with a resurgence of Covid-19. Cases are increasing, hospitals are filling up and health officials are struggling to convince residents in the city and across the state to be vaccinated.
The pace of vaccinations in US states has become starkly correlated with politics, with Republican voters less likely than Democrats to have a jab, just as they are more reluctant to wear a mask or observe social distancing.
About 35 per cent of people in Arkansas are fully vaccinated, according to the Centers for Disease Control and Prevention (CDC), and only two states — Mississippi and Alabama — have lower rates of inoculation. By contrast, 56 per cent of people in the state of New York, a Democratic stronghold, have been fully vaccinated.
That poses a huge challenge for local health officials in red states as they battle the highly transmissible Delta coronavirus variant, which now accounts for 83 per cent of cases nationwide, according to the latest estimate from the CDC.
The public health agency, which last week said the US was experiencing a “pandemic of the unvaccinated”, believes the proportion of Delta cases is even higher in places with low inoculation rates such as Arkansas.
“I am very concerned about the next several weeks and months,” said Jennifer Dillaha, medical director of immunisations at the Arkansas health department. “The Delta variant is spreading in our state. The growth of cases is exponential. The rise in hospitalisations is exponential.”
Surging coronavirus cases risk overwhelming the health system in Arkansas, which serves a population of roughly 3m. More than 780 people are currently hospitalised with Covid in the state, a number that has roughly doubled in the past two weeks.
“If we continue at the same pace of hospitalisation, we will double the number of patients in the hospital by the beginning of August,” Dillaha predicted. “We’ll hit 1,300 patients or more, which is as high as we ever got in this past winter.”
In Willy D’s, customers must agree to a bag search and a pat-down by a security guard, but no one’s temperature is checked and masks are non-existent. Kevin Newman, a 31-year-old estate agent who voted for Donald Trump in November, said he had not been vaccinated because he doubted the severity of the virus.
“If Covid was really serious, we’d have to pay for the vaccine,” said Newman. “Everything else is expensive so why are they giving it out for free? It’s suspicious.”
Similar opinions abound on social networks such as Facebook, which last week was accused by President Joe Biden of “killing people” for allowing vaccine misinformation to spread unchecked.
Health officials in Arkansas are trying to reach more people by offering vaccines at shopping malls and churches, while doling out incentives such as free hunting and fishing licences. But so far their efforts have done little to move the needle.
At a riverfront summer festival in North Little Rock on Saturday, stalls offered free food and toys alongside Covid vaccines. Yet over the space of an hour, just four people took up the offer of a jab.
“Every one that we get now is important,” said Barbara McDonald, a nurse at the University of Arkansas for Medical Sciences (UAMS) who was running the pop-up site. “A lot of it is fear. If they don’t understand it, then they don’t want it. So education is important.”
Some of the reluctance is ideological, underpinned by the belief that being nudged into taking a vaccine imposes on a person’s civil liberties. Others fear the jab poses a significant risk to their health after reading discredited theories online.
Steven Shaw, a 58-year-old Trump voter, said he had read online that Covid vaccines can alter one’s DNA. “That’s my understanding, from what I’ve heard, that it’s not really a vaccine so I’m kind of leery of it.”
Shaw also criticised cruise ships that require vaccinated and unvaccinated people to occupy different areas of the vessel, likening the rules to the Holocaust. “In terms of separation, it’s the same thing what happened with the Jews in Nazi Germany.”
McDonald has worked 60- to 80-hour shifts each week at her hospital since the start of the pandemic, and noted that many of her patients now were people who refused to have a jab. “Inside I’m frustrated, but I can’t show that. I’ve just got to speak to people and educate them.”
Not everyone in Little Rock is against vaccinations. In Doe’s Eat Place, a rustic restaurant chain known for its steaks and hot tamales, the walls are adorned with grinning photos of regular customers, including Bill Clinton, the former US president and Arkansas governor. And the staff must wear masks.
Clinton’s popularity in Little Rock has declined dramatically since he left office, but for the restaurant, which sits in a heavily Republican city, the photos of and letters from the ex-president are a source of pride.
Suzie, a waitress at Doe’s, said vaccine hesitancy and politics were inextricably linked in Little Rock and Arkansas. “It’s become political and it’s hurting a lot of people . . . The rural areas especially are very conservative.”
That hurt is translating into higher hospitalisations across the state. Robert Hopkins, head of general internal medicine at UAMS, said that on one day last week the facility was “completely full” and patients were forced to wait in the emergency room.
Hopkins, who is also chair of the National Vaccine Advisory Committee, said patients now tend to be in their 40s, compared with the 60- or 70-year-olds who made up the bulk of admissions during earlier phases of the pandemic.
The deteriorating situation in Arkansas is replicated in red states across the country. Hospitals in neighbouring Missouri have been forced to transfer patients to other facilities and are seeking funding for more beds and staff.
“I don’t see anything turning it around, except vaccination,” said Dillaha from the Arkansas health department. “So if we’re not able to greatly increase our vaccination rate, then we’re going to be in for a very difficult fall.”
But far from encouraging people to be vaccinated, many Republican officials are pushing the other way. At least eight states with Republican legislatures and governors, including Arkansas, have banned schools and colleges from requiring vaccinations or proof of inoculation, for instance.
In April, Asa Hutchinson, the Republican governor of Arkansas, signed a bill banning government-imposed mask and vaccine mandates as well as vaccine passports, although he appears to have changed tack somewhat in recent days. Last week, he kicked off a statewide tour to encourage people to have a jab.
“It’s like he regrets it,” said Goldie Davis, a dental assistant, of Hutchinson’s apparent about-face, adding that her 34-year-old friend died from Covid on Friday. “Her whole family are Trumpers. It’s really sad. Everyone who’s not getting vaccinated are Trump supporters. It’s a form of brainwash almost.”
McDonald, the UAMS nurse, hopes that vaccine-hesitant people will eventually change their minds. “As more time goes by and they know somebody who’s been vaccinated, and they see that they’re OK, they haven’t grown a tail or something, and then they’ll get vaccinated.”
She added: “You just pray and hope.”
Data reporting by Christine Zhang
- FT
I just can't. If this guy had to pay for the shot, he'd complain it's too expensive and that would be his excuse. And the second guy, I really just can't.
MJ2004 wrote: ↑Tue Jul 20, 2021 10:13 pm
I can't differentiate that Onion article from reality.
I agree - I just had a brief interaction with a person on Facebook who had this to say:
What's the point of getting this vaccine when there's already a 95 percent chance of survival, and it won't prevent you from catching Covid or spreading it?
My reply:
Virtually no vaccine can guarantee 100% immunity to the disease they are designed to protect. You mention that there is a 95% chance of of survival. What this fails to also address is that for many people, they survive, but that doesn't mean that they fully recover. If you choose not to get vaccinated, that is your choice, but please do not discuss this as if there are only 2 consequences - death and full recovery. Vaccination has been highly effective at mitigated the worst effects (besides death) from COVID.
His answer:
I will discuss it. The bottom line is that there really hasn't been enough research on the vaccine and here they are telling us we are better off with the vaccine. With all the evidence I've seen we aren't.
I'm can't really provide the research, because he wouldn't probably believe it anyway.
One other result of being vaccinated, of course, is that vaccinated people are less likely to pass the virus on to others. And the effect of the virus on others is, of course, unpredictable, as well.
Therefore, if you don't think you need to protect yourself from the virus by getting vaccinated, at least get vaccinated to protect other people. Who knows - you may even love some of them.
True - We have some vaccinated friends that we get together with, but one of them has recently been through chemo & radiation treatments, so although she's vaccinated, she is likely still immune compromised. She will not get together with anyone who has not been vaccinated. I'm currently in Vermont, so not too concerned about masking when not in a crowded place, but if I was back home in GA, you bet I would still be masking for any indoor activities where I didn't know the status of those around me.
by ponchi101 Plenty of articles so I will not link to one.
China has decided to stop the W.H.O. investigation into the origin of the virus. Like any country which acted responsibly about this pandemic would.
by JazzNU
by MJ2004 The final paragraph of the article Jazz linked to:
“And the one question that I always ask them is, did you make an appointment with your primary care doctor and ask them for their opinion on whether or not you should receive the vaccine? And so far, nobody has answered yes to that question.”
I swung by here for the sole purpose of sharing the same link, Jazz. It was linked in this morning's NY Times e-newsletter. Very depressing.
by ti-amie
by ti-amie I think Macron's approach is catching on.
Self paid
by ti-amie
by Suliso I have limited sympathy left for those who haven't even started the vaccination process (in EU or US only). If you want to take such a substantial risk go ahead...
by ti-amie
by Deuce Yes, Clapton and Van Morrison are together in their 'anti-vaccine' stance.
I have a once fairly well known musician friend who has worked with Clapton, and he calls Clapton an idiot for his position on COVID-19 and vaccines. He also calls Morrison 'a sociopath' - which I think is a rather accurate description.
by ponchi101 Lately, I come to this and a few other topics, and I really get this urge to lock all topics NOT related to tennis.
It is so despairing.
(And no, I won't. Tog won't let me )
by Togtdyalttai
ponchi101 wrote: ↑Fri Jul 23, 2021 2:14 am
Lately, I come to this and a few other topics, and I really get this urge to lock all topics NOT related to tennis.
It is so despairing.
(And no, I won't. Tog won't let me )
I mean, you could always strip me of administrator privileges I post so infrequently that people might not even realize I'm an administrator anyway.
by ponchi101 Serious question here.
Cases are going up, in several countries. But vaccination continues. As more people get vaccinated, they will return, to one degree or another, back to a more "normal" life. Which means that, if 1 MM people are vaccinated but go out more, a 95% vaccine effectiveness will mean 50,000 people getting the virus.
Yet mortality is not increasing at the same rate.
My question is: the vaccine was never meant to stop the virus completely. it is not 100% effective. But, what the vaccine also does, is that it diminishes the effects of the virus. If I am fully vaccinated and still catch the virus, but it turns it into a weekend flu, it has worked. I am alive and spent nothing more than a few days with the equivalent of a bad cold.
So the reporting of increased cases, but not reporting the new split of cases that end in fatalities, seems to be insufficient, from the point of view of the statistical analysis.
by ponchi101 Unrelated.
The USA has donated 3.5 million MODERNA vaccines to Colombia for VENEZUELAN IMMIGRANTS.
3.5 million more than China or Russia.
by JazzNU
ponchi101 wrote: ↑Fri Jul 23, 2021 3:53 pm
Serious question here.
Cases are going up, in several countries. But vaccination continues. As more people get vaccinated, they will return, to one degree or another, back to a more "normal" life. Which means that, if 1 MM people are vaccinated but go out more, a 95% vaccine effectiveness will mean 50,000 people getting the virus.
Yet mortality is not increasing at the same rate.
My question is: the vaccine was never meant to stop the virus completely. it is not 100% effective. But, what the vaccine also does, is that if diminishes the effects of the virus. If I am fully vaccinated and still catch the virus, but it turns it into a weekend flu, it has worked. I am alive and spent nothing more than a few days with the equivalent of a bad cold.
So the reporting of increased cases, but not reporting the new split of cases that end in fatalities, seems to be insufficient, from the point of view of the statistical analysis.
Well, they aren't really doing that here at least. Cases are going up for sure, but it has been repeatedly emphasized that the unvaccinated are currently making up 99% of the deaths and 97% of the hospitalizations. Louisiana is one place experiencing a crazy surge right now, and I think it was 93 or 94% unvaccinated making up the new cases. They've been giving out stats in most things I've read or watched here to make it clear, yes, cases are going up and yes well all need to be more careful, but those who are vaccinated have very little to worry about in the long run (which is why they gave the guidelines they did), and the unvaccinated are the ones that are seriously at risk. They're calling it the "pandemic of the unvaccinated."
Starting to possibly get through to some of the COVIDIOTS. States with a lot of cases and low vaccination numbers have started seeing an increase in vaccinations in the last week or two, let's hope it's a trend that takes off.
by ti-amie This thread is very interesting. We mentioned this here but here's someone else asking the same questions we did.
by ti-amie I guess she didn't get the briefing or the memo...
by Suliso By the way it has been estimated that ca 4 million people have died of covid in India so far, mostly from the current delta variant. The worst performing country in absolute numbers so far.
by ponchi101 What is our estimated death toll, then? I mean just us here at TAT2.0. I would say that at a minimum you have to double the worldwide figure. Put it at around 7MM. Many countries in the beginning simply were not counting deaths as C19 related. Ecuador would be an example.
by Suliso Another piece of statistics: in EU 50% adults have been fully vaccinated and 70% have received the first dose (US 60% and 69%). Unfortunately just like in US there are very large regional differences.
Switzerland also behind the average - 46% and 53% from the entire population (US 49% and 56%). Modest regional differences here with people in the countryside and in the mountains more against. The bigger gap is between the old and the young. 20-29 age group has not reached 50% yet even for a single dose.
by Suliso
ponchi101 wrote: ↑Fri Jul 23, 2021 5:58 pm
What is our estimated death toll, then? I mean just us here at TAT2.0. I would say that at a minimum you have to double the worldwide figure. Put it at around 7MM. Many countries in the beginning simply were not counting deaths as C19 related. Ecuador would be an example.
I would say somewhere between 10 and 15 million so far (0.13-0.2% world population). The official number is 4.2 million.
by Suliso Also you might think India's death rate is enormous. Actually not really, the natural population growth last year was 0.99% or 13.5 million people. So statically it's just a blip and will only affect families of those who have died.
by JazzNU Many have mentioned it before, but worth repeating. The Republican about-face occurred immediately after the market had that mini-meltdown the other day. That briefing could've easily spelled doom about their stock and retirement portfolios, something they certainly care about more than they care about people.
by ti-amie
JazzNU wrote: ↑Fri Jul 23, 2021 6:11 pm
Many have mentioned it before, but worth repeating. The Republican about-face occurred immediately after the market had that mini-meltdown the other day. That briefing could've easily spelled doom about their stock and retirement portfolios, something they certainly care about more than they care about people.
I'm glad you tied the two events together. I think both the markets and the GOP (and Dems) got the same information one way or another. The market crash was the powers that be telling the Repubs to stop the nonsense. Whatever the news was it was deadly serious, no pun intended.
by dryrunguy Wait. Where are these data indicating that white people in these red states (the Republican base) are dying at higher rates NOW than they were a year ago compared to racial and ethnic minorities? I am not aware of any data indicating anything has changed in terms of the ethnic composition of current COVID-related morbidity and mortality. All along, COVID-related morbidity and mortality has disproportionately affected people of color, particularly Blacks, Hispanics, and Tribes.
That is literally the ONLY kind of data that would cause Republicans to suddenly start giving a rat's ass. Which then begs the question: Since when do Republicans actually care about legitimate data?
by dryrunguy Meanwhile, here's the latest Situation Report. The folks at WHO are clearly NOT impressed with Argentina at the moment. They also took a stab at estimating the true death toll in India, which is pretty consistent with the number mentioned here.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 192.3 million cumulative cases and 4.14 million deaths worldwide as of 11:11am EDT on July 23.
Countries around the world are combating new COVID-19 surges, generally believed to be driven, in part, by increasing prevalence of the Delta variant (B.1.617.2). Unlike in previous surges, there do not appear to be strong regional trends, with the countries facing the largest surges distributed around the world. In fact, looking at the biweekly trends, there are approximately 50 countries where daily incidence has more than doubled, and they are spread across nearly every continent and region, with the notable exceptions of Central and South America.
In terms of total daily incidence, there are 15 countries reporting more than 10,000 new cases per day, including 6 reporting more than 25,000. Among these countries, 5 are in Asia (including Iran in the Eastern Mediterranean region), 4 are in Europe, 3 are in South America, and 2 are in North America. South Africa is the only African country, and none are in Oceania. Ten (10) of these countries are reporting increasing daily incidence over the past 2 weeks, including the US (+142%), Spain (+146%), and France (+287%), which more than doubled over that period. India and Argentina have exhibited decreasing trends since at least mid-June, and Brazil, Colombia, and South Africa passed their respective peaks since the beginning of July. These 16 countries account for nearly 75% of the global daily incidence. Among the countries with available data on the Delta variant, all* are exhibiting sharp increases in Delta prevalence over the past several months. India, where the variant was first reported, was first in March, and Delta prevalence began increasing in most of the other countries by late May/early June. Of the 10 countries with data available for July 12 or later, 8 are reporting higher than 70%, including 6 higher than 90%.
*Argentina does not have data available after May 17.
Similarly, the top countries in terms of per capita daily incidence represent most regions around the world. Among the top 20 countries, nearly half (9) are in Europe, 4 are in Africa, 3 are in Latin America and the Caribbean, and 3 are in Asia. Fiji is the only country in Oceania, and none are in North America. Argentina, Colombia, Malaysia, Spain, and the UK are on both lists, and considering their large populations compared to the other top per capita countries, this further illustrates the severity of their respective epidemics. All but 5 countries—Argentina, Colombia, Mongolia, Namibia, and Seychelles—are reporting increasing daily incidence over the past 2 weeks, including 9 that more than doubled over that period. Notably, Malta’s daily incidence increased nearly 1,500% over the past 2 weeks (peaking at more than 3,000% on July 16), bringing its daily average to approximately 200 new cases per day—up from 1 in mid-June. Only a small handful of these countries have data available regarding the prevalence of the Delta variant, and 4 of the 8 countries were also among the highest total daily incidence. All of these countries** reported major increases in Delta prevalence starting in May, and 5 of the 6 countries with data available for July 12 or later are reporting 80% or higher.
**With the exception of Argentina, which has no data available after May 17.
Global Vaccination
The WHO reported 3.57 billion doses of SARS-CoV-2 vaccines administered globally as of July 20. The WHO reports a total of 1.37 billion individuals have received at least 1 dose, and 656 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered fell sharply once again, now down to 29.1 million doses per day. Our World in Data estimates that there are 2.09 billion vaccinated individuals worldwide (1+ dose; 26.9% of the global population) and 1.05 billion who are fully vaccinated (13.5% of the global population).
UNITED STATES
The US CDC reported 34.2 million cumulative COVID-19 cases and 607,684 deaths. With more than 40,000 new cases per day, the US surpassed both the peak of the initial surge—31,327 on April 12, 2020—and the low reported following the summer 2020 surge—35,082 on September 13, 2020. The current average is more than 3.5 times the most recent low on June 19 (11,467) and is still increasing steadily. Daily mortality also continues to increase, up to 223 deaths per day, which is more than 40% higher than the most recent low on July 11 (159). Notably, the proportion of emergency department patients diagnosed with COVID-19 has tripled since June 21, up from 0.6% to 1.8%, which is an indication of increasing burden on health systems*.
*In an effort to provide a more accurate analysis of the current epidemiology, we are largely focusing on longer-term trends, as the most recent data are more likely to be affected by changes in the frequency of state-level reporting, particularly over the weekend.
The US CDC added a new feature to its COVID-19 Data Tracker, which displays a combination of vaccination coverage and per capita weekly incidence at the county level. The 2-dimensional coloring scheme will take some time to interpret, but it is fairly clear that the major US COVID-19 hotspots are Missouri, Arkansas, and Louisiana, where counties are reporting lower vaccination coverage and higher weekly incidence. Alabama and Mississippi are exhibiting similar trends, but to a lesser degree. Many counties in Florida are reporting elevated weekly incidence, even with higher vaccination coverage than in neighboring states. No data are available for Texas.
US Vaccination
The US has administered 340 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations are increasing slowly, now up to 446,613 doses per day*. A total of 187 million individuals in the US have received at least 1 dose, equivalent to 56.4% of the entire US population. Among adults, 68.6% have received at least 1 dose as well as 10.2 million adolescents aged 12-17 years. A total of 162 million individuals are fully vaccinated, which corresponds to 48.8% of the total population. Approximately 59.7% of adults are fully vaccinated, as well as 7.9 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current value provided here corresponds to 5 days ago.
DELTA VARIANT The US CDC continues to sound the alarm about the rapid spread of the SARS-CoV-2 Delta variant within the United States. Earlier this week, CDC Director Dr. Rochelle Walensky shared that the Delta variant now makes up 83% of domestically sequenced SARS-CoV-2 cases. This is a dramatic rise from the beginning of the month, when the Delta variant made up about half of sequenced cases within the US. There has been a corresponding rise in the number of new COVID-19 cases and related deaths throughout the month, especially impacting unvaccinated parts of the population. In a press conference earlier this week, Dr. Walensky warned that the Delta variant is one of the “most infectious respiratory viruses we know of,” urging individuals to get vaccinated. The CDC has made it clear that this will be another pivotal moment in the United States’ COVID-19 response, cautioning that many communities with low vaccination rates may face challenges of overwhelmed health care systems if preventative actions are not taken.
US CDC ACIP MEETING The US CDC’s Advisory Committee on Immunization Practices (ACIP) on July 22 concluded the benefits of the J&J-Janssen SARS-CoV-2 viral vector vaccine outweigh the risks of some people developing the rare neurological disorder Guillain-Barré syndrome (GBS) after receiving the shot. Earlier this month, the US FDA updated the J&J-Janssen vaccine’s label to warn of a possible increased risk of GBS. According to data presented at the meeting, the FDA’s Vaccine Adverse Event Reporting System (VAERS) recorded 100 preliminary reports of GBS after J&J-Janssen vaccination as of June 30, out of 12.6 million doses administered at that time. Of those cases, 95 required hospitalization, 1 person died, and 5 cases were non-serious. Dr. Hannah Rosenblum, a researcher with the CDC National Center for Immunization and Respiratory Diseases’ Division of Viral Diseases, presented data showing the risk of vaccine recipients developing GBS remained low when compared to the number of COVID-19 cases and deaths prevented by vaccination. The CDC plans to update its guidance for the J&J-Janssen vaccine to recommend that patients with a history of GBS first consider the 2-dose mRNA vaccines from Pfizer-BioNTech and Moderna, if possible. However, some panel members pointed out there are risks associated with those vaccines as well, including myocarditis and pericarditis, and that information on all of the risks associated with SARS-CoV-2 vaccines should be made available so people can make the best choice for themselves.
The ACIP also considered whether to recommend additional, or “booster,” doses of SARS-CoV-2 vaccines for people who are immunocompromised, who represent about 2.7% of the US population. Dr. Sara Oliver with the CDC National Center for Immunization and Respiratory Diseases presented data based on several small studies looking at vaccine response among immunocompromised people and additional doses in this population. Although emerging data suggest an additional SARS-CoV-2 vaccine dose in immunocompromised people enhances antibody response and increases the proportion who respond, the panel did not make an official recommendation on additional shots and will continue to review available data. Dr. Oliver also noted that serologic or cellular immune testing outside of research studies is not recommended in the US at this time. Some panel members expressed concern over immunocompromised patients getting additional vaccine doses without an official recommendation to do so, saying “the issue is almost running away from us.” Although another ACIP meeting is not yet scheduled, the panel is expected to meet again in August.
GAO PREPAREDNESS & RESPONSE REPORT The US is concurrently responding to and recovering from the COVID-19 pandemic, with an ongoing national vaccination campaign and widespread loosening of public health measures amid a recent increase in cases. Recognizing this balance as “fragile,” the US Government Accountability Office (GAO) on July 19 released its 7th comprehensive report on the COVID-19 pandemic, providing an additional 15 recommendations to various US government agencies. Previous reports included a total of 72 recommendations on COVID-19, with agencies agreeing to implement 57 of them and having fully implemented 16 to date. The most recent report makes several recommendations related to national pandemic preparedness, including advice to the CDC to develop a plan to enhance surge capacity for laboratory testing and establish contracts for the manufacturing and deployment of diagnostic test kits prior to public health emergencies. The GAO also made suggestions to the US Department of Health and Human Services’ (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR) regarding the organization and oversight of the country’s Strategic National Stockpile (SNS), which provides medical supplies and other materials to respond to a broad range of emergencies. Several other recommendations relate to the oversight, timely use, and integrity of COVID-19 relief funds allocated to HHS, the US Department of Education, US Department of the Treasury, US Office of Management and Budget (OMB), and Internal Revenue Service (IRS). According to GAO, if effectively implemented, the recommendations “can help improve the government’s ongoing response and recovery efforts as well as help it to prepare for future public health emergencies.”
EXPIRING VACCINES With demand for SARS-CoV-2 vaccination largely leveling off in the US over the past 3 weeks, millions of SARS-CoV-2 vaccine doses are set to expire in the next few months. Several states and some global health experts are calling for the excess doses to be redistributed to other countries, but so far the US government has rejected those requests, citing legal and logistical challenges. However, states are now able to request a specific number of vaccine doses instead of having doses distributed to them based on their population. Delayed reporting, everyday wastage, and waning demand, including those who did not go back for second doses, are among the sources for a pile up of inventory. The FDA previously extended the shelf-life of the Pfizer-BioNTech and J&J-Janssen vaccines, and some hope an additional extension for the Pfizer-BioNTech vaccine will be approved. Meanwhile, the federal stockpile of vaccine doses continues to grow, with approximately 390 million of the 1.41 billion doses purchased by the US having been delivered, and another 562 million doses from Moderna, Pfizer-BioNTech, and J&J-Janssen expected to be delivered by the end of 2021. The White House has pledged to donate 80 million doses of its vaccine supply, and will purchase an additional 500 million doses for low- and lower-middle-income countries. But some experts note the doses currently sitting in states are ready to be administered, not waiting to be manufactured, and those doses could have a positive impact in other countries if states were permitted to redistribute them.
VACCINE MANDATES As SARS-CoV-2 vaccines become more widely available, some organizations, schools, and businesses are considering making them mandatory. This week, a US federal judge ruled to uphold a mandatory vaccination policy implemented by Indiana University, which would require SARS-CoV-2 vaccination for students, faculty, and staff before returning to campus this fall. The ruling acknowledges that the university has the authority under the Fourteenth Amendment to the US Constitution to pursue reasonable measures to protect the “public health for its students, faculty, and staff.” The students who filed the original suit are reportedly appealing the judge’s ruling.
On July 22, the American Hospital Association, the country’s largest association of hospitals and health systems, issued a statement in support of mandatory SARS-CoV-2 vaccination for healthcare workers. The statement argues that the vaccines have been demonstrated to be both safe and effective, and they play a critical role in protecting the health of both healthcare workers and their patients, many of whom are at elevated risk of severe COVID-19 disease. There have been several notable examples of hospitals firing employees who refused the vaccine, and the issue will certainly receive ongoing attention, especially until the vaccines receive full FDA approval.
VACCINE EFFICACY AGAINST VOCs A recent bioRxiv preprint study compared neutralizing antibody titers elicited by the 3 SARS-CoV-2 vaccines authorized for emergency use by the US FDA against pseudotyped variants of concern (VOCs) and variants of interest (VOIs). The small study compared blood samples from 17 people who had the 2-dose mRNA vaccines from Pfizer-BioNTech and Moderna and 10 people who received the single-dose viral vector vaccine from J&J-Janssen. Overall, the study showed a high level of antibody cross-neutralization elicited by the Pfizer-BioNTech and Moderna vaccines against VOCs but significantly decreased neutralization by antibodies generated by the J&J-Janssen vaccine. Because the study was conducted using blood samples, it might not reflect real-world performance, but the results counter previous reports of the J&J-Janssen vaccine’s efficacy against the Delta variant. The authors of the bioRxiv study, which is not yet peer-reviewed, said they hoped the findings did not discourage people from getting the J&J-Janssen vaccine but that future recommendations included advice for an additional second dose of that vaccine or an mRNA vaccine. The authors also called for continued surveillance of breakthrough infections to help determine the real-world effectiveness of the vaccines.
Another study evaluating vaccine effectiveness against the Delta variant was published July 21 in the New England Journal of Medicine. This study compared the effectiveness of the Pfizer-BioNTech mRNA vaccine and AstraZeneca-Oxford viral vector vaccine against the Alpha and Delta variants. Following 1 dose of the 2-dose vaccines, effectiveness was notably lower among persons with the Delta variant (30.7%) than among those with the Alpha variant (48.7%), with the results similar for both vaccines. Following a second dose, the Pfizer-BioNTech vaccine was 93.7% effective against Alpha and 88% effective against Delta. The AstraZeneca-Oxford vaccine after 2 doses was 74.5% effective against Alpha and 67% against Delta. The researchers note the differences in effectiveness between the vaccines are considered modest and support public health efforts to maximize uptake of the full 2-dose regimen to protect against VOCs.
REAL-WORLD VACCINE EFFECTIVENESS A study published July 20 in the Annals of Internal Medicine details a test-negative case-control study examining the short-term effectiveness of authorized SARS-CoV-2 mRNA vaccines in preventing infections. The research team used data collected through the US Department of Veteran Affairs’ (VA) COVID-19 Shared Data Resource, a national database containing extensive demographic, clinical, pharmacologic, laboratory, vital sign, and clinical outcome information derived from multiple validated sources. The researchers identified all individuals who tested positive for SARS-CoV-2 infection between December 15, 2020 and March 4, 2021, and matched them with control participants who had similar factors such as sex, age, race, BMI, and geographic location, but who had tested negative for SARS-CoV-2. The main measure of interest was vaccine effectiveness 7+ days after the second vaccine dose, but the researchers also examined vaccine effectiveness among those who received only 1 dose of either the Pfizer-BioNTech or Moderna vaccines.
The team identified 54,360 matched pairs of veterans. Among those who tested positive, 18% had been vaccinated, compared with 32.8% of those who tested negative. Overall, the vaccines showed 97.1% effectiveness among those who received the second dose at least 7 days prior. Among those who received only 1 dose, effectiveness was 85% overall. The research team concluded the SARS-CoV-2 vaccines being employed by the VA provided a high level of protection against infection. However, they noted several limitations of the study, including a predominantly male study population, a lack of data for currently circulating SARS-CoV-2 variants of concern, and a short follow-up period.
HEALTH EFFECTS OF LOCKDOWNS Researchers continue to explore the potential unintentional health impacts of COVID-19-related lockdowns. A commentary published in BMJ Global Health explores this question, comparing the costs of such lockdowns to their effectiveness in preventing COVID-19. The research team examined the issue through 4 main lenses: short-term mortality, disruption of health services, impacts on mental health, and the effect that lockdowns had on global health programs.
When examining a global dataset containing information on short-term mortality, the research team suggested that lockdowns were not associated with an increase in short-term mortality. The team specifically used Australia and New Zealand as examples, as both countries imposed strict COVID-19 lockdowns, maintained low numbers of COVID-19 cases, and had no excess mortality in 2020. When looking at disruption of health services, a topic that has garnered much attention throughout the pandemic, the authors noted that while there were notable disruptions, it was difficult to disentangle whether the lockdowns or the COVID-19 pandemic itself was the driving factor. The research team posited similar points around mental health, including suicide, stating that it was difficult to disentangle the mental health impacts of dealing with the COVID-19 pandemic with the mental health impacts of lockdowns, both of which increased increased isolation, anxiety, and stress. Lastly, the research team acknowledged that lockdowns did disrupt ongoing global health programs but, again, it was difficult to ascertain if the damage done by these disruptions outweighed the benefits associated with the COVID-19 lockdown interventions. Overall, the authors acknowledged that public health lockdowns have a real cost, but suggested they do not impart excess harm to populations facing a public health threat like COVID-19.
INDIA MORTALITY Researchers at the Center for Global Development published findings from an analysis that aimed to estimate the true COVID-19 mortality in India. India surpassed 400,000 cumulative reported deaths on July 1, but some experts are concerned that this total may be a substantial underestimate of the true COVID-19 burden, due to deficiencies in how the Indian government records mortality data—for COVID-19 and otherwise. The researchers took several approaches to estimating India’s COVID-19 mortality, including estimating excess mortality based on official death data, utilizing age-adjusted case fatality ratios and seroprevalence data, and a household-level longitudinal survey.
The mortality estimates they obtained based on these 3 methodologies ranged from 3.4 million to 4.9 million deaths, and while there are major differences between each estimate, all 3 are at least 8.5 times higher than the official data. Notably, the 3 methodologies yielded much different results for the first and second waves in India. While the second wave is generally believed to be more severe, 2 of the 3 methodologies estimate more deaths for the first wave than the second, perhaps a function of its longer duration. While these findings do not provide a definitive estimate of India’s COVID-19 mortality, this study and similar efforts continue to highlight the undercounting of COVID-19 deaths in countries around the world, and it could be years after the pandemic ends before we have a clear understanding of the global burden.
AFRICA The pace of new COVID-19 cases in Africa has slowed following an 8-week surge driven by the Delta variant, but the reprieve could be short-lived, according to the WHO Regional Office for Africa. The continent-wide decline of 1.7% this week was driven by a steep drop in the number of new cases reported in South Africa, where nationwide violence interrupted testing and, likely, reporting. The WHO warned that removing the country’s data would show an overall 18% increase in cases on the continent, creating an unbroken 9-week wave. Hospitals are overwhelmed, with few if any available intensive care unit beds, oxygen supplies are rapidly dwindling, and healthcare workers are stretched thin. South Africa stands as an example of how the long-term impacts of pandemic lockdowns on personal income, food security, and supply chains can exacerbate political instability, with the eruption of violent riots and looting in the wake of former President Jacob Zuma’s arrest earlier this month. The violence taxed an already overburdened healthcare system and disrupted COVID-19 testing and vaccination sites that were finally gaining momentum. Government officials and scientists warn the mass protests and disruptions to healthcare access could lead to another rise in COVID-19 cases, hospitalizations, and deaths.
Only about 1.5% of Africa’s population is fully vaccinated, and the continent has received less than 2% of the world’s SARS-CoV-2 vaccine doses. Data from the new Global Dashboard for Vaccine Equity estimate that African nations could add $38 billion to their gross domestic product (GDP) forecast for 2021 if they had vaccination rates similar to those in high-income countries. The inequity is creating a “two-track” pandemic and recovery, as high-income nations with higher vaccination rates are projected to recover more quickly while low- and middle-income countries (LMICs) that have not been able to access vaccines might not witness pre-pandemic growth levels until 2024, according to the UN Development Programme (UNDP), one of the dashboard’s sponsors, along with WHO and the University of Oxford. Global vaccine inequity will continue to grow under the status quo, a new analysis from the Kaiser Family Foundation shows. According to the analysis, low-income countries would need to increase their daily vaccination rate by nearly 19 times to reach 40% coverage with at least one dose by the end of the year. Ultimately, ensuring widespread vaccination will improve immunity among the global population and help bring the pandemic under control, but exactly how higher-income nations plan to increase vaccine supplies to LMICs remains an unresolved question.
VACCINE MANUFACTURING IN AFRICA Pharmaceutical company partners Pfizer and BioNTech on July 21 announced they signed a letter of intent with the Biovac Institute (Biovac)—a Cape Town, South Africa-based biopharmaceutical company—to help manufacture the Pfizer-BioNTech SARS-CoV-2 vaccine exclusively for the 55 nations of the African Union (AU). Under the plan, Biovac will “finish and fill” vaccine doses, obtaining large batch ingredients from Europe, blending the product, and filling and packaging vials for distribution, with the goal of producing more than 100 million doses annually. Pfizer-BioNTech will immediately begin to provide technology transfers, including on-site development and equipment installation, with the expectation that Biovac will be incorporated into the supply chain by the end of 2021 and begin producing finished doses in 2022. The agreement represents the first time an mRNA vaccine will be produced in Africa. Another South African firm, Aspen Pharmacare, already is producing the J&J-Janssen viral vector SARS-CoV-2 vaccine in the country, providing the same “fill and finish” services with the capacity to make more than 200 million doses each year.
The announcement received positive responses from some experts, while others called for more to be done to kickstart vaccine manufacturing in Africa. Africa CDC Director John Nkengasong said the move should be celebrated as another step in “the collective action to address technology transfer and intellectual property.” But Strive Masiyiwa, AU Special Envoy and Coordinator of the Africa Vaccine Acquisition Task Team (AVATT) initiative, called on large pharmaceutical firms to license production of SARS-CoV-2 vaccines on the continent rather than create piecemeal deals. WHO Regional Director for Africa Dr. Matshidiso Moeti also called for more local production of vaccines in Africa in order to prepare for future disease outbreaks.
Late last month, the WHO, along with Biovac, Afrigen Biologics and Vaccines, a network of universities, and the Africa CDC, established an mRNA vaccine technology transfer hub in South Africa to act as a training facility for the production of mRNA vaccine raw materials in Africa. However, neither Pfizer, BioNTech, nor Moderna, which makes another mRNA SARS-CoV-2 vaccine, has voiced support for the hub. Additionally, Pfizer reiterated the current deal with Biovac is only among the 3 companies and does not represent a government-supported technology transfer or compulsory licensing agreement. Pfizer CEO Albert Bourla on July 21 again stated the company’s opposition to a proposal at the World Trade Organization that would allow for patent waivers on SARS-CoV-2 vaccines, saying it would discourage innovation and collaboration. But BioNTech CEO Uğur Şahin indicated his company continues to evaluate sustainable approaches to supporting the African development and production of mRNA vaccines, which could be used to develop vaccines for other diseases in the future.
SARS-COV-2 ORIGINS Earlier this month, the WHO outlined a proposal for a follow-up investigation in China to identify the origins of the SARS-CoV-2 virus. On July 22, Chinese officials rejected the proposal. The WHO plan would have included additional investigations of laboratory facilities and markets in Wuhan, among other activities. Numerous governments—including the US—and experts have called for additional investigations into the origin of the pandemic, including access to additional data and specimens, arguing that limited access to the necessary data hindered the initial investigation. Following China’s rejection of the WHO proposal, the WHO called for international cooperation regarding investigations into the virus’s origins and emphasized that associated investigations are not intended to assign blame but rather to provide further understanding of how the virus emerged. As we covered previously, the WHO does not have the authority to initiate such an investigation without support from the host country.
OLYMPICS Tokyo reported its highest daily incidence since January, just as the 2020 Summer Olympics Games commence. The Tokyo Metropolitan Government reported 1,832 cases on July 21, only two days before the Olympics opening ceremony. The spike represents over 600 more cases than last Wednesday’s count. Several athletes already have tested positive for SARS-CoV-2 and will miss the Games, including a US beach volleyball player, an alternate for the US gymnastics team, and a Czech beach volleyball player. Vaccination is not required for Olympic athletes, but the Olympic playbook requires anyone going to the Games to submit two negative tests taken on separate days within 96 hours of leaving for Japan regardless of vaccination status. They are tested again upon arrival. Athletes, coaches, and officials are required to take daily antigen tests, followed by a PCR test if the antigen test returns a positive result. The Tokyo public database reports 79 people with Olympic credentials have tested positive. Close contacts of those who test positive will be allowed to train and compete as long as they receive two negative tests within 6 hours of competition.
by ponchi101 The GOV't in Argentina is facing fires all around them. The pandemic, spiraling inflation, unemployment, it is true madness. The small company that I was supervising in 2019 has fired ALL its personnel. They will be filing bankruptcy soon.
So, them reporting about the pandemic is not going to happen any time soon.
by JazzNU
dryrunguy wrote: ↑Fri Jul 23, 2021 8:15 pm
Wait. Where are these data indicating that white people in these red states (the Republican base) are dying at higher rates NOW than they were a year ago compared to racial and ethnic minorities? I am not aware of any data indicating anything has changed in terms of the ethnic composition of current COVID-related morbidity and mortality. All along, COVID-related morbidity and mortality has disproportionately affected people of color, particularly Blacks, Hispanics, and Tribes.
That is literally the ONLY kind of data that would cause Republicans to suddenly start giving a rat's ass. Which then begs the question: Since when do Republicans actually care about legitimate data?
Don't know if there is data, but there is anecdotal evidence that is starting to scare them more. That's part of why there are some more vaccinations in the places with high case counts and increased deaths, they know someone personally who is sick or has died now. Many of the stories on the news right now are that of white people, not minorities being sickened in the hospital. The ones getting their kids sick and crying they didn't know, these kids falling ill after the outbreak at their camp, the "my nanny lied to me" the "wow, this is no joke" I should've taken it seriously people, just about every story I've seen on the national news in the last two weeks has featured white people.
And if you read that entire original post by the Alabama doc that went viral, she said some of what she's told by the grieving family members is that they thought because they had a certain blood type or skin color, they wouldn't get as sick.
Personally, I think the kids getting sick is the motivating factor for many of the stragglers that are finally getting vaccinated. Opening overnight camps at or near full capacity, for instance, and not requiring all staff and eligible campers to be vaccinated? That's a dangerous game they're playing.
by Suliso NYT article about one of the mighty 12
The Most Influential Spreader of Coronavirus Misinformation Online
Researchers and regulators say Joseph Mercola, an osteopathic physician, creates and profits from misleading claims about Covid-19 vaccines.
SAN FRANCISCO — The article that appeared online on Feb. 9 began with a seemingly innocuous question about the legal definition of vaccines. Then over its next 3,400 words, it declared coronavirus vaccines were “a medical fraud” and said the injections did not prevent infections, provide immunity or stop transmission of the disease.
Instead, the article claimed, the shots “alter your genetic coding, turning you into a viral protein factory that has no off-switch.”
Its assertions were easily disprovable. No matter. Over the next few hours, the article was translated from English into Spanish and Polish. It appeared on dozens of blogs and was picked up by anti-vaccination activists, who repeated the false claims online. The article also made its way to Facebook, where it reached 400,000 people, according to data from CrowdTangle, a Facebook-owned tool.
The entire effort traced back to one person: Joseph Mercola.
Dr. Mercola, 67, an osteopathic physician in Cape Coral, Fla., has long been a subject of criticism and government regulatory actions for his promotion of unproven or unapproved treatments. But most recently, he has become the chief spreader of coronavirus misinformation online, according to researchers.
An internet-savvy entrepreneur who employs dozens, Dr. Mercola has published over 600 articles on Facebook that cast doubt on Covid-19 vaccines since the pandemic began, reaching a far larger audience than other vaccine skeptics, an analysis by The New York Times found. His claims have been widely echoed on Twitter, Instagram and YouTube.
The activity has earned Dr. Mercola, a natural health proponent with an Everyman demeanor, the dubious distinction of the top spot in the “Disinformation Dozen,” a list of 12 people responsible for sharing 65 percent of all anti-vaccine messaging on social media, said the nonprofit Center for Countering Digital Hate. Others on the list include Robert F. Kennedy Jr., a longtime anti-vaccine activist, and Erin Elizabeth, the founder of the website Health Nut News, who is also Dr. Mercola’s girlfriend.
“Mercola is the pioneer of the anti-vaccine movement,” said Kolina Koltai, a researcher at the University of Washington who studies online conspiracy theories. “He’s a master of capitalizing on periods of uncertainty, like the pandemic, to grow his movement.”
Some high-profile media figures have promoted skepticism of the vaccines, notably Tucker Carlson and Laura Ingraham of Fox News, though other Fox personalities have urged viewers to get the shots. Now, Dr. Mercola and others in the “Disinformation Dozen” are in the spotlight as vaccinations in the United States slow, just as the highly infectious Delta variant has fueled a resurgence in coronavirus cases. More than 97 percent of people hospitalized for Covid-19 are unvaccinated, according to the Centers for Disease Control and Prevention.
President Biden has blamed online falsehoods for causing people to refrain from getting the injections. But even as Mr. Biden has urged social media companies to “do something about the misinformation,” Dr. Mercola shows the difficulty of that task.
Over the last decade, Dr. Mercola has built a vast operation to push natural health cures, disseminate anti-vaccination content and profit from all of it, said researchers who have studied his network. In 2017, he filed an affidavit claiming his net worth was “in excess of $100 million.”
And rather than directly stating online that vaccines don’t work, Dr. Mercola’s posts often ask pointed questions about their safety and discuss studies that other doctors have refuted. Facebook and Twitter have allowed some of his posts to remain up with caution labels, and the companies have struggled to create rules to pull down posts that have nuance.
“He has been given new life by social media, which he exploits skillfully and ruthlessly to bring people into his thrall,” said Imran Ahmed, director of the Center for Countering Digital Hate, which studies misinformation and hate speech. Its “Disinformation Dozen” report has been cited in congressional hearings and by the White House.
In an email, Dr. Mercola said it was “quite peculiar to me that I am named as the #1 superspreader of misinformation.” Some of his Facebook posts were only liked by hundreds of people, he said, so he didn’t understand “how the relatively small number of shares could possibly cause such calamity to Biden’s multibillion dollar vaccination campaign.”
The efforts against him are political, Dr. Mercola added, and he accused the White House of “illegal censorship by colluding with social media companies.”
He did not address whether his coronavirus claims were factual. “I am the lead author of a peer reviewed publication regarding vitamin D and the risk of Covid-19 and I have every right to inform the public by sharing my medical research,” he said. He did not identify the publication, and The Times was unable to verify his claim.
by MJ2004 I’d already heard of Dr. Mercola before this. He’s an all-purpose crackpot of the highest order.
by ti-amie
by Suliso No comment
by ponchi101
by ti-amie
by ti-amie
by dryrunguy Serious question... Has anyone seen chatter in far right wing circles about about "vaccine passes" being the Mark of the Beast? If it hasn't surfaced yet, it will soon.
by JazzNU For New York City. Vaccinate or weekly tests.
by Suliso
dryrunguy wrote: ↑Mon Jul 26, 2021 9:43 pm
Serious question... Has anyone seen chatter in far right wing circles about about "vaccine passes" being the Mark of the Beast? If it hasn't surfaced yet, it will soon.
Courtesy of your favorite Republican representative
by ponchi101 Dry's question's time stamp: 4:43
Suliso's answer time stamp: 5:11.
Google can KMA.
by ti-amie Posted without comment. And I'm sorry for the Newsmax clip sullying the site.
by dryrunguy I have to stop asking questions. And I don't DARE click on the Newsmax link. It would adulterate my Twitter and YouTube feeds.
by ti-amie
by ti-amie I'm beginning to think that the current head of the CDC needs to be relieved of her post.
by JazzNU I don't think so at all. I don't see what that would solve.
by JazzNU
by dryrunguy Here's the latest Situation Report. Lots to unpack here, including a variety of vaccination mandates for state employees or employees of certain federal agencies, Vietnam's lockdown, the French vaccination pass, etc. Oh, and the NFL ain't playin' around. Though this was probably already covered in the NFL thread.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 194.1 million cumulative cases and 4.16 million deaths worldwide as of 12:28 EDT on July 26. Global weekly incidence increased for the fifth consecutive week, a 7.89% increase over the previous week. Global weekly mortality increased for the third consecutive week, a 20.77% increase compared to the previous week.
Global Vaccination
The WHO reported 3.7 billion doses of SARS-CoV-2 vaccines administered globally as of July 26. The WHO reports a total of 1.44 billion individuals have received at least 1 dose, and 672 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered is up, now at 33 million doses per day, driven by increases in Asia. Our World in Data estimates that there are 2.14 billion vaccinated individuals worldwide (1+ dose; 27.5% of the global population) and 1.08 billion who are fully vaccinated (13.9% of the global population).
UNITED STATES
The US CDC reported 34.4 million cumulative COVID-19 cases and 608,528 deaths. Daily incidence continues to increase, now up to 42,226 new cases per day, which is nearly 3.7 times the most recent low on June 19 (11,467) and is still increasing steadily. Daily mortality also continues to increase, up to 239 deaths per day, which is more than 45% higher than the most recent low on July 10 (164).
US Vaccination
The US has administered 342.2 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations are increasing slowly, now up to 471,948 doses per day*. A total of 188.7 million individuals in the US have received at least 1 dose, equivalent to 56.8% of the entire US population. Among adults, 69% have received at least 1 dose, as well as 10.5 million adolescents aged 12-17 years. A total of 163.2 million individuals are fully vaccinated, which corresponds to 49.1% of the total population. Approximately 60% of adults are fully vaccinated, as well as 8.1 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current value provided here corresponds to 5 days ago.
US HOSPITALIZATIONS The number of COVID-19-related hospitalizations is beginning to rise in most US states, following increasing numbers of COVID-19 cases driven by the spread of the more transmissible Delta variant. Nationally, hospitalization rates remain low overall, nowhere near the previous pandemic peaks. But the increases in hospitalizations are high and rising in parts of the country that have low vaccination rates, including Florida, Nevada, Arkansas, and Missouri. Some Florida hospitals are seeing the highest number of COVID-19 patients since the beginning of the pandemic, and the pace of this surge is accelerating rapidly. One hospital in Missouri said its increase in patients occurred nearly 5 times as fast as last fall’s surge. An estimated 97% of hospitalized patients are unvaccinated. Patients also are skewing younger, with 69% under the age of 65, according to CDC data as of July 17. Some hospitals are scrambling to find space for intensive care patients, trying to address personnel shortages, and attempting to maintain adequate supplies of medical equipment such as ventilators.
According to new projections released last week by the COVID-19 Scenario Modeling Hub—a consortium of researchers working with the US CDC to track the pandemic—the current US surge will continue throughout the summer and into the fall. In the most likely of 4 scenarios, there would be around 60,000 new cases and about 850 deaths per day, with 70% of eligible Americans vaccinated. Currently, the US is averaging around 42,000 new cases per day and about 250 deaths per day. Nationwide, 57.5% of eligible people are fully vaccinated. The researchers encouraged state and local leaders to take note of the projections, urging them to reimplement mask mandates and physical distancing requirements that could help lessen the surge’s impact.
US GOVERNMENT RESPONSE As the number of new COVID-19 cases continues to rise in the US, the US government is examining further tactics to contain the pandemic. Last week, the White House purchased an additional 200 million doses of the Pfizer-BioNTech vaccine. The purchase is in anticipation that additional doses will be recommended for certain populations and that the vaccine could “soon” be authorized for use in children ages 5-11. The US government also hinted at reinstated mask recommendations.
Overall, the US government is focused on improving national vaccination rates, particularly in communities with low coverage where most new COVID-19 cases are in unvaccinated individuals. On July 22, the government announced US$100 million for rural health clinics to develop vaccine confidence and outreach efforts. Additionally, the US Department of Health and Human Services will invest US$1.6 billion from the American Rescue Plan to support COVID-19 testing and mitigation activities in vulnerable communities. These funds will address the rise in cases among unvaccinated people by detecting, diagnosing, tracing, and mitigating the spread of SARS-CoV-2 in homeless shelters, correctional facilities, and other hard-hit and high-risk areas. In recognizing the 31st anniversary of the Americans with Disabilities Act, the government announced a package of guidance and resources to support individuals experiencing “long COVID,” also known as post-acute sequelae of COVID-19. According to the guidance, long COVID can be considered a disability under certain federal civil rights laws, thereby allowing federal protections and resources for adults and children impacted by long-lasting symptoms of COVID-19.
As the US government focuses on challenges to the nation’s domestic recovery from the pandemic, including rising consumer prices and turbulent financial markets, officials from the US Agency for International Development who are responsible for making the US an “arsenal of vaccines” are struggling to help other countries acquire resources and distribute SARS-CoV-2 vaccines, COVID-19 therapeutics, and personal protective equipment. At issue is more than US$1 billion the White House diverted from the agency in June to pay for the purchase of 500 million additional doses of the Pfizer-BioNTech vaccine, meant to supplement the 80 million vaccine doses the government has already allocated for donations abroad, according to unnamed officials. But the unexpected shift in funding, and the wait time for those doses to be delivered, has put pressure on the US government to maintain its status as a leading donor of COVID-19 assistance. USAID officials tasked with vaccine distribution abroad continue to advocate for increased resources from the White House and US Congress in order to assist countries in need.
VACCINATION MANDATES As the Delta SARS-CoV-2 variant sweeps across the US, more jurisdictions and companies are considering strengthening public health measures to mitigate the virus’s impact. This includes vaccination mandates for employees. On July 26, California, the country’s most populous state, became the first in the nation to announce that all state employees and on-site public and private workers in health care and high-risk congregate settings will be required to show proof of vaccination or submit to mandatory once-or-twice weekly testing. State employees are required to submit vaccination documentation by August 2, and health care and congregate-setting facilities must be in full compliance by August 23. Unvaccinated workers also will be required to wear appropriate PPE. A few hours earlier, New York City, the nation’s largest city, announced that all 340,000 municipal employees of the city, including police officers and teachers, will be required to be vaccinated or start weekly testing by September 13. As of August 2, any employee who is unvaccinated must wear a mask indoors at all times or risk termination. In their announcements, both California Governor Gavin Newsom and New York City Mayor Bill De Blasio encouraged other local governments and private sector employers to implement vaccination mandates.
The Department of Veterans Affairs on July 26 became the first federal agency to implement a vaccination mandate, requiring 115,000 of its frontline healthcare workers to show proof of full vaccination within the next 8 weeks. In its announcement, the VA referenced several organizations that support vaccine mandates. Many of those groups—including the American Medical Association, the American Nurses Association and 55 other groups representing millions of doctors, nurses, pharmacists, and other healthcare workers—issued a joint statement early on July 26 calling for all healthcare and long-term care employers to require their employees to be vaccinated for SARS-CoV-2. The statement cites highly contagious variants, including the Delta variant, and “significant numbers” of unvaccinated people as drivers for rising numbers of COVID-19 cases, hospitalizations, and deaths in the US. The groups also called on other employers across the country to implement policies to encourage vaccination. As we have previously reported, vaccination mandates for employees of a hospital system (Bridges et al v. Houston Methodist Hospital et al) and students of a university (Ryan Klaasen et al v. The Trustees of Indiana University) so far have been upheld in US federal district courts. An appeal from one of those cases is expected, and additional legal challenges likely will result from these, and future, vaccination mandates.
MODERNA VACCINE FOR ADOLESCENTS The European Medicines Agency’s Committee for Medicinal Products for Human Use on July 23 approved the Moderna SARS-CoV-2 vaccine (known as Spikevax in Europe) for use in children aged 12 to 17 years. The vaccine already is authorized for adults aged 18 and older, but it is the first time this vaccine has been authorized for people under age 18. According to the EMA, data from more than 3,700 children ages 12 to 17 showed the vaccine produced an antibody response comparable to the one seen in young adults aged 18 to 25 years. The younger group also experienced similar mild-to-moderate side effects. The agency noted that the trial was unable to detect new, uncommon side effects or evaluate the risk of known ones, including the inflammation of heart muscle and tissue, because of the relatively small number of study participants, but added that the “benefits of Spikevax in children aged 12 to 17 outweigh the risks.” Until now, the Pfizer-BioNTech was the only option for children aged 12 and older in Europe. The US FDA currently is considering whether to authorize the Moderna vaccine for the same age group.
VACCINE TRIALS FOR CHILDREN The US FDA reportedly has urged 2 SARS-CoV-2 vaccine makers, Pfizer-BioNTech and Moderna, to expand the size of their clinical trials among children aged 5 to 11 years in order to assess whether the rare side effects of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the lining around the heart) that have been seen in young adults shortly following vaccination also appear in this younger age group. Federal regulators requested the companies include at least 3,000 children in their studies, reportedly about double the original number of participants. Moderna confirmed its plans to expand the size of its pediatric clinical trial and expects to have data on its vaccine’s use among children ready to submit to the FDA in winter 2021 or early 2022. Pfizer-BioNTech indicated it does not plan to alter its original timeline of submitting a request for the FDA to expand authorization to 5-to-11-year-old children by the end of September, and presenting data for younger children, aged 6 months to 2 years, in October or November. The FDA last month added warnings about the potential for myocarditis and pericarditis to patient and provider fact sheets for both the Moderna and Pfizer-BioNTech vaccines.
LONG COVID/PASC IN CHILDREN Children’s National Hospital (US), in collaboration with the US NIH’s National Institute of Allergy and Infectious Diseases, announced on July 25 they are launching a large, multi-year study to examine the long-term effects of COVID-19 and multisystem inflammatory syndrome in children (MIS-C) following recovery from acute SARS-CoV-2 infection. The study will enroll up to 1,000 children and young adults under age 21 who have recovered from confirmed infection with SARS-CoV-2, with or without symptoms, or MIS-C, as well as up to 1,000 household contacts who will serve as a control group, and 1 parent or guardian per participant to complete questionnaires. Surveys will gather information about quality of life, social impact, and any long-term physical impacts of the virus, and researchers also plan to detail the role of genetics; duration and quality of immune responses following infection; so-called “long COVID,” also called post-acute sequelae of COVID-19 (PASC); and MIS-C.
In the US, more than 4.1 million children have tested positive for SARS-CoV-2, and nearly 500 have died. In the week ending July 22, children accounted for 16.8% of reported weekly COVID-19 cases nationwide. Black, Hispanic/Latino, and Native American children have been hardest hit, accounting for 3 out of 4 deaths among patients under age 21. According to researchers, between 2% and 10% of recovered children have long-term symptoms, and about 2 out of 3 children who develop MIS-C are Black or Hispanic/Latino. The US$40 million study is one of many NIH is supporting to understand the range of SARS-CoV-2 effects on children. Little is known about why some children experience long-term symptoms following COVID-19 recovery, just as long COVID-19 is not well understood in adults. It is hoped that these controlled clinical trials will provide more answers about how these conditions can be more effectively treated and, possibly, prevented.
GLOBAL VACCINE ACCESS The World Bank and the COVAX facility on July 26 announced a new financing mechanism to help improve access to SARS-CoV-2 vaccines for low- and middle-income countries (LMICs), where vaccination rates are lagging. Countries that are seeking to purchase vaccines through the COVAX advance market commitment cost-sharing system via Gavi, the Vaccine Alliance, are facing hurdles in guaranteeing their own payments. Now, COVAX will be able to negotiate advance purchase agreements with vaccine makers based on aggregated demand across several of the 92 LMICs that participate in the advance market commitment, using financial backing from the World Bank and other multilateral development banks. The mechanism should enable more countries to receive bulk vaccine purchases at a lower cost, instead of relying solely on donations through COVAX, and countries would be able to select specific vaccines that align with their preferences. Additionally, it will allow for more transparency regarding vaccine availability, pricing, and delivery schedules, World Bank President David Malpass noted in a statement. Under the AMC cost-sharing arrangement, COVAX plans to provide up to 430 million additional vaccine doses for delivery between late 2021 and mid-2022. COVAX has already delivered nearly 153 million doses to 137 countries, but that number is far below its 2021 goal of 2 billion doses. The new financing mechanism comes amid growing concern over the widening gap in global vaccine access, with experts hoping the arrangement will facilitate vaccine deliveries to countries in need.
VIETNAM LOCKDOWN On July 23, Vietnam’s capital city of Hanoi began a 15-day lockdown amid a spike in new COVID-19 cases. The country’s health ministry reported 7,968 new cases on July 24, a record daily increase and up from the previous day’s count of 7,307. With the addition of Hanoi’s 8 million people, about one-third of Vietnam’s 100 million people are now on lockdown. Residents in larger cities, like Ho Chi Minh City and Hanoi, are no longer allowed to congregate in groups of more than 2 people and are only allowed to leave their homes for food, medication, or in the case of an emergency. According to Our World in Data, Vietnam has fully vaccinated only 0.4% of its population and is taking steps to procure more vaccine doses. On July 25, the country announced it received 3 million doses of the Moderna vaccine from the US through COVAX. Vietnamese officials are in talks with US officials about the domestic production of mRNA vaccines, which could begin late this year or in early 2022, with the goal of producing 100 to 200 million doses a year. The government also indicated it is considering authorizing the domestically produced Nanocovax vaccine. A phase 3 clinical trial testing the vaccine is ongoing, but results are not yet available.
FRANCE HEALTH PASS The French Parliament on July 26 approved a law mandating special health passes for entry to all restaurants, trains, planes, and some other public venues and requiring vaccinations for all healthcare workers and other essential workers such as firefighters beginning September 15. In order to obtain a health pass, people must show digital or paper proof of full vaccination, results of a recent negative SARS-CoV-2 test, or documentation of recent recovery from acute COVID-19. More than 160,000 people demonstrated around France over the weekend to protest the legislation requiring health passes. France President Emmanuel Macron welcomed peaceful demonstrations but added they will not make the pandemic disappear. “My message is simple: to get vaccinated,” he said. Nearly 60% of the French population has received at least 1 dose of vaccine, but the number of new daily COVID-19 cases has risen sharply since the beginning of the month. The Constitutional Council is expected to review the law next week to determine whether it complies with the country’s Constitution.
NFL COVID-19 RULES The US National Football League (NFL) sent a strong message to its 32 teams last week, encouraging clubs to convince players to get vaccinated for SARS-CoV-2 and alerting them that games having to be cancelled due to a COVID-19 outbreak among unvaccinated players would be forfeited and counted as a loss. According to a memo, the league intends to play its entire 272-game schedule over 18 weeks and would not add a “19th week” to accommodate games that cannot be rescheduled during the 18-week regular season. If a game is cancelled due to an outbreak and cannot be rescheduled, neither team’s players would receive their weekly salary and the responsible team would cover all financial losses. Additionally, vaccinated players or staff who test positive but are asymptomatic can return to the field after 2 negative tests 24 hours apart; however, unvaccinated individuals who test positive would be required to complete a 10-day isolation period. Unvaccinated players are required to undergo daily testing, physically distance, wear a mask indoors, and be prohibited from gathering with the team for media events or outside of official team activities, such as at nightclubs, bars, or house parties. If unvaccinated players violate the gathering rules, the NFL and clubs are permitted to issue fines of up to US$50,000 for a first offense, and more for further violations. For violating other COVID-19 protocols, such as not wearing a mask when required, players could be fined US$14,650 every time a transgression occurs. According to the memo, more than 75% of players are in the process of being vaccinated and more than half of the teams have vaccination rates of more than 80% of players. With the NFL placing the burden on teams and players to get vaccinated or else face significant economic consequences, it will be interesting to see if teams can reach near-100% vaccination rates.
by JazzNU And another good thread with information about the new guidance from a familiar name:
by JazzNU ^^ Continued
by ti-amie
by ti-amie My problem with the current CDC head revolves around the, in my totally non medical opinion, idiotic relaxing of mask wearing regulations. It allowed for all of the antivax idiots to wander around with no threat of repercussions with those who have done the right thing and been vaxxed and continued to wear masks. I've never seen the CDC issue a protocol and then have to reverse it less than three months later. The fact that she's Rod Rosenstein's sister also counts against her.
Also, Cuomo, who some of us who live in NYS have always said is a piece of work is now trying to tell people that they have to be back in their offices by Labor Day, something the real estate industry needs to happen.
It's beginning to look as if "they" wanted to get the summer in so money could be made. The fact that Vegas and its environs has reinstated a mask mandate tells you everything you need to know.
by skatingfan The antivax crowd haven't been wearing masks this whole time, so the change in the CDC guidance didn't change or impact their behaviour.
by Suliso What I don't like is that they're asking a lot from people who have already done a lot (getting vaccinated) and nothing at all from those who refuse to get vaccinated. I think without mandates US has reached peak vaccination rate already.
by JazzNU
Suliso wrote: ↑Wed Jul 28, 2021 8:41 pm
What I don't like is that they're asking a lot from people who have already done a lot (getting vaccinated) and nothing at all from those who refuse to get vaccinated. I think without mandates US has reached peak vaccination rate already.
And you'd like to ask what of them that isn't already being asked? Serious question.
Suliso wrote: ↑Wed Jul 28, 2021 8:41 pm
What I don't like is that they're asking a lot from people who have already done a lot (getting vaccinated) and nothing at all from those who refuse to get vaccinated. I think without mandates US has reached peak vaccination rate already.
And you'd like to ask what of them that isn't already being asked? Serious question.
I wish I knew what exactly to do, but how can you suppress the virus efficiently with such large numbers not vaccinated? 70% adults might even suffice, but it's not even that given large regional differences...
As for just asking you can ask whatever and they won't do.
by ponchi101 Live in a split society? Just trying to come up with something here:
1. Public places, such as restaurants, bars, theaters, etc, must clearly state a type of servicing: masked & vaccinated, or not. If you don't want to wear a mask and get vaccinated, then you know which are "your" places.
2. Again, insurance companies are not mandated to cover C19 IF you are not vaccinated. There is no reason why the vaccinated should cover for those that reject the science.
Other than those two ideas, JazzNu's questions is indeed serious. The USA is reaching a break point.
Off Topic
Amazing how all these sprung from the election of one dumb man. Talk about butterfly effects.
by Suliso I'm afraid you're not giving a practical advice ponchi...
by ponchi101 I know. I am trying to think about what can be done IF a large portion of any population refuses to get vaccinated. Because those of us that already went that way and will continue to wear masks really can't do much more.
But I would like to see places posting a clear policy. THIS ESTABLISHMENT DOES NOT REQUIRE MASKS OR VACCINATION. That would let you know whether to patronize it or not.
Amazing how all these sprung from the election of one dumb man. Talk about butterfly effects.
I don't know, ponchi. Perhaps you give Trump too much credit. Let me make the following argument.
I'd argue that you have to look at Trump's "base" in four groups based on the size of each group, with Group 1 being the largest and Group 4 being the smallest.
Group 1: Evangelicals and other conservatives who held their noses and voted for him for a singular reason: He wasn't Hillary Clinton or Joe Biden. My mother fits into this group.
Group 2: Rich people who either knew or believed that Trump would make them richer. Which is exactly what he did. And they laughed all the way to the bank and during tax season.
Group 3: These are the white supremacists, misogynists, and other "deplorables" who Trump lured out from under the rocks where they used to live. Previously disaffected and disjointed from the political process, Trump emboldened them to speak out, to be proud of their "deplorableness", and to advocate for their points of view, which they were not--from a sociopolitical standpoint--previously allowed to do on a widespread and visible basis. They emerged from invisibility because Trump made it okay for them to do so.
Group 4: The hard-core Trumpers who joined forces with Group 3, mostly during the past 4 years. These individuals were largely radicalized by Group 3 in a systematic and diligent manner. Group 4, along with Group 3, are the faces and voices of January 6.
::
So a significant portion, but not the largest portion, of this base was ALWAYS there. Trump gave them a voice and a space unlike any president in recent history. But Trump didn't create them. He just made them worse. That's my 2 cents.
by dryrunguy
ponchi101 wrote: ↑Thu Jul 29, 2021 2:09 am
I know. I am trying to think about what can be done IF a large portion of any population refuses to get vaccinated. Because those of us that already went that way and will continue to wear masks really can't do much more.
But I would like to see places posting a clear policy. THIS ESTABLISHMENT DOES NOT REQUIRE MASKS OR VACCINATION. That would let you know whether to patronize it or not.
Meanwhile, yesterday I drove from PA to OH for my mother's 80th birthday (tomorrow, July 29). At the local Wal-Mark, a large sign on the entrance door tells you, "If you have been vaccinated, you are not required to wear a mask." I wore my mask, and I was 1 of about 3 or 4 people in the store wearing a mask. And I will GUARANTEE you not all of these scads of unmasked people were vaccinated.
When I checked into the hotel, "Masks Required" was the sign on the door. But the young woman who checked me in was not wearing a mask. In fact, dolphins and I are the ONLY people I have seen wearing masks on this property.
So that points to two problems:
1) Establishments rely entirely on the honor system (Wal-Mart)
2) Establishment policies are not enforced (my hotel)
It is the way it is. At least in the part of OH and much of rural/suburban PA.
by Deuce Stupid people were stupid long before Donald J. Trump ran for president.
Trump simply helped to reveal some of them - but they already existed long before he entered politics.
by ponchi101 If Tiny would have come out and say "Get the vaccine, I love it!" they would be getting their fourth or fifth shot.
Remember how they were so ready to drink hydroxychloroquine with their Jack Daniels?
ponchi101 wrote: ↑Thu Jul 29, 2021 2:09 am
I know. I am trying to think about what can be done IF a large portion of any population refuses to get vaccinated. Because those of us that already went that way and will continue to wear masks really can't do much more.
But I would like to see places posting a clear policy. THIS ESTABLISHMENT DOES NOT REQUIRE MASKS OR VACCINATION. That would let you know whether to patronize it or not.
Meanwhile, yesterday I drove from PA to OH for my mother's 80th birthday (tomorrow, July 29). At the local Wal-Mark, a large sign on the entrance door tells you, "If you have been vaccinated, you are not required to wear a mask." I wore my mask, and I was 1 of about 3 or 4 people in the store wearing a mask. And I will GUARANTEE you not all of these scads of unmasked people were vaccinated.
When I checked into the hotel, "Masks Required" was the sign on the door. But the young woman who checked me in was not wearing a mask. In fact, dolphins and I are the ONLY people I have seen wearing masks on this property.
So that points to two problems:
1) Establishments rely entirely on the honor system (Wal-Mart)
2) Establishment policies are not enforced (my hotel)
It is the way it is. At least in the part of OH and much of rural/suburban PA.
The honor system for mask wearing is a joke (and has been from the start). Just as you said, those who refuse to get vaccinated didn't want to wear masks in the first place, so are not going to wear one if it's not required/policed. In any facility using the honor system, it's more likely that those wearing masks are vaccinated.
by JazzNU
dryrunguy wrote: ↑Thu Jul 29, 2021 2:34 am
So that points to two problems:
1) Establishments rely entirely on the honor system (Wal-Mart)
2) Establishment policies are not enforced (my hotel)
It is the way it is. At least in the part of OH and much of rural/suburban PA.
Please don't group suburban PA with rural. Or at least phrase it as "much of PA that isn't Philly or Pittsburgh," because masks, when asked to be worn in this area, are. And I hear it's similar from family in most of the Pittsburgh area. We're also much, much more vaccinated in these areas than rural PA.
My county is more vaccinated than Vermont. And when masks were mandatory, I never saw a single person not wearing one, it was never political around here to wear a mask, we were wearing them before it became an issue and had cases b.
As for enforcement. I have said it before and I will say it again. Asking employees to enforce mask policies is asking too much of them for their meager wages especially given the belligerence we've seen shown by non-mask wearers about wearing masks. But clubs of all kinds have take a mighty hit in the last 18 months and wouldn't it be great to give people jobs? Club bouncers are just sitting there waiting for the job of mask enforcement as far as I'm concerned, check it at the door like it's a license.
by JazzNU The US may have peaked with their vaccinations, but they have by no means stopped. There's been an uptick recently as fear of the Delta variant is growing and the various employer and institution mandates are being implemented with some new ones being announced and put into place in the last week.
We were always going to get a bump in vaccinations around this time for colleges requiring them to return to campus. But in addition to NYC, California, and the VA announcing new mandates, many hospitals are starting to make announcements, and just yesterday Google and Facebook said they will require it of their employees returning to the office as well, along with Netflix requiring cast and crew of US productions to get vaccinated. We might get an announcement today about federal employees as well.
And if you look at the numbers, we're about to hit 70% first dosage for adults and it's ticking up quicker to that mark than it was just two weeks ago. So progress. Slower than we want and more browbeating than should be necessary, but I'm sure most of us don't care about the how at this point.
There are so many outbreaks from summer camps. It's especially perplexing how this is happening when seemingly almost no camps required staff and campers 12 and over to be vaccinated before camp started...
by ti-amie
by ti-amie
by ti-amie
by ti-amie
by JazzNU
by Suliso I don't understand people who are vaccinated and not immuno compromised who're super scared of this virus and test all the time. Sure there is some small chance of catching it in a bad way anyway, but so what? There is also a chance of dying in a car crash or getting a cancer. Both happen - in my 12 years in a large company one co-worker has died in a car crash and two from cancer. None of them were 40 yet. Don't do crazy stuff, but enjoy your life while you can. Who knows how much time fate has reserved for you...
by Suliso Australian government saying that they'll keep locking down till 80% population vaccinated. Whenever that is... I think it's maddness. I've lost a lot of respect for Australia seeing how they abused their own citizens, particularly those living abroad.
by ponchi101 With a population of about 30 Million, they should be able to vaccinate everybody in one month, IF THEY HAVE THE VACCINES. But, as you say, this continuous lockdown has gone too long. I have a friend in Australia that tells me that the number of suicides has skyrocketed. I believe that is an exaggeration, but that such a long lockdown must be affecting people tremendously can't be denied.
Here vaccination continues, but the population simply will no longer accept lockdowns. The result is that unemployment has dropped, by a lot. It now stands at 14.4%, which sounds lousy but it is an improvement over the 19% of a couple of months ago. So people just have decided to go out, get vaccinated ASAP, and wear our masks. The sole thing that can be done.
by mmmm8
Suliso wrote: ↑Fri Jul 30, 2021 3:11 pm
I don't understand people who are vaccinated and not immuno compromised who're super scared of this virus and test all the time. Sure there is some small chance of catching it in a bad way anyway, but so what? There is also a chance of dying in a car crash or getting a cancer. Both happen - in my 12 years in a large company one co-worker has died in a car crash and two from cancer. None of them were 40 yet. Don't do crazy stuff, but enjoy your life while you can. Who knows how much time fate has reserved for you...
I don't do it (testing frequesntly), but I understand it. Testing to find out if you have COVID allows you to catch it early in the odd chance it becomes more serious and ensure you don't infect others. This is particularly important for those who are around people who are unvaccinated like kids or on public transport, etc.
Yes, you can die in a car crash, but chances are lower if you wear a seatbelt, so wear a seatbelt. Yes, you can die from cancer, but chances are lower if you catch it earlier, so do preventive screenings. Doesn't minimize the risk of you getting it, but minimizes the risk of severe impact.
by mmmm8 So I came back this week from 10 days in Greece. Very interesting COVID restrictions, some of which were ridiculous (no dancing... they have used drones to monitor this(!), no MUSIC allowed in Mykonos).
What I think was a good idea was most restaurants/bars, especially in resort destinations, required full vaccination for people to come indoors. Was pretty straightforward and didn't see anyone complaining, even though parts of Greece still haven't gotten to the second dose. It was sometimes overly cautious because, with the weather being beautiful, the places had all their windows and doors open. Staff in client-facing businesses (retail, hotels, salons, restaurants) get tested several times weekly, inspectors drop in to make sure testing and mask mandates are enforced. I felt it was, on average, the right balance.
I went to a wedding... there was dancing.
by Suliso I'm not sure how much these really small things matter. A myriad of various restrictions around Europe and I at least can't derive any trend. In Switzerland it's masks indoors and in public transport, otherwise no restrictions (don't know about nightclubs, but not interested anyway).
Flying to Latvia tomorrow. There need covid certificate to eat indoors. But I also hear that mask compliance much lower, especially outside Riga.
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE NOTE: The Situation Report’s esteemed epidemiologist is on vacation this week, so we will be back next week with a deeper-dive look at trends. Here are the latest numbers:
The WHO COVID-19 Dashboard reports 196.6 million cumulative cases and 4.2 million deaths worldwide as of 12:30 EDT on July 30.
Global Vaccination
The WHO reported 3.8 billion doses of SARS-CoV-2 vaccines administered globally as of July 29. The WHO reports a total of 1.48 billion individuals have received at least 1 dose, and 735 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered continues to rise, now at 37 million doses per day, driven by increases in Asia. Our World in Data estimates that there are 2.17 billion vaccinated individuals worldwide (1+ dose; 27.68% of the global population) and 1.12 billion who are fully vaccinated (14.4% of the global population).
UNITED STATES
The US CDC reported 34.7 million cumulative COVID-19 cases and 609,853 deaths. Daily incidence continues to increase, now up to 66,606 new cases per day, which is nearly 6 times the most recent low on June 19 (11,469) and is still increasing steadily. Daily mortality also continues to increase, up to 296 deaths per day, which is 78% higher than the most recent low on July 10 (166)*.
*In an effort to provide a more accurate analysis of the current epidemiology, we are largely focusing on longer-term trends, as the most recent data are more likely to be affected by changes in the frequency of state-level reporting, particularly over the weekend.
US Vaccination
The US has administered 344 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations are increasing slowly, now up to 513,685 doses per day*. A total of 189.9 million individuals in the US have received at least 1 dose, equivalent to 57.2% of the entire US population. Among adults, 69.4% have received at least 1 dose, as well as 10.5 million adolescents aged 12-17 years. A total of 163.9 million individuals are fully vaccinated, which corresponds to 49.4% of the total population. Approximately 60.3% of adults are fully vaccinated, as well as 8.1 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current value provided here corresponds to 5 days ago.
US CDC MASK GUIDANCE Amid a national surge in COVID-19 cases, hospitalizations, and deaths attributed to the highly transmissible Delta variant, the US CDC this week issued updated guidance recommending indoor mask use in areas with high or substantial transmission rates, regardless of individual vaccination status. The agency also called for universal mask use by teachers, staff, and students returning to K-12 schools this fall, regardless of their vaccination status. According to CDC Director Dr. Rochelle Walensky, the agency reinstated its indoor mask use recommendations based on new research showing that vaccinated people infected with the Delta variant carry viral loads similar to those of people who are unvaccinated. The data comes from a new CDC report released today. Dr. Walensky reiterated that the vaccines remain highly effective at preventing severe disease, that breakthrough infections among vaccinated individuals remain uncommon, and that most of the new COVID-19 cases are among unvaccinated people. US health officials continue to urge those who are not yet vaccinated or partially vaccinated to undergo the shots to help slow the spread.
US FEDERAL WORKER VACCINE RULES US President Joe Biden on July 29 announced sweeping new COVID-19-related requirements for more than 4 million federal employees and hundreds of thousands of contractors who work at federal facilities worldwide, with the goal of increasing vaccination rates among the nation’s workforce and influencing other employers. Though not considered a vaccine mandate, all federal workers will be required to sign forms attesting they are fully vaccinated for SARS-CoV-2 or face inconveniences in their daily work lives. Unvaccinated workers “will be required to wear a mask on the job no matter their geographic location, physically distance from all other employees and visitors, comply with a weekly or twice weekly screening testing requirement, and be subject to restrictions on official travel," according to information released by the White House. In his speech, President Biden also called on states and local governments to use federal funding they have received, including from the American Rescue Plan, to give US$100 to anyone who gets fully vaccinated, and he said the federal government would reimburse small- and medium-sized businesses for providing paid leave so their employees and their families could get vaccinated. He also urged the US Department of Defense to quickly implement a mask mandate for members of the military, many of whom are reluctant to undergo vaccination. The plan received mixed reactions from labor unions and other groups, some of which said giving employees options was a tactic aimed at preventing harsh resistance from some people. Questions about the plan remain, and it will be interesting to see how quickly federal agencies implement the requirements.
ADDITIONAL DOSES/”BOOSTERS” Executives from Pfizer-BioNTech, Moderna, and J&J-Janssen, which manufacture the 3 SARS-CoV-2 vaccines authorized for use in the US, have all said fully vaccinated individuals can expect to eventually need additional doses of the vaccines, or “boosters.” However, there is not enough evidence-based data yet to provide a recommendation, according to a WHO official and the CDC’s Advisory Council on Immunization Practices (ACIP), which met last week to discuss the possibility of additional doses among immunocompromised individuals. Several US government health officials, including National Institute of Allergy and Infectious Diseases (NIAID) Director Dr. Anthony Fauci, have signaled that some Americans who are older or have weakened immune systems might need an additional vaccine dose.
Pharmaceutical companies, officials, and healthcare workers cannot technically recommended additional doses for any of the vaccines in the US, which are being administered under US FDA emergency use authorizations (EUAs) that set specific standards for each regimen: 2 doses given 3 or 4 weeks apart for the Pfizer-BioNTech and Moderna vaccines, respectively, and 1 dose for the J&J-Janssen vaccine. In order to provide additional doses, the FDA would need to change a vaccine’s EUA or fully license the vaccine, which would provide greater leeway for providers to recommend additional doses. But last week, Dr. Amanda Cohn, Chief Medical Officer for the CDC’s National Center for Immunization and Respiratory Diseases (NCIRD), indicated the US government is actively looking into ways to provide access to additional doses prior to regulatory decisions, such as a compassionate use program. Some people are taking it upon themselves to seek out third doses, sometimes traveling to other states or even other countries to obtain shots.
According to media reports, Israel’s Ministry of Health on July 29 became the first country to approve third doses of the Pfizer-BioNTech vaccine for people ages 60 and older who are at least 5 months post-second dose. The country already offers third doses to immunocompromised individuals. In a decision made late on July 28, a health ministry panel concluded offering a third dose to elderly residents might help stem the country’s 6-week surge in COVID-19 cases, driven by the Delta variant. In a televised address, Israel Prime Minister Naftali Bennett, noting the Pfizer-BioNTech vaccine is safe and effective, encouraged those eligible to begin registering for third doses as of August 1. Since the emergence of the Delta variant, the Israel Ministry of Health has twice announced a drop in effectiveness of the Pfizer-BioNTech vaccine in preventing symptomatic infection, although some experts say the data could be skewed because most testing occurred in transmission hotspots and among elderly populations.
PFIZER-BIONTECH EFFICACY/THIRD DOSE On July 28, medRxiv published preprint data from Pfizer-BioNTech showing the efficacy of its vaccine to prevent COVID-19 declined about 6% every 2 months over a period of 6 months. The data were collected from more than 40,000 clinical trial participants in Europe and the Americas. From 7 days to <2 months post-dose 2, vaccine efficacy was 96.2% (95% confidence interval [CI] 93.3-98.1); from 2 months to <4 months, efficacy was 90.1% (95% CI 86.6-92.9); and from 4 months to 6 months, efficacy was 83.7% (95% CI 74.7-89.9). Overall, vaccine efficacy was 91.1% (95% CI 88.8-93.0) for preventing symptomatic COVID-19, and 96.7% (95% CI 80.3-99.9) against severe disease. The companies said the data show the vaccine to be safe and highly efficacious in preventing COVID-19 through 6 months post-second dose in diverse populations but further data are needed to know whether efficacy continues to wane or whether “booster” doses will be necessary, and, if so, the timing of such doses.
Many experts said the not-yet-peer-reviewed data are reassuring, showing that people who are fully vaccinated likely are adequately protected. However, if the observed decline in efficacy steadily continues over time, it would fall below the internationally accepted threshold of 50% within 18 months of vaccination. This would bolster Pfizer-BioNTech’s claim that an additional shot of its vaccine will be needed to maintain long-term protection. The data also do not address the vaccine’s efficacy against the now widespread Delta variant. On July 28, Pfizer officials presented unpublished data in a quarterly earnings report to investors showing a third dose of the Pfizer-BioNTech vaccine could boost neutralizing antibody titers against the Delta variant in a small sample of individuals. The data show a more than 5-fold increase in post-second dose titers among vaccinees aged 18 to 55 and a more than 11-fold increase among those ages 65 to 85. The officials said they plan to seek authorization with the US FDA for a third dose by mid-August and indicated clinical studies of an experimental Delta variant vaccine are awaiting regulatory approval but also are expected to begin in August.
BREAKTHROUGH CASES A study published in the New England Journal of Medicine on July 28 examines breakthrough COVID-19 cases among healthcare workers who received 2 doses of the Pfizer-BioNTech vaccine. From January 20 to April 28, 2021, researchers identified breakthrough cases at Sheba Medical Center in Israel by monitoring healthcare workers for COVID-19 symptoms and testing those with known COVID-19 exposures. Following the identification of a breakthrough case, the research team matched the individual with 4 or 5 uninfected controls using generalized estimating equations. Of 39 breakthrough cases among 1,497 fully vaccinated healthcare workers, the researchers found the infected individuals had lower levels of neutralizing antibody titers than their uninfected controls. Additionally, most of the breakthrough cases were asymptomatic or mildly symptomatic, although 19% of the individuals reported symptoms that lasted longer than 6 weeks. The majority of the breakthrough cases (85%) were caused by the Alpha variant (B.1.1.7), and the research team observed no secondary cases stemming from breakthrough cases.
IMF GLOBAL FORECAST In an updated “World Economic Outlook,” the International Monetary Fund (IMF) on July 27 warned that the gap in economic recovery is widening between higher- and lower-income nations due to the COVID-19 pandemic and uneven access to SARS-CoV-2 vaccines. Overall, the global economy is expected to grow 6% in 2021 and 4.9% in 2022. The IMF upgraded its 2022 estimate, with a 0.5 percentage point increase over its projection made earlier this year, driven by growth in the US and UK markets. However, for emerging and developing markets, the IMF downgraded projections for 2021 by 0.4 percentage points from its previous projection, to 6.3%, noting the biggest risks include low vaccination rates and growing numbers of COVID-19 cases. The IMF called on wealthier nations to take urgent action to share vaccine doses with low- and middle-income countries (LMICs), warning that a worsening pandemic could severely hit those markets as well as impact growth projections for richer nations.
The IMF also cautioned that if inequality worsens, nations risk experiencing political instability and discontent, which is happening already in some countries. The pandemic is sowing a “summer of anger,” with political protests documented in Tunisia, Iraq, South Africa, Thailand, Colombia, Brazil, and Haiti, to name a few. Even some wealthier nations—including France and Australia—recently have witnessed large protests against vaccination mandates and lockdown tactics centered on slowing the number of new COVID-19 cases. Experts from the Council on Foreign Relations (CFR) and Columbia University write that “COVID-19 has acted like lighter fluid for countries where embers of discontent were already smoldering.” In a closed briefing this week, Ramesh Rajasingham, UN Acting Assistant Secretary-General for Humanitarian Affairs and Deputy Emergency Relief Coordinator, warned UN Security Council members that three-quarters of the countries needing humanitarian aid have already recorded more COVID-19 cases and related deaths than in all of 2020. Calling the response so far “inadequate,” Rajasingham urged the international community to not only increase vaccine shipments to fragile and conflict-affected countries but also bolster delivery systems by providing logistical and security support. The need for effective and efficient vaccine delivery to LMICs is an issue that cannot be ignored by the developed nations and the private sector.
US POVERTY REDUCTION The number of poor Americans is expected to decline nearly 45% this year from 2018 levels—a record drop in record time—but pieces of the enormous temporary safety net created amid the COVID-19 pandemic that helped to achieve this reduction have ended or are scheduled to soon revert to their pre-pandemic size. In a report released on July 28, the Urban Institute estimated the American Rescue Plan Act, enacted in March 2021, will reduce the 2021 annual poverty rate to 7.7%, well below the 13.9% rate estimated for 2018. The projected poverty rate is expected to be lowest among children (5.6%), but rise for adults ages 18 to 64 (8.1%) and again for older Americans (9.2%). The rates are higher for Hispanic people (11.8%), Asian American and Pacific Islanders (AAPI; 10.8%), and Black people (9.2%) than for white people (5.8%). The federal stimulus checks have had a larger impact on poverty reduction than any other program, according to the report.
One of these programs, the US CDC’s extended federal eviction moratorium, which has prevented eviction for an estimated 10 million people over the past year, is set to expire on July 31. Some advocates, researchers, and US lawmakers are calling for another extension of the program, citing an analysis showing many of these evictions would occur in communities with low vaccination rates and increasing numbers of COVID-19 cases attributed to the Delta variant. A study published this week in the American Journal of Epidemiology supports calls for extending the moratorium, showing that between March and September 2020, eviction moratorium expirations were associated with increased COVID-19 incidence and deaths and backing up the notion that eviction prevention constitutes an important public health measure to mitigate the pandemic’s impacts.
“MEDICAL FREEDOM” LAW New Hampshire (US) Governor Chris Sununu last week signed into law a so-called “medical freedom” bill that prohibits “any public facility, any public benefit, or any public service” from requiring state residents be vaccinated against SARS-CoV-2 to receive or access such services or facilities. The law states that “every person has the natural, essential, and inherent right to bodily integrity, free from any threat or compulsion by government to accept an immunization.” Notably, the law sets out several exceptions, including vaccination requirements for schools, childcare, county nursing homes, and the state’s mental health system. Additionally, the New Hampshire Department of Corrections may mandate certain medical treatments or immunizations “when a direct threat exists.” The law does not address private businesses. Governor Sununu continues to voice support for SARS-CoV-2 vaccines. According to state data, nearly 54% of the state’s residents are fully vaccinated, above the national average.
TENNESSEE VACCINE OUTREACH The Tennessee (US) state government last week resumed its adolescent vaccine education and outreach activities after earlier this month halting most advocacy in the face of pressure from conservative state lawmakers who accused the department of pressuring teenagers to receive a SARS-CoV-2 vaccine. Tennessee Health Commissioner Dr. Lisa Piercey on July 23 said the state’s health department will restart outreach efforts recommending vaccines for children, except for social media posts specifically targeting teenagers. The department once again will include its logo on public-facing vaccine material and hold vaccination events on school property, including for COVID-19. Dr. Piercey stressed the department never ceased vaccinations among children but only paused its communications and marketing efforts surrounding vaccines. Now that those efforts are restarting, messaging will be targeted toward parents, she noted. Dr. Piercey declared the state will provide vaccines to minors without parental permission in “fringed and nuanced” circumstances. Tennessee is in the bottom 10 states in terms of vaccination coverage, with 39% of its population fully vaccinated.
TANZANIA Tanzania President Samia Suluhu Hassan on July 28 kicked off the country’s SARS-CoV-2 vaccination campaign, publicly receiving the J&J-Janssen vaccine in an effort to bolster confidence in the shots and quell fear stemming from disinformation spread under her predecessor’s administration. Former President John Magufuli, who died in March of heart complications, downplayed the COVID-19 pandemic, endorsed home remedies and prayer as treatments, and called vaccinations “dangerous.” After Magufuli’s death, President Hassan established a COVID-19 expert committee to evaluate the safety and effectiveness of vaccines, as well as make public health recommendations including physical distancing and mask wearing. Tanzania joined COVAX in June, despite having been eligible since the facility’s establishment. The country received more than 1 million doses of the J&J-Janssen vaccine over the weekend from a US donation delivered through COVAX, and President Hassan on July 27 placed an order with the African Union's African Vaccine Acquisition Task Team (AVATT) for an undisclosed number of additional vaccines. The Tanzania government faces challenges to reversing skepticism about vaccines, but President Hassan assured residents the country will obtain enough supplies to reach its goal of vaccinating 60% of the population. Only 2 other African nations—Burundi and Eritrea—have yet to begin national vaccination campaigns.
TOKYO OLYMPICS The Olympics have entered the start of their second week as the COVID-19 situation in Tokyo and Japan continues to worsen. Both the city and the nation on July 29 reported record numbers of new COVID-19 cases, with the nation averaging 6,518 daily new cases. Tokyo, which remains under a state of emergency, recorded 3,865 new cases on July 29, after only the day before passing 3,000 new cases for the first time. The city’s health officials have asked for hospitals to prepare extra beds as the spread of the SARS-CoV-2 Delta variant continues, with more than 75% of new cases caused by the variant. So far, COVID-19 precautions appear to have minimized the spread of SARS-CoV-2 outside of the Olympic “bubble,” although the number of new daily cases reported among Olympic accreditation holders appears to have risen on July 29 and July 30.
COGNITIVE IMPACTS Scientists have long known that areas of the brain involved with smell and taste also are involved in memory, thinking, planning, and mood, and public health officials are increasingly concerned about the long-term impacts of COVID-19 on brain function, memory, and cognition, a phenomenon known as “brain fog.” Scientific evidence is emerging that the virus’s neurological impacts are multi-pronged and not necessarily related to “long COVID,” or post-acute sequelae of COVID-19 (PASC). In a study published in The Lancet journal EClinicalMedicine, researchers from Imperial College London and colleagues examined data from 81,337 people who took exams as part of the Great British Intelligence Test and completed questionnaires regarding self-reports of suspected or confirmed COVID-19. The team found that the 12,689 individuals who had recovered from COVID-19 exhibited significantly more cognitive deficits than their matched counterparts, even among people who said they were no longer experiencing symptoms. Cognitive deficits were found to be especially substantial among those who were hospitalized, those who were hospitalized and on a ventilator, and those who had more severe symptoms but recovered at home.
Researchers with the University of Texas Health Science Center at San Antonio, who recently presented data at the Alzheimer's Association International Conference, found that neurological changes seen after COVID-19 mirror those found in people with Alzheimer’s disease. Genetic studies are showing that the genes responsible for increasing the risk of more severe COVID-19 also increase the risk of Alzheimer’s. Additionally, anecdotal reports suggest Alzheimer’s diagnoses appear to be more common among people in their 60s and 70s who have had severe COVID-19. Further research is ongoing to determine COVID-19’s longer-term impacts on neurological function, including cognition, intelligence, and risk of Alzheimer’s disease.
MUCORMYCOSIS Following India’s most severe COVID-19 surge in the spring, the country has seen an increase in cases of mucormycosis, also called “black fungus,” and related deaths. Since late March, the nation has recorded more than 45,000 cases of the disease, a serious but rare fungal infection caused by the mucormycetes group of molds, and more than 4,300 people have died, with most having contracted COVID-19 prior to their fungal infection. Clinicians have noted that symptoms usually manifest 12-18 days after COVID-19 recovery. In a letter published July 29 in Drug Development Research, researchers warn that because uncontrolled diabetes and other immunosuppressive diseases, as well as corticosteroid treatment, are seen as risk factors for the fungal infection, they suggest avoiding steroids to treat COVID-19, as they might be a contributing factor to the disease. As the number of mucormycosis cases continue to rise, there are questions about unreliable supplies of the drug used to treat the infection, adding an additional challenge to India’s already complicated COVID-19 recovery.
Suliso wrote: ↑Fri Jul 30, 2021 3:11 pm
I don't understand people who are vaccinated and not immuno compromised who're super scared of this virus and test all the time. Sure there is some small chance of catching it in a bad way anyway, but so what? There is also a chance of dying in a car crash or getting a cancer. Both happen - in my 12 years in a large company one co-worker has died in a car crash and two from cancer. None of them were 40 yet. Don't do crazy stuff, but enjoy your life while you can. Who knows how much time fate has reserved for you...
^ As M8 says, surely some of these vaccinated people are concerned about others, and not just about themselves. There are a few unselfish people on the planet. Far too few - but they do exist here and there.
And so testing even after being fully vaccinated can be because, although they may be fine if they contract the virus, they know that they can infect other, non-vaccinated people, and want to avoid doing that.
Suliso wrote: ↑Fri Jul 30, 2021 3:20 pm
Australian government saying that they'll keep locking down till 80% population vaccinated. Whenever that is... I think it's maddness. I've lost a lot of respect for Australia seeing how they abused their own citizens, particularly those living abroad.
^ The only thing I reproach Australia for is for not vaccinating early enough. They did a tremendous job in keeping the initial waves of the virus at bay - yes, their methods were somewhat extreme, but it kept a lot of people healthy and alive who would have otherwise been quite sick and/or died. This, to me, is justification.
But they became arrogant in thinking that they were somehow immune to the significant propagation of the virus seen in other countries, and so didn't get the vaccines as soon as they were available.
Overall, I see that too many people want to have their cake and eat it, too. This is typical human behaviour, sadly. Even after 18 months of this virus, far too many people still want to have the freedom they had before the virus AND be protected from the virus. It's as baffling as it is disappointing.
by Suliso I actually meant to emphasized the scared part. As in testing because they're continuously scared and not because visiting a frail grandmother. That's the part that doesn't make sense to me.
by atlpam If you're running a 103+ fever for 7-10 days, it's not a stretch to think there may be cognitive impacts.
by dmforever So yes, they don't state numbers, but it looks like the number of people in these groups in both cases isn't insignificant.
This is an article about people who didn't get the COVID vaccine in the US and regret it.
In case you don't want to read it or have a paywall, here is an truly mind boggling part:
The recent surge of infections and hospitalizations among unvaccinated people has brought the grim realities of Covid-19 crashing home for many who thought they had skirted the pandemic. But now, with anger and fatigue piled up on all sides, the question is whether their stories can actually change any minds.
Some people hospitalized with the virus still vow not to get vaccinated, and surveys suggest that the majority of unvaccinated Americans are not budging. Doctors in Covid units say some patients still refuse to believe they are infected with anything beyond the flu.
And this article is about people who are afraid to tell their families or loved ones that they are getting vaccinated. I'm really at a loss for words.
I would add:
Plus banned from entering the country until the pandemic is over, as decided by the Canadian Govt.
That would feel good.
---0---
And Deuce may have been right about people forging certificates (may as in 99% may): people down here are selling fake PCR test results.
Vamos, Colombia!!! (their rallying cry at sports events)
by ti-amie
by dryrunguy On my way home back from Ohio, we stopped at the service area in Bedford so Polly the Dog and both of us could pee. When I went inside, approximately half of the people inside were wearing masks. That was an exponential improvement over what I saw in Ohio. But it's worth noting, these were travelers headed EAST. This service area was not accessible to drivers headed WEST. Not sure there would have been a difference. Perhaps the westbound service area would have been better or similar. Just an observation on a late Saturday afternoon.
by ti-amie
by dryrunguy Another observation: I saw my first Trump/DeSantis 2024 flag today. Not a sign, a flag. That was in either eastern Ohio or western Pennsylvania. Not sure. Doesn't matter. They're the same.
by Deuce
ponchi101 wrote: ↑Sat Jul 31, 2021 8:07 pm
And Deuce may have been right about people forging certificates (may as in 99% may): people down here are selling fake PCR test results.
Vamos, Colombia!!! (their rallying cry at sports events)
^ Sadly, my experience in and observation of life has led me to possess little faith in the human animal.
Amazing potential to do wonderful things... but, tragically the potential to do stupid and harmful things is acted upon more than is the potential to do good.
^ Let's contemplate this for a moment...
After 16 months in this pandemic - that is 16 months worth of intense education every day... plus many more people being vaccinated today than were vaccinated in the first 12 months... Florida has more case counts now than at any time in the past 16 months.
This is truly incredible. These people have learned absolutely nothing, even while being intensely educated every day for the past 16 months. That is over 450 consecutive days of intense education - and the result is that they've learned absolutely nothing.
It is truly beyond astounding.
by JazzNU
dryrunguy wrote: ↑Sun Aug 01, 2021 12:50 am
On my way home back from Ohio, we stopped at the service area in Bedford so Polly the Dog and both of us could pee. When I went inside, approximately half of the people inside were wearing masks. That was an exponential improvement over what I saw in Ohio. But it's worth noting, these were travelers headed EAST. This service area was not accessible to drivers headed WEST. Not sure there would have been a difference. Perhaps the westbound service area would have been better or similar. Just an observation on a late Saturday afternoon.
You know I'm a Turnpike expert, so I think I know which service area you are talking about, though I don't think I realized that was in Bedford (is there another one across the highway for the westbound?). I haven't stopped there often, I prefer the next service area, but did you get a look at any of the plates? Saturday is typically the start/end to week-long rentals so it may not mean much, but that might be somewhat of a tell.
But here's the other thing, heading East could be a factor as you're guessing, or more accurately, Southeast. I'm not 100% positive since it's been awhile since I visited the fam. But as you are leaving this service area and get back on the Turnpike, is it before or after the Breezewood exit? I feel like it's before, because the Bedford exit is one before Breezewood. That service station more than likely has a high amount of drivers that are going to get off the Turnpike and continue on 1-70. So Maryland, DC, and Virginia more than likely destinations, not just coming East across the state. Because unless it's your first time making that trip, you best stop at that service area or in Breezewood before you head into Maryland unless you want to get off the road for food or gas as they have rest stops, not service areas, along the road in that part of Maryland unless they've made some improvements recently.
by ti-amie
by ti-amie
by Deuce Maybe - just maybe - the fact that he's getting his 'medication' from a tractor supply store is a slight indication that the guy is not playing with a full deck.
Just maybe...
by ponchi101 Why do I find it fitting that republicans are being treated by veterinarians?
by dryrunguy Ivermectin is a DE-WORMER used in sheep, goats, cattle, and horses that also HAPPENS to be effective in fighting external parasites (lice). It is NOT an anti-viral or antibiotic. For any species.
dryrunguy wrote: ↑Sun Aug 01, 2021 12:50 am
On my way home back from Ohio, we stopped at the service area in Bedford so Polly the Dog and both of us could pee. When I went inside, approximately half of the people inside were wearing masks. That was an exponential improvement over what I saw in Ohio. But it's worth noting, these were travelers headed EAST. This service area was not accessible to drivers headed WEST. Not sure there would have been a difference. Perhaps the westbound service area would have been better or similar. Just an observation on a late Saturday afternoon.
You know I'm a Turnpike expert, so I think I know which service area you are talking about, though I don't think I realized that was in Bedford (is there another one across the highway for the westbound?). I haven't stopped there often, I prefer the next service area, but did you get a look at any of the plates? Saturday is typically the start/end to week-long rentals so it may not mean much, but that might be somewhat of a tell.
But here's the other thing, heading East could be a factor as you're guessing, or more accurately, Southeast. I'm not 100% positive since it's been awhile since I visited the fam. But as you are leaving this service area and get back on the Turnpike, is it before or after the Breezewood exit? I feel like it's before, because the Bedford exit is one before Breezewood. That service station more than likely has a high amount of drivers that are going to get off the Turnpike and continue on 1-70. So Maryland, DC, and Virginia more than likely destinations, not just coming East across the state. Because unless it's your first time making that trip, you best stop at that service area or in Breezewood before you head into Maryland unless you want to get off the road for food or gas as they have rest stops, not service areas, along the road in that part of Maryland unless they've made some improvements recently.
Eastbound on I-76, the Bedford exit, and service area, is BEFORE the Breezewood exit. And yes, I think there is also one westbound. But we never stop there.
by Suliso I'm reading that there is a strong genetic/biochemical component to how ill one does or does not get when exposed. In addition to age, gender and general health.
by ponchi101
Suliso wrote: ↑Mon Aug 02, 2021 4:54 pm
I'm reading that there is a strong genetic/biochemical component to how ill one does or does not get when exposed. In addition to age, gender and general health.
I think the genetics are very important. Just anecdotal, but NBA's Karl Anthony Town's family had several members dying from the disease, and he caught it too. It was as if they were particularly susceptible.
by ti-amie
by ti-amie
by ponchi101 No way this thing stops at DELTA. We should have a pool to see where in the Greek alphabet the virus will end. Or if we will need a second alphabet.
by Deuce
Suliso wrote: ↑Mon Aug 02, 2021 4:54 pm
I'm reading that there is a strong genetic/biochemical component to how ill one does or does not get when exposed. In addition to age, gender and general health.
I think it's been rather obvious since the beginning that there is something within one's personal biological make-up which renders one more susceptible to more severe reactions to the virus (including death), as some people are asymptomatic, while others don't survive it. Discovering that it may be genetic is of little use unless they can specify what it is, exactly... and then begin working on testing everyone for susceptibility and how to protect those who are susceptible. Until then, we all need to be careful.
I don't think that we can factor in general health, age, and gender - simply because people of all ages, from both genders, and otherwise perfectly healthy persons, have all become extremely ill and/or have died from this virus. And not in small numbers.
In other words, until we know much more, it's still extremely unpredictable.
ponchi101 wrote: ↑Mon Aug 02, 2021 7:05 pm
No way this thing stops at DELTA. We should have a pool to see where in the Greek alphabet the virus will end. Or if we will need a second alphabet.
^ I agree.
But we must remember that each new mutation/variant can be more transmissible and/or more severe, or can be less transmissible and/or less severe.
Let's hope for the latter... while still protecting ourselves against the former.
Naming variants for the Greek alphabet will likely only be for the variants which are more transmissible and or more severe.
by Suliso Age is still the main factor. Sure you find some younger victims, but the overwhelming majority is 50+ and most also have other health concerns. After that becomes more complicated.
by dryrunguy Here's the latest Situation Report. The paragraph about transmission among deer was fascinating. You have to wonder about other species... I know from earlier reports that dogs and cats can get it.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 198.8 million cumulative cases and 4.2 million deaths worldwide as of 11:30 EDT on August 3. Global weekly incidence increased for the sixth consecutive week, up 5.1% over the previous week, but weekly mortality decreased for the first time since June, down 8% compared to the previous week.
The US is #1 globally in terms of total daily incidence (85,459 new cases per day), accounting for 14% of the global total, and Indonesia is #1 in terms of total daily mortality (1,789 deaths per day), representing 19% of the global total.
Global Vaccination
The WHO reported 3.89 billion doses of SARS-CoV-2 vaccines administered globally as of August 3. The WHO reports a total of 1.51 billion individuals have received at least 1 dose, and 752 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered continued to increase through August 1, peaking at 41 million doses per day before falling to 39 million on August 2. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.23 billion vaccinated individuals worldwide (1+ dose; 28.6% of the global population) and 1.15 billion who are fully vaccinated (14.8% of the global population).
UNITED STATES
The US CDC reported 34.97 million cumulative COVID-19 cases and 611,051 deaths. Despite considerable vaccination coverage at the national level, daily incidence continues to accelerate, mirroring the early stages of previous surges. At 72,790 reported cases per day on July 30, the current surge is the United States’ second largest to date, surpassing both the spring 2020 and spring 2021 peaks. The average daily incidence is the highest since February 17*.
We expect the US to surpass 35 million cases in this afternoon’s update. If that is the case:
1 case** to 5 million cases- 196 days
5 million to 10 million- 93 days
10 million to 15 million- 29 days
15 million to 20 million- 25 days
20 million to 25 million- 22 days
25 million to 30 million- 61 days
30 million to 35 million- 132 days
**First reported cases on January 22, 2020.
Daily mortality also continues to increase, up to 302 deaths per day on July 30, which is 76% higher than the most recent low on July 10 (172)*. Daily mortality does not appear to be increasing exponentially like daily incidence; however, this could change over the coming weeks as daily incidence increases.
As the US epidemic continues to surge, several states are reporting daily incidence at or near their highest peak to date. According to CDC data, Louisiana (4,119 new cases per day) has already surpassed its previous record—10% higher than its January 2021 peak—and Hawai’i (298) surpassed its highest peak (August 2020). On July 30, Florida reached its second highest average daily incidence to date (15,817). Florida has not yet reported data from this weekend, and we expect that it will set a new record in its next report. Arkansas (1,869) and Mississippi (1,475) are at 61% and 63% of their respective highest peaks, both in January 2021. And Alabama (2,057) and Missouri (2,642) are both approaching 50% of their highest peaks from January 2021 and November 2020, respectively*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the current date.
US Vaccination
The US has administered 347 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations are increasing slowly, now up to 552,647 doses per day*. A total of 191.8 million individuals in the US have received at least 1 dose, equivalent to 57.8% of the entire US population. Among adults, 70.0% have received at least 1 dose—finally reaching the White House’s target—as well as 11.1 million adolescents aged 12-17 years. A total of 164.9 million individuals are fully vaccinated, which corresponds to 49.7% of the total population. Approximately 60.6% of adults are fully vaccinated, as well as 8.4 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
VACCINE-RESISTANT VARIANT RISK With the number of new COVID-19 cases rising in much of the world, scientists are warning that continued transmission provides an opportunity for the evolution of new, and potentially more harmful, SARS-CoV-2 variants. The current increase in cases is being fueled by the highly transmissible Delta variant as well as the loosening and inconsistent use of public health prevention measures, increased social mobility, and inequitable vaccine access, WHO Director-General Dr. Tedros Adhanom Gebreyesus said on July 30, warning that health systems in many countries are overwhelmed and that more variants will emerge as long as the virus continues to spread. US CDC Director Dr. Rochelle Walensky cautioned that a new variant could potentially evade vaccines but added the vaccines authorized in the US continue to protect people from severe disease and death.
In a modeling study published in Nature Scientific Reports on July 30, researchers with the Austria Institute of Science and Technology examined the impact of the rate of vaccination and the strength of non-pharmaceutical interventions on the probability of the emergence and establishment of a vaccine-resistant SARS-CoV-2 strain. The researchers' model identified three factors that could lead to the establishment of a vaccine-resistant strain: the high probability of a resistant strain’s initial emergence, a high number of infected individuals, and a low rate of vaccination. The researchers’ analysis showed that the highest risk of vaccine-resistant strain establishment occurs when a large proportion of the population is vaccinated but viral transmission is high, underlining the importance of controlling transmission through public health interventions while continuing vaccination campaigns. Nevertheless, the researchers conclude “the emergence of a partially or fully vaccine-resistant strain and its eventual establishment appears inevitable.” The UK’s Scientific Advisory Group for Emergencies (SAGE) published an updated theoretical and non-peer-reviewed paper on July 30 essentially coming to the same conclusion, that a vaccine-resistant SARS-CoV-2 variant almost certainly will emerge and public health authorities must continue efforts to reduce transmission as much as possible.
US CDC MASK GUIDANCE The US CDC’s latest masking guidance—calling for all people, even those who are vaccinated, to wear masks in indoor public settings in areas where transmission is categorized as high or substantial—is in direct response to the increased transmissibility of the Delta variant. According to data released last week, data show that individuals fully vaccinated for SARS-CoV-2 who become infected—known as breakthrough cases—carry viral loads similar to those found in infected unvaccinated individuals, suggesting that vaccinated people can transmit the Delta variant of concern just as easily as those who are unvaccinated.
The data are based on a COVID-19 outbreak that began in Provincetown, MA (US) in early July following multiple summer events and large public gatherings. Of the 496 cases reported in the outbreak at the time of data analysis, 346 (74%) cases were among fully vaccinated people and 90% of 133 cases sequenced were caused by the Delta variant. Almost 80% of the breakthrough cases were symptomatic, with common symptoms including cough, headache, sore throat, myalgia, and fever. Among 5 patients who were hospitalized, 3 had underlying medical conditions and 4 were vaccinated. No deaths were reported. The report, published as an early release in the CDC’s MMWR, said even jurisdictions without high or substantial transmission should consider expanding prevention measures, including masking for all individuals in indoor public spaces. Health officials emphasize that breakthrough cases remain rare and that vaccines provide protection against severe symptoms and hospitalization. Lending further credence to the protective power of the vaccines, data show that counties with low vaccination rates are experiencing rapid rises in COVID-19 cases and increases in deaths.
SARS-COV-2 TRANSMISSIBILITY An internal report from the US CDC suggests that the SARS-CoV-2 Delta variant may be capable of causing more severe disease than previous variants and that it may be as transmissible as chickenpox. Studies from Canada, Scotland, and Singapore indicate that individuals infected with the Delta variant are at a higher risk of hospitalization and requiring oxygen supplementation. Evidence discussed in the report shows that the Delta variant may be capable of skirting the protection offered by the vaccines, and fully vaccinated individuals who become infected may carry high viral loads in their noses and throats, possibly making transmission from the vaccinated more common than previously understood. Despite the concerns raised in the report, vaccination remains the best way to protect against severe disease. The report states that vaccines are capable of preventing severe symptoms in at least 90% of cases, even though they might be less effective at preventing infection. Experts acknowledge that discussions around vaccination may need to shift from preventing transmission to personal protection in light of the new data.
US EVICTION MORATORIUM The federal eviction moratorium, administered by the US CDC, expired on July 31, without extension, after the US Supreme Court on June 29 declared that the agency could no longer extend the program without “clear and specific congressional authorization (via new legislation).” A recent surge in COVID-19 daily incidence, driven by the highly transmissible Delta variant, is lending urgency to efforts to keep people in their homes and out of congregate or dangerous living situations, such as in shelters or on the street. More than 11 million adult renters are behind on payments, according to the Center on Budget and Policy Priorities. But it appears the CDC, US Congress, and the White House were caught off guard by the moratorium’s expiration, leaving officials scrambling for solutions.
Over the weekend, White House officials asked the CDC to extend the moratorium, focusing specifically on areas with high or substantial COVID-19 transmission, but the CDC denied the request, saying it has no legal authority to do so under the Supreme Court’s ruling. Additionally, Congress failed to pass legislation that would have provided a last-minute extension of the federal moratorium until October 18. Afterward, Congressional leaders called on the White House to extend the moratorium, but officials said they also lack legal authority to do so. On August 2, US President Joe Biden called on state and local governments to extend or implement eviction moratoria for at least the next 2 months. Approximately one-third of states currently have eviction moratoria through August. Additionally, President Biden, at the request of Congressional leadership, is asking relevant federal agencies to examine why more of US$46.5 billion in Emergency Rental Assistance provided to state and local governments has not yet been distributed. The White House made other requests of federal, state, and local agencies and jurisdictions and committed to “doing everything in its power” to keep people housed.
US GLOBAL VACCINATION PROGRAM The US government announced today that the country has donated and shipped more than 110 million doses of SARS-CoV-2 vaccines to more than 60 countries, fulfilling a June pledge by President Joe Biden to donate at least 80 million doses. The majority of the vaccines were shipped through the COVAX facility, with other portions provided through regional partners such as the African Union and the Caribbean Community (CARICOM). Reportedly, an “initial tranche” of 25 million vaccines is going to African nations, and the US government is supporting vaccine manufacturing efforts in South Africa and Senegal. A White House fact sheet lists the countries and amount of vaccines the US has donated to date.
According to the fact sheet, the US government has purchased 500 million doses of the Pfizer-BioNTech vaccine and expects to begin shipping them to 100 low-income countries at the end of August. The donated vaccine doses, worth $3.5 billion, will be delivered through COVAX, helping the facility get closer to its goal of delivering 2 billion doses in 2021. However, to offset the costs of purchasing the supply, the US reportedly is diverting hundreds of millions of dollars intended to support vaccination drives in low-income countries. COVAX continues to struggle, delivering only 177 million vaccines so far, some of which are going unused in recipient countries due to a lack of funding, shortage of sufficient transportation, a dearth of trained vaccine administrators, or the absence of public interest to receive the shots.
EMERGENT VACCINE PRODUCTION FACILITY After a more than 3-month shutdown of SARS-CoV-2 vaccine manufacturing at Baltimore, MD (US)-based Emergent BioSolutions, the US FDA last week granted permission for the plant to resume manufacturing based on the regulatory agency’s “observations of the implemented corrective actions.” As we previously reported, the FDA published a report in April stating the facility was unsuitable to produce vaccine doses, and Emergent agreed to pause production until issues identified in the report were resolved, which appears to have happened. At the time, Emergent was manufacturing both the J&J-Janssen and AstraZeneca-Oxford vaccines for the federal government; production for the latter has since moved to another company. J&J, which has been in control of the plant since April, confirmed the FDA is permitting manufacturing to resume and said it will continue to work with the agency to gain clearance to use up to 30 million doses of its vaccine made at the facility prior to its shutdown.
In a call with investors on July 29, Emergent officials disclosed a US$41.5 million loss from having to discard vaccine doses deemed unusable by regulators as well as the expenditure of US$12.4 million to address problems at the facility. The following day, Emergent filed documents with the US Security and Exchange Commission disclosing for the first time it has received “preliminary inquiries and subpoenas to produce documents” stemming from shareholder lawsuits and investigations from the SEC, the US Department of Justice, the Financial Industry Regulatory Authority, the state attorney generals of Maryland and New York, and committees in both houses of the US Congress. Additionally, Reuters reports that AstraZeneca-Oxford vaccine doses sent from the plant to Canada and Mexico in late March were cleared without proper regulatory inspections. These reports underscore ongoing troubles for Emergent, which holds a US$628 million federal contract to be the primary domestic manufacturer of both the J&J-Janssen and AstraZeneca-Oxford vaccines, as well as other federal contracts for various products included in the National Strategic Stockpile, most notably the company’s anthrax vaccine.
DELTA VARIANT IN CHINA Once recognized as implementing the world’s strictest COVID-19 prevention measures, China’s zero tolerance COVID-19 policy is facing challenges amid a recent increase in cases caused by the Delta variant. The policy attempts to keep the country’s number of cases to zero by limiting international travel, requiring regular testing, and enforcing stringent quarantine measures, among other regulations. But over a period of 2 weeks, the country’s average number of new daily COVID-19 cases has more than doubled and nearly half of China’s 32 provinces have reported cases caused by the Delta variant, indicating the variant is moving quickly. This current wave is thought to have originated at the international airport in the eastern city of Nanjing, after a case was first detected on July 20. All 9.3 million residents of Nanjing are undergoing testing, and the city of Wuhan, where the virus was first detected in late 2019, plans to test all 12 million residents. Wuhan recently recorded 3 cases of the Delta variant after having reported no cases since mid-May 2020. The variant’s rapid spread has raised concerns over the level of protection provided by Chinese vaccines. So far, China has administered 1.7 billion doses, enough to fully vaccinate about 60% of its population. Public health officials estimate 80% of the population will be fully vaccinated by the end of the year.
INDONESIA Healthcare workers in Indonesia are overwhelmed, as daily COVID-19 incidence remains high, daily mortality continues to climb, patient capacity surges, and medical supplies dwindle. The country’s average number of new daily cases peaked on July 18, reaching a number 4 times higher than the previous peak in January 2020. Average daily incidence is down as of August 2 but still remains high. Average daily mortality continues to rise as of August 2 and is currently 6 times higher than the previous peak in January 2020. Approximately 1,200 healthcare workers in Indonesia have died during the pandemic; nearly half of those were doctors. Many more healthcare professionals have been infected and returned to work after recovering. Facing long hours, stressful working conditions, and greater exposure to infected patients, Health Minister Budi Gunadi Sadikin said the country is prioritizing providing additional vaccine doses to healthcare workers. Most who have been vaccinated received the Chinese Sinovac vaccine, but the additional doses will be the Moderna vaccine.
AUSTRALIA LOCKDOWNS Military personnel are being brought in to help local police enforce a lockdown in New South Wales, Australia. The lockdown comes in response to an outbreak of the highly transmissible SARS-CoV-2 Delta variant in the region. The lockdown was recently extended to August 28 after an outbreak of 170 cases was traced to an infected individual who failed to self-isolate. The 300 unarmed military personnel will aid in enforcing the lockdown by knocking on residents’ doors to ensure everyone is complying with stay-at-home orders. In parts of Sydney, the state’s largest city, residents will be required to wear masks when outdoors and stay within 5 kilometers (3 miles) of their residence. On August 2, Queensland state extended lockdown orders through August 8 in its largest city, Brisbane, after officials detected 13 new locally acquired cases. Australia is expected to continue cycles of stop-start lockdowns until at least 70% of the population is fully vaccinated. Prime Minister Scott Morrison said he expects to reach that goal by the end of the year; only 15.4% of the population is fully vaccinated as of August 2.
BLOOD CLOTS Two studies recently published by The Lancet provide additional insight into the risk of blood clots associated with the AstraZeneca-Oxford SARS-CoV-2 vaccine. A peer-reviewed study conducted by researchers at AstraZeneca included data from all reported cases of thrombosis with thrombocytopenia syndrome (TTS, a blood clotting disorder) within 14 days of vaccination with either dose of the AstraZeneca-Oxford vaccine reported to AstraZeneca’s global safety database through April 30. The researchers identified 399 cases of TTS among 49.2 million individuals who received the first dose of the vaccine, equating to an estimated risk of 8.1 cases per million doses. The risk decreased following the second dose, however, down to 2.3 per million doses—13 cases of TTS among 5.62 million individuals who received the second dose. The researchers estimated that the average over a 14-day period prior to the pandemic was as high as 7.16 cases of TTS per million people. So while the risk following the first dose of the vaccine was a slight increase over the expected risk, the risk following the second dose was “within preliminary estimates.”
A preprint study, conducted in Spain and funded by the European Medicines Agency, included 1.3 million vaccinated individuals as well as 225,000 COVID-19 patients and 4.5 million control participants. The vaccinated participants included 946,000 who received the first dose of the Pfizer-BioNTech vaccine (including 779,000 who received both doses) and 426,000 who received the first dose of the AstraZeneca-Oxford vaccine. The researchers evaluated the risk of blood clotting disorders—including venous thromboembolism (VTE), thrombocytopenia, and thrombocytopenia syndrome (TTS)—following vaccination. Participants who received the Pfizer-BioNTech vaccine had 29% higher occurrence of VTE following the first dose than expected, but there was no significant difference following the second dose. For the AstraZeneca-Oxford vaccine, the researchers did not observe a significant difference in the occurrence of VTE. Notably, the risk of VTE was 8 times higher than expected among COVID-19 patients. Similarly, there was an elevated risk of thrombocytopenia following both doses of the Pfizer-BioNTech vaccine, but not for the AstraZeneca-Oxford vaccine. Neither vaccine exhibited an elevated risk of TTS. The study also provides further analysis of the associated risks by sex and age group; however, the duration was not sufficient to include data regarding clotting risk after the second dose of the AstraZeneca-Oxford vaccine.
MONOCLONAL ANTIBODY The US FDA on July 30 expanded the emergency use authorization (EUA) for the monoclonal antibody REGEN-COV—a combination of casirivimab and imdevimab—to include post-exposure prophylaxis (PEP) among certain people exposed to or at high risk of exposure to an individual infected with SARS-CoV-2. The EUA now allows monoclonal antibody PEP among people at high risk for progression to severe COVID-19, who are not fully vaccinated, or who are not expected to mount an adequate response to vaccination and who have been exposed to a SARS-CoV-2-infected individual or who are at high risk of exposure to an infected individual in congregate or institutional settings such as nursing homes or prisons. Under the EUA, REGEN-COV now can be administered monthly as a subcutaneous injection or intravenous infusion to qualifying people aged 12 and older. The expanded EUA represents the first time an antibody treatment has been authorized for this purpose.
SARS-COV-2 EXPOSURE IN DEER A study conducted by the US Department of Agriculture (USDA) evaluated exposure to SARS-CoV-2 among white-tailed deer in several US states. The USDA’s Animal and Plant Health Inspection Service (APHIS) conducted serological testing on 481 serum specimens collected from white-tailed deer in Illinois, Michigan, New York, and Pennsylvania, from January 2020 through 2021. Antibodies against SARS-CoV-2 were detected in 33% of specimens, including 67% of specimens collected in Michigan. For comparison, only 1 out of 143 specimens collected prior to January 2020 tested positive for SARS-CoV-2 antibodies, and that specimen “was at the minimum threshold of detection,” which could potentially indicate a false-positive result. The researchers did not identify any animals that exhibited signs of illness.
Statements by APHIS note that the study was not sufficient to draw conclusions regarding population-level exposure among deer, but it does provide evidence that deer have been infected by the virus. It is unclear how the animals were exposed or the extent to which the infection is spreading among deer populations. It is also uncertain whether deer can transmit the infection to humans, but information from APHIS indicates there is no evidence that consuming meat from an infected animal could result in SARS-CoV-2 infection. While many questions remain unanswered, this study does provide additional information regarding potential animal reservoirs for SARS-CoV-2, which could potentially impact longer-term epidemic control efforts.
dryrunguy wrote: ↑Tue Aug 03, 2021 7:06 pm
VACCINE-RESISTANT VARIANT RISK With the number of new COVID-19 cases rising in much of the world, scientists are warning that continued transmission provides an opportunity for the evolution of new, and potentially more harmful, SARS-CoV-2 variants. The current increase in cases is being fueled by the highly transmissible Delta variant as well as the loosening and inconsistent use of public health prevention measures, increased social mobility, and inequitable vaccine access, WHO Director-General Dr. Tedros Adhanom Gebreyesus said on July 30, warning that health systems in many countries are overwhelmed and that more variants will emerge as long as the virus continues to spread. US CDC Director Dr. Rochelle Walensky cautioned that a new variant could potentially evade vaccines but added the vaccines authorized in the US continue to protect people from severe disease and death.
Exactly the point for vaccination. Those of us that have done our part may in the end have done very little to stop this thing.
dryrunguy wrote: ↑Tue Aug 03, 2021 7:06 pm
US GLOBAL VACCINATION PROGRAM The US government announced today that the country has donated and shipped more than 110 million doses of SARS-CoV-2 vaccines to more than 60 countries, fulfilling a June pledge by President Joe Biden to donate at least 80 million doses.
For which you will be given zero thanks. You will see.
by ti-amie
by ti-amie
TL;dr
by ti-amie
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The cumulative global COVID-19 incidence surpassed 200 million cases:
1 case to 25 million: 239 days
25 million to 50 million: 69 days
50 million to 75 million: 42 days
75 million to 100 million: 39 days
100 million to 125 million: 58 days
125 million to 150 million: 36 days
150 million to 175 million: 43 days
175 million to 200 million: 53 days
The WHO COVID-19 Dashboard reports 200.8 million cumulative cases and 4.26 million deaths worldwide as of 12:00pm EDT on August 6.
Global Vaccination
The WHO reported 3.98 billion doses of SARS-CoV-2 vaccines administered globally as of August 5. The WHO reports a total of 1.56 billion individuals have received at least 1 dose, and 781 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered approached the record high on August 4, with 43.0 million doses per day*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.30 billion vaccinated individuals worldwide (1+ dose; 29.6% of the global population) and 1.18 billion who are fully vaccinated (15.2% of the global population).
*Over the past several weeks, we have observed a pattern of a sharp decrease in the average doses administered for the most current day. This decrease eventually disappears, which indicates that it is an artifact of reporting. Moving forward, we will attempt to capture the longer-term trends, which may not necessarily align with the most recent update.
UNITED STATES
The US CDC reported 35.4 million cumulative COVID-19 cases and 611,958 deaths. Despite considerable vaccination coverage at the national level, daily incidence continues to accelerate, mirroring the early stages of previous surges. Daily incidence is now up to nearly 90,000 new cases per day, the highest average since February 13. Daily mortality also continues to increase, up to 377 deaths per day, which is more than double the most recent low on July 10 (174)*. It appears that daily mortality may be starting to increase exponentially, but additional data are needed to more fully characterize the longer-term trend.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the current date.
As the current US surge continues, COVID-19 hospitalizations are increasing nationwide. New hospital admissions per day are the highest since February 14 and more than 4 times the most recent low in late June. Several states are setting new records and still increasing, and several others are approaching their current record. Florida is currently reporting 40% higher than its previous highest peak, and Louisiana is reporting 8% higher than its previous record. Numerous states in HHS Region 4 (Southeast) are exhibiting concerning trends in new hospitalizations. In fact, the region as a whole is reporting nearly 80% of its highest peak and increasing rapidly. Nationally, new hospital admissions among children (17 years and younger) are only 13% below the record set in early January and increasing rapidly. Notably, Florida’s new hospitalizations among children are nearly double its previous highest peak in January. Arkansas, Kansas, Maine, Mississippi, Missouri, and Texas also are setting new records for new pediatric hospitalizations, which is particularly concerning as some states begin their school year with in-person learning.
Current COVID-19 hospitalizations also are increasing steadily. The number of currently hospitalized patients has more than tripled from slightly more than 12,000 in late June to nearly 45,000, over only 5 weeks. Similar to new hospitalizations, several states are reporting record high totals, particularly in Region 4. Florida is reporting more than 9,500 hospitalized COVID-19 patients, which is 14% higher than any other day with available CDC data. The earliest data are from August 1, 2020, and Florida’s trend at that time was declining, so it is unclear what the actual peak was during that surge. Louisiana is currently only 4% below its highest peak in January 2021. The current surge is increasing rapidly—much more quickly than in the previous surge—and we expect Louisiana to set a new record in the next several days. As a whole, Region 4 is reporting 65% of its highest peak and increasing rapidly. Hawai’i also is exhibiting a rapid increase in hospitalized COVID-19 patients. It is currently equal to its January 2021 peak, and while it is still 34% lower than its highest peak from August 2020, its trend is accelerating rapidly.
Analysis by The New York Times indicates that every state except Rhode Island is reporting increasing current hospitalizations over the past 2 weeks. Notably, Rhode Island’s COVID-19 hospitalizations have decreased steadily since mid-December 2020. Among the states with increasing trends, 10 have more than doubled over the past 2 weeks, including Alabama (+162%), Louisiana (+156%), and South Carolina (+156%), which have increased by more than 150% over that period. Notably, 6 of the 8 states in Region 4 are reporting biweekly increases greater than 100%. The exceptions are Tennessee and North Carolina, which are reporting +87% and +89%, respectively.
US Vaccination
The US has administered 349 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations are increasing slowly, now up to 582,867 doses per day*. A total of 193.2 million individuals in the US have received at least 1 dose, equivalent to 58.2% of the entire US population. Among adults, 70.4% have received at least 1 dose, as well as 11.3 million adolescents aged 12-17 years. A total of 165.6 million individuals are fully vaccinated, which corresponds to 49.9% of the total population. Approximately 60.8% of adults are fully vaccinated, as well as 8.6 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
PFIZER-BIONTECH VACCINE FULL FDA APPROVAL With the number of new COVID-19 cases surging in the US, the US FDA reportedly has taken an “all-hands-on-deck approach” to reviewing data on Pfizer-BioNTech’s SARS-CoV-2 vaccine, aiming to grant full approval by September 6 or possibly sooner, according to multiple sources familiar with the process. However, some agency and White House officials hope the timetable will be accelerated further, with approval coming as soon as August 15, several sources shared. Speaking at a town hall on July 21, US President Joe Biden said he expects final approval by the fall. Pfizer-BioNTech filed its application for full licensing with the FDA on May 7, and the agency announced the vaccine would undergo priority review on July 16, meaning approval would come no later than January 2022. But it appears the FDA is significantly speeding up that timeline.
Real-world data show that full vaccination dramatically reduces the risk of COVID-19-associated hospitalization or death, but the pace of vaccination has largely stalled in the US, with only about 50% of the total population fully vaccinated and 70% of the adult population having received at least one dose. In an August 4 statement, an FDA spokesperson said the agency’s full approval of SARS-CoV-2 vaccines could engender additional confidence among some people and encourage them to get vaccinated. A June poll by the Kaiser Family Foundation found that 3 in 10 unvaccinated adults said they would be more likely to get vaccinated if one of the vaccines currently being used under emergency use authorization received full approval. Notably, the survey concluded that FDA approval might serve as a proxy for alleviating safety concerns, as many respondents appeared to not understand the regulatory process and two-thirds believed that the vaccines currently available already have full FDA approval or were unsure whether they have full approval. Full licensing of a SARS-CoV-2 vaccine also is expected to spur even more employers to implement vaccine mandates and would provide physicians greater latitude to prescribe additional doses for older adults or people with compromised immune systems.
EMPLOYER VACCINE MANDATES Some of the largest employers in the US recently have announced SARS-CoV-2 vaccination mandates for all or some of their employees amid a surge of COVID-19 cases. The US FDA is expected to fully license the Pfizer-BioNTech vaccine within the next few months, a move that could spark more companies to implement requirements. Tyson Foods, Google, Netflix, Disney, Walmart, Uber, Lyft, Morgan Stanley, The Washington Post, and United Airlines are several of the major companies that are requiring that at least some of their employees be vaccinated, either as a condition of employment or in order to return to corporate office buildings. On August 5, CNN announced it fired 3 employees who violated the company’s policies by returning to the office unvaccinated, one of the first known examples of a major company terminating employment for workers who ignore vaccine mandates.
Reportedly, the Biden administration is considering withholding federal funds from a variety of institutions, including long-term care facilities and universities, in order to encourage more Americans to get vaccinated. The US Equal Employment Opportunity Commission (EEOC) has issued guidance generally permitting employers to institute vaccination mandates in the workplace as long as reasonable accommodations are offered to those with religious beliefs, disabilities, or other conditions that might prohibit vaccination. On July 6, the US Department of Justice published a memorandum explaining that Section 564 of the Food, Drug, and Cosmetic Act, which authorizes the US FDA to issue emergency use authorization (EUA), does not prohibit public and private entities such as businesses and schools from imposing SARS-CoV-2 vaccine requirements. In essence, the regulation permits employers to implement policies requiring vaccination as a condition of employment even when the vaccine is being used under an EUA. Several states have moved to ban future vaccine mandates. As we previously reported, mandatory vaccination requirements twice have been upheld in federal courts. Undoubtedly, additional legal challenges will emerge as more employers, universities, and other entities require proof of vaccination for employees, contractors, and office guests.
NEW YORK CITY VACCINE MANDATE On August 3, New York City Mayor Bill de Blasio announced the Key to NYC Pass program, which requires vaccination for many activities in the city. Starting August 16 (with the program fully implemented by September 13), the program will require individuals to have received at least 1 dose of a SARS-CoV-2 vaccine for indoor dining, indoor fitness facilities, and indoor entertainment venues (eg, theaters, museums). The effort is similar to restrictions implemented in France, but it appears to be the first large-scale program in the US. Last week, Mayor de Blasio announced a vaccine mandate for city employees, which requires weekly testing for unvaccinated personnel.
Notably, Key to NYC Pass does not refer to an actual pass or smartphone application, but rather to the mandate itself. Individuals have the option to use the physical vaccination card issued by the US CDC, the state’s Excelsior Pass app, or the city’s NYC COVID Safe app to provide documentation of vaccination status, but questions remain regarding how businesses are expected to verify vaccination status, particularly regarding how to verify the authenticity of vaccination cards. While both apps also document negative test results, these are not considered a valid substitute for vaccination under the city’s mandate.
US EVICTION MORATORIUM Following the expiration of a federal moratorium on evictions on July 31, the US CDC issued a new temporary moratorium on August 3 that targets areas of “substantial or high [SARS-CoV-2] transmission.” Substantial transmission corresponds to counties with more than 50 new weekly cases per 100,000 population and test positivity of 8% or higher over the past week. Based on the CDC’s COVID-19 risk classification, these counties currently account for approximately 90% of the US population. The new order is scheduled to expire on October 3. The moratorium aims to provide additional time for states to distribute rental assistance funding at a time when the increasing prevalence of the Delta variant is increasing the COVID-19 risk across the country.
As the previous moratorium expired, the White House and the US Congress called on each other to act; however, Congress was unable to agree to a legislative solution, and the White House acknowledged that it did not have the authority to take action. In light of a recent US Supreme Court decision to allow the CDC to extend the previous moratorium through July, in part, due to assurances that it would not be extended further, US President Joe Biden noted that the new moratorium will likely “face obstacles.” In fact, one realtor organization has already filed a lawsuit in federal court, and one local judge has reportedly indicated that he will disregard the order. Even if the moratorium is overturned, President Biden indicated that it could potentially remain in place during the litigation process, which would effectively extend protections for renters.
WHO BOOSTER DOSE MORATORIUM The WHO on August 4 called for a temporary, 2-month moratorium on the administration of “booster,” or third, doses of SARS-CoV-2 vaccines for most people, urging a focus on helping all nations catch up with their vaccination efforts to reach at least 10% of their populations by the end of September. In a briefing, WHO Director-General Dr. Tedros Adhanom Ghebreyesus said, “We cannot—and we should not—accept countries that have already used most of the global supply of vaccines using even more of it, while the world’s most vulnerable people remain unprotected.” Of approximately 4 billion doses administered worldwide, more than 80% have been used in high- or upper-middle-income countries. WHO staff said the science supporting booster doses for the vaccinated general population to enhance immunity is not yet clear, and distinguished those shots from additional doses potentially needed among immunocompromised populations for the development of immunity, which they said should be considered part of the initial series and not a booster. Dr. Tedros called for a moratorium on booster doses through at least the end of September, with the possibility of extension, in order to increase the vaccine supply going to the COVAX facility and encouraged leaders of the Group of 20 countries to make “concrete commitments” to help close the global vaccine gap.
The WHO’s call for a booster moratorium comes as several nations begin or move toward starting such programs. Israel on August 1 began providing third doses to adults over age 60 who are at least 5 months from their second dose, with Prime Minister Naftali Bennett on August 5 warning older Israelis to take extreme caution until they receive the additional shot. In Russia, anyone 6 months post-vaccination can receive an extra dose, and in Hungary, those who are 4 months post-vaccination can get one. Other nations, including Germany, the United Kingdom, and France, are set to roll out additional dose campaigns among various segments of their populations beginning in September. The US FDA is expected to announce a plan for additional doses for all populations by early September, with a plan for immunocompromised individuals possibly coming sooner. Despite the WHO’s calls for a moratorium, most countries appear to be moving ahead with plans for additional doses, claiming they will be able to provide the extra shots and donate millions of doses to low- and middle-income countries. Notably, a WHO internal analysis estimates that if only the 11 wealthier nations planning or expecting to begin additional dose campaigns this year were to provide shots to everyone over age 50, they would use approximately 440 million doses of the already tight global supply. If all high- or upper-middle-income countries began such campaigns, the estimate doubles. With COVAX seeking at least half a billion more vaccine doses to distribute before the year’s end, the onus lies with wealthier countries to fill global vaccination gaps with limited supplies.
VACCINE DIPLOMACY As the Delta variant spreads worldwide, driving up the number of new COVID-19 cases, the US government is under increasing pressure to provide vaccine doses to countries in need. So far, the US has donated more than 110 million doses and plans to donate at least 500 million more. As part of its efforts to improve global vaccine access, the US Department of State is working to support the development of a network of overseas manufacturers to help grow global SARS-CoV-2 vaccine supplies by several billion doses annually. Gayle Smith, US State Department Coordinator for Global COVID-19 Response and Health Security, said she would like to see US vaccine makers—including Moderna, Pfizer, and J&J—support the establishment of low-cost manufacturing facilities and share technological information with other companies to make vaccines available at lower price points.
To this end, the US International Development Finance Corporation has offered US$2 billion to vaccine makers as incentives. So far, agreements have been made with companies in India, South Africa, and Senegal, but these are for companies to “fill and finish” vaccine doses by obtaining large batch ingredients, blending the product, and filling and packaging vials for distribution. One of these companies, South Africa-based Aspen Pharmacare, this week announced it will increase its annual production capacity for the J&J-Janssen vaccine from 300 million to 500 million beginning in January 2022. Some advocates are pushing for the US to pressure pharmaceutical companies to share the technical expertise necessary for overseas companies to produce the vaccines themselves. Notably, the US government retains ownership of one of the main patents used in the Moderna vaccine, but it has not yet charged royalties, giving the government leverage over the manufacturer.
In an effort to counter criticisms it has not done enough to incentivize large pharmaceutical companies to transfer vital technologies, the US—in partnership with nongovernmental organizations and philanthropies—plans to host a high-level leadership summit during next month’s UN General Assembly meeting, with the goal of rallying the international community to increase its pledges for vaccine and public health resources donations. As the US appears to be stepping up its vaccine diplomacy efforts, so does China. Chinese President Xi Jinping on August 5 announced his country hopes to provide 2 billion doses of SARS-CoV-2 vaccines to other countries this year, and will donate US$100 million to the COVAX facility.
MODERNA VACCINE EFFICACY Moderna this week released final analysis of its Phase 3 COVE study data for fully vaccinated individuals at 6 months follow-up. A corresponding preprint published in medRxiv provides details about the study. The placebo-controlled efficacy trial included nearly 45,000 participants aged 16 and older, and roughly 2,250 participants between the ages of 12 and 15. According to the data, the Moderna vaccine’s efficacy after 6 months was 91% among evaluable participants and irrespective of previous SARS-CoV-2 infection. Vaccine efficacy against severe disease was 97%. In South Africa, where the SARS-CoV-2 Beta variant (B.1.351) was dominant during the study, the vaccine efficacy was 100%. However, the study did not evaluate vaccine efficacy against the now widespread Delta variant, and the company acknowledged that additional research is necessary to fully evaluate the vaccine against new variants.
NOVAVAX VACCINE CANDIDATE Novavax issued several statements this week regarding progress on its candidate SARS-CoV-2 vaccine. Novavax has been working on its application to the US FDA seeking emergency use authorization (EUA), but it appears the company will not submit the application until the fourth quarter of 2021. Despite the delay in seeking emergency authorization in the US, Novavax also announced encouraging information on the international front. Novavax submitted applications for emergency use authorization to regulatory authorities in India, Indonesia, and the Philippines, and it expects to submit an application for emergency use listing to the WHO later this month. Reportedly, emergency use applications are expected to be submitted to Australia, Canada, and the UK starting in September. Novavax is partnering with the Serum Institute in India to manufacture its vaccine. Additionally, the company finalized an advance purchase agreement with the European Commission for up to 200 million doses of the vaccine, with an initial commitment of 100 million doses with the option to add an additional 100 million in 2023.
Novavax also announced preliminary results from an ongoing clinical trial of its vaccine, specifically regarding the effect of an additional dose of the vaccine. In the Phase 2 study, participants received a third dose of the vaccine 6 months after the initial 2-dose regimen. According to a press release, the researchers observed “a 4.6-fold increase in...antibody titers” following the third dose. Additionally, the participants exhibited a 6-fold increase in antibodies effective against the Delta variant. The preliminary data suggest that older adults—aged 60-84 years—could exhibit greater benefit from a booster dose compared to younger adults. The statement indicates that complete data will be published to a preprint server and submitted for peer review.
POST-EXPOSURE PROPHYLAXIS A study published this week in the New England Journal of Medicine shows that REGEN-COV—a combination of the monoclonal antibodies casirivimab and imdevimab—reduced the risk of symptomatic COVID-19 disease by 81% among people exposed to a household contact with confirmed SARS-CoV-2 infection. The trial included 1,505 participants, with half assigned to receive REGEN-COV and the other half to placebo. The participants’ mean age was 42.9 years, 45.9% were adolescent boys or men, 9.3% identified as Black, and 40.5% identified as Hispanic or Latinx. Overall, a single 1,200 mg subcutaneous injection of REGEN-COV reduced the risk of symptomatic and asymptomatic infections by 66.4% among household contacts. Additionally, the median time to symptom resolution (1.2 weeks vs 3.2 weeks) and duration of high viral load (0.4 weeks vs 1.3 weeks) were shorter among REGEN-COV recipients who developed symptomatic COVID-19 than for placebo recipients who developed symptomatic COVID-19. The study’s findings were used by the US FDA in its recent revision to REGEN-COV’s emergency use authorization (EUA), which expanded emergency use for the drug as post-exposure prophylaxis (PEP) for COVID-19 in high-risk adults and pediatric individuals. REGEN-COV remains authorized for the treatment of mild-to-moderate COVID-19 among adults and pediatric patients who are at high risk for progression to severe COVID-19.
LONG COVID/PASC IN CHILDREN According to a study published in The Lancet Child & Adolescent Health, so-called “long COVID,” or post-acute sequelae of COVID-19 (PASC), is rare among children, with most children fully recovering from SARS-CoV-2 infection after 8 weeks. British researchers aimed to determine illness duration and symptoms among UK school-aged children who reported data, through adult proxies, to the COVID Symptom Study. The researchers included data from 1,734 children aged 5 to 17 years who tested positive for SARS-CoV-2, with case control matches who reported information to the database but who tested negative for the virus. Of these children, the most common symptoms were headache (62.2%) and fatigue (55%) and illness duration lasted approximately 6 days. Only 25 (1.8%) of 1,379 children who tested positive experienced symptoms for at least 56 days, with a significant regression in symptoms within the first 28 days. Notably, the data showed that while only 0.9% of the children who tested negative had symptoms lingering for 28 or more days, this control group had more symptoms (median: 9) during the first 28 days and in the few in whom symptoms persisted beyond 28 days (median: 5). While the study’s findings suggest that long-lasting symptoms are rare among children diagnosed with COVID-19, the researchers emphasized the importance of following any child with prolonged illness, whether from SARS-CoV-2 infection or another illness.
VACCINATION FOR PREGNANT WOMEN On August 3, the UK government initiated a study to determine the most beneficial dose schedule for SARS-CoV-2 vaccination in pregnant women. The study will include 600 pregnant women who will be vaccinated using either the Pfizer-BioNTech or Moderna vaccines. The women will receive the 2 doses of these vaccines either 4-6 weeks apart or 8-12 weeks apart in order to determine the best interval. Researchers will analyze blood specimens from each participant collected over 9 follow-up visits as well as a single blood specimen from the newborn and from breast milk. While pregnant women in the UK, US, and other countries are already being vaccinated, this study aims to provide further insight into the immune response in pregnant women and their newborns.
“DELTA PLUS” VARIANT As the prevalence of the Delta SARS-CoV-2 variant of concern (VOC) continues to increase around the world, there are emerging reports of infections caused by a sub-lineage of the Delta variant that includes an additional mutation. The subvariant is being widely referred to as “Delta Plus”; however, this appears to be an informal designation, as there is not yet a mention of that term on the WHO or US CDC VOC websites. India designated Delta Plus as a VOC in late June. Delta Plus refers to the B.1.617.2.1 (or AY.1) variant—a subset of the Delta variant B.1.617.2—which includes an additional mutation (K417N) to the spike protein that is not present in the original Delta variant. The K417N mutation also is present in the Beta variant, and it is believed to help the virus evade immune response, including reduced susceptibility to some monoclonal antibody treatments. The Outbreak.info variant tracker reports more than 450 cases involving the Delta Plus variant across at least 30 countries.
In June, Public Health England was among the first to document the K417N mutation in the Delta variant. Information from the Indian Ministry of Health and Welfare indicates that the Delta Plus variant exhibits “increased transmissibility, stronger binding to receptors of lung cells, [and] potential reduction in monoclonal antibody response.” But while the “plus” seems to imply that the variant is more dangerous, it is not yet clear how much it differs from the main Delta variant. As the pandemic continues, new variants will continue to emerge, which could include further evolution of VOCs that possibly result in increased transmissibility, disease severity, and resistance to treatments or vaccines. Genomic surveillance is critical to rapidly identifying and characterizing these variants before they spread widely.
by ponchi101 My sister has an alum over the web that is Chinese. In China, you are not allowed NOT to be vaccinated. That simple.
How terrible that it takes a dictatorship to get things done.
by Suliso
by ti-amie Apparently the first tweet is from a former PM of Australia.
by ti-amie
by MJ2004Trump was vaccinated.
by Ribbons Applicable to more than epidemiology . . .
by ti-amie I was asking myself, after seeing the tweet about how stupid you have to be to let people who have been vaccinated tell you not to be and you believe them, if a lot of this is performative? There are lots of out of work actors, there always are, and how many, for a grand, will stand on a corner or attend a presser and scream a bunch of crap they don't mean at all? It was recently confirmed that a lot of the folks cheering tfg when he announced his candidacy were actors. That makes this even more vile if it's true. Too bad we don't have real reporters like there were back in the day.
by ti-amie And then I see this. A movie is now a source for medical information? Really?
by Suliso
ti-amie wrote: ↑Mon Aug 09, 2021 6:56 pm
I was asking myself, after seeing the tweet about how stupid you have to be to let people who have been vaccinated tell you not to be and you believe them, if a lot of this is performative? There are lots of out of work actors, there always are, and how many, for a grand, will stand on a corner or attend a presser and scream a bunch of crap they don't mean at all? It was recently confirmed that a lot of the folks cheering tfg when he announced his candidacy were actors. That makes this even more vile if it's true. Too bad we don't have real reporters like there were back in the day.
If only it was so simple... Unfortunately I also have a couple of antivaxxers among my relatives/acquaintances. Not maybe the complete flat earthers, but still.
ti-amie wrote: ↑Mon Aug 09, 2021 6:56 pm
I was asking myself, after seeing the tweet about how stupid you have to be to let people who have been vaccinated tell you not to be and you believe them, if a lot of this is performative? There are lots of out of work actors, there always are, and how many, for a grand, will stand on a corner or attend a presser and scream a bunch of crap they don't mean at all? It was recently confirmed that a lot of the folks cheering tfg when he announced his candidacy were actors. That makes this even more vile if it's true. Too bad we don't have real reporters like there were back in the day.
If only it was so simple... Unfortunately I also have a couple of antivaxxers among my relatives/acquaintances. Not maybe the complete flat earthers, but still.
Do you think if it was proved that the folks saying this are being paid it would make a difference to them?
by Suliso You'd be unable to convince them of that being the case. They'll just say it's all lies, big government, big pharma blah, blah, blah...
by ti-amie
Suliso wrote: ↑Mon Aug 09, 2021 7:29 pm
You'd be unable to convince them of that being the case. They'll just say it's all lies, big government, big pharma blah, blah, blah...
Leon (Tallahassee) and Alachua (Gainesville) counties are defying DeSantis no mask mandate. Think Miami is doing the same. Hillsborough County (Tampa) says masks are required but parents can opt out. Haven't heard a peep from DeSantis since this.
by dryrunguy Here's the latest Situation Report. DeSantis is a jackass.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 202.6 million cumulative cases and 4.29 million deaths worldwide as of 1:00pm EDT on August 9. The global weekly incidence increased for the seventh consecutive week. Last week’s total is 3.3% higher than the previous week, but it appears as though case counts may have passed an inflection point and could be approaching a peak or plateau. Global weekly mortality increased again as well, up 1.3% compared to the previous week. Overall, the trend has increased steadily for 5 consecutive weeks, with the exception of a spike during the week of July 19, which was the result of 8,786 deaths reported by Ecuador on July 21.
Global Vaccination
The WHO reported 4.03 billion doses of SARS-CoV-2 vaccines administered globally as of August 9. The WHO reports that a total of 1.59 billion individuals have received at least 1 dose, and 798 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered has leveled off at approximately 41 million doses per day*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.35 billion vaccinated individuals worldwide (1+ dose; 30.2% of the global population) and 1.22 billion who are fully vaccinated (15.6% of the global population).
*Average doses administered is exhibiting a sharp decrease for the most recent several days, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reported 35.8 million cumulative COVID-19 cases and 614,856 deaths. On August 5, the US surpassed 100,000 new cases per day for the first time since February 10. The current average of 102,413 is nearly 9 times the most recent low—11,486 on June 19—and still increasing rapidly. Daily mortality appears to continue its exponential increase up to 457 deaths per day. This is the highest average since May 27, and it is an increase of 46% over the past week and 79% over the past 2 weeks*
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent dates.
Florida in #1 nationally in terms of both total weekly incidence and mortality, representing 22% and 25% of the national total, respectively. Florida is also #1 nationally in terms of per capita weekly incidence with 733 new cases per 100,000 population, 3.5 times the national average (205). Arkansas is #1 in terms of per capita weekly mortality with 4.8 deaths per 100,000 population, nearly 5 times the national average (1.0).
US Vaccination
On August 4, the US surpassed 350 million cumulative doses of SARS-CoV-2 vaccines administered. The current cumulative total is 351.9 million. Daily vaccinations continue to increase slowly, now up to 608,654 doses per day*. The US also surpassed 50% of the total population fully vaccinated. A total of 195.2 million individuals in the US have received at least 1 dose, equivalent to 58.8% of the entire US population. Among adults, 71.1% have received at least 1 dose, as well as 11.7 million adolescents aged 12-17 years. A total of 166.7 million individuals are fully vaccinated, which corresponds to 50.2% of the total population. Approximately 61.1% of adults are fully vaccinated, as well as 8.8 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US SURGE The US continues to face a COVID-19 surge, with the most severe burden faced by states in the South and Southeast regions of the country. The national biweekly relative change peaked at more than +160% in late July—the largest relative increase since the initial surge in March/April 2020—but a slight decrease to +119% indicates that the increase is beginning to taper off.
While full vaccination coverage has surpassed 50% nationally, major disparities remain at the state level. Analysis by The Wall Street Journal found that all 12 states that are reporting per capita hospitalizations greater than the national average have full vaccination coverage below the national average. Additionally, all 20 states with full vaccination coverage higher than the national average are reporting per capita hospitalizations below the national average. At the local level, counties with the lowest vaccination coverage also are experiencing much larger surges in mortality, compared to counties with higher vaccination coverage. These statistics illustrate that low vaccination coverage is a driver of the ongoing surge in severely affected states and that the vaccines are providing protection against severe disease, hospitalization, and death.
In severely affected cities and states, the surge is placing a major burden on health systems. In some instances, the current surge is as severe or worse than the United States’ largest surge in January 2021. Hospitals in Houston, Texas, and Orange County, California, are reporting increased wait times for ambulances to drop off patients at emergency departments (ED). Hospitals in some parts of the country faced similar challenges during the January 2021 surge. Texas Governor Greg Abbott issued a statement to the Texas Hospital Association encouraging hospitals to “voluntarily postpone [some] medical procedures” in order to ensure sufficient capacity is available to treat COVID-19 patients, but at least 1 hospital in Houston is already preparing an emergency tent to handle overflow COVID-19 patients.
As schools resume classes, some school districts in states that have banned mask mandates are pushing back against state-level legislation and policies. In Texas, the Dallas Independent School District (ISD), the second-largest in the state, announced it will temporarily require masks for students, employees, and visitors during the surge, defying Governor Abbott’s statewide ban. Reportedly, the Houston ISD is expected to vote on a similar mandate this week. In Florida, Governor Ron Desantis threatened to withhold pay for school administrators that institute mask mandates during the state’s most severe surge to date, including a record high for pediatric hospital admissions.
US MILITARY VACCINE MANDATE SARS-CoV-2 vaccination will be mandatory for all 1.3 million members of the US Armed Forces no later than mid-September, or as soon as the US FDA fully licenses a vaccine, “whichever comes first,” US Secretary of Defense Lloyd J. Austin III said in an August 9 message to all troops. Secretary Austin implored all US Department of Defense (DOD) military, civilian, and contractor personnel to get vaccinated, regardless of a mandate. US President Joe Biden strongly supports the plan and is prepared to issue a waiver to make the shots mandatory if the FDA’s expected timeline for approval of the Pfizer-BioNTech moves past early-September. In a statement, President Biden said vaccinations “will enable our service members to stay healthy, to better protect their families, and to ensure that our force is ready to operate anywhere in the world,” calling out the Delta variant as a threat to unvaccinated populations. In a related memo, Chairman of the Joint Chiefs General Mark Milley called COVID-19 “a threat to force protection and readiness” and reminded troops that vaccine mandates in the military are common. About 73% of active-duty US service members have received at least one SARS-CoV-2 vaccine dose, according to the Pentagon. But without more members fully vaccinated, the military faces challenges in deploying unvaccinated troops to countries that have strict local rules, and an increase in cases among its ranks could harm military readiness. Secretary Austin added that if COVID-19 incidence increases among military personnel, he could act sooner or recommend a different course of action to President Biden. Earlier this month, the DOD recommended an immediate waiver to institute a mandate before FDA approval, but White House officials urged caution and settled on the current plan.
J&J-JANSSEN VACCINE EFFECTIVENESS Researchers leading the Sisonke clinical trial in South Africa on August 6 presented data showing the J&J-Janssen SARS-CoV-2 single-shot vaccine is highly effective in preventing severe disease and death from COVID-19 among healthcare workers. The Phase 3b study enrolled 477,234 healthcare workers at 122 sites throughout South Africa, administering the J&J-Janssen vaccine between February and May 2021. Data collection ran through July 17, and researchers will continue to monitor participants for another 2 years. Overall, the J&J-Janssen vaccine provided 91-96.2% protection against death from both the Beta and Delta SARS-CoV-2 variants. When the Beta variant was dominant, the vaccine offered 67% protection from hospitalization, and 71% protection against hospitalization when the Delta variant became dominant. When breakthrough cases occurred, healthcare workers experienced mild symptoms and less than 0.05% of those cases resulted in severe disease or death. Two cases of rare blood clots occurred among participants, but both fully recovered.
The data have not yet been peer reviewed nor published in a scientific journal, but they should alleviate some concerns over the J&J-Janssen vaccine’s effectiveness. Some previous studies suggest the vaccine might not be as effective against the Delta variant, leading some people to seek out an additional vaccine dose; however, the researchers concluded additional doses are not warranted at this time based on the data. J&J-Janssen is expected to release results of a trial evaluating a 2-dose regimen in the coming weeks. South Africa granted conditional approval to the J&J-Janssen vaccine in April, and so far has administered more than 1.85 million doses. The country also uses the Pfizer-BioNTech vaccine and has administered more than 6.77 million doses of that vaccine.
REINFECTION AFTER VACCINATION Among people previously infected with SARS-CoV-2, full vaccination provides additional protection from reinfection, according to an early release study published last week in the US CDC’s MMWR. The findings from the retrospective, case-control study underscore the CDC’s recommendation that all eligible individuals receive a SARS-CoV-2 vaccine. Using several databases, researchers identified 246 case-patients, all adult and Kentucky (US) residents with laboratory-confirmed SARS-CoV-2 infection in 2020 and a subsequent positive nucleic acid amplification test or antigen test result between May 1 and June 30, 2021. They also identified 492 control participants, who were adult Kentucky residents matched on a 1:2 ratio based on sex, age, and date of initial positive SARS-CoV-2 test but who did not have evidence of reinfection during those 2 months in 2021. Notably, the data were collected prior to the Delta variant becoming dominant in the US. Among the case-patients, 20.3% were fully vaccinated, compared with 34.3% of the control participants. Unvaccinated Kentucky residents who were previously infected with SARS-CoV-2 had 2.34 times the odds of reinfection (95% confidence interval [CI]=1.58-3.47) when compared with those who were previously infected but also fully vaccinated. Partial vaccination was not significantly associated with reinfection (odds ratio=1.56; 95% CI=0.81-3.01), according to the researchers. They warned that little is known about the durability of natural immunity after initial infection and noted the study suggests that vaccination offers better protection than the natural immunity developed post-acute infection for people who have recovered from SARS-CoV-2 infection.
COUNTERFEIT VACCINATION CARDS As more employers, universities, and venues in the US and Europe implement vaccine mandates, officials are warning of a rise in fake SARS-CoV-2 vaccination certificates. According to investigators and cybersecurity experts, the past few weeks have seen a number of ways to purchase counterfeit vaccine cards on social media, messaging apps, and the dark web. While the European Union has a digital vaccine passport system that assigns a unique QR code to each individual, the US relies on paper cards distributed by the US CDC, which are easy to forge and were never intended to be used as proof of vaccination. Some US states are working to implement digital verification systems, but other states have outlawed the use of such systems or implemented punishments for businesses and other entities that ask for proof of vaccination.
The ease with which US vaccination cards can be forged is alarming both faculty and students at universities and colleges heading back to in-person learning this fall. According to an estimate from the Chronicle of Higher Education, at least 675 colleges and universities now require proof of SARS-CoV-2 vaccination. Many university administrators face challenges in identifying fake vaccination cards digitally uploaded to students’ online portals. The proliferation of counterfeit vaccination cards prompted the US Federal Bureau of Investigation and the US Department of Health and Human Services Office of the Inspector General to issue a statement earlier this year warning the public that buying, creating, or selling fabricated cards is a federal offense. For people in the US with a valid vaccination certificate, there are several options to store the oddly sized CDC card digitally on a smartphone.
UNAUTHORIZED THIRD VACCINE DOSES In the US, the federal government is expected to release a plan for third SARS-CoV-2 vaccine doses in the coming weeks. In the meantime, there seems to be a growing divide between near-stagnant vaccine hesitancy and people seeking unauthorized additional shots, the latter underlining a heightened anxiety over the Delta variant’s spread. According to reports, some people who received the J&J-Janssen vaccine have received additional doses of another authorized vaccine over fears the single-shot dose might not be as effective as others. And it appears some are going to great lengths to obtain extra doses by falsifying vaccine certificates, lying about their name or health insurance status, or traveling to other cities or states. Most experts stress that further research is warranted to determine the safety and efficacy of second or third doses and whether combining doses of various vaccines will provide substantial protection.
But as the Delta variant continues to drive up the number of new COVID-19 cases worldwide, calls for so-called “booster” doses are highlighting global inequities in vaccine access, as wealthier nations with ample vaccine supplies begin to recommend additional doses for some populations while low- and middle-income countries (LMICs) struggle to obtain sufficient supplies to vaccinate even small proportions of their populations. Worldwide, public health experts, international organizations, and ethicists caution countries against offering booster doses until more data become available and to shore up supplies in LMICs. The WHO last week called for a moratorium on offering additional doses for most people, but it appears several nations—including Israel, Germany, France, the UK, and Russia—will move ahead with plans to offer booster shots to some populations.
HEART INFLAMMATION FOLLOWING VACCINATION In a research letter published in the peer-reviewed journal JAMA, researchers examined the clinical records of more than 2 million patients who received at least 1 dose of SARS-CoV-2 vaccination within the Providence Health Care System or recorded through state registries in Washington, Oregon, Montana, and Los Angeles County, California (US) in order to identify post-vaccination cases of myocarditis (heart muscle inflammation) and pericarditis (heart membrane inflammation). Of these individuals, 76.5% received more than 1 vaccine dose, 52.6% received the Pfizer-BioNTech vaccine, 44.1% received Moderna, and 3.1% received J&J-Janssen. Overall, 20 individuals had vaccine-related myocarditis (1.0 [95% confidence interval (CI), 0.61-1.54] per 100,000) and 37 had pericarditis (1.8 [95% CI, 1.30-2.55] per 100,000). Of the cases of myocarditis, 75% occurred in males with a median age of 36, happened on average 3.5 days after vaccination, and resulted in hospitalization in 19 of 20 cases. No mortality was reported, and most patients were discharged after approximately 2 days. Of the pericarditis cases, 73% occurred in males with a median age of 59, happened on average 20 days after vaccination, and resulted in hospitalization in 13 of 37 cases. No mortality was reported, and most patients were discharged after approximately 1 day. Notably, the incidence of myocarditis following SARS-CoV-2 vaccination described in the study—10 per million—is higher than the US CDC’s estimate of 4.8 cases per million, suggesting an underreporting of cases to federal databases. The researchers stressed that the hospitalizations resulting from heart inflammation in the study were unremarkable and cautioned that COVID-19-related heart inflammation is much more common. Overall, vaccination remains the most important tool for protecting individuals from severe symptoms of COVID-19.
COVID-19 TREATMENT RESEARCH Research efforts to find treatments for people with mild-to-severe COVID-19 are underway worldwide. The WHO last week announced it is restarting the Solidarity clinical trial—now dubbed SolidarityPlus—to test 3 repurposed drugs in hospitalized COVID-19 patients: the cancer chemotherapy drug imatinib, a chimeric monoclonal antibody called infliximab that is used to treat several autoimmune diseases, and the antimalarial drug artesunate. The first patients are expected to be enrolled soon in Finland, and 40 other countries are in the process of gaining regulatory and institutional review board approvals. The original Solidarity trial began in March 2020, but in October 2020 researchers published interim results showing no benefit for 4 repurposed drugs—remdesivir, hydroxychloroquine, lopinavir, and interferon beta-1a—in hospitalized COVID-19 patients. An independent expert committee chose the 3 new medications at the beginning of this year, but delays due to negotiations with drug manufacturers, as well as regulatory and ethical approval processes, held up the trial’s restart until now.
In the US, the Duke Clinical Research Institute announced the expansion of a clinical trial testing repurposed medications among people with mild-to-moderate COVID-19 who are recovering at home. Part of the National Institutes of Health (NIH)-funded Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) initiative, the ACTIV-6 study is now testing 3 drugs that are FDA-approved for other conditions—the antiparasitic ivermectin, the inhaled steroid fluticasone, and the selective serotonin reuptake inhibitor fluvoxamine—and expects to add other medications over time. The study is recruiting participants ages 30 and older who recently tested positive for SARS-CoV-2 and are experiencing at least 2 COVID-19 symptoms. Notably, the study is completely remote, meaning people recovering from COVID-19 at home can participate from anywhere in the US and do not need to leave their homes while isolating to obtain medication or visit clinics. With only a handful of medications approved or authorized to treat COVID-19, researchers are hopeful these trials can help broaden the tools available to lower the risk of complications, shorten the time of symptoms, or prevent progression to more severe disease.
US/CANADA TRAVEL RESTRICTIONS On August 9, Canada lifted some travel restrictions for fully vaccinated US citizens and permanent residents. However, prospective travelers must adhere to certain pandemic safety standards before being allowed to cross the border. In order to enter Canada, Americans must show proof of a full SARS-CoV-2 vaccine regimen completed at least 14 days prior, a negative molecular SARS-CoV-2 test taken within 3 days of travel regardless of individual vaccine status, and an in-country, 14-day quarantine plan in case symptoms develop. They must also fill out a detailed application on the country’s arriveCAN app before crossing the border. Canadian authorities have issued warnings to prospective travelers that longer wait times can be expected at border crossings. Canada plans to open its borders to visitors from other countries beginning next month, depending on conditions. The US government recently announced plans to extend its border closures with Canada and Mexico for all nonessential travel until at least August 21, but a plan for a phased reopening of the borders is being formulated, according to officials.
CRUISE LINES & VACCINATION Norwegian Cruise Lines can require passengers to show proof of SARS-CoV-2 vaccination before boarding any of its ships based in Florida, despite that state’s law banning so-called “vaccine passports,” a US District Court judge has ruled. The law, signed by Florida Governor Ron DeSantis in May, fines businesses $5,000 per violation for asking customers to prove they have been vaccinated against SARS-CoV-2. But in an August 8 preliminary ruling, US District Court Judge Kathleen M. Williams of the Southern District of Florida said Norwegian likely will prevail in arguing that the law risks public health and qualifies as an unconstitutional infringement on the company’s First Amendment rights. While Norwegian “has demonstrated that public health will be jeopardized if it is required to suspend its vaccination requirement,” Judge Williams wrote, the “defendant fails to articulate or provide any evidence of harms that the state would suffer if an injunction was entered.” The injunction blocks the state government from enforcing the law against Norwegian, which is scheduled to resume port activity on August 15. In a statement, Norwegian said the order will allow it “to operate in the safest way possible with 100% vaccination* of all guests and crew when sailing from Florida ports.” On August 9, Governor DeSantis said Florida will appeal the ruling to the Eleventh Circuit Court of Appeals.
Cruise ship operators are working to keep up with rapidly changing guidelines as the highly transmissible Delta variant drives an increase in COVID-19 case numbers nationwide, particularly in Florida, where many ships embark. While most cruise lines are requiring passengers to show proof of vaccination, some are adding requirements including proof of a negative SARS-CoV-2 test before boarding and masking in crowded indoor spaces. For all cruise ships operating in US waters, or seeking to operate in US waters, the US CDC has devised a Framework for Conditional Sailing Order (CSO) and Technical Instructions that ships are recommended to follow even when located outside of US waters, as well as a color-coded system for ships. Of the 65 cruise ships listed, 25 are categorized as orange or yellow as of August 9, indicating that those ships have reported COVID-19 cases and the CDC is either monitoring the situation, actively investigating an outbreak, or has concluded its investigation and continues to monitor. The remainder of the listed ships are operating under a green status, meaning they have not reported any COVID-19 cases or COVID-19-like illnesses. If a ship reaches red status, it has been determined through investigation to be “at or above” the threshold for passenger and crew cases and must return immediately to port or delay its next voyage. Notably, cruise lines must report all information on COVID-19 cases aboard ships to the CDC. If a cruise operator chooses not to follow the CSO—which became voluntary under a court order issued in June—the ships are marked as gray but are still required to report cases of illnesses or death due to other causes.
*In a footnote on its release, Norwegian indicated “limited exceptions” for vaccination requirements may be made due to “valid medical or religious exemptions.” Under the CDC’s CSO, 95% of crew and guests must be vaccinated.
by ponchi101 You don't need to "find them". When you get the virus and you end up in the ICU, THEY will find you. If you are lucky.
by ti-amie Isn't Mississippi one of the states screaming about secession? I think Biden is being smart here. You can't let people die due to lack of Federal assistance (unless you're in the GQP) and a not so subtle message is being sent about who is helping.
Simply, WOW! So many a******s in the world with anger issues. Scary.
by ti-amie
by dryrunguy Here's the latest Situation Report. It's packed. The section focused on Senegal was... tough to read.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 204.6 million cumulative cases and 4.32 million deaths worldwide as of 12:15pm EDT on August 12.
Global Vaccination
The WHO reported 4.43 billion doses of SARS-CoV-2 vaccines administered globally as of August 12. The WHO reports that a total of 1.70 billion individuals have received at least 1 dose, and 866 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered has declined steadily from its second-highest peak—43.3 million doses per day—down to 35.9 million*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.40 billion vaccinated individuals worldwide (1+ dose; 30.8% of the global population) and 1.26 billion who are fully vaccinated (16.1% of the global population).
*Average doses administered is exhibiting a sharp decrease for the most recent several days, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent data.
As national SARS-CoV-2 vaccination campaigns continue, some new countries are emerging as successes, while some that were among the top countries earlier in the year have tapered off. This week, we will compare trends among the top countries in terms of full vaccination over the past several months**.
Top 10 as of August 12
1. Malta- 91%
2. Iceland- 75%
3. UAE- 73%
4. San Marino- 70%
5. Seychelles- 70%
6. Uruguay- 68%
7. Singapore- 68%
8. Chile- 67%
9. Nauru- 67%
10. Belgium- 65%
Among these countries, only 4 have remained in the top 10 since May: Chile, Malta, San Marino, and Seychelles. The UAE was only outside the top 10 in June, but this was likely a result of no updated data between April 20 and July 5. While Malta has remained among the top countries over this period, it climbed steadily through the rankings, up from #9 in May to #1 in August. Iceland also quickly rose through the rankings, from nearly 10 percentage points (pp) outside the top 10 in May to #2 globally in August. Seychelles’ vaccination coverage increased rapidly through the end of April, but progress has slowed considerably since then, causing it to fall from #1 to #5 since May. Interestingly, Qatar was not in the top 10 at any of the dates included in this analysis, but it was consistently close, ranking #12 in May and #11 from June through August.
In May, there was a gap of approximately 20pp between Seychelles and Israel and the rest of the top 10 countries—from #3 UAE at 39% to #2 Israel at 59%—but that gap closed over the past several months. Israel was #1 globally through late April, but after reaching 58% by the end of that month, its coverage increased by fewer than 5pp since then, with most of that occurring since mid-July. By virtue of initiating vaccination earlier than most countries, the US was among the top 3 globally through early March, but as progress slowed, it fell to #7 in May and #10 in June before falling outside the top 10 in July. Similar to the US, slowing progress in the UK following steady progress earlier in the year caused it to fall out of the top 10 between June and July. Bahrain and Hungary have exhibited similar trends.
In July, Singapore was 15pp outside the top 10, but rapid progress resulted in an increase in coverage of nearly 30pp in just a month—from 40% to 68%—propelling Singapore to #7 in August. Similarly, Nauru reported a rapid increase between July and August, climbing from just 17% coverage on June 29 (its earliest available data) to 67% on July 27 (its most recent data), good enough for #9 globally in August. After a relatively slow start, Belgium’s vaccination coverage increased rapidly starting in early May, outpacing the European average and moving the country up to #10 globally. Among the countries currently in the top 10, Uruguay and Mongolia initiated vaccination efforts later than most others, with less than 1% coverage reported on March 30 and April 22, respectively. Both countries exhibited rapid progress, however, and have been among the global top 10 since June.
**Data and rankings correspond to the 12th of each month, unless noted otherwise.
UNITED STATES
The US CDC reported 36.3 million cumulative COVID-19 cases and 617,096 deaths. The current average of 114,190 new cases per day is the highest since February 6 and nearly 10 times the most recent low—11,606 on June 19. It appears as though the US may be passing an inflection point, but it is difficult to determine whether this is an artifact of reporting frequency or an early indication of a longer-term trend. Daily mortality appears to continue its exponential increase up to 492 deaths per day, the highest average since May 22*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 353.9 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to increase steadily, up to 640,617 doses per day*. A total of 196.5 million individuals in the US have received at least 1 dose, equivalent to 59.2% of the entire US population. Among adults, 71.5% have received at least 1 dose, as well as 11.9 million adolescents aged 12-17 years. A total of 167.4 million individuals are fully vaccinated, which corresponds to 50.4% of the total population. Approximately 61.3% of adults are fully vaccinated, as well as 8.9 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
THIRD DOSE AMONG IMMUNOCOMPROMISED The US FDA on August 12 authorized the administration of an additional dose of SARS-CoV-2 mRNA vaccines for certain people with compromised immune systems, “specifically, solid organ transplant recipients or those who are diagnosed with conditions that are considered to have an equivalent level of immunocompromise.” The FDA amended the emergency use authorizations (EUAs) for both the Pfizer-BioNTech and Moderna vaccines to allow for a third dose for this population, which is estimated to be about 2.7% of the US adult population. Several studies, including one published this week in the New England Journal of Medicine, show that immunocompromised people experience a significant increase in their immune response after a third dose of vaccine. The agency noted that other fully vaccinated people do not need an additional dose at this time, but several US health officials believe extra doses might be needed in the future. According to the FDA, the EUA for the J&J-Janssen vaccine was not updated because there is not yet sufficient evidence to support additional doses in any population.
The US CDC’s Advisory Committee on Immunization Practices (ACIP) is meeting today to further discuss and vote on clinical recommendations regarding who will be eligible for extra shots and how they will be administered, with CDC Director Dr. Rochelle Walensky expected to sign off on any decisions later in the day. The ACIP also is expected to discuss what type of evidence is needed to inform a decision about whether additional vaccine doses are needed for a larger portion of the population and, if so, which populations should get them first.
US SURGE The US COVID-19 surge continues, its second largest to date, and concerns are growing regarding the impact on health systems and schools. Analysis from The Washington Post illustrates a close correlation between low vaccination coverage and elevated SARS-CoV-2 transmission, with the vast majority of hotspot areas located in counties with full vaccination coverage less than 40%, including much of the South and Southeast regions, and relatively few in counties with moderate or high coverage. Even as the surge grows, some state lawmakers are continuing efforts to curb the authority of local governments and health officials. In Tennessee, all 73 Republican members of the state House of Representatives called for a special legislative session in order to pass measures that would limit local officials’ ability to implement COVID-19 protective measures such as mask mandates.
In severely affected areas, hospitals are being forced to implement emergency plans to manage the influx of COVID-19 patients. In Florida, which represents 22% of the national daily incidence, state health officials requested 200 ventilators and 100 high-flow nasal cannula kits from the federal Strategic National Stockpile (SNS). The state is not yet experiencing a shortage of this equipment, but statewide hospitalizations continue to set new records. Reportedly, officials in Brevard County, Florida, are emphasizing that the 9-1-1 telephone number should be used only for emergencies and encouraging residents to seek care through other means for less urgent conditions in order to reduce the burden on ambulance services and emergency departments. Despite having the country’s largest surge, Florida Governor Ron DeSantis continues to resist protective measures, including mask mandates, to slow transmission. Rather, he touted a state plan to expand infusion centers for monoclonal antibody treatments to mitigate the impact on hospitals. Notably, these treatments require a prescription and could cost thousands of dollars, whereas mask use is relatively inexpensive and vaccination is provided free of charge.
Daily incidence among children continues to increase, setting new records nationally and in severely affected states. In Mississippi, one school district—notably, with no mask mandate—is transitioning to virtual learning only 1 week into the school year, after 40% of students at one high school were required to quarantine. As of August 12, at least 10 cohorts of students at the high school are under quarantine, but the school elected to resume in-person classes and continue quarantining students following exposures prior to the district order to go virtual beginning August 16.
VACCINE MANDATES FOR PUBLIC SCHOOL STAFF California (US) Governor Gavin Newsom on August 11 announced the state will require all teachers and school staff to show proof of SARS-CoV-2 vaccination or undergo weekly testing. The move—which applies to more than 800,000 employees, including about 320,000 public school teachers and many other support and administrative staff—comes after several large state school districts (San Jose Unified, San Francisco Unified, Sacramento City Unified, and Long Beach Unified) announced similar requirements for their employees. The state’s 2 major teachers unions—the California Teachers Association and the California Federation of Teachers—among other unions, support the plan, citing state and national data showing that nearly 90% of educators have been vaccinated. There is debate over whether California is the first state with such a requirement for public school employees, as Hawai’i Governor David Ige last week announced his intention to require vaccinations for all public sector workers, including school staff. However, several public workers unions, including those representing teachers, pushed back on the announcement, saying they were not consulted and arguing there is no detailed plan on implementation.
Over the weekend, Randi Weingarten, President of the American Federation of Teachers, announced support for vaccine mandates for educators as the first line of prevention for unvaccinated, younger students as they return to in-person learning, saying mask wearing is the second most important factor for keeping kids in school. Weingarten cited an increasing number of new COVID-19 cases among children over the past few weeks, as compiled by the American Academy of Pediatrics (AAP). Last week, Becky Pringle, President of the National Education Association, the largest teachers union in the US, said vaccine and mask mandates should be decided on local levels. In an interview on August 10, Dr. Anthony Fauci, Chief Medical Adviser to the President, voiced support for vaccination mandates for public school employees, saying vaccination of all eligible adults would help children more safely return to classrooms this fall. In most states, there are laws dictating vaccination requirements for school children but, to our knowledge, none requiring teachers and school staff workers to undergo immunizations. Some states provide public school employees a list of recommended vaccines—such as those for diphtheria, tetanus and pertussis (DTaP); influenza; and measles, mumps and rubella (MMR)—but there is no requirement or follow-up.
Much of the urgency over vaccinating public school employees centers on the fact that children under the age of 12 remain ineligible for vaccination in the US. In a letter sent last week to the US FDA, AAP President Lee Savio Beers urged the agency to fast-track vaccine authorization for this age group, saying the Delta variant “changes the risk-benefit analysis.” In May, the FDA authorized the emergency use of the Pfizer-BioNTech vaccine for young people aged 12 to 15 years, but the companies have not yet applied for authorization among children aged 5 to 11 years. A Pfizer spokesperson said the company plans to submit an emergency use authorization (EUA) application for that age group by the end of September. For now, the timeline for a vaccine EUA for school-aged children is amorphous, but experts remain hopeful that authorization and recommendations could still come before the end of the year.
COVID-19 AMONG CHILDREN Public health experts, state officials, and healthcare providers are warning about a surge in COVID-19-related hospitalizations among children and cautioning that the Delta variant could be more dangerous for younger individuals. As of August 10, US hospitals admitted an average of 246 children with COVID-19 every day over the previous week, representing a 27.3% increase over the week ending August 3, according to CDC data. While children ages 12 and older are eligible to receive the Pfizer-BioNTech SARS-CoV-2 vaccine, rates of vaccination in that age group remain below the national average, around 31% fully vaccinated.
States experiencing the largest increases in overall COVID-19 cases, such as Louisiana and Florida, also are seeing the greatest increases in hospitalizations among children. Dr. Mark Kline of Children’s Hospital in New Orleans said children with COVID-19 account for about 20% of the facility’s hospitalized patients, with most of them under age 10 and too young to be vaccinated. In Texas, more children are being treated in hospitals for COVID-19 than ever before, and many also are infected with respiratory syncytial virus (RSV). One physician, warning of dwindling hospital capacity, said the 2 viruses are “spreading like wildfire” among younger children, particularly those under age 2. According to the American Academy of Pediatrics, nearly 94,000 cases among children were recorded in the week ending August 5, continuing a “substantial increase” in the number of new cases since the beginning of July.
Although children continue to account for a small percentage of total COVID-19 hospitalizations—between 1.5% and 3.5%—the disease impacts kids of different ages differently, and even those who have asymptomatic or mild infections could experience so-called “long COVID,” or post-acute sequelae of COVID-19 (PASC). Experts are still learning about the condition, which is characterized by a variety of symptoms including memory or concentration difficulties (ie, “brain fog”), trouble sleeping, fatigue, dizziness, headaches, gastrointestinal problems, or changes to smell or taste. The impacts of these long-lasting symptoms could be “huge,” according to some pediatric experts, with the symptoms disrupting school and extracurricular activities especially among those in their formative teen years. Concern over the rising number of COVID-19 cases and hospitalizations among younger populations, and the potential for long-term impacts, is amplified by anecdotal evidence the Delta variant might cause more severe disease among children and that many are returning to in-person learning. These factors, and the fact that about 50 million children remain ineligible for vaccination, places even more importance on utilizing other risk reduction methods, including vaccination among those who are eligible, mask wearing, and physical distancing.
US CDC VACCINATION GUIDANCE FOR PREGNANT WOMEN The US CDC on August 11 recommended that all people who are pregnant, breastfeeding, trying to get pregnant, or might become pregnant in the future be vaccinated for SARS-CoV-2. The agency cited a growing body of evidence showing vaccination during pregnancy is safe, noting new data that found no increased risk of miscarriage among pregnant people who received a SARS-CoV-2 mRNA vaccine during the first 20 weeks of gestation. Previously, the CDC said the vaccine could be offered during pregnancy, but the new recommendation urges all pregnant people to be vaccinated. According to CDC data, only about 23% of pregnant people have received at least one dose of a vaccine. The new recommendation comes amid a surge of new COVID-19 cases, hospitalizations, and deaths in the US, driven by the highly transmissible Delta variant. The CDC’s updated recommendation came 2 days after the release of a joint statement by the American College of Obstetricians and Gynecologists, American Academy of Pediatrics, and 20 other health organizations “strongly” urging pregnant and recently pregnant individuals, as well as those planning to become pregnant, to be vaccinated. The groups noted that pregnant individuals are at an increased risk of severe COVID-19 disease, including death, and the best way to protect themselves is through vaccination.
US GOVERNMENT VACCINE MANDATES The US Department of Health and Human Services (HHS) became the latest federal agency to announce a vaccine mandate for some of its employees, requiring more than 25,000 members of its health care workforce to be vaccinated against SARS-CoV-2. Staff of the Indian Health Services (IHS) and National Institutes of Health (NIH) who work in health and clinical research facilities or who have direct contact with patients and members of the US Public Health Service Commissioned Corps who respond to public health crises nationwide are included in the mandate. The HHS mandate also applies to contractors, trainees, and volunteers who might have patient contact at federal clinical research or medical facilities. IHS, NIH, and Commissioned Corps staff already are required to receive seasonal influenza and other routine vaccinations, with allowances for certain medical and religious exemptions.
The US Department of Veterans Affairs (VA) announced a similar vaccine mandate at the end of July, and on August 12 expanded the requirement to apply to most Veterans Health Administration (VHA) employees, volunteers, and contractors who work in VHA facilities, visit such facilities, or otherwise come into contact with VA patients and healthcare workers as part of their jobs. The US Department of Defense earlier this week announced a plan to require all military members to be vaccinated by mid-September or earlier. All other US government employees are required to show proof of vaccination or be subject to other precautions, including regular testing, mask wearing, and travel restrictions.
VACCINE EFFECTIVENESS & VOCs New information continues to emerge regarding the effectiveness of different SARS-CoV-2 vaccines, particularly with respect to variants of concern (VOCs). This week, several articles were published in academic journals and on preprint servers. In one study, published in The New England Journal of Medicine, UK researchers examined vaccine effectiveness against symptomatic disease for both the Alpha and Delta SARS-CoV-2 variants. They included data on participants who received either the Pfizer-BioNTech or AstraZeneca-Oxford vaccines and stratified the sample for those who had received partial or full doses. The research team found that both vaccines were less effective against the Delta variant than the Alpha variant when the individual only had one dose (30.7% vs 48.7%), and also saw reduced effectiveness against Delta for fully vaccinated individuals when compared to Alpha. The Pfizer-BioNTech vaccine was 93.7% effective in preventing symptomatic disease against Alpha and 88% against Delta among fully vaccinated individuals, while the AstraZeneca-Oxford vaccine was 74.5% and 64% effective, respectively.
Another study, conducted in Utah (US) and posted on the preprint server medRxiv, suggested similar findings. The researchers found a modest reduction in overall vaccine effectiveness for all US FDA-authorized vaccines corresponding to the expansion of the Delta variant in the state, saying the reduction in effectiveness due to the VOC, and not waning immunity, is “highly concerning.” A third study, conducted in Qatar and also posted to medRxiv, examined the effectiveness of the Pfizer-BioNTech and Moderna vaccines against the Delta variant. The research team estimated the effectiveness against symptomatic COVID-19 to be 79.0% for the Pfizer-BioNTech vaccine and 84.8% for the Moderna vaccine. The Pfizer-BioNTech vaccine exhibited 89.7% effectiveness against severe, critical, or fatal COVID-19 disease due to Delta, and the Moderna exhibited 100% effectiveness, although this analysis had a very small sample size.
A fourth preprint study, posted to medRxiv and based on data collected by the Mayo Clinic, retrospectively examined SARS-CoV-2 PCR test data collected between January and July 2021 from 645,109 individuals vaccinated with either the Pfizer-BioNTech or Moderna vaccines. Both vaccines were highly effective during the study period for preventing infection, with Moderna exhibiting 86% effectiveness and Pfizer-BioNTech 76% effectiveness. Additionally, the vaccines worked well to prevent COVID-19 hospitalizations, with an estimated effectiveness of 91.6% for the Moderna vaccine and 85% for the Pfizer-BioNTech vaccine. However, effectiveness against infection dropped in July with the rise of the Delta variant, with Moderna at 76% and Pfizer-BioNtech at 42%. All of these papers reinforce that current SARS-CoV-2 vaccines are effective at preventing COVID-19 disease—particularly severe disease, hospitalization, and death—even in the face of increasing prevalence of VOCs, including the Delta variant.
SARS-COV-2 RAPID ANTIGEN TESTS Researchers from Germany published (preprint) findings from a study on the accuracy of 2 commercially available SARS-CoV-2 antigen rapid diagnostic tests (RDTs), comparing them to the "gold standard" real-time reverse transcription-polymerase chain reaction (rRT-PCR)-based tests. The SD Biosensor SARS-CoV-2 Rapid Antigen Test by Roche Diagnostics and Panbio COVID-19 Ag Rapid Test by Abbott Diagnostics were compared in a German diagnostic center between February 1 and March 31, 2021. Of 2,215 tests conducted, 338 (15%) were rRT-PCR positive for SARS-CoV-2. The Roche RDT exhibited 60.4% sensitivity and 99.7% specificity, and the Abbott RDT exhibited 56.8% sensitivity and 99.8% specificity. The sensitivities of the RDTs were higher among individuals referred by physicians and health departments compared to the total study population, where the Roche RDT performed at 79.5% and the Abbott RDT at 78.7%. The RDTs had substantially lower sensitivities in individuals with at least one comorbidity (Roche 38.2%, Abbott 34.4%) compared to those without comorbidities (Roche 74.4%, Abbott 71.0%). Higher unadjusted sensitivities in RDTs were also observed in symptomatic individuals (Roche 75.2%, Abbott 74.3%) compared to asymptomatic individuals (Roche 23.8%, Abbott 31.9%).
To put these results in context, if 10,000 symptomatic individuals were tested, of which 500 were truly positive, these RDTs would yield 38 false-positive and 124 false-negative results. If 10,000 asymptomatic individuals were tested, of which 50 are true positives, the RDTs would yield 18 false-positive and 34 false-negative results. Based on the study, the authors call into question whether the widespread use of RDTs for screening purposes is beneficial. Since screening often is recommended for asymptomatic individuals, the results of the study are of crucial importance in assessing tests best suited for this use.
CANADA VACCINE MANUFACTURING FACILITY Pharmaceutical company Moderna and the Government of Canada on August 10 announced a memorandum of understanding to build a “state-of-the-art” manufacturing facility in Canada to make the company’s SARS-CoV-2 vaccine and possibly other respiratory virus vaccines that use the mRNA platform. Moderna said the facility will help provide Canada with supplies of its SARS-CoV-2 vaccine, “direct access” to pandemic response capabilities in the future, and access to any vaccines currently in development that might receive approval. About 30% of the SARS-CoV-2 vaccine doses distributed in Canada are from Moderna, and that proportion could go up depending on regulatory approval of additional doses. Though the location of the manufacturing plant has not yet been decided, it will likely be similar to Moderna’s main facility in Norwood, Massachusetts (US), and will employ a couple hundred people. Moderna CEO Stéphane Bancel said the company is in talks to build similar manufacturing facilities in other nations in Europe and Asia, although he did not specify which ones, adding they expect to build 5 to 10 such plants worldwide over the coming years. Earlier this year, Canada announced an agreement with Novavax, which is working on its own SARS-CoV-2 vaccine, to produce its doses at a government-owned facility in Montreal either late this year or early next year. Notably, Novavax has delayed its submission for authorization to the US FDA 3 times, most recently citing efforts to validate production consistency.
SENEGAL The Senegalese health system continues to struggle under a third wave of SARS-CoV-2 infections, where cases have skyrocketed. More than 15,000 cases and 139 deaths were reported in July, according to the Ministry of Health. Prior to July, Senegal reported fewer than 44,000 cases and 1,166 deaths. Ambulance services in Dakar, the current epicenter of the outbreak, also are feeling the strain. Since the beginning of the third wave, more than 90% of calls to the Mobile Emergency Care Service (SAMU) have been for respiratory distress. With the influx of emergency calls, hospitals are low on bed space with supplemental oxygen to care for patients, and delivery workers have been working through the night to keep up with the oxygen demand. Cemetery workers also are among personnel working around the clock to keep up with demand. A cemetery manager close to the Dakar hospital reports an average of 30 burials per day during this wave of infections. During the last surge, the average was 20 burials a day, and prior to the pandemic, 10 each day.
Last month, the government announced construction of a vaccine manufacturing plant in the capital, which is expected to produce 25 million doses per month by the end of 2022. The Institut Pasteur in Dakar will run the plant to reduce outside dependence on vaccine supply. As of August 9, just under 2% of the Senegalese population was fully vaccinated against SARS-CoV-2.
GLOBAL VACCINE ACCESS The WHO is continuing to press wealthier nations and SARS-CoV-2 vaccine manufacturers to reverse the “disgraceful” inequity in global access to vaccines to help low- and middle-income countries (LMICs) vaccinate at least 10% of their populations by the end of September. Speaking during an online Q&A session with WHO officials, Dr. Bruce Aylward, Senior Adviser to the WHO Director-General and head of the Access to COVID-19 Tools (ACT) Accelerator initiative, criticized wealthier nations, saying they should be “disgusted” by the imbalance in the available tools to address the pandemic and calling for US$.7.7 billion to help the WHO supply vaccines, oxygen, and other medical supplies to LMICs. Dr. Aylward’s comments come a week after WHO Director-General Dr. Tedros Adhanom Ghebreyesus called for a moratorium on providing additional, or booster, doses to most people in order to improve global access. Researchers with the Council on Foreign Relations identified 37 high- and middle-income countries that are considering or already administering booster shots as of August 12. They warn—as does the WHO in a recently released interim statement on booster doses—that offering third doses to large swaths of populations, beyond vulnerable groups such as the immunocompromised or people over the age of 80, threatens to further widen the gap between “vaccine-haves and vaccine-have-nots.”
The Pan American Health Organization (PAHO) this week announced a plan to increase SARS-CoV-2 vaccine availability for its member countries. The new COVID-19 initiative, which will be operated through the organization’s well-established Revolving Fund, will purchase “tens of millions” of vaccine doses, syringes, and related supplies and begin delivering them in October to the more than 20 countries in the region that have expressed interest in joining. In making the announcement, PAHO recognized it is not clear whether the COVAX facility will succeed in providing the necessary vaccine doses to its member nations.
On August 10, more than 175 public health experts, scientists, and civil society leaders as well as more than 50 organizations sent a letter to officials in the administration of US President Joe Biden, calling on them to immediately ramp up a global vaccine manufacturing program to help vaccinate the rest of the world and reduce the likelihood of newer, possibly more dangerous variants emerging. In a separate letter addressed to President Biden, they urge him to release millions of stockpiled doses each week to countries in need, noting the US has more than 55 million doses of mRNA vaccines stockpiled but is administering fewer than 900,000 per day. While many experts are focused on the threat of emerging new variants, the UN Development Programme (UNDP) warns vaccine inequities will have long-term economic and social impacts in LMICs, including a widening poverty gap, increased divides in health care spending, and swollen public debt.
HERD IMMUNITY IMPOSSIBLE Consensus is forming among public health experts and scientists worldwide: the highly transmissible Delta variant of SARS-CoV-2 changed the COVID-19 pandemic, dashing hopes of widespread vaccination creating herd immunity that could protect people from infection and guaranteeing the novel coronavirus will become endemic. While the vaccines are highly effective at preventing serious illness or death, they do not fully protect the vaccinated from infection. Additionally, people who had previous SARS-CoV-2 infections are not necessarily protected from infection from future variants. And because infected people can in turn infect others, whether vaccinated or not, the concept of herd or population immunity with COVID-19 “is not a possibility,” according to experts who recently spoke to the UK’s All-Party Parliamentary Group. However, the vaccines still work, and work well, protecting those fully vaccinated from death and keeping them out of the hospital, and vaccine doses should be urgently distributed to "where they can have the greatest impact," especially to countries in need, Professor Sir Andrew John Pollard, Director of the Oxford Vaccine Group, urged. In the meantime, “the world needs to stay alert,” Ed Yong writes in The Atlantic, and make use of all available protective measures that could help stave off the emergence of new, potentially more dangerous variants.
by ponchi101 The paragraph about herd immunity stands out to me. By definition, and with a virus multiplying by the billions/trillions in anybody, some more mutations will happen. And then maybe one of them will be immune against the vaccine, and there we will go again.
Of course, the Delta variant will perhaps remain with everybody, and pretty soon non-vaccinated people will be surrounded, by their unvaccinated peers or by vaccinated people that will still be able to transmit the virus.
by ti-amie
ponchi101 wrote: ↑Fri Aug 13, 2021 7:21 pm
The paragraph about herd immunity stands out to me. By definition, and with a virus multiplying by the billions/trillions in anybody, some more mutations will happen. And then maybe one of them will be immune against the vaccine, and there we will go again.
Of course, the Delta variant will perhaps remain with everybody, and pretty soon non-vaccinated people will be surrounded, by their unvaccinated peers or by vaccinated people that will still be able to transmit the virus.
Ponchi, Lambda variant is on line 1...
by ponchi101 Oh, I know. I was not thinking of Lambda. I was thinking Epsilon through Omega.
(A written down wink as the subject is too extreme for funny emojis)
by Suliso I think this idea of heard immunity needs to abandoned asap. It would be nice to have, but it's not politically and scientifically possible.
by ti-amie This just popped up on my timeline.
by ti-amieDeSantis, faced with covid surge, urges Floridians to use Regeneron antibody treatment given to Trump
By
Timothy Bella
Today at 2:59 p.m. EDT
Florida Gov. Ron DeSantis (R) is vowing to begin dispensing Regeneron monoclonal antibodies — the treatment given to President Donald Trump when he had the coronavirus — through mobile clinics amid a record-breaking stretch of new cases and hospitalizations that have ravaged the state.
DeSantis said at a news conference in Jacksonville on Thursday that while coronavirus vaccines have been effective at preventing illness and death, more was needed to help curb the spread of the virus in a state that has become the U.S. hotbed of the latest surge of infections. The governor championed Regeneron’s monoclonal antibody cocktail for those who have already gotten sick, saying it is “the most effective treatment that we’ve yet encountered for people who are actually infected with covid-19.”
“Covid’s not going to go away,” DeSantis said. “So the question is how are we going to approach it. You can approach it on the front end by protecting yourself, but of course, if you end up in a situation where you are infected and at high risk, getting in here early, this is the best shot we’ve got right now to keep people out of the hospital and keep them safe.”
The antibody treatment, a cocktail of the monoclonal antibodies casirivimab and imdevimab that is made by Regeneron Pharmaceuticals, is designed to prevent infected people from developing severe illness. DeSantis’s promotion of Regeneron, which imitates the body’s natural defenses, is the governor’s latest response to a pandemic in which he has rejected mask mandates and restrictions.
While doctors have noted the treatment’s promise and effectiveness in clinical trials, others have stressed that taking the vaccine remains the most crucial defense to fight the spread of the virus. One physician noted that there is only a small supply, making the Regeneron antibodies “an extremely effective treatment for a limited number of people.”
DeSantis told reporters that the mobile units, which are already operating in parts of the state hit hard by the delta variant, will be expanded throughout Florida. The Trump administration last year initially bought 300,000 doses of Regeneron’s monoclonal antibody treatment, which cost about $1,500 per dose at the time.
A Regeneron spokesperson said in a statement to The Washington Post on Friday that the government has now bought up to 1.5 million doses of the treatment and that it is being made available free to patients. DeSantis did not specify how many Floridians would have access to the shots.
The Food and Drug Administration granted emergency authorization to Regeneron in November, saying that the treatment may be effective in treating mild to moderate covid in adults and children 12 or older, and is recommended for those at high risk of developing severe illness. The FDA expanded Regeneron’s emergency authorized use last month, enabling the treatment for people exposed to someone who has been infected or for those at high risk of exposure in settings such as prisons or nursing homes.
DeSantis urged people at high risk to get the treatment at the first sign of symptoms, suggesting that Floridians “won’t even necessarily need a prescription from a doctor” to obtain Regeneron. Doctors and health professionals have indicated that people who are severely ill from the coronavirus are less likely to see benefits from monoclonal antibodies.
“I do think this is probably the best thing we can do to reduce the number of people that require hospitalization,” DeSantis said.
The state reported 24,730 new cases on Thursday, bringing its seven-day average to more than 18,000 cases a day, according to data compiled by The Post. With 15,796 people hospitalized for the virus, Florida now accounts for 1 out of every 5 covid hospitalizations in the nation. More than 3,200 people are currently occupying beds in intensive care units, an increase of 17 percent from last week.
DeSantis has opposed implementing pandemic restrictions during the fourth wave of the pandemic. The Republican is in a back-and-forth with school districts that are pushing for mask mandates for children returning to school. That debate is expected to intensify after four educators in Broward County died of the virus within 24 hours, CBS Miami reported.
The Regeneron cocktail is best known as the antibody treatment given to Trump when it was still an investigational drug after he contracted the virus last October. Other high-profile Republicans, such as Rudolph W. Giuliani and Ben Carson, also acknowledged receiving the Regeneron drug.
After he was released from the hospital, Trump inaccurately described the Regeneron cocktail as a “cure” and pressed the FDA to quickly clear the medication. While demand was expected to surge when Trump made a laudatory video in which he promised to make the antibody treatments free to patients needing them, officials acknowledged that many patients and doctors did not know much about the medicine and were not asking for it.
Still, Regeneron announced this week in its quarterly earnings report that it had $2.59 billion in sales for its antibody drug, an increase of 163 percent compared to this time last year
DeSantis on Thursday promoted Regeneron as achieving a “70 percent reduction in hospitalization and death for covid patients” in clinical trials, referencing an announcement by the company in the spring. But Dushyantha Jayaweera, a clinical professor at the University of Miami Medical School, told WPLG that the decrease in hospitalizations was more like a “relative risk reduction.”
“So he’s kind of giving the more optimistic, more flowery view,” Jayaweera said. “But the reality is that it is much less.”
Kami Kim, director of the division of infectious-disease and international medicine with the University of South Florida Health Morsani College of Medicine, told the Orlando Sentinel that while Regeneron could help those who have been infected, other options remain easier for helping to address the Sunshine State’s surge.
“The number one strategy is probably going back to social distancing again and wearing masks,” Kim said. “And obviously, Governor DeSantis has his view on that, which most public health people would not entirely agree with.”
Those who choose to get the Regeneron treatment at the Jacksonville site will be given the option of either getting four shots in the stomach, or two in the stomach and two in the arm, according to WTLV. Those patients will then be observed for an hour inside an air-conditioned tent.
In announcing the treatment, DeSantis claimed that the Regeneron treatment should “become part of the standard of care” for Floridians moving forward.
“This is going to be with us for a long time,” he said.
Laurie McGinley and Carolyn Y. Johnson contributed to this report.
by ti-amie Four shots are needed. At a cost of $1500 per shot but wearing a mask that costs very little is being told what to do. I wonder if insurance companies cover the cost of this treatment?
by ponchi101 Even if they do, what are the deductibles? The equivalent to 1,000 masks? 10,000?
2 free vaccines, 1 box of masks = $5?
Anyway, not as I am in need to convince anybody here at TAT2.0.
by MJ2004 My best friend's daughter, age 4, just tested positive. She caught it in daycare, alway a petri dish even in the best of circumstances. They live in Iowa. So far she has mild cold symptoms (congestion and cough) with no fever.
Frightening, indeed.
I don't know how unvaccinated (never mind unmasked) children being sent to school in a couple of weeks can be viewed as anything but a potential disaster in the making.
by ti-amie
by ti-amie
by ponchi101 And, simultaneously, we have a separate topic in which we worry out loud what will happen in Afghanistan when it falls under Taliban control.
It is hard to have faith in Pinker's "we live in the best of times" theory, sometimes.
(No, I still agree. But just not everywhere).
by ti-amie I'm really, really surprised no one told this jerk to eff off and leave the woman alone.
I'm also not surprised that he's from New Jersey.
by ti-amie
by ti-amie
by ti-amie
by dryrunguy Here's the latest Situation Report. Some of it has already been reported in this thread. There's a lot to unpack...
::
EPI UPDATE The WHO COVID-19 Dashboard reports 207.2 million cumulative cases and 4.36 million deaths worldwide as of 12:45pm EDT on August 16. Global weekly incidence continues to increase, but it appears to be approaching a peak or plateau, however this could be a function of reporting delays. Last week, the weekly total increased less than 2% compared to the previous week. Global weekly mortality held relatively steady last week, decreasing less than 0.5% compared to the previous week. The dashboard indicates that there are delayed reports from multiple countries in the African Region for August 15, which are likely impacting the global trends. Notably, the weekly incidence for the African Region was nearly 23% lower than the previous week—a difference of more than 40,000 new cases—and weekly mortality was nearly 18% lower—a difference of 834 deaths. The global trends could shift upward once reporting is complete for Africa for last week.
Global Vaccination
The WHO reported 4.46 billion doses of SARS-CoV-2 vaccines administered globally as of August 16. The WHO reports that a total of 1.70 billion individuals have received at least 1 dose, and 880 million are fully vaccinated. Analysis from Our World in Data shows that the global daily doses administered has leveled off after a week of decline, holding relatively steady at approximately 37 million doses per day*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.47 billion vaccinated individuals worldwide (1+ dose; 31.7% of the global population) and 1.85 billion who are fully vaccinated (23.7% of the global population). Notably, the global total jumped from 1.25 million fully vaccinated individuals on August 11 to 1.81 million on August 12 due to newly reported data from China**.
*The average doses administered may exhibit a sharp decrease for the most recent several days, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent data.
**The previous report from China’s National Health Commission was on June 10. China has not updated data regarding its partially vaccinated population (1+ dose) since June 10.
UNITED STATES
The US CDC reported 36.7 million cumulative COVID-19 cases and 619,564 deaths. The daily average is up to 121,873 new cases per day, the highest since February 4. Daily incidence continues to increase rapidly, but it appears as though the US may be passing an inflection point. It is difficult to determine, however, whether this is an artifact of reporting frequency—particularly over the weekend—or an early indication of a longer-term trend. Daily mortality continues to increase as well, although it is difficult to determine whether the current trend is a linear or exponential increase. The current average of 548 deaths per day is the highest since May 13*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 357.3 million cumulative doses of SARS-CoV-2 vaccines. After approximately 5 weeks of steady increase, the daily vaccinations leveled off over the past several days, holding relatively steady at approximately 650-660,000 doses per day*. A total of 198.6 million individuals in the US have received at least 1 dose, equivalent to 59.8% of the entire US population. Among adults, 72.1% have received at least 1 dose, as well as 12.4 million adolescents aged 12-17 years. A total of 168.7 million individuals are fully vaccinated, which corresponds to 50.8% of the total population. Approximately 61.8% of adults are fully vaccinated, as well as 9.2 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
THIRD DOSE FOR IMMUNOCOMPROMISED INDIVIDUALS The US CDC approved a recommendation to provide a third dose of mRNA-based SARS-CoV-2 vaccines to individuals with moderate-to-severe compromised immune systems on August 13. CDC Director Dr. Rochelle Walensky’s approval of the recommendation followed a unanimous vote by the agency’s Advisory Committee on Immunization Practices (ACIP) and an emergency use authorization by the US FDA. The Pfizer-BioNTech vaccine is authorized for use among individuals aged 12 and older, and the Moderna vaccine is authorized for individuals aged 18 and older. The FDA did not extend the authorization for a third dose to the J&J-Janssen vaccine due to a lack of efficacy data, but officials have stated they are working to develop a recommendation.
A third dose of the mRNA-based SARS-CoV-2 vaccines is recommended for moderately to severely immunocompromised individuals, including those receiving cancer treatment, recent recipients of an organ or stem cell transplant, those with advanced or untreated HIV infection, individuals taking a high dose of corticosteroid, and people who are anticipating treatment that may weaken their immune system. However, a third dose of vaccine is not recommended for adults with chronic conditions that may cause mild immunosuppression, such as people with diabetes and heart disease or residents in long-term care facilities. According to the guidance, the third dose should be given at least 28 days after the second dose for the best results. The CDC urges eligible individuals to try to get the same vaccine for their third dose, but receiving a different vaccine for the third dose is acceptable if the original is unavailable. Notably, immunocompromised people will not need a prescription or doctor’s note to get a third dose but will need to attest to their eligibility, raising questions about the potential for people to lie about their immune status in order to receive a third vaccine dose.
PFIZER-BIONTECH THIRD DOSE Pfizer-BioNTech submitted early-stage clinical trial data to the US FDA on August 16 to seek emergency use authorization for a third SARS-CoV-2 vaccine dose for all people aged 16 years and older. The companies claim the trial data show a third dose administered 6 to 12 months after the second dose generates higher levels of neutralizing antibodies against the Alpha, Beta, and Delta variants of SARS-CoV-2. The companies state that late-stage trial data will be submitted to the FDA and additional worldwide regulatory authorities once available.
The US government is not yet officially recommending third doses of mRNA-based vaccines for the general public despite the recent guidance for booster vaccinations for people with moderate-to-severely compromised immune systems. However, officials are reportedly developing plans to start offering third doses of vaccines to more of the general public as early as the fall. Initial doses given under the plan likely would be reserved for healthcare workers and long-term care facility residents who are at increased risk of severe disease. The FDA must first review the data submitted by Pfizer-BioNTech before an emergency use authorization can be approved and before the US CDC can make an official recommendation.
US EVICTION MORATORIUM The new version of a US CDC eviction moratorium faced its first legal challenge last week, with US District Judge Dabney Friedrich in Washington, DC, allowing the order to stay in place because she is bound by a ruling from the US Court of Appeals for the District of Columbia (DC) Circuit that allowed the previous version of the moratorium to continue. In May, Judge Friedrich ruled the previous nationwide moratorium exceeded the CDC’s authority but she stayed the judgment pending appeal, which allowed the moratorium to remain in force. The plaintiffs then asked the US Court of Appeals to vacate the stay, but the court declined, again allowing the moratorium to continue. In doing so, the court said the moratorium falls within a 1944 public health emergencies law and that the US government “made a strong showing that it is likely to succeed on the merits.” At this point, the plaintiffs asked US Supreme Court Chief Justice John Roberts to vacate Judge Friedrich’s stay, but Chief Justice Roberts denied relief on June 29. Notably, 5 justices indicated they would grant the application to vacate the stay.
When a group of property managers and realtors asked Judge Friedrich to put a hold on the new eviction ban—which is set to expire October 3 and applies only to places in the country experiencing significant SARS-CoV-2 transmission, instead of the entire nation—she wrote that “the minor differences between the current and previous moratoria do not exempt the former from this Court’s order.” Judge Friedrich indicated she would vacate the stay but that she does not have the authority to act on a higher court’s decision. The plaintiffs are expected to ask the US Court of Appeals to reconsider its ruling and likely will go to the US Supreme Court if they don’t get their desired outcome. In a statement, White House Press Secretary Jen Psaki said the administration of US President Joe Biden “believes that CDC’s new moratorium is a proper use of its lawful authority to protect the public health. We are pleased that the district court left the moratorium in place, though we are aware that further proceedings in this case are likely.” She said President Biden is calling on all officials to urgently distribute US$46.5 billion in emergency rental assistance funds made available through Congressional action on COVID relief.
US SUPREME COURT VACCINE MANDATE CHALLENGE The US Supreme Court last week refused to block Indiana University’s requirement that all students, faculty, and staff have a SARS-CoV-2 vaccination, unless they qualify for one of several exemptions. The decision to turn down a group of students’ request for emergency relief was issued independently by Justice Amy Coney Barrett, who handles emergency requests from Indiana, without explanation, without dissents from other justices, and without asking the university for a response. All of these moves could signal the request does not stand on solid legal ground. Both a federal district judge and an unanimous panel of the US Court of Appeals for the 7th Circuit previously rejected requests for emergency relief while the issue moved through the courts. This was the first case involving mandatory SARS-CoV-2 vaccinations to reach the Supreme Court.
FUNDING FOR US RURAL HEALTHCARE The Administration of US President Joe Biden on August 13 announced the US Department of Health and Human Services (HHS) will provide US$8.5 billion in American Rescue Plan (ARP) spending to help aid healthcare providers who serve rural Medicare, Medicaid, and Children’s Health Insurance Plan (CHIP) patients for lost revenue and increased expenses associated with COVID-19. Additionally, the US Department of Agriculture (USDA) will use US$500 million in ARP funding to establish the Emergency Rural Health Care Grant Program to help rural healthcare facilities increase access to SARS-CoV-2 vaccines and testing, medical supplies, telehealth, and food assistance; support construction or renovation; compensate for lost revenue or staffing expenses due to the pandemic; and plan and implement models to improve long-term viability. The announcement also included funding to train new rural healthcare providers and expand telehealth services. In a fact sheet, the White House said the funding “builds on efforts the Administration has already taken to help rural communities tackle the COVID-19 crisis and improve access to health care,” including a previous announcement of US$100 in funding to assist rural health facilities conduct vaccine outreach.
VACCINE INCENTIVES Mercer, an employee benefit consultant company, recently stated that at least 20 companies have approached them to ask about implementing health insurance coverage surcharges of US$20-50 per month for employees who refuse to get a SARS-CoV-2 vaccine. Employers have offered benefits and incentives such as cash payments and paid time off to encourage vaccination among their ranks, but stalling vaccination rates have some companies reconsidering their approach. Health coverage surcharges already are a tool used when insured individuals act against common medical advice, such as continuing to smoke cigarettes. For example, the Affordable Care Act allows insurers to charge smokers up to 50% more than non-smokers for health coverage. The likelihood of health coverage surcharges for not receiving a SARS-CoV-2 vaccine remains unclear, but employers or insurers may decide to implement these measures if the cost of hospitalization for unvaccinated insurance recipients gets too high.
FLORIDA SCHOOL DISTRICT The Hillsborough County School District, which includes Tampa, Florida (US), is expected to hold an emergency school board meeting on August 18 to discuss COVID-19 protective measures only 1 week after resuming in-person classes for the fall semester. Since the start of classes, nearly 6,000 students and employees have been asked to isolate or quarantine due to SARS-CoV-2 infection or exposure. COVID-19 data from the school district indicate that nearly 1,300 new cases have been reported among students and staff since August 2, including 399 students and 88 staff reported on August 16 alone. The school district reported 8,771 cumulative cases from March 2020 to August 1, 2021. Notably, the cases are distributed relatively evenly across the county’s 250 schools, with only one school exceeding 50 cases. The district announced on August 7 that it was implementing a mask requirement through September 3, but parents would be able to opt their children out of the requirement. So far, the district—the 7th largest in the nation with 208,000 students—has received 27,915 opt-out submissions. Florida Governor Ron DeSantis’s office has said the state Board of Education could withhold the salaries of district superintendents or school board members who disregard the governor’s executive order that effectively prohibits school districts from implementing mask mandates. Statewide, Florida’s epidemic continues to surge to record levels.
GLOBAL VACCINE DISTRIBUTION Australia has purchased and received 500,000 doses of SARS-CoV-2 vaccine from the COVAX facility, raising questions about how many of the vaccine-sharing mechanism’s doses should go to low- and middle-income countries (LMICs). Australia received the doses in COVAX’s third round of vaccine distributions. Also in that round, the UK received nearly 540,000 doses and New Zealand received nearly 101,000 doses. Australia is domestically producing the AstraZeneca-Oxford vaccine and has plentiful supplies but has been trying to obtain more doses of the Pfizer-BioNTech vaccine due to medical advice that the vaccine is preferred for people under age 59 and hesitancy among some to receive the AstraZeneca-Oxford vaccine. According to a report in The New York Times, Pfizer-BioNTech expressed its desire for a COVAX shipment of its vaccine to go only to LMICs, but the facility allegedly insisted it first fulfill orders from higher-income nations that paid more for the doses. Concerns remain whether COVAX can move beyond pressures from wealthy countries and pharmaceutical companies, manufacturing delays, and bureaucratic infighting to help reach its goal of supplying 2 billion vaccine doses by the end of 2021.
In the meantime, millions of J&J-Janssen vaccine doses being “filled and finished” by South African-based Aspen Pharmacare are being shipped to Europe for distribution because of “an unusual stipulation” in the contract between the country’s government and the vaccine company. Reportedly, the contract required South Africa to waive its right to impose export restrictions on vaccine doses finished in-country. A South African health ministry official said the government was not pleased with the contract’s stipulation but did not have the leverage to change it. J&J-Janssen has shipped 32 million doses to Europe in recent months, according to an investigation by The New York Times. The company had agreed to sell enough of its vaccine to African countries to eventually vaccinate about one-third of the continent’s residents. However, Africa continues to struggle to obtain enough supplies, and only about 2% of Africans are fully vaccinated. According to a J&J official, the Aspen plant will begin exclusively supplying doses to African countries later this year. In a Guardian opinion piece, former UK Prime Minister Gordon Brown criticized Europe for taking a “neocolonial approach” to global health, saying the shipments of J&J-Janssen vaccine from South Africa to Europe represent a “shocking symbol of the west’s failure to honor its promise of equitable vaccine distribution.”
GERMANY PEDIATRIC VACCINATION Germany’s vaccine advisory committee, known as STIKO, on August 16 updated its guidance to recommend that all individuals aged 12 to 17 years receive a SARS-CoV-2 vaccine. The recommendation expands on the committee’s previous guidance for that age group, which advised only those children and young adults who had an increased risk of severe COVID-19 disease, including those with compromised immune systems or those who might have professional exposure to the virus, be vaccinated. STIKO said its decision was based on surveillance data from the US showing the benefits of vaccination outweigh the risk of very rare side effects, including heart inflammation, and modeling data showing children and adolescents have a higher risk of infection from the Delta variant. Germany’s 16 state health ministers decided on August 2 that all children and teenagers ages 12 and older should be eligible for vaccination, but the STIKO held off on recommending the same until now. The European Medicines Agency (EMA) has authorized both the Pfizer-BioNTech and Moderna vaccines for that age group.
IRAN The spread of the highly transmissible SARS-CoV-2 Delta variant in Iran has led to record numbers of COVID-19 cases and deaths, forcing the country’s health system to the edge of collapse. On August 16, Iran’s Ministry of Health reported a daily record of 655 deaths, although some, including Iran’s state television, estimate the daily totals to be higher, between 720 and 1,000. A 6-day nationwide lockdown began August 16, including the closure of offices, banks, bazaars, and non-essential businesses such as theaters, gyms, and restaurants in all Iranian cities, and a separate 6-day ban on intra-city travel began on August 15.
According to the Ministry of Health, nearly 15.5 million Iranians have received at least one dose of a SARS-CoV-2 vaccine, with 4.4 million having received 2 doses, less than 5% of the total population. Supreme Leader Ayatollah Ali Khamenei earlier this year banned vaccines made in the US and Britain, saying the shots were designed to “contaminate other nations.” Last week, Khamenei appeared to backpedal slightly, calling the pandemic the country’s top priority and saying “efforts must be redoubled so vaccines can be provided for the people through any means necessary.” Following his comments, a health official said vaccines developed by Western countries would be allowed if they are manufactured in other nations. So far, Iran has accepted more than 21 million doses of various vaccines from China, Russia, India, Cuba, Japan, and the COVAX initiative. The country also is using its domestically developed COVIran Barekat vaccine, which the government has said is 85% effective at preventing COVID-19 but has not released any clinical data. In the absence of sufficient vaccine and medication supplies, private dealers and black markets are filling the gaps, affordable only to more wealthy Iranians, with each vaccine dose costing up to US$1,200.
More Iranians are trying to raise awareness about the country’s plight, using the hashtag #SOSIran on social media and speaking anonymously to media outlets. Iranian security forces arrested 5 lawyers and a civil rights advocate over the weekend, allegedly for planning to take legal action against Iranian authorities for mismanagement of the pandemic and a slow vaccination campaign rollout. Critics blame both Khamenei and newly elected President Ebrahim Raisi for the current crisis, while some officials recently shifted blame to the previous government of President Hassan Rouhani.
AFGHANISTAN The WHO today expressed concern over the Taliban’s rapid advance and seizure of power in Afghanistan, as the security situation deteriorates and humanitarian needs increase. At a UN briefing, a WHO spokesperson said the agency is “extremely concerned over the unfolding safety and humanitarian needs in the country, including risk of disease outbreaks and rise in COVID-19 transmission." He indicated WHO mobile teams are on hold in the capital, but the agency remains committed to staying in the country. The Taliban reportedly has banned SARS-CoV-2 vaccines in Paktia province, one of the nation's 34 provinces located in the country’s eastern region. In recent weeks and since the withdrawal of US troops from Afghanistan, the Taliban have captured much of the northern, western, and southern regions of the country.
NEW ZEALAND LOCKDOWN Following its first domestic case of COVID-19 in 6 months, New Zealand is entering a nationwide lockdown. Prime Minister Jacinda Ardern announced the Alert Level 4 restrictions earlier today, which will apply to the entire country for a period of 3 days. The restrictions are scheduled to last for 7 days in Auckland and the Coromandel Peninsula where the case was identified and traveled in the days prior to testing positive. The individual was unvaccinated but was in the process of scheduling an appointment when he tested positive. His wife, who is vaccinated, has tested negative. Prime Minister Ardern noted that it is not yet known if the case was a result of the Delta variant, but she emphasized that all recent infections identified among quarantined travelers have been a result of the Delta variant.
AIR POLLUTION & COVID Wildfires continue to rage across several western US states, and exposure to smoke and soot from the blazes could be associated with an increased risk of COVID-19 disease, including severe disease and death. Like smoking tobacco, exposure to smoke from wildfires can impair lung function, especially due to tiny airborne particles that can penetrate deep into lung tissue. Smoke from wildfires can contain high concentrations of this fine particulate matter, known as PM 2.5 (ie, particulate matter with a diameter of 2.5 microns or less), and exposure to high concentrations of PM 2.5 can impede the exchange of oxygen in the lungs.
The study, published on August 13 in Science Advances, evaluated COVID-19 data and PM 2.5 concentration data from 92 counties in California, Oregon, and Washington from March-December 2020. The researchers from Harvard University estimated air pollution levels based on satellite imagery from the US National Oceanic and Atmospheric Administration (NOAA), and they defined “wildfire days” as heavy PM 2.5 concentration (21-32 μg/m3). Based on the smoke exposure data, the researchers developed a model to estimate the effect of higher-than-expected PM 2.5 concentration on COVID-19 incidence and mortality. The researchers observed increased daily COVID-19 incidence and mortality for up to 4 weeks following exposure to high concentrations of PM 2.5 particles, although they noted several differences across counties. They estimated that even relatively short-term exposure to smoke from wildfires (typically on the order of days or weeks) was associated with nearly 20,000 extra COVID-19 cases and 750 deaths. Numerous complex environmental, social, and epidemiological factors drive COVID-19 incidence and mortality, but the study provides evidence that short-term exposure to elevated concentrations of air pollution, including from wildfire smoke, potentially can increase the risk of COVID-19 disease and death.
by ponchi101 I am sorry, but Australia should NOT be receiving COVAX vaccines. It is an industrialized country, with plenty of cash. They should, at a minimum, and by now, be able to produce their own.
by ti-amie
They were aware requiring a person's vaccine status is not a HIPAA violation all along.
Just as they've all been vaccinated all along.
Someone should really ask these people who are dying because they believed what these clowns an AITA question.
by ponchi101 What would be the possibility of a class action suit (I am not even sure if that is how these are called), suing FOX for disinformation and, of course, possible medical consequences, all the way to death?
by ti-amie From what I read on the bird app a few weeks ago they started dialing back on the "hoax" and "freedumb" nonsense. I would be surprised if a class action suit isn't on its way especially after this notice.
by ti-amie
This is in Oregon.
by ti-amie
by mmmm8 My mom was just telling me about a student of hers whose mother is a nursing home nurse and is anti-vaxx - in New Jersey. I was shocked this wasn't already a requirement from the state.
by ponchi101 I am trying to come up with a good simile for being a nurse and NOT believing in vaccines, and all I can come up with are cliches.
Being a catholic and not believing in communion?
A physicist that does not believe in electrons?
How confused can you be?
by ti-amie
Kailey Tracy @KaileyTracy
6m
State providing more resources to this site and others, FL DOH spokesperson said, to "ensure something like that is not happening." Said healthcare workers make call if someone is too sick to get the treatment and should go to hospital instead.
I'm truly ashamed at my first reaction to these pics.
by ti-amie
by ti-amie You know Dry posts the Situation reports almost daily. I know people with busy lives, jobs, kids, or school (or some combination) can't sit down and read the entire report. But the information is out there and it's not that hard to find. There are countries, continents, geographic areas that would love to have adequate doses of vaccine for their people. And here we are, in (still) the richest and most powerful country in the world being terrorized by not only the uneducated but educated fools who are stopping this pandemic from being the scourge it is here.
I post these little anecdotes to show how ignorance has been sold as a virtue to some many people while those who are the face of the anti movement are quietly and safely vaccinated. This news is out there too but they seem immune to it.
I try not to judge. I try not to ridicule but I'm really tired of this ignorance. I'm really tired of it.
by ti-amie
by ponchi101
ti-amie wrote: ↑Thu Aug 19, 2021 6:16 pm
You know Dry posts the Situation reports almost daily. I know people with busy lives, jobs, kids, or school (or some combination) can't sit down and read the entire report. But the information is out there and it's not that hard to find. There are countries, continents, geographic areas that would love to have adequate doses of vaccine for their people. And here we are, in (still) the richest and most powerful country in the world being terrorized by not only the uneducated but educated fools who are stopping this pandemic from being the scourge it is here.
I post these little anecdotes to show how ignorance has been sold as a virtue to some many people while those who are the face of the anti movement are quietly and safely vaccinated. This news is out there too but they seem immune to it.
I try not to judge. I try not to ridicule but I'm really tired of this ignorance. I'm really tired of it.
I am re-reading Pinker's ENLIGHTNMENT NOW, just because I need something to stop me from descending into further despair. But, as you say, the ignorance of the masses is truly tiring. Plus, it affects us all. Personally, if the world continues to sputter my area of work remains locked, and that is slowly beating me up to a pulp. Yet, I can't do anything as long as these people refuse to do something as simply as get a vaccine, and as you say, I am getting so tired of that. And by now, as I have said, I really don't care for any person that does not get the vaccine. Because they obviously don't care about me or anybody else.
by dryrunguy During my group's staff meeting on Monday (we use Teams), my boss mentioned that her nephew, who has all sorts of pre-existing conditions and has always been frail, had contracted COVID.
Then she went on about how his father, her ex-brother-in-law, has been going on and on about how COVID is just the flu, it's no big deal, etc. And then she talked about what a jerk he is, etc.
Then she went on to say that she is not vaccinated and does not plan to get vaccinated. You see, she falls into the "I have a lot of questions" group. She's very well-informed, she says, and takes all of the recommended precautions (except getting vaccinated), she always wears her mask, and she has a back-up plan in case she gets sick. She mentioned ivermectin. And it was clear that she's operating on the assumption that, if she gets it and gets very sick, she has time to implement this back-up plan.
All of this information was unsolicited. It was rambling stream-of-consciousness and dissonance. Most notably, it was highly defensive. Everything she said was defensive in nature. It was really quite remarkable to watch.
Later that same day, she ended her work day early so she could drive to a family event.
by ti-amie I wasn't going to post this but dry's co worker's comments made me find it again and post it. The non scientist is using a very persuasive tone of voice and presentation but when you listen to what she's saying it's nonsense.
by Suliso You know what? I've started to mostly tune out covid news. I've done what I could for myself - vaccinated and wear mask where it makes sense and all my closest friends/relatives are now vaccinated as well. If you choose to take a bigger risk up to you.
by ti-amie
Suliso wrote: ↑Thu Aug 19, 2021 8:37 pm
You know what? I've started to mostly tune out covid news. I've done what I could for myself - vaccinated and wear mask where it makes sense and all my closest friends/relatives are now vaccinated as well. If you choose to take a bigger risk up to you.
There's no proof stupidity isn't catching. I'm just about there too. Reading what Tsitsipas father and Pat Cash have said though we tennis fans may have to deal with news about 'Rona Delta whether we want to or not.
by mmmm8
dryrunguy wrote: ↑Thu Aug 19, 2021 7:48 pm
During my group's staff meeting on Monday (we use Teams), my boss mentioned that her nephew, who has all sorts of pre-existing conditions and has always been frail, had contracted COVID.
Then she went on about how his father, her ex-brother-in-law, has been going on and on about how COVID is just the flu, it's no big deal, etc. And then she talked about what a jerk he is, etc.
Then she went on to say that she is not vaccinated and does not plan to get vaccinated. You see, she falls into the "I have a lot of questions" group. She's very well-informed, she says, and takes all of the recommended precautions (except getting vaccinated), she always wears her mask, and she has a back-up plan in case she gets sick. She mentioned ivermectin. And it was clear that she's operating on the assumption that, if she gets it and gets very sick, she has time to implement this back-up plan.
All of this information was unsolicited. It was rambling stream-of-consciousness and dissonance. Most notably, it was highly defensive. Everything she said was defensive in nature. It was really quite remarkable to watch.
Later that same day, she ended her work day early so she could drive to a family event.
Hey, maybe you'll be the boss soon.
by dryrunguy Originally published by the NY Times (paywall), so here's the link to the same article published by the Seattle Times. Headline: Those anti-COVID plastic barriers probably don’t help and may make things worse
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 209.2 million cumulative cases and 4.39 million deaths worldwide as of August 20.
As we previously covered, COVID-19 data from August 15 was delayed for multiple countries in the African Region, which gave the appearance of decreasing trends in last week’s data. It appears that reporting for last week is now complete, which corrected the weekly trends. Weekly incidence increased for the eighth consecutive week—an increase of 3.2% over the previous week—although the trend is tapering off toward a peak or plateau. Weekly mortality increased for the sixth consecutive week*, 0.7% higher than the previous week.
*With the exception of the week of July 19, when Ecuador reported 8,786 deaths.
Global Vaccination
More than 1 billion individuals worldwide are fully vaccinated. The WHO reported 4.56 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of August 20. The WHO reports that a total of 1.78 billion individuals have received at least 1 dose, and 1.03 billion are fully vaccinated. Analysis from Our World in Data indicates that the global daily doses administered continues to hold relatively steady at approximately 35-40 million doses per day*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.51 billion vaccinated individuals worldwide (1+ dose; 32.2% of the global population) and 1.88 billion who are fully vaccinated (24.2% of the global population). We expect the global total to surpass one-third of the population with 1+ dose and one-quarter with full vaccination in the coming days.
*The average doses administered may exhibit a sharp decrease for the most recent several days, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reported 37.3 million cumulative COVID-19 cases and 623,244 deaths. Daily incidence is up to 133,055 new cases per day, the highest since February 2. Daily incidence continues to increase rapidly, but it appears that the US has passed an inflection point and is now tapering off. Based on the timeline from the previous peak, this could indicate that the current surge could peak in the next several weeks. While some severely affected states are beginning to peak—including Arkansas, Florida, and Louisiana—many others are still exhibiting increasing trends as the surge spreads to other parts of the country, with some states still early in their respective surges. Daily mortality continues to increase as well, although it is difficult to determine whether the current trend is a linear or exponential increase. The current average of 640 deaths per day is the highest since April 24. On August 18, the US reported more than 1,000 deaths in a single day for the first time since March 19*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent dates.
As the US continues to combat its ongoing surge hospitalizations are setting new records at the national and state level, particularly for individuals under the age of 50. At the national level, new daily hospitalizations are at record highs for all age groups aged 49 years and younger, and the 50-59 years age group is at 91% of its record high. Notably, the 0-17 years age group—most of whom are still not eligible for vaccination—is currently 40% higher than its previous peak and still increasing rapidly, just as schools are resuming classes across the country. In terms of the percent of emergency department (ED) visits for COVID-19, most age groups appear to be peaking at the national level. Similar to new hospitalizations, all age groups aged 49 years and younger are setting new records, ranging from 3.2% for 0-11 years to 8.1% for 40-49 years. The CDC’s COVID-19 dashboard does not provide data for current hospitalizations broken down by age group, but the current average across all age groups (76,077 hospitalized patients) is within 40% of the previous peak and still increasing.
Similar trends are evident across the whole of HHS Region 4 (Southeast), where the current surge is most severe. Current hospitalizations in the region set a new record high last week, and the current average is just shy of 30,000 patients and still increasing. We have paid considerable attention to Region 4, but Region 10 (Northwest) is also exhibiting concerning trends. While Region 10 is not setting records for new daily hospitalizations in the 0-11 years age group—suggesting lower transmission among children—all other age groups 59 years and younger are surpassing their previous records and still increasing sharply. Region 10 is also setting new records in terms of the percent of ED visits for COVID-19, both averaged across all ages and individually for all age groups 64 years and younger. Regions 4 and 10 also are both reporting record high current hospitalizations, and Region 6 (South) is 11% below its highest peak and still increasing steadily. While these 3 regions are exhibiting similar trends, the magnitude of the epidemics are quite different, with Region 10 reporting 2,000 hospitalizations compared to 30,000 and 17,000 in Regions 4 and 6, respectively. On a per capita basis**, COVID-19 hospitalizations in Regions 4 and 6 are 2.3 and 1.9 times higher than in Region 10, respectively.
**Based on 2020 census data.
At the state level, Arkansas, Florida, Hawai’i, Louisiana, Mississippi, Oregon, and Washington are all setting new records in terms of current hospitalizations. A total of 5 other states—3 from Region 4 and 2 others that border it—are within 20% of their records and still increasing. Among the states setting new records for current hospitalizations, all are setting new records in terms of new daily hospitalizations among most age groups 59 years and younger. Notably, all of these states, with the exception of Oregon and Washington, are setting new records for the 0-11 years age group. As with the regional trends, the magnitude of these epidemics varies widely at the state level. Hawai’i, Oregon, and Washington are reporting between 1.7 and 3.5 new daily hospitalizations per 100,000 population, whereas Arkansas, Florida, Louisiana, and Mississippi range from 6 to more than 10. In Florida, all age groups—with the exception of 0-11 years—have equaled or surpassed the record peak for percent of ED visits for COVID-19 set by the 65-74 years and 75+ years age groups in the previous surge—ie, higher than the highest peak for the most vulnerable age groups. Notably, the 40-49 years and 50-64 years age groups are more than 60% higher than that previous record. A similar trend is evident in Louisiana, with all age groups except 0-11 years and 75+ years equaling or surpassing the previous record.
US Vaccination
The US has administered 359.6 million cumulative doses of SARS-CoV-2 vaccines. After approximately 5 weeks of steady increase, the daily vaccinations leveled off over the past several days, holding relatively steady at approximately 670,000 doses per day*. A total of 199.9 million individuals in the US have received at least 1 dose, equivalent to 60.2% of the entire US population. Among adults, 72.5% have received at least 1 dose, as well as 12.6 million adolescents aged 12-17 years. A total of 169.6 million individuals are fully vaccinated, which corresponds to 51.1% of the total population. Approximately 62.0% of adults are fully vaccinated, as well as 9.4 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US PLANS FOR THIRD DOSES US health officials on August 18 announced plans to make third doses of SARS-CoV-2 mRNA vaccines available to all US residents as soon as the week of September 20. The third dose is meant to bolster individuals’ immune responses at least 8 months from their second dose of either the Pfizer-BioNTech or Moderna vaccines. People who received the J&J-Janssen vaccine likely will need an additional dose, but officials are waiting on results from a clinical trial expected to be available later this month. US officials based their decision to offer booster doses on published and unpublished data showing vaccine effectiveness across age groups appears to wane over time and particularly amid the spread of the highly transmissible Delta variant. While they stressed the vaccines remain highly effective at preventing severe disease, hospitalizations, and death, they said the vaccines’ ability to prevent infection or symptomatic disease has declined since the spring. Some of the breakthrough infections seen among vaccinated individuals could be due to weakening immunity, lapses in protective measures such as mask wearing, or the now widespread Delta variant, or a combination of such factors, experts noted, contending that no vaccine was meant to be 100% effective in preventing infection.
At a White House COVID-19 Task Force briefing, US CDC Director Dr. Rochelle Walensky presented data from 3 early release Morbidity and Mortality Weekly Report (MMWR) studies, 1 not-yet-peer-reviewed study published on medRxiv, and unpublished CDC data. One of the MMWR studies included data from New York collected between May 3 and July 25, 2021, showing vaccine effectiveness (VE) against infection declined from 91.7% to 79.8%. A second MMWR study showed the mRNA vaccines’ protection against infection among nursing home residents declined from 75% between March 1 and May 9, 2021, before Delta became the dominant strain, to 53% between June 21 and August 1, when Delta accounted for at least half of new COVID-19 cases. In positive news, a third MMWR publication showed no significant decline in the vaccines’ effectiveness against COVID-19 hospitalization over a 24-week period, ranging from 85% 2-12 weeks post-vaccination and 84% at 13-24 weeks. However, data from a Mayo Clinic preprint in medRxiv showed Moderna VE fell from 86% in January 2021 to 76% in July, while Pfizer-BioNTech VE dropped from 76% to 42% during the same time. According to a joint statement from US Department of Health and Human Services (HHS) experts, data from these sources make the argument for booster doses “very clear” that protection against SARS-CoV-2 infection wanes over time. However, some experts argued the case for third doses remains unclear, saying officials presented no data regarding how much third doses boost immune responses or how long any benefits might last. US officials previously said the logistics of rolling out a booster dose program are too complex to wait for scientific certainty that the extra doses are actually necessary.
Third doses initially will be available for about 5 million people who were first to receive vaccines over the 2020-2021 winter, including healthcare workers, nursing home residents, and older adults. Last week, regulators authorized third doses for people with compromised immune systems, such as cancer patients and organ transplant recipients, who represent less than 3% of the US population. The plan to provide booster doses is contingent upon the US FDA authorizing a third dose of either mRNA vaccine and the CDC’s Advisory Committee on Immunization Practices (ACIP) making subsequent recommendations. Only earlier this week did Pfizer-BioNTech submit initial data to the FDA supporting the evaluation of a booster dose of its vaccine. Moderna has yet to submit data. Some experts speculate that a third dose given 8 months from the second dose could provide a more robust and long-lasting immune response, potentially requiring few or no future boosters, although US Surgeon General Vivek Murthy said “there’s nothing magical” about the 8-month timeframe. Some of the same experts, as well as others, expressed additional concerns over the plan for multiple reasons, including that all US residents might not immediately need boosters, that a timeframe for providing extra doses apparently has been decided prior to regulatory decisions, and that more focus should be placed on vaccinating more people in the US and globally.
THIRD DOSE CONCERNS The announcement reignited criticism about global vaccine inequity, with some experts expressing fear, frustration, and even anger over wealthier nations’ continuing disregard for a WHO call for a moratorium on booster doses. WHO officials and other experts continue to argue that booster programs—also implemented in Israel, France, Germany, and other nations—will further deplete scarce vaccine resources and deprive low- and middle-income countries (LMICs) of needed doses. The WHO estimates 11 billion vaccine doses are needed to help control the pandemic. WHO Regional Director for Africa Dr. Matshidiso Moeti chastised wealthier nations, saying “they make a mockery of vaccine equity” by stockpiling vaccine doses while the situation in Africa remains “very fragile.” WHO chief scientist Dr. Soumya Swaminathan and other researchers warned that a focus on booster programs in wealthy nations could lead to the development of more viral variants and “an even more dire situation” globally, because the virus continues to spread unabated in unvaccinated—not vaccinated—populations. Other experts said there was still not enough conclusive evidence supporting third doses to recommend them to everyone.
But US officials pushed back at the disapproval. White House Press Secretary Jen Psaki said the notion the US would not be able to provide boosters and simultaneously donate doses to countries in need represented a “false choice.” US CDC Director Dr. Rochelle Walensky agreed, saying, “We're going to do both and we have been doing both," noting the country plans to distribute 200 million doses worldwide and administer 100 million booster doses by the end of the year. Global health advocates continue to call on the US to be more of a leader in efforts to bolster global vaccine supplies, including by pressuring pharmaceutical companies to share technologies with LMICs and help scale up manufacturing in those countries.
US CDC DISEASE FORECASTING CENTER On August 18, the US CDC officially announced its new Center for Forecasting and Outbreak Analytics. The center will leverage advanced data and modeling capacities to provide health officials with projections and other analysis during outbreaks and epidemics, aiming to “accelerate access to and use of data for public health decision-makers.” The center also will provide forecasting capacity for emerging infectious disease threats, as the pandemic response highlighted the need to streamline and modernize data collection reporting at the state and local levels. Prior to establishing this center, the US government had relatively little internal capacity for infectious disease modeling, genomic surveillance, and other real-time analytics, requiring it to draw on external support from academic institutions, think tanks, and other organizations, which often volunteered their time and effort. The new center will continue to draw on these external resources, but it establishes a central point within the CDC to provide coordination and support. Initial funding for the program comes from the American Rescue Plan, part of a series of emergency funding packages approved during the COVID-19 pandemic. The center will be led by Dr. Marc Lipsitch, Dr. Dylan George, Dr. Rebecca Kahn, and the Johns Hopkins Center for Health Security’s own Dr. Caitlin Rivers.
US NURSING HOME FUNDING US President Joe Biden announced on August 18 that nursing home staff must be vaccinated against SARS-CoV-2 or their facilities risk losing federal funding that many facilities rely on to maintain operations. The vaccine requirement would affect more than 15,000 facilities and 1.3 million employees nationwide. According to the Centers for Medicare and Medicaid Services (CMS), nursing home residents have a higher rate of vaccination compared to staff, with nearly 83% of residents vaccinated per facility compared to 60% of staff per facility. But that represents the national average; vaccination rates vary by state since many nursing homes have not implemented vaccine requirements. Florida has the lowest percentage of staff with completed vaccinations per facility at 40%. At the other end of the spectrum, Hawai'i boasts the highest percentage, with nearly 87% of staff vaccinated per facility. The new mandate is expected to be formalized by CMS regulation. An official deadline for the requirement has not been set, although it could take effect as soon as next month.
MASKS IN SCHOOLS US President Joe Biden this week ordered Secretary of Education Miguel Cardona to use all available tools to ensure that governors and other state officials are taking appropriate actions to safeguard students' return to in-person schooling, including possibly taking legal action against governors who ban universal masking in schools. Secretary Cardona said he will use the department’s civil rights enforcement capacity to investigate states that ban masking. The Biden administration plans to send letters to the governors of Arizona, Iowa, Oklahoma, South Carolina, Tennessee, and Utah—in addition to those Secretary Cardona already sent to Florida and Texas—reprimanding their efforts to block universal masking in schools and expressing support for local officials who defy mask bans. Secretary Cardona also noted that the department would pay the full salaries of educators if their “states move to withhold pay or levy financial penalties on their schools.” Earlier this year, the department’s Office of Civil Rights published a report outlining the impacts of the COVID-19 pandemic on US students, warning that existing educational gaps are widening during the pandemic, falling disproportionately on those students with the greatest educational needs and fewest opportunities, many from historically marginalized and underserved populations.
In Miami-Dade County, the largest county in Florida, the school board on August 18 voted to require masks for students when in-person learning resumes next week, defying an order from Governor Ron DeSantis that effectively bans mask mandates. Miami-Dade joins Alachua, Broward, and Hillsborough as Florida counties requiring masks for students, employees, and visitors, with only medical exemptions accepted. The school districts cited updated CDC guidance and the rise in pediatric infections, including record high hospitalizations, as the basis for requiring face coverings.
In Texas, the State Supreme Court on August 19 denied Governor Greg Abbott’s request to block temporary restraining orders on his ban on mask mandates issued by Travis County Judge Jan Soifer. As a result, the lower court’s ruling stands, for now, allowing school districts to continue their requirements. The governor now must appeal to the Texas Court of Appeals. On the same day, the Texas Education Agency suspended enforcement of Governor Abbott’s ban in the state’s public school system. The State Supreme Court’s order comes only days after it sided with Governor Abbott, granting a temporary emergency stay of an appellate court ruling and allowing his ban on mask mandates, including those in public schools. Following that order, the Dallas and San Antonio school districts, 2 of the largest in the state, said they would continue to require masks until a final ruling is made. Since then, several other districts have implemented universal masking requirements. The legal battles over masking in schools undoubtedly will continue to work their way through the courts.
SCHOOL VACCINE MANDATES As states around the country return or prepare to return to school in the coming weeks, some state legislatures are taking final steps to increase the proportion of vaccinated public school employees. In Washington state, Governor Jay Inslee announced a vaccination requirement for all employees in K-12 schools at the private, public, and charter levels and those working in childcare settings and higher education institutions. Employees must show proof of full vaccination prior to October 18 or possibly face dismissal. The policy has limited medical and religious exemptions, and there is no test out option, possibly representing the most widespread and strict requirements implemented by a state yet. Governor Inslee also expanded a statewide mask mandate, applicable to all individuals regardless of vaccination status. Other states with vaccine requirements for school staff, such as California and Connecticut, have allowed employees the option of choosing between mandatory vaccination or routine testing for those who wish not to comply. Several major cities across the country, including Los Angeles and Chicago, also are requiring public school employees to get vaccinated. Other states likely will implement vaccine requirements for school staff as students return to in-person learning, with rumors that New Jersey could be next.
MODERNA VACCINE FOR UK ADOLESCENTS The UK Medicines and Healthcare products Regulatory Agency (MHRA) granted Conditional Marketing Authorization (CMA) for the use of the Moderna SARS-CoV-2 vaccine in children aged 12-17 years. The CMA was granted through the European Commission (EC) Decision Reliance Route, which allows for new Marketing Authorizations based on previous authorizations through the centralized EC process, but it means that the CMA only applies to Great Britain. Northern Ireland issued a CMA for 12- to 17-year-olds via the same process on July 23. The approval in Great Britain comes a week after the England Department of Health announced 16- and 17-year-olds will be offered a first dose of SARS-CoV-2 vaccine by August 23, before schools resume classes in September. MHRA Chief Executive Dr. June Raine said “the vaccine is safe and effective in this age group” and that it will be up to the Joint Committee on Vaccination and Immunization (JCVI) to advise on whether adolescents aged 12 and older should receive the Moderna vaccine as part of the deployment program. The Moderna vaccine has not yet been authorized for use in individuals aged 12 to 17 years in the US, but the European Medicines Agency (EMA) recommended its use in this age group on July 23.
ISRAEL Throughout the COVID-19 pandemic, Israel has been one of the countries on the forefront of disease control. Following an early and successful SARS-CoV-2 vaccination campaign, Israel saw a drop in the incidence of new COVID-19 cases. Unfortunately, the region has now seen a drastic increase in cases, despite a large proportion of its adult population having received a SARS-CoV-2 vaccine. With worries that waning vaccine effectiveness contributed to the new surge, Israel announced a campaign of so-called booster doses for senior residents that started at the end of July. However, there is minimal evidence to support the application of booster doses, leading some experts to question the decision. So far, 37 individuals have tested positive for COVID-19 following their third dose. These recent developments have increased concerns over the longevity of vaccine efficacy, especially against more transmissible SARS-CoV-2 variants of concern.
POPE ENCOURAGES VACCINATION In a new public service campaign made in coordination with the Ad Council and directed specifically at the Americas, Pope Francis encourages people to get vaccinated, saying it is “an act of love.” The video features Pope Francis speaking Spanish with English subtitles in the Ad Council’s first campaign outside of the United States. The Pope is joined by church officials from Brazil, Mexico, the United States, and other countries who describe getting vaccinated as a “moral responsibility.” Vaccine hesitancy among religious groups has been a barrier to vaccination during the pandemic, but a survey by the Public Religion Research Institute and Interfaith Youth Core nonprofit groups conducted in June suggests acceptance may be on the rise. Of more than 5,000 people surveyed in the US, acceptance rose from 56% in March to 80% in June among Hispanic Catholics, and from 68% to 79% among White Catholics. Vaccine-hesitant participants also told researchers that faith-based arguments may convince them to get vaccinated, underlining the importance of the Pope’s message. The ad will be run on Telemundo, Universo, and WarnerMedia platforms, and media outlets in various Spanish-speaking countries.
FAKE VACCINATIONS/CARDS As more SARS-CoV-2 vaccine requirements are enacted for everything from employment, to travel, to restaurant dining, the black market for vaccine cards is growing. US Customs and Border Protection (CBP) agents in Memphis, Tennessee (US), recently announced they have seized more than 3,000 fake vaccination cards shipped from China and destined for various US cities since the end of June. Additionally, a Chicago pharmacist was charged with 12 counts of theft of government property after allegedly stealing and selling official US CDC vaccination cards on eBay. The FBI has warned that buying, selling, or using counterfeit vaccination cards is a crime, punishable by a fine and up to 5 years in prison. In France, fake vaccine passes are being sold through social media platforms such as Snapchat and Facebook for up to €400 (US$467). If caught, those who distribute counterfeit passes face up to 5 years in prison and fines up to €150,000 (US$175,000), and users could spend 3 years in prison. Officials in the US and France reminded the public that SARS-CoV-2 vaccines are available at no cost.
In more disturbing developments, the WHO identified counterfeit versions of Covishield—the Indian-made version of the AstraZeneca-Oxford SARS-CoV-2 vaccine—in India and Africa in recent months. The Indian government said it has launched an investigation into the allegations. Last month, around 4,000 people in India paid to receive a SARS-CoV-2 vaccine at a “vaccination camp” but instead got shots of saline solution. Authorities arrested 14 people in connection with the scheme. In Germany, a Red Cross nurse is believed to have injected more than 8,000 residents with shots of saline rather than a SARS-CoV-2 vaccine, authorities there say, although it is unclear whether any arrests have been made or charges filed. Officials continue their work to stop the counterfeiting of vaccine cards and shots worldwide.
NFL VACCINATION This week the Atlanta Falcons became the first and reportedly only US National Football League (NFL) team to achieve 100% SARS-CoV-2 vaccination of its roster. Now, all players are able to work out and eat together and are exempt from daily testing, mask use in team facilities, and quarantine following close contact with someone who tests positive, the team confirmed in a statement. As we previously reported, the NFL implemented strict consequences for teams with unvaccinated players, potentially including forfeiting games that are canceled because of outbreaks. Additionally, unvaccinated players could lose pay for games missed due to testing positive. On August 18, Tampa Bay Buccaneers Head Coach Bruce Arians said his team likely would reach 100% vaccination before the start of the regular season on September 9. The NFL Network on August 11 reported that 92% of NFL players have at least 1 dose of vaccine, well above the national average of 60%. NFL teams could provide insight into vaccine effectiveness in close-contact settings where every individual is vaccinated.
dryrunguy wrote: ↑Thu Aug 19, 2021 7:48 pm
Then she went on to say that she is not vaccinated and does not plan to get vaccinated. You see, she falls into the "I have a lot of questions" group. She's very well-informed, she says, and takes all of the recommended precautions (except getting vaccinated), she always wears her mask, and she has a back-up plan in case she gets sick. She mentioned ivermectin. And it was clear that she's operating on the assumption that, if she gets it and gets very sick, she has time to implement this back-up plan.
All of this information was unsolicited. It was rambling stream-of-consciousness and dissonance. Most notably, it was highly defensive. Everything she said was defensive in nature. It was really quite remarkable to watch.
Later that same day, she ended her work day early so she could drive to a family event.
Sounds like a solid back-up plan.
by ponchi101 It is the treatment of choice for the "holistic", "natural medicine" crowd.
Why they think it is natural or new escapes me. Info from my looney friend that swears for any alternative medicine.
by Jeff from TX
ponchi101 wrote: ↑Fri Aug 20, 2021 8:01 pm
It is the treatment of choice for the "holistic", "natural medicine" crowd.
Why they think it is natural or new escapes me. Info from my looney friend that swears for any alternative medicine.
I do not know how any manufactured drug qualifies as "holistic".
by Suliso It's a fairly complex semi synthetic chemical. What's so natural about it?
by ponchi101 I did mention it was my looney friend, right?
I am as puzzled as you. Why has this veterinary remedy become so popular in this community is insane. Apparently, some guru in Argentina has voiced his opinion/fatwa about its efficacy and that is it.
by JazzNU Even if it was natural, it's just stunning to refuse to take a clinically trialed and approved vaccine deemed safe by just about every reputable scientific and medical organization that researches these things and taken by billions of human beings and opt instead for a drug that is intended for use by HORSES and COWS. The mental gymnastics that is needed to justify that reasoning is just astounding to consider.
by dryrunguy
JazzNU wrote: ↑Sat Aug 21, 2021 12:42 am
Even if it was natural, it's just stunning to refuse to take a clinically trialed and approved vaccine deemed safe by just about every reputable scientific and medical organization that researches these things and taken by billions of human beings and opt instead for a drug that is intended for use by HORSES and COWS. The mental gymnastics that is needed to justify that reasoning is just astounding to consider.
And sheep and goats. Y'all always forget the sheep and goats! I'm hurt and offended!
by ponchi101 Well, as I unfortunately have friends in that camp, I get to hear their lines of reasoning, if they can be called so. It is usually some conspiracy based theory, in which Big Pharma/Agro/Oil/Chemical is trying to make some money (because, you know, they are struggling to do so) and they make this plan to FORCE their ideas and products on everybody, but this one guy, this one EXPERT that no one will listen to except THEM, in Central Patagonia, or Northern Rwanda or the Tibetan Highlands has found that three spoonfuls of Nepalese Tea leaves chewed by Northern Chinese sheep (I am not forgetting the sheep, Dry) mixed with detoxified/hydrogenated water taken in the morning, facing Aquarius, cures you. Just like that.
I have been in conversations in which my problem was: where do I start? How do you take down this level of insanity?
Anyway, preaching to the choir. Nobody here to convince. Tomorrow I am playing with my buddy some padel, and I will see what crazy idea of the week he has developed.
JazzNU wrote: ↑Sat Aug 21, 2021 12:42 am
Even if it was natural, it's just stunning to refuse to take a clinically trialed and approved vaccine deemed safe by just about every reputable scientific and medical organization that researches these things and taken by billions of human beings and opt instead for a drug that is intended for use by HORSES and COWS. The mental gymnastics that is needed to justify that reasoning is just astounding to consider.
And sheep and goats. Y'all always forget the sheep and goats! I'm hurt and offended!
Not forgetting, didn't know. I'm unfamiliar with this ivermectin so I'm just going off what was referenced in the articles I read, so this is all very illuminating, I'm learning something new right now. So, less a pill for horses and cows, and more a pill for livestock in general?
JazzNU wrote: ↑Sat Aug 21, 2021 12:42 am
Even if it was natural, it's just stunning to refuse to take a clinically trialed and approved vaccine deemed safe by just about every reputable scientific and medical organization that researches these things and taken by billions of human beings and opt instead for a drug that is intended for use by HORSES and COWS. The mental gymnastics that is needed to justify that reasoning is just astounding to consider.
And sheep and goats. Y'all always forget the sheep and goats! I'm hurt and offended!
Not forgetting, didn't know. I'm unfamiliar with this ivermectin so I'm just going off what was referenced in the articles I read, so this is all very illuminating, I'm learning something new right now. So, less a pill for horses and cows, and more a pill for livestock in general?
In terms of ivermectin as a livestock wormer, there's one solution for sheep and goats, one solution for hogs, one solution for horses, and one solution for cattle. You can't use the one for horses on sheep, for example. It comes in two forms for sheep--subcutaneous injection or oral drench. I prefer the drench because that way you're absolutely certain it gets into their digestive system and eventually the blood stream where with the injection, the critter might jump at the wrong moment--and next thing you know, you're not 100% sure you got it completely under the skin or if you accidentally injected in the muscle.
As for what version of ivermectin humans are using or what else goes into this "cocktail", I have no clue. I can't imagine folks are drinking it right out of the bottle. But here's part of what's on the warning label and instructions for sheep:
PRECAUTIONS:
Ivermectin Sheep Drench has been formulated for use in sheep ONLY. (But I've used it for goats as well; works fine; no problems.) This product should not be used in other animal species as severe adverse reactions, including fatalities in dogs, may result. This product is not to be used parenterally.
HUMAN SAFETY:
When used as recommended in sheep, Ivermectin Sheet Drench does not pose a hazard to human health. As a routine precaution, it is advisable to wash hands after use. As with all drugs, the product should be kept out of reach of children. Contact with skin and eyes should be avoided, but protective clothing is not required.
KEEP THIS AND ALL DRUGS OUT OF REACH OF CHILDREN: Refrain from smoking and eating while handling. Avoid contact with eyes. Immediately wash hands and any spills on the skin with plenty of soap and water following use.
::
So obviously, the manufacturers never considered the idea that some people might actually be dumb enough to drink it--except children (which is the main reason why we have a nationwide network of poison control centers).
by dryrunguy P.S. The other reason why it would usually be so absurd to think humans might actually drink this stuff is the warning about how ivermectin can cause coughing in sheep (short-term). Spot on. That happens about 50% of the time I administer it to sheep.
by JazzNU Appreciate the rundown @dry, and gotta say, that makes me even more shocked that humans would consider that an acceptable thing to ingest and expect a good outcome.
And yes about the poison control centers. That's part of the Mississippi stories I posted, MS Poison Control has had an uptick in calls relating specifically to people treating covid with ivermectin. And it's adults, not children. And even more ridiculous, they are taking large amounts of it.
by ti-amie Today in covidiocy...
by ti-amie
by JazzNU I support this no matter the location, but especially in an area like Charlottesville. Hospital capacity in rural VA is (expletive), plain and simple, don't overtax the system unnecessarily.
by Deuce .
It's not over by a long shot, people...
by dryrunguy Here we go. Headline: Mississippi officials warn against using livestock ivermectin to prevent COVID-19 after rise in poison control calls Apparently, based on the different pieces I read, most folks are taking the horse version, but people are using other versions as well.
dryrunguy wrote: ↑Sun Aug 22, 2021 7:55 pm
Here we go. Headline: Mississippi officials warn against using livestock ivermectin to prevent COVID-19 after rise in poison control calls Apparently, based on the different pieces I read, most folks are taking the horse version, but people are using other versions as well.
dryrunguy wrote: ↑Sun Aug 22, 2021 7:55 pm
Here we go. Headline: Mississippi officials warn against using livestock ivermectin to prevent COVID-19 after rise in poison control calls Apparently, based on the different pieces I read, most folks are taking the horse version, but people are using other versions as well.
This while there is a FREE vaccine readily available. I don't get it.
And ivermectin isn't cheap, either. I ordered a new bottle a few months ago. $35 for 8 ounces. You can buy larger bottles of it if you have a large operation. (Or REALLY bad COVID.)
by ti-amie I bet someone associated with tfg manufactures and/or has stock in the stuff.
by dryrunguy While my employer continues to shop short of mandating vaccination for our employees, they announced today that the company will pay $500 to each employee who has been vaccinated or gets vaccinated by October 1.
by JazzNU
by JazzNU
dryrunguy wrote: ↑Mon Aug 23, 2021 8:16 pm
While my employer continues to shop short of mandating vaccination for our employees, they announced today that the company will pay $500 to each employee who has been vaccinated or gets vaccinated by October 1.
I'm a little surprised it's not a mandate for you with the federal contracts, but very nice about the bonus.
by ti-amie
by JazzNU I knew I was right not to click and see why Obesity was trending on Twitter. Idiots.
by ti-amie
by dryrunguy Here's the latest Situation Report. The paragraph on Healthcare Worker Resilience was particularly depressing. But then the "You're Not a Horse" paragraph made me chuckle a little.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 212.4 million cumulative cases and 4.44 million deaths worldwide as of August 24. The global weekly incidence increased for the ninth consecutive week, up 1.1% over the previous week. The trend continues to taper off toward a peak or plateau. Over the past several weeks, weekly incidence has decreased in Africa and South East Asia, held relatively steady or peaked in the Eastern Mediterranean region and Europe, and increased steadily or exponentially in the Americas and the Western Pacific region. Global weekly mortality increased for the seventh consecutive week*, up 1.8% compared to the previous week. If the global mortality continues on this trajectory, the cumulative total could surpass 4.5 million deaths in the next week.
*With the exception of the week of July 19, when Ecuador reported 8,786 deaths.
Global Vaccination
The WHO reported 4.62 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of August 23. The WHO reports that a total of 1.80 billion individuals have received at least 1 dose, and 1.06 billion are fully vaccinated. Analysis from Our World in Data indicates that the global daily doses administered is decreasing steadily from its second-highest peak, down from 42.7 million doses per day on August 4 to 35.8 million*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.55 billion vaccinated individuals worldwide (1+ dose; 32.7% of the global population) and 1.92 billion who are fully vaccinated (24.6% of the global population). We expect the global total to surpass one-third of the population with 1+ dose and one-quarter with full vaccination in the next week.
*The average doses administered may exhibit a sharp decrease for the most recent data, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reported 37.8 million cumulative COVID-19 cases and 626,833 deaths. Daily incidence continues to increase, surpassing 140,000 new cases per day, the highest average since January 30. After reaching a low of 11,653 new cases per day on June 18, the current surge is more than 50% of the way back to the United States’ highest peak—254,111 on January 10. Daily incidence continues to taper off, however, and if the trend continues on this trajectory, we expect the surge to peak in the next several weeks. Daily mortality continues to increase as well, up to 745 deaths per day, the highest average since March 22*. The current average is now higher than it was during the lull between the summer 2020 and winter 2020 surges.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the averages reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 363.3 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to increase slowly, up to more than 730,000 doses per day*. Now that the US FDA has issued full approval for the Pfizer-BioNTech vaccine, we will monitor vaccination trends closely to see if there is any associated increase in vaccinations. On August 17, the US surpassed 200 million cumulative vaccinated individuals (1+ dose). The total is now up to 201.7 million, equivalent to 60.8% of the entire US population. Among adults, 73.1% have received at least 1 dose, as well as 12.9 million adolescents aged 12-17 years. The US also surpassed 50 million vaccinated (1+ dose) adults aged 65 years and older, equivalent to 91.4% of that age group. A total of 171.1 million individuals are fully vaccinated, which corresponds to 51.5% of the total population. Approximately 62.5% of adults are fully vaccinated, as well as 9.7 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US FDA APPROVAL FOR PFIZER-BIONTECH VACCINE The US FDA on August 23 granted full approval to Pfizer-BioNTech’s 2-dose SARS-CoV-2 vaccine, which will be marketed as Comirnaty, for the prevention of COVID-19 disease among individuals aged 16 and older. The US regulator’s approval of the vaccine places it on par with other marketed vaccines, possibly reassuring some who have been hesitant to receive the shots, and opens the door for employers and other entities to mandate vaccination. In a statement, FDA Acting Commissioner Dr. Janet Woodcock said the vaccine, the first for SARS-CoV-2 to receive full regulatory approval, “meets the high standards for safety, effectiveness, and manufacturing quality the FDA requires of an approved product.” Notably, the FDA’s approval came only 97 days after Pfizer-BioNTech finished filing its 360,000-page biologic license application, about two-fifths the usual time for such an evaluation. Despite the speedy approval, the agency assured that it kept with its “existing high standards for vaccines in the US.” Regulators are reviewing Moderna’s application for full approval of its SARS-CoV-2 vaccine, and J&J-Janssen is expected to submit its application soon.
The Pfizer-BioNTech vaccine will continue to be available under an emergency use authorization for 12- to 15-year-olds until the company files for full approval for that age group. Usually, physicians can prescribe FDA-approved products for “off-label” purposes, for reasons other than their original intent. However, the FDA and the American Academy of Pediatrics warned against such use for children under age 12. Pfizer said it expects results from studies involving younger children, ages 5 to 11, to be available by the end of September. Additionally, the FDA reminded doctors that third, or “booster,” doses of the Pfizer-BioNTech and Moderna vaccines have only been authorized for people with compromised immune systems, not for the general population, and strongly recommended against providing them until agency regulators can review whether they are safe and effective and the CDC makes a recommendation. More than 92 million people in the US have been fully vaccinated using the Pfizer-BioNTech vaccine.
VACCINE MANDATES The US FDA’s approval of the Pfizer-BioNTech SARS-CoV-2 vaccine, which comes amid a fourth pandemic wave fueled by the highly transmissible Delta variant, spurred a string of vaccination requirement announcements by corporations, universities, hospitals, and other organizations. In an address on the vaccine’s approval, US President Joe Biden called on more employers and state and local officials to implement mandates, saying, “Do what I did last month. Require your employees to get vaccinated or face strict requirements.” In late July, President Biden implemented requirements for all federal workers to be vaccinated or face regular testing, social distancing, mask wearing, and limits on official travel. A recent survey from the National Association for Business Economics showed 79% of the group’s members favor vaccine requirements for workers before they return to the workplace, and the US Chamber of Commerce also has expressed its support for vaccine requirements or weekly testing.
Shortly after the FDA’s announcement on August 23, several entities announced vaccine requirements:
• The US Department of Defense will mandate SARS-CoV-2 vaccination for all military service members now that a vaccine has full approval, with a timeline to be provided in the coming days.
• In New York City, Mayor Bill DeBlasio announced all of the city’s public school teachers and staff must be vaccinated with at least one dose by September 27, with no option to choose weekly testing. The decree affects about 148,000 employees, as well as contractors, of the New York City Department of Education. At least 2 large city workers’ groups are expected to file labor complaints or take legal action.
• In New Jersey, Governor Phil Murphy said all employees of any school in the state, including public and private, will be required to be fully vaccinated by October 18 or be tested once or twice weekly “at a minimum.”
• Several major US energy companies—including Chevron Corporation, Valero Energy Corporation, Pioneer Natural Resources, Schlumberger, and Hess—announced they will require vaccinations for at least some of their employees, several as a condition of employment.
• Pharmacy chain CVS Health is requiring its pharmacists to be fully vaccinated by November 30, while all other employees who interact with patients and corporate staff must be vaccinated by October 31.
• Announcing an agreement with unions representing more than 30,000 employees, Disney World will require workers to get the shots by October 22.
• The University of Minnesota System announced the SARS-CoV-2 vaccine will be added to its list of mandatory immunizations for its 60,000 students. The Louisiana State University, University of Louisiana and Southern University systems and the State University of New York system all announced vaccines will be mandatory for students after previously saying they would require the shots once the FDA granted final approval.
• At least 145 hospitals and health systems nationwide will require the shots for their employees now that the Pfizer-BioNTech vaccine is approved.
More mandates are expected, as some say they might be the only way to significantly increase vaccination rates amid continued hesitancy. A recent Kaiser Family Foundation poll showed that 3 out of 10 unvaccinated people indicated they would be more likely to get a vaccine if it were FDA-approved. However, whether full approval spurs the approximately 85 million unvaccinated but eligible US residents to get the shots remains to be seen.
HEALTHCARE WORKER RESILIENCY As the Delta variant drives surges in new COVID-19 cases across the US, the nation’s hospitals are overwhelmed. Some hospitals have reported emergency departments with wait times up to 30 hours, dwindling intensive care unit (ICU) capacity, and unstaffed beds due to staffing shortages. Frontline healthcare workers are facing burnout and frustration over unvaccinated patients, who represent the sickest and most likely to die due to COVID-19. Their perseverance through the 3 previous surges is turning to distress during this fourth wave. However exhausted, hospital staff continue to treat people with COVID-19, but say they are disturbed over the rising number of advanced cases among young people and the unvaccinated. Doctors say this surge could have been avoided if more people were vaccinated and continued following preventive measures such as masking and physically distancing. One infectious disease specialist at the University of North Carolina likened going to work to “watching the same house burn down time and time again.” The mental health harm to healthcare workers who must watch people die who likely would not have had they been vaccinated is difficult to quantify, but the relentless nature of the pandemic will no doubt have long-term impacts on medical care in the US.
US NURSING SHORTAGE Nursing shortages in the US are not new, but the COVID-19 pandemic has exacerbated the problem, testing the physical and mental health of the nation’s nurses as patients flood emergency departments and fill hospital beds amid a fourth surge of cases driven by the Delta variant. More than a year and a half into the pandemic, myriad nurses have retired, made career shifts, taken higher paying jobs with staffing agencies or hospitals with more resources, or simply walked off the job, increasing staffing shortages and contributing to burnout among all healthcare workers. Nurses also say they are angered that many people—in the general public and among their ranks—refuse to get vaccinated or wear masks. Additionally, more than 1,200 nurses have died of COVID-19.
The staffing shortages are impacting care not only for COVID-19 patients but also others who need urgent medical care because of increased emergency room wait times, postponed surgeries, and, in some cases, an inability to provide adequate care due to the time and attention needed for COVID-19 patients. According to analysis from The New York Times, 1 in 5 intensive care units nationwide is at 95% capacity, a level at which experts say it is difficult to maintain minimum care standards. Various states across the country—including Georgia, Texas, South Dakota, Arkansas, and South Carolina, among others—have said nursing shortages have worsened during the pandemic. Officials indicate that finding ways to recruit, hire, and keep nurses are the main problems, with some hospitals noting they could increase bed capacity with sufficient nursing staff. Many experts fear the nursing shortage will worsen as the pandemic continues to deepen burnout.
IVERMECTIN WARNING: YOU ARE NOT A HORSE Over the weekend, the US FDA renewed its warning that the anti-parasitic animal drug ivermectin should not be used to treat or prevent SARS-CoV-2 infection in humans. The FDA’s message appeared on Twitter with the statement “You are not a horse. You are not a cow. Seriously, y'all. Stop it.” The tweet linked to the agency’s previous statement posted in March 2021. The reiterated warning came a day after the Mississippi State Department of Health issued an alert warning people against using the drug. Ivermectin is commonly used to prevent heartworm and other parasites in animals, and the drug is FDA-approved to treat humans with intestinal complications caused by parasitic worms and for topical use for conditions such as head lice and rosacea. However, ivermectin is not approved for nor recommended by the FDA to treat or prevent COVID-19. According to internal US CDC data reviewed by ABC News, distribution of the drug during the first week of August increased 19-fold. If used improperly, ivermectin can cause several potentially serious side effects, including seizures, coma, or death.
BREAKTHROUGH INFECTIONS & TRANSMISSIBILITY There have been growing levels of concern and conversation surrounding “breakthrough infections,” which are confirmed SARS-CoV-2-positive cases in fully vaccinated individuals. While these cases are still comparatively rare among the larger COVID-19 case burden, experts and the public alike are worried about implications for vaccinated individuals. Most of the recorded breakthrough cases are linked to the Delta variant of concern, which is currently responsible for nearly all new cases in the United States. Encouragingly, a small percentage of breakthrough cases have resulted in severe manifestations of COVID-19 that needed hospitalization.
While the primary objective of vaccination—preventing severe COVID-19 or death—seems to be holding against the Delta variant, the secondary goal of preventing person-to-person transmission may not be as strong against Delta infections as for other variants or wild-type SARS-CoV-2. Some preliminary studies have found that vaccinated individuals with breakthrough infections can exhibit similar viral loads (measured in PCR Ct values) as those in infected unvaccinated individuals. While higher viral loads can be correlated with the amount of virus shed during normal person-to-person interactions, another preprint study found that high viral load did not necessarily result in shed infectious viral particles. More research is needed to understand the risk of transmission from breakthrough cases to both vaccinated and unvaccinated persons and to understand the viral dynamics in the immune systems of vaccinated individuals. Experts maintain that, given the current evidence, vaccination remains the best tool in defeating SARS-CoV-2 and the Delta variant surge.
SARS-COV-2 HOUSEHOLD TRANSMISSION A study published last week in the Journal of the American Medical Association (JAMA) found that younger children are more likely to transmit SARS-CoV-2 to other household members than older adolescents. Between June 1 and December 31, 2020, researchers in Ontario, Canada, conducted a population-based cohort study involving 6,280 households that had one index case of confirmed SARS-CoV-2 infection in a member younger than 18 years old. The mean age of the children with COVID-19 was 10.7 years, and 45.6% were female. Of the total households, secondary transmission occurred in 27.3% of households. According to the researchers, children aged 0 to 3 years had the highest odds of transmitting SARS-CoV-2 to other household members when compared with older children aged 14 to 17 years (odds ratio [OR], 1.43; 95% confidence interval [CI], 1.17-1.75). Additionally, children aged 4 to 8 years and 9 to 13 years also had increased odds of transmission when compared with older children (aged 4-8 years: OR, 1.40; 95% CI, 1.18-1.67; aged 9-13 years: OR, 1.13; 95% CI, 0.97-1.32).
Household settings may aid SARS-CoV-2 transmission due to poor or limited ventilation, shared spaces or materials, and frequent close contact with household members. Additionally, it is often challenging to implement non-pharmaceutical interventions such as physical distancing or mask wearing within homes. Experts note that children are more likely to be underdiagnosed for COVID-19 because many have asymptomatic or mildly symptomatic cases. As children return to school amid a surge driven by the highly transmissible Delta variant, parents are concerned about the potential for household transmission. The study’s findings have implications for infection prevention within households, schools, and daycares, especially those with infants and toddlers who appear to have the highest infectivity. The researchers note that further research is required to determine the differences in viral shedding and presentation of symptoms among age groups in order to better prevent secondary transmission in these settings. In an editorial in the same JAMA issue, scientists from the University of Pennsylvania said vaccination for eligible household members should help alleviate fears of SARS-CoV-2 secondary transmission from infected children.
FLORIDA OXYGEN SHORTAGE Florida’s COVID-19 surge appears to have peaked over the past week in terms of daily incidence, but increasing new hospitalizations and current hospitalizations are placing a major burden on hospital and health system operations, particularly in severely affected areas. On August 20, the Orlando Utilities Commission (OUC) and Orlando Mayor Buddy Dyer requested that customers limit water use, particularly for watering lawns and washing cars, in order to conserve liquid oxygen to support local health systems’ COVID-19 responses. Liquid oxygen is used to treat the city’s potable water—”to remove the slight discoloration and rotten-egg smell that is found naturally in Florida's water supply”—and OUC typically consumes 10 trucks of liquid oxygen per week. The company is aiming to reduce its liquid oxygen consumption by 25-50% in order to divert the remainder to hospitals that are struggling to meet the demand due to the COVID-19 patient surge. As we covered previously, high-flow oxygen therapy has emerged as a primary clinical treatment option for severe COVID-19 patients, and hospitals, cities, and countries have faced major challenges securing sufficient oxygen supply during major surges. The OUC request indicates that customers should expect the conservation efforts to last at least 2 weeks.
AVERTED DEATHS Researchers from Indiana University (US) and the RAND Corporation published findings from their analysis on the impact of early SARS-CoV-2 vaccinations in the US. The study, published in Health Affairs, included data on state-level weekly vaccination rates and COVID-19 mortality during the first 5 months that SARS-CoV-2 vaccines were available to the public. The researchers developed a series of multivariate regression models to identify any associated effects on COVID-19 mortality that accounted for state-level variations in state policies and environments as well as the anticipated lag between vaccine administration and any effects on mortality.
The researchers observed a significant association between higher vaccination rates and decreasing mortality across all states, although the magnitude of the benefit varied from state to state. On average, states exhibited a decrease in the expected COVID-19 mortality of 5 deaths per 100,000 population, equivalent to nearly 140,000 averted deaths nationally over the study period. At the state level, the decreased mortality ranged from Hawai’i with 1.1 fewer deaths per 100k to New York with 11.7. Not surprisingly, the effect of vaccination increased over time, as individuals received their second doses and developed the full protective immune response. The impact of vaccination began to increase noticeably starting in early-to-mid February. Notably, vaccine availability was limited to priority populations during most of the period from December 2020-May 2021; however, this period does cover the majority of the initial wave of vaccinations in the US.
ORIGINS OF NOVEL PATHOGENS The WHO on August 20 issued a call for experts to join its new Scientific Advisory Group for the Origins of Novel Pathogens (SAGO), which will advise the UN health agency on technical and scientific considerations regarding the origins of emerging and re-emerging pathogens capable of causing epidemics or pandemics. The group also will guide the WHO on next steps for investigating the origins of SARS-CoV-2. The multidisciplinary effort is an attempt to depoliticize future investigations into disease origins by creating a global framework for conducting scientific-based studies and data-driven efforts to better predict, detect, prevent, and respond to future outbreaks. SAGO, which will include 25 experts from various fields and with different technical skills, is expected to hold its first meeting virtually in late September or early October.
BOTSWANA VACCINATION With 52 African countries rolling out SARS-CoV-2 vaccination campaigns, lessons from the challenges and successes in each country will help other nations learn about how to implement their own vaccine rollouts. Botswana, along with 3 other African nations, has completed an intra-action review (IAR) of its early vaccine rollout with support from the WHO. According to Dr. Malebogo Kebabonye, Director of Health Services at the country’s Ministry of Health and Wellness, having a National Vaccine Deployment Plan with multi-sectoral involvement and coordination in place before receiving the first shipment of vaccines helped communities take ownership and improve acceptance of vaccines. Additionally, solid financing and monitoring and evaluation tools helped strengthen Botswana’s initial vaccine rollout. However, Dr. Kebabonye noted that tightening supplies of SARS-CoV-2 vaccines and healthcare worker shortages contributed to increased distrust about the rollout, with misinformation spread on- and offline. She urged other countries to take incremental and agile approaches to vaccine rollouts, with emphasis on testing and learning. Chanda Chikwanda, Lead of WHO Africa’s Vaccines Learning Agenda, urged other countries in the region to plan for multiple scenarios and conduct IARs. Nine (9) other African countries have expressed interest in completing IARs.
VARIANT VACCINE The Coalition for Epidemic Preparedness Innovations (CEPI) last week announced it will provide up to US$20.6 million to Gritstone bio, Inc. to support the development of a “next-generation” SARS-CoV-2 vaccine. The funding—part of CEPI’s larger portfolio supporting next-generation vaccine development—will be used for a Phase 1 clinical trial of a self-amplifying mRNA vaccine candidate. A self-amplifying approach could provide a single-shot, low-dose vaccine that would elicit immune responses to specific antigens. As new SARS-CoV-2 variants emerge, novel antigens could be rapidly switched out in the vaccine, so variant-specific versions could be ready for production in about 1 month. Gritstone’s vaccine candidate might also produce T-cell immune responses against non-spike protein gene fragments, which potentially could provide more broad protection against various SARS-CoV-2 strains.
DNA VACCINE India’s drug regulator last week granted emergency use approval for the world’s first DNA platform SARS-CoV-2 vaccine for people ages 12 and older. Zydus Cadila’s 3-dose ZyCoV-D vaccine uses a piece of genetic material from the SARS-CoV-2 virus to help the body’s immune system recognize and respond to the virus if exposed. The company claims the vaccine has 66.6% efficacy against symptomatic COVID-19, but no safety, immunogenicity, nor efficacy data supporting the claims are available publicly, either published or preprint. This is the second time the Indian government has authorized a domestically produced vaccine without Phase 3 trial data. The first was Bharat Biotech’s Covaxin, authorized in January 2021. Some experts called on the company and the Indian government to provide more publicly available data to improve transparency.
by ponchi101 Stephen Smith had a good one: "You are not a horse, you are not a cow" (quoting the FDA). Punchline: "You are a jackass".
---0---
The paragraph about nurses is also worrisome. I know how that one ends: "bilingual nurses in S. America required. Immediate availability, good better pay than back home. No questions asked. Applications at your nearest US Embassy".
by JazzNU Two of the largest universities in the country. Cowardly to have waited, they were on firm legal ground to set a requirement before now, but better late than never.
by Suliso Daily covid hospital entries per 1 million inhabitants in Switzerland (14 day rolling average) since July 1st. Green: fully vaccinated, purple: not vaccinated or partially vaccinated.
by dryrunguy No words.
by JazzNU This is the FDA's plea from last week if you missed it
by atlpam I know someone who had Ivermectin prescribed for him when he had Covid (at least he didn't buy it from a feed store) - it tore his digestive system up. Unbelievable that the same people who are against the vaccine because they want to build up "natural" immunity are willing to take unproven, experimental treatments when they get sick.
by ti-amie
atlpam wrote: ↑Wed Aug 25, 2021 8:33 pm
I know someone who had Ivermectin prescribed for him when he had Covid (at least he didn't buy it from a feed store) - it tore his digestive system up. Unbelievable that the same people who are against the vaccine because they want to build up "natural" immunity are willing to take unproven, experimental treatments when they get sick.
Not only unproven and experimental but not meant for consumption by humans! It makes no sense.
by ti-amie North Carolina checking in.
Via Wiki:
The Research Triangle, or simply The Triangle, are both common nicknames for a metropolitan area in the Piedmont region of North Carolina in the United States, anchored by three major research universities: North Carolina State University, Duke University, and University of North Carolina at Chapel Hill, located in the cities of Raleigh and Durham and the town of Chapel Hill, respectively. The nine-county region, officially named the Raleigh–Durham–Cary combined statistical area (CSA), comprises the Raleigh–Cary and Durham–Chapel Hill Metropolitan Statistical Areas and the Henderson Micropolitan Statistical Area.
by dryrunguy Just to clarify, certain forms of ivermectin at certain doses are routinely used to treat human diseases. It's a common agent used to treat lice in humans. It's also commonly used to treat worms in children. So it does have appropriate medical applications for humans--but only in certain forms and at certain doses. And of course, only under the supervision of a medical professional.
The reason why it has been such a popular wormer for livestock is because it is one of the few medications that treats both internal AND external parasites. Most livestock wormers only treat internal parasites or certain types of internal parasites. This is also how so many internal parasites have over time developed immunity to ivermectin, so it is not as effective as it used to be. And I am not aware of any other dual-purpose livestock de-wormer emerging in the market or even in development.
Anyway, where people seem to get confused is not being able to distinguish between anti-parasitic and anti-viral. (My boss equaled the two in a conversation this afternoon after I politely asked if she had taken ivermectin off her shopping list. She wasn't pleased. I should probably mind my manners since we're currently in the performance review period of the year.) Anti-parasitic and anti-viral are anything BUT interchangeable terms.
by ponchi101 We are still in societies that do NOT understand that antibiotics are worthless against viruses, and you are expecting people to understand the differences between ant-parasitic and anti-viral.
Time to expand that chapter in my book about people not understanding science...
by JazzNU
dryrunguy wrote: ↑Wed Aug 25, 2021 9:26 pm
Anyway, where people seem to get confused is not being able to distinguish between anti-parasitic and anti-viral. (My boss equaled the two in a conversation this afternoon after I politely asked if she had taken ivermectin off her shopping list. She wasn't pleased. I should probably mind my manners since we're currently in the performance review period of the year.) Anti-parasitic and anti-viral are anything BUT interchangeable terms.
I highly approve. They can't function with out you, who are they kidding? You're more than safe.
by ti-amie This is where we are as a country.
by ponchi101 6 months? In a medium security facility?
Nah, he must be home by now. It is Florida.
by dryrunguy Here's the latest Situation Report. It's absolutely packed. As more employers require employees to be vaccinated, Delta Airlines is taking a different approach. Be sure to check that out. Also, the Sturges Bike Rally has struck again. And this time, it's the locals who are bearing the brunt of it.
Meanwhile, the section on the J&J booster data was particularly interesting to me since I received the J&J vaccine. Looks like I should be eligible for my booster around December 22 if these data hold up.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 214.5 million cumulative cases and 4.47 million deaths worldwide as of August 27. If global mortality continues on this trajectory, we expect to surpass 4.5 million cumulative deaths in the next 3-4 days.
Global Vaccination
The WHO reported 4.95 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of August 25. A total of 1.90 billion individuals have received at least 1 dose, and 1.13 billion are fully vaccinated. Analysis from Our World in Data indicates that the global daily doses administered has held relatively steady over the past 2 weeks at approximately 36 million doses per day*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 2.59 billion vaccinated individuals worldwide (1+ dose; 33.0% of the global population) and 1.96 billion who are fully vaccinated (24.9% of the global population). We expect to surpass one-third of the global population with 1+ dose and one-quarter with full vaccination by early next week.
*The average doses administered may exhibit a sharp decrease for the most recent data particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
As global vaccination efforts continue, enormous disparities remain in terms of access and coverage. African countries, in particular, are still struggling to secure sufficient vaccine supply, which is severely hindering vaccination efforts across the continent. In fact, just 10 countries account for nearly 75% of the 5 billion cumulative doses administered globally, including 6 that have each administered more doses than the entire continent of Africa. Africa represents approximately 17.5% of the global population but only 1.9% of the cumulative doses administered.
Daily vaccinations are increasing in Africa, but overall vaccination coverage remains low, with many African countries among the lowest globally. Notably, of the 52 countries reporting partial vaccination coverage (1+ dose) less than 10%, 40 are in Africa**. Additionally, the average across the continent is only 4.6%, the lowest among all continents by a factor of more than 7. Only Seychelles (75%) and Mauritius (62%) are reporting partial coverage greater than 50%, and only 3 others—Morocco (47%), Cabo Verde (38%), and Tunisia (30%)—are reporting more than 20%.
**Data are unavailable for Burundi and Eritrea.
Similarly, among 73 countries reporting fewer than 0.2 daily doses administered per 100 population, 41 are in Africa. The average for Africa as a whole is 0.11 doses per day per 100 population, the lowest among all continents by nearly a factor of 3. In terms of total daily vaccinations, Africa is beginning to approach North America—1.52 million doses per day, compared to 1.89 million. Africa’s current average daily vaccinations is more than 3.5 times its average on July 1 and more than double its average on August 1. The trend continues to increase exponentially, which is a positive sign.
A number of African countries are exhibiting substantial increases in their daily vaccinations. In total, 10 African countries reported increases in daily vaccinations of more than 500% since July 1, including 5 that increased more than 1,000%. Gambia’s average increased 2,539%; Rwanda’s increased 2,637%, and Malawi’s increased 2,882% over that period. While most African countries reported extremely low daily vaccinations as of July 1—on the order of 1,000 doses per day or fewer—this is not necessarily the case for all African countries. For example, Morocco averaged more than 100,000 doses per day on July 1, and its average increased to more than 350,000 doses per day (+243%) since then. And Egypt’s average increased from nearly 28,000 to nearly 170,000 (+510%).
The increasing trends in daily vaccinations across Africa are encouraging; however, supply volume remains a major constraint. This is particularly concerning in light of recent decisions by a number of higher-income countries, including the US, to begin administering additional booster doses to some or all fully vaccinated individuals. Existing global production capacity has still not caught up with demand, and any doses allocated as extra boosters inherently take away from doses that could be allocated to low- and middle-income countries (LMICs).
UNITED STATES
The US CDC reported 38.3 million cumulative COVID-19 cases and 631,440 deaths. Daily incidence continues to increase, up to 142,006 new cases per day, the highest average since January 30. Daily incidence continues to taper off, however, and if the trend continues on this trajectory, we expect the surge to peak in the next several weeks. Daily mortality continues to increase as well, up to 864 deaths per day, the highest average since March 16*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 365.8 million cumulative doses of SARS-CoV-2 vaccines, and daily vaccinations continue to increase slowly, up to 783,239 doses per day*. There are 203.0 million individuals who have received at least 1 dose, equivalent to 61.1% of the entire US population. Among adults, 73.5% have received at least 1 dose, as well as 13.1 million adolescents aged 12-17 years. A total of 172.2 million individuals are fully vaccinated, which corresponds to 51.9% of the total population. Approximately 62.8% of adults are fully vaccinated, as well as 9.9 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
J&J-JANSSEN SECOND DOSE On August 25, J&J-Janssen announced it has interim data showing a second shot of its SARS-CoV-2 vaccine administered 6 to 8 months after the initial dose generates “a rapid and robust increase in spike-binding antibodies,” up to 9-fold higher after 28 days than a single shot. The data—which have not been published in a scientific journal nor peer reviewed—come from 2 Phase 1/2a studies conducted in the US and Europe. The company plans to submit the data to the US FDA in the hopes of receiving authorization for a booster dose and indicated it is in talks with the FDA, US CDC, European Medicines Agency (EMA), and other health authorities regarding the need for second doses of its vaccine. The company also is testing a 2-dose regimen delivered 2 months apart, with data from that clinical trial expected in the next few weeks.
As we covered previously, US health officials have announced plans to begin providing third doses of the mRNA vaccines made by Moderna and Pfizer-BioNTech as soon as mid-September and have indicated boosters likely will be necessary for recipients of the J&J-Janssen vaccine. Initially, officials said the extra doses would be available for people who finished their regimen 8 months prior but now are looking at a 6-month gap instead, perhaps in part because of the J&J-Janssen data. Currently, only people with compromised immune systems are eligible for booster doses in the US.
Pfizer-BioNTech announced on August 25 that it plans to complete an application to the FDA for a third dose of its vaccine by the end of this week. The company received full approval of its vaccine, called Comirnaty, earlier this week. The CDC’s Advisory Committee on Immunization Practices is expected to meet next week and will discuss a framework for SARS-CoV-2 booster doses. While several studies show a higher level of antibody production in extra-dose recipients, it remains unclear whether this will translate to improved protection against SARS-CoV-2 infection or severe COVID-19 disease.
MODERNA FDA APPLICATION Moderna on August 25 completed its submission of a Biologics License Application to the US FDA for full approval of its SARS-CoV-2 vaccine to prevent COVID-19 in people aged 18 or older. The company requested priority review designation, meaning the FDA would have until the end of February to make a decision if it grants the designation. If approved, the vaccine would be the second for the prevention of COVID-19 after the FDA granted full approval to Pfizer-BioNTech on August 23. The agency’s review process for the Pfizer-BioNTech vaccine took 97 days, 40% of the normal time for such a submission, and it is expected regulators will take at least 3 months to review Moderna’s application. Moderna also has filed for emergency use authorization for its vaccine to be used in adolescents aged 12 and older.
VACCINE EFFECTIVENESS Researchers are collecting more proof that protection provided by SARS-CoV-2 vaccines is waning over time. In a study published this week in the US CDC’s Morbidity and Mortality Weekly Report (MMWR), researchers with the HEROES-RECOVER initiative—a US network of longitudinal cohorts including more than 4,000 healthcare workers, first responders, and other frontline workers—report that vaccine effectiveness (VE) fell from 91% in mid-December 2020, before the SARS-CoV-2 Delta variant was predominant, to 66% by mid-August following Delta’s spread. Among participants, 83% were vaccinated, with 65% having received the Pfizer-BioNTech vaccine, 33% Moderna, and 2% J&J-Janssen. The researchers cautioned that while Delta might be more capable of causing breakthrough infections, a reduction in VE could be due to detecting few infections among the cohorts, increasing time since vaccination, an easing of other preventive measures, or a combination of factors. Still, a “sustained two-thirds reduction in infection risk underscores the continued importance and benefits of COVID-19 vaccination,” they write.
In another analysis released on August 25 but not yet published, researchers from the UK’s ZOE COVID Study found a reduction in VE for both the Pfizer-BioNTech and AstraZeneca-Oxford vaccines. The data include more than 1 million self-reported test results among people who received full regimens of either vaccine, as well as test results from more than 75,000 people not yet vaccinated. Protection against infection 1 month after the second dose was 88% for Pfizer-BioNTech and 77% for AstraZeneca-Oxford, prior to the Delta variant’s predominance, but fell to 74% and 67%, respectively, after 4-5 months and after Delta spread throughout the UK. The researchers noted that more data on younger people are needed, as those who were vaccinated in the winter and spring were primarily older individuals.
In yet another study published this week in the MMWR, the CDC presented data from Los Angeles County, California (US), showing unvaccinated individuals were 5 times more likely to get COVID-19 than their vaccinated counterparts, and 29 times more likely to be hospitalized with the disease. These analyses add evidence that VE does appear to be waning over time and in the face of the highly transmissible Delta variant, but they also underscore the importance of vaccination in preventing infection, hospitalization, and serious disease. Still, more effort is needed to collect data on breakthrough infections among vaccinated people, with several officials familiar with the situation alleging the CDC is using “outdated and unreliable data,” Politico reports.
HEART INFLAMMATION The Pfizer-BioNTech SARS-CoV-2 vaccine is associated with an increased risk of myocarditis (inflammation of the heart muscle), but infection with the virus is associated with a much greater risk of the condition, according to a real-world case-control study published on August 25 in the New England Journal of Medicine. Researchers analyzed the health records of more than 2 million people who are members of the Clalit Health Services (CHS), the largest healthcare organization in Israel. Vaccination was associated with a 3-fold increase in the risk of myocarditis (risk ratio [RR], 3.24, 95% confidence interval [CI], 1.55-12.44), as well as several other conditions including swollen lymph nodes (RR, 2.43; 95% CI, 2.05 to 2.78), appendicitis (RR, 1.40; 95% CI, 1.02 to 2.01), and herpes zoster infection (RR, 1.43; 95% CI, 1.20 to 1.73). In a separate cohort, the researchers found SARS-CoV-2 infection is associated with an 18-fold increased risk of myocarditis (RR, 18.28; 95% CI, 3.95 to 25.12), as well as an increased risk of several other serious adverse events such as pericarditis (inflammation of tissue surrounding the heart), irregular heartbeat, blood clots, heart attack, bleeding in the brain, and kidney damage. Pfizer-BioNTech and the US CDC are conducting studies to examine the risks of myocarditis and pericarditis among people who receive the vaccine.
SARS-COV-2 ORIGINS The US Intelligence Community on August 24 delivered a classified report to US President Joe Biden that made no conclusions about the origins of the novel coronavirus, including whether the virus was transmitted to humans naturally through an animal vector or if human transmission was the result of a laboratory mishap. The report, some of which is expected to be declassified in the coming days, is the result of an order from President Biden given in late May for the Intelligence Community to provide another, more thorough assessment of the origins of SARS-CoV-2 within 90 days. The report’s lack of conclusions prompted calls from global health experts, scientists, and politicians for a more urgent international effort to find the source of the pandemic in order to inform future pandemic preparedness. According to The Wall Street Journal, 2 senior US officials said a lack of cooperation from China, where the virus is assumed to have originated, hampered the US investigation.
A lack of Chinese cooperation also challenged a WHO-convened joint WHO-China delegation’s investigation in early 2021, culminating in a March report that concluded a lab leak was “extremely unlikely.” However, WHO Director-General Dr. Tedros Adhanom Ghebreyesus later undercut the team's statement, saying there is not enough evidence to support any conclusion. WHO officials reiterated that stance this week, saying all of the origin hypotheses “are still on the table.” Then, on August 25, the independent international members of the WHO-China team published a detailed piece in the journal Nature, outlining their review process and calling for an expedited second phase of investigation, noting the search is “at a critical juncture.”
On the same day, Chinese officials urged any future investigations to be broadened, possibly to other countries; refused to take blame for stalled efforts; and said the country will continue to participate in “science-based origin tracing efforts.” Chinese officials also accused the US of politicizing the investigation and attempted to shift blame, once again suggesting without evidence that the virus possibly escaped an US Army research facility. The Chinese embassy in Washington, DC, and China’s envoy to the United Nations this week publicly called for investigations into US labs. While understanding the origins of the COVID-19 pandemic is a global priority, the likelihood of quickly finding evidence grounded in science is slim, especially without full and transparent cooperation from Chinese authorities.
GLOBAL VACCINE ACCESS The WHO this week again called for wealthier nations with higher SARS-CoV-2 vaccination rates to delay the deployment of booster doses for 2 months and instead donate those doses to countries with much lower coverage. WHO Director-General Dr. Tedros Adhanom Ghebreyesus expressed disappointment at the scope of vaccine donations worldwide, saying “vaccine injustice and vaccine nationalism” raise the likelihood of new, possibly more deadly SARS-CoV-2 variants emerging as the virus continues to circulate. Dr. Tedros noted that 75% of the 5 billion vaccine doses distributed globally have gone to only 10 countries. Overall, donations from wealthier nations have not reached the level required to provide the 11 billion doses needed to vaccinate 70% of the world’s population.
And now, several countries—including the US, Israel, France, Hungary, and others—have or are planning to implement booster dose programs. For its part, UK scientists are looking into using smaller, fractional doses for boosters, which, in theory, could help increase supplies for other parts of the world if the “extra” amounts were distributed internationally. But countries are running into another issue: a surplus of expiring doses. The 6-month shelf life provided to most SARS-CoV-2 vaccines under emergency authorizations is rapidly approaching and threatens to undermine donations of unused doses, as vaccines close to expiration raise suspicion in many countries, potentially increasing vaccine hesitancy. Some nations are publicly destroying expired vaccines to “stay accountable,” even though most experts agree the doses, if stored properly, could be viable for up to 2 years. While some countries have extended the shelf lives for authorized vaccines based on stability studies, others remain skeptical.
The US so far has donated more than 120 million doses to 80 countries and provided US$4 billion in funding and other resources to the COVAX facility, he noted. While the US has pledged to donate another approximately 500 million doses, as well as made efforts to expand manufacturing domestically and overseas, global health advocates and some members of the US Congress are calling on the US President Joe Biden to do more. An analysis from PrEP4All, an AIDS advocacy organization, criticizes the Biden administration for spending less than 1% of US$16 billion included in the American Rescue Plan meant for procuring and manufacturing COVID-19 treatments, vaccines, diagnostics, and other tools for distribution in other countries. The group, along with others, called on the US government to immediately scale up vaccine production to improve global supply.
In Africa, only 2.5% of the population is fully vaccinated. In an interview on CNBC this week, African Development Bank (ADB) President Akinwumi Adesina said the continent had been “shortchanged” in regard to vaccine access and that “Africa should not depend on the rest of the world for supplying it with critical vaccines and also therapeutics.” In an effort to improve self-sufficiency, Adesina said the ADB plans to invest at least US$3 billion in health care infrastructure and the pharmaceutical sector across the continent.
EVICTION MORATORIUM On August 26, the US Supreme Court granted a request to lift a US CDC moratorium on evictions, ending the measure meant to keep millions of people who owe back rent housed during the latest surge of the COVID-19 pandemic. In an unsigned, 8-page majority opinion, the court said the CDC exceeded its authority, relying “on a decades-old statute that authorizes it to implement measures like fumigation and pest extermination.” If a federal eviction moratorium is to continue, the US Congress must authorize it, the court said. However, Congress failed to do so when the last moratorium expired on July 31. Justices Stephen Breyer, Sonia Sotomayor, and Elena Kagan dissented from the majority opinion, saying the moratorium should remain in place in the midst of a public health crisis and calling on the court to hold a full briefing and arguments. In a statement, White House Spokesperson Jen Psaki said US President Joe Biden “is once again calling on all entities that can prevent evictions—from cities and states to local courts, landlords, Cabinet Agencies—to urgently act to prevent evictions.”
US MASK MANDATE BANS States across the country have begun the transition into a new, in-person school year. In last week’s COVID-19 briefing, we covered a number of states that were requiring masks and vaccinations for eligible students in an effort to minimize the spread and impact of COVID-19. This week, Illinois joined several states, ordering a mask mandate for students and vaccinations for students aged 16 and older. While many states have adopted this approach for the new school year, several states have gone in opposite directions, banning schools’ abilities to mandate mask wearing. In Florida, 10 school districts have fought back against a mask mandate ban from Florida Governor Ron DeSantis, facing potential backlash, including funding freezes, for violating the state-sanctioned ban. In South Carolina, the American Civil Liberties Union (ACLU) filed a new lawsuit challenging South Carolina’s ban on mask mandates in schools. The lawsuit was driven by a number of parents who have school-aged children with risk factors that could lead to more severe COVID-19 cases. The case for masks in schools has federal support, as many policymakers worry about the health and safety of children and the potential for school-based cases to drive up disease incidence. Although only 19 states have gone back to school these past few weeks, 90,000 children already have entered quarantine or isolation following contact with a COVID-19 case. It will be critical to monitor school-based COVID-19 outbreaks as more parts of the country return to the classroom.
INSURANCE SURCHARGE Following the US FDA’s approval of the Pfizer-BioNTech SARS-CoV-2 vaccine, many employers implemented vaccination mandates, but one large US company is taking a different tack. Beginning November 1, Delta Air Lines will charge employees an additional $200 per month to remain enrolled in the company’s health plan if they refuse to be fully vaccinated for SARS-CoV-2. Additionally, unvaccinated employees are required to wear masks in all indoor company settings, will no longer qualify for pay protection if they are diagnosed with COVID-19, and will be required to take weekly tests beginning September 12. In a memo to staff, Delta CEO Ed Bastian noted that 75% of the company’s employees are fully vaccinated but expressed a desire to get “as close to 100% as possible.” Delta said the surcharge is necessary to cover the financial risk unvaccinated employees pose to the company, citing the average cost of a COVID-19-related hospital stay is $50,000. The airline is self-insured and sets its own premiums for its health plans, which are administered by UnitedHealthcare. Delta also requires new employees to be vaccinated.
United Airlines is the only major airline so far to require all of its employees to get vaccinated or risk termination, with religious or medical exemptions reviewed on a case-by-case basis.
STURGIS MOTORCYCLE RALLY Last summer, the Sturgis Motorcycle Rally—held annually in Sturgis, South Dakota (US)—was subsequently linked to more than 300 cases of COVID-19 across more than 20 states, including an outbreak in Minnesota that resulted in at least 77 cases linked directly to the event. Despite the ongoing pandemic, the rally was held again this year—August 6-15—largely without any COVID-19 restrictions or protective measures. Reportedly, the 2021 rally was one of the largest in the event’s history, drawing approximately 700,000 visitors. Even though the event ended only 11 days ago, there are already early indications of a major COVID-19 surge in the area. The experience following the 2020 event and the ongoing nationwide surge, driven largely by the highly transmissible Delta variant, should have been sufficient to inspire event and government officials to implement effective COVID-19 protections this year, but unfortunately, that did not happen.
Meade County, SD—where Sturgis is located—averaged fewer than 1 new case per day from late May through late July, before beginning to increase slightly. At the start of the 2021 rally, Meade County averaged 3 new cases per day, but daily incidence surged to 38 as of August 24, nearly a 13-fold increase and a new record for the county. The 86 cases reported in Meade County on August 23-24 accounted for 10% of the state’s total, despite the county only representing 3% of the state’s population. Analysis by The New York Times indicates that COVID-19 hospitalizations have more than tripled over the past 2 weeks. Test positivity surged past 40% (currently 34%), which indicates that testing may not be fully capturing the true scale of community transmission in the area. Considering that 700,000 visitors have returned to their homes across the US, the Sturgis Motorcycle Rally certainly has the potential to be another national-level superspreader event. While we are observing the early signs of a surge in and around Sturgis, it might be months before we could expect to have a clear idea of the extent to which this single event impacts state- and national-level epidemics.
CRUISE LINES Cruise lines are implementing more strict COVID-19 preventive measures, requiring passengers to be vaccinated, wear masks while in public areas aboard the ship, and show proof of a negative test within a few days of boarding, amid a current surge in cases and reports of breakthrough infections among vaccinated staff and passengers. Last week, Carnival Cruise Lines announced 27 COVID-19 cases aboard the Carnival Vista sailing out of Galveston, Texas (US). Most of the cases were among crew, but the one passenger case—a 77-year-old woman from Oklahoma—received medical care on the ship, was hospitalized in Belize, evacuated to her home state, and later died. In a statement, Carnival expressed condolences to the woman’s family and added that she “almost certainly” did not contract the virus onboard the ship.
On August 20, the US CDC updated its guidance for cruise ship travelers, recommending people who are at a higher risk for severe COVID-19 avoid cruises and asking passengers to have both a recent negative SARS-CoV-2 test and proof of vaccination. Additionally, some popular destinations, including the Bahamas, are requiring all cruise ship passengers aged 12 and older be vaccinated in order for ships to dock. This prompted Disney Cruise Line, Royal Caribbean, and Carnival to adopt vaccination requirements for their passengers. Norwegian Cruise Line already requires all eligible passengers to be vaccinated, after the company successfully challenged a Florida law banning companies from demanding proof of vaccination.
IVERMECTIN POISONINGS On August 26, the US CDC issued a Health Alert Network (HAN) advisory in response to a recent surge in poisonings in individuals who attempted to prevent or treat COVID-19 using ivermectin. As we covered previously, ivermectin is approved by the US FDA to treat parasitic infections in humans, but it is primarily used to treat animals, including livestock. The drug is not authorized for use to treat COVID-19, and currently available data do not indicate a treatment benefit for COVID-19. A study of prescriptions filled at retail pharmacies in the US found that the volume of ivermectin prescriptions in January 2021 was more than 10 times greater than the pre-pandemic baseline, and the volume in mid-August 2021 was more than 24 times greater than before the pandemic and still increasing. The CDC also reported that the volume of “veterinary formulations available over the counter but not intended for human use” increased as well.
The American Association of Poison Control Centers confirmed that poison control centers nationwide are fielding an elevated call volume related to the “misuse and overdose” of ivermectin, including veterinary formulations. The volume of poison control center calls related to ivermectin was 3 times higher than the pre-pandemic baseline in January 2021 and 5 times higher in July 2021. Available data also indicate an increase in associated visits to emergency departments and hospitals.
JAPAN The Japanese government recently halted a rollout of 1.6 million doses of the Moderna SARS-CoV-2 vaccine due to worries over contamination. The cause of the contamination has yet to be disclosed, but there were reports of 40 doses with unspecified contaminants found at 8 different vaccination sites across the country. These 40 doses led to the decision to pull the entire lot in addition to 2 other lots made at the same location in Spain. The Takeda Pharmaceutical Company, which is leading the sales and distribution of the vaccine in Japan, said the decision was made as safety precaution and has requested Moderna conduct an emergency investigation. Japan had a slow start to its vaccination campaign, but now 44% of the population is fully vaccinated.
After reading the post that I've quoted here, and then the post below it, I honestly think that people who are outspoken in their contempt for masking and vaccinations should not be given ICU beds. It's just not fair given the circumstances. Once they get one, they are taking it away from someone else for weeks at a time. I'm really sorry for his wife and family, but what about the guy who died needlessly? It's truly hard to fathom.
Kevin
by dryrunguy And to think, we're not even close to grasping the long-term consequences of these people's decisions. Many of them who ultimately survive will experience long COVID and never be able to go back to work.
Then they'll file for disability, maybe even food stamps. After spending their entire adult lives to this point voting to DECIMATE the social safety net for others. I'm only scratching the surface here.
And they'll never even try to get to the bottom of the dissonance of it all. Too dangerous.
by JazzNU
dryrunguy wrote: ↑Fri Aug 27, 2021 5:27 pm
INSURANCE SURCHARGE Following the US FDA’s approval of the Pfizer-BioNTech SARS-CoV-2 vaccine, many employers implemented vaccination mandates, but one large US company is taking a different tack. Beginning November 1, Delta Air Lines will charge employees an additional $200 per month to remain enrolled in the company’s health plan if they refuse to be fully vaccinated for SARS-CoV-2. Additionally, unvaccinated employees are required to wear masks in all indoor company settings, will no longer qualify for pay protection if they are diagnosed with COVID-19, and will be required to take weekly tests beginning September 12. In a memo to staff, Delta CEO Ed Bastian noted that 75% of the company’s employees are fully vaccinated but expressed a desire to get “as close to 100% as possible.” Delta said the surcharge is necessary to cover the financial risk unvaccinated employees pose to the company, citing the average cost of a COVID-19-related hospital stay is $50,000. The airline is self-insured and sets its own premiums for its health plans, which are administered by UnitedHealthcare. Delta also requires new employees to be vaccinated.
I like it Delta Airlines. I like it a lot.
by ti-amie
by dryrunguy SanAngeloLive is reporting that Caleb Wallace has just hours to live. That was posted 16 hours ago.
by ti-amie
by dryrunguy
dryrunguy wrote: ↑Sat Aug 28, 2021 5:42 pm
SanAngeloLive is reporting that Caleb Wallace has just hours to live. That was posted 16 hours ago.
Caleb Wallace has died. I'd encourage you to read the piece at the link.
He had seven children. So besides not believing in vaccines, he didn't believe in using birth control. Sigh...
by ponchi101 And my problem is that, after you read the piece, and you see that his dad is still not taking the vaccine, I really, really do not feel sorry at all for this guy and, well, what a horrible human being I must be.
I recommend reading today's DOONESBURY. As always, on the money.
He had seven children. So besides not believing in vaccines, he didn't believe in using birth control. Sigh...
I think he only had four children. It's awkwardly worded: "Caleb leaves behind his wife who is expecting the couple’s fourth child and three other children."
by ti-amie
by JazzNU
by ponchi101 How much are the demographics of VOTING must be changing due to these deaths amongst GOP voters? And in states that may be up for grab in upcoming elections?
by dryrunguy This morning's NY Times e-newsletters had an intriguing headline: "Dying for vaccine freedom"
by ti-amie Remember @caslernoel called these stunts "performative"?
by ti-amie
by ti-amie
by dryrunguy Dude, if it's selective "data", contrived "data", or thoroughly debunked "data", then it ain't data.
by ti-amie
by ponchi101 Too much. People with proof of vaccination should be allowed to come in. Vaccination by more than 15 days.
by Suliso
ponchi101 wrote: ↑Mon Aug 30, 2021 7:20 pm
Too much. People with proof of vaccination should be allowed to come in. Vaccination by more than 15 days.
Exactly, we should stop this silos nonsense in both directions. Of course for vaccinated only. It's not like EU is virus free ala New Zealand...
by mmmm8 I wonder if this is a political response for the US still not allowing EU visitors even though things are mostly as bad or worse here.
by JazzNU Non-binding travel guidance, not a ban. Which makes more sense. I was completely unaware of the level of tourism some European towns expect and depend on from Americans until the pandemic happened, so this headline made me wonder how this would go over with places scrambling to recoup losses from the lockdowns. But don't think it's going to have much effect on travel. Anymore than it would that is, the school year is starting, travel was always going to drop in the fall.
Israel, among others, got the same advisory.
In terms of allowing the vaccinated to travel. Color me surprised that almost all of the international airlines haven't made proof of vaccination a requirement by now. Airplanes seem like they are only second to cruises in the Covid Blame Game in terms of people thinking (probably correctly) that they are the source of covid transmission.
by Suliso
JazzNU wrote: ↑Mon Aug 30, 2021 8:19 pm
Non-binding travel guidance, not a ban. Which makes more sense. I was completely unaware of the level of tourism some European towns expect and depend on from Americans until the pandemic happened, so this headline made me wonder how this would go over with places scrambling to recoup losses from the lockdowns. But don't think it's going to have much effect on travel. Anymore than it would that is, the school year is starting, travel was always going to drop in the fall.
Actually me neither. I think it's mostly in Italy and maybe few spots in France and Spain. Americans who travel to Europe are mostly above average financially and tend to spend more per night than say Germans would. Also certain services like guided tours or top class restaurants seem to be particularly in demand among them.
On a side note: I'm continuously surprised how many American travelers are afraid of driving in EU even though they do it every day back home. It's not as wide here, but roads mostly good...
by atlpam The new EU restrictions only apply to unvaccinated travelers.
by ti-amie
by ti-amie
by ti-amie
by ponchi101 This topic is definitely hazardous to your mental health. All other topics, I can go in there and mostly no issues. This one simply makes me feel like alcoholism is actually an honorable option.
by ti-amie
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 216.9 million cumulative cases and 4.5 million deaths worldwide as of August 31. Global weekly incidence decreased for the first time since mid-June, down 3.12% from the previous week. Weekly mortality also decreased, for the first time since late June*, falling 2.41% compared to the previous week.
*With the exception of the week of July 19, when Ecuador reported 8,786 deaths.
The global cumulative mortality surpassed 4.5 million deaths in today’s update:
1 death to 500k: 165 days
500k to 1 million: 86 days
1 to 1.5 million: 70 days
1.5 to 2 million: 44 days
2 to 2.5 million: 37 days
2.5 to 3 million: 52 days
3 to 3.5 million: 38 days
3.5 to 4 million: 51 days
4 to 4.5 million: 54 days
Global Vaccination
The WHO reported 5.02 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of August 30. A total of 1.93 billion individuals have received at least 1 dose, and 1.16 billion are fully vaccinated. Analysis from Our World in Data indicates that global daily vaccinations increased sharply over the past several days, up to 41 million doses per day, which would be the third highest peak to date*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 3.11 billion vaccinated individuals worldwide (1+ dose; 39.45% of the global population) and 2.12 billion who are fully vaccinated (26.9% of the global population)**.
*The average doses administered may exhibit a sharp decrease for the most recent data particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
**China reported 448 million new vaccinated individuals (1+ dose) and 112 million fully vaccinated individuals on August 26, its first report since June 10.
UNITED STATES
The US CDC reported 38.9 million cumulative COVID-19 cases and 636,015 deaths. Daily incidence continues to increase, but the trend is tapering off toward a peak or plateau. The current average of 149,334 new cases per day is the highest since January 29. Daily mortality also continues to increase, and the mortality trend may be starting to taper off as well. The current average of 970 deaths per day is the highest since March 13*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Data from HHS indicate that more than 100,000 COVID-19 patients are currently hospitalized nationwide. This represents the second highest peak to date, and is still increasing. The CDC reports more than 84,000 COVID-19 patients currently hospitalized, 32% below the highest peak.
US Vaccination
The US has administered 369.6 million cumulative doses of SARS-CoV-2 vaccines, and daily vaccinations appear to have peaked over the past several days. The average briefly exceeded 798,000 doses per day on August 23 before falling to 787,000 on August 25*. Notably, we have not observed a marked increase in daily vaccinations since the US FDA issued full approval for the Pfizer-BioNTech vaccine. There are 204.5 million individuals who have received at least 1 dose, equivalent to 61.7% of the entire US population. Among adults, 74.1% have received at least 1 dose, as well as 13.4 million adolescents aged 12-17 years. A total of 173.8 million individuals are fully vaccinated, which corresponds to 52.4% of the total population. Approximately 63.4% of adults are fully vaccinated, as well as 10.2 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US CDC ACIP MEETING At a meeting on August 30, the US CDC's Advisory Committee on Immunization Practices (ACIP) expressed initial support for third doses of SARS-CoV-2 mRNA vaccines for vulnerable populations, such as long-term care facility residents, and healthcare workers but said there is not enough data yet to recommend so-called booster shots for the general population. In a presentation to the committee, Dr. Sara Oliver, Co-Lead for the COVID-19 Vaccines ACIP Work Group, said data through July show the vaccines appear to provide strong protection against severe disease and hospitalization. Vaccine effectiveness (VE) against hospitalization remains high, between 75% to 95%, while VE against infection spans a much broader range, between 39% to 84%, since the predominance of the Delta variant. Dr. Oliver noted the reasons for lower VE “likely include both waning over time and the Delta variant.” Instead of focusing on booster doses, ACIP members emphasized that improving overall vaccination coverage is a “top priority,” as a high percentage of hospitalizations are occurring among unvaccinated individuals. They also said any booster dose recommendation should take into account equitable access to vaccines, both domestically and globally. The committee did not vote on booster doses, noting it intends to do so after the US FDA authorizes their use. The committee expects to meet in a few weeks to discuss data covering August, although a date was not announced. While the administration of US President Joe Biden has endorsed booster shots, saying they will be available by September 20, the FDA and CDC must first make recommendations based on scientific evidence.
At the meeting, the ACIP backed the US FDA’s full approval of the Pfizer-BioNTech SARS-CoV-2 mRNA vaccine, voting 14-0 to recommend the vaccine for individuals aged 16 and older. CDC Director Dr. Rochelle Walensky endorsed the recommendation, 9 months after the committee made an interim recommendation supporting the vaccine’s use. The committee reiterated that though there are rare reports of heart inflammation after mRNA vaccination, especially among males under age 30, the benefits of the vaccine outweigh the risks because the condition can occur at higher rates in COVID-19 patients than among those who received an mRNA vaccination.
DELTA HOSPITALIZATION RISK A study published August 27 in The Lancet Infectious Diseases adds evidence to what many experts already suspected: people infected with the highly contagious SARS-CoV-2 Delta variant are twice as likely to be hospitalized as those infected with the Alpha variant. To compare hospitalization rates, researchers from Public Health England (PHE) and Cambridge University examined data on 43,338 sequencing-confirmed COVID-19 cases between March 29 and May 23, 2021, during which time the Delta variant was becoming the predominant variant in the UK. The majority of the cases were among unvaccinated individuals (74%), while 2% were fully vaccinated and 24% had received one dose. Of 34,656 Alpha cases, 764 (2.2%) were admitted to the hospital within 14 days of a positive SARS-CoV-2 test, while 196 of 8,682 (2.3%) Delta cases were hospitalized. Although the percentages of hospitalized cases were similar between both variants, the risk of being hospitalized more than doubled (adjusted hazard ratio [HR] 2.26, 95% confidence interval [CI] 1.32-3.89) for Delta cases compared with Alpha cases when the researchers adjusted the data to account for certain factors, including age and sex. Delta cases also were more likely to seek emergency medical care or be hospitalized within 14 days versus Alpha cases (adjusted HR 1.45, 95% CI 1.08-1.95).
Although the researchers examined differences between vaccinated and unvaccinated groups for hospitalizations and emergency care or hospitalization, the results were non-significant due to low numbers of cases who were fully vaccinated. Therefore, the results only apply to people who are unvaccinated. In a statement, Dr. Anne Presanis, Senior Statistician at the University of Cambridge and a lead author of the study, emphasized the importance of getting fully vaccinated to reduce the risk of symptomatic infection with Delta, as well as reduce the risk of severe disease and hospitalization. The researchers noted that a previous study conducted in Scotland and published in The Lancet in June showed a similar increase in hospitalization risk among people infected with the Delta variant. While the UK study is the largest to date examining hospitalization risk for the Delta versus Alpha variants based on whole-genome sequenced cases, the researchers called for further assessments into how hospitalization risks differ for vaccinated individuals after infection with either variant.
SCHOOL TRANSMISSION A case study published August 27 in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) shows how quickly the highly contagious SARS-CoV-2 Delta variant can spread within a classroom of children too young to be vaccinated. The outbreak involved an unvaccinated Marin County, California (US), elementary school teacher who began showing COVID-19 symptoms on May 19, but who came to work the next 2 days, attributing the symptoms to allergies. During that time, the teacher read aloud to the class without wearing a mask, even though masks were required for staff and students while indoors. The teacher received a positive SARS-CoV-2 test on May 21 and informed the school on May 23. Several students became symptomatic on May 22, and the Marin County Department of Public Health (MCPH) initiated an investigation on May 26 to characterize the outbreak. Overall, 27 COVID-19 cases were identified, including the teacher. Among the teacher’s 24 students—all of whom were too young to be eligible for vaccination—12 of 22 who were tested received positive results between May 23-26. Notably, 8 out of 10 students who sat in the 2 front rows closest to the teacher became infected, representing an extremely high attack rate of 80%.
In another classroom, located across an outdoor courtyard from the source classroom, 6 of 18 students in a different grade—also too young for vaccine eligibility—tested positive between May 24 and June 1. Additionally, 8 other cases were identified among parents and siblings of the students in the 2 classes, 3 of whom were fully vaccinated. An additional infected adult was unvaccinated. Of the 18 cases sequenced, all were identified as the Delta variant. The report’s authors underlined the importance of vaccination and other preventive measures, “including masking, routine testing, facility ventilation, and staying home when symptomatic” to ensure safe in-person learning in schools. Notably, all of the children were seated 6 feet apart and the classrooms had portable high-efficiency particulate air filters with open doors and windows, raising a question about whether consistent masking could have helped contain transmission in this outbreak.
A separate MMWR report published the same day concluded that in Los Angeles County, California, schools with transmission mitigation and containment protocols in place, “case rates in children and adolescents were 3.4 times lower during the winter peak compared with rates in the community,” showing multi-pronged prevention strategies are critical in helping to prevent new cases as children return to classrooms. However, the authors cautioned the data were collected prior to the predominance of the Delta variant (September 1, 2020-March 31, 2021).
SARS-CoV-2 ORIGIN: US REPORT As expected, the US Office of the Director of National Intelligence on August 27 released an unclassified summary of a report stating that the US Intelligence Community “remains divided on the most likely origin of COVID-19. All agencies assess that two hypotheses are plausible: natural exposure to an infected animal and a laboratory-associated incident." Just over 3 months ago, US President Joe Biden ordered the Intelligence Community to undertake a systematic, detailed review of any evidence that could elucidate the origins of the COVID-19 pandemic. The only strong conclusion expressed in the summary is that SARS-CoV-2 was not developed as a biological weapon. Most agencies also agreed, with low confidence, that the virus probably was not genetically engineered, although 2 agencies believed there was insufficient evidence to make an assessment either way. In a statement following the summary’s release, President Biden said the US will continue to search for answers, adding, “I will not rest until we get them.” In order to do so, however, investigators will need cooperation from China, which continues to deflect blame and resist sharing information, according to the summary.
HURRICANE IDA Southern Louisiana (US) hospitals, already inundated with COVID-19 patients, are now dealing with damage from Hurricane Ida. The Category 4 storm made landfall in Lafourche Parish on August 29, battering the area for 16 hours with heavy rainfall and strong winds that caused widespread power outages, levee failures, flooding, collapsed buildings, and the need for rescues. At least 2 hospitals in Lafourche Parish reported significant damage, including extensive roof damage and partial generator failure. Residents of the parish were ordered to evacuate, but evacuating hospital patients was not an option because no other hospitals had the capacity to take additional patients due to an overwhelming number of COVID-19 patients and staff shortages.
Louisiana Governor John Bel Edwards said that with more than 2,400 COVID-19 patients hospitalized in the state, many in serious or critical condition, the focus is on ensuring there is enough generator power and clean water at hospitals to meet patients’ needs, including providing oxygen and ventilator support, both of which require electricity. Nearly 1 million people within the New Orleans power grid were without power due to the storm’s “catastrophic intensity,” with the Entergy Corporation working to get lines back in operation. Hurricane Ida hit on the 16th anniversary of Hurricane Katrina and, with sustained winds of 150 mph, tied a record for the most intense hurricane on record to hit Louisiana. Notably, lessons learned after Katrina, including the relocation of hospital generators to higher floors, likely helped save lives during this storm.
COURT-ORDERED VACCINATION As the rate of SARS-CoV-2 vaccination slowly creeps up in the US, a significant portion of the population continues to resist getting the shots. In what appears to be efforts to persuade the reluctant, several judges have ordered defendants to be vaccinated as part of their orders. In New York, a Bronx County criminal court judge ordered a man pleading guilty to drug possession and shoplifting to get a SARS-CoV-2 vaccine as part of his plea deal, an action that the judge said would be viewed as rehabilitative. In another case in New York, a federal judge in Manhattan granted bail for a defendant charged with conspiracy to distribute fentanyl on the condition that she be vaccinated so she posed less of a danger to the community. Neither defendant appeared to object.
In a similar case, a Cook County, Illinois, judge on August 10 revoked a woman’s right to visit her 11-year-old son until she is vaccinated for SARS-CoV-2. The 39-year-old woman shares custody of the boy with her divorced husband, who did not seek such an order. The woman’s lawyer said she believes the judge exceeded his authority and hopes an appellate court, which is expected to hear the case this week, reverses the decision. While some legal experts say these judges might have overstepped their authority, others argue that the orders fall within their jurisdiction, highlighting the legal and ethical questions surrounding the interpretation of the line between civil responsibility and civil liberty.
EU TRAVEL RESTRICTIONS The EU on August 30 recommended that member states halt all non-essential travel from the US due to the rising number of COVID-19 cases throughout the country. The EU also recommended the removal of Israel, Kosovo, Lebanon, Montenegro, and North Macedonia from the bloc’s “white list” of places whose tourists could be permitted entry without certain restrictions. In order to be included on the white list, countries have to have no more than 75 new daily COVID-19 cases per 100,000 residents over the last 14 days, and these 6 countries no longer meet that criterion. The decision is non-binding, as each EU member state is able to set its own tourism policies and restrictions. Possible restrictions include testing requirements, quarantine upon arrival, a ban on non-vaccinated travelers, and a ban on all non-essential travelers from the stated countries. The white list now includes 18 countries.
Removal of the US from the white list follows a previous decision in June that recommended lifting restrictions on non-essential travelers from the US and 14 other nations. A majority of countries in the EU lifted non-essential travel restrictions after the decision in hopes of retaining income from the summer tourism season. New travel restrictions are anticipated to cost billions in lost tourism income.
AUSTRALIA Australian Prime Minister Scott Morrison announced that the country is moving past its “COVID zero” goal, arguing that the current level of restrictions “is not a sustainable way to live,” particularly in light of the emergence of the Delta variant. Throughout the pandemic, Australia has responded to local outbreaks with highly restrictive “lockdown” measures, while facing relatively few restrictions in the periods between outbreaks. This plan aimed to interrupt chains of transmission and prevent localized outbreaks from spreading to a regional- or national-level epidemic in order to reach and maintain essentially zero domestic transmission. The policy change appears to be tied to vaccination coverage, and the government could begin easing restrictions once national coverage reaches 70% among eligible individuals. Australia is currently reporting full vaccination coverage of 35% for individuals ages 16 and older, and officials reportedly believe Australia can double this rate by the end of 2021. Notably, Prime Minister Morrison also announced children aged 12-17 years are now be eligible for vaccination.
MEDIGEN VACCINE Taiwan on August 23 launched an island-wide rollout of its domestically produced Medigen SARS-CoV-2 vaccine, produced by Taipei-based Medigen Vaccine Biologics Corporation, with Taiwan President Tsai Ing-wen publicly receiving the first shot. But the rollout quickly hit speed bumps, with experts criticizing the launch of the vaccine without the completion of Phase 3 clinical trial and no efficacy data. Then, over the next 3 days, 4 people died after receiving the vaccine, raising questions about its safety among some experts. Taiwan’s Central Epidemic Command Center (CECC) said it does not plan to halt the campaign, as there is no indication that the deaths are associated with the vaccine. The CECC will continue to investigate whether there is a causal relationship, indicating the news has not affected vaccine uptake among the Taiwanese population. Throughout the pandemic, Taiwan has been successful at curbing dramatic surges in COVID-19 cases and reports fewer than 16,000 total confirmed cases to date.
SPUTNIK V Russia’s Sputnik V SARS-CoV-2 vaccine, officially known as Gam-COVID-Vac, appears to reduce the risk of hospitalization and prevent severe lung damage among COVID-19 patients, according to a preprint paper posted to medRxiv. The analysis, which has not yet been peer-reviewed, includes data from 13,894 patients, 9.3% of whom were fully vaccinated, having completed their second shot at least 2 weeks prior. Among those fully vaccinated, the adjusted vaccine effectiveness (VE) against hospital referral was 81% (95% confidence interval [CI], 68-88). The VE against hospital referral was slightly better among women (84%, 95% CI, 66-92) compared with men (76%, 95% CI, 51-88). The data also show that Sputnik V was 76% effective at protecting against severe lung injury, defined as more than 50% lung involvement. Although the data do not include genetic sequencing for viral variants, Russian health officials say 95% of new infections in July and August, when the study was conducted, were attributable to the Delta variant. The Sputnik V vaccine is authorized for use in 69 countries, but the European Medicines Agency (EMA) and the WHO continue to review the vaccine for authorization.
C.1.2 VARIANT A preprint article posted on medRxiv from a group of South African researchers describes a potential SARS-CoV-2 variant of interest assigned to the PANGO lineage C.1.2. According to the paper, which is not yet peer-reviewed, the variant was first identified in May 2021 and likely originated from the C.1 viral lineage, one of the lineages that dominated the first wave of SARS-CoV-2 infections in South Africa. The C.1.2 variant is believed to have between 44-59 mutations in regions such as the spike protein, receptor binding motif, and furin cleavage site, representing more mutations than previous variants of interest and variants of concern. The mutations described in the article are associated with increased neutralizing antibody evasion, increased transmissibility, and potentially increased viral reproduction.
By August 13, 2021, the variant had been detected in a majority of South African provinces, as well as in the Democratic Republic of the Congo, Mauritius, New Zealand, Portugal, and Switzerland. Despite the wide geographic spread, prevalence of C.1.2 in tested samples remains low. However, monthly increases in prevalence are similar to those seen in the early stages of the Beta and Delta variants. Researchers are currently assessing the effectiveness of vaccines against this lineage and more information is expected soon. Notably, though the researchers say they are “concerned” about C.1.2, it has not yet been named a variant of interest or concern, as more data are necessary to make that determination.
COMPARING mRNA VACCINE IMMUNE RESPONSE A research letter published in the Journal of the American Medical Association (JAMA) describes results from a prospective study comparing antibody responses to the Pfizer-BioNTech and Moderna SARS-CoV-2 vaccines among a cohort of Belgian healthcare workers. For the study, antibodies against the SARS-CoV-2 nucleocapsid protein were measured after vaccination. Among the 1,647 healthcare workers included in the evaluation, 2 doses of Moderna produced higher antibody titers than 2 doses of Pfizer-BioNTech; participants who were previously infected with SARS-CoV-2 had higher antibody titers than participants who were never infected; and higher antibody titers were correlated with younger age groups. The limitations of the study include a lack of information on cellular immunity and neutralizing antibody titers. Neutralizing antibodies can stop a virus from entering a cell and initiating infection while binding antibodies alert white blood cells to the presence of a pathogen and mark them for destruction. Neutralizing antibodies serve a different purpose from binding antibodies and they can result in long-term immunity to certain infections.
BLOOD CLOTTING RISKS The risk of blood clotting events after infection with SARS-CoV-2 is much higher than the risk posed by vaccination with either the Pfizer-BioNTech or AstraZeneca-Oxford vaccines, according to a large UK study published August 27 in the British Medical Journal (BMJ). A team led by researchers from the University of Oxford examined the health records of more than 29 million people who received a first dose of either vaccine between December 2020 and April 2021, as well as nearly 1.8 million who were infected with the virus, looking for complications up to 28 days post-vaccination or infection.
The researchers found that people who received the Pfizer-BioNTech vaccine had an increased risk of ischemic stroke and blood clots in arteries, while those who received the AstraZeneca-Oxford vaccine had an increased risk of low platelets (thrombocytopenia) and blood clots in veins. While the researchers said that people should be aware of the increased risk, they stressed that the risks of the same complications among people infected with SARS-CoV-2 are much higher. For example, the risk of thrombocytopenia is almost 9 times higher with infection than vaccination with the AstraZeneca-Oxford vaccine, and the risk of stroke is nearly 12 times higher after COVID-19 than with the Pfizer-BioNTech vaccine. The risk of blood clotting events also remained elevated for a longer period of time after infection compared with vaccination. Experts continue to stress that the short- and long-term complications of COVID-19 are much more severe than the risks associated with vaccination, and they urge those eligible to get vaccinated.
by ti-amie Maderna? Wasn't she really big back in the day?
Please read who gave her her "shots".
by ponchi101 That is a very poor job of counterfeiting a covid card. They slap a stamp on them, not write the data by hand.
1 month for trying to forge a card, 1 year for the poor quality of the job.
Serious here: if they find you with a fake card, you should get two options: prison time, or get the real vaccine and then you do no time. Let's see how many stick to their principles.
by dryrunguy Mine doesn't have a stamp.
by Jeff from TX
ponchi101 wrote: ↑Wed Sep 01, 2021 7:37 pm
That is a very poor job of counterfeiting a covid card. They slap a stamp on them, not write the data by hand.
1 month for trying to forge a card, 1 year for the poor quality of the job.
Serious here: if they find you with a fake card, you should get two options: prison time, or get the real vaccine and then you do no time. Let's see how many stick to their principles.
Mine has stickers for the vaccine type and lot #, but the date is handwritten. Still, terrible forgery job. You can't fix stupid. But I like the idea of no jail time if you get the vaccine plus fine.
by ponchi101
dryrunguy wrote: ↑Wed Sep 01, 2021 8:04 pm
Mine doesn't have a stamp.
Really? Kroger printed a super professional label for mine. The stickers that Jeff talks about.
Ok, guess I really don't know.
dryrunguy wrote: ↑Wed Sep 01, 2021 8:04 pm
Mine doesn't have a stamp.
Really? Kroger printed a super professional label for mine. The stickers that Jeff talks about.
Ok, guess I really don't know.
No, mine is a CDC COVID-19 Vaccination Record Card with my name, DOB, J&J vaccine, lot number, date, and the initials of the pharmacy where I got it. All hand-written. No stamp.
If it turns out these bozos with fake vaccination cards who are traveling the world and possibly infecting as many people as possible make it more difficult for me, I'm gonna be super moody. Not Miami airport super moody, but yeah, super moody.
by Deuce
ti-amie wrote: ↑Wed Sep 01, 2021 7:32 pm
Maderna? Wasn't she really big back in the day?
Please read who gave her her "shots".
I doubt very much that this ^ is a fake document.
I'm quite sure that it is exactly what it claims to be - a genuine vaccination certificate issued by the NRA when they hold their vaccination clinics.
dryrunguy wrote: ↑Wed Sep 01, 2021 8:04 pm
Mine doesn't have a stamp.
Really? Kroger printed a super professional label for mine. The stickers that Jeff talks about.
Ok, guess I really don't know.
No, mine is a CDC COVID-19 Vaccination Record Card with my name, DOB, J&J vaccine, lot number, date, and the initials of the pharmacy where I got it. All hand-written. No stamp.
If it turns out these bozos with fake vaccination cards who are traveling the world and possibly infecting as many people as possible make it more difficult for me, I'm gonna be super moody. Not Miami airport super moody, but yeah, super moody.
Mine's all handwritten too. But New York State now also has an app that shows your COVID vaccine confirmation and details. I'm sure PA will too if they don't yet.
by ti-amie
by dryrunguy Here's the latest Situation Report. It has a detailed explanation of how Florida is "cooking the books" regarding COVID mortality reporting.
The section on the Mu variant in Colombia and Ecuador made my heart skip a beat.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 218.6 million cumulative cases and 4.53 million deaths worldwide as of September 3.
Global Vaccination
The WHO reported 5.29 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 1. A total of 2.01 billion individuals have received at least 1 dose, and 1.21 billion are fully vaccinated. Analysis from Our World in Data indicates that global daily vaccinations are holding relatively steady at approximately 41 million doses per day, which is the third highest peak to date*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 3.16 billion vaccinated individuals worldwide (1+ dose; 40.1% of the global population) and 2.16 billion who are fully vaccinated (27.4% of the global population). *The average doses administered may exhibit a sharp decrease for the most recent data particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reported 39.5 million cumulative COVID-19 cases and 641,725 deaths. Daily incidence continues to increase, but the trend is tapering off toward a peak or plateau. On August 27, the US surpassed 150,000 new cases per day, and the current average of 153,245 is the highest since January 28. Daily mortality also continues to increase, and the mortality trend may be starting to taper off as well, although Florida’s new reporting scheme is impacting how we interpret the current trend (see below). The US surpassed 1,000 deaths per day on August 24, and the current average of 1,046 deaths per day is the highest since March 11*.
*Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
The Florida Department of Health updated its COVID-19 mortality reporting process, which affects how the official state and CDC data are interpreted. Previously, like other states, Florida assigned dates to COVID-19 deaths corresponding to the date they were reported; however, Florida now assigns dates that correspond to the date of death. While reporting mortality by the date of death is technically the most accurate approach, it makes it difficult to monitor current trends. Deaths can take days or weeks to be identified, confirmed, and reported, which results in a sharp artificial decline in daily mortality over the most recent several days, even though the actual trend could be increasing. As deaths are confirmed, they will be added to the correct date of death, so the data from recent days will fill in over time. These delays mean that it will take extra time to identify changing trends, including the peak during a surge or the start of a new surge. Based on recent trends, we believe Florida is averaging more than 200 deaths per day; however its most recent report includes only 11 deaths for September 1, bringing its average down all the way down to 64. Because Florida represents approximately 20% of the average national daily mortality, its new reporting scheme is affecting how we interpret the national-level trend as well. The US average could easily be 100-150 deaths per day higher than the current reported value.
US Vaccination
The US has administered 372 million cumulative doses of SARS-CoV-2 vaccines, and daily vaccinations have leveled off over the past several days, hovering at slightly more than 800,000 doses per day since August 23*. We have not observed a marked increase in daily vaccinations since the US FDA issued full approval for the Pfizer-BioNTech vaccine. There are 205.9 million individuals who have received at least 1 dose, equivalent to 62.0% of the entire US population. Among adults, 74.5% have received at least 1 dose, as well as 13.5 million adolescents aged 12-17 years. A total of 175.0 million individuals are fully vaccinated, which corresponds to 52.7% of the total population. Approximately 63.7% of adults are fully vaccinated, as well as 10.4 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
As we have covered previously, there are considerable disparities in terms of both vaccination coverage and the impact of the ongoing US surge at the state and regional levels. This week, we will look more closely at COVID-19 mortality since July 1 (ie, during the current surge) and any potential associations with state-level full vaccination coverage. It is well documented that full vaccination provides good protection against severe COVID-19 disease and death, including from the Delta variant. In this analysis, we will compare the raw increase in per capita cumulative mortality from July 1-September 1. Comparing the per capita values will allow us to more directly compare states to each other, and using the raw increase—ie, as opposed to the relative increase—we can mitigate the effects of the baseline cumulative incidence, which varies widely by state. By July 1, all states had removed eligibility restrictions and opened vaccination up to the general public. Daily vaccination progress slowed, so we can reasonably assume that coverage—or at least the relative differences in coverage—remained relatively consistent over that period.
The median state-level increase in per capita cumulative mortality over this period was 8 deaths per 100,000 population, and the mean was 11. This indicates that most states reported lower increases, while a small number of states reported much higher totals. In total, 32 states reported increases of 10 or fewer, and 12 states* reported increases of 15 or more, including 4 states with increases of more than 30: Louisiana (40), Florida (36), Arkansas (35), and Mississippi (34). Of the 12 states reporting increases of more than 15, 10 are in HHS Regions 4 (Southeast), 6 (South Central), and 7 (Central). Among the 16 states reporting increases of 5 deaths per 100k or fewer, the top 5 are all in Region 1 (Northeast)**, 4 states are in Region 3 (Midwest), and 3 are in Region 5 (Mid-Atlantic).
Among the 12 states reporting increases of 15 deaths per 100k or more, all but Florida (#21; 53.4%) are in the bottom half of states in terms of full vaccination coverage. Florida is also the only one of these states with full vaccination coverage greater than 50%. Eight (8) of these states are in the bottom 12 in terms of vaccination coverage, including #48 Wyoming (39.1%), #49 Alabama (38.6%), and #50 Mississippi (38.5%). Among the top 10 states in terms of full vaccination coverage, 6 are also in the top 10 in terms of the increased per capita mortality. Only 1 of the top 28 states in terms of vaccination coverage reported an increase in mortality greater than 10 deaths per 100k: Florida (+49).
Several states reported notably lower or higher increases in per capita mortality than would be expected based solely on their vaccination coverage. As noted above, Florida reported the second-largest increase in mortality, but it ranks #21 in terms of full vaccination coverage. While vaccination is a key tool in terms of mitigating the impact of COVID-19, it needs to be combined with non-pharmaceutical interventions (NPIs), such as physical distancing and mask use, to slow transmission, and Florida officials have exhibited an unwillingness to implement those types of measures during the current surge. Increased transmission and incidence will inevitably lead to increased mortality. New Jersey, Oregon, and Washington also rank considerably lower in terms of increased mortality than they do for vaccination coverage—18, 19, and 20 positions lower, respectively—but it is not immediately clear why these states, in particular, faced elevated COVID-19 mortality compared to their vaccination coverage.
Conversely, North and South Dakota rank much better in terms of increased COVID-19 mortality than their vaccination coverage would suggest. North Dakota is #44 in terms of vaccination coverage (41.8%), but it is #4 in terms of the increase in mortality (4 deaths/100k), a difference of 40 positions. South Dakota also ranks #4 in terms of increased mortality**, but it ranks #26 in terms of vaccination coverage (49.4%), a difference of 22 positions. Similarly, Nebraska and Ohio each rank 18 positions higher in terms of increased mortality than they do for vaccination coverage. Notably, these and other similar states—including Idaho, Michigan, Minnesota, and West Virginia—appear to still be in the early stages of their respective surges, so it is possible that we could observe larger increases in mortality as they move closer to their respective peaks. In contrast, most of the Region 1 states appear to already be peaking in terms of COVID-19 mortality, and their lower mortality during this surge suggests that higher vaccination coverage provided protection against severe disease and death at the state level.
With some notable exceptions, there appears to be an association between higher vaccination coverage and lower COVID-19 mortality during the current surge. The surge first emerged in Missouri, before moving south and east, into Arkansas, Louisiana, Mississippi, Alabama, and Florida, so it has been present there longer than in other parts of the country. The lower vaccination coverage in these states, however, appears to be contributing to elevated hospitalizations and mortality—in some instances, equal to or worse than their previous records. The timing of the geographic spread of the surge could also potentially factor into the lower mortality reported in states that are still in the early stages of their respective surges, particularly those with lower vaccination coverage. Additional analysis, including after more states pass their peaks and on case-fatality ratios over this period, could provide further insight into the association between state-level vaccination coverage and COVID-19 mortality during this surge.
*Delaware reported an overall increase of 20 deaths/100k, but this included a jump of 13 on August 1 due to a bolus of 130 newly reported deaths, most of which were previously unreported. Without this reporting anomaly, Delaware would have had an estimated increase of 7.
**Including ties; 6 states reported increases of 4 deaths per 100k, all tying for the #4 rank.
VARIANT OF INTEREST: MU In its August 31 COVID-19 Epidemiological Update, the WHO announced the addition of another SARS-CoV-2 variant to its list of variants of interest (VOIs), B.1.621 or “Mu.” The Mu variant, which also includes the descendent Pango lineage B.1.621.1, includes several mutations that show the potential for immune escape in both people previously infected with SARS-CoV-2 and those who are vaccinated; however, more research is necessary to confirm the theory. As of August 29, more than 4,500 sequences of the lineage were recorded in 39 countries. The Mu variant was first identified in Colombia in January 2021. Since then, the variant has spread worldwide, with cases reported in the UK, US, Europe, and Hong Kong. While the global prevalence of the Mu variant among sequenced cases is below 0.1% globally and declining, the variant accounts for at least 39% of cases in Colombia and 11% in Ecuador, with prevalence in both countries continuing to increase. But WHO warned that reports on the variant’s prevalence should be “interpreted with due consideration” because of variations in countries’ sequencing capacities. Mu is the fifth variant of interest named by the WHO since March 2021. In August, Public Health England (PHE) released a risk assessment for the variant, which it calls VUI-21JUL-01, highlighting that laboratory findings show it is similar to the Beta variant first detected in South Africa and raising concerns over its potential for immune escape. The WHO said it will continue to monitor and study the variant’s epidemiological evolution.
MASK-USE TRIAL A group of researchers from Stanford Medicine and Yale University this week released findings from the first randomized controlled trial (RCT) in a real-world setting designed to evaluate the effects of mask use on SARS-CoV-2 transmission. The researchers found that mask use, even when worn inconsistently in the community, can lead to a reduction in symptomatic COVID-19 cases. Additionally, relatively low-cost, targeted interventions promoting mask wearing can significantly increase the use of face coverings in rural, low-income countries, according to the results. Although the study is not yet published, the researchers have submitted the paper to the journal Science, whose editors encouraged its public release given the current public health policy relevance, as the pandemic worsens in many parts of the world.
The study included more than 340,000 adults in 600 villages in Bangladesh. In 300 villages, researchers implemented a mask distribution and promotion initiative, now called the “NORM” model, which stands for “No-cost mask distribution, Offering information, Reinforcement to wear masks, and Modeling by local leaders.” The researchers saw a 29 percentage-point increase in mask-wearing in the intervention villages (42%) versus the comparison villages (13%). Overall, the increased mask usage led to a 9% reduction in serologically confirmed symptomatic SARS-CoV-2 infection. Notably, 100 of the villages received cloth masks, resulting in a 5% reduction in symptoms, while 200 villages that received surgical masks saw a 12% reduction in symptoms. The use of surgical masks was especially effective for people aged 60 years or older, leading to a 35% reduction in symptomatic SARS-CoV-2 infections in that age group. The team plans to conduct further research evaluating how masks limit symptomatic cases, whether by reducing exposure to viral load or by preventing infections entirely. For now, the study provides a “gold standard” showing mask wearing is an effective way to limit symptomatic COVID-19, and the interventions are being rolled out in other parts of Bangladesh and in Pakistan, India, Nepal, and areas of Latin America.
LONG-TERM HEALTH EFFECTS The scientific community continues to investigate the long-term impacts of COVID-19 on individual health. Researchers from the University College of London announced earlier this week that their survey of children with positive COVID-19 diagnoses provided reassurance that post-acute sequelae of COVID-19 (PASC), or so-called “long COVID,” does not impact large numbers of adolescents. The research team conducted a survey of 11- to 17-year-olds in England who had positive SARS-CoV-2 tests between September 2020 and March 2021. The study, which is not yet peer-reviewed, suggests that 2-14% of children with a positive test reported having symptoms 15 weeks after their initial diagnosis. While the reported prevalence still presents a public health concern for children with COVID-19, it suggests that these issues may not be as prevalent among younger people as previously thought.
Research also continues into the scope of COVID-19's long-term impacts among adults. A recent article published in The Lancet describes 1-year outcomes of individuals who survived hospitalization due to COVID-19. The study included 1,276 survivors discharged from the Jin Yin-tan Hospital in Wuhan, China, between January 7 and May 29, 2020. The cohort was followed for 12 months, with follow-up visits at 6 and 12 months. The research team found that the proportion of patients with at least 1 residual symptom decreased from 68% to 49% between the 6-month and 12-month follow-up appointments. However, researchers noted a slight increase in the proportion of patients experiencing anxiety and depression symptoms between the 6-month check-in (23%) and the 12-month follow-up (26%). The findings show that while most individuals returned to good health 1 year following their hospitalization, the overall health status of the COVID-19 survivors remained lower than for those in a non-hospitalized control group.
Another study published in The Lancet Infectious Diseases analyzed the risk of PASC among vaccinated adults. The research team conducted a community-based, case-control study among UK-based adults who used the COVID Symptom Study mobile phone app. The study matched individuals who contracted SARS-CoV-2 after vaccination with individuals who contracted the virus before vaccination in an attempt to parse out differences in disease presentation. The research team found that the odds of COVID-19 symptoms persisting for 28 days or more among those who were fully vaccinated was approximately halved (OR 0.51) compared with unvaccinated controls. While this risk reduction provides additional reasons to support COVID-19 vaccination, there is still a low but present risk that vaccinated adults could develop long COVID.
There already are reports of individuals suffering long-term COVID symptoms who feel that the scientific community is leaving them behind. Understanding and minimizing the long-term impacts of COVID-19 disease is an essential part of response and recovery, and research endeavors such as the ones described above can help characterize what could be a long tail on the end of the pandemic.
US SCHOOLS As the school year begins for many in the US, COVID-19 cases among children are rising, with nearly 204,000 new cases added the week ending August 26, representing 22.4% of the total weekly reported cases. This marks the second week with child cases at the level of the winter surge of 2020-21 and a 5-fold increase from July 22 to August 26, according to the American Academy of Pediatrics (AAP). US CDC data show the number of COVID-19 cases and related emergency room visits and hospitalizations among children were 4 times higher in states with low vaccination rates than those with higher vaccination rates during the month of August. CDC Director Dr. Rochelle Walensky said last week that recently opened schools with COVID-19 outbreaks generally are not following federal guidelines for vaccination and universal masking among staff and students. In one Iowa school district where masking is optional, parents are being given the option to quarantine their children if they have a known exposure, as long as they remain symptom-free, increasing the risk of transmission among asymptomatic children. In schools already operating, some outbreaks have caused districts to return to virtual learning, including one Texas school district where 2 junior high teachers died of COVID-19 complications the same week.
The US Department of Education announced this week it has begun investigations into 5 states—Iowa, Oklahoma, South Carolina, Tennessee, and Utah—whose bans on mask mandates in schools might violate civil rights laws meant to protect students with disabilities. The department has not opened investigations in Florida, Texas, Arkansas, or Arizona because all of the bans in those states are not being enforced due to ongoing legal or other actions. On August 27, a Florida judge ruled that Governor Ron DeSantis and the Florida Department of Education had overstepped their authority when they banned mask mandates in the state’s school districts because the policy does not provide a parental opt out. Governor DeSantis’s lawyers on September 2 filed an appeal with the 1st District Court of Appeal in Tallahassee.
A new survey from the National Parent Teacher Association, conducted with support from the CDC Foundation, shows fewer parents want their children attending in-person classes. Prior to July 27, when the CDC updated its health guidance for schools in light of the highly contagious Delta variant, 58% of 1,448 parents and guardians surveyed said they wanted their children back in classrooms, but that figure dropped to 43% by August 8. The proportions were lower for Black (41%) and Hispanic (37%) parents, who expressed a preference for online learning. These results likely reflect the fact that Black and Hispanic children, as well as adults, are disproportionately impacted by COVID-19. On August 31, the CDC released updated FAQs for parents with school-aged children.
US PRISONS & JAILS Reducing the number of people detained in US prisons and jails could have prevented millions of COVID-19 cases and hundreds of thousands of related deaths, as the overcrowded, tight quarters fuel a constant risk of outbreaks among inmates and staff, according to a study published September 2 in JAMA Network Open. Researchers from Northwestern Medicine, the Toulouse School of Economics, and the French National Centre for Scientific Research analyzed data collected in 1,605 US counties from January to November 2020 and found that an 80% reduction in the U.S. jail population—a level achievable simply by finding alternatives to jail detention for people accused of non-violent offenses—was associated with a 2% drop in the growth rate of daily COVID-19 cases. The reduction was greater in counties with large urban areas and when jail turnover was taken into account. The US jail population has a 55% weekly turnover rate, the study notes. This turnover, in addition to staff returning home to their communities daily, has contributed immensely to the overall number of COVID-19 cases in the US, according to the researchers. For comparison, the study also looked at other anticontagion policies, finding that nursing home visitation bans were associated with a 7.3% reduction in COVID-19 case growth rates, followed by school closures (4.3%), mask mandates (2.5%), prison visitation bans (1.2%), and stay-at-home orders (0.8%). Besides mass decarceration efforts, some experts are calling for mandatory SARS-CoV-2 vaccinations for staff and detainees in jails and prisons to help reduce the risk of outbreaks.
US HOSPITAL BURDEN Across the US, hospitals are straining under the volume of COVID-19 patients, and several states are nearly out of ICU beds. Alabama, Arkansas, Florida, Georgia, and Texas have less than 10% of their ICU beds available. Georgia hospitals have topped their January highs on some days, and adult ventilator use has far outpaced the previous high. A US Department of Health and Human Services (HHS) dashboard paints a grim picture, where 42 states are reporting 70% or greater use of inpatient beds, and 7 of the remaining 8 are in the 60-69% use category. In several states, including Montana and Oregon, the National Guard is assisting to help ease staffing shortages. Children’s hospitals are no exception, with many at or near capacity. The CEO of the Children’s Hospital Association wrote a letter to US President Joe Biden requesting federal help to handle the surge. Adding to the stress, about US$44 billion in federal aid from the US$178 billion Provider Relief Fund created last year and $8.5 billion allotted by the US Congress for rural medical care has not been distributed. Healthcare institutions, advocates, and lawmakers are urging the Biden administration to quickly decide how the funds will be divided and when they will be released. HHS has said a plan is being developed.
VACCINE EFFECTIVENESS AMONG HEALTHCARE WORKERS Coincident with the end of California’s (US) mask mandates in June 2021 and the rise of the SARS-CoV-2 Delta variant, the University of San Diego Health (UCSDH) workforce experienced an increase in SARS-CoV-2 infections, despite high vaccination rates. According to correspondence published in the New England Journal of Medicine (NEJM), between March 1 and July 31, 2021, 227 UCSDH healthcare workers tested positive for SARS-CoV-2 by rt-PCR, of whom 57.3% were fully vaccinated. Researchers calculated vaccine effectiveness by month, saying effectiveness exceeded 90% March through June, but fell to 65.5% in July (95% confidence interval [CI], 48.9 to 76.9). Additionally, the July attack rate among vaccinated individuals increased as time from vaccination grew, with those who were fully vaccinated later in the year (March through May; 3.7 per 1,000 persons [95% CI, 2.5 to 5.7]) showing an attack rate nearly half that of those vaccinated earlier in the year (January or February; 6.7 per 1,000 persons [95% CI, 5.9 to 7.8]). For unvaccinated workers, the attack rate was much higher (16.4 per 1,000 persons [95% CI, 11.8 to 22.9]). The authors attribute the change in vaccine effectiveness to the rise of the Delta variant and waning immunity, in addition to the end of masking requirements that likely resulted in increased community exposure.
But some experts have questioned the study’s conclusions, saying the reduction in vaccine effectiveness could be due to several additional or separate factors, including a small sample size for the July data; a single, large outbreak of 70 cases among workers in July; and an increase in close contacts due to loosened preventive measures. As more studies are published showing a possible decrease in vaccine effectiveness over time, it is important to consider behavior changes that could contribute to outcomes, even if the data are not captured in studies.
LATIN AMERICA & CARIBBEAN The Pan-American Health Organization (PAHO) has called on countries with surplus SARS-CoV-2 vaccines to urgently donate them to Latin American and Caribbean nations, where only 1 in 4 people have been fully vaccinated. While vaccination coverage in some countries such as Uruguay and Chile have exceeded 60%, rates are much lower in other countries, including Guatemala and Nicaragua. At a news conference, PAHO Director Dr. Carissa F. Etienne said that while every country in the region has begun administering vaccines, “immunizations are following the fault lines of inequality” in the region. She also announced the launch of the Regional Platform to Advance the Manufacturing of COVID-19 Vaccines and other Health Technologies in the Americas, which hopes to ease vaccine shortages within the region. During a recent virtual meeting, Dr. Etienne invited public and private manufacturers to submit proposals for transferring technologies or producing raw materials for mRNA vaccines, some of which PAHO already is in the process of reviewing.
In a related development, Pfizer and BioNTech announced a deal in late August with Brazilian pharmaceutical company Eurofarma to manufacture at least 100 million doses of the companies’ vaccine annually for distribution within the region, beginning next year. An additional 540 million doses are needed to ensure every country in the region can vaccinate 60% of the population.
INDIA Since mid-July, India has dramatically increased its SARS-CoV-2 vaccination rates in rural areas, where the majority of the population lives, with 70% of the nearly 120 million shots delivered in the past 3 weeks going to individuals in villages. That is up from about half in the beginning of May, when the country opened up vaccine eligibility to all adults. About 11% of the country’s population is fully vaccinated, and 37% have received at least one dose as of September 1, according to Our World In Data. While a boost in acceptance of vaccines in rural areas is promising news, India reported the largest single-day increase in new COVID-19 cases in 2 months on September 2, recording 47,092 cases. The densely populated Kerala state, which recently ended its biggest festival involving family and social gatherings, accounted for 70% of the new cases. The Kerala health ministry warned the public to take “adequate steps” to prevent the virus’s spread into surrounding states, and the federal government has warned that, like Kerala, the rest of India could see an increase in COVID-19 incidence as festival season gets underway this month and runs through early November.
Some parents and health experts are concerned the reopening of schools for the first time in 18 months amid an uptick in new cases could increase the risk of COVID-19 outbreaks. However, others say that without the ability to provide online schooling for poorer children, in-person learning is essential to keep kids on track. In Delhi, only older children will return to schools and strict measures are in place to help limit transmission, including vaccinated staff, limited classroom capacity, mandatory temperature checks, staggered lunch breaks, and physical distancing within classrooms. Several large Indian medical organizations are backing the resumption of in-person classes, urging governments to take a “calculated risk.” A recent serological survey conducted in 70 districts across 21 states showed 57% of 6- to 9-year-olds had antibodies to SARS-CoV-2, and 62% of 10- to 17-year-olds had antibodies, possibly boosting confidence in reopening schools. Still, some parents will be keeping their children at home for fear that a third wave could be looming.
NORTH KOREA North Korea has refused a shipment of nearly 3 million doses of China’s Sinovac SARS-CoV-2 vaccine from the COVAX facility, saying the vaccines should instead be provided to more seriously affected countries due to a limited global supply. Although the country has applied for assistance through COVAX, the government has yet to receive any doses, after the most recent development and a delay in a planned shipment of about 2 million AstraZeneca-Oxford vaccines earlier this year. Reportedly, the government rejected the AstraZeneca-Oxford vaccine over concerns of side effects. North Korea’s state media have reported incidents of breakthrough infections among vaccinated individuals and expressed overall doubt in the vaccines’ effectiveness. North Korea has reported zero confirmed COVID-19 cases to the WHO, but many health experts doubt those claims and worry that a large outbreak could overwhelm the country’s outdated healthcare infrastructure. In June, Supreme Leader Kim Jong-Un said the country’s COVID-19 situation was grave, without specifying details, and publicly chastised several high-ranking officials for failing to implement long-term preventive measures. Both the US and South Korea have discussed possibly offering humanitarian assistance to the impoverished nation, and Russia earlier this year offered to provide its Sputnik V vaccine, although it is unclear whether North Korea accepted.
by ponchi101 Florida: straight out of totalitarian regimes. If you don't report something that is happening, then it is not happening.
Colombia. Country is fully open, with everybody wearing their masks. Vaccination keeps going on; yesterday I received my SMS from my health provider for my appointment, for next week. Of course, I told them I am already vaccinated, but I really wanted to tell them a big F.Y.
Mu variant will test the vaccines down here. But what we need is more vaccines. Nobody here is anti-vaxx in that aspect (except my looney friend).
by ti-amie
ponchi101 wrote: ↑Fri Sep 03, 2021 6:23 pmFlorida: straight out of totalitarian regimes. If you don't report something that is happening, then it is not happening.
Colombia. Country is fully open, with everybody wearing their masks. Vaccination keeps going on; yesterday I received my SMS from my health provider for my appointment, for next week. Of course, I told them I am already vaccinated, but I really wanted to tell them a big F.Y.
Mu variant will test the vaccines down here. But what we need is more vaccines. Nobody here is anti-vaxx in that aspect (except my looney friend).
by dryrunguy It would be one thing if Florida officials (read: DeSantis) were committed to reporting data in the most accurate way possible because it reflects the best scientific integrity (e.g., the dates people actually DO die rather than the day deaths are reported--makes perfect sense).
But that's not the motivation in this case at all. And that's not an appropriate reporting strategy in the midst of a pandemic that refuses to go away because of clowns like DeSantis and his OAN-, Fox- and QAnon-drenched minions.
This happened near me. It wasn't just over a mask. The kid had to quartantine (and miss some kind of field trip, from what I gathered) because of a COVID exposure in the class/school. He wasn't the only one. Still, way over the top, no matter what the circumstance.
by dryrunguy Ponchi asked the question several days back, though I don't recall exactly how he phrased it. It was something to the effect that GOP policy related to COVID is basically killing the Republican base.
Now we have some hard data beginning to document precisely what's happening. Now, I think MSNBC is jumping the gun a little and perhaps being even being a bit selective in terms of how it is interpreting these data (see link), which MSNBC does from time to time. Just because a county voted 70-80% for Trump, who is the other 20-30%? White Democrats? People of color? And then you don't know for sure how many people didn't vote at all, which is going to include a lot of rural people of color, especially in states like Louisiana, Mississippi, and Alabama--just to name a few. What is their representation among COVID deaths in red counties?
But all that said, even if one tried to get highly creative and avoid the statistical probabilities, I don't see how these data are anything BUT completely damning.
by ti-amie How it started:
How it ended:
Even I can see the lawsuit that would come from this sitting at my kitchen table.
ETA:
southpaw @nycsouthpaw
·
39s
Correx: Two different judges on the two decisions; it’s the same case in the same court; and the latter judge reversed the former’s decision. Apologies.
by dryrunguy Meanwhile in Texas...
by ponchi101 That is freaking sickening. This virus is killing you even though YOU DON'T HAVE IT.
Anyone want to set the over/under on how long it takes DeSantis and company to sue?
by patrick What is the goal? I am taking under
by ponchi101 A display of power? If one doctor can decide that he will not treat unvaccinated people, maybe hospitals can switch their triage protocol and stop allowing COVID people in and let in others in need of ICU's and extensive care, who are in danger (as the video posted by Dry shows).
by ti-amie
by ti-amie
by ponchi101 Really, please, Dear God-I-Don't-Believe-In, just come down and stop this charade. Really
(New Age Unicult founder? Where is the line in the sand? )
by Suliso I read up about that woman (my mistake). One of her projects is to establish a brothel with sex dolls where men would pay 7,000 $ to take a virginity of a doll. I wish I was just making it up...
by mmmm8 Is this like the Church of the Flying Spaghetti Monster satire, but for anti-vaxxers?
by Suliso
mmmm8 wrote: ↑Thu Sep 09, 2021 8:00 pm
Is this like the Church of the Flying Spaghetti Monster satire, but for anti-vaxxers?
If you figure it all out let us know as well.
by dryrunguy It's The Onion on Steroids.
by ti-amie I am usually neutral on social media trends - I mostly ignore them hence my ignorance about how to maneuver around Instagram - but this whole thing about "influencers" drives me right up the wall. It's toxic and really needs to be stopped.
by ponchi101 If you are so brainless that you let A TWEET INFLUENCE YOU, well...
$7,000 to take the virginity of a doll? Ok, excuse me for being a male pig here, but for $7K, it has got to be HELEN OF TROY. Alive.
by dryrunguy Here is the latest Situation Report. I don't know what's worse... The use of ivermectin in Arkansas jails or the crisis standards of care in Idaho, and soon, other states.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 223 million cumulative cases and 4.6 million deaths worldwide as of September 9. Global weekly incidence has held relatively steady at 4.5 million new cases per week for the past 4 weeks. Similarly, global weekly mortality has held steady at approximately 67-68,000 deaths per week over that same period.
Global Vaccination
The WHO reported 5.35 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 6. A total of 2.02 billion individuals have received at least 1 dose, and 1.24 billion are fully vaccinated. Analysis from Our World in Data indicates that global daily vaccinations have declined sharply since September 1. Data from the most recent several days have tended to be artificially low due to reporting delays; however, the trend has persisted for more than a week. This indicates that there is an actual decline in daily vaccinations, which appears to be driven by a sharp decline in Asia*. Notably, daily vaccinations in China have decreased by more than 50% since August 29—down from 14.0 million doses per day to 6.5 million—which accounts for the majority of the change in Asia. Our World in Data estimates that there are 3.27 billion vaccinated individuals worldwide (1+ dose; 41.5% of the global population) and 2.32 billion who are fully vaccinated (29.5% of the global population). At the continent level, Oceania (40.5%) is on a trajectory to surpass the global average vaccination coverage (1+ doses), which would leave Africa (5.5%) as the only continent below the global average.
*The average doses administered may exhibit a sharp decrease for the most recent data particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
Toward the end of 2020, the cumulative global case fatality ratio (CFR) appeared to be approximately 2.3%. At that time, the cumulative CFRs in Africa, Europe, and North America—as well as the global average—were all converging on that number. The CFRs in Oceania (3.0%) and South America (3.3%) were slightly higher but declining slowly, and Asia (1.6%) was slightly lower. Since that time, the trends have shifted at the continent level. South America’s CFR has remained elevated, holding relatively steady at approximately 3.0% since January 2021. Oceania’s CFR decreased slowly through March 2021 before declining much more quickly, falling from 2.9% to 1.3% since that time. Africa’s CFR increased slightly to 2.5% and held relatively steady, and Asia’s fell to a low of 1.3% in May 2021 before rising back to 1.5%. Europe and North America have both tracked closely with the global average, declining slowly in 2021 to approximately 2.0%. In terms of the rolling weekly average, CFR trends have generally decreased since the spring or early summer 2021. While Europe’s current average CFR is lower than it was in late June, it has exhibited a marked increase since early August, up from a low of 0.76% on August 1 to 1.25%. Currently, South America (2.2%) is the only continent reporting CFR greater than 2%, and Oceania (0.7%) is the only continent reporting less than 1%.
CFR varies widely at the national level, with countries ranging from well below 1% to nearly 20%**. A total of 17 countries are reporting cumulative CFRs of 0.5% or less, including Bhutan (0.12%), Laos (0.10%), and Singapore (0.08%) with less than 0.25%. On the other end of the spectrum, 14 countries are reporting cumulative CFRs greater than 4% (more than double the global average), including Mexico (7.7%), Peru (9.2%), and Yemen (18.7%) with greater than 7.5%. Over time, as the cumulative incidence and mortality increased, many countries settled into a relatively consistent cumulative CFR value. The trends were generally higher at the beginning of their respective epidemics and then declined to a steady-state value.
**Vanuatu has reported exactly 25.00% consistently since April 2021, and the actual value of its CFR is unclear.
Despite that overall trend, a number of countries’ CFRs have changed substantially in recent months. Since January 1, 2021, 13 countries have reported increases in their cumulative CFRs of greater than 1 percentage point (pp). Notably, 7 of these countries are in Africa, where many national epidemics faced major COVID-19 surges later than other parts of the world. While Taiwan is not a member of the WHO, it is reporting the largest increase in CFR since January, up from 0.9% to 5.2% (+4.3pp). Over that same period, 14 countries reported decreases in their CFRs of greater than 1pp, including Yemen, which fell from 29.0% to 18.7% (-10.3pp) since January 1. Interestingly, this group includes a relatively balanced mix of countries reporting CFRs that are higher (6) and lower (8) than the global average. The decreases in 2 of these countries—Brunei (0.44%) and Mauritius (0.29%)—brought them below the 1% CFR threshold, each cutting their respective CFRs by more than three-quarters. Australia (from 3.2% to 1.5%), Fiji (4.1% to 1.1%), and Iran (4.5% to 2.16%) also cut their respective CFRs by more than half.
UNITED STATES
The US surpassed 40 million cumulative cases on September 4:
1 case* to 10 million: 288 days
10 to 20 million: 54 days
20 to 30 million: 83 days
30 to 40 million: 165 days
*The US CDC now reports 35 cumulative cases on January 23, 2020, the first day included in the official data.
The US CDC reports 40.5 million cumulative COVID-19 cases and 652,480 deaths. Daily incidence appears to have passed a peak; however, this is likely due, at least in part, to delayed reporting over the US Labor Day holiday weekend (September 4-6). We will have a clearer picture of the longer-term trends next week, once reporting catches up from the holiday. A similar trend is evident for daily mortality as well. At more than 1,000 deaths per day, we expect the US to surpass 660,000 cumulative deaths within the next week. This threshold corresponds to 1 death for every 500 people in the US. The US surpassed 1 death per 1,000 population on December 18, 2020**.
**Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 378 million cumulative doses of SARS-CoV-2 vaccines, and daily vaccinations peaked at nearly 830,000 doses per day on August 29. The 5-day window during which we expect delayed reporting still includes most of the US Labor Day holiday weekend, but the trend peaked prior to the holiday, which could indicate the early stages of a longer-term downward trend*. In light of the new US vaccination mandates announced on September 9, we will closely monitor trends in daily vaccinations for any effects of the mandates.
There are 208.3 million individuals who have received at least 1 vaccine dose, equivalent to 62.7% of the entire US population. Among adults, 75.3% have received at least 1 dose, as well as 13.9 million adolescents aged 12-17 years. A total of 177.4 million individuals are fully vaccinated, which corresponds to 53.4% of the total population. Approximately 64.5% of adults are fully vaccinated, as well as 10.8 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US COVID-19 RESPONSE In a speech delivered on September 9 from the White House, US President Joe Biden laid out a 6-pronged COVID-19 pandemic action plan, including new federal vaccine requirements for about two-thirds of the nation’s federal and private workforce, in an effort to stem the surge caused by the Delta variant and jumpstart economic recovery. President Biden excoriated unvaccinated individuals, saying “our patience is running thin” and blaming them for harming fellow Americans. He also pushed back against the politicization of the pandemic, promising to use the power of the federal government to take on state elected officials who are “undermining” the implementation of vaccination requirements, mask mandates, and other preventive measures.
Under the new plan, all private sector companies employing more than 100 people will be required to mandate vaccination or conduct weekly testing, affecting about 80 million people. Workers at healthcare facilities that receive Medicare or Medicaid funding, about 17 million people, also will have to be vaccinated, extending an earlier requirement for workers at nursing homes to include facilities such as hospitals, home-health agencies, and dialysis centers. President Biden also is requiring all executive branch employees and federal contractors to be fully vaccinated, with no testing option, covering several million more workers. Additionally, employees of Head Start programs and schools run by the Department of Defense and Bureau of Indian Education, about 300,000 people, will be required to be vaccinated.
President Biden announced several other pieces of the plan, including a doubling of fines for travelers who refuse to wear masks in transit stations or on airplanes or trains. The government also is working with manufacturers and large retailers, including Walmart, Amazon, and Kroger, to lower the cost of at-home SARS-CoV-2 tests and distribute the tests to easily accessible sites such as shelters and food banks. The Department of Defense plans to send more teams into hard-hit areas, and the federal government will increase shipments of monoclonal antibody treatments and offer new support to small businesses.
Altogether, President Biden’s plan represents the government’s most aggressive steps yet to urge US residents to get vaccinated and help get the economy back on track. However, several of the new measures are expected to undergo political and legal challenges. Reactions to the announcements were mixed, with physicians praising the efforts to get more people vaccinated, some experts saying the plan could be “too little, too late,” and some politicians saying the measures overstep the government’s authority and are “unconstitutional.” Though the White House has repeatedly said the federal government does not have the authority to implement broad vaccine requirements for the general population or require a federal vaccine passport, the new measures likely will help boost the nation’s vaccination rate.
US PANDEMIC PREPAREDNESS The US government on September 3 released a US$65.3 billion plan to improve the nation’s pandemic preparedness strategy over the next 10 years, to be in a stronger position to handle infectious disease outbreaks such as SARS-CoV-2. The plan, titled “American Pandemic Preparedness: Transforming our Capabilities,” outlines 5 key areas that require urgent attention and provide opportunities, including transforming medical defenses, such as vaccines, therapeutics, and diagnostics; ensuring situation awareness regarding disease threats; strengthening public health systems both domestically and internationally; building core capabilities, including manufacturing and supply chains and regulatory strategies; and managing the mission, with a focus similar to the effort that took astronauts to the moon in the late-1960s. Officials called for an immediate outlay of at least $15 billion to “jump start” the efforts and proposed establishing a centralized “Mission Control” that would draw on US government-wide expertise. US President Joe Biden signed an executive order on January 20 directing a whole-of-government review of US national biopreparedness policies and re-establishing the National Security Council Directorate on Global Health Security and Biodefense, and this plan is a core element of a larger government strategy resulting from that review.
On September 8, the Trust for America’s Health (TFAH) released a report saying that 20 years after the attacks of September 11, 2001, the US remains unprepared for public health emergencies. The report, “2021 Ready or Not: Protecting the Public’s Health from Diseases, Disasters and Bioterrorism,” calls on federal, state, and local policy makers to prioritize health security, amid the ongoing COVID-19 pandemic, raging wildfires in the West, and recent damaging weather events in the South and Northeast. The report makes several recommendations, including calling for more investments in public health infrastructure, workforce, and data systems at all levels.
GLOBAL COVID-19 SUMMIT US President Joe Biden is expected to announce plans for a global COVID-19 summit at the UN General Assembly meetings the week of September 20 to discuss vaccine access for low- and middle-income countries (LMICs). Topics could include how to ramp up vaccine manufacturing and distribution, improve oxygen supplies to countries in need, and cooperation on research and development for COVID-19-related products. According to officials, the Biden administration is setting up talks between the President and other national leaders, but a more formal announcement is expected soon. On September 2, administration officials announced the US government plans to invest $2.7 billion to increase domestic production of SARS-CoV-2 vaccine components as part of President Biden’s pledge to make the US an “arsenal of vaccines for the world.”
Additionally, a group of US lawmakers last week launched the COVID-19 Global Vaccination Caucus to advocate for vaccine manufacturing, production, and distribution in LMICs as a means to increase vaccination rates in those countries.
COVAX FORECAST The COVAX initiative, aimed at guaranteeing global access to SARS-CoV-2 vaccines, on September 8 cut its forecast for vaccine doses available for delivery between now and the end of the year, amounting to more disappointing news for the effort already hindered by production slowdowns, regulatory delays, export bans, and vaccine hoarding by wealthier nations. COVAX said it expects to have access to a total of 1.425 billion vaccine doses by the end of 2021, a number about 25% lower than the initiative’s July forecast. About 1.2 billion of those doses will be made available to 92 low-income countries (LICs) participating in the COVAX Advance Market Commitment (AMC). COVAX’s 2021 goal of delivering 2 billion doses is now projected to be reached in the first quarter of 2022. In its first 6 months of operation, the initiative has delivered more than 240 million vaccine doses, but experts predict 11 billion doses are needed worldwide to slow the spread of the virus.
BOOSTER DOSES WHO Director-General Dr. Tedros Adhanom Ghebreyesus this week doubled down on an appeal for a moratorium on vaccine booster dose programs through the end of September, this time calling on wealthy nations to delay administering third doses to large swaths of their populations through the end of 2021 and instead divert those supplies to low- and middle-income countries (LMICs). Dr. Tedros also said he was “appalled” by a pharmaceutical industry projection that SARS-CoV-2 vaccine production could exceed 12 billion doses by the end of the year and reach 24 billion by June 2022, berating manufacturers for fulfilling bilateral contracts with wealthy nations while low-income countries (LICs) are “deprived of the tools to protect their people.” In a statement regarding the projection, which was conducted by London-based Airfinity, the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) called on governments to step up efforts to equitably redistribute doses to LMICs by sharing “a meaningful proportion of their doses in a responsible and timely way through COVAX or other efficient established mechanisms.” About 5.4 billion vaccine doses have been administered globally, but about 80% of those have gone to high- or upper-middle income countries, according to the WHO.
Additionally, 2 of the WHO’s top officials denounced wealthy nations for hoarding SARS-CoV-2 vaccines, treatments, and protective equipment, saying the inequities in distribution are “unfair,” “immoral,” and prolonging the pandemic. The Airfinity model predicts that even if the world’s wealthiest nations vaccinated all those individuals currently eligible and provided third doses to vulnerable populations, they would still have 1.2 billion doses left for redistribution this year. On September 9, Africa CDC John Nkengasong and WHO Africa Regional Director Matshidiso Moeti called on wealthy nations to forego boosters and redirect those extra doses to LICs, particularly on the African continent, which has been struggling to receive adequate supplies.
Notably, in addition to obtaining sufficient vaccine supplies, LICs will need to significantly increase their health expenditures—by almost 57%—to cover the costs of vaccinating 70% of their populations, if a 2-dose regimen costs US$35 and associated distribution cost is US$3.70 per person. These costs—according to estimates from the Vaccine Affordability Index, part of the Global Dashboard on COVID-19 Vaccine Equity supported by the UN Development Programme (UNDP), the WHO, and the University of Oxford—likely will need to be covered by further donations, grants, or loans, as LICs face negative economic consequences due to the pandemic.
VACCINE DEVELOPMENT The COVID-19 pandemic prompted vaccine development to move at record speed, with more vaccines simultaneously being tested in clinical trials than ever before for any infectious disease. However, the development of next-generation SARS-CoV-2 vaccines is under threat, the Coalition for Epidemic Preparedness Innovations (CEPI) warned in a letter published September 7 in the journal Nature. According to Melanie Saville, CEPI’s Director of Vaccine Research and Development, most SARS-CoV-2 vaccines in use today were tested in placebo-controlled trials among unvaccinated individuals. However, as the number of vaccinated people increases, new vaccine candidates will need to be tested against existing vaccines instead of placebos. Therefore, manufacturers and governments must release doses of these “comparator vaccines” to support clinical trials testing new vaccines, particularly to see how they perform against new viral variants. But with most doses already spoken for in bilateral contracts that specifically spell out how the vaccines are to be used, current demand outpacing supply, and the possibility that a new vaccine will work better than the comparator, there is little incentive to release extra doses for studies. CEPI is working with manufacturers and governments to find workarounds to the issue, but unless a solution is found, the world will remain dependent upon the current vaccines authorized for use, even if new, more dangerous variants emerge.
DENMARK After nearly 550 days with restrictions to limit the spread of SARS-CoV-2, Denmark on September 10 lifted the last of its requirements, including no longer needing digital proof of vaccination to enter certain venues. This was the last of the restrictions, most of which have been lifted slowly since mid-August. The government stopped categorizing COVID-19 as a “socially critical disease,” attributing control of the virus to a successful vaccination rollout, strong epidemic control measures, and the efforts of the Danish people. More than 83% of eligible individuals are fully vaccinated, according to the Danish Health Authority. With fewer than 500 new COVID-19 cases reported daily and a reproduction rate less than 1, officials say they have the virus under control. However, they indicated they are prepared to reinstitute control measures if the number of COVID-19 hospitalizations begins to rise. The WHO has urged caution, warning the global situation remains critical. With large concerts already scheduled and people returning to “normal” life, the world is watching whether Denmark can remain restriction-free.
US HOSPITAL CRISIS STANDARDS OF CARE Hospitals in northern Idaho (US) this week began operating under “crisis standards of care,” allowing healthcare workers to ration care as facilities struggle to handle an influx of COVID-19 patients amid an increase in cases and staff shortages. Notably, Idaho has one of the lowest vaccination rates of any US state. The move, enacted by the Idaho Department of Health and Welfare for 10 hospitals and healthcare systems in the panhandle and north-central regions, allows hospitals to apportion certain resources, such as intensive care unit (ICU) beds, to patients they deem most likely to survive. Other patients will still receive care but might go without some life-saving medical equipment. The region is receiving federal assistance, with a 20-person team from the US Department of Defense, 150 National Guard troops, and about 200 federal contractors, but the state says the additional resources are not enough to handle the current surge.
Officials in neighboring Oregon also have warned the state is close to filling its ICU beds and activating crisis standards of care. Notably, Oregon last year said its crisis standards of care document was discriminatory, and in December 2020 replaced the document with 4 “crisis care principles,” developed with community input. The Oregon Association of Hospitals and Health Systems said the lack of crisis standards is “really troubling,” but the state’s Health Authority asked that providers apply the principles if necessary and noted that hospitals can implement their own crisis care standards and triage guidelines amid a public health emergency.
Officials in both states, as well as others including Louisiana and Texas, also are expressing concern over a rising number of child hospital admissions, as many schools around the country are opening. Pediatric ICUs typically have a smaller number of beds than adult ICUs and are filling quickly nationwide. The increase in childhood COVID-19 hospitalizations has led healthcare providers and hospital executives to implore adults to get vaccinated and use other preventive measures, such as mask wearing and physical distancing, to help protect children, especially those under age 12 who are not yet eligible for vaccination in the US.
VACCINE MANDATES Even prior to US President Joe Biden’s September 9 announcement of federal vaccine mandates, including for larger private companies, several other vaccine mandates in the US made the news over the past week. United Airlines, which announced its mandate in early August, is requiring all employees to be vaccinated by September 27 (5 weeks from the Pfizer-BioNTech vaccine receiving full FDA approval). This week, United announced that employees who receive an exemption will be placed on temporary leave while the airline implements appropriate safety precautions for unvaccinated employees. Those who receive a medical exemption will reportedly be placed on temporary medical leave, and those who receive a religious or personal beliefs exemption will be placed on unpaid personal leave. According to United Airlines officials, more than half of its employees who were unvaccinated when the mandate was announced have been vaccinated since then, an indication that the policy could be encouraging vaccination.
The Los Angeles Unified School District (California)—the United States’ second largest school district, covering nearly 650,000 students—is mandating SARS-CoV-2 vaccination for all students aged 12 years and older. The county school board voted unanimously in favor of the mandate (7-0, with 1 recusal). The school district previously mandated vaccinations for all employees, without a testing option that would allow individuals to opt out of vaccination. The student mandate will be implemented in phases, starting with students who participate in in-person extracurricular activities (eg, band, clubs, sports), who must be fully vaccinated by October 31. All other students must be fully vaccinated by December 19, and students who turn 12 must be fully vaccinated no later than 8 weeks after their 12th birthday. The school district began offering vaccinations at schools via a mobile vaccination clinic on August 30. Notably, the US FDA has issued an Emergency Use Authorization (EUA) for use of the Pfizer-BioNTech vaccine in children 12-15 years old, but none of the currently available vaccines have received full approval for this age group. The announcement was met with opposition from some parents, and anti-vaccine organizations have already indicated that they will file lawsuits that aim to overturn the policy.
SCHOOL MASK MANDATES Legal and legislative battles over mask mandates to help mitigate the spread of SARS-CoV-2 in schools continue across the US. In Florida, a Leon County judge ruled against Governor Ron DeSantis on September 8, allowing school districts to mandate mask use while the case challenging the state’s ban on mask mandates continues. Hours later, DeSantis’ administration filed a 41-page emergency motion asking the 1st District Court of Appeal to allow the executive order prohibiting mask mandates to remain in effect. Reportedly, the parents who filed the initial lawsuit filed their response Thursday evening, but it remains unclear when the appeals court will rule on the motion or the lawsuit itself. At least 13 Florida school districts have implemented mask mandates that do not give parents an option to opt out of the mandate, which violates the executive order. At a September 8 news conference, Governor DeSantis said he expects to win the case on appeal.
More school districts across the country are implementing mask mandates as COVID-19 cases due to the Delta variant surge, in some instances leading to the deaths of teachers. But most allow for medical or parental exemptions, allowing many students to opt out of the requirements—up to 30% in one Tennessee district—even amid rising numbers of COVID-19 cases among children. Advocacy groups, some physicians, and even state and local governments are advising parents how to write exemption letters or use federal disability laws to avoid mask mandates. In Kentucky, both houses of the state General Assembly have advanced bills that would abolish a statewide mask mandate in K-12 schools implemented by Governor Andy Beshear. According to a new USA TODAY/Ipsos poll, about two-thirds of those surveyed support school- or state-implemented mask mandates for teachers (65% of the general public, 64% of parents with school-aged children) and mask mandates for students (65% and 62%, respectively).
HYBRID IMMUNITY A preprint published in bioRxiv is the latest among several studies evaluating hybrid immunity to SARS-CoV-2. Hybrid immunity, which some are calling “superhuman immunity,” can exist in people previously infected with SARS-CoV-2 and who are fully vaccinated, as their immune systems can produce an extremely powerful immune response, including very high levels of antibodies with wide variant-neutralizing capability. For the bioRxiv study, which is not yet peer-reviewed, researchers created ‘polymutant’ spike proteins that resisted polyclonal antibody neutralization to a degree similar to already circulating variants of concern (VOCs). They found that 20 naturally occurring mutations in the SARS-CoV-2 spike protein are enough to confer almost complete resistance to the polyclonal neutralizing antibodies produced independently by convalescents and mRNA vaccine recipients. Notably, however, they found that plasma from previously infected individuals who later received mRNA vaccination neutralized the synthetic ‘polymutant’ as well as related but diverse sarbecoviruses, resulting in the so-called hybrid immunity. The sarbecoviruses included SARS-CoV-1, which caused the 2009 SARS pandemic, two viruses found in pangolins, and one in bats.
Another study published in the New England Journal of Medicine last month found similar results among people who had previous SARS-CoV-1 infection and were vaccinated with the Pfizer-BioNTech SARS-CoV-2 vaccine. This study examined the breadth of antibody cross-neutralization against 10 different sarbecoviruses: 7 from the SARS-CoV-2 clade and 3 from the SARS-CoV-1 clade, which overlap with the viruses included in the bioRxiv study. The individuals produced broad-spectrum antibodies capable of cross-clade neutralization of known VOCs and potentially emerging viruses. Though previous infection together with vaccination might help improve immune responses to future exposure, scientists warn that people should not intentionally expose themselves to infection with SARS-CoV-2.
REDUCED RISK OF “LONG COVID” AMONG VACCINATED Individuals who are fully vaccinated against SARS-CoV-2 appear to have a lower risk of developing post-acute sequelae of COVID-19 (PASC), so-called “long COVID,” than unvaccinated people, even when they experience breakthrough infections, according to a study published in The Lancet Infectious Diseases. Researchers examined data self-submitted by more than 1.2 million adults in the UK who use the COVID Symptom Study phone app, and only included the mRNA vaccines from Pfizer-BioNTech or Moderna and the viral vector vaccine from AstraZeneca-Oxford. Of those fully vaccinated, only 0.2% reported a breakthrough infection. Among those people who received 2 doses of vaccine, the risk of long COVID—defined as having symptoms lasting at least 4 weeks after infection—was reduced by almost half, the risk of hospitalization was reduced by 73%, and the risk of acute symptoms was reduced by 31%. While the researchers noted the study had limitations, including that the data were self-reported, they said it is “encouraging” that the overall proportion of cases who had long-lasting symptoms is reduced among fully vaccinated individuals and called for additional research to better characterize long COVID.
UNREPORTED DEATHS IN NURSING HOMES Due to delays in reporting case and mortality data, researchers suspect that nursing homes, with residents already at high risk of SARS-CoV-2 infection and illness, may have a higher burden of COVID-19 than previously reported in federal data. According to a cross-sectional study published in JAMA Network Open and involving 15,307 US nursing homes in the National Healthcare Safety Network (NHSN), researchers estimate there were more than 68,000 COVID-19 cases and 16,000 related deaths nationally that were not recorded in federal data during the early months of the pandemic, through May 24, 2020. These numbers represent 11.6% of COVID-19 cases and 14% of COVID-19 deaths among nursing home residents in 2020. Overall, a mean of 43.2% of all COVID-19 cases and 39.6% of COVID-19 deaths in nursing homes counted by state health departments went unreported in federal databases, the research suggests. Researchers and policymakers are considering that SARS-CoV-2 outbreaks in nursing homes may have been more onerous than previously believed, and a failure to accurately collect case and death data may have led to inaccurate conclusions about the role of nursing homes in COVID-19 outbreaks.
IVERMECTIN USE IN ARKANSAS JAIL A doctor at an Arkansas (US) jail is under investigation after using the drug ivermectin to treat inmates with COVID-19, reportedly without their consent and despite warnings from the US FDA to not use the drug to treat or prevent the disease outside of approved clinical trials. Several inmates at a Washington County jail said they were told the pills were antibiotics, vitamins, or steroids, not ivermectin, which is an antiparasitic primarily used in livestock. Jail physician Dr. Rob Karas and Washington County Sheriff Tim Helder both confirmed that ivermectin was prescribed to inmates, beginning late last year, but they claimed detainees consented to taking the pills. However, at least 3 inmates said they would never have taken the drug if they knew it was ivermectin, indicating they felt as though they were being experimented on. After hearing from inmates, the American Civil Liberties Union (ACLU) called for the administration of ivermectin to end immediately and said inmates are prepared to file a lawsuit to end the practice. As we previously reported, cases of ivermectin poisoning have risen over the past several weeks, as some conservative lawmakers, groups, and celebrities tout the drug, which has not been proven to work as prevention or treatment of SARS-CoV-2 infection. Even the drug's manufacturer, Merck, released a statement in February announcing that the drug was not effective in treating COVID-19 and should not be used to do so. The Arkansas case is a disturbing example of how jail and prison detainees continue to be dehumanized and exploited for medical experimentation in the US.
by ponchi101 "You're livin in your own Private Idaho. Idaho.
You're out of control, the rivers that roll,
you fell into the water and down to Idaho.
Get out of that state,
get out of that state you're in.
You better beware.
Get out of that state!!!
Get out of that state!!!
You're living in your own Private Idaho,
livin in your own Private.... Idaho"
by dmforever I thought people here might appreciate this. If I posted this before, I apologize in advance.
Kevin
by ti-amie
by ti-amie
by dryrunguy Meanwhile, in Toulouse...
by Jeff from TX
dmforever wrote: ↑Sat Sep 11, 2021 5:06 pm
I thought people here might appreciate this. If I posted this before, I apologize in advance.
Kevin
Kevin,
The interesting thing about this video is that it was done over a year ago pre-vaccines, but even more appropriate today given events in Idaho and the vaccine resistance among Trump supporters.
dmforever wrote: ↑Sat Sep 11, 2021 5:06 pm
I thought people here might appreciate this. If I posted this before, I apologize in advance.
Kevin
Kevin,
The interesting thing about this video is that it was done over a year ago pre-vaccines, but even more appropriate today given events in Idaho and the vaccine resistance among Trump supporters.
Great point!
And if I may put in a plug for Jill (Jill Sobule), she's a fabulous, highly underrated singer songwriter. You can check her out on Youtube. Try "America Back", "I Kissed a Girl", " San Francisco", "Mexican Wrester", or "Where is Bobby Gentry?" (Full disclosure--I "produced" one of her CDs, which really just means I donated a little money for her to make one of her CDs.) If you ever get the chance to see her live, do it. She's one of a kind.
Kevin
by mmmm8 That's really cool, Kevin! I think this video popped up somewhere else for me last year, so I had checked her out!
by dmforever
mmmm8 wrote: ↑Mon Sep 13, 2021 7:56 pm
That's really cool, Kevin! I think this video popped up somewhere else for me last year, so I had checked her out!
Just to be clear, I wouldn't know how to even turn on a recording device, let alone produce anything. It was sort of a fun way for her to get support before the whole Patreon thing was a thing. I'm glad you like her. I know very few singer-songwriters who are as consistently excellent as she is.
Kevin
by Deuce .
Interesting that the NHL is requiring all players, coaches, trainers, staffers, and front-line employees be fully vaccinated...
by dryrunguy Here's the latest Situation Report. It's packed. I was most intrigued by the paragraph on France's former Health Minister being charged with "endangering the health of others" based on comments she made early on in the pandemic. Also intriguing was the paragraph on the gorillas at the Atlanta zoo.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 225 million cumulative cases and 4.63 million deaths worldwide as of September 13. Global weekly mortality decreased substantially for the first time since early June, falling 12.7% from the previous week. Weekly mortality decreased as well—for the first time since late June*—down 7.3% compared to the previous week.
*With the exception of the week of July 19, when Ecuador reported 8,786 deaths.
Global Vaccination
The WHO reported 5.53 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 13. A total of 3.2 billion individuals have received at least 1 dose, and 2.3 billion are fully vaccinated. Analysis from Our World in Data indicates that global daily vaccinations leveled off after a week of sharp decline, holding relatively steady at 32-33 million doses per day*. The global trend continues to closely follow Asia. Our World in Data estimates that there are 3.3 billion vaccinated individuals worldwide (1+ dose; 42.3% of the global population) and 2.4 billion who are fully vaccinated (30.1% of the global population). In terms of 1+ dose coverage, we expect Oceania (42.1%) to surpass the global average in the next several days, which would leave Africa (5.8%) as the only continent below the global average.
*The average doses administered may exhibit a sharp decrease for the most recent data particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 41.0 million cumulative COVID-19 cases and 658,410 deaths. Daily incidence appears to have passed a peak; however, this likely still includes some effects from delayed reporting over the US Labor Day holiday weekend (September 4-6). A similar trend is evident for daily mortality as well. Even with the delayed reporting over the Labor Day weekend, the average daily mortality is still more than 1,000 deaths per day, and we expect the US to surpass 660,000 cumulative deaths in the next 1-2 days. This threshold corresponds to 1 death for every 500 people in the US. The US surpassed 1 death per 1,000 population on December 18, 2020**. The US is #22 globally in terms of per capita cumulative mortality.
**Changes in the frequency of state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 381 million cumulative doses of SARS-CoV-2 vaccines, and daily vaccinations peaked at nearly 834,000 doses per day on August 29 and then decreased sharply over the Labor Day holiday weekend. Considering the expected delays in vaccination reporting, it could be another week or so before we can reassess the longer-term trends*. There are 209.7 million individuals who have received at least 1 dose, equivalent to 63.2% of the entire US population. Among adults, 75.7% have received at least 1 dose, as well as 14.1 million adolescents aged 12-17 years. A total of 179.0 million individuals are fully vaccinated, which corresponds to 53.9% of the total population. Approximately 65.0% of adults are fully vaccinated, as well as 11.1 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
VACCINE EFFECTIVENESS With about 54% of the total US population vaccinated, public health officials continue to urge people to get vaccinated and protect themselves from severe illness, hospitalization, and death. As daily incidence and mortality continue to rise, including among younger individuals, evidence continues to emerge regarding the effectiveness of SARS-CoV-2 vaccines. Recent studies from the US CDC show that unvaccinated individuals are 10 times more likely to be hospitalized and 11 times more likely to die from COVID-19 than vaccinated individuals, illustrating the effect of SARS-CoV-2 vaccines in terms of preventing severe disease and death. A study conducted by the CDC’s COVID-19 Response Team evaluated vaccine effectiveness after the Delta variant became dominant in the US, based on data collected from June 20-July 17. The researchers found that vaccinated individuals were 4.5 times less likely to be infected with SARS-CoV-2 compared with vaccinated individuals. While the estimated vaccine effectiveness against infection fell from 91% before June 20 to 78% after that date, effectiveness remained greater than 90% against both hospitalization and death.
ARGUMENT AGAINST BOOSTERS In an expert review published September 13 online in the peer-reviewed journal The Lancet, a group of US and international scientists claim current evidence does not support providing booster doses of SARS-CoV-2 vaccines to the general public. The group—including 2 departing US FDA officials and WHO experts—said that any decision to provide additional vaccine doses should be evidence-based, concluding that despite a small drop in protection against symptomatic disease caused by the Delta variant, authorized vaccine regimens continue to provide high levels of protection against severe disease and hospitalization for all major SARS-CoV-2 variants. The authors acknowledged that some additional doses might be needed immediately for certain elderly and immunocompromised populations, but they encouraged prioritizing primary immunizations over booster shots for the general public.
The authors also acknowledged that booster doses might be necessary in the future due to waning immunity or the emergence of a vaccine-resistant variant but that current evidence does not warrant additional doses now because “efficacy against severe disease remains high.” The authors noted that currently available vaccine doses could save more lives and provide better protection against the emergence of new SARS-CoV-2 variants if used in previously unvaccinated populations, especially those in low- and middle-income countries.
GLOBAL COVID-19 SUMMIT US President Joe Biden plans to call on global leaders to make new commitments to help end the COVID-19 pandemic during a virtual summit to be hosted by the White House next week. The list of goals, obtained by The Washington Post, includes fully vaccinating at least 70% of the world’s population within the next year; improving access to medical supplies and treatments, including the establishment of a US$2 billion strategy to support “oxygen ecosystems”; and forming and financing a global health security financial intermediary fund (FIF) this year. The event, the Global COVID-19 Summit: Ending the Pandemic and Building Back Better, is expected to bring together heads of state, global health experts from non-profit organizations and academia, and private sector representatives, and is scheduled to be held September 22 during the UN General Assembly meetings.
In related news, the US government reportedly is is in discussions with India to lift its ban on vaccine exports. India is the world’s largest manufacturer of vaccines, but the government halted exports of SARS-CoV-2 vaccines in March 2021 when the country was experiencing a surge in COVID-19 cases. The ban has been particularly hard on lower-income countries (LICs) that expected to receive Indian-produced vaccines through the COVAX facility. India sold or donated about 66 million vaccine doses to nearly 100 LICs prior to the ban, the government claims. According to UNICEF, the US is the largest donor of SARS-CoV-2 vaccines globally, based on publicly available data. The US has donated and delivered more than 114 million doses, followed by China at 34 million. The WHO estimates 11 billion doses are needed to fully vaccinate at least 70% of the world’s population.
US CHILD VACCINATION The number of new COVID-19 cases among children in the US has risen exponentially in recent weeks, according to the American Academy of Pediatrics, causing many parents to become increasingly eager to vaccinate their young kids, especially as they return to school. But none of the available vaccines are authorized for children under age 12, prompting the US FDA this week to warn parents to not seek out SARS-CoV-2 vaccines for children who are not yet eligible and physicians not to use the now fully approved Pfizer-BioNTech vaccine “off-label” in younger patients, as they might need smaller dosages. The regulatory agency said it is “working around the clock” to support the review process necessary to safely and expeditiously authorize or approve a vaccine for children. US health officials say they are hopeful that a vaccine will be available for 5- to 11-year-olds by the end of the year. Pfizer and BioNTech said they plan to present data on their vaccine among younger children “in the coming weeks,” raising hopes that a vaccine could be made available by the end of October. Until the FDA authorizes a vaccine, families should continue taking other precautions, including mask wearing.
PREGNANCY LOSS Pregnant people are at risk of severe illness due to COVID-19, and infection with SARS-CoV-2 during pregnancy is associated with several adverse maternal and neonatal outcomes, including death, stillbirth, and miscarriage. In Mississippi (US), health officials are urging pregnant individuals to be vaccinated after noting they have recorded 72 fetal deaths past 20 weeks’ gestation since the beginning of the pandemic, double the pre-pandemic rate. State officials also are investigating the deaths of 8 infected pregnant people over the past 4 weeks, all of whom were unvaccinated. Only about 25% of pregnant people have been vaccinated during pregnancy since December 2020, according to US CDC data.
Several recently published studies support CDC guidance for pregnant people to get vaccinated, showing that expectant individuals who receive a SARS-CoV-2 vaccine are not at an increased risk of miscarriage. In a research letter published online in the Journal of the American Medical Association (JAMA), researchers concluded that among more than 105,000 pregnancies, miscarriages were no more likely to occur within 28 days of vaccination compared with ongoing pregnancies regardless of which vaccine was received and gestational age. Similarly, in a letter published in the New England Journal of Medicine (NEJM), CDC researchers said that although risk of miscarriage rose with increasing maternal age among vaccinated pregnant individuals, the risk was within the expected range of 11-22% of recognized pregnancies. Additionally, CDC researchers updated a previous NEJM study published in June in response to a letter published last week, finding the estimated risks of miscarriage among vaccinated pregnant people remained consistent with the risk reported in the general population. Taken together, the studies and the real-world data support the need for vaccination of pregnant individuals to help lower the risk of adverse maternal and fetal outcomes amid the pandemic.
DISRUPTIONS IN HOSPITAL CARE An influx of COVID-19 patients and staffing shortages continue to plague hospitals across the US, with many having to turn away patients or pause certain services. On September 1, a 73-year-old Alabama man died of cardiac complications after emergency staff contacted 43 hospitals in 3 states searching for a cardiac intensive care unit (ICU) bed, as most were full with COVID-19 patients. The man was transported to a hospital 200 miles from his home, where he died. ICUs in Alabama have been at-capacity in recent weeks amid a surge in cases due to the highly contagious Delta variant and low vaccination rates. In the man’s obituary, his family urged people to get vaccinated “in an effort to free up resources for non-COVID-related emergencies.” Recent data from the US CDC show that unvaccinated people are more than 10 times more likely to be hospitalized and 11 times more likely to die from COVID-19 than people who are vaccinated.
In Washington state, already-stressed hospitals are taking on even more COVID-19 patients from neighboring Idaho, where some hospitals in the northern part of the state are operating under crisis standards of care. Some leaders in Washington—where indoor masking is mandatory and many workers are required to be vaccinated—are expressing frustration over Idaho’s lack of aggressive efforts to confront the pandemic, even amid a surge in cases, saying the situation is an example of how one state's crisis can intensify a crisis in another.
The situation helps to spotlight the importance of vaccination, but in some states, even vaccine requirements are backfiring. A hospital in upstate New York said it will “pause” infant deliveries on September 24 after 6 maternity unit employees resigned over the state’s SARS-CoV-2 vaccination requirements for all hospital and long-term care facility workers. Though the employee vaccination rate among Lewis County Health System employees is 73%, 165 employees remain unvaccinated with the September 27 deadline to get at least one shot looming. The health system’s CEO said he plans to focus on recruiting healthcare workers who are vaccinated or get assistance from the state to be able to restart deliveries in the county.
ENGLAND VACCINE PASSPORTS England has abandoned its previously announced plan to implement a SARS-CoV-2 vaccine passport program by the end of this month that would have required people to show proof of vaccination to enter the country’s nightclubs and certain other crowded venues, UK Health Secretary Sajid Javid told the BBC on September 12. The announcement was made following opposition from some members of Parliament as well as representatives of the hospitality industry, who said such a program would create a burden for businesses and infringe on residents’ rights. Speaking on the Andrew Marr Show, Secretary Javid said the government decided against the passports after “properly” looking at the issue and determining other factors could help keep COVID-19 incidence down, including high vaccine uptake, testing, surveillance, and treatments. Some people suggested the passport proposal simply was a ruse to encourage young people to be vaccinated, although Secretary Javid hinted the government could reverse course again if the number of new cases rises. About 66% of the population of England is fully vaccinated. Several days prior to the announcement, British researchers published a paper in EClinicalMedicine casting doubt on whether vaccination passport programs would incentivize more people to get the shots and calling for additional research into the matter.
FRANCE Former French Health Minister Dr. Agnès Buzyn has been charged with “endangering the lives of others” for her management of the COVID-19 pandemic, after a formal investigation found sufficient evidence to prosecute. Dr. Buzyn, who resigned in February 2020 to run for Mayor of Paris, has come under fire for her initial comments on the pandemic, when she said there was little risk of the new coronavirus first detected in Wuhan, China, spreading among the general population. But before she left her post, Dr. Buzyn backpedaled, warning President Emmanuel Macron that “the tsunami has yet to come.” At a hearing on September 10, Dr. Buzyn said she welcomed “an excellent opportunity for me to explain myself and to establish the truth,” and indicated she plans to appeal. The case, which marks one of the first worldwide where a leading public official is being held legally accountable for their handling of the pandemic, presents a challenge for President Macron, who will be campaigning for reelection over the coming year.
SARS-CoV-2/INFLUENZA VACCINES With research ongoing into the necessity of SARS-CoV-2 vaccine booster doses, at least 2 pharmaceutical companies are banking on the need for annual shots, similar to influenza vaccinations, and working on combining the 2 vaccines. Moderna on September 9 said it is developing a single shot containing a booster dose for its SARS-CoV-2 vaccine and an experimental flu vaccine. The company said it eventually hopes to add vaccines for other respiratory diseases, including respiratory syncytial virus (RSV), into a single annual shot. On September 8, Novavax announced it has begun a Phase 1/2 clinical trial testing a combination vaccine using the company’s vaccine candidates for seasonal influenza and SARS-CoV-2. Both vaccines have been tested in Phase 3 trials, but neither has received regulatory authorization or approval. Combination vaccines have several potential benefits, including lowering the number of shots needed annually, improving vaccine coverage rates, and reducing costs for healthcare facilities and individuals.
COVID-19 IN GORILLAS Several western lowland gorillas at Zoo Atlanta have tested positive for the Delta variant of SARS-CoV-2 after employees of the zoo noticed some members of the gorilla population exhibiting symptoms such as coughing, nasal discharge, decreased appetite, and decreased activity. A total of 20 gorillas live in 4 troops at the zoo, and officials said that 18 of them were experiencing varying degrees of symptoms. Sam Rivera, Senior Director of Animal Health for Zoo Atlanta, said the gorillas are receiving the best care possible and that at-risk members of the population are being treated with monoclonal antibodies. The gorillas will be provided with the Zoetis SARS-CoV-2 vaccine specifically designed for animals when they recover. Zoo Atlanta also announced plans to vaccinate their Bornean orangutan, Sumatran orangutan, African lion, and clouded leopard populations.
Zoo Atlanta expressed concern that the infections occurred despite rigorous safety measures when team members interact with great ape populations. Viral transmission likely happened due to interactions with an asymptomatic but infected team member who was fully vaccinated and donning the appropriate personal protective equipment. The team member did not test positive until after the incident. The zoo provided further assurance that safety measures such as the use of N95 masks, increased ventilation, modified cleaning protocols, and social distancing barriers between the gorillas and team members have been implemented. The distance between the gorillas and visitors to the zoo would make zoonotic transmission of the disease unlikely, and the US CDC states that animals are not a significant source of disease transmission to humans.
by JazzNU She caused a mfcking international incident because her cousin's friend couldn't just admit he cheated, got an STD and that's why his wedding was called off and blamed it on the vaccine thinking that was a brilliant plan and no one in her Mensa crew could figure any of this out before making it public. Can't make this ish up.
by ti-amie Another edition of covidiocy:
by JazzNU Did you read about the 29-year old who was supposed to be getting married and is now going to have her funeral services in the same church she was to be married in?
Her profession? Surgical technician. I'm so very done with these covidiots, but it's doubly offensive when they work in healthcare. Didn't want to get vaccinated because of the fake fertility issues many of this dimwitted crew like to pretend exist. And of course she asked for a vaccine prior to going on the ventilator.
by ponchi101 You know this position is entirely insane when something that is indeed tragic only leaves you shaking your head in disbelief, and feeling absolutely no empathy for the dead person.
by ti-amie
ponchi101 wrote: ↑Fri Sep 17, 2021 3:05 pm
You know this position is entirely insane when something that is indeed tragic only leaves you shaking your head in disbelief, and feeling absolutely no empathy for the dead person.
I struggle with this. I read these tales of woe and all I think is that they've effed around and found out.
by dryrunguy Here's the latest Situation Report. I have included the link to the 4 reports on Black and Hispanic/Latino communities in AL, CA, ID, and MD.
::
New from the Center: The CommuniVax Coalition, led by the Johns Hopkins Center for Health Security and the Department of Anthropology at Texas State University, released 4 new reports that share findings from local rapid research within Black and Hispanic/Latino communities in Alabama, California, Idaho, and Maryland. The reports highlight the urgent need to humanize delivery and communication strategies for SARS-CoV-2 vaccines, develop heterogenous messaging, and implement anchor vaccination efforts in severely affected communities in a holistic “whole person” recovery process.
EPI UPDATE The WHO COVID-19 Dashboard reports 226 million cumulative cases and 4.65 million deaths worldwide as of September 16.
Global Vaccination
The WHO reported 5.63 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 15. A total of 3.25 billion individuals have received at least 1 dose, and 2.34 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline. After peaking 3 times at more than 42 million doses per day between late June and early September, the average has fallen to fewer than 30 million. In mid-July, between the 2 highest peaks, the averaged dropped to 20 million before rebounding, so the longer-term trend remains uncertain*. The global trend continues to closely follow Asia.
Our World in Data estimates that there are 3.37 billion vaccinated individuals worldwide (1+ dose; 42.8% of the global population) and 2.45 billion who are fully vaccinated (31.1% of the global population). Since mid-August, China has updated its cumulative 1+ dose vaccination totals every 7-14 days, which causes a substantial jump in the global totals. Oceania (43.7%) surpassed the global average in terms of 1+ dose coverage. At 5.9% coverage, Africa is now the only continent below the global average, by a factor of more than 7, illustrating the stark disparity in access to SARS-CoV-2 vaccines.
*The average daily doses administered may exhibit a sharp decrease for the most recent data particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 41.6 million cumulative COVID-19 cases and 666,440 deaths. After decreasing following the US Labor Day holiday weekend (September 4-6), daily incidence over the past 5 days. The US appeared to be approaching a peak or plateau prior to the holiday weekend, so it is unclear how the trend over the coming week will compare to the pre-holiday trend. The current average (146,182 new cases per day) is still approximately 13,000 fewer new cases per day than the most recent high on August 31. A similar trend is evident for daily mortality as well, although the current average has already surpassed the pre-holiday peak. With 1,447 deaths per day, the US is at its highest daily mortality since March 1*. The US reported more than 1,900 deaths each of the last 2 days, the highest single-day totals since February 19. The US surpassed 660,000 cumulative deaths on September 13, which corresponds to 1 death for every 500 people in the US. The US surpassed 1 death per 1,000 population on December 18, 2020.
*Changes state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
If California continues on its current trajectory, it could soon drop from the High community transmission (≥100 new weekly cases per 100,000 population) to Substantial (50-99.9). It was briefly categorized as Substantial this week, but it moved back up to High as surveillance data caught up from the Labor Day holiday weekend. Connecticut has also been holding relatively steady at slightly more than 100 and could fall to the Substantial category as well. The CDC also includes test positivity in its community transmission determination, but test positivity is not reported for either California or Connecticut.
California passed its most recent peak in mid-August, but unlike many other states, its current surge was far smaller than its winter 2020 surge. In fact, California’s most recent peak was less than one-third of its highest peak. In contrast, numerous states, particularly in HHS Regions 4 (Southeast), 6 (South Central), and 7 (Central), have approached or surpassed their previous highest peaks during the current surge. For example, Florida spent nearly 3 weeks at its highest peak, reporting more than 21,000 new cases per day from August 10-29—approximately 40% higher than its previous record—before its epidemic began to recede. Louisiana set a new record high of 5,839 new cases per day on August 13, more than 50% higher than its January 2021 peak. And Alabama, Georgia, and South Carolina peaked at 96%, 97%, and 93% of their previous records, respectively.
Texas’ surge continues to increase, up to nearly 20,000 new cases per day on September 14, 86% of its record peak in January 2021. Kentucky, Tennessee, and West Virginia are all setting new records with their current surges as the Delta wave moves north from Alabama, Florida, and Louisiana. Continuing north into Regions 1, 2, and 3, daily incidence trends are increasing in most states, but most are nowhere near their current records. Several states already appear to be approaching or passing their respective peaks—including Connecticut, Massachusetts, New York, New Jersey, and Rhode Island—and Region 2, as a whole appears, to be peaking. The muted impact of the Delta variant in these states is likely driven by a combination of higher vaccination coverage and reinstituting various protective measures. In fact, with the exception of West Virginia (#50, 40.0%), all states in Regions 1, 2, and 3 are in the top 20 nationally in terms of full vaccination coverage, ranging from 56% (Pennsylvania) to 69% (Vermont).
In addition to California, other states on the West Coast (in Regions 9 and 10) were affected early in the Delta wave as well. The West Coast states have leveled off or peaked already, but moving east, Idaho’s epidemic is currently at 77% of its record high and still increasing sharply, mirroring trends in neighboring Region 8 (Mountain) states. Unlike states in the Southeast, however, most of the West Coast states remained well below their record highs. Oregon is the exception, peaking at 50% higher than its previous record daily incidence, even with nearly 60% full vaccination coverage (#12 nationally).
The Delta wave appears to be spreading inward from the coasts. The states in Region 5 (Midwest) are generally exhibiting increasing trends in daily incidence, with most currently around 50% of their highest peak and still accelerating. In Region 7 (Central), Missouri—which was affected very early in the surge—passed its peak in early August, but it did not peak as high as the states in the Southeast region (~57% of its highest peak). Iowa is exhibiting an accelerating trend, but it is still less than 40% of its highest peak. A number of other states in Regions 5 and 7 were exhibiting accelerating trends prior to the Labor Day holiday weekend, but do not appear to have caught up from delayed holiday reporting, including Indiana, Illinois, Kansas, Nebraska, and Wisconsin. States in Regions 5 and 7 generally fall between 47% and 57% full vaccination coverage (ranking #17-39). Considering the accelerating trajectories and low-to-moderate vaccination coverage in some states, Regions 5 and 7 could potentially face a severe COVID-19 surge in the coming weeks.
In Region 6 (South Central), New Mexico appears to have passed its peak as well, although the timing suggests that delayed holiday reporting could be a factor in its recent decrease. Notably, New Mexico only reached approximately 30% of its record high, which could be a result of the state having highest full vaccination coverage outside of Regions 1, 2, and 3 (#11; 62%). All of the states in Region 8 (Mountain) are exhibiting accelerating trends in daily incidence. Most of these states are currently at approximately 30% of their record highs, but Montana and Wyoming are closer to 60%. The accelerating trends indicate that these states may still be early in their respective surges, and most of these states are reporting less than 50% full vaccination coverage—including #49 Wyoming (40%) and #45 North Dakota (43%).
US Vaccination
The US has administered 383 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations peaked at 837,000 doses per day on August 29 and then began to decline going into the Labor Day holiday weekend. The 7-day average window still includes delayed holiday weekend reporting, so it will be at least another several days before we can get a clearer picture of the longer-term trend*. There are 210.7 million individuals who have received at least 1 dose, equivalent to 63.5% of the entire US population. Among adults, 76.1% have received at least 1 dose, as well as 14.2 million adolescents aged 12-17 years. A total of 180.1 million individuals are fully vaccinated, which corresponds to 54.2% of the total population. Approximately 65.4% of adults are fully vaccinated, as well as 11.2 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
UK VACCINE EFFECTIVENESS New real-world data from England offer additional evidence that full vaccination can significantly reduce the risk of COVID-19 mortality. The UK Office of National Statistics (ONS) reported 51,281 COVID-19 deaths in England from January 2-July 2, 2021. Of these, only 256 (0.5%) were classified as “breakthrough deaths”—ie, occurring in individuals who were fully vaccinated at least 14 days before diagnosis*.
*A total of 640 deaths were in individuals who received all necessary doses of the vaccine, including those who were infected prior to receiving the second dose.
The ONS also provides weekly age-standardized mortality rates (ASMRs) for COVID-19 deaths as well as additional information on the overall health of breakthrough deaths. The median age of breakthrough deaths was 84 years, which is 2 years older than the average for other COVID-19 deaths. Among breakthrough deaths, 61.1% were male, compared to 52.2% for other COVID-19 deaths. Notably, 13.1% of breakthrough deaths occurred in individuals who were immunocompromised, compared with 5.4% of other COVID-19-related deaths.Additionally, 76.6% of breakthrough deaths occurred among individuals who were classified as “clinically extremely vulnerable”—based on age, underlying health conditions, and other factors associated with elevated risk of severe COVID-19 disease and death. In comparison—which was slightly higher than for other COVID-19 deaths (74.5%). While experts cautioned the data need to be interpreted in context—considering trends in COVID-19 mortality during the study period and the emergence of the Delta variant in June—the ONS analysis provides additional evidence that full vaccination offers very high protection against death from COVID-19.
UK AUTUMN/WINTER PLAN On September 14, the UK government published its COVID-19 Autumn and Winter Plan 2021, an effort to mitigate impacts on the National Health System (NHS) and mitigate the need for future “lockdowns.” The plan is separated into 2 parts: Plan A lays out a comprehensive approach to pandemic preventive efforts, and Plan B outlines measures that would only be enacted if epidemiological trends illustrate a need for additional risk mitigation. Most notably, Plan A includes a booster shot program for approximately 30 million individuals, despite the WHO’s call for a moratorium on such initiatives in higher-income countries so that additional doses can be allocated to low- and middle-income countries (LMICs).
Beginning next week, the UK government plans to provide booster doses—primarily of the Pfizer-BioNTech vaccine, regardless of which vaccine was administered first—to adults aged 50 years and older, those with underlying health conditions, and healthcare workers, following a recommendation from the UK Joint Committee on Vaccination and Immunization (JCVI) that additional doses be administered at least 6 months after the second dose. According to data published this week by Public Health England (PHE), the level of protection provided by 2-dose vaccines against severe disease and death begins to wane approximately 3 months after the second dose. While the science underpinning the need for booster doses remains unclear, most experts generally agree that additional doses are warranted for individuals who may not have mounted a strong immune response to the initial doses, such as the immunocompromised. The UK has no plans to offer the additional doses to the general population under age 50 this year.
Plan A also includes offering 1 dose of vaccine to adolescents aged 12 to 15 years, after a unanimous recommendation by the Chief Medical Officers (CMOs) from the 4 UK nations that children in this age bracket receive their first dose of the Pfizer-BioNTech vaccine. Additionally, Plan A includes promoting SARS-CoV-2 vaccination for those currently unvaccinated, keeping in place associated travel restrictions and providing additional funding to the NHS to support its COVID-19 response over the next 6 months. If enacted, Plan B would involve requesting the public to act more carefully, instituting mandatory vaccine passports for certain events and settings, and requiring mask use in some settings.
US FDA MEETING ON VACCINE BOOSTERS The US FDA Vaccines and Related Biological Products Advisory Committee (VRBPAC) is meeting today, in part, to discuss a proposed plan to administer a third dose of the Pfizer-BioNTech vaccine 6 months after the initial 2-dose course. Last month, the Biden Administration announced plans to initiate booster dose campaigns for the Pfizer-BioNTech vaccine starting September 20. While the plan was announced weeks ago, the vaccine has not been authorized for a third dose for most people. The CDC’s Advisory Committee on Immunization Practices (ACIP) is scheduled to meet next week to explore the same issue. If either the FDA or CDC advisory bodies push back on the need for booster doses, it would put the country’s leading health authorities at odds with the White House.
The Biden Administration initially announced plans for booster doses after unpublished data from a study in Israel suggested that the Pfizer-BioNTech vaccine demonstrated reduced efficacy months after the initial inoculation. Pfizer’s company leadership echoed these claims, suggesting that a booster dose would be able to counteract waning immunity in individuals who received their full vaccine regimen months earlier. Pfizer released additional data from a booster dose campaign in Israel, in which a third dose increased effectiveness against symptomatic COVID-19 back to approximately 95%, similar to the initial efficacy after 2 doses demonstrated in clinical trials. Moderna also released data suggesting that an increase in breakthrough cases made the idea of booster doses more reasonable. Despite these early claims, Moderna’s president released a statement questioning the necessity of future vaccine doses. Documents released by the FDA earlier this week in advance of the VRBPAC meeting showed that FDA scientists questioned the necessity of booster doses, considering that the vaccines are still exhibiting high levels of protection against severe disease and death in the US. Several FDA scientists published a commentary in The Lancet arguing that there is not enough evidence to indicate waning protection from SARS-CoV-2 vaccination.
VACCINE MANDATES A federal judge in New York state blocked a statewide vaccine mandate for healthcare workers late Tuesday. Former New York Governor Andrew Cuomo issued the mandate last month, and it was scheduled to take effect September 27. Plaintiffs in the lawsuit argue that the absence of a religious exemption violates the US Constitution, the New York State Human Rights Law, and New York City Human Rights Law. The 17 healthcare workers who filed the lawsuit have objected to the vaccine requirement on the grounds that the cell lines of aborted fetuses were used in the vaccine’s development. No major religious denomination has taken an opposing stance to vaccination, and Pope Francis has encouraged vaccination, calling it the “moral choice.” The defendants in the lawsuit have until September 22 to respond, and an additional hearing is scheduled for September 28.
An Arkansas hospital is allowing religious exemptions for employees, but it is also asking them to validate their objections to show it is a “sincerely held belief.” Conway Regional Hospital requires employees to complete a form attesting that they “do not use or will not use” any of more than 30 medications and other vaccines that also utilized fetal cell lines in their development in order to demonstrate their conviction. Notably, some of the medications listed include common pain killers such as aspirin, ibuprofen, Tylenol, and Motrin; antihistamines such as Claritin and Benadryl; antacids such as Pepto-Bismol, Maalox, and Tums; and the MMR vaccine.
LIMITING PUBLIC HEALTH AUTHORITY At least 29 US states have passed laws, enacted other initiatives, or succeeded in lawsuits that permanently weaken state and local government authority to protect public health, and similar efforts are pending in multiple other states. The analysis was published by Kaiser Health News and the Associated Press as part of their ongoing series “Underfunded and Under Threat,” which examines how US public health systems were unprepared to confront the COVID-19 pandemic and face ongoing politicization, funding cuts, and other hindrances. Legislators in at least 16 states have limited public health authorities’ ability to issue mask mandates or quarantines or isolation orders, and in some cases, legislatures gave themselves that authority or shifted it to other elected officials. In at least 17 states, lawmakers passed legislation banning SARS-CoV-2 vaccine mandates or passports or facilitated opt-out options. And in at least 14 states, new laws, executive orders, or court rulings ban or limit mask mandates.
Proponents of the new measures argue that they are a necessary check on executive powers, particularly for appointed officials, and give lawmakers a voice in public health emergencies. Public health officials and experts have expressed frustration with these efforts and warned that the consequences of these actions will extend far beyond the current pandemic. These new limits could also impact public health officials’ ability to prevent and contain future outbreaks for any number of communicable diseases. At least 303 state and local public health department leaders have resigned, retired, or been fired during the pandemic, according to the analysis.
US HOSPITALIZATION COSTS Preventable costs for treating hospitalized, unvaccinated COVID-19 patients in the US reached US$5.7 billion between June and August, with US$3.7 billion of that spending happening during a surge in hospitalizations in August alone. The analysis was conducted by the Kaiser Family Foundation and the Peterson Center on Healthcare. According to the report, which uses data from the US Department of Health and Human Services (HHS) and the US CDC, there were an estimated 287,000 preventable COVID-19-related hospitalizations during the study period—specifically, those among unvaccinated individuals—which cost an average of US$20,000 each to treat. The authors note that the costs are likely an underestimate of the overall burden, if publicly funded programs and private insurance premiums are considered. Recent US CDC data show that vaccinated people are 10 times less likely to be hospitalized with COVID-19 than unvaccinated individuals.
GLOBAL VACCINE ACCESS Ahead of a global COVID-19 summit, many researchers and health advocacy organizations are amplifying their calls to increase support for low- and middle-income countries (LMICs) to manufacture their own SARS-CoV-2 supplies. On September 14, WHO Director-General Dr. Tedros Adhanom Ghebreyesus and a group of global health leaders issued an urgent call for global vaccine equity, with a focus on Africa, which accounts for approximately 17% of the global population but only 2% of the SARS-CoV-2 vaccine doses administered thus far. Speaking at a press conference, Dr. Tedros said African nations “have been left behind by the rest of the world,” with only 2 countries thus far surpassing 40% coverage. He warned that the longer the virus is allowed to persist among unvaccinated populations, the greater the risk of new variants emerging and the greater the risk of further disruption to social and economic systems. Additionally, the Gates Foundation, in its fifth annual Goalkeepers report, urged more investment in health infrastructure—including vaccine research, development, and manufacturing capacities—especially in LMICs, where such investments will help future responses to public health emergencies.
Meanwhile, efforts to develop an African base for manufacturing SARS-CoV-2 vaccines have reportedly stalled. According to a report by Reuters, a senior WHO official recently indicated that negotiations with Moderna regarding the technology transfer necessary to manufacture mRNA vaccines in Africa are not making sufficient progress. Although Moderna has said it will not enforce patents related to its vaccine during the pandemic, officials from a WHO-supported technology transfer hub in South Africa said it could take more than a year to develop the capability to manufacture an mRNA vaccine without Moderna’s assistance. The WHO reportedly is in negotiations with Indonesia to establish a second technology transfer and manufacturing hub for mRNA vaccines. And in a potentially more positive development, a source told Reuters that India could soon resume exporting SARS-CoV-2 vaccines, including to Africa. Additionally, the EU recently committed to donate an additional 200 million doses of vaccine for Africa and LMICs, on top of previous commitments of 250 million, and reiterated its pledge to invest €1 billion (US$1.2 billion) to improve vaccine manufacturing capabilities in Africa.
VACCINATION FOR YOUNGER CHILDREN Many countries have approved vaccinations for children 12 years and older, and expanded eligibility to younger children may be on the horizon. Cuba has reportedly started vaccinating children as young as 2 years old, the only country thus far to vaccinate children that young. The Cuban Ministry of Health has not yet released data on how many children have been vaccinated, but pediatric vaccination efforts are reportedly ongoing in Cienfuegos, where the healthcare system is strained under the burden of a surge driven by the Delta variant. Two Cuban-made vaccines currently in use have not yet been recognized by the WHO, and clinical trial data have not yet been published publicly or been subjected to peer review; however, Cuban researchers say the vaccines are safe and effective, and they will eventually seek an Emergency Use Listing (EUL) and prequalification from the WHO. Children aged 2-18 years will receive the Soberana-2 vaccine, and adults will receive Abdala, according to a state-run media source.
A number of other countries are also expanding vaccination eligibility to younger children. El Salvador will begin vaccinating children aged 6 years and older, and the UAE approved Sinopharm for children aged 3 years and older, but noted that vaccination will be optional.Chile authorized the Sinovac vaccine for children aged 6 years and older, based on data provided by China. Researchers are initiating Phase 3 trials of the Sinovac vaccine in children aged 6 months to 17 years. The trials will be coordinated from South Africa, but trial sites include Chile, the Philippines, Malaysia, Kenya, and South Africa.
US SPORTS Approximately 85% of NBA basketball players have received the SARS-CoV-2 vaccine, but the league announced that, like other US professional sports leagues, it will not mandate vaccinations. Protocol negotiations for the 2021-22 are ongoing, but sources say vaccine mandates remain a “non-starter.” Current protocols keeping vaccinated and unvaccinated players separate in locker rooms as well as while eating and transporting to and from games. NBA referees and NBA staff are required to be vaccinated.
Spectators for Buffalo Bills (NFL) and Sabres (NHL) games will be required to be vaccinated for home games this season. Starting September 25 (Sabres) and 26 (Bills), fans aged 12 years and older attending games at Highmark Stadium and KeyBank Center must have received at least 1 dose of a SARS-CoV-2 vaccine, and they must be fully vaccinated by the end of October. Notably, the 2 venues will not offer a testing option in order to opt out of vaccination, and according to the Buffalo Bills website, no exceptions will be made to the vaccination mandate, including for medical or religious exemptions. Spectators under the age of 12 must wear a mask while inside the venues, but older individuals are not subject to a mask mandate. Unvaccinated fans were allowed at the Bills home game on September 12 while masked, but county health officials reported that fewer than half of stadium attendees wore masks. All events held in the 2 venues are subject to the new rules, including concerts.
by ponchi101 Serious here. I know triage guidelines are well established in the medical profession. But this brings a new factor, for questions that I doubt have been asked before.
Example.
IF a child comes in in need of an ICU, and the child can survive whatever malady is affecting him/her with such care, but there are no ICU's, do you take a COVID AFFECTED ADULT from an ICU bed off support in order to attend to the child? If that adult WAS NOT vaccinated, what are the moral implications?
It is not only training. It can involve revision of triage guidelines.
They could have added that 5 other states were in the same position.
Ok - I'll bite...
In no particular order...
Florida, Texas, Louisiana, Georgia, and... New York.
?
by Suliso Actually I was wrong... It was five states in 2019 before covid. Covid added another 15 to that list so even less clear why Alabama singled out. You can see them all in the picture below.
by Deuce Maybe Alabama was the only state where it occurred for the first time ever, while it's happened at some point previously in the other states?
Hard to believe that Texas - with its COVID-19 problems and love of guns - is in the blue...
They could have added that 5 other states were in the same position.
Well, you understand stats. It is like the ribbon of the CNN report. So Mississippi led the nation in Covid deaths per capita. So? Some state has to lead the nation in deaths per capita. Some state right now is leading the nation in throat cancer deaths per capita, and some state is leading the nation in herpes cases per capita.
Without an explanation of why they are leading the nation, or some explanation that they lead but by a disproportionate number, the verbal statistic is basically meaningless.
by JazzNU
Suliso wrote: ↑Mon Sep 20, 2021 3:56 am
They could have added that 5 other states were in the same position.
They did add it, in the article. Tweets only have so many characters and this one is about Alabama for a reason, which is crystal clear in the article as well. There would be no need to highlight other states in a tweet about an article focused on Alabama.
Not sure what this means exactly, but Chris is definitely vaccinated. Been advocating for people to get vaccinated early in the year before it was widely available and was very public about it once he was able to get one.
by Suliso Anytime you think there is nowhere deeper to fall you get surprised.
by JazzNU As I sit here and wait on news if my fully vaccinated aunt's condition will improve enough that she will be able to get discharged from the hospital after testing positive and coming down with covid pneumonia, I am 100% out of fcks to give about these unvaccinated assholes and their whiny freedom bullsh!t. You better be a child or in a country that doesn't have enough vaccines to get sympathy out of me at this point. Otherwise, 100% done with these stupid, selfish assholes.
by dryrunguy Wishing your aunt the best, Jazz. It has to be an extremely difficult experience for you and yours. We are all thinking of you.
by dryrunguy Here's the latest Situation Report. The paragraph on fake vaccination cards is... quite alarming. To say the least.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 228.4 million cumulative cases and 4.69 million deaths worldwide as of September 21. Global weekly incidence decreased by 8.6% compared to the previous week, and mortality fell by 6.6%.
Global Vaccination
The WHO reported 5.78 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 20. A total of 3.30 billion individuals have received at least 1 dose, and 2.39 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline. After peaking 3 times at more than 42 million doses per day between late June and early September, the average has fallen to 29 million. In mid-July, between the 2 highest peaks, the average dropped as low as 20 million before rebounding, so the longer-term trend remains uncertain*. The global trend continues to closely follow Asia. Daily vaccinations in Europe have steadily declined since early July, and if the continent as a whole continues on this trajectory, it could soon fall below Africa on a per capita basis. On the opposite end of the spectrum, Oceania is currently #1 globally in terms of per capita daily vaccinations. It was second to last (ahead of only Africa) as recently as early July, but its trend has accelerated over the past several months. Our World in Data estimates that there are 3.43 billion vaccinated individuals worldwide (1+ dose; 43.6% of the global population) and 2.51 billion who are fully vaccinated (31.9% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 42.0 million cumulative COVID-19 cases and 672,738 deaths. The US appears as though it may have passed a peak in terms of daily incidence. The most recent high was 159,929 new cases per day on September 1, and the trend began to decline slightly before the Labor Day holiday weekend. The reporting has largely recovered following the holiday, but the average daily incidence has not returned to the pre-holiday level. The current average is approximately 141,000 new cases per day and appears to be decreasing. Daily mortality continues to increase slowly, now up to 1,521 deaths per day—the highest average since February 27. If the daily incidence peaked on September 1, we would expect mortality to peak in the next week or so*.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
At more than 1,500 deaths per day, the US could surpass 675,000 cumulative deaths in the next several days, which would make the COVID-19 pandemic more deadly in the US than the 1918 influenza pandemic. Notably, the US population in 1918 (approximately 105 million) was less than one-third of the current population, so the COVID-19 mortality is much lower on a per capita basis.
California is the only US state categorized as having Substantial community transmission, having fallen below the threshold of 100 weekly new cases per 100,000 population that corresponds to the High category. California’s test positivity is not reported by the CDC. The next 4 states are reporting between 125-150 weekly new cases per 100k: Connecticut (126.5), Colorado (127.9), Maryland (141.5), and Vermont (146.3).
US Vaccination
The US has administered 386 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccination reporting appears to have recovered from the Labor Day holiday weekend, and the longer-term trend continues to decline from the most recent peak on August 29*. There are 212.0 million individuals who have received at least 1 dose, equivalent to 63.9% of the entire US population. Among adults, 76.5% have received at least 1 dose, as well as 14.4 million adolescents aged 12-17 years. A total of 181.7 million individuals are fully vaccinated, which corresponds to 54.7% of the total population. Approximately 65.9% of adults are fully vaccinated, as well as 11.5 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US FDA PANEL BOOSTER DOSE RECOMMENDATION The US FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) on September 17 voted 16-2 against authorizing third doses of the Pfizer-BioNTech SARS-CoV-2 vaccine for the general population, but it unanimously recommended third doses for individuals aged 65 years and older and those who are at elevated risk for severe disease. The panel’s recommendation—made after more than 7 hours of deliberation—is a surprising rebuke to plans previously announced by US President Joe Biden, who expected booster doses to begin for the general population this week. Although the FDA is not required to follow VRBPAC recommendations, it generally does, and both the FDA and the US CDC’s Advisory Committee on Immunization Practices (ACIP) are expected to adopt the recommendation in the coming days and clarify who qualifies for booster doses. VRBPAC also signaled unanimous support for third doses for healthcare workers and others at high occupational risk, but it did not take a formal vote. The panel will likely discuss booster doses for those individuals and individuals who have received the Moderna and J&J-Janssen vaccines at a later date.
Hours before the VRBPAC meeting, the CDC released data indicating the level of protection against hospitalization wanes significantly in the 4 months following vaccination. The study, published in the CDC’s Morbidity and Mortality Weekly Report (MMWR), showed vaccine effectiveness (VE) against hospitalization for the Pfizer-BioNTech vaccine fell from 91% in the first 4 months to 77% beyond 120 days post-vaccination. For the Moderna vaccine, VE against hospitalization remained high, falling only 1 percentage point (pp) after 120 days, from 93% to 92%. Although there were not enough participants to comparatively evaluate the J&J-Janssen vaccine’s effectiveness over time, the study said the single-dose vaccine has been 71% effective at preventing hospitalization.
While most health experts applauded the FDA panel’s decision, arguing that it was evidence-based, some US residents expressed confusion over the recommendation. Biden administration officials appeared to backpedal slightly on the previous announcement that booster doses could be made available to the general public beginning this week, with several saying they still expected US health agencies to recommend the extra shots for the general population in the coming weeks when more data become available. There remains significant debate over the need for widespread booster doses. Some experts instead advocate for increased focus on reaching unvaccinated individuals, who account for the majority of new COVID-19 cases in the US, and others call for equitable allocation and distribution of available doses globally.
J&J-JANSSEN VACCINE SECOND DOSE On September 21, Johnson & Johnson (J&J) announced preliminary findings from a Phase 3 clinical trial that indicate increased protection following a second dose of its SARS-CoV-2 vaccine, developed in collaboration with Janssen Pharmaceuticals. Unlike other major vaccines—including those from Pfizer-BioNTech, Moderna, and AstraZeneca-Oxford—the J&J-Janssen vaccine was originally authorized as a single dose. In the Phase 3 clinical trial, the second dose was administered 2 months after the first dose, and the control group was made up of individuals who received only a single dose. The press release does not indicate the total number of participants.
According to the press release, a second dose increased the vaccine’s efficacy (compared to a single dose) by an estimated 100% against severe disease* and 75% and 94% against symptomatic COVID-19 globally and in the US, respectively. Additionally, antibody levels after the second dose were 4-6 times higher than after a single dose. The study also evaluated a second dose administered 6 months after the first dose. Following a booster 6-month booster, antibody levels increased by a factor of 12 compared to a single dose. The press release does not provide overall efficacy estimates (ie, compared to receiving no vaccine at all). The press release also describes real-world data that indicate the single-dose regimen provides strong, lasting protection against COVID-19. As has been the trend throughout the pandemic, the preliminary findings were presented via press release, and the data have not been published publicly nor subjected to peer review; however, J&J committed to submitting the full dataset for publication “in the coming months.”
*The efficacy against severe disease is based on only 8 cases among the control group and zero among those who received the second dose. The low number of cases yields a large confidence interval (30-100%), and additional data would provide a better understanding of the protective effect.
PEDIATRIC VACCINATION DATA Pfizer and BioNTech on September 20 announced positive results from a Phase 2/3 trial of their SARS-CoV-2 vaccine in children aged 5 to 11 years. The researchers found that a 2-dose regimen of 10µg doses administered 21 days apart demonstrated a favorable safety profile and robust neutralizing antibody response. The findings—which are neither published nor peer-reviewed—are a crucial step toward a SARS-CoV-2 vaccine becoming available for younger children, and the companies expect to submit an application to the US FDA for the vaccine’s authorization for that age group by the end of September. US regulators have issued warnings to the general public to wait for authorization before seeking vaccination for younger children, as the full adult dose of 30µg may put children at a higher risk for adverse side effects, including myocarditis.
The trial included nearly 2,300 children, and two-thirds of them in the vaccine group. The vaccinated children also were compared with a separate cohort of 16-25-year-old individuals who received the full adult course of the vaccine (2 doses of 30µg). The trial found that the neutralizing antibody response was similar between both vaccinated groups, with the neutralizing antibody levels within 5% of each other. Both groups also experienced similar post-vaccination adverse events.
Results from another study evaluating the Sinopharm SARS-CoV-2 vaccine in children were published on September 15 in The Lancet Infectious Diseases. The Phase 1/2 trial examined the safety and immunogenicity of the vaccine in a cohort of children aged 3-17 years, with participants broken into several age groups (3-5, 6-12, and 13-17 years) and dosing groups (0 [control], 2µg, 4µg, and 8µg). Three (3) doses of each vaccine dosage or placebo were administered 28 days apart. All adverse events were categorized as mild or moderate severity, but the article does not report on serious adverse events. The study concluded that children who received the vaccine had robust immune responses and similar levels of neutralizing antibodies to those observed in older vaccine recipients. The study recommended a 2-shot 4µg dose regimen for future Phase 3 trials. Additional data are being collected through a Phase 3 trial currently taking place in the UAE.
UN GENERAL ASSEMBLY & COVID-19 SUMMIT Beginning with an address to the UN General Assembly today, US President Joe Biden will focus his attention on efforts to end the COVID-19 pandemic and attempt to rally other vaccine-producing nations to commit to providing additional doses to countries in need. In addition to the main UN General Assembly meetings, the US will participate in a virtual COVID-19 summit on September 22 and a meeting of the Quadrilateral Security Dialogue (Australia, India, Japan, US) on September 24. The effort to improve vaccine diplomacy is being watched carefully by public health experts, advocates, and organizations eager for President Biden to fulfill his pledge that the US will serve as an “arsenal of vaccines” for the world. The US, along with several other higher-income nations, has faced criticism for ignoring calls from the WHO to postpone vaccine booster dose programs in order to redirect those shots to the COVAX facility, which is behind schedule on its goal to vaccinate at least 10% of the populations in low- and middle-income countries (LMICs). At the COVID-19 summit, the US is expected to make several announcements regarding its own commitments. Reportedly, the US government is negotiating to purchase an additional 500 million doses of the Pfizer-BioNTech vaccine to distribute globally, which would bring the total US donation to 1.15 billion—about one-tenth of the estimated 11 billion the world needs.
US officials have expressed concern that the UN General Assembly meetings could become a superspreader event, with the world body relying only on an honor system to ensure attendees are vaccinated before they speak. More than 100 heads of state and government as well as more than 20 foreign ministers have registered to speak in person at the meeting, with some already openly defying the vaccine honor system. Brazil President Jair Bolsanaro, for example, said he will decide whether to take the vaccine after everyone in his nation is vaccinated—only 36% is currently vaccinated. Other leaders, including Vietnamese President Nguyen Xuan Phuc, have not disclosed their vaccination status, and Russia complained the requirement infringes upon nations’ rights to participate at the UN. The New York City government, which requires proof of vaccination for convention centers, has said the requirement includes the UN assembly hall, although the UN headquarters building is considered international territory. In a goodwill effort, the municipal government has set up a mobile vaccine clinic outside the UN complex to offer free testing and vaccination.
US AIR TRAVEL REQUIREMENTS The US government plans to ease travel restrictions for fully vaccinated foreign nationals beginning in November, marking the end of an 18-month interruption to international on travel. The US currently prohibits travel for most non-US citizens who have visited Brazil, China, the EU, India, Iran, South Africa, or the UK within the past 14 days. Under the new policy, non-US residents traveling to the US will have to show proof of vaccination and proof of a negative SARS-CoV-2 test within 3 days before boarding a US-bound aircraft. Children not yet eligible for vaccination will be allowed to travel with only a negative test. The US CDC is expected to issue an order directing airlines to collect travelers’ phone numbers and email addresses for a new contact tracing system that will enable health officials to follow up with travelers after they arrive in the US. Additionally, unvaccinated US citizens arriving in the US will need to show proof of a negative SARS-CoV-2 test taken within 1 day of traveling to the US and and also complete another test upon arrival (reportedly, at their own expense). This week, the US extended its restrictions on nonessential travel to Mexico and Canada, but there is no indication if or how the vaccination and testing requirements would be applied at land borders.
VACCINATION IN AFRICA With more than 8 million cumulative COVID-19 cases recorded in African countries and rising concern over a fourth wave, WHO Regional Director for Africa Dr. Matshidiso Moeti on September 19 called on wealthy nations to forego third vaccine doses for healthy individuals, donate excess doses, and allow COVAX and the African Union to purchase the vaccine needed to protect the continent’s population. Writing in a New York Times opinion piece, Dr. Moeti warned that with only 4% of the African population fully vaccinated, countries with low vaccination coverage “could act as variant incubators, increasing the risk that more dangerous variants will emerge and enter international travel networks.” Additionally, the COVAX facility recently announced that it is cutting its planned vaccine deliveries to Africa by 150 million doses in 2021, leaving the continent 500 million doses short of the year-end target of fully vaccinating 40% of the population. According to WHO Africa, the 470 million doses now expected to be delivered this year through COVAX is enough to vaccinate only 17% of the population. At a news conference last week, Dr. Moeti blamed vaccine export bans and vaccine hoarding for the shortfall, arguing that higher-income countries are causing “a chokehold on the lifeline of vaccine supplies to Africa.” She noted that African nations recently tripled the weekly doses administered over previous weeks, but the continent will likely not reach the 40% goal until at least March 2022, based on the current pace.
INDIA VACCINE EXPORTS India is expected to resume exporting domestically manufactured SARS-CoV-2 vaccines sometime between October and December 2021. Indian Minister of Health Mansukh Mandaviya indicated that the initial focus will be on supplying the COVAX facility and neighboring countries. India is the world’s largest manufacturer of vaccines, but it prohibited exports of SARS-CoV-2 vaccines in April 2021, when the country was experiencing its largest surge. The announcement comes ahead of Prime Minister Narendra Modi’s visit to Washington, DC, for a summit of Quadrilateral Security Dialogue, which includes Australia, India, Japan, and the US. India's monthly vaccine output has increased recently, and the country expects to produce at least 1 billion doses in the last 3 months of 2021.
CANADA VACCINE APPROVALS On September 16, Health Canada granted full regulatory approval to both the Moderna and Pfizer-BioNTech SARS-CoV-2 vaccines for use in individuals aged 12 years and older. In an announcement, Moderna said the approval marks “an important milestone,” as it is the first full approval for its SARS-CoV-2 vaccine. Notably, the Moderna vaccine is not yet authorized in the US for children under the age of 18.
“TEST-TO-STAY” PROTOCOLS With the school year only beginning across the US, already tens of thousands of students have had to quarantine after coming in close contact with classmates or teachers who test positive for SARS-CoV-2. An increasing number of school districts nationwide are implementing testing programs to try to keep more children in classrooms instead of having to quarantine at home—and possibly disrupting their parents’ work schedules and their education—after being exposed to a known COVID-19 case. The strategy, known as “test to stay” or modified quarantine, allows children to stay in school if they remain asymptomatic, participate in regular testing (eg, daily) and continue to test negative, and follow other preventive measures. Typically, the tests and the staff to conduct them are provided by the school districts, straining already-tight resources.
In a statement to The New York Times, the US CDC said it does not recommend or endorse test-to-stay strategies at this time, saying there is not yet enough evidence to support them. The agency recommends that any unvaccinated student who has close contact with a known COVID-19 case undergo quarantine for 14 days. A study conducted by British researchers and published last week in The Lancet suggests that daily testing of school-based contacts could be effective in mitigating COVID-19 risk while to helping more students stay in school following an exposure. The study showed that COVID-19 incidence rates were not significantly different between schools with "test-to-stay" policies compared with those that required at-home quarantine.
FAKE VACCINATION CARDS Both the price of fake SARS-CoV-2 vaccination cards and the number of online sellers have increased dramatically in recent weeks, following US President Joe Biden’s announcement extending vaccine mandates for most federal workers, healthcare workers, and employees of many US companies, according to cybersecurity company Check Point Software Technologies. As of September 2, the average cost of a fake vaccination card bearing the US CDC logo was US$100, but that price doubled following President Biden’s September 9 announcement. Additionally, the estimated number of vendors increased from approximately 1,200 to more than 10,000. Many of the cards are being sold through the instant messaging app Telegram, which has 500 million monthly users worldwide and exhibited a 10-fold increase in US users following the mandates, up to 300,000. Most sellers require payment in cryptocurrency and collect personal information that is unnecessary to mail a blank fake card. Government authorities have cautioned against providing such information. Though it is unclear how people receive the fake cards, US Customs and Border Protection (CBP) has reportedly intercepted thousands of packages of fake vaccination cards sent to the US from China in recent months. Both the US FBI and CBP have warned that buying, creating, or selling fake vaccination cards is a federal crime.
INACTIVATED VIRUS VACCINE & EGG-BASED MANUFACTURING Researchers in Thailand and the US published (preprint) results from a Phase 1/2 clinical trial of an inactivated recombinant SARS-CoV-2 vaccine. The NDV-HXP-S vaccine* was developed in Thailand, Vietnam, and Brazil, based on components developed at the Icahn School of Medicine at Mount Sinai (New York, US), the University of Texas (US), and it utilizes a Newcastle disease virus (NDV) platform. The trial included 210 participants aged 18-59 years who were randomized into 6 groups. They received 2 injections 28 days apart using either a 1µg dose (with or without an adjuvant), 3µg dose (with or without an adjuvant), 10µg dose (without adjuvant), or placebo. All but 5 participants received both doses. The Phase 1/2 trial was principally designed to evaluate safety, and all doses were generally well tolerated, with no serious adverse events reported. Additionally, 93.9-100% of vaccinated participants had increases in neutralizing antibodies of at least 4 times over baseline, an encouraging indication of immune response.
There are multiple other inactivated virus vaccines already available—including those from Sinopharm and Sinovac in China and Bharat Biotech in India—but the NDV-HXP-S vaccine has the advantage of being produced using chicken eggs, similar to some seasonal influenza vaccines. Facilities around the world have production lines that can manufacture seasonal influenza vaccines using chicken eggs, and a SARS-CoV-2 vaccine that leverages this manufacturing platform could take advantage of substantial and geographically distributed production capacity. As we have covered previously, production capacity for existing SARS-CoV-2 vaccines remains limited, and many countries, particularly in Africa, continue to struggle to access sufficient doses to support their vaccination efforts. It will still take months to complete Phase 3 clinical trials, but a vaccine that utilizes egg-based production could potentially increase vaccine access for low- and middle-income countries (LMICs).
*Unlike previous vaccines and vaccine candidates that were principally developed by 1 or 2 companies or organizations, the NDV-HXP-S vaccine does not have a clear informal designation (eg, Pfizer-BioNTech, Moderna). NDV refers to the Newcastle disease virus platform, and HXP refers to HexaPro, a modified version of the SARS-CoV-2 spike protein used in the vaccine.
ALABAMA Alabama State Health Officer Dr. Scott Harris on September 17 said that the state’s overall mortality rate outpaced its birth rate in 2020 for the first time in recorded history. Alabama recorded 57,641 live births and 64,714 total deaths in 2020. Records from the Alabama Department of Public Health indicate that 7,128 of those deaths were attributable to COVID-19. Historically, Alabama’s birth rate has remained higher than the death rate, even during high-casualty tragedies such as World War I, World War II, and the 1918 influenza pandemic. This unfortunate statistic highlights the devastating toll the current pandemic has inflicted on vulnerable areas of the nation. Currently, 41.4% of Alabama’s population is fully vaccinated, well below the national average of 54.7%. Experts project that Alabama could again experience a higher rate of deaths than births in 2021, if the state continues down its current path.
UN GENERAL ASSEMBLY & COVID-19 SUMMIT Beginning with an address to the UN General Assembly today, US President Joe Biden will focus his attention on efforts to end the COVID-19 pandemic and attempt to rally other vaccine-producing nations to commit to providing additional doses to countries in need. In addition to the main UN General Assembly meetings, the US will participate in a virtual COVID-19 summit on September 22 and a meeting of the Quadrilateral Security Dialogue (Australia, India, Japan, US) on September 24. The effort to improve vaccine diplomacy is being watched carefully by public health experts, advocates, and organizations eager for President Biden to fulfill his pledge that the US will serve as an “arsenal of vaccines” for the world. The US, along with several other higher-income nations, has faced criticism for ignoring calls from the WHO to postpone vaccine booster dose programs in order to redirect those shots to the COVAX facility, which is behind schedule on its goal to vaccinate at least 10% of the populations in low- and middle-income countries (LMICs). At the COVID-19 summit, the US is expected to make several announcements regarding its own commitments. Reportedly, the US government is negotiating to purchase an additional 500 million doses of the Pfizer-BioNTech vaccine to distribute globally, which would bring the total US donation to 1.15 billion—about one-tenth of the estimated 11 billion the world needs.
US officials have expressed concern that the UN General Assembly meetings could become a superspreader event, with the world body relying only on an honor system to ensure attendees are vaccinated before they speak. More than 100 heads of state and government as well as more than 20 foreign ministers have registered to speak in person at the meeting, with some already openly defying the vaccine honor system. Brazil President Jair Bolsanaro, for example, said he will decide whether to take the vaccine after everyone in his nation is vaccinated—only 36% is currently vaccinated. Other leaders, including Vietnamese President Nguyen Xuan Phuc, have not disclosed their vaccination status, and Russia complained the requirement infringes upon nations’ rights to participate at the UN. The New York City government, which requires proof of vaccination for convention centers, has said the requirement includes the UN assembly hall, although the UN headquarters building is considered international territory. In a goodwill effort, the municipal government has set up a mobile vaccine clinic outside the UN complex to offer free testing and vaccination.
by ti-amie
FAKE VACCINATION CARDS Both the price of fake SARS-CoV-2 vaccination cards and the number of online sellers have increased dramatically in recent weeks, following US President Joe Biden’s announcement extending vaccine mandates for most federal workers, healthcare workers, and employees of many US companies, according to cybersecurity company Check Point Software Technologies. As of September 2, the average cost of a fake vaccination card bearing the US CDC logo was US$100, but that price doubled following President Biden’s September 9 announcement. Additionally, the estimated number of vendors increased from approximately 1,200 to more than 10,000. Many of the cards are being sold through the instant messaging app Telegram, which has 500 million monthly users worldwide and exhibited a 10-fold increase in US users following the mandates, up to 300,000. Most sellers require payment in cryptocurrency and collect personal information that is unnecessary to mail a blank fake card. Government authorities have cautioned against providing such information. Though it is unclear how people receive the fake cards, US Customs and Border Protection (CBP) has reportedly intercepted thousands of packages of fake vaccination cards sent to the US from China in recent months. Both the US FBI and CBP have warned that buying, creating, or selling fake vaccination cards is a federal crime.
And the vaccine is free.
by JazzNU My aunt has been discharged from the hospital. While that is a big relief, it's not the relief that typically comes with a hospital discharge as they sent her home on oxygen and with a hospital bed. She's in Atlanta, and my mom (who works in healthcare for those who don't know or remember) said she's fairly certain that if she was up here, she'd have been kept in the hospital for another 2-3 days to make sure she was more stable, test her strength more and potentially begin to ween her off oxygen or get her to a lower amount of it before being sent home. But we have hospital beds up here and they just don't have anything in the South. My aunt waited in the ER for 11 hours before she was seen and clearly those wait times are typical for them right now because she was given oxygen during that extended wait after a very brief evaluation to hold her until she could really be seen. The South is a freaking mess.
But she's home and feeling a bit better and those are all positive signs, so cautiously optimistic. No doubt about it, the vaccine 100% saved her life.
Interesting that this is clearly the common practice down there to free up space in the hospital. I wonder how many areas are doing this. A hospital bed? Not small, quite bulky. My aunt and uncle's house is large, so thankfully not an issue to fit it in their house and my cousin's husband and son went over beforehand to clear away furniture so it could fit in easily. But what about people with more modest homes? I'm grateful my aunt doesn't have to figure this out, but definitely concerned about this approach for others who will have a much harder time working it out.
by JazzNU
dryrunguy wrote: ↑Tue Sep 21, 2021 6:46 pm
Here's the latest Situation Report. The paragraph on fake vaccination cards is... quite alarming. To say the least.
“TEST-TO-STAY” PROTOCOLS With the school year only beginning across the US, already tens of thousands of students have had to quarantine after coming in close contact with classmates or teachers who test positive for SARS-CoV-2. An increasing number of school districts nationwide are implementing testing programs to try to keep more children in classrooms instead of having to quarantine at home—and possibly disrupting their parents’ work schedules and their education—after being exposed to a known COVID-19 case. The strategy, known as “test to stay” or modified quarantine, allows children to stay in school if they remain asymptomatic, participate in regular testing (eg, daily) and continue to test negative, and follow other preventive measures. Typically, the tests and the staff to conduct them are provided by the school districts, straining already-tight resources.
This is misleading at the very least, not sure where they got that idea. Tests may be" provided by" the school districts but they are funded by the federal government, so acting as if would strain the district's resources to implement a testing regime is false. The schools that have implemented weekly testing programs have been fairing very well in controlling outbreaks and avoiding quarantines. If someone wants to read about it, let me know and I can find a link to an article to post. Illinois has a rather robust testing program at many of their K-12 schools using the saliva test developed at Chambana.
by ponchi101 From my side:
Mom almost certainly caught Covid. I can't travel because Venezuela maintains its border with Colombia locked (because of political reasons). I could only travel through Panama.
Yep, for me, 2020 never ended.
I admit I am (expletive) scared ****less.
by JazzNU
ponchi101 wrote: ↑Thu Sep 23, 2021 10:50 pm
From my side:
Mom almost certainly caught Covid. I can't travel because Venezuela maintains its border with Colombia locked (because of political reasons). I could only travel through Panama.
Yep, for me, 2020 never ended.
I admit I am (expletive) scared ****less.
Sorry @ponchi, I really hope she's okay. And sorry you can't go and be with her. The not visiting part is very hard.
by ti-amie
ponchi101 wrote: ↑Thu Sep 23, 2021 10:50 pm
From my side:
Mom almost certainly caught Covid. I can't travel because Venezuela maintains its border with Colombia locked (because of political reasons). I could only travel through Panama.
Yep, for me, 2020 never ended.
I admit I am (expletive) scared ****less.
I hope she comes out of it okay. I'm so sorry you can't be with her.
by ponchi101 Txs. You just went through this, JazzNu, so you know how it feels like. The feeling of uselessness if verifiable.
by dmforever
ponchi101 wrote: ↑Thu Sep 23, 2021 10:50 pm
From my side:
Mom almost certainly caught Covid. I can't travel because Venezuela maintains its border with Colombia locked (because of political reasons). I could only travel through Panama.
Yep, for me, 2020 never ended.
I admit I am (expletive) scared ****less.
I'm so sorry. I hope your mom is OK.
Kevin
by dmforever
JazzNU wrote: ↑Thu Sep 23, 2021 7:48 pm
My aunt has been discharged from the hospital. While that is a big relief, it's not the relief that typically comes with a hospital discharge as they sent her home on oxygen and with a hospital bed. She's in Atlanta, and my mom (who works in healthcare for those who don't know or remember) said she's fairly certain that if she was up here, she'd have been kept in the hospital for another 2-3 days to make sure she was more stable, test her strength more and potentially begin to ween her off oxygen or get her to a lower amount of it before being sent home. But we have hospital beds up here and they just don't have anything in the South. My aunt waited in the ER for 11 hours before she was seen and clearly those wait times are typical for them right now because she was given oxygen during that extended wait after a very brief evaluation to hold her until she could really be seen. The South is a freaking mess.
But she's home and feeling a bit better and those are all positive signs, so cautiously optimistic. No doubt about it, the vaccine 100% saved her life.
Interesting that this is clearly the common practice down there to free up space in the hospital. I wonder how many areas are doing this. A hospital bed? Not small, quite bulky. My aunt and uncle's house is large, so thankfully not an issue to fit it in their house and my cousin's husband and son went over beforehand to clear away furniture so it could fit in easily. But what about people with more modest homes? I'm grateful my aunt doesn't have to figure this out, but definitely concerned about this approach for others who will have a much harder time working it out.
I missed that your aunt was sick, but glad she is doing better. And you are totally right. Not everyone has a home big enough for or can afford a hospital bed. I'm glad your aunt can. I hope she makes a full recovery soon.
Kevin
by Jeff from TX Ponchi, I am so sorry for the situation with you and your mom. Jazznu, glad your aunt is doing better. Hope she makes a complete recovery.
by dryrunguy Here's the latest Situation Report. Britain's new travel policy is... interesting. Also, here's the link to the photo essay mentioned in the last paragraph about COVID-related disparities in rural Black communities in the South: https://www.statnews.com/distanced/
::
EPI UPDATE The WHO COVID-19 Dashboard reports 229.9 million cumulative cases and 4.71 million deaths worldwide as of September 23. Global weekly incidence decreased by 5.9% compared to the previous week, and mortality fell by 3.1%.
Global Vaccination
The WHO reported 5.87 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 23. A total of 3.36 billion individuals have received at least 1 dose, and 2.43 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline, down to fewer than 28 million doses per day*. The global trend continues to closely follow Asia. Our World in Data estimates that there are 3.46 billion vaccinated individuals worldwide (1+ dose; 44.13% of the global population) and 2.54 billion who are fully vaccinated (32.24% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 42.5 million cumulative COVID-19 cases and 680,688 deaths. The US has passed a peak in terms of daily incidence. The most recent high was 160,200 new cases per day on September 1, and the trend began to decline slightly before the Labor Day holiday weekend. The current average is approximately 121,532 new cases per day and appears to be decreasing. Daily mortality continues to increase slowly, now up to 1,556 deaths per day—the highest average since February 27. If the daily incidence peaked on September 1, mortality could peak in the next week or so*.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over the weekend. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
The US surpassed 675,000 cumulative deaths on September 20, which makes the COVID-19 pandemic more deadly than the 1918 influenza pandemic in the US. Notably, the US population in 1918 was less than one-third of the current population (approximately 105 million), so the COVID-19 mortality is much lower on a per capita basis.
US Vaccination
The US has administered 388 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend continues to decline from the most recent peak on August 29*, worrying some officials as flu season approaches. There are 212.6 million individuals who have received at least 1 dose, equivalent to 64.0% of the entire US population. Among adults, 76.7% have received at least 1 dose, as well as 14.4 million adolescents aged 12-17 years. A total of 182.6 million individuals are fully vaccinated, which corresponds to 55% of the total population. Approximately 66.2% of adults are fully vaccinated, as well as 11.6 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
US BOOSTER DOSES Third doses of the Pfizer-BioNTech SARS-CoV-2 vaccine are now recommended for certain US populations at least 6 months after their primary 2-dose series. Following the US FDA’s authorization of third doses of the Pfizer-BioNTech vaccine on September 22, the US CDC’s Advisory Committee for Immunization Practices (ACIP) on September 23 voted to recommend booster doses be offered to people aged 65 years and older, residents in long-term care facilities, people aged 50-64 years with underlying medical conditions, and individuals aged 18-49 who have underlying medical conditions. The ACIP rejected a proposal to offer the shots to people aged 18-64 who are at an increased risk of COVID-19 because they live or work in high-risk occupational and institutional settings, including healthcare workers and teachers. Later the same day, in an unusual move, CDC Director Dr. Rochelle Walensky aligned her recommendation with the FDA’s authorization instead of the CDC committee's recommendations, to include those who work in high-risk settings to be eligible for booster shots. Several ACIP members expressed surprise over Dr. Walensky’s decision, which highlights ongoing divisions and confusion among federal regulators, Biden administration officials, and outside advisers about efforts to bring the pandemic under control.
While the new CDC recommendations authorize millions of US residents to receive a third dose, the plan still falls short of US President Joe Biden’s original announcement that booster shots would be available to all US residents. Biden administration officials are expected to announce a plan for rolling out booster shots as soon as today. The current recommendations only apply to the Pfizer-BioNTech vaccine, but a decision on boosters for the Moderna and J&J-Janssen vaccines could come within weeks.
VIRTUAL COVID-19 SUMMIT One day after UN Secretary-General António Guterres scolded the world for its inequitable distribution of SARS-CoV-2 vaccines on September 21, US President Joe Biden hosted a virtual COVID-19 summit—bringing together world leaders, advocacy groups, nonprofit organizations, and business leaders—in an effort to end the COVID-19 pandemic in 2022 and bolster support for a list of targets that includes vaccinating 70% of the world’s population by September 2022 and alleviating a global oxygen shortage. Calling the COVID-19 pandemic an “all-hands-on-deck crisis,” President Biden confirmed the US will donate another 500 million Pfizer-BioNTech vaccine doses by mid-2022, announced a partnership with the European Union (EU) to improve access to vaccines and therapeutics, and called on other wealthy nations to increase their pledges to countries in need. To facilitate several nations’ purchasing of vaccines through Gavi, the Vaccine Alliance, and the COVAX facility, the US International Development Finance Corporation announced it will provide US$383 million in political risk insurance, one of the conditions for self-financing countries to obtain doses through the initiative.
Questions remain over whether the new vaccine-related commitments will help, as many rich countries’ donation pledges have yet to materialize and the Pfizer-BioNTech vaccine requires specialized infrastructure to store and ship the shots, unavailable in most low-income nations. Advocates said the virtual summit, which was held behind closed doors and involved many pre-recorded speeches, was a missed opportunity to end the piecemeal international approach, increase the urgency for actually delivering vaccines, and coalesce global leadership and coordination to end the pandemic. With growing pressure on US pharmaceutical companies to share vaccine technology, some experts regretted that the summit’s lack of interactive conversation did not permit discussion over the potential for international property rights waivers, which the US has said it supports but has not taken steps to finalize. Additionally, the US government continues to face criticism over its plan to soon begin administering vaccine booster doses for some adults, but officials continue to claim they can vaccinate both US residents and people around the world.
Looking toward the future, US Vice President Kamala Harris announced the US will contribute US$250 million in startup funding for a new global health security fund, with the goal of raising US$10 billion to help confront future pandemics. The Biden administration has asked the US Congress to allocate an additional US$850 million for the new financial intermediary fund (FIF), according to Vice President Harris. Both she and President Biden, in his address to the UN General Assembly on September 21, called for the creation of a Global Health Threats Council that could elevate health threats to heads of state, as well as ensure nations’ transparency and accountability.
ECONOMIC RECOVERY Global vaccine inequity will directly impact economic recovery from the COVID-19 pandemic, and many of those same countries struggling for vaccine access likely will face difficulties financing their healthcare systems as governments cut overall spending, several new reports warn. The global economy has managed to bounce back this year, and likely will be able to rebound close to its pre-crisis trend, driven by growth in wealthy nations that have vaccinated large portions of their populations, a new report from Organisation for Economic Cooperation and Development (OECD) shows. But the gap between rich countries and the developing world is expanding due to continuing unequal access to vaccines. In its report, the OECD urged wealthy nations to share excess vaccine doses with countries in need, invest in resources to facilitate administration of the shots, and not be too quick to withdraw the “extraordinary support” they provided to their own economies during the pandemic. The OECD warned that the outlook remains uncertain, as employment levels in many countries have been severely impacted and not yet recovered.
In a separate report, the World Bank cautioned that at least 52 low- and middle-income countries (LMICs) that are experiencing declines in overall per capita government spending will be unable to adequately fund their healthcare systems, further threatening COVID-19 recovery and health security. Some nations will struggle to finance SARS-CoV-2 vaccine purchases and administration, or prepare for future disease outbreaks, the report noted, calling on wealthier nations to “recognize their interests” in a stable global recovery and commit the necessary resources. Another report, from Pathfinders for Peaceful, Just and Inclusive Societies, based at New York University’s Center on International Cooperation, warns that more than 100 countries are facing cuts to public spending on health, education, and social programs while simultaneously confronting problems paying down debt amid the pandemic, leading to growing inequality. The report cautions that cuts to government spending for vital services could lead to a reversal in development gains and unrest in some of these countries.
ENGLAND TRAVEL RULES England’s new “simplified” international travel rules—which come into effect on October 4—are igniting outrage and frustration across Africa, South Asia, and Latin America, with some calling the government’s decision to recognize only vaccinations in certain countries discriminatory and racist. Under the new rules, people who received the AstraZeneca-Oxford, Pfizer-BioNTech, Moderna, or J&J-Janssen vaccines in countries with approved health bodies—including the US, Australia, New Zealand, South Korea, an EU country, and several other nations—will be considered “fully vaccinated” and exempt from a 10-day quarantine upon arrival in England from an Amber list country, while people vaccinated with the same vaccines in African or Latin American countries or India will be considered “not fully vaccinated” and subject to quarantine when arriving from an Amber list country. The African Union’s lead health official said the policy is confusing and regrettable and asked why England would not recognize vaccination with shots it sent to the continent. England claims its policy is based on concerns over vaccine certification, but other European nations have found ways to alleviate concerns by allowing anyone vaccinated with a shot authorized by the European Medicines Agency to apply for a vaccine certificate before visiting. While the initial guidelines excluded India’s Covishield vaccine, which has been distributed in the UK, the vaccine was added to the travel list this week, even though it has not yet been formally authorized by UK regulators. A UK government spokesperson said additional changes to the policy would be considered during regular reviews every 3 weeks.
REMDESIVIR EFFECTIVENESS Gilead Sciences’ antiviral COVID-19 treatment Veklury, also known as remdesivir, appeared to reduce hospitalization among non-hospitalized patients at high risk of disease progression when given early in the disease, according to Phase 3 clinical trial results released in a September 22 press release. The results have not yet been published or peer-reviewed. The randomized, double-blind study evaluated the efficacy and safety of a 3-day regimen of remdesivir, which is delivered intravenously. Among the 562 patients assigned 1:1 to receive remdesivir or placebo, the remdesivir group experienced a statistically significant 87% reduction in risk of COVID-19-related hospitalization or all-cause death by Day 28 when compared with the placebo group. The treatment group also had an 81% reduction in risk for medical visits due to COVID-19 when compared with the placebo group. No deaths occurred in the study by Day 28. The safety profile between remdesivir and placebo were similar, with the most common adverse events in the remdesivir group being headache and nausea. Veklury was the first COVID-19 treatment to receive full FDA approval, for use among adult and pediatric patients requiring hospitalization. However, there remains controversy over its effectiveness, with clinical trials showing varying success of the drug. Although antivirals tend to work better early in the course of disease, the drug’s intravenous administration presents logistical challenges for its use in non-hospitalized COVID-19 patients.
RONAPREVE/REGEN-COV The WHO today added the combination monoclonal antibody treatment known as Ronapreve, or REGEN-COV in the US, to its list of recommended COVID-19 therapeutics and called for producing companies and governments to address the high price and limited production of the drug, which contains casirivimab and imdevimab. The WHO urged US-based Regeneron Pharmaceuticals, which holds the patent on the combination drug, to share technology to allow for more widespread manufacturing, and said UN agencies are negotiating with Roche, which is currently manufacturing the drug for distribution at lower costs with a focus on low- and middle-income countries (LMICs). The WHO made conditional recommendations for the combination therapy—which is authorized for use in the US and the UK—to be used in patients with non-severe COVID-19 who are at high risk of hospitalization and individuals with severe cases but no existing antibodies.
US HOSPITAL CAPACITY Alaska is the latest US state to impose crisis standards of care this week, as hospitals nationwide are facing a continuing surge in severe cases. Alaska has set new single-day case records over the past several days due to the spread of the Delta variant, which is “crippling the health system,” according to Alaska Chief Medical Officer Dr. Anne Zink. In Idaho, which has seen a surge in COVID-19 cases and related deaths, health officials expanded to the entire state crisis standards of care already in place for health districts in the northern part of the state. Idaho currently has the lowest vaccination rate of any state, according to CDC data. Echoing the early days of the pandemic, elective surgeries again are being postponed across many states—including Idaho, Alaska, Montana, Nevada, and Oregon—in an effort to ration care in areas where hospital bed availability is limited. According to the US HHS Protect Public Health Data Hub, 78.6% inpatient beds across the nation are currently occupied.
SOUTHERN US BLACK COMMUNITIES Rural communities in the US South are disproportionately impacted by the COVID-19 pandemic, most likely due to disparities in social determinants of health such as employment and access to healthcare. In the region's predominantly Black communities, the pandemic has exacerbated ongoing medical and financial inequities. In a photojournalism report, titled “Distanced: Pandemic stories of Black life in the rural South,” STAT News examines the challenges these communities face and how they have found strength in the midst of this unprecedented public health emergency. Although the racial gap in COVID-19-related deaths seems to have shrunk in recent months, data can obscure the nuances in disparities; for example, Black people are less likely to live into older age, when COVID-19 is most lethal. Even when controlling for individual factors such as economic status, housing, education levels, preexisting health conditions, and occupation, researchers warn that structural racism contributes to demographic disparities in COVID-19 deaths, and the recent wave of cases due to the Delta variant have worsened these imbalances.
ponchi101 wrote: ↑Thu Sep 23, 2021 10:50 pm
From my side:
Mom almost certainly caught Covid. I can't travel because Venezuela maintains its border with Colombia locked (because of political reasons). I could only travel through Panama.
Yep, for me, 2020 never ended.
I admit I am (expletive) scared ****less.
I'm sorry, Ponchi (and jazz)
My SO's dad in Caracas is also getting over COVID. He was vaccinated (sister-in-law works at a hospital so they were able to get it) and was able to be treated by an at-home nurse, seems to be doing better. But it's nervewracking of course. Will be thinking about your mom.
by ponchi101 About the UK policy.
I have never understood, from our countries, why we only whine but not impose the same restrictions.
I remember after 9/11, the USA imposed a series of restrictions on many countries. You had to, for example, come into NYC and have your passport photocopied, triple checked and some other measures. The restrictions were applied to S. American countries.
Brasil said nothing. The simply opened a new lane at the Brasilian airports, exclusively for Americans, where they had to go through the same requirements as S. Americans had to go through at American airports. Any American that complained about it was quickly returned to the USA, no further questions asked.
It was the pressure from the same Americans that made the US Govt drop the measures.
My SO's dad in Caracas is also getting over COVID. He was vaccinated (sister-in-law works at a hospital so they were able to get it) and was able to be treated by an at-home nurse, seems to be doing better. But it's nervewracking of course. Will be thinking about your mom.
Txs.
Mom is vaccinated, one dose of Sputnik V. I am counting on that technology to be successful.
She is not overweight, but has a bit or high-blood pressure. Plus, the 82 yo is what is making me nervous. Spoke with her this morning, she feels like dirt but is doing fine. We should get results from her PCR any moment now.
by ti-amie Wishing the best to ponchi's mom and Jazz's aunt.
Meanwhile, covidiocy rages on.
by ponchi101 My looney buddy's son, D, just came back from Spain and is showing signs of some sort of flu. He already caught Covid before (all his family did) so no worries; he has already started him on ivermectin.
It is a disease within a disease.
by ponchi101 Because you all have been so kind.
Mom confirmed with COVID, as this morning her O2 level was 91% (too low) and sister decided it was time for the hospital. After tests, it was confirmed, but no complications. Got better during the day (O2 at 97%) and was discharged. At home and resting.
Txs for your good wishes. Not a fun morning, but I guess if I needed an excuse for an early beer, or several, this is it.
by JazzNU Wonderful news @ponchi! Really glad your sister took her to the hospital too, better safe than sorry. Glad her levels are so stable and hope she's feeling better.
And yeah, I may have had a drink or two (or ten) in the last week.
by ti-amie
by dryrunguy I think I forgot to post the most recent Situation Report from Tuesday. Work has been nuts.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 231.7 million cumulative cases and 4.75 million deaths worldwide as of September 27. Global weekly incidence and mortality continue to decrease for the third consecutive week.
Global Vaccination
The WHO reported 5.92 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 27. A total of 3.38 billion individuals have received at least 1 dose, and 2.46 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline, down to approximately 30 million doses per day*. The global trend continues to closely follow Asia. Our World in Data estimates that there are 3.52 billion vaccinated individuals worldwide (1+ dose; 44.7% of the global population) and 2.59 billion who are fully vaccinated (32.9% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
As we observed previously with 1+ dose coverage, Oceania’s full vaccination coverage (30.8%) is quickly approaching the global average (32.9%). Oceania could surpass this benchmark in the next several days, which would leave Africa (4.2%) as the only continent below the global average. Oceania and Africa were reporting similar full vaccination coverage as recently as late May, but vaccination efforts in Oceania have progressed rapidly over the past several months.
UNITED STATES
The US CDC reports 42.9 million cumulative COVID-19 cases and 686,639 deaths. Daily incidence continues to decline at the national level, down to approximately 115,000 new cases per day, which would be the lowest average since early August. Daily mortality appears to have leveled off at approximately 1,500 deaths per day.
It appears that daily mortality in Florida has continued to increase since late August, when the state changed its COVID-19 mortality reporting policy. The Florida Department of Health shifted from assigning dates to COVID-19 deaths corresponding to the date they were reported to the date of death. This results in lower reports for recent days due to the inherent reporting lag, which can give a false impression of rapidly declining daily mortality. Deaths are then filled in retrospectively on the date of death as they are reported to the state, which can take days or weeks after the death occurs. At the time of the change, we estimated that Florida’s daily mortality was likely greater than 200 deaths per day. Since then, the average increased to at least 363 (September 1), and it has remained greater than 200 from at least August 7 through September 15. Florida’s daily incidence plateaued from approximately August 10-30 before decreasing. If historical trends continue, we can expect to observe a corresponding decrease in daily mortality around this time; however, it could be another several weeks before Florida’s mortality reporting fills in enough for that trend to be evident.
US Vaccination
The US has administered 391 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend continues to decline from the most recent peak on August 29* (approximately 850,000), down to fewer than 600,000 doses per day. There are 213.7 million individuals who have received at least 1 dose, equivalent to 64.4% of the entire US population. Among adults, 77.1% have received at least 1 dose, as well as 14.6 million adolescents aged 12-17 years. A total of 183.9 million individuals are fully vaccinated, which corresponds to 55.4% of the total population. Approximately 66.6% of adults are fully vaccinated, as well as 11.8 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
NOVAVAX WHO EMERGENCY USE LISTING APPLICATION On September 23, Novavax announced its submission to the WHO for Emergency Use Listing (EUL) for its SARS-CoV-2 vaccine candidate. This submission was made in partnership with the Serum Institute of India, which will manufacture the vaccine. Novavax is prioritizing access to low- and middle-income countries (LMICs), and it has already submitted regulatory documents to several individual countries including India, the Philippines, and Indonesia. Novavax and the Serum Institute have jointly pledged to provide more than 1.1 billion doses to the COVAX facility, which also targets LMICs. Phase 3 clinical trials are still ongoing in several countries, including Mexico, the UK, and the US, and preliminary analysis estimates strong efficacy against the original strain of the virus as well as multiple variants of concern (VOCs).
PFIZER-BIONTECH SUBMIT PEDIATRIC PHASE 2/3 DATA Pfizer and BioNTech announced today that they submitted preliminary data from Phase 2/3 clinical trials on pediatric use of their SARS-CoV-2 vaccine to the US FDA. The submission includes data from nearly 2,300 participants ranging from age 5 years to less than 12 years, and the trial tested a regimen of 2 doses of 10μg each—compared to 30μg for the adult formulation. According to a press release from Pfizer, “the vaccine demonstrated a favorable safety profile and elicited robust neutralizing antibody responses” that were comparable to individuals aged 16-25 years. The companies intend to apply for Emergency Use Authorization (EUA)—as and submit applications to the European Medicines Agency and other national regulatory agencies—for this age group in the coming weeks. White House Chief Medical Advisor Dr. Anthony Fauci indicated that vaccinations for this age group could potentially begin before the end of October. The full trial data have not yet been published publicly or subjected to peer review. Phase 2/3 clinical trials are ongoing for younger children—2 years to less than 5 years and 6 months to less than 2 years—who received 2 doses of 3μg each.
PRIOR INFECTION & IMMUNE PROTECTION As we have discussed previously, protection conferred by vaccination has been demonstrated to be better than protection conferred via natural SARS-CoV-2 infection. Two recent studies, however, provide further analysis of the immune response during and following SARS-CoV-2 infection, including possible protection against re-infection. A study from Japan, published in the Journal of Medical Virology, analyzed the IgG and IgM responses against 2 SARS-CoV-2 proteins (N and S1) in 231 COVID-19 patients. The researchers found that mild cases exhibited stronger immune responses (IgM and IgG) against both proteins early after symptom onset than severe or critical cases. As the disease progressed, the IgM and IgG responses increased in severe and critical cases higher and more rapidly than for mild cases. Additionally, the immune responses remained elevated for longer periods of time in patients with severe or critical disease, while they declined more rapidly for patients with mild disease. ELISA analysis demonstrated that a significantly higher proportion of severe and critical patients remained seropositive at 22 days after symptom onset than for mild patients for the S1 protein but not the N protein. The researchers note that lower immune response among mild cases could potentially signal lower levels of neutralizing antibodies and a shorter period of conferred immune protection against re-infection. Further analysis is needed to better characterize the duration and strength of protection, including the role of the innate immune response and memory B and T cells, and any association with disease severity during the initial infection.
A study in rhesus macaques, published in Science Translational Medicine, evaluated the immune response to re-infection with the Alpha and Beta variants of concern (VOCs) following infection with the original strain of SARS-CoV-2. Researchers infected 18 rhesus macaques with the original strain of the virus (WA1/2020) and then exposed them to either the original strain (control), the Alpha variant, or the Beta variant 35 days later. The animals re-infected with the Alpha variant did not exhibit a notable difference in the concentration of breakthrough virus compared to the control group, whereas the animals re-infected with the Beta variant exhibited much higher concentrations of breakthrough virus. Three (3) additional naïve animals were exposed a single time to the Beta variant in order to compare the immune responses to an original infection and a re-infection. Notably, the animals that were re-infected exhibited lower concentrations of virus, and the re-infected animals exhibited increased neutralizing antibody levels after the second infection, compared to the first. These results suggest a boosted immune response conferred by the initial infection. Interestingly, the animals re-infected with the original strain or the Alpha variant exhibited lower neutralizing antibody responses against the Beta variant, whereas the animals re-infected with the Beta variant generated similar neutralizing antibody responses for all 3 variants. This illustrates that natural infection with one variant can provide some, although not complete, protection against re-infection with other variants, including VOCs; however, the degree of protection could be dependent on the strain or variant. The Delta variant, which has become the dominant strain in many countries, was not evaluated in this study, and as we have covered previously, animal models do not always accurately reflect the immune response in humans.
PANDEMIC ORIGINS Origins of the SARS-CoV-2 virus have been at the forefront of international debate since the onset of the COVID-19 pandemic. The WHO’s Scientific Advisory Group on the Origins of Novel Pathogens (SAGO) was created in May 2020 to identify novel pathogens and advise the WHO on technical and scientific considerations regarding their emergence and re-emergence. SAGO recently released a call for international experts to join the group, with an emphasis on increasing global representation and coordination in the effort to identify the origins of SARS-CoV-2. Some studies have linked SARS-CoV-2 virus to other endemic human coronaviruses and identified genetic similarities between SARS-CoV-2 and other coronaviruses. International debate around the origins of SARS-CoV-2 continues, however, with some experts advocating for a revival of scientific investigations in China and elsewhere, to provide additional information regarding various origin scenarios, including zoonotic transmission or laboratory research. Leading WHO infectious disease epidemiologist Dr. Maria Van Kerkhove emphasized that SAGO is not a new fact-finding mission to China. Rather, SAGO advises the WHO on a framework of study to understand the origins of emerging and re-emerging pathogens, and any future missions, to China or elsewhere, will be coordinated directly between the WHO and national governments.
JAPAN EASING COVID-19 RESTRICTIONS Japanese Prime Minister Yoshihide Suga announced yesterday that Japan will lift its nationwide COVID-19 state of emergency on September 30 and begin relax associated restrictions. While Japan will lift many COVID-19 protective measures, it will reportedly implement testing and vaccine passport programs to mitigate risk while facilitating increased social and economic activity. Local governments may continue to recommend voluntary restrictions on businesses, such as reduced hours of operation and alcohol sales at bars and restaurants, after the emergency is lifted. Japan faced a surge in COVID-19 incidence that coincided with the 2020 Summer Olympic and Paralympic Games, but it has receded rapidly in recent weeks.
AFRICA VACCINE HESITANCY In addition to barriers to accessing sufficient SARS-CoV-2 vaccine supply, African countries are also facing challenges with vaccine hesitancy. Dr. John Nkengasong, Director of the Africa CDC, recently commented on a potential link between international travel restrictions in the UK and hesitancy among African populations. The concern stems from the limited list of countries for which travelers arriving in the UK can “qualify as fully vaccinated.” Travelers vaccinated under a UK, EU, or US vaccination program or individuals arriving from a list of 18 countries who can show proof of full vaccination can enter the UK as “fully vaccinated” travelers, with limited restrictions or quarantine or testing requirements. Notably, the list does not include any countries from Africa, which Dr. Nkengasong argues could serve as a disincentive to get vaccinated. If travelers from African countries cannot qualify as fully vaccinated, even with documentation of full vaccination, some individuals may not see value in the vaccination. Similar opposition has been reported in India and other parts of Asia as well as Latin America. Dr Richard Mihigo, an official from the WHO's Africa region, called on countries to develop a cohesive global system for demonstrating vaccination status and lift travel restrictions for vaccinated travelers that are dependent on country.
SOUTHEAST ASIA ECONOMIC IMPACT The COVID-19 pandemic and associated restrictions continue to have long-term negative effects on local, national, and global economies. In Southeast Asia, several major economic forecasts have downgraded their previous projections and warn of slower economic growth in 2021. The Asian Development Bank lowered its previous regional projection from 4.4% to 3.1% growth over the course of 2021, which signals slower economic recovery from the pandemic. Additionally, the bank lowered its growth projections for all national-level economies, with the exception of the Philippines and Singapore, and Singapore is now the only country in Southeast Asia projected to grow its economy by more than 5% in 2021.
Similarly, the World Bank downgraded its economic growth projections for “developing countries in East Asia.” The new 2021 projection for these countries falls from 4.4% growth to just 2.5%, which stands in stark contrast to the projected 8.5% growth in China. Even in countries that are currently exhibiting stronger economic growth, the trend is slowing as COVID-19 surges continue, driven largely by the Delta variant. The report emphasizes that the pandemic is compounding growing inequality in the region, which will have negative impacts on future economic growth.
Following COVID-19 surges tied to Delta variant, some Southeast Asian countries are once again opening borders to allow travel and tourism, including to some population island destinations in the region. Countries are implementing combinations of vaccine mandates and testing requirements in order to allow international travelers to arrive without lengthy quarantines. Some national and local economies rely heavily on tourism to drive their economies, and they have been severely impacted by travel restrictions during the pandemic. Some countries are moving slowly, with initial limits on traveler volume for specific destinations (including some local areas with high vaccination coverage), before expanding. Some countries that limited domestic travel during the pandemic (eg, to remote islands) are also resuming some domestic travel and tourism opportunities.
NEW YORK HEALTHCARE WORKERS The New York Governor Kathy Hochul, signed an executive order on September 27 to address potential worker shortages as the state’s vaccine mandate goes into effect. The executive order allows the Governor to activate the National Guard or bring in healthcare workers from other states to fill critical personnel shortages. Early evidence indicates that thousands of previously unvaccinated healthcare workers showed up to vaccination sites to receive their first dose in the hours before the mandate went into effect. Approximately 5,000 employees remain unvaccinated, which is a sharp decline from 8,000 a week ago. The statewide vaccination coverage for hospital employees is now reported as 92% with at least 1 dose, and the vaccination also increased among nursing home employees, up from 84%to 92%. Despite these encouraging signs, some hospital employees are still threatening to accept being fired rather than get vaccinated. Some of these individuals indicated that they feel betrayed by the hospital system and government, and they do not trust the vaccine, despite widespread evidence of safety and efficacy. Employees who remain unvaccinated could be put on unpaid leave and eventually fired. The CEO of the New York City Health+Hospitals health system reported that all facilities are currently functional and that there are no serious reports of staffing shortages.
US SCHOOL TESTING Inconsistent SARS-CoV-2 testing procedures and requirements at schools across the US are raising concerns with parents and stressing the capacity of the school systems trying to implement them. Even school districts in the same city can have very different testing and isolation standards. In Texas, for example, the San Antonio Independent School District offers weekly testing for all students and staff, which consumes a lot of time and resources, even though only 30% of students are participating in the program. Conversely, nearby Boerne Independent School District offers testing only by appointment, and symptomatic students and staff are not referred for testing or sent home unless they can no longer participate in classroom instruction.
While some school districts are foregoing robust testing programs based on the belief that they are unnecessary, others are unable to implement them due to a lack of resources, including access to test kits and personnel to conduct large numbers of regular tests. In Illinois, the state reported surge of enrollments in its statewide school-based testing program as daily incidence increased across the state and the new school year approached. But because schools enrolled late in the process, most do not yet have the logistics and operational systems in place to implement the testing programs. It can take 3-6 weeks to establish these systems, which has delayed testing in some schools, even after classes have already resumed. The Berkeley (California) Unified School District used state COVID-19 funding as well as its own budget to hire 21 personnel, just to implement its testing program; however, most school districts do not have the funding available to hire new, dedicated staff for testing programs.
US RAPID TEST SHORTAGE A nationwide shortage of SARS-CoV-2 rapid antigen tests has been reported in the US, while capacity for PCR-based tests remains high. PCR tests must be processed by a lab, however, and results can often take between 1-3 days (or longer). Rapid tests and at-home tests may have a slightly lower accuracy than PCR tests, but they can still identify nearly 98% of infectious cases and provide convenient results within 15-20 minutes. The shortage of rapid testing kits means that schools, nursing homes, shelters, and workers that rely on fast testing results to go to work each day or prevent outbreaks among at-risk populations are struggling to access adequate resources. Increased wait times for testing results mean that shelters, clinics, and schools are at increased risk for outbreaks, and workers who require daily testing could be forced to miss work and lose income.
The nationwide shortage of rapid tests may be a function of decreased testing demands and increasing vaccination coverage over the summer. The Delta variant surge and slowing vaccination progress are driving increased demand for rapid tests, and manufacturers have not yet increased production capacity to catch up. Insufficient supply of rapid and at-home tests is driving up testing demand at other locations, including urgent care centers.
The increased demand and supply limitations for rapid tests is driving up the prices of some other testing products. The CARES Act passed in 2020 requires that insurers pay the cost of SARS-CoV-2 testing conducted at out-of-network laboratories. One company, GS Labs, is routinely charging US$380 per test, and insurers argue that the high cost is “price-gouging,” and in some instances, they are refusing the pay. The elevated cost of these tests could result in higher insurance premiums. GS Labs argues that it approached insurers about becoming an in-network provider for reduced costs, but it was generally rejected. The company also cites its excellent service and a high start-up cost as justification for the elevated price for its tests. A representative for the company emphasizes that customers can schedule an appointment for immediate testing and receive results within 15-20 minutes, while many drugstores and pharmacies have no rapid tests available. There are currently several ongoing lawsuits that aim to determine how much insurers have to pay. Increasing the availability of rapid and at-home tests, which typically cost on the order of US$20, would help increase testing access and reduce the need for higher-cost testing options.
by ponchi101 On the anecdotal front.
My mom is at home, recovering. She feels terribly weak. I suspect that this will not kill her, but I think that it will be a considerable time before she can resume any sort of "normal" life. At 82, and a person that was never into any sort of athletics, this may change her lifestyle considerably. Problem 1: if she is able to come here to Colombia, I live up a flight of stairs for which there is no elevator. I wonder how we will deal with that.
But. My sister also came down with covid. AGAIN. She had it last year (she lives upstairs from my mother) and it hit her hard last time. And it is hitting her hard this time too. Both of them were vaccinated with Sputnik V vaccines, but got only one dose (I suspect it has helped my mother). So, while I would be not totally hesitant to recommend the Russian vaccine, I doubt it is effective in keeping symptoms down.
Of course, a sample of two is worthless and knowing Venezuela, there is no way to find out what is really happening down there.
by ti-amie
ponchi101 wrote: ↑Thu Sep 30, 2021 11:49 pm
On the anecdotal front.
My mom is at home, recovering. She feels terribly weak. I suspect that this will not kill her, but I think that it will be a considerable time before she can resume any sort of "normal" life. At 82, and a person that was never into any sort of athletics, this may change her lifestyle considerably. Problem 1: if she is able to come here to Colombia, I live up a flight of stairs for which there is no elevator. I wonder how we will deal with that.
But. My sister also came down with covid. AGAIN. She had it last year (she lives upstairs from my mother) and it hit her hard last time. And it is hitting her hard this time too. Both of them were vaccinated with Sputnik V vaccines, but got only one dose (I suspect it has helped my mother). So, while I would be not totally hesitant to recommend the Russian vaccine, I doubt it is effective in keeping symptoms down.
Of course, a sample of two is worthless and knowing Venezuela, there is no way to find out what is really happening down there.
by JazzNU
ponchi101 wrote: ↑Thu Sep 30, 2021 11:49 pm
On the anecdotal front.
My mom is at home, recovering. She feels terribly weak. I suspect that this will not kill her, but I think that it will be a considerable time before she can resume any sort of "normal" life. At 82, and a person that was never into any sort of athletics, this may change her lifestyle considerably. Problem 1: if she is able to come here to Colombia, I live up a flight of stairs for which there is no elevator. I wonder how we will deal with that.
But. My sister also came down with covid. AGAIN. She had it last year (she lives upstairs from my mother) and it hit her hard last time. And it is hitting her hard this time too. Both of them were vaccinated with Sputnik V vaccines, but got only one dose (I suspect it has helped my mother). So, while I would be not totally hesitant to recommend the Russian vaccine, I doubt it is effective in keeping symptoms down.
Of course, a sample of two is worthless and knowing Venezuela, there is no way to find out what is really happening down there.
Sorry your mom isn't rebounding faster and that your sister is also not feeling well. Hopefully in another week or two they will feel progressively better than they currently do and it's not something that will affect them long term.
by dmforever Gosh I"m so sorry to hear that your mom is still not feeling better and that your sister is sick too. I really hope that they get better soon.
Kevin
by JazzNU I should've mentioned it before, but didn't want to just be unloading on here. But my uncle and cousin also tested positive. Also vaccinated. My uncle doesn't typically get sick much, this did make him sick and it hung on for about 2 weeks from when it first took root in his system. He's finally feeling better. My cousin, she was doing okay til last week, started getting really bad headaches, went to the doctor, got medication but it wasn't working on them and then lost her sense of smell and taste and the doctor called a day late and was like, yeah, you're positive, that's why you're migraine meds aren't doing all that much for you.
Aunt, uncle, and cousin all had that 15-minute covid tests done twice, all came back negative. It is completely unsettling how much Southern states are still using these rapid covid tests like they are anywhere near as good or definitive as a PCR test. My cousin's doctor office used one (now the 3rd rapid test), and I was shocked. But at least they ran both on her, but she was like, "I don't have covid" after her appointment because that's what they confirmed for her for the 3rd time. Wasn't until the over 24 hours later when they called to let her know the PCR results that she knew she needed to isolate. I'm aware of this going on a ton in Florida and Georgia and a few other Southern states, not sure where else. But helps to somewhat explain more why they have more trouble. If you take a test and it says negative and keep going any and everywhere, of course the virus is going to circulate constantly.
So, this is a PSA. Make sure you aren't relying too heavily on rapid covid tests, especially if you have reason to believe you've been around someone positive. If you get one, think about also getting a PCR if you're truly trying to make certain you don't have the virus and aren't spreading it to others.
by ponchi101 My GF has to go to Venezuela inn about two weeks, and she needs a PCR from here (Colombia) and Venezuela is running that same FAST-TEST you are talking about, which they perform on you upon arrival, for $60. Then you need one more before departing, but to enter the airport, you need a real PCR. So, you get to the airport with your PCR, but it is not valid to board the plane, so you need a second "quick" one, at another $60.
But that quick one seems to be unreliable, and your story confirms it.
To all, txs for the good thoughts. One of the things about C19 is, of course, that we have enough literature about it to know that even if you make it trough, you may end up with some other conditions that will linger longer. And, of course, it seems by now pretty obvious that the vaccines do not stop the spread, they stop the symptoms. So, pretty much, I believe we will all get it, sooner or later.
by Jeff from TX My COVID story: I have a house in TX (it's in extremely poor condition) that I am selling that was supposed to close today. It really is just being sold for the lot value. I signed my papers yesterday; the buyers were supposed to sign and close today. Both of them (a mother and daughter) have COVID. The mom (a nice lady) has asthma and diabetes (not on insulin). Apparently they went to a fundraiser last week in a more rural county in Central TX. It seems (from what she said) that it may have turned into a superspreader event. Both husbands and the sheriff caught as well as approximeately half the people in attendance. I don't know whether they were vaccinated but I suspect not knowing the politics of the area.
I called to go over a couple of things regarding the property and talked to mom. She isn't in the hospital, but her O2 stats are at 88% (she has been conferring with her pulmonogist) and is on oxygen at home. I asked her how often she was checking it. Not enough. Asked her if she was on sick day protocols for her diabetes and if she was checking her glucose levels. Not very often (she was coughing constantly). I asked if she was sleeping in a prone position or sitting up. Whether she was doing any kind of deep breathing exercises intermittantly (doubt if she has an IS at home). No. We discussed some things I would be doing and that if the oxygen drops lower, the need to go to the hospital (since her Dr. knows her O2 levels). The need to log and look for trends. Sigh.
SO then I talked to my stepson who has something at the house that he wants. Told him to get vaccinated. That broke down into a heated argument because, you know, it's still experimental. And only 0.3% of people that catch it die. And maybe, after 10 years with data, he might get it. I said I don't know anyone in the hospital with reactions to the vaccine. But, you know, they hide those deaths. Afterward, I thought thank goodness my husband isn't alive to have witnessed this. It would have broken his heart. *Sigh*
Where is Steven when I need some comfort?
by ponchi101 It is that way. It is truly magical thinking. Every time you mention some flaw in the logic, they come up with that. "They" hide that data.
But "they" don't hide the real stuff from "them" (your stepson). They can't see the flaw in reasoning.
by JazzNU
Jeff from TX wrote: ↑Fri Oct 01, 2021 4:01 am
I called to go over a couple of things regarding the property and talked to mom. She isn't in the hospital, but her O2 stats are at 88% (she has been conferring with her pulmonogist) and is on oxygen at home. I asked her how often she was checking it. Not enough. Asked her if she was on sick day protocols for her diabetes and if she was checking her glucose levels. Not very often (she was coughing constantly). I asked if she was sleeping in a prone position or sitting up. Whether she was doing any kind of deep breathing exercises intermittantly (doubt if she has an IS at home). No. We discussed some things I would be doing and that if the oxygen drops lower, the need to go to the hospital (since her Dr. knows her O2 levels). The need to log and look for trends. Sigh.
SO then I talked to my stepson who has something at the house that he wants. Told him to get vaccinated. That broke down into a heated argument because, you know, it's still experimental. And only 0.3% of people that catch it die. And maybe, after 10 years with data, he might get it. I said I don't know anyone in the hospital with reactions to the vaccine. But, you know, they hide those deaths. Afterward, I thought thank goodness my husband isn't alive to have witnessed this. It would have broken his heart. *Sigh*
Where is Steven when I need some comfort?
Sorry to hear your stepson is listening to Facebook medicine and logic. I know that's frustrating.
Very kind of you to check in on the mom and she's lucky you're the one who is selling. Even if she's not doing everything she could or should be right now, it's likely at least in her mind to pay attention to those things more if she deteriorates from her current state, which is something even if it didn't seem like it's enough.
by dryrunguy Here's the latest Situation Report, this time posted in a timely manner.
::
EDUCATIONAL OPPORTUNITIES The Johns Hopkins Center for Health Security provides education and academic training focused on Health Security for students at the Johns Hopkins Bloomberg School of Public Health. For academic year 2022-23, the Center will provide 2 Masters of Public Health scholarships and fund 2 PhD candidates for the Health Security PhD track at the Johns Hopkins Bloomberg School of Public Health. These opportunities are now accepting applications. Find more information and application details here.
EPI UPDATE The WHO COVID-19 Dashboard reports 233.5 million cumulative cases and 4.77 million deaths worldwide as of October 1.
After plateauing since late July and recording slightly fewer than 800 deaths per day, Russia set a new national record this week for daily mortality (816.4), surpassing 800 daily deaths for the first time since the onset of the pandemic. Russia also reported a new single-day record (852 deaths) on September 28. Russia’s daily incidence has been increasing steadily since mid-September, up from approximately 18,000 new cases per day to nearly 22,000 (+22%) over that period. Russia’s highest average daily incidence was 28,500 new cases per day in late December 2020. Russia has fully vaccinated nearly 30% of its population, but daily vaccinations have steadily declined to less than 25% of its record high in mid-July.
Global Vaccination
The WHO reported 6.14 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of September 29. A total of 3.51 billion individuals have received at least 1 dose, and 2.55 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline, remaining at or below 30 million doses per day since September 22*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 3.57 billion vaccinated individuals worldwide (1+ dose; 45.3% of the global population) and 2.65 billion who are fully vaccinated (33.7% of the global population). As we observed previously with 1+ dose coverage, Oceania’s full vaccination coverage (32.3%) is quickly approaching the global average (33.7%). Oceania could surpass this benchmark in the next several days, which would leave Africa (4.4%) as the only continent below the global average. Oceania and Africa were reporting similar full vaccination coverage as recently as late May, but vaccination efforts in Oceania have progressed rapidly over the past several months.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
The WHO’s Regional Office for Africa (AFRO) announced that only 15 African countries surpassed 10% full vaccination coverage by the target date of September 30. The goal was set by the World Health Assembly in May 2021. Despite accounting for 17% of the global population, only 2% of SARS-CoV-2 vaccine doses administered globally have been in Africa, illustrating the magnitude of ongoing disparities in vaccine access. These countries represent nearly one-third of African nations—compared to nearly 90% of high-income countries—but only about 11% of the African population (1.3 billion). Most of the countries that surpassed the 10% benchmark have small populations, and more than half of all African countries are reporting full vaccination coverage of 2% or less. Seychelles and Mauritius remain at the top of African countries in terms of full vaccination coverage, with 72% and 63%, respectively. Morocco surpassed 50% coverage, Tunisia is reporting 32%, and Cape Verde* is reporting nearly 25%. Vaccination progress is accelerating, however, with monthly distributions increasing 10-fold from June to September. The target by the end of 2021 is 40% coverage, but it is unlikely that more than a small handful of African countries will reach that benchmark.
*Or Cabo Verde.
UNITED STATES
The US CDC reports 43.3 million cumulative COVID-19 cases and 694,701 deaths. Daily incidence continues to decline at the national level, down to approximately 106,000 new cases per day, which is the lowest average since early August. Daily mortality appears to have passed a peak and started to decline. While the average decreased over the second half of September—down to 1,476 per day—the single-day total for September 29 was more than 2,000 deaths, the third-highest since February. At the current pace, the US could surpass 700,000 cumulative deaths in the next 4 days*.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over the weekend or for states that are reporting mortality by date of death. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 393 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend continues to decline from the most recent peak on August 29*, from approximately 850,000 doses per day to slightly more than 600,000. There are 214.3 million individuals who have received at least 1 dose, equivalent to 64.6% of the entire US population. Among adults, 77.3% have received at least 1 dose, as well as 14.6 million adolescents aged 12-17 years. A total of 184.6 million individuals are fully vaccinated, which corresponds to 55.6% of the total population. Approximately 66.9% of adults are fully vaccinated, as well as 11.9 million adolescents aged 12-17 years. The CDC recently updated its vaccination tracking dashboard to include booster doses. To date, 4.03 million individuals have received booster doses, the majority of whom are aged 50 years and older (3.35 million), including 2.50 million aged 65 years and older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
VACCINE MANDATES Evidence from several states and private companies that have implemented SARS-CoV-2 vaccine mandates shows the requirements are working to boost vaccination rates among healthcare workers and other employees. In California, major health systems reported a statewide mandate helped increase vaccination rates among their employees to 90% or more, and in New York, 92% of hospital and long-term care facility employees have received at least 1 dose of vaccine after a mandate took effect on September 27, an increase of about 10 percentage points over 1 week ago. However, hospitals in New York continue to fear staff shortages. New York Governor Kathy Hochul signed an executive order earlier this week aimed at providing short-term relief to healthcare systems impacted by staff shortages, but no facilities have closed since the mandate went into effect.
Private employer vaccine mandates are becoming more common, but opposition remains. United Airlines announced this week the company would terminate nearly 600 of its 67,000 employees if they continue to refuse to comply with its vaccination requirement. The company, one of the first large US corporations to impose a mandate, said 99% of its workforce is vaccinated and it is working with employees who decide to get vaccinated after the initiation of their termination proceedings. Tyson Foods, which announced a vaccine mandate for employees in August, said this week that 91% of the company’s 120,000 workers are now vaccinated. Tyson’s frontline workers now have until November 1 to get vaccinated or request an exemption, whereas its 6,000 office workers’ deadline is today. Earlier this month, US President Biden announced a federal vaccine mandate for companies with 100 or more employees, to be enforced by the Occupational Safety and Health Administration (OSHA). The US Armed Forces also are requiring vaccinations for active duty personnel. On September 30, a group of 10 plaintiffs, including US Air Force officers and a Secret Service agent, filed a lawsuit seeking an injunction halting federal vaccination requirements, claiming the mandates violate the First Amendment.
SCHOOL MASK POLICIES Children across the US have had a tumultuous start to the new school year, with more than 900,000 students in 44 states having been affected by COVID-19-related closures between August 1 and mid-September. In 2 new analyses published in the US CDC’s Morbidity and Mortality Report (MMWR), the agency adds to the growing evidence that school mask mandates can help prevent COVID-19 outbreaks in classrooms. Using information from 520 US counties, representing 16.5% of the nation’s total counties, researchers found that pediatric COVID-19 case rates rose more sharply in counties without school mask requirements between July 1-September 4, 2021, when compared with counties that had school mask mandates. The daily case rates remained lower in schools requiring masks even after controlling for covariates. Another analysis examined the association between mask policies and school-associated COVID-19 outbreaks in 2 large Arizona counties that returned to in-person, K-12 schooling in late July/early August 2021. The researchers found that schools without mask mandates were 3.5 times more likely to have a school-related COVID-19 outbreak than those that instituted early mask mandates.
Regardless, legal disputes over mask requirements in schools continue in several states. The US government on September 30 filed a formal statement with the federal district court in Austin, Texas, saying the state’s ban on school mask mandates violates the rights of students with disabilities if it prevents them from safely attending public school in-person. In Iowa, the American Academy of Pediatrics (AAP) and its state chapter filed an amicus brief on behalf of a group of parents and disability rights advocates who filed a federal lawsuit against Governor Kim Reynolds seeking to reverse a law prohibiting school boards from imposing mask mandates. The AAP warned that pediatric COVID-19 cases have risen sharply since the beginning of the school year. Legal proceedings over a law in Arizona banning schools from implementing mask requirements are ongoing, with the state Supreme Court on September 29 setting a briefing schedule to hear arguments. And in Michigan, several local health departments are working to understand language that appears to ban school mask mandates contained within the state’s budget signed this week by Governor Gretchen Whitmer. Although she issued a statement saying a provision that strips state funding from local health departments with school mask mandates is unconstitutional, some districts are rescinding mask requirements over fear of lawsuits.
VACCINE EFFICACY & EFFECTIVENESS REVIEW Researchers from Johns Hopkins University (US) led a systematic review of the efficacy and effectiveness of existing SARS-CoV-2 vaccines. The study (preprint) evaluated clinical trial and observational data for all vaccines that submitted applications for Emergency Use Listing (EUL) from the WHO by August 15, 2021, including data published in peer-reviewed journals and via preprint servers, government public health and regulatory websites and databases, news media, and manufacturers’ websites. The researchers accounted for differences in study population, case definition, follow-up duration, presence of variants of interest or concern (VOIs/VOCs), epidemiological situation (eg, degree of community transmission), and study design.
The study included 24 vaccine products, including multiple vaccine platform technologies, of which 13 had published Phase 3 clinical trial results or data and 6 had received an EUL from the WHO. The researchers provide an overview of the available data and highlight outstanding gaps, including specific types of analysis (eg, effectiveness in previously infected individuals, efficacy/effectiveness against the Gamma variant) and individual products (eg, Sputnik V. Sinopharm-Beijing). Of the 24 products, Phase 3 clinical trial data were available for 15, but only 9 had been subjected to peer review. The researchers also include a set of figures that illustrate the timing of Phase 3 clinical trials in the context of the daily COVID-19 incidence in various countries, which can affect the quality of study data and the duration of clinical trials. Overall, the vaccines currently in use have demonstrated high efficacy/effectiveness against symptomatic COVID-19 disease, severe disease, and death, and analysis exists that also shows some degree of protection against infection. The results vary between products, but among those with available estimates, the efficacy/effectiveness against symptomatic disease was greater than 65% for all of them (and none of the confidence intervals fell below 50%).
ADDITIONAL VACCINE DOSE SAFETY People who received a third dose of an mRNA SARS-CoV-2 vaccine experienced similar adverse events compared with the second dose, according to a report published September 28 in the US CDC’s Morbidity and Mortality Weekly Report (MMWR). Individuals with moderate-to-severe immune-compromising conditions became eligible for an additional dose on August 12, when the US FDA amended the Emergency Use Authorizations (EUAs) for both the Pfizer-BioNTech and Moderna vaccines. The report’s data come from voluntary V-SAFE registrants who completed check-ins for all 3 doses. According to data from 12,591 vaccinees who recorded information for a third dose from August 12-September 19, 2021, 79.4% reported local reactions compared to 77.6% of individuals after a second vaccine dose. Systemic reactions were reported by 74.1% of people after a third dose compared with 76.5% after the second dose. The most frequently reported symptoms included injection site pain, headache, and fatigue, and most commonly occurred the day after vaccination. Overall, no unexpected patterns of side effects were reported among more than 22,000 individuals who received a third vaccine dose and reported to V-SAFE between August 12 and September 19, and their recorded symptoms were categorized as mild or moderate.
PREGNANCY & VACCINATION The US CDC issued a Health Alert Network (HAN) advisory recommending urgent action aimed at vaccinating pregnant individuals against SARS-CoV-2. The advisory encourages those who are pregnant, recently pregnant (including lactating individuals), who are trying to become pregnant, or who may become pregnant in the future to get vaccinated. The advisory comes after the highest reported number of COVID-19-related deaths in pregnant people (n=22) occurred in August 2021, the agency noted, with more than 125,000 laboratory-confirmed cases and 22,000 hospitalizations among pregnant people since January 2020. A similar directive was issued last month, but this is one of the agency’s strongest recommendations yet for pregnant individuals. Vaccination coverage among pregnant individuals remains low, at 32%, but varies by race/ethnicity. The lowest rate for fully vaccinated pregnant persons is among non-Hispanic Black individuals at 17%, followed by Hispanic or Latino individuals at 27%. Asian pregnant individuals have the highest rate of vaccination at 47%. Non-Hispanic White individuals and those in the ‘other’ category fall in at 35% and 32%, respectively.
LONG COVID Ongoing studies are helping to better characterize and determine the prevalence of so-called long COVID, also known as post-acute sequelae of SARS CoV-2 infection (PASC). In a study published in PLOS Medicine, researchers led by scientists with the University of Oxford conducted a retrospective cohort study based on linked electronic health records (EHRs) data from 81 million patients including 273,618 COVID-19 survivors, primarily in the US, and included 114,449 patients with influenza as a control. The researchers found that nearly 37% of COVID-19 patients studied reported having at least 1 or more features of long COVID between 3 and 6 months after their initial diagnosis, a higher percentage than the 10%-30% reported in previous studies and significantly higher than after influenza. The most commonly reported symptoms included abnormal breathing; fatigue; chest, throat, or other pain; headache; abdominal symptoms; and anxiety or depression. While lingering symptoms occurred more frequently among people who had more severe acute COVID-19, including those who were hospitalized, and older individuals, the researchers stressed that people who had mild disease and children and young adult survivors also experienced long COVID.
In a study published September 29 in JAMA Network Open, researchers interviewed 2,433 COVID-19 patients who were discharged from 2 hospitals in Wuhan, China, between February 12 and April 10, 2020. Notably, 45% of patients reported at least 1 symptom at 1-year follow-up, with the most common symptoms being fatigue, sweating, chest tightness, anxiety, and muscle pain. Patients who experienced more severe COVID-19 cases and who were older were more likely to have at least 3 lingering symptoms. In yet another study, posted to the preprint server medRxiv, researchers found that SARS-CoV-2 infection, even mild cases, could reduce gray matter thickness in the brain, possibly contributing to long-term neurological damage. Taken together, the studies highlight the fact that the health impacts from COVID-19 extend far beyond the acute phase, and contribute more knowledge about the risk of long COVID, for both unvaccinated and vaccinated individuals, that could help identify those at greatest risk, plan necessary ongoing health services support, and help develop treatments for the condition.
COVAX 2022 STRATEGY The governing body for Gavi, The Vaccine Alliance, met this week to discuss its primary objective of expanding routine immunization but also welcomed participation of the Co-Chairs of the AMC Engagement Group and the COVAX Shareholders’ Council to assess the vaccine initiative’s “critical challenges” and make progress toward developing the 2022 COVAX strategy. The Co-Chairs and Board members expressed support for COVAX’s urgent call to lift all SARS-CoV-2 vaccine export restrictions; manufacturers to deliver on their commitments to COVAX with transparency on schedules and supply chains; countries with high vaccination coverage rates to relinquish their place in line to allow more vaccine supply to go to COVAX and low- and middle-income countries (LMICs) in need; and global donations to be expanded, fast-tracked, and standardized. With more than 311 million doses shipped, the Board highlighted the importance of quickly scaling up vaccine deliveries, as supply is significantly increasing. Echoing the results of the meeting, Gavi Board Chair José Manuel Barroso, a former president of the European Commission, writing in an opinion piece published in POLITICO Europe on September 30, called on wealthy countries’ governments and manufacturers to do more to “close today’s unacceptable gap in vaccine equity.”
US PANDEMIC PREPAREDNESS More than 20 stakeholder organizations this week sent a letter to the US Congress urging them to provide at least US$16 billion in pandemic preparedness funding included in a version of the Build Back Better Act passed by the US House Committee on the Budget. The funding would go toward efforts to improve the country’s pandemic defenses, including the ability to produce diagnostics, vaccines, and treatments for known and future biological threats; track and monitor potential outbreaks; provide sufficient medical supplies; improve indoor air quality; and build a stronger public health infrastructure. But as journalist Ed Yong highlights in a piece in The Atlantic, much more will have to be accomplished in order to protect the nation from the next pandemic, or natural disaster, or climate change impact. Most importantly, those efforts must include improving equity—in education, labor wages, food security, healthcare access, and other social factors—in order to buffer against the next crisis.
SOCIAL MEDIA & VACCINE MISINFORMATION YouTube on September 29 announced the video platform is expanding its medical misinformation policies, including new guidelines for any vaccine that is approved and confirmed to be safe and effective by local and global health authorities. Since last year, the Google-owned company has removed more than 130,000 videos for violating its COVID-19 vaccine policies, but the new guidelines extend beyond the current pandemic and apply to videos claiming proven vaccines are not effective; including misinformation about vaccines’ ingredients; or claiming that vaccines cause autism, cancer, or infertility, or that they contain tracking devices. YouTube also announced it is removing several channels associated with high-profile anti-vaccine proponents, including Joseph Mercola, Sherri Tenpenny, and Robert F. Kennedy Jr. There are exceptions to the rules, as YouTube will continue to allow content providing scientific discussions on vaccine policies, clinical trials, or historic vaccine successes and failures, as well as testimony about personal experiences with vaccines, as long as it doesn’t spill over into advocating against vaccines. The expanded guidelines mark a turning point for YouTube, which has shown some hesitancy against broadening its policing of content, and brings its policies more in line with other social media platforms, including Facebook and Twitter. While many of the so-called Disinformation Dozen continue to have active accounts across social media platforms, misinformation researchers hope YouTube’s policies will help staunch the flow of false vaccine information, as videos from the channel often lead to viral posts on Facebook and Twitter. Some researchers warn that anti-vaccine activists will simply move to other, newer platforms that have fewer restrictions, including Telegram or Gab.
ANTIVIRAL TREATMENT & PREVENTIVE TRIALS Pharmaceutical companies are pushing to develop more effective, easily administered therapeutics for COVID-19, some of which are being studied for the prevention of SARS-CoV-2 infection. This morning, Merck announced that its investigational oral antiviral molnupiravir, which is being developed with Ridgeback Biotherapeutics, significantly reduced the risk of hospitalization or death among non-hospitalized adult COVID-19 patients with mild-to-moderate symptoms who were considered high risk due to other health conditions such as obesity, diabetes, or heart disease. Among patients who took a 5-day course of the drug, 7.3% (28/385) were hospitalized or died compared with 14.1% (53/377) of patients who took a placebo, according to the interim analysis of the Phase 3 MOVe-OUT trial. Merck said it will file an application for Emergency Use Authorization (EUA) with the US FDA as soon as possible, as well as filing applications for marketing with regulatory agencies globally. Over the summer, the US government announced plans to purchase 1.7 million courses of molnupiravir from Merck for about US$1.2 billion, pending US FDA authorization or approval. If authorized, the drug would become the first oral medication available to treat COVID-19.
Pfizer announced on September 27 that it has begun a large Phase 2/3 clinical trial—named EPIC-PEP (Evaluation of Protease Inhibition for COVID-19 in Post-Exposure Prophylaxis)—to evaluate its investigational oral antiviral drug candidate PF-07321332, administered with a low-dose of the antiviral ritonavir, for the prevention of SARS-CoV-2 infection. The global trial is a randomized, double-blind, placebo-controlled study that intends to enroll up to 2,660 healthy adult participants who live in the same household as someone with confirmed, symptomatic COVID-19 disease. In a different study, Pfizer is testing the experimental antiviral among non-hospitalized, symptomatic adult COVID-19 patients.
Swiss pharmaceutical company Roche also is reportedly developing similar treatments for COVID-19. So far, the FDA has approved only Gilead’s antiviral Veklury (remdesivir) for the treatment of COVID-19 in hospitalized patients. However, the drug’s intravenous or injection administration presents challenges to widespread use, so the authorization or approval of an effective orally administered COVID-19 treatment or preventive could help to lower the burden of patients on hospitals.
WINTER OLYMPICS Less than 2 months from the end of the 2020 Summer Olympic Games—which took place a year late due to the COVID-19 pandemic—organizers are formulating pandemic countermeasures for the upcoming 2022 Olympic and Paralympic Winter Games, set to take place in February and March in Beijing. This week, the International Olympic Committee announced some spectators will be allowed to attend events, but only if they are from mainland China. Athletes and team members will not be required to be fully vaccinated to attend, but those who are not will be subject to a 21-day quarantine upon arrival in Beijing. Additionally, an Olympics bubble, or “closed-loop management system,” including required daily testing, will be established like it was in Tokyo in order to help improve safety. During this summer’s Games in Tokyo, at least 430 people tested positive for SARS-CoV-2, including athletes, officials, journalists, employees, contractors, and volunteers.
dryrunguy wrote: ↑Fri Oct 01, 2021 5:37 pm
SOCIAL MEDIA & VACCINE MISINFORMATION YouTube on September 29 announced the video platform is expanding its medical misinformation policies, including new guidelines for any vaccine that is approved and confirmed to be safe and effective by local and global health authorities. Since last year, the Google-owned company has removed more than 130,000 videos for violating its COVID-19 vaccine policies, but the new guidelines extend beyond the current pandemic and apply to videos claiming proven vaccines are not effective; including misinformation about vaccines’ ingredients; or claiming that vaccines cause autism, cancer, or infertility, or that they contain tracking devices. YouTube also announced it is removing several channels associated with high-profile anti-vaccine proponents, including Joseph Mercola, Sherri Tenpenny, and Robert F. Kennedy Jr. There are exceptions to the rules, as YouTube will continue to allow content providing scientific discussions on vaccine policies, clinical trials, or historic vaccine successes and failures, as well as testimony about personal experiences with vaccines, as long as it doesn’t spill over into advocating against vaccines. The expanded guidelines mark a turning point for YouTube, which has shown some hesitancy against broadening its policing of content, and brings its policies more in line with other social media platforms, including Facebook and Twitter. While many of the so-called Disinformation Dozen continue to have active accounts across social media platforms, misinformation researchers hope YouTube’s policies will help staunch the flow of false vaccine information, as videos from the channel often lead to viral posts on Facebook and Twitter. Some researchers warn that anti-vaccine activists will simply move to other, newer platforms that have fewer restrictions, including Telegram or Gab.
This would be a good time for Google, and the other giants, to come to terms with reality that an uncensored, completely open web is not healthy. Screening is needed, and not solely for Covid.
---0---
Home news. My mother's condition continues to fluctuate wildly, so I have decided to go to Hell-ezuela, on Sunday. My sister is beat, as she also came down with the disease for the second time. While anecdotical, I will repeat: they got one dose of Sputnik and, with my apologies to our Russian members, it seems it leaves a little bit to be desired. It cannot control symptoms.
I guess this will be the test for my Pf/Bntech vaccines. Needless to say, I will be exposed to the virus. Wonder what will work better: beer or rum? Both?
by JazzNU
ponchi101 wrote: ↑Fri Oct 01, 2021 10:18 pm
Home news. My mother's condition continues to fluctuate wildly, so I have decided to go to Hell-ezuela, on Sunday. My sister is beat, as she also came down with the disease for the second time. While anecdotical, I will repeat: they got one dose of Sputnik and, with my apologies to our Russian members, it seems it leaves a little bit to be desired. It cannot control symptoms.
I guess this will be the test for my Pf/Bntech vaccines. Needless to say, I will be exposed to the virus. Wonder what will work better: beer or rum? Both?
You're a good son. Sorry your mother's condition hasn't stabilized. Have a safe trip to Venezuela. Please consider wearing a mask most of the time despite being around your own family, the Delta variant is no joke, as contagious as chicken pox is how they started to describe it here to make it clearer how easy it is to catch now.
I'm not a beer drinker, so rum. If I was a beer drinker, most definitely the answer would be both.
by dmforever Your mother is lucky to have you as a son. As Jazz said, please be extra extra careful. I really hope your trip goes well for everyone involved.
dryrunguy wrote: ↑Fri Oct 01, 2021 5:37 pm
SOCIAL MEDIA & VACCINE MISINFORMATION YouTube on September 29 announced the video platform is expanding its medical misinformation policies, including new guidelines for any vaccine that is approved and confirmed to be safe and effective by local and global health authorities. Since last year, the Google-owned company has removed more than 130,000 videos for violating its COVID-19 vaccine policies, but the new guidelines extend beyond the current pandemic and apply to videos claiming proven vaccines are not effective; including misinformation about vaccines’ ingredients; or claiming that vaccines cause autism, cancer, or infertility, or that they contain tracking devices. YouTube also announced it is removing several channels associated with high-profile anti-vaccine proponents, including Joseph Mercola, Sherri Tenpenny, and Robert F. Kennedy Jr. There are exceptions to the rules, as YouTube will continue to allow content providing scientific discussions on vaccine policies, clinical trials, or historic vaccine successes and failures, as well as testimony about personal experiences with vaccines, as long as it doesn’t spill over into advocating against vaccines. The expanded guidelines mark a turning point for YouTube, which has shown some hesitancy against broadening its policing of content, and brings its policies more in line with other social media platforms, including Facebook and Twitter. While many of the so-called Disinformation Dozen continue to have active accounts across social media platforms, misinformation researchers hope YouTube’s policies will help staunch the flow of false vaccine information, as videos from the channel often lead to viral posts on Facebook and Twitter. Some researchers warn that anti-vaccine activists will simply move to other, newer platforms that have fewer restrictions, including Telegram or Gab.
This would be a good time for Google, and the other giants, to come to terms with reality that an uncensored, completely open web is not healthy. Screening is needed, and not solely for Covid.
---0---
Home news. My mother's condition continues to fluctuate wildly, so I have decided to go to Hell-ezuela, on Sunday. My sister is beat, as she also came down with the disease for the second time. While anecdotical, I will repeat: they got one dose of Sputnik and, with my apologies to our Russian members, it seems it leaves a little bit to be desired. It cannot control symptoms.
I guess this will be the test for my Pf/Bntech vaccines. Needless to say, I will be exposed to the virus. Wonder what will work better: beer or rum? Both?
Oh ponchi. I had hoped it wouldn't come to this for you. Be safe.
by ti-amie'Aladdin' on Broadway Canceled for Two Weeks Following Additional Breakthrough COVID Cases
October 01, 2021
Just a day after resuming performances following breakthrough COVID cases in its company, Disney Theatrical announced that Aladdin will once again shut down this time for two weeks.
Following negative PCR testing ahead of Thursday’s performance that allowed the show to resume, additional breakthrough COVID-19 cases within the company on Friday were detected. As result, the production will shut down for two weeks beginning today, with performances slated to resume on Tuesday, Oct. 12th at 7 p.m.
“Given my evaluation of this real-world data, I believe these positive cases are most likely related to an exposure from one positive case. This 12-day pause allows the Aladdin company ample time to ensure that people with breakthroughs recover, and any other potential breakthroughs are identified before the Aladdin company gathers again,” Blythe Adamson, the epidemiologist working with Disney Theatrical Productions, said in a statement.
“Daily PCR testing allows us the opportunity to detect a positive case before it is contagious,” she continued. “This allows us to isolate it before anyone else is put at risk, as we have done several times with the Aladdin company. Morning and evening swabs collected on Thursday returned highly accurate negative molecular PCR test results for all cast, crew and musicians that affirmed a safe performance environment for our company and audience.”
Tickets for all dates will be refunded. The news follows an earlier decision today by the Broadway League to extend its existing COVID protocols and requirements, agreed upon by all 41 Broadway venues, with no reductions in the vaccine or mask mandates for audiences, performers, backstage crew and theater staff through the end of the year.
Aladdin’s initial shutdown marked the first canceled show since Broadway’s official reopening on Sept. 14, with the Disney Theatrical show also the first production to announce breakthrough COVID cases within its company. The production’s Wednesday performance was canceled due to these initial breakthrough cases.
dryrunguy wrote: ↑Fri Oct 01, 2021 5:37 pm
SOCIAL MEDIA & VACCINE MISINFORMATION YouTube on September 29 announced the video platform is expanding its medical misinformation policies, including new guidelines for any vaccine that is approved and confirmed to be safe and effective by local and global health authorities.
This would be a good time for Google, and the other giants, to come to terms with reality that an uncensored, completely open web is not healthy. Screening is needed, and not solely for Covid.
I said when the internet was first introduced into the mainstream that it would cause a lot of damage - based simply on the reality that the human animal will abuse absolutely everything it comes into contact with. Human beings in general cannot handle absolute freedom without turning it into a negative - they require strict limits being imposed. Sad, but proven true many, many times throughout history.
I met a guy this spring through pickleball - we got along well, drove to pickleball together, etc. Until the discussion about the COVID-19 vaccines, which is when I discovered that he doesn't believe in them, and will not get them. This led me to deciding to no longer ride in the same car as him. Then, a little later, he was excluded from playing in our pickleball club (even outside) because we had to show proof of COVID-19 vaccination.
Because he and I got along before this, I called him. We talked for an hour or so. I learned that he's been to several anti COVID measures protests (where he "hugged people all over the place, and never got sick" - his words). He said he believes that COVID-19 exists, but that it is no worse than the 'flu. And the COVID vaccines "have killed many people", etc.... the usual nonsense.
Toward the end of our phone talk, I said "So you think it's a big conspiracy, then?" He said "Yes - absolutely."
I said "And what is the reason that so many people are conspiring to sell everyone on the planet on this COVID-19 thing?" I expected him to have one or more wacky 'theories' about what the reason for the conspiracy is. But instead, he said "I don't know what the reason is - I'm working on that."
Huh?
You believe it's a big conspiracy - but you have no idea why? Shouldn't you figure out what the reason is BEFORE you BELIEVE that there is a conspiracy about something?!?!
I cannot fathom that it is possible to get so many people in on a conspiracy of this magnitude - it's world-wide... the huge majority of medical professionals, the huge majority of media personnel, the huge majority of politicians - world-wide - would have to be in on the conspiracy, and all of them would have to keep it all completely secret. This is absolutely impossible for human beings to achieve.
But, hey - don't let the facts get in the way of a good story, huh?
The problem with ignoring the facts in favour of illusion and fantasy, though, is that this time, people's lives are on the line...
by ti-amie I just finished a novel that looked at this phenomenon. It was based on the book "Extraordinary Popular Delusions and the Madness of Crowds" by Charles Mackay. It's not a recent book but it's becoming popular again.
by Jeff from TX Ponchi,
Best wishes on your trip. Be careful and safe, my friend, and may both your mother and sister make complete recoveries.
by ti-amie
by JazzNU
New Zealand admits it can no longer get rid of coronavirus
By NICK PERRY
WELLINGTON, New Zealand (AP) — New Zealand’s government acknowledged Monday what most other countries did long ago: It can no longer completely get rid of the coronavirus.
Prime Minister Jacinda Ardern announced a cautious plan to ease lockdown restrictions in Auckland, despite an outbreak there that continues to simmer.
Since early in the pandemic, New Zealand had pursued an unusual zero-tolerance approach to the virus through strict lockdowns and aggressive contact tracing.
Until recently, that elimination strategy had worked remarkably well for the country of 5 million, which has reported just 27 virus deaths.
While other nations faced rising death tolls and disrupted lives, New Zealanders went back to workplaces, school yards and sports stadiums safe from any community spread.
But that all changed when the more contagious delta variant somehow escaped from a quarantine facility in August after it was brought into the country from a traveler returning from Australia.
Despite New Zealand going into the strictest form of lockdown after just a single local case was detected, it ultimately wasn’t enough to crush the outbreak entirely.
One factor may have been that the disease spread among some groups that are typically more wary of authorities, including gang members and homeless people living in transitional housing.
The outbreak has grown to more than 1,300 cases, with 29 more detected on Monday. A few cases have been found outside of Auckland.
Ardern said that seven weeks of lockdown restrictions in Auckland had helped keep the outbreak under control.
“For this outbreak, it’s clear that long periods of heavy restrictions has not got us to zero cases,” Ardern said. “But that is OK. Elimination was important because we didn’t have vaccines. Now we do, so we can begin to change the way we do things.”
New Zealand began its vaccination campaign slowly compared to most other developed nations. Rates rocketed in August after the outbreak began but have dropped off significantly again since then.
About 65% of New Zealanders have had at least one dose and 40% are fully vaccinated. Among people age 12 and older, about 79% have had at least a single jab.
Under Ardern’s plan that starts Tuesday, Aucklanders will be able to meet outdoors with loved ones from one other household, early childhood centers will reopen and people will be able to relax at the beach.
The dates for a phased reopening of retail stores and later bars and restaurants have yet to be decided.
Ardern said the elimination strategy had served the country incredibly well but the government always intended to eventually transition to the protection of vaccines, a change hastened by the delta variant “game changer.”
The government’s elimination approach had been broadly supported by New Zealanders but was facing increasing criticism. Over the weekend, hundreds of people turned out to rallies protesting the lockdown.
Opposition lawmaker Chris Bishop said the government had no clear strategy to deal with the outbreak other than total surrender.
But Ardern said that most measures would remain in place to keep the outbreak under control, including exhaustive contact tracing and isolating those who got infected.
“There’s good cause for us to feel optimistic about the future,” Ardern said. “But we cannot rush.”
by ponchi101 At home (Caracas branch).
Well, upon arrival I found my mom in bed but stable. My sister also has it, and so does my nephew, a 17 yo that is completely asymptomatic. Talking to my sister, she admitted that on Friday she thought we would lose mom; she was that drained and weak. Fortunately, some remdecivir and other medication did the trick.
The problem is that they are both so weak they can barely do anything, so I am needed here for household chores. Cooking, cleaning, etc. Plus, being vennieland, anything becomes herculean. We live in a six floor apartment, but the elevator is broken, so getting groceries was impossible for them. I did so yesterday and getting them up to the apartment meant 4 trips. I will get my legs back before I return to Colombia.
I will start writing a small logbook about this. It is my country but this is no longer recognizable. Thanks to all for you good wishes
by Suliso I really hope it all works out for you. Everyone recovers and you get back to Colombia safely.
by dryrunguy Here's the latest Situation Report. Well done, Portugal.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 235 million cumulative cases and 4.80 million deaths worldwide as of October 4. Global weekly incidence and mortality continue to decline, for the fourth consecutive week. Weekly incidence decreased by 9% from the previous week, and mortality fell by 4%. All WHO regions are exhibiting steady declines over the past 3-11 weeks, with the exception of Europe, which has held relatively steady at approximately 1.1 million new cases per week since mid-July.
The WHO dashboard indicates that October 4 reporting is delayed for a number of countries in the Region of the Americas.
Global Vaccination
The WHO reported 6.19 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of October 3. A total of 3.53 billion individuals have received at least 1 dose, and 2.58 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline steadily, down from the most recent high of 42 million doses per day on August 30 to 27 million on October 3—decreasing by more than one-third over that period*. The global trend continues to closely follow the trend in Asia. Our World in Data estimates that there are 3.61 billion vaccinated individuals worldwide (1+ dose; 45.8% of the global population) and 2.69 billion who are fully vaccinated (34.2% of the global population). Oceania’s full vaccination coverage (34.20%) surpassed the global average (34.19%), which leaves Africa (4.4%) as the only continent below the global average. Oceania and Africa were reporting similar full vaccination coverage as recently as late May, but vaccination efforts in Oceania have progressed rapidly over the past several months.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 43.6 million cumulative COVID-19 cases and 700,176 deaths. Daily incidence continues to decline, down to approximately 103,000 new cases per day, which is the lowest average since early August. Daily mortality appears to have passed a peak and started to decline; however, the trend has not been consistent. The average daily mortality declined from a peak of 1,744 deaths per day on September 15 to 1,460 on September 28 before jumping back up to nearly 1,500 on September 29. The US reported 2,025 deaths on September 29, the third-highest single-day total since mid-to-late February*.
The US surpassed 700,00 cumulative deaths on October 3:
1 death to 100,000: 110 days**
100k to 200k: 109 days
200k to 300k: 89 days
300k to 400k: 33 days
400k to 500k: 33 days
500k to 600k: 122 days
600k to 700k: 112 days
With 87 days still remaining in 2021, the US could surpass 750,000 cumulative deaths by the end of the year. The US reported 371,911 total deaths in 2020, which would make 2021 even more deadly than the first year of the pandemic, despite the availability of multiple highly effective vaccines.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over the weekend or for states that are reporting mortality by date of death. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
**The CDC reports 247 cumulative deaths on February 3, 2020, the first date with available mortality data.
US Vaccination
The US has administered 397 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend increased over the past several days, up from fewer than 600,000 doses per day on September 23 to more than 750,000 on September 29—a 25% increase over that period. Even with expected delays in reporting, it appears that the average is poised to continue increasing. The averages for September 30 and October 1 are already more than 784,000 and 777,000, respectively, despite being within the 5-day window during which we expect reporting delays*. The timing of this increase corresponds to the FDA authorization and CDC recommendations regarding third doses of the Pfizer-BioNTech vaccine for many adults.
There are 215.5 million individuals in the US who have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 64.9% of the entire US population. Among adults, 77.7% have received at least 1 dose, as well as 14.7 million adolescents aged 12-17 years. A total of 185.8 million individuals are fully vaccinated, which corresponds to 56.0% of the total population. Approximately 67.3% of adults are fully vaccinated, as well as 12.0 million adolescents aged 12-17 years. A total of 5.7 million “booster” doses (ie, third doses of the Pfizer-BioNTech or Moderna vaccine) have been administered nationwide**. Adults aged 50 years and older have received 4.8 million “booster” doses, including 3.7 million among adults aged 65 years and older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**The second dose of the Pfizer-BioNTech, Moderna, AstraZeneca-Oxford, and other 2-dose vaccines is technically a booster dose as well (ie, part of a prime-boost regimen), but here, we are specifically addressing additional “booster” doses administered beyond the original full vaccination regimen.
J&J-JANSSEN BOOSTER DOSE Johnson & Johnson (J&J) today announced it has submitted data to the US FDA for an Emergency Use Authorization (EUA) amendment to allow for a booster dose for its SARS-CoV-2 vaccine, developed in collaboration with Janssen Pharmaceuticals. In a press release, J&J reported that Phase 3 clinical trial data indicate that a booster dose administered 56 days after the first dose provided 94% protection against moderate-to-severe COVID-19 and 100% protection against severe disease. The booster dose request follows a previous report that hundreds of thousands of J&J-Janssen vaccine doses in the US will soon expire. The federal government shipped 22 million doses to states in need, but only 15 million were administered. Several independent experts expressed concern at a meeting of the CDC’s Advisory Committee on Immunization Practices (ACIP) in September that J&J-Janssen vaccine recipients were being left behind in discussions over booster doses, as the focus has been on the Pfizer-BioNTech and Moderna mRNA vaccines. J&J-Janssen now joins Pfizer-BioNTech and Moderna as the third vaccine provider to request an EUA for a booster dose. The FDA’s Vaccine and Related Biological Products Advisory Committee (VRBPAC) is scheduled to discuss the possible EUA amendments, as well as vaccines for younger children, on October 15.
EU BOOSTER/ADDITIONAL DOSES The European Medicines Agency (EMA) on October 4 issued recommendations for third doses of the SARS-CoV-2 vaccines from Pfizer-BioNTech (Comirnaty) and Moderna (Spikevax). The EMA’s Committee for Medicinal Products for Human Use (CHMP) differentiated between additional doses—which they recommended for people with severely compromised immune systems who had received either vaccine, given at least 28 days from the second dose—and booster doses—which can now be considered for people aged 18 years and older who received the Pfizer-BioNTech vaccine at least 6 months after their second dose. The committee said it will continue to evaluate data on booster doses of Moderna’s vaccine. Specific recommendations on booster doses will be left up to national-level public health bodies, the CHMP noted. Some EU countries—including France and Germany—already are administering additional doses to people with immunocompromising conditions, whereas few EU countries—such as Hungary—are offering booster doses to all adults. The regulator also warned of the risk of inflammatory heart conditions and other “very rare” side effects following a third dose of vaccine, noting they will continue to collect and examine safety and effectiveness data.
On the same day, the WHO updated its interim statement on booster doses, outlining the differences between booster and additional doses, as well as factors to be considered in the administration of booster doses. The statement underscores WHO’s position that the introduction of booster doses “should be rigorously evidence driven” and limited to populations in greatest need. The WHO continues to discourage broad-based booster dose administration, as it risks worsening global inequities in vaccine access.
US VACCINE MANDATES Vaccine mandates continue to take effect across the US for numerous populations, and could be part of the reason for an increase in daily vaccinations over the past several days. New York City’s requirement that public school employees be vaccinated began October 4, with Mayor Bill de Blasio announcing 95% of full-time Department of Education employees are at least partially vaccinated. US Supreme Court Justice Sonia Sotomayor on October 1 denied a request for an emergency injunction of the policy made by 4 teachers and teaching assistants who claim the city's policy violates their constitutional rights. The decision by Justice Sotomayor, who offered no explanation, echoes one made by Supreme Court Justice Amy Coney Barrett in August when she turned down a request to block Indiana University’s vaccine mandate for students. With about 1,000 colleges and universities nationwide requiring vaccinations for students and staff, some students have decided to withdraw from school rather than get vaccinated, even as other cases are pending.
On October 1, California became the first US state to require SARS-CoV-2 vaccination for all eligible public and private schoolchildren, similar to inoculations for other diseases. Governor Gavin Newsom announced the mandate will take effect during the first school term following the US FDA’s full approval of a vaccine for children aged 12 and older—possibly as soon as January 2022—with vaccinations for younger children to be phased in after approval for their age group. Notably, because the requirement is being implemented through a regulatory process, the rule allows for exemptions due to personal, medical, and religious beliefs; however, the state legislature and governor could later approve a law to eliminate the personal-belief exemption, and individual school districts are able to implement their own vaccine mandates sooner than statewide requirements.
The White House is pushing more US airlines to require vaccination for their employees. Many large US airlines hold federal contracts and therefore are required to vaccinate their employees under rules implemented last month under executive order. American Airlines, JetBlue Airways, and Alaska Airlines all announced last week that they would implement vaccine mandates as early as December 8, the deadline for federal contractors to be vaccinated. United Airlines, one of the first large US companies to announce strict vaccine requirements for its employees, said only about 300 of the airline’s 67,000 US-based staff have not yet complied with the rule and about 2,000 have applied for exemptions. Workers in other industries—including healthcare workers, firefighters, and other first responders—are being fired or suspended for missing vaccine mandate deadlines or are seeking exemptions. Meanwhile, the chronically understaffed US Occupational and Safety Administration (OSHA) is preparing to enforce federal mandates for about 8 million worksites nationwide with only 1,850 federal and state inspectors. Nevertheless, it appears vaccine mandates are convincing more people to get the shots.
COVAX The COVAX facility—with its goal of equitable global vaccine acquisition, allocation, and distribution—this month will for the first time send SARS-CoV-2 vaccines only to countries with the least amount of coverage. The policy represents a shift in dose allocation, as COVAX previously distributed doses proportionally to countries based on population size, not need. According to Our World in Data, only 2.3% of people in low-income countries have received at least one dose of SARS-CoV-2 vaccine, placing the global goal of 40% vaccination coverage far out of reach. Under the new plan, about 75 million doses of the Pfizer-BioNTech, AstraZeneca-Oxford, Moderna, J&J-Janssen, and Sinopharm vaccines will be distributed to 49 countries most in need this month.
While many experts welcomed the policy shift, some argued that the strategy should have been adopted at COVAX’s launch. Despite the WHO’s call for a moratorium on booster shots to ensure equitable global vaccine access, the US and several other countries have begun administering additional doses. Vaccine manufacturers maintain that there are enough shots for everyone, with about 1.5 billion doses being produced each month. The concern now, they say, is that many doses in wealthy nations are sitting unused rather than being redistributed to countries in need.
TRAVEL REQUIREMENTS COVID-19-related travel restrictions and requirements are becoming increasingly confusing worldwide, with each nation implementing various rules pertaining to whether travelers need to be vaccinated, are required to quarantine, or can even enter a country. England’s new guidance came into force on October 4, replacing its previous “traffic light” system with a single “red list” of countries, from which only British or Irish nationals or those with UK residency will be permitted to enter. While the most recent iteration of the rules eliminates pre-travel testing for vaccinated individuals arriving from non-red list countries, a maze of requirements—including pre-departure and post-arrival testing, mandatory quarantining, and completing a locator form—remains, largely determined by a traveler’s vaccination status. Reportedly, the red list of countries is expected to be trimmed from 54 to 9 later this week. The travel guidance continues to not recognize the Indian version of the AstraZeneca/Oxford SARS-CoV-2 vaccine, known as Covishield, and India on October 1 implemented reciprocal restrictions on all British travelers, including pre-departure and post-arrival testing and quarantines.
Beginning November 1, New Zealand will allow only fully vaccinated individuals aged 17 years and older to enter the country from abroad, although travelers will still be required to show a negative pre-departure test result and quarantine for 14 days upon arrival. Beginning in February 2022, Air New Zealand, the nation’s flagship airline, will require all passengers on international flights to be vaccinated, with few exceptions. Australian Prime Minister Scott Morrison announced last week that Australia will allow international travel for fully vaccinated citizens and permanent residents beginning in November, with a required 7 day quarantine upon entry. The Australian government continues to work on plans to allow foreign nationals to visit. The borders of both New Zealand and Australia have been closed since March 2020, and both nations recently have experienced an increase in COVID-19 cases. Japan and Argentina also recently announced changes to their travel rules.
US HEALTHCARE SYSTEM STRAIN Healthcare workers in the US have been battling COVID-19 for over 18 months and continue to experience the crippling impacts of chronic stress, fatigue, and burnout, which in some cases is impacting patient care. A recent influx of COVID-19 patients in several regions has strained healthcare facilities and forced some to implement crisis standards of care. At the beginning of October, 20 out of 31 healthcare facilities in Alaska activated emergency crisis protocols that allow them to ration care in order to cope with the burden of COVID-19 cases. Several factors—including a lack of supplies, resources, bed space, and a shortage of healthcare workers—led the state to implement the protocols, leaving decisions about prioritizing treatment up to doctors. The situation led Alaska Governor Mike Dunleavy to request additional healthcare worker support from the US government at the end of September.
Similarly, intensive care units (ICUs) in New England are filling amid a shortage in healthcare workers and an increase in COVID-19 cases due to the Delta variant, largely among unvaccinated populations. Despite having some of the highest vaccination coverage rates in the US, public health officials continue to plead with the thousands of people who remain unvaccinated and vulnerable to SARS-CoV-2 infection. Notably, some hospital systems in the region are seeing almost 20 times the number of COVID-19 patients than during June 2020 and have no open ICU beds.
MULTICOMPONENT PREVENTIVE STRATEGIES Youth camps in the US that use multicomponent COVID-19 preventive strategies—including high vaccination rates among staff and campers, pre-arrival and frequent onsite testing, podding, masking, physical distancing, focusing on hand hygiene, and wastewater surveillance—provide a safer environment for attendees and counselors, according to 2 studies published last week in the US CDC’s Mortality and Morbidity Weekly Report (MMWR). One study reported on 9 US overnight camps across the country that occurred during June through August 2021 and implemented multiple prevention strategies, including having a vaccination rate over 93% among eligible persons aged 12 years or older. Among 7,173 staff members and campers from 50 states, 13 countries, and US military overseas bases who took tens of thousands of rapid antigen and RT-PCR tests over the 2021 season, 9 COVID-19 cases were detected at 4 camps, and no secondary transmission was detected.
Another study examined COVID-19 outbreaks at 14 overnight and 14 day camps in Louisiana during June and July 2021, as the Delta variant became predominant. During the study period, 321 camp-associated cases were identified, an increase over the number of cases observed in Louisiana camps the previous year. The researchers note the study period also coincided with an “apparent underutilization” of preventive measures such as vaccination, masking, and physical distancing. Together, the studies provide support for the CDC’s guidance that eligible children be vaccinated and highlight the importance of simultaneously using multicomponent strategies to reduce the risk of and prevent SARS-CoV-2 transmission at camps and other youth-focused settings such as schools.
NEW ZEALAND New Zealand announced an end to its zero tolerance approach to COVID-19 and acknowledged that it will need to start a phased reopening through lessening restrictions and increasing vaccination rates. The restrictions in Auckland, which have been in effect for 7 weeks, will gradually ease in 3 stages. The first stage, alert level 3, will allow people to gather outdoors with members from no more than 2 households and 10 individuals. Early childhood education centers will reopen and people will be able to take part in certain outdoor recreational activities. The second stage, alert level 2, will allow the reopening of retail stores, pools, and zoos—with certain preventive measures—and the number of individuals who can meet outdoors will increase to 25. The third and final stage, alert level 1, will allow for the opening of restaurants and hairdressers with some public health interventions and limits on seating, and the number of individuals who can meet outdoors will increase to 50.
The zero tolerance approach to COVID-19 worked well for New Zealand until recently, when the Delta variant proved impossible to eliminate despite intensive lockdowns. New Zealanders were able to live restriction-free for the majority of the pandemic and the government’s strategy was viewed in a highlighly favorable light. But recently, public opinion began to shift when thousands of people protested the restrictive public health measures. Prime Minister Jacinda Ardern stated that strict lockdown measures will be eased once the nation reaches full vaccination for 90% of the eligible population. According to the Ministry of Health, 79% of the eligible population has received at least one dose, but efforts to fully vaccinate the population could take months due to difficulties convincing the remaining 20% to get the shots.
PORTUGAL More than 85% of Portugal’s total population is fully vaccinated against SARS-CoV-2, among the world’s leaders in vaccinations. In fact, about 98% of those eligible for vaccines—those aged 12 and older—are fully vaccinated, and the country has experienced a sharp decline in the number of new COVID-19 cases since the end of August. The number of COVID-19-related deaths are down too, although there has been a slight increase in the 7-day average since the beginning of October.* The government this week lifted most COVID-19 restrictions. However, some health officials are concerned a winter surge in cases is possible, including more hospitalizations, as many people—and especially the elderly—received their vaccinations more than 6 months ago. Several studies, including one conducted in Portugal, provide evidence that a drop in vaccine effectiveness is possible over time, particularly in older populations. The country may soon begin administering third vaccine doses to older people and those with compromised immune systems, with a goal of reaching 100% of them by the end of the year.
Many credit the country’s success to the leadership of Vice Admiral Henrique Gouveia e Melo, a former submarine squadron commander who led a nationwide vaccination campaign that faced many of the same misinformation and hesitancy challenges as other countries. Admiral Gouveia e Melo credited the campaign’s success to consistent and trustworthy communication from elite military personnel, who were distanced from politics, and the use of military-style language that rallied the nation onto a war footing. As the country returns to a sense of normalcy, the remainder of the world will be eagerly watching.
*Due to delays in reporting, estimates for the average daily deaths likely are less accurate for the most recent 5 days.
NEXT-GENERATION MASKS Masks and respirators have played an essential role in the global COVID-19 response; however, the ubiquitous disposable medical/surgical masks and N95 respirators used by healthcare workers have not appreciably improved since the mid-1990s, and the non-medical masks in wide public use during the pandemic are not governed by associated quality or design standards. The Johns Hopkins Center for Health Security published a report outlining recommendations for the US government regarding improvements to mask quality and supply and developing a sustainable market for these products. The approach outlined in the report touches on the development, manufacturing, and stockpiling of masks and respirators for healthcare workers, the non-healthcare workforce, and the broader US public. The report, Masks and Respirators for the 21st Century: Policy Changes Needed to Save Lives and Prevent Societal Disruption, describes a confluence of factors that are hindering the mask market, including industrial inertia, lack of competition, complacent consumers, regulatory barriers, supply chain limitations, an uncertain market, and the absence of US government policy.
The report calls for efforts to improve the design and quality of masks and respirators, including their degree of protection, fit and wearability, and durability and reusability. The report also focuses on the importance of developing a robust supply chain that could mitigate the need for and limitations of stockpiling and provide reliable supply capacity during emergencies. The authors also list specific actions for the US government, including expanding the use of reusable products (eg, elastomer-based respirators), updating federal procurement and stockpiling systems, funding the development of improved products and manufacturing capacity (eg, through BARDA), and encouraging the routine use of masks for other respiratory diseases (eg, seasonal influenza).
PORTUGAL More than 85% of Portugal’s total population is fully vaccinated against SARS-CoV-2, among the world’s leaders in vaccinations. In fact, about 98% of those eligible for vaccines—those aged 12 and older—are fully vaccinated, and the country has experienced a sharp decline in the number of new COVID-19 cases since the end of August. The number of COVID-19-related deaths are down too, although there has been a slight increase in the 7-day average since the beginning of October.* The government this week lifted most COVID-19 restrictions. However, some health officials are concerned a winter surge in cases is possible, including more hospitalizations, as many people—and especially the elderly—received their vaccinations more than 6 months ago. Several studies, including one conducted in Portugal, provide evidence that a drop in vaccine effectiveness is possible over time, particularly in older populations. The country may soon begin administering third vaccine doses to older people and those with compromised immune systems, with a goal of reaching 100% of them by the end of the year.
Many credit the country’s success to the leadership of Vice Admiral Henrique Gouveia e Melo, a former submarine squadron commander who led a nationwide vaccination campaign that faced many of the same misinformation and hesitancy challenges as other countries. Admiral Gouveia e Melo credited the campaign’s success to consistent and trustworthy communication from elite military personnel, who were distanced from politics, and the use of military-style language that rallied the nation onto a war footing. As the country returns to a sense of normalcy, the remainder of the world will be eagerly watching.
*Due to delays in reporting, estimates for the average daily deaths likely are less accurate for the most recent 5 days.
This is what a country can do with strong leadership and determination. Meanwhile this happened in NYC yesterday.
by JazzNU I went to get a flu shot yesterday and decided to go to the county site because I could go with an appointment and not just rely on walk-in and hope for no wait. They combined it this year with the covid vaccine and testing site. When I walked in I was wondering why there was a large police SUV sitting on the curb at the entrance. Not wondering so much anymore. Didn't know people were acting like new fools at covid testing sites too.
by JazzNU
ponchi101 wrote: ↑Tue Oct 05, 2021 2:41 pm
At home (Caracas branch).
Well, upon arrival I found my mom in bed but stable. My sister also has it, and so does my nephew, a 17 yo that is completely asymptomatic. Talking to my sister, she admitted that on Friday she thought we would lose mom; she was that drained and weak. Fortunately, some remdecivir and other medication did the trick.
The problem is that they are both so weak they can barely do anything, so I am needed here for household chores. Cooking, cleaning, etc. Plus, being vennieland, anything becomes herculean. We live in a six floor apartment, but the elevator is broken, so getting groceries was impossible for them. I did so yesterday and getting them up to the apartment meant 4 trips. I will get my legs back before I return to Colombia.
I will start writing a small logbook about this. It is my country but this is no longer recognizable. Thanks to all for you good wishes
So glad you reached Caracas safely. Great to hear your mom is stable. And wonderful that you are able to help out your mom, sister, and nephew right now. And thank god you're able bodied, huh? Your description reminds me of a NYC walkup and my first thought is always about groceries.
Now, I read up on this and if your mom had covid pneumonia (not sure she did, but I know they were concerned about her oxygen levels and she was given the same drug as my aunt), know that her recovery is likely to take a bit of time. Three to six weeks is common for those that have been hospitalized with covid pneumonia. I'd assume that your mom would have a shortened timetable for recovery, but can't be sure. Weakness is very common and regaining strength afterwards can take weeks to months before you bounce back enough to feel like yourself again. I was trying to calm my fears and set some realistic expectations for when we might see some improvements in my aunt's condition so I did some research on covid pneumonia. There is great potential to freak the f out with all of this in my opinion.
Now on the bright side, try to stay positive. My aunt had a doctor's appointment yesterday and the doctor has seen enough improvement with her lung function to begin weaning her off the oxygen. Your mom's condition was never as bad as my aunt, and my aunt's overall health was worse than your mom's to start (she was already handicapped from a massive stroke some years ago). Of course every case isn't comparable, but there is every reason to think positively about your mom's recovery, it's just going to take some time.
by ti-amie It never stops.
by Deuce Among all of the disturbing things associated with the COVID-19 virus - and there has been a ton of disturbing news related to it - this is among the worst I've seen.
A little kid, probably feeling good - if somewhat fearful - about helping others...
It just breaks your heart.
It's also yet another reminder that this virus has no mercy...
Deuce wrote: ↑Wed Oct 06, 2021 1:52 am
Among all of the disturbing things associated with the COVID-19 virus - and there has been a ton of disturbing news related to it - this is among the worst I've seen.
A little kid, probably feeling good - if somewhat fearful - about helping others...
It just breaks your heart.
It's also yet another reminder that this virus has no mercy...
So glad you reached Caracas safely. Great to hear your mom is stable. And wonderful that you are able to help out your mom, sister, and nephew right now. And thank god you're able bodied, huh? Your description reminds me of a NYC walkup and my first thought is always about groceries.
Now, I read up on this and if your mom had covid pneumonia (not sure she did, but I know they were concerned about her oxygen levels and she was given the same drug as my aunt), know that her recovery is likely to take a bit of time. Three to six weeks is common for those that have been hospitalized with covid pneumonia. I'd assume that your mom would have a shortened timetable for recovery, but can't be sure. Weakness is very common and regaining strength afterwards can take weeks to months before you bounce back enough to feel like yourself again. I was trying to calm my fears and set some realistic expectations for when we might see some improvements in my aunt's condition so I did some research on covid pneumonia. There is great potential to freak the f out with all of this in my opinion.
Now on the bright side, try to stay positive. My aunt had a doctor's appointment yesterday and the doctor has seen enough improvement with her lung function to begin weaning her off the oxygen. Your mom's condition was never as bad as my aunt, and my aunt's overall health was worse than your mom's to start (she was already handicapped from a massive stroke some years ago). Of course every case isn't comparable, but there is every reason to think positively about your mom's recovery, it's just going to take some time.
You are ahead of me, and indeed I will try to keep that in mind. We don't think mom got pneumonia and lucky for us, she was never a smoker or any related issues. But, as you say, I don't see myself leaving here before November. It would make no sense.
On another level, I sound this sound cheesy but the fact I am here helps her with her mood. A little TLC helps a lot
by JazzNU
ponchi101 wrote: ↑Wed Oct 06, 2021 2:19 am
On another level, I sound this sound cheesy but the fact I am here helps her with her mood. A little TLC helps a lot
Not cheesy at all. I'm sure she's missed you and is happy your home even if the reason you had to come isn't a good one. A positive attitude makes a difference in recovery and healing. So TLC helps a ton. It'll surely help your sister too, who had to be particularly stressed trying to get better herself and take care of your mom at the same time.
Deuce wrote: ↑Wed Oct 06, 2021 1:52 am
Among all of the disturbing things associated with the COVID-19 virus - and there has been a ton of disturbing news related to it - this is among the worst I've seen.
A little kid, probably feeling good - if somewhat fearful - about helping others...
It just breaks your heart.
It's also yet another reminder that this virus has no mercy...
I don't think this issue is that black and white...
I'm assuming that the teacher meant no harm - and meant only good. Children have been the members of society who've been least affected by COVID-19... The teacher may have simply felt that, because of this, it was safe to have a child accompany sick children to the school nurse - and at the same time, the exercize is good emotionally and morally for both children - it shows the accompanying child the positivity of responsibility and compassion, and it shows the accompanied child that people care.
Of course, the middle of a pandemic is not the best time to teach these valuable lessons in this particular manner - especially since the children are not old enough to be vaccinated. But, again - children have been the ones least affected by the virus.
I assume the teacher feels absolutely terrible. People who become teachers are typically good and caring people (who, sadly, often become bitter and cynical after working within the dysfunctional, unhealthy system for a while).
Rather than trying to lay blame, I see this as a tragically unfortunate situation where everyone involved was profoundly harmed.
by ti-amie I'm normally on the side advocating for more respect and more money for teachers. I still think that in this case the teacher showed poor judgement. Yes the child was being given life lessons BUT there is growing evidence that children can and are becoming just as if not more sick with this thing as adults. Many districts have gone back to remote learning because the outbreaks among children are so high.
As a parent I would be very upset.
by JazzNU The French approach. I approve. This is LA City not LA County.
by dryrunguy Since my company is a federal government contractor, all of our employees will have to be vaccinated, including my boss who still staunchly refuses. The email went out yesterday. I am guessing it also applies to our part-time staff, such as our inspectors and minors who participate in tobacco retailer inspection teams. Which reminds me... I have some news to share. Off to the Work/Job thread...
by JazzNU
dryrunguy wrote: ↑Wed Oct 06, 2021 10:52 pm
Since my company is a federal government contractor, all of our employees will have to be vaccinated, including my boss who still staunchly refuses. The email went out yesterday. I am guessing it also applies to our part-time staff, such as our inspectors and minors who participate in tobacco retailer inspection teams. Which reminds me... I have some news to share. Off to the Work/Job thread...
Obviously I saw the work post before I saw this. Yes, it applies to part time staff too. I was talking to a friend that works for a federal contractor and they did a great job of broadly defining it. Religious and medical exemptions allowed, but no testing opt out and working remotely doesn't exempt you. If you work for a federal contractor or on a federal contract, the mandate applies. Even applies to indirectly working with a contract, like support services.
by Deuce
JazzNU wrote: ↑Wed Oct 06, 2021 9:02 pm
The French approach. I approve. This is LA City not LA County.
This is also happening in most parts of Canada (by provincial mandate, not municipal or federal).
by dryrunguy Amie has posted him before. But this is pretty much gold.
by dryrunguy Here's the latest Situation Report. I didn't know things could get even worse in Syria. Then again, it's highly probable that Syria has no infrastructure for COVID testing and treatment.
In any case, as usual, there's a lot here.
::
UPDATE: Starting next week, the COVID-19 Situation Report will be delivered to your inbox on Tuesdays and Thursdays. We will no longer include detailed epidemiological analysis each week, but we will continue to provide in-depth looks at important and emerging trends as necessary, including for new variants of concern. We appreciate your support as our COVID-19 Situation Report continues to evolve.
We want to thank Matthew Shearer, MPH, who served as the lead editor of the Situation Report since January 2020. His attention to detail and critical lens helped shape these updates.
EPI UPDATE The WHO COVID-19 Dashboard reports 236 million cumulative cases and 4.82 million deaths worldwide as of October 7.
Russia continues to report new records in terms of daily mortality, as its current surge becomes its second largest to date. After surpassing 800 deaths per day for the first time in late September, the trend has continued sharply upward. Russia is now reporting 886 deaths per day, a 15% increase since mid-September and still increasing. Russia reported 910 deaths each on October 6 and 7, its highest single-day totals to date. Russia’s daily incidence is also increasing rapidly, up nearly 40% since early-to-mid September.
Syria is combatting its largest surge to date. Syria’s daily incidence increased from 5 new cases per day on July 23 to more than 350 in late September, increasing by a factor of 70 over that period. The surge appears to have peaked several days ago at more than double the previous record—161 in late March 2021. The daily incidence appears to have fallen sharply over the past several days, but it is still in excess of 275. Daily mortality surged as well, increasing from fewer than 1 death per day in early August to 11.6 in late September. Similar to daily incidence, the trend decreased sharply over the past several days—as low as 8.3 on October 3 before jumping back up to 10.3 on October 4—which potentially indicates that reporting delays could be a factor in the sharp downward trends. Syria’s current daily mortality is 9.6 deaths per day.
Global Vaccination
The WHO reported 6.26 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of October 6. A total of 3.59 billion individuals have received at least 1 dose, and 2.61 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline steadily, down from the most recent high of 42 million doses per day on August 30 to fewer than 25 million—a 40% decline over that period*. The global trend continues to closely follow the trend in Asia. In terms of total daily vaccinations, Africa has been on par with Europe and North and South America since late September, with more than 1.5 million doses administered per day. Africa’s average appears to have decreased sharply over the past several days, which could be a function of reporting. On a per capita basis, Africa has nearly reached the daily progress in Europe, with approximately 0.2 daily vaccinations per 100 population. Our World in Data estimates that there are 3.64 billion vaccinated individuals worldwide (1+ dose; 46.3% of the global population) and 2.73 billion who are fully vaccinated (34.7% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 44.0 million cumulative COVID-19 cases and 707,065 deaths. Daily incidence continues to decline, down to approximately 95,000 new cases per day, which is the lowest average since August 2. Daily mortality is declining as well, down from the most recent peak of 1,764 deaths per day on September 15 to 1,431 on October 6*.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over the weekend or for states that are reporting mortality by date of death. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 399.6 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend continues to increase, up from approximately 603,000 doses per day on September 23 to more than 858,000 on October 1, a 42% increase over that period. The current average is the highest since June 17*. The timing of this increase corresponds to the FDA authorization and CDC recommendations regarding third doses of the Pfizer-BioNTech vaccine for many adults.
There are 216.3 million individuals in the US who have received at least 1 dose of SARS-CoV-2 vaccine, equivalent to 65.1% of the entire US population. Among adults, 78.0% have received at least 1 dose, as well as 14.8 million adolescents aged 12-17 years. A total of 186.6 million individuals are fully vaccinated, which corresponds to 56.2% of the total population. Approximately 67.6% of adults are fully vaccinated, as well as 12.1 million adolescents aged 12-17 years. A total of 6.8 million “booster” doses (ie, third doses of the Pfizer-BioNTech or Moderna vaccine) have been administered nationwide**. Adults aged 50 years and older have received 5.7 million of the “booster” doses, including 4.4 million among adults aged 65 years and older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**The second dose of the Pfizer-BioNTech, Moderna, AstraZeneca-Oxford, and other 2-dose vaccines is technically a booster dose as well (ie, part of a prime-boost regimen), but here, we are specifically addressing additional “booster” doses administered beyond the original full vaccination regimen.
Following the authorization and recommendations regarding third doses of the Pfizer-BioNTech and Moderna vaccines (“booster” doses) in late September, daily vaccinations have increased at the national level. As has been the case throughout the US COVID-19 epidemic, these trends vary widely between states and regions. Analysis from The Washington Post indicates that the national average for daily vaccinations increased 28% over the past week. A total of 30 states are reporting increases greater than the national average, including 11 states with +50% or greater. Notably, Utah (+81%), Texas (+84%), Delaware (+92%), and Vermont (+130%) are all reporting greater than +75%. Illinois and Colorado are reporting the national average (+28%), and the remaining 18 states are reporting less, including 4 states with declining trends***: New York (-1%), Alaska (-10%), Mississippi (-11%), and Alabama (-21%).
The regional trends are slightly less clear than for previous vaccination and epidemiological analyses. Based on the distribution of states with respect to the national average, it is not surprising that most regions have more states reporting higher. Notably, all 6 of the HHS Region 5 states (Midwest) are reporting above the national average, including Michigan and Wisconsin with greater than +50%. All but one state in Regions 1, 7, 8, and 10 are reporting greater than the national average. The lone exceptions are Maine (0% change), Missouri (+16%), South Dakota (+8%), and Alaska (-10%), respectively. On the opposite end of the spectrum, 7 of the 8 states in Region 4 (Southeast) are reporting less than the national average, including Mississippi and Alabama with downward trends. As with other percent change analyses, the magnitude of the difference is highly impacted by the previous level of activity. States that were already reporting high daily vaccinations tend to exhibit less relative change than those reporting lower averages due to the larger denominator, which will certainly impact the trends we observe this week.
***Maine is reporting a decrease of less than 1%, which we are categorizing as no change.
IMPACT OF US VACCINATION MANDATES The White House t released a report this week detailing the impact that vaccine requirements have had on increasing vaccine uptake in the US. According to the report, vaccine requirements helped to increase vaccine uptake in the healthcare, corporate, and education sectors, reduce disease transmission and severity, and, therefore, increase economic output. The report also argues that vaccine requirements increased labor participation, a talking point of White House officials over the past few months. The report notes that at least 25% of all US businesses have implemented federal vaccination requirements ahead of deadline and underscores the positive impacts vaccines have had and will continue to have toward ending the COVID-19 pandemic. US President Joe Biden spoke about vaccine requirements at an event in Elk Grove Village, Illinois, on October 7, praising corporations, workers, and unions for coming together to fight COVID-19 and calling on more businesses to require vaccinations. It will be important to monitor changes in specific industries, as several companies have had to fire or place on unpaid leave workers who refuse to get vaccinated, and some experts say the nation has entered the “Great Resignation,” with millions of Americans resigning or considering quitting their jobs.
AT-HOME TEST KITS Surging demand for over-the-counter (OTC) at-home SARS-CoV-2 antigen tests, as well as point-of-care rapid tests—driven by requirements for unvaccinated employees to undergo weekly testing and parents’ need to test schoolchildren—is squeezing the US supply and driving up costs. In a move aimed at scaling up availability of at-home rapid tests, the US White House this week announced it will purchase an additional US$1 billion worth of the tests in order to quadruple the number of tests available in the US by December. The move follows a previous US$2 billion investment announced in September meant to supply rapid tests to community health centers, food banks, and schools. Expanding access to testing is part of US President Joe Biden’s 6-pronged COVID-19 action plan announced September 9. Lack of access to testing in the US could be contributing to the virus’s spread, as government-subsidized rapid testing is widely available in several other countries—including Britain, France, and Germany—making it easier for people to determine whether they are infected after a known exposure or when experiencing symptoms.
Additionally, the US Department of Defense announced it has awarded 6 contracts worth US$2.78 billion to purchase 150 million at-home and 400 million point-of-care COVID-19 test kits to supply health centers, nursing homes, colleges and universities, and other outlets. On October 4, the US FDA authorized the use of ACON Laboratories’ Flowflex COVID-19 Home Test, a rapid antigen test that shows results within 15 minutes and retails for less than US$10. The test—the eighth rapid test available in the US—will help increase the availability of at-home tests, a White House official said. Also this week, Australian company Ellume recalled nearly 200,000 of its test kits over concerns they have a higher-than-expected false-positive rate. Overall, about 427,000 test kits were affected by the problem, including some provided to the Department of Defense, but about half of those were already used.
US COVID-19 RESPONSE FUNDING The US Department of Treasury this week ordered Arizona Governor Doug Ducey to stop using federal pandemic funding to fund 2 new education grants that are open only to schools without mask mandates, in line with a state law enacted in June. In a letter, US Deputy Treasury Secretary Adewale Adeyemo said the state grant programs’ conditions “undermine evidence-based efforts to stop the spread of COVID-19” and asked the state to explain how it will “remediate” the problems, or face administrative or other action. Governor Ducey’s office indicated they are reviewing the letter and will respond. Arizona is one of at least 8 states that have laws or executive orders banning school mask mandates.
In Florida, one of those states, the State Board of Education on October 7 voted to withhold funding from 8 school districts that have implemented mask requirements despite a state ban and accepted recommendations from Florida Education Commissioner Richard Corcoran to withhold state funds equivalent to local school board members’ salaries and any amount the district receives in federal grants meant to backfill funding to districts with mask mandates. Ahead of the meeting, several districts—including Hillsborough, Sarasota, and Indian River counties—loosened their mask requirements to avoid funds being withheld. Several lawsuits challenging the state’s ban are moving through the courts, and the US Department of Education continues civil rights investigations in Florida and other states with mask mandate bans to determine whether the policies violate the rights of students with disabilities. According to a survey by Burbio, only about 3% of school districts nationwide are banned from implementing mask requirements and three-quarters of the largest districts had mandates at the beginning of October. School districts and parents are wondering what comes next, with the US FDA set to discuss vaccines for children ages 5 to 11 and a future existence with COVID-19 a near certainty.
PEDIATRIC VACCINE As expected, Pfizer and BioNTech on October 7 requested the US FDA grant Emergency Use Authorization (EUA) for use of its SARS-CoV-2 vaccine in children ages 5 to 11. The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) already scheduled an October 26 meeting to discuss the request. If the FDA authorizes the vaccine, about 28 million US children would become eligible for vaccination. The companies are proposing giving children a 2-dose regimen of 10μg doses administered 21 days apart, one-third of the adult dosage. Last month, the companies submitted to the FDA topline results from a Phase 2/3 clinical trial including 2,268 pediatric participants that showed a favorable safety profile and “robust neutralizing antibody responses.” While the FDA could work quickly to review data on the vaccine for younger populations, its availability will depend upon whether the companies can provide evidence they are able to appropriately manufacture and label a new pediatric formulation. Notably, children under age 18 accounted for 26.7% of reported weekly COVID-19 cases in the US for the week ending September 30, a disproportionate share of cases given they make up about 22.2% of the total US population, according to the American Academy of Pediatrics (AAP).
PRE-EXPOSURE PROPHYLAXIS AstraZeneca on October 5 submitted a request to the US FDA for an Emergency Use Authorization (EUA) of its investigational long-acting antibody combination drug AZD7442 for the prevention of symptomatic COVID-19. The monoclonal antibodies—given as a 2-dose subsequent injection—are designed to remain in the body for up to a year and could be used in people who do not mount a strong immune response to a SARS-CoV-2 vaccine and those who have been advised to not take the vaccine, or as an extra precaution among certain populations, such as military personnel. In August, AstraZeneca said ADZ7442 reduced the risk of symptomatic COVID-19 by 77% when compared to a placebo in a Phase 3 trial including 5,197 participants, more than 75% of whom had comorbidities. The trial data are not yet published or peer-reviewed. If the FDA grants an EUA, the antibody therapy would be the first of its kind to be authorized as a pre-exposure prophylaxis option. In September, the FDA authorized Regeneron’s monoclonal antibody combination for post-exposure prophylaxis.
POST-VACCINATION MYOCARDITIS Researchers with Kaiser Permanente published a research letter in JAMA Internal Medicine examining acute myocarditis in adult members of Kaiser Permanente Southern California following vaccination with a SARS-CoV-2 mRNA vaccine between December 2020 and July 2021. Of the nearly 2.4 million individuals who received at least 1 dose of vaccine, the researchers identified only 15 confirmed cases of myocarditis. Two (2) of the cases happened after administration of the first dose and 13 occurred after the second dose for an observed incidence of 0.8 cases per 1 million first doses and 5.8 cases per 1 million second doses over a 10-day observation window. Notably, all of the cases occurred in men ages 20 to 32 (median age 25), but none required intensive care unit (ICU) admission and none were readmitted to the hospital for myocarditis following discharge. Overall, incidence of post-vaccination myocarditis was rare in the study’s diverse population.
A second paper published in the New England Journal of Medicine highlights similar data from approximately 5.1 million individuals vaccinated in Israel. Researchers retrospectively analyzed data on hospitalized cases of myocarditis that occurred from December 2020 to May 2021. They observed 283 myocarditis cases, with 142 cases occurring after receipt of the Pfizer-BioNTech vaccine. Of those 142 cases, 95% presented with mild symptoms. The highest incidence rate—13.73 cases per 100,000 persons—was recorded among male recipients ages 16 to 19 following their second vaccine dose. Researchers of both studies agreed that the risk of myocarditis remained low following mRNA vaccination but the rate of myocarditis in young men receiving a second dose warrants further investigation.
Both studies support some countries’ decisions to recommend that children aged 12 and older receive only a single dose of mRNA vaccine. While the Israeli study looked exclusively at those who received the Pfizer-BioNTech vaccine, data from the Norwegian Institute of Public Health (NIPH) suggest similar concerns for young men who received Moderna’s vaccine. While still rare, myocarditis occurred more frequently in young men who received a second dose of the Moderna mRNA vaccine, the data show. NIPH recommends that all individuals under age 18 be vaccinated with the Pfizer-BioNTech vaccine and that men under age 30 should also consider choosing that vaccine. Other Nordic countries, including Finland and Sweden, have followed suit, limiting their use of the Moderna vaccine in young adults. Denmark also said it was limiting use of the vaccine but later retracted that statement, noting the vaccine is still available for people under age 18.
VACCINE EFFECTIVENESS A study published in the peer-reviewed journal The Lancet on October 4 shows that a decrease in effectiveness of the Pfizer-BioNTech SARS-CoV-2 vaccine may be due to waning immunity rather than the Delta variant escaping the vaccine. The study examined 3.4 million individuals over the age of 12 years who were members of Kaiser Permanente Southern California. Outcomes were determined by measuring positive PCR tests and hospital admissions related to COVID-19. The vaccine was 93% effective at preventing infection with the SARS-CoV-2 Delta variant 1 month after vaccination, but that protection fell to 53% at 4 months post-vaccination. The vaccine was 97% effective at preventing infection with non-Delta SARS-CoV-2 one (1) month after vaccination, but that protection fell to 67% at 4-5 months post-vaccination. Study leader Dr. Sara Tartof noted that waning protection from infection for both Delta and non-Delta variants points to overall waning immunity and not Delta variant escape. If Delta were able to escape the vaccine, 1-month protective effectiveness against the variant would have started low and remained low. According to the study, the vaccine remained 93% effective at preventing COVID-19-related hospitalization for all age groups up to 6 months. The authors noted it is possible that lower viral loads after vaccination could overestimate vaccine effectiveness against the Delta variant due to failed genomic sequencing.
POST COVID-19 CONDITION On October 6, the WHO released a case definition of post COVID-19 condition—also referred to as post-acute sequelae of COVID-19 (PASC) or “long COVID”—based on interviews with international subject matter experts and COVID-19 patients. The effort identified 12 domains that were important for establishing a clinical case definition: SARS-CoV-2 infection, laboratory confirmation of infection, a 3-month minimum from onset of symptoms, a 2-month minimum for duration of symptoms, a set of common symptoms, a minimum number of present symptoms, clustering of symptoms, the time course of symptoms, sequelae of COVID-19 complications, no possible alternative diagnosis, applicability of definition to various populations, and an impact on everyday functioning. Long COVID symptoms include “brain fog,” chest pressure, depression, fatigue, fever, heart palpitations, and shortness of breath, among myriad others. The WHO noted that a separate case definition for long COVID may be necessary for children.
A separate study published in the peer-reviewed journal Cardiovascular Diabetology reported the discovery of microclots containing inflammatory molecules that are resistant to fibrinolysis by the enzyme trypsin in patients with long COVID. The clots contained fibrinogen, which aids clot formation, and alpha 2-antiplasmin, which prevents the breakdown of blood clots. The study authors said the clots may indicate a broader impact on the cardiovascular system and further research is needed into anti-clotting therapies for long COVID.
LATIN AMERICA Although daily COVID-19 incidence is trending downward in Latin America, regional health officials this week expressed concern over the situations in several countries and called on nations to place more focus on a “One Health” approach to more quickly detect and respond to emerging diseases. Overall, about 37% of the population in Latin America and the Caribbean are fully vaccinated. Some nations, such as Chile (74%) and Uruguay (75%), have fully vaccinated more than 70% of their population, but at least 10 countries sit at rates below 25%, including Venezuela (21%), Guatemala (16%), Jamaica (10%), Nicaragua (5%), and Haiti (0.2%). Pan American Health Organization (PAHO) Director Dr. Carissa F. Etienne said the international community must work urgently to close the gap in vaccine availability, the primary factor in lower vaccination rates in both regions. She announced PAHO has struck deals with vaccine manufacturers Sinopharm, Sinovac, and AstraZeneca for doses to be delivered this year and next. On October 6, a WHO official blamed wealthy nations for buying up the global supply and vaccine producers for not prioritizing delivery of doses to the COVAX facility, which will not meet its goals for delivering shots to Latin America and the Caribbean this year. Dr. Etienne also pointed to vaccine hesitancy as one factor in lower vaccination rates, with widespread misinformation regarding the vaccines’ safety also playing a role.
MODERNA VACCINE FACILITY IN AFRICA Only 9 of Africa’s 54 nations met a WHO goal to vaccinate 10% of their population against SARS-CoV-2 by the end of September, and the continent remains far behind others in efforts to reach 40% of its people by the end of the year, with only about 4.5% overall coverage. Efforts to increase vaccine supply on the continent continue, and there were at least 12 established or planned SARS-CoV-2 vaccine production facilities in 6 African countries as of last month. This week, Moderna announced it will invest $500 million in a “state-of-the-art” mRNA vaccine production facility in an African country, with the goal of producing 500 million 50µg doses of vaccines—for COVID-19 and other diseases—annually. The selection process for a country and site is expected to begin soon, but completing construction and validation likely will take 2-4 years, a timeline that does not address Africa’s current vaccine access challenges.
Notably, the Moderna facility will be able to fully manufacture mRNA vaccines on the continent, the first vaccine producer to do so. In July, Pfizer-BioNTech announced a deal with a South African company to “fill and finish” mRNA SARS-CoV-2 vaccines on the continent, with ingredients shipped in from other countries. Moderna’s announcement comes amid ongoing debate between pharmaceutical companies and governments about temporary intellectual property rights waivers. However, talks regarding waivers are deadlocked at the World Trade Organization (WTO), despite the support of more than 100 countries. Additionally, anonymous sources report that tension is growing between Moderna and the administration of US President Joe Biden, with the company showing reluctance to make additional commitments to the US government to increase international vaccine donations.
WHO VACCINATION STRATEGY The WHO on October 7 launched its “Strategy to Achieve Global COVID-19 Vaccination by Mid-2022,” with a goal of vaccinating 40% of the world’s population against SARS-CoV-2 by the end of 2021 and 70% by mid-2022. At a press briefing announcing the strategy, WHO Director-General Dr. Tedros Adhanom Ghebreyesus said the current disparities in vaccination coverage are wholly due to gaps in allocation and that the new goals would only be met if wealthy countries and vaccine producers prioritize contracts for the COVAX facility and the African Vaccine Acquisition Trust (AVAT). To reach the 2022 goal, at least 11 billion vaccine doses are needed, Dr. Tedros noted, and more than 6 billion already have been administered worldwide. Speaking at the same event, UN Secretary-General Antonio Guterres called vaccine inequity “immoral” and “stupid” and urged countries—including G20 nations set to meet later this month—to commit US$8 billion to ensure equitable vaccine distribution by this year’s end.
COVAX REVIEW The Bureau of Investigative Journalism and STAT today published an account of the global COVAX collaboration, founded in April 2020 to serve as a conduit of SARS-CoV-2 vaccines—an “insurance policy” for most nations but a “lifeline” for low-income countries amid the COVID-19 pandemic. The article presents reviews of confidential internal documents and accounts of officials from at least 12 countries, who expressed confusion and frustration over COVAX’s operations and commitments. COVAX has fallen short of its goal to provide 2 billion doses in 2021, contributing less than 5% of all vaccine doses administered globally. The story highlights the misalignment of leadership and power in global efforts to end the COVID-19 pandemic.
by dryrunguy Meanwhile, my boss's boss convened a meeting of our group this morning. After some dancing around, he dove into the issue of the federal mandate and how it applies to federal contractors, subcontractors, and part-time staff who bill to federal contracts or subcontracts.
My boss asked for clarification regarding why the mandate would apply to people who bill entirely to corporate overhead. The head of our group stated that the mandate also applies to us.
At which point all hell broke loose. "50,000 people in the U.S. have died from the vaccine!" "It's my body!" "It's all because big pharma controls government!" "XX% of people in Israel who got vaccinated are getting COVID!" And on and on and on. She also couldn't have her rant without mentioning that virtues of ivermectin. I died a little. Again. And she was so worked up that she was even foolish enough to mention how it's possible to buy fake vaccination cards. Which, as I understand it, would constitute job fraud.
After the rant, she paused and said, "I guess the writing is on the wall."
I'm not sure what that meant.
by ti-amie In the context you provided she sees that if she wants to continue to be paid what I assume is a pretty good salary she's going to have to get vaccinated. If she meant it some other way then she's an idiot.
by ti-amie I don't know who started car rants but I love them. I first saw them done by Noel Casler and I still watch his. This man is good too. When I saw Petra doing one I knew that they were now a meme.
by Suliso The honest thing to do would be to resign, right?
by ti-amie
Suliso wrote: ↑Fri Oct 08, 2021 5:54 pm
The honest thing to do would be to resign, right?
And lose her pension? Not a chance. The way things are going though institutions that have put mandates in place are not effing around. Valid proof or you will definitely find out.
by Suliso Don't you get a partial pension if you say worked 20 years for federal government and then went on to work another 20 in the fully private sector?
by dryrunguy
ti-amie wrote: ↑Fri Oct 08, 2021 5:52 pm
In the context you provided she sees that if she wants to continue to be paid what I assume is a pretty good salary she's going to have to get vaccinated. If she meant it some other way then she's an idiot.
Well, she makes good buck, for sure. But her partner is a retired police officer, so my boss in the breadwinner in that house (a VERY nice house, I might add).
Once you dive into the world of government contracting, it's hard to get out. So it's not like she can just switch to another company that does government contracting. Other segments of the private sector also have their own mandates. But there are probably some sectors completely isolated from federal contracting that would welcome her and other unvaccinated people. Who knows.
When she said, "I guess the writing is on the wall," my gut told me that she expects to get fired. I just don't think she'll get vaccinated. For her, the opposition to vaccination is a cause, an act of defiance that shows she's smarter than everyone else, and losing her job would fall into the category of righteous martyrdom. That's what my gut says.
ti-amie wrote: ↑Fri Oct 08, 2021 5:52 pm
In the context you provided she sees that if she wants to continue to be paid what I assume is a pretty good salary she's going to have to get vaccinated. If she meant it some other way then she's an idiot.
Well, she makes good buck, for sure. But her partner is a retired police officer, so my boss in the breadwinner in that house (a VERY nice house, I might add).
Once you dive into the world of government contracting, it's hard to get out. So it's not like she can just switch to another company that does government contracting. Other segments of the private sector also have their own mandates. But there are probably some sectors completely isolated from federal contracting that would welcome her and other unvaccinated people. Who knows.
When she said, "I guess the writing is on the wall," my gut told me that she expects to get fired. I just don't think she'll get vaccinated. For her, the opposition to vaccination is a cause, an act of defiance that shows she's smarter than everyone else, and losing her job would fall into the category of righteous martyrdom. That's what my gut says.
If she's fired would she still be entitled to her pension?
ti-amie wrote: ↑Fri Oct 08, 2021 5:52 pm
In the context you provided she sees that if she wants to continue to be paid what I assume is a pretty good salary she's going to have to get vaccinated. If she meant it some other way then she's an idiot.
Well, she makes good buck, for sure. But her partner is a retired police officer, so my boss in the breadwinner in that house (a VERY nice house, I might add).
Once you dive into the world of government contracting, it's hard to get out. So it's not like she can just switch to another company that does government contracting. Other segments of the private sector also have their own mandates. But there are probably some sectors completely isolated from federal contracting that would welcome her and other unvaccinated people. Who knows.
When she said, "I guess the writing is on the wall," my gut told me that she expects to get fired. I just don't think she'll get vaccinated. For her, the opposition to vaccination is a cause, an act of defiance that shows she's smarter than everyone else, and losing her job would fall into the category of righteous martyrdom. That's what my gut says.
If she's fired would she still be entitled to her pension?
I don't think we have a pension program. Federal employees have pension plans (for now). My understanding is that we just have our 401K, Roth IRAs, other investments, and savings.
by JazzNU
dryrunguy wrote: ↑Fri Oct 08, 2021 5:37 pm
Meanwhile, my boss's boss convened a meeting of our group this morning. After some dancing around, he dove into the issue of the federal mandate and how it applies to federal contractors, subcontractors, and part-time staff who bill to federal contracts or subcontracts.
My boss asked for clarification regarding why the mandate would apply to people who bill entirely to corporate overhead. The head of our group stated that the mandate also applies to us.
At which point all hell broke loose. "50,000 people in the U.S. have died from the vaccine!" "It's my body!" "It's all because big pharma controls government!" "XX% of people in Israel who got vaccinated are getting COVID!" And on and on and on. She also couldn't have her rant without mentioning that virtues of ivermectin. I died a little. Again. And she was so worked up that she was even foolish enough to mention how it's possible to buy fake vaccination cards. Which, as I understand it, would constitute job fraud.
Whew! This was a tough read. Honey, in front of people that work for you AND your boss? Oh dear.
by JazzNU
dryrunguy wrote: ↑Fri Oct 08, 2021 6:38 pm
When she said, "I guess the writing is on the wall," my gut told me that she expects to get fired. I just don't think she'll get vaccinated. For her, the opposition to vaccination is a cause, an act of defiance that shows she's smarter than everyone else, and losing her job would fall into the category of righteous martyrdom. That's what my gut says.
How could she not have known this was coming? She would've almost had to practice that spiel because if she's not dumb, and I don't see how she could be, she had to know this was on the horizon. So that was the performance she decided to give you all.
My read of the writing is on the wall is that this will force her out. She will think she's getting fired, but I've got news for her, it's really a voluntary quit. She will not be collecting unemployment. People appear to be generally clueless about how unemployment works.
Also, just an FYI. These "freedom fighters" who will soon find out that their misguided morals aren't accepted as payment by the bank holding their mortgage and car note, are in a for a rude awakening that even companies without a vaccine mandate for employees are requiring it of all new hires. Working with existing employees is one thing, taking on a problem with a new hire is quite another.
by dryrunguy Yeah, the whole thing is just very, very sad. And we have our usual staff meeting on Monday, so it will probably be the same thing all over again since business development activities are fairly slow this time of year and there won't be much else to talk about.
I actually spent about 30 minutes earlier today trying to come up with a list of other things to talk about, just so we could avoid the subject, and then I suddenly said to myself, "WTF am I doing?!?!"
Meanwhile, if my boss leaves, I know EXACTLY where all of her responsibilities will go. And that's depressing, too, because I have zero interest in doing much of anything she does. It's just not my wheelhouse.
by Deuce
dryrunguy wrote: ↑Fri Oct 08, 2021 6:38 pm
For her, the opposition to vaccination is a cause, an act of defiance that shows she's smarter than everyone else, and losing her job would fall into the category of righteous martyrdom. That's what my gut says.
That is my take on the majority of people who are against the vaccine.
In my experience, they are insecure people who desperately need to 'prove' something, and so they align themselves with the vocal minority in claiming that they 'know better' than the majority, that they are not followers, etc.
We see the same thing playing out - for the same reasons - in several other elements of life, as well.
I, myself, as anyone who knows me will attest, am quite cynical, and am the opposite of a follower. I also believe that dishonesty, greed, selfishness, and manipulation are inherent elements of politics and politicians at all levels everywhere. But I still got my 2 vaccines as soon as I was able to.
by Deuce A valid argument can definitely be made to make every seat on passenger planes ejectable, with the eject button controlled remotely by airline staff...
by dryrunguy Here's the latest Situation Report. In particular, the second paragraph under Racial/Ethnic Disparities is pretty stunning.
::
EXTENDED PRIMARY VACCINE SERIES On October 11, the WHO’s Strategic Advisory Group of Experts (SAGE) on Immunization recommended additional doses of SARS-CoV-2 vaccines for immunocompromised individuals. The recommendation applies to all 7 vaccines that have received an Emergency Use Listing (EUL) from the WHO and to all individuals who are moderately or severely immunocompromised individuals. SAGE also recommended a third dose of the Sinopharm and Sinovac vaccines for individuals aged 60 years and older. The advisory group emphasized that countries should initially prioritize administering the full original vaccine regimen to increase vaccination coverage, but an additional dose would provide extra protection for individuals at the highest risk for severe disease.
Notably, SAGE clearly distinguished its updated guidance from booster dose policies being implemented in some countries, including several in Europe, Israel, and the US. Specifically, the additional doses recommended under the new SAGE guidance are intended “as part of an extended primary series since [immunocompromised] individuals are less likely to respond adequately to vaccination” rather than as a general boost to protection for otherwise healthy individuals. The SAGE experts met for 4 days to discuss myriad vaccine-related issues, including non-pandemic topics such as the world’s first malaria vaccine, and the full meeting report is expected to be published in December. Reportedly, SAGE will address waning immunity and the need for broader booster doses in healthy individuals at a meeting scheduled for November 11.
MOLNUPIRAVIR EUA REQUEST Merck and Ridgeback Biotherapeutics on October 11 submitted an application with the US FDA for Emergency Use Authorization (EUA) of molnupiravir, an investigation oral antiviral medication, for the treatment of mild-to-moderate COVID-19 in adults at high risk of severe disease. Notably, if authorized by the FDA, the drug would be the first COVID-19 treatment to be administered orally, as all other authorized or approved medications are delivered intravenously or via injection. The companies’ submission is based on a Phase 3 clinical trial interim analysis showing molnupiravir reduced the risk of hospitalization or death by about half when compared with people who received a placebo. The data are not yet published or peer-reviewed. An effective therapeutic that is taken by people recovering at home could relieve some pressure on hospitals, particularly in areas with low vaccination rates.
Two Indian generic drug manufacturers last week requested permission to end late-stage clinical trials of generic versions of molnupiravir, after the drug did not show “significant efficacy” among people with moderate COVID-19 disease. A Merck spokesperson noted that the Indian studies defined moderate disease differently than the FDA and included patients with more severe disease. The Indian companies are continuing to research the treatment among people with mild COVID-19.
COVID-19 IN PREGNANCY Echoing guidance by the US CDC, England’s National Health Service (NHS England) on October 11 encouraged pregnant people to get vaccinated against SARS-CoV-2 and released data showing that, since July, nearly 1 in 5 of England’s most critically ill COVID-19 patients—those who required intensive care unit support including extracorporeal membrane oxygenation (ECMO)—have been unvaccinated pregnant women. Notably, of all women between the ages of 16 and 49 who have required ECMO in an intensive care unit, 32% of them have been pregnant, up from 6% at the beginning of the pandemic. NHS England is working to dispel misinformation and fears surrounding SARS-CoV-2 vaccines, pointing to safety data showing the shots are safe for pregnant individuals and their fetuses. According to data from the CDC, COVID-19 poses a significantly higher risk to pregnant people compared with non-pregnant people.
Several other recently released studies suggest that pregnant people with symptomatic COVID-19 are at a higher risk of emergency complications and other adverse perinatal and neonatal outcomes. A not-yet-peer-reviewed study presented over the weekend at the Anesthesiology 2021 Annual Meeting and a peer-reviewed study published October 10 in the Journal of Maternal-Fetal & Neonatal Medicine showed that pregnant people with COVID-19 who were symptomatic had an increased risk of giving birth in emergency circumstances and were more likely to have complications endangering their newborns, compared with those who had asymptomatic COVID-19 or who were not infected. Researchers writing in the American Journal of Obstetrics and Gynecology found that the recent surge of the Delta variant was associated with increased morbidity among pregnant people with COVID-19, particularly in underserved populations with low vaccine acceptance, prompting them to highlight the urgency of preventive measures during pregnancy, including vaccination. Additionally, experts attending the recent American Academy of Pediatrics (AAP) virtual meeting discussed neonatal outcomes, an apparent increase in preterm birth incidence among infected pregnant people compared with the 2019 incidence, as well as higher-than-expected maternal mortality among pregnant people testing positive at or around the day of delivery. All of the studies support emerging trends showing that COVID-19 can severely impact pregnant people and neonates, and provide evidence that vaccination is critically important for this population.
MENTAL HEALTH Prior to World Mental Health Day on October 10, a study published online on October 8 in The Lancet documented a grim and startling rise in cases of major depressive disorder (53.2 million new cases; 27.6% increase) and anxiety disorders (76.2 million new cases; 25.6% increase) globally from January 1, 2020 to January 29, 2021. The study was a systematic review of the prevalence of major depressive disorder and anxiety orders during the COVID-19 pandemic across various comprehensive sources, culminating in a meta-regression to estimate the rise in these 2 disorder types during the pandemic associated with COVID-19 impact indicators (e.g. mobility, daily SARS-CoV-2 infection rate). Impact indicators were found to be associated with increased prevalence of major depressive disorder and anxiety disorders, particularly among women and younger age groups.
The US CDC Morbidity and Mortality Weekly Report (MMWR) also published a similar study last week on national and state trends related to anxiety and depression during the pandemic. Findings noted that anxiety severity scores and depression severity scores increased from August 2020 to December 2020 before decreasing until June 2021.
RACIAL/ETHNIC DISPARITIES American Indian/Alaska Native (AI/AN), Black, and Latino individuals in the US have been disproportionately affected by the COVID-19 pandemic, with the disease causing more deaths by population size—both directly and indirectly—among these groups when compared with White or Asian populations. In a study published last week in the Annals of Internal Medicine, researchers reported that during the first 10 months of the pandemic (March-December 2020), an estimated 477,200 excess deaths occurred in the US than would have been expected based on 2019 data. Of these deaths, about 74% were directly attributable to COVID-19. After adjusting for age, overall excess deaths per 100,000 persons in 2020 were 2 to 3 times higher among AI/AN, Black, and Latino individuals compared with White and Asian individuals. Although the reasons for excess mortality are unknown, the researchers noted that “structural and social determinants of health with established and deep roots in racism”—including an increased risk of occupational exposure and lack of access to healthcare, possibly caused by fear during the pandemic—or misattribution of causes of death could have played roles.
The racial and ethnic disparities in COVID-19-related deaths spill over into the pandemic’s impacts on children. According to a modeling study published last week in Pediatrics, children of racial and ethnic minorities accounted for 65% of the more than 140,000 children who experienced orphanhood or lost a caregiver due to COVID-19 between April 2020 and June 2021. Compared to White children, AI/AN children were 4.5 times more likely to lose a caregiver, Black children were 2.4 times more likely, and Hispanic children were 1.8 times more likely. The highest burden of caregiver deaths due to COVID-19 occurred in states on the Southern US border, in the Southeast, and those with tribal areas. The researchers concluded there is an “urgent need” to provide affected children access to support services. An October 8 analysis from the Kaiser Family Foundation using CDC data shows that racial disparities in COVID-19 cases and death rates persist among Black, Hispanic, and AI/AN individuals, but data suggest the gap has recently narrowed for Black and Hispanic people. Notably, AI/AN individuals remain at disproportionate risk for COVID-19 disease and death, despite having the highest vaccination rate across racial/ethic groups. While the narrowing disparity in some groups could be due to increasing vaccination rates, other factors definitely play a role in ongoing disparities, and more research is needed to understand and address them.
AUSTRALIA On October 11, Australia began to emerge from its strict pandemic lockdown when New South Wales (NSW) began to allow fully vaccinated residents to return to restaurants, bars, hair salons, and gyms after nearly 4 months of restrictions. About 74% of NSW residents aged 16 and older are fully vaccinated, enabling the state—including Sydney, Australia’s most populous city—to ease its lockdown despite an ongoing outbreak. NSW State Premier Dominic Perrottet called it a “freedom day” and pledged to lead the nation out of the pandemic, but not without challenges. He warned that the number of new COVID-19 cases will rise following reopening, as virus-free Western Australia and Queensland and other so-called “zero COVID” countries in the Asia-Pacific region watch closely to see whether NSW can adapt to living with COVID-19.
ITALY’S GREEN PASS From October 15 through the end of 2021, Italian workers will be required to present a digital or printed “Green Pass” certificate upon entering their workplace, demonstrating that they have recovered from COVID-19 in the last six months, received a negative COVID-19 rapid antigen test result in the last 48 hours, received a negative COVID-19 molecular test result in the last 72 hours, or have been at least partially vaccinated. Workers who do not comply with the new mandate risk fines or suspension. Both civil and violent protests have broken out in response to the September 16 announcement regarding the new mandate in Italy, including reported clashes over the weekend between neo-fascists or other individuals associated with the far right and police. Some employees and policymakers are concerned that a rise in vaccinations may not occur, instead leading to worker shortages due to a lack of available tests.
The Green Pass already is required in Italy in order to access schools and universities, utilize public transport, participate in gatherings related to civil or religious ceremonies, visit medical facilities or long-term care facilities, access certain public gathering events or spaces, and pass through areas with higher COVID-19 risk—so-called “red” or “orange” zones. The Green Pass also is recognized by the European Union to help travelers avoid COVID-19 travel restrictions.
by ponchi101 Ok, great for Australia and NSW, but the word FREEDOM will pretty soon lose all recognizable meaning when it is used for anything that remotely relates to real freedom. If the proper explanation is not given, you simply become a parrot saying the word without understanding it.
Somebody has to coin a word that combines FREEDOM and DUTY so it can explain things better.
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 238.5 million cumulative cases and 4.86 million deaths worldwide as of October 13. Global weekly incidence decreased by 6.7% compared to the previous week, and mortality fell by 9.5%.
Global Vaccination
The WHO reported 6.36 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of October 10. A total of 3.63 billion individuals have received at least 1 dose, and 2.64 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline, down to fewer than 23 million doses per day*. The global trend continues to closely follow Asia. Our World in Data estimates that there are 3.78 billion vaccinated individuals worldwide (1+ dose; 47.97% of the global population) and 2.80 billion who are fully vaccinated (35.56% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 44.5 million cumulative COVID-19 cases and 716,370 deaths. The US has passed a peak in terms of daily incidence. The most recent high was 161,711 new cases per day on September 1, and the trend began to decline slightly before the Labor Day holiday weekend. The current average is approximately 86,181 new cases per day and appears to be decreasing. Daily mortality also appears to have passed a peak, down from a recent high of 1,815 on September 15 to 1,252 on October 12*.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
According to an analysis published October 13 by the Peterson Center on Healthcare and the Kaiser Family Foundation, COVID-19 continues to be a leading cause of death in the US. While daily mortality is now falling, COVID-19 was the second leading cause of death in the US in September 2021, behind heart disease, according to the analysis based on US CDC and other data. The majority of COVID-19-related deaths have been among unvaccinated individuals.
US Vaccination
The US has administered 404 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend rose briefly following authorization of booster doses of the Pfizer-BioNTech vaccine for some populations on September 22 but is now declining after a recent peak on October 1*. There are 217.6 million individuals who have received at least 1 dose, equivalent to 65.6% of the entire US population. Among adults, 78.5% have received at least 1 dose, as well as 14.7 million adolescents aged 12-17 years. A total of 187.9 million individuals are fully vaccinated, which corresponds to 56.6% of the total population. Approximately 68% of adults are fully vaccinated, as well as 12.1 million adolescents aged 12-17 years.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
VACCINE BOOSTERS The US FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) is meeting today to discuss Moderna’s request for authorization of an additional dose of its SARS-CoV-2 vaccine and on October 15 to discuss a similar request from J&J-Janssen. Any recommendations the committee makes are used to help the FDA make decisions but are not binding. Moderna has asked regulators to authorize an additional half-dose of its vaccine for adults aged 65 and older—a decision which appears to already be made based on questions submitted to the committee—and individuals at high risk of severe COVID-19, similar to the authorization granted last month for the Pfizer-BioNTech vaccine. An FDA briefing document released this week suggests that a booster dose of Moderna’s vaccine administered at least 6 months from the second dose increased antibody levels in recipients. However, the difference of the levels before and after the booster dose was not wide, and the agency did not take a position on whether the extra dose was necessary. The panel also will discuss the risk of post-vaccination myocarditis and other adverse reactions and whether data show efficacy of the Moderna vaccine is waning. In separate documents submitted to the FDA, Moderna said a half-dose (50μg) additional shot provided similar increases in antibody levels as the full dose (100μg) but with fewer side effects.
During the second day of meetings, VRBPAC will consider whether data presented by J&J-Janssen supports a booster dose for its single-dose SARS-CoV-2 vaccine, and when the additional dose should be administered. In a briefing document released October 13, the FDA said there “may be a benefit” in giving a second dose about 2 months after the primary dose and made it clear that while the J&J-Janssen vaccine provides protection against severe COVID-19, it is less effective than the mRNA vaccines from Moderna and Pfizer-BioNTech. However, the agency questioned the sample sizes of the studies showing a benefit and did not provide a clear conclusion on whether the panel would recommend booster doses for certain populations.
VRBPAC also likely will discuss “mixing and matching” vaccines but is not expected to make recommendations on the approach. Highly anticipated results from a US NIH-sponsored study were posted to the preprint server medRxiv on October 13, suggesting that recipients of the J&J-Janssen vaccine might produce a more intense immune response to a booster dose of an mRNA vaccine than an additional dose of the J&J-Janssen vaccine. Individuals who initially received either the Moderna or Pfizer-BioNTech vaccines and received a third dose of either shot showed similarly strong immune responses, according to the study, which is not yet peer-reviewed. The US CDC’s Advisory Committee on Immunization Practices (ACIP) is scheduled to meet next week to discuss the FDA’s recommendations on booster doses. If regulators eventually decide to permit mixing and matching vaccines, the FDA will have to amend the authorizations of both mRNA vaccines to permit them to be used to boost the J&J-Janssen vaccine.
US TRAVEL REQUIREMENTS The US plans to ease travel restrictions in November for fully vaccinated individuals crossing its land borders with Canada and Mexico, marking a reopening to travelers and tourists after being closed for more than 18 months. Unvaccinated individuals will continue to be banned from crossing the country’s northern and southern borders for nonessential travel. The new rules—which coincide with and are similar to recently updated guidance for air travelers—will be implemented in phases, with vaccinated visitors traveling for nonessential reasons to be allowed to cross land borders in November, and all inbound travelers, whether essential or nonessential, needing proof of vaccination by January 2022. Canada reopened its US border to nonessential travel by fully vaccinated US residents in August, and Mexico never closed its northern border. Several US Members of Congress representing border states welcomed the rule changes, as closures had separated cross-border families and wrought financial tolls on border cities. Notably, the US will keep in place a separate immigration policy that allows the government to deport or turn away any migrants who are seeking asylum or economic opportunity.
VACCINE MANDATES Since US President Joe Biden announced SARS-CoV-2 vaccination requirements for federal workers and contractors, healthcare systems, and employers with 100 or more employees, most workers have chosen to be vaccinated, despite some predictions mandates might worsen labor shortages by prompting widespread resignations. The requirements boosted vaccination rates by at least 20 percentage points, White House officials said on October 13. Aerospace company Boeing and Southwest Airlines are the latest large corporations to announce their employees must be vaccinated or receive exemptions by December 8, in compliance with new federal guidelines expected to be finalized soon. However, confusion arose for Texas-based Southwest and American Airlines, as well as other companies, on October 11, as Texas Governor Greg Abbott signed an executive order extending bans on COVID-19 vaccine mandates by any entity in the state, including private employers, and broadening reasons for exemptions. A previous executive order from Governor Abbott bans vaccine requirements by government agencies, cities, counties, and school districts in the state. Both Southwest and American indicated they will maintain their vaccine requirements for employees. Most other companies also likely will follow the federal rule, as federal law takes precedence over state law under the Supremacy Clause of the US Constitution. But questions over the conflicting laws remain.
In Florida, the state Department of Health levied a fine of more than US$3.5 million on Leon County for requiring county employees to be vaccinated, in violation of a state law. Under the law, government agencies can be fined US$5,000 for each violation of requiring vaccination as a condition of employment. The state said Leon County violated the law 714 times, for each of its employees, accruing a fine of US$3.57 million it must pay within 30 days. The Leon County administrator called the ban politically motivated and vowed to enforce the county vaccine mandate “using any remedies available.”
In New York, a federal judge on October 12 issued a preliminary injunction barring state health officials from interfering with employers who allow religious exemptions to state-imposed vaccination mandates for all healthcare workers. Judge David N. Hurd of the Northern District said the state overreached by barring all religious accommodations in its mandate and wrote that the 17 healthcare workers who filed the lawsuit were likely to succeed. New York Governor Kathy M. Hochul vowed to appeal the ruling. The case (Dr. A et al v. Hochul) provides a test for strict vaccine mandates covering healthcare workers. At least 23 states require SARS-CoV-2 vaccination for healthcare workers.
SARS-COV-2 ORIGIN The WHO on October 13 announced 26 proposed members of its new Scientific Advisory Group for the Origins of Novel Pathogens (SAGO), which is tasked with creating a global framework to define and guide investigations into the origins of emerging and re-emerging diseases of epidemic and pandemic potential, including SARS-CoV-2. The scientists, hailing from 26 different nations, have expertise in a wide range of areas, from molecular biology to animal health and include 6 members of the previous 10-person joint WHO-China mission that investigated the COVID-19 pandemic’s origins and issued inconclusive findings more than 6 months ago. The WHO said the renewed effort might be the “last chance” to find the virus’s origins, but some questioned whether an advisory board will have the power to make inroads with China, which has not been a very cooperative partner. This week, Chinese officials said the country plans to test up to 200,000 blood bank samples from the city of Wuhan, where the virus was first identified in December 2019. The samples have been in storage for 2 years and could help provide clues as to when and where the virus first appeared in humans.
In an editorial published the same day in Science, WHO leadership encouraged that all origin possibilities be investigated, including the so-called “lab-leak theory” that the virus inadvertently escaped a laboratory in Wuhan. Notably, the previous WHO investigation deemed that theory “very unlikely.” Chinese officials continue to encourage researchers to look in other countries for clues but have said they will work within the framework of SAGO. The WHO plans to finalize the SAGO members following a 2-week public consultation period. Although the window of opportunity for finding the origins of the current pandemic is closing, and many questions remain unanswered, learning more about the origins of SARS-CoV-2 could help prevent the next outbreak.
FLU SEASON Medical professionals and public health experts worldwide are urging everyone to receive their flu vaccine in advance of what could be a particularly severe flu season this coming winter. Last year, SARS-CoV-2 appeared to displace most of the circulating seasonal influenza viruses with 1 pediatric flu death in the US for 2020 compared to 75-150 pediatric deaths in previous seasons. This year, experts are warning of a “twindemic” of COVID-19 and flu cases, as pandemic restrictions are easing. Since there were relatively few cases of flu last year, experts worry that immunity against the flu will be lower in the general population this year, potentially resulting in more cases and hospitalizations. Unlike with SARS-CoV-2 vaccines, flu vaccines are approved for children 6 months and older. Combined with effective respiratory disease control measures, such as masking and physical distancing, it is doubly important this year to obtain a flu vaccine. A recent study published in PLoS One suggested that flu shots could have protective effects against COVID-19 severe outcomes. In a retrospective cohort of more than 74,000 patients hospitalized with COVID-19, those who had received a flu vaccine had significantly lower risks of sepsis, stroke, and subsequent emergency department visits for COVID-19-related outcomes. More studies are needed to further examine this possible correlation, but the results are encouraging to solidify the case for all eligible persons to get their flu vaccine.
CUREVAC CureVac announced October 12 that it is withdrawing its first-generation SARS-CoV-2 mRNA vaccine candidate, CVnCoV, from the current approval process with the European Medicines Agency (EMA) to instead focus on developing second-generation mRNA vaccine candidates in collaboration with GlaxoSmithKline (GSK). The company also terminated an advance agreement with the European Commission (EC) for the sale of 405 million doses of the vaccine after approval. The announcement represents the seventh vaccine candidate to be abandoned after clinical trials, in part due to the success of mRNA vaccines from Pfizer-BioNTech and Moderna.
ABUSE OF SCIENTISTS A self-selecting survey by Nature of more than 300 scientists who have spoken publicly about COVID-19 in media interviews or on social media found 15% said they had received death threats, with nearly 60% of those surveyed saying they had faced other forms of harassment or abuse. Notably, most researchers said their experiences with media interviews were positive but those who reported the highest frequency of personal attacks or trolling were also the most likely to indicate a reduced willingness to speak with the media in the future. Nature predicts that these results could have a “chilling effect” on science communication.
by JazzNU Penn State has done a whole lot of nothing in the way of vaccine mandates for faculty, staff, and students up until now, they have only strongly encouraged getting the vaccine, but they will institute a mandate for faculty and staff by December. And it's to be in compliance with Biden's federal mandate. So I thought I'd mention it to give you guys a better idea of the reach of that mandate.
All PSU faculty and staff must be fully vaccinated by December 8th. "Staff" includes full and part time workers, technical service, and any students or graduate students that get paid by the university in any fashion. The mandate applies whether you work on main campus or remotely.
PSU estimated that between labs and other research projects that they have 1,000 federal contracts at the main campus. One thousand. That's just one school (though granted, a very large one). Given this extends to university research, it be will be very difficult for public or private research universities of any size to avoid this mandate. Some are taking the approach that this doesn't apply in that manner, and that's a bold (and dumb) strategy to take with the federal research gravy train universities ride on. We'll see how it plays out. University of Delaware and PSU appear to be two of the first public universities to take this step, private universities have had similar announcements before this. I'm thinking we'll be seeing more announcements because they can't risk it.
by dryrunguy Our tobacco retailer inspection teams will also be required to be vaccinated. That includes inspectors, underage purchasers (ages 16-20 depending on the state or jurisdiction), and chaperones. These are folks that might bill, on average, only 10-15 hours a month to our inspection contracts.
That might not seem like a big deal, but if you take into account the states and jurisdictions where we conduct/will be conducting inspections--Nevada, Idaho, Pennsylvania, Puerto Rico, New Mexico, Oregon, Alaska, Utah, and Wyoming--well, let's just say most of those are not exactly vaccination-enthusiastic parts of the United States.
To further complicate things, our parent company is providing a one-time incentive payment of $500 for all staff who provide proof of vaccination to HR, but that incentive does not extend to on call personnel, which includes any employees who bill less that 50% per month, such as our inspectors, underage purchasers, and chaperones. I'm trying to get that changed, but I'm not feeling particularly optimistic.
by ponchi101 $500 incentive. I paid two tickets to the USA to get vaccinated.
IATA.
by dryrunguy
ponchi101 wrote: ↑Fri Oct 15, 2021 8:45 pm
$500 incentive. I paid two tickets to the USA to get vaccinated.
IATA.
Yup. The dissonance has been mentioned here before. You have people all over the world begging for a vaccine and not even caring if it's a GOOD vaccine.
Meanwhile, in the U.S., you have companies offering employees incentives to get vaccinated, which is free, and instead you have covidiots paying $300 or more for a fake vaccination card.
It makes no sense.
by MJ2004 Halloween 2021
by ti-amie
MJ2004 wrote: ↑Sat Oct 16, 2021 11:20 pmHalloween 2021
by Deuce For games in Canadian cities, all NHL coaches are required to wear a protective mask during games.
For games in U.S. cities, all NHL coaches are NOT required to wear a protective mask during games.
Yet, the COVID-19 virus is more present (per capita) in American cities than it is in Canadian cities...
by ponchi101
MJ2004 wrote: ↑Sat Oct 16, 2021 11:20 pmHalloween 2021
by ti-amie
MJ2004 wrote: ↑Sat Oct 16, 2021 11:20 pmHalloween 2021
I'd argue that those 4 thousand are in more danger from passengers than vice versa.
by dryrunguy I wasn't able to check in here at all yesterday, but I wanted to pass along something Dr. Fauci said yesterday morning during an interview.
In a nutshell, he basically stated that data suggest the J&J vaccine should actually have been a two-dose vaccine. I had seen that suggested before, and the J&J vaccine has consistently lagged behind the other two in terms of overall efficacy. But I have never seen someone of Fauci's stature state it so flatly.
So I'm not sure what that means for me. (I got the J&J stab.)
by Suliso
dryrunguy wrote: ↑Mon Oct 18, 2021 4:01 pm
So I'm not sure what that means for me. (I got the J&J stab.)
dryrunguy wrote: ↑Mon Oct 18, 2021 4:01 pm
So I'm not sure what that means for me. (I got the J&J stab.)
Get a booster from another vaccine.
Sure. But when? I got my vaccine in June, and I don't think I can just run out and get another one without some kind of formalized recommendation or guideline from the FDA.
by Suliso I suspect it will be formally recommended soon and you'll be able to get it before the end of the year.
by JazzNU
dryrunguy wrote: ↑Mon Oct 18, 2021 4:01 pm
I wasn't able to check in here at all yesterday, but I wanted to pass along something Dr. Fauci said yesterday morning during an interview.
In a nutshell, he basically stated that data suggest the J&J vaccine should actually have been a two-dose vaccine. I had seen that suggested before, and the J&J vaccine has consistently lagged behind the other two in terms of overall efficacy. But I have never seen someone of Fauci's stature state it so flatly.
So I'm not sure what that means for me. (I got the J&J stab.)
Yes, but in case you missed it before, him (and other public health experts) think that it is very likely that ultimately, the Pfizer vaccine should've been a three-dose vaccine, hence the booster that's not a booster, but third dosage. No one was working with an ideal timeline on rollout given the severity of the pandemic and had to make a call on what to trial first. For Moderna, they had wondered if there was a way to lessen the dosage and get a similar good results after initial reports of Pfizer's success with a comparatively weaker dosage. But that higher dosage is proving key as Moderna's immunity response numbers are the highest after 6 months and Moderna is the only one that is getting a legitimate booster shot not a third dosage. All of them had something is the point because no one was working on an ideal timeline for rollout.
Watch the news in the next 2 weeks to see what is approved, word is expected from the CDC advisory panel next week and the CDC director could approve it as soon as next Friday. And the FDA panel already recommended a second dose J&J for everyone, not just certain groups, so they'll likely be moving on that soon. But they also have enough data on mixed dosages apparently and might be weighing in on that in a similar timetable. Some areas, most notably San Francisco, have allowed mixed dosages for J&J recipients for a few months now.
What was the name of that Florida woman that was keeping the side-website with the CORRECT figures? Any way to start a Go-Fund-Her, for services rendered?
by dryrunguy Here's the latest Situation Report. It is absolutely packed.
::
BOOSTER DOSES The US FDA’s Vaccines and Related Biological Products Advisory Committee during 2 days of meetings last week considered several questions related to booster doses for SARS-CoV-2 vaccines. The panel’s recommendations are not binding, although the FDA generally follows the advice of its committees.
Moderna
The vaccine advisory panel on October 14 voted unanimously to endorse a booster dose of Moderna’s SARS-CoV-2 vaccine, administered at least 6 months after the second dose. The vote supports authorizing an additional dose of the vaccine in the same groups authorized for a booster dose of the Pfizer-BioNTech SARS-CoV-2 vaccine, including individuals aged 65 and older, those ages 18 to 64 at a higher risk for severe disease, and people at risk of exposure due to their occupation. The advisory panel also discussed when booster doses should be provided to all adults but concluded it is too soon to make that decision. The Moderna booster under consideration is 50μg, half the dose of the initial 2 shots, while the authorized booster for the Pfizer-BioNTech vaccine is the same formulation as the FDA-approved 2-dose vaccine. Moderna claims a half dose is enough to activate the immune system while still stretching the world's supply of available vaccines. Data from Moderna show that the booster dose did not produce the 4-fold antibody increase set as a guideline by the FDA for authorizing boosters, but Moderna said it was because of existing high levels of antibodies in study participants. Some panel members expressed concern over some of the data provided by Moderna—including on how best to measure correlates of protection and durability provided by a half dose—but not enough to prevent endorsement of booster doses. Others noted that avoiding public confusion over which vaccines were approved for booster doses and why played a role in their decision.
J&J-Janssen
During a second day of meetings on October 15, the vaccine advisory panel voted unanimously to endorse a second dose of the J&J-Janssen SARS-CoV-2 vaccine for all recipients. This meeting saw more controversy than previous meetings on booster shots for the Pfizer-BioNTech and Moderna SARS-CoV-2 vaccines, with some panelists reportedly unhappy with multiple slides presented by J&J-Janssen that contained data not previously vetted by the FDA. Additionally, the companies presented data on boosters given at 6 months from a study with a sample size of only 17 volunteers. Panelists expressed frustration with and hesitancy to make a decision based on the limited data, but all the panelists agreed that anyone who received the J&J-Janssen vaccine should be eligible for a second dose, with some saying the vaccine should be considered as a 2-dose regimen. The concerns revolved around data showing that a single dose of J&J-Janssen offered lower protection than 2 doses of either the Pfizer-BioNTech or Moderna vaccines.
Mix & Match
Following its vote on the J&J-Janssen vaccine, the panel discussed the so-called “mix & match” strategy, which could allow heterologous booster doses for certain populations. Data from an NIH study released last week showed that the antibody levels of those who initially received the J&J-Janssen shot rose 76-fold in 15 days following a booster with Moderna and 35-fold after a booster with Pfizer-BioNTech. By comparison, a second dose of J&J-Janssen only raised antibody levels 4-fold in the same timeframe. It is worth noting that there were concerns because the NIH study results were based on a small number of volunteers and only reported short-term findings. Despite these concerns, some panelists claimed the data are enough to convince them to support a mix & match strategy, something that is fairly common in other countries.
The FDA is expected to authorize boosters for some Moderna and all J&J-Janssen vaccine recipients as early as this week and also could make a decision on the mix & match strategy. The US CDC’s Advisory Committee on Immunization Practices (ACIP) is scheduled to meet this week to make its own recommendations on booster doses, meaning millions more people in the US could be eligible for additional shots by the end of the week.
MYOCARDITIS RISK The US FDA has delayed a decision on authorizing Moderna’s SARS-CoV-2 vaccine for adolescents ages 12-17 years to allow more time to scrutinize whether the vaccine is associated with an increased risk of myocarditis, an inflammatory heart condition, particularly among young males. The move comes after several Nordic countries paused the use of the Moderna vaccine for younger males, reportedly due to an increase in reports of myocarditis. A Moderna official said the company has requested data from those countries but has not yet received the information. The FDA has said the risk of myocarditis and pericarditis—inflammation of the heart’s lining—appears to be low following vaccination with either the Moderna or Pfizer-BioNTech vaccines, and that the benefits of the vaccines outweigh the risks. But most of that data come from the vaccines’ use among adults, and the agency appears to be taking extra caution in reviewing the data on adolescents. For parents eager to vaccinate their children, the delay in authorization could increase anxiety over safety concerns or assuage any hesitancy. The timing of the FDA’s decision on the Moderna vaccine is unclear, although regulators are working expeditiously. The Pfizer-BioNTech vaccine is available for use among people aged 12 and older in the US.
US CDC HOLIDAY GUIDANCE The US CDC on October 15 released new public health guidance for 2021 winter holiday celebrations, with a focus on urging those who are unvaccinated against SARS-CoV-2 to get their shots before traveling or gathering with family and friends. To protect those too young to be eligible for vaccination, the agency recommends all those around them to be vaccinated. According to new data released the same day, the CDC noted that in August, unvaccinated individuals had an 11 times greater risk of dying from COVID-19 than those who were fully vaccinated. Like 2020, the CDC also recommended masking when in crowded indoor settings and trying to be outside as much as possible in group settings. The new guidance was released following some confusion earlier this month, when the CDC mistakenly posted old information to its website. Some public health experts warned that as long as there are gaps in vaccination coverage throughout the country, a winter surge in COVID-19 cases remains a possibility, especially if people do not follow the guidance.
US NAVY The US Navy has formed a COVID Consolidated Disposition Authority to facilitate the administrative separation of Navy service members who refuse a SARS-CoV-2 vaccine without a pending or approved exemption. The Pentagon mandated vaccination for all service members in August, after the US FDA granted full approval to the Pfizer-BioNTech SARS-CoV-2 vaccine. According to an unclassified communication, more than 98% of active duty US Navy service members have begun or completed a vaccination series, and all active duty sailors must be fully vaccinated—defined as 2 weeks after completing an authorized or approved vaccine—by November 28. Those in the Navy Reserves must be fully vaccinated by December 28. Any sailor separated only for vaccine refusal will receive “no lower than a general discharge under honorable conditions,” which could mean losing some veterans’ benefits.
EUROPE SURGE COVID-19 is once again surging in Europe, particularly in the UK and Central and Eastern Europe. The daily incidence at the continent level increased by more than 45% since the most recent low on September 16. Over the past 2 weeks, 16 European countries have reported increases in daily incidence of 25% or greater, including Czechia (+102%), Latvia (+118%), and Poland (+123%) with greater than 100%. Additionally, Ireland and the UK reported increases of 23% and 20% over that period, respectively. Europe is exhibiting similar trends in terms of daily mortality as well, with 9 countries reporting biweekly increases of 50% or more, including Poland (+103%), Romania (+109%), and Luxembourg (+300%) with increases of more than 100%. With the exception of Iceland, Ireland, and the UK, nearly all of these countries are located in the Central and Eastern regions of Europe. As Europe transitions to colder weather and winter holidays, major COVID-19 surges could pose additional risk due to increased social activities and gatherings indoors.
Russia surpassed 30,000 new cases per day for the first time on October 17 and continues to set new records for daily incidence. Russia also continues to set new records in terms of daily mortality, now up to 967 deaths per day, more than 75% higher than the previous peak in late December 2020. Reportedly, some Russian researchers have accused the Russian government of manipulating the official data, and they argue that the true figures are much worse. According to a report by The Washington Post, Russia’s official COVID-19 mortality data may “exclude many deaths” that are determined to be a result of other conditions, potentially including those known to be associated with elevated risk of severe COVID-19 disease and death.
On October 18, Latvia announced a 4-week “lockdown” period, including the closure of schools, restaurants, retail stores, and entertainment venues. Only essential services and activities will be permitted during the lockdown, and essential employees who need to work in person are required to be vaccinated. Additionally, Latvia’s COVID-19 restrictions include a curfew from 8pm-5am, with limited exceptions for traveling to or from work or receiving medical care. All schools will remain closed through October 29, and in-person classes are scheduled to resume on November 1 for grades 1-3 and November 15 for grades 4-12. The Latvian government intends to begin relaxing the lockdown measures on November 15, but initially only in “green” areas (ie, those with lower SARS-CoV-2 transmission) and only for fully vaccinated individuals.
AFRICA The WHO Regional Office for Africa (AFRO) last week estimated that only about 1 in 7 COVID-19 cases is being detected on the continent and suggested the actual cumulative COVID-19 incidence in Africa as of October 10 was about 59 million, and not the 8 million cases in official reports. In order to get a better understanding of the pandemic in Africa, the WHO announced a new initiative aimed at increasing testing access in 8 countries, with the hopes of reaching as many as 7 million people with rapid diagnostic tests in the next year. Burundi, Côte d'Ivoire, the Democratic Republic of Congo, Guinea-Bissau, Mozambique, the Republic of Congo, Senegal, and Zambia will each receive US$1.8 million to scale up testing and preventive measures using a “ring strategy,” which focuses on providing voluntary testing, face masks, and hand sanitizer to people who live within 100 meters of a confirmed COVID-19 case. The strategy successfully helped to contain and eradicate smallpox from the continent in the late 1970s, and a ring vaccination strategy has been used to contain Ebola in recent outbreaks, so it will be interesting to see how the approach works with COVID-19.
Only about 5% of the total African population is vaccinated against SARS-CoV-2, with only 30% of the continent’s 54 nations having fully vaccinated 10% of their population. In a White House meeting with Kenya President Uhuru Kenyatta, US President Joe Biden on October 14 said the US will donate an additional 17 million doses of the J&J-Janssen vaccine to the African Union (AU). The donation, which is available for delivery immediately, adds to 50 million vaccine doses already donated by the US to the AU. However, the US donation is a drop in the bucket of what is needed. In September, WHO Africa estimated that an average 150 million doses need to be delivered to the continent each month if it is to fully vaccinate 70% of the population by September 2022.
SPUTNIK V People living with HIV are at elevated risk of severe or critical COVID-19 disease and death, according to the WHO. Additionally, some researchers have long warned that vaccines that use a specific adenovirus (Ad5) vector could increase the risk of contracting HIV among certain populations. The South African Health Product Regulatory Authority this week said it would not authorize Russia’s Sputnik V vaccine, which uses Ad5, over concerns it could increase the risk of HIV infection among males. The agency said the company that makes Sputnik V did not supply data showing the vaccine is safe when used in areas with high HIV prevalence. South Africa ranks first among all countries for the greatest number of people living with HIV. Notably, South Africa currently offers the J&J-Janssen vaccine—which also uses an adenovirus vector, albeit a different type (Ad26)—as well as the Pfizer-BioNTech and Chinese-made Sinovac vaccines. The Sputnik V vaccine is used in at least 50 countries worldwide but has not yet received emergency use listing status from the WHO.
EFFICACY OF INTERFERON The immunomodulator interferon beta-1a used together with the antiviral remdesivir was no better at treating hospitalized adults with COVID-19 pneumonia than remdesivir alone, according to the results of a study supported by the US NIH. Researchers assigned 969 patients recruited in 63 hospitals across 5 countries 1:1 to receive the study treatment plus remdesivir or a placebo plus remdesivir. According to the results, published online in The Lancet Respiratory Medicine, interferon plus remdesivir was not superior to remdesivir alone, and patients who were on high-flow oxygen at the beginning of the study and took interferon had worse outcomes compared with those who took only the antiviral, possibly due to interferon increasing their inflammatory response.
ABBOTT TEST RECALL Abbott Molecular is recalling 2 of its SARS-CoV-2 laboratory test kits because they have the potential to issue false-positive results, and the US FDA classified it as a Class I recall—the most serious type of recall. The issue is related to the software used with the Alinity m SARS-CoV-2 AMP Kits and Alinity m Resp-4-Plex AMP Kits, and until the software can be updated, positive results should be treated as presumptive, according to the regulatory agency. The FDA previously warned clinical lab staff and healthcare providers of the potential for false positives and urged users to promptly report any adverse events associated with the tests.
dryrunguy wrote: ↑Mon Oct 18, 2021 4:01 pm
So I'm not sure what that means for me. (I got the J&J stab.)
Get a booster from another vaccine.
Sure. But when? I got my vaccine in June, and I don't think I can just run out and get another one without some kind of formalized recommendation or guideline from the FDA.
If you come to the Bay Area, you can. For free. It will take you a total of 1 minute to make an appointment online at Walgreen's and then go the next day. Just sayin'
Kevin
by ti-amie
by ti-amie
by ponchi101 I hate to say this, but maybe MT Greene is right. The country may have to split.
I have a vaccination card that is like 5 pages long. If somebody asks me to have another, what the hell, it is for my benefit. Not that hard to understand.
All the heath and safety regulations they have to follow to keep their doors open and they can't just place someone at the door to check cards? Everyone trying to get some attention with this BS. I seriously doubt the majority of these businesses had the same public outrage at enforcing the no smoking ban.
by ti-amie My sympathy quotient is running on fumes when it comes to covidiots.
by JazzNU
by ti-amie
by ti-amie
Keep in mind most of the people who work for both organizations don't live in NYC proper. they live mostly on Long Island and in Rockland County. If they live in the city it's mostly on Staten Island.
by ti-amie
by Suliso A front runner for the Republican nomination in 2024, isn't he? That is assuming Trump doesn't run.
by Togtdyalttai
Suliso wrote: ↑Tue Oct 26, 2021 12:45 am
A front runner for the Republican nomination in 2024, isn't he? That is assuming Trump doesn't run.
All indications currently are that Trump will run. If not, DeSantis is technically probably the frontrunner, but that means very little this far out.
Suliso wrote: ↑Tue Oct 26, 2021 12:45 am
A front runner for the Republican nomination in 2024, isn't he? That is assuming Trump doesn't run.
All indications currently are that Trump will run. If not, DeSantis is technically probably the frontrunner, but that means very little this far out.
Do most people here think that Trump will get the nomination if he runs?
Kevin
by MJ2004 [quote="dmforever”]
Do most people here think that Trump will get the nomination if he runs?
Kevin[/quote]
Replace “if” with “when” and does a bear s*** in the woods?
by ponchi101 The only options that lead to him not running:
1. The burgers and poor diet do their job.
2. Major, MAJOR stroke, destroying the remaining 10% of his brain that seems to work (the one set to STUPID).
3. Prison, and even then, he will be put in the ballot.
Not only he will run and get nominated. Anybody running AGAINST him will be labeled a traitor and will suffer severe consequences (within the GOP). And if for some reason he can't run, he gets to anoint the successor.
His followers make Scientologists and Ayn Rand's followers look cerebral and independent.
by dryrunguy Here is the latest Situation Report.
::
Webinar Available: The COVID-19 pandemic has shown that accurate and timely health-related information is crucial to mounting an effective response to a public health crisis. As can be seen in setbacks during the COVID-19 response, health-related misinformation and disinformation can lead to more infections, deaths, disruption, and disorganization of the effort. The latest session of The Capitol Hill Steering Committee on Pandemic Preparedness & Health Security, titled “Combating Misinformation and Disinformation for COVID-19 and Future Public Health Threats,” evaluated the role misinformation has played in health emergencies and offered solutions to increase trust in future public health messaging. A recording of the webinar is available for viewing.
VACCINES FOR CHILDREN The US FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) is meeting today to consider recommending the authorization of the Pfizer-BioNTech SARS-CoV-2 vaccine for children ages 5 to 11 years. Last week, the FDA posted Pfizer-BioNTech’s briefing on the vaccine for this age group, which suggested a 2-dose series of 10μg shots delivered 3 weeks apart—one-third of the adult dose—was 91% effective in preventing symptomatic disease among this younger age group, with low incidence of adverse events. The companies said no cases of heart inflammation were reported in 3-months follow-up after the second shot, although the study population was small. In its own briefing, the FDA said the benefits of the Pfizer-BioNTech vaccine among children ages 5 to 11 clearly outweigh the risks of potential side effects. The FDA’s advisory committee is expected to recommend authorizing the lower-dose Pfizer-BioNTech vaccine for young children today. After the FDA issues a final decision—which usually follows the recommendations of its advisors—the US CDC Advisory Committee on Immunization Practices will make recommendations at its next meeting, scheduled for November 2-3. Following the approval of those recommendations by CDC Director Dr. Rochelle Walensky, children ages 5 to 11 could become eligible for SARS-CoV-2 vaccination by November 3-4.
According to 2 recent studies—one published in the New England Journal of Medicine (NEJM) and the other in the CDC’s Morbidity and Mortality Weekly Report (MMWR)—the Pfizer-BioNTech vaccine is effective at preventing symptomatic COVID-19 disease and related hospitalization in adolescents aged 12 to 18 years. The studies demonstrate the importance of vaccines in protecting children from COVID-19, and they could factor into today’s FDA advisory committee meeting.
On October 25, Moderna announced interim results from its Phase 2/3 KidCOVE study evaluating its SARS-CoV-2 vaccine in children aged 6 to 11 years. According to the company, the data—which are not yet published or peer-reviewed—showed that participants in the 6- to 11-year-old range had a robust immune response to a 2-dose 50μg regimen delivered 4 weeks apart. Side effects included mild to moderate symptoms such as fatigue, fever, headache, and pain at the injection site. The company indicated plans to submit their data to US and European regulators soon, although there is no indication when the FDA might review the vaccine for use in children. Moderna’s vaccine currently is authorized for use in adults, and it is awaiting a response from the FDA to its June request for authorization for children aged 12 to 17.
US TRAVEL POLICIES On October 25, US President Joe Biden issued a proclamation on international air travel requiring nearly all inbound international travelers to be fully vaccinated. Notably, there are exceptions to the new policy: children under 18, those with certain medical conditions, and non-tourists traveling from specific countries with low vaccine access will instead be required to report a negative COVID-19 test prior to departure. There are no religious exemptions for inbound passengers, according to the US CDC, which issued new contact tracing rules the same day. Those travelers staying in the US are expected to receive a vaccine within 60 days, a decision which takes advantage of the large repository of vaccine doses in the country. The travel industry is welcoming these changes to the existing regulations, which issued travel restrictions on a country-by-country basis. With a more uniform travel policy, airlines are looking forward to simpler implementation and logistics moving forward. The new air travel policy will take effect on November 8, and more details on a similar plan to lift travel restrictions on land border crossings are expected later this week.
Additionally, the CDC extended its Framework for Conditional Sailing Order through January 15, 2022. While the CDC makes important recommendations for other forms of travel, CDC maintains authority over whether or not cruise ships are allowed to operate in US waters. Given the short, but fraught, history of COVID-19 on cruise ships, the CDC has taken many steps to work with the cruise ship industry to ensure the safety of passengers and crew. The Framework for Conditional Sailing Order was initially implemented in October 2020 following the expiration of the CDC’s No Sail Order. Since then, the cruise industry has adopted numerous COVID-19 prevention measures, such as masking and testing requirements. The temporary extension states that CDC intends to transition to a voluntary program upon the conclusion of the extension deadline, which will involve close coordination between the CDC and the cruise industry.
US BOOSTER DOSES Tens of millions more people in the US became eligible for SARS-CoV-2 vaccine boosters last week following CDC Director Dr. Rochelle Walensky’s endorsement of the agency’s Advisory Committee on Immunization Practices’ (ACIP) recommendation for booster shots in certain populations. Now, all 3 of the vaccines approved or authorized in the US—all of which remain highly effective in reducing the risk of severe disease, hospitalization, and death—are available for additional or booster doses among certain populations. For those who received primary shots with either the Pfizer-BioNTech or Moderna vaccines, booster doses are available 6 months after the initial series for individuals aged 65 or older and those aged 18 or older who live in long-term care settings, have underlying medical conditions, or work or live in high-risk settings. The Moderna booster is half of the initial shots (50 μg versus 100 μg), while the Pfizer-BioNTech booster is the same dosage. Anyone who received the J&J-Janssen vaccine is eligible to receive a booster dose 2 months following their initial shot. Additionally, the CDC’s recommendations allow for people to choose which of the 3 available vaccines they get for a booster, a strategy known as “mix & match” or heterologous dosing. Notably, health experts emphasized that anyone who received 2 mRNA vaccine doses or a single J&J-Janssen dose are—for now—considered fully vaccinated. Several members of the FDA and CDC advisory panels expressed frustration over the limited data on the safety and efficacy of boosters, how questions were posed to the committees, and a burden to approve the extra doses after they were promised by US President Joe Biden in August.
GLOBAL VACCINE ACCESS The US government has now delivered 200 million SARS-CoV-2 vaccines to more than 100 countries, out of a pledge of 1.1 billion doses. A US Department of State official said many of the donated doses are surplus supply and more needs to be done to increase supply to low- and middle-income countries (LMICs), including manufacturers increasing production and other countries donating excess shots. Notably, the US government continues to deny requests from state or local governments to donate soon-to-expire doses to countries in need. In an agreement facilitated by the US government, Moderna announced it will make up to 110 million of its vaccine doses available at the lowest price to the African Union. The US undoubtedly is a leader in global vaccination efforts, but the government—and other wealthy countries—can and should do more to improve access in LMICs, public health advocates urge.
During comments to reporters last week, White House Principal Deputy Press Secretary Karin Jean-Pierre called on all World Trade Organization (WTO) member states to support a proposal to temporarily waive intellectual property rights for COVID-19 medical products, including vaccines. Formal talks on the proposal—which is endorsed by more than 100 countries—are stalled despite US backing. Notably, 2 senior officials in the administration of US President Joe Biden told The Washington Post that the government lacks the authority to share technology of Moderna's SARS-CoV-2 vaccine, despite the company receiving nearly US$10 billion in federal funding to develop, research, and expand manufacturing of the shots. Last week, the WHO urged the G20 nations, which are holding a summit this week, to increase vaccine donations, and finance ministers from member states of the Asia-Pacific Economic Cooperation (APEC) agreed to take steps to support equitable distribution of vaccines and expand manufacturing. The Kaiser Family Foundation (KFF) updated its Global COVID-19 Vaccine Coverage Tool on October 25, providing data on vaccine coverage by country, income-level, region, and globally, as well as estimates on future vaccine coverage levels.
HEALTHCARE WORKERS As many as 180,000 healthcare workers died of COVID-19 between January 2020 and May 2021, according to estimates from a WHO working paper, which urged nations worldwide to do more to support and protect healthcare workers amid the pandemic. In addition to calling for better access to vaccines for healthcare workers—only 2 of 5 are fully vaccinated globally, with greater disparities between poor and wealthy nations—the WHO warned that an increasing proportion of the workforce faces burnout, stress, anxiety, and fatigue, and the industry faces a worker shortage. A study published in the November issue of the American Journal of Nursing shows that in 2017, prior to the pandemic, 5.5% of 7,378 nurse survey respondents reported having suicidal ideation within the past year, and other surveys have shown that 25% to 50% of healthcare providers report high stress, anxiety, work overload, or symptoms of burnout. In the US, which needs more nurses, shortages in nursing school instructors, clinical sites, and financial resources has led to a bottleneck in available slots for students.
AY.4.2 VARIANT UNDER INVESTIGATION The UK Health Security Agency last week designated the Delta sublineage AY.4.2—commonly known as “Delta Plus”—as a Variant Under Investigation (VUI) and officially named the variant VUI-21OCT-01. The agency made the designation because the sublineage has become increasingly common in the UK in recent months, accounting for approximately 6% of all sequenced Delta cases. Currently, there is no evidence AY.4.2 causes more severe disease, although 2 mutations on the spike protein—A222V and Y145H—could be contributing to an increased growth rate, but more evidence is needed. COVID-19 cases caused by the Delta sublineage have been detected in at least 118 countries, including the US, India, Israel, and Russia. At a briefing last week, US CDC Director Dr. Rochelle Walensky said health officials are keeping an eye on the sublineage but that so far there is no evidence it impacts the effectiveness of vaccines or available treatments.
NEUROLOGICAL IMPACTS Many people who recover from COVID-19 suffer various symptoms of cognitive dysfunction, commonly known as “brain fog,” although the prevalence and severity of these symptoms are not well-known. In a research letter published in JAMA Open Network, researchers from the Icahn School of Medicine at Mount Sinai in New York (US) describe results from a study examining rates of cognitive impairment among 740 COVID-19 survivors who were treated in outpatient, emergency department, or inpatient hospital settings between April 2020 and May 2021. They found that up to nearly one-quarter of recovered patients continue to experience some sort of cognitive impairment 7 months post-infection, including problems with memory, processing speed, executive functioning, attention, or phonetic and category fluency. The researchers note the “considerable implications” for COVID-19 patients’ long-term rehabilitation and occupational, psychological, and functional outcomes. Even younger patients, in their 20s, 30s, and 40s, who had milder cases of the disease reported cognitive impairments, potentially heavily impacting their ability to engage in work, community, and family activities.
Another study published last week in Nature Neuroscience describes how SARS-CoV-2 can damage small vessels in the brain, potentially leading to neurological symptoms in COVID-19 patients. The team of European and US researchers suggest a potential therapeutic target to potentially treat or prevent long-term neurological symptoms of COVID-19.
ASTRAZENECA-OXFORD VACCINE A recent study published in Nature Medicine reports an association between the AstraZeneca-Oxford SARS-CoV-2 vaccine and Guillain-Barre Syndrome (GBS), a rare neurological condition. Researchers estimated that there were 38 extra cases of GBS per 10 million persons receiving the AstraZeneca-Oxford vaccine. The same study also estimated that there were 145 extra cases of GBS per 10 million persons with a positive COVID-19 test. Importantly, while there are some rare complications associated with SARS-CoV-2 vaccines, it appears that the risk of developing these neurological complications is much higher following natural infection with SARS-CoV-2. The study also examined the same outcomes among people who received the Pfizer-BioNTech vaccine, but there was no significant association between this vaccine and GBS. There was, however, a positive association between the Pfizer-BioNTech vaccine and hemorrhagic stroke. The European Medicines Agency previously added GBS as a possible adverse event to the AstraZeneca-Oxford vaccine, and the UK added the warning last week. These new findings support the overall safety of vaccines against SARS-CoV-2 and the importance of protecting oneself against the worst outcomes of infection.
CHINA Chinese health officials announced new lockdowns and other measures to contain several local SARS-CoV-2 outbreaks, with the average number of daily new COVID-19 cases more than doubling since October 16. Officials warned the outbreaks, mainly in the northern part of the country, are expected to worsen. Marathons in Wuhan and Beijing were postponed, with organizers citing the safety of runners, staff, and residents. On October 25, health officials announced children as young as 3 years old will be eligible for vaccination, with at least 5 provinces announcing compulsory vaccination for children. SARS-CoV-2 vaccines from both Sinopharm (2 versions) and Sinovac are authorized for use in children, however the shots have only been used among individuals aged 12 and older until now.
China is one of only a few countries continuing to enforce a zero-COVID policy, and the Chinese government is concerned the outbreaks will spread into Beijing, where the 2022 Winter Olympics are set to begin in February. According to new guidelines released this week, athletes at the games must be vaccinated to avoid a 21-day quarantine, will need to take daily SARS-CoV-2 tests, and will be restricted to a closed loop system dictating travel between venues and interactions with other participants. China already has said international spectators will not be allowed at the Olympics, which are set to run from February 4-20. About 75% of the Chinese population is fully vaccinated, and those who received their last dose at least 6 months ago are eligible for a booster dose.
by ponchi101 About "Covid Fog". My sister tells me that she feels it a little bit, not a desirable condition for a therapist. She has had the disease twice (she had just received her Sputnik V second dose when she developed the second bout, and initially thought it was a reaction to the vaccine) and is doing fine, but feels that at times her memory is still a bit jumbled.
by ti-amie I get my booster next Wednesday. I had covid fog from both of my Pfizer shots but being aware of it helped deal with it. It disappeared after a few days.
Also, my doctor said to allow two weeks between the booster and the flu shot. That is not how it's being "sold" to the public.
by Deuce
ti-amie wrote: ↑Wed Oct 27, 2021 7:07 pm
Also, my doctor said to allow two weeks between the booster and the flu shot. That is not how it's being "sold" to the public.
I've heard a few medical people say that one should leave time (it varies from a few days to a few weeks) between getting the flu vaccine and the COVID vaccine.
But I've also heard an equal number of medical people - or even more - say that it's fine to get them both at the same time, because they don't interact.
I assume the advice to get them at the same time would be for people who've already had both the flu and the COVID vaccines, and know that they have had no significant reaction to either. While it's true that the flu vaccine varies from year to year, I assume the primary ingredients are consistent enough so that if some sort of negative reaction is to occur, it will likely occur the first time - and if it doesn't, it's unlikely to occur with subsequent flu shots.
by MJ2004 My aunt in Spain was administered both the booster and the flu shot at the same time. That is standard practice there and I don't believe there's any evidence not to.
That said, I personally would prefer to practice an abundance of caution and space them two weeks apart.
by dryrunguy My guess is that, since there are so many people in the U.S. who have not been vaccinated for COVID coupled with large segments of the U.S. population that do not get vaccinated annually for the flu, and since there is almost certainly significant overlap among those two groups, public health officials are encouraging folks to go ahead an get both. But my other guess is that anyone who refuses to get one vaccine will probably refuse to get the other.
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 244.9 million cumulative cases and 4.97 million deaths worldwide as of October 28. Global weekly incidence increased by 4.81% compared to the previous week, and mortality increased by 5.27%. After falling the previous week, these increases show the curve trending upward again, with numbers of new cases and deaths close to where they were at the end of September.
Global Vaccination
The WHO reported 6.7 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of October 25. A total of 3.8 billion individuals have received at least 1 dose, and 2.85 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations reached a recent high on October 23 at 28.3 million and are beginning to fall again, down to 23.67 on October 27.* The global trend continues to closely follow Asia. Our World in Data estimates that there are 3.85 billion vaccinated individuals worldwide (1+ dose; 48.97% of the global population) and 2.99 billion who are fully vaccinated (37.79% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 45.57 million cumulative COVID-19 cases and 737,990 deaths. The current daily incidence average is approximately 68,151 new cases per day and appears to be increasing. Daily mortality appears to be falling again, with an average of 1,098 as of October 26.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 416.2 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend could be beginning to rise again after falling since October 1, with an average 638,768 vaccines administered as of October 22.* We might expect to see increases in this number after the US government last week authorized booster doses for tens of millions more people. There are 220.9 million individuals who have received at least 1 vaccine dose, equivalent to 66.5% of the entire US population. Among adults, 79.7% have received at least 1 dose, as well as 14.9 million adolescents aged 12-17 years. A total of 191 million individuals are fully vaccinated, which corresponds to 57.5% of the total population. Approximately 69.1% of adults are fully vaccinated, as well as 12.45 million adolescents aged 12-17 years. Since August 13, 14.4 million fully vaccinated individuals have received a booster or additional dose of vaccine, including 19.2% of fully vaccinated adults aged 65 or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
PEDIATRIC VACCINE As expected, the US FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) on October 26 voted to recommend the regulatory agency issue an Emergency Use Authorization (EUA) for the Pfizer-BioNTech vaccine to be available for 28 million US children aged 5 to 11 years. The vote was 17 in favor with one abstention. The FDA is expected to follow the panel’s advice in the coming days, although it is not bound to do so. After the FDA’s decision, the US CDC’s Advisory Committee on Immunization Practices (ACIP) will take up the issue at its next meeting, scheduled for November 2-3. The CDC Director would then issue the agency’s final guidance, potentially making pediatric vaccinations available by the end of next week. The US government has 15 million doses ready to immediately ship to states for distribution to pediatrician offices, hospitals, and pharmacies, and Pfizer-BioNTech announced today that the US has purchased an additional 50 million pediatric doses, which are one-third the dose of the version authorized for people aged 12 and older. Researchers say a SARS-CoV-2 vaccine for children will save lives in that age group and could help keep overall case counts lower, especially if a new variant of concern emerges. But some parents remain concerned over the vaccine’s safety. New data from the KFF COVID-19 Vaccine Monitor show parents of 5- to 11-year-olds are about evenly split, with about 30% saying they will get the shots for their children, one-third saying they will wait, and 30% saying they will definitely not allow their children to get the vaccine.
FOURTH DOSE FOR SOME WITH IMMUNOCOMPROMISE The US CDC updated its guidance on SARS-CoV-2 vaccine booster doses for people who are moderately or severely immunocompromised. Those individuals who received an initial 2-dose series with an mRNA vaccine (Pfizer-BioNTech or Moderna), followed by a third, or “additional,” dose after ≥28 days, may receive a fourth shot—this one considered a booster dose versus the additional dose—at least 6 months after the third dose with any available booster dose (full dose of Pfizer-BioNTech or J&J-Janssen or half dose of Moderna). The agency advised any moderately or severely immunocompromised individual who initially received a single dose of the J&J-Janssen vaccine should receive a single booster dose of any vaccine booster at least 2 months after the initial shot. Notably, if the person initially received the J&J-Janssen shot, they should not receive more than 2 vaccine doses at this time. An estimated 2% of the US population—about 9 million people—are considered to be moderately or severely immunocompromised.
PANDEMIC CONTINUES During its ninth meeting regarding COVID-19, a WHO Emergency Committee of advisors agreed that the pandemic is “far from finished,” 21 months after the group initially named the disease a public health emergency of international concern (PHEIC). Noting that progress has been made in combating the virus, the group called on the international community to use all available tools to mitigate the pandemic’s impacts and recognized the additional burden on addressing humanitarian emergencies, population migration and displacement, and other crises. The committee also expressed concern over challenges responding to the pandemic in the Africa region, including access to sufficient vaccines, diagnostics, and treatments, as well as adequate surveillance and monitoring capabilities. COVID-19 likely will move from a pandemic to an endemic disease at some point in the future, although experts agree that the benchmarks for determining endemicity are unclear. The WHO Emergency Committee will meet again in 3 months, or sooner as needed, to reevaluate the state of the COVID-19 pandemic.
MERCK LICENSING DEAL Merck and the Medicines Patent Pool (MPP) announced a voluntary licensing agreement that will allow MPP to issue sublicenses to permit manufacturers—mostly in Africa and Asia—to make and distribute Merck’s investigational antiviral COVID-19 treatment in 105 low- and middle-income countries (LMICs), following necessary regulatory approvals. Merck is developing the drug, named molnupiravir, in partnership with Ridgeback Biotherapeutics, which acquired the license for the drug from inventor Emory University. Under the deal, Merck, Ridgeback, and Emory will not receive royalties for sales of molnupiravir in LMICs as long as the WHO continues to classify COVID-19 as a public health emergency of international concern (PHEIC). Merck will continue to make the drug for wealthy nations and some middle-income countries, selling it at significantly higher prices. Merck previously licensed production of molnupiravir to several generic drug manufacturers in India, but made the deal with MPP so as not to rely too heavily on production in a single region.
Earlier this month, Merck announced interim Phase 3 clinical trial data showing molnupiravir, which is administered orally, reduced the risk of hospitalization or death by about half in people with mild-to-moderate COVID-19. The companies applied to the US FDA for Emergency Use Authorization (EUA), and the European Medicines Agency (EMA) announced this week it launched a rolling review of the antiviral. If approved for use, the easy-to-administer pill will be the first available that does not need to be administered by injection or infusion and could help curb COVID-19 outbreaks and alleviate pressure on healthcare systems by helping people recover at home. Health experts have voiced concerns over the potential for inequitable distribution of molnupiravir, but this deal, and a US$120 million pledge from the Gates Foundation to support access to the drug for lower-income countries, provide some hope that the rollout of the treatment will not follow along the lines of the vaccines.
BIONTECH VACCINE MANUFACTURING IN AFRICA BioNTech, which developed the Pfizer-BioNTech SARS-CoV-2 vaccine, announced this week it has signed agreements with Senegal and Rwanda to build mRNA vaccine manufacturing facilities, with construction on at least one plant to begin mid-2022. Initially, BioNTech will own and operate the facility, which will be able to produce up to 50 million vaccine doses annually, with capacity expected to expand. Dr. Matshidiso Moeti, Director of the WHO Regional Office for Africa, said the state-of-the-art facilities could be “game-changers” for the continent, although much needs to be done on the continent to improve vaccine access. Health advocates welcomed the announcement but said the effort is too little, too late. Only 6% of the African population is fully vaccinated, and only 5 nations—less than 10% of the continent’s 54 countries—will reach the year-end target of fully vaccinating 40% of their people, WHO announced today. The UN also warned that limited access to necessary commodities—such as auto-disable syringes used to administer the Pfizer-BioNTech vaccine—could further slow the vaccines’ rollout in Africa.
MORTALITY TRENDS Overall, the risk of death from COVID-19 increases with age. But according to a working paper published by the World Bank Group, this reality varies depending upon where one lives. In high-income countries, COVID-19 deaths generally are concentrated among people over age 65, with only 11% of both official deaths and excess deaths occurring among people younger than age 65. In the upper-middle-income nations for which data were available, the mortality curve became flatter, with 40% of official deaths and 37% of excess deaths occurring among people younger than 65. Among the lower-middle-income nations that had available data, 54% of official deaths were among those under age 65.* Notably, the US has a much younger profile of death—for both official COVID-19 deaths and excess mortality—than countries with similar income levels, even after controlling for differences in population age distribution. With flatter mortality curves, developing countries face the loss of large numbers of people of working age, many of whom provided income to their families or were caregivers to children or family members. These losses likely will have long-term social and economic impacts on these nations into the future and underline the importance of equitable vaccine and resource distribution to close the gaps between wealthy and poorer nations.
*Data for excess deaths were not available for lower-middle-income countries, and no data were available for any low-income countries.
FLUVOXAMINE A study published in The Lancet Global Health showed the inexpensive antidepressant fluvoxamine lowered the odds of hospitalization and death when administered to COVID-19 patients early in their symptom onset. The trial, conducted in Brazil, included 741 individuals who received fluvoxamine and 756 who received placebo, 58% of whom were female, and the cohort had an average age of 50. The study included only high-risk patients and those who enrolled were largely unvaccinated, raising questions about the antidepressant's applications as a therapeutic among vaccinated individuals. Additionally, the study mentioned that some patients were unable to fully tolerate the intended study dosage, raising concerns about the most beneficial dose. Nonetheless, the study results represent positive news in continuing global efforts to reduce the need for COVID-19 hospitalization in a more accessible manner. The current cost of a 10-day course of fluvoxamine is about $4, significantly lower than many of the options currently used to treat COVID-19.
AT-HOME RAPID TESTS Earlier this week, the US HHS announced the agency is expanding its efforts to make at-home COVID-19 testing more accessible. HHS will invest US$70 million to help developers move through the regulatory process and develop a plan with the US FDA to streamline authorization decisions in an effort to bring more over-the-counter tests to market. At the federal level, there has been a push to increase the accessibility of at-home diagnostics ahead of the winter season. The administration of US President Joe Biden announced these plans as businesses move closer to having to implement a “vaccinate-or-test mandate.” The goal of the announcements are two-fold: to increase the supply of available tests and potentially lower the price threshold which currently limits their widespread usage. The FDA has authorized several at-home test kits.
PANDEMIC PREPAREDNESS The Global Preparedness Monitoring Board (GPMB) is warning world leaders that the window of opportunity to address the COVID-19 pandemic and prepare for future disease outbreaks is quickly closing, as the world begins to move on to other pressing issues. In its third annual report, GPMB says the failures of the COVID-19 pandemic response were markedly bogged down by geopolitical divisions and closed-door negotiations that neglected to include key stakeholders. GPMB called for renewed international cooperation and outlined 6 recommendations. In November 2021, the World Health Assembly will hold a special 3-day session to discuss the plausibility of developing a "pandemic treaty."
In the US, discussions over the federal government’s response to COVID-19 have been sidelined in the US Congress, as negotiations over US President Joe Biden’s domestic agenda and the federal budget take precedence. Efforts to present a bipartisan bill in the US Senate to bolster pandemic preparedness have been postponed until later this year or early 2022. Public health experts are advocating for improvements to data collection systems and supply chain vulnerabilities that continue to present significant challenges during the COVID-19 pandemic. The Biden administration has indicated it is prioritizing global health security, earlier this month releasing an annual report on strengthening the Global Health Security Agenda (GHSA).
FINANCIAL DRAIN ON HOSPITALS The COVID-19 pandemic has exacerbated existing inequities in healthcare systems and exposed disparities in funding allocations. In a recent study published in JAMA, researchers examined how US federal COVID-19 relief funding was allocated, how CARES Act funding was utilized, and disparities in funding allocations. They found that academic-affiliated hospitals, hospitals with higher pre-pandemic assets, and hospitals with higher numbers of COVID-19 cases received higher levels of funding, while critical access hospitals received lower levels of financial assistance. The lack of transparency behind CARES Act funding allocation possibly resulted in resource-limited hospitals suffering under the demands of the pandemic, and the researchers emphasized the need to base funding allocations on hospitals’ pre-disaster finances in future resource allocations. Hospitals also took an economic hit due to the postponement of elective surgeries during the beginning of the COVID-19 pandemic, according to 2 studies presented at a conference of the American College of Surgeons (ACS). One healthcare system lost 42% of its net revenue in 2020 after delaying surgeries from mid-March to July 2020, while US children’s hospitals lost $1.53 billion due to delays or cancellations of pediatric surgeries. The researchers said the results show the need for long-term financial planning and preparations for sustained operations management during crises.
by JazzNU I took an antibody test last week to see if my numbers were decent enough where I could be comfortable with delaying the booster shot for a little bit. Among other things, I want to see more information about mixing and matching and whether that's something I should consider for this booster shot. To my shock, my numbers were much better than I was expecting to see, higher than what I had in my mind said I'd be happy with and more than I had wished for in a best case scenario.
Got my flu shot about 3 weeks ago. Initially the CDC wanted vaccines to be 2 weeks apart, but they said that was precautionary as they studied the interactions more and there wasn't data supporting giving them at once being a problem so they updated the advisory language. BUT, I can have reactions to either and don't need to test out the scenario of dealing with that at once so it was never in the cards for me. It was a good plan, I had a reaction to the flu shot for the first time in several years.
by ponchi101
dryrunguy wrote: ↑Thu Oct 28, 2021 4:40 pm
PANDEMIC PREPAREDNESS The Global Preparedness Monitoring Board (GPMB) is warning world leaders that the window of opportunity to address the COVID-19 pandemic and prepare for future disease outbreaks is quickly closing, as the world begins to move on to other pressing issues. In its third annual report, GPMB says the failures of the COVID-19 pandemic response were markedly bogged down by geopolitical divisions and closed-door negotiations that neglected to include key stakeholders. GPMB called for renewed international cooperation and outlined 6 recommendations. In November 2021, the World Health Assembly will hold a special 3-day session to discuss the plausibility of developing a "pandemic treaty."
Yes. The world needs to address other things. CC, world automation and the related drop in employment, specially for youth, the rise of totalitarian regimes around the world, and some other things.
Yes, the pandemic is very important. But not all policies and resources have to revolve around it.
by Suliso After about 14 months the company I work for has decided that masks at work are no longer required. They were already only partially required (not while sitting at your desk) since September. We'll see how it goes, our site is 85% fully vaccinated but outside it's significantly less and the numbers are going up again.
by Suliso‘People are starting to wane’: China’s zero-Covid policy takes toll
Latest Delta variant outbreak is testing the limits of people’s patience with aggressive containment measures
Helen Davidson in Taipei and Vincent Ni, China affairs correspondent
Sat 30 Oct 2021 10.00 BST
On Friday, the Beijing Daily published an intricate graphic identifying two people sick with Covid-19 and everyone they had infected, detailing the spread of the latest Delta outbreak in the country. The map came amid growing frustration, some panic, and rare protests over the ramifications of China’s effort to remain a “zero Covid” country.
Since the first coronavirus cases were reported nearly two years ago, China has run a zero-tolerance Covid policy. Its success in preventing the virus from spreading across the vast country serves as a stark contrast to the situations in many western countries. Since last year, fewer than 100,000 cases have been officially recorded, among a population of about 1.4 billion. At least 4,634 have died.
By comparison, the US has reported nearly 46m cases and more than 740,000 deaths. The UK has reported nearly 9m cases and more than 140,000 deaths.
But the policy is intense. For just a handful of cases, measures have included strict border closures, localised lockdowns, travel restrictions, and the mass testing of tens of millions of people. Homebound flights booked by Chinese citizens who live abroad are often cancelled at the last minute.
On Thursday, a high-speed train from Shanghai was ordered to halt midway before arriving in Beijing, after an attendant was identified as a close contact of a Covid-positive patient. All the other 211 passengers onboard were immediately quarantined in designated places.
But as the world begins to slowly open up, having decided to live with the virus mitigated by vaccinations, China is one of the few still clinging to a strategy of elimination. Analysts and health experts are starting to ask how long it can last, and the latest outbreak – which began early this month – is again testing the limits.
As of Friday the latest Delta outbreak had infected more than 300 people across 12 provinces, including the capital, Beijing, in little more than a week. The outbreak is centred on the province of Inner Mongolia but was linked to travellers.
In response authorities again launched mass testing, halted transportation and enacted local lockdowns.
“Such scenes have become a norm in recent months,” said Yanzhong Huang, a China public health policy expert at the Council on Foreign Relations in New York. “It’ll get more and more difficult over time. But costs are getting higher, and returns are diminishing quickly.”
On Chinese social media, while the majority of commenters support the government’s approach, frustration is also being voiced in Beijing, where one resident said fear had returned to their daily life, while another described people “panicking” as the situation there gets more tense.
“There is banning of dining and lockdowns everywhere. It is too difficult to even just eat normally,” said another resident.
There is also frustration in Ejina Banner in Inner Mongolia, where trapped tourists have posted on social media in recent days.
On Saturday, one tour leader said his guests had been stranded for six days and some elderly participants were running out of medicine. One alleged some guests were showing symptoms but there was no medical institution nearby. “It seems Ejina Banner doesn’t care about people’s life or death,” they said.
“People are starting to wane,” said Prof Chunhuei Chi, the director of Oregon State University’s centre for global health. “As with anywhere in the world we can see dragged into this pandemic for nearly two years, and everywhere we observe pandemic fatigue. That would surely also be affecting Chinese people.”
The current crisis is the second major outbreak of the highly transmissible Delta variant this year; both spread to multiple cities. The first reportedly sparked rare social unrest in Yangzhou this summer, over a government failure to deliver food to residents who had been locked down for three weeks.
At the time, some high-profile Chinese public health experts began to suggest that China should consider moving towards a policy of coexisting with the virus. Their comments received some support from citizens and scientific colleagues, but were drowned out by government censure.
Chi said China’s government was sticking to the strategy because it had little other choice, politically. Citing energy shortages and the housing industry crisis, he said ensuring there was no major outbreak of Covid was “possibly their last stronghold of credibility and legitimacy” domestically.
But there is another motivation, stemming from the international blame directed at China for the pandemic itself, Chi said.
“From the beginning China has persistently wanted to show the world both its capability and credibility in terms of controlling this pandemic. They want to demonstrate how successful China has been in containing the outbreak and its ability to mobilise all available resources.
“They want to be seen as not the cause but as the saviour.”
There is still support for the government’s efforts.
“Personal freedom, personal work, privacy, dignity, and mental health can all be sacrificed,” said one social media user, urging others to look at the bigger picture.
Beijing has admitted the pandemic is the biggest challenge to the forthcoming Winter Olympics in February and Winter Paralympics in March. Recently released guidelines showed entrants will quarantine before entering the “closed loop” of the competition world, completely separated from the rest of China to avoid cross-infection.
Chi said China may be able to use accumulated wealth to sustain the country and itself through another year – crucially, past the date Xi Jinping will probably be seeking a third presidential term – but it is a different story for the people.
“The people are already suffering, particularly the sizeable proportion who are in low to middle income,” he said. “They can’t sustain it. The limit to their mobility and economic activity will worsen their livelihood.”
Both big Delta outbreaks were sourced to domestic tourism – the only remaining market for the industry with no sign of international visitors returning soon, even with Olympic events around the corner.
Huang said that, to some extent, Beijing was also in a dilemma. “We’ve already seen flareups in the countries that adopt a ‘coexistence with Covid’ approach, such as Singapore. If this happens to China too, then people will turn to the government and ask: ‘Why did you not manage to protect us?’
“This is the last thing China wants to see, especially in the run-up to the Winter Olympics early next year.”
Suliso wrote: ↑Sat Oct 30, 2021 10:38 am
After about 14 months the company I work for has decided that masks at work are no longer required. They were already only partially required (not while sitting at your desk) since September. We'll see how it goes, our site is 85% fully vaccinated but outside it's significantly less and the numbers are going up again.
Are employer mandates on vaccines common or uncommon in Switzerland? Wondering why it can't be 100% vaccinated and masks allowed off. Are unvaccinated going maskless as well? Do they need to get tested regularly?
Regardless, I hope it goes well and hope you're comfortable with the change.
Suliso wrote: ↑Sat Oct 30, 2021 10:38 am
After about 14 months the company I work for has decided that masks at work are no longer required. They were already only partially required (not while sitting at your desk) since September. We'll see how it goes, our site is 85% fully vaccinated but outside it's significantly less and the numbers are going up again.
Are employer mandates on vaccines common or uncommon in Switzerland? Wondering why it can't be 100% vaccinated and masks allowed off. Are unvaccinated going maskless as well? Do they need to get tested regularly?
Regardless, I hope it goes well and hope you're comfortable with the change.
Private sector vaccine mandates are not currently allowed in Switzerland. We can and do require nonvaccinated to be tested 2x per week. Therefore I think 85% is as good a number as we could have hopped for.
by ti-amie
by Suliso In Latvia there is a new trend among antivaxxers of bringing in chemtrails conspiracy. You see government is poisoning us from the air and causing covid...
by ponchi101 I wonder if all these ridiculous ideas and movements come from the fact that people no longer get proper science education. They don't develop a proper skeptical mind, they develop a "conspiracy driven" way of thinking. And they feel that, because they doubt everything without thinking it over, they are "smarter" than the rest.
It is truly a puzzling social phenomena.
by Suliso I think to some extent this has always been there. Chemtrails conspiracy, for example, date back only to 1996, but other crazies existed before. There were riots against polio vaccination in 19th century London.
by skatingfan The Internet has just created a way to spread the conspiracy theories with more efficiency. The other day I saw video on SciManDan's YouTube channel - he takes the time to debunk flat earth and other pseudoscience conspiracy theories - where he talked about a YouTuber who thinks Koalas are CGI, and points to video of a koala with a zookeeper as evidence.
by Suliso
skatingfan wrote: ↑Sun Oct 31, 2021 1:51 pm- he takes the time to debunk flat earth and other pseudoscience conspiracy theories - where he talked about a YouTuber who thinks Koalas are CGI, and points to video of a koala with a zookeeper as evidence.
Is it really worth spending time debunking stuff like this? Besides at the outer edge it's difficult to tell who's the true believer and who's just trolling.
by skatingfan
Suliso wrote: ↑Sun Oct 31, 2021 2:43 pm
worth spending time debunking stuff like this? Besides at the outer edge it's difficult to tell who's the true believer and who's just trolling.
I'm not sure. Some of the videos are really good at breaking down & explaining the physics, and physics was always a weak spot for me so I appreciate the explanations.
by Suliso Sure, I meant specifically the koala one
by ti-amie Wait koala's are CGI? That person must've been trolling. Does he think Australia doesn't exist?
by skatingfan
ti-amie wrote: ↑Sun Oct 31, 2021 6:27 pm
Wait koala's are CGI? That person must've been trolling. Does he think Australia doesn't exist?
'Australia isn't real' is a common conspiracy theory in the flat Earth community.
ti-amie wrote: ↑Sun Oct 31, 2021 6:27 pm
Wait koala's are CGI? That person must've been trolling. Does he think Australia doesn't exist?
'Australia isn't real' is a common conspiracy theory in the flat Earth community.
by ti-amie
by ponchi101 I wonder: if you do not debunk the obviously absurd, how long will you have to wait to be in need to explain the obvious?
by Deuce
skatingfan wrote: ↑Sun Oct 31, 2021 1:51 pm
The Internet has just created a way to spread the conspiracy theories with more efficiency.
And spread many other negative, harmful, and useless things.
“Our inventions are wont to be pretty toys, which distract our attention from serious things. They are but improved means to an unimproved end... We are in great haste to construct a magnetic telegraph from Maine to Texas; but Maine and Texas, it may be, have nothing important to communicate. As if the main object were to talk fast and not to talk sensibly... We are eager to tunnel under the Atlantic and bring the old world some weeks nearer to the new; but perchance the first news that will leak through into the broad flapping American ear will be that Princess Adelaide has the whooping cough.
After all, the man whose horse trots a mile in a minute does not carry the most important messages...” - Henry Thoreau
The internet has made the transfer and spread of the good and the bad much easier, more convenient, and much faster than ever before. With that comes the very real potential for danger - as in conspiracy theories, terrorist recruitment, suicide instructions, child pornography, and many, many other unhealthy things.
by mmmm8
Suliso wrote: ↑Sat Oct 30, 2021 10:38 am
After about 14 months the company I work for has decided that masks at work are no longer required. They were already only partially required (not while sitting at your desk) since September. We'll see how it goes, our site is 85% fully vaccinated but outside it's significantly less and the numbers are going up again.
We're masks optional but from today, you have to be vaccinated to come to the office. of course, unlikely your teams, the vast majority of us can do our jobs from home.
by mmmm8
ti-amie wrote: ↑Sun Oct 31, 2021 6:27 pm
Wait koala's are CGI? That person must've been trolling. Does he think Australia doesn't exist?
Suliso wrote: ↑Sat Oct 30, 2021 10:38 am
After about 14 months the company I work for has decided that masks at work are no longer required. They were already only partially required (not while sitting at your desk) since September. We'll see how it goes, our site is 85% fully vaccinated but outside it's significantly less and the numbers are going up again.
We're masks optional but from today, you have to be vaccinated to come to the office. of course, unlikely your teams, the vast majority of us can do our jobs from home.
Right, our site is ca 70% lab based and another 15% (including myself) are overseeing lab work. The remaining 15% who could be fully home based are HR, computational modeling of various types, some project leaders and upper management.
Something keeps pooping on cars and sidewalks. Impressively thorough job by the CIA, I guess, equipping those drones with real bird (expletive).
by Suliso Did you know that city pigeons are immortal? No one has ever seen a young one or a dead one. Could indeed be biological drones.
by JazzNU
by Suliso That's a bit of sophistry. Another 6,500 are applying for a medical or religious exemption (most will be denied).
by ti-amie I think it's significant because all of the NYC tabloids were hinting that there would be murder and mayhem because most of the police force would decide not to be vaccinated. I think there are 35,000 police officers in NYC. 6,500 is still a pretty low number.
by dryrunguy Here's the latest Situation Report from Johns Hopkins.
::
New Report: Together with our partner The Council on Foreign Relations, we released a new report urging governments, multilateral and international institutions, and private actors to act immediately to strengthen planning for future pandemic vaccines by incorporating lessons learned from successes and failures of the current global rollout of COVID-19 vaccines. The new report, Navigating the World that COVID-19 Made: A Strategy for Revamping the Pandemic Research and Development Preparedness and Response Ecosystem, identifies how the COVID-19 pandemic has exposed and redefined the realities of the global vaccine research, development, production and delivery ecosystem, one which has so far failed in rapid, equitable allocation and distribution of vaccines globally. You can read the full report here.
PEDIATRIC VACCINES The US FDA on October 29 authorized the emergency use of the Pfizer-BioNTech SARS-CoV-2 vaccine for children ages 5 to 11 years, making the vaccine the first to be authorized in the US for about 28 million US school-age children. The 2-dose regimen for this younger age group is one-third the dosage given to individuals aged 12 and older (10μg versus 30μg), administered 3 weeks apart. The US CDC’s Advisory Committee on Immunization Practices (ACIP) is meeting today and will vote around 4:15 pm EDT on whether to recommend the vaccine. If the panel votes that the CDC should recommend the Pfizer-BioNTech vaccine for 5- to 11-year-olds, which is likely, CDC Director Dr. Rochelle Walensky is expected to sign off on the recommendation, possibly within a few hours. While that scenario will make the vaccine available for some by the end of this week, a White House official on November 1 said the pediatric vaccination program will be “hitting full strength” the week of November 8, after vaccine doses are shipped to pediatrician offices, pharmacies, and other vaccine administrators.
Moderna recently provided an update on the FDA’s review of its SARS-CoV-2 vaccine for adolescents aged 12 to 17, saying the regulatory agency needs additional time to evaluate data on the risk of myocarditis after vaccination—inflammation of the heart muscle characterized by a rapid or irregular heartbeat. The FDA informed Moderna that regulators expect the assessment will not be completed by January 2022. Both the Moderna and Pfizer-BioNTech vaccines have been associated with rare instances of myocarditis, but COVID-19 disease is more likely to lead to the condition, and possibly cause lasting damage. The absolute risk of vaccine-associated myocarditis remains very small, and most cases are mild and recover fully quickly. So far, data suggest that the risk is highest after the second dose of an mRNA vaccine among males ages 16 to 29. Some researchers have seen a possible association between puberty hormones and myocarditis—which typically develops annually in about 10-20 people out of every 100,000 after a viral or bacterial infection—and that could explain why the condition seems to be less common among younger children. Moderna said it will wait to request authorization for its vaccine in younger children ages 6 to 11 until after an FDA decision on adolescent use.
NOVAVAX The National Agency of Drug and Food Control of the Republic of Indonesia, or Badan Pengawas Obat dan Makanan (Badan POM), on November 1 authorized the use of a SARS-CoV-2 vaccine developed by Novavax and manufactured by the Serum Institute of India (SII), marking the first authorization for the company’s recombinant nanoparticle protein-based vaccine. The company said shipments to Indonesia are expected to begin soon, with the country set to receive 20 million doses this year. Novavax has applied for authorization in India, the Philippines, the UK, and Australia, and announced on November 1 it submitted for authorization with Health Canada and completed rolling review submissions with the European Medicines Agency (EMA). The vaccine, NVX-CoV2373, appeared to provide 100% protection from moderate-to-severe COVID-19 based on data from a large Phase 3 clinical trial conducted in the US and Mexico, with 90.4% overall efficacy. Notably, Indonesia is not on the list of countries recognized by the WHO as having strict regulatory processes, so Novavax still has to win authorization elsewhere before it can fulfill a promise to COVAX to supply 1.1 billion vaccine doses. The company expects to request authorization from the US FDA by the end of this year.
NATURAL/INDUCED IMMUNITY The scientific community’s understanding of natural and induced COVID-19 immunity continues to evolve with the increasing number of vaccinated and recovered individuals. Late last week, the US CDC published a study in its Morbidity and Mortality Weekly Review (MMWR) examining the odds of hospitalization among adults with COVID-19 whose previous infection or vaccination occurred 90-179 days earlier. The study found that the odds of hospitalization were 5.5 times higher in individuals who previously had COVID-19 compared to people fully vaccinated with an mRNA vaccine and no previous SARS-CoV-2 infection. The CDC said the study affirms their recommendation for those who have had SARS-CoV-2 infections to get vaccinated. Throughout vaccination rollouts in the US, some unvaccinated individuals cite their own natural immunity from previous SARS-CoV-2 infection as a reason to avoid vaccination. An essay published in The New York Times on October 28 suggests there should be a strong effort to promote the power of so-called “hybrid immunity,” the protection previously infected individuals get when they are vaccinated. Some research suggests that individuals who have recovered from COVID-19 have a stronger immune response to new coronavirus exposures after vaccination when compared to vaccinated people who had not been previously exposed. In theory, this should allow these groups to have a better immune response to new variants.
Overall, the general consensus is that recovered individuals have a lot to gain from SARS-CoV-2 vaccination. A new poll from Axios/Ipsos shows people in the US are confused about SARS-CoV-2 vaccines’ effectiveness. According to the poll, 40% of respondents either don't believe or don't know that unvaccinated people are at least 10 times more likely to die of COVID-19. The results show the importance of public health officials underlining that vaccination continues to be the best protection from severe COVID-19 and not equating an individual’s decision to rely on natural immunity as being “anti-vax.” Research continues to explore the benefits of both natural and vaccine-induced SARS-CoV-2 immunity to develop a better understanding of the pathways that lead to more successful antibody responses.
HOUSEHOLD TRANSMISSION A study led by researchers from Imperial College of London and the UK Health Security Agency found that individuals vaccinated against SARS-CoV-2 had a reduced but still significant risk of transmission among household contacts. Published in The Lancet Infectious Diseases, the analysis determined a secondary attack rate (SAR) in household contacts exposed to contacts with the Delta variant was 25% for fully vaccinated individuals compared with 38% in unvaccinated individuals. The SAR among household contacts exposed to fully vaccinated index cases was similar to household contacts exposed to unvaccinated index cases (25% vs 23%). Peak viral loads were similar among vaccination groups and viral variants, but vaccinated individuals had a faster rate of viral load decline, implying they might become less infectious more quickly. The time interval between vaccination and study recruitment was greater in fully vaccinated PCR-positive contacts than fully vaccinated PCR-negative contacts, which the researchers note may indicate increased susceptibility to infection consistent with waning immunity as soon as 2-3 months following vaccination. They concluded that vaccination continues to protect against serious COVID-19 disease and that booster doses are warranted.
OVERWEIGHT & OBESITY People with overweight or obesity (OWOB) who become infected with SARS-CoV-2 are at a higher risk of severe COVID-19 and long-term symptoms, according to research published recently in the journal Influenza and Other Respiratory Viruses. Notably, adolescents with OWOB had longer-lasting respiratory symptoms (7 vs 4 days) and were more likely to be symptomatic than adolescents without OWOB (67% vs 34%). Recognizing these disparities, some countries—including the UK, Mexico, and Chile—are acknowledging diet-related diseases such as obesity and diabetes as risk factors for more severe COVID-19 and taking actions to curb sales of junk food, sugary drinks, and fast food and encourage people to exercise more. Less attention is being given to the association between OWOB and more severe COVID-19 in the US, where nearly 75% of adults and about 20% of children have OWOB. Additionally, almost two-thirds of COVID-19 hospitalizations in the US are estimated to be related to obesity, diabetes, hypertension, or heart failure. With no national strategy to address OWOB in the US, some researchers worry the problem could worsen in the future, as the rate of obesity during the first year of the pandemic rose among children ages 2 to 19 from 19.3% in 2019 to 22.4% in 2020. A study published November 1 in JAMA Pediatrics estimates that screen time spent outside of virtual schooling—also known as recreational screen time—among teenagers doubled from 3.8 hours a day before the pandemic to 7.7 hours per day during the pandemic. The findings imply that teenagers are spending more time engaging in sedentary behaviors, increasing their risk of developing OWOB, and could have mental health implications.
US SCHOOL SCREENING TESTING PROGRAMS In a joint effort between the US Department of Education, the US CDC, and the Rockefeller Foundation, the Biden administration is launching a new push to accelerate school-based COVID-19 screening testing for students and staff. The effort hopes to expand the reach of federal and state partners through additional resources, including a guide on how to start a school testing program, and will establish weekly “office hours” to connect schools to national testing experts for assistance in setting up and maintaining screening testing programs beginning November 2 and running through December 22. Additional personnel will be available to assist state health departments coordinate school testing programs through the CDC Foundation and the COVID Workforce Initiative as well as assist with contact tracing and other public health activities. A new directory, launched by the CDC, also aims to simplify the search for testing providers for schools to establish their testing programs. As part of the COVID-19 Action plan announced in September, US President Joe Biden allocated $10 billion for screening testing for teachers, staff, and students in K-12 schools, but not all states have accepted or utilized their share of the funding. According to a survey by the Center on Reinventing Public Education of the nation’s 100 largest school districts, less than 15% of those schools are utilizing that funding to establish COVID-19 screening testing programs.
G20 SUPPORT FOR ACT-A The Access to COVID-19 Tools Accelerator (ACT-A) last week launched a new strategic plan and budget for the next year, calling on nations to contribute US$23.4 billion through September 2022 to help the partnership close gaps in access to COVID-19 vaccines, diagnostics, treatments, and other resources in low- and middle-income countries (LMICs). Under the new plan, ACT-A partner agencies will aim to support LMICs in vaccinating 70% of their populations, increasing testing rates to at least 1 per 1,000 people per day, and treating up to 120 million COVID-19 cases by improving access to existing and emerging therapeutics. In announcing the new plan, a WHO official said 5 billion additional vaccine doses will be needed to reach the vaccination goal, requiring more transparency from manufacturers and countries with existing vaccine contracts or those that have pledged doses to COVAX, the vaccines arm of ACT-A.
WHO Director-General Dr. Tedros Adhanom Ghebreyesus called on the Group of 20, which met over the weekend in Rome, to use their political and financial power to fund ACT-A and create a legally binding treaty on pandemic preparedness and response. In a joint communiqué issued at the end of their meeting on October 29, G20 health and finance ministers agreed to continue to support ACT-A and take steps to reach a goal of vaccinating 70% of the world’s population by mid-2022—earlier than its previous goal—by “helping boost the supply of vaccines, medical countermeasures, and inputs in developing countries and remove relevant supply and financing constraints.” The ministers also agreed to establish a G20 Joint Finance-Health Task Force to prepare for future pandemics. Notably, the G20 ministers did not make any firm financial commitments, instead calling for further cooperation and exploration of funding mechanisms to address the current pandemic or future preparedness efforts. G20 leaders concluded their meeting on October 31, agreeing to “work together towards the recognition of COVID-19 vaccines deemed safe and efficacious by the WHO and in accordance with national legislation and circumstances, and to strengthen the organization’s ability regarding approval of vaccines.” The language apparently is in response to comments from both Russia President Vladimir Putin and China President Xi Jinping, who separately complained about lags in review time and lack of mutual recognition for the countries’ domestically produced SARS-CoV-2 vaccines.
LOCKDOWNS RISE & FALL Australia, Israel, and Thailand on November 1 significantly eased international border restrictions for the first time since the beginning of the COVID-19 pandemic, while parts of Eastern Europe and China took steps to tighten lockdowns amid rising cases. Australia opened its borders to permanent residents, citizens, and their families, allowing reunions after more than 18 months apart. Australians are now free to travel internationally without an exemption, and fully vaccinated individuals are no longer required to quarantine for 2 weeks upon arrival. All other non-resident international travelers need an exemption to enter the country, even if they are fully vaccinated. In Thailand, the government hopes the return of foreign visitors will help boost the economy, for which tourism accounts for about 20%. Israel is allowing international travelers who have received vaccine boosters, but not if more than 6 months has passed since their last dose.
In contrast to its Asia-Pacific neighbors, China is becoming more isolated, implementing new lockdowns and continuing its efforts to maintain a “zero COVID-19” policy. In an extreme example, officials kept more than 30,000 visitors to the Shanghai Disneyland in the park and forced them to undergo SARS-CoV-2 testing before being able to leave after one visitor tested positive for the virus. The South Pacific island nation of Tonga entered lockdown today, after recording the country’s first imported COVID-19 case last week. The case—a traveler from New Zealand incoming on a repatriation flight—spurred thousands of residents to get vaccinated. Meanwhile, parts of Russia have implemented their strictest lockdowns in more than a year, as the country continues to hit record numbers of daily new cases, with an average of 38,194 on November 1, more than double its recent low on September 10.
SARS-COV-2 ORIGIN The US Intelligence Community last week released a declassified report on the origins of SARS-CoV-2, the novel coronavirus that caused the COVID-19 pandemic. The nation’s intelligence agencies were unable to conclude whether the pandemic began as a result of animal-to-human viral transmission or a laboratory incident, saying that while both are both plausible, analysts could not agree on which was more likely or whether an assessment can be made at all based on current knowledge. In order to provide a more clear picture of the pandemic’s origin, the agencies would need more information from China or another breakthrough in new information, according to the report. Notably, the intelligence report does rule out allegations that the virus was developed as a bioweapon, although with low confidence. Additionally, the report clarifies that intelligence analysts agree that Chinese officials did not know about the novel coronavirus until after its detection in the general population. In response to the report, a Chinese official said the fact that a potential lab leak was included as a plausible origin was “a lie,” and he called for an investigation led by a cooperative of scientists from around the world.
In a process to name such a group, the WHO on November 1 reopened its call for applications for experts to join its newly established Scientific Advisory Group for the Origins of Novel Pathogens (SAGO). Interested individuals have until November 3 24:00 CET to submit their documents. Last week, only a day before the public comment period closed for a group of 26 previously named nominees, the investigative research group US Right to Know submitted a letter to the WHO expressing concerns over several of the nominees. It is expected that the WHO will choose additional applicants and reopen a 2-week comment period, further delaying the finalization of the group.
by ponchi101 So Thiem can get his Novavax. I hope he posts a picture of him getting the vaccine.
I wonder why he wanted that one specifically.
by JazzNU
ti-amie wrote: ↑Tue Nov 02, 2021 12:16 am
I think it's significant because all of the NYC tabloids were hinting that there would be murder and mayhem because most of the police force would decide not to be vaccinated. I think there are 35,000 police officers in NYC. 6,500 is still a pretty low number.
Correct. Also, they were quoting the police commissioner when providing that number. Because that's how many police officers are off no longer working their assignment from Sunday to Monday. Given the union was saying 10,000 were quitting on the spot on Monday and no one would be available to respond to emergencies so murder and mayhem could ensue, there only being 34 (the number is up to 90 from the most recent press conference) no longer working so far is a massive difference.
by JazzNU
ponchi101 wrote: ↑Tue Nov 02, 2021 5:44 pm
So Thiem can get his Novavax. I hope he posts a picture of him getting the vaccine.
I wonder why he wanted that one specifically.
I'm thinking he'll put his arm out for that the same way the skeptics said they would when the vaccine had full not emergency authorization.
ponchi101 wrote: ↑Tue Nov 02, 2021 5:44 pm
So Thiem can get his Novavax. I hope he posts a picture of him getting the vaccine.
I wonder why he wanted that one specifically.
I'm thinking he'll put his arm out for that the same way the skeptics said they would when the vaccine had full not emergency authorization.
I posted in the related thread, but Thiem got vaccinated or at least got his first dose. I'm glad I was wrong. He clearly didn't wait for Novavax, so not sure why that was his party line.
by ti-amie
by ti-amie
by atlpam Surprised not to see GA in the bottom 10 - we must be #11
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 247.5 million cumulative cases and 5.01 million deaths worldwide as of November 3. Global weekly incidence and mortality both increased for the second consecutive week. Weekly incidence increased by 4.1% compared to the previous week, and mortality increased by 7.9%. At the current rate, we expect the global cumulative incidence to surpass 250 million cases within the next week.
The global cumulative mortality surpassed 5 million deaths on November 2:
1 death to 1 million- 246 days
1 to 2 million- 116 days
2 to 3 million- 90 days
3 to 4 million- 90 days
4 to 5 million- 115 days
Global Vaccination
The WHO reported 7.0 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of November 5.* A total of 3.9 billion individuals have received at least 1 dose, and 3.0 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations has increased over the past week, up from 25.4 million doses per day on October 27 to 29.0 million on November 1.** The global trend continues to closely follow Asia. Since mid-October, daily vaccinations have increased in Europe and Asia and declined in Oceania. Africa is holding relatively steady near its highest rate, but it is still well below the other continents on a per capita basis. The overall trend in South America is unclear due to large fluctuations over the past several weeks. North America exhibited a spike in daily vaccinations on October 30, as a result of reporting from Mexico.
Our World in Data estimates that there are 3.93 billion vaccinated individuals worldwide (1+ dose; 49.9% of the global population) and 3.08 billion who are fully vaccinated (39.1% of the global population).
*This date might be an error but appears as such on the WHO page.
**The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 46.1 million cumulative COVID-19 cases and 746,705 deaths. The current daily incidence average is approximately 68,151 new cases per day and appears to be increasing. The decline in daily incidence has tapered off, and the average has held relatively steady at approximately 71,000 new cases per day since October 26. While this is considerably lower than the January 2021 and September 2021 peaks, it is still higher than the peaks from all other surges. The decline in daily mortality appears to have passed an inflection point and is beginning to taper off as well. The US is currently averaging 1,190 deaths per day, more than the summer 2020 peak, despite the widespread availability of SARS-CoV-2 vaccines.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
If the US continues at this rate, we expect it to surpass 750,000 cumulative deaths within the next 2-3 days. If the US surpasses this benchmark on November 5:
1 death to 250k- 258 days
250k to 500k- 95 days
500k to 750k- 264 days
US Vaccination
The US has administered 425 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend has increased sharply since October 21, up from 684,000 doses per day to 1.2 million on October 29, the first time above 1 million doses per day since June 13.* Notably, this corresponds to the date on which CDC Director Dr. Rochelle Walensky endorsed the recommendation by the CDC’s Advisory Committee on Immunization Practices (ACIP) to expand eligibility for booster doses. We expect to see some associated increase in daily vaccinations as a result of the recent decision to authorize use of the Pfizer-BioNTech vaccine in children aged 5-11 years.
There are 222 million individuals who have received at least 1 vaccine dose, equivalent to 66.9% of the entire US population. Among adults, 80.2% have received at least 1 dose, as well as 15.2 million children under the age of 18. A total of 193 million individuals are fully vaccinated, which corresponds to 58.1% of the total population. Approximately 69.8% of adults are fully vaccinated, as well as 12.8 million children under the age of 18. Since August 13, 20.6 million fully vaccinated individuals have received an additional or booster dose, including 26.6% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
MOLNUPIRAVIR The UK Medicines and Healthcare products Regulatory Agency (MHRA) today authorized the use of the oral antiviral molnupiravir for the treatment of mild-to-moderate COVID-19 in adults with diagnostic-confirmed SARS-CoV-2 infection and who have at least one risk factor for developing severe illness, making it the first country to authorize a COVID-19 treatment that can be administered at home. Molnupiravir, which is branded as Lagevrio in the UK, was developed by Merck and Ridgeback Biotherapeutics. An interim analysis of a Phase 3 clinical trial released last month showed the antiviral reduced the risk of hospitalization or death among COVID-19 patients recovering at home by approximately 50% when given early in their infection. A US FDA advisory committee is scheduled to meet later this month to discuss Merck and Ridgeback’s request for emergency use authorization (EUA) for the drug. In a statement, UK Health and Social Care Secretary Sajid Javid called molnupiravir a “gamechanger for the most vulnerable and the immunosuppressed.” Merck is making efforts to accelerate access to the drug, including entering into advance purchase agreements with individual nations, implementing tiered pricing, and granting voluntary licenses to generic manufacturers and the Medicines Patent Pool. The company expects to produce 10 million treatment courses by the end of this year.
COVAXIN The WHO on November 3 issued an emergency use listing (EUL) for Covaxin, a SARS-CoV-2 vaccine developed by Indian drugmaker Bharat Biotech. The EUL adds an eighth vaccine to a growing list of shots validated by WHO for the prevention of COVID-19 and facilitates Covaxin’s use in many countries that depend on WHO guidance for their regulatory decisions. A WHO-convened Technical Advisory Group (TAG) determined Covaxin meets quality, safety, efficacy, and production standards, and that the benefits of the vaccine far outweigh the risks. Notably, the WHO said current data are insufficient to assess vaccine safety or efficacy in pregnancy. The panel’s decision had been delayed after it sought additional information from Bharat Biotech to assess the vaccine’s risks and benefits for global use. The WHO’s Strategic Advisory Group of Experts on Immunization (SAGE) in early October recommended Covaxin be administered in a 2-dose regimen, 4 weeks apart, for adults aged 18 years and older. The vaccine—which has 78% efficacy after 2 doses—is easily stored, making it very suitable for use in low- and middle-income countries (LMICs) that might lack adequate cold chain storage and distribution capabilities. The listing also paves the way for COVAX to acquire and distribute the vaccine. Covaxin is the first vaccine fully developed and manufactured in India to receive an EUL, and the decision will help millions of Indians who have received the vaccine travel outside the country.
US AUTHORIZES PEDIATRIC VACCINE As expected, US CDC Director Dr. Rochelle Walensky on November 2 endorsed a unanimous recommendation from the CDC’s Advisory Committee on Immunization Practices (ACIP) that children aged 5 to 11 years receive a pediatric formulation of the Pfizer-BioNTech SARS-CoV-2 vaccine. The vaccine is the first to be authorized for that age group in the US, making about 28 million children immediately eligible to be vaccinated. The pediatric vaccine—a 2-dose regimen of 10μg administered 21 days apart, one-third of the dose recommended for individuals aged 12 and older—represents “a turning point” in the nation’s efforts against COVID-19, US President Joe Biden said. According to the CDC, every 1 million doses given to children aged 5 to 11 should prevent about 58,000 COVID-19 cases and 226 hospitalizations in that age group, and could prevent about 600,000 new cases in all age groups through March 2022. Widespread use of the vaccine among children will help slow the spread of the virus, make returning to in-person schooling safer, lower the risk of transmission during upcoming family holiday gatherings, possibly spur recovery in the travel industry, and generally “bring us closer to returning to a sense of normalcy,” acting US FDA Commissioner Dr. Janet Woodcock said in a statement.
Concerns remain over whether children in this age group will be at risk of myocarditis and pericarditis—inflammation of the heart muscle or tissue surrounding the heart, respectively—rare but potentially serious adverse events associated with the Pfizer-BioNTech and Moderna mRNA vaccines. The risk is highest among adolescent and young adult males aged 12 to 29 years, and experts agree the risk in younger children likely will be lower. They also concur that the benefits of vaccination in preventing COVID-19 outweigh any risks in young kids, as COVID-19 itself can lead to heart damage and other complications, including multisystem inflammatory syndrome in children, or MIS-C, and long COVID. Already, about 15 million pediatric doses are in place and ready to be administered nationwide. Those parents who are eager to get their children vaccinated—about 27%, according to the KFF COVID-19 Vaccine Monitor—can contact their pediatrician, local pharmacy, or health department to make an appointment. The children’s vaccination program is expected to be fully operational next week, and Vaccines.gov will soon be updated with available locations.
US VACCINE MANDATES The administration of US President Joe Biden today announced the details of 2 policies covering more than 100 million workers in an effort to get more people in the US vaccinated against COVID-19. The first rule, issued by the US Department of Labor’s Occupational Safety and Health Administration (OSHA), applies to employers with 100 or more employees and requires them to ensure their workers are either fully vaccinated or undergo weekly testing for SARS-CoV-2, for which employers are not required to pay. The rule also requires employers to provide paid-time off for employees to get vaccinated and compel unvaccinated workers to wear a face mask while at work. Employers who willfully do not comply with the mandate could face fines of up to $14,000 per violation, with the possibility of multiple citations per business. The second rule, issued by the Centers for Medicare & Medicaid Services (CMS) at the US Department of Health and Human Services (HHS), requires all healthcare workers employed at facilities that participate in Medicaid and Medicare—approximately 76,000 facilities nationwide—be fully vaccinated, with no option for testing but allowances for medical and religious exemptions.
Notably, under the new guidelines, all employees who fall under the OSHA, CMS, or previously announced federal contractor rules are now required to be fully vaccinated by January 4, 2022. The new deadline satisfies requests from businesses to wait until after the holiday season to implement vaccine mandates, expressing concerns over workforce shortages and soaring demand for services. Additionally, OSHA and CMS clarified that the agencies’ new rules preempt any inconsistent state or local laws, such as those banning or limiting employers’ authority to require vaccination, testing, or masking. In rolling out the new policies, the Biden administration clarified its legal authority in implementing the rules, citing OSHA’s responsibility in keeping workers safe and in healthy environments. Nonetheless, legal challenges to the rules are expected in the coming days.
Last week, 10 US states with Republican leaders filed a joint lawsuit challenging the vaccine mandate for federal contractors, saying the rule is unconstitutional. According to new vaccination mandate protocols published earlier this week, federal contractors will have more flexibility in how they enforce vaccination and testing mandates for workers who remain unvaccinated and who do not seek or receive a valid exemption. Federal contractors who do not comply with the new policies could face losing contracts. Some large federal contractors, including airlines Southwest and American and aerospace engineering company Boeing, have said their employees must abide by the original December 8 deadline to be fully vaccinated or apply for an exemption, although that deadline could be pushed back under the new guidance. According to results from the KFF COVID-19 Vaccine Monitor released last week, 5% of unvaccinated workers say they have left a job because of a vaccine requirement.
J&J-JANSSEN VACCINE A retrospective comparative-effectiveness study published in JAMA Open Network shows a single dose of the J&J-Janssen SARS-CoV-2 vaccine is 74% effective in preventing SARS-CoV-2 infection. The study—conducted by researchers from nference, a US-based software company affiliated with Janssen—examined the electronic health records (EHRs) of Mayo Clinic patients in several US states from February 27 to July 22, 2021, including 8,889 vaccinated and 88,898 matched unvaccinated adults. Both the Alpha and Delta variants were circulating at the time, although the Delta variant emerged toward the end of the study period. Overall, 0.7% of those vaccinated with the J&J-Janssen vaccine contracted SARS-CoV-2 compared with 2.5% of unvaccinated patients, corresponding to an overall vaccine effectiveness of 73.6% and 74.2% beginning 14 days post-vaccination. Vaccine recipients also had a lower risk of hospitalization and ICU admissions, although the groups had no difference in mortality due to a low number of deaths.
In a research letter published in JAMA Internal Medicine, researchers from the Mayo Clinic compared the age- and sex-specific rates of cerebral venous sinus thrombosis (CVST), a type of blood clot, after vaccination with the J&J-Janssen vaccine with pre-pandemic CVST rates in the general population in Olmsted County, Minnesota (US). CVST remained a rare occurrence following vaccination, with the overall age- and sex-adjusted incidence at 2.34 per 100k person-years between 2001 and 2015, compared with a peak incidence of 8.65 per 100k person-years 15 days post-vaccination, calculated using data from the US CDC’s Vaccine Adverse Event Reporting System (VAERS) collected between February 28 and May 7, 2021. The post-vaccination CVST rate among women was 5.1 times higher compared with the pre-pandemic rate, and the risk was highest among women aged 40 to 49 years, followed by women aged 30 to 39 years. The researchers note that the absolute CVST risk remained low for women in these age groups and the reasons for the higher incidence is unclear.
IMPACT ON LIFE EXPECTANCY & PREMATURE MORTALITY A study conducted by an international collaboration of researchers estimated that the COVID-19 pandemic has contributed to an excess loss of life of more than 28 million years in 2020. The study, published in The BMJ, collected all-cause mortality data for 37 upper-middle- and high-income countries and regions and compared data from 2020 to data from 2005-19. The researchers estimated the decrease in life expectancy and excess years lost—which is similar to “excess deaths,” but accounts for the age at death compared to the life expectancy.
Only Denmark, Iceland, New Zealand, Norway, South Korea, and Taiwan reported lower mortality than expected in 2020, and only New Zealand, Norway, and Taiwan reported an increase in life expectancy. The remaining countries accounted for more than 28 million years of life lost above the expected value, based on the WHO’s standard life table. Notably, the decrease in life expectancy was significantly greater among men than women, with an estimated 17.3 million years lost globally for men and 10.8 million for women. On a per capita basis, the largest excess years lost were observed in Bulgaria (7,260 years/100k population in men; 3,730 in women), Russia (7,020; 4,760), and Lithuania (5,430; 2,640). The researchers estimate 4,350 years lost per 100k population for men and 2,430 for women in the US. The largest decreases in life expectancy were observed in Russia (-2.33 years in men; -2.14 years in women), the US (-2.27; -1.61), and Bulgaria (-1.96; -1.37). This study includes only a small fraction of the global population and omits the vast majority of Asia and South America—including China and India and the entire continent of Africa—so it is highly likely that the actual excess loss of life is much greater than this estimate. Additionally, more deaths have been reported in 2021 than in the first year of the pandemic, so the total impact of the pandemic is likely far greater than 28 million excess years lost.
INDIGENOUS COMMUNITIES The Navajo Nation—the largest indigenous US tribe, with nearly 400,000 members—is experiencing an increase in COVID-19 cases despite a relatively high vaccination rate of about 70%, according to tribal data. Other tribes with high vaccination rates also are seeing a surge in cases, leaving experts and tribal leaders to wonder what is driving the increases. There remain pockets of unvaccinated tribal members, with most in the 17- to 45-year-old range, leading some to conclude that those of working age, many of whom travel off of reservations for employment, could be driving the increase in cases on reservations, where many live in multigenerational housing that can facilitate virus transmission among age groups.
View the impact of COVID-19 on Tribal Nations (New on JHU Coronavirus Resource Center).
Around the globe, indigenous leaders in Australia and New Zealand are concerned that as those countries reopen their borders, COVID-19 incidence will rise in their communities, many of which are remote and have limited access to medical services. And in one isolated area of Peru’s Amazon rainforest, members of the Urarina indigenous community only learned of the pandemic last month, when healthcare workers arrived to vaccinate residents. The trip to vaccinate members of the community took 3 days by boat, highlighting the challenges of vaccinating villagers in remote areas where access to healthcare is sorely lacking.
That's great about PA. Didn't know we were ranked so highly now. I'm guessing the mandates have helped the numbers here in the non-Philly and non-Pittsburgh areas. A healthy number of federal or federal adjacent workers along with healthcare and education to make a difference would be my guess.
by ponchi101
dryrunguy wrote: ↑Thu Nov 04, 2021 6:54 pm
IMPACT ON LIFE EXPECTANCY & PREMATURE MORTALITY A study conducted by an international collaboration of researchers estimated that the COVID-19 pandemic has contributed to an excess loss of life of more than 28 million years in 2020. The study, published in The BMJ, collected all-cause mortality data for 37 upper-middle- and high-income countries and regions and compared data from 2020 to data from 2005-19. The researchers estimated the decrease in life expectancy and excess years lost—which is similar to “excess deaths,” but accounts for the age at death compared to the life expectancy.
Only Denmark, Iceland, New Zealand, Norway, South Korea, and Taiwan reported lower mortality than expected in 2020, and only New Zealand, Norway, and Taiwan reported an increase in life expectancy. The remaining countries accounted for more than 28 million years of life lost above the expected value, based on the WHO’s standard life table. Notably, the decrease in life expectancy was significantly greater among men than women, with an estimated 17.3 million years lost globally for men and 10.8 million for women. On a per capita basis, the largest excess years lost were observed in Bulgaria (7,260 years/100k population in men; 3,730 in women), Russia (7,020; 4,760), and Lithuania (5,430; 2,640). The researchers estimate 4,350 years lost per 100k population for men and 2,430 for women in the US. The largest decreases in life expectancy were observed in Russia (-2.33 years in men; -2.14 years in women), the US (-2.27; -1.61), and Bulgaria (-1.96; -1.37). This study includes only a small fraction of the global population and omits the vast majority of Asia and South America—including China and India and the entire continent of Africa—so it is highly likely that the actual excess loss of life is much greater than this estimate. Additionally, more deaths have been reported in 2021 than in the first year of the pandemic, so the total impact of the pandemic is likely far greater than 28 million excess years lost.
Sobering figures. We have spoken about it and I still don't believe that the 5MM lives lost during these two years is correct. So, being conservative, this virus has perhaps killed around 7MM, which would mean 1/1000th of the world population.
Certainly not the black plague, but concerning. And, of course, I have no data to back that up. But, for example, the Venezuelan figures are totally fictitious. There must be other countries too.
by Deuce The important message here is that COVID-19 is still very much with us and among us - despite more and more people pretending that it's gone (which is dangerous, by the way)...
So I think I need to call BS on Mr. Rodgers. But please correct me if I'm wrong. How does someone know that they are allergic to an ingredient in a vaccine? I guess it could be possible, most people only know they are allergic to something if they have had an allergic reaction to it, and from what I read, it sounded like he found doctors who would say he had an allergy to something. And most allergic reactions are not strong, so unless he had gone into anaphylactic shock because of some ingredient in the vaccine, wouldn't the risk of Covid outweigh the allergic reaction?
But OK, maybe I'm wrong. Maybe he somehow knew that he had an allergy to an ingredient in the vaccine. So then he decides that some of the NFL protocols to separate vaccinated from unvaccinated players have been put in place just to shame unvaccinated players. EXCEPT THAT YOU WENT TO A HALLOWEEN PARTY UNMASKED and you ended up getting Covid. So yeah, stupid protocols.
So yeah dude, the woke mob (i.e. people who actually understand that the vaccines work and that if you haven't been vaccinated you shouldn't be at a party unmasked) is on your case.
Maybe he'll be in Nole and Konta's boxes at the AO.
Kevin
by ponchi101 The thing with people like Rogers is that when they say "I am doing my own research" what they are really saying is "I am looking for confirmation information for my already set theory". "I am looking for the ONE DOCTOR in 500 that will tell me I am right".
Other than that, vaccines that have been administered by the Billions and no reports of allergies being side effects. Wow, how peculiar that reaction must be, Mr. Rogers.
He already went out and said he is treating himself with Ivermectin and HydroQ. My friend N will become a Packers fan in a couple of days.
by JazzNU He's not allergic to anything, that's just what he's claiming. But he won't name what it is that he's allergic to, his explanation for not getting J&J is slim at best (6 clotting issues in women of roughly child-bearing years in just under 7 million doses led to the shot being paused for 11 days). And this asshat is openly admitting to taking medical advice from "his new good friend" Joe Rogan. He's not allergic to a damn thing.
And FYI, if he had a legitimate allergy or medical condition that prevented him from getting all of the vaccines, he could've told the NFL, but he didn't because that allergy doesn't exist. And none of that explains standing up there and lying. Other than he's a lying liar who lies.
by JazzNU
by JazzNU ^^ And now we know even more than we did 2 weeks ago why Dominic Thiem not being vaccinated was met with pushback in Austria and had even the country's health minister reaching out to him about the safety of the current vaccines. They didn't need one more thing to discourage people from getting vaccinated as cases were rising.
by Suliso Covid numbers going up in Switzerland in near geometric progression again...
I have a couple of "bold" predictions regarding USA. According to NYT currently 72,000 cases (flat) and 1,200 deaths (-19%) per day. I think your country has reached the lowest number of cases for a while and now the new wave is upon you. Deaths will go down for another two weeks to a low of ca 1,000 before starting to increase rapidly again. USA is not any better vaccinated than Austria or Switzerland.
by MJ2004 It's schizophrenic here in the U.S. We went out to dinner Saturday night to a restaurant in a town that has been at the forefront of mask mandates and vaccination rates in the state. I was shocked that NOBODY in the very full restaurant was wearing a mask. Just a few patrons like us wore masks on their way to their tables, but the staff was all unmasked, including in the open kitchen. The restaurant was packed too. It felt like pre-Covid era, and this town was the last place where I expected that. In the meantime, we continue at a steady rate of between 1500-2000 new cases daily in the state (1600 yesterday), so, I don't get it?
by meganfernandez
MJ2004 wrote: ↑Mon Nov 08, 2021 1:54 pm
It's schizophrenic here in the U.S. We went out to dinner Saturday night to a restaurant in a town that has been at the forefront of mask mandates and vaccination rates in the state. I was shocked that NOBODY in the very full restaurant was wearing a mask. Just a few patrons like us wore masks on their way to their tables, but the staff was all unmasked, including in the open kitchen. The restaurant was packed too. It felt like pre-Covid era, and this town was the last place where I expected that. In the meantime, we continue at a steady rate of between 1500-2000 new cases daily in the state (1600 yesterday), so, I don't get it?
does the restaurant require the unvaccinated to wear a mask when they aren't eating? Massachusetts has the highest vaccination rate, right? How many hospitalizations from those new cases? Evidently people are feeling pretty safe, and are also letting their guard down a bit, but maybe because they feel safe.
I still wear a mask indoors in some public settings, partly out of courtesy and partly out of extra caution - my state is toward the bottom of vaccination rates. I wonder if people think I'm unvaccinated because I'm wearing a mask. Kind of embarrassing.
by meganfernandez
dryrunguy wrote: ↑Sat Nov 06, 2021 1:39 am
I'd be just fine if Aaron Rodgers was sterile.
Like he doesn't already have a kid or two out there.
MJ2004 wrote: ↑Mon Nov 08, 2021 1:54 pm
It's schizophrenic here in the U.S. We went out to dinner Saturday night to a restaurant in a town that has been at the forefront of mask mandates and vaccination rates in the state. I was shocked that NOBODY in the very full restaurant was wearing a mask. Just a few patrons like us wore masks on their way to their tables, but the staff was all unmasked, including in the open kitchen. The restaurant was packed too. It felt like pre-Covid era, and this town was the last place where I expected that. In the meantime, we continue at a steady rate of between 1500-2000 new cases daily in the state (1600 yesterday), so, I don't get it?
does the restaurant require the unvaccinated to wear a mask when they aren't eating? Massachusetts has the highest vaccination rate, right? How many hospitalizations from those new cases? Evidently people are feeling pretty safe, and are also letting their guard down a bit, but maybe because they feel safe.
I still wear a mask indoors in some public settings, partly out of courtesy and partly out of extra caution - my state is toward the bottom of vaccination rates. I wonder if people think I'm unvaccinated because I'm wearing a mask. Kind of embarrassing.
If we see someone wearing a mask, we should only be thinking one thing: That person is exercising good public health practice. Nothing more.
If we see someone wearing a mask, we should only be thinking one thing: That person is exercising good public health practice. Nothing more.
You know there is a reason why this forum has 270 members, 50 of which are bots?
by JazzNU
MJ2004 wrote: ↑Mon Nov 08, 2021 1:54 pm
It's schizophrenic here in the U.S. We went out to dinner Saturday night to a restaurant in a town that has been at the forefront of mask mandates and vaccination rates in the state. I was shocked that NOBODY in the very full restaurant was wearing a mask. Just a few patrons like us wore masks on their way to their tables, but the staff was all unmasked, including in the open kitchen. The restaurant was packed too. It felt like pre-Covid era, and this town was the last place where I expected that. In the meantime, we continue at a steady rate of between 1500-2000 new cases daily in the state (1600 yesterday), so, I don't get it?
Been that way here for months. My sister came down from North Jersey for brunch in early October and though we were in an area she knows, she was like, is this area conservative now or what, why are there no masks? Just the way it's been here. I want to say in early Summer, masks started disappearing gradually at restaurants, from people wearing them in the building and mid to late summer, they weren't as common on the workers any longer. Now, pretty rare on the workers and the customers. The restaurant experience looks very pre-pandemic.
Retail is more hit or miss. Some places have workers wearing them, some it's their choice. The customers have in large part seemed to have decided they are done with their masks. Only mildly encouraging that I've seen a good deal more masks in the last week than I did a month ago.
by MJ2004
meganfernandez wrote: ↑Mon Nov 08, 2021 2:21 pm
How many hospitalizations from those new cases?
500 hospitalizations from those new cases. Certainly not negligible.
We rarely eat out. We went because it was our anniversary. Agree that retail is more hit or miss.
by ti-amie I went out to eat for the first time since the pandemic started. The restaurant we went to, on it's website, said that you must be vaccinated to enter. Everyone came in wearing masks. Once people were eating and drinking though no one was. When people left they, including me, put their masks back on.
I guess this is normal?
by JazzNU
by Suliso It is like that in Basel. Vaccination is important, but masks in this particular case are useless. You come in for like 2 min with it and then sit for two hours without in a possibly crowded restaurant. The virus is after all airborne.
Similar silliness when I go to play badminton once a week. Masks to enter and to move from the locker room to the court while you're alone 99% of the time. No mask while playing, but also not for obvious reasons in the most crowded place - the locker room. So basically lots of people - no masks, alone - masks.
by JazzNU
ti-amie wrote: ↑Mon Nov 08, 2021 7:12 pm
I went out to eat for the first time since the pandemic started. The restaurant we went to, on it's website, said that you must be vaccinated to enter. Everyone came in wearing masks. Once people were eating and drinking though no one was. When people left they, including me, put their masks back on.
I guess this is normal?
I think it's way more common in NYC and North Jersey for people to wear masks both into the restaurant and out of the restaurant. Probably in a few other areas like LA and San Fran. In terms of not wearing a mask after sitting, yes, very normal.
What I've noticed is that at times if people do wear masks into restaurants, they largely forget about wearing them out of the restaurant.
Hope you enjoyed your first time eating out in 18 months
Happy Anniversary @MJ!
by Deuce
ti-amie wrote: ↑Mon Nov 08, 2021 7:12 pm
I went out to eat for the first time since the pandemic started. The restaurant we went to, on it's website, said that you must be vaccinated to enter. Everyone came in wearing masks. Once people were eating and drinking though no one was. When people left they, including me, put their masks back on.
I guess this is normal?
^ Did the restaurant actually and properly check to ensure that everyone entering is fully vaccinated? By 'properly', I mean some form of proof that the person is 'fully vaccinated', along with I.D. proving that they are the person whose name appears on the proof of full vaccination.
Here in Canada, we have QR codes - on the cell phone or on paper - that are scanned before people can enter restaurants, gyms, and basically any indoor public place except for stores (masks are mandatory in stores in most provinces still).
But, of course, there are places (some restaurants, some gyms, etc.) where they CLAIM that one must be 'fully vaccinated' to enter, but they never check - which renders the claim entirely useless, of course.
Suliso wrote: ↑Mon Nov 08, 2021 7:19 pm
It is like that in Basel. Vaccination is important, but masks in this particular case are useless. You come in for like 2 min with it and then sit for two hours without in a possibly crowded restaurant. The virus is after all airborne.
Similar silliness when I go to play badminton once a week. Masks to enter and to move from the locker room to the court while you're alone 99% of the time. No mask while playing, but also not for obvious reasons in the most crowded place - the locker room. So basically lots of people - no masks, alone - masks.
^ Indeed, I see the same thing happening. It's mind boggling.
Do people honestly think that they can only spread - or contract - COVID-19 while upright, and that, when they are sitting, there is an invisible force-field which prevents the virus from either entering or exiting their small personal orbit?
I've gone back to curling (the sport, not my hair) this season, and after the games, there are 24 people sitting at the tables (8 people per table), all unmasked. But as soon as they stand up - like to go to the bar to get a drink -, they put the mask on.
I, personally, keep my mask on at all times when I am in the main hall where the 24 maskless people are seated - and I don't sit at a table with my team. In fact, I usually go outside, or stay around the locker room downstairs, where I am alone, when the main hall is full of unmasked people like that.
I'm also one of the only players who keeps the mask on during games.
I swear that the majority of people are trying desperately to convince themselves that the threat of COVID-19 is finished, just because they want it to be.
Sigh...
by dryrunguy Here's the latest Situation Report from Johns Hopkins. The section on vaccine misinformation was sobering--though not at all surprising. And what a bold move by the government of Singapore. More of that, please. Also be sure to read the section on REGEN-COV.
::
US VACCINATION REQUIREMENTS The administration of US President Joe Biden on November 5 released an interim final rule regarding SARS-CoV-2 vaccination for private employers with 100 or more workers in an effort to increase vaccination rates among the US population. The next day, the US Court of Appeals for the Fifth Circuit in New Orleans granted an emergency stay of the federal Occupational Safety and Health Administration (OSHA) temporary emergency rule that employees of those companies be fully vaccinated by January 4 or be required to undergo weekly testing, although it is unclear whether the stay is applicable nationwide or only in those states under the court’s jurisdiction.* According to the 3-judge panel, the petitioners bringing the request—including 5 states, all led by Republican governors, and various companies—"give cause to believe there are grave statutory and constitutional issues with the Mandate."
The court—considered to be one of the nation’s most conservative appeals courts—gave the federal government a deadline of 5 pm on November 8 to respond. Late that day, the US Department of Justice requested the court lift its stay, stating that the petitioners’ claims of harm are “premature,” given the rule’s first deadline—for large businesses to require masking of unvaccinated employees in the workplace—does not go into effect until December. The Biden administration said employers should move forward with efforts to get their employees vaccinated, saying the rule “will save thousands of lives and prevent hundreds of thousands of hospitalizations.” OSHA rules apply to private workplaces in 29 states, while the remaining states have their own state-run OSHA agencies that are required to adopt any federal rules. In October, OSHA threatened to take over the operations of the state-run OSHA agencies in Arizona, South Carolina, and Utah for failing to adopt a similar SARS-CoV-2 vaccination rule for healthcare workers; Arizona and South Carolina have begun the process to adopt that standard. Several other lawsuits challenging the vaccine rule have been filed in federal courts, including by at least 21 other Republican-led states. The Fifth Circuit must now decide whether to lift the stay or make it permanent. If the latter, OSHA could appeal to the US Supreme Court. So far, courts have largely upheld vaccination mandates issued by local and state governments and private companies, but the federal rule is more far-reaching. Despite opposition to the OSHA standard and other vaccine requirements, data show they are working to increase vaccination rates, with some companies reporting nearly 100% of their workers have received at least one dose of vaccine.
*Those states include Texas, Louisiana, and Mississippi.
PFIZER ANTIVIRAL CANDIDATE Pfizer announced last week that its investigational antiviral pill to treat COVID-19 reduced the risk of COVID-19-related hospitalization or death from any cause by 89% when compared to a placebo among patients treated within 3 days of symptom onset. The planned interim results come from a Phase 2/3 clinical trial examining the pill—which is called Paxlovid and is taken in combination with an older antiviral named ritonavir—among COVID-19 patients recovering at home who are at high risk of developing severe disease. The company said it plans to submit the data to the US FDA as soon as possible to request emergency use authorization (EUA) for the antiviral. This is the second oral pill that has shown positive results in clinical trials for treating people with COVID-19 at home and could help alleviate the strain of the pandemic on hospitals. The other antiviral, molnupiravir, being developed by Merck and Ridgeback Biotherapeutics, reduced the risk of hospitalization and death by about half, and UK regulators granted conditional authorization to the pill last week. Clinical trial data for both drugs have not yet been peer-reviewed or published in a journal.
Access to any new therapy is a global concern, and Pfizer said it will institute a tiered-pricing approach to promote equitable access if the drug receives regulatory clearance. Merck also has taken steps to facilitate manufacturing and distribution of its antiviral, including entering into advance purchase agreements with individual nations, implementing tiered pricing, and granting voluntary licenses to generic manufacturers and the Medicines Patent Pool. Notably, wealthy nations are already contracting with both companies for supplies of the antivirals, raising questions about when low- and middle-income countries (LMICs) might be able to access the treatments, with limited supply expected to be produced through the end of the year.
REGEN-COV Regeneron Pharmaceuticals on November 8 announced positive results from a Phase 3 clinical trial of its combination monoclonal antibody REGEN-COV for SARS-CoV-2 prevention. The trial—jointly run with the US National Institute of Allergy and Infectious Diseases (NIAID)—enrolled SARS-CoV-2-negative individuals who lived in the same household as someone who tested positive for SARS-CoV-2 within the prior 4 days. Participants received either one 1,200mg dose of REGEN-COV, administered via 4 subcutaneous injections, or a placebo. The trial found that REGEN-COV reduced the risk of developing COVID-19 by 81.5% during an 8-month timeframe. Notably, by the end of the follow-up period, about 35% of participants had also received at least 1 dose of a SARS-CoV-2 vaccine. REGEN-COV also reduced the risk of COVID-19-related hospitalization by 100%, with 0 individuals hospitalized in the REGEN-COV group and 6 individuals hospitalized in the placebo group. There were no deaths during the trial, and the trial did not record any new safety concerns for the treatment. REGEN-COV is currently authorized for the treatment of individuals with mild-to-moderate COVID-19 who are not hospitalized and to prevent infection in individuals exposed to COVID-19. The new data provide some indication that REGEN-COV could provide long-lasting immunity for immunocompromised individuals and others who are unresponsive to vaccines. Regeneron said it plans to submit the data, which is not yet published or peer-reviewed, to the US FDA as soon as possible in hopes of gaining authorization for the drug to be used as pre-exposure prophylaxis.
CHILDHOOD VACCINATION Now that a SARS-CoV-2 vaccine is authorized for children ages 5 to 11 years in the US, state regulators—along with parents, pediatricians, and public health officials—are contemplating when and if the shots should become mandatory for children. All 50 US states have requirements for school-age children to be immunized against other diseases such as polio, chickenpox, and measles. The nation’s second-largest school district, Los Angeles Unified School District in California, already has said children aged 12 and older must be vaccinated by mid-December to continue in-person learning, and several other jurisdictions and states have plans to make SARS-CoV-2 vaccination mandatory for children and adolescents to attend school as soon as the US FDA grants a vaccine full approval for those age groups.
Costa Rica will require SARS-CoV-2 vaccination for all children aged 5 and older beginning in March 2022, making it one of the first countries to implement such a policy for youth. So far, nearly 75% of the country’s adolescents ages 12 to 19 years have received at least one dose of vaccine. In the UK, the number of breakthrough infections among vaccinated individuals is increasing, and health officials say children—who remain largely unvaccinated—are partly to blame, with unvaccinated kids passing the virus to their vaccinated parents. A recent study published in The Lancet Infectious Diseases showed that fully vaccinated individuals who were exposed to a household contact infected with the Delta variant had an appreciable risk of becoming infected in the home, although the risk was lower than for unvaccinated individuals (25% vs 38%). Another study published in The Lancet Regional Health Europe highlights the role the Delta variant plays, showing increased transmissibility among household contacts when compared with the Alpha variant. While no vaccine is 100% effective in preventing COVID-19, evidence shows vaccination can help reduce the risk of infection and transmission to others, as well as significantly reduce the risk of hospitalization and death.
INTERNATIONAL TRAVEL TO US The US on November 8 reopened its borders to fully vaccinated travelers from 33 countries that were subject to previous restrictions implemented in early 2020. The countries—including Mexico, Canada, the UK and most European nations, China, India, South Africa, Iran, and Brazil—accounted for more than half of international visitors to the US in 2019, prior to the pandemic. Travelers entering the US by air will be required to show proof of vaccination status and a negative SARS-CoV-2 test, while those entering through land borders with Canada and Mexico will only need to show proof of vaccination. Notably, the loosening of restrictions comes just as Europe is experiencing a new surge of COVID-19 cases, with the WHO last week warning the region is again “at the epicenter” of the pandemic. Notably, Germany this week recorded its highest 7-day incidence since the beginning of the pandemic. Additionally, several countries, including Austria and Iceland, have implemented new or reinstated previous restrictions, and vaccination rates have plateaued across the region. A WHO official urged the US to pay close attention to Europe’s current situation and to not delay in reinstating public health measures, especially prior to the upcoming holidays.
EMERGENT BIOSOLUTIONS The US government has ended its contract with Emergent BioSolutions, a Baltimore, Maryland-based SARS-CoV-2 manufacturer that had to pause production earlier this year after an inspection revealed a batch of J&J-Janssen vaccine doses had been contaminated. The more than US$650 million contract—which only involved production of the AstraZeneca-Oxford vaccine that is not authorized for use in the US but is widely used in Canada, the EU, and South Africa—originally was awarded in May 2020, and Emergent will not receive about US$180 million after the government stopped making payments following the contamination discovery. Notably, J&J-Janssen will continue to use Emergent to produce its vaccine under a separate agreement even though the facility continues to lack federal regulatory approval to manufacture vaccine doses for use in the US.
VACCINE MISINFORMATION Tackling COVID-19 misinformation is far from simple. Sources and believers of misinformation range from high-profile NFL players to religious institutions, and efforts to combat vaccine hesitancy are often hodgepodge with unclear or mixed efficacy. According to new findings from the KFF COVID-19 Vaccine Monitor, 78% of adults have heard at least 1 of 8 different false statements about COVID-19 and believe it to be true or are uncertain if the statement is true or false. Only 22% did not believe any of the 8 false statements, the survey found. Belief in misinformation was associated with unvaccinated status, identification as Republican, rural residency, lack of a college degree, and age under 50 years. Belief in misinformation also was correlated with individuals who listed One America News, Fox News, or Newsmax as their trusted news source. In an effort “to understand, identify, and stop misinformation, and help others do the same,” US Surgeon General Dr. Vivek Murthy released a community toolkit for the general public this morning. Dr. Murthy previously identified COVID-19 misinformation as a threat to public health, and he hopes health professionals, faith leaders, teachers, parents, and others will use the new toolkit to engage in in-person conversations to dispel myths and rumors, especially regarding vaccination.
In a new analysis from the Center for Health Security, its estimated that COVID-19 vaccine misinformation and disinformation costs an estimated $50 to $300 million each day.
LOSS OF BENEFITS The US military has implemented SARS-CoV-2 vaccine mandates as a matter of readiness, a US Department of Defense official recently told the Senate Veterans' Affairs Committee. If service members refuse to get vaccinated, discharge decisions will be left to individual commanders, and those personnel that receive other-than-honorable discharges might lose certain US Department of Veterans Affairs (VA) benefits, including GI Bill funding, home loans, transition assistance, and some healthcare services. The military’s first vaccine mandate deadline passed on November 2, when active-duty members of the US Air Force and US Space Force (USAF/USSF) were to be fully vaccinated against COVID-19. As of last week, about 3% of the USAF/USSF active-duty members were not vaccinated and face possible expulsion. Deadlines for the other branches are looming. According to the Pentagon, 97% of the nation’s 1.3 million active-duty service personnel have had at least one vaccine dose, with 99% of the Navy with at least one shot, 93% of Marines, and 90% of the Army. Notably, the US Department of Defense has issued only a handful of exemptions, although none for religious reasons.
Outside of the military, other workers who remain unvaccinated may face financial repercussions, including increases in health insurance premiums, costs of weekly testing to comply with mandates, or even job loss. Now, some employers are rescinding death benefits for unvaccinated workers who die of COVID-19. New York’s Metropolitan Transportation Authority (MTA) is one of the highest-profile employers to do so, no longer paying a $500,000 death benefit to the families of subway, bus, and commuter rail employees who are unvaccinated and die of COVID-19. Other employers also are considering limiting benefits, such as short-term disability, to unvaccinated workers. Insurers—including MetLife, Hartford Financial Services Group, and Prudential Financial—have reported increases in the number of death-benefit claims for COVID-19 deaths among working-age people amid the Delta variant surge, causing them to payout higher-than-normal amounts through their employer-sponsored life insurance and international life insurance businesses.
SINGAPORE Currently, the government of Singapore fully covers medical costs for COVID-19 treatment for all nationals, permanent residents, and long-term visa holders. However, because unvaccinated individuals are causing a disproportionate strain on the healthcare system, the Ministry of Health announced this week that individuals who are “unvaccinated by choice” will be ineligible to receive full government coverage for COVID-19 medical bills beginning December 8. These unvaccinated individuals will still have access to normal healthcare financing options where applicable, such as private insurance or government subsidies. As of November 8, 85% of Singapore’s population is fully vaccinated, and vaccination is free to all nationals and long-term residents.
by ti-amie
SINGAPORE Currently, the government of Singapore fully covers medical costs for COVID-19 treatment for all nationals, permanent residents, and long-term visa holders. However, because unvaccinated individuals are causing a disproportionate strain on the healthcare system, the Ministry of Health announced this week that individuals who are “unvaccinated by choice” will be ineligible to receive full government coverage for COVID-19 medical bills beginning December 8. These unvaccinated individuals will still have access to normal healthcare financing options where applicable, such as private insurance or government subsidies. As of November 8, 85% of Singapore’s population is fully vaccinated, and vaccination is free to all nationals and long-term residents.
by JazzNU
dryrunguy wrote: ↑Tue Nov 09, 2021 5:21 pm
LOSS OF BENEFITS The US military has implemented SARS-CoV-2 vaccine mandates as a matter of readiness, a US Department of Defense official recently told the Senate Veterans' Affairs Committee. If service members refuse to get vaccinated, discharge decisions will be left to individual commanders, and those personnel that receive other-than-honorable discharges might lose certain US Department of Veterans Affairs (VA) benefits, including GI Bill funding, home loans, transition assistance, and some healthcare services. The military’s first vaccine mandate deadline passed on November 2, when active-duty members of the US Air Force and US Space Force (USAF/USSF) were to be fully vaccinated against COVID-19. As of last week, about 3% of the USAF/USSF active-duty members were not vaccinated and face possible expulsion. Deadlines for the other branches are looming. According to the Pentagon, 97% of the nation’s 1.3 million active-duty service personnel have had at least one vaccine dose, with 99% of the Navy with at least one shot, 93% of Marines, and 90% of the Army. Notably, the US Department of Defense has issued only a handful of exemptions, although none for religious reasons.
Outside of the military, other workers who remain unvaccinated may face financial repercussions, including increases in health insurance premiums, costs of weekly testing to comply with mandates, or even job loss. Now, some employers are rescinding death benefits for unvaccinated workers who die of COVID-19. New York’s Metropolitan Transportation Authority (MTA) is one of the highest-profile employers to do so, no longer paying a $500,000 death benefit to the families of subway, bus, and commuter rail employees who are unvaccinated and die of COVID-19. Other employers also are considering limiting benefits, such as short-term disability, to unvaccinated workers. Insurers—including MetLife, Hartford Financial Services Group, and Prudential Financial—have reported increases in the number of death-benefit claims for COVID-19 deaths among working-age people amid the Delta variant surge, causing them to payout higher-than-normal amounts through their employer-sponsored life insurance and international life insurance businesses.
SINGAPORE Currently, the government of Singapore fully covers medical costs for COVID-19 treatment for all nationals, permanent residents, and long-term visa holders. However, because unvaccinated individuals are causing a disproportionate strain on the healthcare system, the Ministry of Health announced this week that individuals who are “unvaccinated by choice” will be ineligible to receive full government coverage for COVID-19 medical bills beginning December 8. These unvaccinated individuals will still have access to normal healthcare financing options where applicable, such as private insurance or government subsidies. As of November 8, 85% of Singapore’s population is fully vaccinated, and vaccination is free to all nationals and long-term residents.
All of this is excellent and is to be expected. Hopefully more companies and more countries move in this direction.
by ti-amie
Suliso this looks like the maps you used to post here.
by ti-amie
by dryrunguy Here's the latest Situation Report from Johns Hopkins. A few observations: 1) It's precisely stunts like what Moderna is trying to pull now that explain broad-based mistrust of the pharmaceutical industry; 2) be sure to check out the sections on measles and mismanaged plastic waste.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 250.7 million cumulative cases and 5.06 million deaths worldwide as of November 10. Global weekly incidence increased for the third consecutive week, while global weekly mortality fell slightly over the previous week. Weekly incidence increased by 2.68% compared to the previous week, and mortality decreased by 3.68%. The global cumulative incidence surpassed 250 million cases early this week, with several countries in Europe experiencing record numbers of new cases.
Global Vaccination
The WHO reported 7.08 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of November 8. A total of 3.9 billion individuals have received at least 1 dose, and 3.0 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations has decreased over the past week, down to 27.83 million doses per day on November 10 from a recent high of 30.83 million doses per day on November 4.*
Our World in Data estimates that there are 4.04 billion vaccinated individuals worldwide (1+ dose; 51.34% of the global population) and 3.16 billion who are fully vaccinated (40.13% of the global population). Europe, South America, North America, and Oceania all have fully vaccinated at least 50% of their populations, while Asia sits at 44.52% and Africa lags far behind at 6.34%.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 46.6 million cumulative COVID-19 cases and 755,201 deaths, passing 750,000 cumulative deaths on November 4. The current daily incidence average is approximately 74,584 new cases per day and appears to be increasing. The decline in daily mortality appears to have passed an inflection point and appears to be holding relatively steady. The US is currently averaging 1,078 deaths per day.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 434.5 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend reached a recent peak at 1.2 million doses on October 29 but has declined slightly to 1.17 million doses as of November 5.* Since CDC Director Dr. Rochelle Walensky endorsed the recommendation by the CDC’s Advisory Committee on Immunization Practices (ACIP) to authorize use of the Pfizer-BioNTech vaccine in children aged 5 to 11 years, an estimated 1 million elementary-age kids have received their first dose, according to a White House official.
There are 224.7 million individuals who have received at least 1 vaccine dose, equivalent to 67.7% of the entire US population. Among adults, 80.9% have received at least 1 dose, as well as 15.1 million children under the age of 18. A total of 194 million individuals are fully vaccinated, which corresponds to 58.5% of the total population. Approximately 70.3% of adults are fully vaccinated, as well as 12.8 million children under the age of 18. Since August 13, 26.1 million fully vaccinated individuals have received an additional or booster dose, including 32.4% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
PFIZER-BIONTECH BOOSTER Pfizer and BioNTech on November 9 submitted a request to the US FDA to authorize their SARS-CoV-2 vaccine as a booster dose for all adults aged 18 years and older. If the FDA grants an amendment to the existing emergency use authorization (EUA)—which it is expected to do, possibly ahead of the Thanksgiving holiday—all 181.5 million fully vaccinated adults in the US would become eligible for an additional shot. Such a move would represent a turnaround from 2 months ago, when an FDA expert panel overwhelmingly recommended against the companies’ request for booster doses for all adults. Notably, that committee is not scheduled to meet in November, meaning the FDA could grant the request without seeking external advice. Pfizer-BioNTech made the request based on unpublished data from a randomized, controlled clinical trial of more than 10,000 people aged 16 and older who previously received a primary 2-dose series of the vaccine. Among those who received a booster dose, relative vaccine efficacy reached 95.6% when compared to those who did not receive a booster. Currently, a booster dose of the Pfizer-BioNTech vaccine is authorized for individuals aged 65 years and older, individuals ages 18 to 64 years who are at high risk of severe COVID-19 or who have frequent institutional or occupational exposure to SARS-CoV-2, as well as eligible people who completed primary vaccination with a different SARS-CoV-2 vaccine.
Health Canada on November 9 authorized the Pfizer-BioNTech vaccine as a booster dose for all people aged 18 years and older, at least 6 months following the primary 2-dose regimen. A booster dose of the Pfizer-BioNTech vaccine is the same, 30 μg, as those used in the primary series. Mounting evidence shows a third dose of the Pfizer-BioNTech vaccine significantly increases the antibody response among recipients, although it remains unclear how long any resulting immunity lasts.
MODERNA Moderna and the US National Institutes of Health (NIH) are currently in a dispute over which entity should receive patent rights to the SARS-CoV-2 mRNA vaccine the company and the agency developed in partnership. The collaboration to develop the vaccine was widely hailed as a shining example of successful interaction between public and private entities for the benefit of the global population. However, Moderna’s patent paperwork noticeably does not include the government scientists involved in the vaccine development process as co-inventors. Moderna’s stance on this dispute is that they “reached the good-faith determination that these individuals did not co-invent” the vaccine. The NIH and consumer advocacy group Public Citizen disagree with this assessment, believing that federal scientists were core to the invention of the vaccine and should be included on the patent. The NIH and Moderna currently are engaged in talks to resolve the dispute, but if left unresolved, the issue could be taken into the court system for resolution.
Ownership of patents vital to vaccine manufacturing has implications beyond the financial aspect; decisions about distribution of the product and information-sharing on patented technology fall under the patent owner’s control. Moderna has repeatedly come under fire for not providing technical information with vaccine manufacturers in low- and middle-income countries (LMICs), although the company has said it will not enforce patents during the pandemic. Both Moderna and Pfizer—which developed a SARS-CoV-2 mRNA vaccine in partnership with BioNTech—have limited licensing opportunities with other vaccine manufacturers in an effort to protect their large investments in the technology. But this tight hold on mRNA vaccine technology inhibits other countries with vaccine manufacturing capabilities from negotiating access to the information needed to make the products. Following the successful procurement of ample vaccines for the US population, the US government is now making concerted efforts to send more vaccine doses to the rest of the world. However, those efforts are being significantly stymied by strict contractual language with Moderna that prevents the US from sending doses abroad or sharing manufacturing information. Increased scrutiny on Moderna’s tight grip on vaccine supply and technology have led to promises from the company to play a more significant role in global vaccine distribution, but many have stated these pledges are too little, too late and do not guarantee enough action. Some progress in changing contractual language was made in June, but additional efforts still need to be made to improve worldwide availability of vaccine doses and technology.
AT-HOME TEST RECALL The FDA has issued a recall for additional batches of Australia-based company Ellume’s at-home COVID-19 test kits for potentially false-positive results. This recall is for the same issue that was previously reported in early October and classified as a Class I recall, the most serious recall designation that may result in “serious adverse health consequences or death.” Product batches with a manufacture date between February 24 and August 11, 2021, and distribution dates between April 13 and August 26, 2021, are included in the recall, which includes more than 2.2 million of the 3.5 million tests shipped to the US; Ellume’s previous estimate of faulty tests was 427,000. Those who attempt to use the affected tests will be notified through the app of the recall status, and replacement tests can be requested online. Thus far, the FDA has received reports of 35 false positives from the tests. The Biden administration made a $231.8 million deal with Ellume in February to boost availability of the at-home testing kits in the US, which also helped fund the company’s first manufacturing plant in the US in Frederick, Maryland, with a 500,000 test production capacity per day. The White House made an additional $1 billion allocation for the purchase of the 8 types of at-home testing kits available in the US shortly after the first Ellume recall was publicized.
VACCINE ACCESS The global rollout of SARS-CoV-2 vaccines continues to face various challenges, including hoarding and inequities in vaccine distribution, unfulfilled pledges, vaccine production backlogs, export restrictions, supply chain disruptions, communication breakdowns, logistical hurdles, and misinformation and hesitancy. Experts warn that if wealthy nations continue to put their own interests ahead of the rest of the world and continue to stockpile vaccines, the COVID-19 pandemic will remain two-pronged, with some nations working toward recovery while others continue to be threatened by ongoing outbreaks. Increasingly, public health officials and policymakers are looking toward the future, highlighting lessons learned from this pandemic and drafting an international treaty on pandemic preparedness and response.
The fact remains that the world needs to take steps to fix inequities in vaccine access now in order to reach a goal of vaccinating 70% of the world’s population by September 2022. On November 10, US Secretary of State Antony Blinken hosted a virtual COVID-19 ministerial, during which he said the US will step up efforts to boost vaccine production, increase vaccine donations, and fulfill current pledges. He announced the US helped broker a deal between Johnson & Johnson (J&J) and COVAX to help deliver more doses of the J&J-Janssen SARS-CoV-2 vaccine to conflict zones, humanitarian settings, and frontline workers such as UN peacekeepers, including a US donation of 1.5 million doses of surplus supply. Secretary Blinken also announced a new public-private partnership, called the Global COVID Corps, to facilitate private sector companies in lending expertise and resources to support vaccination campaigns, including supply chain management and on-site vaccine administration. Earlier this week, the heads of the International Monetary Fund (IMF), World Bank Group, WHO, and World Trade Organization (WTO) met with the CEOs of vaccine manufacturing companies, acknowledging the urgency of delivering more vaccine doses to low-income countries and calling on G20 nations to join efforts to meet the end-of-year goal to vaccinate 40% of the population in all countries.
The Center for Health security released a report on October 29, Navigating the World that COVID-19 Made: A Strategy for Revamping the Pandemic Research and Development Preparedness and Response Ecosystem, urgently calling on governments, international institutions, and private sector actors to immediately act to address gaps and explore opportunities at each step along the vaccine value chain.
MEASLES In a report published in an early edition of the US CDC’s Morbidity and Mortality Weekly Report (MMWR), researchers from the CDC and WHO voiced concern over diminished progress toward measles elimination, as more than 22 million infants missed their first dose of measles vaccine in 2020 amid the COVID-19 pandemic. Also in 2020, only 70% of children received their second dose. Additionally, 24 vaccination campaigns in 23 countries were planned in 2020 but were postponed due to the pandemic, leaving more than 93 million people at risk for the disease. Notably, reported measles cases decreased more than 80% in 2020 compared to the previous year, but surveillance activities significantly dropped, with the lowest number of specimens sent in for testing in more than a decade. Missed vaccination doses and gaps in disease surveillance programs highlight the largest increase in unvaccinated children in decades and put many more children at risk of contracting the disease. Major measles outbreaks occurred in 26 countries in 2020, accounting for 84% of all reported cases last year. Despite disruptions to immunization services worldwide, 81 countries (42%) maintained their measles elimination status through the end of 2020, but no new countries were verified as having achieved measles elimination.
PLASTIC WASTE Global plastic waste was a problem prior to the COVID-19 pandemic, and an increase in demand for single-use plastics—especially those used in medical settings—has intensified the problem over the past 2 years, according to a research article published in the Proceedings of the National Academy of Sciences (PNAS). Worldwide, 193 countries have generated about 8 million tons of mismanaged plastic waste (MMPW). Of that waste, nearly 26,000 tons has entered the oceans, where it threatens to have a “long-lasting impact” by disturbing marine life and polluting coasts. The researchers, from China and the US, urged all nations, particularly low- and middle-income countries, to better manage medical and other plastic waste as the pandemic continues. A separate crowd-sourced project is tracking instances of wildlife being killed or disrupted by pandemic-related waste, with researchers noting cases of animal entanglement, entrapment, and ingestion of COVID-19 trash.
I wish I could say I'm surprised about what Moderna is doing.
by JazzNU
dryrunguy wrote: ↑Thu Nov 11, 2021 5:05 pm
Here's the latest Situation Report from Johns Hopkins. A few observations: 1) It's precisely stunts like what Moderna is trying to pull now that explain broad-based mistrust of the pharmaceutical industry; 2) be sure to check out the sections on measles and mismanaged plastic waste.
Unpopular opinion I'm sure. But I wouldn't call what Moderna is doing a stunt. They are the MRNA company, the science and tech they have worked to perfect is basically the savior of this pandemic. But if they don't see a healthy return on the development they've invested in for the last decade to get to this point, I have no idea what their future is.
People hate pharma, I get it. But pharmaceutical development isn't a non-profit business because it costs a freaking mint and acting as if it should be then paid for at cost is just a Utopian ideal. Happy mediums should be explored even in a pandemic so developers don't shy away from future investment or we may not land on solutions as quickly as we did this time. Moderna is actual chump change compared to true Big Pharma. Acting like Moderna is in a similar financial position to be more permissive of patent sharing like a Pfizer, J&J, or Merck is just unfair. This is their first and only commercial product.
by ponchi101 People hate Big Everything. Big Oil is hated because we pollute the world and create economic distortions and world problems. People hate Big Agra because they create economic distortions and wipe out the small farmers. They hate Big Data because they create economic distortions and invade our privacy. They hate Big Insurance, Big Military and here, Big Pharma, because of all the profits.
Yet, we power, feed, heal, cover and protect the world, on many occasions. These companies are not there to be charities. They are not a group of nuns running a soup kitchen. They are for profit entities.
The sole thing I would like to see would be for them to set up shop again in countries lime mine, so they can produce their miracle drugs in country, and help the local economy and progress.
And yes, Moderna has developed something unique. They have all the right to profit from that.
by dryrunguy I just re-read the section on Moderna to make sure I understood it correctly. I'm still not sure I do.
But I can tell you this... In my line of work (which does not get into patents), all contract deliverables are the property of the federal government. This was a contract. The federal government should own all contract deliverables.
That said, there's clearly something in the contract language that either muddies the patent issue or gives Moderna ownership of the patent. I would have to see the actual contract language, but that would require a FOIA request, which would probably take months.
So I'll step back from calling it a stunt.
If nothing else, it is, at least, really bad optics for Moderna--during a global pandemic when so many people are still dying or face the possibility of long-term disability due to Long COVID. I highly doubt that Moderna is hurting financially. There's a stark difference between safeguarding corporate profitability and downright greed. To me, this feels like the latter.
One other thing... We routinely develop scientific papers, produced under CONTRACT, not a GRANT, that are published in peer-reviewed journals. IT WOULD NEVER EVEN OCCUR TO US to exclude a federal or state client and their colleagues from authorship in journal publication. Even if their sole contribution to a journal article was to change "happy" to "glad" in a journal manuscript.
You. Just. Don't. Do. THAT.
But since most of the work we do is funded by government contracts, the government is not in any way required to acknowledge our contribution to the development of contract deliverables. Sometimes they do, as a courtesy. But not always. And we know that going in.
I just find the whole thing.... really icky.
by Suliso
Nobody really has a convincing (to me) theory why this is the case.
Nobody really has a convincing (to me) theory why this is the case.
I don't know what any of the proposed theories are... but the first thing I thought of is that German language media is spreading more BS than the media outlets of other languages.
I have no idea if this is the case or not - and if it is the case, I have no idea why it's happening - but it would possibly explain it.
by MJ2004 Here is the complete article that graph came from in the FT:
‘Nein Danke’: the resistance to Covid-19 vaccines in German-speaking Europe
Hesitancy in Austria, Germany and Switzerland intersects with anti-establishment and populist politics
As Switzerland kicked off a mass Covid-19 vaccination drive, riot police formed lines around Zurich’s main train station. Their mission: to protect a new “vaccination village” in the station hall from angry protesters.
“We are a civil rights movement,” said Nicolas A Rimoldi, a 26-year-old protester from the city of Lucerne who was one of several people arrested during the Monday protests but later released without charge. “The huge pressure that is being put on people, against morality, against the constitution, is just not right.”
Some protesters carried Trycheln, the giant cowbells that are a symbol of rural Switzerland, where vaccine hesitancy is high.
Despite being one of the wealthiest countries in the world, Switzerland has the lowest Covid-19 vaccination rate in western Europe. More than one-third of the Swiss population — 33.6 per cent — have not had a first dose of a Covid vaccine.
Switzerland is part of a cluster of wealthy — and predominantly German-speaking — European nations at the heart of Europe with surprisingly poor vaccination rates. In neighbouring Austria, 33.1 per cent have yet to take a single shot of the vaccine, and in Germany it is 30.4 per cent. Case numbers are surging in all three countries.
The high levels of hesitancy, evident among adults of all age groups and political persuasions, have increased scrutiny of the factors driving vaccine scepticism in German-speaking countries.
In Germany, resistance to the vaccine is marked in the affluent southern states of Bavaria and Baden-Württemberg as well as in eastern regions such as Saxony. Markus Söder, the Bavarian prime minister, said the three regions had a large proportion of Querdenker (“lateral thinkers”) — members of a protest movement that form the loudest voice against the government’s pandemic curbs.
“We have two viruses in the country,” Söder told a German talk-show. “We have coronavirus and we have this poison [of vaccine scepticism], which is being spread on a massive scale by the Querdenker and by parties like the [far-right] Alternative for Germany [AfD]”.
In Switzerland, vaccine uptake in rural, German-speaking eastern cantons is often far lower than in the country’s French-speaking west and Italian-speaking south. In Appenzell Innerrhoden, 45 per cent of the population is still completely unvaccinated. But the pattern is not clear-cut. The mountainous, German-speaking canton of Graubünden has administered more first doses than urban, French-speaking Geneva.
Suzanne Suggs, professor of communication at the University of Lugano’s public health institute, suggests that authorities in German-speaking countries have tended to be far more dispassionate in their health messaging. “It has been functional rather than emotional,” she said. The lack of emotionally resonant pro-vaccine messaging “has meant conspiracy theories have filled that void — they are often easier for [uninformed] people to believe”, Suggs added.
Daily cases in Austria and Germany hit their highest levels of the entire pandemic on Tuesday. The province of Upper Austria — a centre of vaccine scepticism, with a population of 1.5m — has recorded more new coronavirus cases this week than the whole of the Iberian peninsula.
In Germany, 14m people who are eligible to receive the jab have so far decided not to. In the Berlin suburb of Hohenschönhausen, locals queueing for injections at a pop-up “vaccination bus” gave a range of reasons for having waited.
“I am generally a champion of vaccination, but I’m just not sure that this one is safe,” said Jutta, who declined to give her surname. She said she was still opposed to the Covid vaccine, “but I have no choice any more. They’re saying I won’t be able to go to work unless I’ve received the jab.”
Polling by Erfurt University gives some indication why many Germans don’t want jabs: 80 per cent of unvaccinated respondents said they needed to weigh up the risks and benefits first, and 41 per cent simply considered vaccination “unnecessary”.
Anti-vaccine sentiment intersects strongly with anti-establishment and populist politics. A Forsa poll conducted on behalf of the German health ministry found that half of unvaccinated respondents had voted for the rightwing populist AfD in the recent federal election.
In Austria, the rightwing populist Freedom party has become vociferous in its opposition to vaccination measures. Last month party boss Herbert Kickl spoke about “terrifying” links between vaccines and tumours.
Switzerland is gearing up for a November 28 referendum that will codify the federal government’s emergency pandemic powers. The populist Swiss People’s party — the country’s largest — is openly campaigning against the government. According to an October poll by Sotomo, 51 per cent of its supporters are unvaccinated.
While it has become convenient for the German-speaking political mainstream to deride vaccine-sceptics as Schwurbler — which loosely translates in this context as “burbling yokels” — the reality is more complex.
When MFG, a newly established vaccine-sceptic party, won seats in an Austrian regional election in September, 30 per cent of its voters were previous supporters of the far-right. But another 30 per cent were former moderate conservative voters, while 16 per cent were former socialists and 12 per cent ex-Greens.
Many young people in the three countries are also opposed to Covid-19 vaccination — and government measures to encourage it. In Austria, around 37 per cent of adults under the age of 35 are unvaccinated.
The average age of supporters of the Mass-Voll! (“Enough is Enough”) protest group that organised Monday’s demonstration in Zurich is just 20. It already has more followers on Instagram than the youth movement of Switzerland’s Green party or its Social Democrats.
“This is about the future of a younger generation,” said Rimoldi.
by mmmm8
ti-amie wrote: ↑Mon Nov 08, 2021 7:12 pm
I went out to eat for the first time since the pandemic started. The restaurant we went to, on it's website, said that you must be vaccinated to enter. Everyone came in wearing masks. Once people were eating and drinking though no one was. When people left they, including me, put their masks back on.
I guess this is normal?
I've found it's hit or miss in Manhattan although most places are diligently checking vaccination proof, asking for a matching ID. Most places, staff are wearing masks on the floor but not in the kitchen...
by ponchi101
MJ2004 wrote: ↑Fri Nov 12, 2021 12:27 pm
“I am generally a champion of vaccination, but I’m just not sure that this one is safe,” said Jutta, who declined to give her surname. She said she was still opposed to the Covid vaccine,
Over 1 billion people have been vaccinated. Not one single death from the vaccine, directly.
How much safer can this crap be?
This has got to be the most tested vaccine in history.
by mmmm8
ti-amie wrote: ↑Thu Nov 11, 2021 6:30 pm
The news about measles is distressing.
I wish I could say I'm surprised about what Moderna is doing.
I just listened to a podcast about the vaccine rollout and why all these patent/contracting issues are going to pop up and it's essentially because everything was moved through so quickly, no one really focused on figuring these things out. That was a good thing in the moment, since it sped up vaccine creation and production, but, in the balance, it'll probably mean taxpayers subsidized Pfizer/Moderna/J&J R&D without getting any kind of percent of potential profits.
by ti-amie
by ponchi101 Extremely brave from Brix to say all this. NOW.
I know, I know, I know. I was not there and I was not in her shoes. But I wish that if I ever get into such a position, I will have the cojones to get BBC on the line and spill everything out.
by JazzNU
ponchi101 wrote: ↑Fri Nov 12, 2021 10:29 pm
Extremely brave from Brix to say all this. NOW.
I know, I know, I know. I was not there and I was not in her shoes. But I wish that if I ever get into such a position, I will have the cojones to get BBC on the line and spill everything out.
But you very likely wouldn't. In your shoes, maybe, but not in hers. She's a military doctor, that's her training and that's her chain of command. Rarely do they break ranks in the fashion many expected of her. She's also a woman and was a very convenient public punching bag who came under much more fire for similar acquiescence than her male colleagues. For instance, the same could be said of Azar and Redfield, but rarely is.
by ponchi101 I am only mentioning Birx because the news are about her. But those two you mention are also non-paragons of bravery.
by JazzNU
ponchi101 wrote: ↑Fri Nov 12, 2021 11:52 pm
I am only mentioning Birx because the news are about her. But those two you mention are also non-paragons of bravery.
Oh I understood completely. It's just news like this is almost always about her, not about any of her male colleagues, who were in greater positions of power than she was no less, and who also made mistakes in how permissive they were of dangerous nonsense.
by ti-amie From the AP:
A person cannot remove a vaccine from their body once they have been injected, doctors and fact checkers report
NBC News reported that some people on social media were advocating that those who are vaccinated against COVID-19 have attempted to bathe in a substance called Borax. This substance will not remove a COVID-19 vaccine from a person's body, NBC News, Marketwatch, and doctors said. There are no methods of removing a vaccine from a person's body, The AP reported.
by ponchi101 I don't mind. I don't care. Let them bathe in Borax, Chlorine, Agent Orange, diluted Napalm (mildly), liquified poison ivy, enhanced rattle snake saliva.
Just let them.
by ti-amie
by Deuce "hospitalized for 4 days with lung & oxygen issues" does not sound like "mild COVID-19".
To me, 'mild COVID-19' would be having mild symptoms which don't prevent you from doing much, and staying at home, not going anywhere near a hospital because of your symptoms.
The psychosis could be physically related to the COVID-19, or could be a product of anxiety he may have felt due to having the disease, being hospitalized, etc.
Or the psychosis could be entirely unrelated to any element of his COVID-19. Until we hear of many more cases of psychiatric issues from people who have, or who have had, COVID-19, I don't think it's cause for concern.
No matter the cause, it's certainly tragic for this man and his family, though.
by ti-amie
by dryrunguy My apologies. I am in proposal hell and totally forgot to share yesterday's Situation Report.
::
US VACCINE MANDATE The United States’ “vaccine mandate”* was put on hold following a ruling by a 3-judge panel of the 5th US Circuit Court of Appeals. The panel concluded that the mandate, an Emergency Temporary Standard (ETS) issued by the Occupational Safety and Health Administration (OSHA) that generally applies to companies and organizations with 100 or more employees, is “staggeringly overbroad” and does not sufficiently account for variations in working conditions and environments. The panel concluded that the policy should be suspended until the case can be argued in court. Lawyers from the Biden Administration appealed the initial panel ruling, arguing that a delay in implementing the mandate could result in many unnecessary deaths, but the judges upheld the initial decision. In its ruling, the panel described the policy as “fatally flawed” and indicated that lawsuits aiming to overturn it “are likely to succeed on their merits,” which suggests that the White House could face an uphill battle to institute the mandate in January.
The original deadline was scheduled for January 4, 2022, at which time employers would be required to implement weekly testing requirements for unvaccinated employees. Lawsuits have been filed across multiple jurisdictions in opposition to the policy, including by several state governments as well as private companies and religious organizations. Reportedly, these lawsuits may be consolidated into a single jurisdiction, but it is unclear which court could try the case.
*The policy does not actually mandate SARS-CoV-2 vaccination. Rather, it mandates routine testing for unvaccinated employees. The ETS also includes requirements for other aspects of workplace-based COVID-19 protective measures, including mask use.
AUSTRIA LOCKDOWN On November 15, Austria implemented increased COVID-19 restrictions on unvaccinated individuals that resemble "lockdown" measures implemented early in the pandemic. Last week, Austria announced that negative tests would no longer be permitted as a substitute for vaccination or proof of prior infection required for individuals to enter many public spaces, including restaurants and Christmas markets, or for gatherings of more than 25 people. But the new measures take the protective measures a step further by restricting unvaccinated individuals to their homes except for essential activities such as grocery shopping and going to work. Reportedly, police can perform “spot checks” to verify individuals’ documentation of vaccination or prior infection, and individuals who violate the restrictions could be fined up to €1,450 (US$1,660). The new policies essentially implement restrictions similar to the “lockdowns” previously implemented across Europe, but they will apply only to individuals aged 12 years and older who are not fully vaccinated or recovered from SARS-CoV-2 infection. The affected population constitutes approximately 2 million individuals nationwide.
Austria’s full vaccination coverage is approximately 65%. This is currently lower than many central and western European countries but higher than both the European average and the US. Like multiple other European countries, Austria is in the midst of its largest surge to date. At more than 11,000 new cases per day, the daily incidence is already 50% higher than Austria's previous record and increasing rapidly. The daily incidence has increased by a factor of 6 since mid-October and a factor of 170 since early July. On a per capita basis, Austria’s daily incidence ranks #3 globally. Austria’s daily mortality is also accelerating on a concerning trajectory. Austria is currently averaging 33 deaths per day, which is essentially equal to its second highest peak (April 2021).
In addition to Austria, several other countries in Europe are strengthening COVID-19 restrictions in response to the current surge. Multiple European countries, particularly across the central portion of the continent, are facing their most severe surges to date. Like Austria, several German states are eliminating negative tests as an option to eat indoors at restaurants or bars, which limits those spaces to individuals who are fully vaccinated or recovered from prior infection. The Netherlands is reportedly reinstating a nationwide “partial lockdown” for 3 weeks, which will mandate that nonessential businesses close at 6pm and essential businesses (eg, supermarkets) and restaurants close at 8pm. Additionally, the restrictions limit large indoor gatherings, such as at sporting events and museums. The Netherlands also reinstated a mask mandate on November 6 for public spaces where individuals are not required to show their COVID-19 entry pass, including public transit, retail shops, and colleges and universities.
AFRICA: DIABETES & COVID-19 Since early in the pandemic, evidence has shown that certain underlying health conditions can elevate the risk of severe COVID-19 disease and death. A team of WHO researchers analyzed COVID-19 data from 13 African countries and identified a four-fold increase in the case fatality ratio among COVID-19 patients with diabetes—10.2% compared to 2.5% in other COVID-19 patients. Additionally, the case fatality ratio for individuals with diabetes was twice as high as for individuals with other underlying health conditions (eg, hypertension, heart disease), although individuals with diabetes frequently suffer from multiple comorbidities. Preliminary findings from the study were presented to coincide with World Diabetes Day on November 14.
Diabetes can result in inflammation and decreased blood circulation, which increases the risk of complications from COVID-19 disease. The elevated risk of severe disease and death appears to affect individuals with both type 1 and type 2 diabetes, but the prevalence of type 2 across Africa is increasing rapidly. There are currently an estimated 24 million people across Africa who have diabetes—approximately 1.7% of the total population—but this number is expected to more than double by 2045—to 55 million; 4.0% of the population. The WHO estimates that 70% of affected individuals do not know they have the disease and, therefore, are not aware that they are at higher risk for severe COVID-19. The WHO’s Regional Director for Africa, Dr. Matshidiso Moeti, commented that “fighting the diabetes epidemic in Africa is, in many ways, as critical as the battle against the current pandemic.” African countries continue to struggle to access SARS-CoV-2 vaccines, with only 6.6% of the continent fully vaccinated, compared to the global average of 40%.
PFIZER ORAL ANTIVIRAL Pfizer announced today that it signed a voluntary license agreement with the Medicines Patent Pool, which is supported by the UN, to allow sub-licensed generic pharmaceutical manufacturers to produce its candidate oral antiviral COVID-19 treatment—a combination of ritonavir and a new antiviral, PF-07321332—pending regulatory authorization or approval. Interim analysis from Phase 2/3 clinical trials found that the treatment demonstrated an 89% risk reduction in COVID-19-related hospitalization or death among high-risk adults when administered within 3 days of symptom onset. Under the terms of the agreement qualified manufacturers would be allowed to supply the treatment to 95 countries, including all low- and lower-middle income countries. Pfizer will not collect royalties on sales to low-income nations or other countries covered under the agreement while COVID-19 is classified as a Public Health Emergency of International Concern (PHEIC) by the WHO.
HEART INFLAMMATION France and Germany joined Finland, Norway, and Sweden in recommending that the Moderna SARS-CoV-2 vaccine not be used for individuals under the age of 30 due to increased risk of myocarditis in that age group. Denmark has similarly recommended against offering the vaccine to individuals under the age of 18. French authorities recently emphasized, however, that vaccine effectiveness was slightly higher for the Moderna vaccine than for the Pfizer-BioNTech vaccine, and the Moderna product should be preferentially utilized for individuals aged 30 years or older. The European Medicines Agency (EMA) has authorized the Moderna vaccine for use in individuals aged 12 years and older.
PLANNING FOR ENDEMICITY As we approach the 2-year anniversary of the onset of the COVID-19 pandemic, many around the world are starting to plan for a future in which COVID-19 is an endemic threat. Early on, many public health experts discussed the potential for reaching herd immunity at some point in the pandemic, which could effectively contain community transmission in the absence of other protective measures. At the time, estimates suggested that at least 85% of the population would need to have immunity, whether through natural infection or vaccination. Some scientists are now calling for a shift away from herd immunity as the “end goal” and toward preparing for COVID-10 to become endemic.
The rationale behind this paradigm shift is multi-factored. First, the emergence of more transmissible variants, including the Alpha and Delta variants of concern, has increased the immunity threshold needed to achieve herd immunity. Pairing this reality with low vaccination coverage and stalled vaccination progress in many countries, including the US, shifts the goal of herd immunity even further away. Many scientists calling for this shift recognize that it would be difficult for governments to backtrack on the promise of herd immunity, which could further damage confidence in public health agencies and potentially harm ongoing vaccination efforts. But this process is already in motion in some countries. Last month, for example, White House Chief Medical Advisor Dr. Anthony Fauci acknowledged that elimination of the virus may not be achievable.
Over the past several months, many news media outlets have featured articles with input from public health experts regarding the potential outcomes for the US COVID-19 epidemic. Many of these experts projected that the virus will be a permanent fixture for the foreseeable future. While many unknowns remain that could impact how SARS-CoV-2 spreads in the future, including the potential for new variants and the duration of vaccine effectiveness, now is the time to prepare for the distinct possibility that COVID-19 will transition from a pandemic to an endemic global threat that will require continual investment and response activities in countries around the world.
by ponchi101 The endemicity paragraph sounds so true. We will always be able to thank all the people in the world that decided not to get the vaccine, or simply wear a mask. Their valiant efforts will make us wear a mask for the rest of our lives.
Meanwhile, in Colombia.
I went to the movies yesterday. Perfect day, as there were 3 people in the theater (including me; that is what happens when you go see DUNE, directed by Villeneuve). But, the important thing: as of yesterday, you are not allowed to go into any enclosed, public space UNLESS you can show physical proof of vaccination. I was so happy to show my CDC card.
Poor Colombians; there went their freedoms (the other two people at the theater also showed theirs).
by ti-amie Because of the covidiots I wondered how public health officials would deal with a never ending "pandemic" as the virus continues to mutate. Along with the Alpha and Delta variants I heard about a Lambda variant a couple of months ago. Sadly, we are going to have to learn to live with this. It makes what TFG didn't do even worse, if that's possible.
by ti-amieA couple convicted of stealing Covid funds is on the run, the F.B.I. says.
Richard Ayvazyan, who was convicted in a scheme to steal $20 million in Covid-19 relief funds, at the federal courthouse in Los Angeles in June.Credit...Gary Coronado/Los Angeles Times, via Getty Images
By Maria Cramer
Nov. 17, 2021
Updated 4:20 p.m. ET
When the Covid-19 pandemic began last year, a Southern California man recruited his brother, his wife and many others to use the identities of older people, foreign exchange students who had left the country and dead relatives to apply for $20 million in federal relief funds, the authorities said.
The man, Richard Ayvazyan, 43, bought a $3.25 million mansion and filled it with gold coins, luxury watches and imported furniture using the stolen Covid-19 disaster-relief funds, federal prosecutors in California said.
In June, Mr. Ayvazyan; his wife, Marietta Terabelian, 37; and Artur Ayvazyan, Mr. Ayvazyan’s brother, were convicted of scheming to fraudulently obtain funding that was meant for people and businesses that had sustained economic losses as a result of the pandemic.
In August, as they awaited sentencing at their home in the San Fernando Valley, Mr. Ayvazyan and Ms. Terabelian removed their bracelet monitors and fled, according to the F.B.I. They left their children behind, according to federal prosecutors.
On Monday, they were both sentenced in absentia. Mr. Ayvazyan received 17 years in prison and his wife received six. Artur Ayvazyan, 41, was sentenced to five years.
During the hearing on Monday, Judge Stephen V. Wilson of the U.S. District Court for the Central District of California said he could not recall a fraud case done in such a “callous, intentional way without any regard for the law” and described Mr. Ayvazyan as “an endemic, coldhearted fraudster.”
Mr. Ayvazyan’s lawyer, Ashwin J. Ram, said that his client’s family believed the couple was kidnapped but that the authorities had made no serious effort to investigate the claim.
“There are dozens of people who potentially have exposure,” Mr. Ram said. “My fear was that someone wanted to silence my client.”
Mr. Ram said a one-sided picture of Mr. Ayvazyan was presented at sentencing.
“The entire point of sentencing is not whether a crime occurred,” he said. “The point of sentencing is what is just punishment in this case.”
Editors’ Picks
Adele Has a Lot of Big Feelings on ‘30’
To Honor His Indigenous Ancestors, He Became a Champion
One Chaste Marriage, Four Kids, and the Catholic Church
Mr. Ayvazyan’s background as a churchgoer, a father and a prominent member of the Armenian community in Southern California who invested in small start-ups did not come up at the hearing.
“That story didn’t get told at sentencing because he wasn’t there,” the lawyer said. According to Mr. Ram, the couple has three children, ages 13, 15 and 16, who are living with their grandparents.
Prosecutors said in court filings that Mr. Ayvazyan left a typed letter for their children explaining they had to flee because he has brought “danger and fear” to their lives.
“We will be together again,” he wrote, according to a copy of the letter. “I will find a way, that’s a promise.”
Mr. Ayvazyan had a history of loan fraud, according to a sentencing memorandum filed by prosectors.
He pleaded guilty to conspiring with Ms. Terabelian to fraudulently obtaining a line of credit and was charged with conspiring to use stolen identities to secure mortgage loans and green loans for environmentally friendly home projects, the memo stated.
Ms. Terabelian used to work at a children’s hair salon, according to the F.B.I.
Marietta Terabelian, right, in Los Angeles in June. On Monday she was sentenced in absentia to six years in prison.Credit...Gary Coronado/Los Angeles Times, via Getty Images
Ryan Fraser, a lawyer for Ms. Terabelian, described her as a “loving mother and devoted wife who has tirelessly supported not only her three children, but also her parents, mother-in-law and sister.”
Mr. Fraser noted that Judge Wilson sentenced Ms. Terabelian to “less than one-third the time” that prosecutors had sought. They asked for 21 years in prison.
Mr. Ayvazyan began stealing disaster-relief funds as soon as they became available in March 2020, according to the prosecutors’ memo.
In messages to his co-conspirators, he joked that the federal government would run out of money and told them to move quickly to get the funds.
“This program is over by end of the month so get as much as you can,” he wrote, according to the memo.
Mr. Ram said the court sentenced Mr. Ayvazyan on guidelines based on the theft of about $1.5 million from the government. He added that he did not believe that prosecutors proved that Mr. Ayvazyan himself stole anyone’s identity.
The government “was handing out money with no checks and a lot of people took advantage of that,” Mr. Ram said.
“It’s a honey trap,” he added. “Richard Ayvazyan fell into that trap.”
The F.B.I. said it was offering a $20,000 reward for anyone with information that could lead to the couple’s arrest.
by dryrunguy Here's the latest Situation Report. I read it very quickly, but the sections on healthcare worker burnout and U.S. overdoses stood out.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 254.3 million cumulative cases and 5.1 million deaths worldwide as of November 17. Global weekly incidence increased for the fourth consecutive week, while global weekly mortality rose slightly over the previous week. Weekly incidence increased by 7.84% compared to the previous week, and mortality increased by 1.45%. During the week ending November 14, 3.3 million cases were reported, with Europe accounting for 2.15 million of those, according to the WHO COVID-19 Weekly Epidemiological Update.
Global Vaccination
The WHO reported 7.3 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of November 15. A total of 4.05 billion individuals have received at least 1 dose, and 3.06 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations has decreased over the past week, down to 29.6 million doses per day on November 17 from a recent high of 33.48 million doses per day on November 14.*
Our World in Data estimates that there are 4.13 billion vaccinated individuals worldwide (1+ dose; 52.41% of the global population) and 3.25 billion who are fully vaccinated (41.23% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 47.2 million cumulative COVID-19 cases and 762,994 deaths. The current daily incidence average is approximately 85,944 new cases per day and appears to be increasing. Daily mortality appears to be holding relatively steady, with the US currently averaging 1,028 deaths per day.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 434.5 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend reached a recent peak at 1.2 million doses on October 29 but has declined slightly to 1.17 million doses as of November 5.* Since CDC Director Dr. Rochelle Walensky endorsed the recommendation by the CDC’s Advisory Committee on Immunization Practices (ACIP) to authorize use of the Pfizer-BioNTech vaccine in children aged 5 to 11 years, an estimated 1 million elementary-age kids have received their first dose, according to a White House official.
There are 228.2 million individuals who have received at least 1 vaccine dose, equivalent to 68.7% of the entire US population. Among adults, 81.7% have received at least 1 dose, as well as 15.3 million children under the age of 18. A total of 195.6 million individuals are fully vaccinated, which corresponds to 58.9% of the total population. Approximately 70.7% of adults are fully vaccinated, as well as 12.9 million children under the age of 18. Since August 13, 31.5 million fully vaccinated individuals have received an additional or booster dose, including 37.3% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
BOOSTER DOSES The US FDA is expected to expand eligibility for booster shots of mRNA-based SARS-CoV-2 vaccines to all adults who received their second dose at least 6 months prior, as early as today. Both vaccines from Pfizer-BioNTech and Moderna already are authorized as booster doses* for adults aged 65 years and older, adults at risk of severe disease due to underlying health conditions, and adults at risk of disease due to their occupation. According to some estimates, between 30-40% of adults are not eligible for booster doses under current authorizations. The FDA is expected to decide on Pfizer-BioNTech’s and Moderna’s requests to expand their vaccines’ emergency use authorizations (EUAs) without convening the Vaccines and Related Biological Products Advisory Committee (VRBPAC) for discussion. VRBPAC previously rejected initial requests for booster doses for all adults for both vaccines in favor of scaled back authorizations focusing on at-risk populations. There are some concerns that not convening the expert panel could undercut its influence and skip important public discussions about the use of limited global vaccine resources and breakthrough cases. A meeting of the US CDC Advisory Committee on Immunization Practices (ACIP) is scheduled to discuss booster dose efficacy on November 19. Some US states—amid rising COVID-19 cases and frustration with what they see as a delay in federal approval for widespread booster shots—have moved forward to expand eligibility among their populations.
Meanwhile, the UK Joint Committee on Vaccination and Immunization (JCVI) expanded SARS-CoV-2 mRNA vaccine booster eligibility in England from all adults aged 50 and older to all adults aged 40 years and over in an effort to stem new infections, as mainland Europe experiences a large surge. The panel also recommended a second dose of the Pfizer-BioNTech vaccine for adolescents ages 16-17 years, a minimum of 12 weeks after their initial dose. Many in Europe are expecting a difficult winter with high SARS-CoV-2 transmission. But as wealthier nations continue to expand booster dose eligibility to larger swaths of their populations, WHO Director-General Dr. Tedros Adhanom Ghebreyesus last week called SARS-CoV-2 vaccine disparities between high-income and low- and middle-income countries a “scandal.” There are currently 100 countries at risk of falling short of the WHO’s previous goal of fully vaccinating 40% of the global population by year’s end. The WHO claims that this goal could still be achieved if COVAX immediately received 500 million additional doses of vaccine. Experts warn that ongoing global vaccine disparity could lead to the rise of additional SARS-CoV-2 variants with the potential to escape current immunity and vaccine design.
*The Pfizer-BioNTech dose is the full dose of the prime-boost series (30μg) while the Moderna booster is administered as a half dose of the original 2 shots (50μg vs 100μg).
VACCINE SUPPLY The administration of US President Joe Biden this week announced plans to invest billions of dollars to expand domestic manufacturing capabilities to increase the supply of SARS-CoV-2 mRNA vaccines to low- and middle-income countries (LMICs) by 1 billion doses annually. According to the White House, the funds will go to companies that make mRNA vaccines—including Pfizer, BioNTech, Moderna, and other subcontractors—to expand vaccine infrastructure and capacity, such as facility space, equipment, and staff. Funding will come from the American Rescue Plan that President Biden signed into law in March. So far, the US has pledged to donate at least 1.1 billion doses to LMICs and is requesting that other wealthier countries make similar commitments to address global inequities in vaccine access and distribution. The Biden administration is under increasing pressure to do more to close vaccine access gaps and reach global vaccination goals, and while this latest announcement is welcomed, no agreement has been reached with the pharmaceutical companies and any results in increased manufacturing are not expected until the latter half of 2022. In a US House of Representatives Appropriations subcommittee hearing this week, some lawmakers focused their criticism on Moderna, saying the company has not contributed enough to global vaccine supplies and criticizing it for its reluctance to give credit and share vaccine technology patent rights with government scientists. For its part, the US government has asked Moderna to take steps to help increase vaccine supplies, particularly in Africa—where less than 7% of the population is vaccinated— and with COVAX. It is unclear whether these latest steps by the Biden administration will help quell the growing anger among some activists.
US HEALTHCARE WORKER EXODUS Due to the protracted nature of the COVID-19 pandemic, many US healthcare workers are facing extreme burnout and leaving their posts in droves. About 18% of healthcare workers in the US have quit since the beginning of the pandemic and another 12% have been laid off. The stressors of the current emergency have nearly doubled the risk of burnout among physicians, with up to 75% reporting symptoms of exhaustion, depression, sleep disorders, or post-traumatic stress disorder (PTSD). Healthcare workers also are reporting higher rates of “moral injury,” prolonged moral trauma caused by factors including staffing shortages, a lack of equipment necessary to treat patients, decreasing wages, or feelings of helplessness. The exodus is increasing strain on already pressured healthcare systems as they struggle to fill vacancies and ensure patients' needs are met. Some experts—worried about how to restore and reinvigorate an essential, yet exhausted, workforce—are calling on the federal government for help to address healthcare worker shortages and urging healthcare systems to implement better preventive measures, such as creating chief wellness officer positions to oversee employees’ needs. With so many healthcare workers leaving their jobs, steps must be taken to ensure continuity in patient care and to prevent an implosion of the nation’s healthcare system.
PFIZER ORAL ANTIVIRAL Pfizer submitted a request for emergency use authorization (EUA) of its candidate oral antiviral COVID-19 treatment PAXLOVID—a combination of a new antiviral, PF-07321332, and ritonavir—with the US FDA on November 16. The submission is based on an interim analysis from a Phase 2/3 clinical trial showing the treatment demonstrated an 89% risk reduction in COVID-19-related hospitalization or death among high-risk adults when administered within 3 days of symptom onset. If authorized, the medication could help people with COVID-19 recover at home instead of seeking treatment at a hospital, and therefore reduce the strain on the healthcare system. Another similar COVID-19 treatment could be authorized soon, with an FDA advisory committee set to consider an EUA application from Merck and Ridgeback Biotherapeutics for their candidate antiviral drug molnupiravir on November 30. The US government plans to purchase 10 million courses of Pfizer’s treatment at a cost of $5 billion, although the deal is not yet finalized. Both Pfizer and Merck have announced voluntary license agreements with the Medicines Patent Pool to allow sub-licensed generic medicine manufacturers to produce the antivirals for 95 countries, including all low- and lower-middle income countries. However, availability will remain a challenge, as Merck expects to supply around 3 million courses of its treatment before February 2022 and Pfizer expects to supply only about 300,000 courses prior to February. For context, an average of more than 500,000 cases are confirmed daily worldwide.
ANTIMICROBIAL RESISTANCE An increasing number of countries are pledging to address antimicrobial resistance (AMR), but the COVID-19 pandemic has stalled progress and potentially drove an increase in the prevalence of AMR infections, according to a survey supported by the WHO, Food and Agriculture Organization (FAO), and the World Organization for Animal Health (OIE). Funding reductions, coordination challenges, lack of political commitment, and delays in surveillance are some of the factors impacting the development and implementation of national AMR plans, according to the 163 countries that responded to the Tripartite AMR survey. Part of the problem is a lack of regulatory enforcement in many countries, with only 33% of nations saying they have guidelines and practices in place to improve the use of antimicrobials in healthcare settings.
The Pan American Health Organization (PAHO) this week warned that the overuse of antimicrobial medicines has risen to unprecedented levels during the pandemic and some nations are reporting surges of drug-resistant infections. A large majority of hospitalized COVID-19 patients in the region are given antimicrobials for treatment—90% to 100%—but only 7% have a secondary infection that warranted the use of those drugs. The UK Health Security Agency (UKHSA) also released new data this week showing antibiotic-resistant bloodstream infections fell in 2020 for the first time since 2016. However, the agency cautioned the world could move from one pandemic into another “hidden pandemic” of AMR and warned the number of resistant infections could increase in the coming years if efforts to reduce them are not sufficient. For years, experts have been calling for more investment into ways to address AMR and prepare for potential outbreaks of drug-resistant diseases. World Antimicrobial Awareness Week (WAAW) is recognized November 18-24.
US OVERDOSE DEATHS An estimated 100,000 people died of drug overdoses in a yearlong period ending in April, a record high number spurred by the COVID-19 pandemic and a more deadly drug supply, according to new data from the US CDC. Social isolation and a lack of access to treatment during the beginning of the pandemic likely drove the increase, leading to what US President Joe Biden called “a tragic milestone.” The number of overdose deaths rose 28.5% from the same period a year earlier and has nearly doubled over the past 5 years. Experts warn that even if the COVID-19 pandemic ended today, the increasing use of the synthetic drug fentanyl will continue and urgent steps must be taken to improve access to treatment.
US HEALTHCARE WORKER EXODUS Due to the protracted nature of the COVID-19 pandemic, many US healthcare workers are facing extreme burnout and leaving their posts in droves. About 18% of healthcare workers in the US have quit since the beginning of the pandemic and another 12% have been laid off. The stressors of the current emergency have nearly doubled the risk of burnout among physicians, with up to 75% reporting symptoms of exhaustion, depression, sleep disorders, or post-traumatic stress disorder (PTSD). Healthcare workers also are reporting higher rates of “moral injury,” prolonged moral trauma caused by factors including staffing shortages, a lack of equipment necessary to treat patients, decreasing wages, or feelings of helplessness. The exodus is increasing strain on already pressured healthcare systems as they struggle to fill vacancies and ensure patients' needs are met. Some experts—worried about how to restore and reinvigorate an essential, yet exhausted, workforce—are calling on the federal government for help to address healthcare worker shortages and urging healthcare systems to implement better preventive measures, such as creating chief wellness officer positions to oversee employees’ needs. With so many healthcare workers leaving their jobs, steps must be taken to ensure continuity in patient care and to prevent an implosion of the nation’s healthcare system.
The problem is just anyone can't roll up to a hospital or ER and volunteer. I think staff levels will be critical for the next two to three years. That's just my opinion. If this thing continues as an endemic what happens then? There are lots of covidiots out there.
by dryrunguy The nursing shortage in the U.S. was quite palpable even before COVID hit. I mean, not a lot of young folks or people looking to revamp their careers by being trained as a health professional wake up one morning and say to themselves, "Gee, wouldn't it be fun to constantly be exposed to a deadly disease every day at work!"
by ti-amie In NYC many nurses are from either the Philippines or the English speaking Caribbean. If it wasn't for these men and women I don't know what staffing would look like.
by Suliso Is there any country with no nursing shortage? I can't think of one...
by ponchi101
Suliso wrote: ↑Thu Nov 18, 2021 10:23 pm
Is there any country with no nursing shortage? I can't think of one...
Easily solvable for the USA.
"2021 Medical Personnel Emergency Visa Program. Medical personnel get automatic visas if willing to relocate to American Under Developed Areas (i.e. Mississippi, Alabama, Kentucky, Parts of Texas). First come, first serve, simply show academic credentials".
In two months you will have 1/2 of Venezuelan medical personnel there, 3/4 of Argentina, and further miscellaneous countries.
Suliso wrote: ↑Thu Nov 18, 2021 10:23 pm
Is there any country with no nursing shortage? I can't think of one...
Easily solvable for the USA.
"2021 Medical Personnel Emergency Visa Program. Medical personnel get automatic visas if willing to relocate to American Under Developed Areas (i.e. Mississippi, Alabama, Kentucky, Parts of Texas). First come, first serve, simply show academic credentials".
In two months you will have 1/2 of Venezuelan medical personnel there, 3/4 of Argentina, and further miscellaneous countries.
Like that you can solve in Europe too. I meant no shortage because enough nurses are educated locally and stay in the profession. Do you know such a place?
Like that you can solve in Europe too. I meant no shortage because enough nurses are educated locally and stay in the profession. Do you know such a place?
No. Which was the reason I thanked your post. You are 100% right.
It has got to be one of the toughest ways to earn a living, nowadays.
by Deuce .
So much for the theory that one must possess intelligence to get into university...
I think mRNA works differently than a regular vaccine (I think) but the poster is right to ask the question.
Also, thanks to covidiots like him the virus has been able to mutate and work against the vaccines that are available.
Indeed, it is a valid question. But the answer is out there, and it is a technical one.
I actually think that it would be good for people to know why this virus' vaccine does not work that way.
by Deuce It's amazing that, even with the vaccines, some countries are seeing a record number of COVID-19 cases these days. This is very likely a testament to how easily transmissible the Delta Variant is.
Imagine what would be happening without the vaccines!
Deuce wrote: ↑Mon Nov 22, 2021 3:38 am
It's amazing that, even with the vaccines, some countries are seeing a record number of COVID-19 cases these days. This is very likely a testament to how easily transmissible the Delta Variant is.
Imagine what would be happening without the vaccines!
We basically saw what would happen without vaccines when Delta first emerged in India (I think their vaccination rate was around 10% at the time), and it wasn't pretty.
by ti-amie
by dryrunguy A new COVID variant has been identified in South Africa though it has not yet been designated by WHO as a Variant of Interest.
by ponchi101 On the good news side: Colombia has advanced enough to start providing boosters for people. Only "catch" is that if you get a booster it has to be from a different kind than the one you had already. So, for example, I could get J&J or Moderna, but not a third Pf/Bio.
Have to go and find out how that works.
by ti-amie
This fresh hell is named Omicron.
Have you noticed that as soon as folks start relaxing stuff the virus is like
by ti-amie
by ponchi101 Waiting for the rest of the world to ban flights from the USA. I mean, there is 45% of people there that will not get vaccinated.
(Sure, they are the ones that don't travel abroad, but I hope I am being clear).
by dryrunguy The new variant has already been found in Israel, Hong Kong, and I think one or two other places based on other reports I read this morning. So I guarantee you--that new variant is already here.
And WHO today classified it as a Variant of Interest.
by ti-amie
by ti-amie
by Suliso There has been some speculation why Southern Africa. One theory is that many immunocompromised and unvaccinated HIV positive patients (ca 8 million in SA alone) have trouble fully clearing the virus and thus serve as particularly good vessels for virus evolution and adaptation.
Contrary to the popular opinion the developed countries hoarding vaccines is long since not a problem any more, at least not in SA itself. Problem is very high vaccine hesitancy. Only about 70% coverage of childhood vaccines and less than 40% for covid. They have had to turn away fresh shipments and even destroy existing expiring stocks.
by ponchi101 And this is starting to look like Einstein's definition of madness. If you could not stop all the other variants from spreading, through travel restrictions and closing borders, why would THIS variant be any different?
It has not worked in over two years, it will not work now. Omicron, meet the world.
by Deuce Closing borders may not stop the spread, but it can potentially slow it down enough so that there is more time to study each variant as they occur, and thus learn more about it (is it more transmissible? are its effects more severe?, etc.), as well as buying some time to modify the vaccines to be able to better protect against it, if needed.
While closing borders may not be a universal 100% solution, to say that it has no significant effect would be incorrect.
by mmmm8
Suliso wrote: ↑Sat Nov 27, 2021 4:35 pm
There has been some speculation why Southern Africa. One theory is that many immunocompromised and unvaccinated HIV positive patients (ca 8 million in SA alone) have trouble fully clearing the virus and thus serve as particularly good vessels for virus evolution and adaptation.
Contrary to the popular opinion the developed countries hoarding vaccines is long since not a problem any more, at least not in SA itself. Problem is very high vaccine hesitancy. Only about 70% coverage of childhood vaccines and less than 40% for covid. They have had to turn away fresh shipments and even destroy existing expiring stocks.
SA also has a severe problem with availability of community medical services, a huge shortage of medical professionals outside of the more affluent areas (mostly served by private healthcare). I haven't looked into how they are distributing vaccines to those underserved areas, but the vaccination rate - COVID and otherwise - might not be driven by vaccine hesitancy but hesitancy around/poor access to facilities that offer vaccination.
by ti-amie
by ti-amie
by MJ2004
ti-amie wrote:
You can’t fix stupid.
by dryrunguy This morning's NY Times newsletter was something I really needed to read. It made some excellent points--all of which end up falling into the category of "duh!" when you really think about them.
The main points:
1) Whenever a new variant hits, we tend to jump to two assumptions. First, we assume it is more contagious. Second, we assume it is more deadly. These assumptions are not always accurate. So why do we automatically jump to these assumptions? Is it as simple as the alarmist headlines that scream at us everywhere we go?
2) Preliminary evidence, though very limited, suggests that existing vaccines remain effective against the Omicron variant in terms of preventing serious illness or death. This evidence, however, is limited because so few people in southern Africa are fully vaccinated. We should continue to take comfort in the effectiveness of our existing vaccines until new evidence indicates otherwise.
::
Again, when you really think about it, this is all "duh!" stuff. But as I wrote at the beginning, I needed to read it because I am especially guilty of #1.
by atlpam
dryrunguy wrote: ↑Mon Nov 29, 2021 4:17 pm
This morning's NY Times newsletter was something I really needed to read. It made some excellent points--all of which end up falling into the category of "duh!" when you really think about them.
The main points:
1) Whenever a new variant hits, we tend to jump to two assumptions. First, we assume it is more contagious. Second, we assume it is more deadly. These assumptions are not always accurate. So why do we automatically jump to these assumptions? Is it as simple as the alarmist headlines that scream at us everywhere we go?
2) Preliminary evidence, though very limited, suggests that existing vaccines remain effective against the Omicron variant in terms of preventing serious illness or death. This evidence, however, is limited because so few people in southern Africa are fully vaccinated. We should continue to take comfort in the effectiveness of our existing vaccines until new evidence indicates otherwise.
::
Again, when you really think about it, this is all "duh!" stuff. But as I wrote at the beginning, I needed to read it because I am especially guilty of #1.
Additionally, masking & distancing are still effective. Despite being fully vaccinated, we have continued to mask when going to stores. I expected to encounter few people wearing masks after returning to GA, but have been pleasantly surprised to still see many people masked at grocery stores, Target, etc. even though there are not any mask recommendations posted.
I fully expect Covid to become an annual vaccine like the flu vaccine where they do their best to predict the strains that will be circulating.
In the meantime, I am scheduled for my booster tomorrow.
dryrunguy wrote: ↑Mon Nov 29, 2021 4:17 pm
This morning's NY Times newsletter was something I really needed to read. It made some excellent points--all of which end up falling into the category of "duh!" when you really think about them.
The main points:
1) Whenever a new variant hits, we tend to jump to two assumptions. First, we assume it is more contagious. Second, we assume it is more deadly. These assumptions are not always accurate. So why do we automatically jump to these assumptions? Is it as simple as the alarmist headlines that scream at us everywhere we go?
2) Preliminary evidence, though very limited, suggests that existing vaccines remain effective against the Omicron variant in terms of preventing serious illness or death. This evidence, however, is limited because so few people in southern Africa are fully vaccinated. We should continue to take comfort in the effectiveness of our existing vaccines until new evidence indicates otherwise.
::
Again, when you really think about it, this is all "duh!" stuff. But as I wrote at the beginning, I needed to read it because I am especially guilty of #1.
Additionally, masking & distancing are still effective. Despite being fully vaccinated, we have continued to mask when going to stores.
I do, too, sometimes, just out of an abundance of caution for myself and others. But I think everyone else assumes I'm wearing a mask because I'm unvaccinated! I got a new job and quit a couple months beore my company's vaccine mandate went into effect, and someone (who isn't vaxxed) said to me slyly in private, "You're not vaccinated?" wink wink.
by dmforever I had a similar experience minus the wink winker. I went to an outdoor concert. You had to show either proof of vaccination or a negative Covid test less than 48 hours old. The people who were vaccinated were allowed to take off their masks. The others were not. Of course, they had zero way of enforcing that once people went inside. I kept my mask on. I'm sure people thought I was unvaccinated, which was fine by me. It was sort of lawn seating, so people gave me a ton of space. It was awesome.
Luckily in SF people very rarely go inside anywhere unmasked.
Kevin
by ti-amie We've never stopped masking either. It just never "felt" right to do so. NYC just issued a "strong recommendation" re masking indoors.
by ti-amie
"Change the definition of 'fully vaccinated'."
Hindsight is 20/20 but maybe we should've suspected something was up when all of a sudden boosters went from the medically vulnerable to "do not pass go" and get a booster shot?
by ti-amie
by Deuce I believe masks are still mandatory in most indoor locations across Canada here - with the exception of those sitting at a restaurant, playing sports, etc. But in stores, etc., masks are still a must in most - if not all - provinces.
And our number of infections has still been rising.
I still find it mind-boggling how people can think that that they're protected from the virus if they are 3 or 5 or 7 at a table in a restaurant/bar, all unmasked, all talking for an hour or so. Yes, you must show proof of double vaccination to enter the restaurant - but we've known for a long time now that even doubly vaccinated people can contract the virus. Symptoms are usually relatively mild in these cases - but not always. I'm not going to gamble, merely hoping that I'll be included in the 'usually' group.
by dryrunguy Here's the latest Situation Report. It's packed.
::
OMICRON VARIANT OF CONCERN Scientists, policymakers, and the general public are on high alert since the WHO on November 26 designated the newly identified SARS-CoV-2 variant B.1.1.529 a variant of concern (VOC), named Omicron*, based on the advice of the agency’s Technical Advisory Group on Virus Evolution (TAG-VE). The advisory group felt there was enough evidence that Omicron might be more transmissible, cause more severe disease, or escape immune defenses based on its large number and concerning types of mutations, particularly those on the spike protein that helps the virus bind to and enter cells in order to replicate. The WHO warned on November 29 that Omicron could have “severe consequences” in some parts of the world, urging its member states to speed up vaccinations of high-priority groups and take other steps to prepare. So far, no deaths due to the VOC have been recorded and younger patients with Omicron have had mild symptoms, according to South African doctors, but scientists need more data to determine severity. Preliminary evidence shows there may be an increased risk of reinfection with Omicron, meaning people who have infection-induced immunity may be at an increased risk of infection, just as we saw with Delta. Vaccination reduces the risk of severe disease, even with Delta infection, and the same could be true with Omicron. But many uncertainties remain, regarding whether Omicron is more transmissible or capable of immune escape, and public health advice likely will shift as more is learned about the VOC over the coming weeks. Despite global anxiety over Omicron, the WHO said most of the new COVID-19 cases globally are due to infection with the widely circulating Delta VOC.
South African officials first reported the new variant to the WHO on November 24, with the first known confirmed B.1.1.529 infection from a specimen collected on November 9. Notably, Dutch officials today announced they detected Omicron in samples collected nearly 2 weeks ago, days before 2 flights carrying infected passengers arrived in the Netherlands from South Africa and an indication the variant has been circulating for much longer than initially suspected. The number of Omicron cases appears to be increasing in nearly all South African provinces, as the country experiences a sharp increase in the daily number of new COVID-19 cases nationally and hospitalizations locally near the epicenter in Gauteng. South Africa has recorded 124 Omicron cases and at least 16 other nations have confirmed cases of Omicron. The US CDC on November 26 said no cases of Omicron have been detected in the country to date; we expect the first US cases to be identified over the coming days. International health officials and national leaders, including the G7 Health Ministers, commended the governments of South Africa and Botswana for quickly sharing information about the new variant with the WHO.
But that praise likely fell on deaf ears, as more and more countries implement travel restrictions on southern African nations, giving rise to even greater resentment among many Africans who already feel neglected because of continued vaccine hoarding among wealthy nations. For example, Israel closed its borders to all foreign nations for 14 days after confirming 1 case of Omicron in the country, and Japan and Morocco suspended all incoming flights for 1 month and 2 weeks, respectively. Several other countries have implemented travel restrictions, including the US, which on November 26 announced it will restrict travel from Botswana, Eswatini, Lesotho, Malawi, Mozambique, Namibia, South Africa, and Zimbabwe. Notably, of those nations, only South Africa and Botswana have confirmed Omicron cases. US President Joe Biden on November 29 said Omicron should be “a cause for concern, not a cause for panic,” adding that he does not anticipate more travel bans “at this point.” The comments raised questions about the effectiveness of the travel restrictions on southern African nations, especially as more countries outside the continent record Omicron cases.
The WHO called on nations with travel restrictions to ensure they are scientifically based and in line with the International Health Regulations (IHR). South Africa’s President Cyril Ramaphosa went a step further, urging nations to drop their travel restrictions and calling the measures “completely unjustified” and discriminatory. It is unlikely that travel restrictions will have any impact on the spread of the respiratory illness, especially after the variant clearly has spread worldwide, having now been detected on 5 continents—Africa, Asia, Australia, Europe, and North America—and community transmission is already occurring. The most effective individual preventive measures continue to include being fully vaccinated, wearing a well-fitting mask, frequent handwashing, avoiding crowds, and isolating if symptomatic, diagnosed with COVID-19, or exposed to someone with COVID-19. On a population level, it is imperative, now more than ever, that wealthy nations provide the support and resources necessary to help vaccinate, diagnose, and treat people in low- and middle-income nations (LMICs).
*The next 2 letters in the Greek alphabet naming convention were “Nu” and “Xi.” However, the WHO skipped those 2 letters because “Nu” could be confused with the word “new” and “Xi” is a common surname in China.
VACCINE MAKERS’ RESPONSE TO OMICRON Emergence of the Omicron SARS-CoV-2 variant in southern Africa has vaccine manufacturers discussing vaccine effectiveness and the possibility of updating vaccines to make them variant-specific. Omicron has around 50 mutations, and more than 30 of the mutations are located on the viral spike protein that is responsible for entry into host cells. The SARS-CoV-2 spike protein also is one of the primary antibody targets for the immune system. According to some analysis, most of the antibody target sites on Omicron’s spike protein are mutated, and several of those differences could indicate that Omicron is capable of escaping current vaccine formulations. A subset of Omicron’s spike mutations have been previously reported in the Beta and Delta variants, but 26 spike mutations are believed to be unique. Scientists are anticipating a decrease in antibody neutralization of the virus, and doctors in South Africa are reporting reinfections in patients who have already recovered from COVID-19.
Pfizer-BioNTech, Moderna, AstraZeneca, and J&J-Janssen—as well as laboratories worldwide—are working to determine how well the current vaccine formulations hold up against Omicron. Data from these experiments are expected within the next 2 weeks. Pfizer-BioNTech and Moderna said they could have variant-specific booster doses ready to ship in about 3 months. It will likely take several weeks before we know if current vaccine formulations are effective against Omicron, but they are expected to continue to help reduce the risk of hospitalization and death due to COVID-19. As a result, primary vaccination and booster doses are recommended for every person who is eligible to receive one.
VACCINE ACCESS The swift emergence and potential threat of the newly identified Omicron variant of concern (VOC) is being called a “We told you so” moment, as SARS-CoV-2 continues to spread in unvaccinated populations, largely located in low- and middle-income countries (LMICs). Wealthy nations and pharmaceutical companies have failed African nations and low-income countries by not delivering and helping distribute SARS-CoV-2 vaccines efficiently under a coordinated global plan, instead cutting in line, buying up supplies, not sharing technology, and therefore leaving large swaths of people vulnerable to infection. In a joint statement, the African Vaccine Acquisition Trust (AVAT), the Africa Centres for Disease Control and Prevention (Africa CDC), and COVAX said that while more than 90 million donated doses have been delivered to Africa through COVAX and AVAT—and millions more through bilateral agreements—most of the donations have been ad hoc, giving countries little notice before having to use doses close to expiration. The organizations called for the international community to commit to establishing reliable, consistent supply chains beginning January 1, 2022. One development that possibly could help to make this request a reality is the resumption of vaccine deliveries from the Serum Institute of India, following an 8-month pause of vaccine exports.
On November 26—the same day the WHO designated Omicron a variant of concern (VOC)—US President Joe Biden urged countries expected to attend the World Trade Organization (WTO) 12th Ministerial Conference (MC12) this week to approve a proposal that would temporarily waive intellectual property (IP) protections for SARS-CoV-2 vaccines, therapeutics, and diagnostics technology. Such a waiver would make it easier for vaccine manufacturers in other countries to make vaccine doses for distribution to LMICs. However, late that day, the WTO indefinitely postponed the meeting, which was set to run from today through December 3, due to the announcement of travel restrictions and quarantine requirements implemented due to the designation of Omicron. This is the second time the WTO directorate has postponed MC12. WTO Director-General Ngozi Okonjo-Iweala urged countries to continue negotiations until an in-person meeting can be held. Nursing unions from 28 countries and territories have filed a complaint with the UN Special Rapporteur on the Right to Health Dr. Tlaleng Mofokeng, calling for an investigation into how the actions of several nations to not support an IP waiver at the WTO allegedly violate the “right to physical and mental health of everyone” during the COVID-19 pandemic.
To date, the companies that make the mRNA SARS-CoV-2 vaccines have refused to share information and technology that would enable other companies to make generic versions. South Africa-based Afrigen Biologics and Vaccines is working to replicate Moderna’s vaccine formula, but that process could take 3 years. Notably, the company could begin manufacturing a replica within a year if Moderna supplied the relevant information. Until a vaccine formula is hacked or shared, only a handful of countries will continue to manufacture vaccines—including China, several European nations, India, and the US—furthering supply chain bottlenecks.
US/UK BOOSTER GUIDANCE With prevailing uncertainties on the characteristics of the Omicron variant, the US and UK governments have strengthened their recommendations for all adults to receive booster doses of a SARS-CoV-2 vaccine. Previously, the US CDC had authorized booster doses for all adults but said young adults may get a booster if they wanted. In their revised language, the CDC recommends that all adults, regardless of age, should get a booster dose. Specifically, all adults should get their booster once they are 6 months post-Moderna or Pfizer-BioNTech vaccination, or 2 months post-J&J-Janssen vaccination. CDC Director Dr. Rochelle Walensky stated that booster doses “have demonstrated the ability to safely increase people’s protection against infection and severe outcomes,” and cited the upcoming winter holiday season and the Omicron variant as extra incentives to get boosted to prevent another winter surge. Dr. Walensky also emphasized the importance of getting tested if you feel sick, which could further help identify the spread of the Omicron variant. Pfizer-BioNTech reportedly plans this week to apply for US regulatory approval for booster doses for 16- and 17-year-olds.
The UK also expanded booster dose eligibility to all adults and halved the gap time from 6 months to 3 months in an effort to stave off the new variant. The UK has reported 11 cases of Omicron. The Joint Committee on Vaccination and Immunisation (JCVI) made a series of recommendations that were accepted by the government, including saying children aged 12 to 15 should be eligible to receive a second vaccine dose and severely immunocompromised people can receive a fourth dose after their 3-dose primary series. The government also announced new rules requiring face masks be worn in shops and on public transportation in England and all contacts of Omicron cases will be required to self-isolate regardless of vaccination status.
WHA SPECIAL SESSION With the designation of Omicron as the latest variant of concern showing the COVID-19 pandemic is far from over, the World Health Assembly (WHA) began a special session on November 29 with the intent of formally beginning talks on a global pandemic treaty. Following recent breakthroughs in negotiations, the final resolution says that member nations will establish “an intergovernmental negotiating body” to “draft and negotiate a WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response,” with a focus on the final document being adopted as a binding international treaty under Article 19 of the WHO constitution. The US, along with several other nations, had opposed a legally binding treaty, but it appears the US has at least partially relented. The only other such WHO treaty is the Framework Convention on Tobacco Control. In his opening statement, WHO Director-General Dr. Tedros Adhanom Ghebreyesus said Omicron “demonstrates just why the world needs a new accord on pandemics,” noting that COVID-19 “is not done with us.” If member states agree to work on new international rules for pandemic preparedness and response, the process would begin no later than March 1, 2022, and a final outcome would come into force in 2024, but only if the process runs smoothly. In a November 28 opinion piece, Dr. Tedros noted that the COVID-19 pandemic will not be the last, and preparing for “more inclusive, equitable, and accountable” governance will help bolster future global health security systems.
US HEALTHCARE WORKER VACCINE REQUIREMENT A federal judge has issued a preliminary injunction against the Biden administration’s SARS-CoV-2 vaccine requirement for certain healthcare workers. The mandate, issued through the Centers for Medicare and Medicaid Services (CMS), requires healthcare workers to get vaccinated against COVID-19 or risk their facilities losing Medicare and Medicaid funding. It states that workers must receive their first dose by December 6 and their second dose by January 4. The preliminary injunction blocks the mandate from taking effect in 10 states: Missouri, Nebraska, Arkansas, Kansas, Iowa, Wyoming, Alaska, South Dakota, North Dakota, and New Hampshire. US District Judge Matthew Schelp handed down the injunction citing possible flaws in the policy’s language and a lack of input from Congress. He also cited the potential for healthcare facilities to become severely understaffed while multiple healthcare workers take sick leave to recover from vaccine side effects. While the injunction is a step back in efforts to vaccinate all healthcare workers, it is not a final ruling on whether the mandate can move forward. Legal experts have commented that the mandate appears to be firmly based in the authority that CMS has over how facilities receiving federal funding are run. Regardless, the lawsuit must now move through the court system, and possibly end up before the US Supreme Court.
MOLNUPIRAVIR Merck and Ridgeback Biotherapeutics announced new results from their MOVe-OUT study examining the companies’ investigational COVID-19 treatment molnupiravir, a ribonucleoside analog drug designed to inhibit replication of SARS-CoV-2. The data indicate that molnupiravir may be less effective than initial studies suggested. The initial results, released in October, demonstrated a 48% relative risk reduction among a group of 775 participants. The new results show a 30% relative risk reduction among a group of 1,433 participants. There were 9 deaths in the placebo group of the study and 1 death in the group that received molnupiravir. Merck published the data ahead of a meeting of the US FDA’s Antimicrobial Drugs Advisory Committee, set for today. The committee is expected to discuss questions involving whether the drug should be available to people who are pregnant, whether the drug could lead to the development of new SARS-CoV-2 variants, and whether molnupiravir should be authorized for everyone or only certain groups of people. Another potential topic of discussion include the potential risk of mutations, which were detected with an Ames test but not detected in a follow-up animal study.
by ti-amie Re US District Judge Matthew Schelp:
Matthew T. Schelp is a judge on the United States District Court for the Eastern District of Missouri. President Donald Trump (R) nominated Schelp on December 2, 2019. The United States Senate confirmed Schelp on February 12, 2020, by a vote of 72-23.
by ponchi101 Silly question here. Anybody knows why they called it OMICRON (Greek alphabet #15) as opposed to Epsilon? Or did we go through all the others in the middle and I missed them?
by JazzNU
dryrunguy wrote: ↑Mon Nov 29, 2021 4:17 pm
2) Preliminary evidence, though very limited, suggests that existing vaccines remain effective against the Omicron variant in terms of preventing serious illness or death. This evidence, however, is limited because so few people in southern Africa are fully vaccinated. We should continue to take comfort in the effectiveness of our existing vaccines until new evidence indicates otherwise.
Evidence is also limited because South Africa has comparatively fewer senior citizens to many other countries. Population over 60 is something in the single digits, like 5-7% of the population (which is very sad if you think about it). So as you hear these preliminary reports of "mild symptoms" keep in mind they are talking mostly about younger patients, for instance, the outbreak among college students in Pretoria. And the articles I read said they also have fewer comorbidities.
by JazzNU
ponchi101 wrote: ↑Tue Nov 30, 2021 8:33 pm
Silly question here. Anybody knows why they called it OMICRON (Greek alphabet #15) as opposed to Epsilon? Or did we go through all the others in the middle and I missed them?
Not a silly question, it's mentioned briefly in the report, but here's a more complete explanation.
I'm not posting the article here since it's mega long, but I thought it was interesting enough to mention.
The link won't work unless you have an FT account, but I've found that if you google the name of the article you can typically access it that way. If you can't get to the article and would like to read it, just let me know.
dryrunguy wrote: ↑Mon Nov 29, 2021 4:17 pm
2) Preliminary evidence, though very limited, suggests that existing vaccines remain effective against the Omicron variant in terms of preventing serious illness or death. This evidence, however, is limited because so few people in southern Africa are fully vaccinated. We should continue to take comfort in the effectiveness of our existing vaccines until new evidence indicates otherwise.
Evidence is also limited because South Africa has comparatively fewer senior citizens to many other countries. Population over 60 is something in the single digits, like 5-7% of the population (which is very sad if you think about it). So as you hear these preliminary reports of "mild symptoms" keep in mind they are talking mostly about younger patients, for instance, the outbreak among college students in Pretoria. And the articles I read said they also have fewer comorbidities.
You think because they don't live long enough? That's probably true as well, but the other factor is much larger number of children.
JazzNU wrote: ↑Tue Nov 30, 2021 9:31 pm
Evidence is also limited because South Africa has comparatively fewer senior citizens to many other countries. Population over 60 is something in the single digits, like 5-7% of the population (which is very sad if you think about it). So as you hear these preliminary reports of "mild symptoms" keep in mind they are talking mostly about younger patients, for instance, the outbreak among college students in Pretoria. And the articles I read said they also have fewer comorbidities.
You think because they don't live long enough? That's probably true as well, but the other factor is much larger number of children.
Yes, unfortunately I think good deal of it has to do with a much lower life expectancy age than we're typically used to seeing in the Western World. But I'm sure a large number of children is a factor as well.
by Suliso To the surprise of no one Omikron has been found in Europe in older samples. Several weeks before SA announced it.
by meganfernandez
Suliso wrote: ↑Wed Dec 01, 2021 4:44 pm
To the surprise of no one Omikron has been found in Europe in older samples. Several weeks before SA announced it.
Yeah, isn't SA just really good at the epidemiology part of this and that's likely why they found it? Not because people think it originated there?
by patrick Now, Omicron is in USA (First case was in California)
by Suliso In Switzerland as well, in two separate places including my city. Maybe Australia and New Zealand can lock it away again for some time (not forever), but no one else in the West has a chance. Not even worth trying.
by JazzNU I wouldn't say it's not worth trying while scientists figure out the severity of this variant. There was some success with containment with the measures imposed of I believe they are now called the Beta and Gamma variants.
by JazzNU
by ponchi101 Down here, just got my Pfizer booster. 5 hours in line, because, surprisingly, the private companies are running it now, and they are worse at doing stuff than the Govt. But, got my shot, and by now, after 7 negative PCR tests in one year, traveling to the USA in May, then to Vennieland in October, spending time with two severely sick patients and never even catching the damn thing, with this booster I gather I can say: "COVID, Foxtrot Yucatan!!!"
(Achoo...)
by Deuce But you said that in Colombia, people had to get a booster which was from a different company from their original shots...
What changed so that you could get the Pfizer booster?
ponchi101 wrote: ↑Fri Nov 26, 2021 3:44 pm
On the good news side: Colombia has advanced enough to start providing boosters for people. Only "catch" is that if you get a booster it has to be from a different kind than the one you had already. So, for example, I could get J&J or Moderna, but not a third Pf/Bio.
Have to go and find out how that works.
by ponchi101 The initial information was given by a friend. The real information was given by the nurse that gave me the shot.
by dryrunguy Here's the latest Situation Report from Johns Hopkins. We have some new info about Omicron, new research on mortality associated with long COVID, a significant increase in the number of lung transplants being performed in the U.S., and ethical considerations surrounding who gets a lung transplant--and who does not.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 262.2 million cumulative cases and 5.2 million deaths worldwide as of December 1. Global weekly incidence increased for the sixth consecutive week, while global weekly mortality declined from the previous week. Weekly incidence increased by 5.61% compared to the previous week, and mortality decreased by 9.4%. During the week ending November 30, nearly 3.8 million new cases were reported, with the African, Western Pacific, and European regions reporting increases, according to the WHO COVID-19 Weekly Epidemiological Update. While the overall number of deaths decreased, 2 regions—South-East Asia and Africa—reported increases of 26% and 7%, respectively. Notably, the European region reported the highest weekly incidence in deaths of 3.1 per 100,000 population, while <1 new death per 100,000 was reported in all other regions.
The newly designated variant of concern (VOC), Omicron, appears to be in at least 23 countries and continues to be detected in new areas, according to the WHO. GISAID reports 25 countries and territories have confirmed Omicron cases, while BNO News reports cases of the VOC have been confirmed in 31 countries and territories, totaling 379. In South Africa, where Omicron was first identified, health authorities are reporting a dramatic surge in the number of new COVID-19 cases. Since November 24, when health officials notified the WHO about the new variant, the 7-day average of daily cases has increased nearly 6-fold. The number of newly confirmed cases doubled on December 1 over the previous day’s count, rising from 4,373 to 8,561, and experts are bracing for even greater increases. The US has confirmed 2 cases of Omicron, while 15 nations in the European Union and European Economic Area (EU/EEA) have reported a total of 79 Omicron cases as of today, with 20 of those cases being confirmed since yesterday. Notably, the majority of the cases have a history of travel to African countries, but several cases of apparent community transmission have been documented, including in the US.
It appears Omicron is outpacing the Delta VOC in South Africa, but it remains unclear whether the new VOC will overtake Delta in other regions, such as Europe, where Delta remains the dominant circulating variant. Notably, prior to Omicron, South Africa did not have much circulating Delta. While Omicron certainly seems to be more transmissible than Delta—and appears to be capable of causing breakthrough cases among vaccinated individuals—we continue to await lab and real-world data about how Omicron’s mutations impact transmissibility, vaccine-induced and natural immunity effectiveness, and disease severity.
Global Vaccination
The WHO reported 7.9 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of December 1. A total of 4.2 billion individuals have received at least 1 dose, and 3.28 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations has increased over the past week, up to 32.78 million doses per day on December 1 from a recent low of 30.74 million doses per day on November 27.*
Our World in Data estimates that there are 4.3 billion vaccinated individuals worldwide (1+ dose; 54.62% of the global population) and 3.45 billion who are fully vaccinated (43.61% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 48.5 million cumulative COVID-19 cases and 780,131 deaths. The current daily incidence average is approximately 80,230 new cases per day and appears to be holding relatively steady since mid-November, although there may be reporting delays due to the Thanksgiving holiday. Daily mortality appears to have dropped over the holiday—likely due to lags in reporting—but appears to be rising again, with the US currently averaging 816 deaths per day.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 462.3 million cumulative doses of SARS-CoV-2 vaccines. The daily vaccination trend reached a recent peak at 1.44 million doses on November 23 but has declined sharply to 1.03 million doses as of November 26.*
There are 233.6 million individuals who have received at least 1 vaccine dose, equivalent to 70.4% of the entire US population. Among adults, 82.8% have received at least 1 dose, as well as 19.8 million children under the age of 18. A total of 197.4 million individuals are fully vaccinated, which corresponds to 59.4% of the total population. Approximately 71.2% of adults are fully vaccinated, as well as 13.5 million children under the age of 18. Since August 13, 41.9 million fully vaccinated individuals have received an additional or booster dose, including 44.7% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
FIRST OMICRON CASES IN US The US has confirmed 2 cases of SARS-CoV-2 caused by the Omicron variant of concern (VOC). The first case was confirmed by California state health and US CDC officials on the afternoon of December 1. That patient is a fully vaccinated (not boosted) teacher from San Francisco, who returned from a trip to South Africa on November 22 and tested positive on November 29. The patient’s symptoms were mild, and they are recovering at home. The second case was confirmed today in a fully vaccinated man who traveled to New York City to attend the Anime NYC 2021 convention at the Javits Center from November 19-21. That patient has since recovered. In both cases, officials are conducting contact tracing but have not yet identified linked cases. More Omicron cases likely will be confirmed in the US over the coming days, especially considering the second case—who did not travel outside of the US—indicates Omicron is spreading within the nation. Additionally, domestic viral sequencing has increased significantly since the start of the pandemic, increasing the likelihood that other cases will be identified.
In response to the emergence of Omicron, US President Joe Biden is scheduled to deliver a speech at 1 pm ET today outlining a domestic plan for COVID-19 in the winter months. He is expected to announce an extension to mask mandates on public transit into March 2022. The mandate was set to end on January 18, 2022, and this new extension will extend until March 18, 2022. Reportedly, President Biden also will announce tighter restrictions for all individuals entering the US via air travel, including providing proof of a negative COVID-19 test taken within 24 hours of entering the country. Other pieces of the Biden administration’s 9-pronged plan likely will include efforts to increase SARS-CoV-2 vaccine and booster dose uptake and access to at-home COVID-19 tests.
As of now, many unknowns remain about how the Omicron VOC will impact the US and other nations, with uncertainties regarding economic recovery looming. On one hand, there is hope that people with vaccine-induced or natural immunity will be somewhat protected against severe disease, although the CEO of Moderna recently predicted that the current cadre of SARS-CoV-2 vaccines likely will be less effective against Omicron. All of the vaccine manufacturers are working on strategies to combat the new VOC, with new vaccines or booster doses expected to be ready within 3 months.
US VACCINE REQUIREMENTS A federal judge in Louisiana on November 30 temporarily halted enforcement of the Biden administration’s SARS-CoV-2 vaccine requirements for healthcare workers employed at institutions receiving Medicare or Medicaid funding, 1 of 3 court decisions this week that call for a freeze on vaccination rules as they make their way through the courts. One of the emergency regulations in question, issued by the Centers for Medicare and Medicaid Services (CMS), requires healthcare workers be fully vaccinated against COVID-19 by January 4, 2022, or risk their facilities losing Medicare and Medicaid funding. The day before, a federal judge in St. Louis, Missouri issued a preliminary injunction on the CMS requirement that blocked its enforcement in 10 states. The ruling from US District Judge Terry Doughty of the Fifth Judicial District Court in Louisiana applies nationwide, except in the 10 states covered under the prior order. In his opinion, Judge Doughty cited protection of the separation of powers under the US Constitution, saying the Biden administration does not have the authority to bypass the US Congress during “indefinite states of emergency.” The US Department of Justice did not comment on the order, but the department already has asked the 8th US Circuit Court of Appeals to revive the mandate blocked on November 30 by the Missouri district court, and it is expected to do so in the Louisiana case.
In a separate case, US District Judge Gregory Frederick Van Tatenhove of the US District Court for the Eastern District of Kentucky granted a preliminary injunction of the Biden administration’s vaccine requirements for employees of government contractors, which prevents the rule’s enforcement in Kentucky, Ohio, and Tennessee while it makes its way through the courts. The White House defended the regulation and said the Justice Department will defend it in court. Another temporary standard issued through the US Department of Labor’s Occupational Safety and Health Administration (OSHA) requiring employers with 100 or more employees to compel their employees to be vaccinated or undergo weekly testing is on hold due to a separate court order. In the latest KFF COVID-19 Vaccine Monitor, released today, more than half of employees who work for such companies either say their employer already requires vaccination (36%) or say they want their employer to require it (17%). Four (4) in 10 employees (41%) say they do not want their employer to require SARS-CoV-2 vaccination.
PANDEMIC TREATY At the conclusion of a special session of the World Health Assembly (WHA) on December 1—only the second to ever be held since the WHO’s founding in 1948—WHO member states agreed to begin negotiations on an international agreement, or “pandemic treaty,” meant to strengthen pandemic prevention, preparedness, and response. Looking ahead, a newly formed intergovernmental negotiating body will meet at least once by March 1, 2022, and a second time by August 1, 2022; deliver a progress report to the 76th World Health Assembly in 2023; and submit a final document for consideration by the 77th World Health Assembly in 2024. WHO Director-General Dr. Tedros Adhanom Ghebreyesus said the consensus decision—which came less than a week after the designation of Omicron as a new SARS-CoV-2 variant of concern—said the action “is cause for celebration, and cause for hope.” Notably, the adopted resolution stops short of calling for a legally binding instrument, which has seen support from the WHO Director-General, the EU, and Britain. The US said it supports the development of “a new WHO convention, agreement or other international instrument and making agreements to improve the effectiveness and agility of international health regulations.” Other nations, including China and Russia, have shown hesitation toward approving a legally binding agreement. The process resulting from the WHA’s decision will be long and likely fraught with politicization and setbacks.
POST-SEVERE COVID-19 MORTALITY RISK Researchers are learning more about the post-acute sequelae of COVID-19 (PASC), including the symptoms of so-called long COVID, and a recent report published in Frontiers in Medicine raises concerns for people who are recovered from severe COVID-19 requiring hospitalization. The analysis of more than 13,500 patients conducted by researchers in Florida (US) found that severe COVID-19 patients were significantly more likely to die in the year following recovery than patients who had mild disease or never contracted the illness. For patients with severe COVID-19, the adjusted all-cause mortality risk was significantly higher compared with both COVID-19-negative patients (HR 2.50; 95% CI 2.02, 3.09) and patients who had mild COVID-19 (HR 1.87; 95% CI 1.28, 2.74). A majority of the deaths (79.5%) were due to causes other than respiratory or cardiovascular reasons, and the risk of death within 1 year was 3 times as high for patients younger than 65 years compared with COVID-19-negative patients under age 65 (HR 3.33; 95% CI 2.35, 4.73). The study’s findings suggest that patients with severe COVID-19 experienced an overall decline in their health after recovery, leaving them vulnerable to other health conditions, and underline the importance of vaccination, which is highly effective at preventing severe COVID-19.
LUNG TRANSPLANTS Prior to the COVID-19 pandemic, about 2,000 lung transplants occurred each year in the US, primarily for patients with lung diseases such as emphysema, cystic fibrosis, and pulmonary fibrosis. But the number of lung transplants for COVID-19 patients is rising quickly, increasing tenfold in the first 2 years of the pandemic, while the overall number of lung transplants is down compared with previous years, according to data from the United Network for Organ Sharing (UNOS). Currently, almost 1 in 10 lung transplants are performed in COVID-19 patients, and nearly 240 people nationwide have received lung transplants due to COVID-19 since August 2020. The rising demand for COVID-related lung transplants is forcing medical professionals to confront the complicated ethical issue of who should get the few available transplants. The American Society of Transplant Surgeons says in a position statement that “‘good medicine’ is to mitigate against known risks, and vaccination is an effective tool that decreases the risk for the transplant candidate and recipient.” In line with this recommendation, some transplant centers have stated outright that patients on waiting lists will lose their spot if they are not vaccinated against COVID-19. Part of this reasoning is because transplant recipients, who need to take immune-suppressing drugs for life, are more vulnerable to acquiring infections, including COVID-19, that could threaten their lives.
ponchi101 wrote: ↑Thu Dec 02, 2021 2:44 pm
The initial information was given by a friend. The real information was given by the nurse that gave me the shot.
And this is what makes What'sApp so dangerous. I mean granted it wasn't Nicki Minaj's cousin's friend who told you but imagine how many other people your friend told this to and that it found its way to that app?
by ti-amie Meanwhile...
This used to be a majority African Caribbean/African American neighborhood. I believe there is also a large Orthodox Jewish population as well. An interesting choice for whoever is behind this.
ponchi101 wrote: ↑Thu Dec 02, 2021 2:44 pm
The initial information was given by a friend. The real information was given by the nurse that gave me the shot.
And this is what makes What'sApp so dangerous. I mean granted it wasn't Nicki Minaj's cousin's friend who told you but imagine how many other people your friend told this to and that it found its way to that app?
I would not say his comment would have been troublesome. He was actually telling me that Colombia was approving boosters for people in my age group, but that I would get something different than my initial one on a "mix" policy. He was never implying not to get the booster.
The issue yesterday for vaccination was the extremely long line, which, in retrospect, is good. The Anti-vaxxers, "Covid is a plot" crowd is very lightly represented here. Some people like my buddy N, who simply is an alternative-medicine fanatic, but other than that, no real crowds of people marching because their freedoms are being trampled.
We just want to get back to normal ASAP. So vaccination it is.
by ti-amie
by ti-amie
I think for younger people in the field, with no family to support or mortgage to pay this is a great option.
by ti-amie
by JazzNU In what world is 2020 the year the traveling nursing industry took off? Most definitely the words of someone who doesn't know people that work in healthcare. 2020 is maybe the year the general public learned it was as big of an industry as it is, but hardly the year it took off, not even close.
by ti-amie
JazzNU wrote: ↑Mon Dec 06, 2021 9:28 pm
In what world is 2020 the year the traveling nursing industry took off? Most definitely the words of someone who doesn't know people that work in healthcare. 2020 is maybe the year the general public learned it was as big of an industry as it is, but hardly the year it took off, not even close.
This is the first I've heard of it. When would you say it started?
JazzNU wrote: ↑Mon Dec 06, 2021 9:28 pm
In what world is 2020 the year the traveling nursing industry took off? Most definitely the words of someone who doesn't know people that work in healthcare. 2020 is maybe the year the general public learned it was as big of an industry as it is, but hardly the year it took off, not even close.
This is the first I've heard of it. When would you say it started?
I don't know when it started, but my sister, an NP, has been talking about it for about 10 years, as something she might want to do. FWIW.
JazzNU wrote: ↑Mon Dec 06, 2021 9:28 pm
In what world is 2020 the year the traveling nursing industry took off? Most definitely the words of someone who doesn't know people that work in healthcare. 2020 is maybe the year the general public learned it was as big of an industry as it is, but hardly the year it took off, not even close.
This is the first I've heard of it. When would you say it started?
A good while ago, maybe the 90s. Grew exponentially in the 21st century, but certainly not something new for 2020. Been a growing industry for years, took off long ago. My cousin worked as a traveling nurse in the early 2000s, hard to remember the exact year but I'd ballpark it around 2002-2004 when she took a few contracts. I remember her getting a $10k signing bonus* and a paid 3BR apartment in addition to the regular pay while she worked here for 3 months in the summer.
**Though a caveat on her level of bonus, pay and benefits. This was before there was a proliferation of a million online university programs that offer nursing degrees with low admission standards, so I'm not certain, but I believe that her bonus along with her pay was higher than others because she is a BSN, a rarer nursing degree at that time and in demand.
by dryrunguy Here's the latest situation report. A brief note about nomenclature: Apparently we don't use the word "illiteracy" anymore. It's now "learning poverty." I've never seen that term used before. In any case, the section on education losses is pretty alarming.
::
OMICRON EARLY DATA As scientists worldwide continue to learn more about the newly identified SARS-CoV-2 variant of concern (VOC) Omicron (B.1.1.529), early data from South Africa suggest that the VOC could be more transmissible and more likely to evade existing immunity from vaccination or natural infection but may cause less serious illness than previous variants. However, experts cautioned about placing too much emphasis on these early indications because of Omicron's novel nature and information on hospitalizations and deaths typically lag several weeks behind initial outbreaks. In South Africa, where some of the earliest Omicron cases were detected, the variant is spreading at an alarming pace, with a near vertical spike in the number of new COVID-19 cases. One estimate, which is not yet peer-reviewed, shows a doubling time of about 3.3 days, more than twice as quickly as Delta. A preprint report on Omicron’s clinical presentations at a large hospital in South Africa suggests the variant may cause less severe disease, although it is still too early to draw conclusions.
There are concerns that Omicron could be more transmissible due to its large number of spike protein mutations, some of which have not been seen in other variants. One preprint analysis (not yet peer-reviewed) conducted by the US-based research firm nference speculates Omicron could have acquired a specific insertion mutation (ins214EPE) from the genome of a different virus, such as a seasonal coronavirus that causes the common cold. The researchers said this genetic code, which has not been detected in other SARS-CoV-2 variants, could make the virus more likely to evade some immune system responses and make it more accustomed to human hosts. Another preprint study (not yet peer-reviewed) from South Africa suggests Omicron may carry an increased risk of reinfection, indicating the virus could escape some immune system defenses and raising questions about vaccine-induced immunity. Previous infection offered some protection against the Beta and Delta variants, but reinfections have increased since the emergence of Omicron. Additional research is needed into Omicron’s potential for immune escape, and experts note that existing immunity—whether from previous infection or vaccination—could still provide some protection from severe disease, hospitalization, or death.
MIX & MATCH BOOSTERS A study published online December 2 in The Lancet describes a randomized, controlled trial investigating the reactogenicity and immunogenicity of 7 SARS-CoV-2 vaccines* administered as third dose boosters to 2,878 patients aged older than 30 years who already received a primary 2-dose regimen of either the AstraZeneca-Oxford vaccine at least 70 days earlier or the Pfizer-BioNTech vaccine at least 84 days earlier. Reactogenicity was acceptable and most brands elicited a strong immune response to wild-type virus and the Delta variant, particularly the Moderna and Pfizer-BioNTech vaccines as boosters. A majority of the boosters raised antibody levels and neutralizing responses, even in mix-and-match scenarios, although Pfizer-BioNTech and Moderna produced much higher levels than the other brands. More research is needed into longer-term immune response and protection from infection after booster dose administration, but the findings provide a basis for policymakers who can now recommend people who initially received the Pfizer-BioNTech or AstraZeneca-Oxford vaccines get whichever vaccine booster is available, possibly increasing access to usable booster options.
Another study posted on the medRxiv preprint server (not yet peer-reviewed) on December 5 studied the use of the J&J-Janssen vaccine as a booster for individuals fully vaccinated with the Pfizer-BioNTech vaccine at least 6 months prior. Findings indicate that using the J&J-Janssen vaccine as a booster produced a slower and more sustained response to wild-type virus and Beta and Delta variants, while a Pfizer-BioNTech booster produced a faster and stronger response that dipped more quickly. These results mildly contradict findings from a US National Institutes of Health clinical trial in which a smaller antibody level increase was documented for the J&J-Janssen booster, but this may be due to a difference in timing between second and third dose boosters for the studies.
*The 7 vaccines used as boosters included those from J&J-Janssen, Moderna, AstraZeneca-Oxford, Pfizer-BioNTech, Novavax, and Valneva, the latter 2 of which are under review in Europe. The investigational SARS-CoV-2 vaccine from CureVac also was used in the study, but the company has since withdrawn the vaccine candidate from the approval process.
US GLOBAL VAX PROGRAM On December 6, USAID announced a new initiative aimed at increasing international coordination of SARS-CoV-2 vaccine administration through identifying and overcoming barriers to access, dubbed the Initiative for Global Vaccine Access (Global VAX). Sub-Saharan Africa was noted as a priority region for the initiative, which will be a whole-of-government effort. USAID Administrator Samantha Power announced that US$400 million from the American Rescue Plan Act will be allotted to the program, adding to the US$1.3 billion that the US already has committed globally for vaccine readiness. Of the new commitment, US$315 million will support country-specific needs for vaccine delivery and administration in low- and middle-income countries (LMICs), and US$10 million will support in-country vaccine manufacturing. The remaining US$75 million will be utilized for additional support of USAID’s Rapid Response Surge Support to deliver life-saving resources to COVID-19 hotspots, including an effort to improve oxygen production and delivery. Global VAX efforts supported by these funds include improving cold chain supply and logistics, service delivery, vaccine confidence and demand, human resources, data and analytics, local planning, and vaccine safety and effectiveness.
The US is the leading donor of SARS-CoV-2 vaccines to other countries, but a WHO official said on December 5 that the donations “are not enough” and called on other nations to do more. The Biden administration announced that it is sending 9 million vaccine doses to Africa and 2 million vaccines to other areas of the world. Only about 7.5% of the African population is fully vaccinated against COVID-19, compared to the 60% of the US population and 66% of Europeans. With this donation, the US has provided a total of 100 million vaccine doses to Africa and a total of 291 million doses to 110 countries. The announcement was made December 3—with shipments made the same day—and comes 1 day after US President Joe Biden announced new measures to combat COVID-19 through the winter months, both domestically and abroad. Included among those measures is the aim to send more than 200 million vaccine doses abroad in 100 days—focusing on delivery to high-risk countries—and increasing vaccine manufacturing capacity to meet global demand. The latter is 1 of the 3 divisions of funds outlined in the Global VAX initiative.
NEW YORK CITY VACCINE MANDATES On December 6, New York City Mayor Bill de Blasio announced expansions to the city’s “Key to NYC” program, including a new vaccination mandate that will apply to approximately 184,000 private employers and their in-person employees. The city already has the most sweeping local requirements in the nation, mandating vaccinations for city employees; hospital and nursing home workers; employees and customers aged 12 and older of indoor restaurants, entertainment venues, and gyms; and children engaged in high-risk extracurricular activities such as sports, band, or dance. Under the new expansion, those people will now have to show proof of full vaccination by December 27, and children aged 5 to 11 will be required to show at least partial SARS-CoV-2 vaccination (at least 1 dose for 2 dose regimens) beginning December 14 to visit those venues or engage in high-risk extracurricular activities. Mayor de Blasio noted that there would be exemptions on the basis of medical or religious reasons, but the mandates likely will face legal challenges. Enforcement processes of the mandate are currently unclear but are expected to be announced next week. As of today, 78% of New York City residents have received at least one dose of a SARS-CoV-2 vaccine and 70% of New Yorker City residents are fully vaccinated.
RESTRICTIONS IN EUROPE Tens of thousands of people gathered this weekend in various northwest European cities to protest newly instituted COVID-19 restrictions amid the region’s ongoing surge in cases. In Vienna, Austria, more than 40,000 demonstrators rallied to show disapproval of the government’s recent announcement of a 20-day lockdown and plans to make vaccinations mandatory beginning in February 2022. The Netherlands saw its first major demonstration against restrictions that began last weekend, including nighttime closures of bars, restaurants, and most stores. Two weeks ago, violent protests erupted after the Dutch government announced plans to ban most unvaccinated people from such public places. In Brussels, Belgium, about 8,000 people protested the government’s recent mitigation requirements, including making mask-wearing mandatory for children older than age 6 and closing kindergartens and primary schools beginning December 20. Police had to use water cannons and tear gas to disperse demonstrators who were throwing objects at them at a roadblock.
In Germany, the government approved plans to make vaccinations mandatory next year and allow only vaccinated and recovered people to access retail shops (excluding essential shops like groceries, pharmacies, and gas stations) and all cultural and recreational events. Additionally, bars and clubs will only be able to operate if the COVID-19 incidence rate is below 350 per 100,000 in a region; most of Germany currently sits above that rate. Police had to break up a protest this past weekend in Frankfurt, and politicians denounced a demonstration that took place on December 3 outside the home of the health minister of Saxony, one of the hardest hit states. And in Greece, Prime Minister Kyriakos Mitsotakis announced that people aged 60 and older are required to get vaccinated or face monthly fines of 100 euros, about US$113, calling the fees “the price to pay for health.” About 69% of the total population in Greece has received at least 1 dose of vaccine. Speaking today at a press conference, WHO Regional Director for Europe Dr. Hans Kluge cautioned countries that are instituting vaccine mandates, saying they should be used as “an absolute last resort” because they risk eroding public confidence and trust of authorities.
EDUCATION LOSSES In a new report, the World Bank, UNICEF, and UNESCO highlight the COVID-19 pandemic’s negative impacts on education efforts worldwide. The report, launched with an online event, also outlines a resilient path forward, including how to accelerate learning recovery. Pandemic-related school closures have affected more than 1.6 billion learners, not all of whom were offered remote alternatives, and an estimated 24 million children are at risk of never returning to education. Because of these impacts, lifetime earnings losses could hit US$17 trillion, representing a 70% increase over a 2020 estimate. Other education gaps have dramatically increased. The proportion of children who experience learning poverty—described as the inability to read and understand age-appropriate text at age 10—could increase nearly 20% in low- and middle-income countries (LMICs) due to the pandemic. The pandemic also has exacerbated inequity, particularly among children with disabilities, children from low-income households, and girls. The report notes the educational impacts could affect gender equity progress, citing a potential 10 million girls who are at risk of early marriage due to school closures. Globally, a mere 3% of governments’ stimulus packages have been allocated to education. The report called for much more funding and investment in the education sector to facilitate learning recovery in an equitable and resilient education system for all youth.
MONOCLONAL ANTIBODIES FOR PEDIATRIC PATIENTS The US FDA on December 3 expanded the emergency use authorization (EUA) for Eli Lilly and Company’s bamlanivimab and etesevimab—monoclonal antibody treatments administered together—for the treatment of mild to moderate COVID-19 in all younger pediatric patients (birth to <12 years old) who are at high risk of progressing to severe disease, including hospitalization or death. The FDA also authorized the drugs to be used for post-exposure prophylaxis for prevention of COVID-19 in all younger pediatric patients at high risk of severe COVID-19, although the agency noted this should not be considered a substitution for vaccination. The revised EUA is the first for an antibody treatment for young children, as the drugs previously were authorized for pediatric patients aged 12 and older weighing at least 40 kilograms (about 88 pounds). The drugs’ dosages are calculated based on body weight and administered by injection or intravenously at a clinic or hospital. The authorization is based on data from a clinical trial of 125 pediatric patients. Lilly said that more than 700,000 patients have been treated with bamlanivimab or bamlanivimab and etesevimab to date, estimating that the treatment has potentially prevented more than 35,000 hospitalizations and about 14,000 deaths.
by ti-amie Dry posted:
NEW YORK CITY VACCINE MANDATES On December 6, New York City Mayor Bill de Blasio announced expansions to the city’s “Key to NYC” program, including a new vaccination mandate that will apply to approximately 184,000 private employers and their in-person employees. The city already has the most sweeping local requirements in the nation, mandating vaccinations for city employees; hospital and nursing home workers; employees and customers aged 12 and older of indoor restaurants, entertainment venues, and gyms; and children engaged in high-risk extracurricular activities such as sports, band, or dance. Under the new expansion, those people will now have to show proof of full vaccination by December 27, and children aged 5 to 11 will be required to show at least partial SARS-CoV-2 vaccination (at least 1 dose for 2 dose regimens) beginning December 14 to visit those venues or engage in high-risk extracurricular activities. Mayor de Blasio noted that there would be exemptions on the basis of medical or religious reasons, but the mandates likely will face legal challenges. Enforcement processes of the mandate are currently unclear but are expected to be announced next week. As of today, 78% of New York City residents have received at least one dose of a SARS-CoV-2 vaccine and 70% of New Yorker City residents are fully vaccinated.
I saw this earlier today.
Will Eric Adams Keep N.Y.C.’s Newest Vaccine Mandate? Check Back Later.
It was unclear if the incoming mayor, Eric Adams, who is on vacation in Ghana, intended to enforce a vaccine mandate for private employers.
By Dana Rubinstein
Dec. 6, 2021
In the lengthy run-up to this year’s New York City mayoral election, an obvious question overshadowed the campaign: How would the victor handle the city’s response to the coronavirus?
For the mayor-elect, Eric Adams, the answer is still not clear. He has both expressed support for vaccine mandates for city employees, and, in November, also said he would revisit them.
On Monday, Mr. Adams had another chance to clarify his position, after the current mayor, Bill de Blasio, announced his intention to mandate that all private employers require their staff be vaccinated by Dec. 27 — five days before he leaves office, and Mr. Adams takes over.
Mr. de Blasio on Monday expressed confidence that Mr. Adams would make similar public health decisions. Yet by day’s end, it remained unclear if Mr. Adams intended to enforce Mr. de Blasio’s edict, or defend it from potential legal challenges.
The mayor-elect, who is on vacation in Ghana, intends to “evaluate this mandate and other Covid strategies when he is in office and make determinations based on science, efficacy and the advice of health professionals,” Mr. Adams’s spokesman, Evan Thies, said.
So even as Mr. de Blasio won ample publicity in advance of his likely run for governor, it remained far from clear what would happen to this private-sector mandate — or Mr. de Blasio’s pandemic policies in general — once he leaves office.
Four members of Mr. Adams’s transition team’s health committee did not respond to requests for comment. A committee contributor, the president of the Latino Commission on AIDS, Guillermo Chacón, encouraged the incoming mayor to keep the mandate in place.
dryrunguy wrote: ↑Tue Dec 07, 2021 6:27 pm
Here's the latest situation report. A brief note about nomenclature: Apparently we don't use the word "illiteracy" anymore. It's now "learning poverty." I've never seen that term used before. In any case, the section on education losses is pretty alarming.
...
I guess I am too intellectually challenged (formerly known as "stupid") to understand this drive to stop using perfectly normal words that describe a phenomenon properly.
by ti-amie I don't see any stigma attached to the word "illiterate". You're either literate or you're not.
by dryrunguy
ti-amie wrote: ↑Tue Dec 07, 2021 9:46 pm
I don't see any stigma attached to the word "illiterate". You're either literate or you're not.
I can see how the word "illiterate"--when attached to a specific person--could be stigmatizing. But the broad term "illiteracy" to describe a thing--I'm not seeing that.
It was the same deal with "hunger", which some time back was shelved and replaced with "food insecurity". At least for me.
But perhaps there's an angle or perception I'm not aware of.
by Deuce My god (or should I say 'supreme power'?) - how did we ever survive without 'political correctness'?
The manner in which 'political correctness' insists that everyone should be insecure and have zero self-confidence and self-esteem, and should feel very hurt and greatly offended at least 18 times per day, is tragic. Based on that premise, we all should have committed suicide before the 'political correctness' machine came along to 'save' us.
It is so incredibly hypocritical.
Sigh...
I much preferred the days when we were encouraged to use GOOD JUDGMENT, rather than have NO judgment of anything or anyone (it is humanly impossible, by the way, to have no opinion on situations, actions, and people), and when self-esteem and self-confidence were not discouraged, as it is with 'political correctness', but were instead ENCOURAGED via things like the mantra of "Sticks and stones may break my bones, but names will never hurt me".
by JazzNU
ti-amie wrote: ↑Tue Dec 07, 2021 7:24 pm
I saw this earlier today.
Will Eric Adams Keep N.Y.C.’s Newest Vaccine Mandate? Check Back Later.
Yes, this was rumored many weeks ago. Especially if you follow the NBA, potentially what Kyrie was waiting on because there's a question if most of the mandates would remain.
Eric's allegiances seem pretty cut and dried, but I guess we'll see.
by ponchi101 I got stuck in the "Learning Poverty" idiom, and thought that maybe, just maybe, they are using it because it includes both ILLITERACY and INNUMERACY, a term accepted by the Webster as "marked by an ignorance of mathematics and the scientific approach". So, and being very lenient here, maybe they are expanding illiteracy to include this second condition and simply cannot find an appropriate term; for example, "ignorancy" (which I just made up) would be too harsh.
I doubt that would be the case, but maybe somebody is ahead of some other people, at least in this situation.
ti-amie wrote: ↑Tue Dec 07, 2021 7:24 pm
I saw this earlier today.
Will Eric Adams Keep N.Y.C.’s Newest Vaccine Mandate? Check Back Later.
Yes, this was rumored many weeks ago. Especially if you follow the NBA, potentially what Kyrie was waiting on because there's a question if most of the mandates would remain.
Eric's allegiances seem pretty cut and dried, but I guess we'll see.
I always felt Adams is a closet Republican. It's why I didn't vote for him.
by dmforever
ti-amie wrote: ↑Tue Dec 07, 2021 9:46 pm
I don't see any stigma attached to the word "illiterate". You're either literate or you're not.
It's awesome that you don't attach a stigma to the word "illiterate". I wish the world were filled with more people like you. However, I think in most societies being "illiterate" is highly stigmatized, especially since it often intersects with racism and classism.
I also used to think in terms of a "literate" vs "illiterate" binary, but it's actually more of a range. For example, some people can read simple words but not more complicated ones. Some people can write their names and some words they have memorized but that's it. Some people can read more complicated texts but not really understand a lot.
If anyone is interested in literacy, a great way to really get how it works is to put yourself in the position of trying to become more literate. Try learning how to read and write in a foreign language that doesn't use an alphabet that you know. You can go for Hindi, Arabic, Thai, Mandarin, Japanese, Russian (except for the Russian speakers here), Farsi, Urdu, Korean, or a bunch of other languages. Sorry if I've left yours out. It's a very very humbling experience and most people become immediately more empathetic with people who are struggling to become more literate.
Thanks for your post and I apologize for kind of hijacking it and going off on a tangent.
ti-amie wrote: ↑Tue Dec 07, 2021 9:46 pm
I don't see any stigma attached to the word "illiterate". You're either literate or you're not.
It's awesome that you don't attach a stigma to the word "illiterate". I wish the world were filled with more people like you. However, I think in most societies being "illiterate" is highly stigmatized, especially since it often intersects with racism and classism.
I also used to think in terms of a "literate" vs "illiterate" binary, but it's actually more of a range. For example, some people can read simple words but not more complicated ones. Some people can write their names and some words they have memorized but that's it. Some people can read more complicated texts but not really understand a lot.
If anyone is interested in literacy, a great way to really get how it works is to put yourself in the position of trying to become more literate. Try learning how to read and write in a foreign language that doesn't use an alphabet that you know. You can go for Hindi, Arabic, Thai, Mandarin, Japanese, Russian (except for the Russian speakers here), Farsi, Urdu, Korean, or a bunch of other languages. Sorry if I've left yours out. It's a very very humbling experience and most people become immediately more empathetic with people who are struggling to become more literate.
Thanks for your post and I apologize for kind of hijacking it and going off on a tangent.
Kevinterat
I always learn things from TATeurs and the posts about "literate" vs "illiterate" have made me rethink my views. Thanks for this.
ti-amie wrote: ↑Tue Dec 07, 2021 7:24 pm
I saw this earlier today.
Will Eric Adams Keep N.Y.C.’s Newest Vaccine Mandate? Check Back Later.
Yes, this was rumored many weeks ago. Especially if you follow the NBA, potentially what Kyrie was waiting on because there's a question if most of the mandates would remain.
Eric's allegiances seem pretty cut and dried, but I guess we'll see.
I always felt Adams is a closet Republican. It's why I didn't vote for him.
My feeling is that he is a Democrat, but very old school. I can't properly give you a good example of what I mean by that (the person that comes to mind is a very bad example to mention unfortunately), but some of the things he's said and done over the years in articles written about him make me think that. But I don't think he's a closeted Republican. He had plenty of years to go deeper in that direction and didn't. Especially at a time when doing so wouldn't have been nearly as polarizing and didn't, so I think he's a Democrat. But like a 1970s version of a Democrat.
by ti-amie Many pics of him during the election showed him with prominent NYC GOP'ers. There was one taken at Rao's, the exclusive East Harlem Italian eatery that has like five tables and a waiting list that literally goes on for years. I'll see if I can find it. If you watched L& O original flavor that cozy Italian place they showed all the time was Rao's. I also don't like the fact that as Brooklyn Borough President and now as Mayor he really lives in Jersey.
ti-amie wrote: ↑Tue Dec 07, 2021 9:46 pm
I don't see any stigma attached to the word "illiterate". You're either literate or you're not.
I can see how the word "illiterate"--when attached to a specific person--could be stigmatizing. But the broad term "illiteracy" to describe a thing--I'm not seeing that.
It was the same deal with "hunger", which some time back was shelved and replaced with "food insecurity". At least for me.
But perhaps there's an angle or perception I'm not aware of.
I'm not familiar with "learning poverty" so that's a new one. Food insecurity is one that I'm familiar with, that change in phrasing has been advocated for several years now. But I think it's rather strange that illiteracy would be considered stigmatizing but attaching the word 'poverty' to something would not be? I don't understand that part. I think the word poverty carries as much if not a higher stigma than the word illiterate.
I also don't think of illiterate as stigmatizing. But here's the one thing that occurred to me reading the replies.
The prefix -ill means bad or unpleasant. There are exceptions to how it is used of course. but there are many words with that prefix that are tied to a negative connotation - illegal, illegitimate, illicit, come to mind - so maybe that's the other part of this.
That being said, my original point remains. If this is about removing stigma, I don't think they landed on the right phrase.
Without looking into it, I would guess the change in illiteracy has more to do with the spectrum/range of literacy that dmforever pointed out than with just the stigma.
by mmmm8 I don't think Eric Adams is a closet Republican. I think he's an opportunist.
by JazzNU
ti-amie wrote: ↑Wed Dec 08, 2021 10:14 pm
Many pics of him during the election showed him with prominent NYC GOP'ers. There was one taken at Rao's, the exclusive East Harlem Italian eatery that has like five tables and a waiting list that literally goes on for years. I'll see if I can find it. If you watched L& O original flavor that cozy Italian place they showed all the time was Rao's. I also don't like the fact that as Brooklyn Borough President and now as Mayor he really lives in Jersey.
I think he'll get rid of the mandates.
Skimming Catsimatidis Wiki doesn't change my original opinion of Adams. Catsimatidis has been a high level donor to many Dems in the past as well, especially the Clintons. 1970s Dem, the very, very, very pro-union kind is how I think of Adams
I will not be remotely shocked if he gets rid of the mandates, I'm basically expecting it, or at the very least modifies them, such as changing it back to what it previously was with the testing opt out. I'm guessing if he does, that was part of the support he received during the election, an agreed upon deal once he took office. That being said, it'll be real interesting if he decides to do that in the midst of an Omicron and Delta surge.
by JazzNU
mmmm8 wrote: ↑Wed Dec 08, 2021 10:41 pm
I don't think Eric Adams is a closet Republican. I think he's an opportunist.
It's awesome that you don't attach a stigma to the word "illiterate". I wish the world were filled with more people like you. However, I think in most societies being "illiterate" is highly stigmatized, especially since it often intersects with racism and classism.
I also used to think in terms of a "literate" vs "illiterate" binary, but it's actually more of a range. For example, some people can read simple words but not more complicated ones. Some people can write their names and some words they have memorized but that's it. Some people can read more complicated texts but not really understand a lot.
If anyone is interested in literacy, a great way to really get how it works is to put yourself in the position of trying to become more literate. Try learning how to read and write in a foreign language that doesn't use an alphabet that you know. You can go for Hindi, Arabic, Thai, Mandarin, Japanese, Russian (except for the Russian speakers here), Farsi, Urdu, Korean, or a bunch of other languages. Sorry if I've left yours out. It's a very very humbling experience and most people become immediately more empathetic with people who are struggling to become more literate.
Thanks for your post and I apologize for kind of hijacking it and going off on a tangent.
Kevin
But if you take that route, aren't you going to an extreme? By that definition, I am illiterate in almost all languages in the world, and that is not the usual definition. The definition of illiterate is, basically, that you can't read and/or write the language which you speak. Therefore, the sole source of information and knowledge for you is oral tradition, which of course limits your capacity for improvement.
Take the concept of innumeracy, which I talked about above. Are you innumerate? If I decide that you are so because you, for example, don't know how to do integral calculus, differential calculus or analysis, then I am the one designating you as such when in reality maybe you are brilliant in trigonometry, topology or some other math field. A final point is that I may be illiterate in Russian, but that does not mean that I cannot be versed in Russian literature and be an expert in Tolstoy and Dostoyevsky, since I can read my language and read their translations.
You also make a point of illiteracy as a "Yes/No" condition, when professionals on the subject will agree with you that illiteracy comes in gradients. For example, I am convinced that Donald Trump is technically illiterate and really can't read a book above nursery rhymes level, yet he is not considered illiterate.
I guess the point for some of us was: why the strange denomination? Why not use the word "illiterate"? It is not a crime to be one and the goal should be to help everybody in that condition overcome it, but now declaring that "illiterate" is a "bad word" is, to me, indeed raising an unwelcomed condition to the level of stigma.
Off Topic
BTW. The English language capacity to use terms such as "knowledge poverty" to convey messages does not easily translate to other languages. I am trying to find a Spanish equivalent and nothing rings the same (POBREZA DE CONOCIMIENTO can be easily thought of but that can be misconstrued as poverty of knowledge in ONE subject). As this is the WHO, an international organism, the choice of words may not be useful when you translate to other languages
BTW. The English language capacity to use terms such as "knowledge poverty" to convey messages does not easily translate to other languages. I am trying to find a Spanish equivalent and nothing rings the same (POBREZA DE CONOCIMIENTO can be easily thought of but that can be misconstrued as poverty of knowledge in ONE subject). As this is the WHO, an international organism, the choice of words may not be useful when you translate to other languages
Don't disagree with you, but what's real interesting is that this appears to be a concept that originated with the World Bank. First Google result is theirs. Second is UNESCO.
Also @ponchi, is there an equivalent phrase used in Spanish for functioning illiterate?
by ponchi101 Yes. That concept is acceptable: ANAFALBETO FUNCIONAL. Our word for "ILLITERATE" is "ANALFABETO", which carries quite a punch. Although the translation is one to one (there is no ambiguity), I gather you can see the latin origins: from AN (non) and ALFABETO (Alphabet). Basically, you don't have an alphabet.
And THAT one you can use as an insult.
It's awesome that you don't attach a stigma to the word "illiterate". I wish the world were filled with more people like you. However, I think in most societies being "illiterate" is highly stigmatized, especially since it often intersects with racism and classism.
I also used to think in terms of a "literate" vs "illiterate" binary, but it's actually more of a range. For example, some people can read simple words but not more complicated ones. Some people can write their names and some words they have memorized but that's it. Some people can read more complicated texts but not really understand a lot.
If anyone is interested in literacy, a great way to really get how it works is to put yourself in the position of trying to become more literate. Try learning how to read and write in a foreign language that doesn't use an alphabet that you know. You can go for Hindi, Arabic, Thai, Mandarin, Japanese, Russian (except for the Russian speakers here), Farsi, Urdu, Korean, or a bunch of other languages. Sorry if I've left yours out. It's a very very humbling experience and most people become immediately more empathetic with people who are struggling to become more literate.
Thanks for your post and I apologize for kind of hijacking it and going off on a tangent.
Kevin
But if you take that route, aren't you going to an extreme? By that definition, I am illiterate in almost all languages in the world, and that is not the usual definition. The definition of illiterate is, basically, that you can't read and/or write the language which you speak. Therefore, the sole source of information and knowledge for you is oral tradition, which of course limits your capacity for improvement.
Take the concept of innumeracy, which I talked about above. Are you innumerate? If I decide that you are so because you, for example, don't know how to do integral calculus, differential calculus or analysis, then I am the one designating you as such when in reality maybe you are brilliant in trigonometry, topology or some other math field. A final point is that I may be illiterate in Russian, but that does not mean that I cannot be versed in Russian literature and be an expert in Tolstoy and Dostoyevsky, since I can read my language and read their translations.
You also make a point of illiteracy as a "Yes/No" condition, when professionals on the subject will agree with you that illiteracy comes in gradients. For example, I am convinced that Donald Trump is technically illiterate and really can't read a book above nursery rhymes level, yet he is not considered illiterate.
I guess the point for some of us was: why the strange denomination? Why not use the word "illiterate"? It is not a crime to be one and the goal should be to help everybody in that condition overcome it, but now declaring that "illiterate" is a "bad word" is, to me, indeed raising an unwelcomed condition to the level of stigma.
Off Topic
BTW. The English language capacity to use terms such as "knowledge poverty" to convey messages does not easily translate to other languages. I am trying to find a Spanish equivalent and nothing rings the same (POBREZA DE CONOCIMIENTO can be easily thought of but that can be misconstrued as poverty of knowledge in ONE subject). As this is the WHO, an international organism, the choice of words may not be useful when you translate to other languages
My point about other languages wasn't that we are illiterate in them. Sorry if that wasn't clear. My point was that those of us who were lucky enough to be taught how to read and write a young age have probably forgotten what it was really like to learn that. Trying to learn a new alphabet and the sight and sound correlation that go with it, even with the advantage of already being literate in another language, can be really hard, and might give people a better understanding of what other people who are less literate go through. It was only meant as a way to have a more experiential understanding of the literacy/illiteracy spectrum.
As for the stigma part, I totally agree. But whether you or I stigmatize the word doesn't really matter if the rest of the world does. If I'm wrong and most of the world thinks the word "illiterate" has no negative connotations, then awesome.
And I agree 100% with your Trump example. There are many many other people like him.
Kevin
by JazzNU
by JazzNU
by ponchi101 Singapore, the tiny island nation that is usually ahead of the curve.
by mmmm8 Non-regulatorily, we're seeing also issues in private insurance coverage at work (working on employer benefits). In India, a new trend is that some insurers won't provide life insurance coverage for unvaccinated employees on company plans.
by dryrunguy Here's the latest Situation Report from Johns Hopkins. It includes VERY preliminary, small sample evidence regarding potential Omicron resistance to existing vaccines.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 267 million cumulative cases and 5.3 million deaths worldwide as of December 8. Global weekly incidence increased for the seventh consecutive week, up 4.6% from the previous week. At 4.2 million new cases, last week was 74% of the highest weekly total (April 2021). Europe accounts for the vast majority of the increase, and it continues to set new weekly records. Last week, European countries reported 2.80 million new cases, which is more than double the previous record (November 2020). Weekly incidence in Africa has more than tripled over the past 2 weeks, up from 22,632 new cases the week of November 15 to 79,491 new cases last week. Global weekly mortality has held relatively steady at approximately 50,000 deaths per week since late October.
Global Vaccination
The WHO reported 7.95 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of December 6. A total of 4.28 billion individuals have received at least 1 dose, and 3.38 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations has increased steadily since mid-October, up from 21.3 million doses per week to 37.8 million on December 4.* Our World in Data estimates that there are 4.36 billion vaccinated individuals worldwide (1+ dose; 55.4% of the global population) and 3.55 billion who are fully vaccinated (45.1% of the global population).
Our World in Data now provides 6-month, 9-month, and 12-month rolling windows for doses administered, which provides a smoother long-term perspective on vaccination efforts. Looking at the 6-month trends, North America peaked in August, and Europe peaked in September. The global trend as well as Oceania and South America appear to be reaching their highest peaks. And Africa’s trend continues to increase steadily, although at a much slower rate than the other continents.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC reports 49.3 million cumulative COVID-19 cases and 788,903 deaths. Daily incidence has increased steadily since the most recent low on October 24, up from 64,151 new cases per day to 117,488 on December 7—+83% over that period. Daily mortality is currently 1,097 deaths per day, which is higher than the average prior to the US Thanksgiving holiday weekend.*
At the current pace, the US could surpass 800,000 cumulative deaths in the next 11 days and 2.5 deaths per 1,000 population—or 1 death per 400 population—in the next month. The US is #19 globally in terms of per capita cumulative mortality. Daily incidence began to increase in the last week of October, so we expect to see an associated increase in daily mortality starting around the week of Thanksgiving—which could shorten those timelines. The CDC’s daily COVID-19 data appear to have largely recovered from reporting delays due to Thanksgiving, but it could still be another week or so before we have a clearer picture of the longer-term trends.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 476 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations have increased steadily since early July, up from 446,000 doses per day to 1.5 million on December 3, which is higher than the average prior to the Thanksgiving holiday weekend. There was a substantial decline in reported vaccinations over Thanksgiving, but it is unclear to what extent this was a result of an actual decrease in vaccinations (eg, due to clinic closures) compared to reporting delays. It will likely be another week or so before we have a clearer picture of the longer-term trends in daily vaccinations.*
There are 237 million individuals who have received at least 1 vaccine dose, equivalent to 71.4% of the entire US population. Among adults, 83.8% have received at least 1 dose, as well as 20.7 million children under the age of 18. A total of 200 million individuals are fully vaccinated**, which corresponds to 60.4% of the total population. Approximately 71.8% of adults are fully vaccinated, as well as 15.0 million children under the age of 18. Since August 13, 48.9 million fully vaccinated individuals have received an additional or booster dose, including 48.6% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
VACCINE EFFICACY AGAINST OMICRON Having only been on the global radar since late November, early analysis around the world regarding the Omicron variant of concern (VOC) is providing insight into its characteristics and risks. Some preliminary laboratory analyses suggest that the Omicron variant could exhibit some resistance to SARS-CoV-2 vaccines. One study conducted by researchers in Germany (preprint) found that blood serum collected from fully vaccinated individuals had reduced efficacy in neutralizing the Omicron variant. The researchers tested sera from a variety of vaccinated patients, including those who received the Moderna, Pfizer-BioNTech, and AstraZeneca-Oxford vaccines, including some with heterologous combinations and some who received booster doses. The researchers observed reductions in neutralizing capacity on the order of 10-30 times, compared to the Delta variant. Additionally, sera from participants who received a heterologous combination of the AstraZeneca-Oxford and Pfizer-BioNTech vaccines exhibited “no efficacy against Omicron.” Preliminary findings from studies conducted by researchers in South Africa and Sweden (both preprint) are similar.
Pfizer-BioNTech announced (via press release) preliminary findings from their study on efficacy against the Omicron variant. This study identified sufficient neutralizing antibody titers among individuals who received 3 doses of the Pfizer-BioNTech vaccine, but there was a 25-fold reduction in neutralizing capacity for individuals who received only 2 doses of the Pfizer-BioNTech vaccine. Notably, these findings are based on the volume of neutralizing antibodies against the Omicron variant present in the sera, and not a direct assessment of efficacy against the variant.
These studies provide initial insight into the efficacy of existing SARS-CoV-2 vaccines against the emerging Omicron variant, but we currently only have data from small, in vitro laboratory studies on which to base these analyses. The in vivo immune response varies widely, and it is unclear exactly how the current vaccines will function among the broader public or to what degree booster doses are necessary to provide sufficient protection. Current evidence suggests that existing vaccines may be less effective against the Omicron variant, but some experts indicate that fully vaccinated individuals would likely maintain some protection against severe disease. Larger studies among vaccinated individuals are necessary to gain the necessary insight.
In a likely effort to help control the Omicron variant, the US FDA today expanded its authorization for booster doses of the Pfizer-BioNTech vaccine to 16- and 17-year-olds, available 6 months after their initial 2-dose series. The CDC is expected to make formal recommendations soon, possibly today. Additionally, the WHO today recommended that only people who are immunocompromised or who received an inactivated SARS-CoV-2 vaccine receive a third vaccine dose after a primary 2-dose series. The WHO is not yet recommending third or booster doses for all vaccine recipients in order to promote equity in the global distribution of vaccines.
Dr. Mike Ryan, Director of the WHO’s Health Emergencies Programme, addressed speculation that the Omicron variant results in milder disease. He emphasized that while viruses tend to evolve to become more transmissible, the idea that a more transmissible virus results in milder symptoms is “an urban legend.” Even if the Omicron variant causes milder disease, increased transmission can put additional pressure on health systems. In addition to more patients with mild disease seeking care, milder disease that goes untreated can progress to more severe symptoms, and increased transmission can facilitate further mutations to the virus.
“STEALTH” OMICRON Scientists have identified a version of the SARS-CoV-2 Omicron (B.1.1.529) variant of concern (VOC) that cannot be distinguished from other variants using certain PCR tests that many public health officials use to quickly identify probable cases. The so-called “stealth” variant has many of the same genetic mutations as the originally identified Omicron VOC, but it lacks a certain deletion on the spike protein making it undetectable as the original Omicron lineage. Researchers have expanded the breadth of the B.1.1.529 lineage, creating 2 sub-lineages: BA.1 for the original VOC and BA.2 for the new outlier lineage. All of the usual tests are still effective at identifying the new lineage as SARS-CoV-2, but the new form of Omicron will make it more difficult to track Omicron infections because they need to be sequenced in genomic testing that takes a longer time to process. The US FDA updated its information on which molecular tests could be impacted by various mutations in the Omicron VOC. The new sub-lineage could vary from the original in transmission or disease severity, although it is too soon to say whether or if it behaves differently.
ENGLAND ENTERS “PLAN B” On December 8, England enacted its COVID-19 “Plan B” contingency plan, with British Prime Minister Boris Johnson stressing that the new restrictions “do not amount to a lockdown” ahead of the busy Christmas season. Under the plan, people are required to work from home when possible, wear masks in public places, and show vaccine passports or proof of a negative lateral flow test in order to enter certain venues such as nightclubs and theaters. Additionally, people who have come in contact with an infected person will be allowed to take daily tests instead of isolating. Prime Minister Johnson said moving into Plan B—which was intended to be used only if new COVID-19 case numbers increased to an extent that could burden the health system—was necessary in response to the variant of concern (VOC) Omicron. Some scientists estimate the number of new Omicron cases is doubling every 2-3 days and predict the VOC will likely overtake the Delta variant in the next 2-4 weeks. Scotland also announced a return to working from home, and Scotland, Northern Ireland, and Wales all have similar vaccine passport requirements and mask mandates either in place or planned. The UK recorded a 7-day average of 47,827 new COVID-19 cases on December 7, surpassing its most recent high of 47,115 on October 22 as well as the previous peak reached in July. The UK has found 568 Omicron cases as of December 8, but the UK Health Security Agency estimates the number to be closer to 10,000.
US VACCINATION REQUIREMENTS A US judge on December 7 issued a nationwide preliminary injunction against the Biden administration’s SARS-CoV-2 vaccine mandate for employees of federal contractors. Judge R. Stan Baker of the US District Court for the Southern District of Georgia concluded that US President Joe Biden likely overstepped his authority under the Procurement Act in issuing the mandate and that the rule could “have vast economic and political significance.” The vaccine-or-test mandate already was on hold for contractors and subcontractors in Kentucky, Ohio, and Tennessee after a separate preliminary injunction was issued last week. Notably, it does not appear that the injunction applies to other aspects of the COVID-19 safety rules for contractors, including those related to masking and social distancing. The White House said the US Department of Justice plans to “vigorously defend” the vaccine requirement. With the issuance of this preliminary injunction, all 3 of the Biden administration’s vaccine requirements affecting the private sector—one for federal contractors, another for healthcare workers, and one for companies with more than 100 employees—are now on hold nationwide. It is likely that 1 or more of the various cases challenging federal vaccine rules will reach the US Supreme Court. To date, the vaccine mandate for federal employees has not been enjoined.
In a move that is largely seen as symbolic, the US Senate late on December 8 voted to overturn the proposed rule requiring large companies to mandate their employees be vaccinated, undergo weekly testing, or risk losing their jobs. The vote was 52-48, with 2 Democrats voting for the measure to overturn the regulation. The US House is not expected to pass the resolution, but if it did, President Biden has indicated he would veto.
WHO ON CONVALESCENT PLASMA The WHO on December 6 issued a strong recommendation against using convalescent plasma to treat people with non-severe COVID-19 and a recommendation against its use in people with severe and critical illness, saying the therapy shows no improvement in survival nor a reduction in the need for mechanical ventilation. Additionally, the WHO said convalescent plasma therapy is expensive and time-consuming to administer. The agency did say the treatment could continue to be used in severe and critical patients who are participants of a randomized controlled trial (RCT). The recommendations are based on the outcomes of 16 clinical trials involving more than 16,000 COVID-19 patients and are part of the WHO’s living guideline on drugs for the disease. The WHO’s updated recommendations contradict a US FDA revision to the emergency use authorization (EUA) of convalescent plasma therapy issued earlier this year, which limits the authorization to the use of high-titer COVID-19 convalescent plasma for the treatment of hospitalized patients early in the disease course and hospitalized patients who have impaired antibody responses.
EVUSHELD EUA The US FDA on December 8 issued an emergency use authorization (EUA) for AstraZeneca’s long-acting monoclonal antibodies tixagevimab and cilgavimab—which are co-packaged and administered together under the brand name Evusheld—for the prevention of COVID-19 in certain adults and youth aged 12 years and older weighing at least 88 pounds who have moderate to severe immune system compromise or for whom a SARS-CoV-2 vaccine is contraindicated. Individuals also must not have active SARS-CoV-2 infection or have had a recent exposure. The long-acting antibody therapy—the first authorized to prevent COVID-19 prior to an exposure—is administered as 2 separate but immediately consecutive intramuscular injections and may be effective as pre-exposure prophylaxis for up to 6 months. While the authorization provides an alternative prevention method for certain individuals, vaccination remains the best defense available to prevent SARS-CoV-2 infection, severe disease, hospitalization, or death.
LONG COVID Researchers worldwide continue to learn more about the constellation of long-lasting COVID-19-related symptoms known formally as post-acute sequelae of COVID-19 (PASC) and more commonly as long COVID. A retrospective, observational analysis of data collected from patients of the Mount Sinai Health System in New York (US) found the most common symptoms of long COVID among a group of 156 unvaccinated individuals to be fatigue, cognitive impairment or “brain fog,” headache, sleep disturbance, and dizziness, with many reporting continuing symptoms nearly 1 year after their initial diagnosis. Some people report a long-lasting loss or distortion of their sense of smell, anosmia or parosmia, respectively. One preprint study examined the experiences of some people with long COVID who have protracted internal vibration, pain, and tremors, which could have mental health implications if left untreated, the researchers warned. Many long COVID patients complain of shortness of breath, and a study published online November 29 in the Journal of the American College of Cardiology: Heart Failure suggests that cardiopulmonary exercise testing (CPET) could uncover respiratory and circulatory abnormalities that are undetectable on normal chest imaging and pulmonary function tests. The most serious circulatory impairment complications have led to some patients to undergo amputations of their extremities. Many questions regarding long COVID still remain, including how to properly diagnose the condition, how vaccines might impact long-term symptoms, and how to properly treat and rehab patients. The condition also has implications for the workforce, with the Mount Sinai analysis showing a significant proportion of patients did not return to full-time work after their COVID-19 diagnosis and a preprint analysis from South Africa cautioning that long COVID among frontline healthcare workers could impact health service delivery.
Dr. Mike Ryan, Director of the WHO’s Health Emergencies Programme, addressed speculation that the Omicron variant results in milder disease. He emphasized that while viruses tend to evolve to become more transmissible, the idea that a more transmissible virus results in milder symptoms is “an urban legend.” Even if the Omicron variant causes milder disease, increased transmission can put additional pressure on health systems. In addition to more patients with mild disease seeking care, milder disease that goes untreated can progress to more severe symptoms, and increased transmission can facilitate further mutations to the virus.
“STEALTH” OMICRON Scientists have identified a version of the SARS-CoV-2 Omicron (B.1.1.529) variant of concern (VOC) that cannot be distinguished from other variants using certain PCR tests that many public health officials use to quickly identify probable cases. The so-called “stealth” variant has many of the same genetic mutations as the originally identified Omicron VOC, but it lacks a certain deletion on the spike protein making it undetectable as the original Omicron lineage. Researchers have expanded the breadth of the B.1.1.529 lineage, creating 2 sub-lineages: BA.1 for the original VOC and BA.2 for the new outlier lineage. All of the usual tests are still effective at identifying the new lineage as SARS-CoV-2, but the new form of Omicron will make it more difficult to track Omicron infections because they need to be sequenced in genomic testing that takes a longer time to process. The US FDA updated its information on which molecular tests could be impacted by various mutations in the Omicron VOC. The new sub-lineage could vary from the original in transmission or disease severity, although it is too soon to say whether or if it behaves differently.
by ponchi101 USA. If it gets to 1/400, pretty soon it will be very difficult to NOT know or have heard of somebody that has died of the disease.
I am going to look up the numbers for Colombia.
by atlpam
ponchi101 wrote: ↑Thu Dec 09, 2021 6:42 pm
USA. If it gets to 1/400, pretty soon it will be very difficult to NOT know or have heard of somebody that has died of the disease.
I am going to look up the numbers for Colombia.
I knew one person personally (a former co-worker), and know of several others (sister of a college friend, cousin of another college friend, parent of a grade school friend).
by ti-amie
by atlpam Interesting article - offers some explanation to the high death rate from Covid in the USA.
Article is from the NY Times, so may require an account to read it.
ponchi101 wrote: ↑Thu Dec 09, 2021 6:42 pm
USA. If it gets to 1/400, pretty soon it will be very difficult to NOT know or have heard of somebody that has died of the disease.
I knew one person personally (a former co-worker), and know of several others (sister of a college friend, cousin of another college friend, parent of a grade school friend).
Do you happen to know if any of those people who died were fully/partially vaccinated, or completely unvaccinated?
by ponchi101
atlpam wrote: ↑Thu Dec 09, 2021 8:17 pm
Interesting article - offers some explanation to the high death rate from Covid in the USA.
Article is from the NY Times, so may require an account to read it.
ponchi101 wrote: ↑Thu Dec 09, 2021 6:42 pm
USA. If it gets to 1/400, pretty soon it will be very difficult to NOT know or have heard of somebody that has died of the disease.
I knew one person personally (a former co-worker), and know of several others (sister of a college friend, cousin of another college friend, parent of a grade school friend).
Do you happen to know if any of those people who died were fully/partially vaccinated, or completely unvaccinated?
Other than my co-worker, the others contracted Covid early in the pandemic before vaccines were available.
I don’t know if my co-worker was vaccinated (we’ve all been working from home since March 2020), but based on the timing, it was likely Delta.
by atlpam
atlpam wrote: ↑Thu Dec 09, 2021 8:17 pm
Interesting article - offers some explanation to the high death rate from Covid in the USA.
Article is from the NY Times, so may require an account to read it.
So a few months ago when there was word that they would mandate for the military and they weren't sure everyone would take it, etc. there was someone who was former military talking about the level of BS their refusals are. Several steps up from us wondering why people suddenly care about what's in a vaccine when they've never asked a single question before during all their schooling. Said during boot camp they were lined up, and he was jabbed in the both arms quickly with whatever vaccines they were handing out to the recruits and kept it moving to the next guy right down the line. Others concurred that's exactly what happens and some have said at different times it's been up to 20 different vaccines given because you don't know what your orders will be, so truly suck it up and follow orders like you do with everything else because you're in the damn military.
by JazzNU
by dryrunguy Here's the latest Situation Report.
::
OMICRON POSES “VERY HIGH” RISK As nations worldwide brace for predicted COVID-19 case surges due to the Omicron variant of concern (VOC), the WHO has warned Omicron poses a “very high” global risk. The VOC has been reported in more than 70 countries, and while new data are helping to clarify initial impressions of the variant’s transmissibility, severity, and ability to evade immunity, many uncertainties remain.
The UK continues to experience a surge in COVID-19 cases—in England, new cases are doubling every 2.5 days—and health officials there expect that Omicron will soon overtake Delta to become the most prevalent SARS-CoV-2 variant. A recent technical brief from the UK Health Security Agency estimates that someone infected with Omicron is about 3 times as likely as a person with Delta to pass the virus on to a close contact. On December 12, the UK government raised its official COVID-19 alert level, and on December 13 UK Prime Minister Boris Johnson confirmed the country’s first-known death of a patient from Omicron. He cautioned putting too much emphasis on initial reports of Omicron possibly causing less severe symptoms, instead focusing on the speed with which the variant is spreading. He also announced vaccine booster doses will be made available to anyone over age 18 who is at least 3 months from their last vaccine. Early analyses are showing 2 doses of the AstraZeneca-Oxford or Pfizer-BioNTech vaccines have a substantial fall in neutralizing antibodies against Omicron compared with other variants, and a third dose is expected to help boost immune response. Authorities across Europe are warning of the variant’s quick spread; the European Centre for Disease Prevention and Control today reported an additional 441 confirmed Omicron cases in the region in the past day, bringing the region's total number to 2,127 since the variant’s emergence.
In South Africa, where early cases of Omicron were first detected, the VOC has caused a faster surge in test positivity than previous variants. The 7-day average number of daily new confirmed COVID-19 cases has more than doubled since December 5. South Africa President Cyril Ramaphosa tested positive for SARS-CoV-2 on December 12, several days after returning from a trip to 4 West African nations, and is showing mild symptoms. South African doctors say most patients with Omicron are recovering at home within the 10- to 14-day isolation period, including older patients and those with preexisting conditions. Still, the volume of new COVID-19 cases has the potential to overwhelm the healthcare system and strain hospitals, a scenario that could result in more severe cases and deaths.
The US CDC last week released its first report on Omicron, discussing 43 cases detected in 25 states between December 1 and December 8. Since then, Omicron cases have been detected in at least 5 more states and Washington, DC. Nearly 80% (34) of the patients were fully vaccinated and one-third (14) had received a booster dose, although 5 of those were not 2 weeks from their last dose. Additionally, 6 of the patients were previously infected with SARS-CoV-2, and nearly all cases experienced mild cold-like symptoms, including congestion, cough, and fatigue. Only 1 patient was hospitalized. State-level community transmission is listed as high across nearly the entire country, which does not bode well in the face of what appears to be the more infectious Omicron variant. As the US nears 50 million cumulative COVID-19 cases and 800,000 related deaths, the CDC predicts the weekly number of COVID-19 related deaths will rise from 8,800 last week to 10,000 next week and to more than 11,000 in 4 weeks. The full impact of Omicron in the US, and around the world, will become more apparent as we enter 2022, the third year of the pandemic.
VACCINE EFFECTIVENESS AGAINST OMICRON Preliminary studies of the Omicron variant of concern (VOC) are revealing lower vaccine effectiveness compared with previous SARS-CoV-2 variants. While still under review, full doses of current vaccines* appear to be around 30-40% effective in preventing infection against Omicron. With booster doses, that estimate increases to between 70-75%. A recent study out of South Africa involving 78,000 persons infected with Omicron indicated that the Pfizer-BioNTech vaccine was about 33% effective in preventing infection but about 70% effective in preventing severe disease. Another study from the UK estimated that a full course of the Pfizer-BioNTech vaccine resulted in around 40% effectiveness in preventing infection.
The decreases in vaccine effectiveness can be attributed to significant changes in the S gene of the Omicron variant compared to previous SARS-CoV-2 variants. The S gene codes for the spike protein, which sits on the outside of the virus and contributes to its ability to infect host cells. Omicron’s totality of mutations in its S gene have resulted in a variant that is different enough from previous variants to be less recognizable by vaccine-induced immunity or by previously acquired immunity following recovery from infection. An Oxford preprint study examined blood sera from 43 fully vaccinated individuals and reported significant decreases in neutralization titers against Omicron. Neutralization titers refer to the ability of neutralizing antibodies to detect and inactivate the virus when it enters the body. All of the studied serum samples showed greatly decreased neutralization capability against Omicron compared to previous variants; some samples showed no neutralization capability at all. With decreased ability of previously vaccinated individuals’ immune systems to recognize and rapidly eliminate Omicron, more breakthrough infections are expected compared with previous VOCs.
Most studies do appear to reinforce the need for booster doses, which are posited to significantly increase protection against Omicron. However, with very little of the world having access to booster doses, or even first doses, Omicron likely will result in another large wave of infections over the next several months. While overall infections are currently on the rise, fully vaccinated persons still appear less likely to be hospitalized with infections due to Omicron. The variant also appears to cause less severe disease than its predecessor variants; however, given the apparent high transmissibility of Omicron, healthcare facilities are still likely to undergo severe strain to remain on top of the wave of incoming patients.
*Full original course of the vaccine, not including additional or booster doses.
GLOBAL VACCINE ACCESS Low- and middle-income countries (LMICs) continue to wait for vaccine supply, as wealthier nations and those producing the supply retain vaccine doses. Despite donations to COVAX, vaccine hoarding has negatively impacted supply to those countries, including COVAX’s mission to equitably distribute vaccines. Experts note that there is a global supply chain risk of reverting to higher-income countries holding on to vaccines for boosters as the Omicron situation, and the potential of future variants, is assessed. Some argue there is a need for some sort of rule against vaccine hoarding, as well as more transparency among manufacturers. WHO warns vaccine hoarding is a detriment to the global targets of vaccinating 40% of the population in each country this year and 70% by mid-2022, leading to a prolongation of the pandemic.
The Duke Global Health Innovation Center and the COVID Collaborative estimate that 11 billion doses of SARS-CoV-2 vaccine will have been manufactured by the end of 2021, which should cover 70% of those 5 and older around the world, but doses are not being equitably distributed. Globally, 8.5 million doses have been distributed, with 56% of the world population having received at least 1 dose of SARS-CoV-2 vaccine; however, only 7.2% of people in low-income countries have received at least 1 dose. Some countries are utilizing most of their supply but still have low vaccination rates because supplies are not adequate to cover the population. Other nations face challenges with delivery capacity and logistics, cold-chain requirements, and vaccine hesitancy. COVAX aimed to deliver 800 million doses by the end of this year, down from its initial 2.3 billion dose goal, but now estimates that less than half of that figure will be delivered. GAVI last week announced a new agreement with Moderna for an additional 150 million doses to be delivered next year to COVAX and priced in the lowest-tier. GAVI and Moderna also agreed to advance access to 20 million doses that will now be available in Q4 of 2021, rather than Q1 of 2022.
ORAL ANTIVIRALS Oral antivirals could transform the treatment of COVID-19, allowing some patients to take medicines while recovering at home instead of having to visit health clinics or be admitted to hospital to receive injections or infusions of currently available therapies. Pfizer this morning released final analysis of its oral antiviral candidate PAXLOVID (the protease inhibitors nirmatrelvir and ritonavir, taken together), showing the treatment retained its 89% efficacy in preventing hospitalization and death among 2,246 high-risk COVID-19 patients. The results were released in a press release and have not yet been peer-reviewed. The data are similar to an interim analysis released in November, which included about 1,200 patients. The company also released interim results from a different study testing PAXLOVID in standard-risk patients and fully vaccinated patients* with 1 or more risk factors. The primary endpoint of self-reported symptom alleviation for 4 consecutive days was not met, but a secondary endpoint showed a 70% reduction in hospitalization and no deaths. Notably, patients in the treatment groups of both studies showed a significant reduction in viral load when compared with patients in the placebo groups. A lower viral load could help lower the risk of transmission. Because PAXLOVID works to inhibit the protease enzyme the virus uses to reproduce—instead of working to inhibit the virus itself—scientists feel the treatment could be effective against Omicron and other variants.
Over the past month, excitement over Merck and Ridgeback Biotherapeutic’s oral antiviral COVID-19 treatment molnupiravir has waned, after full clinical trial data showed the therapy’s efficacy in reducing hospitalization was much lower than initially anticipated based on preliminary data. On November 30, a US FDA advisory panel voted 13-10 to recommend the investigational drug for emergency authorization. The narrow endorsement came after hours of spirited debate centered on several concerns, including whether molnupiravir—which hinders the ability of SARS-CoV-2 to properly replicate its genetic material—could lead to the development of new viral variants, increase the risk of birth defects if used in pregnant individuals, or cause other DNA mutations in humans. The concerns over variants and birth defects are resurfacing just as Britain launches a national clinical trial examining molnupiravir and other COVID-19 treatments, known as PANORAMIC. The trial aims to recruit more than 10,000 people aged 50 and older or who are classified as clinically vulnerable because of pre-existing conditions and who have been infected for less than 5 days. Britain became the first country to approve molnupiravir (Lagevrio) in early November, but the government then said the drug would be rolled out as part of a clinical trial. The results of the trial, as well as other research into the drug, will be useful in showing its real-world effectiveness and evaluating the risks. We expect the FDA to make decisions on emergency use authorization (EUA) applications for both PAXLOVID and molnupiravir in the coming weeks.
*Full original course of the vaccine, not including additional or booster doses.
J&J-JANSSEN WHO EUL The WHO on December 9 updated its emergency use listing (EUL) for the J&J-Janssen SARS-CoV-2 vaccine, saying countries can choose to use the vaccine as a single or 2-dose regimen given at least 2 months and up to 6 months apart. The agency noted that clinical trials show that 2 doses of the vaccine have higher efficacy than 1 dose but also stated that an initial J&J-Janssen vaccine followed by a dose of an mRNA vaccine as a second dose induces higher neutralizing antibody concentrations than a second dose of the J&J-Janssen vaccine. Single-dose administration remains efficacious and optimal in some circumstances, such as in hard-to-reach populations, but countries can consider a second dose among higher-risk populations, including healthcare workers, older individuals, or people with comorbidities, and as vaccine supplies and accessibility increase. The recommendations could help some countries use their excess supplies of the J&J-Janssen vaccine. For example, South Africa last month requested J&J and Pfizer-BioNTech delay further deliveries of the companies’ vaccines due to oversupply. But the country on December 9 announced booster doses of both vaccines will soon become more widely available.
HEALTHCARE WORKER VACCINE MANDATE The US Supreme Court refused to block New York’s vaccine mandate for healthcare workers in a 6-3 vote on December 13. In a previous and similar order, the court allowed Maine’s vaccine requirements for healthcare workers to stay in force. In the New York case, the unsigned order included no reasoning, which is common in response to emergency requests. However, Justice Neil M. Gorsuch filed a 14-page dissent, joined by Justice Samuel A. Alito Jr., saying the majority had betrayed the court’s commitment to religious liberty because the mandate does not include allowance for religious exemption. New York’s vaccine mandate for healthcare workers only allows a narrow medical exemption for those who have had a severe allergic reaction to a previous dose of the SARS-CoV-2 vaccine or a component of the vaccine. Justice Clarence Thomas also dissented, although he gave no reasoning. Challenges to mandates for federal contractors, healthcare workers, and companies of more than 100 employees are pending in lower courts, and additional challenges against federal vaccine requirements or other state mandates could soon reach the Supreme Court.
PANDEMIC HEALTH COSTS The COVID-19 pandemic is set to dismantle nearly 2 decades of global progress toward Universal Health Coverage and increase the number of people pushed into extreme poverty due to out-of-pocket healthcare costs, already at more than half a billion people prior to the pandemic, according to 2 new reports from the WHO and the World Bank. In 2020, the pandemic disrupted health services, caused immunization rates to drop for the first time in 10 years, spurred increases in tuberculosis and malaria deaths, and sparked the worst economic crisis since the 1930s, the agencies said, warning that further financial hardships are likely as governments and households face tighter fiscal constraints. WHO Director-General Dr. Tedros Adhanom Ghebreyesus called on governments to “immediately resume and accelerate” efforts to rebuild and strengthen healthcare and social support systems so that every person can access services without financial consequences. The reports were released to mark International Universal Health Coverage Day on December 12.
by ponchi101 I gather I can take my 4th dose sometime around... May?
by ti-amie
FAFO
by ti-amie Interesting conversation here...
by JazzNU
dryrunguy wrote: ↑Tue Dec 14, 2021 5:58 pm
GLOBAL VACCINE ACCESS Low- and middle-income countries (LMICs) continue to wait for vaccine supply, as wealthier nations and those producing the supply retain vaccine doses. Despite donations to COVAX, vaccine hoarding has negatively impacted supply to those countries, including COVAX’s mission to equitably distribute vaccines. Experts note that there is a global supply chain risk of reverting to higher-income countries holding on to vaccines for boosters as the Omicron situation, and the potential of future variants, is assessed. Some argue there is a need for some sort of rule against vaccine hoarding, as well as more transparency among manufacturers. WHO warns vaccine hoarding is a detriment to the global targets of vaccinating 40% of the population in each country this year and 70% by mid-2022, leading to a prolongation of the pandemic.
I understand what WHO's mission is, so I get that there is some framing here that they do intentionally, but many people rely on their reports as objective information. The shaming of wealthy nations has gotten rather interesting and I feel like I'm missing something. Did the low-to-middle income nations suddenly get a ton of cold storage and logistical support and I just missed it?
This is a serious question, because I knew they've increased it, but I feel like I missed where they got a substantial amount, enough to almost vaccinate their entire populations. Because I don't know how Astra Zeneca is stored, but Pfizer and Moderna were never the vaccines that were going to vaccinate the globe. J&J and Novavax, easy to store and cheap to make, were the ones that were supposed to do that (besides whatever China and Russia are doing) and Novavax's bizarre 8 month delay from "we're almost ready" to actually applying for official approval was the real reason along with J&J health concerns for the slow rollout in many of the poorer regions of the world. Did something change?
For instance, with Omicron, there's been a lot of South Africa coverage with a "had vaccines been shared with Africa." I'm in total agreement that more of Africa should be vaccinated by now, but South Africa is a very poor example. They have many more vaccines available than they have people willing to take the shots, same as the so-called wealthier nations. They've delayed receiving some shipments since they don't run out of their existing vaccines supply, falling well short of their vaccination goals. These facts seems to be left out of many of the articles I've seen for Omicron even though most are talking specifically about South Africa and not Africa as a whole.
So what am I missing here? Is it just the bad optics that has fueled the wealthy nation narrative with little mention of the other issues? When did "we know that J&J and Novavax are the vaccines that will get us out of the global pandemic" and problems associated with both those vaccine rollouts turn into just "wealthy nations are constantly hoarding the vaccines?" Not saying they don't have many more than they need, but they've been donating hundreds of millions of doses as well funds to manufacture more doses and there are quite a few other issues and just wondering why they rarely get mentioned anymore. Feel like if you weren't paying close attention at the beginning of the year then you'd have no idea now because only one thing gets blamed.
by ponchi101 Colombia has been getting vaccines. Venezuela has been using Russian Sputnik V and Sinovax (for the younger population).
And, mixing narratives. Colombia is currently negotiating a package of jet fighters (and support crafts) to modernize its Air Force for when they go to war with... Venezuela, Panama, Ecuador, Peru or Brazil? What TF do they need these planes for?
Plans to open and start operating factories to manufacture vaccines (which they wiped out ten years ago)? Nah, we can buy those from the USA. Or beg for them.
Sorry, but this subject always pissed me off. It is the same narrative I always hear when things go wrong in S. America; It is NEVER our fault, it is always the gringos or our European colonizers, or the transnationals or the IMF or the World Bank. It is never us.
by ti-amieCovid deaths in the United States surpass 800,000.
Coronavirus deaths in the United States surpassed 800,000 on Wednesday, according to a New York Times database, as the pandemic neared the end of a second year and as known virus cases in this country rose above 50 million.
The new death toll — the highest known number of any country — comes a year after vaccines against the coronavirus began rolling out in the United States. It also comes at a tenuous moment in the pandemic: Cases are rising once again, hospitals in some parts of the country are stretched to their limits with Covid patients and the threat and uncertainties of a new variant loom.
More than 1,200 people in the United States are dying from Covid-19 each day.
The last 100,000 deaths occurred in less than 11 weeks as the pace of death has picked up, moving faster than at any time other than last winter’s surge. The current uptick is being driven by the Delta variant. It is not yet known how the Omicron variant, which continues to emerge in more states, might affect those trends in the coming weeks and months.
Naoko Muramatsu, a professor at the University of Illinois at Chicago’s School of Public Health, said that from the beginning of the pandemic in 2020, older people have suffered disproportionately.
“Early on, Covid was considered to be an older people’s problem,” she said. Nearly two years later, those difficulties have persisted, whether in the form of a high death rate or isolation, which in many cases already existed but expanded significantly as the months wore on. Older people steered clear of crowded public gatherings and younger relatives stayed away, fearful of exposing those more vulnerable to the virus.
Some 75 percent of the 800,000 Covid-19 deaths have involved people 65 or older. One in 100 older Americans has died. Countless others have found themselves isolated.
“Covid really made something visible that was already going on for older adults,” she said. “Older people were so vulnerable.”
After the first known coronavirus death in the United States in February 2020, the virus’s death toll in this country reached 100,000 people in only three months. The pace of deaths slowed throughout summer 2020, then quickened throughout the fall and winter, and then slowed again this spring and summer.
Throughout the summer, most people dying from the virus were concentrated in the South. But the most recent 100,000 deaths — beginning in early October — have spread out across the nation, in a broad belt across the middle of the country from Pennsylvania to Texas, the Mountain West and Michigan.
The benchmark of 800,000 deaths in the United States occurred despite the wide availability of vaccines for most of 2021.
Older people have been vaccinated at a much higher rate than younger age groups and yet the brutal effects of the virus on them has persisted. The share of younger people among all virus deaths in the United States increased this year, but, in the last two months, the portion of older people has risen once again, according to data from the Centers for Disease Control and Prevention.
By now, Covid-19 has become the third leading cause of death among Americans 65 and older, after heart disease and cancer. It is responsible for about 13 percent of all deaths in that age group since the beginning of 2020, more than diabetes, accidents, Alzheimer’s disease or dementia.
by JazzNU Found this article from a few days ago while searching for information about the vaccine shortage in Africa
Arrival of 1bn vaccine doses won’t solve Africa’s Covid crisis, experts say
With 1bn doses of Covid vaccines expected to arrive in Africa in the coming months, concern has shifted to a global shortage of equipment required to deliver them, such as syringes, as well as insufficient planning in some countries that could create bottlenecks in the rollout.
After a troubled start to vaccination programmes on the continent, health officials are examining ways to encourage take-up as some countries have had to throw away doses.
Critics have blamed hoarding of vaccine doses by a handful of western countries for a situation in which only 7.5% of people in African countries have been vaccinated – which some argue led to the emergence of the Omicron variant in southern Africa – but health experts point to a wider series of issues.
The World Health Organization says a shortage of syringes – in particular a 0.3ml syringe version required to deliver the Pfizer dose – may slow delivery, and it has stepped up technical assistance missions in 15 countries that have lagged behind.
Figures show a wide disparity in what has been achieved, with 15 countries reaching a target of 10% of the population vaccinated by the end of September, and more than half struggling to reach a third of that number.
Among the success stories have been some smaller island states, including Seychelles and Mauritius, which have vaccinated more than 60% of their populations, and Morocco has reached 48%.
The case of South Africa – which had vaccinated 40% of its population as of 3 December – highlights some of the complexities involved.
With sufficient doses for an estimated 150 days of vaccination, it has cancelled some vaccine shipments as it has tried to reinvigorate a campaign that had met resistance from some sections of the population, not least in the 18-34 age group.
Some of South Africa’s vaccine supply problems were self-inflicted, including being slow to initially secure stock. There have also been technological issues, with requirements to register using a phone or computer creating a digital barrier in a country where only 60% of people are internet users.
Dr Richard Mihigo, a WHO programme coordinator, said there had been a “start and stop” approach to vaccine drives in Africa in recent months.
“The first doses arrived in Ghana in March and there were a lot of promises from Covax [the global vaccine consortium] that countries would receive their allocations. But that delivery was stopped when India halted delivery from the Serum Institute [in the midst of its own outbreak] earlier this year,” he said.
“That start was not ideal. Since then, however, the situation has stabilised. Now the prospects through March 2022 looks very good with almost 1bn doses forecast to arrive, which in theory could cover 70% of the African population.”
Set against that, however, has been the struggle of some countries to deliver what doses they have – because of instability, for example in the Democratic Republic of the Congo and Nigeria; health systems with poor reach, especially outside big cities; and vaccine hesitancy around the Covid jab.
Nigeria’s underfunded health system lacks everyday supplies such as cotton swabs. Spotty power supply means fridges holding vaccines need to be kept on expensive fuel generators, and millions of citizens live in areas racked by banditry or Islamist insurgencies that medics cannot reach.
Nigeria’s health minister, Osagie Ehanire, said last week: “The foundation is not strong. And if you don’t have a strong foundation, there’s not much you can build on top.”
Hesitancy has been driven by a combination of factors on a continent that in general, studies suggest, has far higher rates of vaccine acceptance than the US. The huge amount of misinformation that has circulated globally is partly to blame, but there are also economic reasons.
David Harrison, the head of the nonprofit DG Murray Trust in South Africa, said some were reluctant to give up a day’s work or pay to travel to a vaccination site. “Twelve million people applied for an R350 (£16) emergency Covid-19 relief grant,” he said. “If you’re asking those people to pay R20 for a taxi fare to and from a vaccine site, it’s a significant trade-off.”
Mihigo, of the WHO, echoed this point. “To make sure more and more of the available vaccine can be put in arms of the people, we need to focus attention on providing additional incentives to people to get vaccinated without compromising their livelihoods.
“I was in DRC recently and I heard someone say precisely this. They can’t afford to travel and then wait in a vaccination centre for two hours.”
Writing in South Africa’s Mail and Guardian this week, Anand Madhvani, a co-founder of Covid Kenya – a group of volunteers that uses social media to create awareness about Covid-19 issues – raised local inequalities in vaccine access.
“In many African countries we have some existing systems for vaccinations, but these require massive expansion and support for mass adult campaigns – even once a steady supply of vaccines is available,” he wrote. “In Kenya, where I work, we needed high-profile local language vaccination campaigns. There is deep inequality within our countries. Relative elites in capitals quickly got themselves vaccinated but stopped pushing for everyone.”
The numbers are a bit higher, proportionally, than the USA. Colombia has a population of about 48 MM, so, if you extrapolate to the USA's 360MM, we would get a death toll of 970,000, considerably higher than in the States.
Even though our vaccination seems to be slight ahead.
Starting Tuesday: no foreigners WITHOUT vaccination can enter the country. Not even with a negative PCR test. Residents and citizens need to show full vaccination schedule OR a PCR test.
2022, here we go, full deja vu.
-->
by ponchi101 This is the current data for Colombia:
Screenshot 2021-12-16 103931.jpg
The numbers are a bit higher, proportionally, than the USA. Colombia has a population of about 48 MM, so, if you extrapolate to the USA's 360MM, we would get a death toll of 970,000, considerably higher than in the States.
Even though our vaccination seems to be slight ahead.
Starting Tuesday: no foreigners WITHOUT vaccination can enter the country. Not even with a negative PCR test. Residents and citizens need to show full vaccination schedule OR a PCR test.
2022, here we go, full deja vu.
by ti-amie
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 270.8 million cumulative cases and 5.32 million deaths worldwide as of December 15. Global weekly incidence increased for the eighth consecutive week, up 0.89% from the previous week. At 4.2 million new cases, last week was 75% of the highest weekly total (April 2021). Europe continues to account for the vast majority of the increase, especially as the Omicron variant of concern (VOC) spreads throughout the region. The UK reported a record number of 78,610 new COVID-19 cases on December 15, 16% higher than its previous record set in January. Weekly incidence in Africa has more than doubled over last week, up from 79,491 new cases the week of November 29 to 167,682 new cases last week. Global weekly mortality has held relatively steady at approximately 50,000 deaths per week since late October.
Global Vaccination
The WHO reported 8.2 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of December 13. A total of 4.35 billion individuals have received at least 1 dose, and 3.47 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations has increased since mid-October, up from 21.3 million doses per week to 36.4 million on December 15.* Our World in Data estimates that there are 4.45 billion vaccinated individuals worldwide (1+ dose; 56.55% of the global population) and 3.67 billion who are fully vaccinated (46.4% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
On December 13, the US surpassed 50 million cumulative COVID-19 cases:
1 case to 10 million: 289 days
10 to 20 million: 54 days
20 to 30 million: 85 days
30 to 40 million: 162 days
40 to 50 million: 100 days
As of December 14, the US CDC reports 50.2 million cumulative COVID-19 cases and 797,877 deaths. Daily incidence has increased steadily since the most recent low on October 24, up from 64,152 new cases per day to 117,950 on December 14—+84% over that period. Daily mortality is currently 1,143 deaths per day and likely will rise as daily incidence continues to increase.*
At the current pace, the US likely will surpass 800,000 cumulative deaths today or tomorrow. More people have died of COVID-19 in the US than are estimated to have died in the Civil War, the nation’s deadliest conflict (750,000 deaths). And the official number of COVID-19-related deaths likely is an undercount. If the US surpasses this benchmark on December 16:
1 death to 100k: 87 days
100k to 200k: 111 days
200k to 300k: 88 days
300k to 400k: 35 days
400k to 500k: 33 days
500k to 600k: 121 days
600k to 700k: 105 days
700k to 800k: 78 days
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 488.3 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations have remained relatively steady over the past week, but have increased steadily since early July, up from 446,000 doses per day to 1.53 million on December 10, which is higher than the average prior to the Thanksgiving holiday weekend.*
There are 240 million individuals who have received at least 1 vaccine dose, equivalent to 72.3% of the entire US population. Among adults, 84.6% have received at least 1 dose, as well as 21.5 million children under the age of 18. A total of 202.8 million individuals are fully vaccinated**, which corresponds to 61.1% of the total population. Approximately 72.2% of adults are fully vaccinated, as well as 16.4 million children under the age of 18. Since August 13, 56.1 million fully vaccinated individuals have received an additional or booster dose, including 42.3% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
IMMUNITY AGAINST OMICRON Preliminary results from laboratory studies examining the durability of immune responses following SARS-CoV-2 vaccines, and particularly booster doses, or previous SARS-CoV-2 infections in the face of the Omicron variant of concern (VOC) are coming fast and furious. While it is clear that the quickly spreading variant can cause breakthrough infections in fully vaccinated individuals and those who have recovered from previous infections, questions remain over how well the vaccines and their boosters will help prevent severe disease, hospitalization, or death.
The WHO held a global consultation on December 15 to examine evidence about Omicron’s ability to evade immunity, and heard reports on several studies suggesting that T cells—a type of white blood cell that play an important role in the human immune system—in vaccinated people can mount a robust defense against the VOC. While it seems increasingly likely that Omicron’s immune evasion will lead to an increase in new infections, even in fully vaccinated and previously infected individuals, researchers predict that T cells will maintain their ability to perform at a high level to help prevent severe disease.
A preprint study—published on medRxiv and not yet peer-reviewed—from researchers working at Massachusetts General Hospital, Harvard University, and the Massachusetts Institute of Technology (MIT), reinforces the potential positive impact of booster doses. The research team explored how well the 3 vaccines authorized in the US (Moderna, Pfizer-BioNTech, and J&J-Janssen) withstood a pseudovirus that was built to imitate the Omicron VOC. The findings showed “low to absent” antibody neutralization from blood sera taken from people who received a complete regimen of vaccine. In positive results, individuals who had received booster doses of an mRNA vaccine exhibited potent neutralization of the Omicron pseudovirus, highlighting the potential importance of boosters in mounting stronger immune responses.
The idea of immune escape raises several questions about the future of currently available SARS-CoV-2 vaccines, with several schools of thought emerging. Some experts argue that individuals who have received full regimens of 2-dose SARS-CoV-2 vaccines will be sufficiently protected against severe outcomes of COVID-19, while others are pushing booster doses for fully vaccinated individuals based on several laboratory studies showing the extra dose might provide some additional protection. Other researchers are calling for a rapid investment into tailored vaccines specifically designed to address the Omicron variant. All 3 arguments have merits, and it remains unclear which direction the global community—at least those nations with sufficient vaccine access and capacity—will go. The conversation surrounding vaccine booster doses and SARS-CoV-2 variants will continue for the foreseeable future, changing as new data become available.
BREAKTHROUGH CASES With the proportion of COVID-19 cases caused by the Omicron variant of concern (VOC) expected to surge in the coming weeks in the US, more data are being collected on who is becoming infected, including people who are fully vaccinated.* According to US CDC data published last week, 34 of the 43 Omicron cases initially recorded were in fully vaccinated people, 14 of whom had received a booster.** While much is still unknown about Omicron’s ability to dodge vaccine-induced immunity, it appears Omicron is able to skirt at least some protection garnered from vaccination and cause breakthrough cases. A new report from the Peterson-KFF Health System Tracker—which was conducted prior to Omicron’s detection and is based primarily on COVID-19 cases caused by the Delta variant—suggests that COVID-19 breakthrough cases are highly correlated with age (more common among those aged 65 and older) and underlying health conditions. A recent Wall Street Journal analysis came to the same conclusions. According to CDC data posted on November 22, unvaccinated persons had 14 times the risk of dying in September compared to vaccinated persons, showing that vaccination continues to be the best way to reduce the risk of severe disease, hospitalization, and death from COVID-19.
*Full original course of the vaccine, not including additional or booster doses.
**Of those who had received a booster dose, 5 were within a 14-day window.
ASYMPTOMATIC CASES In a global meta-analysis published in JAMA Network Open, researchers from China found that 40.5% (95% CI, 33.50%-47.50%) of people who had confirmed positive tests for SARS-CoV-2 never became symptomatic. Although they represented only 0.25% (95% CI, 0.23%-0.27%) of the overall pooled tested population, the study highlights the potential transmission risk of asymptomatic cases in communities. The researchers included data from 95 individual studies covering 29,776,306 individuals undergoing testing. The pooled percentage of asymptomatic cases varied among different populations: 4.52% in nursing home residents or staff; 2.02% in air or cruise travelers; 2.34% in pregnant women; 1.46% in close contacts; 0.75% in healthcare workers or in-hospital patients; and 0.40% in community residents. Among confirmed cases, the pooled percentage of asymptomatic cases was notably highest among pregnant women (54.11%), followed by air or cruise travelers (52.91%), nursing home residents or staff (47.53%), community residents (39.74%), healthcare workers or in-hospital patients (30.01%), and close contacts (26.94%). In addition to the risk that an asymptomatic infected person could unwittingly pass the virus to others, infected asymptomatic individuals likely do not have robust immune responses and might not develop lasting neutralizing antibodies that could help ward off another infection. Additionally, people with asymptomatic COVID-19 still remain susceptible to post-acute sequelae of SARS-CoV-2 infection, or “long COVID.” The findings underline the importance of comprehensive, widespread testing and highlight the suspicion that many COVID-19 cases go undetected.
J&J-JANSSEN VACCINE CONTRAINDICATION The US FDA on December 14 updated its fact sheets on the J&J-Janssen SARS-CoV-2 vaccine for healthcare providers and the general public to include a contraindication for individuals with a history of thrombosis with thrombocytopenia following the vaccine or any other adenovirus-vectored vaccine for COVID-19, as well as updated information about the risk of thrombosis with thrombocytopenia syndrome (TTS) following vaccination. The risk of TTS after vaccination using the J&J-Janssen vaccine remains low, but about 15% of cases have been fatal, according to the FDA. The highest reporting rate is among females between the ages of 30 and 49 (about 1 case per 100,000 doses administered). The US CDC’s Advisory Committee for Immunization Practices (ACIP) is meeting today to discuss the data and possibly recommend limitations on the use of the J&J-Janssen vaccine. The clotting issues also have been linked to the AstraZeneca-Oxford vaccine, which is not authorized in the US, but have not been reported with the mRNA vaccines from Moderna or Pfizer-BioNTech.
VACCINE PASSPORTS Many nations, localities, and businesses are beginning to mandate proof of SARS-CoV-2 vaccination, or so-called vaccine passports, for entry onto public transportation and into venues such as restaurants, night clubs, and stadiums. Public health officials agree that vaccination is the best way to prevent COVID-19 or lower the risk of severe disease, but others question the utility of vaccine certificates, with some nations experiencing protests and riots. A modeling study published this week in The Lancet Public Health suggests that countries that required proof of vaccination, recent infection, or negative SARS-CoV-2 test to engage in activities or travel generally saw an increase in uptake of the vaccines. The researchers examined the effects of vaccine requirements in 6 countries and found that COVID-19 certifications lead to increased uptake of vaccines 20 days prior to implementation and up to 40 days following, with the highest increases among populations aged 49 and younger. More widespread vaccinations help to protect individuals from severe illness but also help curb the spread of SARS-CoV-2 in vulnerable communities and demographics, a critical issue amid the current Omicron variant of concern-associated surge. Policymakers should consider vaccine certification as part of their COVID-19 strategies to address vaccine complacency and hesitancy and potentially increase uptake but keep in mind ethical considerations, as the requirements will not work among all populations.
US COLLEGES & UNIVERSITIES The heightened transmissibility of the Omicron variant of concern (VOC) presents a number of new challenges for institutions that have returned to in-person or hybrid activities. US colleges and universities—which can be hotbeds for disease transmission given the frequency of large group gatherings and the existence of communal living spaces—are now revisiting their COVID-19 mitigation strategies to account for Omicron. Already, several schools have reported cases of the Omicron variant in addition to their weekly reports. Cornell University this week reported more than 900 new COVID-19 cases, with many suspected to be Omicron infections among fully vaccinated students, some of whom had received booster doses. Cornell decided to close in-person activity at its Ithaca branch in response to the outbreak. Other schools, including New York University, have begun to cancel nonessential gatherings and events and are requiring booster shots for students who plan to return to campus for the spring semester. While many colleges and universities are keeping their current mitigation strategies in place for the remainder of the fall semester, school officials are watching data closely to prepare for the larger challenge of what to do when students return in the new year.
by dmforever My dentist told me yesterday that her brother's son (20 something) got Covid and was hospitalized for 5 days. Her brother and SIL still wouldn't get, and aren't, vaccinated. It defies all rational thought.
Kevin
by ponchi101 I will go the other way. On Saturday, I went to play padel with friends. We were OUTDOORS, and the girl from the sport complex showed up and asked for our reservation and OUR VACCINE card. I had left mine in my other back pack and was about to be told "sorry, but you are out" (and, again, we were outdoors) when I remembered that I had scanned it and kept a PDF in my phone. I showed it to her, we could keep playing.
it is that simple here. No vaccines, no indoor anything. Or, in our case, not even outdoor playing.
(Private facility so they decide how to handle it).
by dryrunguy I finally got my booster this morning (Moderna). Let's just say that didn't go as well as my first dose (J&J). I'm still not quite "right". But I'm better than I was during most of the drive home. It was a little scary because what I was feeling felt a lot like what I THINK myocarditis would feel like. Not that I really know what that would feel like.
I figured my brain was playing tricks on me, but I'm 99% sure that wasn't the case. Especially since I'm still not quite right. Hopefully I will feel better in the morning.
by JazzNU
dryrunguy wrote: ↑Fri Dec 17, 2021 1:59 am
I finally got my booster this morning (Moderna). Let's just say that didn't go as well as my first dose (J&J). I'm still not quite "right". But I'm better than I was during most of the drive home. It was a little scary because what I was feeling felt a lot like what I THINK myocarditis would feel like. Not that I really know what that would feel like.
I figured my brain was playing tricks on me, but I'm 99% sure that wasn't the case. Especially since I'm still not quite right. Hopefully I will feel better in the morning.
Definitely might take a day or two til you feel like yourself. Some feel better the next day, but many had symptoms for 48-72 hours too.
FYI, and this goes for everyone, if you're willing to share the symptoms you have, it's helpful to report it to the CDC thru their V-Safe program. After registering, they'll text you a reminder each day and you'll report any symptoms you have. Takes a minute each day.
by JazzNU My aunt is off continuous flow oxygen this week for the first time since her hospitalization in early September. Still needs to use it at night. I didn't even mention it here, but she was re-hospitalized for several days a few weeks after her initial discharge. She's now going to be seeing a pulmonologist and cardiologist regularly for the foreseeable future to monitor recovery issues and lasting damage it's done.
So go get the vaccine, get your booster, wear a mask, get tested if you're going to be around a larger group or if you've just finished attending a larger gathering. Be as responsible as you can be during the holidays while still trying to enjoy them with your friends and family. And don't assume anyone's vaccination status, ask it. You don't want covid, especially a severe case.
by Deuce With COVID-19 numbers rising significantly in North America over the past few weeks, and many pro sports games being postponed because too many players on the teams have contracted the virus, extreme measures are returning...
by ti-amie When I got my booster I thought "hey this is better than my first or second shot". About four hours later I was looking at something tennis related and not one thing on the printed page looked like an alphabet I am familiar with. I shut down my computer, took two arthritis strength acetaminophen, and went to bed. It took a day or two for my brain to come out of the fog.
by ti-amie This is not good.
by Deuce Indeed, it was simply a matter of time before the term 'fully vaccinated' was re-defined to include the third shot.
We should expect this re-definition to spread. At least, I hope it does.
And this will very likely not be the last re-definition of 'fully vaccinated'.
by ponchi101 Adding to Dry and Ti's comments. I also got a reaction from my booster, spending the night with a mild fever. I got nothing from my 1st and 2nd shots.
Nothing to deter me from recommending getting your booster, or that will stop me from getting my fourth when the time comes.
by ti-amie
by dryrunguy This morning's NY Times e-newsletter included the following language. I cannot read the links substantiating them because they are behind paywalls.
::
2. Most of the world’s vaccines provide almost no defense against infection from Omicron, studies show.
All vaccines still seem to provide a significant degree of protection against serious illness from Omicron, which is the most crucial goal. But only the Pfizer and Moderna shots, when reinforced with a booster, appear to have success at stopping infections, and these vaccines are unavailable in most of the world. (https://www.nytimes.com/2021/12/15/heal ... f11dfcd63a)
The other shots — including AstraZeneca, Johnson & Johnson and vaccines made in China and Russia — do little to nothing to stop the spread of Omicron, early research shows. The gap could have a profound impact on the course of the pandemic. (https://www.nytimes.com/2021/12/19/heal ... f11dfcd63a)
by ponchi101 I said it above. 2022, deja vu of 2020.
by ti-amie This thing will be with us a very long time.
by dryrunguy I see #COVIDIOTS is trending on Twitter... Right above #FJBiden.
by ponchi101
ti-amie wrote: ↑Sun Dec 19, 2021 6:30 pm
This thing will be with us a very long time.
I don't want OMICRON. I want OMYGODCRON, a variant that will kill the unvaccinated through a violent stack of sneezing and coughing, in public, on the street.
"I am asymptomatic".
True question. Can this virus also be the calamity it is because over the last 50 years the teaching of science, all over the world, has been declining and people really do not understand the basic tenets of what is being talked about?
(I am not sure if the teaching of science has been declining all over the world. I am only trying to find an explanation for people like above).
by mmmm8 Things in NY are getting pretty bad again in terms of infections, as per a post above. Almost everyone I know has been informed about a close contact with someone who's tested positive for COVID, including myself (I've done two rapid tests that were negative and am waiting for PCR results). The lines at testing sites are crazy again. And my company just sent an email requesting we work from home.
A potential silver lining for Omicron from my cousin, who is a pulmonologist is that she is glad that this is the strain that's so infectious because it seems to be milder than the previous Greek letter versions and if we all get this one, at least it might help eliminate the more dangerous ones and help mutate the virus into something more manageable.
by atlpam I saw a doctor interviewed who said omicron seems to stay in the upper respiratory, more like a cold. Of course there are still plenty of colds that can lead to bronchitis, but hopefully not the lung impact that earlier variants have caused.
by Suliso I have no personal experience with what's happening at work or in Switzerland now (took entire December off), but from press reports doesn't look good. Clearly I'll have to work from home again in January...
by MJ2004 My husband's company had plans for workers to return to the office in January, they just sent an email indefinitely postponing it. Harvard just announced classes will be mostly remote in January, which is a sign that the rest of the universities in the area will likely follow suit and I will also be back home. Here we go again...
We are flying to Florida on Wednesday and fingers crossed on the trip. We'll boosted, but we'll still be double-masking.
by ti-amie Wishing you a safe trip MJ.
by MJ2004
ti-amie wrote:Wishing you a safe trip MJ.
Thanks. I hope this doesn’t turn out to be a bad idea.
by ponchi101 Nope. Trust your boosters and your good judgement. And enjoy the sun!
Thanks. I hope this doesn’t turn out to be a bad idea.
Enjoy the sun and the nice weather, wear masks, avoid the Floridians. We're going on the 28th, this will be our 3rd pandemic trip there and these tips had served us on the first two!
by Suliso Everyone so much in love with Florida?
Btw I'm in Texas today (last night).
by ponchi101 We are only hoping and wishing MJ has a great vacation.
Nobody is suggesting "Go, MJ! And NEVER LEAVE!!!!!"
by MJ2004
Suliso wrote:Everyone so much in love with Florida?
It’s not so much love of Florida as my parents are there. Not that I mind the sun and warm temps. It was a high of 32 here today and getting dark at 4pm.
by mmmm8 It's not so much love of Florida as love of a free apartment and car available to us in a warm climate a cheap flight away (this time, my partner's family will be there from Venezuela whom he hasn't seen in 4 years)
Where in Texas are you, Suliso?
by Suliso
mmmm8 wrote: ↑Mon Dec 20, 2021 4:56 am
Where in Texas are you, Suliso?
El Paso.
We're at the end of a two week road trip through Arizona, NM and Texas (arranged before the omicron...). Mostly hiking through national parks, last 3 days in Big Bend. I highly recomend that park for anyone who likes being outdoors.
Been very lucky with the climate here. Today the first somewhat cold day of the trip.
mmmm8 wrote: ↑Mon Dec 20, 2021 4:56 am
Where in Texas are you, Suliso?
El Paso.
We're at the end of a two week road trip through Arizona, NM and Texas (arranged before the omicron...). Mostly hiking through national parks, last 3 days in Big Bend. I highly recomend that park for anyone who likes being outdoors.
Been very lucky with the climate here. Today the first somewhat cold day of the trip.
Did you go to Bandelier in NM?
My advice on avoiding Floridians to avoid Covid extends to avoiding Texans
by Suliso No, actually not heard of that place... Our approximate route was Saguaro NP, Chiricahua NM, White Sands NP, Carlsbad Caverns NP, Guadelupe mountains NP, Big Bend NP. The first two are in Arizona, the second two in NM and the last two in Texas. Except for flying in and out we avoided cities. They are not much to write home about in these parts anyway.
by Suliso Btw Marfa, Texas is a nice cute town. There is a breakfast place there which could be a contender for the best in USA. At least I can't recall any even close.
by mmmm8
Suliso wrote: ↑Mon Dec 20, 2021 2:36 pm
No, actually not heard of that place... Our approximate route was Saguaro NP, Chiricahua NM, White Sands NP, Carlsbad Caverns NP, Guadelupe mountains NP, Big Bend NP. The first two are in Arizona, the second two in NM and the last two in Texas. Except for flying in and out we avoided cities. They are not much to write home about in these parts anyway.
Disagree about the cities in NM (Santa Fe and Albuquerque are both lovely) and San Antonio is nearby. Wouldn't live in any of these, but worth a visit for sure. But I'm a city lover.
Bandelier is a preservation land that also maintains historic dwellings of Southwest native populations. The vast majority of it is just a park though with cool hiking and waterfalls. It's also right next to Los Alamos (of the nuclear bomb fame).
by ponchi101 When I am in CO, I am only 20 miles North of NM, so I get to go there.
Agree with M8 that Santa Fe is lovely. I can't tell about ABQ because I have only been to the airport. Taos is great, and Los Alamos is straight out of a postcard from the 1950's. The town in frozen in time. Plus, the Atom Museum is a must for any science lover. A rather balanced exposition of what went on there during the Manhattan project.
About San Antonio: if I were forced to live in TX, but I can choose the place, SA it is. I really liked it.
(But no way I get to live in TX by my own choice).
by Suliso Well, I can only speak of places I have been to in the area (Phoenix, Tucson, Carlsbad, El Paso). Didn't particularly like any of them. Not that it matters, we were there for the nature and that certainly didn't disappoint.
by mmmm8 Now I know two people who've been to Carlsbad, New Mexico, you and Bojana Jovanovski
by Suliso What's the story with Jovanovski?
by Deuce .
Interesting article about the difference in COVID-19 perspectives between Canada and the USA...
by ashkor87 Oh I have been there, to see the bats..awesome sight
by dryrunguy Here's the latest Situation Report from Johns Hopkins. What a mess.
::
RISE OF OMICRON The Omicron variant of concern (VOC) has become the predominant variant across North America and Europe, while the rest of the world braces for the eventual takeover. The WHO announced on December 18 that 89 countries have now reported Omicron within their borders, with high likelihood that cases are in many other countries but have simply not yet been confirmed. While the Delta VOC previously overtook other circulating variants to become the predominant SARS-CoV-2 variant, Omicron’s rise in these regions occurred precipitously, within 1 month after it was first reported in South Africa on November 24. While preliminary data out of South Africa indicated that infection with the Omicron variant was less likely to lead to hospitalization, the sheer number of cases resulting from the highly transmissible variant appear to be causing significant healthcare strain and societal disruption.
In the US, Omicron now accounts for 73.2% of the total number of SARS-CoV-2 infections, compared to 1 week ago when it accounted for only 12.6% of all infections. As of December 20, 48 states, Puerto Rico, and Washington, DC, have reported cases of Omicron; South Dakota and Oklahoma have yet to report cases. This rapid increase in Omicron cases has startled public health officials. With cases currently doubling every 1.5 to 3 days, healthcare facilities are bracing for a surge in hospitalizations, with some regions already experiencing these challenges. In the Northeast, where cases are currently surging, states like Rhode Island and Maine are reporting that their hospitals are being strained to their limits. As community members seek medical care in high numbers, healthcare staff are also testing positive for SARS-CoV-2, further exacerbating the strain on resources. Some states are activating their National Guards to help bolster medical, testing, and vaccination efforts. With testing lines wrapping around city blocks and holiday travel quickly approaching, public health officials are urging all who are able to get fully vaccinated and receive their booster shots. US President Joe Biden is set to address the nation tonight and is expected to announce plans to supply free tests and more aid for hospitals.
Outside of the US, other countries are facing the same challenges with the added difficulties of lower vaccination rates due to decreased access and supply. While most world leaders seem hesitant to initiate lockdowns akin to the initial March 2020 responses, many are implementing restrictions in an effort to slow the entry of Omicron into their nations. Israel has banned travel to North America and many European countries, while Asia Pacific island nations are moving to close their borders to international travelers or at least increase surveillance and quarantine measures for inbound travelers. In many European countries where Omicron is already spreading at high rates, some leaders are considering implementing stricter measures ahead of the holiday season. In the UK, Prime Minister Boris Johnson stated he is considering a number of measures, including lockdowns, as COVID-related hospitalizations rise. Regardless of strategy, all countries are trying to accelerate their vaccination programs to prevent a collapse of their healthcare systems.
VACCINE EFFICACY As the Omicron variant of concern (VOC) continues to rapidly spread around the world, preliminary data all of the vaccines appear to provide protection against severe disease, but most of the SARS-CoV-2 vaccines used worldwide may offer little defense against infection from the highly contagious variant. According to a not-yet-peer-reviewed analysis from Imperial College London, Omicron can largely evade vaccine-induced immunity or immunity from a past infection, with the risk of reinfection estimated to be 5.4 times greater than that with the Delta VOC. The researchers estimated that vaccine effectiveness (for AstraZeneca-Oxford and Pfizer-BioNTech vaccines) against symptomatic Omicron infection is between 0% and 20% after 2 doses and between 55% and 80% after a booster dose. Preliminary laboratory results from Moderna released this week in a press release showed a 50 μg booster dose—the same formulation authorized as a booster by the US FDA—produced a 37-fold increase in neutralizing antibodies compared with the primary 2-dose series, while a full 100 μg dose booster produced an 83-fold increase over 2 doses. The full dose had slightly more side effects than the half dose. Pfizer-BioNTech earlier this month announced a booster dose of their vaccine also helped increase neutralizing antibodies against Omicron. All of the studies are preliminary and do not take into account the full spectrum of the human immune response.
Still, some experts are saying that a 3-dose vaccination schedule will be necessary and some evidence shows the time between a second and third dose can be shortened from 6 months to 3 months. Several countries—such as South Korea, UK, Thailand, Belgium, France, Singapore, Taiwan, Italy, and Australia—have decreased the required wait time between doses to between 3 and 5 months to prepare for the arrival of Omicron. Others—including the US, South Africa, and Germany—are sticking to a 6-month schedule. Though there is some concern that shortening the gap could compromise immune response to vaccinations, others say a 6-month interval is arbitrary and urge booster doses sooner to counter waning antibody levels. Many uncertainties remain about how pre-existing immunity, whether from vaccination or previous infection, will help during infection with Omicron, and some evidence suggests Omicron-specific vaccine boosters will be necessary. While many higher-income nations are focused on vaccinating, and boosting, their populations, only 8% of the populations in low-income countries have received at least 1 dose of vaccine. It is important that the international community not lose focus on global goals pertaining to vaccine access and administration.
OMICRON SEVERITY An initial study (unpublished) on the severity of the SARS-CoV-2 Omicron variant of concern (VOC) conducted in South Africa suggests that adults are approximately 30% less likely to be hospitalized due to severe COVID-19 now than during the Delta surge. Health experts from the region also claim that hospitalized patients are less likely to end up on ventilators or require intensive care, on average, than during previous surges of COVID-19. However, scientists and public health officials have been quick to point out that the mild reactions to Omicron in South Africa may not be seen in Europe and the US. A large percentage of the South African population is young, by comparison, and many already have some immunity to SARS-CoV-2 due to prior infection during previous surges or vaccination. This immunity is believed to be a prominent factor driving the reduced disease severity observed in South Africa. In the US, researchers from the Covid-19 Modeling Consortium at the University of Texas at Austin looked at 18 different scenarios for Omicron, warning that under the most pessimistic model, “Omicron could lead to the largest healthcare surge to date, unless measures are taken to slow spread.” The data have not yet been peer-reviewed.
As such, concerns over hospital capacity are rising, as many individuals are expected to travel and spend time with family during the holiday season, increasing the risk of transmission of the highly contagious VOC. US states such as New York and New Jersey are already reporting high hospitalization rates and an increased demand for testing. The US Department of Health and Human Services (HHS) reports that more than 76% of ICU beds are currently in use, with 21% of those beds being used for COVID-19 patients. Additionally, Regeneron and Eli Lilly are warning that their antibody treatments for COVID-19 might be less potent against Omicron. The US reported its first Omicron-related death on December 20. The UK offers an unsettling potential lens into the future for the US. The UK Health Security Agency reports at least 14 deaths due to Omicron and 129 hospitalizations as of December 20, up from 7 and 85 on December 18. While it remains too early to tell the damage Omicron will inflict, the growing number of deaths and hospitalizations indicate that the variant should not be viewed as a slightly worse form of the common cold.
NOVAVAX VACCINE Following months of manufacturing delays, the 2-dose SARS-CoV-2 vaccine from biotechnology company Novavax, NVX-CoV2373, received conditional marketing authorization by the European Commission on December 20 and an emergency use listing (EUL) from the WHO on December 17. In Europe, the vaccine is known as Nuvaxovid and is the fifth vaccine to receive authorization to prevent COVID-19 in adults aged 18 years and older. Novavax expects to begin shipping the vaccine to the European Union in the first quarter of 2022. The WHO’s EUL—the ninth for a SARS-CoV-2 vaccine—is for a version of the vaccine manufactured and marketed by the Serum Institute of India (SII), under license from Novavax, known as Covovax. The WHO listing allows the COVAX facility to distribute the vaccine with hopes of bolstering global vaccine supply. Covovax—an adjuvanted, recombinant spike protein nanoparticle vaccine—is less expensive and simpler to manufacture than some of the other vaccine types and easier to distribute, as it can be stored for 6 months in normal refrigeration.
The New England Journal of Medicine last week published results from a phase 3 clinical trial testing the vaccine in nearly 30,000 adults in the US and Mexico, showing vaccine efficacy against symptomatic infection to be 90.4%, with 100% efficacy against moderate-to-severe disease. Most of the COVID-19 cases sequenced in the study were caused by B.1.1.7 (Alpha), and the vaccine’s efficacy against any variant of concern (VOC) or interest was 92.6%. The vaccine’s efficacy against the new Omicron VOC is unknown, but having another effective vaccine is important in helping to control the pandemic. In November, Indonesia was the first country to grant emergency use authorization (EUA) to the Novavax vaccine, followed by the Philippines. The company has plans to apply for an EUA with the US FDA by the end of the year.
PFIZER-BIONTECH VACCINE IN YOUNG CHILDREN Pfizer-BioNTech last week released an update on its ongoing phase 1/2/3 study evaluating their SARS-CoV-2 vaccine among children ages 6 months to under 5 years of age. An immunogenicity analysis showed that 1 month after the second 3 µg dose of the vaccine, participants aged 2 to under 5 did not show a robust immune response to the lower-dose shots when compared to the immune responses seen in older teens and young adults. The companies said the trial will continue but they plan to evaluate a third 3 µg dose of vaccine administered at least 2 months after the second dose to all age groups in the study, with the hope that a 3-dose regimen will elicit more protective immune responses. The companies said no safety concerns have arisen. The data have not been released publicly and many questions remain, including what the immune response was in the 2 to under-5 age group, if any.
The shift in plans also pushes back the companies’ expected timeline to submit results to the US FDA from the end of this year to the second quarter of 2022, if the results are positive. They also announced plans to test a third dose of the already authorized 10 µg formulation in children ages 5 to 12 years; a trial to evaluate a third dose of 10 µg or 30 µg in adolescents ages 12 to 17 in order to assess safety and immunogenicity; and the development of an Omicron variant-specific vaccine. The companies also last week filed with the FDA to request that adolescents ages 12 to 15 years be included in the vaccine’s full approval, with filings in the European Union and other regulatory authorities expected soon. The Pfizer-BioNTech vaccine, known as Comirnaty, received full FDA approval as a 2-dose (30 µg) regimen for individuals ages 16 years and older in August.
“TEST TO STAY” GUIDANCE The US CDC on December 17 said unvaccinated students exposed to a person with COVID-19 can remain in school if they are tested twice in the week following exposure and both tests are negative. The new guidance, known as “test to stay,” is an effort to keep children in school instead of having to quarantine at home and miss class, while also alleviating the burden on parents to arrange child care. The new protocol—which should be used as one method in a layered prevention approach—is based on 2 studies published in the CDC’s Morbidity and Mortality Weekly Report (MMWR), one examining the policy in Los Angeles County, California, and the other in Lake County, Illinois. The studies were conducted prior to the detection of the fast-spreading Omicron variant of concern, but CDC officials said they have confidence the mitigation strategy will work and will update guidance as needed. Agency officials also urged parents to vaccinate their children if they are eligible, as it remains the best way to prevent infection or severe disease. Under current CDC guidance, vaccinated people do not have to quarantine after a known exposure unless they have symptoms but should be tested 5-7 days after the exposure and wear a mask until testing negative.
US VACCINE MANDATES A federal appeals court last week lifted the stay on the Biden administration’s “vaccine or test” COVID-19 mandate for businesses with 100 or more employees, prompting confusion over whether companies need to comply with the Occupational Safety and Health Administration (OSHA) temporary rule. Following the order, several appeals were filed with the US Supreme Court requesting Justice Brett Kavanaugh, who has jurisdiction over the appeals court that lifted the stay, to consider the rule and immediately enjoin enforcement of the rule. Justice Kavanaugh likely will refer the case to the full court, and the justices have not acted on the emergency request. The Supreme Court asked the Biden administration to file its response by December 30, and the court is expected to make a decision in early 2022. Separately, the Biden administration has asked the court to stay lower-court decisions enjoining enforcement of a Centers for Medicare and Medicaid Services (CMS) vaccine mandate for healthcare workers. The Supreme Court has generally supported vaccine mandates implemented by state governments and universities but shown more nuance when considering federal pandemic-related rules.
Meanwhile, the US Armed Forces are beginning disciplinary actions, including dismissals, for members of the military who have not yet been vaccinated. As many as 20,000 troops risk being discharged. The US Department of Defense also is requiring members of the National Guard to be vaccinated against COVID-19. But governors from 5 states—Iowa, Wyoming, Alaska, Mississippi, and Nebraska—are pushing back on the mandate, arguing in a letter that National Guard members fall under the jurisdiction of their state, unless they are federally deployed, and would therefore not be subject to federal mandates. The Defense Department has not responded to the letter. Notably, the department last month rejected a request from Oklahoma Governor Kevin Stitt to exclude the state’s National Guard members from the federal mandate, instead releasing new guidance saying members who refuse vaccination will receive a general officer memorandum of reprimand, which could be grounds for administrative separation.
MODERNA VACCINE PATENT DISPUTE Moderna has paused a dispute with the US government by not taking the final step in obtaining a patent for technologies used in its SARS-CoV-2 mRNA vaccine. The company said making the payment to obtain the patent “could interfere with further discussions aimed at an amicable resolution” with the US National Institutes of Health (NIH) and wanted to “avoid any distractions” in ongoing collaboration amid efforts to respond to the quickly spreading Omicron variant of concern (VOC). At issue is who should be credited with developing the genetic sequence technology used in the company’s mRNA vaccine. Scientists from Moderna and NIH worked quickly in early 2020 to invent the technology, but Moderna has disputed claims that the NIH researchers are co-inventors. Moderna maintains that only its scientists deserve credit and has filed an application to pursue a patent at a later date. Moderna is projected to bring in as much as US$18 billion in sales of the vaccine this year and has been under increasing pressure to share its vaccine technology with low- and middle-income countries in order to increase global supply. At this time, it is unclear whether Moderna’s decision to pause its patent application has implications for the US government’s global vaccination strategy.
by ti-amie
by ponchi101 The usual suspects, but the mail is from August 25, 2020. So, this was set up by Tiny and his minions?
Not terribly confusing, but this was last year. So she is NOT declining to participate. It happened last year.
by ti-amie
ponchi101 wrote: ↑Tue Dec 21, 2021 10:01 pm
The usual suspects, but the mail is from August 25, 2020. So, this was set up by Tiny and his minions?
Not terribly confusing, but this was last year. So she is NOT declining to participate. It happened last year.
I took this as Birx trying to rehabilitate her image. In other words "look I didn't go along with all of the clown show! I'm still a professional." Everything she did afterwards though led to how she's regarded now by some members of the public and I assume by her peers.
by mmmm8
Suliso wrote: ↑Mon Dec 20, 2021 10:51 pm
What's the story with Jovanovski?
by Jeff from TX Sorry to have been absent for awhile, but at the beginning of December I got COVID (I assume Delta) - the week I was supposed to get my booster shot. I assumed it was the flu since my rapid test came back negative but a later test confirmed COVID. Fever for almost 10 days, lots of fatigue, slight cough but no real respiratory issues fortunately. Thankfully, I had finished my preceptorship hours so my graduation was not affected. Graduated Dec. 15th with my nursing degree.
by ponchi101
Jeff from TX wrote: ↑Wed Dec 22, 2021 5:01 pm
Sorry to have been absent for awhile, but at the beginning of December I go COVID (I assume Delta) - the week I was supposed to get my booster shot. I assumed it was the flu since my rapid test came back negative but a later test confirmed COVID. Fever for almost 10 days, lots of fatigue, slight cough but no real respiratory issues fortunately. Thankfully, I had finished my preceptorship hours so my graduation was affected. Graduated Dec. 15th with my nursing degree.
First, glad you are back and that C19 did not affect you badly. Keep us posted on how you feel and possible effects later (I hope there are none) as we can learn from your experience. I believe we all will have a date with Omicron eventually, so any advice from you would be priceless.
And second, CONGRATS on that degree! I wish you all the best in your professional life
by MJ2004 I’m at the airport terminal surrounded by people who are sniffling and coughing. If the double mask doesn’t hold it off, my date will be sooner rather than later. Unfortunately just in time for Christmas.
Sorry Jeff that happened to you. It sounds terrible. Glad you’re recovered now. Congrats on graduating - what a wonderful accomplishment!
by ti-amie
Jeff from TX wrote: ↑Wed Dec 22, 2021 5:01 pm
Sorry to have been absent for awhile, but at the beginning of December I go COVID (I assume Delta) - the week I was supposed to get my booster shot. I assumed it was the flu since my rapid test came back negative but a later test confirmed COVID. Fever for almost 10 days, lots of fatigue, slight cough but no real respiratory issues fortunately. Thankfully, I had finished my preceptorship hours so my graduation was affected. Graduated Dec. 15th with my nursing degree.
I'm so sorry to hear you were so ill!
CONGRATULATIONS to you for receiving your degree!
by ti-amie
That guy with his arms crossed in defiance perfectly captures the attitude of the folks inside.
by ti-amie So we just found this out.
A friend of my daughter just found out that on Monday her son was exposed to the virus. A kid he hangs out with was sick on Monday. They share a lunch table. The mother, my daughter's friend, just found out today. Her husband is a cancer survivor and immunocompromised.
Her son had a tummy ache today and was told by the school nurse he was exposed. No notice was sent to parents about the child who showed up sick on Monday. Her son just went to take a test.
What is wrong with people?
by JazzNU
Jeff from TX wrote: ↑Wed Dec 22, 2021 5:01 pm
Sorry to have been absent for awhile, but at the beginning of December I got COVID (I assume Delta) - the week I was supposed to get my booster shot. I assumed it was the flu since my rapid test came back negative but a later test confirmed COVID. Fever for almost 10 days, lots of fatigue, slight cough but no real respiratory issues fortunately. Thankfully, I had finished my preceptorship hours so my graduation was not affected. Graduated Dec. 15th with my nursing degree.
So happy to hear you had more minor symptoms and are doing better.
Congrats on getting your nursing degree, I know you've been working hard for it. Hope your bout with covid didn't dim your celebration of this achievement too much.
by JazzNU FWIW, I've started using a KF94 mask as of last week for greater protection when I'm out and about with omicron raging. They are similar to the KN95, just slightly different design and from Korea (with tighter production controls). I like them a lot. I haven't double masked since getting vaccinated, but prefer this greatly to double masking, which for me, was slightly harder to breathe in, made my face hot, and was a real setback with my glasses fogging up.
by JazzNU
Pfizer pill becomes 1st US-authorized home COVID treatment
By MATTHEW PERRONE
WASHINGTON (AP) — U.S. health regulators on Wednesday authorized the first pill against COVID-19, a Pfizer drug that Americans will be able to take at home to head off the worst effects of the virus.
The long-awaited milestone comes as U.S. cases, hospitalizations and deaths are all rising and health officials warn of a tsunami of new infections from the omicron variant that could overwhelm hospitals.
The drug, Paxlovid, is a faster way to treat early COVID-19 infections, though initial supplies will be extremely limited. All of the previously authorized drugs against the disease require an IV or an injection.
An antiviral pill from Merck also is expected to soon win authorization. But Pfizer’s drug is all but certain to be the preferred option because of its mild side effects and superior effectiveness, including a nearly 90% reduction in hospitalizations and deaths among patients most likely to get severe disease.
“The efficacy is high, the side effects are low and it’s oral. It checks all the boxes,” said Dr. Gregory Poland of the Mayo Clinic. “You’re looking at a 90% decreased risk of hospitalization and death in a high-risk group — that’s stunning.”
The Food and Drug Administration authorized Pfizer’s drug for adults and children ages 12 and older with a positive COVID-19 test and early symptoms who face the highest risks of hospitalization. That includes older people and those with conditions like obesity and heart disease, though the drug is not recommended for patients with severe kidney or liver problems. Children eligible for the drug must weigh at least 88 pounds (40 kilograms).
The pills from both Pfizer and Merck are expected to be effective against omicron because they don’t target the spike protein where most of the variant’s worrisome mutations reside.
Pfizer currently has 180,000 treatment courses available worldwide, with roughly 60,000 to 70,000 allocated to the U.S. The company said it expects to have 250,000 available in the U.S. by the end of January.
Federal health officials are expected to ration early shipments to the hardest hit parts of the country. Pfizer said the small supply is due to the manufacturing time — currently about nine months. The company says it can halve production time next year.
The U.S. government has agreed to purchase enough Paxlovid to treat 10 million people, and it will be provided free to patients. Pfizer says it’s on track to produce 80 million courses globally next year, under contracts with the U.K., Australia and other nations.
President Joe Biden said the pill marks a “significant step forward in our path out of the pandemic” and said his administration will work with states to ensure equitable distribution.
Health experts agree that vaccination remains the best way to protect against COVID-19. But with roughly 40 million American adults still unvaccinated, effective drugs will be critical to blunting the current and future waves of infection.
The U.S. is now reporting more than 140,000 new infections daily and federal officials warn that the omicron variant could send case counts soaring. Omicron has already whipped across the country to become the dominant strain, federal officials confirmed earlier this week.
Against that backdrop, experts warn that Paxlovid’s initial impact could be limited.
For more than a year, biotech-engineered antibody drugs have been the go-to treatments for COVID-19. But they are expensive, hard to produce and require an injection or infusion, typically given at a hospital or clinic. Also, laboratory testing suggests the two leading antibody drugs used in the U.S. aren’t effective against omicron.
Pfizer’s pill comes with its own challenges.
Patients will need a positive COVID-19 test to get a prescription. And Paxlovid has only proven effective if given within five days of symptoms appearing. With testing supplies stretched, experts worry it may be unrealistic for patients to self-diagnose, get tested, see a physician and pick up a prescription within that narrow window.
“If you go outside that window of time I fully expect the effectiveness of this drug is going to fall,” said Andrew Pekosz, a Johns Hopkins University virologist.
The FDA based its decision on company results from a 2,250-patient trial that showed the pill cut hospitalizations and deaths by 89% when given to people with mild-to-moderate COVID-19 within three days of symptoms. Less than 1% of patients taking the drug were hospitalized and none died at the end of the 30-day study period, compared with 6.5% of patients hospitalized in the group getting a dummy pill, which included nine deaths.
Pfizer’s drug is part of a decades-old family of antiviral drugs known as protease inhibitors, which revolutionized the treatment of HIV and hepatitis C. The drugs block a key enzyme which viruses need to multiply in the human body.
The U.S. will pay about $500 for each course of Pfizer’s treatment, which consists of three pills taken twice a day for five days. Two of the pills are Paxlovid and the third is a different antiviral that helps boost levels of the main drug in the body.
by ti-amie I was thinking today about how much damage Tiny and his people did early on. They made it seem that if you were young, in good shape, and not brown, black or yellow you wouldn't be in too much danger. That message took hold and that is why so many have been ignoring sound medical advice.
Don't get me wrong. As we see there are a lot of non white people who have gone for the okey-doke with consequences that are only now becoming clear. I have family members who have been going to concerts and hanging out with no concern about anything happening to them. Tiny had one chance to do something right and being who he is he blew it. I'm sure the virus is already mutating into some new Greek letter designation that a country like South Africa will find before scientists do here.
It's hard to see that so many have been led astray - by people who are vaccinated.
It's really a shame what is happening now.
by dryrunguy My issue with it has always been that the "I'm young and healthy, so I don't need to worry and don't need to be vaccinated" argument is never predicated on the qualifier that should follow it, if you're going to go there: "But I'm going to do everything I can to avoid contact with more vulnerable populations to reduce THEIR risk of exposure from me." Which immediately renders it an intellectually lazy and socially irresponsible stance.
But when it's all said and done, people just don't care.
They just don't care.
by Deuce .
It's difficult - but necessary - to maintain a balanced perspective...
This is quite interesting...
ti-amie wrote: ↑Thu Dec 23, 2021 1:49 am
I was thinking today about how much damage Tiny and his people did early on. They made it seem that if you were young, in good shape, and not brown, black or yellow you wouldn't be in too much danger. That message took hold and that is why so many have been ignoring sound medical advice.
For months now, since Delta has been a larger concern in the US, it has seemed as if white people were told a secret that the rest of us weren't let in on because the less diverse the area, the less masks being worn around this region as if they had nothing at all to worry about. I can't count the number of stores I've been in the last 4 months where almost every minority has been wearing a mask and almost every white adult is not, with the exception of employees. Mild uptick of masks in November, and a greater one in the last 2 weeks.
My favorite are the senior citizens and young children that are maskless. I don't it. And this is an area that was universally masked earlier in the year, it was never a battle here. Definitely seems like they are privy to some information that I'm not that gives them quite a bit of confidence.
by ti-amie I see a lot of young black and brown people maskless - the FB, TikTok and WhatsApp people. I wonder what disinformation they were targeted with?
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 275 million cumulative cases and 5.36 million deaths worldwide as of December 22. Global weekly incidence increased for the ninth consecutive week, up 4.7% from the previous week. Europe’s surge, which is believed to be largely driven by the Omicron variant, appears to be peaking, and the trend in Africa continues to accelerate sharply, setting a new weekly record (90,450 new cases; +55% from the previous week). The overall trends in the Americas and the Western Pacific are increasing as well. Global weekly mortality decreased for the second consecutive week, down 5.2% from the previous week. With 46,554 new deaths, last week's total fell slightly below the average since mid-October, but it is unclear whether this is the beginning of a longer-term trend, particularly in the context of increasing trends in weekly incidence.
Global Vaccination
The WHO reported 8.4 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of December 20. A total of 4.38 billion individuals have received at least 1 dose, and nearly 3.5 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations increased from mid-October (21.3 million doses per day) through mid-December (39.9 million). Daily vaccinations have decreased since December 15, down to 34.5 million, but it is unclear whether this is a result of short-term fluctuations or the start of a longer-term trend.* Our World in Data estimates that there are 4.49 billion vaccinated individuals worldwide (1+ dose; 57.1% of the global population) and 3.77 billion who are fully vaccinated (47.9% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
On December 16, the US officially surpassed 800,000 cumulative COVID-19 deaths. The US CDC is currently reporting 51.3 million cumulative cases and 807,397 deaths. The US reported 288,381 new cases on December 20 and 204,913 on December 21, surpassing 200,000 new cases in a single day for the first time since January 18. The December 20 total is the second-highest single-day total since the onset of the pandemic. These 2 reports caused the average daily incidence to jump from 135,911 new cases per day to 161,261, a 19% increase in only 2 days. The current average is the highest since September 5 and only 1.8% below the United States’ second-highest peak in September 2021 (164,241). Daily incidence has increased by a factor of 2.5 since the most recent low on October 24 (64,162), and the trend appears to be accelerating. The sharp increase at the national level is a result of similar trends across states in multiple regions of the country. Analysis by The New York Times indicates that the daily incidence has more than doubled in 7 states—plus Puerto Rico (+1,302%) and Washington, DC (+541%)—over the past 2 weeks, including Florida (+509%) and Hawai’i (+670%) that have increased by a factor of 5 or greater.*
Daily mortality continues to increase steadily, up to 1,223 deaths per day, an increase of more than 20% since before the US Thanksgiving holiday weekend.*
Following a cybersecurity incident, Maryland suspended reporting for COVID-19 data. As of December 20, approximately 2 weeks after the incident, the state reported that 90% of its COVID-19 data have been restored. Maryland’s COVID-19 dashboard is once again available, and it has resumed reporting to the CDC.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Genomic sequencing data from the CDC show a rapid increase in the prevalence of the Omicron variant across the US. At the national level, the estimated prevalence increased from 0.1% the week of November 27 to 0.7% the week of December 4. In the 2 weeks since then, the prevalence surged to an estimated 73.2% nationwide, replacing Delta as the dominant variant.** Additionally, 8 of the 10 HHS regions are reporting Omicron prevalence greater than 50%, including 5 with greater than 90%: Regions 2 (New York/New Jersey), 4 (Southeast), 5 (Midwest), 6 (South), and 10 (Pacific Northwest).
**US CDC Nowcast projection.
US Vaccination
The US has administered 499 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations peaked on December 6, with 1.71 million doses administered per day. The trend has declined steadily since then, down to 1.36 million doses on December 17—a 20% decrease over that period.* A total of 241 million individuals have received at least 1 vaccine dose, equivalent to 72.8% of the entire US population. Among adults, 85.0% have received at least 1 dose, as well as 22.2 million children under the age of 18. A total of 204.8 million individuals are fully vaccinated**, which corresponds to 61.7% of the total population. Approximately 72.7% of adults are fully vaccinated, as well as 17.2 million children under the age of 18. Since August 13, 63.2 million fully vaccinated individuals have received an additional or booster dose, including 55.8% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
US OMICRON PREDICTIONS & PLAN Analysis from the University of Washington predicts that a new surge in COVID-19 incidence driven by the Omicron variant could produce nearly 3 million new cases per day in the US during the peak. Similarly, retired US NIH Director Dr. Francis Collins warned that the US could see as many as 1 million new cases per day as Omicron spreads. Some evidence suggests that daily incidence could peak quickly, possibly within the next 4-5 weeks, and that Omicron infections are associated with a lower risk of hospitalization and severe disease when compared to Delta. However, experts warn it is impossible to predict how individual countries’ populations and healthcare systems will be impacted by surges in Omicron cases. Individuals who are unvaccinated and have never been exposed to SARS-CoV-2 may still be at risk of severe disease. A large increase in COVID-19 cases also still runs the risk of overwhelming healthcare systems in the US and abroad.
On December 21, US President Joe Biden gave a speech on his administration’s plans to respond to Omicron. The plan includes procuring 500 million rapid tests for free shipment to US residents, beginning in January. This represents a pivot for the administration, which recently said people would have to seek reimbursement from their healthcare insurance plans for tests purchased on their own. Experts said the new policy is a step in the right direction but noted that countries such as the UK and Germany have been distributing billions of test kits and recommending citizens check their status twice a week. The US would need to ship 2.3 billion tests monthly to hit this same benchmark. Biden also announced plans to deploy more federal aid to hospitals and testing sites, including military personnel, ventilators from the national stockpile, and more ambulances and teams of paramedics to aid in transporting patients. President Biden called on unvaccinated individuals to fulfill their “patriotic duty” and seek out the shots, encouraged fully vaccinated individuals who are eligible to get a booster, and said those who are vaccinated should go ahead with holiday celebrations with friends and family. Meanwhile, WHO Director-General Dr. Tedros Adhanom Ghebreyesus encouraged people worldwide to cancel their holiday plans, saying, “An event canceled is better than a life canceled.”
US AUTHORIZES ORAL ANTIVIRALS The US FDA this week authorized the use of 2 oral, at-home antiviral therapies for COVID-19, a significant step in treatment of the disease that comes as the number of new cases begins to surge in the US, driven primarily by the Omicron variant of concern (VOC). The agency today authorized the use of the oral antiviral molnupiravir, developed by Merck and Ridgeback Biotherapeutics, for COVID-19 patients aged 18 years and older who have a positive SARS-CoV-2 viral test result, are within 5 days of symptom onset, are at high risk of severe disease or hospitalization, and who cannot access or do not qualify for alternative authorized COVID-19 treatments. Molnupiravir reduced the risk of hospitalization among high-risk patients by 30%, according to clinical trail data, but some experts are concerned over the potential for side effects and the development of drug resistance. The drug is not recommended for use during pregnancy, and men and women of childbearing age are recommended to use birth control, with men suggested to continue using it for 3 months post-administration. Molnupiravir—administered as capsules taken twice a day for 5 days—works by causing errors in the virus’s genetic code, disabling its reproduction capacity but also raising concerns that it could cause mutations in people who take it or lead to new variants.
On December 22, the FDA authorized the first oral antiviral to treat COVID-19 patients. The emergency use authorization (EUA) is for Pfizer’s Paxlovid—a new antiviral called nirmatrelvir co-packaged with the older antiviral ritonavir—that is taken as tablets twice a day for 5 days. Paxlovid is indicated to treat mild-to-moderate COVID-19 in individuals ages 12 and older weighing at least 40 kg (about 88 pounds) who have a positive SARS-CoV-2 test result and are at high risk of progression to severe disease. Administration of the pills, which are available by prescription only, should be started within 5 days of symptom onset and could be available to patients as early as this weekend, although initial supplies will be limited due to manufacturing constraints. Pfizer’s clinical trial results (not yet peer-reviewed) showed Paxlovid reduced the overall risk of hospitalization by 88% if started within 5 days of symptom onset, and the company’s laboratory studies show the pills should be effective against Omicron.
The authorizations come as healthcare providers face the realization that 2 of the 3 authorized monoclonal antibody treatments—previously shown to be highly effective at keeping high-risk patients out of the hospital—are not working against Omicron. The European Medicines Agency (EMA) has made recommendations for both Paxlovid and molnupiravir (known as Lagevrio outside of the US) for use in certain COVID-19 patients, paving the way for authorization in Europe.
CONVALESCENT PLASMA The results of a clinical trial evaluating antibody-rich plasma as an outpatient treatment for people with symptomatic COVID-19 was posted as a preprint to medRxiv on December 21, reopening debate over the use of convalescent plasma therapy. The study, conducted in the US and led by researchers from Johns Hopkins Medicine and the Johns Hopkins Bloomberg School of Public Health, showed outpatient treatment with convalescent plasma, when given within 8 days of symptom onset, reduced the risk of hospitalization by 54% compared with the placebo-control group. The trial primarily used plasma collected before vaccines were widely available and ended prior to the arrival of the Omicron SARS-CoV-2 variant in the US. However, the authors of the study believe that antibody-rich plasma could be an effective treatment against Omicron and other variants if taken from patients who are fully vaccinated and recovered from a breakthrough case of COVID-19. Individuals who fall into this category are believed to have higher levels of neutralizing antibodies than either individuals who are only vaccinated or only recovered from previous infection.
The study’s data come only a few weeks after the WHO recommended against the use of convalescent plasma to treat COVID-19. The WHO recommendation was made using information from 16 clinical trials with more than 16,000 participants that indicated convalescent plasma does not improve chances of survival or reduce the risk of needing mechanical ventilation. In the US, convalescent plasma is available under a US FDA emergency use authorization (EUA) to treat hospitalized COVID-19 patients early in the course of disease. The authors of the current study hope their results will prompt the WHO and FDA to revisit their guidance, especially because most of the currently authorized monoclonal antibody treatments might prove useless against Omicron and convalescent plasma is relatively easy to produce in low- and middle-income countries.
VACCINE INEQUITY In 2022, the international community must focus on global vaccine equity in order to end the COVID-19 pandemic. This past year saw vaccination goals fall far short, particularly in low- and middle-income countries (LMICs), in what has been called a “year of vaccine inequity” and a “failure for humanity.” Public health experts warn that the rapid spread of the Omicron variant could cause further setbacks in efforts to end vaccine inequity, leaving large populations unvaccinated and providing circumstances in which SARS-CoV-2 could continue to mutate. Additionally, the effects of these inequities will be felt for decades: 8 out of 10 people pushed into poverty during the pandemic are estimated to live in the poorest nations, and socioeconomic inequalities—such as access to schools and healthcare—will worsen for women and girls. Access to vaccine supplies, capacity to deliver the shots, and vaccine hesitancy all must be addressed in order to improve global vaccination rates. The world has the tools necessary to end the pandemic in 2022, but unless those tools are implemented effectively, including vaccinating the world’s population, the next year will not see the end of the current pandemic and we will remain unprepared for the next pandemic.
WHO Director-General Dr. Tedros Adhanom Ghebreyesus this week warned that widespread vaccine booster programs could prolong the pandemic, increase inequity, and provide a false sense of security in the face of Omicron. The WHO issued an update to its interim guidance on boosters, saying nations considering booster vaccination policies should consider their strategic and programmatic priorities; data on the performance of booster doses; how targeted booster dose administration could prevent healthcare system strain; and importantly, how booster programs impact globally limited vaccine supplies. Notably, Israel this week became the first country to begin rolling out a fourth dose of SARS-CoV-2 vaccine to certain populations, including adults ages 60 and older, medical workers, and people with compromised immune systems. Other nations might be considering similar policies on boosters. In the US, a group of more than 80 Democratic lawmakers has requested at least US$17 billion be included in the fiscal year 2022 appropriations omnibus to support global vaccination, testing, and treatment of COVID-19. In a US House of Representatives select subcommittee hearing on December 14, experts warned that continued inequity in vaccine access will continue to threaten the global population, including in the US, and prolong social and economic recovery.
US LIFE EXPECTANCY Life expectancy for the US population in 2020 dropped 1.8 years over 2019—down to 77 years in 2020 from 78.8 years in 2019—the largest single-year reduction in more than 75 years, according to new data from the US CDC’s National Center for Health Statistics (NCHS). The top 10 causes of death in 2020 were heart disease, cancer, COVID-19, unintentional injuries (including drug overdose), stroke, chronic lower respiratory diseases, Alzheimer’s disease, diabetes, influenza and pneumonia, and kidney disease. The drop in life expectancy was driven by increases in mortality due to COVID-19, unintentional injuries, heart disease, homicide, and diabetes. Of the 10 leading causes of death in 2020—which accounted for 74.1% of all deaths in the US in 2020—9 remained the same as in 2019, although 5 causes switched rank. Heart disease and cancer remained the top 2 leading causes. COVID-19 debuted in the ranking list in 2020, becoming the third leading cause of death and pushing suicide off the list. This is the first time a novel disease has entered the top 10 causes of death so quickly, and many feel much of the elevated death rate in 2020 is attributable directly or indirectly to COVID-19, as people might have had underlying conditions worsened by COVID-19, had limited access to health care, or feared accessing emergency or maintenance care.
In total, more than half a million more US resident deaths were recorded in 2020 than in 2019, and COVID-19 was the underlying cause of death for 350,831 people, representing 10.4% of the total number of deaths in 2020. The decrease in life expectancy was larger for men—2.1 years, from 76.3 years in 2019 to 74.2 years in 2020—than for women—1.5 years, from 81.4 in 2019 to 79.9 in 2020. Notably, age-adjusted death rate increases from 2019 to 2020 were highest among racial and ethnic minorities, reflecting an increased risk of death from COVID-19. The greatest increases in death rate were seen among Hispanic males (42.7%), Hispanic females (32.4%), non-Hispanic Black males (28.0%), and non-Hispanic Black females (24.9%), compared with non-Hispanic White males (13.4%) and non-Hispanic White females (12.1%). Death rates for non-Hispanic Black males were highest in 2020—1,399 deaths per 100,000 people—and lowest among Hispanic females—570 per 100,000. On a positive note, the infant mortality rate (IMR) decreased 2.9% from 558.3 infant deaths per 100,000 live births in 2019 to reach a record low of 541.9 in 2020.
US SPORTS As daily COVID-19 incidence and the prevalence of the Omicron variant surge in the US, professional and collegiate sports have been forced to rapidly adapt their COVID-19 protocols and mitigation plans.
National Hockey League: The NHL postponed a number of games already this season due to COVID-19 outbreaks on affected teams. But this week, the league suspended all games and team activities through Saturday, December 25, starting the scheduled Christmas break 2 days early. Including the games during this period, the NHL has postponed 50 games since the season began on October 12. Notably, more than 15% of all NHL players are currently under the league’s COVID-19 protocols. The NHL and the NHL Players Association also announced that NHL players will not be participating in the 2022 Winter Olympic Games in Beijing, China, due to the disruptions to the NHL schedule. The NHL is expected to reschedule postponed games during that period.
National Football League: At the start of the season, the NFL (American football) announced that it would not reschedule games due to COVID-19, but last week, it reversed its position due to more than 150 players and coaching staff testing positive across multiple teams. The league rescheduled 3 games last week, moving an extra game to Monday and 2 games to Tuesday. In response to increasing positive tests, the NFL updated its COVID-19 protocols in an effort to allow players to return sooner after a positive test. Following a number of asymptomatic or mild cases among NFL players, including those infected with the Omicron variant, the NFL shifted from weekly testing for vaccinated players to “a random cadence” or if a player develops symptoms. Less frequent testing will allow more players to be available, but it will likely miss some asymptomatic infections, including individuals who could be infectious. Additionally, vaccinated, asymptomatic players may be able to return to practice and games sooner under the new protocol.
National Basketball Association: While the NHL and NFL are updating their COVID-19 protocols and adjusting the league schedule, the NBA reportedly intends to continue with its season. While some NBA games have been postponed, NBA Commissioner Adam Silver indicated that there are no plans to suspend the season. Additionally, the NBA currently does not have any plans to update its COVID-19 protocols to allow players to return sooner after a positive test. The NBA suspended 7 games over the past week alone, and more than 90 players are under the league’s COVID-19 protocols. Commissioner Silver commented that approximately 90% of new cases are a result of the Omicron variant.
College Football: As the NCAA looks ahead to the College Football Playoff (CFP), it announced that the National Championship could be decided by forfeit if teams are unable to compete due to COVID-19. If teams are unable to play in the CFP semifinals, there is no opportunity to reschedule the game. That team would be forced to forfeit, and their opponent would move on to the championship game, and if neither team is able to play, the winner of the other semifinal game would automatically be declared the National Champion. If teams in the championship game are unable to play, that game could be moved from January 10 to as late as January 14. If the game cannot be held by then, a team that cannot play would forfeit and its opponent would be declared the National Champion. If neither team can play, then the National Championship will be vacated for this season. In preparation for the CFP, several of the competing teams have implemented additional protective measures to reduce the risk of COVID-19 impacting the coaches and players. The University of Alabama has reportedly reinstated its original COVID-19 protocols, including mask use and physical distancing at team facilities. Similarly, the University of Michigan restored masking and physical distancing as well as grab-and-go meals, and the players reportedly received booster doses of the SARS-CoV-2 vaccine as a team on December 22.
ti-amie wrote: ↑Thu Dec 23, 2021 6:53 pm
I see a lot of young black and brown people maskless - the FB, TikTok and WhatsApp people. I wonder what disinformation they were targeted with?
That's pretty rare here in the last two months or so. But very common throughout the summer. And I can't stress this enough, they are never without a mask when there is a real adult with them, which is always real interesting. Like exactly how much does your family know you are putting them at risk with how you're acting when it's just you and your friends? Not much at all is my guess. I know multiple people who have been hospitalized and one who died now because of the recklessness of their younger family members that was unknown to them at the time.
by ti-amie Just in time for the Christian Holidays. I'm not going to panic until dry posts his update.
P1 via @DrEricDing
ADJUSTED SEVERITY of Omicron vs Delta—Need to discuss *intrinsic severity* versus *observed severity* of #Omicron, which reinfects & evasive against 2-vaccine shots. New study found that after adjusting for factors, Omicron is only slightly intrinsically milder—2%-12% (red)
2) Let’s look at this way… the raw crude rates of Omicron vs Delta doesn’t reflect that Delta isn’t as evasive against vaccines— Omicron **looks** milder because breakthrough (and reinfected) people have higher protection from severe disease. But raw numbers don’t adjust that!
3) from earlier study we see that #Omicron is highly evasive against past immunity from surviving Alpha, Beta, or Delta variant. Little to no neutralization of Omicron among convalescent blood of those people. But they are milder—but this hides the true severity in raw rates. https://pbs.twimg.com/media/FHTNullXoAMdQft.jpg[img][/img]
4) KEY REMINDER— “milder” won’t save us, even if it’s 50% milder — because the exponentially fast doubling time of #Omicron can easily swamp out a 50% lower severity by doubling the case count! And doubling in 2 days!! https://twitter.com/DrEricDing?ref_src= ... 66515.html
5) My top explanation above is the SIMPLIFIED lay explanation of the Omicron vs Delta severity issue. I recommend people reading this detailed deep dive into the data by @dgurdasani1 — she shares more details if you are curious. Follow her for deeper version insights. https://twitter.com/dgurdasani1?ref_src ... 66515.html
Due to url limit there will be additional pages
by ti-amie P2
6) Also really key… though 3 dose effectiveness against severe disease is good, against infection not so good (and 2 dose poor)—we don’t know what it means for all the countless “mild” #Omicron COVID that we see on impacting actual #LongCovid! Mild infection still ==>Long COVID! https://twitter.com/dgurdasani1?ref_src ... 66515.html
7) and there will be BILLIONS of cases of new #Omicron infection in the coming 3 months according to @IHME_UW models. Billions with a B. That is not a typo. The “it’s mild” folks conveniently ignore the bigger picture. https://twitter.com/DrEricDing?ref_src= ... 66515.html
8) here is a good visual way to see how somehow can merely **look** milder but actually have the same “severe” effects. By enlarging the denominator of the “infected”, the same severe box below is a smaller % of the whole that you detect as cases. https://twitter.com/nataliexdean?ref_sr ... 66515.html
9) So how does #Omicron add so many cases so that it looks overall milder in the raw %? Well it is highly evasive (for mere infection) against 2 shots of vaccine and evasive against past convalescent immunity— look how they all have little to no neutralization against Omicon https://twitter.com/DrEricDing?ref_src= ... 66515.html
by ti-amie P3
10) But those with break thoughts and reinfections are definitely milder - the same UK study (top of ) showed 50-70% lower severity among those with a reinfection. This is good. But this also “waters down” the observed severity to artificially *look milder*. Hope it’s clear?
12) overall, reinfection is NOT a good thing, even if milder than if never had infection before. Reinfection can lead to #LongCovid too. And #Omicron is king of inducing reinfections while Delta not so much. https://twitter.com/WesElyMD?ref_src=tw ... 66515.html
13) What irks me about the “it’s mild” minimizers out there is that when shown data how hospitalizations are surging in UK, Denmark, or NYC—they just shrug it off with some dismissive remark that “oh they are old / got comorbidities anyway” — AS IF THOSE PEOPLE DO NOT MATTER! https://twitter.com/DrEricDing?ref_src= ... 66515.html
14) Reinfections absolutely soaring in UK—nearly all #Omicron. Let this be a lesson for those who tout “natural immunity” or their past infection as if it’s enough. It’s not. https://twitter.com/chrischirp?ref_src= ... 66515.html
by ti-amie
by atlpam
Suliso wrote: ↑Mon Dec 20, 2021 2:36 pm
No, actually not heard of that place... Our approximate route was Saguaro NP, Chiricahua NM, White Sands NP, Carlsbad Caverns NP, Guadelupe mountains NP, Big Bend NP. The first two are in Arizona, the second two in NM and the last two in Texas. Except for flying in and out we avoided cities. They are not much to write home about in these parts anyway.
Bandelier is north of Santa Fe. Sounds like you were hitting the parks farther south.
I’m planning to hit a lot of National Parks the next few years after I retire.
by Suliso
atlpam wrote: ↑Thu Dec 23, 2021 9:00 pm
Bandelier is north of Santa Fe. Sounds like you were hitting the parks farther south.
I’m planning to hit a lot of National Parks the next few years after I retire.
Indeed, we tried to maximize our chances of good weather.
I assume by 'criminalizing', this means a more severe penalty. Because fraud has been illegal for a long time.
It's good that people will actually be punished with more than a slap on the wrist now. It's also long overdue.
by ti-amie
And it may be worse than this because they've been cooking the books for a while now.
by JazzNU
ti-amie wrote: ↑Fri Dec 24, 2021 8:15 pm
And it may be worse than this because they've been cooking the books for a while now.
Yeah. The only reason there's any idea of the daily numbers is because the CDC is trying to keep a daily count to track increases and decreases. Florida reports their skewed numbers once a week, that's it. It's beyond pitiful.
by ponchi101 My mom crossed messages today with a friend in Florida, who is very worried because HER ENTIRE family is locked down with Covid.
I just did not have the time or care enough to ask about vaccination.
by JazzNU
ponchi101 wrote: ↑Fri Dec 24, 2021 10:03 pm
My mom crossed messages today with a friend in Florida, who is very worried because HER ENTIRE family is locked down with Covid.
I just did not have the time or care enough to ask about vaccination.
That is rough. Hopefully they'll all be okay. And hope they were vaccinated, or at least those that are older or have pre-existing conditions.
by mmmm8
ponchi101 wrote: ↑Fri Dec 24, 2021 10:03 pm
My mom crossed messages today with a friend in Florida, who is very worried because HER ENTIRE family is locked down with Covid.
I just did not have the time or care enough to ask about vaccination.
The outdoor sitdown and safe event we were supposed to go to for New Year's got canceled, a surprisingly safe move for Miami. Of course, now we are going to be inside an apartment which seems less safe (everyone is vaccinated)
by Suliso If I were in Miami I'd just go to a beach at midnight. Would be exotic for me...
by ponchi101 You would not be alone. Lot's of people do that, with drinks. Not a bad idea to go to the beach at midnight with a nice bottle of wine, way after hours.
But you are right, in that it would be less crowded.
by dryrunguy
ponchi101 wrote: ↑Mon Dec 27, 2021 6:08 pm
You would not be alone. Lot's of people do that, with drinks.
Indeed. I saw that movie. It's called Jaws.
by ti-amie
by ti-amie ...and Track and Trace is still running...
by ti-amie Will travel warnings have to be issued?
by ti-amie
Red: Counties where the death rate increased since adult vaccine eligibility
Blue/Green Counties where the death rate decreased since adult vaccine eligibility
This was funny, but I've clearly watched too much horse racing in my life. That call, especially the first half, felt like amateur hour, I definitely expect better out of real horse racing announcers.
by dryrunguy COVID is hitting where I live. The elderly lady next door with fairly advanced dementia was transported to the hospital yesterday afternoon. She tested positive.
Her daughter also has it. The daughter and her husband live nearby. No word yet on our neighbor's husband. He's not mentally well, either. But he's in better mental shape than his wife. At least for now.
It's just so depressing.
by JazzNU
dryrunguy wrote: ↑Wed Dec 29, 2021 12:22 am
COVID is hitting where I live. The elderly lady next door with fairly advanced dementia was transported to the hospital yesterday afternoon. She tested positive.
Her daughter also has it. The daughter and her husband live nearby. No word yet on our neighbor's husband. He's not mentally well, either. But he's in better mental shape than his wife. At least for now.
It's just so depressing.
With that many underlying issues, I hope they are all vaccinated. But I know that's hoping for a lot in your area.
by ponchi101 My GF got her booster today. No Pfizer/BN available so they gave her Moderna. "Only" three hours on line (compared to my 5, an improvement).
Sole side effect: her arm is dead. I mean dead as in "can't lift it from the side". But a minor issue, and better to get this done here.
by JazzNU
ponchi101 wrote: ↑Wed Dec 29, 2021 3:43 am
My GF got her booster today. No Pfizer/BN available so they gave her Moderna. "Only" three hours on line (compared to my 5, an improvement).
Sole side effect: her arm is dead. I mean dead as in "can't lift it from the side". But a minor issue, and better to get this done here.
FYI, Moderna tested the highest in booster responses among people that got the first series with Pfizer in the testing they did here when deciding on emergency approvals. So that's a good one to get with plenty advising it as the first option to choose.
by ponchi101 It is also one issue down here. They seem to have mixed info. As you say, the literature I have read (including here) says that mixing a Moderna shot with your Pf/BT is a good choice, but when I went to get mine they stuck with a 3rd Pf/BN. Yesterday they ran out of Pf/BN so they gave her a Moderna, which is good, but they seem to not have a totally set up protocol.
On the bad side: my niece came down with Covid. She is vaccinated but got her booster on Dec 23rd, so maybe it did not have time to kick in. Mild symptoms but she is the one in the family that I worry about, as she has high blood pressure and a few extra pounds that should not be there, plus asthma. But again, just some mild symptoms so far. From my limited sampling, the vaccines are working for my family.
by ti-amie
by JazzNU
ponchi101 wrote: ↑Wed Dec 29, 2021 5:07 pm
It is also one issue down here. They seem to have mixed info. As you say, the literature I have read (including here) says that mixing a Moderna shot with your Pf/BT is a good choice, but when I went to get mine they stuck with a 3rd Pf/BN. Yesterday they ran out of Pf/BN so they gave her a Moderna, which is good, but they seem to not have a totally set up protocol.
On the bad side: my niece came down with Covid. She is vaccinated but got her booster on Dec 23rd, so maybe it did not have time to kick in. Mild symptoms but she is the one in the family that I worry about, as she has high blood pressure and a few extra pounds that should not be there, plus asthma. But again, just some mild symptoms so far. From my limited sampling, the vaccines are working for my family.
I hope your niece is okay. And the original vaccine without the booster is very likely to be enough to bolster her immunity against severe illness. Is she in Venezuela or in the US? If it's early in testing positive and she's here, she can likely go to get the monoclonal antibody treatment if she's concerned about her outcome and has one of the high risk conditions associated with severe illness. Something to keep in mind if she's here, but needs to be done early on.
I hope your niece is okay. And the original vaccine without the booster is very likely to be enough to bolster her immunity against severe illness. Is she in Venezuela or in the US? If it's early in testing positive and she's here, she can likely go to get the monoclonal antibody treatment if she's concerned about her outcome and has one of the high risk conditions associated with severe illness. Something to keep in mind if she's here, but needs to be done early on.
She is my niece in Georgia. She is doing well, I spoke with her a bit earlier. Feeling as if it was a terrible cold, but so far, nothing serious. So I gather it will be a few days of delivery apps for food, and not much more.
She was mostly worried about her kid, my severely premature-born grand niece, but she is doing fine too. As I say, as far as this family is concerned, vaccines work.
by Owendonovan I tested positive on 12/16, a sore throat was my indicator. I tested negative on 12/23. It wasn't more than the sore throat for a couple days, so I feel lucky to have gotten vaccinated and boosted the first days they became available to me. I take 3 subway lines to my job teaching, it was just a matter of time for me.
by JazzNU
Owendonovan wrote: ↑Thu Dec 30, 2021 1:36 am
I tested positive on 12/16, a sore throat was my indicator. I tested negative on 12/23. It wasn't more than the sore throat for a couple days, so I feel lucky to have gotten vaccinated and boosted the first days they became available to me. I take 3 subway lines to my job teaching, it was just a matter of time for me.
Happy to hear that you are okay and only had mild symptoms.
by ti-amie I'm so glad to hear that you're okay Owen. Vaccines work.
by Deuce
Owendonovan wrote: ↑Thu Dec 30, 2021 1:36 am
I tested positive on 12/16, a sore throat was my indicator. I tested negative on 12/23. It wasn't more than the sore throat for a couple days, so I feel lucky to have gotten vaccinated and boosted the first days they became available to me. I take 3 subway lines to my job teaching, it was just a matter of time for me.
Are all subway passengers supposed to be masked there?
Owendonovan wrote: ↑Thu Dec 30, 2021 1:36 am
I tested positive on 12/16, a sore throat was my indicator. I tested negative on 12/23. It wasn't more than the sore throat for a couple days, so I feel lucky to have gotten vaccinated and boosted the first days they became available to me. I take 3 subway lines to my job teaching, it was just a matter of time for me.
Are all subway passengers supposed to be masked there?
Yes, there's a $50 fine for not wearing a mask, but when the police are wandering around the subways maskless.....
Owendonovan wrote: ↑Thu Dec 30, 2021 1:36 am
I tested positive on 12/16, a sore throat was my indicator. I tested negative on 12/23. It wasn't more than the sore throat for a couple days, so I feel lucky to have gotten vaccinated and boosted the first days they became available to me. I take 3 subway lines to my job teaching, it was just a matter of time for me.
Are all subway passengers supposed to be masked there?
Yes, there's a $50 fine for not wearing a mask, but when the police are wandering around the subways maskless.....
Thanks.
Should be a $500 fine. Minimum.
As for the police... now is a really good time for them to stop being 'above the law'.
by Deuce Here I am again posting something which really defies description.
I hope no-one else has posted this yet, as I'm not sure you all can handle another round of this...
"At the San Diego County Board of Supervisors meeting... The board was contemplating whether to support a local health-emergency order extension and the woman, among other local residents, addressed her thoughts when invited to speak."
Try to watch all of it.
I know, I know... but please try to.
by Suliso Masks are very useful, but they're not going to protect you forever if you regularly take public transport in ultra high spread environment. That's just how it is...
by ponchi101 Natural immunity. Wonder where that misconception came from?
Nah, I do know. I have friends from that side of the asylum.
by dryrunguy I had a bizarre conversation with my brother the other day (the brother I like). He is traveling to Ohio to bring in the New Year with my mother, my oldest brother, and my oldest brother's children + spouses and grandson (4 months old). Everyone is fully vaccinated (whatever THAT means these days) except for the infant. They have discussed whether everyone should wear masks, especially with a new infant around, and I guess they landed on "do whatever your conscience dictates". I am not aware of any protocols or guidance regarding what people should do around an infant, so I assume the best thing to do is to exercise an abundance of caution. That said, masks will be optional, I guess.
Toward the end of the conversation, I remember saying, "Even just 2 years ago, these types of conversations would have been unimaginable." But I'm glad they at least talked about it.
Obviously, I'm not going. That's not so much because I'm worried about being around them. It's more an issue of having very limited control over who we would potentially come in contact with between here and there.
by mmmm8
Suliso wrote: ↑Mon Dec 27, 2021 5:10 pm
If I were in Miami I'd just go to a beach at midnight. Would be exotic for me...
So, in the rich area where we are (which is Key BIscayne, an island, so not as easy to get elsewhere), all the beaches are either part of national parks (closed at night) or private. The place where the party got canceled was actually a beach club, so it would have been on the beach. We are now at a restaurant outside, so still safe and exotically warm for me.
Incidentally, yesterday I went to Crandon Park, the site of the former Sony Ericsson Open here on the island, and it's still pretty much intact and semi-abandoned. What I would do if I were with fellow tennis fans is sneak onto the court at midnight and celebrate there, would've been fun + great views of the city.
by MJ2004 Welp.. the in-laws both tested positive a couple of days after they went to a family member's house for Christmas Eve (lots of kids present and almost everyone in attendance has tested positive). I'm not aware of anyone getting tested before the gathering, just afterwards once symptoms appeared. Sigh...
My mother-in-law has cold symptoms and my father-in-law is asymptomatic. She has Parkinson's, so we're hoping she recovers quickly.
At the current rate of around 290,000 cases daily, about 1% of the U.S. population will have gotten it in a ten day span.
by JazzNU
dryrunguy wrote: ↑Thu Dec 30, 2021 4:29 pm
I had a bizarre conversation with my brother the other day (the brother I like). He is traveling to Ohio to bring in the New Year with my mother, my oldest brother, and my oldest brother's children + spouses and grandson (4 months old). Everyone is fully vaccinated (whatever THAT means these days) except for the infant. They have discussed whether everyone should wear masks, especially with a new infant around, and I guess they landed on "do whatever your conscience dictates". I am not aware of any protocols or guidance regarding what people should do around an infant, so I assume the best thing to do is to exercise an abundance of caution. That said, masks will be optional, I guess.
Toward the end of the conversation, I remember saying, "Even just 2 years ago, these types of conversations would have been unimaginable." But I'm glad they at least talked about it.
Obviously, I'm not going. That's not so much because I'm worried about being around them. It's more an issue of having very limited control over who we would potentially come in contact with between here and there.
I would say that's a pretty normal conversation these days @dry, minus the "whatever your conscience dictates."
The only thing different about your conversation and the one I had recently is that we all agreed to get tested the week prior to getting together for Christmas as well. And that's what many have clearly agreed to hence the sudden crazy demand for testing.
by JazzNU
MJ2004 wrote: ↑Thu Dec 30, 2021 7:13 pm
Welp.. the in-laws both tested positive a couple of days after they went to a family member's house for Christmas Eve (lots of kids present and almost everyone in attendance has tested positive). My mother-in-law has cold symptoms and my father-in-law is asymptomatic.
At the current rate of 280,000 cases daily, about 1% of the U.S. population will have gotten it in a ten day span.
Hope your in-laws and the rest of the family are okay. Mild symptoms and asymptomatic are encouraging signs.
by ti-amie
Deuce wrote: ↑Thu Dec 30, 2021 6:07 am
Here I am again posting something which really defies description.
I hope no-one else has posted this yet, as I'm not sure you all can handle another round of this...
"At the San Diego County Board of Supervisors meeting... The board was contemplating whether to support a local health-emergency order extension and the woman, among other local residents, addressed her thoughts when invited to speak."
Try to watch all of it.
I know, I know... but please try to.
I made it 29 seconds.
by Suliso
JazzNU wrote: ↑Thu Dec 30, 2021 7:13 pm
The only thing different about your conversation and the one I had recently is that we all agreed to get tested the week prior to getting together for Christmas as well. And that's what many have clearly agreed to hence the sudden crazy demand for testing.
I'd say the best is a self test few hours before going. A test a week prior, no matter how accurate, seems pretty meaningless to me...
We went on a vacation instead of traveling to see family this year, but that was decided before Omicron appeared. Next year we're going for sure covid or no covid.
dryrunguy wrote: ↑Thu Dec 30, 2021 4:29 pm
I had a bizarre conversation with my brother the other day (the brother I like). He is traveling to Ohio to bring in the New Year with my mother, my oldest brother, and my oldest brother's children + spouses and grandson (4 months old). Everyone is fully vaccinated (whatever THAT means these days) except for the infant. They have discussed whether everyone should wear masks, especially with a new infant around, and I guess they landed on "do whatever your conscience dictates". I am not aware of any protocols or guidance regarding what people should do around an infant, so I assume the best thing to do is to exercise an abundance of caution. That said, masks will be optional, I guess.
Toward the end of the conversation, I remember saying, "Even just 2 years ago, these types of conversations would have been unimaginable." But I'm glad they at least talked about it.
Obviously, I'm not going. That's not so much because I'm worried about being around them. It's more an issue of having very limited control over who we would potentially come in contact with between here and there.
I would say that's a pretty normal conversation these days @dry, minus the "whatever your conscience dictates."
The only thing different about your conversation and the one I had recently is that we all agreed to get tested the week prior to getting together for Christmas as well. And that's what many have clearly agreed to hence the sudden crazy demand for testing.
Yeah, the testing agreement is muddy though, isn't it? General consensus seems to be that the incubation period for Omicron is about 3 days. So someone could get tested a week before, be exposed a few days later, and still show up in an unknowingly infected, asymptomatic, and contagious condition.
That said, it's better than no testing at all, so I commend the intent behind it. I know my middle brother will be tested. He'll have to be to fly. But I don't know about anyone else.
And yes, I suppose it's a normal discussion. What's bizarre is that we have to have it.
by JazzNU
dryrunguy wrote: ↑Thu Dec 30, 2021 8:57 pm
Yeah, the testing agreement is muddy though, isn't it? General consensus seems to be that the incubation period for Omicron is about 3 days. So someone could get tested a week before, be exposed a few days later, and still show up in an unknowingly infected, asymptomatic, and contagious condition.
Not at all. You guys are taking the week part in a very strict manner. No one was tested on Dec. 18th. Christmas was on a Saturday. So everyone got tested the week prior, meaning the days leading into Christmas day. We didn't go as some family troupe to get tested, we live in different places. Some of us managed to get PCR tests and the rest did rapid tests, though neither was all that simple to get last week so we're lucky that we were all able to do so. No one was painting the town red from the time of their test to Christmas day, at best someone went grocery store to grab a forgotten item and was masked while in the store.
by dryrunguy
dryrunguy wrote: ↑Wed Dec 29, 2021 12:22 am
COVID is hitting where I live. The elderly lady next door with fairly advanced dementia was transported to the hospital yesterday afternoon. She tested positive.
Her daughter also has it. The daughter and her husband live nearby. No word yet on our neighbor's husband. He's not mentally well, either. But he's in better mental shape than his wife. At least for now.
It's just so depressing.
Just got word that our neighbor lady died this evening. I talked to her husband this afternoon. He is also sick, but he's at home, and Shirley's children are checking on him regularly.
dryrunguy wrote: ↑Wed Dec 29, 2021 12:22 am
COVID is hitting where I live. The elderly lady next door with fairly advanced dementia was transported to the hospital yesterday afternoon. She tested positive.
Her daughter also has it. The daughter and her husband live nearby. No word yet on our neighbor's husband. He's not mentally well, either. But he's in better mental shape than his wife. At least for now.
It's just so depressing.
Just got word that our neighbor lady died this evening. I talked to her husband this afternoon. He is also sick, but he's at home, and Shirley's children are checking on him regularly.
dryrunguy wrote: ↑Wed Dec 29, 2021 12:22 am
COVID is hitting where I live. The elderly lady next door with fairly advanced dementia was transported to the hospital yesterday afternoon. She tested positive.
Her daughter also has it. The daughter and her husband live nearby. No word yet on our neighbor's husband. He's not mentally well, either. But he's in better mental shape than his wife. At least for now.
It's just so depressing.
Just got word that our neighbor lady died this evening. I talked to her husband this afternoon. He is also sick, but he's at home, and Shirley's children are checking on him regularly.
Crushed. Just crushed.
I'm so sorry dry.
by dryrunguy Before the dementia got her, Shirley routinely delivered fresh-baked pies to us. They were wonderful. Strawberry rhubarb, apple.... Shirley was a highly skilled baker.
And such a sweet spirit.
But I am also relieved for her. No more moments of thinking her husband is a stranger. No more moments of thinking there is a stranger in her house and feeling like she needed to escape to us for protection.
We will focus our attention on Elmer, her husband. It's awkward now since he is sick with COVID, but we'll do what we can to take care of him, their dog, and their chickens.
You see a lot of couples in their late 70s/early 80s who are together because they have no other choice/don't want to be alone.
Elmer and Shirley were a love story to the end. You could see that clearly every time you saw them together.
by JazzNU
by dryrunguy About J&J, these things always seem to come out a week or two after I make a decision and take action. But when I got my booster, the best evidence at the time was that those of us who started out with a J&J vaccine would be best served by getting a Moderna booster. So that's what I did.
I wonder if J&J immunity will last longer against Omicron than it did against previous variants.
And of course, we know nothing about how any of the existing vaccines will hold up against future variants.
Owendonovan wrote: ↑Thu Dec 30, 2021 1:36 am
I tested positive on 12/16, a sore throat was my indicator. I tested negative on 12/23. It wasn't more than the sore throat for a couple days, so I feel lucky to have gotten vaccinated and boosted the first days they became available to me. I take 3 subway lines to my job teaching, it was just a matter of time for me.
Are all subway passengers supposed to be masked there?
Yes, there's a $50 fine for not wearing a mask, but when the police are wandering around the subways maskless.....
I've finally started seeing the police consistently in masks on the subway! Just the last couple of weeks.
by mmmm8
Suliso wrote: ↑Thu Dec 30, 2021 2:36 pm
Masks are very useful, but they're not going to protect you forever if you regularly take public transport in ultra high spread environment. That's just how it is...
If everyone's masked, it doesn't eliminate but does dramatically reduce the chances of transmission. The problem is that the people who are in general taking fewer precautions and are more likely to be infected are likely to be unmasked.
Suliso wrote: ↑Thu Dec 30, 2021 2:36 pm
Masks are very useful, but they're not going to protect you forever if you regularly take public transport in ultra high spread environment. That's just how it is...
If everyone's masked, it doesn't eliminate but does dramatically reduce the chances of transmission. The problem is that the people who are in general taking fewer precautions and are more likely to be infected are likely to be unmasked.
Certainly, but if you're taking say 0.1% risk of being infected every time you take a subway eventually statistics will catch up with you. Unless of course general infection levels reduce by at least an order of magnitude soon.
Suliso wrote: ↑Thu Dec 30, 2021 2:36 pm
Masks are very useful, but they're not going to protect you forever if you regularly take public transport in ultra high spread environment. That's just how it is...
If everyone's masked, it doesn't eliminate but does dramatically reduce the chances of transmission. The problem is that the people who are in general taking fewer precautions and are more likely to be infected are likely to be unmasked.
Certainly, but if you're taking say 0.1% risk of being infected every time you take a subway eventually statistics will catch up with you. Unless of course general infection levels reduce by at least an order of magnitude soon.
Quality of the mask is also relevant to the degree of risk. If others (and/or yourself) are wearing a flimsy 1 or 2 layer cloth mask, or an old surgical mask, or an ill-fitting mask, the risk of transmission in indoor, crowded, public places, where you are basically in one place for more than 5 minutes (such as a bus or subway) obviously increases over wearing a well fitting KN95 mask, for example.
But the risk is never zero.
Open the windows on the bus whenever the weather permits (and if the bus windows actually can be opened - some of the newer city buses have sealed windows, which was idiotic before the pandemic, and is now downright dangerous).
by Suliso Indeed it's never zero. I guessed that 0.1%, I'd not be shocked if it's actually 0.01% or 1% instead. Nobody really knows...
It's zero only if you go absolutely nowhere (not even grocery store), meet no one ever and live in a single building with no close neighbors. That's an impossible life though, even for a month let alone a year. Actually not only impossible practically, but also not worth living.
Deuce wrote: ↑Thu Dec 30, 2021 2:12 am
Are all subway passengers supposed to be masked there?
Yes, there's a $50 fine for not wearing a mask, but when the police are wandering around the subways maskless.....
I've finally started seeing the police consistently in masks on the subway! Just the last couple of weeks.
I've noticed different subway lines have different rates of mask wearing (L being best). It's a struggle to keep from popping off on the unmasked in the subway, but a 55 yo 5'7" 125lb man isn't all that intimidating.....
Yes, there's a $50 fine for not wearing a mask, but when the police are wandering around the subways maskless.....
I've finally started seeing the police consistently in masks on the subway! Just the last couple of weeks.
I've noticed different subway lines have different rates of mask wearing (L being best). It's a struggle to keep from popping off on the unmasked in the subway, but a 55 yo 5'7" 125lb man isn't all that intimidating.....
Just summon your inner Mick Belker. It worked for him in NYC...
by dryrunguy I don't understand this common "I refuse to ask for help" thing that happens in this part of the country.
Elmer, the neighbor who lost his wife to COVID, and has COVID himself, showed up today. Because he was hungry and had no food. His stepdaughter was supposed to bring food to him this morning. He looked awful (skinny and pale).
I offered to make him sausage and eggs.
While I was cooking, his stepdaughter and her husband showed up, with food, and berated him in my driveway for bothering us (according to dolphins). They drove him home.
Then I delivered the sausage and eggs to his house.
Shirley's funeral is on Wednesday. Obviously, we're not going.
Everything about this SUCKS big donkey *****.
Thanks for listening.
by ti-amie That rugged individualism now known as toxic masculinity was force fed to generations of men (and women). They in turn passed it on with devastating results.
He came to your house although he is positive. Make sure you test yourselves.
by ti-amie
by ponchi101
ti-amie wrote: ↑Mon Jan 03, 2022 1:42 am
That rugged individualism now known as toxic masculinity was force fed to generations of men (and women). They in turn passed it on with devastating results.
He came to your house although he is positive. Make sure you test yourselves.
Sorry, disagree. Not everything boils down to "toxic masculinity". When you are a person that has been able to support himself/herself all your life, being unable to do so is a belittling experience. When you are a productive person and then, one day, for reasons not related to your capacities or skills, you can no longer support yourself, it is a sobering blow to your self esteem.
I have friends that are going down that road at a rapid pace, because our industry is disappearing. And they are not only men.
(And I am surely on that road, even if I am at the toll booth).
ti-amie wrote: ↑Mon Jan 03, 2022 1:42 am
That rugged individualism now known as toxic masculinity was force fed to generations of men (and women). They in turn passed it on with devastating results.
He came to your house although he is positive. Make sure you test yourselves.
Sorry, disagree. Not everything boils down to "toxic masculinity". When you are a person that has been able to support himself/herself all your life, being unable to do so is a belittling experience. When you are a productive person and then, one day, for reasons not related to your capacities or skills, you can no longer support yourself, it is a sobering blow to your self esteem.
I have friends that are going down that road at a rapid pace, because our industry is disappearing. And they are not only men.
(And I am surely on that road, even if I am at the toll booth).
I think I used the wrong words. It's very hard for older people to ask for help. It is a very difficult adjustment from being a contributing member of society to someone who has a lot of time on their hands. I know that. But at the base of it is that idea of not needing anyone else, that we exist in a universe made up of ourselves. My internist told me one day that men are the worst as they age. I found that out the hard way.
I hope your friend isn't sliding into dementia.
by ponchi101 Oh, no. I did not mean that they were losing they capacities. That is the sad thing. My friend P, in Buenos Aires, is still one of the sharpest minds I can think of. My friend R, in Colorado, is also still a man that could be as productive as anybody else. All my friends that are spread around the world, and most of them are from S. America, are simply waiting for a job offer, for them to be able to work again. This for a group of people with 20 + years of experience in an industry, almost all of them bilingual, most with considerable academic credentials.
And, personally, it is not about not needing anyone else. It is not being a burden to others. It is not the same thing.
by ti-amie
ponchi101 wrote: ↑Mon Jan 03, 2022 3:00 am
Oh, no. I did not mean that they were losing they capacities. That is the sad thing. My friend P, in Buenos Aires, is still one of the sharpest minds I can think of. My friend R, in Colorado, is also still a man that could be as productive as anybody else. All my friends that are spread around the world, and most of them are from S. America, are simply waiting for a job offer, for them to be able to work again. This for a group of people with 20 + years of experience in an industry, almost all of them bilingual, most with considerable academic credentials.
And, personally, it is not about not needing anyone else. It is not being a burden to others. It is not the same thing.
Agree
by Suliso My boss at work has cought omicron. The first one among co-workers on our site I know off, but undoubtedly not the last.
by ponchi101 Will you have to quarantine? If you have been in contact with him?
by Suliso
ponchi101 wrote: ↑Mon Jan 03, 2022 9:42 pm
Will you have to quarantine? If you have been in contact with him?
He has not been at work since December 18th so no one on site affected. He got it somehow during the holiday season. I last talked with him in late November.
by Owendonovan 1st day back at school teaching after winter break where 1/5 of the students were absent from COVID infections or travel issues. 1/2 of my dept., athletics, is out sick and admin is telling us not to be too hard on the kids about wearing masks. None of the teachers or students I had contact (10+minutes < 6 feet) with, including the teacher I work in the same gym with all day, were contacted by the school as a contact for COVID after I let the school know I had COVID. I gave them a very detailed account of my time spent with everyone I would have considered a contact. At this point, I have no idea what the school considers a contact.
by Deuce
Owendonovan wrote: ↑Tue Jan 04, 2022 1:55 am
1st day back at school teaching after winter break where 1/5 of the students were absent from COVID infections or travel issues. 1/2 of my dept., athletics, is out sick and admin is telling us not to be too hard on the kids about wearing masks. None of the teachers or students I had contact (10+minutes < 6 feet) with, including the teacher I work in the same gym with all day, were contacted by the school as a contact for COVID after I let the school know I had COVID. I gave them a very detailed account of my time spent with everyone I would have considered a contact. At this point, I have no idea what the school considers a contact.
Probably only anyone who gets sick and tells them "I was near Owen."
Contact tracing is not all it's claimed to be. Not even close, really.
by ti-amie
by Owendonovan Of course they choose a picture during lunch where no children are wearing masks.
by ti-amie
by ti-amie
by Deuce I think pretty much all of us would agree that those who refuse to wear a mask in public indoor settings are either dumb or selfish - or both...
If a person doesn't wear a mask because he/she doesn't believe that COVID-19 is real, or doesn't believe it's serious, or doesn't believe it's transmissible - ok, the person is dumb/selfish.
Regardless of his beliefs regarding the virus, though, this guy had a very good reason to wear a mask. The fact that he didn't is mind boggling...
by JazzNU The number of positives in my orbit are increasing rapidly. Some more concerning than others. Please be careful when you're out, and seriously, if you haven't upgraded your mask in whatever way you can, be it the type or thru double masking, please give it serious consideration. Omicron is wily.
by ponchi101 If "The Jews" are bent in trying to kill everybody with the vaccine, it is working well as self-genocide, as Israel is one of the highest vaccinated countries.
By now, I can "understand" the hatred for "the Jews" (understand, not CONDONE or AGREE) in the sense that it is something that entire groups of people foster in their children. The hatred and meme is truly well planted in too many people's psyches, as sickening as it is.
But when what you say is plain stupid, man, you are the one that looks, well, stupid.
Owendonovan wrote: ↑Tue Jan 04, 2022 1:55 am
1st day back at school teaching after winter break where 1/5 of the students were absent from COVID infections or travel issues. 1/2 of my dept., athletics, is out sick and admin is telling us not to be too hard on the kids about wearing masks. None of the teachers or students I had contact (10+minutes < 6 feet) with, including the teacher I work in the same gym with all day, were contacted by the school as a contact for COVID after I let the school know I had COVID. I gave them a very detailed account of my time spent with everyone I would have considered a contact. At this point, I have no idea what the school considers a contact.
Probably only anyone who gets sick and tells them "I was near Owen."
Contact tracing is not all it's claimed to be. Not even close, really.
Depends on the place. I was a close contact with a colleague and got two emails and a voicemail from work (I had already known because she also let me know personally).
by mmmm8
ponchi101 wrote: ↑Wed Jan 05, 2022 9:14 pm
If "The Jews" are bent in trying to kill everybody with the vaccine, it is working well as self-genocide, as Israel is one of the highest vaccinated countries.
By now, I can "understand" the hatred for "the Jews" (understand, not CONDONE or AGREE) in the sense that it is something that entire groups of people foster in their children. The hatred and meme is truly well planted in too many people's psyches, as sickening as it is.
But when what you say is plain stupid, man, you are the one that looks, well, stupid.
As a Jew, just continue to be very ashamed that we've been so unsuccessful in our centuries-old quest for world domination via sky lasers, global genocide and general baby-killing.
As a Jew, just continue to be very ashamed that we've been so unsuccessful in our centuries-old quest for world domination via sky lasers, global genocide and general baby-killing.
ponchi101 wrote: ↑Wed Jan 05, 2022 9:14 pm
If "The Jews" are bent in trying to kill everybody with the vaccine, it is working well as self-genocide, as Israel is one of the highest vaccinated countries.
By now, I can "understand" the hatred for "the Jews" (understand, not CONDONE or AGREE) in the sense that it is something that entire groups of people foster in their children. The hatred and meme is truly well planted in too many people's psyches, as sickening as it is.
But when what you say is plain stupid, man, you are the one that looks, well, stupid.
As a Jew, just continue to be very ashamed that we've been so unsuccessful in our centuries-old quest for world domination via sky lasers, global genocide and general baby-killing.
You're just not among the elders in the know. Domination long achieved. :p
by dryrunguy After taking a break for the holidays, the Situation Report from Johns Hopkins is back. And of course, it's depressing.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 294 million cumulative cases and 5.45 million deaths worldwide as of January 5. Global weekly incidence increased substantially last week, up 72% over the previous week. This is the 11th consecutive week of increasing weekly incidence, setting a new record with 9.73 million new cases. The increase is largely due to surges in the Americas (+100%) and Europe (+66%), but all WHO regions reported increases last week. Notably, the WHO reported increases of 38.1% in the Western Pacific, 39.8% in the Eastern Mediterranean, and 77.6% in South-East Asia, but the magnitude of those surges are much smaller than those in the Americas and Europe. Global weekly mortality decreased for the fourth consecutive week, down 8.3% from the previous week. The weekly total of 41,990 deaths is the lowest since the week of October 19, 2020.
Several countries in Europe are setting new records in terms of per capita daily incidence. To our knowledge, the previous record per capita daily incidence was 3,385 daily cases per million population in Seychelles (May 2021). Over the past several days, Greece (3,418), Ireland (3,927), San Marino (4,364), Andorra (4,554), and Cyprus (4,855) all surpassed that record. A number of other countries in Europe, as well as the US, are exhibiting rapidly increasing trends and could surpass the previous record in the coming days or weeks.
Global Vaccination
The WHO reported 9.12 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of January 5. A total of 4.57 billion individuals have received at least 1 dose, and 3.86 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations increased from mid-October (21.3 million doses per day) through mid-December (39.9 million). Daily vaccinations have decreased since December 15, down from 40.6 million doses per day to 30.4 million. The trend has persisted since before the holiday season, but some of the decline could be due to vaccination clinics being closed during that time.* Our World in Data estimates that there are 4.63 billion vaccinated individuals worldwide (1+ dose; 58.8% of the global population) and 3.91 billion who are fully vaccinated (49.7% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 57.2 million cumulative cases of COVID-19 and 827,879 deaths. The US is averaging 554,328 new cases and 1,238 deaths per day.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Since December 27, 2021, the US has continually set new records for both single-day incidence and average daily incidence. Notably, the US exceeded 300k, 400k, 500k, 600k, 700k, 800k, and 900k new cases reported in a single day for the first time since the onset of the pandemic. The United States’ average daily incidence also exceeded 300k, 400k, and 500k new cases per day for the first time. We expect that part of these massive reports are a result of delays in reporting over the Christmas and New Year’s holiday weekends; however, even reports from the holidays themselves, both of which fell on weekends, were considerably higher than the weekends leading up to the holiday season. The US reported more than 100,000 new cases on Christmas Day and another 200,000 on Sunday, December 26, which is more than 75% higher than the previous weekend total. Similarly, the average from January 1 and January 2 exceeded the previous single-day record from January 2021. On January 3, 2022, the US reported 956,893 new cases. For context, only 45 other countries have reported more cumulative cases than the new US single-day record. The new US record is also a global single-day record, surpassing India’s May 2021 peak of 414,188 new cases by more than double, despite India having nearly 4 times as many people.
Since the US Thanksgiving holiday weekend, daily incidence in the US has increased by a factor of nearly 6, and it has quadrupled since just December 19. The current average of 554,328 new cases per day is more than double the previous record—250,435 on January 11, 2021. The US has reported more than 6 million new cases since December 20.
COVID-19 hospitalizations in the US are rapidly approaching a record high as well. The record is 16,497 new hospitalizations per day (January 8, 2021), and the CDC reported 14,776 on January 2, 2022. The average has nearly doubled since December 18, 2021. The CDC is also reporting a surge in the number of current hospitalizations, up from an average of 61,574 hospitalized COVID-19 patients on December 20 to 85,423 on January 2, an increase of nearly 40% over that period. The current average is 31% below the record high—124,031 on January 11, 2021—but the trend is increasing rapidly. Daily mortality appears to have increased slightly over the past several weeks, but reporting fluctuations over the holidays make it difficult to determine whether this is the start of a longer-term trend. A surge in hospitalizations could place severe stress on health systems nationwide, particularly in the context of staffing shortages in many parts of the country, which could contribute to increased mortality for COVID-19 patients as well as those seeking care for other conditions.
Genomic sequencing data from the US CDC show a continued increase in the prevalence of the Omicron variant across the US. When we last looked at the genomic data, the estimated prevalence at the national level was 73.2% for the week of December 18, 2021; however, the CDC revised its estimate that week down to 37.9%. While that estimate fell substantially, the increasing trend continues, up to an estimated 95.4% for the week of January 1, 2022.** Omicron is estimated to be the dominant variant in all 10 HHS regions, including 8 regions with more than 90%. The lowest estimates are 82.4% in Region 1 (New England) and 77.4% in Region 7 (Central).
**US CDC Nowcast projection.
US Vaccination
The US has administered 514 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations peaked on December 6, with 1.71 million doses administered per day. The trend in daily vaccinations continues to decline, down from a recent high of 1.74 million doses per day on December 6 to 971,000 on December 31, a 45% decrease over that period.* Some of this decline could be a result of vaccination clinics, pharmacies, and other vaccination sites being closed over the Christmas and New Year’s holiday weekends, but the trend was already decreasing prior to the holidays.
A total of 245 million individuals have received at least 1 vaccine dose, equivalent to 73.9% of the entire US population. Among adults, 85.9% have received at least 1 dose, as well as 23.3 million children under the age of 18. A total of 207 million individuals are fully vaccinated**, which corresponds to 62.3% of the total population. Approximately 73.0% of adults are fully vaccinated, as well as 18.2 million children under the age of 18. Since August 13, 72.3 million fully vaccinated individuals have received an additional or booster dose. An estimated 34.9% of fully vaccinated individuals have received a booster, including 59.4% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
RAPID ANTIGEN TEST PERFORMANCE As the SARS-CoV-2 virus mutates over time, changes in its genetic makeup could impact the ability of certain tests to recognize and detect viral antigens. A preprint study posted to medRxiv this week raises questions about the reliability of at-home rapid antigen tests in the early days of infection with the highly mutated Omicron variant of concern (VOC). The small real-world study, which is not yet peer-reviewed, examined test results from 30 people who, because of their workplace rules, were undergoing both rapid antigen and polymerase chain reaction (PCR) tests on a daily basis. On days 0 and 1 following a positive PCR test, both of the at-home rapid antigen tests in use—Abbott BinaxNOW and Quidel QuickVue—produced false-negative results despite the presence of viral loads high enough for transmission. The researchers confirmed that 4 cases transmitted the virus between false-negative test results and noted there likely were more transmissions that were unconfirmed. On average, it took 3 days for people to test positive on a rapid antigen test after testing positive on a PCR test. The researchers shared their results with US CDC and US FDA officials and called for the real-world performance of rapid antigen tests to be reassessed for each new VOC.
The study’s results suggest that even if the supply and accessibility of at-home tests were sufficient, rapid antigen testing might not be reliable as an early warning, when people are most infectious and before symptoms begin. Although these findings warrant further study, scientists and public officials are urging the public to continue rapid testing but to use caution when interpreting the results. Some evidence suggests that Omicron might replicate more quickly and efficiently in the throat and mouth than in the nose. And while some individuals have reported swabbing their throats and noses in the hope of increasing the accuracy of test results, the FDA maintains the at-home tests should be used only as authorized. The agency recently updated its information on how SARS-CoV-2 variants could impact tests’ performance.
PFIZER-BIONTECH BOOSTER & ADDITIONAL DOSES This week, the US FDA and US CDC made several adjustments to the emergency use authorization (EUA) and recommendations for the Pfizer-BioNTech SARS-CoV-2 vaccine. On January 3, the FDA made 3 amendments to the EUA, including expanding the use of booster doses to include adolescents aged 12-15 years; shortening the time between primary series and booster to 5 months from 6 months for people who received the Pfizer-BioNTech vaccine; and allowing for a third primary series dose for certain immunocompromised children ages 5 to 11 years. The following day, the CDC updated its recommendation for booster dose timing to 5 months, noting the interval recommendations for other vaccines remains the same (2 months for J&J-Janssen; 6 months for Moderna). The agency also recommended that moderately or severely immunocompromised 5- to 11-year-olds receive an additional primary dose of vaccine 28 days after their second shot. The CDC’s Advisory Committee on Immunization Practices (ACIP) on January 5 voted 13-1 in favor of expanding eligibility of and strengthening the recommendation for Pfizer-BioNTech booster doses in adolescents aged 12-15 years, and the CDC later that day endorsed the recommendation. In a statement, CDC Director Dr. Rochelle Walensky said booster doses 5 months after a primary series “will provide optimized protection against COVID-19 and the Omicron variant” for adults and adolescents aged 12-17. Only the Pfizer-BioNTech vaccine is authorized for individuals under age 18.
During a White House press briefing, Dr. Walensky cited outcomes from several studies conducted in Israel that suggest booster doses decrease the risks of infection, severe disease, and death. Notably, the studies were conducted when the Delta variant of concern was predominant, but Dr. Walensky said “we expect to see a similar trend of increased protection” for the Omicron variant. Israel on January 2 became the first country to officially recommend a fourth dose of SARS-CoV-2 vaccine to people aged 60 and older and medical workers who had their last dose at least 4 months ago. Fourth doses already were available to people with weakened immune systems and residents and staff of nursing homes. The Israeli government said preliminary data show a fourth dose of the Pfizer-BioNTech vaccine spurred an average fivefold increase in antibodies 1 week post-shot. However, some experts question the move, saying too many booster rounds could further vaccine inequity and potentially dampen the immune response if too many doses of the same vaccine are administered. Israel is reporting a record number of new COVID-19 cases, with nearly 12,000 recorded on January 5. Little data on the safety and efficacy of additional doses is not stopping some in the US from seeking fourth, fifth, or even sixth shots, particularly those with compromised immune systems who fear infection. However, some researchers believe that certain immunocompromised people may never generate immune system responses to the vaccines, no matter how many doses they receive.
US CDC QUARANTINE & ISOLATION GUIDANCE In late December, the US CDC updated its guidance regarding isolation for individuals who test positive for SARS-CoV-2 infection. The CDC shortened the recommended isolation period to 5 days for individuals who are asymptomatic or whose symptoms have resolved. After that point, those individuals should wear masks in public to mitigate the risk of transmission to others. The shortened isolation period is based on data that indicate that “the majority of SARS-CoV-2 transmission occurs…in the 1-2 days prior to onset of symptoms and the 2-3 days after.”
Notably, the updated isolation guidance did not include a negative test as a condition to end the isolation period. In response to criticism regarding the absence of a testing requirement—particularly in the context of a shorter isolation period in the midst of the United States’ largest surge to date—the CDC issued a subsequent update on January 4. But rather than including a testing requirement, the CDC provides recommendations regarding how an individual should proceed if s/he “has access to a test and wants to test.” The American Medical Association on January 5 released a statement expressing concern over the guidelines’ exclusion of testing, saying the “recommendations put our patients at risk and could further overwhelm our healthcare system.”
The CDC also updated its guidance regarding quarantine following exposures to known COVID-19 cases. Individuals who are not fully vaccinated should quarantine for 5 days following the exposure, followed by strict mask use for an additional 5 days. If a 5-day quarantine is not practicable, then exposed individuals should wear a mask for 10 days. Individuals who are fully vaccinated do not need to quarantine following an exposure, as long as they remain asymptomatic; however, they should wear a mask in public for 10 days. In this context, the CDC defines fully vaccinated as having received a full original course of the vaccine—eg, 2 doses for the Moderna and Pfizer-BioNTech vaccines and 1 dose of the J&J-Janssen vaccine—as well as a booster dose as recommended—6 months after the second dose of the Moderna or Pfizer-BioNTech vaccines and 2 months after the J&J-Janssen vaccine for adults. Individuals who have tested positive for SARS-CoV-2 in the past 90 days are treated similarly to fully vaccinated individuals. The CDC also recommends testing for all exposed individuals at Day 5 or later after the exposure. As with the previous guidance, anyone who develops symptoms should self-isolate until they receive a negative test or an alternate diagnosis that explains the symptoms.
On December 23, the CDC updated guidance specifically for healthcare workers following exposures to SARS-CoV-2. The new recommendations include updates regarding the process and timeline for returning to work following an exposure as well as the definition of “higher-risk exposures.” The update includes specific testing requirements and timelines for healthcare workers to return to work following SARS-CoV-2 infection, depending on their vaccination status and the presence and severity of symptoms. Largely, fully vaccinated and boosted healthcare workers do not face any work restrictions following an exposure, as long as they remain asymptomatic and do not test positive for SARS-CoV-2 infection, even with a higher-risk exposure. Under the updated guidance, healthcare workers wearing a face mask are no longer considered to have a higher-risk exposure if the patient is also wearing a face mask. Previously, exposures were considered to be higher risk if the healthcare worker was not wearing a respirator. At least 4 nursing organizations have expressed concern over the guidance for healthcare workers, with the American Nurses Association saying the “guidance is premature given what is known about the Omicron variant and tips toward economic needs as opposed to the health needs of nurses and other healthcare workers.”
COVID-19 TREATMENTS As the number of new COVID-19 cases skyrockets in the US, hospitalizations too are beginning to rise. While some nations—including South Africa and the UK—have seen lower hospitalization rates due to the Omicron variant of concern (VOC) compared with previous variants, it remains unknown whether this will be the case in the US. Full vaccination with a booster dose remains the best way to prevent severe COVID-19, but keeping people with the disease from progressing to more severe disease requiring hospitalization is imperative, to both save lives and lessen the strain on the healthcare system. Two highly anticipated and recently authorized antivirals—Pfizer’s Paxlovid and Merck and Ridgeback Biotherapeutics’ molnupiravir—are administered to patients recovering at home to help prevent progression to more severe disease, but the medications are in limited supply, causing dismay among healthcare providers. US President Joe Biden on January 4 announced the government will double its order of Paxlovid to 20 million courses, but long manufacturing times means only 435,000 of those courses are expected to be delivered over the next 2 months. The US government also has purchased 3 million of molnupiravir, with about 300,000 courses already delivered to states based on population. With the limited supply, doctors must make choices about who might benefit the most from the antivirals, both of which are recommended to be administered within 5 days of symptom onset.
While both of the newly authorized antivirals are expected to work against Omicron, 2 of the 3 monoclonal antibody treatments available under FDA emergency use authorization (EUA) do not work against the VOC. After a short pause in distribution, the US government restarted shipments of both Eli Lilly’s bamlanivimab plus etesevimab and Regeneron’s casirivimab plus imdevimab (REGEN-COV) monoclonal antibody therapies, which should be used for patients in areas where the Delta VOC represents a significant portion of cases and other options are not available. The US Health and Human Services (HHS) in a statement warned that the treatments would be ineffective if given to patients with the Omicron VOC and noted other therapeutics—including oral and intravenous (IV) antivirals and GSK/Vir Biotechnology’s sotrovimab monoclonal antibody—are effective alternatives against Omicron. A study published December 22, 2021, in the New England Journal of Medicine (NEJM) examining the IV antiviral remdesivir (Veklury) in symptomatic, non-hospitalized patients with COVID-19 at high risk of disease progression showed a 3-day course of the drug was safe and resulted in an 87% lower risk of hospitalization or death than placebo. Notably, Gilead Sciences, the drug’s maker, funded the study and submitted the trial results to the US FDA to consider expanding the drug’s approval for use in earlier stages of COVID-19.
On December 28, the FDA both expanded and limited the EUA for convalescent plasma to treat COVID-19 by restricting the use of high-titer convalescent plasma to patients with immunosuppressive disease or receiving immunosuppressive treatment but allowing its use in either outpatient or inpatient settings. Previously, the therapy was allowed to be used among any hospitalized COVID-19 patients early in their disease course, but EUA revisions have narrowed the treatment’s use since it was first authorized in August 2020. Additionally, a group of physician-scientists led by Dr. David Boulware of the University of Minnesota filed an EUA application with the FDA for fluvoxamine—a generic selective serotonin reuptake inhibitor (SSRI) that is used to treat several mental health conditions such as depression—to treat COVID-19. Technically, physicians could prescribe the medication off-label for COVID-19 but some might be reluctant to or work in settings that prohibit the practice. The EUA application is based primarily on 2 randomized controlled clinical trials supporting fluvoxamine’s use to prevent disease progression, and Dr. Boulware noted several other studies are looking at whether the drug can help prevent hospitalizations or death among COVID-19 patients.
OMICRON SCHOOL DISRUPTIONS The Omicron variant of concern (VOC) is causing disruptions in nearly every country worldwide. While there is still uncertainty regarding the variant’s clinical presentation, evidence suggests it causes less serious disease, is more transmissible than its predecessors, and is able to at least partially evade preexisting immunity. But a rapid increase in the number of cases worldwide has led to interruptions and staffing shortages in the healthcare, travel, and other industries. Schools are no exception. Analysis from Burbio's School Tracker shows nearly 5,000 pandemic-related disruptions to K-12 US public schools in this week alone. In Chicago, Illinois, the third largest school district in the US closed schools again for a second day, sending more than 350,000 students home as the teachers union and city officials continue a standoff over COVID-19 safety protocols. School closures, delays in returning to in-person learning after the winter holidays, and returns to remote learning in other districts nationwide have parents scrambling for resources and clarity, with some desiring children return to schools and others relieved their children do not have to return to classrooms. According to US CDC data, a record high number of children are being hospitalized with confirmed COVID-19.
In Europe, countries are prioritizing the reopening of schools. France, Greece, and Ireland—which boasts 91% of ages 12 and older fully vaccinated—are returning to in-person schooling with strategies including increased testing and expanded inoculations to kids as young as 5 years old. In England, school leaders are witnessing high levels of staff absences at schools and daycare centers due to COVID-19. Some teachers and one union have expressed concern about government guidance that advises combining classes in the event of staff shortages, citing the possibility of increased transmission. Like the US, countries across the European region are loosening quarantine and isolation restrictions to ease staffing shortages and missed time in class.
PREGNANCY & BIRTH OUTCOMES Pregnant people with COVID-19 have an increased risk for severe illness and adverse birth outcomes. Still, many are reluctant to receive vaccination against COVID-19, with only about 40% of pregnant people in the US fully vaccinated as of mid-December. A retrospective cohort study involving more than 45,000 pregnant people published this week in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) found that SARS-CoV-2 vaccination during pregnancy was not associated with increased risks of preterm delivery or underweight newborns. The data—drawn from 8 healthcare organizations in 6 US states—support the CDC’s recommendation of vaccination and booster doses for all people who are pregnant, recently pregnant, or who are trying to become pregnant. Notably, most of the people involved in the study became pregnant prior to the availability of vaccines and those who were vaccinated received the shots in the second or third trimester, so the study does not include information on first-trimester vaccinations. Experts continue to recommend vaccination for all pregnant people, as the risk of preterm birth is higher among those infected with SARS-CoV-2 and vaccination may help protect infants by passing along beneficial antibodies. A study published in Pediatrics this week suggests that vaccine-induced SARS-CoV-2 antibodies in human breast milk, including IgG and neutralizing activity, persist for up to 6 months.
Another study, published in JAMA Pediatrics, found that in utero exposure to maternal SARS-CoV-2 infection was not associated with differences in neurodevelopment at age 6 months. However, the researchers did find that birth during the pandemic, regardless of SARS-CoV-2 exposure, was associated with slightly lower scores on developmental screening tests of social and motor skills at 6 months compared to infants born right before the pandemic. The researchers said the results suggest that pandemic-related stresses among parents or caregivers, such as job loss or housing insecurity, could have contributed to the small differences between infants born before and during the pandemic. They noted the results of the small study do not necessarily mean infants born during the pandemic will have lasting neurodevelopmental impairment, and they plan to follow the 255 newborns involved in the study.
B.1.640.2 VARIANT Researchers late last year identified a new SARS-CoV-2 variant with 46 mutations and 37 deletions compared with the original novel coronavirus, but the WHO has said the variant is of little concern, for now. The B.1.640.2 variant was first recognized in October 2021 by researchers in France, who dubbed the variant “IHU” after the Méditerranée Infection University Hospital Institute (IHU) that helped to identify it. The isolate came from a vaccinated person who had recently traveled to Cameroon, where the variant is assumed to have originated. So far, fewer than 20 samples have been sequenced, and only 1 in December, compared to the more than 120,000 Omicron variant sequences that have been uploaded to the Gisaid database since its discovery in late November. Many SARS-CoV-2 variants have been identified since the beginning of the pandemic, but many of them never cause widespread infections. The B.1.640.2 variant is likely piquing interest due to the publication of a preprint article (not peer-reviewed) describing it posted on December 29, as well as the heightened anxiety surrounding the recently discovered, highly transmissible, and extensively disruptive Omicron variant of concern. Although experts are not worried about the B.1.640.2 variant at this time, new variants continue to be a threat until more of the world is vaccinated.
These idiots are social media 'influencers' (who would have ever thought that we'd descend to the lowly societal level of calling pitiful, desperate, attention seeking people 'influencers'?)... Reportedly, 25 or so of them have tested positive for COVID-19 in Mexico. Well deserved.
Some who have been identified have been fired from their jobs. Also well deserved.
by ti-amie Just in case you haven't heard about the latest scam treatment.
I'll see myself out
by Suliso Found on twitter
by ponchi101 , Yep, I have seen it too.
A new thing now is also that PCR testing "can give false negatives".
Yes, at a known rate.
The level of scientific illiteracy is insane.
by ti-amie
via Protection Circle @protectioncirc
by dryrunguy Here's the latest Situation Report. I can't pinpoint the reasons why, but this was one of the most frustrating briefs I've read to date.
::
US COVID-19 STRATEGY Amid a record surge in new COVID-19 cases driven by the Omicron variant of concern (VOC), the administration of US President Joe Biden is facing criticism over its handling of the pandemic, particularly surrounding public health guidance and communication. Several top government health officials are testifying today in a US Senate Health Committee hearing, where they will face tough questions regarding the US COVID-19 response. CDC Director Dr. Rochelle Walensky, who will appear before the committee, will face questions regarding the agency’s guidelines on masking, isolation and quarantine, and testing, which have led to several messaging missteps among administration officials and confusion among the public. Dr. Walensky reportedly has undergone media training in recent months and earlier this week held the CDC’s first solo press briefing since heading the agency.
Other questions witnesses could face include how the US is faring during the Omicron wave; how well rapid antigen tests are working and when 500 million free tests will be available; and whether the US needs to reframe its COVID-19 strategy. New daily COVID-19 cases are at a record high and related hospitalizations are on track to soon reach a record high, with some hospitals nearing capacity and facing critical staffing shortages. The Biden administration announced this week that, as of January 15, private health insurers will be required to cover up to 8 at-home rapid antigen tests per month per person on their plans.* The administration also is finalizing plans for 500 million free at-home tests to be available for order through a new website and delivered via the US Postal Service. The administration hopes the strategies to provide easy-to-use, free tests to people at home can help slow the spread of the virus, allow people to gather more safely, and help get kids back to school and people back to work more quickly. It remains unclear how the efforts address the nationwide limited supply of tests, questions surrounding the sensitivity of the tests to detect Omicron, and whether a positive test indicates infectiousness.
Late last week, several former advisors to President Biden’s transition team published a series of articles calling for the administration to revamp its COVID-19 response strategy and set clear goals for a “new normal.” The viewpoint pieces, published in the Journal of the American Medical Association (JAMA), lay out dozens of explicit recommendations on strategies for testing, surveillance, mitigation, vaccines, and therapeutics, including modernizing public health data infrastructure; investing in more tests; providing more high-quality masks free to US residents; implementing more far-reaching vaccine mandates; developing variant-specific and universal coronavirus vaccines; and rebuilding public trust in health institutions. According to The Washington Post, White House officials are pulling together a longer-term funding request to Congress for additional COVID-19-related health spending, including tens of billions more dollars for treatments and vaccine efforts domestically and abroad.
*Most of the authorized SARS-CoV-2 test kits contain 2 tests. We are interpreting this as insurers will be required to cover 8 test kits per person per month containing a total of 16 tests.
US HOSPITALS US COVID-19 hospitalizations are on track to reach a record high, as early as this week. The current 7-day average is at 109,874 as of January 8, up 34% over the prior week and far surpassing the US CDC’s forecast. Pediatric hospitalizations among children with COVID-19, while still lower than any other age group, also are up, with the rise attributed to hospitalizations of children under the age of five who are not yet eligible for vaccination and driven by the increased transmissibility of Omicron. However, hospitalization data does not always provide an accurate picture of COVID-19 severity and may include incidental infections; for example, in New York, 42% of patients hospitalized with COVID-19 were hospitalized for reasons unrelated to COVID-19 and tested positive during routine testing.
Even incidental COVID-19 cases place incredible strain on hospitals, as coronavirus patients need to be isolated and require a greater amount of hospital resources than non-infected patients. Around 80% of hospital and ICU beds are occupied nationwide, according to US government data, with about 21% and 31%, respectively, occupied by COVID-19 patients. Hospitals continue to report that patients admitted for COVID-19 who experience poor outcomes are mostly unvaccinated. Additionally, nearly one-quarter of hospitals nationwide report critical staffing shortages. Many healthcare workers are out sick with breakthrough infections—even after changes to CDC guidelines that allow for a shortened period of isolation—and burnout is causing droves of workers to leave their positions or the healthcare profession entirely. In order to compensate for the strain, some hospitals have been forced to cancel or postpone elective procedures and hospitals in several states are implementing crisis standards of care.
BOOSTER & ADDITIONAL VACCINE DOSES Last week, the US FDA amended the authorization and the US CDC updated recommendations for reducing the interval period between the primary vaccination series and booster doses from 6 months to 5 months for both the Pfizer-BioNTech and Moderna SARS-CoV-2 vaccines. According to the FDA, the change was made in response to the dramatic rise in US cases attributable to the highly transmissible Omicron variant. Third doses of the mRNA vaccines have been shown to increase immune system responses that could help protect against infection with or severe disease from Omicron. In New York, healthcare workers are now required to receive vaccine boosters in addition to the full primary series, with exemptions only allowed for medical reasons.
Now, discussion among the pharmaceutical and scientific community is turning to whether a fourth dose (ie, second booster) is warranted later this year. Moderna’s CEO publicly voiced that recipients of the company’s vaccine may need an additional fourth dose in the fall to compensate for waning antibody levels. Researchers from Israel recently announced findings from unpublished studies documenting a 5-fold increase in antibodies after a second Pfizer-BioNTech booster. Israel already is offering a fourth dose to certain populations, including healthcare workers and higher-risk older adults. West Virginia Governor Jim Justice has requested permission from US health agencies to follow Israel’s example to provide fourth doses to some residents. The state has the third oldest population of all US states, and many residents have underlying conditions that raise their risk of severe COVID-19. Additionally, the US CDC updated its guidance to allow some moderately or severely immunocompromised individuals to receive 4 doses of COVID-19 vaccine, including a third primary dose and a fourth booster dose. However, the WHO warns that providing continual boosters every few months is not a fiscally or operationally sustainable long-term strategy, and some experts predict continuous boosters could dampen immune responses. Pfizer-BioNTech and Moderna both have plans to roll out vaccine booster doses that target Omicron later this year.
US VACCINE REQUIREMENTS The US Supreme Court on January 7 heard nearly 4 hours of oral arguments in 2 sets of cases involving federal SARS-CoV-2 vaccine requirements. At issue are 2 federal regulations: the Occupational Safety and Health Administration’s (OSHA) Emergency Temporary Standard (ETS) that requires all workers at firms with 100 or more employees either get vaccinated or be tested weekly and wear a mask to work (National Federation of Independent Business v. Department of Labor, No. 21A244) and a Centers for Medicare and Medicaid Services (CMS) regulation issued by the US Department of Health and Human Services (HHS) requiring vaccination for nearly all workers at hospitals, nursing homes, and other medical facilities that receive federal funds through Medicare and Medicaid (Biden v. Missouri, No. 21A240). Both cases came to the court last month on an emergency basis, and the justices elected to fast-track the cases for oral arguments to determine whether the Biden administration can continue enforcement of the rules while litigation continues.
The court’s conservative majority signaled it is unlikely to permit the Biden administration to enforce the OSHA rule, with several justices questioning the agency’s authority to issue such a wide-ranging emergency regulation without explicit congressional authorization. The court’s 3 liberal justices, on the other hand, indicated the regulation clearly meets OSHA’s authority to take actions to protect workers from “grave danger.” The rule is currently being enforced after the US Court of Appeals for the Sixth Circuit dissolved a stay of the ETS issued by the Fifth Circuit. If the court allows the rule, OSHA expects to begin issuing citations for noncompliance no sooner than February 9.
In the CMS case, more justices appeared to support the Biden administration’s authority to require certain healthcare workers to be vaccinated, unless they qualify for a medical or religious exemption. Notably, Chief Justice John Roberts suggested a clear association between healthcare workers and the safety of patients. Additionally, Associate Justice Brett Kavanaugh noted that none of the facilities or workers covered under the mandate are challenging the requirement and questioned whether the Republican-led states behind the challenge had the legal authority to do so because they operate only some of the facilities affected by the mandate. The CMS requirement is currently blocked in 25 states due to a lower court injunction. The federal government is asking the Supreme Court to lift that injunction. CMS said on December 28 it plans to begin phased enforcement for facilities located in states not covered under the stay, and those facilities’ employees will need to be fully vaccinated by February 28.
NOVAVAX Novavax expects its SARS-CoV-2 vaccine to receive regulatory approval in multiple countries, including the US, over the next several months, the company’s CEO, Stanley Erck, said on January 10. As expected, Novavax completed its data submission on its protein-based vaccine to the US FDA on December 31, a prerequisite for emergency use authorization (EUA) application. The company expects to file a request for an FDA EUA at the end of this month, and it has recently applied for authorization in other nations, including Japan, the United Arab Emirates, Singapore, New Zealand, Australia, South Africa, and the UK. Shipments of the vaccine have begun to the European Union, which authorized the vaccine last month. The WHO has issued emergency use listings for 2 versions of the vaccine (NVX-CoV2373): Nuvaxovid, which will be manufactured in Europe and is authorized for use by the European Medicines Agency; and Covovax, which will be manufactured by the Serum Institute of India and is authorized for use by the Drugs Controller General of India. Some experts feel the vaccine’s 6-month stability under simple refrigeration storage will make it particularly useful in low-income countries.
INDIA Several states in India are imposing COVID-19 restrictions amid a sharp increase in the number of new cases due to the Omicron variant of concern (VOC). The country experienced an 8-fold rise in new cases in the 10 days since January 1, reporting the most daily COVID-19 cases since early June. More than 1 million healthcare and frontline workers and high-risk older adults received a third dose of SARS-CoV-2 vaccine on January 10, the first day of the country’s “precaution” dose rollout. The government reported an additional 277 deaths on January 11, bringing the official total to 484,213. Notably, an analysis published last week in Science questions the official count, suggesting instead that close to 3 million people have died of COVID-19 in the country. The analysis—which several outside experts praised for its robust design—shines a light on the potential for undercounting COVID-19 mortality in other countries with anomalously low death rates, including Russia, Tajikistan, Nicaragua, Uzbekistan, Belarus, and Egypt.
CORBEVAX & PAN-SARS VACCINES Researchers in Texas (US) are celebrating India’s recent regulatory authorization of CORBEVAX, a SARS-CoV-2 vaccine designed using traditional technology specifically for use in resource-poor settings. Researchers from Texas Children’s Hospital Center for Vaccine Development (Texas Children’s CVD) and Baylor College of Medicine developed the protein subunit vaccine and licensed it, without patents, to Biological E. Limited (BioE) for manufacturing. India already has ordered 300 million doses, and BioE plans to deliver more than 1 billion doses to other countries. While some questions remain about CORBEVAX’s effectiveness against Omicron and a lack of publicly available data, the vaccine’s development—funded by private philanthropies with no strings attached—represents a model for future vaccine development and vaccine equity. Unlike vaccines using newer technology, CORBEVAX’s intellectual property is available to manufacturers worldwide.
Similarly, scientists with the US Department of Defense’s Walter Reed Army Institute of Research are developing a pan-SARS vaccine aimed at providing broad protection against SARS-CoV-2 variants and other coronaviruses that could be useful in low- and middle-income countries because it does not require ultra-cold freezer storage. The investigational Spike Ferritin Nanoparticle (SpFN) vaccine completed phase 1 clinical trials in December with positive results that are currently under analysis. The vaccine uses a ball-shaped ferritin nanoparticle that allows scientists to attach up to 24 spike proteins of various coronaviruses, which they hypothesize will induce potent and broad immune responses. The SpFN vaccine has not yet been tested against Omicron and needs to undergo phase 2 and phase 3 clinical trials.
by ponchi101 Indeed, a sobering read.
I wrote it two years ago, when this started. I hate to sound so arrogant, but I said it then: this disease has defeated us. Between the anti-vaxxers, the lack of scientific understanding, the pressures for economies to re-open, and the speed of mutation for this virus, it is hard to see a path to victory. And if in the USA the SCOTUS decides that OSHA and related agencies cannot enforce procedures to reduce this wave, then there is really no way out, other than some miracle pill that will stop the virus on its track once detected.
by ti-amie
Late last week, several former advisors to President Biden’s transition team published a series of articles calling for the administration to revamp its COVID-19 response strategy and set clear goals for a “new normal.” The viewpoint pieces, published in the Journal of the American Medical Association (JAMA), lay out dozens of explicit recommendations on strategies for testing, surveillance, mitigation, vaccines, and therapeutics, including modernizing public health data infrastructure; investing in more tests; providing more high-quality masks free to US residents; implementing more far-reaching vaccine mandates; developing variant-specific and universal coronavirus vaccines; and rebuilding public trust in health institutions.
This was discussed on the financial podcast I listen to.
The point has been made that technically the 1918 flu is still with us and is the reason there is a new flu vaccine every year. There will be no going back to the way we were.
by ti-amie
by atlpam Heard from a good friend that her sister is in ICU after suffering a Covid blood clot induced heart attack (also has double-pneumonia).
This was the result of a family gathering over the holidays. Her daughters flew in for the visit with grandkids under 5. All of the adults were double-vaxed and boosted. All 9 of them have tested positive for Covid. (Not sure if her sister has other health issues that increased her risk).
In more positive news, from looking at trend data, it looks like we may be on the downslope in Georgia from our Omicron peak.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 312 million cumulative cases and 5.5 million deaths worldwide as of January 12. Global weekly incidence again increased substantially last week, up 59% over the previous week. This is the 12th consecutive week of increasing weekly incidence, setting another new record with 15.58 million new cases. The increase continues to largely be due to surges in the Americas (+78.8%) and Europe (+37%), but nearly all WHO regions reported increases last week. Notably, the WHO reported a decrease in the Africa region (-11%), potentially signaling the Omicron surge there has peaked. The Omicron surge in the UK also appears to have peaked, with government data showing the weekly average number of cases down 19% over the previous week. However, weekly average mortality within 28 days of a positive SARS-CoV-2 test is up 44.3%. Global weekly mortality increased for the first time in 5 weeks, up 2.7% from the previous week with 43,522 total deaths.
Global Vaccination
The WHO reported 9.2 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of January 11. A total of 4.59 billion individuals have received at least 1 dose, and 3.89 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations increased from mid-October (21.7 million doses per day) through mid-December (39.1 million). Daily vaccinations have decreased since December 20, down to 35 million.* Our World in Data estimates that there are 4.69 billion vaccinated individuals worldwide (1+ dose; 59.53% of the global population) and 3.98 billion who are fully vaccinated (50.5% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 62.5 million cumulative cases of COVID-19 and 840,286 deaths. The US is averaging 761,535 new cases and 1,656 deaths per day.* Notably, the US reported 1.35 million new COVID-19 cases on January 10. This exceeds the previous single-day record, set on January 3, by 397,521 cases.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
COVID-19 hospitalizations in the US set a record high this week, passing the previous record of 16,497 new hospitalizations per day (January 8, 2021). The 7-day average as of January 10 is 20,269. The CDC is also reporting a surge in the number of current hospitalizations, up from an average of 91,030 hospitalized COVID-19 patients on January 3 to 124,163 on January 10, an increase of 36.4% over that period. The current average is slightly above the previous record high—124,031 on January 11, 2021. Daily mortality is increasing, and the surge in hospitalizations is placing severe strain on health systems nationwide, which could contribute to increased mortality for COVID-19 patients as well as those seeking care for other conditions.
US Vaccination
The US has administered 522.5 million cumulative doses of SARS-CoV-2 vaccines. The trend in daily vaccinations continues to decline, down from a recent high of 1.74 million doses per day on December 6 to 1 million on January 7.*
A total of 247.7 million individuals have received at least 1 vaccine dose, equivalent to 74.6% of the entire US population. Among adults, 86.6% have received at least 1 dose, as well as 24 million children under the age of 18. A total of 208 million individuals are fully vaccinated**, which corresponds to 62.7% of the total population. Approximately 73.4% of adults are fully vaccinated, as well as 18.7 million children under the age of 18. Since August 13, 77.1 million fully vaccinated individuals have received an additional or booster dose. An estimated 37% of fully vaccinated individuals have received a booster, including 60.8% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
WHO ON SARS-COV-2 VACCINES A WHO panel of vaccine subject matter experts known as the Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC) released an interim statement on January 11 regarding vaccination strategies to combat the ongoing pandemic. The TAG-CO-VAC advised increasing access to primary and booster doses of current vaccines in low- and middle-income countries (LMICs) to prevent the emergence of new SARS-CoV-2 variants and updating vaccine composition to cover currently circulating variants. Vaccine inequity is an issue often discussed by the WHO, and it is believed to be a large driver for the emergence of new variants that have the potential to escape vaccine-induced immunity, such as Omicron. Increasing efforts to provide initial vaccination doses to under-immunized nations has the potential to slow the emergence of new variants and take pressure off health systems that are buckling under the weight of new cases. TAG-CO-VAC also stated that promoting a vaccination strategy that relies on multiple booster doses of the original vaccine design is unlikely to be effective. TAG-CO-VAC called for an updated vaccine design that protects against infection and severe disease, is based on currently circulating variants, and elicits a robust immune response. The best options for new vaccine design include multivalent vaccines that protect against many circulating variants or pan-SARS vaccines that provide protection from current and future variants.
OMICRON SEVERITY Real-world evidence is supporting the theory that the highly infectious SARS-CoV-2 Omicron variant of concern (VOC) causes less severe disease than the Delta VOC, but officials are warning that Omicron cannot be described as “mild” and unvaccinated individuals remain at risk for severe outcomes. A study posted January 11 to the preprint server medRxiv examined the outcomes of nearly 70,000 COVID-19 patients in California and suggests Omicron causes less severe disease than previous variants. The findings, which are not yet peer-reviewed, align with similar data from research conducted in South Africa, the UK, and Denmark. Additionally, laboratory studies show Omicron’s lower virulence might be due to its tendency to replicate more in cells of the upper respiratory tract instead of the lungs, where the virus can lead to more serious breathing problems. While more is being learned about how well vaccine-induced or natural immunity helps to protect against severe outcomes in Omicron cases, early reports indicate infections are less severe in people with some prior immunity. Additionally, it is too soon to conclude whether Omicron is less lethal than previous variants. While real-world anecdotes suggest people infected with Omicron are less likely to need intensive care including breathing support, COVID-19 hospitalizations set a new record this week in the US. Hospitals nationwide already are overwhelmed with an enormous number of people with COVID-19—as well as with other health conditions—all while facing staffing shortages exacerbated by workers themselves becoming ill. Most agree that this surge of Omicron will help push the world further toward COVID-19 endemicity, but the short- and long-term costs remain to be realized.
SARS-COV-2 IMMUNITY Emergence of the SARS-CoV-2 Omicron variant, which has a highly mutated spike protein when compared with the Beta or Delta variants, has increased international attention on how mutations impact immunity and neutralizing antibody production. A preprint study from Japan provides evidence that fully vaccinated individuals who have also had breakthrough infections—known as hybrid immunity—may be better protected against infection with Omicron. According to the study, which is not yet peer-reviewed, the greater the span of time between the last vaccination and a breakthrough infection directly correlates with the quality of protection. The results of this study imply that countries that were hit harder by the Delta wave could be in a better position to withstand the current Omicron wave, but the authors urged a cautious approach when trying to understand how population immunity interacts with new and future variants.
An additional preprint study from India suggests that Omicron’s rapid global spread may be due to decreased efficacy of neutralizing antibodies in both vaccine-only and hybrid immunity populations. According to the study, which also is not yet peer-reviewed, neutralizing antibodies were extremely effective against the original strain of the virus but efficacy was much lower against the Omicron variant. Despite the lower efficacy, the study also provided further confirmation that hybrid immunity provides better protection than vaccine-only immunity.
Discussions about the impact of spike protein mutations on immunity typically focus on neutralizing antibodies, but a subset of immunologists are highlighting the importance of T-cells. Current evidence shows that new SARS-CoV-2 variants, such as Omicron, remain susceptible to T-cell mediated immunity. Susceptibility of Omicron to T-cell immunity means that vaccinated populations are likely to be protected from severe disease, hospitalization, and death despite a drop in neutralizing antibody titers. Vaccination remains the best tool to defend against severe outcomes, and it is becoming increasingly clear that natural immunity from prior infection alone is not sufficient for protection. Unvaccinated populations in the US are 20 times more likely to die from COVID-19 than fully vaccinated populations.
GLOBAL ECONOMIC GROWTH SLOWDOWN The quick rise of the SARS-CoV-2 Omicron variant of concern (VOC), as well as the threat of other potential variants, is helping to fuel a global economic slowdown, endangering economic recovery in emerging and developing economies, scaling back progress on reducing poverty, and disrupting social cohesion and global cooperation, according to 2 reports released this week. The World Bank’s latest Global Economic Prospects report predicts the pandemic will continue to disrupt economic activity in the near term, causing a deceleration in global growth from 5.5% in 2021 to 4.1% in 2022 and 3.2% in 2023. Notably, growth in emerging and developing countries is expected to drop from 6.3% in 2021 to 4.4% in 2023, at an output level 4% below the pre-pandemic trend. President of the World Bank Group David Malpass said more international action and national-level policy responses are needed to address the pandemic, inflation, inequality, security challenges, and general uncertainty. The report highlights prioritizing vaccine equity and alleviating vaccine deployment bottlenecks in low- and middle-income countries as one way to bring the pandemic under control.
The World Economic Forum’s (WEF) Global Risks Report 2021 also warns that the pandemic and vaccine inequality are causing lost opportunities for large parts of the global population—including job losses, a widening digital divide, and shifts in markets—that will result in social unrest, political fragmentation, and geopolitical tensions impacting how the global community responds to other key economic threats such as cyberattacks, space exploitation, weapons of mass destruction, and, “most notably,” climate change. Of about 1,000 global experts and leaders from academia, business, civil society, government and other organizations surveyed in the WEF’s Global Risks Perception Survey (GRPS), more than 84% are worried or concerned about the global outlook. Vaccine inequality is driving growing gaps in economic recovery—a “global divergence”—which threatens to compound pre-existing social cleavages and geopolitical tensions. The WEF said policymakers must prepare for the next pandemic now and outlined 4 governance opportunities to improve overall resilience, including taking a holistic and systems-based approach to risk impacts; investing in “risk champions” to encourage national and international action; improving risk communications and combating misinformation; and exploring new forms of public-private partnership.
SCHOOL IMPACTS As many schools worldwide reopen to in-person learning, some scientists, public health experts, and teachers are wondering why more mitigation measures—including vaccination, masking, regular testing, contact tracing, improved ventilation, desk-spacing, outdoor area use, and handwashing—are not in place. In the US, COVID-19 cases among school-aged children are increasing exponentially, according to the American Academy of Pediatrics. Pediatric hospitalizations are at the highest rate in the pandemic; the vaccination rate among 5- to 11-year-olds remains low, just over 17%; and children under age 5 remain ineligible for any SARS-CoV-2 vaccine and likely will remain so for at least a few more months. With teachers’ unions and local governments at odds over returning to in-person instruction in some districts, including Chicago, students are organizing to have their voices heard. In Massachusetts, an online petition has gained nearly 6,000 signatures in favor of a remote learning option, and students in New York and Michigan walked out of classrooms in protest over their schools’ COVID-19 policies. The Biden administration on January 12 announced it will increase the number of SARS-CoV-2 tests available to schools by 10 million per month*, in addition to other testing capacities, which they hope will help schools operate safely.
In France today, members of 11 educator unions took part in a walkout in protest over pandemic work conditions, forcing the closure of schools and classrooms nationwide. France is in the midst of a record-breaking surge in Omicron cases, and government changes to school rules have caused a “mess,” teachers say. In Uganda, students this week celebrated the reopening of schools after being closed nearly 2 years because of COVID-19. However, not all students celebrated. Officials warned at least 30% and as much as 50% of students may never return, with those from low-income and rural families impacted the most. Some students instead began working, while others became pregnant or married early. Many cannot afford tuition fees for high school. Some educational experts feel an entire generation of learners may have been lost during the pandemic, though others disagree. Additionally, some teachers could not go without pay and found other employment, and thousands of schools, both public and private, are likely to remain closed permanently. COVID-19 school closures and other indirect damage in several African nations have hit young women harder than men, and the extent is difficult to measure. But the pandemic likely has set girls’ progress back, leaving questions about whether recovery is possible.
*The administration intends to send 5 million rapid tests and 5 million lab-based PCR tests to schools per month at no cost.
US LAW ENFORCEMENT For the second year in a row, COVID-19 was the leading cause of death among US law enforcement officers. According to preliminary data from the National Law Enforcement Officers Memorial Fund, 458 local, state, tribal, and federal officers died in the line of duty in 2021, a 55% increase over 2020 and the highest total since 1930. Of those deaths, 301 were related to COVID-19, with the virus reportedly contracted in the line of duty. Some law enforcement and police unions have pushed back against local government regulations requiring vaccines for workers, threatening resignations and legal action. A federal judge this week dismissed a lawsuit brought by Los Angeles police officers challenging the city’s SARS-CoV-2 vaccination and testing mandate, saying the rule did not violate their constitutional rights.
by JazzNU
atlpam wrote: ↑Thu Jan 13, 2022 8:13 pm
Heard from a good friend that her sister is in ICU after suffering a Covid blood clot induced heart attack (also has double-pneumonia).
This was the result of a family gathering over the holidays. Her daughters flew in for the visit with grandkids under 5. All of the adults were double-vaxed and boosted. All 9 of them have tested positive for Covid. (Not sure if her sister has other health issues that increased her risk).
In more positive news, from looking at trend data, it looks like we may be on the downslope in Georgia from our Omicron peak.
So sorry to hear this, that is rough. Really hope you friend's sister is okay and doesn't have any long term effects and hopefully the others are feeling okay and have mild symptoms at best.
by atlpam Update on my friend's sister: She is doing much better and is at home recovering. They broke up ~20 clots via a catheter! Hoping there are no further repercussions.
by MJ2004The true toll of the antivax movement
By rejecting modern medicine, antivaxxers have recreated past eras when people died like flies
Simon Kuper - FT
There’s a 13-year-old boy whose antivax father — an intelligent, accomplished man in his early fifties — died last month of Covid-19. Go to the father’s Twitter feed and it’s the usual story: he warns followers that governments have “radicalised”, that Pfizer jabs are perilous and long Covid is an invention, then tweets casually that he has tested positive, before his feed suddenly goes silent, for ever.
Many vaccinated people enjoy mocking deaths like his. That’s harsh. We all make wrong choices every day, but they don’t usually kill us. Above all, though, vaxenfreude, as it’s now called, ignores the people left behind.
The worst harm that antivaxxers do is to their families, whom they expose to daily danger and then sometimes plunge into a grief that cannot speak its name. The harm will reverberate down the generations. How will it shape the millions of bereaved and their relationship to the rest of us?
For most inhabitants of rich countries, Covid-19 is no longer lethal, but for the voluntarily unvaccinated, it’s a slaughter they don’t understand. Their risk of Covid-related death is 14 times that of vaccinated people, says Rochelle Walensky, director of the US’s Centers for Disease Control.
Just between June and November, 163,000 Covid-19 deaths in the US alone could have been prevented by vaccination, estimates the Kaiser Family Foundation. That’s nearly double all the American deaths in war in Korea, Vietnam, Afghanistan and Iraq combined — and the unvaccinated continue to die, pointlessly.
For each unvaccinated American death, about nine people lose a grandparent, parent, sibling, spouse or child. Probably the most distressing thing about Covid-19 is its relentless orphaning, which recalls the HIV epidemic in Africa or the Great Flu of 1918. Think of the children of Kevin and Misty Mitchem, a couple in their forties who chose not to be vaccinated and who died of Covid within days of each other in October.
Losing a parent young is one of the great life traumas. Bereaved children are often cast into depression (which is why my own chief life goal is to plug on until my kids are at least 18). Yet when the parent is an antivaxxer taken by Covid, the child may feel shamed into silence over an unnecessary death that some people will always regard as farcical.
Meanwhile, antivaxxers will tend to blame the victim’s supposed physical weakness or pretend that the death wasn’t from Covid-19. They can’t easily change their mind about the disease, because that would mean giving up their antivax identity and the community that comes with it.
Then there are people who won’t discuss the cause of death for fear of politicising a tragedy. (A new trend in parts of the US is to keep Covid-19 out of the obituary.) So children may not have anyone to talk to about the worst moment of their lives.
This is known as “disenfranchised grief” — a term coined by the psychologist Kenneth Doka to describe the feelings of mourners who cannot discuss their loss because the cause of death is stigmatised. This was common during the Aids epidemic, and still is when somebody dies by suicide or an overdose or fighting on the unpopular side of a war. A friend of mine suffered disenfranchised grief when his former mistress died, and he couldn’t tell the person he loved most, his wife.
Today, the antivaxxer’s bereaved relatives — who may themselves be vaccinated, or conflicted doubters — sometimes feel angry with the dead person, and/or with the society that mocks their pain.
Survivors can be saddled with lifelong guilt, especially if the death occurred after a large unvaccinated family gathering. And the death often worsens tensions in families already riven between the unvaccinated and vaccinated. Almost the first thing the bereaved may have to decide together is whether masks must be worn at the funeral.
By rejecting modern medicine, antivaxxers have recreated past eras when people died like flies. Both my grandmothers, for instance, lost their fathers as teenagers, and each went on to lose a child. That was normal a century ago. It was also unbearable, especially because there was almost no language to talk about grief then. For all the angst today about the horrors of social media, that generation was probably more damaged than ours. And the damage was bequeathed to their descendants: both my parents were shaped by their mothers’ unhappiness, and so those long-ago deaths shaped me, too.
Imagine the fear, stress and confusion of a child being raised by antivaxxers now. The virus is everywhere like never before and is slaying people around you. It would be natural to start wondering whether the rest of the world is right and Mummy and Daddy have joined a death cult. It’s an experience that may set these children apart into the 22nd century.
by JazzNU
atlpam wrote: ↑Fri Jan 14, 2022 1:32 pm
Update on my friend's sister: She is doing much better and is at home recovering. They broke up ~20 clots via a catheter! Hoping there are no further repercussions.
That is just the best news. But wow that is super scary. Amazing that she's already doing well enough to be at home recovering. Covid is no joke, it is maddening how many people try to equate it with a cold.
by ponchi101 Txs for that piece, MJ. Excellent.
One has to remember that memes, and antivaxx is a meme, follow very much evolutionary pressures. if the meme grants an advantage, it will thrive. If not, it will vanish. Now, the antivaxx meme offers nothing but downside. I understand that the article is about being compassionate, but there is the practical aspect. There is a limit to how much you can explain the antivaxxers how wrong they are. After that, they have to step back into reality by themselves.
by ti-amie
by ponchi101 Joy!
by Deuce This is an interesting and fairly detailed account - mostly in layman's terms - of how mRNA vaccines came to be (from the New York Times)...
by JazzNU FYI. One order per address is the max right now, each order has 4 tests, won't ship until late January at the earliest. Site goes live officially tomorrow, this is an early limited rollout,, likely stress testing the site today. Super simple order process.
by ti-amie
by mmmm8
JazzNU wrote: ↑Tue Jan 18, 2022 6:15 pm
FYI. One order per address is the max right now, each order has 4 tests, won't ship until late January at the earliest. Site goes live officially tomorrow, this is an early limited rollout,, likely stress testing the site today. Super simple order process.
Ordered these yesterday, one for self, one for my parents... who incidentally found out yesterday that they have COVID (mild symptoms)
by ti-amie
by ti-amie I ordered my tests. It doesn't even take five minutes.
by Deuce I picked up my rapid test kit today - left my name at a local drug store about a week ago and they called me yesterday (free). 5 tests.
I don't really see the practicality of them... Firstly, they're not very reliable. The value of a test that tells you that you MIGHT have COVID-19 is... questionable, at best.
The only reason I got it is in case it is discovered in the relatively near future that they are significantly more accurate than is currently claimed.
In fact, these rapid tests could sometimes do more harm than good - like if it gives a negative to a person who IS infected. That person will then feel that it's safe to go out and be among people...
Anyone who experiences any of the symptoms of COVID-19 should isolate for a time (the amount of time seems to depend what time zone you're in these days).
It's pretty simple - if you have symptoms, assume it's COVID and do the right thing.
by JazzNU
mmmm8 wrote: ↑Wed Jan 19, 2022 10:02 pm
Ordered these yesterday, one for self, one for my parents... who incidentally found out yesterday that they have COVID (mild symptoms)
Hope they are okay, great to hear they only have mild symptoms.
by ponchi101 Flew into the States today. I did get an antigen test yesterday, and then I did upload it into the UNITED.COM site.
But still, nobody asked me for it today at the airport. Then again, it was Houston. So no good to rely on the Colombian authorities for enforcement (which they did).
by dryrunguy Here's the latest Situation Report. They hadn't issued one in a while, so much of this falls into "we already knew this" territory.
But there were a few items that raised my eyebrows: 1) the Delta-based study that examined the risk of COVID-related hospitalization or severe illness based on previous infection, vaccination status, etc.; 2) the section on racial and ethnic differences in COVID treatments by treatment type and ethnicity; and 3) I had no idea that Tonga has recorded only one official case of COVID and is considered a COVID-free zone--that has significant implications as relief workers come into the country to provide much-needed aid and assistance, but without the usual 21-day quarantine period.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 332.6 million cumulative cases and 5.55 million deaths worldwide as of January 19. Global weekly incidence increased again last week, up 29.77% over the previous week. This is the 13th consecutive week of increasing weekly incidence, setting another new record with 20.32 million new cases. All WHO regions except Africa (-27.24%) reported increases last week. The Omicron variant drove the greatest percentage increases in South-East Asia (+144.58%), Eastern Mediterranean (+68.25%), and the Western Pacific (+38.49%), followed by the previous leaders of the Americas (+32.46%) and Europe (+17.01%).
Global weekly mortality increased for the second week, up 10.88% from the previous week with 48,911 total deaths. Cumulative global mortality passed 5.5 million the week ending January 10, up from 5 million on November 1, 2021. The true global death toll of the pandemic is estimated to be much higher, with models from the Institute for Health Metrics and Evaluation and The Economist suggesting COVID-19-related deaths to be between 2 and 4 times higher.
Global Vaccination
The WHO reported 9.57 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of January 11. A total of 4.7 billion individuals have received at least 1 dose, and 4.0 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations increased from mid-October (21.36 million doses per day) through late-December (38.87 million). However, daily vaccinations continue to decrease, down to 30.15 million on January 19.* Our World in Data estimates that there are 4.73 billion vaccinated individuals worldwide (1+ dose; 60.11% of the global population) and 4.05 billion who are fully vaccinated (51.59% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 67.9 million cumulative cases of COVID-19 and 853,230 deaths. The US is averaging 755,095 new cases and 1,669 deaths per day.* Some models estimate that the cumulative number of deaths could rise above 1 million by mid-March, when the Omicron wave is expected to subside.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
COVID-19 hospitalizations in the US set another record high this week, with a 7-day average of 21,086 new hospitalizations per day. The CDC is also reporting a surge in the number of current hospitalizations, up from an average of 125,106 hospitalized COVID-19 patients on January 10 to 142,595 on January 17, an increase of 14% over that period. The current average is the highest since the beginning of the pandemic.
US Vaccination
The US has administered 530.4 million cumulative doses of SARS-CoV-2 vaccines. The trend in daily vaccinations continues to decline, down from a recent high of 1.74 million doses per day on December 6 to 1.04 million on January 14.*
A total of 249.7 million individuals have received at least 1 vaccine dose, equivalent to 75.2% of the entire US population. Among adults, 87.1% have received at least 1 dose, as well as 24.7 million children under the age of 18. A total of 209.5 million individuals are fully vaccinated**, which corresponds to 63.1% of the total population. Approximately 73.6% of adults are fully vaccinated, as well as 19.3 million children under the age of 18. Since August 13, 81.7 million fully vaccinated individuals have received an additional or booster dose. An estimated 39% of fully vaccinated individuals have received a booster, including 62.3% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
COVID-19 IMMUNE LANDSCAPE With cases of COVID-19 continuing to surge worldwide due to the Omicron variant of concern (VOC), scientists are looking to recent experiences with the Delta variant to shed insight into what the immune landscape might look like for individuals who are unvaccinated and have recovered from previous SARS-CoV-2 infection, those who are vaccinated, and those who are both recovered and vaccinated. The world will be in a significantly different place after Omicron subsides, with millions of people having at least short-term immune memory of its distinct S-gene mutations. More people than ever before will have some form of natural immunity against SARS-CoV-2, but it is unclear the extent to which recent infection might protect against future infection or hospitalization. In a new report published in the US CDC’s Morbidity and Mortality Weekly Report (MMWR), researchers examined case and hospitalization rates in New York and California during the surge of the Delta VOC. They describe a complex immune landscape through the beginning of Delta’s takeover to the time when it became the predominant global variant.
Initially, in May 2021, vaccinated persons with no prior infection had the lowest rates of hospitalization, but as Delta began to infect more people and cause breakthrough cases, individuals with previous infection were less likely to be hospitalized compared to unvaccinated persons with no prior infection. From May 2021 to June 2021, vaccinated persons with no prior infection had the lowest hospitalization rates of any other group at 27.7-fold lower compared with unvaccinated persons with no prior infection. But from October 2021 to November 2021, hospitalization rates among vaccinated persons with prior infection were 57.5-fold lower and 55.3-fold lower among unvaccinated individuals with prior infection, compared with unvaccinated individuals with no prior infection. By comparison, hospitalization rates in vaccinated persons with no prior infection were 19.8-fold lower. These data suggest that natural immunity from prior infection can play an important role in preventing severe consequences of subsequent SARS-CoV-2 infections, even among those who have not been fully vaccinated.
Some important context to these findings is that the shift in protection from vaccine-alone to vaccine-plus-prior infection occurred during a time of known waning immunity from initial rounds of vaccination. Additionally, people who were fully vaccinated with an additional booster dose were not evaluated as a separate group in this study. All of these data point to having high levels of antibodies—whether vaccine-induced, naturally acquired, or a combination—as vital in protecting against hospitalization and severe COVID-19 outcomes. It is still unclear whether these patterns will hold for the Omicron VOC, which has a greatly different viral profile compared with previous variants. Hospitals are still reporting that the unvaccinated have the highest risk of severe COVID-19, while the group with the lowest risk of severe COVID-19 are those who are fully vaccinated and boosted, underscoring the continuing need for vaccines and booster doses.
A word of caution: Some might interpret these findings as a “green light” to ignore all COVID-19 precautions and take unnecessary risks for themselves and others. Even if natural immunity does confer protection for an extended time, the consequences of contracting and recovering from COVID-19 cannot be overstated; it is estimated that 15-80% of people recovering from illness will experience “long COVID,” or prolonged symptoms including brain fog, dizziness, loss of taste and smell, and other symptoms which can alter daily life for those affected. While those who might get COVID-19 twice do seem fortunate in that their bodies are better able to fight off the newest infection, it is still better never to become infected with SARS-CoV-2 because of the uncertainties of long-term sequelae. Vaccines, masks, and physical distancing are all still vital tools in bringing an end to the pandemic with as few deaths as possible.
US RESPONSE Beginning next week, the administration of US President Joe Biden will supply 400 million “high-quality” masks at no cost to the US population through community health centers and pharmacies. The N95 respirators, which will come from the Strategic National Stockpile, offer the highest level of protection from SARS-CoV-2, according to new guidance from the US CDC, filtering out 95% of all airborne particles. It is not clear yet how many masks will be available to each person at one time, and recipients will not be prioritized based on vulnerability, income, or other criteria.
Late last week, the CDC updated its guidance on the types of masks and respirators recommended for use during the COVID-19 pandemic, removing concerns related to shortages of N95 or KN95 respirators and saying “people can choose” those respirators. The agency clarified that some types of masks and respirators provide more protection to the wearer than to others and that “surgical N95s”—respirators that provide additional protection against certain hazards present during medical procedures, such as blood splatter—should be reserved for healthcare professionals. Overall, the CDC continues to encourage people to “wear the most protective mask you can that fits well and that you will wear consistently.” Nearly 150 manufacturer applications to sell N95 masks are backlogged at the CDC, which is being criticized for taking months to review the applications.
The US government on January 18 quietly launched its new website, COVIDtests.gov, that allows 4 at-home SARS-CoV-2 tests to be shipped to “valid residential addresses” at no cost. According to the site, orders usually will ship within 7-12 days—meaning they are not appropriate for people who need to be tested immediately—and will be delivered by the US Postal Service. The website’s launch comes 1 month after US President Joe Biden announced the government will obtain an additional 500 million free tests and 1 week after he doubled that number to 1 billion tests. White House officials noted a telephone hotline to request tests is also being established, with more information available at the end of this week. Additionally, most US residents with private insurance are now eligible to purchase tests online or in stores and have them covered at the time of purchase or be reimbursed by submitting a claim to their insurer. Only tests bought on or after January 15 are eligible, and insurers are required to pay for up to 8 tests per covered individual per month. Tests available for purchase online or in stores remain difficult to find in many areas of the country, and the Biden administration’s efforts to distribute tests and masks to millions are being viewed by some as a push to regain the trust of the American public in the federal pandemic response.
US VACCINE REQUIREMENTS The US Supreme Court last week issued opinions in response to 2 sets of cases involving federal SARS-CoV-2 vaccine requirements. In one unsigned opinion, the court halted the Biden administration’s enforcement of the Occupational Safety and Health Administration’s (OSHA) Emergency Temporary Standard (ETS) that would have required all workers at firms with 100 or more employees to either get vaccinated or be tested weekly and wear a mask to work (National Federation of Independent Business v. Department of Labor, No. 21A244). In a 6 to 3 decision, the justices concluded that OSHA overstepped its authority in issuing the requirement covering 84 million workers and issued a stay pending a decision from the US Court of Appeals for the Sixth Circuit. The stay undercuts one of US President Joe Biden’s most significant efforts to encourage widespread vaccination and leaves states and companies responsible for making their own policies. For example, Starbucks—which employs 228,000 people in the US—will no longer require employees to be vaccinated following the Supreme Court’s ruling. President Biden expressed disappointment over the court’s decision, saying that the “common sense life-saving requirements” are “grounded squarely in both science and the law.”
In a separate unsigned opinion, the Supreme Court allowed the Biden administration to continue enforcing a Centers for Medicare and Medicaid Services (CMS) regulation issued by the US Department of Health and Human Services (HHS) requiring vaccination for nearly all workers at hospitals, nursing homes, and other medical facilities that receive federal funds through Medicare and Medicaid (Biden v. Missouri, No. 21A240). The vote in that case was 5 to 4, with Chief Justice John G. Roberts Jr. and Associate Justice Brett M. Kavanaugh joining the liberal justices to form a majority. They concluded that the rule is necessary to protect the safety of patients and “is consistent with the fundamental principle of the medical profession: first, do no harm.” The court’s ruling overturns lower federal court injunctions in 2 dozen states, requiring that facilities participating in federally funded programs vaccinate their employees. Some concerns remain that the mandate will exacerbate existing staffing shortages, especially at some long-term care facilities and smaller rural hospitals.
TREATMENT DISPARITIES New research published in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) examines racial and ethnic disparities in the use of medications to treat COVID-19 cases within the US. The researchers looked at patient electronic health record data collected between March 2020 and August 2021 at 41 US healthcare systems. They focused on 3 main countermeasures used to treat patients with confirmed SARS-CoV-2 infection during that time period: monoclonal antibodies (mAb) delivered through intravenous infusion or subcutaneous injection, the steroid dexamethasone, and the antiviral remdesivir. Overall, mAb were rarely used to treat individuals with SARS-CoV-2 infection, but when administered, Hispanic patients received mAb 58% less often than did non-Hispanic patients, and Black, Asian, or Other race patients received mAb 22%, 48%, and 47% less often, respectively, than did White patients during November 2020-August 2021. The disparities were different and less pronounced for the other 2 treatments, with Black inpatients receiving remdesivir 9% more often than other racial groups and Hispanic patients receiving dexamethasone 6% more often than non-Hispanic groups. The researchers stressed the importance of better understanding this data and addressing gaps to build more equitable healthcare systems.
In an attempt to bridge these gaps, some states—including New York, Utah, and Minnesota—updated guidance to include formulations offering race as a preferential factor for receiving mAb treatment. However, at least Minnesota has dropped the scoring system that took race into account after the threat of a lawsuit. A fact sheet from the FDA also lists race and ethnicity as potential risk factors that may put patients at high risk for progression to severe COVID-19. That language has drawn criticism from some conservative US lawmakers.
BEIJING WINTER OLYMPICS China this week announced that tickets to the Beijing Winter Olympics will no longer be sold to the general public, with the announcement coming less than 2 days after health authorities detected the city’s first case of the SARS-CoV-2 Omicron variant of concern (VOC). Ticket sales already were limited to domestic spectators, and now will be further limited to certain approved groups that will need to undergo strict screening and quarantining measures. In a statement, the International Olympic Committee said the new rules were intended to “help create an absolutely safe environment for the athletes.” In recent weeks, China has switched from a “zero tolerance” approach to COVID-19 to a new “dynamic clearing” policy, which accepts that cases will happen and empowers local authorities to implement strategies to deal with them. However, the thinking behind the previous approach continues to prevail, with authorities taking aggressive steps to quell a series of outbreaks and more than 20 million people across the country in some stage of lockdown.
The highly transmissible Omicron variant poses a significant test to the country’s policies, especially after several studies have shown that the Chinese-produced vaccines from Sinovac Biotech and Sinopharm produce significantly lower neutralizing antibodies against Omicron than other major vaccines. Additionally, some evidence suggests that prior natural immunity gained from previous infection plus vaccination provides the most robust immune response to protect from severe disease. With low levels of natural immunity among China’s population, as well as weak health systems in some areas, hospitals could become overwhelmed if Omicron were to spread. Pfizer-BioNTech has licensed its vaccine to Shanghai Fosun Pharmaceutical Group, allowing the company to domestically manufacture the shots and the government to roll out a booster program using them. In the meantime, companies worldwide are preparing for continuing supply chain disruptions as Chinese officials continue to impose community- and citywide lockdowns.
ENGLAND British Prime Minister Boris Johnson announced on January 19 that all COVID-19 mitigation measures implemented under the government’s “Plan B”—including mandatory mask-wearing on public transportation and in retail shops and the use of vaccine certificates—will be dropped in England late next week. The guidance to work from home and the need for students to wear masks at secondary schools both ended immediately. Prime Minister Johnson noted England is moving back to “Plan A” due to the successful rollout of booster doses and what appeared to be a peak in the Omicron surge. Notably, while the number of new COVID-19 cases is dropping, the level still remains well above the previous high peak in January 2021. Scotland and Wales have also announced similar easing of mitigation measures. While the news was welcomed by many businesses, some teaching and health unions and public health representatives raised concern over the loosening of restrictions. Teachers warned that COVID-19-related disruptions continue at schools; National Health Service (NHS) officials cautioned that nearly 20,000 COVID-19 patients remain in hospital and the system is stretched thin; and health groups said the abrupt switch could send the wrong message to the public as more of a political move than one grounded in science. Indeed, Prime Minister Johnson is facing political challenges over allegations that he held several large events at Downing Street that breached lockdown policies.
TONGA While more continues to be learned about the devastation in Tonga after a massive volcanic eruption on January 15, life is beginning to return to normal on the main island of Tongatapu after it was covered in a thick coating of ash and hit by a tsunami resulting from the blast. As many as 150 homes were damaged or destroyed and at least 3 people were killed as a result of the eruption and tsunami. UN humanitarian flights have been delayed as ash is cleared from the airport runway, and aid agencies are working to coordinate delivery of aid without direct contact with residents. Tonga is a COVID-free zone, logging only one COVID-19 case during the pandemic, and fears are high that outside assistance—without the nation's mandatory 21-day quarantine—could bring the virus to the country, complicating recovery efforts. UN officials have noted that they are taking action to follow necessary protocols for entry into the country.
Also rolled back the school mask mandate and the state employee vaccine mandate on his first day in office.
Avoidable sickness and death are fine though, cause these kids ain't got to learn anything about racism.
by ti-amie Nothing is ever real until it happens to them. And once it happens to them heaven help you if you ask why they're for Program A now. You'll get a word salad of "we have to look out for each other" and so on.
by ponchi101 Well. Republicans have zero empathy. They are fairly sociopathic in that aspect. Unless it happens to them, directly, nothing matters.
by Deuce It's certainly not only Republicans. This is very common among all politicians. Unless they are directly affected by it - be it COVID, homelessness, drug abuse, alcoholism, spousal abuse, incest - what have you... until it becomes part of THEIR life, they simply don't care.
This is the rule for politicians everywhere. Sure, there are exceptions to every rule - but for all intents and purposes, no matter how they market themselves, politicians are extremely self-serving.
by JazzNU
ponchi101 wrote: ↑Sat Jan 22, 2022 10:36 pm
Well. Republicans have zero empathy. They are fairly sociopathic in that aspect. Unless it happens to them, directly, nothing matters.
He's a Democrat FYI, that's why there was a mask mandate in the first place. With few exceptions (Jacksonville is one), bigger cities typically have Democratic mayors.
I think this was a very phrased poorly Tweet honestly after watching the video. The video doesn't draw a correlation between keeping the mandate and his kid having covid. I'm sure it strengthened his resolve, but not sure it's much more than that. The mask mandate in Kansas City schools has been there, Missouri's AG has been out for them.
by ponchi101 Thanks for the correction. I assumed KC = GOP.
by JazzNU
by ti-amie
Like night follows day...
by JazzNU I find myself having the most un-Christian thoughts every time I see something new from him....
by dryrunguy Here's the latest Situation Report. The last section on shifts in vaccine hesitancy is interesting.
::
GLOBAL VACCINE & TREATMENT ACCESS The COVID-19 pandemic is at a critical stage, and it is dangerous for the world to assume “we are in the endgame,” WHO Director-General Dr. Tedros Adhanom Ghebreyesus warned at the opening of a WHO Executive Board meeting on January 24. The conditions are ideal for new variants to emerge, but the world can end the acute phase of the pandemic this year by achieving the target of vaccinating 70% of each nation’s population and improving testing and surveillance, Dr. Tedros encouraged. Globally, at least 5.6 million people have died of COVID-19 as the pandemic enters its third year, but only about 10% of people in low-income countries have received at least 1 dose of vaccine.
The global vaccine sharing scheme COVAX announced last week that it has delivered 1 billion SARS-CoV-2 vaccine doses to 144 countries, only half of its goal to deliver 2 billion doses by the end of 2021. The scheme was hampered by wealthier nations’ hoarding of the shots, export restrictions, and numerous changes within the organization. Gavi, the Vaccine Alliance and other partners in the initiative last week warned that COVAX is “basically out of money” and needs at least US$5.2 billion in new funding over the next 3 months to support the quick rollout of already-donated doses and to purchase more vaccines. Leading African public health authorities recently called for donated shots to have a shelf life of at least 3 to 6 months to allow countries time to plan distribution and avoid situations where the doses expire. According to the Africa Centres for Disease Control and Prevention (Africa CDC), approximately 0.5% of the 572 million doses delivered to the continent so far have expired before being administered. Efforts continue to increase vaccine manufacturing in Africa. Last week, South African-American businessman Dr. Patrick Soon-Shiong opened a new vaccine plant in Cape Town to address the lack of capacity.
The Africa CDC said it also is in talks with pharmaceutical companies to increase supplies of COVID-19 treatments. Merck and Ridgeback Biotherapeutics, which make the antiviral molnupiravir, last week said they will provide 3 million courses of the drug to UNICEF for use in low- and middle-income countries (LMICs) throughout the first half of this year. In another development, the Medicines Patent Pool announced agreements with 27 generic drug manufacturers in Africa, Asia, and the Middle East to produce low-cost versions of molnupiravir for use by LMICs. The consumer advocacy group Public Citizen sent a letter to Pfizer on January 24, asking the company to commit to reserve at least two-thirds of its annual supply of the COVID-19 treatment Paxlovid for LMICs, to be purchased at lower prices. Public Citizen said it is trying to discourage a repeat of vaccine inequity as newer treatments become available.
The Center for Health Security is hosting a webinar on Thursday, January 27 at 1pm on this topic. Please join us for Protecting U.S. National Security by Increasing Vaccination Globally.
BOOSTER DOSES Several new peer-reviewed studies provide additional evidence that SARS-CoV-2 vaccine booster doses elicit antibody responses that help protect against severe disease from the Omicron variant. Two of the studies were published in the US CDC’s Morbidity and Mortality Weekly Report (MMWR). The first study examined data on hospitalizations and emergency room and urgent care center visits in 10 states from August 2021 to January 2022, spanning both Delta- and Omicron-predominant periods. In that study, researchers found that vaccine effectiveness (VE) of the 2-dose mRNA vaccine regimens dropped around 6 months after the second dose, during both periods. However, VE increased following a third dose of mRNA vaccine during both waves and was highly protective against emergency room and urgent care encounters (94% during Delta and 82% during Omicron) and hospitalization (94% and 90%, respectively). A second study examined incidence and death rates between April and December 2021, again across both Delta- and Omicron-predominant periods, among unvaccinated and fully vaccinated adults with and without booster doses. In 25 US states, individuals who had received a booster dose of mRNA vaccine had the highest protection against SARS-CoV-2 infection across both periods when compared to unvaccinated and vaccinated but unboosted individuals.
Another study, published in the Journal of the American Medical Association (JAMA) and led by CDC researchers, examined data collected from 4,666 COVID-19 testing sites across 49 US states between December 10, 2021, and January 1, 2022. The findings show that individuals who had 3 doses of vaccine were better protected against both Omicron and Delta variants when compared with those who were unvaccinated and with those who received only 2 vaccine doses, although higher odds ratios for Omicron suggest less protection for Omicron than for Delta. Yet another study, published online in The Lancet, funded by the Brazil Ministry of Health, and conducted by researchers from Brazil and the University of Oxford, shows that a third booster dose of the Oxford-AstraZeneca, Pfizer-BioNTech, J&J-Janssen, or Sinovac (CoronaVac) SARS-CoV-2 vaccines induces a significant increase in antibody levels among individuals who previously received 2 doses of the Sinovac vaccine. The researchers note that the most robust responses were seen in those who received heterologous (mixed) boosters, a finding that could be most relevant to older populations.
The studies released by the CDC represent the most comprehensive data to date on the impact of booster doses in the US during the pandemic. The data from these reports also indicate that booster doses of the mRNA vaccines provide the most benefit to adults older than 50 years. However, uptake of booster doses has started to slow since the initial days of the Omicron wave despite advice from public health officials to stay “up to date” on vaccinations and recent evidence showing the boosters help prevent severe disease caused by Omicron. In updated data on breakthrough cases, the CDC notes that in November 2021, unvaccinated adults had 13 times the risk of testing positive for SARS-CoV-2 and 68 times the risk of dying from COVID-19 compared with fully vaccinated adults with booster doses.
VACCINE FOR UNDER-5 CHILDREN Many in the US continue to eagerly wait for the authorization of a SARS-CoV-2 vaccine for children under age 5. White House Chief Medical Advisor Dr. Anthony Fauci said last week he hopes the US FDA will soon authorize a vaccine for the youngest children, perhaps within the next month. More than 250 physicians recently sent a letter to the FDA concerning the issue and suggesting 2 options to expedite the process, such as joint decision making for parents and physicians to immunize children with off-label use of the Pfizer-BioNTech 10 μg dose vaccine formulation or removing the age de-escalation barrier to vaccine approval. The letter also urges the FDA to review and authorize the Moderna vaccine for children aged 6 months to 5 years as soon as data become available showing the vaccine is safe and effective, arguing the Moderna vaccine offers better protection against the Omicron variant and severe disease than other vaccines. Pfizer-BioNTech in December announced their plans to submit data to the FDA on a 3-dose study in the first half of 2022, after initial trials of the 3 μg 2-dose regimen given to 2- to 4-year olds did not produce as much of an immune response as it did in other age groups.
The American Academy of Pediatrics reports that, based on state-level data, the number of pediatric cases during the Omicron surge has drastically risen to nearly 5 times the rate of the peak of last winter’s surge. Parents continue to struggle with efforts to keep their children safe, stuck in limbo between daycare closures and child care crises. According to an analysis from the Center for the Study of Child Care Employment, 110,00 fewer people are working in childcare now than in February 2020. Outside of COVID-19 fears, some parents might take solace knowing that the rates of pediatric hospitalizations for other types of infections fell dramatically during the pandemic in England, including a 94% reduction in influenza-related hospitalizations, 90% reduction in measles-related hospitalizations, and an 82% drop in bronchitis-related hospitalizations in children under 14 years of age from March 1, 2020 to June 30, 2021 compared to March 1, 2017 to February 20, 2020. The researchers at the University of Oxford attribute the decreases to a range of behavioral and societal changes implemented to reduce transmission of SARS-CoV-2 and urge continued monitoring of other infections as COVID-19 mitigation strategies evolve. It is not clear whether similar reductions occurred in the US.
OMICRON-SPECIFIC VACCINES Though current SARS-CoV-2 vaccines continue to offer protection against severe COVID-19 disease and death, vaccine manufacturers are working to update the shots to hopefully provide better protection against the Omicron variant. Pfizer and BioNTech announced today they have begun a study to evaluate a SARS-CoV-2 vaccine based on the Omicron variant among adults aged 18 to 55 years. The study will enroll up to 1,420 healthy adults to test the Omicron-based shot as an initial (third shot) or secondary (fourth shot) booster dose or as primary vaccinations in previously unvaccinated individuals.
According to reporting from STAT News, a senior US FDA official said that if the agency moves to update vaccines to better confront Omicron or other variants, it will likely participate in an internationally coordinated program with other regulatory agencies and the WHO to decide if, when, or how to update the shots. The program could operate in a similar way to the one already in place to decide which strains to include in influenza vaccines, the unnamed official said. Even with Pfizer-BioNTech expecting to apply for authorization of an Omicron-specific vaccine by the end of March, the current surge in cases is already waning in Africa, Europe, and the US, suggesting it could end within or close to that timeframe. And while Omicron might remain the globally predominant strain, it is possible future variants will emerge with potentially very different mutations. Already, scientists are tracking an Omicron subvariant called BA.2, which has some new mutations, including several on the spike protein. The variant is not viewed as a “gamechanger,” but it already accounts for most new cases in India, Sweden, and Denmark and has been detected in the US.
COVID-19 THERAPIES On January 24, the US FDA revised the emergency use authorizations (EUAs) for 2 monoclonal antibody treatments—bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab)—to restrict their use to only when a patient is likely to have been infected with or exposed to a variant that is susceptible to these therapies. The treatments have been shown to be highly unlikely to be effective against the Omicron variant of concern (VOC), and because that VOC is currently responsible for more than 99% of COVID-19 cases in the US, “these treatments are not authorized for use in any US states, territories, and jurisdictions at this time,” the FDA said in a statement. As a result, the US Department of Health and Human Services (HHS) has halted distribution of the therapies. However, the therapies could be useful in certain geographic regions or against new variants in the future. The FDA noted other therapies are available and expected to work against Omicron, including the monoclonal antibody sotrovimab, and the antivirals Paxlovid, remdesivir (Veklury), and molnupiravir.
Late last week, the FDA expanded the EUA for the COVID-19 treatment remdesivir to include certain non-hospitalized adults and pediatric patients ages 12 and older with mild-to-moderate disease. Previously, the use of the intravenous antiviral was limited to hospitalized patients. Additionally, the FDA authorized the drug’s use for pediatric patients younger than 12 years of age who weigh at least 3.5 kg but under 40 kg who are at high risk for progression to severe COVID-19, including hospitalization or death. A 3-day course of the drug is recommended as a third option behind the oral antiviral Paxlovid and sotrovimab. A 5-day course of remdesivir is recommended for hospitalized patients who are not on mechanical ventilation or extracorporeal membrane oxygenation (ECMO), while critically ill hospitalized patients should receive a 10-day course.
US VACCINE REQUIREMENTS On January 21, a federal judge in Texas issued a nationwide injunction against US President Joe Biden’s SARS-CoV-2 vaccine requirements for federal government employees, saying the president had exceeded his executive authority in issuing the rule. US District Judge Jeffrey Vincent Brown cited a recent US Supreme Court opinion blocking a different federal rule that would have required employees of companies with 100 or more workers to be vaccinated or submit weekly testing. Notably, the Supreme Court allowed a separate vaccine rule pertaining to workers at medical facilities that receive Medicare or Medicaid funding to remain in force. The US Department of Justice immediately filed notice that it plans to appeal the decision to the US Court of Appeals for the 5th Circuit. The case likely will go to the Supreme Court. At the beginning of December 2021, the Office of Management and Budget said 97.2% of the federal workforce was compliant with the rule, including those who had pending or approved exemptions. The plaintiff in the case, a Nevada-based group called Feds for Medical Freedom, also asked the judge to enjoin the rule applying to federal contractors, but that executive order is already subject to a nationwide injunction. Over the weekend, thousands of anti-vaccination protestors gathered in Washington, DC, for a rally against vaccine mandates.
VACCINE HESITANCY The results of a survey of 1,200 US adults led by researchers from the Ohio State University and published in JAMA Network Open found that vaccine hesitancy has decreased more rapidly among Black individuals than White individuals since December 2020. Hesitancy rates were comparable at the start of the survey, but Black individuals experienced larger increases in intention to vaccinate than White individuals relative to baseline. The belief that vaccines were necessary for protection also increased more among Black individuals than White individuals. The new survey data showing declines in hesitancy among Black individuals suggest there may be other factors to consider, including barriers to access. The study’s discussion notes Kaiser Family Foundation surveys that document the substantial portion of Black individuals who worry about access barriers. For example, 55% of Black individuals (vs 41% of White individuals) are very or somewhat concerned about missing work if the vaccine makes them sick; 37% of Black individuals (vs 24% of White individuals) worry they will have to pay for the vaccine; 23% of Black individuals (vs 16% of White individuals) are concerned about taking time off of work to get vaccinated; and 17% of Black individuals (vs 9% of White individuals) worry about finding transportation to vaccination sites. Though the administration of US President Joe Biden has taken some steps to alleviate such barriers—including paid sick leave and free Uber and Lyft rides to vaccination sites—some people remain unaware of these programs.
by dryrunguy Here's the latest Situation Report. The big news? It turns out COVID infection likely decreases sperm quality--at least in the short term. This also marks the first time I have seen experts linking long COVID to the need to expand our thinking as to what constitutes long-term disability. I'm surprised it took so long.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 357 million cumulative cases and 5.61 million deaths worldwide as of January 26. Global weekly incidence increased again last week, up 11.03% over the previous week. This is the 14th consecutive week of increasing weekly incidence, setting another new record with 22.77 million new cases. The Omicron variant drove the greatest percentage increases in the WHO regions of Eastern Mediterranean (+38.58%), South-East Asia (+36.05%), Europe (+19.29%), and the Western Pacific (+1.26%). Both Africa (-31.04%) and the Americas (-2.01%) experienced declines in weekly incidence.
While there is optimism among some public health experts that the rapid rise and fall of the Omicron surge in some regions could usher in an end to the pandemic, the WHO determined last week that the COVID-19 pandemic continues to constitute a Public Health Emergency of International Concern (PHEIC). Other experts warn that as long as the threat of new variants exists, calls for reaching COVID-19 endemicity are misguided.
Meanwhile, global weekly mortality increased for the third week, up 8.49% from the previous week with 53,935 total deaths. The Pan American Health Organization (PAHO) on January 26 warned that the average number of COVID-19-related deaths is up 37% in the region over the previous week.
Global Vaccination
The WHO reported 9.68 billion cumulative doses of SARS-CoV-2 vaccines administered globally as of January 26. A total of 4.7 billion individuals have received at least 1 dose, and 4.0 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decrease, down to 25.08 million on January 26 from a recent high of 38.88 million on December 23.* Our World in Data estimates that there are 4.78 billion vaccinated individuals worldwide (1+ dose; 60.79% of the global population) and 4.12 billion who are fully vaccinated (52.3% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 72.3 million cumulative cases of COVID-19 and 870,195 deaths. The US is averaging 627,294 new cases—down from 726,941 on January 20—and 2,246 deaths per day—up from 1,860 one week ago and at the highest level since mid-February 2021.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
COVID-19 hospitalizations in the US are down 7.7% this week over last, with a 7-day average of 19,640 new hospitalizations per day. The recent surge in current hospitalizations appears to have peaked around January 19, down 1.7% to an average of 142,194 for the week ending January 24. According to analysis from The New York Times, the overall downward trend in hospitalizations belies the reality in some regions, where the number of cases and hospitalizations continue to grow significantly.
US Vaccination
The US has administered 537.2 million cumulative doses of SARS-CoV-2 vaccines. The trend in daily vaccinations continues to decline, down significantly from a recent high of 1.77 million doses per day on December 6 to 760,975 on January 21.*
A total of 251.5 million individuals have received at least 1 vaccine dose, equivalent to 75.8% of the entire US population. Among adults, 87.6% have received at least 1 dose, as well as 25.3 million children under the age of 18. A total of 210.9 million individuals are fully vaccinated**, which corresponds to 63.5% of the total population. Approximately 73.9% of adults are fully vaccinated, as well as 19.9 million children under the age of 18. Since August 13, 85.2 million fully vaccinated individuals have received an additional or booster dose. An estimated 43.5% of fully vaccinated individuals have received a booster, including 63.3% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
GLOBAL VACCINE GAP US officials announced on January 26 that the government has shipped a total of 400 million SARS-CoV-2 vaccine doses to 112 countries, part of its efforts to fulfill its pledge to donate 1.2 billion doses. At a briefing, White House COVID-19 Coordinator Jeff Zients noted that the US has donated 4 times more doses than any other country. Still, 5 billion to 6 billion doses are needed in low- and middle-income countries to help protect them against COVID-19, and vaccine access gaps in those areas create fertile grounds for the emergence of new, possibly more dangerous, SARS-CoV-2 variants, the WHO has warned. The divide is stark: about 78% of people in high- and upper-middle-income countries have received at least one dose of vaccine compared with about 10% in low-income nations. According to calculations from the International Monetary Fund (IMF), 86 of 206 countries had immunized less than 40% of their populations as of the end of 2021, far from the fund’s goal of vaccinating 70% of the world’s population in the first half of this year. Experts agree that vaccine inequities led to the emergence of the Omicron variant and warn of future variants if a concerted global effort is not undertaken to manufacture, distribute, and administer more vaccines to prevent the virus from circulating among the unvaccinated. A group of Democratic US lawmakers is calling for the government to immediately provide an additional US$17 billion for global vaccination delivery and infrastructure and to streamline federal efforts to coordinate the nation’s global COVID-19 strategy. Some experts say additional funding could be useful but drumming up international political will is more important. Others warn the next variant—if it is capable of immune evasion—could be like starting from scratch.
US HEALTHCARE UTILIZATION The Omicron variant of concern (VOC) has caused massive surges in COVID-19 cases and, subsequently, in people seeking healthcare. A recent study published in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) examined hospital-associated disease severity markers, including ICU admissions, length of stay, and death. The study found that disease severity, measured by US healthcare utilization, appeared to be lower during the Omicron VOC surge compared to both the Delta VOC surge and the previous winter season. ICU admissions during the beginning of the Omicron surge were 26% lower and 29% lower than during the Delta and winter 2020-2021 surges, respectively. Mean length of hospital stay was also comparatively lower. However, due to the massive number of positive cases, overall staffed hospital bed usage was 7% higher than during Delta and 3% higher than during winter 2020-2021.
The study was not able to directly assess the impact that vaccines had on disease severity markers or hospital stay lengths, but the authors posit that decreased admissions to the ICU and lower overall hospital stays during the Omicron surge can likely be attributed to higher vaccine coverage as well as higher levels of infection-acquired immunity. Supporting this hypothesis, high relative increases in hospital admittance were only observed in children 0- to 4-years-old who are currently not eligible for vaccination. Although people infected with Omicron appeared to require less intensive care at the hospital level, the sheer number of cases and burden on the healthcare system overall required significant resources and resulted in severe strain. The authors state that this analysis “underscores the importance of national emergency preparedness, specifically, hospital surge capacity and the ability to adequately staff local health care systems.”
HEALTHCARE WORKER BURNOUT As the world enters its third year of response to the COVID-19 pandemic, burnout in the global healthcare workforce continues to grow. In the US, a rapid increase in the number of COVID-19 cases due to the Omicron variant of concern (VOC) has led to a record surge of individuals requiring medical attention across healthcare settings. In California, hospitals have canceled operations and other elective procedures and ambulances have experienced backlogs for patient delivery. Healthcare professionals warn that the continued high intensity of care, a limited amount of life-saving countermeasures, and a large number of staff out sick are creating a continuously stressful work environment. Notably, the country has experienced a mass exodus of healthcare workers. In the Southern US, this trend has hit nonprofit safety-net hospitals particularly hard, reducing the capacity of necessary resources for many throughout the region. Earlier this year, the US Department of Health and Human Services (HHS) announced that US$103 million of funding from the American Rescue Plan will be committed to strengthening resilience and addressing burnout in the domestic healthcare workforce. However, STAT reports that another fund meant to support hospitals and clinics during the pandemic has run out of money, after the Biden administration quietly redirected nearly US$7 billion from the fund and used it to buy SARS-CoV-2 vaccines and therapeutics.
Workforce mental health issues are not exclusive to the US. Researchers in Canada analyzed anonymous data from 34,000 physicians working in Ontario. The analysis found a 27% increase in the number of doctors seeking care for burnout or substance misuse in the first year of the pandemic compared with the prior year. Burnout of nurses and other healthcare professionals is a universal issue and has led to wealthier countries recruiting healthcare workers from other less-wealthy countries. This phenomenon has intensified during the Omicron surge, raising many questions about the ethics of the practice.
US VACCINE REQUIREMENTS FOR LARGE EMPLOYERS The US Department of Labor’s Occupational Safety and Health Administration (OSHA) on January 25 withdrew its emergency temporary standard (ETS) that called for employers with 100 or more workers to require their employees to be vaccinated for COVID-19 or undergo regular testing and wear face masks while at work. The withdrawal, which took effect January 26, follows the US Supreme Court’s January 13 opinion that halted enforcement of the rule. In a 6 to 3 decision, the justices concluded that OSHA overstepped its authority in issuing the requirement covering 84 million workers and issued a stay pending a decision from the US Court of Appeals for the Sixth Circuit. Though OSHA withdrew the requirement as an enforceable emergency regulation, the agency said it is maintaining the ETS as a proposed rule. On its website, OSHA stated it is “prioritizing its resources to focus on finalizing a permanent Healthcare Standard” and that it continues to “strongly encourage” workers to be vaccinated.
ISRAEL Israel’s Ministry of Health on January 25 said its vaccine advisory panel has recommended making all adults eligible to receive a fourth dose of SARS-CoV-2 vaccine. If the ministry approves the recommendation, it would be the first country in the world to make a fourth vaccine dose available to all adults. Israel already offers fourth doses to people aged 60 and older, healthcare workers, and people with compromised immune systems. About 600,000 Israelis have already received a fourth dose. Over the weekend, the health ministry shared preliminary data from its own researchers suggesting a fourth dose provides 3 to 5 times as much protection against severe disease in older adults when compared with those in the same age group who had received a booster dose at least 4 months prior. It is not clear when the ministry’s director-general will decide on the panel’s recommendation. Israel is in the midst of a surge in new COVID-19 cases driven by the Omicron variant.
POST-ACUTE SEQUELAE Researchers continue work to learn more about the clinical presentation and duration of persistent symptoms of SARS-CoV-2 infection, known as post-acute sequelae of COVID-19 (PASC) or “long COVID.” Prevalence of the condition—which is characterized by fatigue, shortness of breath, brain fog, stress and anxiety, and other symptoms that last for weeks or years after acute infection—is unknown but estimated to be between 7% to 80% of recovered patients. A study published this week in Cell suggests an association between the development of long COVID and 4 factors, including the presence of certain autoantibodies that mistakenly turn on the body’s own tissues, reactivation of previous Epstein-Barr virus infection, viral load levels in early infection, and having Type 2 diabetes. Because 2 of the factors are virus levels in the blood, the researchers speculate that antiviral administration early in SARS-CoV-2 infection might help lower the risk of longer-lasting symptoms in some people. However, authorized antivirals in the US are in very short supply and difficult to obtain. Additionally, preliminary data from Israel and the UK suggest that people who were fully vaccinated when infected were much less likely to report long COVID symptoms than people who were unvaccinated when infected. Other studies are looking at ways to predict who might be at risk of long COVID and underlying causes of the condition.
In the US, 2 Democratic lawmakers this week sent a letter to the US CDC requesting the agency release data on the number of Americans with long COVID, including information on race, gender, and age. The lawmakers, healthcare providers, and experts nationwide say more data are needed on how many people suffer from long-term symptoms in order to better target resources and provide a more equitable recovery from the pandemic. A recent article published in Nature Medicine examined inequities in understanding and addressing neurological complications of COVID-19 among marginalized US communities, with the authors calling for more equity in COVID-19 research and “a dismantling of structural barriers that perpetuate disparities in clinical care.” Advocates and health experts are pressuring the government for more attention on long COVID, including greater financial assistance, access to disability benefits, and improved healthcare. The US National Institutes of Health (NIH) early last year launched an initiative to identify the causes and means of prevention and treatment of long COVID, but the research is expected to take years. Some say the condition could be contributing to a worker shortage in the US, with a recent analysis from the Brookings Institution estimating that long COVID could account for 15% of the nation’s 10.6 million unfilled jobs.
VACCINATION & FERTILITY New research provides evidence that SARS-CoV-2 vaccination has no negative impact on reproduction—whether conception is achieved through heterosexual intercourse or in vitro fertilization—but men who become infected with the virus appear to have a short-term decline in fertility. In a study published in the American Journal of Epidemiology, researchers from the Boston University School of Public Health found no association between vaccination of males or females with any of the vaccines available in the US—Pfizer-BioNTech, Moderna, or J&J-Janssen—and the likelihood of conception, with fertility rates among female participants with at least 1 dose of vaccine almost identical to rates among unvaccinated female participants. In the same study, researchers report that men who tested positive for SARS-CoV-2 within 60 days of a woman’s menstrual cycle had reduced fertility when compared with men who never tested positive or who tested positive at least 60 days prior to the cycle. Previous research has linked COVID-19 in men to poor sperm quality and other reproductive dysfunction. A separate study, published in Obstetrics & Gynecology, showed that IVF patients who were vaccinated had similar fertilization rates compared with unvaccinated patients after undergoing controlled ovarian hyperstimulation, single frozen-thawed embryo transfer, and other procedures such as egg or mature oocyte retrieval. Additionally, both groups had similar rates of early pregnancy loss. These studies provide further evidence that SARS-CoV-2 vaccination is safe for people who are trying to conceive. The CDC and other medical groups recommend all people trying to become pregnant to get vaccinated.
Separate studies—including one conducted in the US and another in Norway—showed that vaccination can change menstruation cycles, but the impacts are short-lived and small when compared to natural variation. All of the data should be reassuring to pregnant people and those trying to become pregnant as well as the approximately two-thirds of US parents who cite future fertility as a concern when it comes to vaccinating younger children ages 5 to 11. The vaccination rate among this latter cohort remains quite low in the US and the rates vary widely among US states.
OMICRON-SPECIFIC VACCINES Moderna announced on January 26 it has begun a Phase 2 clinical trial testing an Omicron variant-specific booster candidate. The study will evaluate the booster in 2 cohorts of participants: individuals who received the 2-dose primary series of the company’s mRNA vaccine and individuals who received the primary series plus a 50 µg booster dose. Moderna also announced the publication of neutralizing antibody data against the Omicron variant 6 months after receipt of the authorized booster dose. The study, published in the New England Journal of Medicine (NEJM), shows that the authorized 50 µg booster dose increased Omicron neutralizing titers to 20-fold higher than peak Omicron titers post-dose 2. However, 6 months later, Omicron neutralization declined 6.3-fold from peak titers at day 29 post-boost but remained detectable in all participants. Neutralizing titers against Omicron declined faster after the booster than for the wild-type virus.
dryrunguy wrote: ↑Thu Jan 27, 2022 6:25 pm
Here's the latest Situation Report. The big news? It turns out COVID infection likely decreases sperm quality--at least in the short term. This also marks the first time I have seen experts linking long COVID to the need to expand our thinking as to what constitutes long-term disability. I'm surprised it took so long.
::
...
Not putting you on, but a serious question: how would you define long term disability? What would constitute one?
dryrunguy wrote: ↑Thu Jan 27, 2022 6:25 pm
Here's the latest Situation Report. The big news? It turns out COVID infection likely decreases sperm quality--at least in the short term. This also marks the first time I have seen experts linking long COVID to the need to expand our thinking as to what constitutes long-term disability. I'm surprised it took so long.
::
...
Not putting you on, but a serious question: how would you define long term disability? What would constitute one?
No, it's a good question.
The answer is... I'm not sure. I know how it worked for dolphins. He collapsed at work in 2011. They thought it was a cardiac episode at first, but tests confirmed that it was related to his blood pressure. Then, it turned out his blood pressure was related to degenerative disc disease.
He applied for disability because he could no longer work. It simply wasn't possible. His disability was denied at first. That took several months.
Then we hired an attorney. Several months later, dolphins appeared with his attorney before the administrative law judge with the fourth highest denial rate in the Commonwealth of Pennsylvania. The hearing was scheduled for 30 minutes.
Dolphins was out of there in 10 minutes. Disability approved, including all back benefits from the time he applied. (Almost all of which went to the attorney.)
::
Now, back to your question... If you can't work, and the likelihood that you could ever return to work is pretty low, then you deserve disability. How do you define that? I don't know. And the internet is full of videos of disabled people doing all sorts of physical activities. Some of that criticism is legitimate. But at other times, is there really something wrong with a person who can't do manual things 6 days a week doing something manual on the 7th day? When they are feeling pretty good?
As it relates to COVID, I don't think we really know how it applies. The evidence suggests long COVID can linger for months or years. (We're not yet 2 years into the pandemic. So what does "years" mean?)
But in the end, I suspect we'll have a very large number of people with long COVID who will never work again--nor should they. It would be either impossible or dangerous.
And then you'll have a lot of people diagnosed with long COVID that actually get better, but they'll try to abuse the system as it relates to disability to avoid work.
And then you'll have a lot of people who have long COVID, refuse to apply for disability (maybe because of pride, maybe because of refusal to apply for "assistance"), continue to work, perform poorly because they really can't work, and get fired. What happens next? Not sure.
And then you'll have a lot of people with long COVID who continue to work, get injured or have poor health outcomes, and then sue their employers for workers' compensation when really the problem was long COVID.
::
Those are just a few scenarios. The possibilities are endless.
Ponchi, did I answer your question? Or just muddy the waters? But yes, I know from personal experience that long-term/permanent disability is a real thing. I see it every day.
dryrunguy wrote: ↑Thu Jan 27, 2022 6:25 pm
Here's the latest Situation Report. The big news? It turns out COVID infection likely decreases sperm quality--at least in the short term. This also marks the first time I have seen experts linking long COVID to the need to expand our thinking as to what constitutes long-term disability. I'm surprised it took so long.
::
...
Not putting you on, but a serious question: how would you define long term disability? What would constitute one?
Shorter answer...
If your body is such that you have to say to your employer, "Yes, I can physically work. Some days. I'll let you know when those days are. On those days," then you're probably a good candidate for long-term disability.
Obviously, I'm not talking about days when you are physically able to work but just don't feel like it.
Ponchi, did I answer your question? Or just muddy the waters? But yes, I know from personal experience that long-term/permanent disability is a real thing. I see it every day.
I don't think is a question that can be answered algorithmically. You know, if you have A and B, but C is suspect, go to D...
That was the reason I was asking. Taking an extreme example: Stephen Hawkins. The man was clearly disabled, yet he led a very productive life because he had special abilities that were suited for his line of work. And then I bet we all know that friend or person that is physically in perfect conditions, yet really can't work at anything.
That was the reason I was asking. Your exposition is very helpful but, as you say, there is not one metric.
by JazzNU They've needed to expand the definition of long term disability for a long time, so that would be a very positive development out of all of this mess and hopefully it wouldn't just be about covid because the general things they list are among those that people struggle getting approved for. Which also makes me skeptical many changes will happen.
Short term disability tends to be one or two weeks to 6 months and then long term disability is longer than 6 months. The length of time depends on your employee benefits basically.
What @dry is talking about is SSDI, which are governmental benefits for those that are disabled long term. Administered by Social Security Administration. Eligible to those that have worked for a certain period of time and paid into SS.
There are many things that qualify someone for disability, but the general idea is that they are too sick to work, that they have a medically verifiable ailment or physical or mental impairment that severely limits their daily activity and ability to work. For SSDI/SSI, there are some diagnoses that get presumptively approved, diseases with outlooks so poor, they'll basically be rubber stamped.
As for @dry's story of getting Dolphins disability. Disability denial rates in appeals are vastly, and I do mean vastly, different for those that hire an attorney and those that skip them. So let this be a PSA for anyone that doesn't know this - Always hire an attorney if you need it to be approved for SSDI the first time you appeal, don't go through the motions thinking you'll figure it out on your own if time is of the essence. If you can afford to wait, you might be able to save some money, assuming you get approved on your own. But it will never be that expensive, there are SSA rules capping the amounts you have to pay disability attorneys and you don't have to pay them upfront. So, it's good to think of the mental toll in addition to what you would save. It's a stressful process for many especially dealing with the denials and appeals, so drawing it out may not be worth the savings for some
by JazzNU
ponchi101 wrote: ↑Fri Jan 28, 2022 4:10 am
I don't think is a question that can be answered algorithmically. You know, if you have A and B, but C is suspect, go to D...
That was the reason I was asking. Taking an extreme example: Stephen Hawkins. The man was clearly disabled, yet he led a very productive life because he had special abilities that were suited for his line of work. And then I bet we all know that friend or person that is physically in perfect conditions, yet really can't work at anything.
That was the reason I was asking. Your exposition is very helpful but, as you say, there is not one metric.
ALS is one of the conditions that gets approved quickly. But Stephen wouldn't have qualified because he was working, there are rules on what you can earn if you're on SSDI/SSI. Many, many disabled persons work, so it's not just the disease, but how it limits your overall livelihood. As for people in perfect physical condition and not being able to work, assuming you don't mean someone with a mental illness that is severely limiting their daily life, that person is unlikely to get approved for SSDI/SSI. It takes a lot of verifiable information to get approved. And the SSA will happily prosecute anyone if they attempt to defraud them. Happily. They've got thousands devoted to it. So if anyone's goal is to spend several months to a few years in federal prison, this is a good way to go about it.
by ponchi101 I was only using Hawkins as an example of a disabled person that was still very productive, just to be clear. All your points are very valid (you are obviously more versed on the subject than I am) but I am in this conversation as a listener.
So thanks
by dryrunguy
JazzNU wrote: ↑Fri Jan 28, 2022 4:12 am
They've needed to expand the definition of long term disability for a long time, so that would be a very positive development out of all of this mess and hopefully it wouldn't just be about covid because the general things they list are among those that people struggle getting approved for. Which also makes me skeptical many changes will happen.
Short term disability tends to be one or two weeks to 6 months and then long term disability is longer than 6 months. The length of time depends on your employee benefits basically.
What @dry is talking about is SSDI, which are governmental benefits for those that are disabled long term. Administered by Social Security Administration. Eligible to those that have worked for a certain period of time and paid into SS.
There are many things that qualify someone for disability, but the general idea is that they are too sick to work, that they have a medically verifiable ailment or physical or mental impairment that severely limits their daily activity and ability to work. For SSDI/SSI, there are some diagnoses that get presumptively approved, diseases with outlooks so poor, they'll basically be rubber stamped.
As for @dry's story of getting Dolphins disability. Disability denial rates in appeals are vastly, and I do mean vastly, different for those that hire an attorney and those that skip them. So let this be a PSA for anyone that doesn't know this - Always hire an attorney if you need it to be approved for SSDI the first time you appeal, don't go through the motions thinking you'll figure it out on your own if time is of the essence. If you can afford to wait, you might be able to save some money, assuming you get approved on your own. But it will never be that expensive, there are SSA rules capping the amounts you have to pay disability attorneys and you don't have to pay them upfront. So, it's good to think of the mental toll in addition to what you would save. It's a stressful process for many especially dealing with the denials and appeals, so drawing it out may not be worth the savings for some
Just to clarify, dolphins doesn't get SSDI. He gets Social Security and Medicare. He made too much as a worker to qualify for SSDI. As you know, qualifying for disability and qualifying for SSDI are two different things.
A coal miner in West Virginia experiencing long COVID who earned a modest salary would probably qualify for SSDI. Dolphins made decent coin before all hell broke loose. And that's why he doesn't qualify for SSDI. He receives the maximum benefit possible. And what he gets is enough to cover his bills.
But the story for a lot of other people is quite different.
by dryrunguy That said, should people who experience long COVID who weren't vaccinated be punished when it comes to receiving disability benefits associated with long COVID?
I really struggle with that question.
by ponchi101 Indeed. It opens the door for people that have made bad choices in their lives (i.e. smoking) and get affected by that.
Punishing idiocy would a bad precedent.
by JazzNU
dryrunguy wrote: ↑Fri Jan 28, 2022 6:27 am
Just to clarify, dolphins doesn't get SSDI. He gets Social Security and Medicare. He made too much as a worker to qualify for SSDI. As you know, qualifying for disability and qualifying for SSDI are two different things.
A coal miner in West Virginia experiencing long COVID who earned a modest salary would probably qualify for SSDI. Dolphins made decent coin before all hell broke loose. And that's why he doesn't qualify for SSDI. He receives the maximum benefit possible. And what he gets is enough to cover his bills.
But the story for a lot of other people is quite different.
SSDI doesn't have an income qualification, it's essentially getting your Social Security benefits earlier once you are ruled to have a long term disability. SSI is what you're referring to, which is need-based and has different qualifying criteria. For instance, you can qualify even if you don't have the required work history with this one. Children with severe disabilities, the blind, they can qualify for SSI. Both administered by SSA.
by mmmm8 There is not only no definition (other than the general "incapacity to work"), there are not really any standards in most jurisdictions around the world. Although some conditions as noted are likely/likelier to be approved, whether by the government or private insurance, these vary by country/region (and by private insurer). And then of course the subjectivity of a bunch of people comes in from doctors to judges. One of the most difficult areas is mental health. Claims around this are increasing almost everywhere.
With some long COVID effects being kind of nebulous (brain fog, fatigue), good luck indeed figuring out how disability would apply.
by JazzNU That is why I'm skeptical. Not saying it's not good that some in Congress are looking into it because it is sure to have an effect on the numbers in the work force, but the problems listed in the report associated with long Covid - fatigue, shortness of breath, brain fog, stress and anxiety - typically have a much harder time with getting federal disability when there's not another diagnosis along with it. Much better chance at getting short or long term disability with your employer if your condition is debilitating. And maybe that's part of what they'll do, make certain private insurers are carving out broader definitions for disability to be approved. And if it's not permanent (something they can't possibly know right now), that might be a good solution because you'd hope that most of those suffering from long covid that aren't over retirement age would eventually return to their job or at least the workforce just as most do with other drawn out illnesses.
Gonna try to remain hopeful on this one, it would be a welcome change in general to be more open to what the definition of disability is. People tend to think it can only look a certain way unfortunately.
Somewhat related, there was a great thread on Twitter the other day of people posting about their chronic illnesses and pre-existing conditions to try to get people thinking differently about what someone who is at high risk for covid looks like. It went viral so a good number of people saw it and others started posting their own and those too went viral, but only time will tell if it has any effect in starting to change how people think about these things.
by ti-amie
by ti-amie
by JazzNU Those numbers are stark. And that's what Meat Loaf was facing as a 74 year old and why Howard Stern was advocating for his family to speak out about getting the vaccine. Saying you'd rather be free and die than get a vaccine, and now you're dead doesn't feel the flex these guys think it is. Or maybe it is, can't ask them cause they're dead.
by JazzNU
by JazzNU
by ti-amie It makes you wonder what the real situation is with police and vaccinations doesn't it?
by JazzNU
ti-amie wrote: ↑Mon Jan 31, 2022 6:49 pm
It makes you wonder what the real situation is with police and vaccinations doesn't it?
Police, fireman, EMT, and teachers. Highly suspect right now, especially those that got their shots in the final week or two or later on after their medical or religious exemption didn't get approved. Since they weren't just giving charging for fake cards but were also entering them into the state database, gotta start combing thru every record they entered. There must be a few thousand that ought to get fired off of this, I'm sure the actual number won't be that high, but I can dream.
by dryrunguy Here's the latest Situation Report. I kept seeing all sorts of references to Spotify over the weekend but didn't have the chance to look into it. Now I understand.
The section on the Omicron subvariants was interesting, too... That is, the speculation as to where these subvariants might originate and the possibility that existing vaccines may actually be more effective against one or more of these subvariants compared to previous variants. Science.
::
PANDEMIC VS ENDEMIC Even as the number of COVID-19 cases continue to reach record levels in some regions, those in the general public, members of the scientific community, and politicians are debating when the world can move on from the pandemic, arguments summarized as “pandemic vs endemic.” Some health officials from the US and Europe have recently expressed cautious optimism that their regions could be moving out of a pandemic state and into a period of endemic disease control, citing a different immunological landscape due to vaccination and previous infections, continued mitigation measures such as mask-wearing and testing, and newly available antiviral treatments. Other experts warn it is too soon to declare a pandemic endgame, saying global vaccination gaps and the threat of new, possibly more dangerous variants make predicting the pandemic’s path impossible. Still others are warning that endemicity does not mean COVID-19 becomes harmless, as other endemic diseases continue to cause substantial suffering and death. For example, HIV, malaria, and tuberculosis—all considered to be endemic in certain regions—continue to kill millions of people each year and, although relatively controlled in wealthy nations, linger in poorer, more vulnerable countries.
The surge of COVID-19 cases caused by the Omicron variant is beginning to recede in regions of the US hit first, but other areas of the nation continue to experience record numbers of hospitalizations and deaths, creating various pandemic scenarios nationwide. In Europe, Denmark lifted all of its remaining COVID-19 restrictions last week, the first country on the continent to do so, while other nations, such as the UK and Austria, also are relaxing their rules. Thailand on January 27 adopted guidelines outlining how COVID-19 could become an endemic disease, but officials said it likely will still be between 6 months to a year before the country reaches that point. Research from Malawi, supported by evidence from other countries, suggests that a very high prevalence of the population in several African nations have already been infected with SARS-CoV-2, providing high levels of natural immunity and possibly signaling endemicity. While it remains unclear how the pandemic will reach an end, scientists agree that there is a light at the end of the tunnel.
OMICRON BA.2 Only about 2 months from first being detected, the highly transmissible Omicron variant of the SARS-CoV-2 virus—the most common form of which is called BA.1—has become the predominant variant worldwide, accounting for nearly 99% of all sequenced cases as of the end of January. Scientists are now tracking a sublineage of the original Omicron variant known as BA.2, or “stealth Omicron,” as well as 2 other subvariants, BA.1.1529 and BA.3. A growing number of cases are being attributed to BA.2, including 82% of new cases in Denmark,* 9% in the UK, and 8% in the US. Though BA.2 appears to be even more transmissible than its cousin, according to a Danish study, vaccines remain effective—perhaps more so—against it than BA.1. The WHO has urged health agencies worldwide to begin investigating BA.2, and the US CDC last week said that while the subvariant is circulating at low levels in the country, there is no evidence it causes more severe disease than the BA.1 lineage.
In a study posted online last week on the preprint server bioRxiv, researchers describe unusual genetic mutations in Omicron’s BA.1 lineage and postulate that it likely evolved under unusual conditions, such as within the body of a person with a compromised immune system. The research—which suggests that Omicron developed over time and not in a stepwise fashion from the last variant, Delta—makes it clear that scientists are unable to predict how and where the next variant will evolve, nor whether it will be more transmissible or virulent.
*This high percentage could be attributable to Denmark’s robust sequencing program.
MODERNA VACCINE APPROVAL The US FDA on January 31 granted full approval to Moderna’s SARS-CoV-2 vaccine for the prevention of COVID-19 in adults aged 18 and older, the second such vaccine to receive approval in the US. The vaccine, to be marketed under the brand name Spikevax, is administered as 2 shots given 28 days apart and is the same formulation that has been available under emergency use authorization (EUA) since December 2020. The mRNA vaccine remains available under EUA as a third primary series dose for adults with certain types of immunocompromise and as a single booster dose for adults who originally received the same or different SARS-CoV-2 vaccine. Moderna’s vaccine—which is already licensed in several other countries and regions, including Canada, Japan, Israel, UK, and the EU—is the company’s first FDA-approved product. The FDA is currently reviewing Moderna’s EUA application for authorization among teenagers ages 12 to 17.
Also on January 31, Novavax filed for authorization of its SARS-CoV-2 vaccine, NVX-CoV2373, which uses nanoparticles of the viral spike protein to elicit an immune response. According to the Associated Press, US regulators have urged Pfizer-BioNTech to apply for emergency authorization for a 2-dose regimen of their SARS-CoV-2 vaccine for children ages 6 months to 5 years while awaiting data on a 3-dose course. The companies’ vaccine, marketed as Comirnaty, was the first vaccine to receive FDA approval for people aged 16 years and older, and it is authorized for use among children aged 5 to 15 years.
PAXLOVID The European Medicines Agency (EMA) last week recommended Pfizer’s antiviral COVID-19 treatment Paxlovid for conditional marketing authorization. The European Commission will fast-track review the recommendation, and if approved, EU member states would be able to use the oral antiviral to treat adults with COVID-19 who are at risk of severe illness while they recover at home. Italy, Germany, and Belgium are among several European countries that have already purchased the drug.
VACCINE EFFECTIVENESS New findings from the UK Health Security Agency provide further evidence that booster doses of SARS-CoV-2 vaccines are critical for protection against the Omicron variant. Two doses of a vaccine provided 60% protection from death around 6 months after the last dose in individuals 50 years and older, but a booster dose raised the protective efficacy to 95% 2 weeks after receipt of the shot. Uptake of booster doses is increasing in Europe but only approximately 50% of adults have received one as of late January. Modeling of the Omicron variant surge in Europe predicts that current levels of booster vaccinations could reduce the number of hospital admissions by 500,000-800,000, with further reductions of another 300,000-500,000 admissions if all previously vaccinated people received boosters. The assessment from the European Centre for Disease Prevention and Control (ECDC) also warns that countries with low vaccination rates are expected to face significant pressures on their hospital systems. Vaccines and booster doses remain one of the best tools for protecting individuals against death and reducing pressure on chronically overworked hospital staff.
Recent evidence indicates that current vaccine designs are still capable of providing protection against the Omicron variant sublineage BA.2. Protection against symptomatic infection 25 weeks after a second dose of vaccine is only around 13%, but the protective efficacy jumps to 70% 2 weeks after a booster dose. The jump in protective efficacy against symptomatic disease further highlights the role that booster doses can play in mitigating the severity of disease during the pandemic. The evidence that BA.2 does not escape immunity more than the original Omicron variant is welcome news after the immune escape shift seen between Delta and Omicron. However, a preprint report from Denmark suggests that the BA.2 variant may be 1.5 times more infectious than Omicron.
AT-HOME SARS-COV-2 TESTS Only 2 weeks after launching COVIDtests.gov, a website for US residents to order SARS-CoV-2 tests through the US Postal Service, about 60 million households have requested the tests so far, according to White House officials. The orders leave enough tests for about 65 million more households—about 260 million tests of the US government’s initial order of 500 million. Reportedly, the government plans to order an additional 500 million tests to increase availability. The US has been criticized for not having federal guidance on how to use testing as a COVID-19 mitigation strategy. But even when given FDA-authorized test instructions, a substantial proportion of test users misinterpret negative results of at-home self-tests by not taking into account the implications of a high-risk, pretest exposure and ignoring federal self-quarantine recommendations, according to a study published on January 31 in JAMA Internal Medicine. The researchers suggest that pilot-tested decision science-based instructions might help to increase test takers’ understanding of results and the tests’ usefulness to public health.
ADDITIONAL DOSES FOR IMMUNOCOMPROMISED Public health agencies around the world continue work to determine the effectiveness of additional or booster SARS-CoV-2 mRNA vaccine doses for various populations, including healthcare workers, older adults, and people with compromised immune systems. A report published January 28 in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) aimed to better understand the effects of a third mRNA vaccine dose in immunocompetent and immunocompromised individuals. In the study, a third dose increased vaccine effectiveness (VE) against COVID-19-associated hospitalization from 82% to 97% among individuals with healthy immune systems and from 69% to 88% among people with immunocompromise. The researchers concluded the results support recommendations for a third mRNA vaccine dose as part of a primary series for immunocompromised adults or as a booster dose among immunocompetent adults.
Third doses of both the Pfizer-BioNTech and Moderna vaccines are authorized in the US as part of a primary series for people with immunocompromise, and in October 2021, the CDC recommended certain immunocompromised individuals receive a fourth, or booster, dose 6 months after their third shot. But some immunocompromised people say pharmacies have turned them away for a fourth dose. Last week, the CDC was expected to reinforce its messaging regarding fourth doses for certain immunocompromised individuals in a conference call with pharmacies. An estimated 7 million people in the US live with compromised immune systems, such as those with HIV or those taking immunosuppressive treatments for cancer or following an organ transplant. The US NIH announced this week it plans to study antibody responses to additional vaccine doses among kidney and liver transplant recipients who have had 2 to 4 previous vaccine doses but who did not have a detectable immune response. The study also will examine whether a concurrent reduction in immunosuppressive medication impacts antibody response.
CANADIAN PROTEST Thousands of Canadian truckers and other protesters made their way to Ottawa on January 29 as part of a so-called “Freedom Convoy” to protest vaccine mandates and other public health measures implemented during the COVID-19 pandemic. The rally originated in British Columbia the week prior and consisted of trucks and their supporters driving across the country to the nation’s capital. The original goal of the rally was to protest a mandate put in place on January 15 that required all unvaccinated cross-border truckers to quarantine upon returning home, but the message has since shifted to a general condemnation of all public health interventions. Media reported that people and vehicles clogged the streets of Ottawa making noise and bringing the city to a standstill, but the rally was largely peaceful.
The “Freedom Convoy” rally has been shrouded in controversy since before the event. The Canadian Trucking Alliance (CTA) directly opposed the rally and urged the public to be aware that many of the individuals who are speaking out have no direct connection to the trucking industry. Canadian government officials and the CTA also claim that approximately 90% of the nation’s truckers are already vaccinated and that the individuals participating in the rally represent a fringe minority group. The controversy began heating up when a GoFundMe for the rally raised C$5.5 million (US$4.3 million) in a short time. GoFundMe froze the account for discussions with the organizers, and a former intelligence analyst stated that the speed and anonymity of the donations raised red flags. The analyst also said there is clear activity from foreign countries on the GoFundMe page. Additionally, there are reports that some protestors espouse anti-Semitic and racist views and waved Nazi flags during the rally, defecated in the streets, harassed staff at a local homeless shelter, and at least one protester danced on Canada’s Tomb of the Unknown Soldier. Some protestors called for an attack on the Canadian Parliament similar to the attack on the US Capitol on January 6, 2021. By midday on January 31, many of the protestors had left the area. Prime Minister Justin Trudeau—who is isolating at an undisclosed location after announcing this week he tested positive for COVID-19—said he would not be intimidated by the protestors. The rally notably garnered support from a former US president’s son, Donald Trump Jr., and a tech billionaire, Elon Musk.
COVID-19 MISINFORMATION The music streaming platform Spotify was in the spotlight over the weekend after Canadian music icon Neil Young criticized the service for hosting a podcast by comedian Joe Rogan, who has come under fire for spreading COVID-19 misinformation. Late last week, Young called for his music to be removed from Spotify in protest, and he was later joined by other legendary artists Joni Mitchell and Nils Lofgren. Other popular podcast hosts on Spotify, including Brene Brown and Prince Harry and Meghan Markle, expressed concerns over the platform’s handling of pandemic misinformation. The hashtags #CancelSpotify, #DeleteSpotify, and #ByeSpotify were trending on social media. Spotify removed Young’s music over the weekend, and Spotify Chief Executive Daniel Ek on January 30 published transparency rules, saying the streaming service would add advisories before any content that discusses the virus and link to Spotify’s COVID-19 hub. Rogan responded in a video posted to Instagram, saying he would interview doctors with different opinions right after he talks to “the controversial ones.” WHO Director-General Tedros Adhanom Ghebreyesus thanked Young on Twitter “for standing up against misinformation and inaccuracies around #COVID19 vaccination.”
Meanwhile, in an address to the International Catholic Media Consortium on COVID-19 Vaccines on January 28, Pope Francis said that spreading misinformation and fake news regarding COVID-19 and vaccines constitutes a violation of human rights. His comments were the second time in less than a month that he has addressed misleading information about COVID-19. Pope Francis called on journalists to help the public better understand scientific facts and address the spreading “infodemic.”
by mmmm8 Can you imagine how strongly you have to believe the 5G microchip BS to PAY for a fake card and risk being fired or charged with fraud when you can just easily get the vaccine for free?
by SulisoJoe “just conversations” Rogan defends misinformation like a classic grifter
Money, misinformation, & snake oil: Joe Rogan has a lot in common with Gwyneth Paltrow.
Long before the pandemic took the lives of more than 5.6 million people and created a lucrative market for COVID grifts, misinformation, and snake oil, there was Goop.
The aspirational lifestyle brand and its lustrous "contextual commerce" products are helmed by actor Gwyneth Paltrow, who has used her fame, wealth, and enviable genetics to peddle all manner of wellness pseudoscience and quackery. With the manipulative mantra of "empowering" women to seize control of their health and destinies, Paltrow's Goop has touted extremely questionable—if not downright dangerous—products. Perhaps the most notorious is the jade egg, a $66 egg-shaped rock Goop advised women to shove up their vaginas while claiming it could treat medical conditions, "detox" lady bits, and invigorate mystical life forces (of course).
But let's not forget the $135 "Implant O'Rama" enema device intended to squirt scalding coffee into your colon, the $90 luxury vitamins that almost certainly do nothing, or the $85 "medicine bag" of small, polished rocks that Goop suggests have magical wellness properties. Then there was the bee-sting therapy—no, not therapy for bee stings but therapy imparted from bee stings. Paltrow personally endorsed the practice, which was blamed for the death of a 55-year-old Spanish woman in 2018.
And, of course, Goop embraces the long-standing hokum known as homeopathy, which essentially claims ritualized dilutions of poisons can cure disease and anthropomorphic water molecules can remember how to heal you. (A startling number of homeopathic products are for sale in the US, including baby teething tablets and gels linked to the deaths of 10 infants and poisonings of 400 others.)
Lucrative business
Since Goop's pre-pandemic heyday of generating startling headlines with brazen balderdash, the company has toned down some of its marketing, added disclaimers to products and endorsements, settled lawsuits, and paid out six-figure penalties for making false health claims. But in case you're concerned that any of this hurt Goop's bottom line or had Paltrow reconsidering her business, don't worry. As of late last year, Goop was valued at more than $430 million. The Goop website is still happy to tell you that your liver and kidneys don't work and you need to "detox."
Alas, Goop's success is yet another example of how hawking misinformation, pseudoscience, and nostrum to the disaffected is extremely lucrative. Though, to be fair, most peddlers of nonsense don't have anything close to Paltrow's glamorous flare. In fact, as Goop responded to backlash from health experts in 2017, we all got to witness the Oscar winner-turned-CEO's deft defense of her chic bottles of snake oil. It was truly a master class of elite-level quackery—one that clearly reverberates today.
Paltrow's 2017 defense of Goop sprung to my mind as I read the transcript of Joe Rogan's recent nonapology for hosting, elevating, and endorsing an endless stream of harmful misinformation about COVID-19 on his $100 million podcast. Among other things, he has promoted unproven and potentially dangerous treatments, spread falsehoods and misinformation about vaccines, and downplayed the risks of the virus, which—again—has killed more than 5.6 million people worldwide and counting.
I won't spend time debunking all of Rogan's bunkum. Plenty of outlets have done that work—see here, here, here, here, here, here, here, here, here, etc. The fact that his podcast is rife with misinformation and falsehoods is not in question. Last month, hundreds of doctors and public health experts called out Spotify in an open letter for allowing Rogan to continue spewing "false and societally harmful assertions" about the pandemic. The misinformation is why he gave his nonapology in the first place.
Instead, I'll focus on his defense of platforming misinformation because, just like Paltrow's defense of Goop, Rogan's rationalizations are a modern, skillful take on a classic snake oil sales pitch. In fact, if you plucked sentences from each without attribution, you'd have a killer quackery-themed Mad Libs, as well as a challenging guessing game of "who said it best?"
The defense
To start, the Paltrows and Rogans of the world just want to ask questions and have conversations to get to the truth—like, the real truth. Rogan is famous for defending misinformation presented on his podcast by saying he's "just asking questions." In addressing the Spotify controversy on Instagram, Rogan repeatedly noted that his podcast is "just conversations."
"I'm interested in finding out what the truth is," he elaborated. "And I'm interested in having interesting conversations with people that have differing opinions. I'm not interested in only talking to people that have one perspective."
"We always welcome conversation," Paltrow agreed back in 2017. "That's at the core of what we're trying to do. What we don't welcome is the idea that questions are not OK. Being dismissive... seems like the most dangerous practice of all."
Being dismissive of debunked, absurd, or verifiably incorrect ideas is bad because, well, maybe those ideas are actually correct, Paltrow and Rogan seemed to suggest. You never know until you ask! "Asking questions is the job of all of us," Paltrow emphasized. "There is much that we do not know."
And of course, one can't always just ask experts what the answers are and take them at face value. People should do their own research and figure things out on their own to be sure they can completely trust that information, Paltrow and Rogan argued. "I'm interested in finding out what is correct and also finding out how people come to these conclusions and what the facts are," Rogan explained.
Paltrow echoed the point: "We simply want information; we want autonomy over our health. That's why we do unfiltered Q&As, so you can hear directly from doctors; we see no reason to interpret or influence what they're saying to tell you what to think."
Slide into misinformation
After all, expertise is a slippery business; it's both something to be skeptical of and something to bolster whatever your opinion is, according to Rogan and Paltrow. For instance, highly credentialed, intelligent, and accomplished experts often come to a scientific consensus based on current evidence and sound analysis, forming a mainstream opinion. Yet fringe scientists who spout misleading information or falsehoods or have a clear agenda could still be worth amplifying because, as Paltrow and Rogan argued, they do have fancy credentials, too. As Rogan noted of two particularly troubling guests of his show, "These people are very highly credentialed, very intelligent, very accomplished people. And they have an opinion that's different from the mainstream narrative."
Paltrow presented a similar conundrum. "These are the doctors we regularly feature on Goop: doctors who publish in peer-reviewed journals; doctors who trained at the best institutions; doctors who are repeatedly at the forefront of medicine; doctors who persistently and aggressively maintain an open mind," she said.
With expertise in question, the slippery slope into misinformation continued as both questioned whether evidence-based medicine and scientific consensus can even be trusted at all. "The thing about science and medicine is that it evolves all the time," Paltrow noted. "Studies and beliefs that we held sacred even in the last decade have since been proven to be unequivocally false, and sometimes even harmful," she added, without providing any examples of such disproven "sacred" scientific "beliefs."
Rogan, too, made such a claim. "The problem I have with the term 'misinformation,' especially today, is that many of the things that we thought of as misinformation just a short while ago are now accepted as fact," Rogan said.
In this world where conversations are always innocent, facts can't be verified, experts can't be vetted, and science can't be trusted, there's a lot of room to peddle unproven products and harmful misinformation. It's exactly the world Paltrow and Rogan want you to buy into.
"I want to show all kinds of opinions so that we can all figure out what's going on—and not just about COVID, about everything about health, about fitness, wellness, the state of the world itself," Rogan said.
In the meantime, you can check out products from a health company he promotes called Onnit, which sells Alpha Brain Black Label vitamins for $124.95 per 80-count bottle. There's also the $147.95 Quad Mace, which Onnit claims has origins in ancient Persia and represents the company's embrace of various "training modalities."
by ponchi101 Thanks for that. I like that this person is calling out Paltrow, who is truly a menace to critical thinking. She is the epitome of that disease my smart friend N suffers: smart people that are actually unable to spot falsehoods. And she is smart: she has that $430 MM company so, that is a big achievement.
They are unable to spot the logical flaws in their reasoning and always come back to a few, key points: "Some things in the past that were considered wrong now are considered right". They miss the point that they were considered right AFTER applying proper science, not their bogus ideas.
Anyway, preaching to the choir.
by ti-amie Grifters gonna grift.
by dryrunguy Here's the latest Situation Report. The issue about vaccinating children under 5 is really complicated stuff, and the data are seriously lacking.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 380 million cumulative cases and 5.68 million deaths worldwide as of February 2. The global weekly incidence increased for the 15th consecutive week, up to 23.2 million new cases (+1.4% compared to the previous week)—once again, setting a new record. The trend appears to be tapering off, which could indicate that the Omicron surge is peaking on the global level. The Eastern Mediterranean, European, and Western Pacific regions continue to report record high weekly totals, but the other regions appear to be past their respective Omicron peaks. Notably, South-East Asia’s peak appears to be only its second highest since the onset of the pandemic, while all of the other regions recently set new weekly incidence records. Global weekly mortality increased for the fourth consecutive week, up 13.9% from the previous week. The weekly total of 63,298 deaths is the highest since the week of August 30, 2021. Based on trends observed over the course of the COVID-19 pandemic, we expect the weekly mortality to continue increasing over the next several weeks before it peaks.
Global Vaccination
The cumulative global SARS-CoV-2 vaccine doses administered surpassed 10 billion. The WHO reported 10.04 billion cumulative doses administered globally as of February 2. A total of 4.79 billion individuals have received at least 1 dose, and 4.13 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline steadily from the most recent high of 38 million doses per day in early January 2022 to 20.7 million.* Our World in Data estimates that there are 4.82 billion vaccinated individuals worldwide (1+ dose; 61.2% of the global population) and 4.18 billion who are fully vaccinated (53.1% of the global population).
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 75.3 million cumulative cases of COVID-19 and 888,784 deaths. The US is averaging 415,552 new cases and 2,369 deaths per day.* Sufficient time has elapsed since the Martin Luther King Jr. Day holiday to assess the longer-term US trends, and it appears that the US has passed the peak of its Omicron surge at the national level—although this varies at regional and state levels. The surge began in earnest in mid-December 2021, and daily incidence peaked at a record high of 805,904 new cases per day on January 15, 2022. The trend has decreased rapidly since then, falling by nearly half over the second half of January. Daily mortality continues to increase, surpassing the spring 2020 peak—2,297 on April 21, 2020—which makes the Omicron surge the second highest peak daily mortality to date. Based on trends observed over the course of the pandemic, we expect daily mortality to peak sometime in the next week or so, lagging the trend in daily incidence by 3-4 weeks.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US surpassed 250 million individuals who have received at least 1 vaccine dose, which corresponds to more than 75% of the entire US population. The US has administered 668 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to decline, down from the most recent peak of 1.77 million doses per day on December 6 to 644,000 on January 28.* Among adults, 87.0% have received at least 1 dose, as well as 25.6 million children under the age of 18. A total of 212 million individuals are fully vaccinated**, which corresponds to 63.9% of the total population. Approximately 74.2% of adults are fully vaccinated, as well as 20.5 million children under the age of 18. Since August 13, 88.6 million individuals have received an additional or booster dose. This corresponds to 41.8% of fully vaccinated individuals, including 64.5% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
VACCINE FOR <5 CHILDREN At the request of the US FDA over concerns about an increase in COVID-19 cases and hospitalizations among children, Pfizer and BioNTech announced they have initiated a “rolling submission” that seeks an amendment to the Emergency Use Authorization (EUA) for the companies’ SARS-CoV-2 vaccine that would expand eligibility to children as young as 6 months. The companies expect to complete the application in “the coming days,” and it will cover the first 2 doses of an expected 3-dose primary series using a 3 µg dosage for this age group. Data on the third dose, which is administered at least 8 weeks after the second dose, is expected to be available in the coming months, and a subsequent determination on further expanding the EUA to a full 3-dose series would need to be addressed at that time. Pfizer Chairman and CEO Albert Bourla indicated that Pfizer expects 3 doses to be necessary to provide adequate protection, but the initial EUA for 2 doses will enable children to begin that series while awaiting the final determination on the third dose. Review by the FDA and US CDC could potentially be completed this month. The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) will discuss the issue at its meeting scheduled for February 15.
The unusual and aggressive plan is raising concerns among some vaccine experts who argue that the FDA’s willingness to consider an EUA for a vaccine that has yet to demonstrate efficacy could risk increasing vaccine hesitancy and anti-vaccine sentiment and negatively affect vaccine uptake among young children. There are 2 principal concerns. First, the FDA is evaluating data from only 2 doses of a possible 3-dose series, without any data available yet for that third dose. And second, the small-scale trials may not be sufficient to capture adverse events that would emerge in larger trials.
Early clinical trial data published in December 2021 showed that a 2-dose series failed to elicit sufficient antibody responses in children aged 2-4 years, although children aged 6-23 months produced antibodies similar to older individuals. Notably, the Phase 2b/3 clinical trials were designed only to determine if the vaccine stimulated an immune response similar to older individuals—since previous trials demonstrated efficacy corresponding to that degree of antibody response—so traditional efficacy estimates are not available for young children. The early clinical trial data showed minimal adverse events, but there is concern that additional adverse events could be missed without larger trials. To date, only about 20% of children aged 5-11 years are fully vaccinated. A recent poll found that only 31% of parents of children under 5 years plan to vaccinate their child as soon as a vaccine is available, and some experts argue that speeding the EUA process is unlikely to make a substantial impact on vaccination coverage.
BOOSTER EFFECTIVENESS An early release published in the US CDC’s Morbidity and Mortality Weekly Report examining infection and hospitalization rates in Los Angeles County, California, depicts stark differences among vaccinated and unvaccinated individuals from November 7 to January 8, a period spanning the end of Delta variant predominance and the beginning of Omicron’s predominance. Data were further stratified among vaccinated individuals to include those with and without a booster to show booster effectiveness. For the 14-day period ending December 11, also the last week of Delta predominance, incidence and hospitalization rates among unvaccinated individuals were 12.3 and 83.0 times, respectively, those of boosted fully vaccinated individuals, and 3.8 and 12.9 times, respectively, those of fully vaccinated individuals without a booster. During the period ending January 8, when Omicron gained predominance, the rate ratios dropped, but vaccinated persons remained better protected. Unvaccinated individuals had infection and hospitalization rates 3.6 and 23.0 times, respectively, those of fully vaccinated persons with a booster and 2.0 and 5.3 times, respectively, those of fully vaccinated persons without a booster. According to Los Angeles County Department of Public Health data, 71% of county residents were fully vaccinated as of January 8.
During a White House briefing on February 2, US CDC Director Dr. Rochelle Walensky shared data from 25 US jurisdictions showing unvaccinated individuals were 14 times more likely to die of COVID-19 than fully vaccinated individuals and unvaccinated individuals were 97 times more likely to die than people who were fully vaccinated and boosted. According to an analysis of Omicron’s impact conducted by the Financial Times, nearly half of US COVID-19-related hospitalizations this winter could have been prevented if the nation had vaccination coverage similar to leading European countries. About 64% of the total US population is fully vaccinated, and only 42% of eligible individuals have received a booster dose.
PANDEMIC PREPAREDNESS An analysis of pandemic preparedness across 177 countries and territories published this week in The Lancet suggests that trust—both in the government and among people—could be a driving factor behind why COVID-19 hit some countries harder than others. Trust in government and fellow citizens was strongly associated with higher vaccination rates and decreased mobility, an indicator of social distancing. Notably, no associations were found between COVID-19 outcomes and democracy, populism, government effectiveness, universal healthcare, pandemic preparedness metrics, economic inequality, or trust in science. The researchers estimated that if every country had the same level of government or interpersonal trust as Denmark, which ranks in the 75th percentile for these indicators, global infections between January 1, 2020, and September 30, 2021, might have been reduced by 12.9% for government trust and 40.3% for interpersonal trust. Other factors that explained the most variation in COVID-19 infection-fatality rate (IFR) included a country’s age profile, GDP per capita, and national mean body mass index (BMI). The researchers suggest that countries prepare for the next pandemic by investing in risk communication and community engagement to improve trust in public health guidance, as well as improving health promotion to reduce risks, such as BMI, associated with fatality.
Meanwhile in the US, a bipartisan duo of US Senate lawmakers is expected to introduce a new bill aimed at strengthening the government’s response to a future pandemic. The draft bill includes measures that would establish a 9/11-style bipartisan commission to formally investigate the US pandemic response and require Senate confirmation for the director of the US CDC. The effort—being led by Senators Patty Murray, a Democrat from Washington, and Richard Burr, a Republican from North Carolina—includes several other proposals outlining CDC oversight and tasks, better defining the role of the Assistant Secretary for Preparedness and Response (ASPR), requiring collaboration between the US NIH and other agencies, and ensuring manufacturing capabilities for pandemic tools such as vaccines and therapeutics. Additionally, senior administration officials, public health experts, and US lawmakers are taking stock of the US global COVID-19 strategy, urging more investment in global vaccination coverage and warning that leaving unfilled gaps risks the emergence of new variants. A group of Democrats in the US House is calling for an additional US$17 billion in federal funding for global vaccination delivery and infrastructure. Others are expressing concern over US President Joe Biden’s structuring of authority overseeing the US global COVID-19 strategy. The White House recently published a fact sheet on the Biden administration’s commitment to global health, and NIH issued a press release outlining the National Institute of Allergy and Infectious Diseases’ (NIAID) Pandemic Preparedness Plan.
COVID-19 IN US PRISONS Deaths among incarcerated populations in the US increased 46% from 2019 to 2020, as well as increased 32% among people on parole and 6% among people on probation, according to new data from the Bureau of Justice Statistics (BJS) analyzed by the Prison Policy Initiative. While researchers cannot yet say specifically that the increase is due to COVID-19, they do attribute many of the deaths to the pandemic in some way: directly from infections, a lack of access to regular health care, increases in overdoses and suicides, or a general burden on the correctional system. Since the start of the pandemic, nearly 3,000 incarcerated people have died of COVID-19, including about 300 in federal custody. Notably, imprisoned people are about 3 times more likely to die of COVID-19 than the general population, when data are adjusted for the population’s younger age. Since the emergence of Omicron, prisons across the US are witnessing an alarming increase in COVID-19 cases. In mid- to late-January, at least 7 federal prisons had triple-digit increases in new COVID-19 cases.
US President Joe Biden’s National Strategy for the COVID-19 Response, released in January 2021, included 2 pledges specifically addressing COVID-19 in prisons. One called for the distribution of SARS-CoV-2 vaccines to facility staff and incarcerated individuals in jails, prisons, and detention centers. Today, nearly 70% of the federal prison population is fully vaccinated, but the US Bureau of Prisons (BOP) has not conducted the educational efforts needed to address people with questions regarding medical concerns or distrust of the system, according to advocates. A second pledge promised an executive order to require the BOP and the US Immigration and Customs Enforcement (ICE) to evaluate their COVID-19 protocols, release data on cases, and use federal grant funding for state and local facilities to also follow public health guidance, but the order never came. Advocates say there has been some progress, including on accessibility to SARS-CoV-2 PCR testing and allowing people who were released to home confinement to remain so instead of returning to prison. However, the deteriorating situation in several prison systems since the emergence of the Omicron variant suggests that the response inside of federal, state, local, and private prisons remains inadequate 2 years into the pandemic.
HUMAN CHALLENGE TRIAL The first COVID-19 human challenge clinical trial was found to be safe in healthy young adults, according to the latest not-yet-peer-reviewed data. The Human Challenge Programme—run by Open Orphan, Imperial College London, and other partners—exposed 36 healthy adult volunteers aged 18 to 29 with no immunity to SARS-CoV-2 to the original strain of the virus and monitored them in a quarantine setting, where no serious adverse events occurred. The trial produced several clinical outcomes that could inform public health policy, including that symptoms in infected persons began to develop an average of 2 days following exposure—earlier than the widely accepted 5 days—and that infectious virus peaks around 5 days, when the virus is more concentrated in the nose versus the throat. The researchers plan to monitor participants for 12 months following discharge. Imperial College said it plans to use the trial model with the Delta variant and share the framework to allow similar research around the world, aiming to provide an accelerated route for testing new vaccines, antivirals, and diagnostics.
HEALTHCARE WASTE The COVID-19 pandemic response has generated tens of thousands of metric tons of extra medical waste, straining healthcare waste management systems, threatening human health and the environment, and highlighting an urgent need to improve waste management protocols, according to a WHO report released this week. The analysis only takes into account the amount of potential waste generated through shipments from a joint UN emergency initiative and does not account for COVID-19-related commodities procured outside of the initiative or waste generated by the public. The report estimates that 87,000 metric tons of personal protective equipment (PPE); 2,600 metric tons of non-infectious mainly plastic waste, such as test kits; 144,000 metric tons of vaccine-related waste including syringes, needles, and safety boxes; and 731,000 liters of chemical waste were produced solely through the UN initiative. Overall, the WHO estimates the pandemic has increased healthcare waste loads up to 10 times, potentially exposing workers to needle-stick injuries, burns, and infections, and local communities to poorly managed landfills and carcinogens from improperly incinerated waste. The report encourages countries to see this as an opportunity to revamp waste streams, recommending healthcare facilities and the public responsibly use and dispose of waste and calling for investment into innovative waste treatment technologies and the use of more reusable, recyclable, or biodegradable materials.
TONGA The South Pacific archipelago nation of Tonga went into lockdown on February 2 after at least 5 people were diagnosed with COVID-19. Two port workers in the capital city Nuku’alofa contracted the virus and then transmitted it to 3 family members, marking the first time the country has recorded community transmission. Concerns were high that an influx of international ships and planes delivering needed food, water, and supplies following a devastating volcanic eruption and tsunami would bring SARS-CoV-2 to Tonga, which previously had only 1 recorded COVID-19 case in a visitor. It is unclear how the workers contracted the virus. All foreign aid deliveries have been conveyed using contactless protocols, but the workers dealt with commercial ships at a different wharf. Under the lockdown, domestic flights are grounded, boats are disallowed from traveling between islands, schools are closed, most people are required to remain at home, and masking is encouraged in all public spaces. The lockdown will be reviewed every 48 hours, according to officials.
by ponchi101 I have started a poll because I am truly at odds with what to do with the pandemic, and I am hoping for some TAT2.0 wisdom to help me through.
Vote will be anonymous. Your name will not show. I will vote only after some people have done so, to avoid prompting others.
Comments are, of course, welcome.
by atlpam
ponchi101 wrote: ↑Fri Feb 04, 2022 4:25 pm
I have started a poll because I am truly at odds with what to do with the pandemic, and I am hoping for some TAT2.0 wisdom to help me through.
Vote will be anonymous. Your name will not show. I will vote only after some people have done so, to avoid prompting others.
Comments are, of course, welcome.
Voted, but I'm not really sure what "back to normal" really means anymore.
I am planning to retire in a couple months and haven't seen any of my co-workers in 2 years. Intent is to do some travelling for the next few years, but will likely start domestically as it's still complicated to plan international travel with all the different requirements in play. It may sound crazy but 2 years into this, I have yet to take a Covid test. (knocking on wood)
by JazzNU
ponchi101 wrote: ↑Fri Feb 04, 2022 4:25 pm
I have started a poll because I am truly at odds with what to do with the pandemic, and I am hoping for some TAT2.0 wisdom to help me through.
Vote will be anonymous. Your name will not show. I will vote only after some people have done so, to avoid prompting others.
Comments are, of course, welcome.
Clarification. In the third option, does "drop some mandates" mean get rid of some mandates or impose some mandates? And do you view restrictions differently than mandates in option 2? I'm assuming Option 2 is more lenient than Option 3 just based on the order of the choices.
by Deuce
atlpam wrote: ↑Fri Feb 04, 2022 5:58 pm
Voted, but I'm not really sure what "back to normal" really means anymore.
I am planning to retire in a couple months and haven't seen any of my co-workers in 2 years. Intent is to do some travelling for the next few years, but will likely start domestically as it's still complicated to plan international travel with all the different requirements in play. It may sound crazy but 2 years into this, I have yet to take a Covid test. (knocking on wood)
I haven't been tested, either. I never really saw the purpose...
Firstly, I've never had any symptoms at all. Secondly, I'm very careful about not being exposed to the virus. Thirdly, the result of a test (PCR) is only good for that specific moment in time. If you test negative, it means only that you were negative at that precise moment. Three hours later, you could be positive. And so, a negative result is essentially useless unless you get tested every day. A positive result could help, I suppose, by telling you that you should isolate yourself... but there are far more negative results than positive ones, and it's rather evident that many, many people don't understand what a result of negative means. Many seem to believe that a result of negative means that they are negative for a month or more - and so they're not careful. They don't realize that it means only that you were negative at the exact moment you were tested - it does not mean that you're still negative an hour after the test.
I have a box of rapid tests at home. Because their accuracy is reportedly far less than 100%, they are essentially useless. Any test which tells you that you MIGHT have COVID means nothing. The only reason I got the box of rapid tests is in case they realize at some future point that these tests are 98% accurate. Until that happens, though (and it likely never will), I don't see myself using them, even if I have symptoms - because I'll be completely unsure if the result is accurate or not. If I have symptoms, I'll assume I have COVID and simply stay home for a week or so.
ponchi101 wrote: ↑Fri Feb 04, 2022 4:25 pm
I have started a poll because I am truly at odds with what to do with the pandemic, and I am hoping for some TAT2.0 wisdom to help me through.
Vote will be anonymous. Your name will not show. I will vote only after some people have done so, to avoid prompting others.
Comments are, of course, welcome.
Clarification. In the third option, does "drop some mandates" mean get rid of some mandates or impose some mandates? And do you view restrictions differently than mandates in option 2? I'm assuming Option 2 is more lenient than Option 3 just based on the order of the choices.
Get rid of some mandates.
I truly asked these questions because I am truly unsure of what to do. To the point that I even had a hard time figuring out what to ask.
For example: I would give restaurants and entertaining places the option to decide whether they will enforce vaccination or not, as long as it is CLEARLY STATED AT THE ENTRANCE. Then the patrons can decide if they go in or not.
Txs to all for the votes.
To Atlpam: Indeed, what does back to normal mean? Again, I know I am asking half-baked questions here.
by ti-amie
Dr. Hotez ( MD & PhD) is apparently being attacked by the fully vaxxed and boosted folks at Faux.
by dryrunguy Here's the latest Situation Report. My apologies for being a day late in posting it.
::
WASTEWATER SURVEILLANCE The US CDC has added wastewater surveillance of SARS-CoV-2 RNA to its COVID Data Tracker, as virus levels in sewage water may be capable of providing an early warning signal for transmission surges. The tool comprises data from more than 400 testing sites in 37 states, with more than 34,000 samples representing 53 million US residents collected so far. Hundreds of additional testing sites are expected to begin submitting data to the system in coming weeks. The CDC initiated the National Wastewater Surveillance System (NEWS) in September 2020, and it has become a critical tool for public health officials since it can show where viral loads are changing, which communities are at risk of a surge in cases, and where medical supplies should be deployed.
An additional benefit of the COVID wastewater tracking system is the identification of novel and “cryptic” variants of SARS-CoV-2. Cryptic variants are lineages of SARS-CoV-2 that contain mutations never before observed in humans. A number of cryptic lineages have been detected in the New York City sewer system. The origin of these out-of-the-ordinary lineages, which also have been detected in Missouri and California, has not yet been determined, but the most popular hypothesis is the mutations arose simultaneously in similar animal hosts, such as rodents that live in the sewer systems. Whatever the source, the new surveillance system could be critical in identifying and tracking the next major variant of concern.
US CDC ACIP MEETING The US CDC's Advisory Committee on Immunization Practices (ACIP) met on February 4 to provide updates to clinical considerations for utilization of COVID-19 vaccines. Topics of discussion included the FDA-approved Spikevax SARS-CoV-2 vaccine from Moderna, vaccination recommendations specific to immunocompromised individuals, and lengthening the gap between the first two doses of mRNA COVID-19 vaccines.
ACIP voted unanimously to recommend the use of a 2-dose primary series of Spikevax among US adults aged 18 years and older, and CDC Director Dr. Rochelle Walensky endorsed the recommendation later that day. ACIP members also discussed concerns regarding the risk of myocarditis following vaccination. Results of investigations into 13 deaths from myocarditis following mRNA vaccination found that the myocarditis was not caused by vaccination, and most other myocarditis cases among mRNA vaccine recipients were resolved within 90 days with no reported impact on quality of life. Additional discussions centered on potentially widening the time interval between initial mRNA vaccine doses from the current 21-28 days to 8 weeks apart. The change might reduce the risk of myocarditis among some recipients and increase vaccine effectiveness. However, no official vote was taken on the suggestion.
Officials also presented anticipated changes to vaccine guidance for certain immunocompromised individuals. The proposed revised guidance notes that people who are moderately or severely immunocompromised should receive a booster dose at least 3 months—instead of the current 5 months—after the last dose of a 3-dose primary series of mRNA SARS-CoV-2 vaccine. For immunocompromised individuals who received the single-dose J&J-Janssen vaccine, the guidance likely will change from the current recommendation—a primary dose followed by a booster 2 months later—to a 3-dose schedule of an additional mRNA dose at least 28 days after the initial dose and then an mRNA booster dose 2 months after the second dose. The guidance was expected to be updated on February 7 but the new recommendations are not yet published on the CDC’s website.
OMICRON-ONLY VACCINES As noted in previous briefings, both Moderna and Pfizer are pursuing the development and testing of Omicron variant-specific vaccines. Some health officials, such as those from the European Medicines Agency, support the efforts. However, research from the US National Institutes of Allergy and Infectious Diseases' (NIAID) Vaccine Research Center posted on February 3 to the preprint server bioRxiv suggests that an Omicron variant-specific booster developed by Moderna might not provide additional or greater protection beyond the company’s already authorized mRNA vaccine booster dose. The research, which is not yet peer-reviewed, tested the boosters in primates. These findings mirror the results of other small animal studies testing vaccines targeting other individual variants. But predicting the future emergence or dominance of SARS-CoV-2 variants is difficult, with scientists uncertain if a new dominant variant might evolve from Omicron, a past variant, or have mutations very different from either Omicron or other past variants. This concern has led some scientists and health officials to advocate publicly for broad protection in future vaccines—to multiple variants, all betacoronaviruses, or even all coronaviruses. Several NIAID researchers recently published a commentary in the New England Journal of Medicine (NEJM) calling for a universal coronavirus vaccine to help mitigate the impacts of any future coronavirus pandemic.
LONG COVID/PASC Long COVID, or post-acute sequelae of COVID-19 (PASC), are both terms that represent a broad range of symptoms that individuals with SARS-CoV-2 infection can develop days to months after initial infection. Some public health experts are warning that the most recent surge in Omicron cases could lead to a different type of public health crisis, with extended burdens on patients and the healthcare system long after the pandemic ends. Some studies suggest that convalescent COVID-19 patients, especially those who had more severe disease or certain symptoms during acute infection, could be at higher risk of long-term cardiovascular complications or abnormal brain changes. Many patients experiencing long COVID already are waiting months for care, as physicians and clinics try to determine the best way to treat the huge constellation of symptoms that characterize the condition. Research continuously suggests that vaccination could blunt the development of long-term symptoms.
A new cohort study published February 4 in JAMA Network Open sought to better understand certain new symptoms and their prevalence among individuals who test positive and negative for SARS-CoV-2 infection, stratified by age and disease severity. New-onset shortness of breath, heart rhythm abnormalities, and type 2 diabetes were more common 31 to 150 days after testing positive than among those with negative results. Among positive individuals over 20 years old, fatigue, shortness of breath, and sleep disorders were the most common new symptoms, whereas change in bowel habits, fatigue, and shortness of breath were the most common new symptoms for positive individuals under 20. The researchers also found that new symptoms—such as anxiety, depression, neuromuscular disorders, peripheral nerve disorders, and uncoordinated movements—were more common among hospitalized and ventilated patients. They called for healthcare providers to be aware of symptoms that might develop among patients after SARS-CoV-2 infection, particularly those who required hospitalization.
ANTIBODY DURABILITY Researchers are continuing to gain insight into SARS-CoV-2 immune responses—and the durability of antibody production—following infection. A study published February 3 in JAMA Network Open suggests that antibodies targeting the receptor-binding domain (RBD) of the spike protein can persist for up to 20 months in unvaccinated individuals who reported test-confirmed COVID-19. While the data are encouraging, it remains unclear how the antibody levels correlate to protection against future infections, especially with new variants. Another study, published February 7 in Nature Microbiology, had similar results, with researchers finding the magnitude of persistent antibody responses were correlated with COVID-19 severity in unvaccinated individuals. They note that while the neutralizing antibody (nAb) response seen in most individuals in the study would be sufficient to provide protection against reinfection and severe infection at 480 days from disease onset, people who had asymptomatic or mild infections likely would need to be vaccinated to maintain antibody-mediated protection against future SARS-CoV-2 infection. With more people becoming infected with SARS-CoV-2 and recovering from COVID-19, the future of the pandemic may see surges of infections due to new variants, but hopefully those cases will result in fewer hospitalizations and deaths. Vaccination remains the most reliable way to help prevent infection, severe disease, and death.
NOVAVAX Novavax on January 7 said it has received expanded US government funding to support late-stage clinical trials for its 2-dose SARS-CoV-2 vaccine among adolescents aged 12 to 17, including a booster component. The company has filed with the US FDA for Emergency Use Authorization (EUA) of its vaccine among adults, and the vaccine has received clearances for use in adults in Great Britain and Germany, as well as endorsement in New Zealand. Israel recently signed a deal to purchase 5 million doses of the protein-based vaccine, and Australia this week received its first shipment of a total order of 51 million doses. Some experts hope that Novavax’s use of protein-based technology will help win over individuals who are reluctant to be vaccinated with shots using newer mRNA technology.
SOUTH AFRICAN VACCINE REPLICATION Scientists at South Africa’s Afrigen Biologics and Vaccines announced last week that they have used publicly available information to produce a close copy of Moderna’s SARS-CoV-2 mRNA vaccine, without the company’s support. The effort—which is backed by the WHO-supported mRNA technology transfer hub launched in June 2021—represents the first mRNA vaccine designed, developed, and produced in an African lab. Scientists are using Moderna-patented technology because the company has vowed to not enforce its COVID-19-related patents against those making vaccines intended to combat the pandemic. However, without the involvement of an mRNA vaccine producer, the process to bring the new vaccine to market could take up to 3 years, instead of about 1 year with support from an outside company, according to the WHO’s Initiative for Vaccine Research. Human clinical trials using the Moderna mimic are expected to begin in the fourth quarter of this year after production is scaled up. Though the long timeline for vaccine production and testing does not address Africa’s urgent need for vaccines, many scientists are enthusiastic that the effort will lay the groundwork for the future development and production of mRNA vaccines on the continent.
OTTAWA STATE OF EMERGENCY The mayor of Canada’s capital declared a state of emergency this week to help police and city staff obtain the resources they need to address a 12 day-long demonstration involving a convoy of truck drivers and other protestors who are blocking the streets of Ottawa, running their large vehicle engines, honking horns, and bringing the city to a standstill. The initial purpose of the “Freedom Convoy,” which arrived in the city on January 29, was to protest vaccine mandates for cross-border truckers, but it has since evolved into a broader demonstration against general COVID-19-related public health measures and now involves others with ties to far-right groups. Over the weekend, police began ticketing and arresting people who were caught bringing fuel, food, or other “material aid” to protestors and cautioned that demonstrators “exhibited extremely disruptive and unlawful behavior” that presents risks to public safety. Some residents reported being harassed for wearing masks.
Additionally, the crowdfunding platform GoFundMe is facing allegations of fraud from the Florida Governor and Texas State Attorney General after the fundraising platform froze nearly US$10 million in donations to the Freedom Convoy’s fundraiser and said it would redistribute the money to a different charity. After threats of investigations, GoFundMe said it instead will automatically issue refunds to donors, based on police determinations that what began as a peaceful protest has became an occupation. Donors are now using a Christian crowdfunding site called GiveSendGo, which has raised more than US$6 million as of today. The Ottawa demonstrations have become a rallying cry for far-right and anti-vaccine groups worldwide. In Australia today, hundreds of anti-vaccine demonstrators blocked the streets of the capital Canberra, as politicians and their staff return to the city for a week of parliamentary proceedings.
WHITE-TAILED DEER White-tailed deer infected with SARS-CoV-2 have been identified in at least 15 US states—Arkansas, Illinois, Iowa, Kansas, Maine, Massachusetts, Minnesota, New Jersey, New York, North Carolina, Ohio, Oklahoma, Pennsylvania, Tennessee, and Virginia—adding to concerns that the wild animals could become a potential source of new variants. Researchers looking at deer in Iowa found 1,200 of 2,000 lymph node samples collected from deer that were killed by hunters or car strikes tested positive for the virus. Additionally, white-tailed deer on Staten Island, New York, have been found to be carrying the Omicron variant, the first time the variant has been detected in wild animals. Researchers say it is likely deer are being infected through human contact, then spreading the virus to other deer, and so far there is no evidence that the animals have transmitted the virus back to humans. But more widespread infection among the estimated 30 million deer in the US raises the risk that the animals could become a viral reservoir, which could lead to spillover into humans or other animal species.
by ponchi101 So we may have two reservoirs for C19: white tailed deer, and white nationalists.
Sounds about right.
by ti-amie In case you haven't seen this gem:
by JazzNU
dryrunguy wrote: ↑Wed Feb 09, 2022 3:03 pm
Here's the latest Situation Report. My apologies for being a day late in posting it.
WHITE-TAILED DEER White-tailed deer infected with SARS-CoV-2 have been identified in at least 15 US states—Arkansas, Illinois, Iowa, Kansas, Maine, Massachusetts, Minnesota, New Jersey, New York, North Carolina, Ohio, Oklahoma, Pennsylvania, Tennessee, and Virginia—adding to concerns that the wild animals could become a potential source of new variants. Researchers looking at deer in Iowa found 1,200 of 2,000 lymph node samples collected from deer that were killed by hunters or car strikes tested positive for the virus. Additionally, white-tailed deer on Staten Island, New York, have been found to be carrying the Omicron variant, the first time the variant has been detected in wild animals. Researchers say it is likely deer are being infected through human contact, then spreading the virus to other deer, and so far there is no evidence that the animals have transmitted the virus back to humans. But more widespread infection among the estimated 30 million deer in the US raises the risk that the animals could become a viral reservoir, which could lead to spillover into humans or other animal species.
I don't know enough about a few of those to be certain, but the majority of those states have deer hunting and it's not a small or insignificant hobby. The way this is phrased, it's like human contact is the only concern. Seems like they'd need to say very clearly whether eating venison from an infected deer is a possible way to transmit the virus.
by ponchi101 On personal news:
The husband of a cousin here in the USA is in the hospital, tubed and with no hopes of making it.
Former cancer patient, unvaccinated because... well, you know who they voted for.
I don't know if to feel sorry or what.
by JazzNU
ponchi101 wrote: ↑Thu Feb 10, 2022 2:21 am
On personal news:
The husband of a cousin here in the USA is in the hospital, tubed and with no hopes of making it.
Former cancer patient, unvaccinated because... well, you know who they voted for.
I don't know if to feel sorry or what.
Sorry to hear this. It's your family, so hard to not feel bad when it's more personal even if I'm generally done (so, so done) and unsympathetic to the unvaccinated. I'm not unmoved by (some) personal stories.
I also feel sorry for the doctors and nurses treating them and any family members that tried to prevent any of this from happening and have to deal with his care and anything that comes if he doesn't pull through.
by ponchi101 And we received news today that he died overnight.
A totally preventable death. It is the thing that one really wonders about: how can't they see it?
by JazzNU
ponchi101 wrote: ↑Thu Feb 10, 2022 5:18 pm
And we received news today that he died overnight.
A totally preventable death. It is the thing that one really wonders about: how can't they see it?
Sorry for your family's loss. And it is very hard to understand how they don't see it, particular those with pre-existing conditions or age factors that make the risk higher.
by dryrunguy Here's the latest Situation Report. Haven't read it yet. Just way too many meetings today.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 399.6 million cumulative cases and 5.76 million deaths worldwide as of February 9.
We expect the global cumulative incidence to surpass 400 million cases in the WHO’s next update. If that is the case:
1 case to 100 million- 389 days
100 to 200 million- 190 days
200 to 300 million- 155 days
300 to 400 million- 34 days
The global weekly incidence decreased for the first time since mid-October 2021, down 15% from the previous week. It appears that the global trend has passed the Omicron peak. If the global trend follows what we have observed at the national level in many countries, we expect the decline to be relatively steep. Notably, all WHO regions with the exception of the Eastern Mediterranean region (+35.6%) reported decreasing weekly incidence last week. Global weekly mortality increased for the fifth consecutive week, up 9.6% from the previous week. The weekly total of 70,718 deaths is the highest since the week of August 23, 2021—the peak of the previous wave. Based on trends observed over the course of the COVID-19 pandemic, we expect the weekly mortality to peak in the next 2-4 weeks.
Global Vaccination
The WHO reported 10.1 billion cumulative doses administered globally as of February 7. A total of 4.81 billion individuals have received at least 1 dose, and 4.16 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline steadily from the most recent high of 37 million doses per day in early January 2022 to 18.1 million on February 8.* The global weekly average jumped to 26.2 million doses per day on February 9, corresponding to a large jump reported in Asia, although this may be a reporting error.** Our World in Data estimates that there are 4.85 billion vaccinated individuals worldwide (1+ dose; 61.6% of the global population) and 4.23 billion who are fully vaccinated (53.7% of the global population). A total of 1.17 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
**The OWID data show 18.9 million doses reported in Asia on February 8 and 71.6 million on February 9 (+52.8 million), but it is not immediately clear what country or countries accounted for that increase. Only 20 total countries and territories reported an increase in doses administered from February 8 to February 9, and the largest increase was China with +1.01 million doses.
UNITED STATES
The US CDC is currently reporting 77.0 million cumulative cases of COVID-19 and 906,603 deaths.
The US surpassed 900,000 cumulative deaths on February 6:
1 death to 100k- 87 days
100k to 200k- 111 days
200k to 300k- 88 days
300k to 400k- 35 days
400k to 500k- 33 days
500k to 600k- 121 days
600k to 700k- 105 days
700k to 800k- 78 days
800k to 900k- 52 days
Daily incidence continues its sharp decline, down from a record high of 806,176 new cases per day on January 15 to 230,602 on February 8, a 71% decrease over only 3 weeks. Daily mortality has largely leveled, holding relatively steady at approximately 2,300-2,400 deaths per day since January 24—with a slight decline since February 1.* Daily mortality has not yet exhibited a decrease commensurate with the decline in daily incidence, but if this represents a peak, it would correspond to a lag of approximately 3 weeks behind the daily incidence trend.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 674 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to decline, down from the most recent peak of 1.77 million doses per day on December 6 to 479,000 on February 4.* A total of 251 million individuals have received at least 1 vaccine dose, which corresponds to 75.7% of the entire US population. Among adults, 87.3% have received at least 1 dose, as well as 26.0 million children under the age of 18. A total of 213 million individuals are fully vaccinated**, which corresponds to 64.2% of the total population. Approximately 74.4% of adults are fully vaccinated, as well as 21.0 million children under the age of 18. Since August 13, 90.5 million individuals have received an additional or booster dose. This corresponds to 42.5% of fully vaccinated individuals, including 65.2% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
GLOBAL RESPONSE During the week ending February 6, the number of new COVID-19 cases decreased 17% globally compared to the prior week but the number of new deaths increased by 7%, according to the WHO. The situation varies widely depending upon the region, leading WHO Director-General Dr. Tedros Adhanom Ghebreyesus to warn that “COVID isn’t finished with us,” while appealing for more support from wealthy nations to bring equity to the distribution and administration of vaccines, tests, therapeutics, and personal protective equipment (PPE). To date, only 0.4% of the 4.7 billion SARS-CoV-2 tests administered globally have been used in low-income countries, and only about 11% of people in those countries have received at least one dose of vaccine.
The WHO, along with world leaders and high-level officials, on February 9 called for higher income countries to fund their “fair share” of financial support to the Access to COVID-19 Tools (ACT) Accelerator—including the COVAX initiative—to help end the pandemic by delivering necessary tools for pandemic response to low- and middle-income countries (LMICs). The ACT-Accelerator is budgeted to need US$23.4 billion through September 2022, of which it expects wealthy countries to donate US$16.8 billion. However, those nations so far have pledged only US$814 million—about 5% of the amount—leaving a US$16 billion gap. The remaining US$6.5 billion is expected to be self-financed by middle-income countries. Separately, US$6.8 billion is necessary for in-country resource delivery, which is anticipated to come from domestic resources, multilateral development bank support, and additional international grant financing support. In January, COVAX appealed for US$5.2 billion to continue operations over the next 3 months.
A new analysis from the Center for Global Development lauds the global vaccine rollout during the COVID-19 pandemic as the fastest and most widespread in history. But the paper singles out low-income countries as the exception, noting that other vaccination efforts have provided more coverage more quickly. Both the US and the EU recently indicated they will shift their focus from increasing vaccine supplies flowing into low-income countries, particularly those in Africa, to increasing vaccination administration and uptake. A paper posted February 9 to the preprint server medRxiv presents model-based estimates of deaths averted and cost per life saved by scaling up mRNA vaccinations in low- and lower-middle-income countries. According to the paper, which is not yet peer-reviewed, if every person living in those countries received 2 doses of mRNA vaccine this year, the effort would avert 1.2 million deaths at a cost between US$7,400 and US$81,500 per life saved. Despite the broad range, the price per life saved is considerably lower than some had estimated, showing the overall cost effectiveness of vaccinating the entire world.
US STATE MASK MANDATES As the number of new COVID-19 cases continues to decline across the US, a growing number of states—including California, Connecticut, Delaware, Illinois, Massachusetts, New Jersey, New York, Oregon, and Rhode Island—have either dropped or announced plans to end certain mask mandates, including some for schools, and other COVID-19 restrictions meant to reduce transmission of the virus. The moves, made largely in states controlled by Democratic governors, have put pressure on the White House, which said it is working on plans to move into a “new normal.” US President Joe Biden’s Chief Medical Advisor Dr. Anthony Fauci cautioned that the pandemic remains unpredictable and urged leaders to take gradual steps to transition out of the current surge. US CDC Director Dr. Rochelle Walensky noted her agency is working on new guidance for states and expressed optimism that new cases are dropping. But she warned that hospitalization and death rates remain high and that the nation is not yet at a point to drop mask mandates for indoor public spaces. The CDC currently recommends wearing masks in schools and in localities where coronavirus transmission is high—with case rates higher than 50 cases per 100,000 or positive test rates exceeding 8%—which at present accounts for 99% of the country. The agency reportedly is considering changing the metrics on which it bases its masking guidance, possibly shifting from case rates to data on hospitalizations.
Some parents expressed concern over the end of mask mandates for schools, saying more students over age 5 should be vaccinated before masks come off. Currently, only about 23% of children ages 5 to 11 years old are fully vaccinated and only about 56% of older children, aged 12 to 17, are fully vaccinated. Experts remain divided over when and on what metrics school mask mandates should be removed. However, all agree that masking in schools should not last forever.
US VACCINE MANDATE FOR FEDERAL EMPLOYEES In a 2-1 vote, the 5th US Circuit Court of Appeals on February 9 declined to block a lower court injunction on US President Joe Biden’s mandate requiring federal employees be vaccinated against COVID-19. The ruling, which was unexplained, signals the court will conduct a full review of the case and potentially sets the stage for the case to head to the US Supreme Court. In a dissenting opinion, Judge Stephen A. Higginson noted that a single district judge issued an injunction after several district courts rejected requests to block the mandate, writing the Supreme Court was the “only court that can now provide timely relief.” According to the US Office of Management and Budget, 97.2% of the federal workforce is compliant with the mandate, including those who are vaccinated or have pending or approved exemptions.
In a similar case, Louisiana and 15 other states filed an amended complaint last week against the federal vaccine mandate for healthcare workers at facilities that receive funding through Medicare or Medicaid. While experts agree the changes likely will not impact the rule’s fate, the new arguments—which include that state surveyors were improperly added to covered employees and that the Omicron variant’s ability to cause breakthrough infections renders vaccination meaningless—could raise new questions. The Supreme Court upheld the mandate in a January 13 opinion.
VACCINE UPTAKE Since the onset of mass SARS-CoV-2 vaccination in the US, and even before, the federal government has struggled to communicate effectively about vaccination recommendations, benefits, and risks, particularly in the context of engaging with vulnerable populations. In an effort to improve engagement with racial and ethnic minorities and communities with low vaccination coverage, the Health Resources and Services Administration (HRSA) is distributing more than US$66 million to community groups across the country to support vaccine outreach and education efforts. The funding aims to build confidence in SARS-CoV-2 vaccines through trusted local leaders who know better how to effectively engage with communities. The funding is part of the US$1.9 trillion American Rescue Plan that was signed into law in March 2021.
A recent study published in Nature found significant racial and ethnic disparities in terms of SARS-CoV-2 vaccine hesitancy and uptake in the US and UK. The study included data collected via a smartphone-based COVID-19 symptom monitoring study from more than 2 million individuals between March 2020 and February 2021. Among US participants, vaccine hesitancy was significantly higher for Black, Hispanic, and multi-racial individuals, compared to White participants. Similar trends were found among individuals in the UK. In the US, Black participants reported significantly lower vaccine uptake, even among those who were willing to be vaccinated; however, this trend was not observed in any other racial or ethnic minority group in the US, nor in any group in the UK. The low uptake among Black participants who were willing to get vaccinated suggests that access was also a barrier to vaccination.
The US CDC COVID-19 Emergency Response Team published findings from a study on SARS-CoV-2 vaccine uptake among lesbian, gay, bisexual, and transgender (LGBT) communities, in the CDC’s Morbidity and Mortality Weekly Report (MMWR). The CDC notes that LGBT individuals are at elevated risk for severe COVID-19 and death as a result of higher prevalence of underlying health conditions. The CDC also was concerned about the “potential for low vaccine confidence and coverage” in LGBT communities due to long-standing mistrust of healthcare systems and numerous barriers to accessing health services. Data collected through the National Immunization Survey Adult COVID Module (NIS-ACM) between August 29 and October 30, 2021, indicate that vaccination coverage was actually higher among LGBT adults (85.4%) than heterosexual adults (76.3%). While overall coverage was higher, some racial and ethnic minority groups within the LGBT community reported lower coverage than corresponding heterosexual groups, including non-Hispanic Black women. In fact, vaccination coverage was the lowest among non-Hispanic Black LGBT individuals across all categories of sexual orientation. Notably, the study also found higher degrees of confidence in vaccine safety and protection among portions of the LGBT community than among heterosexual adults. A separate study by health officials in New York found that SARS-CoV-2 vaccination coverage among individuals diagnosed with HIV infection (63.5%) was lower than among the broader New York adult population (75.0%), including across all racial and ethnic, economic, and other demographic subgroups. The analysis was conducted by matching data from New York state’s HIV surveillance registry and immunization registries for New York state and New York City.
MATERNAL ANTIBODIES People who receive SARS-CoV-2 vaccinations during pregnancy pass along more durable antibodies to their newborns than do unvaccinated individuals who had COVID-19 during pregnancy, according to a research letter published February 7 in the Journal of the American Medical Association (JAMA). The small study examined 77 vaccinated pregnant women who completed their 2-dose mRNA vaccine series between weeks 20 and 32 of gestation and 12 women who had symptomatic SARS-CoV-2 infection during pregnancy. The infants of vaccinated mothers had significantly higher immunoglobulin G (IgG) antibodies in umbilical cord blood at delivery and in blood draws at 2 and 6 months postpartum than infants who received antibodies from their unvaccinated convalescent mothers. The researchers note that while the antibody titer necessary for protection against SARS-CoV-2 infection or severe disease is unknown in infants, the findings further support recommendations for pregnant individuals to be vaccinated and provide evidence that antibodies in newborns of vaccinated individuals could persist until the infant becomes eligible for vaccination at 6 months. The US FDA is expected to authorize the Pfizer-BioNTech vaccine for young children ages 6 months to under-5 later this month.
J&J-JANSSEN VACCINE PRODUCTION Johnson & Johnson (J&J) late last year temporary halted production of its SARS-CoV-2 vaccine at the only plant making usable batches of the shots, a facility run by J&J subsidiary Janssen in the Netherlands capable of manufacturing more than 50 million doses per month, according to a report in The New York Times. The single-dose vaccine, which does not need ultra-cold storage, is the first choice for many low- and middle-income countries (LMICs), and the move caught officials with the African Union and the COVAX initiative off guard when they learned about the production suspension from Times reporters. The facility where the vaccine was being produced is instead manufacturing an experimental vaccine against a different virus, which some noted could be a more profitable venture. A J&J representative said the company has millions of finished doses in inventory, continues to deliver vaccine to fill-and-finish facilities, and intends to deliver on its vaccine commitments to LMICs. Notably, the company failed to deliver on commitments made to COVAX last May. Last year, J&J ran into regulatory problems with Maryland-based contractor Emergent BioSolutions when it did not pass US FDA inspections. The Emergent facility continues to require FDA review of vaccine batches manufactured at the plant, and none have been cleared for distribution. J&J has plans to produce SARS-CoV-2 vaccine at 2 other plants, one in the US and another in India, but those facilities are not expected to be operational until late spring. The Dutch production plant is expected to begin producing the J&J-Janssen vaccine again next month, although those doses will not be shipped until May or June.
PFIZER-BIONTECH VACCINE Pfizer this week reported US$36.78 billion in 2021 direct sales from the SARS-CoV-2 vaccine it makes with BioNTech, making the vaccine the top-selling pharmaceutical product ever in a single year. The next highest—the drug Humira, which is used to treat rheumatoid arthritis and other autoimmune and inflammatory conditions—registered US$20.7 billion in 2021 sales. In its full-year results, Pfizer predicted it will sell US$32 billion of its vaccine, called Comirnaty, and US$22 billion of its antiviral COVID-19 treatment Paxlovid in 2022. Pfizer CEO Albert Bourla this week said he expects the US FDA to soon authorize a low-dose version of the Pfizer-BioNTech vaccine for young children aged 6 months to under-5 years under a fast-track review process. Data from clinical trials of the vaccine among this age group are expected to be published later this week in preparation for a February 15 meeting of the FDA Vaccines and Related Biological Products Advisory Committee. The US CDC has begun preparations to deliver the vaccine once it is authorized, telling state and local officials they could expect to start receiving shipments on February 21.
AUSTRALIA & NEW ZEALAND Several countries with the strictest closed border policies have announced they will reopen to international travelers. Australia announced it will allow fully vaccinated citizens, permanent residents, and visa holders into the country without a travel exemption beginning February 21; unvaccinated visa holders will still require a valid travel exemption. Notably, the Australian Technical Advisory Group on Immunisation (ATAGI) announced today that Australians will need 3 vaccine doses to be considered “up to date” on their shots. If an individual has gone more than 6 months from their second dose without a booster shot, they will be considered “overdue.” The new definition will only apply to COVID-19 management within Australia and will not affect rules for “fully vaccinated” people entering the country. However, each state will continue to set its own requirements for booster doses, which could impact visitors.
Neighboring New Zealand announced a phased reopening of its borders beginning at the end of this month. The country expects to welcome all international travelers from October. Everyone entering the country will be required to self-isolate at home for 10 days. Both nations’ borders have been closed for most of the past 2 years.
by dryrunguy Here's the latest Situation Report. Now they're suggesting that booster vaccines begin to wane in effectiveness after about 4 months. Oh, and all those firings of unvaccinated employees of the State of New York? The majority of them were employed by the Department of Education. EDUCATION. The U.S. has NO chance of making it to the 22nd century.
::
VACCINE FOR <5 CHILDREN The US FDA on February 11 postponed an advisory committee meeting set for today to discuss data on the Pfizer-BioNTech SARS-CoV-2 vaccine for young children ages 6 months through 4 years. According to an FDA statement, Pfizer notified the agency of new data from an ongoing clinical trial, and the postponement will allow the FDA time to consider that data. As previously reported here, the companies originally tested the vaccine as a 2-dose regimen, with each dose containing 3 μg, one-tenth of the dose given to those ages 12 and older. However, the companies announced late last year that among children aged 2 to 4 years old, 2 doses generated only 60% of the antibody levels seen in individuals aged 16 to 25 years who received 2 doses. Notably, 2 doses did appear to elicit antibody levels among the youngest children aged 6 months to 23 months similar to those in the older individuals.
The FDA originally pushed Pfizer and BioNTech to request authorization for an initial 2-dose regimen while collecting data on a third dose, but Dr. Peter Marks, Director of the FDA Center for Biologics Evaluation and Research, implied the new data showed that 2 doses were not sufficient in protecting against symptomatic infection, particularly during the latest Omicron surge. Former FDA Administrator and current Pfizer Board Member Dr. Scott Gottlieb said the delay was due to a “low number of cases” in the trial, perhaps insufficient for data analysis. The companies expect data on the 3-dose regimen to be available in early April.
Efforts last week by the US CDC to open preordering of the vaccine indicated the decision to authorize a 2-dose regimen while waiting on further data on 3 doses was nearly a done deal, with the agency predicting shipments of the lower-dose version could begin the week of February 21. While some experts breathed a sigh of relief that the FDA is taking extra time to review the scientific evidence, some parents expressed dismay and frustration over what they say feels like a string of setbacks. Still, not all parents are eager to vaccinate their younger children. The Pfizer-BioNTech vaccine has been available for children aged 5 to 11 since early November 2021, yet only about one third of the 28 million children in that age group have received at least 1 dose so far. A recent survey from the Kaiser Family Foundation showed about 30% of parents of children younger than age 5 intend to get them vaccinated as soon as shots become available. Approximately 400 children under age 5 have died of COVID-19 since the beginning of the pandemic.
BOOSTER DOSE EFFECTIVENESS Booster doses of SARS-CoV-2 mRNA vaccines are strongly recommended by public health and medical professionals—even more so during the recent surge in cases caused by the Omicron variant of concern—to lower the risk of symptomatic COVID-19 and more severe cases requiring hospitalization. Emerging data continue to support booster doses as both safe and effective for these purposes. A recent study published in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) found that vaccine effectiveness at preventing severe COVID-19 was higher after a booster dose than after the second dose of mRNA vaccine. The effectiveness of boosters wanes after about 4 months but remains highly protective against severe disease. These findings were consistent across both the Delta-dominant and Omicron-dominant periods. The findings support further consideration of additional booster doses that could be valuable against future outbreaks or variants.
Despite booster doses being highly effective in preventing emergency department visits and hospitalizations due to COVID-19, public uptake of booster doses has slowed in recent months in the US. A survey from the Kaiser Family Foundation found that 60% of vaccinated but not boosted respondents stated that the Omicron wave did not greatly impact their decision whether or not to get a booster. Only around 29% of respondents reported that the Omicron wave made them more likely to get a booster shot. Additional data from the CDC on hospitalizations and deaths show that booster doses are most beneficial to older adults. The argument for booster doses is strongest in those aged 65 years and older, for whom booster doses reduced the death rate per 100,000 cases by around 90 times. More work still needs to be done to better understand the durability of immunity following booster doses as well as to encourage more people, particularly those in higher-risk populations, to receive their booster doses.
COVID-19 THERAPEUTICS Late last week, the US FDA authorized a new monoclonal antibody (mAb) treatment that reportedly retains activity against the SARS-CoV-2 Omicron variant in laboratory experiments. The treatment—known as bebtelovimab and made by Eli Lilly—received Emergency Use Authorization (EUA) for adults and certain pediatric patients who are at high risk of severe COVID-19 outcomes but was not authorized for hospitalized COVID-19 patients or those requiring supplemental oxygen. Eli Lilly has signed a contract with the US government to supply up to 600,000 doses of the treatment by March 31, with the option for an additional 500,000 doses to be delivered later this year, at a cost of at least US$720 million. The company said it will immediately begin shipments to fulfill the agreement. Many providers expressed gratitude for the authorization, after the US government halted the use of 2 of the most common monoclonal antibody treatments due to a loss of effectiveness against Omicron.
Also late last week, the WHO prequalified a different mAb treatment, tocilizumab, that inhibits the interleukin-6 (IL-6) receptor. The prequalification includes 3 different presentations of the treatment and represents the first mAb to receive the designation. Tocilizumab—which is used primarily to manage arthritis and has been the subject of many COVID-19 clinical trials, including the large RECOVERY trial—is prequalified only for patients diagnosed with severe or critical COVID-19. The RECOVERY trial continues its work to establish an empirical baseline of effectiveness for other therapeutics. In a study published February 12 in The Lancet, the RECOVERY Collaborative Group summarized the results of evaluation of the monoclonal antibodies casirivimab and imdevimab used in combination. Between September 2020 and May 2021, the combination treatment reduced 28-day mortality in patients who were seronegative at baseline—meaning they had not mounted their own immune response—but not among individuals who were seropositive at baseline. However, when all patients were considered together, the treatments had no significant difference in outcomes. The results support the use of the combination therapy only among hospitalized individuals who are seronegative.
Questions remain over how well mAb treatments work against Omicron, as well as its BA.2 sublineage. Vir, the producer of the mAb sotrovimab, published a press release last week stating that its treatment retains neutralizing activity against the BA.2 sublineage of Omicron. The laboratory data, which are expected to be posted to a preprint server this week, are not yet peer-reviewed. Conversely, a separate study posted to bioRxiv (also not yet peer-reviewed) found BA.2 exhibited resistance to sotrovimab. Other therapies, including the antivirals Paxlovid and remdesivir, remain effective at reducing the risk of COVID-19-associated hospitalization or severe disease, but supply constraints and administration challenges are limiting access to only the highest-risk patients.
US VACCINE MANDATES New York City last week fired 1,430 municipal employees—less than 1% of the city’s workforce—for not complying with the city’s SARS-CoV-2 vaccination mandate. About 95% of the city’s 370,000 workers have received at least 1 dose of vaccine. Approximately 9,000 workers remain unvaccinated and are seeking exemptions but still could face termination. A majority of the fired employees, about 900, worked at the Department of Education. On February 11, the US Supreme Court denied a request from a group of New York City public school teachers, administrators, and staff seeking to block the mandate for employees who were not granted religious exemption. Those involved in the lawsuit were told they would be fired if they did not get vaccinated by February 14.
In compliance with the US Department of Defense vaccine mandate for military personnel, the US Navy and US Army announced they have begun discharging unvaccinated soldiers. The US Air Force last week said it has granted 9 religious exemptions and continues to process 2,556 pending requests and 732 pending appeals. Overall, the Air Force has turned down more than 3,200 requests for exemptions and approximately 440 appeals. The US Navy has not yet granted any religious exemptions.
CANADIAN PROTESTS After being closed for nearly a week because of demonstrations against COVID-19 vaccine mandates and restrictions, the Ambassador Bridge—the busiest US-Canada border crossing—reopened late February 13 after police made more than 2 dozen arrests, towed 7 vehicles, and seized 5 others. The bridge, which links Ontario to Detroit, is a major artery for the transport of vehicle parts from Canada to automotive plants in the US. Protests continue to block border crossings between Emerson, Manitoba, and Pembina, North Dakota, and Coutts, Alberta, and Sweet Grass, Montana. Additionally, demonstrations that began January 29 continue in the Canadian capital of Ottawa, disrupting transportation and daily activity. On February 14, Canada Prime Minister Justin Trudeau announced he is invoking the Emergencies Act, allowing the government the authority to “restore order.” The unusual move is meant to counter acts of lawlessness seen during the protests, according to Canada Public Safety Minister Marco Mendicino, who called the move “very careful and deliberate.”
Earlier on February 14, TD Bank—short for Toronto-Dominion Bank—froze approximately US$1.1 million that was intended to go to groups supporting the “Freedom Convoy” leading the Ottawa demonstrations, most of which came from a GoFundMe account that was shut down. TD Bank has said it wants the courts to decide where the money should go. After the GoFundMe account was shuttered, a crowdsourcing site on GiveSendGo began to raise money. Late last week, an Ontario Superior Court decision to grant the Canadian government authority to freeze access to any money raised to back the blockade. Meanwhile, GiveSendGo said it could continue to deliver money to protestors, but the site was hacked late on February 13, with hackers releasing the names of donors. Also on February 14, Ontario Premier Doug Ford announced the province will no longer require proof of vaccination to enter indoor spaces as of March 1 due to a decreasing number of COVID-19 cases and hospitalizations. He clarified that the restrictions were not being lifted in response to the demonstrations.
ASIA Several nations and regions in Asia have experienced increases in new COVID-19 cases following Lunar New Year celebrations held early this month, with governments grappling with how to respond to the Omicron variant that has found its way through strict border controls. Hong Kong is experiencing a record surge in cases, reporting more than 2,000 new cases on February 14. The outbreak is overwhelming hospitals, forcing schools to remain closed, and necessitating help from China to address what Hong Kong Chief Executive Carrie Lam called an “aggravating situation.” Hong Kong has been following the mainland’s zero-COVID strategy by isolating all patients in hospitals to suppress transmission, but this outbreak is testing the limits of that policy. For now, there are no plans for a strict lockdown in Hong Kong, although a more-intrusive contact-tracing app is being used to restrict the movements of unvaccinated individuals.
China is continuing to enforce its zero-COVID policy, shutting down entire cities and holding the Beijing Winter Olympics in a strict “closed-loop” bubble that some have criticized as excessive. A paper published last week in the weekly bulletin of the China Center for Disease Control and Prevention (CCDC) estimated that if the global vaccination rate was 95% and population mobility returned to 2019 levels, zero-COVID regions would see more than 234 million new cases in 1 year, including 2 million deaths. Without the development of more effective and durable vaccines, a constellation of public health mitigation measures will need to be continued to stave off further crises, although most experts agree that China’s widespread lockdowns are extreme.
by Suliso Swiss government has decided to "cancel" covid from tomorrow. All regulations are overturned except masks in hospitals, retirement homes and public transport (till the end of March). Covid certificates will be no longer in use within the country and government's covid task force will be disbanded at the end of the March.
Not sure if individual businesses and municipalities will play any role or how quickly my company will follow. Interesting times...
by Deuce ^ I used to do something similar when I was 3 years old... I believed that others couldn't see me if I closed my eyes.
Apparently, 2 years is all humans can tolerate of a potentially deadly virus. At that point, they begin to believe they can simply wish it away.
"We don't want to deal with COVID-19 anymore, so if we pretend hard enough that it no longer exists, it will surely disappear."
Protective measures are being lifted in many countries - despite many medical professionals saying that doing so is ill-advised. These decisions to lift protective measures have a far more political foundation than a medical one.
by Suliso Also Djokovic is welcome too - all entry restrictions have been canceled as well. Nobody cares anymore about your vaccination status or where you come from.
by ponchi101 So I guess it becomes a truly personal decision.
Just to be sure: vaccination is still available, right? If you feel like keeping up with some sort of protection scheme.
by Suliso
ponchi101 wrote: ↑Wed Feb 16, 2022 3:53 pm
Just to be sure: vaccination is still available, right? If you feel like keeping up with some sort of protection scheme.
Yes of course. Available, free and encouraged. Albeit I doubt those who haven't had their 3 shots already will bother now.
by ti-amie
by dryrunguy Here's the latest Situation Report. Lots of interesting stuff here. First, I cannot believe there are serious discussion underway to reduce or completely eliminate U.S. funding for global vaccination. Unbelievable. After that, the sections on excess deaths, vaccination during pregnancy, and the Swedish study of estrogen levels among older women were super interesting reads. The last section on the plight of immunocompromised people as everyone rushes to "get back to normal" was downright depressing.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 414.5 million cumulative cases and 5.83 million deaths worldwide as of February 16. The global cumulative incidence passed 400 million cases on February 9, only 33 days after reaching 300 million. The global weekly incidence continues to decline, down 18.2% from the previous week. Notably, all WHO regions with the exception of the Western Pacific region (+18.7%) reported decreasing weekly incidence last week.
Global weekly mortality remained relatively steady, up 0.5% from the previous week. The weekly total of 73,145 deaths is the highest since the week of August 23, 2021—the peak of the previous wave.
Global Vaccination
The WHO reported 10.2 billion cumulative doses administered globally as of February 14. A total of 4.84 billion individuals have received at least 1 dose, and 4.21 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations began to increase last week, closely following the trend in Asia. The trend is up from the most recent low of 18.32 million doses per day on February 7 to 22.1 million per day on February 15.* The global weekly average jumped to 29.5 million doses per day on February 16, corresponding to a large increase reported in Asia and may be a reporting error.** Our World in Data estimates that there are 4.88 billion vaccinated individuals worldwide (1+ dose; 62% of the global population) and 4.28 billion who are fully vaccinated (54.4% of the global population). A total of 1.23 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
**The OWID data show 16.3 million doses reported in Asia on February 15 and 24.1 million on February 16 (+7.8 million), but it is not immediately clear what country or countries accounted for that increase.
UNITED STATES
The US CDC is currently reporting 77.95 million cumulative cases of COVID-19 and 923,067 deaths. Daily incidence continues its sharp decline, down from a record high of 807,120 new cases per day on January 15 to 134,468 on February 15, an 83% decrease over 4 weeks. Average daily incidence is now below the peak of the previous wave. Daily mortality appears to have peaked on February 1 at 2,516 deaths per day, down to 2,100 on February 15.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 677.8 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to decline, down from the most recent peak of 1.78 million doses per day on December 6 to 429,530 on February 11.* A total of 252.4 million individuals have received at least 1 vaccine dose, which corresponds to 76% of the entire US population. Among adults, 87.6% have received at least 1 dose, as well as 26.3 million children under the age of 18. A total of 214 million individuals are fully vaccinated**, which corresponds to 64.5% of the total population. Approximately 74.6% of adults are fully vaccinated, as well as 21.5 million children under the age of 18. Since August 2021, 92.2 million individuals have received an additional or booster dose. This corresponds to 46.3% of fully vaccinated individuals, including 65.7% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
US RESPONSE Daily COVID-19 incidence has dropped sharply over the past month in the US, and many states are rolling back mitigation measures, including masking requirements for public spaces and schools. Additionally, some Republicans in the US Congress are urging US President Biden to end the designation of COVID-19 as a public health emergency. Based on comments from the White House COVID-19 Response Team on February 16, it appears the Biden administration is working on a plan for the next phase of the pandemic. White House Coronavirus Response Coordinator Jeff Zients said the country has made “tremendous progress” and the Biden administration is actively planning for a future “when COVID isn’t a crisis.” US CDC Director Dr. Rochelle Walensky said the agency wants to “give people a break” from mask wearing and expects to update its indoor masking guidelines as early as next week. The CDC reportedly is shifting its focus to COVID-19 hospitalizations as a key benchmark for determining when mitigation measures can be lifted or tightened. The Biden administration this week requested US$30 billion in additional funding for the domestic pandemic response. According to an anonymous source, the majority of the money would go toward vaccines and therapeutics (US$17.9 billion), with the remainder split among testing, care for uninsured individuals, and future variants. There is bipartisan skepticism surrounding the need for additional pandemic funding, with several members of Congress saying the American Rescue Plan provided plenty of support.
Notably, the funding request does not contain additional money for global vaccination efforts in low- and middle-income countries (LMICs), efforts that are running low on funds. A group of Democratic lawmakers is pushing for an additional US$17 billion for the global COVID-19 response, and USAID has said it needs an additional US$19 billion in 2022 to complete its COVID-related work. According to reporting from Politico, the White House’s proposed global COVID-19 supplemental funding request is US$10.95 billion, although it is unclear whether the Biden administration will officially request that money. In a virtual meeting with other countries earlier this week, US Secretary of State Antony Blinken acknowledged the world is not on pace to reach the goal of vaccinating 70% of the world’s population by later this year. Secretary Blinken announced a “Global Action Plan,” with a focus on overcoming last-mile challenges to deliver and administer vaccines in LMICs. President Biden is expected to hold another international vaccine summit next month, although details on the meeting are not yet available.
US EXCESS DEATHS The US CDC’s National Center for Health Statistics (NCHS) has been tracking excess deaths associated with the COVID-19 pandemic in the United States, crossing the threshold of 1 million excess deaths last week. Excess deaths are defined as the number of unexpected observed deaths to occur during a specific time period. This statistic can aid in further elucidating the burden of COVID-19, documenting both mortality directly caused by the virus as well as deaths indirectly caused by the pandemic’s impact. The NCHS’s excess death dashboard associated with COVID-19 breaks down deaths by direct cause, time, age and race/ethnicity. Dr. Robert Anderson, Chief of Mortality Statistics at NCHS, noted to The Washington Post that 91% of the excess deaths associated with COVID-19 were directly attributed to the disease, while the other 9% of excess deaths had COVID-19 listed as a contributing factor. These non-COVID-19 deaths were attributed to 13 other conditions, with Alzheimer’s disease and dementia, hypertensive diseases, and diabetes showing the greatest increases. Excess deaths not directly attributable to COVID-19 could be due to undiagnosed COVID-19 or conditions exacerbated by the pandemic’s impacts on society, including poorer healthcare due to health system strain or patients reluctant to seek care for other conditions while trying to avoid COVID-19. Timing of excess deaths appears to coincide with surges in SARS-CoV-2 transmission during the pandemic beginning in late March 2020.
US CDC TRAVEL GUIDANCE The US CDC is warning travelers to avoid at least 135 destinations, this week moving several countries—including South Korea, Azerbaijan, and Belarus—to its level 4 COVID-19 risk category due to “very high” transmission levels. The agency warned that people who must travel to these areas be fully vaccinated before going. Several nations moved into the “high” level 3 category, with Eswatini and Mauritius dropping a level and El Salvador and Indonesia moving up from lower levels. Notably, the CDC lowered the cruise travel warning from “very high” to “high,” recommending that travelers be “up to date” on vaccinations—meaning completing a primary series and a booster dose—before vacationing on a cruise ship. The agency recommended prospective cruise ship passengers get tested prior to departures, check to see if the ship has reported COVID-19 cases, and see if the majority of crew and passengers will be vaccinated. CDC’s Conditional Sailing Order, which outlined mandatory rules cruise companies had to follow to operate in US waters, expired on January 15, allowing operators to implement voluntary mitigation measures and choose whether to participate in the agency’s COVID-19 Program for Cruise Ships. According to the agency, 14,803 COVID-19 cases were reported on cruise ships between December 30, 2021, and January 12, 95 times the number reported during the first 2 weeks of December 2021.
VACCINATION DURING PREGNANCY As reported here previously, evidence shows people who receive SARS-CoV-2 vaccinations during pregnancy pass along more durable antibodies to their newborns than do unvaccinated individuals who had COVID-19 during pregnancy. Now, a study published in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) suggests that completion of a 2-dose primary mRNA vaccination series during pregnancy is associated with a reduced risk for COVID-19 hospitalization among infants aged <6 months. For women who completed the series at any time during pregnancy, vaccine effectiveness against COVID-19-associated hospitalization in infants aged <6 months was 61% (95% CI: 31% to 78%). Vaccine effectiveness against infant hospitalization was 32% (95% CI: –43% to 68%) for women who completed vaccination during the first 20 weeks of pregnancy and 80% (95% CI: 55% to 91%) for women who completed vaccination late in pregnancy, at 21 weeks’ gestation through 14 days before delivery. The case-control study recruited participants from 20 pediatric hospitals in 17 states from July 2021 to January 2022, with 176 hospitalized infants with COVID-19 and 203 hospitalized infants without COVID-19. This news could bring some comfort to prospective parents concerned by the recent increase in hospitalization among children under the age of 5 who are not yet eligible for vaccination against COVID-19. Further research results on the effects of COVID-19 variants and vaccination among pregnant women and newborns is expected in May 2022 with the University of Oxford launching a global study this week involving 40 medical institutions and 4,500 pregnant women.
ESTROGEN LEVELS Higher estrogen levels may be associated with a decreased risk of dying from COVID-19 among older women who take supplements of the hormone, according to a study published in the February issue of BMJ Open. All of the 14,685 postmenopausal Swedish women, aged 50 to 80 years, included in the study had COVID-19 between February 1 and September 14, 2020. They were grouped based on estrogen levels, with women receiving endocrine therapy because of breast cancer representing lower estrogen levels, women on hormone replacement therapy representing higher levels, and a control group of women who had received neither therapy. The adjusted odds ratio (OR) for death following COVID-19 remained statistically significant for only the higher estrogen group with OR 0.47 (0.34 to 0.63), a risk reduction of more than half. Absolute risk of death was 4.6% for the control group versus 10.1% and 2.1%, for the decreased and increased estrogen groups, respectively. The researchers noted that the risk of death from COVID-19 was significantly associated with age, annual income, and education, and they recommended further clinical trials testing the use of estrogen supplementation as a COVID-19 therapy among postmenopausal women.
LONG COVID/PASC Researchers continue to examine potential causes for post-acute sequelae of SARS-CoV-2 infection (PASC), otherwise known as post-COVID condition or long COVID, with recent findings pointing to vagus nerve dysfunction (VND), microclots, or inflammation as possible underlying factors or opportunities for treatment. The range of symptoms that people with long COVID experience—including fatigue, shortness of breath, joint and muscle pain, cognitive problems, depression, headache, and rapid heartbeat—call for a multidisciplinary approach to treatment, according to researchers who are developing a consensus statement (preprint) on core outcomes of long COVID in adults.
Studies differ on how many people experience long COVID symptoms, with one US CDC study estimating 1 in 10 will develop symptoms more than a month after acute infection and another from Oxford University estimating 1 in 3 individuals. While some see their symptoms resolve within weeks or months, others are experiencing nagging symptoms that have lasted a year or more. Additionally, evidence is emerging that people who have had COVID-19—including those with mild cases and who do not have typical long COVID symptoms—have an increased risk of cardiovascular disease and mental health conditions when compared with individuals who have never had the disease. Therefore, millions of people worldwide could experience long COVID or future health implications, with lasting societal and economic impacts. In a survey of 804 organizations representing more than 4.3 million employees in the UK, the Chartered Institute of Personnel and Development (CIPD) found that 46% of the organizations had employees who experienced long COVID and 26% of those employers now include long COVID as a primary cause of long-term sickness absence. In the UK, 1.3 million people—2% of the population—reported experiencing long COVID symptoms for more than 4 weeks after their initial infection.
This week the UK Health Security Agency released a rapid review examining available evidence from 15 studies conducted around the world prior to January 12, 2022, to determine the effectiveness of SARS-CoV-2 vaccination against long COVID. The analysis suggests that individuals who are fully vaccinated against COVID-19 have a significantly reduced risk of developing long COVID symptoms compared to partially vaccinated or unvaccinated individuals, and those currently suffering long COVID who are unvaccinated may experience some improvement if they get the shots. The review underscores the importance of vaccination in lowering the risk of infection in the first place and the potential to lower the risk of long-term symptoms if a breakthrough infection occurs.
IMMUNOCOMPROMISED INDIVIDUALS US states’ rollbacks of certain COVID-19 restrictions and mask mandates signal a bit more freedom is on the horizon for some. But for immunocompromised people, who are at high risk of infections including SARS-CoV-2, the relaxation of public health measures places them in a sort of limbo, unsure about their safety in a world where the coronavirus continues to circulate and people are returning to pre-pandemic activities. At least 7 million people in the US take immunosuppressive drugs, and millions more have conditions that inhibit immune responses, including HIV and genetic disorders. They are less likely to mount a significant immune response to SARS-CoV-2 vaccinations, even after 3, sometimes 4, doses. Many immunocompromised people feel vulnerable, left behind by a nation that is increasingly loosening precautions such as masking and working from home without any consideration of how to keep them safe. Vaccinating more of the US population, improving ventilation systems, and taking other steps to limit the amount of circulating virus would help. Additionally, making prophylactic antibody treatments such as Evusheld more widely available to immunocompromised people—as Israel did this week—and improving access to other COVID-19 treatments for the highest-risk patients could help some return to more of a sense of normalcy. The US government has announced it plans to convene a working group of advocates for people with vulnerabilities, but in the meantime, immunocompromised people continue to feel abandoned, isolated, frustrated, and fearful.
by JazzNU FYI, I got my covid tests in the mail yesterday. Email shipping notification with tracking number from USPS came around midnight early yesterday morning saying delivery by Saturday, then 6 hours later received an email saying out for delivery. So it may happen pretty quick like that just so you know if you have yet to receive yours.
by dmforever I got mine a couple of days ago too.
Kevin
by Deuce Nothing was more predictable than this...
(complete with predictable government 'spin')
This is a perfect example of what happens when politics drive decisions, and common sense is ignored in favour of merely trying to wish something away.
by ponchi101
dryrunguy wrote: ↑Thu Feb 17, 2022 6:46 pm
Here's the latest Situation Report. Lots of interesting stuff here. First, I cannot believe there are serious discussion underway to reduce or completely eliminate U.S. funding for global vaccination. Unbelievable. After that, the sections on excess deaths, vaccination during pregnancy, and the Swedish study of estrogen levels among older women were super interesting reads. The last section on the plight of immunocompromised people as everyone rushes to "get back to normal" was downright depressing.
...
Serious questions.
How should the world pay for the vaccination of countries? Should the US/EU/Rich countries pay for the rest of the world vaccines? I gave an example of something Colombia is NOT doing: they are not planning for any kind of local vaccination production, while at the same time, they are paying for $300 million for combat planes, to defend themselves from who knows who.
What can be done for the immunocompromised population? Is there a way that they can remain protected while the rest of the population returns to activities?
Again, serious questions. I don't know how to manage these scenarios.
by ti-amie
Deuce wrote: ↑Fri Feb 18, 2022 12:16 am
Nothing was more predictable than this...
(complete with predictable government 'spin')
This is a perfect example of what happens when politics drive decisions, and common sense is ignored in favour of merely trying to wish something away.
by Deuce ^ I suppose it was inevitable that eventually, human beings - the most arrogant and stupid of Earth's species - would become victims of themselves to the point of eliminating themselves.
We may have reached that point now.
dryrunguy wrote: ↑Thu Feb 17, 2022 6:46 pm
Here's the latest Situation Report. Lots of interesting stuff here. First, I cannot believe there are serious discussion underway to reduce or completely eliminate U.S. funding for global vaccination. Unbelievable. After that, the sections on excess deaths, vaccination during pregnancy, and the Swedish study of estrogen levels among older women were super interesting reads. The last section on the plight of immunocompromised people as everyone rushes to "get back to normal" was downright depressing.
...
Serious questions. How should the world pay for the vaccination of countries? Should the US/EU/Rich countries pay for the rest of the world vaccines? I gave an example of something Colombia is NOT doing: they are not planning for any kind of local vaccination production, while at the same time, they are paying for $300 million for combat planes, to defend themselves from who knows who.
What can be done for the immunocompromised population? Is there a way that they can remain protected while the rest of the population returns to activities?
Again, serious questions. I don't know how to manage these scenarios.
There are no clean answers to either of your questions, ponchi. The question you post about Colombia's spending on planes could be easily re-directed right back to the U.S. Why are we giving obscene tax breaks to those who are already rich? Should we punish poor countries for funding indiscretions when we are guilty of far worse fiscal indiscretions and irresponsibility? Who really deserves to be punished more harshly?
As for the immunocompromised, in an ideal world, unvaccinated and COVID-positive people would stay home and not risk the well-being of others by venturing out. Those people should be staying in their home caves watching OAN and Duck Dynasty re-runs. But we don't live in that world--at least not in the U.S. Because, you know, freedumb. If we actually cared about each other and respected science, as a society, this wouldn't be a thing. Period. But it is. And that's the unfortunate and harsh reality in which immunocompromised people live.
by JazzNU
dryrunguy wrote: ↑Fri Feb 18, 2022 4:25 am
As for the immunocompromised, in an ideal world, unvaccinated and COVID-positive people would stay home and not risk the well-being of others by venturing out. Those people should be staying in their home caves watching OAN and Duck Dynasty re-runs. But we don't live in that world--at least not in the U.S. Because, you know, freedumb.
dryrunguy wrote: ↑Thu Feb 17, 2022 6:46 pm
Here's the latest Situation Report. Lots of interesting stuff here. First, I cannot believe there are serious discussion underway to reduce or completely eliminate U.S. funding for global vaccination. Unbelievable. After that, the sections on excess deaths, vaccination during pregnancy, and the Swedish study of estrogen levels among older women were super interesting reads. The last section on the plight of immunocompromised people as everyone rushes to "get back to normal" was downright depressing.
...
Serious questions.
How should the world pay for the vaccination of countries? Should the US/EU/Rich countries pay for the rest of the world vaccines? I gave an example of something Colombia is NOT doing: they are not planning for any kind of local vaccination production, while at the same time, they are paying for $300 million for combat planes, to defend themselves from who knows who.
What can be done for the immunocompromised population? Is there a way that they can remain protected while the rest of the population returns to activities?
Again, serious questions. I don't know how to manage these scenarios.
From an altruistic point of view, it would be awesome if countries with more resources gave vaccines to poorer countries regardless of their military spending because, as others have said, we are hardly ones to talk in that regard. However, even if you as a country want to be super selfish and only think about your own people, it sill makes sense to make sure the rest of the world gets vaccinated. If it isn't painfully clear by now that viruses don't respect borders, then it will never be clear.
That' said, the point becomes sort of moot when such a large percentage of the population won't get vaccinated.
Kevin
by Suliso Is it really a problem anywhere at this stage that vaccines are not available?
by ponchi101 I am reading a book, totally unrelated to the pandemic, which made a great point that applies here to the USA. The author mentions (and I do remember this) that when seatbelts laws made them mandatory, there were plenty of people that would not wear them because (get ready for this) it was trampling on their freedoms. Exactly like now.
And I do remember some of those people. With time, we all accepted that reality.
by dryrunguy
ponchi101 wrote: ↑Fri Feb 18, 2022 3:18 pm
I am reading a book, totally unrelated to the pandemic, which made a great point that applies here to the USA. The author mentions (and I do remember this) that when seatbelts laws made them mandatory, there were plenty of people that would not wear them because (get ready for this) it was trampling on their freedoms. Exactly like now.
And I do remember some of those people. With time, we all accepted that reality.
I was a kid when seat belt laws went into effect in Ohio. I don't remember anyone complaining about loss of freedom. I'm sure it happened, though.
When those laws went into effect, what I DO remember is hearing story after story after story about people who were in serious car accidents and how, as the story always seemed to go, the paramedics always said the same thing to people standing around or to family members: "Oh yes, if she had been wearing her seat belt, she certainly would have been killed."
::
And while we're talking about horribly oppressive laws, how about drivers' licenses? Speed limits? Having to register a car or livestock trailer? Using turn signals? Being required to get a permit to build a structure on your own property or to make an addition to your home? Passing meat or food inspections? Tobacco or alcohol sales to people under 21? Drunk or drugged driving? Yielding to pedestrians? Stopping at stop signs or red lights? Having proof of insurance? I could go on and on...
by JazzNU One of my favorite doctors that appears now and then on MSNBC has said many times that visualizations are necessary to drive the point home. That the anti-smoking campaign was successful by leveraging visceral images that conveyed facts. He's a pulmonologist and has repeated shown on TV and on his social media the difference between lungs with covid and lungs without covid. There are articles in medical journals with similar photos that get appreciably more views than the other articles. It's a strategy that has worked before and is working again, they just need more and more people with knowledge conveying the danger of covid in a similar manner.
by ponchi101 I see only one problem with C19. I will take my looney friend N as an example.
One of the reasons he says that this is not important is because he and his 28 & 26 yo sons got it, and they all did well. A bit of a fever, and of course, the ivermectin worked (yes, I know).
With smoking, there is no ambiguity. A few years of smoking will leave its marks. One has to admit that C19 is not as destructive and many people got it and are doing fine. But it is only when you see a family member (you had your aunt, I had my mom) that you get how damaging this can be. And I agree that my mom was lucky, as she has fully recovered.
So I agree that conveying the danger is crucial. But with people that do not grasp the stats, it will be difficult.
ponchi101 wrote: ↑Fri Feb 18, 2022 3:18 pm
I am reading a book, totally unrelated to the pandemic, which made a great point that applies here to the USA. The author mentions (and I do remember this) that when seatbelts laws made them mandatory, there were plenty of people that would not wear them because (get ready for this) it was trampling on their freedoms. Exactly like now.
And I do remember some of those people. With time, we all accepted that reality.
I was a kid when seat belt laws went into effect in Ohio. I don't remember anyone complaining about loss of freedom. I'm sure it happened, though.
When those laws went into effect, what I DO remember is hearing story after story after story about people who were in serious car accidents and how, as the story always seemed to go, the paramedics always said the same thing to people standing around or to family members: "Oh yes, if she had been wearing her seat belt, she certainly would have been killed."
So, I wasn't even in existence, but yeah, that's what happened.
Boring recap - basically what it is now, grumbling about infringements on freedom. Can't think of the correct acronym for the agency, but it's like NTSB, but for highways. They passed some rule requiring seat belts. People were in an uproar about their freedoms. So Congress acted and essentially invalidated the rule. Then the agency passed something else a few years later, this time under Carter, a similar but slightly different rule that required safety restraints to help with preventing injuries over a certain speed limit. Before that rule could take effect, Reagan was elected. He was promising massive deregulation of consumer and environmental protections. Took office, got rid of the rule very soon into his presidency. And I believe it was a lobby on behalf of the insurers, obviously quite the vested interested in safety restraints, that sued the Reagan administration to re-instate the the discarded safety rule. Reached the Supreme Court, and the Court agreed with the insurers in an unanimous decision. Big loss for Reagan. It's a landmark decision. Administrations can't just get rid of a rule that an agency passed arbitrarily.
Now in practice, one of the main things that got more people wearing seat belts were the mandatory laws imposing fines that passed in almost every state. And in many states, it became a primary offense, meaning that can be the sole reason you are pulled over, it doesn't have to be you're speeding and then they see someone isn't wearing a seatbelt and ticket you for that too.
Not sure if it'll jog anyone's memory, hard for me to understand how big his profile was at the time, but seatbelts and ensuring advancements in car safety were one of Ralph Nader's main crusades at one point in time, so you might remember him pushing for it and who was against it more than the details I'm giving above.
by JazzNU
ponchi101 wrote: ↑Sat Feb 19, 2022 4:12 am
I see only one problem with C19. I will take my looney friend N as an example.
One of the reasons he says that this is not important is because he and his 28 & 26 yo sons got it, and they all did well. A bit of a fever, and of course, the ivermectin worked (yes, I know).
With smoking, there is no ambiguity. A few years of smoking will leave its marks. One has to admit that C19 is not as destructive and many people got it and are doing fine. But it is only when you see a family member (you had your aunt, I had my mom) that you get how damaging this can be. And I agree that my mom was lucky, as she has fully recovered.
So I agree that conveying the danger is crucial. But with people that do not grasp the stats, it will be difficult.
Actually this isn't necessarily true. So this is part of what some doctors have tried to message. It just hasn't gotten thru loudly all the time. People get covid and they think they are fine, and they may actually be in the long term. But a scan of their lungs pre- and post-covid would likely exihibit something that doesn't resemble "recovered." In patients with symptoms there was scaring almost 100% of the time, and I believe it was 70% of the time in those who were asymptomatic. It was startling. The more acute the infection, the worse the scarring. But, people think they've fully recovered from a mild infection or no symptoms at all, but can have lung scarring. They are just highly unlikely to have a lung scan to know this. Sort of like smoking, which is another reason they've used that as an example. In both cases, the scarring can heal in time for many, maybe not back to a resemble a perfectly healthy lung, but something relatively close. I'm not sure if the numbers were the same with the Delta and Omicron variants, this was something that was studied by many in 2020 and early 2021 for sure.
Also, I have had a few family members die from covid long before my aunt got sick, she just happens to be one of my closest family members. But I've known personally very early on in the pandemic how damaging this disease can be.
ponchi101 wrote: ↑Fri Feb 18, 2022 3:18 pm
I am reading a book, totally unrelated to the pandemic, which made a great point that applies here to the USA. The author mentions (and I do remember this) that when seatbelts laws made them mandatory, there were plenty of people that would not wear them because (get ready for this) it was trampling on their freedoms. Exactly like now.
And I do remember some of those people. With time, we all accepted that reality.
I was a kid when seat belt laws went into effect in Ohio. I don't remember anyone complaining about loss of freedom. I'm sure it happened, though.
When those laws went into effect, what I DO remember is hearing story after story after story about people who were in serious car accidents and how, as the story always seemed to go, the paramedics always said the same thing to people standing around or to family members: "Oh yes, if she had been wearing her seat belt, she certainly would have been killed."
So, I wasn't even in existence, but yeah, that's what happened.
Boring recap - basically what it is now, grumbling about infringements on freedom. Can't think of the correct acronym for the agency, but it's like NTSB, but for highways. They passed some rule requiring seat belts. People were in an uproar about their freedoms. So Congress acted and essentially invalidated the rule. Then the agency passed something else a few years later, this time under Carter, a similar but slightly different rule that required safety restraints to help with preventing injuries over a certain speed limit. Before that rule could take effect, Reagan was elected. He was promising massive deregulation of consumer and environmental protections. Took office, got rid of the rule very soon into his presidency. And I believe it was a lobby on behalf of the insurers, obviously quite the vested interested in safety restraints, that sued the Reagan administration to re-instate the the discarded safety rule. Reached the Supreme Court, and the Court agreed with the insurers in an unanimous decision. Big loss for Reagan. It's a landmark decision. Administrations can't just get rid of a rule that an agency passed arbitrarily.
Now in practice, one of the main things that got more people wearing seat belts were the mandatory laws imposing fines that passed in almost every state. And in many states, it became a primary offense, meaning that can be the sole reason you are pulled over, it doesn't have to be you're speeding and then they see someone isn't wearing a seatbelt and ticket you for that too.
Not sure if it'll jog anyone's memory, hard for me to understand how big his profile was at the time, but seatbelts and ensuring advancements in car safety were one of Ralph Nader's main crusades at one point in time, so you might remember him pushing for it and who was against it more than the details I'm giving above.
I think you're thinking of NHTSA--National Highway Traffic and Safety Administration?
Fun fact--my first boss in the federal government was the woman who came up with the creative concept of the crash test dummies that were used in seat belt ads for ages. She was at NHTSA before she came to HHS.
by JazzNU
dryrunguy wrote: ↑Sat Feb 19, 2022 5:49 am
I think you're thinking of NHTSA--National Highway Traffic and Safety Administration?
Fun fact--my first boss in the federal government was the woman who came up with the creative concept of the crash test dummies that were used in seat belt ads for ages. She was at NHTSA before she came to HHS.
Yes, exactly.
by JazzNU
by JazzNU It was also approved in Canada last week.
by dryrunguy Here's the latest Situation Report. It includes a lengthy description of what we know so far about the family of Omicron subvariants. It also includes a discussion of fourth doses that completely contradicts the guidance provided last week or the week before.
::
BA.2 OMICRON SUBVARIANT The BA.2 subvariant of the SARS-CoV-2 Omicron variant of concern (VOC) is increasing in prevalence, but questions remain regarding whether it results in more severe disease. The Omicron VOC spans multiple subvariants, including the main B.1.1.529 lineage and the BA.1 and BA.2 sublineages. When Omicron emerged in the US, the rapid increase in prevalence was predominantly due to the B.1.1.529 and BA.1.1 lineages, which combined to account for nearly 99% of US cases the week of January 29. Since that time, the BA.2 lineage prevalence has increased from an estimated 0.8% to 3.8% of US cases, approximately doubling each of the past 2 weeks. The increase in prevalence indicates that BA.2 is more transmissible than the other Omicron lineages, possibly 30% more. Notably, genomic surveillance for the BA.2 lineage is difficult, because it does not result in the S-gene target failure (SGTF) in PCR-based assays, which has been used to track other VOCs—including Omicron—without requiring genomic sequencing. The BA.2 lineage has not yet taken off in the US, but the next several weeks will provide important information regarding the potential for a second Omicron surge.
Research is ongoing to better characterize protection against the BA.2 subvariant from vaccination, booster doses, and prior infection. Like the original Omicron variant, BA.2 is less susceptible to SARS-CoV-2 vaccines than previous VOCs, but booster doses can increase the vaccine effectiveness against symptomatic COVID-19 disease to 74%. The BA.2 lineage also appears to evade antibodies generated in response to prior infections with earlier strains, including the Alpha and Delta VOCs. There is some evidence that BA.2 is able to reinfect individuals who were previously infected with the BA.1 lineage, although the combination of prior infection and vaccination appears to provide moderate protection. Researchers in Denmark recently conducted a study to evaluate reinfection with the BA.2 lineage. Out of a sample of 187 reinfection cases (within 20-60 days), 47 were the result of BA.2 infection following infection with the BA.1 lineage. Conversely, a recent study by the UK government found “no detected sequence-confirmed BA.2 reinfection following a BA.1 infection at any interval.”
The data on disease severity for the BA.2 lineage are mixed. Some countries where BA.2 has become more prominent are exhibiting declining trends in daily COVID-19 mortality, such as the UK, whereas Denmark is exhibiting an increasing trend. Through the use of animal models, researchers have identified more extensive damage to lung tissue in hamsters infected with the BA.2 lineage compared to BA.1, but this may not necessarily hold true for humans. A study in South Africa found similar disease severity among patients infected with the BA.1 and BA.1 subvariants, and US CDC Director Dr. Rochelle Walensky indicated that “there is no evidence that the BA.2 lineage is more severe than the BA.1 lineage.” Evidence also indicates that the BA.2 subvariant exhibits strong resistance to many monoclonal antibody treatments, including sotrovimab, which is currently being used to treat patients infected with the Omicron variant. The lack of an effective treatment option could impact disease severity and mortality.
MENTAL HEALTH Results from the largest cohort study to date on the impact of acute COVID-19 on mental health were published February 16 in The BMJ. The cohort consisted of 153,848 individuals who survived 30 days after initial SARS-CoV-2 infection, and 2 control groups: 5.6 million individuals who did not have recorded SARS-CoV-2 infection and 5.8 million historical control individuals pulled from pre-pandemic data. All of the data came from a US Department of Veterans Affairs database. Overall, the study found that people who had COVID-19 were 60% more likely to experience subsequent mental health problems than people who never had the disease. Individuals who had COVID-19, even mild cases, had a 41% increased risk of developing sleep disorders, 39% increased risk of developing depression, 38% increased risk of heightened stress levels, 35% increased risk of developing anxiety, 34% increased risk of developing an opioid use disorder, and 80% higher risk of developing other cognitive symptoms, such as “brain fog.” Limitations of the study include that it was performed before vaccines were widely available and that the population primarily included older white men, although controlling for race, gender, and age found no difference in risk.
Growing evidence indicates that SARS-CoV-2 infection has the potential to impact nearly every organ system, including the nervous system. The exact mechanism behind the observed increase in mental health risks after SARS-CoV-2 infection is currently unclear, but one hypothesis suggests that the virus can enter the brain and damage areas responsible for mood and emotional regulation. An association between acute COVID-19 and long term increases in mental health disorders raises the likelihood that a wave of mental health symptoms could occur in the near future, given that nearly 425 million people worldwide have had COVID-19. The National Health Service (NHS) in England recently warned that millions of patients face dangerously long wait times for mental health services. Concerns are rising that a lack of investment in mental health care infrastructure could lead to an increase in suicide, self-harm, and eating disorders. Mental health services historically have been neglected worldwide, but they will need an increase in funding and attention if we want to be prepared for the coming increase in patient needs.
FOURTH VACCINE DOSE Questions about the necessity of a second SARS-CoV-2 vaccine booster, or fourth dose, arose shortly after announcements regarding the importance of an initial booster. Several new studies attempting to shine a light on the durability of vaccine-mediated immunity provide evidence that a 3-dose regimen of mRNA-based vaccines—possibly only 2 doses—may be able to protect most people against severe COVID-19 disease for months or even years. Evidence for possibly lengthy protection from vaccination includes an increase in neutralizing antibody diversity, T cells that can recognize the Omicron variant, and germinal center activation for up to 15 weeks post-vaccination. Leading immunologists have stated that fourth or fifth doses of the vaccine might lead to diminishing returns for the majority of the population when compared to 3 doses. However, a fourth vaccine dose may still be necessary for certain populations, including older and immunocompromised individuals.
Several nations have begun offering fourth vaccine doses to specific populations or openly discussing that possibility. Many health officials in the US have agreed that it is too early to officially recommend a fourth vaccine dose, but the US FDA is continually examining emerging data to determine if and when another booster may be necessary. If a fourth dose does appear to be warranted, for all age groups or only older adults, experts say it likely would be recommended in the fall to coincide with annual flu shots and the rise of respiratory virus transmission. Additional considerations include whether the vaccine should be reformulated for novel variants. Other nations are moving forward with plans to provide fourth doses to certain populations, including the UK, Italy, South Korea, Sweden, and Israel. While fourth doses of SARS-CoV-2 vaccine may be necessary for certain populations, it is critical to ensure that populations in low- and middle-income countries (LMICs) are not left behind. Vaccine equity must be addressed now so the world can be prepared for future pathogens with pandemic potential.
VACCINES IN AFRICA Egypt, Kenya, Nigeria, Senegal, South Africa, and Tunisia will be the first 6 countries in Africa to receive the technology needed to produce SARS-CoV-2 mRNA vaccines, WHO Director-General Dr. Tedros Adhanom Ghebreyesus announced February 18 at an event held at the European Union-African Union summit in Brussels. The technical information and training will come from the global mRNA technology transfer hub established by the WHO last year in Cape Town, South Africa, in order to expand mRNA vaccine manufacturing—for COVID-19 and other diseases in the future—to low- and middle-income countries (LMICs). As a hub partner, South Africa's Afrigen Biologics announced earlier this month that it has developed a version of the Moderna vaccine using publicly available information. While the EU is supporting the effort, the bloc received criticism at the summit for continuing to block a proposal at the World Trade Organization (WTO) for a temporary waiver of the TRIPS Agreement. South Africa President Cyril Ramaphosa, who has accused Europe of hoarding the vaccines, called on the EU to drop its opposition to a waiver, saying it is a matter of saving millions of lives rather than padding the pockets of a few pharmaceutical companies. At the summit’s closing press conference, European Commission President Ursula von der Leyen committed to reaching a solution on the matter by spring.
Moderna has said it will not enforce existing patents on its SARS-CoV-2 vaccine during the pandemic. But the company recently applied for patents related to its vaccine in South Africa, raising concerns the company will move to prevent the technology transfer hub from making its own version of the shot once the pandemic phase is declared over. Moderna Chief Executive Officer Stéphane Bancel said the company has not yet decided whether it will enforce patents in LMICs when the pandemic ends. In an interview with STAT, WHO Chief Scientist Dr. Soumya Swaminathan said the global health agency would like Moderna to not enforce its patents on its SARS-CoV-2 vaccine during and beyond the pandemic. Without Moderna’s assistance, the Afrigen-developed mRNA vaccine must go through human clinical trials and could take another 2 years to come to market. But the effort is seen as building a foundation for the production of future mRNA vaccines on the continent. Additionally, BioNTech last week announced it is deploying modular vaccine production facilities—housed in shipping containers and dubbed BioNTainers—to several African nations to help increase production of the company's current and future mRNA vaccines for COVID-19, malaria, tuberculosis, and cancer. The increased manufacturing capacity could be a sign of improving global vaccine equity, but much more needs to be accomplished to reach that goal, including billions more dollars of investment and efforts to increase vaccine uptake.
Meanwhile, the US Agency for International Development (USAID) last week released case studies from Côte d'Ivoire, Uganda, and Zambia detailing successful efforts to increase vaccination uptake, including actions by its Global Vaccine Access, or Global VAX, initiative. US officials announced the government will intensify assistance to 11 African countries under the initiative, efforts worth more than US$250 million. The countries—Angola, Côte d'Ivoire, Eswatini, Ghana, Lesotho, Nigeria, Senegal, South Africa, Tanzania, Uganda, and Zambia—were selected based on their COVID-19 incidence, healthcare system capacity, readiness to administer the vaccines, and ability to deploy additional US investments. On February 18, the administration of US President Joe Biden requested an additional US$5 billion for overseas COVID-19 response efforts, far less than the approximately US$19 billion USAID originally recommended would be needed. Of that funding, US$2.55 billion would be used for vaccinations, US$1.7 billion for therapeutics and supplies, and $750 million for humanitarian aid.
US STATES’ PANDEMIC ESCAPE PLANS Two days after the White House COVID-19 Response Team signaled that the administration of US President Joe Biden is planning for the pandemic to cease being a crisis, President Biden on February 18 announced he is continuing the designation of COVID-19 as a national emergency. Meanwhile, most US states have announced the end of or plans to end statewide indoor mask mandates—leaving Hawaii as the lone holdout. Many states and cities also have lifted their proof-of-vaccination requirements and called state and municipal employees back into the office after 2 years of work-from-home rules. Governors and mayors cite plummeting numbers of new COVID-19 cases, with the 7-day national average down 87% since January 15. California Governor Gavin Newsom last week announced California will move into the “next phase” of managing the pandemic, with a focus on early detection of variants, keeping schools open, wastewater surveillance, and stockpiling masks and tests. Newsom’s SMARTER plan—which stands for Shots, Masks, Awareness, Readiness, Testing, Education, and Rx—is billed as a response plan for COVID-19 as well as future health emergencies. Some state legislatures are taking additional steps to roll back public health measures, introducing legislation to restrict mask mandates, ban vaccine requirements, and revise visitation policies for long-term care facilities and hospitals.
A model from the Institute of Health Metrics and Evaluation (IHME) estimates that about three quarters of the US population currently is immune to Omicron due to natural immunity, vaccine-mediated immunity, or a combination. However, many experts warn that the currently circulating Omicron BA.2 sublineage or future variants could escape current immunity, and most are confident that existing immunity will wane. While the number of deaths is beginning to decline nationwide, around 2,000 people continue to die of COVID-19 each day, with unvaccinated individuals making up the majority of those deaths. Even California Governor Newsom acknowledged that there is no end date to the crisis, “not a moment where we declare victory.” But he said California’s plan will allow residents to shift from a “crisis mentality” to one relying on prevention and adaptability, with health officials stepping up measures to quell outbreaks when they occur. Still, experts who encourage control measures such as vaccination and masking continue to experience backlash and warn that trust in public health is at an all-time low. Notably, some evidence suggests trust, between people or in government or scientists, is the most critical factor in addressing crises such as COVID-19.
US CDC DATA According to reporting by The New York Times, the US CDC is sharing only a small portion of the data it collects on COVID-19, 2 full years into the pandemic. The data could help state and local officials better understand how and when to use specific mitigation measures, what populations are most at risk, who needs booster doses, and where outbreaks might occur or new variants emerge. CDC representatives gave various reasons why the agency has been slow to release some information, including outdated systems incapable of handling large amounts of data, fear that the information might be misinterpreted, and concerns over some data representing only a sampling of the US population. A string of necessary bureaucratic approvals also adds to the delays. Several epidemiologists and scientists said gaps in data have the potential to erode trust in public health and science and countered that the release of detailed data analyses and effective communication of that information can help bolster public trust and provide a better understanding of the pandemic.
OTTAWA PROTESTS Police in Ottawa, Canada, regained control of most of the capital city over the weekend after a push to disperse the so-called “Freedom Convoy.” The demonstration, which began in late January with protestors and far-right organizations denouncing COVID-19 vaccination requirements and other pandemic restrictions, turned into a 3-week-long occupation. Police arrested nearly 200 people, having to use pepper spray, stun grenades, and other anti-riot tactics, and vowed a months-long investigation leading to financial sanctions and criminal charges. The Ottawa police chief resigned last week after receiving criticism about why it took so long to break up the convoy.
The demonstration led Canada Prime Minister Justin Trudeau to invoke the Emergencies Act for the first time ever, in order to help quell the protests by permitting authorities to freeze bank accounts associated with the convoy and seize protestors’ vehicles. Last night, the House of Commons approved the Emergencies Act, extending its use for an additional 30 days. Prime Minister Trudeau said there “continues to be real concerns” and that the government will evaluate daily whether to continue the state of emergency. Royal Canadian Mounted Police (RCMP) said they have frozen more than 200 bank and corporate accounts worth several million Canadian dollars in relation to the protests. Now that the convoy has ended, many Canadians—including Ottawa residents, politicians, policy experts, and the demonstrators themselves—are wondering how the organized and financially backed protests might affect the country’s future political landscape.
by ti-amie
by ti-amie Dry posted:
Growing evidence indicates that SARS-CoV-2 infection has the potential to impact nearly every organ system, including the nervous system. The exact mechanism behind the observed increase in mental health risks after SARS-CoV-2 infection is currently unclear, but one hypothesis suggests that the virus can enter the brain and damage areas responsible for mood and emotional regulation. An association between acute COVID-19 and long term increases in mental health disorders raises the likelihood that a wave of mental health symptoms could occur in the near future, given that nearly 425 million people worldwide have had COVID-19. The National Health Service (NHS) in England recently warned that millions of patients face dangerously long wait times for mental health services. Concerns are rising that a lack of investment in mental health care infrastructure could lead to an increase in suicide, self-harm, and eating disorders. Mental health services historically have been neglected worldwide, but they will need an increase in funding and attention if we want to be prepared for the coming increase in patient needs.
US CDC DATA According to reporting by The New York Times, the US CDC is sharing only a small portion of the data it collects on COVID-19, 2 full years into the pandemic. The data could help state and local officials better understand how and when to use specific mitigation measures, what populations are most at risk, who needs booster doses, and where outbreaks might occur or new variants emerge. CDC representatives gave various reasons why the agency has been slow to release some information, including outdated systems incapable of handling large amounts of data, fear that the information might be misinterpreted, and concerns over some data representing only a sampling of the US population. A string of necessary bureaucratic approvals also adds to the delays. Several epidemiologists and scientists said gaps in data have the potential to erode trust in public health and science and countered that the release of detailed data analyses and effective communication of that information can help bolster public trust and provide a better understanding of the pandemic.
OTTAWA PROTESTS Police in Ottawa, Canada, regained control of most of the capital city over the weekend after a push to disperse the so-called “Freedom Convoy.” The demonstration, which began in late January with protestors and far-right organizations denouncing COVID-19 vaccination requirements and other pandemic restrictions, turned into a 3-week-long occupation. Police arrested nearly 200 people, having to use pepper spray, stun grenades, and other anti-riot tactics, and vowed a months-long investigation leading to financial sanctions and criminal charges. The Ottawa police chief resigned last week after receiving criticism about why it took so long to break up the convoy.
The demonstration led Canada Prime Minister Justin Trudeau to invoke the Emergencies Act for the first time ever, in order to help quell the protests by permitting authorities to freeze bank accounts associated with the convoy and seize protestors’ vehicles. Last night, the House of Commons approved the Emergencies Act, extending its use for an additional 30 days. Prime Minister Trudeau said there “continues to be real concerns” and that the government will evaluate daily whether to continue the state of emergency. Royal Canadian Mounted Police (RCMP) said they have frozen more than 200 bank and corporate accounts worth several million Canadian dollars in relation to the protests. Now that the convoy has ended, many Canadians—including Ottawa residents, politicians, policy experts, and the demonstrators themselves—are wondering how the organized and financially backed protests might affect the country’s future political landscape.
Thank you Dry. I will continue to wear my mask.
by ponchi101 Special thanks this week, Dry. As I am here in the USA we were wondering whether to get our 4th dose here, which will be easier than in Colombia. I gather now we can be as confused as what to do as the rest
(Still, serious thanks. We still need all the data we can get to make these decisions).
by dryrunguy You're welcome, ponchi. Tomorrow morning, I'll have a few hours to kill while dolphins is having a nerve kill done, so I'll use part of that time to swing by the pharmacy where I received both of my shots (once it opens) to ask them what they have been told and what they recommend regarding those of who started with J&J, then went Moderna, but don't fall into "waiting for fourth dose" territory. No one ever talks about our situation.
by JazzNU
dryrunguy wrote: ↑Wed Feb 23, 2022 10:12 pm
You're welcome, ponchi. Tomorrow morning, I'll have a few hours to kill while dolphins is having a nerve kill done, so I'll use part of that time to swing by the pharmacy where I received both of my shots (once it opens) to ask them what they have been told and what they recommend regarding those of who started with J&J, then went Moderna, but don't fall into "waiting for fourth dose" territory. No one ever talks about our situation.
I think that's a good idea.
Here's additional guidance from the CDC for immunocompromised who got J&J and then a MRNA booster. They say to get 2nd MRNA booster for a total of 3 doses.
dryrunguy wrote: ↑Wed Feb 23, 2022 10:12 pm
You're welcome, ponchi. Tomorrow morning, I'll have a few hours to kill while dolphins is having a nerve kill done, so I'll use part of that time to swing by the pharmacy where I received both of my shots (once it opens) to ask them what they have been told and what they recommend regarding those of who started with J&J, then went Moderna, but don't fall into "waiting for fourth dose" territory. No one ever talks about our situation.
I think that's a good idea.
Here's additional guidance from the CDC for immunocompromised who got J&J and then a MRNA booster. They say to get 2nd MRNA booster for a total of 3 doses.
Thanks, Jazz. So that's different than anything I've read to this point. According to that, what does "at least 2 months after" of the second done of Moderna mean? Right now, I'm at the 2 month threshold after my second dose and my first dose of Moderna. Is there a reason to believe it would preferable to wait another month or two to get the third jab? And to what degree does the fact that 6 months lapsed between my initial J&J dose and my first Moderna dose mean? (Because that was the guidance at the time. I got my second dose as soon as I read that existing evidence (again, at that time) indicated that the J&J vaccine MIGHT only be good for 4 months.
And I am not immunocompromised (as far as I know).
It's all so confusing.
by JazzNU
dryrunguy wrote: ↑Wed Feb 23, 2022 10:37 pm
Thanks, Jazz. So that's different than anything I've read to this point. According to that, what does "at least 2 months after" of the second done of Moderna mean? Right now, I'm at the 2 month threshold after my second dose and my first dose of Moderna. Is there a reason to believe it would preferable to wait another month or two to get the third jab? And to what degree does the fact that 6 months lapsed between my initial J&J dose and my first Moderna dose mean? (Because that was the guidance at the time. I got my second dose as soon as I read that existing evidence (again, at that time) indicated that the J&J vaccine MIGHT only be good for 4 months.
And I am not immunocompromised (as far as I know).
It's all so confusing.
To my knowledge, the CDC hasn't advised those who are not immunocompromised to get an additional booster shot yet. I've seen the same echoed by other public health professionals, that if you're not immunocompromised and also not working in healthcare, then you're fine with the original course plus the booster. But that's a good question to ask the pharmacist, maybe they are moving in a new direction soon and they have different advice.
Personally, the uncertainty you have about when to get a shot and if it's needed, is part of why I got an antibodies test last fall. I wanted some idea of where I was and thought it might be a good measuring stick if I'm not exactly sure about when in the future. But also, I believe I'm higher risk than you are, so I'm a bit paranoid about trying to stay ahead of the curve knowing I don't have the best outcome if I get it. But I think it's really hard to know now matter what series of shots you got, though I understand that J&J is talked about by far the least.
Also, meant to say this in my last post. I hope Dolphins is doing okay and please tell him I said hi.
by dryrunguy Thanks, Jazz. Dolphins is fine. They'll do the same nerve kill tomorrow--but on his right shoulder.
by dryrunguy So, I did talk to the woman who oversees vaccinations at the pharmacy where I got my jabs. She admitted the guidance is constantly changing based on emerging evidence. But at this point in time, I am actually NOT eligible for a booster (she referred to it as the fourth dose, even though I've only had two doses so far... they are still counting the initial J&J vaccine as two doses), and there is currently no timeline for when "normal" people like me should seek the fourth those. Currently, fourth doses are only available to people who are immunocompromised.
It was nice to at least get some clarity.... Clarity that will probably change again next week.
by dryrunguy Meanwhile, here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 426.6 million cumulative cases and 5.9 million deaths worldwide as of February 23. The global weekly incidence continues to decline, down 21.1% from the previous week. Notably, all WHO regions with the exception of the Western Pacific region (+28.8%) reported decreasing weekly incidence last week. Global weekly mortality fell 10.85% from the previous week. We expect the cumulative number of deaths to pass 6 million within the next 2 weeks.
Global Vaccination
The WHO reported 10.4 billion cumulative doses administered globally as of February 21. A total of 4.87 billion individuals have received at least 1 dose, and 4.29 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to increase, closely following the trend in Asia. The trend is up from the most recent low of 18.34 million doses per day on February 7 to 24.8 million per day on February 22.* The global weekly average jumped to 33.4 million doses per day on February 23, corresponding to a large increase reported in Asia and may be a reporting error.** Our World in Data estimates that there are 4.93 billion vaccinated individuals worldwide (1+ dose; 62.6% of the global population) and 4.36 billion who are fully vaccinated (55.4% of the global population). A total of 1.27 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
**The OWID data show 17.65 million doses reported in Asia on February 22 and 26.75 million on February 23 (+9.1 million), but it is not immediately clear what country or countries accounted for that increase.
UNITED STATES
The US CDC is currently reporting 78.52 million cumulative cases of COVID-19 and 936,162 deaths. Daily incidence continues its sharp decline, down from a record high of 807,285 new cases per day on January 15 to 79,539 on February 22, a 90% decrease. Daily mortality appears to have peaked on February 2 at 2,597 deaths per day, down to 1,602 on February 22.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 687.7 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to decline, down from the most recent peak of 1.78 million doses per day on December 7 to 337,874 on February 18.* A total of 253.2 million individuals have received at least 1 vaccine dose, which corresponds to 76.3% of the entire US population. Among adults, 87.8% have received at least 1 dose, as well as 26.5 million children under the age of 18. A total of 215.1 million individuals are fully vaccinated**, which corresponds to 64.8% of the total population. Approximately 74.9% of adults are fully vaccinated, as well as 21.8 million children under the age of 18. Since August 2021, 93.4 million individuals have received an additional or booster dose. This corresponds to 43.4% of fully vaccinated individuals, including 66% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
RUSSIAN INVASION OF UKRAINE Russia began a military invasion of neighboring Ukraine this morning, destroying more than 70 military targets through land, sea, and air assaults. The invasion represents the largest attack by one state against another in Europe since World War II. Although the COVID-19 pandemic has played no role in the Russian invasion of Ukraine, the incursion likely will impact virus transmission, testing, surveillance, and treatment for the foreseeable future. The current surge of COVID-19 cases due to the Omicron variant appears to have peaked in both Ukraine and Russia, but the numbers of new cases in both countries remain at record-high levels, and Ukrainian authorities have warned that, despite a 99% vaccination rate among its army, transmission is occurring on the Russian battlefront. The fighting is forcing people to travel west, crowding trains and roads in an effort to reach smaller towns and villages on the European Union border or cross the border into neighboring countries. Poland, Hungary, Slovakia, and Romania are preparing for an influx of refugees. Amid the pandemic, the Ukraine crisis indicates that balance-of-power politics have returned, confirms that pandemics can threaten military power, and reminds us that war has innumerable impacts on human health.
VACCINATION INTERVALS To increase the safety profile of mRNA vaccines, the US CDC is now recommending that certain groups wait longer between their first and second doses. The standard timeline between doses for the Pfizer-BioNTech and Moderna vaccines is 3 and 4 weeks, respectively. Some groups, including men between the ages of 12-39 years old, are now recommended to wait 8 weeks between doses in order to further decrease the risk of myocarditis. Men in this age group appeared to be at a higher relative risk of developing myocarditis following vaccination with an mRNA vaccine, which has prompted further research on ways to mitigate this outcome. Myocarditis associated with vaccination has a low relative risk, around 3.24, compared to the relative risk of COVID-associated myocarditis, around 18.28. Still, new evidence indicates that an 8-week interval between doses can further decrease the risk, which prompted CDC’s change in advice. People not in this group, such as the elderly and immunocompromised, are still recommended to receive their doses on the original 3- and 4-week schedules to prevent severe illness from COVID-19 should they be infected. However, more studies are continuing to evaluate whether a slightly longer period between doses, such as 6 weeks, might result in greater protection for all vaccine-eligible groups.
SANOFI-GSK VACCINE Sanofi and GSK are planning to request US FDA and European Medical Agency (EMA) authorization for their SARS-CoV-2 vaccine candidate—as a primary series and booster dose—following promising results in phase 3 clinical trials. The Sanofi-GSK candidate is an adjuvanted recombinant protein-based vaccine, which is a more traditional vaccine platform compared to the relatively new mRNA vaccines. These vaccines tend to have a good safety profile and have less complicated storage requirements, but mediocre results from a previous iteration kept Sanofi and GSK from applying for authorization last year. This modified candidate has now shown strong efficacy and safety in trials, with 100% efficacy against severe COVID-19 disease and hospitalization. While efficacy against symptomatic infection was around 58%, the vaccine creators assert that these numbers are in line with expected efficacy in the current variant-dominant environment and point to its strong performance against severe and moderate disease outcomes. Novavax, another manufacturer with a protein-based vaccine candidate, is awaiting US FDA review of its request for authorization. Canada and Singapore recently cleared the Novavax vaccine, known as Nuvaxovid, for use among adults.
TESTING & SURVEILLANCE A WHO official recently expressed concern that reduced SARS-CoV-2 testing and surveillance could be contributing to a decline in global COVID-19 cases, saying the falling number of cases and deaths “may not be real.” WHO COVID Technical Lead Dr. Maria Van Kerkhove urged countries to continue their surveillance systems, especially as the number of cases caused by the more transmissible Omicron variant of concern (VOC) BA.2 sublineage begins to climb worldwide. In addition to tracking cases among humans, some experts are encouraging more attention be paid to the hundreds of animal species that are potentially able to be infected with SARS-CoV-2. Cats, dogs, mice, tigers, red fox, deer, and other mammals can be infected by the virus, which could establish itself, mutate, and spread to other species, including back into the human population. Scientists worldwide are collecting genomic surveillance data on various animals, and the World Organisation for Animal Health (OIE) publishes monthly situation reports on SARS-CoV-2 animal investigations. A preprint study posted to medRxiv shows the detection of both the Alpha and Delta variants in Pennsylvania (US) white-tailed deer, the first time those variants have been found in deer. The data for the study, which is not yet peer-reviewed, was collected prior to the emergence of the Omicron variant. Additional long-term funding is needed for research to better understand how animal health is linked to human health, and vice versa.
POST-VACCINATION MIS-C The risk of developing multisystem inflammatory syndrome in children (MIS-C) is very low among young people who were vaccinated against COVID-19, according to a study published in The Lancet Child & Adolescent Health. Using surveillance data from the nationwide Vaccine Adverse Event Reporting System (VAERS), researchers identified 21 young individuals who experienced MIS-C following vaccination between December 14, 2020, and August 31, 2021. All 21 individuals were hospitalized but all were discharged home. As of August 31, 2021, 21.3 million individuals aged 12 to 20 years had received 1 or more doses of SARS-CoV-2 vaccine, making the overall reporting rate of MIS-C following vaccination 1 case per million. Among those individuals who had no evidence of previous or current SARS-CoV-2 infection, the reporting rate was 0.3 cases per million vaccinated individuals.
The rare condition—which can cause dangerous inflammation in major organs as well as vomiting, diarrhea, and low blood pressure—can also follow SARS-CoV-2 infection, showing up sometimes weeks after acute infection. The US CDC updates its data on MIS-C cases monthly. As of January 31, there have been 6,851 cases with 59 associated deaths reported by state and local jurisdictional health departments. Those cases represent a very small portion of the more than 12.5 million COVID-19 cases that have been reported in children since the beginning of the pandemic. Some experts worried that the number of MIS-C cases would spike during the recent wave of cases caused by the Omicron variant, but fortunately that concern has not yet become reality. The CDC and others are working to learn more about why and how MIS-C occurs, and several studies investigating the long-term consequences of MIS-C, its presentation in children, and pathways for treatment and recovery are underway.
FRACTIONAL VACCINE DOSES Administering fractional, or reduced, SARS-CoV-2 vaccines doses could increase global supply, produce fewer side effects, and hasten vaccination uptake. While additional data must be collected, evidence suggests that half or quarter doses of some SARS-CoV-2 vaccines—used as part of a primary series or as booster shots—could be nearly as or even more efficacious than currently used doses of the same or similar vaccines. The Coalition for Epidemic Preparedness Innovations (CEPI) and Australia’s Murdoch Children’s Research Institute (MCRI) announced the launch of a global clinical trial to investigate the efficacy and acceptability of fractional booster doses. Up to 3,300 healthy adults who have received a primary vaccination series with either Pfizer-BioNTech, Oxford-AstraZeneca, Sinovac, or Sinopharm vaccines will receive either a full or fractional booster dose of either the Pfizer-BioNTech, Moderna, or Oxford-AstraZeneca vaccine. The trial, supported with up to US$8.7 million from CEPI, is part of the organization’s Call for Proposals to evaluate the impact of reduced SARS-CoV-2 vaccines in an effort to stretch global supplies and improve vaccine equity.
VACCINE SUPPLY & DEMAND Only about 12% of people in low-income countries are fully or partially vaccinated against COVID-19, but for the first time since the beginning of the pandemic, global vaccine supply is outpacing demand. The COVAX initiative is working to place more than 300 million vaccine doses in countries that need them, but those nations now face other challenges such as gaps in cold-chain storage, lack of funding for distribution networks and administration supplies such as syringes, and stalled vaccination uptake. Additionally, the Africa Centres for Disease Control (Africa CDC) plans to ask all vaccine donations be paused until later this year so countries can avoid wasting the shots if they expire and focus instead on bolstering vaccination logistics and last-mile strategies.
In countries with sufficient supplies, efforts are being made to get more people vaccinated. In South Africa, the government is shortening the required intervals between the first and second doses of a primary series and between the second dose and a booster shot, as well as offering heterologous booster dosing. In Uganda, which has a history of passing controversial public health-related laws, the parliament is considering adopting a vaccination mandate that would result in harsh penalties for people who refuse to comply, including steep fines of about US$1,137 or imprisonment for 6 months. Rights groups criticize the proposal and have called for officials to institute a more organized and inclusive vaccine rollout. Although governments hold much of the power to make vaccines accessible and acceptable, it will take coordinated efforts involving multiple stakeholders to improve vaccine uptake in many low- and middle-income countries.
US TRUCK CONVOYS After police in Ottawa, Canada, earlier this week cleared demonstrators who occupied the capital city for more than 3 weeks in protest against SARS-CoV-2 vaccine mandates and other pandemic restrictions, spin-offs of the so-called “Freedom Convoy” are taking shape across the US. Convoys of trucks are threatening to inundate the Washington, DC, metropolitan area as soon as this week, arriving from as near as Pennsylvania and as far as California, as well as hold a rally near the Washington Monument on March 1, the day US President Joe Biden is scheduled to deliver the annual State of the Union address. In anticipation of the protests, the US Department of Defense approved the deployment of 700 unarmed National Guard troops, at the request of the DC government and the US Capitol Police, to assist with traffic and mitigate possible disruptions. The California convoy—dubbed the “People’s Convoy”—departed Adelanto, California, on February 23 amid much fanfare and is expected to arrive in the DC area on March 5. The convoy is demanding an end to the national emergency first declared by former US President Donald Trump and recently extended by President Biden; a congressional investigation into the origin of SARS-CoV-2; and an end to government-issued public health measures including mask mandates and vaccination requirements. Unlike the Canadian truck convoy demonstrators, American truckers have no vaccination requirement to cross the US-Canada border, and most states have eased masking and vaccination requirements as the number of new COVID-19 cases fall.
The Freedom Convoy protests also have inspired similar demonstrations against pandemic mitigation measures in other countries. Authorities in Austria, Belgium, and France earlier this month banned motor protests in their capital cities. In New Zealand, people protesting the nation’s vaccination mandate have occupied Parliament grounds for at least 17 days, with what began as a peaceful demonstration turning violent this week. Today, protestors chased Prime Minister Jacinda Ardern’s vehicle down a driveway as she visited a Christchurch primary school. Earlier this week, Prime Minister Ardern expressed concern for police safety after several officers were hospitalized after protestors threw an unidentified liquid in their faces. She has resisted calls to use emergency powers or defense forces to dispel protesters. The convoys and occupations represent a show of frustration at the years-long pandemic and associated efforts to control transmission of the virus and expose ideological rifts that can be exacerbated by misinformation, disinformation, and conspiracy theories.
dryrunguy wrote: ↑Thu Feb 24, 2022 6:22 pm
So, I did talk to the woman who oversees vaccinations at the pharmacy where I got my jabs. She admitted the guidance is constantly changing based on emerging evidence. But at this point in time, I am actually NOT eligible for a booster (she referred to it as the fourth dose, even though I've only had two doses so far... they are still counting the initial J&J vaccine as two doses), and there is currently no timeline for when "normal" people like me should seek the fourth those. Currently, fourth doses are only available to people who are immunocompromised.
Yeah, so if people on here don't personally know anyone who is immunocompromised and understand why they have different guidance than others, this will helpfully give you some idea.
My mom is immunocompromised. She's on a medication that suppresses her immune system and it is vital that she stays on the medication for her to remain in good health.
My mom and I both got vaccinated with Pfizer and it was only days apart. In the fall when I got my antibodies test, right before she went to get her booster shot, she decided why not also get an antibody test as well. Glad we did that. It was 6 months after our initial series. It's not a definitive showing of your antibody levels, only measures the one thing, but still, it was good to know something. My antibody levels were almost 3x that of hers. And I do not have a great immune system, I can get sick at the drop of a dime and have a chronic illness that has affected it as well. So for those to be the differences, are the reason for the different guidelines.
Their antibody levels dip much quicker than others and they are much more prone to a negative outcome. There are a ton of stories about what levels come back for the immunocompromised, some have trouble showing almost any antibodies shortly after getting the vaccine, others do okay to start, but drop off much quicker than the norm. My mom, though more vulnerable than the norm, is one of the lucky ones, in that she kept at least some antibodies 6 months after the fact. It's part of why there's hope for one of the pills in late development, it's shown to to boost antibody levels in the immunocompromised that have struggled to keep their levels up thru the vaccine.
by JazzNU
by JazzNU ^^ This is of course on top of a host of cities and states that have previously announced expiring or expired mask mandates as Omicron wanes.
by ti-amie
Let's talk to Denmark about this...
Also, keeping my mask on.
by dryrunguy Here's the latest Situation Report.
::
US CDC MASK GUIDANCE The US CDC issued new guidance on February 25 on when US residents should consider wearing masks to lower the risk of SARS-CoV-2 transmission. The strategy moves beyond using the number of new COVID-19 cases and percentage of positive test results over the previous week as benchmarks and instead considers 3 different metrics—new COVID-19 admissions per 100,000 population in the past 7 days, the percent of staffed inpatient beds occupied by COVID-19 patients*, and total new COVID-19 cases per 100,000 population in the past 7 days—to determine US counties’ COVID-19 community level. Using that data, community level is classified as low (green), medium (yellow), or high (orange), and the CDC released an interactive map allowing people to search visually or by county name to determine counties’ COVID-19 community level. The agency advises universal indoor masking, including in schools, only in counties with a “high” COVID-19 community level. In medium-risk communities, the agency recommends those who are at an increased risk of severe disease ask their doctor about wearing a mask. Others in medium- and low-risk communities may choose whether or not to wear a mask, regardless of vaccination status. However, the agency continues to recommend vaccination and boosters for all eligible people, and anyone with symptoms, a positive SARS-CoV-2 test, or exposure to someone with COVID-19 should wear a mask in public. The new strategy does not apply to travelers on airplanes, trains, and buses and at airports and train stations. The CDC plans to soon revisit those requirements, which are set to expire on March 18.
Many public health experts agreed the changes make sense, with some saying masks should become a normalized courtesy, where people wear them out of respect if they have symptoms. Others, including individuals made vulnerable to severe COVID-19 because of compromised immune systems or other conditions, feel left behind under the new guidance. The administration of US President Joe Biden announced last week it is taking steps to make masks and tests more accessible to people with certain disabilities, but some advocates say the efforts have been slow to materialize and viewed as an afterthought. The new CDC mask recommendations, as well as the waning number of new COVID-19 cases nationwide, also led some experts to warn that, while hopeful, these conditions do not signal the end of the pandemic. According to a recent poll from the Kaiser Family Foundation, most adults disagree about what a return to normal means and when it should occur. And while most agree that the worst of the pandemic is over, there remains uncertainty about the future, with 17% of adults saying the worst is yet to come. With mask mandates and other pandemic-related restrictions being dropped across the country, President Biden is expected to address the state of the pandemic in his first State of the Union address this evening but stop short of declaring victory.
*Hospitalizations are counted as all patients with COVID-19, regardless of reason for admission.
VACCINE EFFECTIVENESS Data compiled by the New York State Department of Health indicates that the smaller Pfizer-BioNTech SARS-CoV-2 vaccine is less effective at preventing infection and COVID-19-related hospitalization in children ages 5 to 11 years compared with older children ages 12 to 17. The findings, which are not yet peer-reviewed, showed quicker declines in vaccine effectiveness (VE) in the younger cohort. VE against cases declined from 66% to 12% in the 5- to 11-year-old cohort, while VE in the 12- to 17-year-old group declined from 66% to 51% between December 13, 2021, and January 30, 2022. A similar trend was shown in VE against hospitalizations over the study period: 100% down to 48% among the youngest cohort and 85% to 73% in the young adolescent group. The authors note that dosing could be a factor in the VE decline, as children ages 5 to 11 receive smaller doses of vaccine. The adult dose, also given to those aged 12 to 17 years, is a 2-dose regimen of 30 µg, while those aged 5 to 11 receive 2 10μg doses in the trial. In clinical trials, children ages 6 months to <5 years are receiving even lower doses of the Pfizer-BioNTech vaccine, 2 or 3 shots of 3μg. The US FDA and the companies recently delayed review of an application for authorization among this group to await trial results of a 3-dose regimen, expected in April, after 2 doses did not produce antibody levels in 2- to 4-year-olds on par with people aged 16 to 25. The Pfizer-BioNTech vaccine is currently the only one authorized in the US for use among children ages 5 to 11.
Results of a test-negative case-control study evaluating Moderna’s vaccine effectiveness against the Delta and Omicron variants found the vaccine to be more effective against infection with the Delta variant but highly protective against hospitalizations for both variants. Three-dose (2-dose primary series plus a booster dose) VE against hospitalization with Delta and Omicron was >99% across the entire study population. Evaluated at 14-60 days and >60 days, 3-dose VE against infection showed high, durable immunity against Delta, with VE declining slightly from 93.7% to 86.0%, but lower effectiveness against Omicron, with VE falling from 71.6% to 47.4%. In immunocompromised individuals, the 3-dose VE was 29.4% against Omicron.
The study aligns with US CDC findings that vaccine protection against Omicron was weaker compared to other variants, but vaccination continued to provide protection against hospitalization during the Omicron surge. The likelihood of unvaccinated people being hospitalized was 15 times greater than that of fully vaccinated people during earlier variants and fell to about 7 times the risk with the Omicron variant. Despite waning effectiveness, vaccines continue to protect against death amid the Omicron surge. At the end of December 2021, unvaccinated people were 10 times more likely to die of COVID-19 than fully vaccinated individuals.
ASIA The number of new COVID-19 cases continues to drop globally except in Asia, where the number of confirmed cases increased nearly 32% the week ending February 21. In Hong Kong, an Omicron variant-fueled surge has overwhelmed the city’s “dynamic zero” strategy—the same as mainland China’s—raising panic and fear among residents who emptied grocery store shelves over the weekend. The COVID-19 fatality rate in Hong Kong is now the highest in the developed world, leaving the healthcare system overloaded with patients and mortuaries at capacity. Older residents, who are most at risk, remain the least vaccinated. Leaders have implemented vaccine passports, mask mandates, and mandatory mass SARS-CoV-2 testing—3 tests for each resident over a 9-day period—and many are concerned lockdowns could soon follow. Some expatriate residents are leaving the city in order to avoid testing and potential lockdowns and keep their children in school, after the city announced school closures this month.
The number of new COVID-19 cases and related deaths also are soaring in South Korea, with the nation setting a single-day mortality record on February 28 with 114 deaths. Notably, the nation dropped its “anti-epidemic pass” mandate today, which required people to show proof of vaccination or negative test to enter any indoor area, in order to allow more healthcare workers to move freely to care for the nearly 800,000 patients with mild-to-moderate COVID-19 who are isolating at home to preserve hospital beds. Some say the new strategy to monitor patients at home felt like “home abandonment,” with government-sponsored shipments of medical supplies—such as thermometers, pulse oximeters, and other supplies—failing to arrive on time.
Across the border in North Korea, the government continues to claim it has recorded no COVID-19 cases since the beginning of the pandemic. Last week, an independent UN human rights investigator called on the international community to provide North Korea with at least 60 million doses of SARS-CoV-2 vaccines in order to ward off a humanitarian crisis and persuade the country to ease lockdowns that have left much of its population at risk of starvation. Notably, the COVAX initiative recently scaled back the number of vaccine doses allocated to the country since the government has failed to arrange for any deliveries and previously rejected planned shipments.
CARIBBEAN While the number of new COVID-19 cases are declining across the Americas, the Caribbean is falling behind, the Pan American Health Organization (PAHO) warned last week. In the region, 10 out of the 13 countries and territories that have yet to reach the WHO goal of vaccinating 40% of their populations are in the Caribbean. Experts caution against interpreting declines in case numbers as evidence that the virus is disappearing, as some locations continue to experience outbreaks. Although barriers to vaccination persist in the Caribbean—including vaccine hesitancy, lack of rural vaccination centers, insufficient staff, and limited cold-chain infrastructure—PAHO called on governments and healthcare workers to use available tools to “to turn the tide on vaccinations” by providing communities with more information, education, and accessible vaccination opportunities.
CHILDREN WHO LOST CAREGIVERS Globally, more than 5.2 million children lost a parent or caregiver during the first 19 months of the COVID-19 pandemic, according to a study published in The Lancet Child & Adolescent Health. A collective of international researchers and experts from various health organizations and universities collected data from more than 20 countries. The research estimates the number of children experiencing COVID-19-associated orphanhood or caregiver death increased 90% from April 30 to October 31, 2021, from 2,737,300 to 5,200,300. Paternal orphans represented 76.5% of the orphaned children, compared to 23.5% who lost their mother. Beyond the tragic numbers, the study warns that children who lose a parent are at greater risk of poverty, sexual abuse, mental challenges, and severe stress.
PLANT-BASED VACCINE After authorizing Novavax’s protein-based SARS-CoV-2 vaccine Nuvaxovid for adults aged 18 and older on February 17, Canada’s drug regulator last week cleared a second non-mRNA vaccine against COVID-19, authorizing Medicago’s Covifenz vaccine for adults ages 18 to 64. The 2-dose vaccine uses plant-based, non-infectious virus-like particles (VLP) of spike protein from the original SARS-CoV-2 strain, as well as an adjuvant from GlaxoSmithKline to boost immune response. Quebec-based Medicago has agreed to supply up to 76 million vaccine doses to the Canadian government, the first shipments of which are expected in May. In a study of 24,000 adults, the overall vaccine efficacy rate was 71% against all SARS-CoV-2 variants, although the clinical trial was performed prior to the emergence of the Omicron variant of concern. The authorization represents the first of a vaccine manufactured using plant-based technologies, and public health officials are hopeful Covifenz and Nuvaxovid will provide options to people who are not willing to receive an mRNA-based vaccine. However, since 81% of the total Canadian population is fully vaccinated, many of the vaccine doses likely will be shipped overseas. Health Canada has authorized the use of 6 SARS-CoV-2 vaccines.
SARS-COV-2 ORIGIN In 3 preprint studies posted online last week, scientists provide additional evidence that the COVID-19 pandemic originated in a Wuhan, China, market due to a zoonotic viral spillover event. The studies, posted on February 25 and 26, have not yet been peer-reviewed or published in a professional journal. The first study presents analyses of 1,380 samples collected in early 2020 from the Huanan Seafood Market (HSM), the surrounding environment, and animals within the market. Researchers detected SARS-CoV-2 in the stalls of the HSM western zone and other environmental samples, but they did not detect the virus in samples taken from 18 animal species present at the market, including some stray animals. A second study uses geospatial analyses to show that the earliest COVID-19 cases diagnosed in December 2019 were located close to and centered on the market and that environmental samples positive for SARS-CoV-2 were strongly associated with vendors selling live animals. A third study suggests that SARS-CoV-2 arose in humans after at least 2 separate cross-species transmission events in late 2019, possibly from live animals sold at the HSM.
Many scientists agree that the preponderance of evidence, included in these studies and others, supports a zoonotic origin story of SARS-CoV-2 instead of an accidental laboratory leak. However, none of the studies provide definitive evidence about what animal species might have hosted the virus prior to it jumping to humans. Nor do the studies rule out that the HSM could have simply served as the location of a large amplifying event in which an infected person transmitted the virus to many others. Researchers around the world continue to analyze available evidence, but without additional samples from early human cases and animals, the world may never know the true origin of the novel coronavirus that has so far killed at least 6 million people worldwide in just over 2 years.
by dryrunguy Here's the latest Situation Report. You can imagine what the section on Ukraine is about. The section on increases in maternal mortality in the first year of the pandemic in the U.S., particularly among Black women, is quite sad as well.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 437.3 million cumulative cases and 5.96 million deaths worldwide as of March 2. The global weekly incidence continues to decline, down 15.5% from the previous week. Notably, the Western Pacific region continues to report increasing weekly incidence (+31.7%), while all other regions reported decreasing weekly incidence last week. Global weekly mortality fell 14.4% from the previous week. We expect the cumulative number of deaths to pass 6 million this week.
Global Vaccination
The WHO reported 10.58 billion cumulative doses administered globally as of February 27. A total of 4.9 billion individuals have received at least 1 dose, and 4.32 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations appears to have stabilized over the past 2 weeks. As of March 2, 23.5 million doses per day were recorded, a relatively small decline compared to the 25.5 million doses per day on February 17.* The trend continues to closely follow that of Asia. Our World in Data estimates that there are 4.97 billion vaccinated individuals worldwide (1+ dose; 63.13% of the global population) and 4.39 billion who are fully vaccinated (55.7% of the global population). A total of 1.41 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 78.9 million cumulative cases of COVID-19 and 950,112 deaths. Daily incidence continues its sharp decline, down from a record high of 807,843 new cases per day on January 15 to 56,253 on March 1. Daily mortality appears to have peaked on February 2 at 2,627 deaths per day, down to 1,674 on March 1.*
According to CDC COVID-19 Seroprevalence Estimates released this week, more than 140 million US residents have been infected with SARS-CoV-2, about 43% of the total population. The data are based on 72,000 blood samples taken through the end of January 2022 and only include people who have antibodies from natural symptomatic or asymptomatic infection, not vaccination.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 691 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to decline, down from the most recent peak of 1.79 million doses per day on December 7 to 284,281 on February 25.* The number of daily vaccinations is at its lowest level since late December 2020, right after the vaccines were authorized. A total of 253.7 million individuals have received at least 1 vaccine dose, which corresponds to 76.4% of the entire US population. Among adults, 87.9% have received at least 1 dose, as well as 26.7 million children under the age of 18. A total of 215.8 million individuals are fully vaccinated**, which corresponds to 65% of the total population. Approximately 75% of adults are fully vaccinated, as well as 22.1 million children under the age of 18. Since August 2021, 93.6 million individuals have received an additional or booster dose. This corresponds to 43.8% of fully vaccinated individuals, including 66.3% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent 5 days. The most current average provided here corresponds to 5 days ago.
**Full original course of the vaccine, not including additional or booster doses.
US NATIONAL COVID-19 PREPAREDNESS PLAN Moving the US from a state of pandemic crisis to a time when COVID-19 does not disrupt daily life will require focus on 4 primary goals: protecting people from infection and treating COVID-19; preparing for the emergence of new variants; keeping businesses and schools open and operating; and leading global vaccination efforts, according to a new roadmap released on March 2 by the administration of US President Joe Biden. To achieve its objectives, the 96-page National Covid-19 Preparedness Plan depends on the US Congress approving billions of dollars in new funding. The Biden administration has informally indicated it will request US$30 billion for domestic needs and US$5 billion for global vaccination efforts. Some US lawmakers and advocates have said at least triple that amount will be needed for international efforts. A formal budget request is expected soon.
The plan’s release follows President Biden’s first State of the Union address delivered the night before, during which he touched on several aspects of the plan. President Biden emphasized that “COVID need not control our lives,” touting new US CDC guidance that allows much of the country’s population to remove masks, but he simultaneously expressed caution that the nation must remain “on guard.” He announced that people soon will be able to order additional rapid antigen tests through the COVIDtests.gov website. Nearly half of the 500 million free SARS-CoV-2 tests remain unclaimed, with 40% of the already-mailed tests having gone to households in low-income areas, according to the White House. President Biden also announced a “Test to Treat” initiative set to launch later this month that will allow people to receive immediate COVID-19 therapy—likely Pfizer’s Paxlovid antiviral—if they test positive at a participating pharmacy. Noting that variants remain a threat, President Biden restated his administration’s commitment to being able to quickly develop and ship variant-specific vaccines as well as accelerating efforts to detect, prevent, and treat long COVID.
White House and US Health and Human Services (HHS) public health officials further expanded on details of the new National COVID-19 Preparedness Plan during a March 2 briefing. They noted a priority to keep businesses and schools open, including efforts to improve ventilation and air filtration as well as calls for Congress to reinstate tax credits for small- and mid-size businesses to provide sick or family leave for people affected by COVID-19. High-quality masks will continue to be made available at participating locations including grocery stores, pharmacies, and community health centers, and the administration plans to launch a new website to help people locate vaccines and masks in their communities. COVID-19-specific testing, treatment, and prevention tools such as masks, including those for children, will be added for the first time to the nation’s Strategic National Stockpile, and federal plans to develop a pan-SARS-CoV-2 vaccine—and later a universal coronavirus vaccine—are moving forward. Additionally, the roadmap includes strategies for rolling out a vaccine for children under age 5 when and if one is authorized and recommended by health authorities.
Notably, some public health experts criticized the plan and the US CDC’s recent shift in masking guidance, saying a move toward a medical framework focused primarily on testing and treatment places too much onus on individual responsibility versus community-level intervention. This shift adds burdens on vulnerable individuals and populations, including the immunocompromised, rural and low-income communities, those who live or work in high-exposure environments, and young children who remain ineligible for vaccination.
UKRAINE Ukraine already has experienced immediate downstream impacts of the Russian invasion. One of these far-reaching impacts is the damage that the invasion has played on Ukraine’s ability to control the COVID-19 pandemic. Dr. Bruce Aylward, a senior advisor at the WHO, said in a statement earlier this week that “infectious diseases ruthlessly exploit the conditions created by war,” while WHO Director-General Dr. Tedros Adhanom Ghebreyesus called for increased humanitarian channels to provide lifesaving medical supplies to those remaining in the country. Notably, the WHO avoided naming Russia as an aggressor during their press conference, instead focusing on calls to stop attacks on civilians and medical institutions. Healthcare systems already face supply chain challenges. The WHO warned on February 27 the country has dangerously low supplies of medical oxygen, a key tool in treating people hospitalized with COVID-19 and other diseases. The agency announced its first shipment of medical aid for Ukraine will arrive in Poland today, but details about last-mile delivery to Ukrainians in need remain unclear.
Experts warn that the conflict also threatens to disrupt efforts to control the pandemic, as well as other vaccine-preventable diseases, in neighboring countries. At least 1 million refugees already have fled across the borders since the start of the invasion. Prior to the conflict in the country, COVAX had delivered more than 8 million vaccine doses to Ukraine, but this disruption may offset hard fought gains in vaccination. Prior to last week’s events, only 35% of Ukraine’s population was fully vaccinated, creating an atmosphere for increased SARS-CoV-2 transmission and the potential for a greater number of severe health outcomes. The country’s low vaccination coverage is not sufficient to prevent the virus from spreading among large populations living in crowded shelter situations and increases the potential for new variants to emerge. COVAX indicated it will continue to support Ukraine’s vaccination efforts and has a “Humanitarian Buffer” mechanism for delivering vaccines in humanitarian crises, but the coordination and cooperation needed to establish such services will take time.
US MATERNAL MORTALITY Pregnant people or those recently pregnant are at an increased risk for severe illness from COVID-19 when compared to people who are not pregnant. As of February 19, about 68% of pregnant people were vaccinated before or during pregnancy, a sharp increase from the beginning of the summer when the proportion was around 40%. Some pregnant people say they feel they were left behind in rushed efforts to vaccinate the population, having been excluded from vaccine clinical trials for safety reasons and receiving mixed guidance when vaccines first became available. While the full scope of impacts from maternal SARS-CoV-2 infection remain unclear, some evidence suggest even mild or moderate infection can increase the risk of premature birth or stillbirth.
Additionally, a new report from the US CDC National Center for Health Statistics shows that the number of women in the US who died during pregnancy or shortly after giving birth rose sharply during the first year of the pandemic. The data show that 861 women died of maternal causes in the US during 2020, an increase of 14% over the prior year. The maternal mortality rate increased to 23.8 deaths per 100,000 live births, up from 20.1 per 100,000 in 2019. Notably, the rate for non-Hispanic Black women was 2.9 times higher than the rate for non-Hispanic white women, a gap that increased between 2019 and 2020. Although the report does not provide details on potential causes for the increases, experts said some of the deaths likely were directly or indirectly related to the COVID-19 pandemic. As in other aspects of healthcare, the pandemic helped to magnify disparities in access to quality maternal care. There has been a push to address this critical issue at the federal level, including language in the American Rescue Plan that gave states the opportunity to extend Medicaid coverage for new mothers from 60 days to up to a year postpartum. The CDC supports multiple efforts to better understand the impact of COVID-19 on pregnant people and infants and encourages those who are pregnant or considering pregnancy to get vaccinated, citing the growing amount of data that show the protective measures that SARS-CoV-2 vaccines offer this vulnerable group.
COVID-19 THERAPIES During the State of the Union address, US President Joe Biden announced his administration is launching a new “Test to Treat” initiative that will provide free antiviral treatment to qualified individuals who test positive for SARS-CoV-2 at pharmacies or community health centers. The US has ordered more authorized COVID-19 treatments than any other country, with Pfizer expected to increase its supply of Paxlovid—which reduced the risk of COVID-related hospitalization by about 90% in clinical trials—to more than 2 million pills in April. But questions remain about the initiative’s details. The program is not set up yet, although CVS, Walgreens, and Walmart have indicated they will participate. Still, people will need to find and access participating locations and obtain a prescription for treatment from either an on-site doctor or their primary care provider, if they have one. Alternatively, pharmacists may be permitted under federal guidance to assess patients and order the oral therapies. Notably, some pharmacies are complaining that the costs of filling the prescriptions are not adequately covered by commercial and government health plans, which could cause some to drop out of supplying the antivirals at all.
Following the December 2021 authorization of the antiviral therapies Paxlovid and Merck’s molnupiravir—which has limited use and is much less effective than Paxlovid—nationwide supplies are increasing, making the treatments more easily accessible. Since December, the federal government has sent more than 500,000 courses of Paxlovid and about 1.85 million courses of molnupiravir to the states. Additionally, more than 100 vaccines, antivirals, and other treatments, such as monoclonal antibodies and repurposed medicines, are currently being tested in late stage clinical trials globally. New SARS-CoV-2 variants continue to be a wildcard for existing therapies and those under investigation. The US has paused or limited the use of certain monoclonal antibodies because the Omicron variant of concern is not susceptible to the drugs.
VACCINE EFFECTIVENESS AMONG CHILDREN According to new data published this week in the US CDC’s Morbidity and Mortality Weekly Report (MMWR), 2 doses of the Pfizer-BioNTech SARS-CoV-2 vaccine provided strong initial protection against urgent care and emergency department visits and hospitalization for children aged 5 to 17 years (overall vaccine effectiveness [VE] against hospitalization was 73%-94%). As seen in other age groups, VE weakened over time and was lower during Omicron predominance. However, the data show that a booster dose was able to restore vaccine effectiveness to 81% among individuals aged 16-17 years. The new MMWR findings supplement earlier data from New York state, discussed in our March 1 briefing. The New York data, which is not yet peer-reviewed, asserted that the Pfizer-BioNTech vaccine’s protection against infection and hospitalization for children aged 5 to 11 years waned quickly compared to children aged 12 to 17. Scientists from the CDC and other institutions warn that the New York study might be too small to draw solid conclusions and might not take into account children who were tested at home instead of a clinic. They assert that some drop in protection was the result of the Omicron variant, which affected all age groups. The CDC currently recommends that all eligible children and adolescents remain up-to-date on their vaccinations, including receipt of a booster dose for individuals aged 12 and older. A separate MMWR study examined the safety of booster doses for children aged 12 to 17 years, showing that local and systemic reactions are expected but that serious adverse events are rare.
US MILITARY VACCINE MANDATE The 5th US Circuit Court of Appeals this week upheld a lower court’s injunction barring the US Navy from considering the vaccination status of 35 special forces personnel in making deployment decisions. The US Department of Defense requires all service members to receive SARS-CoV-2 vaccination, and although the rule allows for religious exemptions, only 15 of about 16,000 requests have been approved so far. The US Justice Department argued that the courts did not have jurisdiction to rule on military deployment decisions, but the appeals panel in its decision said the judiciary does have the power to consider the plaintiffs’ objections on religious grounds. The case represents another setback for government-imposed broad-reaching vaccination requirements. The 5th Circuit previously ruled against the Occupational Safety and Health Administration’s (OSHA) emergency temporary standard (ETS) that required businesses with 100 or more staff to ensure their employees were either vaccinated or tested weekly and wore masks. OSHA withdrew that rule after the US Supreme Court ruled against the requirement.
Separately, the US Senate on March 2 voted 49-44 to strike down the Centers for Medicare and Medicaid Services' (CMS) vaccine mandate for healthcare workers. The measure, allowed under the Congressional Review Act, passed in the evenly divided Senate due to the absence of 6 Democratic members.
WHITE-TAILED DEER As previously discussed in this report, animal reservoirs of SARS-CoV-2 present a risk of viral mutation and spillback into humans. The virus is known to infect several non-human mammalian species, including mink, hamsters, mice, and white-tailed deer. Researchers examining coronavirus in Canadian white-tailed deer populations have identified a new, highly divergent lineage of SARS-CoV-2 in deer. Additionally, they report the identification of a very similar viral sequence in a single person in the same geographical region who had close contact with deer. No other human-derived genetic sequences were similar, leading the researchers to speculate it likely was an isolated case with no evidence of recurrent deer-to-human or sustained human-to-human transmission. The preprint report, posted in bioRxiv and not yet peer-reviewed, is the first evidence of possible deer-to-human transmission of SARS-CoV-2. The researchers noted that SARS-CoV-2 circulating among wild deer populations posed more of a containment challenge than farmed or domestic animals and stressed the need for a broader, interdisciplinary One Health approach to SARS-CoV-2 surveillance.
by ponchi101 Now the question will be: do you suffer these symptoms to the same degree if you are vaccinated? Since we know that vaccination does not stop you from getting infected, is the vaccinated/controlled infection as serious a non-vaccinated infection?
And, of course:
The people that are not vaccinated will have their brains shrink even more. Where does the joke end?
by Suliso In the grand scheme of things covid seems so unimportant now...
by ti-amie I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
by Suliso
ti-amie wrote: ↑Wed Mar 09, 2022 8:26 pm
I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
Interesting... Hardly anyone is masked here (maybe 10%) except in public transport where it's still mandatory till the end of the month.
by dryrunguy Here's yesterday's Situation Report. Sorry for the delay. I haven't read it yet. (In proposal start-up hell.)
::
6 MILLION DEATHS The official global death toll from COVID-19 likely will pass 6 million today. The actual total of COVID-related deaths could be 2 to 4 times higher than the official number, based on estimates of global excess deaths. As the pandemic enters its third year, the milestone is a reminder that the crisis is not over in many countries—with the highly transmissible Omicron variant continuing to drive a surge in cases, especially in the Western Pacific region—even as other nations move to drop public health restrictions and requirements. COVID-19 has breached the strict border controls of several Pacific island nations, which until recently held off the virus. New Zealand recorded a new record of nearly 24,000 new cases today, causing severe healthcare system strain. In China, the government is quietly moving away from its aggressive “zero COVID” policy to a “dynamic clearing” model aimed at controlling local outbreaks as soon as possible. China’s National Health Commission reported 526 cases from local transmission on March 6, the highest daily total since the initial outbreak in Wuhan. Hong Kong reported more than 43,000 new cases today after the launch of a new system that allows residents to self-report at-home test results. Over the weekend, city residents cleared supermarket shelves for a seventh consecutive day, despite authorities’ calls for calm. In Ecuador’s largest city, Guayaquil, which faced one of the world’s worst COVID-19 outbreaks, violence has replaced contagion as the population struggles to recover from the pandemic’s social, economic, and mental health impacts. Highly vaccinated—and mostly wealthy—countries appear to be moving on from the pandemic, and many global health organizations are shifting their priorities away from COVID-19 to focus on preparing for the next pandemic. Still, only about 14% of people in low-income countries have received at least 1 dose of vaccine. These countries remain vulnerable to the unpredictability of the pandemic and risk being left to languish without needed vaccine doses, treatments, and testing tools.
US COVID-19 FUNDING On March 7, members of US President Joe Biden’s administration warned that the federal government is nearly out of funding for its COVID-19 pandemic response and urged the US Congress to quickly replenish the funds. Last week, the Biden administration formally requested US$22.5 billion in emergency spending as part of its new COVID-19 Preparedness Plan. The “urgent” request is lower than the US$30 billion originally floated and is coupled with a request for US$10 billion for humanitarian and military aid for Ukraine. The emergency funding request includes money for research into a pan-SARS-CoV-2 vaccine, testing capacity, purchase of additional antiviral treatment courses, and support for the purchase of vaccines to be distributed globally. The US continues to be a large contributor to global vaccination efforts, representing 36% of the money donated to COVAX and 41% of pledged vaccine doses, according to analysis from the Kaiser Family Foundation. In a letter sent last week, Shalanda Young, the Acting Director of the Office of Management and Budget, urged lawmakers to “act expeditiously” on the request by March 11, citing a need to increase funding for the US Department of Defense and other agencies, which are operating at levels negotiated in late 2020.
However, it is unclear if Congress will heed the urgency, as debates over the necessity of new COVID-19 funding fall along partisan lines. At least 3 dozen Republican Senators are asking for more transparency from the Biden administration about how more than US$4 trillion in previously authorized funding has been spent before supporting additional funds. Democrats warned opposition to approving emergency pandemic funds could jeopardize the nation’s return to a sense of normalcy. This news comes alongside other signals from some federal lawmakers that they are working to move past the COVID-19 pandemic. The US Senate last week passed a Republican-sponsored bill to end the national emergency declaration for COVID-19. The measure passed narrowly, with a 48-47 vote, drawing the threat of a veto from President Biden.
COVID ROADMAP A report written by nearly 2 dozen experts charts a course for living with COVID-19, outlining recommendations to reach a “new normal.” The report, titled Getting to and Sustaining the Next Normal: A Roadmap for Living with COVID, describes 12 core elements fundamental to the roadmap, principally shifting focus from COVID-19 to major viral respiratory illnesses like influenza and respiratory syncytial virus (RSV); creating a dashboard to serve as an infectious diseases information hub for the introduction, modification, and lifting of public health measures; issuing guidance for therapeutics and additional protective measures; and increasing surveillance, testing, and data infrastructure. The report includes 3 scenarios in which the COVID-19 pandemic will continue, dependent on vaccine- or infection-derived immunity and the characteristics of new variants. Other key recommendations of the report include developing indoor air quality standards to protect from inhalation exposure; conducting additional long COVID research; and supporting the development of new therapeutics to be distributed in an accessible, equitable test-to-treat platform. Strategies to rebuild trust and credibility among public agencies like the US CDC include building in more transparency in how guidance is set and overhauling the Vaccine Adverse Event Reporting System, which relies on self-reported data and has been exploited by anti-vaccine groups to spread misinformation. The group consulted with the White House earlier this year, and some of the recommendations are similar to those included in the National COVID-19 Preparedness Plan, albeit with much more detail. The 136-page report contains more than 250 discrete recommendations that go beyond the current and proposed changes.
COVID MISINFORMATION US Surgeon General Dr. Vivek Murthy last week formally requested that major technology companies send data and analysis on the prevalence of COVID-19 misinformation on their social networks, search engines, instant messaging systems, e-commerce sites, and crowdsourced platforms, as well as information on the primary sources of that misinformation. Additionally, Dr. Murthy requested that healthcare professionals and the public submit information about how COVID-19 misinformation has impacted patients and communities. Companies have until May 2 to comply with the request, which is part of US President Biden’s new National COVID-19 Preparedness Plan. Separately, a group of physicians called No License for Disinformation is calling on state medical boards to take disciplinary action against doctors who deliberately spread misinformation regarding COVID-19 therapies, vaccines, and public health measures including masking.
VACCINES FOR CHILDREN Children under age 5 in the US remain ineligible for vaccination against COVID-19, and a series of ups and downs regarding expected authorization for this age group has left some parents feeling abandoned, frustrated, and fearful as mask mandates and other restrictions are dropped. Additional data on a 3-dose regimen of the Pfizer-BioNTech vaccine in young children is expected this spring, and Moderna is expected to request authorization for its vaccine among young children by May.
Last week, the US FDA rejected an application from pharmaceutical company Ocugen seeking Emergency Use Authorization for an India-made SARS-CoV-2 vaccine for children aged 2 to 18. Covaxin, manufactured by the Indian pharmaceutical company Bharat Biotech, is not yet authorized for any age group in the US nor has the vaccine been tested in the US. A clinical trial conducted in India among individuals between ages 2 and 18, prior to the emergence of the Omicron variant, showed 2 doses of the vaccine were safe and generated robust immune responses. Ocugen contracted with Bharat to try to bring the vaccine to the US market. Covaxin is authorized in about 20 countries and has Emergency Use Listing by the WHO. Ocugen said it will continue working with US regulators to evaluate the vaccine’s use in children.
In Florida (US), the state’s surgeon general on March 7 announced that the state will issue guidance urging parents to not vaccinate their healthy children against COVID-19. Although Florida’s decision likely will have little impact on parents’ abilities to vaccinate their children, the recommendation breaks with US CDC guidance and some experts say the move could sow confusion and distrust, potentially harming individuals and communities.
MODERNA In a new Global Health Policy Strategy published March 7, Moderna announced several new and expanded commitments related to COVID-19 and mRNA technologies. The company said it will expand its global health portfolio to 15 vaccine programs targeting pathogens identified as posing the greatest threat to global health by the Coalition for Epidemic Preparedness Innovations (CEPI); launch a program that will offer the company’s mRNA technology to researchers investigating new vaccines for emerging or neglected infectious diseases; and pledge to “never enforce” patents related to its SARS-CoV-2 vaccine only in the Gavi COVAX Advanced Market Commitment (AMC) for 92 low- and middle-income countries. Previously, the company said it would not enforce its patents during the pandemic but retained the right to do so in the future. As part of the new pledge, Moderna said it will not enforce patents for its SARS-CoV-2 vaccines against South Africa-based Afrigen Biologics—which has used publicly available information to replicate Moderna’s vaccine as part of the WHO-supported mRNA vaccine technology transfer hub—even though the company holds patents in South Africa and the nation is not included in the COVAX AMC.
Additionally, Moderna announced a preliminary agreement with the government of Kenya to establish Africa’s first mRNA manufacturing facility. Moderna plans to invest US$500 million to build the facility, which is expected to produce up to 500 million vaccine doses annually for COVID-19 and other diseases. The facility will focus on manufacturing vaccine substances but could expand to fill and finish vaccine vials as early as 2023. Moderna currently is locked in a patent dispute with the US National Institutes of Health (NIH) over portions of the technology used to make its mRNA vaccine. Last week, Arbutus Biopharma and Genevant Sciences filed a lawsuit alleging Moderna infringed on a patent held by the companies for lipid nanoparticle technology, an important element of Moderna’s mRNA vaccine.
US FEDERAL BUREAU OF PRISONS Official statistics from the US Federal Bureau of Prisons (BOP) show that 287 inmates in the 122 federal prisons nationwide have died of COVID-19 since the beginning of the pandemic. In 2020, the death rate in BOP prisons was 50% higher than the 5 years prior to the pandemic. Despite memos from the US Attorney General sent early in the pandemic asking BOP to prioritize appropriate transfers to home confinement, BOP did not move quickly to review cases nor did it move forward with many transfers.
Some prisoners turned to the judicial system to ask for compassionate release, but the process can be long and the spread of SARS-CoV-2 in prisons outpaced the reviews. According to an analysis from NPR, nearly 13,000 compassionate release motions were filed in federal court in 2020, and federal judges denied more than 80% of the motions filed between January 2020 and June 2021. Of the federal inmates who have died of COVID-19, nearly all had a higher risk of dying from the virus due to older age or medical condition and at least 1 in 4 filed motions with the judicial system asking for compassionate release, according to the analysis. At least 3 inmates had their requests granted but died before they could be released, and many others died while awaiting decisions. While most of the US is loosening COVID-19 mitigation measures, federal prison inmates and staff continue to contract the virus and die. Notably, a review by STAT found that Pfizer’s COVID-19 antiviral treatment Paxlovid—shown in clinical trials to be highly effective at preventing progression to severe disease and possibly able to reduce the risk of transmission—is not being made available to most federal inmates who test positive for SARS-CoV-2.
Separately, the American Civil Liberties Union (ACLU) last week filed a lawsuit on behalf of 4 medically vulnerable detainees who have been denied SARS-CoV-2 vaccine booster doses while being held in federal immigration detention. The suit, which the ACLU hopes to transition into a class-action suit, names the US Immigration and Customs Enforcement (ICE) and US Department of Homeland Security and the agencies’ acting director and secretary, respectively. The lawsuit—which claims ICE does not have an updated policy regarding booster doses—is the second filed by the ACLU requesting access to boosters for people in ICE detention.
GENETIC FACTORS Researchers have identified 16 new genes and confirmed 7 previously identified genes that they say significantly predispose people to critical COVID-19 disease, some of which could provide targets for treatments, according to a study published in Nature. The researchers compared whole genome sequences of 7,491 COVID-19 patients admitted to intensive care units (ICUs) with those of 1,630 people who experienced mild COVID-19 as well as 48,400 people who never had COVID-19 and who were part of the UK government’s 100,000 Genomes Project. In addition to helping to identify new or existing drugs to treat COVID-19, the research could be used to help predict which patients are at risk of severe disease and which might need intensive care.
by Deuce
ti-amie wrote: ↑Wed Mar 09, 2022 8:26 pm
I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
ti-amie wrote: ↑Wed Mar 09, 2022 8:26 pm
I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
Interesting... Hardly anyone is masked here (maybe 10%) except in public transport where it's still mandatory till the end of the month.
^ How long has it been now since all protective mandates have been dropped there (except for public transport)?
And how are your case, hospitalisation, ICU, and death numbers doing? Are they rising? Falling? Moderately? Significantly?
ti-amie wrote: ↑Wed Mar 09, 2022 8:26 pm
I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
Interesting... Hardly anyone is masked here (maybe 10%) except in public transport where it's still mandatory till the end of the month.
In Georgia. Not a mask in sight.
by Suliso
Deuce wrote: ↑Thu Mar 10, 2022 3:27 am
Interesting... Hardly anyone is masked here (maybe 10%) except in public transport where it's still mandatory till the end of the month.
^ How long has it been now since all protective mandates have been dropped there (except for public transport)?
And how are your case, hospitalisation, ICU, and death numbers doing? Are they rising? Falling? Moderately? Significantly?
[/quote]
About four weeks now. Case numbers are no longer reliable (lots of self testing and not reporting). Deaths, ICU and hospital entries falling moderately. In absolute numbers still relatively high.
ti-amie wrote: ↑Wed Mar 09, 2022 8:26 pm
I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
Interesting... Hardly anyone is masked here (maybe 10%) except in public transport where it's still mandatory till the end of the month.
In Georgia. Not a mask in sight.
It depends where you are in Georgia - I still see a good portion of people with masks when I go to the grocery store or Target. Very rare to see anyone wearing one outdoors and rarely see any in restaurants anymore. Granted, other than occasional grocery trips, my primary outings are outdoor walks or weekend hiking.
by dryrunguy Here's the latest Situation Report. In case you missed it, the U.S. is closing in on 1 million official COVID deaths.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 448.3 million cumulative cases and 6.01 million deaths worldwide as of March 9. The global weekly incidence continues to decline but more slowly, down 3.5% from the previous week. Increased weekly incidence (+46.36%) in the Western Pacific region is driving the slowing decline. All other regions reported decreasing weekly incidence last week. Global weekly mortality fell 9.0% from the previous week. As expected, the cumulative number of deaths passed 6 million on March 8, serving as a reminder that the pandemic is far from over.
Global Vaccination
The WHO reported 10.7 billion cumulative doses administered globally as of March 6. A total of 4.96 billion individuals have received at least 1 dose, and 4.37 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations appears to be declining again. As of March 9, 18.05 million doses per day were recorded, down from the 25.9 million doses per day on February 14.* The trend continues to closely follow that in Asia.** Our World in Data estimates that there are 4.99 billion vaccinated individuals worldwide (1+ dose; 63.43% of the global population) and 4.45 billion who are fully vaccinated (56.5% of the global population). A total of 1.44 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
**Data for China are reported at irregular intervals.
UNITED STATES
The US CDC is currently reporting 79.2 million cumulative cases of COVID-19 and 959,533 deaths. Daily incidence continues its sharp decline, down from a record high of 809,345 new cases per day on January 15 to 37,879 on March 8, a more than 95% decrease. Daily mortality appears to have peaked during this surge on February 2 at 2,642 deaths per day, down to 1,161 on March 8.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 556 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations continue to decline, down from the most recent peak of 1.79 million doses per day on December 6 to 246,106 on March 3.* The number of daily vaccinations is at its lowest level since late December 2020, right after the vaccines were authorized. A total of 254.3 million individuals have received at least 1 vaccine dose, which corresponds to 76.6% of the entire US population. Among adults, 88.1% have received at least 1 dose, as well as 26.9 million children under the age of 18. A total of 216.4 million individuals are fully vaccinated**, which corresponds to 65.2% of the total population. Approximately 75.1% of adults are fully vaccinated, as well as 22.3 million children under the age of 18. Since August 2021, 95.5 million individuals have received an additional or booster dose. This corresponds to 44.1% of fully vaccinated individuals, including 66.6% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent several days.
**Full original course of the vaccine, not including additional or booster doses.
SIGNIFICANCE OF MASS MORTALITY As the world passed 6 million official COVID-19 deaths this week, and the US moves closer to 1 million official deaths, journalist Ed Yong poses an important question in The Atlantic: “How did this many deaths become normal?” Yong notes that when the death toll in the US hit 100,000 in May 2020, The New York Times described the loss as “incalculable.” But as the nation nears another milestone 2 years later, many are left wondering how this happened and why the death rate in the US has far surpassed that of any other large, wealthy nation. As life in the US heads back toward something resembling a pre-pandemic normal, those who lost loved ones to COVID-19 know life will never be the same. Some are working to ensure the nation does not forget the pandemic and remembers those who died. A group called Marked By COVID is lobbying to establish a national COVID memorial day as well as physical memorials in cities nationwide. Following the 1918 influenza pandemic, no effort was made to commemorate those who died or suffered substantial losses. This time must be different, advocates say, to help future generations understand the significance of public health crises.
US COVID-19 RESPONSE FUNDING In a surprising last-minute revision to a US$1.5 trillion fiscal year 2022 omnibus spending package, Democratic leaders of the US House of Representatives stripped US$15.6 billion in emergency funding for the COVID-19 pandemic response from the legislation in order to salvage the measure, which includes aid for Ukraine and money to keep the federal government running through September. The House approved the measure on March 9, and the US Senate is expected to pass the bill over the weekend. Although government funding is set to expire on March 11, the House also passed a stopgap measure to keep the government running through March 15. In a letter to colleagues, House Speaker Representative Nancy Pelosi blamed Republicans for the move, but it was also discord among Democrats that led to the cut. A proposal to offset the US$15.6 billion in additional COVID-19 spending by using unspent money sent to at least 30 states as part of last year’s US$1.9 trillion American Rescue Plan riled Democrats from affected states. Facing pressure from both sides, Speaker Pelosi cut the COVID funding from the omnibus measure. The administration of US President Joe Biden originally suggested it would ask for US$30 billion but formally requested US$22.5 billion in funding for testing, vaccines, therapeutics, and efforts to address future variants.
Administration officials have said they are quickly running out of money for COVID-19 response, and the cut leaves the future of the Biden administration’s National COVID-19 Preparedness Plan uncertain. The situation also highlighted the deep political divides over the pandemic and underlined that the pandemic is no longer a national political priority. US House Democrats later introduced a stand-alone bill that would provide US$15.6 billion in COVID-19 funding, but the measure is not expected to pass the Senate. Notably, the Biden administration estimates that monoclonal antibody treatment supplies will last through May, preventive treatments for immunocompromised individuals are expected to run out by July, and antiviral stocks will be depleted by September. Additionally, if additional spending is not authorized, the administration does not have funding to purchase more vaccines if another round of booster shots are deemed necessary, and ongoing research and pandemic preparedness efforts face funding shortfalls.
WHO ON BOOSTERS The WHO’s Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC) this week said it “strongly supports urgent and broad access” to primary series and booster doses of SARS-CoV-2 vaccines, particularly for groups at high risk of severe disease. The interim statement represents a policy shift for the agency after Director-General Dr. Tedros Adhanom Ghebreyesus last year urged wealthy nations to forgo booster doses through the end of the year and instead donate the shots to countries in need of additional supplies. The TAG-CO-VAC in January said evidence increasingly supported the use of booster doses, especially for vulnerable populations, but the group did not support “broad access” then as it did this week. Numerous studies have shown that booster doses of authorized vaccines help revive waning immune responses and help protect against severe disease, hospitalization, and death from COVID-19. The TAG-CO-VAC noted that although global vaccine supplies have increased, vaccine equity remains a challenge and efforts to rectify inequities are “strongly encouraged.” The statement also notes the potential need to update vaccines to address SARS-CoV-2 variants, as the currently authorized vaccines are based on the original form of the virus.
LONG COVID Long COVID, or post-acute sequelae of COVID-19 (PASC), is an emerging disease state that is poorly understood. Long COVID is characterized by several symptoms that last from 1 month to years after an acute SARS-CoV-2 infection clears. Symptoms of long COVID can include, but are not limited to, anxiety, depression, "brain fog," chronic fatigue, fever, myalgia, shortness of breath, and sleep problems. Long COVID already has led to an increase in the number of individuals suffering from long-term illness, and this trend may worsen as the pandemic continues. The UK-based disability charity Scope recently claimed that the number of people with mental health problems and chronic chest or breathing problems has risen by 800,000 individuals and 570,000 individuals, respectively, from 2018-19 to 2020-21. Worries are growing that an increase in the number of individuals suffering from long-term disabilities in the UK could also mean an increase in the number of people suffering from poverty and a lack of resources. In the US, Democratic Senator Tim Kaine introduced a bill to improve and expand research into long COVID. Senator Kaine suffers from long COVID and has become a champion for the issue as a result. The White House also has released a plan that includes support for Americans with long COVID.
A series of studies released over the last week have begun to shine a light on the impact of SARS-CoV-2 infection on brain function and cognitive health. The first study, published in Nature on March 7, compared brain scans from 401 individuals before and after SARS-CoV-2 infection. The initial brain scans were part of the UK Biobank that was collecting data before the pandemic began. Individuals were invited back for a second scan approximately 5 months after a SARS-CoV-2 infection. The study also had 384 SARS-CoV-2-negative controls. According to the study, individuals who had a SARS-CoV-2 infection lost between 0.2-2% more gray matter—mostly in areas associated with the sense of smell—than the control group. Additionally, individuals who had been infected had lower scores on cognitive function tests. The findings are significant, but it is still possible that the changes are reversible. A second study, published March 8 in JAMA Neurology, examined cognitive health in a cohort of 1,438 COVID-19 patients who were 60 years and older and who were discharged from hospitals in Wuhan, China, during the first few months of the pandemic. The study found a 12.45% increase in cognitive impairment 12 months after discharge when compared to controls. The authors noted that 21% of individuals who experienced severe cases of COVID-19 experienced cognitive decline within 12 months. A third study, posted March 7 in Open Forum Infectious Diseases, examined new-onset dementia in patients who experienced COVID pneumonia. According to the study, 3% of individuals who experienced COVID pneumonia developed new-onset dementia within 182 days compared with 2.5% of individuals who experienced pneumonia from other causes. Risk factors for new-onset dementia included ages 55 years and older, alcohol use or abuse, Hispanic race, history of depression, and stroke during COVID-19 hospitalization.
Additional complications related to long COVID include cardiovascular issues and nerve damage. A study published February 7 in Nature Medicine compared US Department of Veterans Affairs (VA) electronic health records from 150,000 patients who were infected with SARS-CoV-2 to millions of VA patients who did not have recorded infections. The study found a 4% increase in cardiovascular health issues in the SARS-CoV-2-positive individuals. Individuals who were hospitalized for COVID-19 were twice as likely to experience a significant cardiac event within 12 months of infection when compared to individuals who had milder cases of COVID-19. Another study, published in Neurology Neuroimmunology & Neuroinflammation on March 1, examined data from patients diagnosed with long COVID who did not have a prior history of nerve dysfunction. The study found that long COVID may lead to long-lasting nerve damage and pain. The growing body of research on long COVID indicates that the world may experience a surge in chronic illness once the emergency phase of the pandemic winds down. More research and support will be needed in the coming years to develop appropriate long COVID treatments and ensure that those suffering from long-term consequences of the pandemic are not forgotten.
EVUSHELD Evusheld—a monoclonal antibody treatment that is authorized by the US FDA for pre-exposure prophylaxis of COVID-19 among certain immunocompromised individuals—is going unused. US President Joe Biden has promised to protect the more than 7 million people in the US with weakened immune systems and those who cannot be vaccinated for medical reasons, and Evusheld, which was developed by AstraZeneca with support from the federal government, is a large part of that strategy. The Biden administration has ordered 1.7 million doses, enough to treat 850,000 people. Nearly 200,000 doses will be distributed this week, bringing the total shipped to states and territories close to 850,000. However, confusion about the drug among healthcare providers and a lack of awareness about its availability has left about 80% of those doses unused, sitting in warehouses and on pharmacy shelves.
The FDA recently revised Evusheld’s Emergency Use Authorization, updating the dosing regimen to a higher dose so the treatment might be more likely to protect against infection with certain Omicron subvariants. Additionally, Evusheld is expected to have greater neutralizing activity against the BA.2 sublineage of Omicron. However, the recommendation for doubling the dose will make the treatment even more scarce and could further confuse prescribers and patients. The Biden administration has accelerated its distribution schedule, but without further communication about the therapy’s availability and more equitable distribution, it appears access to the drug will remain complicated.
US MASK MANDATES After Hawai’i lifts its mask mandate on March 25, there will be no state-wide mask mandates in effect in the US. Under new US CDC masking guidance, more than 90% of the nation’s population can choose not to wear masks. However, the agency and other experts maintain that people who want to keep wearing masks can do so and in some cases should, particularly individuals who are immunocompromised or otherwise at high risk of infection or severe disease. However, some who are continuing to mask are reporting harassment and bullying from peers, strangers, and even political leaders. Individuals and communities faced with these new changes to masking guidance may feel liberation, confusion, or anxiety based on their own masking preferences. Experts have had equally mixed reactions. Some praised the move by CDC to adapt to fatigue for COVID-19 precautions, while others criticized the guidance for echoing past mistakes of relaxing measures only to end up facing another surge in cases, and simultaneously placing undue burden on those who are immunocompromised or too young to be vaccinated.
The US Transportation Security Administration (TSA) announced today that it will extend the mask mandate for people using public transportation through April 18. The requirement was set to expire on March 18 and has been extended twice previously. TSA said it will continue to assess the duration of the requirement in consultation with the CDC.
MASKING IN US SCHOOLS As new US CDC masking guidance encourages many communities to drop mask mandates and unmask in public places, a new study published in the CDC’s Morbidity and Mortality Weekly Report (MMWR) has left some school officials in a confused position about whether to continue requiring masking among students and staff. The study compared COVID-19 incidence across 233 school districts in Arkansas that had different masking policies—from universal and partial requirements to no rules—and made additional adjustments for vaccination rates, incidence in the surrounding communities, and socioeconomic status. The researchers found that between August and October 2021, districts with universal masking requirements had a 23% lower incidence of COVID-19 among students and staff compared to districts without masking requirements (incidence rate ratio = 0.77 [95% CI = 0.66–0.88]). While data collection occurred during Delta variant predominance rather than Omicron predominance and adjustments for differences in ventilation were not done, outside experts judge that the evidence is strong that masking requirements had a powerful effect on lowering COVID-19 incidence in schools and remain an important part of multifaceted prevention strategies.
NURSE ADVOCACY Nurses in the US have been celebrated since the start of the COVID-19 pandemic, hailed as heroes in an unprecedented time. Now, the nation’s 4 million nurses and their advocates are using that spotlight to bring attention to healthcare worker shortages and unsatisfactory working conditions. The advocacy push includes plans for a Washington, DC, National Nurses March on May 12 and lobbying efforts with federal and state lawmakers. The primary issue is increased scrutiny of travel nurses, whose wages have risen, sometimes doubling, during the pandemic. Some lawmakers argue that fees for such temporary health workers are too high and are calling for wage caps, while nurses are left wondering why no caps are placed on the pay of doctors or CEOs. Other issues under discussion include caps on patient-to-nurse ratios; antidiscrimination protections and stricter penalties for people who assault healthcare workers; loan repayment and better wages; and additional help to prevent health worker burnout, including more reasonable work hours and sufficient supplies of personal protective equipment (PPE).
ti-amie wrote: ↑Wed Mar 09, 2022 8:26 pm
I was out today and with one major exception - a woman in her slippers walking to her car - everyone was masked.
^ Even people outside?
Yes.
by ti-amie This rise is being fueled by the new variant.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
PANDEMIC MILESTONE March 11 marked 2 years since the WHO named COVID-19 a pandemic. More than 6 million people—and possibly many more—have lost their lives to SARS-CoV-2, and more than 450 million people have been infected. Notably, the WHO first declared the novel coronavirus a public health emergency of international concern (PHEIC) on January 30, 2020—when there were no deaths outside of China—but global levels of concern did not rise until the agency characterized COVID-19 as a pandemic. At that time, there were more than 118,000 cases and 4,291 deaths in 114 countries. Now, 2 years and millions more deaths later, many wealthy nations are reopening, having benefited from high levels of vaccination coverage and access to diagnostics and treatments, while some middle- and low-income countries (LMICs) continue to endure pandemic-related restrictions with low vaccination coverage and limited-to-no access to tests and therapies. To be sure, the pandemic has laid bare—and in some cases worsened—healthcare inequities among and within nations.
As some of the world seemingly moves on from the pandemic, conditions in other areas remain ideal for new variants to emerge. In the past week, there are signs that some of the sharp declines in new COVID-19 cases due to the Omicron variant could be reversing; Europe and Africa experienced an increase in cases last week, while the Western Pacific region continues to chart record numbers. More than 130 world leaders, economists, humanitarians, scientists, celebrities, and others signed an open letter urging more action to quickly vaccinate people in LMICs and “do what is necessary” to end the pandemic. Even as countries make moves to return to a “new normal” and many SARS-CoV-2 vaccines continue to prove safe and effective at preventing severe disease and death, the pandemic is not over. The virus is impossible to predict, and a new variant could develop the ability to slip past the vaccine- or infection-induced immune protection that much of the world’s population now has. That means public health measures might need to be reinstated and additional vaccine booster doses—or new vaccine formulations that address multiple variants—could be recommended in the future to combat waning protection.
EUROPEAN UPSWING Several European countries—including Austria, Germany, Netherlands, and the UK—are experiencing upswings in COVID-19 case trends over the past week, following weeks of decline. France lifted most of its restrictions on March 14 but is already seeing an increase in cases. Some nations, including the Netherlands and the UK, also are seeing increases in COVID-related hospitalizations. Several factors could be causing the increasing trends, including behavior changes following the removal of mitigation measures or waning vaccination protection. The WHO warned on March 13 that the war in Ukraine, which has forced more than 3 million people to flee to neighboring countries, could worsen the pandemic in Europe. The agency is working to keep medical supplies moving into the region. Hungary, Romania, Slovakia, and Moldova are providing testing, treatment, and vaccines at no charge to Ukrainian refugees.
Other experts posit the Omicron variant of concern (VOC) sublineage BA.2 could be driving an increase in cases. In the UK, researchers with the REACT monitoring program estimate that as of February 21, nearly half (47.2%) of sequenced samples were the BA.2 subvariant. In their previous report from late January, less than 1% of the samples were BA.2. Analysis from the Wellcome Sanger Institute shows that in the week to March 4, BA.2 is responsible for more than 75% of new COVID-19 cases in the country, suggesting the subvariant is now predominant. Notably, the REACT surveillance program, as well as several other UK COVID studies, are losing funding and will cease operations at the end of March. Several experts criticized the moves as shortsighted, saying the recent uptick in cases could portend the beginning of a sixth wave of COVID-19 cases.
In the US, daily cases, hospitalizations, and deaths continue to decline, but some warn the nation—much of which has recently dropped public health measures—should take note. With lower rates of vaccination and booster coverage than many European countries, and the BA.2 sublineage believed to be more transmissible than BA.1, the US could face rising hospitalizations if a new surge develops. The US CDC estimates that BA.2 is now responsible for about 11.6% of new COVID-19 cases in the country as of March 5, up from about 1% at the end of January. Still other experts predict the rising percentage of cases caused by BA.2 should not be cause for alarm in the US, expressing doubt that the subvariant will cause a new surge. They cite the protective effects of vaccines and natural immunity and the effectiveness of some treatments against the Omicron subvariant.
Last week at a briefing, the WHO discussed another variant, AY.4/BA.1 recombinant, or so-called “Deltacron,” which has been detected in a small number of cases in France, Netherlands, Denmark, and the US. WHO officials noted that little is known about the recombinant variant, which combines attributes from the Delta and Omicron variants of concern, but said many studies are ongoing. Several experts outside of WHO said the variant should not be cause for concern at this time.
WASTEWATER SURVEILLANCE Wastewater disease surveillance, which can detect viral fragments shed in feces, has been used for decades to track infectious agents, from polio to norovirus, but the method has moved into the spotlight during the COVID-19 pandemic. The inexpensive method can help monitor infections, predict where outbreaks might occur, and, using the added step of genetic sequencing, provide clues about how SARS-CoV-2 is evolving. In Europe, 26 of the 27 EU Member States have established SARS-CoV-2 wastewater monitoring systems.
The US CDC last month launched a dashboard for its National Wastewater Surveillance System to track SARS-CoV-2 levels in sewage so communities can quickly adapt their public health responses. But with 400 sites in 34 states, focused mainly in areas of high population, and only a dozen states routinely reporting results, the US system has enormous gaps in what could otherwise be a robust monitoring program. Instead of working with local labs to help states stand up surveillance programs, the CDC contracted a large, private commercial lab to assist states. But privacy concerns, logistical challenges, and a lack of trust in the national company have hindered progress in expanding the system. A system with wider coverage would be able to give a more detailed picture of the current pandemic’s fluctuations and also serve as a monitoring system for future disease outbreaks. But some wastewater scientists expressed concern that without permanent and more thoughtful use of funding, wastewater surveillance may never be established in the US as a long-term tool for protecting public health.
US IMMIGRATION POLICIES Early in the COVID-19 pandemic, the US CDC issued an order under Title 42 suspending the right of certain asylum seekers to enter the US at any border crossing or port of entry in order to control the situation in congregate settings where noncitizens are processed and held. Children traveling alone were exempted from the order shortly after US President Joe Biden took office in January 2021. Over the weekend, the CDC terminated the order as it relates to unaccompanied minors after determining the “expulsion of unaccompanied noncitizen children is not warranted to protect the public health.” Testing and other preventive measures now allow these children to be released to sponsors in the US, typically close relatives. The change went into effect shortly before a court order would have forced the CDC to include, not exempt, children from Title 42. The order remains in effect for all other migrants.
However, pressure is mounting for the Biden administration to end the pandemic-related border restrictions for all noncitizen migrants. President Biden made a campaign promise to end what he called the “moral and national shame” of immigration policies put into place under former US President Donald Trump, but is now facing the reality of managing what could amount to record numbers of people seeking asylum in the coming weeks. Refugees from Ukraine are making their way to the US, and last week US Vice President Kamala Harris committed to taking in more asylum seekers from the country during an overseas trip. The same day, a Ukrainian family was barred from entering the country under Title 42. Although US immigration authorities later allowed the family to enter, the situation highlighted the order that some advocates call “absurd and untenable,” especially with the availability of COVID-19 diagnostics, vaccines, and therapies. The CDC has the authority to lift the order, which is set to expire in early April.
THIRD & FOURTH VACCINE DOSES Experts are beginning to look toward the future of preventing COVID-19 cases and hospitalizations, even as many areas of the world continue to recover from surges caused by the Omicron variant of concern. Among potential strategies under review is the need for third and fourth vaccine doses, particularly of mRNA vaccines. Studies are showing that a third dose of mRNA vaccine is needed to reach the same protective levels against Omicron compared to 2 doses for the Delta and Alpha variants. Many people in the US received their third, or booster, dose before and during the Omicron wave to demonstrated efficacy in keeping people out of the hospital; a recent CDC Morbidity and Mortality Weekly Report (MMWR) study showed that unvaccinated persons were hospitalized at a rate 23.0 times higher than boosted, vaccinated persons but at a rate only 5.3 times higher than unboosted, vaccinated persons. Notably, vaccine-derived immunity does wane over time, thus necessitating future doses in order to maintain protective levels. With this expected dip in mind, some are calling for a fourth dose of mRNA vaccines. Pfizer is already planning to submit data on fourth-dose efficacy to the US FDA. A small trial conducted in Israel found that a fourth dose restored immunity levels to where they had been with a third dose, although those levels also are expected to wane.
Nevertheless, many experts are highlighting the pitfalls in continually chasing the next dose of the same vaccine, especially in the context of future variants. For this reason, vaccine manufacturers are also looking at new formulations of vaccines to cover future variants and provide longer-lasting protection. Amidst its plans to submit for authorization of a fourth dose, Pfizer also has committed to developing a longer-lasting vaccine candidate that can cover more potential SARS-CoV-2 variants. The speed and efficacy of first generation SARS-CoV-2 vaccines was remarkable and a technological feat; now vaccine manufacturers must transition to a long-term outlook for maintaining protection against SARS-CoV-2.
CHINA China is facing its largest COVID-19 outbreak since the early days of the pandemic. On March 15, the National Health Commission reported the detection of 3,507 new cases due to community transmission, more than double the 1,337 recorded in the previous 24 hours. At least 15,000 cases have been recorded in recent outbreaks in 28 provinces, with about 80% of cases caused by the highly transmissible Omicron variant. A little more than half of those testing positive are asymptomatic, and no new deaths have been reported. Authorities attribute the large proportion of asymptomatic and less serious cases to the country’s high vaccination rate, which is estimated to be about 87%.
Although the total number of cases is low compared with some other nations, China continues to enforce its “dynamic zero-COVID” approach. In response, China has locked down tens of millions of people in several neighborhoods and cities, including Jilin, where most of the new infections have occurred, and Shenzhen, the nation’s technology hub. The shutdowns are impacting car and tech manufacturing and likely will further disrupt global supply chains. Notably, Shenzhen, in Guangdong Province, shares a border with Hong Kong, which also is experiencing an Omicron-fueled surge in cases. Additionally, Jilin province shares a long border with North Korea, which continues to claim it has recorded no COVID-19 cases. The quick surge is expected to overwhelm healthcare facilities and hospitals, particularly in rural areas, and the country has moved quickly to construct temporary facilities to house thousands of people who test positive. A forecasting model run by Lanzhou University predicted the current surge of infections will be brought under control in early April, racking up about 35,000 cases. However, if the current exponential rise in daily case numbers continues, many more cases will be recorded. The current outbreak is testing China’s costly zero tolerance approach in the face of the highly infectious Omicron variant, but there is no sign the nation will pivot to a “living with the virus” mentality anytime soon, despite deep economic disruption.
HONG KONG Hong Kong is experiencing the worst Omicron variant-fueled COVID-19 surge in the world, recording the highest daily death toll of the pandemic in recent days. As of March 14, Hong Kong reported 19,844 new daily confirmed COVID-19 cases and 285 new daily deaths. It appears the city has moved beyond its peak in cases, and the number of daily deaths might be stabilizing. Still, Hong Kong’s healthcare system is overwhelmed and morgues are over capacity. The primary factor driving the surge is a low vaccination rate among those over age 80—only about 30% have received at least 1 dose—despite the availability of the shots. Comparatively, about 80% of older adults are vaccinated in the US. Additionally, the type of vaccine could be playing a role in the city’s higher death rate. A majority of vaccinated elderly received the Chinese-made CoronaVac, which has been shown to offer little to no protection against Omicron.
About 70% of assisted-living homes are experiencing outbreaks, and thousands of older adults have died of COVID-19. Hong Kong is working to maintain its “zero COVID” strategy of mass testing, contact tracing, border closures, and quarantines that kept SARS-CoV-2 at bay for the past 2 years. Nearly 300,000 of Hong Kong’s 7.4 million residents are isolating at home, and many have left the city to avoid compulsory testing, travel bans, and quarantines. Those who test positive on a rapid test—including those with mild or no symptoms—can be prosecuted if they refuse to enter a government-run quarantine center, unless the facilities are full. The government is working to construct additional isolation centers out of shipping containers. Some experts warn the initially successful “zero COVID” policy might have bred complacency, leading some people to forgo vaccination and catching the government off guard for the arrival of Omicron. Hong Kong’s situation also highlights the importance of vaccination in helping to prevent widespread disruption and protect people from hospitalization and death.
by Deuce
ti-amie wrote: ↑Tue Mar 15, 2022 7:21 pm
This rise is being fueled by the new variant.
But... but... but... the governments said the virus is gone, everything is ok now, and we can return to 'normal'.
They wouldn't lie to us, would they?
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
US PREPAREDNESS FOR BA.2 Public health professionals are warning state and federal government officials of a potential uptick in COVID-19 cases and hospitalizations due to the increasing prevalence of the Omicron subvariant BA.2. During a briefing this week, White House Chief Medical Advisor Dr. Anthony Fauci shared that current evidence suggests BA.2 is 50%-60% more transmissible than the original Omicron variant (BA.1), with similar clinical presentations. The US CDC estimates that 35% of new cases are caused by the BA.2 subvariant, and officials predict that it likely will become the predominant variant over the coming weeks.
US health officials are watching the situation in other countries, including the UK and France, for clues about how the BA.2 subvariant might impact the US. In the UK, new COVID-19 case numbers have doubled in the past 3 weeks, and hospitalizations also are rising. Case numbers also are rising in France, where most COVID-related mitigation protocols were recently lifted. There is some hope that the increased proportion of individuals with immune protection from vaccination, natural infection, or a combination could help blunt a new wave of infections in the US, leading to a less stark surge in new cases. However, many states and jurisdictions are dropping mitigation measures, reporting COVID-19 data less frequently, and closing testing sites, leaving many experts to worry these changes will create blindspots that could lead to delayed responses. Others warn the country is letting its guard down too early. Additionally, the administration of US President Joe Biden said it is quickly running out of funding to address the pandemic. All of these developments have left many, especially vulnerable populations, worried about the weeks to come.
MODERNA VACCINE Late last week, Moderna submitted a request to the US FDA for Emergency Use Authorization (EUA) of a second booster dose of its SARS-CoV-2 vaccine for all adults. Moderna’s application extends beyond the scope of Pfizer-BioNTech’s recent EUA request for a second booster dose, as that submission was limited only to adults 65 years of age and older who have received an initial booster. In a press release, Moderna explained its rationale for including an extended population pool is to provide greater flexibility to the US CDC and other healthcare providers when determining future vaccination guidance for the people in the US. Like Pfizer-BioNTech, Moderna cited data from Israel showing increased immune resilience among populations who received a fourth dose during Omicron predominance. The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) is scheduled to meet on April 6 to discuss considerations for future vaccine booster doses, as well as the process for selecting specific strains of SARS-CoV-2 for vaccines to address current and emerging variants. However, the committee will not be discussing specific applications and no vote is planned. Moderna also announced that Canada joined Australia and the EU in authorizing its SARS-CoV-2 vaccine for children aged 6-11 years.
VACCINE EFFECTIVENESS Once SARS-CoV-2 vaccines were developed, tested, and authorized for use, focus shifted toward evaluating their effectiveness in the broader population. Two of the principal concerns are the duration of protection and effectiveness against emerging SARS-CoV-2 variants. With the US past its Omicron peak, the US CDC has a wealth of data available for these analyses. The CDC’s COVID-19 Emergency Response Team published findings comparing vaccine effectiveness (VE) against hospitalization during the Omicron surge, based on data from 14 states collected from July 2021 to January 2022. At the peak of the Omicron surge, weekly per capita hospitalizations peaked at 38.4 per 100k population, compared to 15.5 during the Delta surge, and full vaccination with a booster reduced the risk of hospitalization by a factor of 12 compared to unvaccinated adults and a factor of 4 compared to adults with full vaccination and no booster. Additionally, hospitalizations during the Omicron surge were higher than during the Delta surge among both vaccinated and unvaccinated individuals. Hospitalization risk among non-Hispanic Black adults was the highest among all racial and ethnic groups and nearly 4 times the risk among non-Hispanic White adults. The researchers noted that non-Hispanic Black adults represented a larger proportion of unvaccinated adults during the Omicron surge than during the Delta surge, which likely factored into the higher hospitalization risk.
The COVID-19 Emergency Response Team also published findings from a study on mRNA SARS-CoV-2 vaccine effectiveness against invasive mechanical ventilation (IMV) and death. The researchers conducted a case-control study across 21 US medical centers from March 2021-January 2022, spanning both the Delta and Omicron surges. The study included more than 7,500 hospitalized COVID-19 patients—1,440 hospitalized adult COVID-19 patients who received IMV or died (case) and 6,104 hospitalized adult patients who tested negative for SARS-CoV-2 infection (control). Most of the vaccinated COVID-19 patients who received IMV or died “had complex underlying conditions, commonly immunosuppression.” The researchers estimated the overall VE against IMV or death to be 90%, including 88% for 2 doses and 94% for 3 doses (eg, including a booster). Specifically during the Omicron surge, the researchers estimated the effectiveness to be 79% for 2 doses and 94% for 3 doses. The overall VE among individuals who received their second dose more than 150 days prior was 84%, compared to 92% for those who received theirs 14-150 days prior. This study provides further evidence that mRNA vaccines provide substantial protection against severe COVID-19 disease and death—particularly with booster doses—including over prolonged periods and against emerging variants.
As the BA.2 subvariant begins to overtake the original Omicron subvariant (BA.1), experts have raised concerns about the continued effectiveness of SARS-CoV-2 vaccines against yet another variant. A study (preprint) of nearly 140,000 individuals conducted by researchers in Qatar found that the Pfizer-BioNTech and Moderna vaccines exhibited high effectiveness against symptomatic COVID-19 disease caused by BA.1 or BA.2 for 4-6 months after the second dose, but protection declined sharply after that point, down to approximately 10%. Booster doses restored some efficacy against both subvariants, back up to 30-60%. These data align closely with data from the UK, which show effectiveness less than 20% at 25 weeks or longer, but a third dose can increase effectiveness to approximately 70%.
A study by researchers in the UK evaluated VE for the Pfizer-BioNTech and Moderna vaccines against symptomatic disease after 1 dose among adolescents. The study utilized a case-control design and included data from children aged 12-17 years collected starting September 13, 2021, when vaccination was authorized for children aged 12-15 years. Because the UK recommends the 2 doses be administered 8-12 weeks apart, as opposed to 3, it provides the opportunity to evaluate 1-dose efficacy in this age group. The 1-dose effectiveness against the Delta variant among the 12-15 year age group peaked at 74.5% between 14 and 20 days after vaccination, before declining to 45.9% at 70-83 days. Against the Omicron variant, the 1-dose effectiveness peaked at 49.6% and declined to 16.1%. After the second dose, effectiveness peaked at 93.2% against the Omicron variant and 83.1% against the Delta variant. Similar results were observed among the 16-17 year age group, although the 2-dose effectiveness declined rapidly for the Omicron variant at Day 34 after the second dose. The vaccines exhibited 83.4% and 76.3% effectiveness against hospitalization for the Delta variant after 1 dose among the 12-15 year and 16-17 year age groups, respectively, but follow-up was not completed for 2 doses or the Omicron variant. This study provides further insight into the protection conferred against the Omicron variant, but the timing of the doses makes it difficult to compare against the efficacy estimates from clinical trials.
TYPE 2 DIABETES People who recover from acute SARS-CoV-2 infection, whether mild or severe, could experience myriad post-acute sequelae and long-term symptoms lasting weeks or months, including fatigue, shortness of breath, anxiety, depression, and cognitive impairments. The condition is known as post-acute sequelae of COVID-19 (PASC), or long COVID. Evidence is growing that people who recovered from COVID-19 within the past year have an increased risk of cardiometabolic conditions, including new onset diabetes. A study published online in The Lancet Diabetes & Endocrinology examined the post-acute risk and burden of incident diabetes in people who recovered from COVID-19. Researchers examined US Department of Veterans Health Administration (VHA) records of a cohort of 181,280 US Veterans who survived the first 30 days of SARS-CoV-2 infection between March 2020 and September 2021 and compared them with 2 large control groups—a contemporary cohort of more than 4.1 million non-infected participants who used VHA services during the same time period and a historical cohort of another 4.28 million non-infected participants who used VHA services during 2017.
Overall, COVID-19 was significantly associated with an increased risk of incident diabetes. Individuals who survived COVID-19 were 46% more likely than those with no history of COVID-19 to develop new onset diabetes (primarily Type 2) or be prescribed medication to control their blood sugar. In another calculation, the researchers found an excess burden of 1.8 per 100 people would develop diabetes or blood sugar control issues at 12 months. People older than 65 years and those with cardiovascular disease, high blood pressure, high cholesterol, or prediabetes had higher risks and burdens than younger individuals or those without underlying conditions. Additionally, Black participants had higher risks and burdens than White participants, although the researchers note that the cohort consisted primarily of White males, possibly limiting the generalizability of the findings. Notably, the risks and burdens increased according to the severity of the acute infection. Even those patients at low risk of diabetes prior to SARS-CoV-2 infection showed an increased risk of developing the condition compared to controls. The researchers concluded that diabetes and hyperglycemia should be considered in treating people recovered from COVID-19 and included in the definition of long COVID. They also warn the association between COVID-19 and incident diabetes could have significant global implications.
Another study, published recently in Diabetologia and based on records from a nationwide primary care database in Germany, found those recovered from COVID-19 had a 28% greater risk of developing Type 2 diabetes than people who never had COVID-19. Those researchers also encouraged blood sugar monitoring for all recovered COVID-19 patients. An international group of researchers have established the global CoviDIAB Registry to track COVID-19-related diabetes and severe metabolic disturbances and to examine the conditions’ pathogenesis, management, and outcomes.
US INDOOR AIR QUALITY As part of US President Joe Biden’s National COVID-19 Preparedness Plan, the US Environmental Protection Agency (EPA) last week launched the “Clean Air in Buildings Challenge” to reduce the risk of airborne viruses, including SARS-CoV-2, and other indoor contaminants. The Challenge includes a call to action for building owners and operators, schools, colleges and universities, and other organizations to assess indoor air quality and make improvements to ventilation and air filtration. Additionally, the EPA published a best practices guide, developed collaboratively with other federal agencies, that provides recommendations grouped into 4 categories: creating clean indoor air action plans, optimizing fresh air ventilation, enhancing air filtration and cleaning, and engaging those in the building community. The plan does not provide technical guidance nor discuss the cost of implementing air quality upgrades, although the EPA noted that funds from the American Rescue Plan and Bipartisan Infrastructure Law can be used to supplement investments in improving indoor air quality in public spaces.
The EPA has worked for many years to help schools improve their air quality, and the COVID-19 pandemic has brought renewed attention to the issue. Research shows that air quality improvements in schools can greatly impact health and learning, beyond reducing the risk of SARS-CoV-2 transmission. Improvements in ventilation and filtration are associated with lower rates of influenza, asthma, and absenteeism, as well as higher reading and math test scores. Advocates hope the Challenge will spur more schools and other buildings to make short- and long-term improvements as part of a layered mitigation approach to disease prevention.
PFIZER ANTIVIRAL The United Nations-backed Medicines Patent Pool (MPP) has signed agreements with 36 generic drug manufacturers in 13 countries to produce a generic version of Pfizer’s oral COVID-19 treatment for use in 95 low- and middle-income countries (LMICs) representing more than half of the world’s population. The oral treatment, known by the brand name Paxlovid, is a combination of the antiviral medications nirmatrelvir and ritonavir. The sublicense agreements are the direct result of a November 2021 voluntary licensing agreement between MPP and Pfizer. Under the agreements, the manufacturers will not need to pay royalties as long as the WHO continues to classify the COVID-19 pandemic as a public health emergency. When that designation ends, the companies can continue to sell the medication royalty-free to low-income countries but will be required to pay 5%-10% royalties on sales to certain middle-income nations. Not all of the manufacturers will fully produce the generic medication; 6 will produce ingredients, 9 will perform fill-and-finish operations, and the remaining will conduct both services. Most of the manufacturing companies—which are located in Asia, the Middle East, North and South America, Eastern Europe, and the Caribbean—indicated it will take them months to begin production. Merck and Ridgeback Biotherapeutics, which produce the oral antiviral molnupiravir, made a similar deal with the MPP in October 2021.
In a separate agreement, Pfizer will sell the United Nations Children’s Fund (UNICEF) up to 4 million courses of Paxlovid to distribute to the same 95 LMICs. Shipments of the pills will begin next month and are intended to bridge the gap in supplies until generic production is up and running. The company is providing a tiered pricing system, with low-income countries receiving the pills at lower pricing than more wealthy nations. The exact financial terms of the agreement were not disclosed.
500 MILLION DOSES US Secretary of State Antony Blinken announced last week that the US has donated more than 500 million doses of SARS-CoV-2 vaccines to more than 110 countries worldwide, bringing it closer to US President Joe Biden’s pledge to donate at least 1.2 billion doses. Notably, the US does not have data on how many of those doses have been administered and needs the US Congress to authorize additional funding for global vaccination efforts to continue. In marking the milestone, US Agency for International Development (USAID) Administrator Samantha Power said a lack of additional funding would “devastate” the agency’s efforts to help other nations deploy vaccines, as well as COVID-related diagnostics, treatments, and other supplies. Administrator Power called on the US Congress to urgently supply additional funding. Additionally, the White House has warned it will soon run out of money to purchase COVID-19 treatments and vaccines, and to maintain testing capacity domestically. A supplemental COVID-19 funding bill currently under consideration in the US Senate could provide up to US$15.6 billion, but with Republicans reluctant to approve the plan, it appears the US is set to continue its cycle of pandemic panic and neglect.
by MJ2004 Dry, I want to thank you for continuing to post the Situation Reports. They've been a source of invaluable information all along for those of us who are too lazy to look them up ourselves.
Especially now that Covid news stories have fallen by the side.
by dryrunguy
MJ2004 wrote: ↑Tue Mar 22, 2022 10:48 pm
Dry, I want to thank you for continuing to post the Situation Reports. They've been a source of invaluable information all along for those of us who are too lazy to look them up ourselves.
Especially now that Covid news stories have fallen by the side.
I'm glad you said that, MJ, because I've been toying with the idea of not posting them anymore. But the news of the past few days underscores why they may still be valuable--at least for now.
by ponchi101 No, please post them. We have no access to this info other than you. I have thanked you about it in all the posts, but MJ's words speak for many of us.
---0---
So the new variant is even more transmissible than the original Omicron. So eventually what will these variants be like? You can catch it from a person in the other side of town?
by Suliso China still fighting windmills. Now Shanghai will be locked down in two stages...
by ponchi101 I am still in Colorado and should be going back home soon. I have to look up the requirements for entry to Colombia, as I am not sure anymore if a negative test is required. By now, I just see all this as some sort of exercise; with the people that still refuse vaccination going around as if this never happened, our efforts to get the vaccine and practice some semblance of responsible behavior has gone for nothing.
It is truly despairing.
by ti-amie
by dryrunguy It's not difficult to dupe people who don't understand the fundamental difference between an antiviral and an anti-parasitic.
by ponchi101 I don't think they were even looking at that level of technicality. They just heard that people were taking it, they were feeling well, and bingo, it caught fire.
My crazy friend gave his 28 & 26 yo sons their dose of Ivermectin and "they got cured". The entire issue that they are young, sporty kids simply did not enter the equation. The reality is that "he is not being fooled by 'them'", and he reads and listens to the real doctors. It is a deep rabbit hole, and once you go in, it is almost impossible to come out.
by dryrunguy Here's the latest Situation Report. I hadn't received one in over a week, which makes me wonder if they are starting to wind these things down. Have not read it yet.
::
US COVID-19 FUNDING US Congressional negotiators on April 4 reached a deal for US$10 billion in additional funding for the federal COVID-19 response. The bipartisan legislation, if passed, would provide less than half of the US$22.5 billion initially requested by US President Joe Biden for current and future pandemic response and preparedness. Notably, the compromise does not include US$5 billion for global vaccination efforts, funding that was dropped last month from a large omnibus spending package because legislators could not agree on where that money would come from. In a statement, USAID warned that additional funding for international efforts is needed to help prevent the emergence of new variants and move the world beyond the pandemic. Domestically, the Biden administration has cautioned it is out of money to pay for the purchase of additional COVID-related treatments, vaccines, and diagnostics, as well as reimburse providers for services for those without insurance. The compromise package would provide at least US$5 billion to purchase and develop COVID-19 treatments and US$750 million for the development of variant-specific vaccines and the future expansion of vaccine manufacturing. The US$10 billion would come from repurposed unspent funds from previous stimulus packages from the Departments of Agriculture, Education, Transportation, and Treasury, as well as the Small Business Administration.
The White House urged the US Congress to move quickly to approve the funding and said it will continue to seek additional aid for domestic and global COVID-19 efforts. The US Senate could vote on the measure as soon as this week, and if approved, the bill would move to the US House. Notably, the legislation’s lack of funding for international aid could stymie progress in the House, where some Democrats already have raised objections. Negotiators could not agree on how to pay for that aid and said they intend to work toward proposing separate legislation that would provide funding for the global COVID-19 response.
US SECOND BOOSTER Health officials in the US have authorized a fourth dose, or second booster dose, of mRNA-based SARS-CoV-2 vaccines for certain segments of the population. Individuals are now eligible for a second booster dose (fourth total dose) of the Pfizer-BioNTech vaccine if their first 3 vaccines were either Pfizer-BioNTech or Moderna, it has been at least 4 months since their initial booster, and they are aged 50 years and older. Individuals also are eligible for a second booster dose of the Pfizer-BioNTech vaccine if their first 3 vaccines were either Pfizer-BioNTech or Moderna and they are aged 12 years and older with an immunocompromising condition. Additionally, individuals are now eligible for a second booster dose (fourth total dose) of the Moderna vaccine if their first 3 vaccines were either Pfizer-BioNTech or Moderna, it has been at least 4 months since their initial booster, and they are aged 50 years and older. Individuals also are eligible for a second booster dose of the Moderna vaccine if their first 3 vaccines were either Pfizer-BioNTech or Moderna and they are aged 18 years and older with an immunocompromising condition. Additionally, individuals who received J&J-Janssen for their initial and booster doses are eligible for a booster dose of either Pfizer-BioNTech or Moderna if at least 4 months have passed since their last booster.
The complex second booster dose guidelines have led to widespread confusion among patients and primary care physicians alike. In response, the US FDA released a vaccine eligibility chart and simplified guideline breakdown in an attempt to make the recommendation easier to understand. However, the situation is further complicated by debate surrounding the potential risks and benefits of a second booster dose. The risks, in many cases, appear minimal and have little scientific support. The known risks include symptoms such as fever and body aches that are common adverse events of the currently approved vaccines and the costs that some individuals might have to pay to receive an additional booster due to a lack of federal funds to reimburse providers to administer the shots to uninsured patients. Other risks that are often discussed but remain unproven include: immune exhaustion from multiple vaccinations, vaccine imprinting that could leave individuals susceptible to a SARS-CoV-2 variant, and missing out on a variant-specific vaccine if one is released shortly after receiving a second booster of the original vaccine design. These risks are of relatively low concern because vaccinations are unlikely to cause immune exhaustion since they do not cause chronic exposure to an antigen; imprinting for current SARS-CoV-2 vaccine designs is not currently supported by scientific evidence; and most variant-specific vaccine designs do not appear to offer better protection than the original formula. The benefit of a fourth mRNA-based vaccine dose includes a small boost in immediate protection that may fade over time. That small benefit may be greater in the populations approved under the new guidelines. Many public health experts, including the Johns Hopkins Center for Health Security’s Dr. Amesh Adalja, have recently warned that repeatedly boosting immunity with the same vaccine design is not a viable strategy to end the pandemic.
J&J-JANSSEN VACCINE A new report from the US CDC’s Morbidity and Mortality Weekly Report (MMWR) examined the impact of receiving booster doses from various SARS-CoV-2 vaccines among individuals who originally received the J&J-Janssen (Ad.26.COV2) vaccine. The single-dose, adenovirus vector-based vaccine has been the subject of many studies since its authorization in 2021, with data initially suggesting that it may offer slightly less protection than the mRNA-based vaccine candidates produced by Pfizer-BioNTech and Moderna. More recent data counter these claims, showing similar levels of effectiveness in preventing infection, hospitalization, and death. The MMWR report acknowledges the vaccine’s effectiveness and provides data suggesting that a mixed-dose booster regimen using an mRNA vaccine performs better at preventing severe disease than a vaccine-booster regimen of only the J&J-Janssen vaccine, particularly during Omicron predominance. The study examined 80,287 emergency department/urgent care visits and 25,244 hospitalizations that occurred across 10 US states between December 16, 2021, and March 7, 2022. According to the data, vaccine effectiveness against preventing COVID-19 hospitalizations was 24% after 1 dose of the J&J-Janssen vaccine, 54% after 2 J&J-Janssen doses, 79% after 1 J&J-Janssen plus 1 mRNA dose, and 83% after 3 mRNA doses. The WHO on April 4 updated its Emergency Use Listing (EUL) of the J&J-Janssen vaccine to recommend the shot as both a prime and homologous or heterologous booster vaccine candidate for adults aged 18 and older.
OMICRON SUBVARIANTS Public health officials in the UK recently identified a new subvariant of the SARS-CoV-2 Omicron variant of concern (VOC). The subvariant, called XE, is a recombinant variant that includes genetic material from both the original BA.1 strain of Omicron and its subvariant BA.2. The emergence of the recombinant subvariant is not particularly surprising, considering the high transmission rates of both BA.1 and BA.2, and scientists so far have expressed little concern over the subvariant’s potential impact. In a WHO epidemiological update published last week, the agency shared that XE may be slightly more transmissible than BA.2, suggesting that the subvariant may have a growth rate advantage of around 10%. To date, the subvariant makes up a small proportion of the samples sequenced in the UK, and the WHO said more data are needed to provide definitive statements on XE’s overall risk. One potential pitfall to collecting more data is the recent announcement that the British government is scaling back its COVID-19 surveillance programs. The UK has submitted more than 1 million sequenced Omicron samples to GISAID—a global repository of SARS-CoV-2 genetic information—a key factor in the identification of the XE subvariant. Other nations, including Denmark, also are scaling back their sequencing efforts, potentially creating blind spots in the early identification of newly emerging variants and limiting the speed at which countries will be able to respond to new threats.
Chinese public health officials also recently reported the identification of a new Omicron subvariant amid an increase in daily case numbers. According to an in-country report, the subvariant stems from the original BA.1 Omicron and was isolated in a mildly symptomatic COVID-19 patient. The report adds that sequencing of the subvariant does not match other cases in the country nor any variants listed on GISAID. The Chinese government has been working to contain a recent surge in new COVID-19 cases fueled by the Omicron VOC as well as low vaccination coverage among the elderly population.
SHANGHAI China’s largest city and a global financial center is experiencing a record number of daily COVID-19 cases, driven by the Omicron BA.2 subvariant. Over the weekend, Shanghai entered an indefinite citywide lockdown, the latest example of the government’s efforts to adhere to its “zero COVID” strategy. All 26 million Shanghai residents were tested for SARS-CoV-2 in 24 hours, with many strictly confined to their homes and unable to leave even to obtain essentials. Some residents are reporting difficulties ordering food and water online due to restrictions and supply and delivery staff shortages. A policy to separate children who test positive from their families is drawing fierce criticism from city residents as well as Western diplomats. Isolation facilities are overflowing with patients, with some mixing symptomatic and asymptomatic patients, and people with non-COVID illnesses are being turned away by hospitals. The government has sent more than 2,000 military medical personnel and at least 30,000 healthcare providers to Shanghai to assist in the “dynamic clearing” of cases. China recorded about 16,400 new local COVID-19 cases on April 4—the highest daily total in 2 years—with more than 80% of those cases in Shanghai. Other provinces and cities, including Guangdong, Jilin, and Shandong, are recording medium or high risk of transmission and are required under official guidance to enter some form of lockdown. Nationwide, nearly 25 cities are under total or partial lockdown, impacting about 193 million people in areas accounting for nearly 14% of the country’s gross domestic product and causing widespread disruptions.
COVID-19 THERAPEUTICS The US FDA on March 25 amended the Emergency Use Authorization (EUA) of the monoclonal antibody sotrovimab, limiting its use to treat COVID-19 only in US regions where the Omicron BA.2 subvariant is not predominant. Recent data show that the authorized dose of sotrovimab is unlikely to be effective against BA.2. As of April 2, the US CDC estimates BA.2 is responsible for approximately 72% of new COVID-19 cases nationwide. The FDA noted that several other treatments—including Paxlovid, Veklury (remdesivir), bebtelovimab, and Lagevrio (molnupiravir)—are expected to remain effective against BA.2. GlaxoSmithKline and Vir Biotechnology, which manufacture sotrovimab, said they plan to submit data supporting the use of a higher dose of the therapy to treat Omicron BA.2.
Several studies set to be presented at the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID) in Lisbon, Portugal, later this month suggest that the oral antiviral molnupiravir can reduce symptoms of COVID-19 by day 3 of administration, clear active SARS-CoV-2 virus equally well in immunocompromised and immunocompetent patients, and lower viral load by day 3 of treatment. The results, which are based on findings from the MOVe-OUT clinical trial, were collected throughout 2021 and are not yet peer-reviewed. Molnupiravir is authorized for use in the US, UK, Australia, Japan, and 12 other jurisdictions.
The results of a randomized clinical trial published in the New England Journal of Medicine (NEJM) show that high-titer convalescent plasma administered within 9 days after the onset of COVID-19 symptoms helped to reduce disease progression leading to hospitalizations in a largely unvaccinated population. COVID-19-related hospitalization or death within 28 days occurred among 2.9% of patients who received the high-titer plasma compared with 6.3% of those who received control plasma (P=0.005), for a 54% relative risk reduction that was entirely accounted for by hospitalization. The researchers, led by Dr. David J. Sullivan of Johns Hopkins Bloomberg School of Public Health, encouraged the use of high-titer convalescent plasma in early outpatient treatment when other therapies are unavailable or ineffective, including in low- and middle-income countries. Under an amended FDA EUA, high-titer convalescent plasma is authorized in the US for the treatment of COVID-19 in patients with immunosuppressive disease or receiving immunosuppressive treatment, in either outpatient or inpatient settings.
COVAXIN The WHO on April 2 suspended the supply of the Covaxin SARS-CoV-2 vaccine produced by India-based Bharat Biotech and available under WHO Emergency Use Listing (EUL), after an inspection found good manufacturing practices (GMP) deficiencies. The suspension will result in an interruption of Covaxin supply for export through UN procurement agencies, as Bharat addresses the deficiencies and upgrades its facilities. The WHO noted that the suspension does not affect the vaccine’s efficacy or safety and asked countries that received the vaccine to take appropriate actions, though no details on those actions were given. Last week, Bharat indicated it is slowing production of Covaxin due to decreasing demand, a fall in COVID-19 cases, and wider vaccination coverage in India.
WHO COVID-19 RESPONSE PLAN Last week, the WHO published a new strategic plan outlining several key objectives meant to bring the world out of the global COVID-19 pandemic emergency. The organization said if efforts to reduce infections and diagnose and treat cases are implemented at national, regional, and global levels, the acute phase of the epidemic can come to a close. Those activities include increasing surveillance and monitoring, improving vaccine equity, strengthening healthcare systems, and fortifying research and data analyses activities. In a forward to the plan, WHO Director-General Dr. Tedros Adhanom Ghebreyesus highlighted “the equitable use of vital COVID-19 tools” as a key factor in ending the pandemic and making COVID-19 a “manageable disease.”
The WHO acknowledged that vaccines are proving to be less effective than hoped in reducing infection with and transmission of the predominant Omicron variant of concern but maintained that a goal of vaccinating 70% of the world’s population by the middle of 2022 remains relevant, particularly if national programs prioritize vulnerable populations, including elderly individuals, healthcare workers, and those with underlying health conditions. The report also conceded that adjustments to the 70% goal are under consideration. While some experts argue that altering the target could leave low- and middle-income countries open to greater impacts from future surges or SARS-CoV-2 variants, other global health organizations say focusing on vaccinating 90% of vulnerable populations in every country would help focus short-term goals and makes more sense in terms of resource allocations. Only 14.7% of people in low-income countries have received at least 1 dose of a SARS-CoV-2 vaccine, according to Our World In Data. Additionally, 21 of WHO’s 194 Member States have vaccinated less than 10% of their population, and 75 have vaccinated less than 40%, meaning the goal of reaching 70% in the next few months remains far out of reach for many.
by ponchi101
dryrunguy wrote: ↑Tue Apr 05, 2022 6:25 pm
Here's the latest Situation Report. I hadn't received one in over a week, which makes me wonder if they are starting to wind these things down. Have not read it yet.
::
US COVID-19 FUNDING US Congressional negotiators on April 4 reached a deal for US$10 billion in additional funding for the federal COVID-19 response. The bipartisan legislation, if passed, would provide less than half of the US$22.5 billion initially requested by US President Joe Biden for current and future pandemic response and preparedness. Notably, the compromise does not include US$5 billion for global vaccination efforts, funding that was dropped last month from a large omnibus spending package because legislators could not agree on where that money would come from. In a statement, USAID warned that additional funding for international efforts is needed to help prevent the emergence of new variants and move the world beyond the pandemic. Domestically, the Biden administration has cautioned it is out of money to pay for the purchase of additional COVID-related treatments, vaccines, and diagnostics, as well as reimburse providers for services for those without insurance. The compromise package would provide at least US$5 billion to purchase and develop COVID-19 treatments and US$750 million for the development of variant-specific vaccines and the future expansion of vaccine manufacturing. The US$10 billion would come from repurposed unspent funds from previous stimulus packages from the Departments of Agriculture, Education, Transportation, and Treasury, as well as the Small Business Administration.
The White House urged the US Congress to move quickly to approve the funding and said it will continue to seek additional aid for domestic and global COVID-19 efforts. The US Senate could vote on the measure as soon as this week, and if approved, the bill would move to the US House. Notably, the legislation’s lack of funding for international aid could stymie progress in the House, where some Democrats already have raised objections. Negotiators could not agree on how to pay for that aid and said they intend to work toward proposing separate legislation that would provide funding for the global COVID-19 response.
...
But right on cue, the GOP did not approve it.
But honestly, it seems to me as if one of the reasons (at least partially) is that there is no money for this. An interesting point: the USA finally reached a point in which it could not pay for something.
(I know, if it had been a new weapons' system the money would have been there, but I still find it interesting).
by ti-amieAfter Gridiron Dinner, a covid outbreak among Washington A-list guests
Raimondo, Schiff, Castro, Garland and several other officials or journalists tested positive after the elite Gridiron dinner
By Paul Farhi, Roxanne Roberts and Yasmeen Abutaleb
Today at 1:11 p.m. EDT|Updated today at 5:29 p.m. EDT
More than a dozen guests who attended Saturday night’s Gridiron Club dinner — including two Cabinet members, two members of Congress and a top aide to Vice President Harris — have since tested positive for coronavirus, sending ripples of anxiety through a city on the cusp of restarting its traditional social whirl after a two-year pause.
A-list guests were asked to show proof of vaccination but not negative tests, and many mingled freely without masks at the dinner at the downtown Renaissance Washington Hotel.
But by Wednesday, Reps. Adam B. Schiff (D-Calif.) and Joaquin Castro (D-Tex.) and Commerce Secretary Gina Raimondo had announced they had tested positive. They were soon followed by Attorney General Merrick Garland, who requested a test Wednesday afternoon after learning he may have been exposed — and discovered that he, too, carried the virus. Thus far, none have reported serious illness.
Jamal Simmons, the communications director for Vice President Harris, said later Wednesday he, too, had tested positive and is now isolating at home. But since he had been in close contact with Harris, she would also be consulting with a physician, her press secretary said.
The Washington Post has learned of about a half-dozen journalists as well as members of the White House and National Security Council staffs who said they tested positive after the event. Their names are being withheld because they have not announced their status publicly.
Tom DeFrank, a contributing columnist for National Journal and president of the Gridiron Club, said that as of Wednesday afternoon, the group knew of 14 guests who had tested positive.
“There is no way of being certain about when they first contracted covid,” he said in a statement. “But they did interact with other guests during the night and we have to be realistic and expect some more cases.”
About half of the cases appeared to have been clustered at three tables, he said, and the club was taking steps to notify anyone who sat next to or across from the infected guests.
How many of the infections began at the dinner and how serious the outbreak will prove to be remains unclear. Many of the guests have jobs that require regular testing that catches some asymptomatic cases. Castro and Raimondo said they are suffering only mild symptoms while Schiff said he is “feeling fine” — and touted the value of vaccinates and boosters.
But the outbreak at the Gridiron — where some of the comic skits featured actors dressed as the coronavirus, like large, green bouncing balls with red frills — highlights the personal risk-benefit balancing act much of the country will be negotiating as the pandemic subsides.
Administration officials and many experts have said that, more than two years into the pandemic, individuals now have the tools they need to decide what level of risk they’re willing to tolerate — and that every social interaction, large or small, comes with a nonzero risk of covid-19 and other respiratory illnesses.
“The virus isn’t going to go anywhere. There’s not going to be any activity that isn’t going to have some level of covid risk associated with it,” said Amesh Adalja, an infectious-disease doctor and senior scholar at the Johns Hopkins Center for Health Security. “People are out at bars every day. People are having dinners, watching sports games, doing whatever they want but when it happens to a celebrity or politician, then it becomes something you have to talk about.”
Several of the White House aides who tested positive did so after traveling to Poland last week with President Biden and before the Gridiron dinner. White House press secretary Jen Psaki — who attended the Gridiron dinner — reiterated Wednesday that all White House employees who come in proximity to Biden are regularly tested.
Biden didn’t attend the dinner but appeared via video.
The white-tie-and-gowns dinner attracted about 630 guests, including members of Congress, the Cabinet, diplomatic corps, military and business.
Among those in attendance were Anthony S. Fauci, the nation’s top infectious-disease expert and Rochelle Walensky, the director of the Centers for Disease Control and Prevention.
Other guests included Sens. Susan Collins (R-Maine), Edward J. Markey (D-Mass.), Amy Klobuchar (D-Minn.), Kirsten Gillibrand (D-N.Y.) and Roy Blunt (R-Mo.); Reps. Jamie B. Raskin (D-Md.) and Debbie Dingell (D-Mich.); Agriculture Secretary Tom Vilsack and special presidential envoy John F. Kerry; Federal Reserve Chair Jay Powell; Govs. Larry Hogan (R-Md.) and Chris Sununu (R-N.H.); and New York Mayor Eric Adams (D).
The possibility that senators at the dinner were infected could conceivably delay a Senate vote to confirm Biden’s Supreme Court nominee, Ketanji Brown Jackson. A vote could come later this week; no delays have been announced.
The dinner’s guest list also included former NFL great Emmitt Smith; NBA Commissioner Adam Silver; CBS host Jane Pauley and her spouse, “Doonesbury” cartoonist Garry Trudeau; Ukraine’s ambassador to the United States, Oksana Markarova; “Face the Nation” host Margaret Brennan, PBS NewsHour anchor Judy Woodruff; ABC chief Washington correspondent Jonathan Karl, and Washington Post publisher Fred Ryan and editor Sally Buzbee.
After a predinner cocktail reception, guests sat together at long, narrow tables for hours and watched satirical skits and songs performed by members. At the event’s conclusion, guests joined hands for the traditional singing of “Auld Lang Syne.”
The dinner was supposed to reflect a return to normalcy after being canceled the past two years because of the pandemic. Few guests wore masks or observed social distancing, according to people in attendance. Only the serving staff was consistently masked throughout the evening. While organizers asked attendees to show their vaccination cards at the door, there was no requirement to be tested.
(...)
The Gridiron dinner is a smaller, more elite precursor to the better-known White House Correspondents’ Association gathering in late April. That organization’s president, Steven Portnoy, said earlier this week that it will require its dinner’s 2,600 guests to show a same-day negative coronavirus test, which they will be able to upload to an app.
The president typically attends the WHCA dinner, though Trump never did during his years in the White House. Biden has not yet announced his plans.
The Gridiron Club dinner appears to have been conducted with respect to the latest official guidelines for covid safety.
The CDC updated its guidelines on Feb. 25 to ease mask recommendations for the vast majority of the country, and all 50 states have lifted their mask mandates in recent weeks. More than 95 percent of the country, including D.C., is classified by the CDC as having a low burden of disease, meaning the agency does not recommend a mask mandate.
But some experts have cautioned that the new CDC guidelines could leave the country unprepared in the event of another wave. The BA.2 variant caused a sharp rise in cases in Europe and has become the dominant strain in the United States, although cases have not yet begun rising nationally. Some parts of the country, including the Northeast, are beginning to experience a modest increase in infections.
Outbreaks from events such as the Gridiron dinner could signal what is to come, said Abraar Karan, an infectious-disease physician at Stanford University. “You’ll have these big outbreaks that start slowly and then you’ll notice more of them. It’s not surprising to me there was this big outbreak at a gathering where people were testing afterward,” Karan said.
“We’re constantly testing the boundaries. Everybody is testing the boundaries a little bit. … We’re trying to see what’s a tolerable level of risk, but when you have a big outbreak, that makes everybody pause,” Karan said.
Fauci, who said he has not tested positive, said he abided by CDC guidelines when deciding to attend the dinner. He said he made a personal decision that the risk of attending was low for three reasons: He is vaccinated and boosted, there was a requirement for proof of vaccination to enter the dinner, and D.C. is classified as having a low burden of disease by the CDC’s metrics. That classification also means individuals can go unmasked in indoor settings.
Fauci said he wore his mask during the reception but took it off to eat.
“We are in a situation where, as a population, we need to make a decision that is based on data as well as our own individual willingness to take whatever level of risk happens to be present that you’re making the decision about,” Fauci said. “I followed the CDC guidelines, which says it’s okay to be in an indoor setting without a mask. But if cases go up and CDC says now wait a minute, you’re in a red zone, you can be darn sure I won’t be going to any dinners. You go with what the situation is.”
Staff writer Tyler Pager contributed to this report.
by dryrunguy This morning's NY Times e-newsletter dedicated its opening section to, basically, "Why is the latest variant leading to increasing caseloads in Europe and not the U.S.?"
I think we have part of the answer to this question. The variant is omnipresent in the U.S. But only certain folks are getting tested. Plus, lots of free testing sites have shut down in the U.S., and many poor folks have to pay for their own tests if they want one.
Meanwhile, based on the CDC's most recent guidance, I'm eligible to get my second booster (because I am over 50) the next time I'm in Chambersburg. Looks like that will be April 14.
I'm not wild about the idea of having to get vaccinated every 4 months--especially since my first booster wasn't particularly nice to me. Not to mention, I have some questions (please don't take that the wrong way!) about the effectiveness of existing vaccines when it comes to the latest (and future) variants and some evidence suggesting that we may actually be over-vaccinating ourselves.
I'm so sick of this.
by MJ2004 I haven't seen compelling evidence that this fourth booster is necessary just yet. Just because you're eligible doesn't mean you should get it right away.
The efficacy of the fourth shot was lower than the third shot with the Israeli study. I've heard it might be better to wait until fall to be vaccinated before the winter when there's a higher incidence of infections and to plan on once per year. I know they're experimenting with a combined flu/covid vaccine, I don't think it's quite there yet, but it would be great if that could happen.
by Deuce Anyone who has thought for one second that COVID-19 is over, or that we are well on our way out of it should read this, and/or who feels that we no longer need masks or vaccines... should read this below, written by a medical doctor and scientist.
While it is convenient and comforting to believe that this virus is on its way out of our lives, and/or that it will soon be rather insignificant, the scientific facts show otherwise. Illusions - no matter how pretty and comfortable they may be - can be hazardous to our health.
As some scientists and medical people are saying: Complacency could well end up being the most dangerous element of all...
MJ2004 wrote: ↑Thu Apr 07, 2022 12:30 am
I haven't seen compelling evidence that this fourth booster is necessary just yet. Just because you're eligible doesn't mean you should get it right away.
The efficacy of the fourth shot was lower than the third shot with the Israeli study. I've heard it might be better to wait until fall to be vaccinated before the winter when there's a higher incidence of infections and to plan on once per year. I know they're experimenting with a combined flu/covid vaccine, I don't think it's quite there yet, but it would be great if that could happen.
Together with Dry, I don't know what to do with the 4th shot (I have my 3rd). Your post makes me wonder even more. I don't know if to rush to the drugstore here while I am in the USA and get it, or wait some more and get it in Colombia . I am just past the 4th month deadline (by days) so, again, I am not sure what to do.
by dryrunguy Meanwhile, my new gas stove was supposed to be delivered and installed this afternoon. They called this morning to reschedule because the person who was supposed to install it (it's a propane stove) called in sick... You guessed it... COVID. Now we rescheduled (again) for April 13 (different installer).
So, yeah... That bug is still very much around and quite alive and well.
by Deuce Another potential advantage of waiting a bit before getting the 4th vaccine (2nd booster) is that it increases the chances that a vaccine which more specifically targets the current variant may be available.
by dryrunguy Here's the latest Situation Report. I was most interested in the section on Biden's FY 23 budget request related to long COVID funding. There's also more detail about the Israeli study MJ mentioned, as well as initial findings of a Brazilian ivermectin study that showed exactly what anyone with two functioning brain cells already knew about ivermectin as a potential COVID therapeutic.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 493.4 million cumulative cases and 6.17 million deaths worldwide as of April 7. The global weekly incidence decreased for the second consecutive week, down 14% from the previous week, and notably, all regions reported decreasing trends in weekly incidence last week. After a 1-week spike in reported global weekly mortality 2 weeks ago—46,479 deaths the week of March 21; +41% from the previous week—the trend is once again decreasing, down 42% from the previous week and -18% compared to the week of March 14.
Global Vaccination
The WHO reported 11.3 billion cumulative vaccine doses administered globally as of April 5. A total of 5.06 billion individuals have received at least 1 dose, and 4.54 billion are fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline, down from nearly 40 million doses per day in late December 2021 to 13.8 million on April 6, a decrease of nearly two-thirds over that period.* The trend continues to closely follow that in Asia. Our World in Data estimates that there are 5.09 billion vaccinated individuals worldwide (1+ dose; 64.7% of the global population) and 4.58 billion who are fully vaccinated (58.2% of the global population). A total of 1.71 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US surpassed 80 million cumulative cases on April 4.
1 case to 20 million: 343 days
20 to 40 million: 247 days
40 to 60 million: 126 days
60 to 80 million: 86 days
The US CDC is currently reporting 80.1 million cumulative cases of COVID-19 and 980,220 deaths. The decline in daily incidence tapered off at approximately 25-26,000 new cases per day from March 25-April 4, but the average jumped to 26,845 on April 5. Daily mortality continues to decline, down to 533 deaths per day on April 5, an 80% decline from the recent high in early February.* Notably, the average daily mortality is at its lowest level since August 2, 2021. At this pace, the US would surpass 1 million cumulative deaths in slightly more than 1 month; however, the decreasing trend is encouraging, and the timeline will likely be longer than this.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 563 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations have increased slightly over the past several days, with the average climbing from 154,000 on March 28 to 227,000 on March 31. Based on the timing of the increase, it is likely a result of the US FDA’s authorization of a second booster dose of the mRNA-based SARS-CoV-2 vaccines for certain individuals. A total of 256 million individuals have received at least 1 vaccine dose, which corresponds to 77.1% of the entire US population. Among adults, 88.5% have received at least 1 dose, as well as 27.4 million children under the age of 18. A total of 218 million individuals are fully vaccinated**, which corresponds to 65.7% of the total population. Approximately 75.6% of adults are fully vaccinated, as well as 22.9 million children under the age of 18. A total of 98.3 million individuals have received an additional or booster dose. This corresponds to 45.1% of fully vaccinated individuals, including 67.6% of fully vaccinated adults aged 65 years or older.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent several days.
**Full original course of the vaccine, not including additional or booster doses.
ISRAELI FOURTH DOSE STUDY Researchers from Israel published findings from a study on the effectiveness of fourth doses of the Pfizer-BioNTech SARS-CoV-2 vaccine (ie, second booster dose). The study, published in the New England Journal of Medicine (NEJM), evaluated health records data from more than 1.2 million adults aged 60 years and older who were eligible for a fourth dose of the vaccine during Israel’s Omicron surge. Israel authorized fourth doses for several high-risk groups in January, including adults aged 60 years and older and healthcare workers.
The researchers compared the rate of SARS-CoV-2 infection and severe COVID-19 disease between individuals who received 4 doses of the vaccine and those who received 3 doses. The rate of severe COVID-19 among the 4-dose group at 4 weeks after the fourth dose was 3.5 times lower than the 3-dose group. Similarly the rate of infection in the 4-dose group was half of that among the 3-dose group. Protection against infection waned, however, with no significant increase in protection by week 8. The study period for severe disease was only 6 weeks, but the fourth dose’s increased effectiveness remained significant through that period and actually increased from a factor of 3.5 at week 4 to 4.3.
The study illustrates that additional booster doses can provide increased protection against infection and severe disease beyond the effect of the first booster dose; however, the effects may provide only moderate additional benefit and for a relatively short duration. The added protection against infection faded within 8 weeks, and the 6-week study period for severe disease does not provide evidence of prolonged protection. The study also does not compare the fourth dose to unvaccinated individuals or fully vaccinated individuals without a booster or for adults under the age of 60. So while a fourth dose provides a statistically significant benefit beyond the effect of the third dose, it is possible that the third dose provides sufficient protection and that the added benefit of an additional booster is relatively minimal and unnecessary. Many questions remain regarding the value and strategy regarding future booster doses for SARS-CoV-2 vaccines, and this study contributes analysis necessary for those debates.
FUTURE VACCINE STRATEGY US federal regulators and vaccine science experts met on April 6 to discuss the future of SARS-CoV-2 vaccination, including what a strategy and framework might look like. Last week, the US FDA authorized and the US CDC recommended that adults aged 50 years and older and individuals with certain kinds of immunocompromise can receive a fourth dose, or second booster, of an authorized mRNA vaccine. During this week’s meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC), regulators were careful to say that the recent decision on boosters is a “stopgap measure” to protect these certain vulnerable groups until a more comprehensive booster plan can be considered. One framework being considered is based on the process used to update influenza vaccines. But presenters at the meeting underscored the challenges in predicting future SARS-CoV-2 variants, updating vaccine formulations, and collecting enough rigorous data in time to produce sufficient supplies.
The committee did not hold a vote during this meeting but is expected to reconvene later this spring or early summer to consider updated booster formulations for this fall. In order to achieve this goal, manufacturers would need to begin collecting new data within the next few weeks. This is a tight timeline in order to meet a fall authorization deadline, but some manufacturers are hoping to soon submit data on reformulated vaccines. Pfizer has announced its intention of making new vaccine formulations that would potentially cover emerging SARS-CoV-2 variants and provide coverage on an annual schedule. The panel also discussed what information is still needed to help solidify future vaccine strategy, including consensus on correlates of immune protection from both antibodies and memory cells and vaccine efficacy level against severe disease.
In Europe, the European Centre for Disease Prevention and Control (ECDC) and the European Medicines Agency (EMA) issued advice on a fourth vaccine dose, concluding there is not enough evidence yet to recommend the extra shots for the general population. However, both agencies agreed that data supports second boosters for people aged 80 and older in order to reduce the risk of severe disease.
US LONG COVID PLAN US President Joe Biden on April 5 directed government agencies to redouble their efforts to mitigate the long-term impacts of COVID-19, including making additional strides to research and treat post-acute sequelae of COVID-19 (PASC), commonly known as long COVID. The condition, which can last for weeks, months, or even years, is characterized by a variety of symptoms including brain fog, fatigue, shortness of breath, muscle weakness, depression and anxiety, and other symptoms. President Biden’s announcement follows criticism from patients and experts who say the federal government is not moving quickly enough to better define the condition, ascertain its prevalence, and learn more about who might be at increased risk of developing long COVID.
The plan includes several components, including the creation of a new national council to coordinate interagency efforts on long COVID focused on improving care, enhancing outreach and education, and advancing research. Specific actions include accelerating the enrollment of 40,000 people in the ongoing US NIH RECOVER Initiative; publishing a report within 120 days detailing available federal agency services for people with long COVID, those experiencing COVID-related loss, and individuals with pandemic-related mental health and substance use problems, with a focus on “high-risk communities”; establishing “Centers of Excellence” and better referral and care models for people with long COVID; educating healthcare providers to help detect, understand, and improve care for long COVID; ensuring health insurance coverage for long COVID care; increasing awareness of long COVID as a potential cause of disability and updating relevant policy; and strengthening support for workers experiencing the condition. Some of the efforts are dependent upon funding contained in President Biden’s fiscal year 2023 budget request, which includes US$20 million for the development of long COVID clinics and US$25 million for the US CDC to boost its long COVID research efforts. Outcomes of US Congressional budget negotiations will not be known for months.
COVID-19 CASE DEFINITION The US daily COVID-19 incidence has declined more than 95% from its record high in January, at the height of the Omicron surge, and current hospitalizations are down nearly 93%. These decreasing trends signal decreases in community transmission, but this may not be the only factor. On March 29, the New Hampshire Department of Health and Human Services (NHDHHS) updated how it reports COVID-19 hospitalizations, with a new metric that only includes patients treated with remdesivir and/or dexamethasone, drugs typically reserved for severe patients. After the change, the current statewide hospitalizations reportedly fell to fewer than 10, down from 20-25 the previous week. The New Hampshire Hospital Association (NHHA) reports explicitly note that the “Treated for COVID-19” numbers are a subset of the total hospitalized COVID-19 patients. The NHHA includes additional data for “COVID-Recovering,” which includes hospitalized COVID-19 patients that no longer qualify under the state case definition, such as patients who are still hospitalized and receiving treatment for COVID-19-related conditions. On April 6, NHHA reported 51 “COVID-Recovering” patients statewide, compared to only 6 “Treated for COVID-19” patients.
The NHDHHS announcement argued that the new metric aligns with treatment guidelines issued by the US NIH and better reflects the current epidemiological situation by focusing on patients hospitalized with severe COVID-19 disease. Several other states are reporting similar metrics; however, they do so alongside the total number of hospitalized COVID-19 patients, whereas New Hampshire lists only the new metric. New Hampshire removed the previous hospitalization metric from its COVID-19 dashboard, and historical data are only available in archived form.
The new approach excludes both patients hospitalized for other conditions that happen to test positive for SARS-CoV-2 infection and patients hospitalized for mild or moderate COVID-19 who are not treated with the designated drugs. A representative from NHHA emphasized that the total number of hospitalized patients more accurately reflects the burden on local health systems, because COVID-19 patients that do not meet the new case definition are still occupying beds and consuming hospital resources. Additionally, patients hospitalized for other conditions may require additional resources (eg, separate rooms, infection prevention protocols) if they test positive for COVID-19, which places additional burden on hospitals.
Both metrics provide valuable information, but they serve different purposes. It is critical to understand the methods of classifying and reporting COVID-19 data as well as their intended purpose, because these factors have major effects on what the data mean and how they are interpreted.
IMF GLOBAL STRATEGY The International Monetary Fund (IMF), in partnership with the Wellcome Trust, Coalition for Epidemic Preparedness Innovations (CEPI), and the Global Fund, this week warned that the pandemic is not over and published a working paper calling for a new strategy to manage the long-term risks of COVID-19, including the uncertainty surrounding how the pandemic will evolve. The groups urged the international community to recognize that pandemic financing and preparedness not only helps individual countries prepare for infectious disease crises but also addresses systemic threats to the global economy. According to IMF projections, the pandemic will result in a cumulative output loss of US$13.8 trillion through 2024 and will leave lasting economic impacts in many countries. Additionally, global economic recovery will continue to be constrained without more equitable access to prevention and treatment tools and the development and implementation of policies addressing the pandemic’s consequences.
The paper outlines 4 key policy implications of a long-term plan, including achieving equitable access to a comprehensive toolkit of treatment and prevention strategies such as diagnostics, vaccines, treatments, and healthcare system strengthening; monitoring viral evolution and responsively upgrading the toolkit; transitioning from an acute response to sustainable, balanced, and integrated health and social strategies that encompass COVID-19; and developing a cohesive risk-mitigation approach to future pandemic threats. To do this, the paper calls for US$15 billion in grants this year to fill the gap in the ACT Accelerator’s financing framework and US$10 billion annually moving forward to support pandemic preparedness and response (PPR) activities.
In related news, US Treasury Secretary Janet Yellen met with WHO Director-General Dr. Tedros Adhanom Ghebreyesus on April 5 to discuss ongoing COVID-19 pandemic responses and future efforts to strengthen global pandemic preparedness and financing. Secretary Yellen and Dr. Tedros agreed on the need to address these issues now, before global attention turns elsewhere. Secretary Yellen underscored the US commitment to working with the WHO, the World Bank, and G20 partners to develop a financial intermediary fund (FIF) on pandemic preparedness to be housed at the World Bank, and they agreed a FIF would serve as a vital component of the global architecture for pandemic preparedness. Additionally, Secretary Yellen and Dr. Tedros agreed on the importance of working toward the goal of vaccinating 70% of the world’s population this year, with Secretary Yellen emphasizing the US commitment to helping to achieve that goal. However, a compromise measure currently under consideration in the US Senate that would provide an additional US$10 billion for the COVID-19 response includes no additional funding for global vaccination efforts. Notably, the bill is stalled because of debate over immigration issues.
INFLAMMATORY RESPONSE Scientific evidence is mounting that SARS-CoV-2 infection can elicit massive inflammatory responses that contribute to severe COVID-19. In a study published April 6 in Nature, researchers describe how SARS-CoV-2 infection might cause these so-called cytokine storms, when the bloodstream is overrun with inflammatory proteins that then kill tissue and damage organs. The study demonstrates that SARS-CoV-2 can infect and replicate in certain types of white blood cells—macrophages in the lungs and monocytes in the blood—which, when infected, stimulate the release of inflammasomes, a type of molecule that triggers a rush of inflammatory responses. One of those responses is pyroptosis, a programmed cell death that leads infected cells to release even more inflammatory proteins and becomes a difficult process to treat. The study could help to explain why older adults or those with underlying health conditions such as obesity or diabetes are more vulnerable to severe COVID-19, as those people tend to already have some level of inflammation in the body.
The results support the findings of another paper posted recently on bioRxiv, which is not yet peer-reviewed, that also found SARS-CoV-2 can infect and replicate in macrophages found in human lung cells and in a mouse model of the human immune system. Those infected macrophages also triggered the release of inflammasomes and died by pyroptosis. Typically, the virus uses ACE2 receptors to enter cells and replicate. However, monocytes and macrophages lack ACE2 receptors, so SARS-CoV-2 uses another cell-surface protein, Fcγ receptors, to enter cells, but only with the help of antibodies already attached to the Fcγ receptors. Notably, the antibodies in people who had received the Pfizer-BioNTech mRNA vaccine did not assist the virus in entering monocytes and therefore prevented subsequent inflammatory responses. Although additional research is needed to understand which antibodies facilitate viral uptake by monocytes, the finding is reassuring and could help researchers identify targets for future treatments.
IVERMECTIN The antiparasitic drug ivermectin showed no significant benefit in preventing hospitalization or prolonged emergency department visits due to COVID-19, according to the results of a large clinical trial published last week in the New England Journal of Medicine (NEJM). The study included nearly 1,360 COVID-19 patients in Brazil who were randomly assigned to receive either ivermectin or placebo within a week of developing symptoms, with some patients receiving a relatively high dose of the drug. The researchers underscored that the overall number of events in their study is larger than the number of all combined events in previous meta-analyses that provided inconsistent results. Despite ivermectin’s continued popularity as an alternative treatment, most experts agree that these findings provide conclusive evidence that the drug offers no treatment benefit for people with COVID-19 and question the value of additional studies examining the drug as a COVID-19 therapy.
by ponchi101 It will make no difference with the crowd that believes that Ivermectin works. Plus, there is a big market for it, so the peddlers will continue the "wonder drug" promotion. And with every single young person that "recovers" by taking it, it will continue to be used massively.
by ti-amie
by ponchi101 Ran into an acquaintance today. He stayed away from the skiing area (where he worked) because he has mild emphysema from his years of smoking, but now that they dropped the mask mandate, he went back.
Proudly unvaccinated. His years in the military taught him "how to deal with these things".
Let's drop all mandates. Let nature takes its course. I really like the guy, but I really can't make sense of this.
by Deuce Human beings have been trying in many ways to eradicate their own species from the planet for many years.
They may have finally found a formula that will actually accomplish this.
by atlpam Also on the fence about another booster dose. Waiting to see if US drops the airline mask mandate in April. I will likely get dose 4 the end of April (6 months after dose 3) since we have air travel planned later in May.
by ti-amie
by ti-amie
by Deuce ^ Better late than never? ^
But it seems to me that the saying that "An ounce of prevention is worth a pound of cure" has been around for a long, long time - long before the pandemic began.
Prevent a mess, or clean up mess after mess?
It would seem that the intelligent choice is rather evident.
by dryrunguy Yeah... The U.S. seems to have mostly moved into "if we pretend it's not there, then it's not there" territory... We have all struggled with what's the right things to do in the biggest possible picture (e.g., public health vs. local/state/national/global economies). I doubt any of us have a good answer.
I would love to have a night where I could go out for dinner without fear--and not have to plan a meal and cook it. I took that basic privilege for granted for so long. But with this latest variant flying about locally, here I am, feeling sorry for myself, thinking about what I have to cook tomorrow night. Not what I COULD cook, or what I WANT to cook... But what I HAVE to cook.
I have a lot of moments where I say to myself, "Just go ahead, go out, do what you want, take your chances--all the data suggest you're not at risk for serious illness."
And then I'll be watching something on TV, with thousands upon thousands of people gathered in a fairly small space, and I scream, "YOU IDIOTS!!!"
by dryrunguy Here's the latest Situation Report. There's a lot here. I was particularly struck by the section on the discrepancy between documented COVID infections in Africa and the likely actual number of infections. And then there's the numbers from the northeastern U.S. I need some time to process that. And then there's new info about the Gridiron super-spreader event. I didn't realize it was THAT bad. But here we go again: "If we pretend it's not there, then it's not really there..." Sigh.
::
NEW OMICRON SUBVARIANTS The WHO is tracking cases of 2 new sublineages of the Omicron variant, adding BA.4 and BA.5 to the monitoring list alongside BA.1, BA1.1, BA.3, and the globally dominant BA.2. Dr. Tulio de Oliveira, Director of the Centre for Epidemic Response & Innovation (CERI) in South Africa, tweeted about the presence of BA.4 and BA.5 in South Africa, one of the first countries to identify the original Omicron variant in November 2021. The series of tweets said the sublineages have been found in samples from Botswana, Belgium, Germany, and the UK but not yet caused a rise in cases in South Africa. BA.4 and BA.5 have mutations on their spike proteins similar to BA.2, in addition to several other mutations. De Oliveira said that where the subvariants differ from each other is in amino acid mutations outside of the spike protein and work is underway to further characterize the 2 Omicron sublineages.
COVID-19 OUTBREAKS IN US Since the middle of March, the US has averaged between 25,000 and 30,000 new daily COVID-19 cases. But some health experts believe the country may be experiencing a new surge of cases, fueled by the Omicron BA.2 subvariant and masked by incomplete data from unreported at-home testing, a lack of testing among milder cases, and reduced access to testing centers. Numbers of new cases are beginning to rise in the northeast region of the country; of the 10 states with the highest 7-day case rates per 100,000 people, 7 are in the northeast. Average daily COVID-19 case numbers have increased approximately 53% in Rhode Island and 64% in both New Jersey and New York over the last 2 weeks. Other northeastern states experiencing increases in COVID-19 case loads include Connecticut, Maine, and Vermont. COVID-19 levels in wastewater have increased nationwide over the last 3 weeks, with the northeast showing the highest levels, according to Biobot Analytics. The Philadelphia Department of Public Health announced April 11 it will reinstate a citywide indoor mask mandate beginning April 18, including all public spaces such as schools, restaurants, government buildings, and other settings. The city’s number of new COVID-19 cases has increased 50% over the last 10 days, according to the department. Additionally, the federal government may extend the mask mandate for public transportation, which is set to expire April 18, according to White House Coronavirus Response Coordinator Dr. Ashish Jha.
Several recent outbreaks among high-profile politicians and celebrities could represent the tip of the iceberg in understanding ongoing SARS-CoV-2 transmission in the US. Health officials note that politicians and celebrities are tested more frequently than the average individual, and increases in cases among their ranks might signal that more people are becoming infected but experiencing mild or no symptoms. More than 70 high-profile people tested positive after an event known as the Gridiron Dinner in Washington, DC, including New York City Mayor Eric Adams, US Agriculture Secretary Tom Vilsak, US Attorney General Merrick Garland, US Commerce Secretary Gina Raimondo, several US lawmakers, and many others. Some of those who were infected are reportedly up-to-date on their vaccinations. Meanwhile, less than 10% of the US population feels that COVID-19 represents a serious crisis in the country, 17% say it is not a crisis at all, and 73% feel the pandemic is a manageable problem, according to an Axios-Ipsos poll. Notably, an average of 500 people in the US die daily from COVID-19.
VACCINATION IMPACTS In an update to a December 2021 report, the Commonwealth Fund released new estimates on the impact of US SARS-CoV-2 vaccination efforts to include the winter Omicron surge. The report estimates that 2.27 million COVID-19-related deaths were averted in the US between mid-December 2020, when vaccines first became available, and March 31, 2022, when the Omicron surge was over. Additionally, the report estimates that vaccinations prevented 17 million COVID-19-related hospitalizations, about 66 million infections, and saved approximately $900 billion in healthcare costs. The report highlights the ongoing impact of US vaccination efforts and encourages efforts to increase vaccine uptake, while recognizing that nearly 1 million people have died of COVID-19 in the US since the start of the pandemic. In a statement, the White House said the report underscores the success of the nation’s historic vaccination effort and called on the US Congress to urgently authorize additional funding for the COVID-19 response. Lawmakers last week negotiated a US$10 billion COVID-19 spending deal, with no additional money for global vaccination efforts. However, debate over immigration policies delayed a vote on the legislation until after the US Senate returns from its spring recess at the end of the month.
US STATE DEPARTMENT CHINA TRAVEL ADVISORY The US Department of State on April 11 ordered all non-essential personnel and their family members in Shanghai, China, to leave and issued an advisory for US citizens to reconsider travel to China due to surges in COVID-19 cases. The State Department also cited the “arbitrary enforcement of local laws and COVID-19-related restrictions,” including the separation of children from parents, as reasons for the order and advisory. Many of Shanghai’s 26 million residents have been under strict lockdown, some for up to 3 weeks, as the nation continues to enforce its “zero COVID” strategy amid its worst COVID-19 outbreak since the beginning of the pandemic. Some residents have described being unable to obtain sufficient food, water, and other essentials while confined to their homes. Mass isolation facilities are reportedly overcrowded and unsanitary. In a shocking incident, a health worker beat a pet dog to death in the street as it was chasing a bus carrying its owner to an isolation facility.
The State Department’s orders elevated diplomatic tensions, with the Chinese government expressing “strong dissatisfaction and firm opposition to the US side's groundless accusations about China's epidemic control policy” in a Foreign Ministry statement. Additionally, the situation in Shanghai is raising fears nationwide that similar stringent measures will be imposed in other regions as COVID-19 cases rise. The WHO said it is closely monitoring the situation in China, which reported a record 27,595 new COVID-19 cases in 31 provincial-level regions on April 10.
US FEDERAL EMPLOYEE VACCINE MANDATE A panel of the US Court of Appeals for the 5th Circuit last week lifted a nationwide injunction of US President Joe Biden’s requirement that all federal government employees be vaccinated against COVID-19. In the 2-1 ruling, Judges Carl Stewart and James Dennis said the US District Court judge who originally issued the injunction did not have jurisdiction in the case, noting the plaintiffs should have raised their grievance through the Civil Service Reform Act (CSRA), not in the court system. On April 11, the US Department of Justice formally asked the appeals court to immediately issue its order to allow the ruling to take effect and enable federal agencies to once again enforce the executive order. Notably, in its last accounting, the White House said 96.5% of federal employees had at least 1 dose of vaccine or are seeking religious or medical exemption from the requirement.
US LIFE EXPECTANCY The estimated US life expectancy dropped for a second year in a row in 2021, falling by just under a half a year to 76.6 years, the lowest in at least 25 years, according to a new analysis. The report, posted to medRxiv and not yet peer-reviewed, shows that US life expectancy decreased from 78.86 years in 2019 to 76.99 years in 2020, falling another 0.4 years in 2021. In the 10 years prior to the pandemic, life expectancy changed by an average of less than 0.1 year annually, according to US CDC data. The findings reflect the toll of the COVID-19 pandemic, with the disease causing more US deaths in 2021 than in 2020. As more people became vaccinated in 2021, many other high-income countries began to see life expectancies rebound, and the researchers expected to find a similar trend in the US. However, that was not the case. For comparison, they examined data from 19 peer countries, which averaged a life expectancy decrease of 0.4 years between 2019 and 2020 and an increase of 0.28 years between 2020 and 2021, with a net loss of only 0.3 years—versus 2.26 years in the US—over the 2-year period.
US Black and Hispanic populations experienced the largest declines in life expectancy between 2019 and 2021, with the researchers blaming the country’s history of structural racism in healthcare and other inadequacies in how the country handled the pandemic for the discrepancies. Notably, the drop in US life expectancy in 2021 was driven primarily by an increase in deaths among the white population, according to the analysis, which said multiple factors—including slow vaccine uptake and the Delta variant surge—helped to fuel an increase in mortality. As more people gain some immunity to SARS-CoV-2, either through vaccination or natural infection, US life expectancy should rise again in the coming years, unless a more virulent variant emerges or another pandemic disease arises. However, a recent report from the Peterson-KFF Health System Tracker shows an ominous start to the current year. In January, COVID-19 was the leading cause of death for people between the ages of 45 and 84, and in February, COVID-19 killed as many people as the typical number of deaths from heart disease, according to the report.
EARLY REINFECTION A report published April 8 in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) describes 10 individuals who were reinfected with the Omicron variant of SARS-CoV-2 within 90 days of initial infection with the Delta variant. The report represents a significant finding, as reinfection within 90 days of infection is not well understood. Early reports of reinfection were difficult to verify because a positive reading on a nucleic acid amplification test (NAAT) could signal prolonged viral shedding from the initial infection rather than a new infection if taken within 3 months of acute infection. For the report, researchers conducted whole genome sequencing on 10 individuals—8 children and 2 adults—to determine which variant caused the initial and subsequent infections. Only 1 of the patients had received a 2-dose primary vaccine regimen, 2 had received 1 dose, and 7 were unvaccinated. Of 8 patients with available data on symptoms, 6 experienced symptoms during both infections. The authors noted that the patients may have been at increased risk for infection due to lack of vaccination and the high likelihood of exposure to SARS-CoV-2 in schools and the work and living settings of the adults.
The CDC’s report comes at a time when health officials in Canada are warning residents about the possibility of reinfection with Omicron. Experts say global data continue to support evidence that reinfection is becoming more common but symptoms during reinfection often are not worse than the initial infection. The Omicron variant has proven adept at evading immunity from natural infection and infecting individuals with 2-3 doses of mRNA-based vaccines, dashing any last hopes of herd immunity. However, vaccination remains highly protective against severe consequences of COVID-19, including hospitalization and death, and being up-to-date on vaccinations remains the best way to protect against severe COVID-19 outcomes.
COVID-19 ESTIMATES IN AFRICA A new meta-analysis of standardized seroprevalence studies indicates that the true number of SARS-CoV-2 infections across Africa may be 97 times higher than the number of reported confirmed cases. The study—led by the WHO Solidarity Response Fund and the German Federal Ministry of Health COVID-19 Research and Development and posted to the preprint server medRxiv—evaluated more than 150 seroprevalence studies from January 2020 to December 2021 and suggests that more than two-thirds of the African population have been infected with SARS-CoV-2. From Q2 2020 to Q3 2021, seroprevalence increased markedly from 3% to 61.5%. According to the study, which is undergoing peer review, rather than the reported 8.2 million cumulative cases in September 2021, there were actually more than 800 million infections. The study also determined that seroprevalence was higher in urban areas than rural areas, with varied seroprevalence among African sub-regions, where Middle, Western, and Eastern Africa exhibited higher seroprevalence.
WHO Regional Director for Africa Dr. Matshidiso Moeti noted in the press conference that testing strategy and capacity is a significant factor in the discrepancy between reported cases and the estimated true number of infections. Testing across the continent has largely focused on symptomatic people, particularly where there were supply constraints, resulting in an undercount of exposures and infections. Dr. Moeti highlighted the need for sustained routine testing and surveillance capacity on the continent in order to identify cases among the estimated 67% of people with COVID-19 in Africa who are asymptomatic and monitor for emerging variants.
BREAK COVID NOW SUMMIT An international donor conference last week secured US$4.8 billion in pledges for the Gavi COVAX Advance Market Commitment (AMC), the mechanism supporting the global vaccine-sharing initiative that delivers doses to lower-income countries. While reaffirming the international community’s support for COVAX, the 2022 Break COVID Now Summit—hosted by Gavi, the Vaccine Alliance in partnership with the governments of Germany, Ghana, Indonesia, and Senegal—fell short of its previously stated need of US$5.2 billion. Of the total commitments, innovative financing mechanisms, including the European Investment Bank (EIB) and the US Development Finance Corporation (DFC), pledged US$2.1 billion; individual nations committed US$1.7 billion; and 3 multinational development banks, including the World Bank, Asian Development Bank (ADB), and EIB, promised US$1 billion. The funds will allow COVAX to continue shipping and supporting the delivery and administration of SARS-CoV-2 vaccines in lower-income countries, as well as launch the new Pandemic Vaccine Pool to help ensure equitable access to updated SARS-CoV-2 vaccines in the future. In opening remarks, UN Secretary-General António Guterres excoriated the unequal distribution of vaccines, saying one-third of the global population has yet to receive a single dose creating ideal conditions for the emergence of new variants, more deaths, and further social and economic impacts.
by ti-amie
The Philadelphia Department of Public Health announced April 11 it will reinstate a citywide indoor mask mandate beginning April 18, including all public spaces such as schools, restaurants, government buildings, and other settings. The city’s number of new COVID-19 cases has increased 50% over the last 10 days, according to the department.
Thank you again for posting this Dry.
by ponchi101 I find the news about Africa to be a bit of a 'non-news'. It was well expected that the testing in the continent was really not enough.
Other than that, I keep saying it: this thing has defeated us, and now we can only keep "living with it". As terrible as that is.
(And I don't mean don't do anything. Tomorrow I return to Colombia and I plan to, and have to, wear my mask all the way. I will see if I am lucky and do not catch the bloody thing on the way home).
by Deuce Do you at times not take precautions to protect yourself from COVID-19?
Do you figure that it’s OK if you get COVID-19, because it will have a minimal effect on you and you’ll easily recover?
Have you become complacent about COVID-19 in recent months, viewing it as being benign in the long term?
Read this article.
This is why I take precautions to not contract the virus...
by Deuce I just read this article about why the U.S. has far more COVID cases, ICU admissions, and deaths than Canada does (per capita).
It's from a couple of months ago - but it's definitely still an interesting read.
Before you begin planning your move to Canada, though, consider that we may be catching up to the U.S., as politics has sadly won out here, as well, with almost all of the protective measures having been lifted in provinces here over the past month or so. To no intelligent person's surprise, case counts, hospitalisations, ICU admissions, and Deaths began to rise as a direct result of the lifting of protective measures.
People in general are not intelligent enough to protect themselves, and are not caring enough to protect others - not surprisingly, they need to be mandated to do these things - otherwise, it simply doesn't happen.
We had something that was obviously working well... but the politicians decided to be self-serving and eliminate the things which were working well.
by dryrunguy I ate in a restaurant for the first time is over 2 years. It was lunch on Thursday at about 2 in the afternoon. I figured the restaurant would be close to empty--and it was.
Progress.
But it will still be a while before I am brave enough to try dinner out on a Friday or Saturday night.
by ponchi101 The ambivalence is:
We have tried everything. The long lockdowns, wearing masks that are reported to work or not, depending on who you read, vaccines that will not stop you from getting the disease but will prevent severe symptoms and death. In the meantime, the virus has mutated into several strands, each more contagious but less deadly, and many, many people have suffered disastrous financial consequences due to this pandemic.
So. The question remains the same. Do we stop doing what we have been doing, because it has not been working, or do we keep going on with it, hoping that this virus will eventually be defeated?
I say this thing is here to stay. People with co-morbidities will suffer the worst lot, but the rest of the world has to accept this as a new, more virulent flu that will mow down a fixed number of people a year.
I still will wear my mask and get my vaccines.
by dryrunguy I don't know, ponchi. I'd argue that I have consistently made good decisions for myself and for this household. I've done all of the things I am supposed to do. And so far, knock on wood, I haven't caught it. I call that a victory.
Yes, I have denied myself a lot. I have avoided many things I REALLY want to do or places I REALLY want to go. But is that such an enormous sacrifice? I don't think so. I have become a better cook, and I have learned that I am not necessarily entitled to recreation or amusement. We live in a society where we are expected to go out, do things, attend events, spend money... Commercial, commercial, commercial.
I do miss the human interaction, though. Face to face human interaction. Hugs. A kiss on the cheek. But there are also other ways to show our friends and loved ones that we care about them.
The bottom line remains the same as it has been throughout this entire pandemic. I can make all the right decisions until I'm blue in the face.
But I have ZERO control over the decisions others make. Hence my trepidation about sitting at a table in a packed restaurant or being in packed public spaces when I have ZERO control over who is at the next table, who is standing next to me, or who is coughing in the seat behind me--and the decisions they have made.
by ponchi101 We are not in that much disagreement. I have also avoided getting the virus (despite a full week in a household with three people that had tested positive) by not going out much, and spending a lot of time at home with my girl. But part of that has also been due to the verifiably sickening reality that I simply can't find a job, either here of abroad, and therefore there really is no reason for me to go out.
I really don't know how many people have been in this position, in which not going out and forsaking human interaction has been "easy" since we have been not needed.
I also don't know how to handle this anymore. I just came back from the USA so my GF and I are in some sort of quarantine. We did spend, after all, 14 hours in planes and airports, of which two were American airports where NO checking of vaccination was done (we had to show vaccination records to come back here, but that was only the last leg). And indeed, we were in places with people with no masks whatsoever, and as I said above, ran into one friend that openly said he was not vaccinated because he was not going to "let them put their (expletive) into me".
My point is the same as I wrote in May 2020. This thing has defeated us. We can't beat it with 100 million Americans refusing to get vaccinated and the virus mutating rapidly. So most of us will remain taking precautions but there are enough that won't. The virus will pool there and continue.
We have said it above. I don't know what else to do. To me, this is not 2022. This is 2020, season 3.
by Suliso Interesting observation. In Switzerland maybe 20% of people still wear masks, some even outdoors. Here in the Netherlands absolutely no one. Literally in three days I'm yet to see a single person doing that.
We personally have decided to ignore the virus since few months ago. We've been three times vaccinated and enough is enough. I go to work anyway.
By the way Amsterdam yesterday was incredibly crowded. More so than I remember NYC from before.
---0---
@Suliso. That is where my dilemma comes from. Here in Bogota, masks are still mandated, and I don't mind. But the entire city is open, and there are no more restrictions. I am not sure if restaurants and public spaces are requiring proof of vaccination (I have mine in my back pack, anyway) but if not, then it is everybody on their own. So by now, if we are going to make individual choices, sure, get your vaccine and carry on.
Until you think about the population that cannot be vaccinated.
It is still confusing to me, at least a little bit.
by Suliso I think some of what we're doing still in certain countries (for example Germany) is more like a safety theatre akin to removing your shoes at airport security check. Whom exactly is showing covid certificate at a restaurant helping? Same with masks in the same restaurant - use it to go in for 2 min and then take off for an hour long dinner... I could see some point in public transport still for a while.
by Deuce
Suliso wrote: ↑Mon Apr 18, 2022 4:18 pm
I think some of what we're doing still in certain countries (for example Germany) is more like a safety theatre akin to removing your shoes at airport security check. Whom exactly is showing covid certificate at a restaurant helping? Same with masks in the same restaurant - use it to go in for 2 min and then take off for an hour long dinner... I could see some point in public transport still for a while.
I will preface my response by stating that I am not at all a rules person. I believe much more in personal freedom than in rules, and have lived my life thus. That said, I also believe that rules are sometimes necessary to protect people from themselves and from others.
What you refer to as ‘safety theatre’ is more than that. While you are correct in saying that wearing a mask to enter a restaurant, and then removing it for your entire stay at the restaurant is rather silly, I still believe that having such ‘rules’ does good overall - because when we remove these mandates, it gives the very loud and obvious message to the populace that this situation (COVID-19) is ‘under control’, and/or that it’s ‘not that serious’.
And this is precisely what has absolutely been happening for the past month or so - most protective measures have been lifted, and the general public has very much interpreted this as a message that everything is OK now, and that everyone has ‘carte blanche’ to do whatever they wish because things are back to normal. The (predictable) result is that positive COVID cases are rising, hospitalisations are rising, ICU admissions are rising, and deaths are rising.
Meanwhile, the medical experts are going nuts saying “NO! NO! This is crazy! COVID-19 is still very much with us, and is still very dangerous to us all, and we need to protect ourselves and each other.” I see everywhere that medical and infectious disease experts are contradicting governments these days. The science, obviously, is on the side of medical experts, while the only thing on the side of the politicians is their old and trusted ally - utter self-serving selfishness.
You ask who showing a vaccine certificate (‘vaccine passport’) at a restaurant is helping.
If everyone in a restaurant or other indoor setting is vaccinated, it then constitutes a safer environment than does a setting of unvaccinated people. Again, this is the science speaking. This is because vaccinated people are A) less likely to contract COVID-19, and B) if they do contract COVID-19, vaccinated people are less symptomatic, and therefore shed less viral load, and therefore are less likely to transmit the virus to others.
Also, ensuring that people must show a ‘vaccine passport’ encourages people to get vaccinated. This then decreases the likelihood of virus transmission, and is therefore an overall positive element for everyone. For the small ‘price’ of getting vaccinated, I, as well as the huge majority of medical professionals and infectious disease specialists, feel this is a good thing.
Not surprisingly, individual people, as well as governments, have viewed the COVID situation from an increasingly selfish perspective as time has gone on. This does not bode well for any society in an overall sense. Allowing people to decide for themselves whether or not to wear masks, for example, results in selfish behaviour - i.e. ‘I don’t want to wear a mask, so I won’t’. Lost in this is the scientific fact that wearing a mask protects others from you at least as much as it protects you from others. Therefore, the decision to not wear a mask is a very selfish one which completely discounts the rights of others to not be harmed by you.
If it were merely that those who choose to not wear a mask were exposing only themselves to the potential for harm, then I’d say ‘Fine - it’s your choice’. But we’re all in this together - and that is being lost in this new selfish approach.
by ti-amie
by mmmm8
Suliso wrote: ↑Mon Apr 18, 2022 4:18 pm
I think some of what we're doing still in certain countries (for example Germany) is more like a safety theatre akin to removing your shoes at airport security check. Whom exactly is showing covid certificate at a restaurant helping? Same with masks in the same restaurant - use it to go in for 2 min and then take off for an hour long dinner... I could see some point in public transport still for a while.
I think requiring vaccination for restaurants is considerably different from masks in restaurants. Knowing everyone else in an indoor place is vaccinated confirms a reduced risk of me getting infected. The requirement is lifted here in NY and domestic tourists are back and I don't feel great about it. For a few weeks after Omicron and before the mandate was lifted, I did feel safe (at this point, I'm dining indoors even with the increased risk - it's still too cold for outdoors and my colleagues no longer care, so no one is making me but peer pressure).
It must be noted that the judge who ruled to end the mask mandate on airplanes is a Trump appointed judge in Florida. So this kind of idiocy is pretty much obligatory.
Here in Canada, our medical science experts are saying that this decision is insane.
Any system which allows a single solitary judge like this to make such a hugely important decision, AND HAVE IT STAND, is an extremely defective system.
On Judge Kathryn Kimball Mizelle: "While Mizelle has not been in her position for long, she's found herself at the center of controversy before: During her Senate confirmation process, the American Bar Association (ABA) said she was not qualified for the position because she had not been practicing law for long enough."
"The Leadership Conference of Civil and Human Rights specifically opposed Mizelle's confirmation because of her lack of legal experience, as well as her involvement in civil rights cases in the Trump Justice Department and what it called her "extreme right-wing ideology.""
mmmm8 wrote: ↑Tue Apr 19, 2022 9:42 pm
I think requiring vaccination for restaurants is considerably different from masks in restaurants. Knowing everyone else in an indoor place is vaccinated confirms a reduced risk of me getting infected.
But does it really? It seems to me that this new variant infects equally well vaccinated and unvaccinated the only difference being that unvaccinated risk a worse outcome. Encouraging vaccination would be a more sound argument except that those who haven't still are hard antivaxers. Nothing could convince them...
mmmm8 wrote: ↑Tue Apr 19, 2022 9:42 pm
I think requiring vaccination for restaurants is considerably different from masks in restaurants. Knowing everyone else in an indoor place is vaccinated confirms a reduced risk of me getting infected.
But does it really? It seems to me that this new variant infects equally well vaccinated and unvaccinated the only difference being that unvaccinated risk a worse outcome. Encouraging vaccination would be a more sound argument except that those who haven't still are hard antivaxers. Nothing could convince them...
I wonder where you derive your information that Omicron (or its derivatives) "infects equally well vaccinated and unvaccinated".
No. While ‘breakthrough’ infections among the vaccinated are more likely with Omicron than they were with Delta, these ‘breakthrough’ Omicron infections among the vaccinated are still much more rare per capita than are Omicron infections among the unvaccinated. “The agency defines a breakthrough COVID-19 infection as “a small percentage of fully vaccinated persons” who “will still get COVID-19 if they are exposed to the virus that causes it.”
Does requiring proof of vaccination in restaurants, etc. provide a 100% guarantee that no-one in the restaurant, or cinema, etc. will be infected with COVID-19?
No.
Does NOT requiring proof of vaccination in those locations increase the chances that some people in those locations will be infected with COVID-19 when compared with requiring proof of vaccination?
Yes.
Also... unvaccinated people in general are more likely than vaccinated people are to be reckless and go to restaurants and other indoor locations even if they are symptomatic to some degree. Because a significant degree of unvaccinated people do not believe that COVID-19 is a serious matter.
As well... requiring people to show proof of vaccination prior to accessing events, establishments, etc. has proven to boost the number of people opting to get vaccinated. While it is true that some unvaccinated people will never get vaccinated, if requiring proof of vaccination to access certain locations convinces even as little as 5% of the unvaccinated to get vaccinated, it is worth it (and it’s likely considerably more than 5%).
by Togtdyalttai I had the good fortune to be flying home yesterday (from Baltimore to San Diego). I'd say there were still a majority of people wearing masks in both airports, but not a healthy majority.
by ti-amie
by ti-amie
by Deuce At this point, I wonder if there's even a mandatory age requirement to be a federal judge in the U.S.
I'd trust a 10 year old child's perspectives and opinions far more than I'd trust any judge who was appointed by the Trump 'administration'.
How can this possibly happen in a civilized country?
by dryrunguy Here's the latest Situation Report. My apologies. I believe I forgot to post the one from Friday.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 504 million cumulative cases and 6.2 million deaths worldwide as of April 20. As expected, the number of cumulative cases surpassed 500 million on April 14.
The global weekly incidence decreased for the fourth consecutive week, down 22% from the previous week. Most regions reported decreasing trends in weekly incidence last week, except for Africa, which remained relatively stable from the previous week (+0.23%). The trend in reported global weekly mortality decreased for a third consecutive week, down 19% from the previous week.
Global Vaccination
As of April 18, WHO reported 11.3 billion cumulative vaccine doses administered globally, with 5.1 billion individuals receiving at least 1 dose, and 4.58 billion fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline, down from nearly 40 million doses per day in late December 2021 to 10.7 million on April 20, a decrease of 70% over that period.* The trend continues to closely follow that in Asia. Our World in Data estimates that there are 5.12 billion vaccinated individuals worldwide (1+ dose; 65% of the global population) and 4.63 billion who are fully vaccinated (58.76% of the global population). A total of 1.77 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is currently reporting 80.6 million cumulative cases of COVID-19 and 987,034 deaths. The average 7-day daily incidence was 40,985 on April 19, an increase of nearly 40% since a recent low of 24,845 on March 29. Average daily mortality appears to have declined over the past week, with a 7-day average of 385 on April 19, down slightly from 459 on April 12, the date of our last report.* Notably, the 7-day moving average number of new hospital admissions of people with confirmed COVID-19 continues to trend upwards, up 7.2% over the prior 7-day average, for the week ending April 18, reflecting the increasing trend in incidence.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 570.5 million cumulative doses of SARS-CoV-2 vaccines. Daily vaccinations have mostly leveled off over the past 2 weeks, with a slight increase from 455,258 on April 6 to 459,655 on April 14. A total of 256.9 million individuals have received at least 1 vaccine dose, which corresponds to 77.4% of the entire US population. Among adults, 88.8% have received at least 1 dose, as well as 27.6 million children under the age of 18. A total of 219 million individuals are fully vaccinated**, which corresponds to 66% of the total population. Approximately 75.9% of adults are fully vaccinated, as well as 23 million children under the age of 18. A total of 99.7 million individuals have received an additional or booster dose. This corresponds to 45.5% of fully vaccinated individuals, including 68.1% of fully vaccinated adults aged 65 years or older. Only about 50% of those eligible for a first booster dose have received one.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent several days.
**Full original course of the vaccine, not including additional or booster doses.
US TRAVEL MASK MANDATE The US Department of Justice has filed an appeal seeking to reverse an April 18 ruling by a federal District Court judge in Florida that voided a national mask mandate for mass transit. The federal judge ruled that the US CDC’s mask mandate exceeded the agency’s statutory authority, immediately ending the requirement put in place to reduce the risk of SARS-CoV-2 among travelers on public transportation and in transit stations. The ruling left decisions to enforce mask wearing up to individual transportation companies and transit authorities. Following the ruling, the Transportation Security Administration (TSA) said it will not enforce its mask mandate in transportation settings, as it awaits future court proceedings. Additionally, most major domestic airlines rescinded their mask requirements, as did Amtrak, rideshare companies Uber and Lyft, and several major transit authorities. The White House called the ruling “disappointing,” especially as the number of new COVID-19 cases in the US begin to rise again. Reactions were more mixed among the public and transportation employees, with some flight attendants gleefully announcing mid-flight that passengers could remove their masks. Other airline employees, TSA agents, and members of the public reacted with confusion and concern, especially for those who are ineligible for vaccination or at higher risk of severe disease.
As such, the CDC issued a statement calling the mandate “necessary for the public health,” prompting the Department of Justice to appeal the case to the US Court of Appeals for the 11th Circuit. However, federal officials are uncertain how the appeal will be received in this court given its conservative lean. Additionally, some legal experts expressed concern that if the lower court ruling stands, the precedent could severely handicap CDC’s ability to exercise its mandate to protect public health in the future. In the meantime, US residents will face a patchwork of policies that may or may not be enforced by employers, state or local governments, or private businesses. Nevertheless, the science behind mask-wearing as a means of lowering the risk of SARS-CoV-2 transmission in indoor public spaces remains solid, and people who wear high-quality masks can still protect themselves even if others are not masked.
OMICRON SUBLINEAGES Scientists around the world have been closely monitoring SARS-CoV-2 variants and their relative dominance to better inform response activities. In the US, the original Omicron variant has been displaced by its sublineage BA.2, but now, BA.2 may be competing with BA.2.12.1, its own sublineage. The US CDC estimates that BA.2 makes up 75% of current COVID-19 cases in the US, while BA.2.12.1 makes up 19% of COVID-19 cases. The remaining 6% are attributable to BA.1.1 and B.1.1.529, which have been waning. Initial signs point to Omicron descendent lineages not substantially differing from the original variant in terms of virulence or evasion of immunity. That evidence, relatively higher population immunity for the moment, and warmer weather indicate that there is not a need for panic regarding BA.2.12.1. However, caution and vigilance are warranted. The New York State Department of Health notes that BA.2.12.1, along with another new sublineage, BA.2.12, have contributed to a recent spike in cases in the state’s northern region, estimating the new sublineages have a 23-27% growth advantage over BA.2.
CDC ADVISORY PANEL ON BOOSTERS Since the US FDA authorized fourth doses, or second boosters, of the Pfizer-BioNTech and Moderna mRNA SARS-CoV-2 vaccines last month for people 50 and older and additional doses for immunocompromised people 12 and older, there has been widespread confusion among some healthcare providers and eligible individuals about when to get the shots and why. Public health officials maintain that continuous vaccination is only a stopgap measure aimed at lowering the risk of hospitalization and death among vulnerable populations, as they work to develop future vaccination strategies. On April 20, the US CDC’s Advisory Committee on Immunization Practices (ACIP) met to consider exactly who might benefit most from additional doses and what the ongoing vaccination strategy will entail, although there were no votes taken on any topics of discussion.
A CDC researcher told the panel that based on current data, individuals who are immunocompromised, live with an immunocompromised person, and those who are at increased risk of severe COVID-19 should consider getting a second booster now, while healthy older adults and those who have had COVID-19 within the past 90 days can wait until later in the year to get an additional shot. The panel also reviewed data showing that incidence of vaccine-associated myocarditis and pericarditis is lower after fourth doses than after the primary 2-dose series; there is no evidence boosters lead to immune tolerance that could cause lower antibody levels; and there is no evidence of immunological imprinting, with patients showing responses to several variants after a booster dose. Several of the panel members encouraged clear communication of a shared vision regarding vaccines, their effectiveness, and their purpose to help prevent “booster fatigue” and reduced public confidence in the vaccines. Others expressed the need for future vaccine strategies to be tailored to different populations, such as providing antibody tests prior to booster administration.
Additionally, the panel discussed the importance of future SARS-CoV-2 vaccines, including different formulations and platforms. Several companies, including Pfizer-BioNTech and Moderna, are developing variant-specific vaccines, but it is unclear how long testing and manufacturing of any newer vaccine versions might take. Moderna this week released preprint data on a bivalent vaccine candidate, mRNA-1273.211, that contains equal mRNA amounts of spike proteins from the ancestral SARS-CoV-2 strain and the Beta variant and could be used as a booster dose. According to the data—which is not yet peer-reviewed—the vaccine produced stronger, longer-lasting antibody responses against SARS-CoV-2 variants, including Omicron, than the company’s original vaccine. Results from a different Moderna bivalent vaccine candidate that uses mRNA from the original virus and Omicron are expected later this spring. Additionally, Moderna announced it plans to submit a request for Emergency Use Authorization (EUA) of its SARS-CoV-2 vaccine among young children ages 6 months to 5 years by the end of this month.
OMICRON IN CHILDREN A report published April 19 in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) highlights both the importance of SARS-CoV-2 vaccination among children to provide protection against the Omicron variant, as well as racial disparities regarding vaccination coverage and hospitalization during the Omicron surge. Researchers analyzed data from the COVID-19-Associated Hospitalization Surveillance Network to describe characteristics of 1,475 hospitalized children aged 5-11 years, focusing on Omicron predominance from December 19, 2021, to February 28, 2022. Among 397 children hospitalized during Omicron predominance, 87% were unvaccinated, with the cumulative hospitalization rate of unvaccinated children (19.1 per 100,000) over twice as high as that of vaccinated children (9.2 per 100,000). Severe disease was more common among children with diabetes and obesity, although 30% of hospitalized children with COVID-19 had no underlying medical conditions.
The most concerning finding showed that non-Hispanic Black children made up 34% of unvaccinated children and one-third of COVID-19 hospitalizations overall, making it clear that racial disparities of the pandemic extend to children. An analysis published earlier this month by the Kaiser Family Foundation also found that Black children were less likely to be vaccinated than White children in 5 out of 7 states that report vaccination status by race/ethnicity for children aged 5-11 years.
SARS-COV-2 BREATH TEST The US FDA on April 14 issued an Emergency Use Authorization (EUA) for the first COVID-19 diagnostic test that analyzes breath to detect chemical compounds associated with SARS-CoV-2 infection. The InspectIR Covid-19 Breathalyzer is a moderately sized instrument, about the dimension of a piece of carry-on luggage, and must be operated by a qualified and trained worker in a medical office, hospital, or mobile testing site. Test results are returned within about 3 minutes, but positive results should be confirmed with a molecular test. While the breath-based test represents an innovative, noninvasive diagnostic method, restrictions on who can conduct the test, where it can be conducted, and how many samples it can analyze per hour, as well as unknown pricing and a 10-12 week wait for the first devices to come to market, could limit the test’s real-world applications.
GLOBAL COVID-19 SUMMIT The US will co-host a second Global COVID-19 Summit on May 12 to discuss coordination and funding for global vaccination efforts, work to end the emergency phase of the pandemic, and preparedness for future health threats. The US will co-host the virtual summit with Belize, as CARICOM Chair; Germany, holding the G7 Presidency; Indonesia, holding the G20 Presidency; and Senegal as African Union Chair. The first summit was led by the US in September 2021, and this second meeting was originally scheduled for March but was postponed due to Russia’s invasion of Ukraine. Notably, the US might not be able to offer additional support for global vaccination initiatives because the US Congress has not renewed funding for those programs. Without the incentive of more funds for global efforts, the US might face difficulty obtaining further financial commitments from other countries, non-profit organizations, philanthropists, and the private sector.
US EARLY WARNING SYSTEM The US this week launched the Center for Forecasting and Outbreak Analytics (CFA), a US CDC-run initiative its leaders are likening to a National Weather Service for infectious diseases. (Dr. Caitlin Rivers from the Center for Health Security is currently helping lead this new Center at CDC.) With about 100 scientists, CFA will analyze technical data and communicate—in easy-to-understand language—evidence-based policies and strategies for COVID-19 or future infectious disease outbreaks to decisionmakers and the public. The center will work with experts within the government, academia, and the private sector to examine data on new cases, hospitalizations, who is most affected, how transmission is occurring and among whom, and which public health prevention and mitigation strategies work best to reduce transmission. These analyses should help decisionmakers adopt policies that are the most effective and least disruptive. Notably, CFA also is focused heavily on communicating information to the public, particularly vulnerable and historically underserved communities, to help them understand risk and make decisions based on scientific understanding. CFA begins with US$200 million in coronavirus relief funding but will need additional technical and financial support from inside and outside of the federal government as the nation moves beyond the emergency phase of the COVID-19 pandemic.
by ponchi101 Infections can go undetected if people do not get tested enough. But deaths can't go undetected, so I gather that the drop in deaths down to a bit below 400 can be seen as "good news".
Maybe the new variants are really not as deadly as the first ones.
by Deuce It's amazing to me that there are many people who don't realize this, as it seems incredibly obvious...
When vaccinated and unvaccinated people mix together in an indoor setting (like restaurants, movie theatres, sporting events, etc.), the vaccinated help to protect the unvaccinated - as a sort of 'buffer' -, while the unvaccinated pose a threat to the vaccinated.
This is why 'vaccine passports' - restricting access to indoor locations to only people who have proof of vaccination - is a very good thing.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
PAXLOVID The administration of US President Joe Biden this week announced plans to increase awareness and availability of the antiviral treatment Paxlovid (nirmatrelvir and ritonavir), which can reduce the risk of COVID-19-associated hospitalization and death by nearly 90% if taken within the first 5 days of symptom onset. The administration has purchased 20 million doses of the treatment from Pfizer, creating a sufficient stockpile, and will work with the manufacturer to speed delivery of the drug to pharmacies nationwide. Additionally, the White House plans to educate providers and the public about the drug’s availability and effectiveness, part of its effort to expand the federal Test-to-Treat initiative. Currently, about 2,200 pharmacies, long-term care facilities, and community health centers are operating as test-to-treat sites.
Demand for Paxlovid has increased in recent weeks, but many patients have reported difficulty obtaining the pills and physicians have been hesitant to prescribe it for fear of depleting once limited supplies and a lack of clarity on who can and cannot receive the treatment. The US CDC on April 25 issued a health advisory updating healthcare providers about the availability and use of COVID-19 therapies, as well as advising against unproven treatments, including antibiotics. Paxlovid, along with Merck’s molnupiravir, currently are available in about 20,000 locations nationwide, and the Biden administration hopes to double that number in the coming weeks, as well as allow some pharmacies to order oral antiviral treatments directly from the federal government at no cost. Some experts expressed concern that individuals who are more vulnerable to COVID-19 because they lack access to quality health care, have underlying health conditions, or live in rural areas, including many people of color, do not know Paxlovid is a treatment option or cannot travel to obtain the drug, worsening inequities. However, raising awareness, ensuring access, and securing more and better treatments requires additional funding from the US Congress, the White House noted in a fact sheet.
The Biden administration’s announcement comes days after the WHO announced it strongly recommends Paxlovid for the treatment of mild-to-moderate COVID-19 in individuals at the highest risk of hospital admission. The WHO’s living guidelines for COVID-19 treatment were updated on April 22, calling Paxlovid “the best therapeutic choice for high-risk patients to date.” Notably, the WHO outlined several challenges to accessibility, particularly in low- and middle-income countries (LMICs). The agency said questions about availability, lack of price transparency in bilateral sales made by Pfizer, and the need for quick and accurate testing before administering the drug will limit its use in LMICs. Under a deal between Pfizer and the Medicines Patent Pool (MPP), several generic manufacturers are licensed to produce Paxlovid to supply about 95 countries, but few companies have begun making the treatment and some need time to comply with international standards to be able to export the pills. Pfizer currently is facing criticism for resisting efforts by the Dominican Republic to issue a compulsory license for Paxlovid, with advocates saying the company claimed its intellectual property is a human right that would be violated if a compulsory license were issued. In a press release announcing the updated treatment guidelines, the WHO expressed concern that poorer nations will once again be “pushed to the end of the queue,” as happened with SARS-CoV-2 vaccines.
REMDESIVIR FOR UNDER-12 CHILDREN The US FDA on April 25 expanded the approval of the COVID-19 antiviral treatment remdesivir to include children as young as 28 days and older who weigh at least 6.6 pounds and who are hospitalized with COVID-19 or not hospitalized but at high risk of progression to severe disease. The treatment, which is made by Gilead Sciences and sold under the brand name Veklury, was already available for this pediatric population under Emergency Use Authorization (EUA), but the approval makes remdesivir the first approved COVID-19 treatment for children under age 12. The drug is administered as an injection and is already approved to treat pediatric and adult patients aged 12 and older who weigh at least 88 pounds. Early treatment with remdesivir, during the first 5 days of acute infection, is highly effective in preventing disease progression in older adults, according to a randomized, double-blind, placebo-controlled clinical trial. The FDA’s approval for pediatric patients was based on a small study including only 53 participants that showed similar safety and pharmacokinetic results to those in adults.
Although COVID-19 generally causes less severe disease in children, severe illness does still occur in this population. Children aged 5-11 became eligible for vaccination with Pfizer-BioNTech’s SARS-CoV-2 vaccine in November 2021, but those under age 5 are not yet eligible for vaccination. In its approval, the FDA noted that remdesivir is not a substitute for vaccination in those who qualify but is an effective treatment option for pediatric patients. Data published last week in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) show that during the winter Omicron surge, COVID-19-associated hospitalization rates were approximately twice as high among unvaccinated children aged 5-11 as among vaccinated children of the same age. The FDA’s approval of remdesivir for the youngest COVID-19 patients could help lower their risk of disease progression and keep some children out of the hospital.
VACCINE FOR UNDER-5 CHILDREN The approximately 19.5 million children younger than age 5 in the US remain ineligible for vaccination against COVID-19, and the US FDA likely will postpone any action to authorize a vaccine for the youngest children until June, according to several sources. Moderna is expected to submit a request for Emergency Use Authorization for its SARS-CoV-2 vaccine by the end of this month, and Pfizer-BioNTech earlier this year postponed its rolling application for their vaccine to wait for data on a 3-dose primary series. Those familiar with FDA discussions said the regulator might wait until early summer to simultaneously authorize both vaccines rather than push one through before the other, thereby simplifying communication about the vaccines to the public. However, those plans could change, particularly if the current uptick in COVID-19 cases accelerates. The administration of US President Joe Biden is under increasing pressure to move on authorizing a vaccine for the youngest children, from members of his own political party and parents who are eager to vaccinate their children. Notably, less than 30% of children aged 5-11—who became eligible for vaccination in November 2021—have received their primary 2-dose vaccine series, and some polls show parents of young children might be hesitant to vaccinate their younger children. The FDA has called on its Vaccines and Related Biological Products Advisory Committee (VRBPAC) to set a tentative meeting for June, although the topic of that meeting is not yet known.
CHINA After weeks of lockdowns in China’s largest city, Shanghai, due to surging numbers of new COVID-19 cases driven by the Omicron variant of concern, the nation’s capital of Beijing this week rolled out a 5-day mass testing drive and locked down several residential areas. Cultural holidays, mass gatherings, and holiday travel have all been suspended. The swift response prompted panic buying, as residents crowded grocery stores and swamped food delivery services with requests. Since the outbreak was detected 5 days ago, authorities have identified 92 cases in Beijing, a small number compared with the more than 500,000 cases confirmed in Shanghai, where the number of new cases is beginning to fall. However, the number of new deaths in Shanghai tripled in a 24-hour period between April 22 and April 23. This is expected, as increases in deaths typically follow increases in the number of new cases by 3-4 weeks. China’s lockdowns are not only disrupting life for residents but also are significantly impacting domestic and global economies, crippling supply chains, increasing unemployment, and affecting stock markets.
SOUTH AFRICA The number of new COVID-19 cases is once more rising in South Africa, signaling a potential fifth wave of infections. The country has reported its highest rate in 3 months. South Africa’s National Health Department reported 4,406 new COVID-19 cases in a 24-hour period ending April 21, just over 1.5 times more cases than were reported the day before. The nation’s positivity rate rose from 16% over the weekend to 19.3% on April 25, with an additional 1,954 new cases. The increase is being driven by Omicron sublineages, with a rising proportion of cases attributable to BA.4 and BA.5. No new variant has been reported. Notably, the pandemic may have given a boost to South Africa’s efforts to reform its health system through a national insurance scheme by highlighting the need to improve health equity.
CORONAVAC BOOSTERS New data from Chile estimates vaccine effectiveness with the use of homologous and heterologous booster administration in individuals aged 16 years and older. Published in The Lancet Global Health on April 23, the study evaluates a national-level prospective cohort of more than 4 million individuals who completed a primary immunization schedule (2 doses) of CoronaVac and subsequently received a booster. Of the cohort, 46.5% received a booster of Oxford-AstraZeneca, 48.9% Pfizer-BioNTech, and 4.5% CoronaVac. Both homologous and heterologous booster administration with a primary vaccination schedule of CoronaVac showed a high level of protection against symptomatic COVID-19, including severe disease and death. Notably, vaccine effectiveness (VE) in preventing symptomatic COVID-19 was higher among the heterologous booster cohorts compared to homologous booster administration. The Pfizer-BioNTech booster adjusted VE for preventing symptomatic COVID-19 was 96.5% (96.2–96.7), 93.2% (92.9–93.6) for Oxford-AstraZeneca, and 78.8% (76.8–80.6) for CoronaVac. Adjusted VEs against hospitalization, intensive care unit (ICU) admission, and death followed a similar trend. The study enforces the need for boosters for the Chinese-made CoronaVac vaccine to improve effectiveness, and could help inform policymaking in China, which is experiencing a surge in COVID-19 cases.
LONG COVID No one knows what causes post-acute sequelae of COVID-19 (PASC), commonly known as long COVID, but researchers worldwide are working to uncover clues about what causes the condition, its prevalence in COVID-19 survivors, and potential therapies. A study published April 23 in The Lancet Respiratory Health describing results from the Post-hospitalisation COVID-19 study (PHOSP-COVID) suggests that fewer than 1 in 3 people (28.9%) who were hospitalized for COVID-19 felt fully recovered 1 year after being discharged. Factors associated with being less likely to report full recovery were female sex, obesity, and invasive mechanical ventilation during hospitalization. The most common ongoing symptoms were fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness, all of which were reported by more than 51% of the patients 1 year after discharge. Another study—which was presented at the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID) in Lisbon, Portugal, by researchers from the Luxembourg Institute of Health—found that 6 in 10 people continue to have at least 1 symptom a year after their initial infection. The study, Predi-COVID, suggests that severity of initial disease is associated with the likelihood of persistent symptoms and their intensity, reinforcing the need for vaccination to prevent severe disease.
Based on previous research, some scientists believe long COVID could be the result of an overactive immune response, but the results of a small study published in Clinical Infectious Diseases suggest the persistent symptoms could be the result of a suppressed immune system. The researchers, from the David Geffen School of Medicine at UCLA, suggest that certain antibody treatments could help some patients improve. Notably, the study was funded by the manufacturer of the antibody treatment used in the research. Another preprint paper, conducted by researchers at Stanford Medical School and not yet peer-reviewed, raises the question of whether viral reservoirs, possibly in the gastrointestinal system, could contribute to long COVID symptoms. After 4 months from initial infection, researchers were unable to detect SARS-CoV-2 in nasal or oral swab samples from any of the 113 participants who had mild or moderate COVID-19, but nearly 13% had detectable viral RNA in fecal samples. Nearly 4% continued to shed viral RNA in their stool 7 months after initial diagnosis. Ongoing research shows long COVID can impact people far after initial infection. While there currently are no proven effective pharmacological or non-pharmacological interventions for patients with long COVID, some research suggests that SARS-CoV-2 vaccination can reduce but not eliminate the risk of longer-term symptoms, reinforcing public health recommendations to remain up to date on vaccination.
US DEATHS As the US edges closer to marking 1 million deaths from COVID-19, many are grappling with how to explain this reality. In an attempt to describe the seemingly unfathomable death toll, Eric Boodman of STAT equates it to about “5,500 commercial airplanes crashing in a little more than 2 years,” but says trying to account for human loss through analogy is meaningless and does not make those who have lost loved ones feel less alone. In the US, the pandemic’s death toll has been concentrated among elderly populations, including those at long-term care facilities, and mortality rates are highest among Black and Hispanic populations. For a second year, COVID-19 was the third leading cause of death in the US in 2021, although racial and ethnic disparities narrowed compared with 2020, most likely showing the impacts of public health interventions such as contact tracing, mask mandates, and, most importantly, vaccination. According to recent analysis from the Peterson-KFF Health System Tracker, about 234,000 COVID-19-related deaths in the US could have been prevented since June 2021 with a primary vaccination series. Additionally, many could have been spared immense amounts of grief with more widespread and quick vaccine uptake. According to a study published April 25 in JAMA Internal Medicine, most families who had loved ones in intensive care units (ICUs) due to COVID-19 have experienced symptoms of post-traumatic stress disorder (PTSD). Ed Yong of The Atlantic notes that for every person lost to COVID-19, an average of 9 close relatives are left bereaved, meaning no fewer than 9 million US residents are learning to cope with grief and adjust to their new realities, processes often intensified by the continuing politicization of the pandemic.
by ponchi101 1. Good to see that some treatments are coming along.
2. Pardon me for being callous. How can the loss of a loved one, or them being in an ICU due to covid, is different than losing them or having them in an ICU DUE TO ANY OTHER FACTOR? Mourning is like that. My brother passed away in January of 2018 and I still can't go a day without thinking of him. Of course, it was not C19 (it was cancer) but why is it being singled out due to the disease?
by Deuce
ponchi101 wrote: ↑Tue Apr 26, 2022 7:22 pm
2. Pardon me for being callous. How can the loss of a loved one, or them being in an ICU due to covid, is different than losing them or having them in an ICU DUE TO ANY OTHER FACTOR? Mourning is like that. My brother passed away in January of 2018 and I still can't go a day without thinking of him. Of course, it was not C19 (it was cancer) but why is it being singled out due to the disease?
Certainly any death of a loved one is an enormous blow...
Maybe they're thinking of the difference being that when someone is in ICU with COVID-19, it's often difficult - or even impossible - for family to be allowed to visit/see them/say 'goodbye'...
by dryrunguy Here's the latest Situation Report. The paragraph on measles is interesting. I'm not so sure that increase is solely due to COVID interrupting vaccination schedules. I'd bet increases in general vaccine skepticism is part of the problem. The section on viral spillover also caught my attention.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 509 million cumulative cases and 6.2 million deaths worldwide as of April 27. As expected, the number of cumulative cases surpassed 500 million on April 14. The global weekly incidence decreased for the fifth consecutive week—down 19% from the previous week—to the lowest weekly total since mid-December 2021. Most regions continued to report decreasing trends in weekly incidence. Africa’s weekly total increased 32% over the previous week, which appears to be largely driven by the surge in South Africa. Weekly incidence also increased in the Americas, up 8.7% over the previous week. The trend in reported global weekly mortality decreased for a third consecutive week, down 19% from the previous week.
Global Vaccination
As of April 18, WHO reported 11.4 billion cumulative vaccine doses administered globally, with 3.82 billion individuals receiving at least 1 dose, and 3.35 billion fully vaccinated*. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations continues to decline overall—down from nearly 40 million doses per day in late December 2021—although the global average increased from 10.7 million doses per day last week to 11.7 million on April 27**. The trend continues to closely follow that in Asia. Our World in Data estimates that there are 5.13 billion vaccinated individuals worldwide (1+ dose; 65.2% of the global population) and 4.64 billion who are fully vaccinated (59.0% of the global population). A total of 1.84 billion booster doses have been administered globally.
*The WHO data for cumulative global vaccinated individuals decreased substantially from the previous week—down from 5.1 billion with 1+ dose and 4.58 billion fully vaccinated. It is not immediately clear why the current numbers are lower.
**The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is reporting 80.9 million cumulative cases of COVID-19 and 989,408 deaths. The average daily incidence has nearly doubled from the recent low of 24,982 new cases per day on April 4 to 48,692 on April 26. The daily mortality continues to decline, down to 299 deaths per day—the first day below 300 since July 23, 2021.* Notably, new COVID-19 hospital admissions continue to trend upwards, with an increase of 17.6% over the past week.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 574 million cumulative doses of SARS-CoV-2 vaccines. After a slight increase starting in late March, following US FDA authorization of a second booster dose, daily vaccinations are once again declining, down from 485,000 doses per day on April 12 to 394,000 on April 21 (-18.6%). A total of 257 million individuals have received at least 1 vaccine dose, which corresponds to 77.5% of the entire US population. Among adults, 89.0% have received at least 1 dose, as well as 27.7 million children under the age of 18. A total of 219 million individuals are fully vaccinated**, which corresponds to 66.1% of the total population. Approximately 76.0% of adults are fully vaccinated, as well as 23.1 million children under the age of 18. A total of 100.3 million individuals have received an additional or booster dose. This corresponds to 45.7% of fully vaccinated individuals, including 68.5% of fully vaccinated adults aged 65 years or older. Only 49.5% of individuals eligible for a first booster dose have received one.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent several days.
**Full original course of the vaccine, not including additional or booster doses.
VACCINES FOR YOUNGEST CHILDREN Moderna this morning submitted a request with the US FDA for Emergency Use Authorization (EUA) of its SARS-CoV-2 vaccine for children ages 6 months to under age 6. The submission is based on data from the Phase 2/3 KidCOVE study, which tested a 2-dose primary series in young children using a low-dose 25 μg version of the vaccine. According to Moderna, the lower dosage led to a similar immune response in young children as the higher 100 μg 2-dose primary series in adults, with a favorable safety profile. In a revised analysis based on data first released in March, the data showed the vaccine was 51% effective at preventing symptomatic COVID-19 in the youngest children, ages 6 months to under 2 years, and 37% effective at preventing symptomatic disease in children ages 2 through 5. These results were collected during the Omicron surge and showed similar declines in protection as adults due to the variant’s ability to partially evade vaccine-induced immunity. Moderna also is expected to soon seek authorization of its vaccine for children ages 6-11, as well as file an update to its EUA for adolescents aged 12-17. The FDA has not ruled on the company’s EUA request for adolescents, submitted in June 2021, citing concerns over the rare side effect of myocarditis and pericarditis, particularly in teen boys. Currently, only the Pfizer-BioNTech vaccine is authorized for children aged 5-11.
A top FDA official this week suggested the agency has not yet reviewed data on SARS-CoV-2 vaccines for the youngest children because the manufacturers have not completed their EUA applications. The agency is expected to release a timeline for expert review this week. Despite growing pressure, a decision on whether to authorize a vaccine for the nation’s 18 million youngest children likely will not happen until June. Moderna is expected to complete its EUA submission for the youngest children next week, and Pfizer and BioNTech plan to complete their application for a 3-dose vaccine regimen for children younger than 5 years in late May or early June. A White House official suggested the FDA might prefer to review both applications simultaneously in order to compare the vaccines side-by-side and simplify communication about the vaccines if and when one or both are authorized for young children.
BOOSTERS FOR CHILDREN AGES 5-11 Pfizer and BioNTech on April 26 submitted a request to the US FDA for Emergency Use Authorization (EUA) of a booster dose of the companies’ SARS-CoV-2 vaccine for children aged 5 to 11 years. The booster would be a third shot of the same 10 µg dosage used in the 2-dose primary series, administered about 6 months after the second dose. Currently, third doses of the Pfizer-BioNTech vaccine are authorized for children aged 5 to 11 who are moderately to severely immunocompromised, and booster doses are authorized for all individuals aged 12 years and older, who receive a higher dose (30 µg). Experts are divided over whether a booster dose is necessary in healthy children. Some say data show vaccine effectiveness wanes over time and support the use of boosters in children to maintain a higher level of protection. Others remain skeptical, contending that 2 doses continue to protect recipients against serious illness from the currently circulating SARS-CoV-2 variants and because children have an overall lower risk of severe disease and hospitalization from COVID-19. Only 28% of children aged 5 to 11 years are fully vaccinated, signaling that demand for a booster dose among this age group likely would be low. Pfizer and BioNTech also plan to submit data for booster authorization to the European Medicines Agency (EMA) and other regulatory agencies worldwide in the coming weeks.
ANNUAL BOOSTERS The US FDA has authorized second booster, or fourth, doses for parts of the US population, raising questions over how frequently boosters will be required moving forward. Several companies, including Novavax and Moderna, have begun initiatives to develop joint influenza and COVID-19 shots, creating what would be a new annual vaccine administered each fall. But several US scientists and researchers recently urged more involved dialogue regarding future plans for the use of SARS-CoV-2 vaccine boosters, pushing back on the idea of annual boosters and calling for more data on the value of annual SARS-CoV-2 booster doses. While there is no evidence suggesting any harm from additional booster doses, the experts have shared several concerns that could stem from a policy requiring annual vaccinations. First, they worry that an emphasis on boosters diminishes the long-lasting protection that current vaccine doses provide against severe COVID-19 disease. Second, experts worry that a lack of evidence in regulatory decision making could set a dangerous precedent moving forward. The group specifically urged the FDA to measure T-cell responses, in addition to antibody responses, when conducting SARS-CoV-2 vaccine trials. Lastly, they noted the lack of response for both first and second booster doses signals fatigue from the US public. More than 100 million US residents have received the first COVID-19 booster, roughly 50% of eligible people. Some worry that “booster fatigue” will be a problem, adding to calls for a more prudent, data-driven approach to annual boosters.
US SEROPREVALENCE A study published April 26 in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) estimates that 58% of the US population, including 75% of children, have been infected with SARS-CoV-2. Many of those infections occurred during the winter’s Omicron surge. The study reports on data from national commercial laboratories across all 50 states, Washington, DC, and Puerto Rico. Between September 2021 and February 2022, labs conducted convenience samples on blood specimens that were submitted for clinical testing in their labs, excluding samples that were testing for SARS-CoV-2 antibodies upon initial receipt. The median sample size for the group of labs was 73,869 each month, with a drop in the number of tests to 45,810 in February 2022, likely caused by disruptions from the surge in domestic infections fueled by the Omicron variant. The research team weighted samples by demographic data to produce estimates of seroprevalence.
The team saw a slight, but steady, increase in seroprevalence between September and December 2021, increasing between 0.9-1.9% every 4 weeks. At the end of this collection period, the seroprevalence across the US sample was estimated to be 33.5%. Between December 2021 and February 2022, at the height of the Omicron surge, the team observed a spike in national seroprevalence, rising from 33.5% to 57.7%. Notably, during this period, children aged 0-11 saw an increase from 44.2% to 75.2% and those aged 12-17 saw a similar increase from 45.6% to 74.2%. Adult populations saw spikes in seroprevalence from 36.5% to 63.7% for individuals aged 18-49, 28.8% to 49.8% for those 50-64, and 19.1% to 33.2% among those aged 65 and older. The researchers noted several limitations in their study design, including restrictions of applicability tied to convenience sampling; limited race and ethnicity data; the potential for sampling bias due to the setting of sample collection; and the possibility that infection following vaccination resulted in reduced antibody titers.
SARS-CoV-2 testing is only able to catch a fraction of cases occurring in the country, so serosurveys present an opportunity to better understand the scale of infections. Still, the study may not represent a full picture of COVID-19 in the country, nor does it indicate whether or not individuals with SARS-CoV-2 antibodies have persistent immunity to new infections. CDC Director Dr. Rochelle Walensky noted the study’s results and vaccine uptake show an increased level of community protection from SARS-CoV-2. She added that vaccination remains key in creating a more resilient population, urging those who remain unvaccinated, including those previously infected, to get vaccinated.
PANDEMIC TRANSITIONING COVID-19 remains a pandemic, constituting a serious health threat in many parts of the world. Even as COVID-19-related deaths reach their lowest point since the pandemic began, several Asian nations are experiencing their largest surges to date and countries in Africa—which currently is experiencing an increase in cases—continue efforts to ramp up vaccination programs. But other countries, particularly in North America and Europe, are taking steps to move beyond an emergency phase, relaxing public health mitigation guidelines and reducing or eliminating COVID-19 funding from budgets. Global health experts note the pandemic is at a critical juncture, as wealthy nations—criticized for not doing enough to help low- and middle-income countries throughout the pandemic—cut back even more.
The EU this week declared an end to the COVID-19 emergency, saying the disease should be treated similarly to influenza. Denmark announced an end to its widespread vaccination program, saying “the epidemic has reversed.” However, the Danish Health and Medicines Authority said additional vaccinations against COVID-19 likely will be needed in the future as new variants emerge. In the US, debate over additional funding for the pandemic response is at a standstill in the US Congress, and the administration of US President Joe Biden has warned that without new funds, the nation’s domestic and international response efforts will falter. White House Chief Medical Advisor Dr. Anthony Fauci said this week that the US is “out of the pandemic phase,” but later clarified those remarks, noting the pandemic is ongoing but that the US is in “a transitional phase,” moving out of an acute emergency state and into a more controlled phase. Mexico’s government declared the nation has moved into an endemic stage, and authorities will treat COVID-19 as a seasonal disease. Still, as long as COVID-19 outbreaks continue, the virus will continue to evolve and potentially develop the ability to further evade vaccine-induced or natural immunity, creating high levels of uncertainty around the future of the pandemic.
GLOBAL DECLINE IN TESTING As the pandemic continues, the WHO is receiving less testing data, which is compounding challenges in monitoring epidemiological trends and emerging variants. Earlier this week, WHO Director-General Dr. Tedros Adhanom Ghebreyesus called on governments to maintain sufficient SARS-CoV-2 surveillance, in part to ensure that the WHO has the data necessary to track the pandemic and provide guidance. Global testing has reportedly declined by 70-90% over the past 4 months, although the exact cause remains uncertain. Over that period, the global daily incidence fell from a record high of 3.4 million new cases per day in late January to fewer than 700,000, a decline of 80%. It is difficult to get a reliable global estimate for test positivity, because it is not reported consistently by many countries; however, the trends vary considerably among countries with the highest cumulative incidence. Test positivity in some countries—including Argentina, India, Russia, Turkey, and the United States*—has declined substantially from peaks in January-February, while it remains elevated or has increased sharply in others—such as Brazil, France, Germany, Netherlands, South Korea, and Vietnam. Without additional data, the extent to which the decline in testing is a function of slowing transmission, changes in national policies or capacities, or other factors is unclear. One potential factor is the expanded availability of at-home rapid tests in many countries. Many of these test results (positive and negative) go unreported to public health authorities, and therefore, to the WHO. As the pandemic continues, epidemiological and genomic surveillance are needed to provide critical data for health and elected officials at all levels of government.
*Although the US estimate has more than doubled since its recent low in mid-March.
TWITTER & MISINFORMATION The WHO has worked with social media platforms prior to and throughout the COVID-19 pandemic to mitigate the spread of online misinformation and disinformation. With the news that billionaire Elon Musk has reached a US$44 billion deal to purchase Twitter—a previously publicly owned influential platform with 217 million daily active users worldwide—WHO officials are warning of the dangers of health and vaccine misinformation on social media. During a briefing this week, several WHO officials said Musk—who has said he plans to hold up free-speech standards similar to those of the US government—has a “huge responsibility” to combat health-related falsehoods, which can lead to mistrust, confusion, or risk-taking and potentially prolong or intensify disease outbreaks.
According to the WHO, false information is 70% more likely to get shared than accurate news on social media. In a paper published April 26 in Nature Scientific Reports, researchers from Indiana University and the Polytechnic University of Milan suggest that online misinformation posted during the pandemic is associated with early COVID-19 vaccination hesitancy and refusal. The researchers underscored the importance of combating online misinformation, writing that although people in the US have a constitutional right to free speech, providing access to trustworthy information is vital to maintaining public health. Another study from Germany, published April 27 in BMC Public Health, reinforces these findings, concluding that online misinformation is an important reason for vaccination refusal and providing access to quality information sensitive to the needs of the target audience is vital. It is unclear how or if Musk will continue Twitter’s work with the WHO or other health agencies, and many fear that his insistence on free speech could create a fertile platform for the dissemination of even more health misinformation, myths, and conspiracy theories.
MEASLES Over the past 2 years, the COVID-19 pandemic interrupted routine childhood vaccinations globally, resulting in a backslide of immunization efforts in many regions. As a potential signal of future vaccine-preventable disease outbreaks, the number of reported measles cases increased 79% during the first 2 months of 2022, compared to the same period in 2021, according to UNICEF and the WHO. In 2020, 23 million children missed out on routine childhood immunizations, the highest number since 2009. The agencies urged nations to rapidly get vaccination programs back on track to help mitigate the impacts of missed shots, the effects of which will be felt for decades.
VIRAL SPILLOVERS At least 10,000 virus species have the ability to infect humans, but most of those are currently silently circulating in mammalian species other than humans. But as the planet warms and humans are forced to move into new habitats, the risk that these diseases will pass from their animal hosts to humans increases enormously over the next 50 years, according to research published today in Nature. Using a computational model, the researchers estimate that more than 4,000 spillover events could occur among 3,139 species as the climate changes and their habitats overlap. This situation is already happening, and some experts say the world is moving from the Anthropocene era—when humans dominated influence over the Earth’s environment—into a Pandemicene, an era characterized by diseases’ influence on humanity. Several SARS-CoV-2 spillover events have been documented, including one involving mink in the US and another involving white-tailed deer in Canada. Hence, global health experts are promoting a One Health approach to tracking COVID-19 and other viruses and warning that more pandemics will occur as the Earth warms, making pandemic preparedness one of the most urgent issues of our time.
dryrunguy wrote: ↑Thu Apr 28, 2022 4:37 pm
...
VIRAL SPILLOVERS At least 10,000 virus species have the ability to infect humans, but most of those are currently silently circulating in mammalian species other than humans. But as the planet warms and humans are forced to move into new habitats, the risk that these diseases will pass from their animal hosts to humans increases enormously over the next 50 years, according to research published today in Nature. Using a computational model, the researchers estimate that more than 4,000 spillover events could occur among 3,139 species as the climate changes and their habitats overlap. This situation is already happening, and some experts say the world is moving from the Anthropocene era—when humans dominated influence over the Earth’s environment—into a Pandemicene, an era characterized by diseases’ influence on humanity. Several SARS-CoV-2 spillover events have been documented, including one involving mink in the US and another involving white-tailed deer in Canada. Hence, global health experts are promoting a One Health approach to tracking COVID-19 and other viruses and warning that more pandemics will occur as the Earth warms, making pandemic preparedness one of the most urgent issues of our time.
C'mon, this is ridiculous. We can't have "eras" with a 50 year span. That is geologically and scientifically bogus. Why not split them even more: "C19 era", or we can re-baptize the Middle Ages as "the Black Plague era".
Humanistically, sure, it can be done. But as a marker of the passage in time on geological terms, it makes no sense. If we were not to document this and we were to go extinct, a future civilization would not even find traces of what has happened. It has been too short.
by ti-amie
MEASLES Over the past 2 years, the COVID-19 pandemic interrupted routine childhood vaccinations globally, resulting in a backslide of immunization efforts in many regions. As a potential signal of future vaccine-preventable disease outbreaks, the number of reported measles cases increased 79% during the first 2 months of 2022, compared to the same period in 2021, according to UNICEF and the WHO. In 2020, 23 million children missed out on routine childhood immunizations, the highest number since 2009. The agencies urged nations to rapidly get vaccination programs back on track to help mitigate the impacts of missed shots, the effects of which will be felt for decades.
This is frightening. Measles is highly contagious and in some causes more than a pimply outbreak. This has more to do with the original antivaxx nonsense and has probably gotten worse because of the current situation. When my daughter was an infant and it came time for her MMR I was really worried but went ahead with it anyway. That's how long this antivaxx stuff has been around.
by Deuce It's best to not fool oneself into the rather arrogant comfortable belief that this virus is under control, and things should return back to normal...
There is still much, much more that we DON'T know about COVID-19 than there is that we know. (When I say 'we', I mean mankind.)
by ti-amie My daughter told me that she knows 6 people who, in the last two weeks, have been infected, one severely. The infected include her mother-in-law who came down with symptoms after the Passover Seder.
I'm getting my second booster tomorrow. And avoiding a Mother's Day brunch at the above mother-in-laws house. To show you how clueless people are she is still testing positive, some quack told her it's okay, she will for a few days after the five day quarantine he gave her, so she went and got a haircut.
And she wants to know why I said I'll skip the brunch this go around.
Edited because I counted on person twice.
by Deuce Yes... Many people are confusing what they wish for with what reality is.
When reality is ugly or uncomfortable, people fabricate nice, comfortable illusions. The problems come when they interpret those illusions as reality.
It's not the first time that humans are afflicted with this condition, and it certainly won't be the last...
by dryrunguy Here's the latest Situation Report. There's a lot here. I took particularly interest in the fact that the vaccine manufacturing plant somewhere in Africa hasn't received a single order. It will be difficult to address vaccination inequity if no one wants it--or doesn't know it's there.
::
NEW COVID-19 TESTING TOOLKIT FAQS The Johns Hopkins Center for Health Security COVID-19 Testing Toolkit has launched a new Frequently Asked Questions (FAQs) tool to help answer users’ questions about COVID-19 testing. Questions can be browsed by 8 topics or 54 keywords. Questions and answers are regularly updated to reflect new information, federal guidance, and topics of interest. Access the FAQs here: http://covidtestinganswers.org/
BA.4/BA.5 SUBVARIANT IMMUNE EVASION The BA.4 and BA.5 sublineages of the Omicron variant of concern (VOC)—both characterized by L452R and F486V mutations on the spike receptor binding domain—are increasing in prevalence in South Africa, and more countries around the world are detecting the presence of these emerging SARS-CoV-2 subvariants. There is concern that the early signs of another surge in South Africa could indicate that the new subvariants are more transmissible or are capable of evading immune protection conferred by prior infection or vaccination. As of the middle of April, the WHO had not reported any notable changes in transmissibility or disease severity compared with other Omicron subvariants; however, this was based on very limited available data, with fewer than 200 sequences available at that time.
Researchers in South Africa recently published (preprint) findings from analysis of natural and vaccine-induced immune protection against the BA.4 and BA.5 subvariants. The researchers compared the neutralization capacity of blood specimens collected from 39 individuals infected with the BA.1 subvariant during South Africa’s initial Omicron surge—24 unvaccinated and 15 fully vaccinated. The unvaccinated participants exhibited a 7.5-fold decrease in neutralizing capacity against BA.4 and BA.5, compared to BA.1. Vaccinated participants exhibited a better immune response against BA.4 and BA.5, but neutralizing capacity was still decreased by a factor of 2.6-3.2 compared to BA.1. The neutralizing capacity among the vaccinated individuals was significantly better than for the unvaccinated participants.
This study is based on a small number of participants—including only 8 participants who received the Pfizer-BioNTech vaccine, 7 who received the J&J-Janssen vaccine, and only 1 individual who had received a booster dose—although the differences in immune response were statistically significant. Notably, the researchers only included participants who were previously infected with the BA.1 subvariant and compared the neutralizing capacity against that same subvariant. We would expect the immune response to be stronger against reinfection with the same subvariant, so while the neutralizing capacity was lower against BA.4/BA.5, it could still be sufficient to provide meaningful protection. And with only 1 boosted participant, additional data are needed to evaluate the protection conferred by booster doses.
The WHO and other health experts continue to emphasize that full vaccination and booster doses provide the best protection against circulating and emerging SARS-CoV-2 variants. This study provides some evidence that immunity conferred by recent BA.1 infection and vaccination may be less effective against the emerging BA.4 and BA.5 subvariants; however, additional research is needed before we can have a clear picture of how well natural and vaccine-induced immunity protect against infection, symptomatic COVID-19 disease, and severe symptoms or death associated with the BA.4 and BA.5 subvariants.
US SITUATION While daily COVID-19 incidence remains relatively low across the US, the 7-day moving average of new cases has increased by about 50% over the last month. In New York City, daily incidence jumped from about 600 daily cases in early March to nearly 2,500 new cases per day, with cases driven by the BA.2 subvariant of Omicron. While hospitalizations and deaths remain low, the city this week entered a higher risk level (medium, or yellow, for virus transmission). If the number of new cases continues to rise, another move to a higher level could trigger reinstatement of certain public health measures, including masking requirements. California also is experiencing a rise in cases, with the state recording a 30% increase in new COVID-19 cases over the last week, as well as a smaller increase in hospitalizations.
The rising case numbers coincide with relaxed public health measures and many states scaling back their frequency of COVID-19 data reporting to only once a week or every 2 weeks. These data reporting delays could produce misleading trends and hinder subsequent interventions. Additionally, shifting testing practices—including the shuttering of public testing sites and more people using at-home tests and subsequently not reporting their results—could be masking a significant number of infections. With these changes in data reporting, capturing the number of people infected in the general population has become nearly impossible. Therefore, epidemiologists have turned to different metrics to better estimate COVID-19’s impact, looking instead at hospital data to estimate severe disease levels in communities and strain on healthcare systems. Others are watching wastewater surveillance to help predict where and when outbreaks might occur. As the nation shifts its response from an acute emergency phase to a more long-term response, and as immunity from vaccination and natural infection wane, the country will continue to rely on these imperfect data to help inform individuals and jurisdictions about their current and future risks of contracting COVID-19.
US FDA VACCINE ADVISORY COMMITTEE On Friday, April 29, the US FDA announced tentative dates for a meeting of its Vaccine and Related Biological Products Advisory Committee (VRBPAC) to evaluate applications for Emergency Use Authorizations (EUAs) for multiple SARS-CoV-2 vaccines, including for use in young children. The announcement notes that the submissions are not yet complete, but the FDA anticipates that it will receive full applications from multiple vaccine manufacturers over the coming weeks. On June 7, the VRBPAC is scheduled to meet to discuss the EUA application for use of the Novavax vaccine in adults aged 18 years and older. This would be the first authorization for use of the Novavax vaccine in the US. The FDA reserved June 8, 21, and 22 for the advisory group to meet on the applications to authorize the use of the Moderna and Pfizer-BioNTech vaccines in young children. On June 28, the group will follow up on its April 6 meeting to discuss whether the target strains in existing SARS-CoV-2 vaccines should be modified and, if so, what strains should be used in Fall 2022.
The committee will provide recommendations to the FDA regarding these vaccines, and if the reviews are positive, SARS-CoV-2 vaccines could potentially be available for young children (eg, aged 6 months and older) by this summer. Scheduling the meetings in anticipation of receiving the full submissions will mitigate delays in reviewing the data. The FDA has been under growing public pressure due to the absence of a vaccine option for young children, particularly in light of the increased impact on children during the Omicron surge.
Regulatory officials from Health Canada are currently reviewing an emergency authorization application from Moderna for use of its SARS-CoV-2 vaccine in children aged 6 months to 5 years. The application was submitted on April 29, and while there is not yet a timeline for the review, Moderna officials reportedly indicated that they hope to complete it “shortly.”
POST-TREATMENT RELAPSE US health authorities are prioritizing research into why and how often some people with COVID-19 who take Pfizer’s antiviral treatment Paxlovid see rebounds in symptoms and viral load levels after completing the therapy. The relapses—when a person who tested positive takes Paxlovid, tests negative after taking the 5-day course of treatment, then tests positive again several days after completing the therapy—appear to be rare, but healthcare providers should warn patients to watch for symptoms after taking Paxlovid and test again if they begin to feel ill. The need to unravel the mystery is urgent, as it presents another hurdle in expanding the Biden administration’s Test-to-Treat initiative aimed at improving access to COVID-19 treatments, including Paxlovid and Merck’s molnupiravir. US NIH officials are working to develop clinical and epidemiological studies that could help shed light on how often viral rebounds occur, who might be at risk for relapse, and whether a longer regimen could knock out the virus instead of what appears to be simply suppressing it. One preprint case study of relapse was posted in late April, describing a fully vaccinated and boosted 71-year-old with asthma who experienced relapse 4 days after completing Paxlovid. Both the US FDA and Pfizer have noted a small number of people in clinical trials who took Paxlovid or a placebo experienced viral load rebound 10-14 days after starting treatment. Because patients in both groups experienced the phenomenon, investigators did not relate it directly to the medication. The scenarios also raise concerns of emerging antiviral resistance if the virus is suppressed and then is able to begin replicating again.
POST-EXPOSURE PROPHYLAXIS Pfizer’s COVID-19 treatment Paxlovid is falling short of being a possible means of preventing infection following exposure, according to new Phase 2/3 trial data. In a trial of 2,957 adults who were household contacts of a person with COVID-19 but themselves tested negative via antigen test, people who took Paxlovid for 5 or 10 days were only 32% and 37% less likely to subsequently test positive, respectively. In addition to not having a marked impact on reducing the risk of household contacts, these results also are not statistically significant compared with the placebo groups and could be due to chance. The trial, known as EPIC-PEP (Evaluation of Protease Inhibition for COVID-19 in Post-Exposure Prophylaxis), is part of Pfizer’s series of clinical trials to evaluate the efficacy and safety of Paxlovid. A post-exposure prophylaxis for SARS-CoV-2 would be helpful in preventing infection in people who were exposed to the virus but have not yet developed an infection. In persons with pre-existing conditions or for people who do not want to risk losing time at work, preventing infection following exposure altogether could be a gamechanger. Unfortunately, Paxlovid does not appear to be the drug to provide this outcome. Although many are disappointed in these outcomes, physicians say they are no less hesitant to prescribe Paxlovid for its originally intended purpose of treating people with COVID-19, especially for those at risk of severe outcomes.
CHINA After more than 1 month in strict lockdown, some residents of Shanghai, China, were able to leave their homes today for short walks and to obtain supplies, as a recent COVID-19 surge there shows some signs of waning. However, the capital city of Beijing continued mass testing and announced that schools, gyms, entertainment and theme park venues, and indoor dining will remain closed, as authorities hope to prevent citywide lockdowns like those in Shanghai, which now appear to be easing slightly. Although the number of new cases remains low, Beijing is prepping hospitals and reopening isolation facilities in hopes of preventing the virus’s spread and avoiding widespread lockdowns similar to those implemented in Shanghai. Throughout the pandemic, China has maintained its “zero-COVID” policies, including mass testing and quarantining of infected individuals, leading some public health experts in the country to quietly wonder whether the strategy is tenable over the long-term. Notably, China’s economy—as well as the global economy—are feeling a pinch from the pandemic, and economists are skeptical about whether the country will be able to achieve its 2022 5.5% growth target if the zero-COVID policy continues.
INDIA SUPREME COURT In what some are calling a landmark decision, India’s Supreme Court on May 2 ruled that people cannot be forced to be vaccinated against COVID-19 but simultaneously upheld the government’s vaccination policy, including its ability to regulate issues of public health concern and grant emergency use authorizations to vaccines. The 2-justice panel maintained the government is entitled to implement certain restrictions on individual rights to regulate community public health but said policies cannot be viewed as “arbitrary and unreasonable.” The court called on State and Union Territories to review any current vaccine mandates to ensure that any restrictions on unvaccinated individuals are proportionate with the country’s current COVID-19 situation. According to the ruling, individuals’ bodily integrity and personal autonomy, including their ability to reject vaccination or treatment, are protected under Article 21 of the Constitution. The court also ordered the government to establish without delay a public-facing database to collect and disclose SARS-CoV-2 vaccine clinical trial results, including data on adverse events. In response, the government claimed no one is forced to be vaccinated, and lawyers for Indian pharmaceutical companies Serum Institute of India and Bharat Biotech International said clinical trial data are already publicly available. India’s daily test positivity rate this week rose above 1.0 for the first time in 2 months, possibly indicating the country could be entering a fourth wave. About 72% of India’s population has received at least 1 dose of SARS-CoV-2 vaccine but hesitancy remains high in many rural areas.
GLOBAL VACCINATION EFFORTS South African drugmaker Aspen Pharmacare has warned that a plant established to package, sell, and distribute the J&J-Janssen SARS-CoV-2 vaccine under its own brand name—Aspenovax—throughout Africa risks shutting down because the company has not received a single order. Initially touted by the WHO as a “transformative moment” in global efforts to resolve vaccine inequity, the licensing agreement was meant to bolster Africa’s vaccine production and launch a manufacturing plant that could support the making and distribution of other vaccines in the future. Now, those aspirations, as well as the fate of similar vaccine manufacturing initiatives in Africa, are under threat. Some experts speculate that the now widespread availability of free SARS-CoV-2 vaccine doses on the continent might have created a sense of complacency. Additionally, many African countries continue to face challenges with last-mile vaccine distribution and administration, including cold chain logistics and healthcare staff shortages. According to the Africa CDC, two-thirds of the continent’s vaccine supply has been administered but only about 16% of the continent’s population is fully vaccinated against COVID-19.
Meanwhile, international aid commitments from many wealthy nations—including several in the European Union, the UK, and the US—to help low- and middle-income countries (LMICs) purchase vaccines or overcome logistical challenges have recently slowed or evaporated. The US is co-hosting a second Global COVID-19 Summit on May 12 to spur new commitments and discuss further efforts to deliver vaccines to “everyone, everywhere.” The US Congress is deadlocked over negotiations to authorize additional funding for both domestic and international COVID-19 efforts, and without that show of support, experts are curious whether the US can maintain its leadership and motivate others to make donations. Additionally, many wealthy nations have an excess of vaccine doses as vaccination campaigns wind down. Denmark has said it will destroy 1.1 million SARS-CoV-2 vaccine doses in the coming weeks as they reach their expiration dates and efforts to donate them to LMICs have failed.
In related news, the UN Committee on the Elimination of Racial Discrimination (CERD), a body of experts that monitors the implementation of the International Convention on the Elimination of All Forms of Racial Discrimination, released a strongly worded statement last week expressing concern that global vaccine equity and the pandemic’s disproportionate impact on people of African and Asian descent, as well as those belonging to national or ethnic minorities, Roma communities, Indigenous Peoples, are in part attributable to “the historic racial injustices of slavery and colonialism that remain largely unaccounted for today.” CERD also urged nations to support a proposal at the World Trade Organization (WTO) to temporarily waive intellectual property rights on COVID-19 vaccines and therapies.
OMICRON-SPECIFIC VACCINES Global vaccine manufacturers are racing to update their vaccines to target the Omicron variant of concern (VOC) and its subvariant descendants. Although booster shots have been fairly successful in preventing severe outcomes from COVID-19, they have not been nearly as effective in preventing infection altogether as Omicron has swept many areas of the world. Moderna announced that it is aiming for a Fall release of its Omicron-specific mRNA vaccine booster. The company earlier this year began trialing various formulations of Omicron-specific candidates and stated recently they have identified at least 2 strong candidates for further trials and possible authorization. Pfizer also is set to launch human trials for its own Omicron-specific mRNA vaccine candidates soon.
In China—where surges in Omicron cases have caused lockdowns in several major cities—vaccine manufacturers already have large-scale trials underway in an attempt to protect larger swaths of the population against Omicron subvariants. China’s Sinopharm has produced an inactivated vaccine specific to the Omicron VOC and is currently testing it in a large clinical trial in Hangzhou province. A similar trial to evaluate Omicron-specific booster efficacy also is approved to begin in Hong Kong. Elsewhere, China’s Abogen Biosciences has obtained approval from the United Arab Emirates to begin a clinical trial there using the company’s Omicron-specific mRNA vaccine. When they are available, data from all of these trials will be essential to determine whether we can better protect the world’s population against current and future Omicron subvariants.
by ponchi101 Ok. AITA: Sure, no GOV can mandate you to get vaccinated. But you then have to accept that other people have the right to NOT let you come into their business/restaurant/office/place of work or contact with them.
It has got to cut both ways.
by ti-amie
ponchi101 wrote: ↑Tue May 03, 2022 6:23 pm
Ok. AITA: Sure, no GOV can mandate you to get vaccinated. But you then have to accept that other people have the right to NOT let you come into their business/restaurant/office/place of work or contact with them.
It has got to cut both ways.
NTA
by ti-amie So far the only side effect of my second booster is a sore arm.
by dryrunguy Here's the latest Situation Report.
::
VISUALIZING 1 MILLION DEATHS In the coming days, the official number of US residents who have died of COVID-19 will pass 1 million, although some estimate that threshold has already been exceeded. Globally, the WHO estimates about 15 million people have died due to causes directly or indirectly related to the pandemic. News reporting is applying different lenses to this immense loss, at levels difficult for humans to comprehend. Axios presents a timeline of the pandemic, comparing the numbers of deaths to historical events. Forbes published a series of photos accompanied by various pandemic-related facts. STAT breaks down the death toll into “5 different pandemics,” based on when and where you lived and who you were. The Washington Post notes that at least 9 million people nationwide lost a spouse, parent, grandparent, child, sibling, or friend to COVID-19 and tells the stories of several of those people. On May 9, the Washington National Cathedral rang its largest bell 1,000 times, one toll for every 1,000 US residents who have died of COVID-19. An additional toll rang out to acknowledge the ongoing threats of the virus, the final time the bell will ring to memorialize the pandemic. The White House is expected to commemorate the moment when the nation officially passes 1 million deaths.
US FALL/WINTER SURGE PREDICTIONS The US government has begun to prepare the public for and warn the US Congress of a potential surge in COVID-19 cases this coming fall and winter. Some experts predict as many as 100 million new COVID-19 cases will occur during the colder months. The estimate is based on several variables, including waning immunity, a growing sense of relaxation about the pandemic, and the potential for new variants. On May 8, White House COVID-19 Response Coordinator Dr. Ashish Jha called on Congress to authorize US$22.5 billion for vaccines, treatments, and diagnostics. The White House’s original request of US$30 billion dollars was pared down to US$10 billion in what appeared to be a compromise before negotiations hit a wall over US-Mexico border public health policies. Without additional funding, the administration has said it likely will run out of SARS-CoV-2 vaccines if the nation moves forward with authorizations for a second booster dose for all adults. White House documents suggest the country would need an additional 87 million vaccine doses for adult boosters and an additional 5 million for boosters for children, if authorized. The administration is discussing contingency plans if vaccine supplies run short, with some reporting that boosters could be limited to high-risk groups in the fall if additional funding is not secured.
BOOSTER DOSE EFFECTIVENESS A fourth dose of SARS-CoV-2 vaccine significantly boosts immune protection, according to data from the COV-BOOST subtrial published in The Lancet Infectious Diseases. The study evaluated antibody and cellular immune responses of a fourth dose of either Pfizer-BioNTech or Moderna, administered to participants who previously received 3 doses of Pfizer-BioNTech or 2 doses of AstraZeneca-Oxford and 1 dose of Pfizer-BioNTech. Participants who received the Moderna booster saw a 16-fold increase in anti-spike IgG titers, the metric used in the study for immunogenicity, while Pfizer-BioNTech recipients’ levels increased 12-fold. Compared to 28 days after the third dose, the Moderna booster more than doubled antibody levels and the Pfizer-BioNTech booster increased levels more than 1.5 times. Participants who received 3 doses of Pfizer-BioNTech and a Moderna booster exhibited significantly higher T-cell responses 14 days after the fourth dose compared to 28 days after the third dose, whereas participants who received other vaccine combinations all exhibited similar T-cell responses at the same time point. The researchers suggested there may be a ceiling for antibody levels with mRNA boosters.
Several studies also have evaluated vaccine effectiveness of third dose boosters to Omicron. Researchers with Sweden’s Skane University Hospital conducted a vaccine-registry study across 3 periods of variant dominance: Omicron BA.1, transition period, and Omicron BA.2 beginning in the last week of 2021 through week 11 of 2022. Pfizer-BioNTech, Moderna, and AstraZeneca-Oxford vaccines were used in the vaccination program, but Pfizer-BioNTech represented 77% of all administered doses. A total of 593 severe cases were documented during the period, representing 65, 78, and 56 cases each week for the corresponding periods of BA.1, transition, and BA.2 dominance. Severe cases were older during the BA.2 period and had a more even sex distribution compared to those recorded during the BA.1 period. Following 3 doses, vaccine effectiveness remained above 80% through the study period, but decreased from 90% to 54% during BA.2 in participants who received 2 vaccine doses regardless of age, sex, or chronic conditions.
A second study, also published in Eurosurveillance, included a subset of 20 participants from a previous study comparing levels of plaque reduction neutralization test (PRNT) antibodies against the wild-type and BA.1 SARS-CoV-2 variants. Participants included previously infected and infection-naive individuals who were vaccinated with 3 doses of Pfizer-BioNTech or CoronaVac, or 2 doses of CoronaVac and 1 dose of Pfizer-BioNTech, as well as unvaccinated individuals who were previously infected. The researchers, who noted that there are no universally even a single dose of vaccine in participants previously infected elicited higher PRNT antibody responses than even 3 doses of the respective vaccine in infection naive individuals. Breakthrough infections with either BA.1 or BA.2 in previously vaccinated participants appeared to provide broad cross-neutralization against a range of variants of concern. Notably, BA.2 infection in unvaccinated participants produced low levels of PRNT antibody responses indicating they could remain susceptible to infection from other variants.
A third study, detailed in last week’s Morbidity and Mortality Weekly Report, analyzed surveillance and vaccination data during Omicron dominance from 15,000 nursing homes in the beginning of 2022 to estimate relative vaccine effectiveness against infection for any additional primary or booster dose compared to primary series vaccination, defined as 2 shots of Pfizer-BioNTech or 1 shot of J&J-Janssen. A relative vaccine effectiveness of an additional primary or booster dose was determined to be 46.9% against infection, suggesting that an additional or booster dose provides greater protection against Omicron infection than primary series vaccination alone. While weekly case rates decreased among all vaccination status groups during the study period, cases were consistently lower among residents with an additional primary or booster dose compared to those with primary series vaccination only or were unvaccinated, suggesting additional doses should be administered to all skilled nursing facility residents when they are eligible.
LONG COVID As many wealthy nations move into recovery phases of the COVID-19 pandemic, some are saying the next crisis will be addressing the millions of people worldwide who experience post-acute sequelae of COVID-19 (PASC), commonly known as long COVID. Researchers are continuing work to characterize the condition, attempting to answer questions including who might be more susceptible to long-term symptoms, how long symptoms might last, what treatments could provide some relief, and the impact long COVID symptoms have on long-term health. Globally, estimates range from 10% to 80% of COVID-19 survivors who experience at least 1 lasting symptom. Some estimate as many as 1 billion people worldwide could suffer from the poorly understood condition over the next few years. In the US, as many as 24 million people have experienced long-COVID symptoms since the start of the pandemic.
Growing evidence suggests that getting vaccinated against COVID-19 could reduce the risk of developing long COVID, although more research is needed to definitively assess the impact. And a recently reported case series posted to the preprint server Research Square shows some evidence that individuals experiencing long COVID symptoms might be able to use Pfizer’s antiviral treatment Paxlovid as a therapy for the condition. Because Paxlovid is authorized only for people who have recently tested positive for the virus, clinical trials are needed to more thoroughly assess its potential to treat long COVID.
J&J-JANSSEN VACCINE The US FDA on May 5 limited the authorized uses of J&J-Janssen’s single-dose SARS-CoV-2 vaccine to only certain adults who are unable or unwilling to get vaccinated with another approved or authorized vaccine. The agency made the decision based on an updated analysis on the risk of J&J-Janssen vaccine recipients experiencing thrombosis with thrombocytopenia syndrome (TTS), a rare but potentially life-threatening condition characterized by blood clots and low platelet counts that occurs 1-2 weeks post-vaccination. FDA officials determined that the known and potential benefits of the J&J-Janssen vaccine outweigh its risks for individuals aged 18 and older who cannot access other vaccines; for whom other authorized or approved vaccines are not clinically appropriate, like those who have had an allergic reaction to another SARS-CoV-2 vaccine; or who would not otherwise get vaccinated with an mRNA vaccine from Pfizer-BioNTech or Moderna. Out of about 18 million doses administered in the US, the FDA has identified 60 cases of TTS, including 9 deaths.
In April 2021, the FDA temporarily paused the use of the J&J-Janssen vaccine after the risk of TTS was identified, lowering vaccine confidence in and demand for the vaccine. Then in December 2021, the US CDC recommended individuals receive one of the mRNA shots instead of the J&J-Janssen vaccine. This most recent move could further diminish confidence in the vaccine, especially in low- and middle-income countries (LMICs) where the single-shot vaccine originally held promise. In response, J&J said the vaccine’s benefits outweigh its risks, especially when compared to being unvaccinated. Experts note that COVID-19 also carries a risk of serious or fatal blood clots, although a different type than those associated with the J&J-Janssen vaccine.
GLOBAL VACCINE & TREATMENT ACCESS COVAX has shipped nearly 1.5 billion SARS-CoV-2 vaccine doses to 145 countries worldwide and says it has access to enough doses to help all countries meet their national vaccination targets. While vaccine supplies have ramped up over the past few months, lower demand for the vaccines and complex logistics surrounding their delivery and administration pose ongoing challenges to getting vaccinations in arms. Global efforts have focused primarily on vaccines, but demand for COVID-19 antiviral treatments, diagnostics, and other medical supplies, such as oxygen, is rising in low- and middle-income countries (LMICs). Critically, COVID-19 treatments must be started within 5 days of initial symptoms, and infections must first be confirmed with testing. Notably, only about 20% of the 5.7 billion SARS-CoV-2 tests conducted globally have been in LMICs—and only 0.4% in low-income nations—according to the WHO-supported ACT Accelerator.
Many global health experts say the obstacles and inequities countries face today are highly—and tragically—reminiscent of those that prohibited the widespread use of HIV therapeutics in LMICs in the early 2000s. Some experts say the concentration of vaccine and medical supply manufacturers centered in only a few high-income countries continues to be a structural driver of inequity. Others are calling on pharmaceutical companies to provide more transparency, technology transfers, and prioritization of LMICs in distribution. Some say additional investments in global organizations such as Gavi, the Vaccine Alliance, would help build off lessons already learned in distributing and administering childhood vaccinations. And still others call for more innovation in the planning and delivery of all immunization services. Notably, an Africa CDC 27-country analysis shows those nations that acted quickly to establish and scale-up vaccination programs saw greater benefit than nations that lagged behind. Additionally, the paper calls on countries to focus on vaccinating the most vulnerable populations to achieve the greatest cost-benefit.
The upcoming second Global COVID-19 Summit is a reminder that even after more than 2 decades of lessons from the HIV epidemic, the global community has a long way to go to resolve inequities during the COVID-19 pandemic and prepare for the next global health emergency. On May 12, national leaders and representatives of private companies, philanthropies, and non-profit organizations will gather for the summit, co-hosted by the US, Belize, Germany, Indonesia and Senegal and aimed at increasing financing for the COVID-19 response in LMICs.
Ahead of the summit, US President Joe Biden called on upper-middle and high-income nations to pledge US$2 billion for COVID-19 therapeutics, such as the antivirals Paxlovid and molnupiravir, and US$1 billion for oxygen supplies. But President Biden—who is scheduled to deliver remarks, possibly virtually—likely will come to the table without additional US support, as the US Congress has yet to agree on additional COVID-19 aid. Administration officials say that without future financing, the US is at a disadvantage when asking other nations to step up their global response efforts and could face challenges in its domestic response. A group of former heads of state and Nobel laureates are calling on the US to immediately authorize US$5 billion for its global COVID-19 response, and activists are urging President Biden to take a stronger international leadership role. Congressional Democrats were working to pass new COVID-19 spending attached to a proposal for nearly US$40 billion in new Ukraine aid. But after continued disagreement over public health policies on the US-Mexico border, Democrats have uncoupled the proposal for an additional US$10 billion in new COVID-19 spending from the Ukraine aid and put it on a separate track. In a statement, President Biden conceded that new COVID-19 funding could wait but urged Congress to act quickly on the additional pandemic aid.
WHO HEALTH EMERGENCIES PREPAREDNESS A working group formed to propose ways to strengthen the WHO’s preparedness and response to health emergencies last week released a draft report outlining its recommendations. The 56-page document will be considered by the 75th World Health Assembly convening later this month. The draft report proposes, among other suggestions, recommendations on strengthening the International Health Regulations (IHR); a timeline for the regulations’ possible amendment; an evaluation of the status and future of WHO-supported initiatives such as the Access to COVID-19 Tools Accelerator and vaccine technology transfer hub; and a reconsideration of the acronym for public health emergencies of international concern, PHEIC, which some pronounce as “fake.” Public health experts agree that now is the time to prepare for future pandemics. An editorial in The Lancet calls on individual countries to evaluate their responses to COVID-19, learn from their mistakes, and work to strengthen their health systems, and the editorial board of the Washington Post urges international cooperation to form a global and national early-warning system for new and emerging diseases.
by ponchi101 15 million dead is about 1/500 of the entire world's population, in a span of 2 years. This was not just a flu (or still is not, as this thing continues to roam the planet).
And, my issue with LMIC remains the same. Sure, we don't have the resources to develop the vaccines. But, two years into the pandemic, not one single country in L. America, or any of our Organizations of State, have made plans to manufacture vaccines locally.
I will get my booster around Mid June, just so my GF and I can go back in sync. That would be around 6 months after the 3rd. I gather we will then continue on a 1/2 a year regime, if any.
by ponchi101 I had not noticed this. By decree, here in Colombia, you cannot go into restaurants, bars or other enclosed spaces without showing proof of vaccination.
No (expletive) exceptions. Because, you know, (expletive) your freedoms.
(Totally in agreement, of course)
by Deuce I think pretty much every province in Canada and every state in the U.S. lost the proof of vaccine requirement for restaurants, stores, cinemas, concert halls, and other indoor locations at least a month or two ago. It's good to see that Colombia has more sense.
Is this just for restaurants, or other indoor locations (like stores), as well?
And are masks still required in indoor public places there, as well?
As of this Saturday, I don't think there will be a province or state that still requires masks to be worn in indoor public spaces.
Meanwhile, pretty much all of the doctors, medical experts, infectious disease specialists, etc. who ARE NOT government employees are saying that masks and proof of vaccination should still be required in indoor public spaces.
Because, despite what people are desperately forcing themselves to believe, the COVID-19 virus is still very much alive and circulating and causing many hospitalisations and deaths.
by dryrunguy Here's the latest Situation Report. Haven't read it yet. I have two proposals going. Things are crazy.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 516 million cumulative cases and 6.3 million deaths worldwide as of May 11. The global weekly incidence decreased for the seventh consecutive week, although at a slower pace, down 9% last week compared to a 16% decrease over the previous week. Europe, South-East Asia, and the Eastern Mediterranean regions continued to report decreasing trends in weekly incidence, while the Americas, Western Pacific, and Africa regions reported increasing trends. The increasing trends are being driven by Omicron subvariants. The trend in reported global weekly mortality decreased for a sixth consecutive week, down 23.5% from the previous week.
Global Vaccination
As of May 4, WHO reported 11.65 billion cumulative vaccine doses administered globally, with 5.2 billion individuals receiving at least 1 dose, and 4.7 billion fully vaccinated. Analysis from Our World in Data indicates that the overall trend in global daily vaccinations increased slightly over the past few days—up to 8.6 million per day on May 11 from a recent low of 8 million on May 8*. However, the number of daily doses is at its lowest level since the beginning of March 2021. The trend continues to closely follow that in Asia. Our World in Data estimates that there are 5.16 billion vaccinated individuals worldwide (1+ dose; 65.5% of the global population) and 4.69 billion who are fully vaccinated (59.5% of the global population). A total of 1.9 billion booster doses have been administered globally.
*The average daily doses administered may exhibit a sharp decrease for the most recent data, particularly over the weekend, which indicates effects of reporting delays. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent data.
UNITED STATES
The US CDC is reporting 81.9 million cumulative cases of COVID-19 and 995,747 deaths. The average daily incidence has more than tripled over the past 2 weeks, up from 25,292 new cases per day on March 28 to 78,236 on May 10. The daily mortality is remaining fairly stable, at an average of 326 deaths per day on May 10*. If daily mortality continues at this pace, the cumulative mortality will reach 1 million deaths within the next 12-13 days. Notably, new COVID-19 hospital admissions continue to trend upwards, with an increase of 20% over the past week. New cases are being driven by the BA.2 subvariant of Omicron, with an increasing proportion of cases due to the BA.2.12.1 sublineage.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US Vaccination
The US has administered 580 million cumulative doses of SARS-CoV-2 vaccines. After a slight increase starting in late March, following US FDA authorization of a second booster dose, daily vaccinations are once again declining. A total of 258 million individuals have received at least 1 vaccine dose, which corresponds to 77.8% of the entire US population. Among adults, 89.2% have received at least 1 dose, as well as 27.8 million children under the age of 18. A total of 220.3 million individuals are fully vaccinated**, which corresponds to 66.3% of the total population. Approximately 76.3% of adults are fully vaccinated, as well as 23.3 million children under the age of 18. A total of 101.5 million individuals have received an additional or booster dose. This corresponds to 46.1% of fully vaccinated individuals, including 68.9% of fully vaccinated adults aged 65 years or older. Only 49.4% of individuals eligible for a first booster dose have received one.
*Due to delays in reporting, estimates for the average daily doses administered are less accurate for the most recent several days.
**Full original course of the vaccine, not including additional or booster doses.
SECOND GLOBAL COVID-19 SUMMIT This morning, US President Joe Biden marked 1 million US deaths from COVID-19, saying the nation “must not grow numb to such sorrow.” US flags will be flown at half-staff to remember those lost in the pandemic. Later today at the second Global COVID-19 Summit, President Biden is expected to forcefully call on Congress to take urgent action to pass additional COVID-19 funding, according to unnamed administration officials. A US$10 billion proposal for more funding is stalled in Congress over disagreements regarding pandemic-related immigration policies. Notably, that package only includes money for the domestic response after lawmakers stripped the proposal of global COVID-19 aid in March. The summit—co-hosted by the US, Belize, Germany, Indonesia, and Senegal—is aimed at securing new investments for pandemic responses in low- and middle-income countries (LMICs), even as momentum for vaccinating the world dwindles. Only 16% of people in low-income countries have received at least 1 dose of vaccine, whereas 65.5% of the total world population has received at least 1 dose.
The global COVID-19 response needs approximately US$17 billion this year, according to the WHO, but only about US$2 billion has been secured. With no new funding from Congress for international efforts, President Biden is not expected to make significant pledges at the summit. Other nations—including France, Germany, Canada, and the UK—could pledge additional funds. The US is expected to increase its pledge to the new Global Pandemic Preparedness and Health Security fund hosted by the World Bank to US$450 million, up from an initial promise of US$250 million. The US also is expected to offer US$20 million for pilot projects testing the implementation of “test-and-treat” initiatives in LMICs. Additionally, the US will announce that the US NIH will license its stabilized spike protein technology that is critical to manufacturing some types of SARS-CoV-2 vaccines and treatments to companies through the WHO-backed Medicines Patent Pool. On May 11, the White House released a fact sheet on its work to strengthen the global health workforce through a new US$1 billion initiative. While the funding is contained in the President’s Fiscal Year 2023 Budget, Congress must first approve the funds.
NORTH KOREA Throughout the pandemic, North Korea has claimed it has never experienced a single case of COVID-19. That assertion has long been widely doubted by international experts who have dubbed the country’s public health measures, including sealing its borders, unsustainable. However, until now, experts have conceded that there has not been any signs of a large-scale outbreak in the country. Today, North Korea announced for the first time that it is in the midst of a COVID-19 outbreak with cases in Pyongyang attributed to a lapse in public health measures that allowed the BA.2 Omicron subvariant to sneak in. The outbreak has led to sweeping new public health measures, including health system mobilization, masking among officials, and increased movement limitations among the public. Experts have voiced concern over the newly acknowledged outbreak because of North Korea’s fragile healthcare system and refusal to initiate SARS-CoV-2 vaccinations thus far. Foreign nations have offered or are considering offers of aid to North Korea, including China and South Korea, but it is uncertain if North Korea will accept such offers of assistance at this time.
CHINA’S ZERO-COVID POLICY China’s strict “zero-COVID” approach has been controversial among international public health experts due to its adverse effects on human rights and the Chinese economy, but censure increased when WHO Director-General Dr. Tedros Adhanom Ghebreyesus on May 10 criticized the strategy as unsustainable due to the transmissibility of Omicron. Chinese officials have called the WHO Director-General’s remarks “irresponsible” and, for now, plan to continue the current approach of strict lockdowns, including limiting movement of residents. Censorship efforts on Weibo and WeChat, Chinese social media platforms, have now been deployed to suppress access to Dr. Tedros’s comments. Adding to the debate, a new modeling study published in Nature Medicine asserts that a relaxation of measures in China leading to a wave of Omicron cases could overwhelm the existing healthcare system and currently insufficient population immunity, leading to more than 1.5 million deaths nationwide.
BREAKTHROUGH CASES Cases of COVID-19 are beginning to rise again in the United States, and hospitalizations also are on the rise, especially in areas such as New England and Puerto Rico. Previous surges have been characterized by much higher rates of hospitalization and death among unvaccinated populations when compared to the vaccinated. However, the gap between these 2 groups is narrowing. Breakthrough infections among the vaccinated have become increasingly common, and elderly populations seem to be bearing the brunt of this trend. Many US residents aged 65 and older received their first 2 primary series vaccine doses approximately 1 year ago in the summer of 2021, and nearly one-third have yet to receive their first booster dose. As a result, the Delta surge in 2021 was characterized by younger populations being at higher risk of hospitalization and death, while this year’s Omicron surge was marked by a shift back toward elderly populations once again being at a higher risk.
However, elderly populations will not be the only group at risk for breakthrough infections if a new surge occurs later this year. Vaccine uptake has slowed in the US, and less than half of all eligible US residents have received their first booster dose. Waning immunity, slow vaccine and booster uptake, increasingly transmissible SARS-CoV-2 variants, and a lack of pandemic funding in the US could put nearly 100 million individuals at risk of COVID-19 later this year.
US HOSPITAL STRAIN COVID-19 caseloads in the United States are rising again and are projected to continue rising over the next several weeks. Approximately 15,000 COVID-19 positive patients are currently receiving care in US hospitals, and about 2,600 new patients are being admitted daily. This rate of new hospitalizations represents a nearly 20% increase over last week. Additionally, about 5,000 new deaths are anticipated over the next 2 weeks, as the nation rapidly approaches the harrowing number of 1 million dead from the pandemic. These increasing numbers are especially troubling because more than half of US adults have at least one underlying health condition that puts them at an increased risk of hospitalization or death.
The increase in COVID-19 caseloads is further complicated by a lack of federal funding to treat uninsured COVID-19 positive patients. A US$20 billion program that covered testing, treatment, and vaccination for uninsured individuals has run out of money, and Medicaid coverage for certain individuals promised under a 2020 coronavirus relief bill could soon end. According to a new analysis from the Kaiser Family Foundation, between 5.3 million and 14.2 million people could lose Medicaid coverage when the nation’s public health emergency ends. Once that declaration ends, states will begin removing people no longer eligible for Medicaid from the program, a move that was prohibited under the 2020 bill. Even the new test-to-treat initiative, which provides treatment using federally funded doses of Paxlovid, could become inaccessible for many due to the costs associated with necessary medical consultations. Though the nation came close to universal health coverage for COVID-19 during the height of the pandemic, it appears those safety nets are drying up, putting many US residents at risk of forgoing necessary healthcare and experiencing significant financial hardships due to rising costs.
MASK MANDATES Despite the recent rise in COVID-19 cases across the country, localities and federal authorities have generally not reinstated mask mandates, instead recommending the measure in appropriate circumstances, such as crowded events or public indoor spaces. Several school districts across the country—including some in North Carolina, Massachusetts, Maine, New Jersey, and Pennsylvania—are the exceptions, reinstating mask mandates for staff and students. Some authorities attribute the move away from mandates to a lack of desire among the public to return to masking, which could result in a lack of compliance with the public health tactic. Experts also have noted that while cases are rising, protection from severe disease due to vaccination has remained strong and health systems are not currently overwhelmed; however, if metrics related to those outcomes were to change, perhaps a return to mask mandates would be more appropriate.
Additionally, recent legal challenges to public health measures, such as the overturned federal mask mandate for transit systems, also serve as a deterrent to reinstating mitigation requirements. Some experts worry that the shift away from mask mandates came too soon and contributes to inequity in the COVID-19 response with those who are immunocompromised, children too young to be vaccinated, low-income workers, and communities of color bearing the brunt of the consequences of lifted mandates. Others have also voiced concerns that the decisions to drop pandemic requirements could be politically motivated as midterm elections approach.
VACCINE QUALITY CONTROL INVESTIGATION Emergent BioSolutions, which was contracted by the US government to produce hundreds of millions of SARS-CoV-2 vaccine doses, last year concealed quality control problems from US FDA inspectors weeks prior to announcements that the company destroyed millions of doses due to a contamination incident, according to a joint report from the US House Committee on Oversight and Reform and the US House Select Subcommittee on the Coronavirus Crisis. The yearlong investigation uncovered evidence showing that 400 million doses of SARS-CoV-2 vaccines—significantly more than the 75 million previously revealed—were destroyed because of quality control failures. Emergent disputes allegations it intentionally misled FDA investigators and the claim that 400 million vaccine doses were rendered unusable. Despite regulatory concerns over the company’s SARS-CoV-2 vaccine production, Emergent maintains a federal contract to develop anthrax vaccines.
US FIREARM DEATHS Firearm deaths are a continuing and growing public health problem in the United States. During the first year of the COVID-19 pandemic, the firearm homicide rate in the US reached its highest level since 1994, according to analysis published in the CDC’s Vital Signs. In 2020, 79% of all homicides and 53% of all suicides in the US involved guns, with the firearm homicide rate increasing about 35% from 2019 to 2020 and the firearm suicide rate remaining relatively stable but high. Notably, firearm-related deaths increased disparities along racial, ethnic, and income divides, but no group was affected more than Black people. Black boys and young men ages 10 to 24 had firearm homicide rates 21 times that of White males of the same ages. Counties with the highest poverty level in 2020 had firearm homicide rates 4.5 times as high and firearm suicide rates 1.3 times as high as counties with the lowest poverty level. The study did not examine reasons for the dramatic increase in firearm homicide rate but recognized the reasons likely are complex. The CDC acknowledged stressors associated with the COVID-19 pandemic—including disruptions and changes to services and education, mental stress, social isolation, and economic stressors—could have contributed to the increase.
Another study—published May 9 as a research letter in JAMA Internal Medicine—also blames the COVID-19 pandemic for racial and ethnic disparities in estimated excess deaths from external causes between March and December 2020. The researchers, led by University of California scientists, suggest that structural racism is the fundamental cause of these disparities, but also propose the opioid epidemic contributed to higher rates of murder, suicide, vehicle crashes, and drug overdoses among American Indian/Alaska Native and Black individuals than among White and Asian/Pacific Islander individuals. Both of the studies underscore the urgency of addressing structural determinants of violence, mental health, substance abuse, and transportation safety, particularly among racial and ethnic minority groups.
If you or someone you know is considering suicide, contact the National Suicide Prevention Lifeline at 1-800-273-8255 (Español: 1-888-628-9454; deaf and hard of hearing: 1-800-799-4889) or the Crisis Text Line by texting HOME to 741741.
BARICITINIB The US FDA on May 10 granted full approval to Lilly and Incyte's Olumiant (baricitinib) for the treatment of COVID-19 in hospitalized adults requiring supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO). The FDA first authorized the drug for certain COVID-19 patients in November 2020, and it will continue to be available under Emergency Use Authorization (EUA) for hospitalized pediatric patients aged 2 to less than 18 years who require various forms of oxygen support. Baricitinib, which is already approved to treat moderate-to-severe rheumatoid arthritis, is a Janus kinase (JAK) inhibitor, a class of drug that can modulate immune cell function and the production of blood cell components. According to Lilly, nearly 1 million COVID-19 patients in about 15 countries have been treated with baricitinib.
RESEARCH ROUNDUP The research roundup provides quick synopses of COVID-19-related research.
From The Lancet Respiratory Medicine, a study of nearly 1,200 individuals hospitalized with COVID-19 in Wuhan, China, followed up at 6 months, 12 months, and 2 years post-discharge to determine the persistent health effects of COVID-19. While physical and mental health improved over time, 68% of participants reported experiencing at least 1 original COVID-1 symptom at 6 months, and 55% reported at least 1 original symptom 2 years later. Around half of participants had symptoms of long COVID such as fatigue and sleep difficulties at 2 years, and those participants reported poorer quality of life, reduced ability to exercise, more mental health problems, and increased use of healthcare services than those without long COVID symptoms. Additionally, recovered patients tended to be in poorer health 2 years after discharge compared with the general population.
From JAMA Psychiatry, a cohort study of data from more than 8 million adults in England quantifying the risks of new-onset neuropsychiatric conditions and new neuropsychiatric medication prescriptions after discharge from hospitalization due to COVID-19 or other severe acute respiratory infections (SARI) during the pandemic. Relative to the general population, the COVID-19 and SARI survivors were at a higher risk of subsequent diagnosis of neuropsychiatric conditions, but the absolute risks were low. There were no significant differences in rates of newly diagnosed disorders or new prescriptions when the SARI and COVID-19 survivor groups were compared. The researchers posit that disease severity, not the causative agent, could be more strongly associated with elevated risks of neuropsychiatric disorders following recovery from severe respiratory disease.
From the New England Journal of Medicine, a study examining the effectiveness of the 2-dose primary series of the Pfizer-BioNTech vaccine and 2 doses of the J&J-Janssen vaccine against the SARS-CoV-2 Omicron variant. This study used a test-negative design to measure vaccine effectiveness among individuals in South Africa. The researchers note that after 2 doses, both vaccines were equally effective against severe disease from the Omicron variant, underlining the importance of continued vaccination campaigns.
From the New England Journal of Medicine, a study examining the safety and efficacy of a plant-based adjuvanted SARS-CoV-2 vaccine. The Phase 3 randomized, placebo-controlled trial included 24,141 participants and showed that the tested vaccine, CoVLP+ASO3, was effective against multiple SARS-CoV-2 variants. The study reported 69.5% efficacy in preventing symptomatic infection and 78.8% efficacy in protecting against moderate-to-severe disease.
From the New England Journal of Medicine, a study examining the efficacy and confirming the safety of the experimental ZF2001 vaccine. The randomized, placebo-controlled trial included 28,873 adult participants in Uzbekistan, Indonesia, Pakistan, Ecuador, and China. The safety analysis of the 3-dose regimen concluded it is safe. Additionally, the researchers found that the vaccine efficacy of the full regimen at 6 months was 75.7% against symptomatic COVID-19, 87.6% against severe-to-critical disease, and 86.5% against death.
From The Lancet Regional Health, a study examining the clinical characteristics of maternal COVID-19 deaths that occured in Latin America between March 1, 2020, and November 29, 2021. The observational study looked at maternal deaths across 8 Latin American countries, for a total of 447 deaths. The study provides an important clinical picture of maternal health in the region during the COVID-19 pandemic and emphasizes challenges including access to intensive care.
From Open Forum Infectious Diseases, a study examining the impact of SARS-CoV-2 vaccination on post-acute sequelae of COVID-19 (PASC). This retrospective study used data from 1,578,719 patients to match a pool of 25,225 patients who completed a primary series vaccination with a similar pool of patients who had not received complete vaccination. The study found that complete vaccination was protective against several prolonged COVID-19 symptoms tied to PASC.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
BA.4/BA.5 SUBVARIANTS On May 12, the European Centre for Disease Prevention and Control (ECDC) reclassified the Omicron BA.4 and BA.5 sublineages from variants of interest to variants of concern (VOC). BA.4 and BA.5 were first identified in South Africa in January and February 2022, respectively. Since their identification, they have spread to other parts of the world, including to Portugal, where BA.4/5 currently account for around 37% of cases. Similar to other Omicron subvariants, such as BA.2, BA.4 and BA.5 appear to be significantly more transmissible than previous variants. BA.5 has an estimated growth advantage of 13% over BA.2 under laboratory conditions. Even individuals previously infected with an Omicron variant do not appear to be well protected against infection from BA.4/BA.5. Notably, BA.4/BA.5 contain enough mutations in key sites to evade both naturally acquired immunity and previous vaccinations. Fortunately, BA.4 and BA.5 do not appear to cause more severe disease than previous variants, although more studies are needed to solidify this observation. In the US, BA.2 and BA.2.12.1 still remain the dominant subvariants at this time, but it is likely that more cases will result from BA.4/BA.5 infection as the summer approaches and as more cases are imported from South Africa and Europe.
VACCINE BOOSTERS FOR CHILDREN The US FDA today authorized a booster dose of the Pfizer-BioNTech SARS-CoV-2 vaccine for children aged 5 to 11 years, administered at least 5 months after completing the 2-dose primary series. In a statement, the FDA said that although COVID-19 is largely less severe in children than in adults, more children have gotten sick and been hospitalized during the Omicron wave, and the agency acknowledged that children also can experience long-term effects of COVID-19, even after mild disease. The US CDC’s Advisory Committee on Immunization Practices is expected to discuss its recommendations for the booster dose at a meeting on May 19. The FDA has authorized the Pfizer-BioNTech vaccine for use in individuals aged 5 years and older and has approved the vaccine, under the brand name Comirnaty, for those aged 16 years and older. Booster, or third, doses are now authorized for anyone aged 5 years and older. Less than one-third of the 28 million 5- to 11-year-old children in the US have received 2 doses of a SARS-CoV-2 vaccine.
In related news, Moderna last week released data showing its 2-dose SARS-CoV-2 vaccine is safe and effective in inducing strong immune responses and preventing COVID-19 in children aged 6 to 11 years. The data, from an ongoing Phase 2/3 clinical trial, were published May 11 in the New England Journal of Medicine (NEJM). Also last week, Moderna submitted a request to the FDA for emergency use authorization (EUA) of its vaccine for children ages 6 to 11 years. The company already has submitted requests for its vaccine to be authorized for children 6 months to 6 years old, as well as adolescents. An FDA advisory committee is expected to discuss updates to the EUAs of both the Moderna and Pfizer-BioNTech vaccines to include younger populations at upcoming meetings in June.
SEVERE ACUTE HEPATITIS IN CHILDREN Growing evidence suggests fragments of SARS-CoV-2 can linger in the gastrointestinal tract for months after acute infection. Some researchers believe these viral “ghosts” could be associated with post-acute sequelae of COVID-19 (PASC), often called long COVID, but more research is needed to draw firm conclusions. Additionally, researchers are examining whether these viral reservoirs could be associated with hundreds of cases of severe acute hepatitis cases of unknown origin among young children. At least 450 children in 20 countries have been diagnosed, 11 have died, and more than 2 dozen have received liver transplants. Most of the children with severe acute hepatitis do not show active SARS-CoV-2 infection and are unvaccinated. However, between 75-95% of cases in the US and UK have tested positive for SARS-CoV-2 antibodies and about 60-70% test positive for adenovirus,a family of viruses that is not known to attack the liver but can cause everything from pinkeye to common colds. These results have led some experts to hypothesize that SARS-CoV-2 and a type of adenovirus could both be culprits.
On May 14, a team led by researchers from Case Western Reserve University Medical School posted a study to medRxiv (preprint) showing that children infected with SARS-CoV-2 were at significantly increased risk of elevated liver enzymes and bilirubin than children who had non-COVID other respiratory infections (ORIs). They theorize that children with severe hepatitis of unknown origin could have recovered from mild or asymptomatic COVID-19, causing SARS-CoV-2 particles to linger in their gastrointestinal tracts. If the children were subsequently infected with an adenovirus or a different virus, the lingering SARS-CoV-2 particles could prompt immune system overreaction leading to high amounts of inflammatory proteins that could then cause liver damage. The researchers suggested that children with severe acute hepatitis be evaluated for SARS-CoV-2 particles in their stool, as more data need to be collected to test the theory.
US EMERGENCY DECLARATION The number of new US COVID-19 cases is at its highest level since November, when the initial Omicron surge began. Experts say the true size of the wave is unknown, but people can expect the number of new cases in their communities to be 5 to 10 times the official counts. Cases—which are being driven by the BA.2 and BA.2.12.1 subvariants—are rising across the nation, but the Northeast and Midwest regions are experiencing surges that are now higher than during last summer’s peak caused by Delta. Most of New York state, including New York City, has moved to or is close to a “high alert” level, under which people are urged to wear masks indoors and take other precautions. Hospitalizations are up nationwide as well, and while the average number of new daily deaths are falling, an average of 260 people continue to die of COVID-19 each day. The US CDC released data showing that more than 1 million people have died with COVID-19 since the beginning of the pandemic.
The administration of US President Joe Biden is expected to extend the COVID-19 public health emergency declaration past mid-July. The declaration allows the US to grant emergency use authorization (EUA) of therapeutics, diagnostics, vaccines, and other medical tools, as well as provide those products at no cost to millions of residents and extend Medicaid benefits to allow millions to receive health coverage. However, the US Congress has stalled on negotiations over new funding to address the virus. While the nation is in a different place in the pandemic than in earlier periods, the government has run out of money to purchase additional vaccine doses, oral antiviral courses, and other treatments, as well as to develop next-generation vaccines and therapies. Without new funding, the government will have to limit access to no-cost vaccines and treatments, and funding for pandemic-era Medicaid coverage already has expired. And soon, those countermeasures will be bought and sold through regular healthcare systems, meaning the costs will be passed on to consumers and the potential for inequitable access widens.
US & AUSTRALIA RESPONSES More than 1 million people have died of COVID-19 in the US since the beginning of the pandemic, more than any other country. For every 100,000 US residents, about 303 people have died of the novel disease, according to the Johns Hopkins University Coronavirus Resource Center. But the death toll did not have to be so high. Many public health experts attribute the pandemic’s impact in the US to underinvestment in public health departments, primary healthcare, and long-term care, making people more vulnerable to the virus. Marginalization made some communities more vulnerable to the virus and its impacts. Political polarization of the pandemic also contributed, as did misinformation regarding vaccines, which is partly to blame for the nation’s relatively low vaccination rate among wealthy countries. According to a new estimate from Brown University and Microsoft AI Health, nearly 319,000 deaths could have been prevented if 100% of US adults were fully vaccinated.
Around the globe, Australia’s death rate is about one-tenth of the rate in the US. In other words, if the US had the same death rate as Australia, 900,000 people might have been saved. One important trait differentiates the US and Australian responses: trust. At the beginning of the epidemic, 76% of Australians said they trusted the healthcare system, compared with about 34% of Americans, and 93% of Australians said they felt supported by their friends, colleagues, or communities. Australia’s leadership worked quickly to translate much higher levels of public trust in science and institutions, as well as interpersonal trust, into action, urging individuals to take steps that would prove vital to protecting themselves and their communities. Early in the pandemic, Australia’s politicians and public health officials—who adopted a “one voice” cooperative approach—moved to close borders; quarantine international travelers; implement isolation, surveillance, and contact tracing tactics; and enforce long-term lockdowns. Unlike the US, Australia’s non-partisan response to the pandemic, national health insurance program, smaller gaps in income inequality, and a concept of “mateship”—of not wanting to let down one’s neighbor—helped the nation comply with public health guidance and vaccination requirements. All of these measures helped Australia weather the pandemic and reach a vaccination rate of more than 95% among people aged 16 years and older, which is proving vital during its latest surge of cases due to the Omicron variant.
NORTH KOREA The Democratic People's Republic of Korea (DPRK), commonly known as North Korea, continues to experience what it says is an “explosive” outbreak of SARS-CoV-2 reporting nearly 1.5 million people have become ill with fever, believed to be COVID-19, and 56 have died since late April. The nation lacks test kits to confirm whether the fevers are due to SARS-CoV-2 infections, and its 26 million people remain unvaccinated. As of today, the nation said at least 663,910 people were in quarantine. North Korea Leader Kim Jong Un, who has berated officials for delays in pandemic responses, this week mobilized the nation’s military to help distribute medications and support healthcare workers to trace potential patients. Experts feel the death toll likely is underreported and will surge over time. The WHO expressed concern over the North Korean outbreak on May 16, saying it is ready to support the country’s pandemic response.
SECOND GLOBAL COVID-19 SUMMIT The second Global COVID-19 Summit—co-hosted by the US, Belize, Germany, Indonesia, and Senegal and held on May 12—garnered new financial commitments totaling US$3.2 billion, including US$2.5 billion for COVID-19 response efforts and US$712 million in new pledges for the pandemic preparedness and global health security financial intermediary fund (FIF) at the World Bank. Leaders from more than 35 nations and representatives of the private sector, philanthropy, and civil society made commitments, both financial and non-financial. Many public health experts praised the meeting’s outcomes for being better than expected, but others expressed concern that complacency played a role in preventing the summit from reaching its goal of raising US$10 billion to support vaccination access and US$3 billion to improve access to treatments and oxygen.
Without new funding from the US Congress, US President Joe Biden only announced relatively small commitments at the meeting. The US pledged an additional US$200 million for the FIF, bringing its total commitment to total US$450 million, as well as US$20 million for pilot projects to bring testing and treatment to low-income countries. Additionally, the US NIH announced it finalized an agreement to share 11 COVID-19-related technologies to the WHO’s COVID-19 Technology Access Pool (C-TAP) and the Medicines Patent Pool (MPP) to help improve access to tools needed to manufacture and develop vaccines, treatments, and tests. However, it is unclear how quickly the deal will result in improved access to existing or new products.
In related news, the G7 Foreign Ministers of Canada, France, Germany, Italy, Japan, the UK, and the US, and the High Representative of the European Union on May 13 endorsed an action plan on COVID-19, with a focus on improving access to, delivery, and production of vaccines, particularly in low-income countries.
US MEAT INDUSTRY In the early stages of the COVID-19 pandemic, the largest meatpackers in the US successfully lobbied members of then-US President Donald Trump’s administration and pushed “baseless” claims of meat shortages to keep their processing plants operating, prioritizing profits over the health of thousands of workers, according to a report based on an investigation conducted by the US House Select Subcommittee on the Coronavirus Crisis. The report alleges meatpacking executives knew the acute risks of COVID-19 to workers in their plants but worked with the Trump administration to force workers to remain on the job. An estimated 334,000 COVID-19 cases nationwide have been tied to meatpacking plants, and at least 269 meatpacking workers died of COVID-19. The investigation, based on a review of 151,000 pages of documents, showed that although meat production slowed to about 60% of normal levels during spring 2020, 4 of the nation’s largest meat processors collectively increased their profits 120% compared with before the pandemic and at least 2 companies significantly increased their pork exports to China during the first 3 quarters of 2020, belying claims of shortages. Meatpacking corporations and trade groups said the report “distorts the truth” of their efforts to protect employees during the pandemic.
AT-HOME VIRAL RESPIRATORY INFECTION TEST The US FDA granted Emergency Use Authorization (EUA) to the first non-prescription, at-home test that can detect various respiratory viral infections. The test—which requires nasal swabs to be collected at home and sent by mail to Labcorp, the test’s manufacturer—can detect influenza A and B (flu), respiratory syncytial virus (RSV), and SARS-CoV-2. Once processed, the user can access their test results via an online portal. This is the first of what many public health experts hope is an expansion of at-home diagnostics.
by ponchi101 So.
The USA, which accounts for roughly 5% of the world population, has 1MM deaths, of about 5MM acknowledged by world authorities as the planet's toll.
Which there is NO WAY can be realistic. it just points out to the level of undercounting around the world. Even with the lousy American health system, and the no-longer-just-an-american-issue of overweight people, the numbers don't match.
Triple that count to 15MM, and it means this thing has killed 1/500 people around the world. Not trivial at all.
by ti-amie
by ponchi101 What measures will be taken? Mask mandates again? Restrictions for people that are not vaccinated?
As I wrote earlier. Here things have relaxed a bit, but proof vaccination is required to go indoors, and people are still wearing their masks when outdoors.
I got a SMS from my health provider. I am scheduled for my 3rd dose on May 28th. Most likely a typo because I already got it, so I will shot up for my 4th.
by ti-amie We just found out that my daughter's sister-in-law has Covid. She went to Florida (!) to visit her in-laws, one of whom is a cancer survivor.
by ponchi101 My sister tested positive again. FOR THE THIRD TIME.
She simply has built no immunity to it. Fortunately, she is vaccinated and boosted. Her symptoms are minor (not like when I had to go to Caracas to help her and my mom).
by ti-amie
This is not much different from what the snake oil salespeople were promoting here though.
^ This is why I am doing everything I can to protect myself from contracting this virus... and why I feel that the growing number of people who have the attitude of "Whatever - I'm going to live my life normally, and if I get it, it's no big deal" are both downright stupid and quite selfish.
by mmmm8 I have two colleagues with completely different backgrounds (woman in early 20s with British roots and man in 40s from LatAM) with very similar and scary long COVID symptoms (inner ear problems, heart palpitations, fatigue, brain fog). The woman had it at the start of the pandemic and the issues still continue. The man's brother, in his early 60s, died suddenly from a heart issue they linked to COVID. Another totally healthy colleague had a mysterious blood clot form 2 years ago that they're now linking to the mild form of COVID he may have had at the very start of the pandemic. Another friend has smell issues now.
I've been a little more relaxed about socializing (maybe more than I should) but am still masking in stores and on transportation.
by atlpam Getting ready to take a commercial flight for the first time since Dec 2019. Excited about my trip but not the air travel. I really wish the mandatory masking in airports & on planes was still in effect. We will be masking, but based on feedback from friends who traveled recently, most people were not.
Wish me luck!
by dmforever i'm not planning on getting on an airplane this summer for the reasons that you've stated here. Good luck and let us know how it goes.
Kevin
by Owendonovan The dropping of mask mandates was as stupid a move with this pandemic as any. I have certainly hardened my feelings towards those not willing to participate in solutions in ending it who contract it. I can't bring myself to hope for the best for those folks, quite the opposite.
by Suliso "Funny" how politicised this issue still is in US. Here we all masked half a year ago, but now we have stopped. Point is not that the latter is right or wrong, but that it's not strongly tied to someone's political spectrum.
by ponchi101 I can still report that people in enclosed spaces (supermarket, shopping malls, etc) are wearing their masks. When we go outside and, for example, are walking towards those places, we don't wear it (at least I don't). 50 Meters before the entrance, I put it on.
My mother is on her way to Buenos Aires today (CCS-Panama-Baires) and she will wear her mask all the way. She can still remember how she felt when she got the virus.
My sister is doing better, but has felt pretty bad for a couple of days.
Preaching to the choir. It is NOT the flu.
by Owendonovan Over 1,000,000 Americans have now died from COVID.
by ponchi101 I can still remember that criminal saying it would "just go away, like magic".
That is what happens when you enter a cult. The consequences can be deadly.
by atlpam I would be surprised if 15% of people in the airport and on the flight were wearing masks. So now the CDC is “recommending” testing before domestic travel. Considering they are also “recommending” masking, I have low expectations that it will have any impact.
Completed an amazing hike in the Columbia River Gorge today in support of the Leukemia & Lymphoma Society after being postponed for 2 years. Planning to enjoy our trip with lots of outdoor activities as we work our way back to Colorado before braving the airports again for our flight home.
by mmmm8
atlpam wrote: ↑Mon May 23, 2022 4:03 am
I would be surprised if 15% of people in the airport and on the flight were wearing masks. So now the CDC is “recommending” testing before domestic travel. Considering they are also “recommending” masking, I have low expectations that it will have any impact.
Completed an amazing hike in the Columbia River Gorge today in support of the Leukemia & Lymphoma Society after being postponed for 2 years. Planning to enjoy our trip with lots of outdoor activities as we work our way back to Colorado before braving the airports again for our flight home.
Thanks for the warning - we are flying this weekend for the first time since the mandate was lifted (short distance so at least we can keep the masks on for the duration of the flight).
LLS is a great organization!
by dryrunguy Here's the latest situation report. Haven't read it yet. (I'm pretty sure I forgot to post the one from Friday. My apologies.)
::
SARS-COV-2 VACCINE FOR YOUNG CHILDREN Three doses of the Pfizer-BioNTech SARS-CoV-2 mRNA vaccine were 80.3% effective at preventing infection among children 6 months to under 5 years of age when the Omicron variant was predominant, according to preliminary data. The companies cautioned that the data are based on only 10 cases diagnosed among the 1,678 study participants by the end of April, a number lower than the study’s 21-case threshold for analysis. The dose for the youngest children is at the 3 mcg level, one-tenth the adult dose, chosen for its tolerability and safety data. The companies plan to complete their submission for emergency use authorization (EUA) of the vaccine for children under age 5 this week.
Hours after the companies released the preliminary data, the US FDA announced its Vaccines and Related Biological Products Advisory Committee (VRBPAC) will meet on June 14 and June 15 to review EUA requests from both Moderna and Pfizer-BioNTech. On June 14, the committee will discuss Moderna’s request for EUA of its SARS-CoV-2 mRNA vaccine for older children and adolescents aged 6 to 17 years, and on June 15, the committee will review the companies’ data on the youngest children. Moderna is requesting EUA for its vaccine for children aged 6 months to 5 years and Pfizer-BioNTech for its vaccine for children aged 6 months to 4 years. The Pfizer-BioNTech vaccine is currently authorized for use among individuals aged 5 years and older and Moderna’s is available for adults aged 18 and older.
Children under 5 are the last group for which the FDA has not yet authorized a SARS-CoV-2 vaccine, and the agency is under increasing pressure to do so. Some parents are eager to vaccinate their children, although many do not plan to vaccinate their children unless required to do so, according to polls. As of May 18, about 35% of US children ages 5 to 11 years had received at least 1 dose of vaccine and 28% had completed the 2-dose series. If the VRBPAC recommends either or both vaccines for young children, the FDA could quickly authorize the vaccines, making it possible toddlers and kindergartners could be eligible to begin receiving their shots by the summer.
US CDC BOOSTER RECOMMENDATIONS Last week, the US CDC Advisory Committee on Immunization Practices (ACIP) expanded SARS-CoV-2 vaccine booster eligibility to include everyone aged 5 years and older. The CDC recommends that children ages 5 to 11 should receive a Pfizer-BioNTech booster, or third, shot 5 months after completing the 2-dose primary series with the same vaccine, the only one currently authorized for use among that age group. In its announcement, the CDC noted that more than 4.8 million children in this age group have been diagnosed with COVID-19, 15,000 have been hospitalized, and at least 180 have died of the disease. The agency said a third dose would help enhance immunity among this age group to help protect against severe disease. Notably, many ACIP members acknowledged that data suggest mRNA SARS-CoV-2 vaccines are really 3-dose primary series vaccines versus 2-dose primary series plus a booster dose.
However, some parents have hesitated to get their children vaccinated, arguing that children have a lower risk of severe disease, despite record numbers of children being hospitalized during the height of the Omicron surge. Additionally, nearly 4,000 children have been diagnosed with multisystem inflammatory syndrome (MIS-C), a rare but potentially severe condition, since the start of the pandemic. Altogether, less than one-third of children in this age group have both doses of the vaccine, leaving them vulnerable to serious illness, according to CDC Director Dr. Rochelle Walensky. Dr. Walensky also announced the CDC strengthened its recommendation that people aged 50 and older and immunocompromised people aged 12 and older “should,” instead of “may,” get a second booster shot (fourth dose) to remain current on their vaccinations and help protect themselves from severe disease as the US experiences a sixth wave of COVID-19.
US MASK RECOMMENDATIONS/MANDATES As of May 19, at least 45% of the US population lived in areas experiencing medium-to-high COVID-19 community levels, meaning people should be wearing masks or considering masking based on their personal risk. COVID-19 community levels are calculated using new COVID-19 hospital admissions and percent of inpatient beds occupied by patients with COVID-19, both lagging indicators of COVID-19 transmission. But the agency’s data on community transmission shows more than 75% of the country is experiencing high or substantial numbers of new cases, suggesting much of the nation should be wearing masks in indoor public spaces and prompting some experts to recommend localities, businesses, and other entities reinstate mask mandates. The 7-day moving average of new daily cases is at 102,940 as of May 22, rising over 100,000 cases for the first time since February.
While no states have reissued mask mandates, the CDC on May 13 reissued its recommendation that people ages 2 and older wear masks while on public transportation and in transit stations, after the federal mandate was struck down by a judge on April 18. Additionally, some school districts are reinstating mask mandates as the number of cases increase among students and staff. Mask mandates have returned to schools in Philadelphia, PA, Brookline, MA, and Providence, RI, in recent days. New York City and most school districts in the Washington, DC-region are not bringing back mask mandates despite having high levels of community transmission. Despite the nationwide increase in cases, many US residents feel the country has moved beyond the pandemic being a crisis, making the reinstatement of public health measures difficult for local and national leaders.
TRAVEL GUIDANCE Ahead of the summer travel season, the US CDC has added new advice regarding testing to their domestic travel guidance page. The agency now recommends that all individuals get tested for COVID-19 3 days or less prior to domestic travel, regardless of vaccination status. Prior to this change, CDC only recommended testing prior to domestic travel for individuals who were not up-to-date on their SARS-CoV-2 vaccinations (ie, primary series and booster if eligible). CDC also now recommends testing after travel if the traveler engaged in higher risk activities, such as being in a crowded space without a well-fitting mask.
In addition to recommendations for domestic travel, CDC requires that individuals aged 2 years and older flying from international locales to the US show documentation of a negative COVID-19 test within 1 day of departure or proof of recovery from COVID-19 in the last 90 days. However, there is massive public pressure, particularly among travel industry businesses, for CDC to remove the international requirement due to the agency’s inability to fully articulate the rationale behind the rule. Attendees of a recent side event at the International Migration Review Forum (IMRF)—including representatives of the International Organization for Migration (IOM), Migration Policy Institute, governments, and non-governmental partners—called for the establishment of common appropriate standards for international travel to reduce confusion and impediment of cross-border mobility while supporting equitable pandemic recovery among nations.
PAXLOVID Following multiple anecdotal reports of symptoms and positive SARS-CoV-2 test results returning among some people who take a 5-day course of the COVID-19 treatment Paxlovid, the US NIH announced last week it in talks with manufacturer Pfizer to study a longer course of the antiviral. More than 660,000 courses of Paxlovid have been administered in the US, and it is unclear how often patients who take the drug experience so-called “Paxlovid rebound.” Experts from the Infectious Diseases Society of America (IDSA) briefed reporters on May 20 about the rebound effect and potential drug interactions, with information on the latter also contained in the organization’s recently updated guidance. While access to Paxlovid has increased in the US over the past several months, some physicians remain reluctant to prescribe the pills. Additionally, access to the treatment in low- and middle-income countries (LMICs) remains scarce due to limited production and affordable pricing. Experts hope that Pfizer’s licensing agreement with the Medicines Patent Pool (MPP) and supply agreement with UNICEF will improve access in LMICs later this year and into next.
ASTRAZENECA-OXFORD VACCINE The European Medicines Agency (EMA) has authorized the AstraZeneca-Oxford SARS-CoV-2 vaccine to be used as a booster (third) dose among adults who have completed the primary 2-dose course or the primary series of an approved mRNA vaccine, according to a company statement. The authorization is based on review by the EMA’s Committee for Medicinal Products for Human Use (CHMP). The AstraZeneca-Oxford vaccine, branded as Vaxzevria and Covishield, has received conditional marketing or emergency use authorization (EUA) in more than 125 countries, as well as emergency use listing (EUL) from the WHO, allowing it to be distributed through the COVAX initiative. The vaccine was AstraZeneca’s second bestseller last year, but sales are expected to fall in 2022 due to setbacks in production, rare but potentially serious adverse events, limited shelf life, global oversupply, and preferences for the mRNA vaccines made by Pfizer-BioNTech and Moderna. AstraZeneca never filed for EUA in the US, and the White House quietly canceled its contract with the company in December. The cancellation, though it saved the government some money, could hurt its global vaccine donation program, which was expected to give tens of millions of those doses to low-income countries.
WHO EUL FOR 11TH SARS-COV-2 VACCINE The WHO last week issued an emergency use listing (EUL) for CONVIDECIA, a SARS-CoV-2 vaccine made by China’s CanSino Biologics. In clinical trials, CONVIDECIA had 58% efficacy against symptomatic infection and 92% efficacy against severe COVID-19, and the single-dose vaccine can be used in adults aged 18 years and older, according to the WHO’s Strategic Advisory Group of Experts on Immunization (SAGE). The vaccine is the 11th SARS-CoV-2 vaccine to receive WHO EUL.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 524.3 million cumulative cases and 6.28 million deaths worldwide as of May 25. The global weekly incidence decreased slightly (-0.8%) over the previous week. The weekly trends are increasing in the Americas (+13.2%) and Western Pacific (+5.7%) regions, while decreasing trends were observed in the remaining 4 regions. The trend in reported global weekly mortality decreased for a seventh consecutive week, down 6% from the previous week. The number of new weekly deaths increased in the Eastern Mediterranean region (+30%) after the region reported major increases in daily incidence over the past couple weeks. The number of new weekly deaths remained stable in the Western Pacific and the Americas regions (both <1%), and decreased in the other 3 regions.
UNITED STATES
The US CDC is reporting 83.4 million cumulative cases of COVID-19 and 1,000,254 deaths. As expected, the cumulative number of COVID-19 deaths surpassed 1 million on May 24. The current average daily incidence continues to increase, up to 104,399 on May 24 from 99,215 new cases per day on May 17. The daily mortality is fairly steady at an average of 288 deaths per day*, and we have not yet observed an increase corresponding to the surge in daily incidence. New COVID-19 hospital admissions continue to trend upwards, with an increase of 14% over the past week. New cases are now being driven by the the BA.2.12.1 sublineage of Omicron (58%), which this week became the predominant variant over the BA.2 subvariant (39%).
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
OMICRON SUBVARIANTS The US recently began averaging more than 100,000 new daily COVID-19 cases for the first time since February. As of the end of last week, 58% of new US cases are caused by the Omicron subvariant known as BA.2.12.1. There is no indication the variant causes more severe disease than previous Omicron variants, but new hospitalizations also are increasing. However, BA.2.12.1—as well as the other Omicron sublineages BA.4 and BA.5, which the European Centre for Disease Control and Prevention (ECDC) have deemed variants of concern and are currently circulating at low levels in the US—are even more transmissible than the BA.1 version of Omicron that caused high caseloads in early 2022. The 3 sublineages also likely are capable of escaping some of the immunity produced by infection with BA.1 and BA.2. The consistent resurgence of viral variants creates challenges to maintaining long-lasting defense against COVID-19, but the best defense against severe disease and death remains staying up-to-date on vaccinations.
US CDC PAXLOVID ADVISORY The US CDC on May 24 issued a Health Alert Network (HAN) Health Advisory to inform healthcare providers and the public about the possible recurrence of COVID-19 following Paxlovid treatment, commonly referred to as “COVID-19 rebound” or “Paxlovid rebound.” Paxlovid, an oral antiviral drug for early-stage treatment of mild-to-moderate COVID-19, was authorized for emergency use in December 2021 for persons aged 12 years and older who are at high risk for progression to severe illness. The drug has shown to reduce the risk of hospitalization and death due to COVID-19. In the advisory, the CDC emphasized that brief recurrence of COVID-19 symptoms could be part of the natural history of infection, regardless of treatment and vaccination status. However, individuals with recurrent symptoms or a new positive viral test are advised to follow current CDC recommendations for isolation by re-isolating for at least 5 days and when fever has resolved for 24 hours.
Today, the administration of US President Joe Biden announced plans to make Paxlovid even more accessible as the nation experiences another surge in new COVID-19 cases. The nation’s first federally supported test-to-treat site opened today in Rhode Island to provide Paxlovid to individuals who test positive. Other test-to-treat sites are expected to open soon in Massachusetts and New York City, and established testing sites across the country will soon be equipped to transition to test-to-treat locations, according to the administration.
LONG COVID/PASC In the third year of the COVID-19 pandemic, researchers are beginning to learn more about post-acute sequelae of SARS-CoV-2 (PASC), commonly known as long COVID. The condition—characterized by a broad range of symptoms lasting anywhere from 4 weeks to 2 years or longer—could prove one of the biggest hurdles to pandemic recovery. Estimates of the proportion of people who have had COVID-19 and continue to experience symptoms range from 5% to 80%, although the WHO puts the range at 10% to 20%. Results from a large study published this week in the US CDC’s Morbidity and Mortality Weekly Report (MMWR) estimates that 1 in 5 COVID-19 survivors aged 18-64 and 1 in 4 survivors aged 65 or older experienced at least 1 of 26 conditions often attributable to long COVID at 30 days and up to 1 year following diagnosis. Both age groups had twice the risk of uninfected people of developing respiratory symptoms or other lung problems, including pulmonary embolism. The older cohort was at greater risk than the younger group to develop kidney failure, neurological conditions, and mental health conditions. The authors of the study, members of the CDC COVID-19 Emergency Response Team, encouraged people who survive COVID-19 to undergo routine assessment for post-COVID conditions.
Another study, published in Nature Medicine on May 23, found that 1 in 8 adults who were hospitalized with COVID-19 developed myocarditis 28 to 60 days post-discharge, and many COVID-19 survivors experienced reduced exercise capacity, lower quality of life, and persistent abnormalities in heart, lung, and kidney exams. The researchers said study participants’ post-COVID conditions were more closely correlated with the severity of their COVID-19 infection, not their underlying health condition prior to infection, and they cautioned these persistent health problems could place a substantial demand on healthcare services in the future, as more people survive COVID-19.
US NIH researchers conducting an ongoing study comparing 189 COVID-19 patients to 120 similar patients who did not have COVID-19 found no indications of underlying cause for the COVID-19 group to have more persistent symptoms. The study, published in the Annals of Internal Medicine, showed no evidence of persistent viral infection, autoimmunity, or abnormal immune activation among long COVID patients. They did note that women and those with a history of anxiety disorder were at increased risk of PASC/long COVID, but they also stressed the findings do not mean the condition is psychological. A third study, published in the Annals of Clinical and Translational Neurology, found that neurological symptoms—including brain fog, numbness/tingling, headache, dizziness, blurred vision, tinnitus, and fatigue—among many of the 52 non-hospitalized COVID-19 patients in the study persisted for nearly 15 months after initial diagnosis. Some symptoms, including variations in heart rate and blood pressure and gastrointestinal problems, increased over time, but loss of taste and smell generally improved. Among the participants, 77% were vaccinated against COVID-19, but vaccination did not have a positive or negative impact on cognitive function or fatigue.
Notably, a large study conducted by the US Department of Veterans Affairs (VA) and published in Nature Medicine showed that SARS-CoV-2 vaccination appears to reduce the risk of lung and blood clot disorders among COVID-19 survivors, but vaccination does little to protect against long-term symptoms among those who had breakthrough infections, about 1% of the study participants. Overall, vaccinated people who had breakthrough infections had lower risks of death (HR=0.66, 95% CI: 0.58, 0.74) and long-term symptoms (HR=0.85, 95% CI: 0.82, 0.89). The data confirm that vaccination strongly protects against serious disease and death but suggest that vaccination prior to infection confers only partial protection against PASC and should not be relied upon as a sole mitigation strategy, the researchers noted. The VA study was conducted prior to the emergence of the Omicron variant, and a preprint study conducted in Japan and posted this week to medRxiv suggests the prevalence of long-term symptoms following infection with Omicron might be less than with other variants.
PFIZER PRICING DEAL During the World Economic Forum annual meeting in Davos, Switzerland, this week, Pfizer pledged to provide 23 of its patented medicines and vaccines to treat infectious diseases, certain cancers, and rare and inflammatory diseases—including those for COVID-19—at not-for-profit pricing to 45 lower-income countries. The company’s “An Accord for a Healthier World” also includes future products and is expected to benefit 1.2 billion people. Rwanda, Ghana, Malawi, Senegal, and Uganda are the first nations included in the deal. Haiti, Bangladesh, and Tajikistan also are on the list. Pfizer CEO Albert Bourla said the plan also includes strategies aimed at improving access to diagnostics, technical assistance, and training of healthcare workers. Some advocates welcomed the announcement, while others criticized the effort as being too little, too late.
Also at the meeting, the Serum Institute of India (SII), the world's largest vaccine manufacturer, announced it is looking into establishing a manufacturing plant in Africa. SII CEO Adar Poonawalla said he is working to distribute a draft global treaty to help ensure more equitable access to vaccines and other healthcare during this pandemic and future outbreak emergencies.
PANDEMIC PREPAREDNESS The World Health Assembly (WHA) is meeting this week in Geneva, the first time the WHO decision-making body has met in person since the beginning of the COVID-19 pandemic. On May 24, the WHA approved a report from the Working Group on Preparedness and Response to Health Emergencies that includes a roadmap for the creation of a new instrument for pandemic preparedness and response. The report proposes actions to address critical gaps in prevention, preparedness and response to health emergencies, including pandemics; categorizes 131 recommendations by priority, feasibility, and implementation pathway; and highlights which steps are currently underway. High priority recommendations include recommitment to the binding obligations of the International Health Regulations (IHR). Other priorities include building capacity for local manufacturing with the support of technology transfer and research hubs, international coordination to quickly identify and sound alerts to emerging zoonotic diseases, and expanding regional capacities for genomic sequencing. In June, the Intergovernmental Negotiating Body will meet to discuss the roadmap and recommendations.
The WHA has faced online conspiracy theories regarding the discussion of a pandemic treaty, with misinformation accusing the WHO of attempting to impede national sovereignty. While Member States agreed that a new agreement is needed, negotiations for such an agreement will take years to produce a final draft. The false ideas of the treaty being used to take power from national governments have been popularized by various internet figures and boosted by mainstream politicians. Despite these statements, the WHA remains focused on navigating the end of the COVID-19 pandemic and preparing for the next health emergency.
CHILDHOOD LEARNING LOSS The COVID-19 pandemic caused the greatest disruption to education in history, causing students worldwide to miss an average of 4.5 months of schooling or up to 22 weeks of learning. Many students fell behind in standards of learning, and some developed behavioral or psychological problems. Those students in the poorest countries have been hit hardest, as have disadvantaged and vulnerable children in wealthier nations, exacerbating existing inequities. As school systems and teachers try to get students back on track, some nations are looking to decades of research to inform their COVID-19 responses, with a focus on tutoring, voluntary summer school, and other evidence-based education recovery strategies. Proponents of evidence-informed education encourage more quality research be conducted and urge educators and policymakers to seriously consider the results and implement reforms specific to their settings in order to strengthen education systems. Additionally, they encourage the coupling of education research and continuing education for teachers, making teachers researchers and vice versa. But advocates warn that national, state, and local leaders must act quickly to fill the educational gaps created by school closures during the pandemic.
CHINA Full economic recovery from the COVID-19 pandemic is expected to be a gradual process for China. But the country is taking the matter seriously, with China’s cabinet holding an emergency meeting of more than 100,000 provincial, city, and council leaders to discuss new measures to stabilize the economy. Shanghai, the nation’s financial hub, looks to be making steps toward normalization after dealing with months of severe pandemic prevention restrictions. China continues to pursue a “zero COVID” policy, but increasingly strict control measures are causing tension in some metropolitan areas. The government has used extreme measures, including locking residents in their buildings, relocating thousands of residents to other cities for quarantine, and invading private residences to spray disinfectants. Now, some cities and provinces are instituting regular mass SARS-CoV-2 testing to try to keep the virus at bay. The 99 million residents of Henan Province will be required to take PCR tests every other day as of June, and people in Beijing must test in order to ride the subway or enter any public space. The intense restrictions on personal life and freedom have been a major cause of discontent among younger populations, and many are now seeking to leave China or are protesting the restrictions by refusing to have children. The discontented populations claim they do not want to have children because they feel they could never protect them from an authoritarian regime that has little regard for personal liberties.
RESEARCH ROUNDUP The research roundup provides quick synopses of COVID-19-related research.
From JAMA Network Open, a small cohort study of 50 healthy young and middle-aged individuals examining factors associated with blood levels of anti-SARS-CoV-2 antibodies at 6 months following vaccination. The study found that anti-SARS-CoV-2-specific antibody levels were inversely correlated with bodyweight, body mass index, body fat amount, and body weight to height ratio, sustained up to 6 months post-vaccination. The researchers concluded that young and middle-aged healthy persons with low body weight could wait at least 6 months after finishing a primary 2-dose vaccination series to receive a booster dose.
From The Lancet Respiratory Medicine, a randomized, open-label, controlled clinical trial evaluating the safety and immune response of a heterologous high- or low-dose booster of an adenovirus vector-based SARS-CoV-2 vaccine (CanSino Biologic’s Convidecia) administered via oral aerosolization or a homologous intramuscular vaccination with CoronaVac among Chinese adults who previously received 2 doses of CoronaVac. The researchers found that participants in both the high- and low-dose heterologous booster groups had fewer side effects and higher neutralizing antibody responses compared with the CoronaVac group. The interim analysis serves as a proof of concept for an inhaled aerosolized vaccination, and an additional trial to evaluate the vaccine as a booster is planned.
From eClinicalMedicine, a systematic review of 156 studies published through March 13, 2022, analyzing social media use and attitudes toward and behaviors related to SARS-CoV-2 vaccination. The researchers—from Italy, Serbia, and the US—conclude that public health interventions could effectively use social media platforms to promote vaccine uptake.
From JAMA, a research letter describing a prospective study examining the outcomes of children with multisystem inflammatory syndrome (MIS-C) as a complication of SARS-CoV-2 infection who were evaluated at 12 Israeli hospitals over 16-week periods in each of the Alpha, Delta, and Omicron variant waves. The researchers found that cardiac outcomes were more favorable, fewer children were admitted to intensive care units (ICUs), and median hospital length of stay was shorter during the Omicron wave compared with the Alpha and Delta waves. None of the patients needed mechanical ventilation during the Omicron wave, compared with 8.5% during Alpha and 8.9% during Delta. The results suggest that MIS-C was less severe during the Omicron wave compared with other COVID-19 pandemic waves, a finding that is consistent with other studies.
From BMJ, a retrospective, test-negative, case-control study examining the relative vaccine effectiveness (VE) of a fourth dose of the Pfizer-BioNTech mRNA SARS-CoV-2 vaccine compared with 3 doses over a 10-week span. The study included nearly 97,500 individuals aged 60 and older in Israel. The researchers concluded that a fourth vaccine dose appears to provide additional protection from COVID-19-related severe disease and death but the relative VE of the fourth dose against infection wanes sooner than that of a third dose, peaking at 65% 3 weeks following the booster and falling to 22% at the end of week 10. However, relative VE against severe disease remained high (72%) through the 10-week follow-up, although severe disease was rare among participants who had received 3 or 4 doses.
From The Lancet Oncology, a population-based, test-negative, case-control study examining overall SARS-CoV-2 vaccine effectiveness (VE) against breakthrough infections at 3-6 months after the second dose among people with cancer and a control population in the UK. The researchers found that although SARS-CoV-2 vaccination is effective in most individuals with active or recent cancer, vaccination provides lower levels of protection against infection, hospitalization, and death than in the general population. Additionally, VE wanes more quickly among cancer patients than the general population and is lowest and wanes most quickly in those with lymphoma and leukemia. The researchers encouraged those with active or recent cancer, and especially those with blood cancers, to stay up-to-date on their vaccine doses, in some cases meaning 5 doses.
From Scientific Reports, a longitudinal study evaluating COVID-19 containment strategies across 50 different countries and territories, differentiating between pre-vaccine and vaccinating phases. The ranking shows that countries in Oceania and Asia outperformed countries in other regions on pandemic containment during the pre-vaccine phase, with success related to nonpharmaceutical interventions (NPIs), early action, and policy adjustment when necessary. In the vaccinating phase, the researchers found that maintaining NPIs was the best way to protect populations, providing insight into the effectiveness of various infectious disease containment policies in different regions.
by ponchi101 The pandemic preparedness paragraph looks promising.
by dryrunguy
ponchi101 wrote: ↑Thu May 26, 2022 7:57 pm
The pandemic preparedness paragraph looks promising.
How? They indicate it will take YEARS to produce. I don't see anything promising in that. It's essential. It needs to happen. But we can't wait YEARS for it to come to fruition.
by Deuce Also, it is not possible to prepare anywhere near completely for something which is not understood. COVID-19 is still very much a mystery to the best doctors and scientists, even after more than 2 years.
One could prepare a plan of rather general conduct, I suppose... but nothing specific to an individual virus or bacteria.
ponchi101 wrote: ↑Thu May 26, 2022 7:57 pm
The pandemic preparedness paragraph looks promising.
How? They indicate it will take YEARS to produce. I don't see anything promising in that. It's essential. It needs to happen. But we can't wait YEARS for it to come to fruition.
Yes. And here in Latin America, just for example, years is the usual time-frame. If you put that in the hands of the politicians here, at least a frame of 10 years is to be expected. We have no infrastructure, not to mention the people with the skills, to produce any vaccines.
I said it early in the pandemic. Colombia dismantled ALL of its vaccine production industry about 12 years ago (it was ten when the pandemic started). So, we would have to start from scratch.
And remember: we need to buy Jet Fighters (Colombia and Chile) to protect ourselves and be ready for war. Vaccines can wait.
(I saw it a bit more positive, sorry. It is a bit of a start).
by Deuce .
By the way (again)... the virus has not disappeared...
by ponchi101 Got my second booster. 10 minute deal (if you don't count the 2, 1 hour bus rides).
I expect another strong reaction as with my 1st booster, so tonight might be rough.
Enough people there to believe that Colombians are still taking this seriously and people are getting their shots.
by JazzNU
by JazzNU ^^ Just some food for thought. I know people here have travelled and will travel again in the near future. This is something you should consider when travelling abroad. It's not rare enough of an occurrence that you should ignore the possibility. I personally have friends who were in this situation. Fortunately they were able to extend their stay at the hotel they were already in, but that isn't always the case, and do make sure you consider the additional cost you will incur if this happens.
by Suliso It could have happened before too with some other disease or injury. A co-worker once broke her shoulder while cycling in India...
by Deuce Just (another) reminder that COVID-19 is still very much a dangerous element...
by dryrunguy My apologies for falling behind on the Situation Reports. I have five proposals in the hopper. Here's the latest. Just arrived. Haven't read it yet.
::
SARS-CoV-2 ORIGINS On June 9, the WHO Scientific Advisory Group for the Origins of Novel Pathogens (SAGO) published the first preliminary report from its efforts to determine key analyses necessary to identify the origin of SARS-CoV-2 and future emerging and re-emerging pathogens. While SAGO was not explicitly tasked with identifying the original source of SARS-CoV-2, the report indicates that the available evidence remains insufficient to fully characterize the circumstances around the emergence of the virus. The experts indicate that the available evidence suggests that the closest ancestor of the virus likely circulated in wild bat populations before the spillover event into humans. The report indicates that it is not possible to rule out that the virus escaped from a research laboratory, but additional investigation is required to more fully characterize that scenario. Several SAGO members included a note in the report, however, to emphasize that they identified “no new scientific evidence” to support this theory and did not support continuing this line of investigation.
The report includes a series of recommendations regarding data and analyses that would further support efforts to identify the original source of the COVID-19 pandemic. SAGO recommends further analysis of environmental specimens from the Hunan seafood market and of potential animal and environmental sources to identify the route of SARS-CoV-2 introduction to the market. Additionally, analysis of human respiratory pathogen specimens (eg, influenza, enteroviruses) collected prior to the emergence of COVID-19 could help identify previously undetected SARS-CoV-2 infections. Genetic analysis of infections in wild and livestock animal populations could similarly help identify related coronaviruses or intermediate hosts that may have facilitated spillover into human populations. The SAGO report also highlights the need for these types of analyses regarding the emergence of new SARS-CoV-2 variants. Some independent experts continue to call attention to the lack of transparency by the Chinese government, including restrictions on access to specimens, facilities, and personnel necessary to conduct these investigations.
SAGO also outlines key components of a global framework to guide response activities and investigations into the emergence or re-emergence of future pathogens. This framework largely mirrors SAGO’s calls for additional data related to SARS-CoV-2. Specifically, the group notes the importance of investigating human and animal specimens; interactions between humans, animals, and the environment; genomics and phylogenetics; biosafety and biosecurity systems and processes; and research activities or other human interaction with related pathogens.
ACUTE HEPATITIS & LONG COVID Researchers from Israel published findings from their study on instances of long-term COVID-19 liver manifestation among children. The study, published in the Journal of Pediatric Gastroenterology and Nutrition, involved a retrospective investigation of 5 patients hospitalized in an Israeli children’s hospital. Each of the patients had a confirmed SARS-CoV-2 infection and presented with long-term liver injury stemming from their infection. Two of the patients in the study, both under 6 months of age, presented with acute liver failure, the other 3 patients, ranging between ages 8 and 13 years, presented with acute hepatitis and cholestasis.
This review adds to the growing list of evidence tying post-acute sequelae of COVID-19 (PASC/Long COVID) to cases of acute hepatitis of unknown origin. Last month, multiple technical and news media publications documented an international cohort of children with severe hepatitis. Many experts have suggested that COVID-19 could be a potential source for this unexplained manifestation, considering the lack of apparent epidemiological explanations. The US CDC is examining a series of US cases of acute hepatitis as well, and a recent update indicates that adenovirus type 41 could be a possible causative agent as well. While much has been written about Long COVID, many questions remain, and advocates continue to call for expanded research efforts into explanations and treatments.
US PEDIATRIC VACCINATION Last week, the Biden Administration outlined its SARS-CoV-2 vaccination plans for children under 5 years of age. The current estimates suggest that up to 18 million children may become eligible for SARS-CoV-2 vaccination once the US FDA authorize existing vaccines for emergency use in younger children. The White House has allocated 10 million doses for states to distribute to dispensing sites. Notably, the White House estimates that 85% of the newly eligible pediatric population lives within 5 miles of one of these sites. The allotment of vaccines is approximately even between the Pfizer-BioNTech and Moderna vaccines. Despite a ready supply of vaccines and a plan to make them accessible to a large number of children in this age group, questions remain regarding the willingness of parents and caretakers to get the children vaccinated. In the age group of children from 5-11 years, only one-third of eligible children have received the vaccine.
US TRAVEL RESTRICTIONS On June 12, the US CDC lifted its testing requirement for travelers arriving in the US on flights originating in other countries. In the CDC’s announcement rescinding the policy, CDC Director Dr. Rochelle Walensky noted that the availability of vaccines, therapeutics, and alternative testing options (eg, rapid at-home test kits)—as well as the current prevalence of vaccination coverage in the US—largely render the testing restrictions obsolete, and she emphasized that the CDC continues to recommend full vaccination against SARS-CoV-2, including with the appropriate booster dose/s.
Previously, international air travelers with destinations in the US were required to obtain a negative PCR-based or antigen test within 1 day of departure—or provide documentation of recent recovery from SARS-CoV-2 infection—regardless of vaccination status. The policy was instituted in the final days of the Trump Administration and continued under President Joe Biden. Notably, the restrictions only applied to international air travel and did not cover individuals entering the US via land borders nor domestic air travel. The travel industry, particularly airlines, has long called for the testing requirement to be eliminated, arguing that it was originally instituted at a time when the vast majority of the US was unvaccinated. Additionally, some health officials and other experts have argued that the testing mandate provided little protection for travelers or benefit in terms of slowing domestic transmission or the introduction of new SARS-CoV-2 variants into the US.
US SEROPREVALENCE The US CDC COVID-19 Response Team published updated analysis of infection- and vaccine-induced SARS-CoV-2 seroprevalence in the US. The findings, published in JAMA, are based on more than 2.4 million blood donations collected from individuals aged 16 years and older across all 50 states; Washington, DC; and Puerto Rico from July 2020-December 2021. The research does not include individuals with active SARS-CoV-2 infection or who were suspected COVID-19 cases, and results were weighted by demographic factors, including age, sex, race, and ethnicity.
The researchers observed increases in both infection-induced seroprevalence and combined seroprevalence between May 2021 and December 2021, increasing from 20.2% to 28.8% and 83.3% to 94.7%, respectively. At the end of the timeframe for the study, researchers observed the highest level of infection-induced seroprevalence in multiple demographic groups—including individuals aged 16-29 years (40.0%), non-Hispanic Black individuals (32.5%), and Hispanic individuals (32.5%)—as well as the Midwest (31.7%) and South (33.5%) regions.
Notably, regions with higher vaccine coverage seroprevalence exhibited a significantly smaller increase in infection-induced seroprevalence. In regions with vaccine-induced seroprevalence less than 60%, infection-induced seroprevalence increased by 19.8% over the course of 2021, compared to only 10.6% in regions with vaccine seroprevalence greater than 80%. Despite widespread combined seroprevalence at the end of 2021, the Omicron variant was still able to drive a major surge in early 2022, and the researchers note that this illustrates the transmissibility and immune escape potential of new variants.
BA.4 & BA.5 SUBVARIANTS IN EUROPE The European CDC published an epidemiological update on the emergence and prevalence of the BA.4 and BA.5 sublineages of the SARS-CoV-2 Omicron variant of concern (VOC). The subvariants were first detected in Europe in March, and in May, Portugal was the first European country to report a COVID-19 surge associated with one of the subvariants (BA.5). Notably, Portugal’s daily incidence appeared to peak in late May/early June. While most European countries have reported relatively low prevalence of these subvariants, they represent an increasing proportion of new sequenced specimens in multiple countries over the past several weeks, including Austria, Belgium, Denmark, France, Germany, Ireland, Italy, Netherlands, Spain and Sweden. In particular, the BA.4 and BA.5 subvariants represent more than 25% of sequenced specimens in Belgium over the second half of May, and more than 10% in some communities in Spain. The increasing prevalence of BA.4/BA.5 corresponds to increasing COVID-19 daily incidence in most of those countries as well.
The ECDC projects that BA.4 and BA.5 will become the dominant variants across Europe “in the coming weeks” and that the continent can expect an associated COVID-19 surge like those in the countries noted above. The daily incidence in Europe has increased nearly 30% since June 6, with even larger increases in the UK. While there is “no evidence” these subvariants pose higher risk of severe disease, the ECDC notes that an overall increase in transmission can be associated with subsequent increases in hospitalizations and mortality.
WASTEWATER SURVEILLANCE Researchers from the University of Illinois and University of Florida published (preprint) findings from a study on the implementation of neighborhood-scale SARS-CoV-2 wastewater surveillance systems. The COVID-19 pandemic has popularized wastewater surveillance as a tool to provide early warning of impending outbreaks; however, most of these efforts have focused on large-scale sewer systems. Neighborhood-scale systems can provide more targeted early warning capacity, but as the catchment population decreases, the volume of fecal matter is less consistent, which can make it more difficult to analyze the concentration of SARS-CoV-2 and accurately detect emerging outbreaks.
This study covered 7 neighborhood-scale wastewater surveillance systems in Champaign County, Illinois, from January-November 2021, with catchment populations ranging from 853 to 2,402 individuals. In an effort to improve the system’s accuracy, the researchers developed a methodology to normalize the concentration of SARS-CoV-2 N gene fragments by the concentration of pepper mild mottle virus (PMMOV) detected in the system. The presence and concentration of PMMOV served as an analogue for the presence of fecal matter in the sample, which enabled the researchers to establish more accurate baseline metrics and better analyze the relative concentration of SARS-CoV-2. Based on the concentration of SARS-CoV-2 N gene fragments to PMMOV, the system output a binary risk assessment (ie, Low or High).
Over the 11 months of the study, the 7 neighborhoods experienced 26 total local COVID-19 outbreaks, and the surveillance system identified High COVID-19 risk corresponding to 19 of those time periods (73% sensitivity). The system identified 17 total High-risk time periods, and 12 of those corresponded to local COVID-19 outbreaks (71% specificity). The researchers also indicated that the surveillance system was capable of providing sufficiently accurate risk assessment for specific variants of SARS-CoV-2, which could provide early warning of the geographic spread of variants of concern. This study provides evidence that smaller-scale wastewater surveillance systems can provide indication of increased transmission risk among specific communities, particularly during periods of relatively low local incidence.
by ponchi101 We will never know where this originated because the Chinese will never cooperate.
I was reading the USA indeed had dropped the requirement for testing prior to entry, but will keep the mandate to show proof of vaccination. That spells real trouble for Novak, when the US summer circuit arrives.
by Suliso Expect a lot more foreign travelers in US now. Europe is already super busy except with Asians.
by dryrunguy Here's the latest Situation Report. Two things of particular note: 1) Florida continues to seek out new and innovative ways to reach new lows (see section on Pediatric Vaccines) and 2) The section on Universal Healthcare in the U.S. was fascinating. I don't put a lot of stock in those types of analyses because that have to be built on a series of assumptions (e.g., if someone has universal healthcare, they'll actually access the services available to them, which is not at all true--at least in the U.S. Yet, I always find them interesting because if their analyses are even close to correct, so much tragedy and heartbreak could have been avoided.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 534 million cumulative cases and 6.31 million deaths worldwide as of June 15*. The global weekly incidence increased 4.3% from the previous week, following 3 consecutive weeks of decline. Global weekly mortality increased as well—for the first time since early February**—up 7.1% from the previous week.
*The WHO COVID-19 dashboard indicates that there is a delay in reporting for the African Region, so the current totals may not be complete.
**With the exception of a 1-week spike the week of March 21, which appears to be the result of a reporting anomaly in the Americas and South-East Asia.
UNITED STATES
The US CDC is reporting 85.7 million cumulative cases of COVID-19 and 1,007,374 deaths. The average daily incidence has plateaued over the past several weeks, holding relatively steady at approximately 100-110,000 new cases per day. Despite the ongoing elevated daily incidence, we have not observed a corresponding increase in daily mortality. Daily mortality has held relatively steady at approximately 275-325 deaths per day since late April*. *Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Despite the absence of a surge in COVID-19 mortality, both new hospital admissions (+6.5% over the past week) and current hospitalizations (+1.8%) continue to increase. Notably, both trends appear to be tapering off to some degree. Considering the plateau in daily incidence, it is possible that hospitalizations could also remain elevated, rather than peaking and then declining.
Community transmission in the US continues to be driven by the BA.2.12.1 sublineage of Omicron (64.2%), followed by BA.2 (14.2%), BA.5 (13.3%), and BA.4 (8.3%). The prevalence of BA.2.12.1 increased slightly from last week, but the prevalence of BA.4 and BA.5 are increasing more rapidly. These 4 sublineages of the Omicron variant represent essentially all new SARS-CoV-2 infections in the US.
PANDEMIC TREATY On June 14, the WHO published an annotated draft outline of the prospective pandemic prevention, preparedness, and response treaty. The treaty is currently being drafted by an intergovernmental negotiating body representing WHO Member States, with the aim of establishing a global system for building and maintaining resilience to pandemics and other large-scale disease threats. The draft outline does not contain much detail, but it presents a framework of priority topic areas to be included in the treaty. The outline is organized such that it addresses equity, systems and tools, governance and leadership, and financing for the 4 key phases of pandemic readiness: prevention, preparedness, response, and recovery. The draft includes some specific items under some sections as well as placeholders for sections on One Health, access and benefit sharing, scientific cooperation, health literacy, and broader governance issues. The stated goal is to finalize the text of the treaty in time for consideration at the 77th World Health Assembly in 2024, and considerable uncertainty remains regarding the treaty’s final structure and content.
Importantly, independent experts around the world are publishing their own recommendations regarding the scope and content of the treaty. In a letter published this week, Women in Global Health emphasize the importance of including explicit language to protect healthcare workers. They argue that a treaty that focuses solely on government responsibilities and actions, pharmaceutical and non-pharmaceutical supplies and products, and patients would be insufficient to ensure a safe and supportive environment to protect frontline healthcare workers, who are critical for pandemic response. Researchers from Georgetown University (US) emphasize that the treaty should be informed by current available evidence to identify appropriate policies, systems, and capabilities. They outline 12 key elements that should be included in an evidence-based treaty, which broadly address 4 key facets of pandemic resilience: “(1) reducing spillover risk, (2) reducing pandemic risk, (3) reducing pandemic impacts, and (4) ensuring recovery and resilience.” Their 12 key elements address the human/animal/environmental interface, strengthening public health and healthcare systems and capacities, medical countermeasure (MCM) research and development, selecting appropriate government response policies and actions, government transparency and accountability, legal issues, and equity and justice.
PEDIATRIC VACCINE In their June 15 meeting, members of the US FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) voted unanimously in favor of authorizing the Moderna and Pfizer-BioNTech SARS-CoV-2 vaccines for use in children aged 6 months to 5 years (21-0 for both vaccines). The 3-dose Pfizer-BioNTech vaccine series demonstrated an overall 80.3% efficacy against symptomatic COVID-19, and the 2-dose Moderna series demonstrated 50.6% efficacy among children aged 6-23 months and 36.8 among those aged 2-5 years. Notably, the top-line efficacy estimate for the Pfizer-BioNTech vaccine is based on only 10 total cases of COVID-19 (7 in the placebo group, 3 in the vaccine group), which contributes to the wide confidence interval, particularly for children aged 6-23 months. The US CDC’s Advisory Committee on Immunization Practices (ACIP) is scheduled to meet June 17-18, and it is expected to issue its recommendation regarding the 2 vaccines. The final FDA authorization and CDC guidance is still required, but it is possible that the first doses for this age group could be available by early next week.
Despite the long-anticipated decision for some parents, it is still unclear how many will choose to vaccinate their youngest children. As health experts have pointed out, infants and preschool-aged children already have a considerable number of recommended routine vaccinations, including several multi-dose series. Adding another 2- or 3-dose series could be a barrier for some parents due to the extra logistical hurdles of additional visits to the doctor’s office. Most states are still anticipating demand for the newest pediatric series and have already ordered millions of doses. Notably, Florida is the only state not to place a pre-order with the federal government. Still, as more evidence continues to surface on the severe illness faced by children hospitalized with COVID-19, many with no underlying health conditions, the scales may tip further in the direction of vaccination.
PAXLOVID CLINICAL TRIAL On June 14, Pfizer announced plans to halt enrollment in its current clinical trial for Paxlovid, a SARS-CoV-2 antiviral drug. This decision came after preliminary data did not show a reduction in hospitalization and death among “standard-risk” participants—ie, those who do not have underlying health conditions that put them at elevated risk for severe disease and death. The risk decreased by approximately 50%, but it was not a statistically significant benefit. The drug also failed to demonstrate benefit in terms of alleviating COVID-19 symptoms. Due to the lower risk of severe disease and death among these individuals—and therefore, low benefit from the drug—Pfizer elected to terminate the trial. The current Emergency Use Authorization (EUA) for Paxlovid only applies to high-risk patients. Pfizer indicated that it will include data from this clinical trial in its New Drug Application (NDA) for full US FDA approval for use in high-risk patients.
VARIANT-SPECIFIC VACCINE On June 15, Pfizer and BioNTech announced that the European Medicines Agency (EMA) has initiated a rolling review for their variant-specific candidate SARS-CoV-2 vaccine. Major SARS-CoV-2 vaccine manufacturers have been working to update their vaccine profiles as evidence shows diminishing protection against new variants, particularly against the now-dominant Omicron variant. The Pfizer-BioNTech candidate is among the first updated vaccines to begin a formal regulatory review process. With the rolling submission process, the EMA will be able to review data as they become available. The EMA stated that its review will initially focus on manufacturing quality assurance and safety, followed by clinical trial safety and efficacy data as they become available. The announcement also indicated that the companies intend to submit an application to the US FDA in the near future.
CANADA TRAVEL RESTRICTIONS The Canadian government announced that it will lift some SARS-CoV-2 vaccination requirements for domestic and international travel. Starting June 20, Canada will no longer require vaccination for domestic or outbound air, bus, or rail passengers nor for federally regulated transportation sector personnel. Despite these changes, international travelers may still be subject to vaccination requirements. Notably, Canadian citizens and permanent residents who are not fully vaccinated must provide documentation of a negative SARS-CoV-2 test prior to entering the country, and they are subject to testing and quarantine requirements after their arrival. Travelers who are not citizens nor residents are still required to be fully vaccinated to enter Canada, but vaccination is no longer required for international rail or flights departing Canada. Due to the high risk of transmission, vaccination requirements will remain in effect for cruise ships, and other risk mitigation measures will continue for domestic travel, including mandatory mask use. Canada also announced that it will temporarily suspend mandatory random testing at airports through June 30, in an effort to reduce traveler wait times. Starting July 1, all required testing will be moved off-site to reduce the burden on airports.
UNIVERSAL HEALTH CARE Researchers from several US universities, led by the Yale School of Public Health, published findings from their research on the projected benefit if the US had a universal healthcare system during the COVID-19 pandemic. The study, published in PNAS, found that the US could have prevented nearly 339,000 COVID-19 deaths and saved more than US$105 billion in just hospitalization costs under universal health care, based on excess hospitalizations and mortality attributable to the loss of employer-sponsored insurance and low insurance coverage during the pandemic. At the time the study was conducted, the cumulative COVID-19 mortality in the US was 973,459 deaths, so the projected total benefit of universal healthcare would have reduced US COVID-19 mortality by approximately one-third. In 2020 alone, the researchers estimate that universal health care could have prevented more than 200,000 total deaths, including from COVID-19 and non-COVID-19 causes. The absence of universal health care results in myriad barriers to accessing health services, including screening and testing critical to early diagnosis of COVID-19 and other health conditions as well as preventive services, such as vaccination. And the high cost of care can delay care-seeking behavior, which can result in more severe disease. The additional patient burden from COVID-19 also negatively impacted hospital capacity, which compounds increases in mortality. The researchers argue that the fragmented healthcare system and existing societal vulnerabilities left the US ill-prepared to combat the pandemic.
dryrunguy wrote: ↑Thu Jun 16, 2022 4:41 pm
...Despite the absence of a surge in COVID-19 mortality, both new hospital admissions (+6.5% over the past week) and current hospitalizations (+1.8%) continue to increase.
...
C'mon, that is poor statistics. An increase of +1.8% is a normal variation; you can't expect to have the same number one week after another.
If this is a long term trend (several weeks of +1.8%) then yes, it is increasing, but on a one week basis, it is not significant.
by Deuce Brace yourselves, people...
It's not 'back' - because, despite people's comfortable illusions, it never actually left (and pretending it was gone has only helped it to continue)...
by dryrunguy Here's the latest Situation Report. The section on Antibody Escape definitely piqued my interest--and not in a good way. I also don't quite understand what they mean by "COVID-19 Rebound" after Paxlovid treatment. It's the first time I've seen that term. Does that mean you were sick, got Paxlovid treatment, got better, and then got sick again? Is that what they're talking about? Google seems a bit confused about it, too. So I ask the experts here.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 538 million cumulative cases and 6.32 million deaths worldwide as of June 22.* The global weekly incidence remained relatively stable (-0.68%) from the previous week, when incidence was up nearly 8% after 3 weeks of decline. Global weekly mortality decreased as well, down 11% from the previous week. At the regional level, Europe (+17%), Southeast Asia (+46%), and the Eastern Mediterranean (+52%) experienced increases, while the other 3 regions had decreasing trends.
*The WHO COVID-19 dashboard indicates that there is a delay in reporting for the African Region, so the current totals may not be complete.
UNITED STATES
The US CDC is reporting 86.4 million cumulative cases of COVID-19 and 1,009,444 deaths. The average daily incidence has plateaued over the past several weeks, holding relatively steady at approximately 100-110,000 new cases per day. The current 7-day average is 99,365 new cases per day. Likewise, the average daily mortality has held relatively steady at approximately 250-300 deaths per day since late May.* Notably, the current 7-day average is 248, the lowest level since July 13, 2021.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions (+1.5% over the past week) and current hospitalizations (+1.1%) continue to increase, although they appear to have stabilized over the past week. Considering the plateau in daily incidence, it is possible that hospitalizations could also remain elevated, rather than peaking and then declining.
Community transmission in the US continues to be driven by the BA.2.12.1 sublineage of Omicron (56%), but BA.5 (23.5%) and BA.4 (11.4%) are now outpacing BA.2 (9.1%). The prevalence of BA.4 and BA.5 now appears to be increasing more rapidly than BA.2.12.1. These 4 sublineages of the Omicron variant represent all new SARS-CoV-2 infections in the US.
PEDIATRIC VACCINES Taking the recommendation of its advisory committee, the US FDA on June 17 authorized pediatric formulations of both the Moderna and Pfizer-BioNTech SARS-CoV-2 vaccines for children as young as 6 months old. The following day, US CDC Director Dr. Rochelle Walensky endorsed the agency’s Advisory Committee on Immunization Protection (ACIP)’s recommendation that all children younger than age 5 get vaccinated against COVID-19. US President Joe Biden visited a vaccine clinic in Washington, DC, on June 21 to mark the rollout of the last major phase of vaccinations in the nation, with virtually all individuals now eligible to receive at least 1 of 3 authorized or approved SARS-CoV-2 vaccines. In his remarks, President Biden said the availability of vaccines for the youngest children marks a “monumental step forward” and provides “some peace of mind” for parents who have been waiting 18 months since the first vaccines were authorized for adults. There are about 19 million children aged 6 months to 5 years in the US.
The Biden administration has said 10 million doses are available for distribution to states and healthcare providers, but only 2.5 million doses of the Pfizer-BioNTech vaccine and 1.3 million doses of the Moderna vaccine have been ordered to date. While some parents have expressed excitement and relief at the vaccines’ availability, it remains unclear how many will vaccinate their young kids. Only 29% of 5-11 year-olds are fully vaccinated, while 59% of those aged 12-17 years are fully vaccinated. Some parents already are facing challenges securing an appointment to get their children vaccinated, despite a federal operational plan released and implemented earlier this month. While neighborhood pharmacies and pharmaceutical chains are included in this phase of the vaccination campaign, many are expecting families to go to primary care physicians and pediatricians because of trust, familiarity, and relationships that may not exist at the pharmacy. Additionally, some parents are weighing the differences between the 2-dose Moderna and 3-dose Pfizer-BioNTech vaccines for children.
The FDA also authorized Moderna’s vaccine for children and adolescents ages 6-17 last week. The CDC’s ACIP is meeting today to discuss clinical considerations and recommendations for the vaccine in that age group. The Pfizer-BioNTech vaccine is already available for adolescents and older children.
ANTIBODY ESCAPE A correspondence letter in the New England Journal of Medicine published June 22 by authors from the Beth Israel Deaconess Medical Center in Boston provides new evidence that Omicron subvariants, including BA.4 and BA.5, are showing substantial escape from neutralizing antibodies provided by vaccination or infection. The authors evaluated neutralizing antibody titers against against the original wildtype SARS-CoV-2 and Omicron subvariants BA.1, BA.2, BA.2.12.1, and BA.4 or BA.5 among 27 participants vaccinated with the Pfizer-BioNTech vaccine who had no indications of prior infection and 27 participants with recent infection with the BA.1 or BA.2 subvariants a median of 29 days earlier (range: 2-113 days), a majority of whom were vaccinated. Among vaccinated but never infected participants, neutralizing antibody titers compared to wild-type SARS-CoV-2 were lower by “a factor of 6.4 against BA.1, by a factor of 7.0 against BA.2, by a factor of 14.1 against BA.2.12.1, and by a factor of 21.0 against BA.4 or BA.5.” Participants with a prior history of infection with BA.1 or BA.2 showed similar trends with neutralizing antibody titers compared to wild-type SARS-CoV-2 lowered by “a factor of 6.4 against BA.1, by a factor of 5.8 against BA.2, by a factor of 9.6 against BA.2.12.1, and by a factor of 18.7 against BA.4 or BA.5.” The authors asserted that these findings indicate that the Omicron variants continue to feature further neutralization escape, which may lead to increased infection among populations with prior immunity against the virus. Findings in a recent Lancet Infectious Diseases correspondence provided similar evidence of substantial escape from neutralizing antibodies against Omicron variants among individuals vaccinated with the Sinopharm vaccine, with only partial recovery after a booster shot of the same vaccine.
SARS-COV-2 REINFECTION The newest Omicron subvariants of BA.4 and BA.5 are driving increases in new SARS-CoV-2 infections in several regions, with many people experiencing reinfections despite immunity from prior infection or vaccination (1+ shots). These subvariants appear to be able to evade antibodies more easily than their predecessors, possibly due to new and different spike proteins. Though global COVID-19-associated mortality appears to be decreasing, a new preprint study posted on Research Square cautions that reinfections pose an increased risk of hospitalization (HR 2.98), all-cause mortality (HR 2.14), and sequelae in pulmonary and other organ systems. The risk of these adverse outcomes—including those impacting the heart, blood, kidneys, lungs, and brain—were most pronounced in the acute phase of infection but persisted throughout the 6-month follow up. Additionally, for every reinfection (1, 2, 3+) there was a stepwise increase in risk for all sequelae evaluated, including hospitalization. Although not yet peer-reviewed, the study serves as a signal that the COVID-19 pandemic remains a threat to the health of the world’s population, and individuals must continue to take precautions to prevent infection.
MODERNA BIVALENT BOOSTER Moderna announced June 22 that it plans to seek regulatory approval for an updated booster vaccine, mRNA-1273.214, after new clinical data on the bivalent candidate showed success against newer Omicron variants. The announcement comes in anticipation of fall booster shots, with the company saying it could ship doses as early as August. Moderna found that mRNA-1273.214 increased neutralizing titers against BA.4 and BA.5 Omicron subvariants among all participants (95% CI: 5.0, 5.9). Neutralizing titers increased by 6.3-fold (95% CI: 5.7, 6.9) among specifically seronegative patients. However, the boost to neutralizing titers for BA.4 and BA.5 was not quite as high as the boost in neutralizing titers against the original Omicron variant, BA.1, or the Delta variant. Moderna noted that a peer-reviewed manuscript describing clinical trial data should be available soon.
Scientists are hopeful that this new booster, as well as others under investigation, will aid in improving protection against a potential surge in the fall. However, both Moderna and BioNTech leadership expressed concern that regulatory processes needed to update boosters could cause delays, hoping that future updates to the most recent strains can be done without clinical trials. In a separate announcement, Moderna said it will establish a new research and manufacturing center in the UK, allowing that country to gain access to mRNA platform-based vaccines.
COVID-19 REBOUND Following a US CDC health advisory issued last month warning about the potential for recurrence of COVID-19 or “COVID-19 rebound” following treatment with the antiviral Paxlovid, several new studies suggest potential causes of the occurrence and support initial studies’ findings that rebound happens in only a small proportion of patients. A study published June 20 in Clinical Infectious Diseases examined the experience of one patient with rebound following Paxlovid treatment. The researchers, from the University of California San Diego School of Medicine, isolated the SARS-CoV-2 BA.2 variant from the patient with symptom relapse and sampled their plasma to test for viral immunity. They found the isolate had not developed drug resistance, nor did the patient have impaired immunity, leading them to hypothesize the rebound likely was the result of insufficient exposure to the drug.
Another study (preprint), posted to medRxiv and conducted by US NIH researchers, examined clinical, virologic, and immune measurements of 7 patients with COVID-19 rebound, 6 who had taken Paxlovid and 1 without previous treatment. Again, the researchers found no evidence of drug resistance, viral mutation, or impaired immune response. Instead, they found the rebounds were associated with elevated SARS-CoV-2-specific antibody and cellular immune responses, possibly due to the body trying to clear residual viral antigens possibly shed from dying infected cells. Both studies were very small and may not be generalizable to all COVID-19 rebound cases; additional larger studies are needed to confirm their findings. On June 21, the US CDC’s Morbidity and Mortality Weekly Report (MMWR) published a study examining 5,287 Paxlovid-treated patients aged 12 years and older, finding less than 1% experienced COVID-19-related hospitalization or emergency room visits 5-15 days after treatment was dispensed.
PANDEMIC INEQUALITY The COVID-19 pandemic has drastically impacted people’s health, income, and various social risk factors, worsening existing inequalities and exposing others. Nature uses 6 graphs to explore the pandemic’s effects. The graphs express various data sets examining specific issues globally, in low- and middle-income countries, and in the US, UK, and Brazil. Notably, by the end of this year, 75 million more people will be pushed into poverty—living on less than US$1.90 per day—than was expected before the pandemic, derailing gains made prior to 2020 and highlighting the need for increased efforts to get the world back on track toward the UN Sustainable Development Goals.
US NATIONAL PUBLIC HEALTH SYSTEM A bipartisan commission of health leaders this week released a set of recommendations to overhaul public health in the US, with the aim of creating a “national public health system” to protect and improve health, advance health equity, and effectively respond to emergencies. The authors call for changes that could address current health challenges—including rising maternal mortality, overdoses, and diabetes—and avoid a repeat of what it called a “splintered” response to COVID-19 that led to widely disparate outcomes nationwide. The Commonwealth Fund Commission on a National Public Health System proposal outlines actions for the US Congress; the administration of US President Joe Biden; and state, local, tribal, and territorial governments to create a coordinated and collaborative national public health system.
by ti-amie
by ponchi101
dryrunguy wrote: ↑Thu Jun 23, 2022 5:00 pm
Here's the latest Situation Report. The section on Antibody Escape definitely piqued my interest--and not in a good way. I also don't quite understand what they mean by "COVID-19 Rebound" after Paxlovid treatment. It's the first time I've seen that term. Does that mean you were sick, got Paxlovid treatment, got better, and then got sick again? Is that what they're talking about? Google seems a bit confused about it, too. So I ask the experts here.
...
I think it is kind of odd, too. They say a small percentage of people "rebounded", so I wonder why are they singling out the drug.
by dryrunguy Here's the latest Situation Report. No mention of Wimbledon. Yet.
::
US FDA CONSIDERS VACCINE UPDATES Today, the US FDA Vaccines and Related Biological Products Advisory Committee (VRBPAC) is meeting to discuss if and how the strain compositions of COVID-19 vaccines should be modified going forward. The meeting will be livestreamed on the FDA website here with presentation materials also available for download. Presentations and discussion points expected to be covered include: evolution of SARS-CoV-2 variants thus far, as well as models predicting future evolution; current effectiveness of COVID-19 vaccines; related recommendations from the WHO on the subject; clinical trial data evaluating COVID-19 vaccines with varying strain composition; and the FDA perspective on the issue, including considerations for and data required to support authorization of any modified vaccines. The committee will then vote regarding recommendations for a COVID-19 vaccine strain composition, weighing the potential expected increases in immunity against the expense and complexity of a change in composition. Experts are hopeful that an updated strain composition could help provide increased protection from a potential fall surge, although there is concern that the speed of SARS-CoV-2 mutations and slowness of updates to formulations could reduce efficacy of boosters, as vaccine protection wanes and composition becomes outdated compared with circulating variants.
PFIZER-BIONTECH OMICRON-ADAPTED VACCINES Pfizer-BioNTech shared new data over the weekend of 2 Omicron-adapted vaccine candidates, both exhibiting positive safety, tolerability, and immunogenicity, and even outperforming the companies’ current vaccine. Given at 30 microgram and 60 microgram doses as a fourth booster dose, the monovalent candidate elicited a 13.5- and 19.6-fold increase in neutralizing geometric titers against Omicron BA.1, respectively, compared to pre-booster levels. The bivalent candidate, which contains antigens to both Omicron and the original strain, exhibited a 9.1- and 10.9-fold increase at the same dosages against BA.1. Both candidates were well-tolerated among participants of the phase 2/3 trial of adults over age 56. Preliminary lab studies show both candidates neutralize BA.4 and BA.5, but to a lesser extent than BA.1. The companies have shared the data with the US FDA ahead of its Vaccines and Related Biological Products Advisory Committee (VRBPAC) meeting today, alongside data from ongoing COVID-19 booster studies. The companies also shared the data with the European Medicines Agency (EMA) ahead of the June 30 meeting of the International Coalition of Medicines Regulatory Authorities (ICMRA).
MODERNA VACCINE FOR OLDER CHILDREN Children and adolescents aged 6 through 17 years can now receive the Moderna COVID-19 vaccine in the US, following publication of the US CDC Advisory Committee on Immunization Practices’ (ACIP) recommendations and CDC Director Dr. Rochelle Wallensky’s endorsement. The US FDA authorized the vaccine for that age group last week. Adolescents and teens ages 12-17 receive the same dosage as adults, while younger children ages 6-11 receive half of that dose, administered in 2 shots separated by 4-8 weeks. The Pfizer-BioNTech vaccine is already available for adolescents and older children.
A decision on the Moderna vaccine for this age group was delayed due to FDA review of data on the risk of heart problems, including myocarditis and pericarditis, among adolescent boys. However, the FDA said the vaccine’s benefits outweigh the risks, which are very small and also observed with the Pfizer-BioNTech vaccine. COVID-19 carries a much greater risk of heart problems than either vaccine, which are both safe overall. To minimize the risk of transient heart problems related to the vaccines, the CDC recommends that boys and men aged 12 through 39 years space their doses by 8 weeks. That recommendation, particularly for young adult men, is supported by findings from a recent study from Canada published in JAMA Network Open.
LONG COVID/PASC Researchers worldwide are investigating the potential causes of post-acute sequelae of SARS-CoV-2 infection (PASC), commonly known as long COVID. Blood clots, persistent virus, and immune system abnormalities—or a combination of those or other underlying mechanisms—are leading theories about what could be causing long-term symptoms following recovery from acute infection. To date, there is no agreement on how to define and diagnose long COVID, and estimates of its prevalence range from 5% to 50% of recovered patients. Recent data published by the US CDC, collected between June 1 and June 13, 2022, show that nearly 1 in 5 US adults who previously had COVID-19 continue to experience symptoms of long COVID, such as fatigue, rapid heartbeat, shortness of breath, muscle weakness, chronic pain, or cognitive difficulties. Overall, about 1 in 13 US adults, or 7.5% of the population, have symptoms lasting 3 or more months after COVID-19 recovery that were not experienced prior to infection. Women were more likely than men to currently have long COVID (9.4% vs. 5.5%), according to the data, findings that are supported by a review published June 20 in Current Medical Research and Opinion.
The CDC data show that older adults are less likely to have long COVID than younger adults, but the symptoms are often overlooked in older individuals and some research suggests seniors are more likely to develop long-term symptoms. A study from Denmark published June 22 in The Lancet Child & Adolescent Health found that among children ranging in age from 0 through 14 years, those who previously tested positive for SARS-CoV-2 were more likely to experience at least 1 symptom for 2 months or more than children who never tested positive. Additionally, one-third of children who previously tested positive experienced at least 1 long-term symptom they did not have prior to infection, including mood swings, rashes, and stomach aches, memory and concentration problems, and fatigue. While any person of any age can experience long COVID, the question of why remains a mystery. But most scientists and public health officials agree that unraveling that mystery, including standardizing the condition’s definition and diagnosis and finding treatments, represents an urgent global emergency to prevent mass suffering.
ESTIMATES OF DEATHS AVERTED Last week, a study published in The Lancet Infectious Diseases reported results from transmission modeling efforts estimating that COVID-19 vaccination programs may have prevented 19.8 million deaths (95% CI: 19.1-20.4 million) worldwide during their first year of rollout, even though global vaccination targets were not reached. The figure is based on using excess deaths to determine the true mortality burden of COVID-19, although modelers also found that using COVID-19 mortality alone and not excess deaths yielded a finding of 14.4 million deaths prevented (95% CI: 13.7-15.9 million), including 7.4 million (95% CI: 6.8-7.7 million) deaths prevented in countries provided vaccine by the COVID-19 Vaccines Global Access (COVAX) Advance Market Commitment. However, if vaccination coverage targets of 20% or 40% had been met in low-income countries, further reductions in mortality in those nations of 45% (95% CI: 42-49%) and 111% (95% CI: 105-118%), respectively, could have been reached. Experts noted that the study highlighted not only the importance of vaccination but also equitable access, with the majority of predicted prevented deaths occurring among high-income and upper-middle-income nations. Notably, China was not included in the analysis due to its status as the origin of the outbreak and its large influence on estimates due to its population size.
CHINA The National Health Commission of China today announced a reduction of the country’s quarantine policy for overseas travelers to 7 days in a centralized facility and an additional 3 days at home. Previously, travelers were required to stay 14-21 days in centralized quarantine depending on the city of entry and destination. The announcement also includes similar guidelines for close contacts of confirmed COVID-19 cases, requiring 7 days in centralized quarantine and 3 days of health monitoring at home, compared to the prior minimum 14-day requirement. China remains an outlier, as most nations have dropped their vaccination and quarantine requirements for international travelers.
Over the weekend, Beijing said it would allow primary and secondary schools to reopen for in-person instruction, with youth sports soon to follow at non-school locations. Shanghai officials also declared that the city reported no new local cases in 2 months, following a 2-month citywide lockdown that ended June 1. The lockdown effort was in line with China’s zero-COVID policy to stop all outbreaks. The policy is being discussed with renewed interest after authorities in Beijing mentioned that the strict policy could be in place for 5 years. The notice was published Monday on the official Communist Party newspaper of the capital, Beijing Daily, and republished by other media outlets, but officials quickly removed the reference to “5 years” from most online publications, as well as a hashtag on the microblogging site Weibo.
COVID-19 RECOVERY As world leaders drop the COVID-19 pandemic from their agendas, and US federal, state, tribal, and local governments roll back pandemic-related funding and mitigation efforts—such as mask mandates—local officials, grassroots organizations, and frontline community health workers continue to push for and implement piecemeal strategies to help increase vaccination rates, draw attention to the need for research into long COVID, and improve trust in and funding for public health systems. There is a need for the US to create “a sustainable infrastructure that can keep more people from getting COVID, regardless of their social circumstances,” writes Ed Yong in The Atlantic. Indeed, the US Government Accountability Office (GAO) last week released a report recommending that the US Department of Health and Human Services (HHS) prioritize the development of a real-time, public health situational awareness network to help raise public awareness to facilitate the early detection of and rapid response to future and potentially catastrophic disease outbreaks, such as COVID-19.
by ponchi101 So, the vaccines saved around 20MM people. Roughly the size of a medium country.
But science sucks.
by Suliso Somebody refered to this article on TW. Yahoos went on on how many people have been maimed and killed by the vaccine. Not a shred of evidence of course. It's like a religion...
by ponchi101
Suliso wrote: ↑Wed Jun 29, 2022 4:23 am
Somebody refered to this article on TW. Yahoos went on on how many people have been maimed and killed by the vaccine. Not a shred of evidence of course. It's like a religion...
About to get me started.
My loony friend N and I went to play padel a few days ago. We used to play at a facility that is a vaccination center too. I mentioned that I went there for my second booster, and was going to talk about how hellacious traffic had been, but he interrupted me with "let's not talk about THAT, we will never agree".
I did say I was talking about the traffic, but I still felt it was odd. So, there is NO evidence that can convince you that the vaccines are safe and effective? Because, for us, there is certainly evidence and data that could prove they are unsafe and detrimental: just show us the number of people truly hurt by them, compiled by a reputable organization.
Yes, it is a cult.
by ti-amie
Suliso wrote: ↑Wed Jun 29, 2022 4:23 am
Somebody refered to this article on TW. Yahoos went on on how many people have been maimed and killed by the vaccine. Not a shred of evidence of course. It's like a religion...
It's like a religion It's like a cult.
Fixed it for ya!
by ti-amie Polio is rearing its head again. So is measles.
by Deuce Last year, I met a guy who played pickleball in our league. We live near each other, and so would drive to the courts together (where we play mostly doubles, switching partners pretty much every game). In addition, we'd call each other to play outside of league times.
Nice guy... in the car we would inevitably talk of various elements of life... We got along well, and a friendship was establishing itself rather naturally.
You can see where this is going...
One day in the car, the subject of COVID vaccines came up. That is when I discovered that he doesn't believe in the vaccines. From that point, I decided not to drive in the same car as him - but we remained friendly, and still played pickleball together for another month or so... After playing one day, we had a discussion about COVID. He says he believes COVID exists, but that it's no more serious than the typical 'flu. He said that he thinks the vaccines are dangerous. I also learned within this discussion that he regularly attended anti-mask and anti-vaccine protests.
I asked him if he thinks that all of the measures to protect against COVID are part of a conspiracy. He said "Yes." I asked him what he thinks the reason for the conspiracy is. He said "I don't know yet."
I then told him that it would be absolutely impossible for 95% of the politicians in the world, 95% of the media in the world, and 95% of the medical professionals in the world to all agree to manipulate the population of the world in the same manner at the same time, and also keep that conspiracy hidden. Absolutely 100% impossible.
Then a few days after that, I saw him inside a grocery store (when masks were mandatory). He was wearing his mask under his nose, and not covering his mouth properly. And the mask was obviously an old one. In other words, the mask was entirely useless - it had the same effect as wearing no mask.
At that point, I decided that I did not want to associate with this person any longer. His beliefs are one thing - but not having enough respect for other people to wear a mask in public indoor places was unacceptable to me.
And so I do not talk with or associate with him anymore. If he is at pickleball at the same time as I am, I'll play on the same court as him - because it's outside - I've even partnered with him for a few games... but I don't say a word to him. He is persona non grata in my life.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 543 million cumulative cases and 6.33 million deaths worldwide as of June 29. The global weekly incidence increased 21.32% from the previous week. Global weekly mortality increased as well, up 7.43% from the previous week. At the regional level, Europe (+40%), the Americas (+15%), Southeast Asia (+32%), and the Eastern Mediterranean (+47%) experienced increases, while the Western Pacific (-3%) and Africa (-34%) had decreasing trends. The number of new weekly deaths increased in the Eastern Mediterranean (+22%), Southeast Asia (+15%), and the Americas (+11%) and decreased in the Western Pacific (-6%), Europe (-5%) and Africa (-1%).
UNITED STATES
The US CDC is reporting 87.2 million cumulative cases of COVID-19 and 1,012,166 deaths. The average daily incidence has plateaued over the past several weeks, holding relatively steady at approximately 100-110,000 new cases per day. The current 7-day average is 108,505 new cases per day. The average daily mortality has held relatively steady at approximately 250-300 deaths per day since late May* However, the 7-day average appears to be rising and currently is 321 deaths per day.
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions (+13% over the past week) and current hospitalizations (+5%) continue to increase. Considering the plateau in daily incidence, it is possible that hospitalizations could also remain elevated, rather than peaking and then declining.
Community transmission in the US is now being driven by the Omicron BA.5 (36.6%) and BA.4 (15.7%) sublineages, which together are now more prevalent than the BA.2.12.1 sublineage (42%). Along with BA.2 (5.7%), these 4 sublineages of the Omicron variant represent all new SARS-CoV-2 infections in the US.
OMICRON BA.4/BA.5 SARS-CoV-2 Omicron subvariants BA.4 and BA.5 have overtaken BA.2.12.1 as the dominant strains in the US. While BA.2.12.1 still makes up approximately 42% of new cases as of June 25, BA.4 accounts for 15.7% and BA.5 accounts for 36.6%, for a combined total of 52.3%. BA.4 and BA.5 were first detected in South Africa in November 2021, and they are now fueling a worldwide increase in cases. Additionally, hospitalizations are on the rise in Israel, Portugal, South Africa, the UK, and the US. The increases in case and hospitalization numbers are likely due to the fact that BA.4 and BA.5 contain mutations that are believed to aid in immune evasion. This means that prior infection with an earlier Omicron strain, such as BA.1 from winter 2022, might not be enough to protect against disease. BA.4 and BA.5 also are capable of escaping some immunity from vaccines, but vaccinated individuals still tend to fare better than those relying on natural immunity alone. It is increasingly likely that more individuals will start experiencing reinfections. There are concerns that multiple reinfections could put individuals at a higher risk for health problems, but research on the matter is ongoing.
In a June 29 briefing, WHO Director-General Dr. Tedros Adhanom Ghebreyesus noted that BA.4 and BA.5 are responsible for an approximately 20% increase in the number of COVID-19 cases worldwide. COVID-19 cases are on the rise in 110 countries and deaths are increasing in half of the 6 regions monitored by the WHO. Dr. Tedros also spoke out against complacency in the face of the pandemic, stressing that the pandemic is changing and not yet over. He urged the international community to quickly work toward achieving 100% vaccination rates for healthcare workers and individuals over age 60 years. Dr. Tedros also re-emphasized the need for a pan-coronavirus vaccine that can stand up to the rapid evolutionary rate of SARS-CoV-2. Notably, BioNTech announced this week that the company and its partner Pfizer will begin human trials of a pan-coronavirus vaccine in the second half of the year.
VACCINE UPDATES FOR OMICRON The US FDA Vaccines and Related Biological Products Advisory Committee (VRBPAC) on June 28 voted 19-2 to recommend the agency take steps to authorize updated COVID-19 booster shots targeting some form of the SARS-CoV-2 Omicron variant that has been dominant since the beginning of this year. A confluence of factors makes the US population more susceptible to a winter COVID-19 surge, including waning immunity, the possible emergence of a new variant, and colder weather that pushes more people indoors. Current vaccines and boosters are based on the spike protein structure and characteristics of only the original SARS-CoV-2 virus, so introducing individuals to an Omicron spike protein should broaden the body’s immune response against additional versions of the virus, whether currently circulating or a future but similar variant. Many committee members expressed dismay over the limited amount of data on updated vaccine formulations—including if or how well they might provide additional protection—and unknowns about which variants will be circulating this fall.
In an announcement released today, the FDA said that based on the committee’s discussions, it has advised manufacturers seeking to update their COVID-19 vaccines to develop modified versions that add spike protein components of the Omicron BA.4/BA.4 subvariants to current vaccine formulations to create a 2-component, or bivalent, booster vaccine. The decision paves the way for vaccine companies to start manufacturing Omicron-containing doses to potentially be ready for use beginning in early to mid-fall. The FDA did not recommend a change to the primary vaccination formulations.
Introducing another booster this year may come with its own suite of challenges in terms of communication, including possibly moving away from the term booster to something like “another annual shot.” A significant proportion of individuals in the US who are eligible to receive third or fourth shots have yet to do so, leaving them more vulnerable as BA.4 and BA.5 become predominant and highlighting the need for a comprehensive communication strategy about who should get additional shots, when, and why. The administration of US President Joe Biden on June 29 announced an agreement to purchase 105 million doses of the Pfizer-BioNTech COVID-19 vaccine for US$3.2 billion for a fall vaccination campaign, with options for an additional 195 million doses. Pfizer-BioNTech will provide its new formulation based on FDA recommendations. Both Pfizer-BioNTech and Moderna are working on vaccine booster reformulations.
US MATERNAL MORTALITY A new study examining maternal mortality rates in the US before and during the COVID-19 pandemic was published June 28 in the peer-reviewed journal JAMA Network Open. The study compared pre-pandemic and pandemic maternal mortality using de-identified records from the National Center for Health Statistics. Deaths occurring in 2018, 2019, or January-March 2020 were classified as pre-pandemic. Deaths occurring from April-December 2020 were classified as during the pandemic. The study found that maternal mortality rose from 18.8 per 100,000 live births to 25.1 per 100,000 live births. This represents an increase of 33%, higher than the 22% increase in mortality expected as a result of the pandemic. Late maternal mortality increased 41%.
The largest increases in maternal mortality were seen in Hispanic populations, at 74.2%, and non-Hispanic Black populations, at 40.2%, compared to an increase of 17.2% in non-Hispanic White populations. The largest increases in maternal mortality were seen for underlying cause-of-death codes related to indirect causes of death such as other viral diseases (2,374.7%), diseases of the respiratory system (117.7%), and diseases of the circulatory system (72.1%). Maternal mortality increases associated with direct causes of death were largely due to diabetes (95.9%), hypertension disorders (39%), and other pregnancy-related conditions (48%). The authors call for future studies that examine ethnic and racial disparities along with specific causes of COVID-19-related maternal mortality. They also expressed hope that improvements due to the rollout of vaccines could be realized in future analyses.
The new study further confirms a trend seen before the pandemic, when maternal mortality rates were twice as high in the US as in many other high-income countries. More resources are needed to protect pregnant populations from the dangers associated with COVID-19, but pre-existing issues that lead to high maternal mortality must also be addressed to protect this often overlooked high-risk population in the US.
MONOCLONAL ANTIBODY THERAPIES The US government is expected to use up its supplies of Eli Lilly’s monoclonal antibody therapy for COVID-19 in late August because its pandemic funding is running out. Lilly said it agreed to supply the US with an additional 150,000 doses of bebtelovimab for about US$275 million in order to meet demand through the end of August. The agreement includes an option for an additional 350,000 doses that must be applied no later than September 14. Currently, the federal government is distributing about 30,000 doses per week. The antibody received US FDA emergency use authorization earlier this year for use among non-hospitalized patients with mild-to-moderate COVID-19 who are at high risk of disease progression, and the drug has shown effectiveness against the Omicron variant. If the federal government is unable to procure more doses than currently agreed upon, Lilly will need to sell the treatment directly to hospitals and states, a move that would represent a first test of shifting a COVID-19-related drug to the commercial market.
The US FDA and the Assistant Secretary for Preparedness and Response (ASPR) authorized a shelf-life extension for another monoclonal antibody therapy, Evusheld (tixagevimab co-packaged with cilgavimab) made by AstraZeneca. The shelf life of certain lots of the refrigerated treatment can be extended from 18 months to 24 months. Evusheld is authorized for pre-exposure prophylaxis of COVID-19 in certain adults and pediatric individuals. Several experts are hoping for more funding and research into antibody treatments for COVID-19 and other ailments, with some noting that antibodies can have more long-lasting impacts than vaccines, especially among people with immunodeficiencies, and could serve as a key solution during the next pandemic.
DIGITAL SOLUTIONS FOR INFODEMIC During the COVID-19 pandemic, the public has been faced with an overabundance of information, including false or misleading content, in both online and offline environments. To address the online information epidemic, the WHO Regional Office for Europe published a policy brief on how digital solutions can be used to address this so-called “infodemic” to help improve the public health response to COVID-19 and future health emergencies. The brief outlines what WHO is doing to address the infodemic in Europe and globally and highlights 6 specific policy considerations for policymakers and other key stakeholders to help improve infodemic management, including reinforcing multistakeholder networks for infodemic management; strengthening overall risk communication and community engagement; implementing continuous monitoring of harmful and false online content; improving digital literacy approaches and organizing infodemic management trainings; advocating for infodemic management through communication campaigns; and ensuring safe online platforms, which protect people from harmful content.
RESEARCH ROUNDUP The research roundup provides quick synopses of COVID-19-related research.
From Emerging Infectious Diseases, a case report from Thailand of a veterinarian who was diagnosed with COVID-19 after treating and being sneezed on by a domestic cat owned by a person infected with SARS-CoV-2 at the time. Genetic analysis supports the hypothesis that viral transmission occurred from the owner to the cat and then from the cat to the veterinarian. Notably, the veterinarian was wearing an N95 during the cat’s examination, leading the researchers to postulate her eyes were left vulnerable to infection when the cat sneezed in her face, highlighting the importance of face shields or goggles, in addition to masks, to prevent transmission.
From JAMA Internal Medicine, a study suggesting that patients of African ancestry with sickle cell trait (SCT) and associated history of one of several kidney conditions were at increased risk of mortality and acute kidney failure following COVID-19. The results strongly support advising that patients with SCT be regarded as at high-risk of COVID-19.
From The Journal of Infectious Diseases, a cohort study evaluating the risk of SARS-CoV-2 infection and severe COVID-19 disease in persons with Down syndrome (DS) and matched controls prior to available vaccination. Though the risk of infection among individuals with DS was 32% lower than their matched counterparts (aHR 0.68, 95% CI: 0.56-0.83), the rate of severe COVID-19 disease was 6-fold higher (aHR 6.14, 95% CI: 1.87-20.16). The results support better infection monitoring, early treatment, and vaccination for individuals with DS.
From the New England Journal of Medicine, a cohort study of US children aged 5-11 who were vaccinated on or after November 23, 2021, compared with matched controls who were unvaccinated to estimate the effectiveness of the Pfizer-BioNTech vaccine at the start of the Omicron surge. The estimated vaccine effectiveness against symptomatic COVID-19 was 18% (95% CI: -2 to 34) at 14 to 27 days after the first dose and 48% (95% CI: 29 to 63) at 7 to 21 days after the second dose, showing moderate protection as Omicron was becoming dominant.
From Pediatrics, a multicenter prospective observational cohort study conducted in 25 US pediatric hospitals that followed COVID-19 patients under age 21 who were hospitalized between May 2020 and May 2021 for COVID-19 or multisystem inflammatory syndrome in children (MIS-C) for 2-4 months after admission. The researchers found that more than 1 in 4 children with COVID-19 or MIS-C experienced persistent symptoms or activity impairment for at least 2 months. Those patients with MIS-C who have respiratory problems or obesity had a higher risk of prolonged recovery.
From Scientific Reports, a mathematical modeling study examining how human movement—from home to other locations such as school, work, and elsewhere—social distancing behavior, and other restrictive measures such as quarantine affect COVID-19 dynamics within a population. The study’s model showed that SARS-CoV-2 transmission is most attributable to the home location, including gatherings of relatives and close friends. Therefore, limiting encounters or travel to other locations is only effective if the same social distancing measures are also effectively implemented in the home setting.
by dryrunguy So, the neighbor across the road, Bob, hasn't left his house since he got home from work yesterday. (He works at the local stone quarry.) He's in his early 60s and has diabetes, heart problems, and other ailments. His daughter-in-law bought four COVID tests and delivered them this morning. Bob's wife refused to test him, insisting that it wasn't COVID, even though she knew some of the guys the neighbor works with at the quarry had it a few days ago--and still came to work. Instead, she left to go do a beer run, yes, a beer run, and left Bob alone in the house for over an hour.
So their son went to check on Bob, found the unused COVID tests on the kitchen counter, and also found Bob passed out. He finally got Bob to wake up and administered the test. Positive.
Bob needs to go to the hospital. He needs paxlovid or some other treatment. But I don't see anything going on down there.
I know there are several things wrong with this story--people showing up for work knowing they have COVID, prioritizing a beer run over a spouse's health, etc. But it is what it is. I hope this ends as well as it can. Bob has always been very good to us.
by ponchi101 sigh...
by Cuckoo4Coco Is Bob capable of calling 911 to take him to the hospital for himself?
by Suliso Covid is just a viral disease. How did it manage to become so political?
by ponchi101
Suliso wrote: ↑Sat Jul 02, 2022 5:59 pm
Covid is just a viral disease. How did it manage to become so political?
1. One political figure that is really a cult figure, said it was nothing and peddled lunacy to his followers.
2. A general misunderstanding of basic tenets in science.
3. An impossibility to detect fictional conspiracy theories.
But yes, how did it get to this point?
by dryrunguy
Cuckoo4Coco wrote: ↑Sat Jul 02, 2022 5:59 pm
Is Bob capable of calling 911 to take him to the hospital for himself?
Not from the sound of it. Someone would have to call for him. The good news is that the local ambulance is less than 2 miles away. But it still takes a few minutes because they have to sound the siren, wait for volunteers to arrive, and then drive 2 miles up the mountain. (Don't worry, that's not as daunting as it sounds. We have a decent road.) And the ambulance service is free for any household in the community that makes a $100 donation to the local fire hall each year. That's the first "bill" I pay each January.
Cuckoo4Coco wrote: ↑Sat Jul 02, 2022 5:59 pm
Is Bob capable of calling 911 to take him to the hospital for himself?
Not from the sound of it. Someone would have to call for him. The good news is that the local ambulance is less than 2 miles away. But it still takes a few minutes because they have to sound the siren, wait for volunteers to arrive, and then drive 2 miles up the mountain. (Don't worry, that's not as daunting as it sounds. We have a decent road.) And the ambulance service is free for any household in the community that makes a $100 donation to the local fire hall each year.
I hope for Bob's sake someone makes the smart decision to call it.
by ti-amie So my 80+ year old cousin invited me and my family to a bbq tomorrow July 3. I asked her if she and all the members of her household (she has an adult son) are vaccinated. At first she ducked the question. I asked again. 10 hours later she responded and said they were "good".
I'm not going.
Any update on Bob?
by dryrunguy
ti-amie wrote: ↑Sat Jul 02, 2022 8:09 pm
Any update on Bob?
It's awfully quiet over there today, especially for a Saturday when there's usually a constant buzz of tractors, 4-wheelers, and diesel trucks. I'm wondering if perhaps his son drove him to the hospital instead of calling an ambulance. I hope so (in spite of how inherently dangerous it would be to drive 35 miles with a person sick with COVID in the truck). It's never this quiet on a beautiful Saturday afternoon. I meant that. NEVER.
by Deuce
Suliso wrote: ↑Sat Jul 02, 2022 5:59 pm
Covid is just a viral disease. How did it manage to become so political?
I'll assume you're asking the question seriously - though I kind of hope you're not...
The rather obvious answer is because governments - the politicians - are the ones who were deciding upon the restrictions, protective measures, compensations, etc. directly relating to COVID-19.
And this was occurring worldwide.
And that COVID-19 is deadly to some, debilitating to many others, and is the first declared worldwide viral pandemic in a long time.
by dryrunguy I am pleased to report I just saw Bob walk from his house to their garage. He was moving slowly, but he was moving slowly before COVID. At least he's up and around. So that is encouraging.
He's a tough cookie.
by Cuckoo4Coco
dryrunguy wrote: ↑Sun Jul 03, 2022 6:33 pm
I am pleased to report I just saw Bob walk from his house to their garage. He was moving slowly, but he was moving slowly before COVID. At least he's up and around. So that is encouraging.
He's a tough cookie.
Glad to see he is at least up and moving around. Do you know if he went to the hospital for some treatment and at least got on some medicine?
dryrunguy wrote: ↑Sun Jul 03, 2022 6:33 pm
I am pleased to report I just saw Bob walk from his house to their garage. He was moving slowly, but he was moving slowly before COVID. At least he's up and around. So that is encouraging.
He's a tough cookie.
Glad to see he is at least up and moving around. Do you know if he went to the hospital for some treatment and at least got on some medicine?
He didn't go to the hospital. Chances are he fought that notion tooth and nail if anyone mentioned it.
by ti-amie My daughter just told me another of her friends has come down with C19. This is in addition to four of her co-workers, one of whom had had C19 during its first go around.
by ti-amie
by ponchi101 Here we go again. Please, no.
by Deuce It never stopped.
People only pretended it stopped.
Well, the great majority of people pretended it stopped.
I didn't.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
REINFECTION RISK The Omicron BA.5 subvariant has quickly become the most predominant circulating variant in the US due to its ability to evade immunity from either previous infection or vaccination, dashing hopes of a COVID-19 pandemic reprieve. The subvariant is more likely to cause reinfections and is driving a wave of new infections across the country, with official US CDC data showing a daily average of around 100,000 new cases. But experts warn this represents a severe undercount of new cases, as many people are using home tests and not reporting their results to health authorities. Notably, the Walgreens COVID-19 Positivity Tracker shows a weekly 41.6% positivity rate, up nearly 9% over the prior week and the highest since the tracker began.
Prior to the emergence of the Omicron variant and its family of evasive subvariants, reinfections were rare; but now, some countries are seeing reinfections account for a larger proportion of new cases, including the UK, where roughly a quarter of new cases are reinfections. Though many believe BA.5 does not cause more severe disease than other variants, hospitalizations in many countries are rising and evidence suggests that multiple infections can increase the risk of long-term morbidities, including long COVID. Some major U.S. cities, such as New York City and Los Angeles, have reinstated or are considering reinstating mask mandates for indoor spaces, citing concerns over BA.5. Despite these actions, some worry it will be increasingly difficult to convince people to take public health precautions, as funding and mitigation measures have largely been rolled back.
BA.2.75 & BA.5.2.1 SUBVARIANTS Scientists have identified 2 new Omicron subvariants. BA.2.75 was first identified in India—where it makes up at least 25% of sequenced cases and is competing with BA.5 and BA.2—and has been identified in at least 10 other countries, including at least 3 cases in the US. Though BA.2.75 has not yet been named a variant of interest or variant of concern, several virologists are urging continued monitoring of the variant, as mutations in its spike proteins may lead to increased immune escape and an ability to outcompete BA.5. Additionally, officials in Shanghai, China, this week reported a single case of another new subvariant, BA.5.2.1. The subvariant was linked to a case in an overseas traveler and so far has not been identified in other cases.
US PUBLIC HEALTH EMERGENCY The US government is expected to once again renew its determination that the COVID-19 pandemic constitutes a public health emergency, first set in January 2020. The current extension is set to expire on July 15, when the next extension is set to take effect. The emergency designation allows millions of low-income Americans who might not otherwise be eligible to access Medicaid coverage; US regulators to authorize vaccines, diagnostics, and therapeutics for COVID-19; flexibilities around telehealth services; and states to access pandemic-related funds. The government has said it will give 60 days’ notice before ending the emergency designation to allow states and companies time to prepare. The US has averaged between 100,000 and 110,000 new daily COVID-19 cases and about 300 daily COVID-19 deaths since May.
SECOND BOOSTERS Officials in the administration of US President Joe Biden are in discussions with US FDA and CDC officials over whether to expand eligibility of second SARS-CoV-2 vaccine booster shots, or fourth doses, to adults under age 50 in an effort to counter waning immunity amid a wave of new infections and increasing hospitalization rates due to the Omicron BA.5 subvariant. Such a move requires regulatory authorization from the FDA and the CDC. Currently, adults aged 50 and older and those aged 12 and older who are immunocompromised are eligible for fourth doses. Experts are divided over allowing additional boosters now, with some arguing more clinical data is needed to support the shots for younger adults, while others say that people in that age group who wish to receive a fourth dose should be allowed to do so. Still others argue the Biden administration and health officials should be focused on improving primary series and first booster rates, and some experts warn that pushing a fourth dose now may diminish the importance of reformulated booster doses that are expected in the fall. Notably, Moderna released data this week showing its Omicron-containing bivalent booster candidate elicits significantly higher neutralizing antibody responses against the Omicron subvariants BA.4 and BA.5 compared to the currently authorized booster. Initial booster doses currently are available for anyone aged 5 years and older who has received the 2-dose primary series, but only 34% of eligible US residents have received their first booster dose.
The European Centre for Disease Prevention and Control (ECDC) and the European Medicines Agency (EMA) this week updated guidance to recommend a second vaccine booster, or fourth dose, for all individuals over age 60 as well as medically vulnerable people in Europe, as COVID-19 cases and hospitalizations increase across the continent. In a joint statement, European Commissioner for Health and Food Safety Stella Kyriakides issued an urgent call for all eligible individuals to get vaccinated and boosted, saying, “There is no time to lose.” Previously, only adults over age 80 were recommended to receive a booster. In the UK, people aged 75 and older, residents in long-term care facilities, and those with weakened immune systems are eligible for second boosters.
ACCESS TO ANTIVIRALS & VACCINES Senior WHO officials are calling on nations to fill immunity gaps through increased vaccination rates and on antiviral manufacturers to improve access to COVID-19 therapeutics. The COVAX initiative has a surplus of vaccines, according to officials, and lower-income countries should focus on vaccinating healthcare workers, older adults, and other vulnerable populations to minimize the risk of COVID-19-related morbidity, including long COVID, and mortality. Additionally, the WHO called specifically on Pfizer to quickly increase access to its COVID-19 oral antiviral medication, Paxlovid, to countries that are struggling to afford or gain access to stocks of the treatment.
In the US, regulatory authorities last week expanded the emergency use authorization (EUA) of Paxlovid to allow state-licensed pharmacists to prescribe the medicine to eligible patients. Previously, only doctors, nurses, and physician assistants were permitted to prescribe the treatment. The move raised concerns among some experts, as the use of Paxlovid can be complicated by a patient’s health status and concurrent treatments. The treatment is available at no cost to qualified patients. The US has secured the purchase of 20 million courses of Paxlovid, but only 1.7 million courses have been distributed to pharmacies nationwide. In related news, the Biden administration on July 11 announced it has secured 3.2 million doses of the Novavax protein-based SARS-CoV-2 vaccine, which is expected to soon receive US authorization.
The ACT-Accelerator (ACT-A) program—a collaboration among the WHO, governments, and nongovernmental organizations that works to provide equitable access to COVID-19 related tools, including vaccines through COVAX—is set to wind down operations in their current form this fall due to a lack of funding. While ACT-A likely will continue in a scaled-down form—and COVAX, which is housed at Gavi, the Vaccine Alliance is set to continue through 2023—the transition raises questions about how lower-income countries will access adequate supplies of vaccines, diagnostics, and treatments. Notably, a new analysis from the health data group Airfinity estimates that 1.1 billion doses of SARS-CoV-2 vaccines—about 10% of all manufactured doses—have been wasted since late 2020 due to the inequitable global rollout of shots, vaccine hesitancy, and incorrect storage.
PFIZER-BIONTECH VACCINE FOR ADOLESCENTS The US FDA last week expanded full approval of the Pfizer-BioNTech SARS-CoV-2 vaccine to adolescents aged 12 to 15 years. The vaccine, known as Comirnaty, has been available for this age group since the FDA provided emergency use authorization (EUA) in May 2021, and the agency originally approved the vaccine for individuals aged 16 years and older in August 2021. To date, more than 9 million 12-15-year-old children have received the 2-dose primary series. Pfizer and BioNTech indicated they have also filed clinical trial data for approval among this age group with the European Medicines Agency (EMA) and other regulatory agencies around the world.
PULSE OXIMETRY Pulse oximeters are an important tool for measuring the amount of oxygen in the bloodstream and have been widely used in healthcare and home settings during the COVID-19 pandemic. But the devices can overestimate blood oxygen levels in people with dark skin, causing Asian, Black, and Hispanic intensive care unit (ICU) patients to receive less supplemental oxygen than White ICU patients, according to a retrospective cohort study conducted prior to the pandemic and published on July 11 in JAMA Internal Medicine. These differences in performance may contribute to racial and ethnic disparities in care, including among COVID-19 patients. Another recent study showed racial and ethnic differences in pulse oximetry delayed the recognition and treatment of COVID-19 among Black and Hispanic patients.
The US FDA is convening a public meeting of its Medical Devices Advisory Committee later this year to discuss available data and provide guidance to healthcare providers. The agency issued a safety communication about the issue in February 2021 urging patients and providers to be aware of the multiple factors that can affect pulse oximeter accuracy and to consider limitations when using pulse oximeters to make diagnoses and treatment decisions. Some experts are warning of the potential for continued disparate outcomes among racial and ethnic groups as technology becomes more common in healthcare and calling for more diversity in clinical trials.
WASTEWATER SURVEILLANCE Wastewater surveillance can provide first-look data on the spread of SARS-CoV-2 in communities, offering an early warning system for public health officials, healthcare providers, policymakers and others, but low-quality data prohibits estimating prevalence or identifying variants. To address these shortcomings, a team of scientists from Scripps Research Institute and the University of California San Diego (UCSD) developed a new method to increase the amount of viral RNA available to be sequenced in a small wastewater sample and a surveillance tool, called “Freyja,” that uses an algorithm to detect new variants more quickly and reliably, up to 2 weeks before they are identified in clinical sequencing and with enough time to take action. The study describing the work was published July 7 in the journal Nature. The testing technique shortens the time to sequence samples, from weeks to days, which may help to identify and rapidly respond to emerging variants in the future.
by ponchi101 Not cheerful news. Summary: this is not longer a pandemic, it is a societal condition. Will remain with us forever.
by dryrunguy That section on Pulse Oximetry... Wow. Who knew something like that was even possible? How on Earth does skin color cause a MACHINE to overestimate oxygen levels? It makes no sense at all. Clearly, I'm missing something.
by Cuckoo4Coco
ponchi101 wrote: ↑Tue Jul 12, 2022 5:54 pm
Not cheerful news. Summary: this is not longer a pandemic, it is a societal condition. Will remain with us forever.
It is something that I think we will have to get a shot for every year just like the Flu.
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 555 million cumulative cases and 6.35 million deaths worldwide as of July 13. The global weekly incidence increased for the fifth consecutive week, up 12.5% from the previous week. As the WHO’s IHR Emergency Committee noted, there appears to be a “decoupling” of cases from deaths, as we are not observing a commensurate increase in weekly mortality at the global level. Global weekly mortality remained relatively steady at slightly more than 10,000 deaths, an increase of 1.1% over the previous week.
The African region continues to report decreasing trends in weekly incidence, down to 16,404 new cases last week—a 27% decrease from the previous week and the lowest weekly total since May 2020. South-East Asia increased for the sixth consecutive week, but it appears to be reaching a peak or plateau. The Americas reported a slight decrease last week, but considering that included the US Independence Day holiday weekend, it could be a residual effect of delayed reporting. All other regions reported substantial increases last week: Eastern Mediterranean (+24.7%), Europe (+15.9%; and now its third-highest peak), and Western Pacific (+27.9%).
UNITED STATES
The US CDC is reporting 88.8 million cumulative cases of COVID-19 and 1,017,391 deaths. The average daily incidence has essentially plateaued over the past several weeks, holding relatively steady at approximately 100-110,000 new cases per day, although it may be exhibiting early signs of increasing. The weekly average jumped from 109,828 new cases per day on July 10 to 123,365 on July 12 (+12%); however, additional data are needed to determine if this is the beginning of a longer-term trend or just recovery from delayed reporting over the US Independence Day holiday weekend. The 185,786 new cases reported on July 12 is the second-highest single day total since the plateau began, and it is the highest in a non-holiday week since February.* Like we observed at the global level, there appears to be a “decoupling” of cases from deaths in the US. The average daily mortality has held relatively steady at approximately 275-350 deaths per day since late April.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions (+12.0% over the past week) and current hospitalizations (+11.4%) continue to increase, despite the ongoing plateau in daily incidence. New hospitalizations among children aged 17 years and younger are approaching its second-highest peak (November 2021). The most rapid increases in current hospitalizations are being reported in Alabama (+22%), Arkansas (+30%), Louisiana (+21%), New Hampshire (+24%), Oklahoma (+21%), Rhode Island (+22%), South Carolina (+39%), and West Virginia (+24%).
Community transmission in the US is increasingly driven by the Omicron BA.5 sublineage. BA.5 is projected to have accounted for more than half of sequenced specimens starting the week of July 2, and the estimate reached 65% for the week of July 9. The BA.4 sublineage is also increasing in prevalence, although much more slowly than BA.5. The BA.4 sublineage increased from an estimated 16.1% to 16.3% over the past 2 weeks, and we expect it to replace BA.2.12.1 as #2 nationally in the coming weeks. Together, Omicron variants represent essentially all new cases in the US.
COVID-19 REMAINS PHEIC In a meeting on July 8, the WHO’s International Health Regulations (IHR) Emergency Committee recommended that the COVID-19 pandemic continues to constitute Public Health Emergency of International Concern (PHEIC), the committee’s twelfth such meeting since the onset of the pandemic. On July 12, WHO Director-General Dr. Tedros Adhanom Ghebreyesus issued a statement indicating that he concurred with the committee’s recommendation and presented minutes from the meeting. He also called on national governments to implement appropriate protective measures, noting that many countries have essentially lifted all COVID-19 restrictions, which is allowing transmission to spread largely unabated.
The committee members emphasized the ongoing uncertainty and unpredictability of the pandemic, particularly in the context of emerging variant characteristics and the evolution of the SARS-CoV-2 virus. Additionally, the global daily COVID-19 incidence has increased 30% over the past 2 weeks, although the committee acknowledged that recent data indicates a “decoupling” of cases from hospitalizations and mortality, due in large part to vaccination coverage and therapeutic availability. As has been the case since the onset of the pandemic, the expert committee also highlighted shortcomings in disease surveillance capacity around the world, and it specifically addressed challenges posed by rapid at-home tests and the need to incorporate those results into national surveillance data. The COVID-19 pandemic was first declared a PHEIC on January 30, 2020.
NOVAVAX VACCINE EUA The US FDA on July 13 granted emergency use authorization (EUA) to Novavax, a small Maryland-based biotechnology company, for use of its 2-dose primary series COVID-19 vaccine among adults ages 18 years and older. The FDA authorized the vaccine based on data from the company’s Phase 3 clinical trial, PREVENT-19, which demonstrated 90.4% efficacy in preventing mild, moderate, or severe COVID-19 among about 17,200 study participants who received the vaccine. The vaccine is the first COVID-19 vaccine authorized in the US that uses a more traditional protein-based platform. FDA advisors expressed hope that the vaccine’s authorization may convince individuals skeptical of mRNA vaccines to seek vaccination. On July 12, prior to the FDA’s EUA announcement, the US government announced it secured an initial 3.2 million doses of the Novavax vaccine. The US CDC’s Advisory Committee on Immunization Practices (ACIP) is scheduled to meet next week and is expected to recommend use of the vaccine for adults.
VACCINE PLATFORM COMPARISON According to an expert review of 79 real-world studies, available 2-dose vaccines meant to prevent COVID-19 are equally protective against hospitalization (91-93%) and death (91-93%) from COVID-19 whether they use a viral vector or mRNA platform. The study, published in the journal Expert Review of Vaccines, compared data for 2 doses of Pfizer-BioNTech’s and Moderna’s mRNA vaccines, or a combination of the shots, and AstraZeneca-Oxford’s viral vector vaccine Vaxzevria. The data reflected protection against Delta and earlier SARS-CoV-2 variants, although emerging data from the UK Health Security Agency and public health agencies in Brazil indicate similar levels of protection from severe COVID-19 health outcomes due to the Omicron variant after a booster, or third, dose. New analysis from Airfinity, a London-based data firm, shows that the Pfizer-BioNTech and AstraZeneca-Oxford vaccines saved an estimated 12 million lives in their first year of use (December 2020 to December 2021), with the Pfizer-BioNTech vaccine accounting for 5.9 million and the AstraZeneca-Oxford vaccine for 6.3 million lives saved.
VACCINE ACCESS Health officials worldwide continue to warn of the risks of increasing COVID-19 cases and hospitalizations due to the Omicron subvariant BA.5, now predominant in several regions, with many recommending fourth vaccine doses, or second booster shots, for specific populations. In the US, in an effort to stem increasing COVID-19 hospitalizations, fourth doses may soon become available to all adults, according to health officials. In Europe, the European Centre for Disease Prevention and Control (ECDC) and the European Medicines Agency (EMA) this week updated guidance to recommend a second vaccine booster for all individuals over age 60 as well as medically vulnerable people in Europe. Additionally, the WHO European Technical Advisory Group of Experts on Immunization (ETAGE) urged EU member states to ensure people are up-to-date on their vaccinations and encouraged expanding eligibility for second booster doses to include moderately and severely immunocompromised individuals aged 5 years and above and their close contacts, older adults, healthcare workers, and pregnant women.
Meanwhile, Africa—where only 20% of the population is fully vaccinated—continues to be left behind. Without the ability to manufacture vaccines or outcompete wealthier nations in securing purchases directly from pharmaceutical companies, the continent, as well as low- and middle-income countries (LMICs) in other regions, are relying on charity from higher-income countries, including the US. But rather than global solidarity, vaccine nationalism and hoarding during the first year of COVID-19 vaccine availability resulted in a 2-tier vaccine rollout that ultimately led to vaccine waste and low vaccination rates in LMICs. Now, health leaders in Africa and elsewhere are calling for a restructuring of the global health architecture with a focus on inclusivity, equity, and partnership to enable LMICs to establish vaccine and medicine research, development, and manufacturing capabilities. In one effort, 15 nations in the global south are working with the WHO and other groups to establish the mRNA vaccine technology transfer hub, an initiative aimed at empowering lower-income countries to develop and produce their own vaccines for COVID-19 and other diseases and ultimately lessen their dependence on higher-income countries.
ANTIMICROBIAL RESISTANCE Between 2012 and 2017, the number of deaths from antimicrobial-resistant (AMR) infections in the US declined 18% overall and nearly 30% in hospitals due in large part to prevention efforts such as improving infection prevention and control and antimicrobial stewardship. But those gains were largely reversed during the first year of the COVID-19 pandemic, as both drug-resistant hospital-acquired infections and deaths increased at least 15% in 2020, according to a new US CDC analysis. Several factors likely contributed to the setback, including a shift in public health resources from tracking and preventing antimicrobial resistance to COVID-19 efforts; the incorrect use of antibiotics to treat COVID-19 patients, which is a viral, not bacterial, disease; sicker patients needing more frequent and longer use of invasive care, such as catheters and ventilators; and overwhelmed hospitals that experienced shortages of staff, personal protective equipment, and other supplies.
The CDC estimates that more than 2.8 million AMR infections occur annually in the US, with 35,000 people dying of those infections. But the total number of AMR-related deaths in 2020 is likely much higher, according to the report. In a forward, CDC Director Dr. Rochelle Walensky wrote that the setbacks in preventing AMR infections “can and must be temporary,” noting that the COVID-19 pandemic’s major takeaway is that “prevention is preparedness.” In related news, the WHO this week released its first-ever report on the pipeline of vaccines currently in development for AMR bacterial pathogens, including several in late-stage development that address diseases on the bacterial priority pathogens list.
PEOPLE WITH DISABILITIES Many people with disabilities in the US, including those who are immunocompromised, feel left behind as COVID-19 mitigation measures are lifted and the world attempts to find a new sense of normalcy. According to a survey conducted in April by Data for Progress, 57% of disabled people surveyed believe masks should be required on public transportation and 64% feel they should be required for air travel. People with disabilities and their advocates are calling for additional efforts to stop the spread of COVID-19, such as requirements to wear a mask in public spaces, investments in indoor air filtration improvements, and more widespread wastewater surveillance to help predict community transmission levels. They point out that as the number of people with disabilities increases—specifically those who develop post-acute sequelae of SARS-CoV-2 infection (PASC), commonly known as long COVID—more public health measures aimed at stemming disease transmission are vital to provide a sense of safety for everyone.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
CONCERN OVER BA.5 SUBVARIANT As the Omicron subvariant BA.5 drives increases in COVID-19 cases and hospitalizations in several regions and countries worldwide, health officials are, for the most part, holding back on sounding alarms. In the US, where the average number of cases and hospitalizations are at their highest levels since February, many state and local health authorities are characterizing the increase in cases as concerning but not disturbing, with many saying repeated warnings about COVID-19 surges are falling on pandemic-fatigued ears. However, US health officials are speaking out. White House COVID-19 Coordinator Dr. Ashish Jha has warned the BA.5 subvariant is the most immune evasive variant yet, urging US residents to stay up to date on their vaccines and expressing support for the reinstatement of mask mandates. Chief Medical Advisor to the US President Dr. Anthony Fauci called on eligible people to get vaccine boosters and said a decision about boosters for those under age 50 likely will soon be announced. In Europe, the WHO announced today that COVID-19 case numbers have tripled and hospitalizations have doubled across Europe over the past 6 weeks. WHO Europe Director Dr. Hans Kluge warned that people should not underestimate BA.5, calling on nations to bolster vaccine uptake and require mask wearing.
A dearth of data is complicating the true picture of how big BA.5-driven surges are, or will get, as publicly reported data has become less common due to the closing of testing sites and an increase in at-home test use. Some experts estimate that for every 1 reported case, there are 7-10 unreported cases. Additionally, BA.5 has several spike protein mutations that make it better at infecting human cells and evading immunity from vaccination or previous SARS-CoV-2 infection. These capabilities allowed the subvariant to gain predominance in the US in just over 2 months, and it is now causing 3 of every 4 new COVID-19 cases in the nation. BA.5 is so adept at skirting immune defenses that many people who were recently infected with a different Omicron variant are becoming reinfected. Some studies suggest that reinfections could cause lasting symptoms. And as the virus continues to circulate, there is a real risk of further mutations, meaning we likely will be living with some form of the virus for the foreseeable future.
VACCINE BOOSTERS The administration of US President Joe Biden is pressing the need for US residents aged 50 years and older and immunocompromised individuals to get their second COVID-19 vaccine booster as soon as possible due to the immune-evasive nature of the Omicron subvariant BA.5, as well as said a decision is expected soon about additional booster doses for all adults. According to US CDC estimates, BA.5 is now responsible for 78% of all new COVID-19 cases. Officials have stressed that booster doses provide additional protection against earlier Omicron subvariants and potentially later subvariants as well. However, current boosters have not yet been updated to more specifically target Omicron and its subvariants, leaving a dilemma for eligible individuals about whether to get a booster now or wait for updated versions. Additionally, some experts wonder and worry whether BA.5 will even be the predominant variant in the fall, potentially making new boosters less effective than expected.
Only 34% of the US population aged 5 years or older has received their first booster dose, COVID-19 pandemic response funding is dwindling, and public appetite for continued vaccinations is diminishing. All of these uncertainties create a perfect storm for risk communication difficulties for experts and officials alike, uncertain of the best course to recommend and how to inform the public about their choices. Some experts hope that next-generation vaccines, such as nasal vaccines—which may have a higher chance of preventing not just severe disease outcomes but also infection—or pan-coronavirus vaccines—which may work better against future variants as well as current variants—may help to boost vaccination rates. Additionally, the CDC is expected to make an announcement about its recommendations for the newly authorized Novavax vaccine later today. Some hope the protein-based vaccine also will help boost vaccination rates among unvaccinated individuals.
In related news, the British government on July 15 announced that individuals aged 50 or older, certain individuals in high-risk professions, and individuals over age 5 who are more likely to be at risk of severe disease outcomes will be eligible for a second booster dose in the fall. The announcement broadens eligibility beyond those who are aged 65 years and older.
YOUNG CHILD VACCINATIONS US medical experts and public health officials are expressing concern over low demand for COVID-19 vaccinations for the youngest children under age 5 and those ages 5-11. States were charged with ordering doses commensurate to expected demand, but some states’ orders only cover a small fraction of their child residents. For example, Mississippi has ordered enough vaccine doses to cover only 16% of its under-5 population with 1 dose. Florida did not preorder any doses for its under-5 population. Many parents there are struggling to find medical practitioners and health systems, which were able to independently order doses, that can provide the shots. The impacts are highest among families in underserved areas and those who rely on government-run health services. However, other experts caution that some states’ initial orders may not reflect future demands and childhood COVID-19 vaccination coverage. They say several factors may change over time, such as available vaccine storage, rampant misinformation, limited initial appointment slots, pushback from parents, reimbursement and logistical challenges, and some practitioners preferring to wait for full FDA approval prior to delivering vaccinations to younger populations.
Relatedly, Europe also may soon be administering vaccines to young children, as the European Medicines Agency (EMA) on July 18 began reviewing Pfizer-BioNTech’s vaccine for use in children aged 6 months to 4 years. Notably, increasing vaccination rates among young children at this point in the global response is paramount and could provide high impact. A recent study in JAMA Network Open found that antibody levels in previously infected individuals waned quickly over the first 200 days post-infection, with levels dropping most quickly in children under age 6.
WESTERN PACIFIC REGION A new wave of COVID-19 cases has hit the Western Pacific region, largely driven by the BA.4 and BA.5 Omicron subvariants. In Japan, cases are rising in every prefecture. The 7-day rolling average of new daily cases has surpassed February’s Omicron peak, and transmission does not seem to be slowing. The situation was further complicated by a 3-day weekend that saw high levels of activity at beaches and other tourist hotspots. The Japanese government is now trying to balance keeping the nation running with few restrictions while preventing hospitals from becoming overwhelmed. Cases also are rising in South Korea, where experts are predicting 200,000 daily cases by late-August, which would amount to half of the nation’s previous Omicron wave in March.
Hospitals in several Australian states are reaching capacity under the nation’s latest surge. Experts warn that while many emergency rooms are overwhelmed, most areas of the nation remain weeks away from their expected peak hospitalization rates. The situation is further complicated by a worse than average influenza season. According to data from the New York Times, New Zealand—a nation famous for early successes against COVID-19—now has the third highest daily confirmed rate of cases per 100,000 people of all nations, after Brunei and San Marino. Experts are concerned that the strain of new cases could lead to a collapse of the nation’s healthcare workforce. As a result, New Zealand officials are urging a renewed sense of urgency around COVID-19 precautions, including masking and testing.
In China, approximately 264 million people across 41 cities are under full or partial lockdown as part of the nation’s zero-COVID policy. Health experts are worried that the zero-COVID policy could become difficult to maintain given the increased transmissibility of the Omicron BA.4 and BA.5 subvariants. Some larger Chinese cities are rolling out new measures, such as mass testing and intense lockdowns, to try to curb the spread of the virus. There are growing concerns that increased COVID-19 prevention measures could further destabilize a struggling global economy.
ECONOMIC IMPACTS Fears of a global economic recession are on the rise. The global economic web was unsettled earlier this year when Russia invaded Ukraine, lowering the availability of energy, fertilizer, and food supplies. However, the largest disruptor of economic growth is the ongoing COVID-19 pandemic. The early phases of the pandemic disrupted the production of goods and the availability of services when governments implemented lockdowns to prevent transmission of the SARS-CoV-2 virus. However, the lockdowns prompted those stuck at home to begin ordering enormous volumes of goods over the internet. The combination of laborers stuck at home plus sky-high demand resulted in a global supply chain crisis. The supply chain crisis pushed prices for goods and services higher, and some industries have taken advantage of the global instability and their market dominance to secure record-breaking profits. Additional factors impacting inflation in the United States include an aggressive stimulus initiative and hesitancy by the Federal Reserve to increase interest rates.
The COVID-19 pandemic also is responsible for economic downturns in other nations with a large impact on the global market, including China. China has adopted an aggressive and highly controversial zero-COVID policy that has led to forced lockdowns in many of the country's large cities. The lockdowns have prevented normal industrial operations that supply a large portion of the world’s manufactured goods. The disruption in production and shipping of goods has significantly slowed growth for the Chinese economy, which shrank by 2.6% during the latest quarter. This slowdown, which denotes a growth of only 0.4% from the end of June last year, represents the lowest growth rate since early 2020, when the nation completely shut down to fight the pandemic. The latest economic reports have cast doubt on whether China can reach its 5.5% growth target for the year set by the ruling Communist party.
However, a couple of recent studies hint that aggressive COVID-19 responses might limit economic damage in the long-term. One study, an assessment of business closure policies in New York City published by the International Monetary Fund, set out to determine the impact of closures in specific industries on the spread of COVID-19. According to the results, reopening businesses early allowed New York City to recover functionality as an economic hub but at the cost of a large wave of infections in 2020. The study also found that an alternative policy that extended lockdowns made future travel safer and was ultimately more cost-effective. Another study, examining the impact of long COVID on the workforce of the UK, estimated that 80,000 people have left the UK workforce due to long COVID as of March 2022. According to the authors, continued pandemic waves will lead to more people missing work, losing jobs, or permanently leaving the workforce due to long COVID. While many experts agree that a zero-COVID policy is unrealistic, it is becoming rapidly apparent that pretending like the pandemic is over may also lead to long-term and impactful health and economic consequences.
GLOBAL VACCINE ACCESS Last month, the 12th World Trade Organization (WTO) Ministerial Conference agreed to a version of a proposal for a global intellectual property waiver to allow countries to more easily use patented technologies to develop COVID-19 vaccines. Originally proposed only a few months into the pandemic by India and South Africa, and endorsed by more than 100 other nations, the approved deal on a Trade-Related Aspects of Intellectual Property (TRIPS) waiver is much narrower in scope than the original proposal and likely comes too late to make a significant impact on vaccine access. The deal does not include intellectual property waivers for diagnostics, treatments, or other COVID-19-related medical tools, and it excludes countries with “existing” production capacity. The power imbalances in both the COVID-19 pandemic and the WTO negotiations are apparent, from vaccine nationalism to sluggish negotiations. But over the past 2 years, low- and middle-income countries (LMICs) from South America to Africa have worked to solidify plans to cooperate on mRNA technologies in order to develop and produce their own versions of vaccines for SARS-CoV-2 and other diseases. This effort to collaboratively develop an mRNA vaccine technology transfer hub, which is supported by the WHO and the US NIH, must overcome significant challenges but provides hope for a new model to enable more LMICs to overcome future disease outbreaks more effectively, without having to rely on high-income countries or corporations.
MENSTRUAL CYCLES When COVID-19 vaccines became widely available in 2021, recipients were made aware of the potential for adverse events—including fever, fatigue, headache, and pain at the injection site—because the side effects were documented in clinical trials. But those clinical trials did not track effects on the menstrual cycle. After hearing hundreds of anecdotes from people who experienced temporary irregularities in menstruation after receiving a vaccination, such as heavier bleeding or breakthrough or unexpected bleeding, researchers from the University of Illinois at Urbana-Champaign and Washington University School of Medicine in St. Louis surveyed more than 39,000 menstruating or previously menstruating people ages 18 to 80 years old who were fully vaccinated and had no history of COVID-19.
The survey results, published July 15 in Science Advances, show that 42% of people with regular menstrual cycles bled more heavily than usual after receiving a vaccine dose, 44% reported no change, and about 14% reported lighter bleeding. Among people who were not menstruating at the time of vaccination, including those who are post-menopause or who use long-term contraceptives or hormones, many experienced breakthrough bleeding. The authors note the study has several limitations, such as not having a control group, but they say more attention to people’s experiences can help to gain a better understanding of the issue, provide evidence for further research, and build trust in medicine by offering vaccine recipients warning that they may experience menstrual irregularities.
CRUISE SHIPS The US CDC announced on July 18 that its COVID-19 Program for Cruise Ships is no longer in effect. Although the agency will continue to publish guidance to help cruise ships provide safer and healthier environments for crews and passengers, the color-coded chart and spreadsheet that detailed the level of spread on ships is no longer available. According to a statement in the webpage’s FAQ section, the CDC is ending the program because it depended on each cruise line having the same testing and screening guidelines, which now all differ among companies. However, cruise ships will continue to report COVID-19 cases to the CDC, and passengers have the option of directly contacting their cruise line for information on outbreaks aboard their ship.
by ponchi101
dryrunguy wrote: ↑Tue Jul 19, 2022 6:44 pm
A dearth of data is complicating the true picture of how big BA.5-driven surges are, or will get, as publicly reported data has become less common due to the closing of testing sites and an increase in at-home test use. Some experts estimate that for every 1 reported case, there are 7-10 unreported cases.
I gather that is how it will be. Just came back from the market and there was a C19 testing site. A few people, but nothing out of the ordinary. So people simply will not get tested, until the symptoms are severe. It will mean more people walking the streets with full bloom infections.
dryrunguy wrote: ↑Tue Jul 19, 2022 6:44 pm
A dearth of data is complicating the true picture of how big BA.5-driven surges are, or will get, as publicly reported data has become less common due to the closing of testing sites and an increase in at-home test use. Some experts estimate that for every 1 reported case, there are 7-10 unreported cases.
I gather that is how it will be. Just came back from the market and there was a C19 testing site. A few people, but nothing out of the ordinary. So people simply will not get tested, until the symptoms are severe. It will mean more people walking the streets with full bloom infections.
And then when the symptoms get severe for tons of people and the lines are huge for testing and they become short of supplies for testing then people will complain about that.
by MJ2004 Boston.com has had a Covid-19 link on their home page for the daily numbers, etc. Today, just as cases are increasing and the city of Boston is once again asking people to wear masks indoors, the link has disappeared from the site.
Nothing to see here.
by dryrunguy Here's the latest Situation Report. Lots going on here...
::
EPI UPDATE The WHO COVID-19 Dashboard reports 562.7 million cumulative cases and 6.37 million deaths worldwide as of July 20. The global weekly incidence remained relatively stable after an increasing trend for the past 5 weeks, up 1.54% from the previous week. Global weekly mortality also remained stable, rising 0.5% over the previous week with 11,257 total reported deaths.
At the regional level, the Western Pacific (+37.83%), Americas (+9.53%), and Southeast Asia (+5.25%) experienced increases in new cases, while Europe (-13.88%), the Eastern Mediterranean (-3.88%), and Africa (-21.91%) regions had decreasing trends. The number of new weekly deaths increased in the Southeast Asia (+20%), Eastern Mediterranean (+15%), and Americas (+7%) regions, decreased in the Africa (-39%) and Europe (-14%) regions, and remained stable in the Western Pacific region.
UNITED STATES
The US CDC is reporting 89.7 million cumulative cases of COVID-19 and 1,020,355 deaths. After plateauing over the past several weeks around 100-110,000 new cases per day, the weekly average increased to 126,018 on July 19. The average daily mortality has held relatively steady at approximately 275-350 deaths per day since late April.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions (+7.8% over the past week) and current hospitalizations (+6.9%) continue to increase, possibly reflecting the slight increase in daily incidence.
Community transmission in the US is primarily driven by the Omicron BA.5 sublineage. BA.5 is projected to have accounted for more than half of sequenced specimens starting the week of July 2, and the estimate reached 77.9% for the week of July 16. The BA.4 sublineage accounts for a smaller proportion of cases and appears to be decreasing in prevalence. The BA.4 sublineage fell from an estimated 16% over the past 2 weeks to 12.8% the week of July 16, and is now outpacing BA.2.12.1 as the second most prevalent sublineage. Together, Omicron variants represent essentially all new cases in the US.
NOVAVAX VACCINE The CDC Advisory Committee on Immunization Practices (ACIP) on July 19 voted 12-0 to recommend the use of the Novavax recombinant protein COVID-19 vaccine as a 2-dose primary series for adults aged 18 years and older. Within hours of the vote, CDC Director Dr. Rochelle Walensky endorsed the recommendation, prompting a rollout over the coming weeks of 3.2 million doses the US has secured. As the fourth COVID-19 vaccine to be authorized in the US, the Novavax vaccine offers a more traditional vaccine technology, which some hope will prompt US vaccination holdouts wary of the newer mRNA technology to get vaccinated. The approach is similar to that of vaccines for influenza and HPV—protein-based vaccines that make the immune system recognize modified pieces of the target virus. In a statement, US President Joe Biden, who today tested positive for COVID-19, applauded the news and noted vaccines continue to protect people from serious COVID-19-related illness, hospitalizations, and death. President Biden, who is up to date on his vaccinations, also encouraged US residents to vaccinate their children and get a booster dose if they are eligible.
VACCINE-INDUCED IMMUNITY Virologists and health officials are trying to stay one step ahead of the constantly mutating SARS-CoV-2 virus in order to develop future vaccines, treatments, and other interventions. However, those predictions are complicated, with experts depending on modeling based on what we already understand about the virus. Several recently published studies examine how well current vaccines elicit immunity against Omicron variants.
Published July 19 in Science, a study of spike protein function and neutralizing capability of 7 different SARS-CoV-2 vaccines against Omicron sublineages shows that a large number of the sublineage mutations lead to enhanced ACE2 binding and reduced plasma neutralizing activity. However, homologous or heterologous boosters markedly increased neutralizing antibody titers against BA.1, BA.2, BA.2.12.2, and BA.4/5 across all vaccines evaluated to provide sufficient protection against Omicron-induced severe disease. The vaccines evaluated included mRNA vaccines from Moderna and Pfizer-BioNTech, viral-vectored vaccines from J&J-Janssen, AstraZeneca-Oxford, and Sputnik V, as well as the Novavax and Sinopharm vaccines that use different platforms.
Another study, published in Cell Reports Medicine and led by researchers at NIAID, examined a “mix and match” booster strategy. The findings suggest that nearly all vaccine combinations elicited high levels of neutralizing antibodies against the BA.1 sublineage, but antibody levels remained low in the group that received the J&J-Janssen vaccine for both primary series and booster dose. Notably, the neutralizing antibody levels of all groups decreased substantially (2.4-5.3 fold) by the third month following the booster dose, which is consistent with real-world reports of waning immunity over time.
Another preprint study posted to medRxiv evaluated a 3- or 4-dose regime of the Pfizer-BioNTech vaccine, showing that the fourth dose elicited “significant rise in antibody binding and neutralizing titers against multiple variants” and reduced the risk of symptomatic infection. In the 3-dose group, 45% of participants developed infection during the 90-day follow up period compared to 30% in the 4-dose group. The study notes that several IgG and IgA markers and their combinations were correlates of protection (COP). The paper also recommends further study of a subpopulation identified with low-baseline antibody levels after 3 doses who were at increased risk of infection despite receiving a fourth dose.
COVID-19 TREATMENTS Researchers continue efforts to develop COVID-19 treatments for people with mild disease or those who are not at high risk of progressing to severe illness. Several treatments, including monoclonal antibodies and antivirals, are authorized for people at high risk of severe disease, but those medicines might not benefit people who fall into lower risk categories. Pfizer recently announced it is ceasing enrollment into its clinical trial evaluating whether the antiviral Paxlovid would help standard-risk patients, saying they could not obtain sufficient data on whether the drug prevented hospitalization or death in this population. Some COVID-19 patients are turning to unproven or alternative treatments, whether they qualify for authorized medicines or not. Additionally, some individuals with long COVID are seeking out experimental therapies, such as “blood washing,” due to a lack of treatments for lasting COVID-19 symptoms. For some, distrust—in the healthcare system, research methods, or doctors—is the reason they seek out often expensive and potentially useless or even harmful therapies. But others feel desperate for help when they test positive, as there are no COVID-19-specific treatments currently recommended for people who do not fall into a high-risk category.
US PANDEMIC PREPAREDNESS The administration of US President Joe Biden is reorganizing the US Department of Health and Human Services to elevate the Office of the Assistant Secretary for Preparedness and Response (ASPR) from a staff division into an independent operating division—similar to the US CDC, FDA, and NIH—responsible for leading the nation’s responses to future pandemics and health emergencies. Under the reorganization, ASPR will now be known as the Administration for Strategic Preparedness and Response, and efforts to stand up the new division will be phased in over the next 2 years. ASPR oversees the Strategic National Stockpile, the national Medical Reserve Corps, and contracts for and distribution of vaccines and certain medicines in health emergencies. Though many current and former HHS officials welcomed the move, other experts say that shifting some health emergency coordination responsibilities to ASPR could undercut response efficacy, create confusion and tension, and does not address ongoing challenges at CDC, which has much closer relationships with states.
US GLOBAL RESPONSE Funding for the US Agency for International Development’s (USAID) global COVID-19 response efforts will soon run dry if the US Congress does not authorize additional financing, USAID Assistant Administrator for Global Health Dr. Atul Gawande warned at a healthcare summit this week. USAID is responsible for coordinating US global COVID-19 response efforts, helping more than 120 countries address the pandemic over the past 2.5 years, delivering nearly 566 million vaccine doses of the 1.1 billion the US has pledged to donate, as well as providing diagnostics, treatments, and other tools. But funding for the agency’s COVID-19 task force ran out last month, and Congress has not moved to reauthorize financing for the program, which needs a minimum of US$5 billion to continue operations.
Also this week, US Secretary of State Antony Blinken and Minister of Foreign Affairs of Japan Hayashi Yoshimasa co-hosted a virtual COVID-19 Global Action Plan (GAP) Foreign Ministerial Meeting with representatives of more than 25 countries, the African Union, WHO, and World Bank. The meeting was a follow-up to the June 15 COVID-19 Senior Officials Meeting, and came in the same week Japan set a record for new daily COVID-19 cases, exceeding 180,000 cases today. Participants discussed the ongoing need for equitable and sustainable access to vaccines, diagnostics, and treatments, as well as ways to close gaps in vaccine confidence, distribution, uptake, and funding, for both the current pandemic and future health emergencies. In remarks, WHO Director-General Dr. Tedros Adhanom Ghebreyesus cautioned that the number of global COVID-19 cases is elevated again, lauded the establishment of a new Financial Intermediary Fund (FIF) at the World Bank, and called on nations to work toward ending the acute phase of the pandemic by focusing on vaccinating at-risk populations and reaching the WHO goal of 70% vaccination coverage in all nations.
BERLIN DECLARATION Many nations remain significantly behind in their efforts to reach a WHO goal of vaccinating 70% of the global population against COVID-19. The latest data from Our World in Data show that only 1 in 7 people in low-income countries are fully vaccinated compared with 3 in 4 people in high-income countries. Activists across the world are calling for a renewed push to close this gap, particularly as circulating and emerging variants threaten to put additional strain on healthcare systems and avert available response tools. As new COVID-19 cases rise once again in several regions, many organizations are focused both on COVID-19 and future pandemic responses, including bolstering healthcare system infrastructure.
On July 19, the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) published the Berlin Declaration, a set of recommendations for strengthening equitable vaccine access for future health crises. IFPMA represents many biopharmaceutical players, including many of the companies involved in COVID-19 product development, like Pfizer, Moderna, AstraZeneca, GSK, and Merck. The Berlin Declaration lays out lessons learned in the global response to COVID-19 and proposes using several approaches—including donations, not-for-profit supply, voluntary licenses, and tiered-pricing systems—to help ensure pandemic interventions are available to countries of all income levels. However, the declaration says the first step is for lower-income countries to develop infrastructure to receive and deliver vaccines and other medical countermeasures and calls on the G7, G20, and other global stakeholders to take steps to accelerate resource and financial capacity for countries to strengthen product delivery infrastructure. In reaction to the Berlin Declaration, which is not legally binding, some advocates accused the pharmaceutical industry of shifting blame and onus onto lower-income nations and shirking public responsibility to equitably supply health interventions, some of which were developed using public funding.
dryrunguy wrote: ↑Tue Jul 19, 2022 6:44 pm
A dearth of data is complicating the true picture of how big BA.5-driven surges are, or will get, as publicly reported data has become less common due to the closing of testing sites and an increase in at-home test use. Some experts estimate that for every 1 reported case, there are 7-10 unreported cases.
I gather that is how it will be. Just came back from the market and there was a C19 testing site. A few people, but nothing out of the ordinary. So people simply will not get tested, until the symptoms are severe. It will mean more people walking the streets with full bloom infections.
People are getting tested at home. The trend with this latest variant, anecdotally, is that it doesn't show up on tests until days in, after symptoms have started subsiding for those who are symptomatic.
I think the 7-10 unreported for every reported is a low estimate. I know more than 10 people who'd been sick in the last 2-3 weeks. I think only one of them got tested at a testing site and all the people I know are fairly responsible and believe in the science.
by ponchi101 Flew yesterday into Vennieland. As part of immigration policies, I had to take a test upon entry (PLUS showing my vaccination status).
In total, 12th C19 test I have taken. 12 negatives. I am suspicious that I am one of those lucky ones that are immune to this stuff.
Lucky me, I know. I will still wear my mask and get my shots (double boosted already).
by Cuckoo4Coco
ponchi101 wrote: ↑Sun Jul 24, 2022 4:13 pm
Flew yesterday into Vennieland. As part of immigration policies, I had to take a test upon entry (PLUS showing my vaccination status).
In total, 12th C19 test I have taken. 12 negatives. I am suspicious that I am one of those lucky ones that are immune to this stuff.
Lucky me, I know. I will still wear my mask and get my shots (double boosted already).
I think it is better to be safe then sorry. My mom is a Physician's Assistant and she is a big advocate of still wearing masks and washing hands, using hand sanitizer and stuff like that. Glad you have never had Covid.
by Suliso Right now I wouldn't fly anywhere on vacation where I needed a test. A giant waste of money (here ca 150 $/person).
by ponchi101
Suliso wrote: ↑Mon Jul 25, 2022 11:21 am
Right now I wouldn't fly anywhere on vacation where I needed a test. A giant waste of money (here ca 150 $/person).
Agree. But of course I am not here on vacation.
by Suliso I know...
by dryrunguy Here's the latest Situation Report. Two sections caught my attention: 1) COVID Virgins (several of us seem to fall in that rapidly declining group--at least as far as we know) and 2) the appalling lack of COVID therapeutics used within the Bureau of Prisons system.
BTW, you can add one more to the number of COVID deaths in the United States. COVID claimed my oldest brother's life this morning at about 4:15 a.m. He had been in intensive care for 5 weeks. It started out as treatment for a serious bladder infection. But while in the ICU, he contracted COVID about 3 weeks ago. He was intubated for a third time on Saturday while I was in Ohio this past weekend to see him and my mother. Last night, his heavily infected lungs just gave out. They heavily sedated him, removed the ventilator, and he quickly passed away in his sleep.
::
VACCINATION STRATEGIES The WHO last week published an updated COVID-19 vaccination strategy prioritizing vaccination of certain populations, including healthcare workers, older people, individuals with underlying conditions, and other vulnerable groups. The focus is on reaching 100% of those populations while continuing efforts to achieve the goal of vaccinating 70% of the global population. The latter target was missed this month, as only 58 countries had vaccinated 70% of their population by mid-year. The new goal remains a challenge; only 28% of older adults and 37% of healthcare workers in low-income countries have received a primary vaccination series and most have not had booster doses. The WHO also called for greater equity in locating vaccine manufacturing facilities across all regions; said it will continue to collaborate with the COVAX initiative and other partners to support vaccine rollouts; and urged innovation to develop new vaccines that can substantially reduce SARS-CoV-2 transmission, are easier to administer, and provide longer-lasting and broader protection against current and emerging variants. Efforts are underway globally to create a Coronavirus Vaccines Research and Development (R&D) Roadmap focused on preventing a broad range of coronavirus infections.
In the US, the administration of US President Joe Biden is hosting a meeting today of federal officials, leading scientists, and pharmaceutical representatives to discuss next-generation COVID-19 vaccines, including new technologies and a timeline for development. Current vaccines are highly effective at preventing severe COVID-19-related illness and death, but researchers hope new vaccines will be capable of preventing infection and transmission of current and possibly future SARS-CoV-2 variants, as well as be more easily administered, such as through nasal sprays or skin patches. While some companies are developing Omicron-specific booster shots to be delivered this fall, that strategy—of trying to keep up with variants—is unsustainable over the long term. In related news, the Biden administration has slowed its push to quickly authorize second booster doses for adults under age 50 in the hopes that vaccine makers can have updated Omicron-inclusive shots as early as mid-September.
POST-COVID CONDITIONS IN CHILDREN An international study published July 22 in JAMA Network Open examined the prevalence of post-COVID-19 conditions (PCCs) in children infected with SARS-CoV-2 90 days after they were treated in emergency rooms. Overall, the study enrolled a total of 8,642 children who visited 36 emergency departments (EDs) in Argentina, Canada, Costa Rica, Italy, Paraguay, Singapore, Spain, and the United States between March 2020 and late January 2021. A total of 1,884 of the enrolled children tested positive for SARS-CoV-2 and completed a 90-day followup appointment. The study found that, overall, 5.8% of the children with COVID-19 who attended a followup appointment reported PCCs, including symptoms such as fatigue or weakness, cough, shortness of breath, and other respiratory issues that are in line with what most call “long COVID.” The rate was higher among children who were hospitalized (9.8%), regardless of symptom severity, compared with those who were discharged from the ED (4.6%). Most children (59.1%) reporting PCCs at 90 days had 1 persistent, new, or recurring health problem, most commonly including respiratory and systemic issues such as fatigue. Additionally, PCCs at 90-day followup were more common among children who were hospitalized for 48 hours or longer compared with those who were not hospitalized; children who had 4+ reported symptoms during their ED visit compared to those with 1-3 symptoms; and children who were aged 14 years or older compared to those younger than 1 year.
The researchers noted that the rates of PCCs among children with COVID-19 were only slightly higher than the rates among uninfected controls but called for appropriate guidance for follow up and treatment of children with COVID-19, as well as appropriate mitigation strategies. Overall, the study showed that children had a lower prevalence of PCCs than has been shown in most studies looking at long COVID in adults, but it is still possible that COVID-19 could lead to additional, future health problems among children. The best way to prevent the possibility of these impacts is to prevent infection. Notably, the study comes at a time when vaccinations for children between the ages of 6 months and 5 years appear to be slowing down in the US, with only 2.8% of the population having received their first dose. This rate of vaccine uptake is much slower than it was for kids between the ages of 5 and 11 years. Parents should be further encouraged to seek vaccinations for their children.
“COVID VIRGINS” An estimated 82% of US residents have been infected with SARS-CoV-2 at least once, according to the Institute of Health Metrics and Evaluation. Some of those individuals may think they have never had COVID-19 because they had an asymptomatic infection, but that leaves about 18% of the US population who have managed to avoid infection, even in times when the risk is high, such as during the winter Omicron surge or now, with the more transmissible BA.5 subvariant circulating widely. But that club of “super-dodgers” or “COVID virgins” becomes more exclusive each day. For example, in the UK, 55% of new COVID-19 cases are occurring among the approximately 15% of people who have never been infected.
The reasons why some people have yet to be infected likely vary, including engaging in preventive behaviors such as mask wearing or having vaccine-induced immunity. Beyond these factors, scientists are examining several others—including individuals’ genetics, immune system function, and the effects of inflammatory conditions such as allergies—that could influence their risk of SARS-CoV-2 infection. A specific genetic mutation in some individuals prevents most HIV strains from entering human cells, effectively rendering them immune to the virus. Something similar could be happening among certain people who have never had a SARS-CoV-2 infection, although some experts say the theory is a long shot. If scientists can identify such a mutation, they could use that knowledge to better understand who is most susceptible to infection and potentially develop new COVID-19 therapeutics.
US HOSPITALS Hospital systems in the US are struggling with funding shortfalls, staffing shortages, and pandemic fatigue as the SARS-CoV-2 Omicron BA.5 subvariant spreads across the nation. Once again, hospitals are reporting staffing problems due to burnout, high staff turnover, and absences due to COVID-19. Officials are worried that burnout could create additional challenges to providing treatment during a new surge of patients. Additional stress is being felt because federal funding for the COVID-19 response is running out. A deal in the US Congress on a $22.5 billion pandemic funding bill fell apart in March due to partisan infighting, leaving hospitals with no additional funds and significantly less flexibility to hire new staff or ramp up COVID-19 response efforts, even if BA.5 or a future variant leads to higher numbers of hospitalizations.
Meanwhile, CDC predictions for how hospitalizations and deaths will change due to BA.5 are uncertain. A forecast of new hospitalizations from 16 modeling groups predicted that the increase could range from 3,100-13,800 new COVID-19 hospitalizations per day by August 12. A similar forecast on new COVID-19 deaths from 17 modeling groups predicted that the increase could range from 1,800-5,600 new deaths per day by August 13. Additionally, a study published July 22 in the CDC’s Morbidity and Mortality Weekly Report (MMWR) showed that 40% of state and local governmental public health agency workers plan to leave their jobs within the next 5 years. More than half (51%) of the survey respondents reported the need for additional staff to adequately respond to COVID-19. The study only highlights public health and healthcare workforce staffing issues that existed prior to the pandemic and continue today. Sustained investments and large-scale healthcare reform is needed to adequately respond to COVID-19 and to prepare for future health emergencies such as a “Disease X” pandemic.
TREATMENT ACCESS IN US PRISONS The Federal Bureau of Prisons (BOP) is under scrutiny for its minimal use of COVID-19 therapeutics. The latest critique comes in a letter from 14 US Senators demanding an explanation for the limited use of therapeutics. Data show that federal prisons issued only 363 prescriptions for COVID-19-authorized antivirals from March 31, 2020, to March 24, 2022. Of those, only 3 prescriptions were for one of the preferred therapeutics, Paxlovid. Officials with the US Department of Health and Human Services said the BOP also has declined distribution of additional therapeutics despite the agency offering assistance. STAT News previously reported on BOP’s poor usage of allotted therapeutics, citing it as the latest example of BOP’s failure to effectively respond to outbreaks, leading to a disproportionately negative impact on inmates who already receive limited healthcare. The BOP reports 55,351 positive SARS-CoV-2 tests of the 128,703 tests completed by inmates in current BOP custody, noting that not all tests are reported to BOP. Currently, 71 of the 97 BOP facilities are listed as Level 3 facilities, operating at the highest level of modifications based on COVID-19 medical isolation rate, combined percentage of staff and inmate completed vaccinations series, and respective community transmission rates.
CHINA In an attempt to alleviate public concerns over SARS-CoV-2 vaccine safety, Chinese health officials this week disclosed that state and ruling Communist Party leaders had received domestically developed and manufactured shots. About 90% of the population is vaccinated against COVID-19 and 56% have received a booster dose. However, only 61% of people above age 80 have finished their primary series, prompting officials to make the unusual disclosure regarding the nation’s leaders. The announcement comes about 2 years after the nation launched its vaccination drive, primarily using vaccines made by Sinovac and Sinopharm. As of July 23, nearly one-fifth of China’s population was under COVID-19-related full or partial lockdown, and the country is experiencing another increase in cases, reporting 976 cases on July 25, versus 800 cases the day prior. China continues to enforce its “zero COVID” strategy, despite the policy’s unpopularity and damage to the national economy.
by ti-amie I'm so sorry for your loss Dry.
by Cuckoo4Coco dryrunguy, I am so sorry for your loss. I will keep you and your family in my thoughts and prayers.
by atlpam Very sorry to hear about your brother dry.
by ponchi101 Losing a sibling is always very difficult. May you remember him with love, Dry.
by dryrunguy My oldest brother and I were not close. But we had a wonderful visit on Friday (the day after his 62nd birthday). That was the first positive interaction he and I had in... about a decade or so.
I worry about my mother. No parent should have to bury a child. But when I talked to her earlier today, she said, "I'm moving on."
At some point, I'll share about the options that were communicated to us on Saturday by medical personnel. All of those were far worse than what actually happened--my brother died heavily sedated, peacefully, and mercifully in his sleep. We couldn't have dreamed of a better passing for him.
by dryrunguy Here's the latest Situation Report. The news from the Western Pacific remains Not Good. And now the percentage of people who get stuck with Long COVID after infection could be as high as 1 in 5. That's pretty astronomical.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 570 million cumulative cases and 6.38 million deaths worldwide as of July 27.* The global weekly incidence remained relatively stable from the previous week, falling 1.2%. Global weekly mortality also remained stable, rising 1.8% over the previous week. However, global weekly mortality has steadily increased since mid-June.
At the regional level, the Western Pacific (+52%), Eastern Mediterranean (+45%), and South-East Asia (+13%) experienced increases in new weekly cases, while Africa (-44%), Europe (-24%), and the Americas (-12%) had decreasing trends. The number of new weekly deaths increased in the Eastern Mediterranean (+88%), Western Pacific (+19%), and South-East Asia (+8%) regions, decreased in the Africa (-47%) and Europe (-6%) regions, and remained stable in the Americas region.
*The WHO notes the case and death data for the Africa region are incomplete and will be updated as soon as more information becomes available.
UNITED STATES
The US CDC is reporting 90.6 million cumulative cases of COVID-19 and 1,023,382 deaths. The 7-day moving average of new daily cases rose slightly over last week, up to 127,786 on July 26. The average daily mortality has risen slightly over the past 2 weeks, up to 366 on July 26, after holding relatively steady at approximately 275-350 deaths per day between late April and July 11.**
Both new hospital admissions (+6.1% over the past week) and current hospitalizations (+5.1%) continue to increase, possibly reflecting the slight increase in daily incidence.
Community transmission in the US is primarily driven by the Omicron BA.5 sublineage. BA.5 is now projected to account for 82% of sequenced specimens, up from 78% for the week of July 16. The BA.4 sublineage continues to account for about 13% of cases, whereas BA.2.12.1 now accounts for only about 5% of cases. Together, Omicron variants represent essentially all new cases in the US.
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
WESTERN PACIFIC For the past several weeks, several countries in the Western Pacific region have reached record high numbers of new daily COVID-19 cases and have led global cases per 100,000 million population compared to countries in other regions. In particular, previous bastions of relative safety from COVID-19, Australia and New Zealand, have undergone their worst surges to date. In the last 7 days, on average, Australia has reported around 45,000 daily new cases while New Zealand has reported around 8,100 daily new cases. Experts predict that some areas of Australia will peak in cases around mid-August, while New Zealand appears to have turned away from its worst-case prediction scenario as case numbers are falling. This rapid rise in cases is likely attributable to the various Omicron subvariants that recently have established predominance worldwide. Australia and New Zealand had strong initial public health responses that helped prevent COVID-19 from gaining a foothold in their populations and have since made great strides to vaccinate their populations. In Australia, around 86% of the eligible population has received at least one dose of vaccine. In New Zealand, that figure is around 84%. However, as has been seen in other countries, high vaccination rates and natural infection-acquired immunity do not appear to be as protective against the BA.5 subvariant, currently the main driver of cases in the Western Pacific region. According to serology samples, Australia predicts that around 47% of its population has been infected with SARS-CoV-2 between January and June of this year, compared to only 17% of the population at the beginning of 2022.
In addition to Australia and New Zealand, other island nations have been going through some of their first experiences with COVID-19 outbreaks. Micronesia is likely the last nation in the world with a population over 100,000 to experience COVID-19, with its number of cases rising to more than 1,000 in one week. In response, the Micronesian government has mandated masks in all public places, even outdoors, or risk a fine of up to US$1,000. Additionally, the government had previously instituted a broad vaccine mandate for all eligible citizens. At last count, around 75% of the island-nation’s eligible population had been vaccinated, with more coming forward to get their shots in light of this most recent outbreak.
Japan also is struggling with its largest surge to date, far eclipsing any previous waves. The nation reported 233,100 new cases today, hitting a new record for the second day in a row. Osaka and Tokyo prefectures are reporting their highest numbers of cases and hospitalizations and have raised COVID-19 alert levels to discourage non-essential travel. However, the Japanese government has not been keen to renew stricter COVID-19 measures, such as lockdowns and travel restrictions, amid high compliance with mask wearing. On the other hand, the government is looking to shorten the isolation period from 5 days to 3 days for those who have tested positive. Officials say the decision is based on data that would indicate it is safe for people who are feeling well to leave isolation earlier, but it is perhaps ill-timed with the current exponential rise in cases. Still, the government also is preparing to distribute rapid antigen tests and possibly to expand eligibility for a fourth booster shot.
FUTURE VACCINE & BOOSTERS At a July 26 White House vaccine summit, US government officials, scientists, and pharmaceutical industry representatives discussed their ideals for future COVID-19 vaccines, including wishes for vaccines that could prevent infection, not only prevent hospitalizations and deaths; be administered easily, possibly through nasal sprays or skin patches; or provide broader and more durable protection against a range of coronaviruses, including potential future variants of SARS-CoV-2. Officials and scientists also discussed ways to speed research and streamline regulatory hurdles. Notably, officials from the US FDA and US CDC did not appear on panels during the summit, and no US lawmakers attended the meeting. Many attendees stressed the need for government support to develop next-generation vaccines, although funding was not a broad topic of discussion. The US Congress has not yet agreed to new emergency funds for COVID-19 after a deal crumbled in March. US Senate Democrats are expected to propose US$21 billion in new emergency funds for the COVID-19 response and other pandemic preparedness.
Additionally, top White House officials this week laid out an ambitious timeline for updating current vaccines to be more protective against the Omicron variant of concern and its sublineages. The FDA is hoping vaccine makers Moderna and Pfizer-BioNTech can ready "bivalent" boosters that target both the original virus strain and Omicron subvariants by September, earlier than the previously discussed October or November timeline. Pfizer-BioNTech announced this week they have begun a phase 2 randomized clinical trial testing their bivalent vaccine candidate, while Moderna last month announced preliminary data from an ongoing phase 2/3 study of its bivalent candidate. A new analysis from the Commonwealth Fund estimates that an aggressive fall COVID-19 booster vaccination campaign could save up to 160,000 lives and avert US$109 billion in medical costs, noting that policymakers must take quick action to implement such a nationwide campaign.
RACIAL/ETHNIC DISPARITIES Across the US, racial/ethnic gaps in COVID-19 mortality rates decreased between the first and second year of the pandemic. These inequities decreased due to several factors, including narrowing gaps in vaccination rates among Black and Hispanic residents and reductions in mortality for these populations alongside increases in non-Hispanic white mortality. However, substantial racial/ethnic inequities in COVID-19 mortality persist, particularly in rural areas. A preprint study posted to medRxiv showed that during the second year of the pandemic, through February 2022, Black and Hispanic people died at higher rates than their non-Hispanic white counterparts in non-urban areas, and those rates increased for some racial/ethnic groups. The researchers highlighted the need for improved access to healthcare, especially to COVID-19 therapeutics and vaccination, and increased public health messaging surrounding vaccination, mitigation strategies, and how to access care. The study underscores that residency in urban or rural areas has as much to do with individuals’ COVID-19 experiences as their region of residence and highlights the need to refocus efforts to prioritize health equity—among racial and ethnic groups but also between rural and urban areas—and address systemic racism that continues to contribute to racial/ethnic health inequities.
ANTIVIRALS Researchers from McMaster University in Canada recently conducted a systematic review and frequentist network meta-analysis, finding that use of molnupiravir (made by Merck and marketed as Lagevrio) and nirmatrelvir-ritonavir (made by Pfizer and marketed as Paxlovid) reduced the risk of hospitalization and death among COVID-19 patients with mild or moderate disease when compared to placebo or standard of care. The findings also indicated that Paxlovid may be superior to molnupiravir for treatment of mild and moderate COVID-19. For example, across 32 trials, 10,837 patients, and 291 deaths, researchers found that molnupiravir and Paxlovid each reduced the risk of death with moderate certainty although Paxlovid more so (10.9 fewer deaths per 1,000; 95% CI 12.6 to 4.5 fewer for molnupiravir; and 11.7 fewer deaths per 1,000; 95% CI 13.1 fewer to 2.6 more for Paxlovid) when compared to standard of care or placebo. Across 10 trials with 5,575 patients and 252 events, Paxlovid further reduced the risk of hospital admission (46.2 fewer admissions per 1,000; 95% CI 50.1 to 38.9 fewer; high certainty) while molnupiravir probably reduced risk of admission but less so (16.3 fewer admissions per 1,000; 95% CI 27.2 to 0 fewer; moderate certainty) compared to standard of care or placebo. The researchers also included trials related to 38 other antivirals, notably finding that remdesivir likely had no effect on risk of death but may have lowered hospitalizations, albeit with low certainty (39.1 fewer admissions per 1,000; 95% CI 48.7 to 13.7 fewer).
Findings from this study hopefully will help increase uptake of the high performing antivirals, particularly Paxlovid, as both drugs have suffered from high supply and lower-than-expected demand due to low testing and need for a physician’s prescription in some settings outside the US. While Paxlovid has been seen as a game changer by many, uptake has further suffered from concerns regarding COVID-19 symptoms rebounding post-treatment, which occurs in an estimated 5% of patients.
LONG COVID Long COVID continues to pose a threat to a portion of patients who have recovered from SARS-CoV-2 infection. Diagnosis proves difficult due to lack of quality research on the subject, and treatment options are limited, with a focus on symptom management. Symptoms of the disease range widely and are still being discovered, such as new research indicating that some people may experience lower sex drive or hair loss. Prevalence, mechanism of disease, and risk factors are still under investigation, although some studies suggest that up to one-fifth of COVID-19 patients may experience lasting symptoms. Additionally, individuals with severe COVID-19 symptoms and those with comorbidities are most likely to experience long COVID. One recent BMJ study found that 5% of COVID-19 patients could experience permanent dysfunction in taste or smell. Another recent study published in Nature Medicine noted that sneezing and ejaculation difficulty were significantly associated with long COVID, with ethnic minority, socioeconomic deprivation, smoking, and female sex also being risk factors of note. It is now more imperative than ever that the evidence base for the condition expands, as increasingly desperate patients turn to unproven or dangerous treatments such as ivermectin or “blood washing.”
ISOLATION PERIOD An article in Nature has renewed the debate among some experts over how long individuals should isolate after testing positive for SARS-CoV-2. The US CDC currently recommends that people with COVID-19 isolate for 5 full days after testing positive and can end isolation if they are fever-free for 24 hours (without the use of fever-reducing medication) and their symptoms are improving. The agency recommends all people with COVID-19 take precautions, such as wearing a mask, for 10 full days after a positive test. However, some experts say there is not sufficient evidence to support a 5-day isolation period and maintain that many people remain infectious beyond that timeframe. One preprint study, posted to medRxiv, suggests 25% of people with COVID-19 could be infectious after 8 days. Another preprint study, also posted on medRxiv, suggests that a significant number of vaccinated adults who had mild COVID-19 symptoms may have ongoing transmission risk of Omicron subvariants beyond current isolation periods, specifically days 7-10. Additionally, a small number of people could remain infectious beyond 10 days, experts warn. Notably, a small proportion of people who take the antiviral Paxlovid experience a rebound of symptoms or test positive again after completing the treatment and could be infectious. Most experts agree that individuals should continue to isolate and take precautions until they test negative on a rapid antigen test.
US SCHOOLS As many US students prepare to return to classrooms this fall amid a surge in COVID-19 cases, school districts nationwide are making decisions about whether to require masks. Jefferson County Public Schools, Kentucky’s largest school district, will require masks for everyone, regardless of vaccination status in buildings and on buses, and Gwinnett County Public Schools outside Atlanta, Georgia, recently reinstated a mask mandate for all employees and could extend the requirement when the school year begins on August 3. But while some districts are reinstating mask mandates, others are dropping them. Prince George's County in Maryland, which had the longest-running school mask mandate in the state, recently announced optional masking for the upcoming school year. Notably, a recent ruling from the 5th US Circuit Court of Appeals upheld Texas Governor Greg Abbott’s executive order forbidding the state's school districts from imposing mask mandates to help curb COVID-19. Experts agree that schools should fluctuate their masking policies based on COVID-19 data within their communities.
Millions of school-age children remain unvaccinated as they prepare to return to classrooms. Everyone older than 6 months is eligible for vaccination, and those ages 5 and older are eligible for a booster. About 23.9 million children aged 5-17 years in the US are fully vaccinated against COVID-19, about 45% of that age group, according to US CDC data. A recent study published in Science Translational Medicine found that mRNA vaccination among children aged 6-11 years can elicit strong immune system responses against SARS-CoV-2, often stronger than those observed in children diagnosed with COVID-19. The study highlights the importance of vaccination in this age group. However, vaccine uptake among children ages 5-17 appears to have slowed, according to a recent poll from KFF, which also found that 43% of parents of the youngest children aged 6 months to 4 years say they will “definitely not” get their child vaccinated against COVID-19 and 13% said they will do so “only if required.”
SARS-COV-2 ORIGIN In June, a WHO-backed team working to better understand the origins of SARS-CoV-2, the virus behind the COVID-19 pandemic, issued a report calling for additional investigations into all possible origins, including that the virus could have escaped from a laboratory. But 2 studies published this week in Science both support the theory that the Huanan Seafood Market in Wuhan, China, likely was the epicenter for the COVID-19 pandemic. Both studies were posted online as preprints in February but now have been peer-reviewed. One study examined what evidence there was for the virus in the market and found there appeared to be a correlation between where the virus was first detected and the area where wildlife was being sold. The other study analyzed the genomes of viruses isolated from early cases and concluded there were at least 2 different spillover events from an unknown animal host to people, likely around mid-November 2019. The virus began spreading from human to human more frequently in December 2019.
Many scientists agree that the preponderance of evidence, included in these studies and others, supports a zoonotic origin story of SARS-CoV-2 instead of an accidental laboratory leak. None of the studies provide definitive evidence disproving the lab leak theory, but many experts feel these studies help make that scenario less plausible. The WHO-supported group, known as the Scientific Advisory Group for the Origins of Novel Pathogens, continues its work to collect information about viral outbreaks in Wuhan in late 2019, although its work is progressing slowly. In related news, officials in Wuhan shut down the city’s Jiangxia district this week, saying it would enforce “temporary control measures” for the area’s more than 970,000 residents after detecting 4 asymptomatic COVID-19 cases.
CORRECTION In a story on US hospitals in our July 26 issue, we incorrectly stated the results of a forecast as predicting "1,800-5,600 new deaths per day by August 13." The metric should be "1,800-5,600 new deaths per week by August 13." We apologize for any confusion.
by ti-amie Ebony Jade Hilton, MD
@EbonyJHilton_MD
·Jul 31
It shouldn’t take the @POTUS to repeatedly test COVID positive for the @CDCgov & @CDCDirector to admit their suggestion of 5 day return without testing is not only flawed but completely anti-science…but here we are.
by dryrunguy Here is the latest Situation Report released much earlier today. (Today was my brother's funeral.) I haven't read it yet.
::
COVID-19 REBOUND US President Joe Biden once again tested positive for SARS-CoV-2 infection this week, following several days of negative tests last week. His symptoms are reportedly mild, and he returned to isolation after the positive tests. The phenomenon is commonly referred to as “Paxlovid rebound” or “COVID-19 rebound,” and it occurs in COVID-19 patients who take the drug, test negative for SARS-CoV-2 infection, and then test positive again. The phenomenon was not seen as an issue during clinical trials of the drug but appears to be more frequently reported since Paxlovid became widely available, although it remains unclear what proportion of people experience rebound. Typically, the recurrence of COVID-19 symptoms tends to be relatively mild.
President Biden’s rebound case has called attention to the US CDC’s guidance regarding isolation after COVID-19 diagnosis or a positive SARS-CoV-2 test. The CDC currently recommends isolation for a minimum of 5 days after the onset of symptoms or positive test. To end isolation, those who were symptomatic should wait until their fever has subsided for at least 24 hours and other symptoms are improving—and those leaving isolation should wear a mask in public through Day 10. Notably, the CDC indicates that individuals can test before they end their isolation, but the guidance emphasizes that testing is optional (ie, as opposed to recommended) for anyone who “wants to.” Those who elect to test and obtain a positive result should remain in isolation. The isolation and testing protocol implemented for President Biden went “above and beyond” the CDC recommendations, and CDC Director Dr. Rochelle Walensky indicated that the CDC must issue guidance that is feasible for most people to follow. Recent studies have demonstrated that many individuals continue to test positive for 6 days or longer, and most can shed the virus for 8 days or longer, which could enable them to infect others if they end isolation after 5 days. In light of this evidence, some experts have called on the CDC to revisit its guidance to slow transmission, particularly in light of the current Omicron surge.
PUBLIC HEALTH OFFICIAL HARASSMENT Over the course of the COVID-19 pandemic, an increasing number of public health officials in the US have received personal threats and harassment. A study, published July 29 in JAMA Network Open and led by researchers from the Johns Hopkins Bloomberg School of Public Health, set out to examine the share of US adults who thought it was acceptable to threaten or harass public health officials because of business closures and the basis for those beliefs. Overall, the study suggests that 1 in 5 survey respondents feel that threatening or harassing public health authorities is acceptable. From November 2020 to July and August 2021, the share of surveyed US adults who believed that harassing or threatening public health officials over pandemic-related closures rose from 20% to 25% and 15% to 21%, respectively, according to the study. The most significant increases were among respondents who identified as male, Hispanic, and Republican. Increases also were observed among those with higher incomes. The study identified a concerning uptick in support of these attacks among economically advantaged groups, as well as individuals who are historically more trusting of science. Researchers emphasized that restoring trust in public health officials and the entire public health workforce will require tailored approaches to reach diverse groups.
Such harassment and threats can have devastating consequences. In Austria this week, national leaders appealed for solidarity and medical representatives urged greater protections for healthcare providers after a physician who received death threats and harassment from people opposed to COVID-19 vaccination committed suicide.
IMPACTS ON US HEALTH Beyond the immediate health risks of SARS-CoV-2 infection, we are beginning to gain more clarity about the long-term impacts of COVID-19 on US residents’ health. Notably, more than 1 million people in the country have died of COVID-19, and an additional 350 people are dying of the disease each day. But other health indicators have worsened during the pandemic, as people missed routine appointments, changed their habits, felt isolated or stressed, or experienced loss. Overall, deaths and death rates from heart disease and stroke increased in the US over the past 2 years, with some studies suggesting COVID-19 can increase the risk for both, even after recovery. Drug overdose deaths, excessive alcohol consumption, serious mental illness, gun-homicide rates, and hospital-associated antimicrobial resistant infections all increased in 2020.
Additionally, millions of people in the US have post-COVID-19 conditions, also known as long COVID. The US CDC estimates that nearly 1 in 5 individuals who have had COVID-19 continue to report long-term symptoms lasting 3 months or longer. Many of them have left their jobs because they have symptoms, such as fatigue or brain fog, that hinder their ability to perform daily or work tasks. Under federal guidance, people with long COVID can qualify for disability, meaning employers must offer accommodations to their workers. But many people with long COVID say negotiating accommodations or finding support from social assistance programs remains difficult. Some experts advocate for a better definition of the condition to facilitate diagnosis, more robust educational campaigns to warn people of the risk for long COVID, and more support for people with the condition. More than 100,000 US residents are diagnosed with COVID-19 everyday, some for a second or third time, and evidence suggests people who are infected more than once are at greater risk of long-term health consequences. It will be years before we fully understand the disease’s impacts on the public health, employment, and health coverage landscapes.
RACIAL/ETHNIC DISPARITIES IN VACCINATIONS The COVID-19 pandemic has disproportionately affected racial and ethnic populations in the US, with substantial racial and ethnic inequities in COVID-19 mortality persisting, particularly in rural areas. Several recent studies examine racial and ethnic disparities in US COVID-19 vaccine distribution and uptake. According to a study published in the August issue of Health Affairs, researchers used CDC data to illustrate that uptake rates for the first COVID-19 vaccine dose were higher among Hispanic and Asian populations than among White and Black populations, while booster uptake was higher among Asian and White populations than among Black and Hispanic populations.
Many factors could influence this disparate uptake of COVID-19 vaccines and boosters, including systemic and structural inequalities in vaccine rollout and distribution. A study published July 28 in PLOS Medicine found that healthcare facilities were less likely to serve as vaccine administration locations if they were in urban counties with large populations of Black residents or rural counties with large populations of Hispanic residents. Additionally, racial and ethnic populations may be skeptical about getting vaccinated due to a long history of discriminatory and predatory medical research and practices in the US. According to another recent study published in Social Science & Medicine, vaccine hesitancy was higher among Black adults than among White adults and US-born Hispanic adults, largely due to lack of trust in the government’s communication about risk, concerns that vaccines were developed too quickly, beliefs that vaccines would give people COVID-19, and fears that vaccines may cause infertility. The study also suggests that foreign-born Hispanic adults were not more hesitant to get vaccinated than US-born White and Hispanic adults, which counters perceptions that immigrants may be less likely to opt for vaccination out of fear of being deported. These recent findings suggest that a concerted effort is needed to combat structural inequities in vaccine rollouts, for COVID-19 and other diseases, as well as to address the misinformation and mistrust that underlines vaccine hesitancy among racially and ethnically diverse communities in the US.
AFFORDABLE HOUSING In order to help prevent the further spread of SARS-CoV-2 in overcrowded housing conditions caused by evictions, the US CDC imposed a nationwide temporary federal moratorium on residential evictions for nonpayment of rent in September 2020. The moratorium ended in August 2021 after the US Supreme Court ruled to end a temporary stay on a lower court ruling seeking to overturn the rule, ending protections that had kept millions of people in their homes during the pandemic. Despite the moratorium, at least 4 corporate landlords attempted to aggressively push nearly 15,000 renters out of their homes between March 2020 and July 2021, according to a US House subcommittee investigation report. During the period covered by the report, the Eviction Lab at Princeton University documented 495,216 eviction actions.
As the pandemic progressed, many renters left urban areas to move to midsize cities—what became known as “Zoom towns”—leaving landlords with no choice but to slash rents to attract tenants. Some renters moved into those lower-priced, but often not rent-controlled, homes, only to have their rents increase immensely over the past year, often by 30-65%. Now, with a shortfall of 1.5 million homes and skyrocketing rents and home prices in communities nationwide, the US Treasury this week announced state, local, and tribal governments will have more flexibility to use COVID-19 funds from the American Rescue Plan to fill financing gaps for affordable housing projects, which could help increase the housing supply for families hit hard with high rent and inflation. The new rules allow the use of rescue funds to finance long-term affordable housing loans that extend at least 20 years and offer affordable units to households earning 65% or less of the area’s median income over the same period; to be directed to 6 additional federal housing programs; and to finance the development, repair, or operation of existing affordable rental housing units.
JAPAN Japan’s current COVID-19 surge, and largest to date, surpassed 200,000 new cases per day, ranking #1 globally in terms of total daily incidence and #6 on a per capita basis. The surge is driven largely by the BA.5 sublineage of the Omicron variant of concern (VOC), and reportedly, individuals younger than 20 years old represent approximately 30% of new cases in July, and those less than 30 years old accounted for approximately half. For comparison, these 2 age ranges comprise approximately 16% and 26% of Japan’s total population, respectively. While Japan reports relatively high vaccination coverage (including boosters) in older adults, it is much lower among younger adults and children. Only one-third of those aged 12-19 years have received their first booster, and only 17% of children aged 5-11 years have received the original 2-dose course of the vaccine. Despite facing the country’s largest surge, Japanese Prime Minister Fumio Kishida indicated that there are no plans to implement national restrictions, and Daishiro Yamagiwa, the government’s COVID-19 response lead, emphasized the importance of balancing COVID-19 protections against economic and social activity. Rather, prefecture governments can issue requests for local populations and businesses to take recommended protective measures, such as voluntary movement restrictions or increased remote work.
Reportedly, the Japanese government is considering changes to its COVID-19 reporting requirements, in an effort to reduce the burden on hospitals and laboratories. Currently, Japan requires all COVID-19 cases to be reported, but potential changes could reclassify COVID-19 under the same category as seasonal influenza. While this shift could ease reporting requirements, it would also limit the ability to identify and quarantine close contacts, which could facilitate further transmission. Additionally, it could eliminate measures for the national government to cover the costs of testing.
Since the onset of the pandemic, Japan’s travel and tourism sector has faced severe impacts. Amid reports of a travel resurgence in many regions, particularly in Europe, Japan has not benefited from a similar windfall. In June, Japan announced decisions to resume international travel, albeit with specific COVID-19 restrictions in place, just in time for the summer travel season. While international travelers would once again be able to enter Japan, restrictions mandate that their activities be part of organized group itineraries, and visitors must remain with designated chaperones throughout their trip. Additionally, travelers also face quarantine measures upon arrival. These measures have reportedly factored into travelers’ decisions, and many have opted for other destinations, including South Korea. Both global and regional travel have been impacted in Japan, and one report indicates that approximately 10% of hotels and travel agencies have shut down over the course of the pandemic. Historically, Japan’s largest tourism market is China, but prolonged national-level quarantine and travel restrictions have resulted in substantial decreases in Chinese tourists.
NEW ZEALAND New Zealand fully reopened its borders on July 31 after more than 2 years of strict pandemic restrictions. The final stage of the country’s phased reopening began in April, when tourists from countries on a visa-waiver list could enter. Now, visitors from all over the world are allowed into New Zealand, including those on student visas and from non-visa waiver countries. Per New Zealand’s Ministry of Health, electronic or paper proof of vaccination is required to enter, as well as a rapid antigen test conducted upon arrival and on the fifth or sixth day post-arrival. Masks are required indoors, including museums, grocery stores, and pharmacies. In a speech on August 1, Prime Minister Jacinda Ardern emphasized the reopening was part of a carefully staged plan to keep people safe. As the nation reopened, the Ministry of Health reported 5,312 new COVID-19 cases. Daily new COVID-19 deaths began to increase in February 2022 and remain elevated at an average of 3 deaths per day.
by ponchi101
dryrunguy wrote: ↑Wed Aug 03, 2022 3:33 am
PUBLIC HEALTH OFFICIAL HARASSMENT Over the course of the COVID-19 pandemic, an increasing number of public health officials in the US have received personal threats and harassment. A study, published July 29 in JAMA Network Open and led by researchers from the Johns Hopkins Bloomberg School of Public Health, set out to examine the share of US adults who thought it was acceptable to threaten or harass public health officials because of business closures and the basis for those beliefs. Overall, the study suggests that 1 in 5 survey respondents feel that threatening or harassing public health authorities is acceptable. From November 2020 to July and August 2021, the share of surveyed US adults who believed that harassing or threatening public health officials over pandemic-related closures rose from 20% to 25% and 15% to 21%, respectively, according to the study. The most significant increases were among respondents who identified as male, Hispanic, and Republican. Increases also were observed among those with higher incomes. The study identified a concerning uptick in support of these attacks among economically advantaged groups, as well as individuals who are historically more trusting of science. Researchers emphasized that restoring trust in public health officials and the entire public health workforce will require tailored approaches to reach diverse groups.
Such harassment and threats can have devastating consequences. In Austria this week, national leaders appealed for solidarity and medical representatives urged greater protections for healthcare providers after a physician who received death threats and harassment from people opposed to COVID-19 vaccination committed suicide.
That is horrifying.
I know, I know, I know. I side with Pinker in that we live in the best of possible times. BUT: we might be hitting some sort of flipping point, and it has nothing to do with governments. CIVIC attitudes are disappearing. it sounds simple to say "1 in 5", but that is 20%. If that large number of people are Ok with harassing medical personnel simply for dealing with a pandemic, we are in a situation of flipping morality.
And in a country with all the lunatics carrying guns like the USA, this is a recipe for some terrible tragedy eventually happening.
by Owendonovan These people don't seem to understand that if you blow it all up, there's nothing left.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 577 million cumulative cases and 6.4 million deaths worldwide as of August 3.* The global weekly incidence dropped 7.14% from the previous week, falling for the first time since the end of May. Global weekly mortality remained stable, rising only 0.34% over the previous week. However, global weekly mortality has continued to increase since mid-June.
At the regional level, the Western Pacific (+20%) and Africa (+5%) regions experienced increases in new weekly cases, while the number of new cases increased or remained stable in Europe (-35%), Eastern Mediterranean (-12%), South-East Asia (-2%), and the Americas (-2%). In the Western Pacific region, the highest increases were in Japan (+42%) and South Korea (+25%). The number of new weekly deaths increased in the Western Pacific (+44%), Eastern Mediterranean (+26%), South-East Asia (+20%), and Africa (+12%) regions; decreased in Europe (-26%); and remained stable in the Americas region.
*The WHO notes the case and death data for the Africa region are incomplete and will be updated as soon as more information becomes available.
UNITED STATES
The US CDC is reporting 91.5 million cumulative cases of COVID-19 and 1,026,723 deaths. The current 7-day moving average of new daily cases is down slightly over last week, dropping to 119,034 on August 2. The average daily mortality remains relatively stable, at 387 on August 2. Daily mortality has risen since the beginning of June, when it was around 275 deaths per day.**
Both new hospital admissions (-1.7% over the past week) and current hospitalizations (-0.4%) remained relatively stable over the previous week, possibly reflecting the slight decrease in daily incidence.
Community transmission in the US is primarily driven by the Omicron BA.5 sublineage. BA.5 is now projected to account for 85.5% of sequenced specimens. The BA.4 sublineage accounts for about 7.7% of cases, while the newly delineated BA.4.6 accounts for 4.1% of cases and appears to represent a growing proportion of BA.4 sublineages. Together, BA.2.12.1 and BA.2 now account for only about 2.7% of cases. According to the data, Omicron variants represent all new cases in the US.
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US COVID PLATEAU The US appears to have settled into a persistent pattern of high levels of SARS-CoV-2 transmission—around 120,000 new infections per day, which is likely a massive undercount due to a lack of surveillance—and a relatively steady number of daily deaths—averaging between 350-400 per day. The currently high number of infections disrupt society and the economy and could result in millions more people experiencing long COVID. Although the COVID-19 death rate has dropped due to widespread immunity from vaccination or natural infection or both, as well as improved treatments, the virus is still killing hundreds of people each day, rarely dropping below 300 daily deaths. Some estimates predict 100,000, or more, annual COVID-19 deaths, far higher than the number associated with other respiratory diseases. Most individuals dying from COVID-19 now are those who are elderly, immunocompromised, unvaccinated, have lung or heart conditions, or have a combination of factors. Early treatment, in addition to vaccination, appears to provide good protection from death, even among people at higher risk.
Retooled booster vaccines, tailored to the Omicron subvariants BA.4 and BA.5, might provide additional protection when they become available in late summer or early fall, and the Biden administration is urging US residents who are not up to date on their vaccinations and booster doses—around 70% of the population as of July 21—to get those shots now. Several new studies suggest that people who received 3 or 4 vaccine doses are better protected against infection with Omicron than those who received 2 doses. But at the same time, the US CDC is expected to release updated guidance for COVID-19 community control, including easing quarantine recommendations for people who are exposed to the virus, such as those who are unvaccinated or not up to date on their vaccines; de-emphasizing 6 feet of social distancing; and downplaying the use of regular screening tests in schools. Some wonder how the new guidance—which remains under review but could be released this week—meshes with stubbornly high new infections and deaths. Additionally, no one knows what variant might emerge in the future, or how much existing levels of immunity might wane over time.
LONG COVID RESEARCH & SERVICES On August 3, the Biden administration announced new government initiatives to address the long-term health impacts of COVID-19, often referred to as long COVID, in 2 reports: the National Research Action Plan on Long COVID and Services and Supports for Longer-Term Impacts of COVID-19. The National Research Action Plan outlines what is currently known about long COVID—including defining 2 technical terms, post-COVID-19 conditions (PCC), broadly equivalent to long COVID, and post-acute sequelae of SARS-CoV-2 infection (PASC), focused on the direct effects of the virus—and directs future research toward certain vital areas. The Services and Supports report acts as a guide for those with long COVID to access services and care; additionally, it acts as a guide for healthcare providers seeking more information about how to care for their patients. These reports have been anticipated by the millions of US residents diagnosed with long COVID and their healthcare providers who are searching for answers. An estimated 7 to 23 million US residents have experienced long COVID, often with debilitating and life-interrupting symptoms.
While advocates say these actions are a good step forward, many raise concerns that they are inadequate to address the real-time needs of those with long-term symptoms. In a memorandum posted in April, US President Joe Biden emphasized the need for a whole-of-government approach to addressing the research gaps and assistance needs for individuals with long COVID. The memorandum also recommended the US HHS set up an Office of Long COVID Research and Practice but did not provide specifics on how to do so or how such an office would be funded. Relatively little is still known about the incidence of long COVID and any underlying factors that might predispose someone to experience long-term conditions. The US CDC estimated in May that 1 in 5 adults had a health problem that may be attributable to a prior SARS-CoV-2 infection. Aside from incidence, new research suggests long COVID appears to manifest in 3 different forms: nervous system problems (brain fog, fatigue, headaches), respiratory problems (chest pain, shortness of breath), and other myriad symptoms (heart palpitations, muscle aches, changes to skin and hair, etc.). Individuals with long COVID and their advocates hope the new action plans will help improve our understanding of long COVID and effective treatments or cures.
CARDIAC COMPLICATIONS As the COVID-19 pandemic continues, more people around the world are experiencing SARS-CoV-2 infections, some multiple times. Many individuals are able to recover from the disease, due in part to widespread implementation of vaccines and therapeutics. However, research evidence and clinical experience suggest that COVID-19 can drastically alter health after infection. Post-COVID conditions, sometimes called long COVID, can include a wide variety of symptoms and complications, but many experts are showing concern over research suggesting SARS-CoV-2 infection is associated with a higher risk of post-infection cardiovascular problems. In one study published earlier this year using records from the US Department of Veterans Affairs (VA), researchers found individuals with COVID-19 have an increased risk of incident cardiovascular issues, ranging from heart attack, heart inflammation, blood clots, and stroke, within the first year following infection. Unpublished analysis of the VA data from the University of Washington’s Institute for Health Metrics and Evaluation (IHME) predicts that COVID-19 may have led to 12,000 extra strokes and 44,000 extra heart attacks in 2020 and 18,000 extra strokes and 66,000 extra heart attacks in 2021. A preprint study posted to medRxiv on July 7 indicates that risk factors for cardiovascular complications may include prior cardiovascular disease, pre-existing conditions, older age, and hospitalization for COVID-19. Therefore, COVID-19 may be capable of worsening the cardiovascular prognosis of individuals already experiencing poor health.
The mechanism for cardiovascular damage may be related to the virus spike protein binding with human ACE2 to enter cells. ACE2 is a cellular protein that is found on many cell types throughout the human body. This means that the virus can thrive in a wide variety of human tissues. In the cardiovascular system, blot clots that form to heal damage done by the virus may also be responsible for much of the observed complications. Plaques can also accumulate after infection, leading to a higher risk of stroke and heart attack. Additional ongoing research hints that SARS-CoV-2 may also damage the heart by activating the TLR4 immune system signaling pathway. More research is needed, but understanding the mechanisms of injury can help scientists develop preventive and therapeutic strategies. The growing body of evidence suggesting that COVID-19 can have long-term impacts on human health highlights the need for continued measures to prevent infection and heightened awareness of and resources for the management of complications.
NASAL VACCINES Scientists worldwide are hard at work designing the next generation of SARS-CoV-2 vaccines and boosters. When they were first authorized, mRNA vaccines were approximately 95% effective at preventing symptomatic infection, but that efficacy has waned as new viral variants emerge and spread. The currently approved and authorized vaccines continue to remain effective at reducing rates of hospitalization and death, but each novel emerging variant brings fears that it could better escape immunity from vaccination or natural infection. US health officials stated during a recent summit at the White House that the next generation of vaccines should focus on the development of a pancoronavirus vaccine and various delivery mechanisms, including nasal delivery.
A report published July 19 in Science Immunology shows that currently available mRNA vaccines are not very good at eliciting immune responses in the respiratory tract of vaccinated individuals compared to people with previous SARS-CoV-2 infection. However, using an animal model, the study suggests that coupling mRNA shots with an adenovirus vector booster administered intranasally could provide a much higher level of protection against the virus entering the body through mucosal tissue and establishing infection. The Indian biotechnology company Bharat Biotech recently reported the completion of clinical trials using an adenovirus vector intranasal vaccine (BBV154) as a booster dose. The trial included 4,000 participants, and no adverse events were reported. Bharat Biotech is hopeful the Drug Controller General of India will authorize the vaccine this month.
VACCINE EFFECTIVENESS AMONG CHILDREN Since many countries authorized Pfizer-BioNTech’s mRNA SARS-CoV-2 vaccine, marketed as Comirnaty, for the 5- to 11-year-old age group, researchers continue to study the vaccine’s efficacy in that age group, particularly in the wake of the rise of Omicron variant predominance. Recently published studies appear to reinforce evidence that Comirnaty remains highly effective at preventing hospitalizations and severe outcomes from COVID-19, but its effectiveness against symptomatic infection wanes over time and against Omicron subvariant infections. A study in Singapore estimated vaccine effectiveness in 5- to 11-year-old children to be 82.7% against hospitalizations but 65.3% against PCR-confirmed infections during the initial Omicron wave. These approximations are echoed in a preprint out of Canada in which researchers estimated a range of 29-65% effectiveness against Omicron infections but 68-100% effectiveness against hospitalization due to Omicron. Interestingly, another study in the European Union found that vaccine effectiveness was higher among the youngest in this age cohort compared to the oldest. Children aged 5-6 years appeared to be more protected against symptomatic infection compared to those aged 10-11 years, with children aged 7-8 years falling between the 2 groups. Depending on the starkness of this difference moving forward, it could be valuable to investigate the tolerance and protectiveness of higher dosages in older children. Still, these studies taken together demonstrate the continued importance of vaccinating children to protect them against severe disease as we wait for Omicron-specific vaccines to become available.
MONOCLONAL ANTIBODIES Eli Lilly & Co plans to begin commercial sales of its COVID-19 monoclonal antibody treatment, bebtelovimab, to states, hospitals, and other healthcare providers this month. Most COVID-19 therapeutics and vaccines have been distributed at no cost through the US government, but the federal supply of bebtelovimab is running out and the government has no funds to purchase more, unless the US Congress moves to appropriate additional money. The move likely is the first test of how accessible COVID-19 treatments and vaccines will be once they are shifted to a commercial market. Bebtelovimab is available for use under US FDA emergency use authorization (EUA) for the treatment of mild-to-moderate COVID-19 among certain children and adults.
In a research letter published in JAMA, researchers from the Netherlands report that a large proportion of high-risk COVID-19 patients treated with the monoclonal antibody sotrovimab—one of a few such treatments to maintain neutralizing activity against Omicron BA.1—developed spike protein mutations associated with resistance to the treatment. The study included a small sample size and lacked a control group but provides additional evidence that treatment of high-risk patients with a single monoclonal antibody is associated with mutation development. The researchers called for further investigations into combination therapies and continuous genomic surveillance of immunocompromised patients during treatment. As of April 5, sotrovimab was no longer authorized by the FDA to treat patients in the US due to inactivity against Omicron BA.2, which was predominant at the time.
by ponchi101 At 400 deaths/ day (rounding up) and 300 days/year, that means the USA can expect a 12,000 death toll yearly, if no more changes take place.
That is about twice the yearly influenza death toll (around 6,000).
Of course, that is if the death toll is accurately counted.
by dryrunguy My former boss (the anti-vaxxer who thinks ivermectin is an antiviral) will miss at least a few days of work this week because she has COVID. She was on vacation last week.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
OMICRON-ADAPTED VACCINES The European Medicines Agency (EMA) announced today that it has started a rolling review of an Omicron-adapted vaccine developed by Pfizer and BioNTech. This update follows a large push from national governments for vaccine companies to develop a variant-adapted version of SARS-CoV-2 vaccines to protect individuals against more transmissible variants, including the Omicron subvariants BA.4 and BA.5. Pfizer and BioNTech expect to begin clinical trials later this month using an enhanced vaccine candidate targeting the original strain identified in Wuhan, China, in late 2019 and the Omicron BA.4 and BA.5 subvariants, which are the dominant drivers of outbreaks in Europe. The companies said they would be able to begin delivering doses as early as October. The EMA’s rolling review constitutes an ongoing process in which the agency will assess data as it becomes available. Notably, US FDA officials previously said they anticipate an updated Pfizer-BioNTech vaccine to be available as early as September, and the agency has indicated that it would approve the variant-adapted vaccine while trials are ongoing. However, both the EMA and FDA will still require clinical data from this month’s trial to guide their decisions on the companies’ candidate targeting BA.4/5. Pfizer and BioNTech also are testing vaccine candidates encoding for Omicron BA.1 and BA.2. Both the US and European Union are hoping to use updated SARS-CoV-2 vaccines for fall booster campaigns.
The Biden administration on July 29 announced an agreement to purchase 66 million doses of a version of Moderna’s Omicron-adapted vaccine booster, with intentions to distribute the shots this fall and winter. In July, Moderna announced that its bivalent Omicron (BA.1) booster (mRNA-1273.214) elicited higher neutralizing antibody responses than the currently available booster and said it is simultaneously developing a booster specific to BA.4/5 (mRNA-1273.222). The US government previously purchased 105 million doses of a Pfizer-BioNTech bivalent vaccine for use later this year, although it is unclear which version of the companies’ booster candidate is covered under the agreement.
US EMERGENCY DECLARATION The Biden administration is deliberating whether to once again extend the COVID-19 public health emergency, which facilitates federal assistance for pandemic-related healthcare coverage and access to vaccines and treatments. The deadline to announce a decision is August 15, if the US Department of Health and Human Services is to give states 60 days’ notice before allowing the declaration to expire. If approved, the proposed extension could last into 2023, beyond the November elections and into the pandemic’s fourth year. Reportedly, debate surrounding the declaration has grown more contentious, with some officials pushing for the declaration to expire in October after the expected rollout of updated booster vaccines. The US government has repeatedly renewed the emergency declaration since first instituted in January 2020.
US PANDEMIC VIEWS According to a national survey conducted July 12-18 by the Annenberg Public Policy Center, the majority of Americans (54%) say they rarely or never wear a mask indoors around people outside their household to help prevent COVID-19, and 41% say they have returned to their normal, pre-pandemic lives. Among these individuals, the majority are aware of the risks of infection but say they have adjusted to the “new normal,” with a growing number having returned to pre-pandemic routines and activities. In another poll from Axios and Ipsos conducted July 15-18, 29% of respondents said they believe the pandemic is over. The results varied by political affiliation: 48% of Republicans said the pandemic is over, compared with only 9% of Democrats. Despite this, 4 of 5 respondents agreed with the statement, "We will never fully be rid of the coronavirus in my lifetime." Although the number of new COVID-19 cases has risen significantly with the emergence of the BA.5 Omicron subvariant, reported mask use continues to decline and these polls suggest growing numbers of US residents are returning to their pre-pandemic lives, with limited precautions.
POST-COVID SYMPTOMS IN CHILDREN Researchers led by the CDC COVID-19 Emergency Response Team published a report on post-COVID-19 symptoms and conditions in children in the August 5 Morbidity and Mortality Weekly Report (MMWR). The researchers compared the symptoms of 781,419 children with confirmed COVID-19 to 2,344,257 children without COVID-19 from March 1, 2020, to January 31, 2022. Children with confirmed COVID-19 were more likely than were those without COVID-19 to develop certain post-COVID conditions, including blood clots in the lung (adjusted hazard ratio [aHR]=2.01), heart muscle inflammation (1.99), venous blood clot (1.87), acute renal failure (1.32), type 1 diabetes (1.23), blood clotting or bleeding disorders (1.18), type 2 diabetes (1.17), and abnormal heart rhythms (1.16). Additional symptoms were associated with COVID-19, including smell and taste disorders and malaise or fatigue. Still, the incidence of these conditions remained uncommon in the post-COVID pediatric population. Notably, children who had COVID-19 reported lower rates of respiratory, mental health, muscle, and sleeping disorders than those without COVID-19. Reasons for the observation are thought to include the fact that the general population for this study was selected from patients with a healthcare encounter possibly related to COVID-19. As a result, the general population may have been less healthy than patients with COVID-19 at baseline.
LONG COVID DIAGNOSIS & TREATMENT Post-COVID-19 symptoms and conditions, which can linger for months or years in both children and adults, are often referred to as long COVID. However, there is no test for the condition, and there is little agreement around a standard definition for the condition, which is estimated to affect 1 in 5 to 1 in 8 COVID-19 patients. Treatments typically involve symptom management, but researchers are beginning to hone in on the condition’s pathology and begin clinical trials on medicines that target the immune system, blood clots, or lasting fragments of the virus itself. Some researchers are examining the similarities between long COVID and an older condition known as ME/CFS, or myalgic encephalomyelitis/chronic fatigue syndrome. The US government recently released a set of reports that sketch out an action plan to address long COVID, including calling for the establishment of a new office at the US HHS, new funding, and additional focus on the condition from the private sector. Though the full impact of the COVID-19 pandemic is hard to predict, it is becoming increasingly clear that individuals with long COVID may face health challenges for years to come.
DISRUPTIONS TO ROUTINE HEALTHCARE During the early stages of the COVID-19 pandemic, lockdowns prevented many US residents from accessing routine, and sometimes emergency, healthcare. Among households that had a serious illness in the past year, about 1 in 5 respondents to a new poll by NPR, the Robert Wood Johnson Foundation, and the Harvard T.H. Chan School of Public Health said they had trouble accessing care during the pandemic. Some experts are concerned these disruptions, which continue to occur, could have lasting impacts on people’s health as well as the nation’s healthcare system. The poll found the difficulties accessing healthcare hit some racial/ethnic minority populations harder. Among those households with a serious illness in the past year, 35% of Native American households, 24% of Black households, 18% of Latino households, 18% of White households, and 10% of Asian households had difficulty accessing care when they needed it. The survey, conducted from May 16 to June 13, 2022, also examined other problems facing racial/ethnic minorities, including issues concerning finances, housing, neighborhood conditions, and personal safety.
COVID-19 IN ANIMALS A recent report published July 23 in Scientific Data describes a dashboard that monitors COVID-19 cases in animal populations. The online dashboard, called SARS-ANI, is an open-access curated global dataset of SARS-CoV-2 events in animals containing a wide variety of information, including total number of infection events, number of animal species described, number of countries where animal infections have been reported, clinical signs of infection categorized by animal, a SARS-CoV-2 variant breakdown by animal, and more. The majority of animal cases have occurred in mink, with cats and dogs following closely behind. Cases of COVID-19 also have been reported in wild and captive animals, such as deer, gorillas, hippos, hyenas, and marmosets. A separate online dashboard tracking COVID-19 in animals around the world reports that cases have also occurred in certain avian populations, such as swans.
The detection of so many COVID-19 cases in animal populations raises questions about how the pandemic will look in the future. The SARS-CoV-2 virus can mutate in an animal just like it can mutate in humans, so it is entirely possible that SARS-CoV-2 could circulate widely within a population of animals before spilling back into humans to cause a completely new variant through a process known as zoonotic transmission. Additionally, an expansion of the virus into more avian populations could enhance the ability of new variants to be transported and emerge in unexpected places. One of the other concerning aspects of COVID-19 in animals is potential establishment of “viral reservoirs.” Viral reservoirs are animal populations that maintain low levels of circulating virus within their species, which could allow the virus to jump back to humans years or decades after the last human case. One of the reasons smallpox was successfully eradicated was the absence of animal or insect viral reservoirs. The presence of COVID-19 in animals means that a “One Health” approach is needed to properly address the pandemic. One Health focuses on treating the health of humans, animals, plants, insects, and the environment as a connected web.
CHINA China’s tourism-dependent island province of Hainan on August 8 expanded lockdowns amid a growing COVID-19 outbreak during the summer school holiday. The tropical resort of Sanya began an indefinite lockdown on August 6, confining about 80,000 vacationers to their hotel rooms. Tourists who test negative 5 times over 7 days can leave, but many flights to the area have been canceled. Additionally, 4 other cities and 4 counties in Hainan—a total population of about 7 million—began lockdowns of 2 or more days on August 7 and August 8. Hainan reported 471 new COVID-19 cases on August 8, out of a total of 939 new local and imported cases nationwide. It is the province’s largest outbreak since the pandemic began.
In related news, the Chinese autonomous region of Tibet has imposed various restrictions in its capital city Lhasa, as well as in its second-largest city, Shigatse. Residents in the 2 largest cities and other areas will undergo mass testing. Until now, the region had remained COVID-19-free for more than 900 days, the best record of enforcing China’s “zero COVID” policy. The region reported 22 new cases on August 8. The fresh lockdowns came as Hong Kong, a semi-autonomous Chinese city, announced it will reduce mandatory hotel quarantine for international travelers from 1 week to 3 days, followed by 4 days of at-home surveillance, beginning Friday.
NEW ZEALAND & AUSTRALIA According to analysis from the New Zealand Herald, COVID-19 became a leading cause of death in the country, tied with heart disease, in the week ending July 17. During that week, 836 people died nationwide, and nearly 15% of those deaths were attributed to COVID-19. Experts expressed concern that at the same time the nation is experiencing its highest COVID-19 mortality impact, public attention to the pandemic appears to be at its lowest levels. Overall, New Zealand’s cumulative death rate from COVID-19 remains low—at 316 per million population—compared with the US and UK, with 3,062 and 2,753 deaths per million population, respectively. Public health officials predict COVID-19 will continue to be a significant contributor to overall mortality for the foreseeable future—with annual COVID-19 deaths at about 5 times influenza deaths—and could have a significant impact on the country’s life expectancy.
In Australia, modelers with the Actuaries Institute Covid-19 Mortality Working Group estimate that COVID-19 was the primary cause of 7,100 deaths in the country from the beginning of this year through the end of July, making the virus the third most common cause of death this year so far. Only ischemic heart diseases and dementia, which caused about 10,000 deaths each, beat out COVID-19, with deaths from cardiovascular disease (primarily stroke; about 5,500 deaths) and lung cancer (5,400 deaths), following behind.
THAILAND Beginning in October, Thailand will downgrade COVID-19 from a “dangerous” communicable disease, similar to plague and smallpox, to one that “need monitoring,” a group that includes influenza and dengue. In an announcement, Thailand Health Minister Anutin Charnvirakul said the action reflects the readiness of the nation’s public health system, public acceptance of “self-protection behavior,” and the availability of treatments. Thailand’s number of newly confirmed daily COVID-19 cases has remained relatively stable since mid-July. While the number of daily deaths is elevated, officials said they expect to see a decline in both cases and deaths by mid-August.
by ti-amie Interesting about Tibet.
by dryrunguy Just read it. The section on US Pandemic Views says it all. What I saw at my brother's funeral last week demonstrated these sentiments on steroids. There were probably 50 or 60 people who attended the funeral. My middle brother, his partner, and I were the ONLY people wearing masks. I'd even venture to guess very few of those in attendance had EVER worn a mask.
by ti-amie
dryrunguy wrote: ↑Tue Aug 09, 2022 6:54 pm
Just read it. The section on US Pandemic Views says it all. What I saw at my brother's funeral last week demonstrated these sentiments on steroids. There were probably 50 or 60 people who attended the funeral. My middle brother, his partner, and I were the ONLY people wearing masks. I'd even venture to guess very few of those in attendance had EVER worn a mask.
Was there any discussion about what caused your brother's death at all?
dryrunguy wrote: ↑Tue Aug 09, 2022 6:54 pm
Just read it. The section on US Pandemic Views says it all. What I saw at my brother's funeral last week demonstrated these sentiments on steroids. There were probably 50 or 60 people who attended the funeral. My middle brother, his partner, and I were the ONLY people wearing masks. I'd even venture to guess very few of those in attendance had EVER worn a mask.
Was there any discussion about what caused your brother's death at all?
Well, everyone knew. At least everyone in the family, which was 95% of the people who attended. (My brother didn't have any friends. The people who attended were there for my mother and his two adult children.) But I didn't hear anyone talking about it.
by dryrunguy Here's the latest Situation Report. Two words of note: Florida, Korea.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 584 million cumulative cases and 6.4 million deaths worldwide as of August 10.* The global weekly incidence (August 1) increased 3.9% from the previous week. Global weekly mortality fell 7.9% over the previous week, representing the first notable decline since the end of May.
At the regional level, the number of new weekly cases rose in the Western Pacific (+29%) region and fell or remained stable in the Africa (-46%), Americas (-22%), Eastern Mediterranean (-22%), Europe (-7%), and South-East Asia (-3%) regions. The number of new weekly deaths increased in the Eastern Mediterranean (+19%) region and decreased or remained stable in the Africa (-73%), Europe (-15%), the Americas (-10%), South-East Asia (-1%), and the Western Pacific (+4%) regions.
*The WHO notes the case and death data for the Africa region are incomplete and will be updated as soon as more information becomes available.
UNITED STATES
The US CDC is reporting 92.3 million cumulative cases of COVID-19 and 1,030,010 deaths. The current 7-day moving average of new daily cases is down over last week, dropping to 107,077 on August 9 from 121,260 on August 2. The average daily mortality remains relatively stable, at 395 on August 9. Daily mortality has risen since the beginning of June, when it was around 280 deaths per day.**
Both new hospital admissions (-0.8% over the past week) and current hospitalizations (-2.6%) remained relatively stable over the previous week, possibly reflecting the slight decrease in daily incidence.
Community transmission in the US is primarily driven by the Omicron BA.5 sublineage. BA.5 is now projected to account for 87.1% of sequenced specimens. The BA.4 sublineage accounts for about 6.6% of cases, while the BA.4.6 sublineage accounts for 4.8% of cases. Together, BA.2.12.1 and BA.2 now account for only about 2.9% of cases. According to the estimate, Omicron variants represent all new cases in the US.
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
IMMUNE EVASION Immune escape, or immune evasion, is driving the COVID-19 pandemic’s extended life cycle. As the virus continues to infect humans, it will mutate and likely adapt to find its way around existing levels of vaccine-induced and natural immunity. The scientific community is not surprised that SARS-CoV-2 continues to evolve to evade our ever-changing immune systems, as many other viruses do the same. But because SARS-CoV-2 is a new virus to humans, attention is focused on emerging new variants and global anxiety is heightened, wondering what variant lies around the corner.
Currently, there are many questions about whether the Omicron subvariants BA.2.75 or BA.4.6 will cause the next wave of infections. BA.2.75, which has been circulating widely in India for more than a month and has been detected in at least 20 other countries, does not currently appear likely to outcompete BA.5, the global leader of SARS-CoV-2 variants. BA.4.6, which is growing in prevalence in the US and Europe, appears to be just as transmissible as BA.2.75, but it remains unclear whether either subvariant will become predominant. Scientists continue to worry that either one of these Omicron subvariants, or an as-yet undetected variant, could gain global, regional, or local dominance. This cycle of new variant-driven waves, each with increased immune evasion, describes the global experience with COVID-19 to date, and many assume the pattern will continue into the future. This is what allowed BA.4 and BA.5 to spread widely despite widespread recent infections with the Omicron BA.1 and BA.2 subvariants.
In addition to increased variant surveillance, more must be done to help further prepare for future increases in COVID-19 cases. The first priority is to address current infections by reducing transmission of circulating virus, limiting its chances to adapt and evade existing levels of immunity. However, limiting transmission is increasingly challenging, as many countries roll back mitigation measures and as funding for testing and vaccination programs dwindles. Many appear to be placing hope in the next generation of SARS-CoV-2 vaccines, which are expected to protect against a wider array of viral lineages. Several studies, including one conducted in non-human primates published this week in Science Translational Medicine, suggest that these vaccines may be a possibility, and they may be able to provide protection that extends to other coronaviruses, so-called pancoronavirus vaccines. While those vaccines remain a distant goal, manufacturers continue to work on current vaccine platforms that enable the fast production of variant-specific boosters. The CEO of Moderna recently compared the future of SARS-CoV-2 vaccines to the iPhone’s constant updates, with new generations developed as more data and technologies become available.
NOVAVAX VACCINE Last month, the US FDA granted emergency use authorization (EUA) for a protein-based COVID-19 vaccine made by US-based manufacturer Novavax. Many public health advocates hoped that the vaccine’s authorization would lead to an increase in vaccinations among unvaccinated populations, having faith that the more traditional protein-based vaccine technology would ease concerns surrounding vaccination with vaccines using newer mRNA platforms. However, in the month since the EUA was issued, only about 7,400 doses have been administered in the US, with only 2,300 people receiving a 2-dose primary series using Novavax. According to the US CDC, 332,000 doses of the vaccine have been distributed nationwide. Originally, the vaccine was available at only 385 locations, although that number has grown to 986 sites. Notably, more than 53,000 locations have been used to provide other vaccinations throughout the pandemic. The limited uptake of the Novavax vaccine has received criticism given the large investment the company received from Operation Warp Speed. While it is too early to decide the fate of the vaccine in the US, Novavax recently reset its sales expectations, halving its forecast to US$2 billion to US$2.3 billion from US$4 billion to US$5 billion.
PEDIATRIC VACCINATIONS Efforts to vaccinate young children against COVID-19 in the US got off to a sluggish start and continue to lag. Results of a survey published August 3 in JAMA Network Open indicate that only about half of the 2,031 parents of young children aged 6 months to 4 years surveyed intend to vaccinate their children at some point, and only about one-fifth said they intend to do so within 3 months of the child’s eligibility. The research team surveyed the parents in early February 2022, about 4 months prior to the US FDA’s decision to issue an EUA for this youngest age group. According to the survey, 45.6% of the respondents would “definitely” or “probably” vaccinate their child after eligibility, and 66% said they plan to wait 3 months or longer before deciding whether or to vaccinate their child. Just over one-third of the participants said they did not know if they would seek vaccination. Overall, only 4-5% of children in this age group have been vaccinated since the EUA, with concerns over vaccine safety driving the scarce uptake.
Looking at older pediatric age groups, a study published August 8 in The Lancet Infectious Diseases examines the effectiveness of the 2-dose primary series of the Pfizer-BioNTech vaccine in preventing symptomatic infection and severe disease among adolescents aged 12 to 17 years living in Brazil and Scotland between August 2021 and April 2022. The test-negative, case-control study found that protection against symptomatic infection from a 2-dose series administered at least 21 days apart peaked at 14-27 days after the second dose and then began to wane. However, protection against severe COVID-19 disease remained high at 98 days or more after the second dose during the Omicron-dominant period, suggesting that booster doses for this age group should be considered.
TRANSPORTATION MASK REQUIREMENTS A group of 23 state attorneys general filed a brief in a US federal appeals court this week claiming the CDC lacks the authority to impose a nationwide transportation mask mandate to address COVID-19. Led by Florida’s State Attorney General, the group called CDC’s actions an “overreach” and expressed their support of an April ruling by a Florida federal judge who blocked the transportation-related mask mandate requiring travelers to wear masks on planes, trains, buses, ride-share vehicles, and in transit stations. Additionally, 17 Republican US lawmakers filed a similar brief the same day. The US Department of Justice appealed the April ruling to the 11th U.S. Circuit Court of Appeals, filing a May 31 brief saying the mask requirement "falls easily within the CDC's statutory authority.” The Biden administration stopped enforcing the order following the April ruling.
VACCINE PRODUCTION IN AFRICA According to the Africa CDC, only 20% of adults on the continent have been fully vaccinated against COVID-19, but demand for vaccination has fallen. South Africa-based Aspen Pharmacare produces the J&J-Janssen vaccine for member states in Africa, which comprises almost 30% of vaccines acquired in the region, and in March finalized a deal to produce its own Aspenovax vaccine for African markets. However, the company has not received any orders for the Aspenovax shot, this week saying it will have to shut down or convert its production lines beyond this month if it does not receive orders. However, the Africa CDC, which does not want the continent’s vaccine manufacturing capacity shuttered, last month said it is in detailed discussions with buyers to generate demand for Aspenovax.
Vaccine hoarding by high-income nations deprioritized low- and middle-income countries’ (LMICs) access to vaccines during the early stages of the COVID-19 pandemic. Subsequently, many donors from high-income countries established COVID-19 response as a top funding priority, treating it as a once-in-a-century threat to public health. Global health experts have questioned this reprioritization of funding, arguing the money would be better spent on a holistic approach to healthcare and disease, as COVID-19 is one of many public health priorities that LMICs need donor support to address. A new study, published in The Lancet Global Health, highlights the disruptions the COVID-19 pandemic had on essential health services in Kenya, including access to cervical cancer screening, testing for HIV and malaria, tuberculosis therapies, and routine immunization. Donors’ shift in focus to COVID-19, and restrictions on how that funding can be used, illustrates a missed opportunity to more effectively address pressing public health concerns on the continent.
NORTH KOREA Since May, North Korea has reported more than 4.7 million cases of patients with “fever” and 74 related deaths, widely believed to be COVID-19. After not registering any new fever cases since July 29, North Korean leader Kim Jong Un on August 10 gave a speech in which he “solemnly declared a victory” over the virus, despite the nation’s limited testing capacity. North Korea and Eritrea are the only 2 countries without a SARS-CoV-2 vaccination program, and North Korea’s hospitals are poorly equipped, lacking reliable electricity and modern medical technologies. At a meeting on COVID-19 policy attended by thousands of unmasked officials, Kim vowed “deadly retaliation” against South Korea, which he blames for causing the outbreak. North Korean defectors to South Korea and activists often send balloons carrying anti-Pyongyang leaflets, and sometimes food, medicine, and money, across the border, which leaders believe brought the virus into the country. Kim called such actions an “influx of rubbish” and threatened to “wipe out” South Korean authorities, who responded by calling the claims “groundless” and “rude and threatening.” Regional experts said the meeting announcing an end to the fever outbreak could be a signal to China that North Korea is ready to reopen trade. Also at the meeting, Kim’s sister, Kim Yo Jong said the leader was “seriously unwell” with fever as the nation faced the outbreak, but she did not specify that his fever was caused by COVID-19.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
UK APPROVAL OF BIVALENT VACCINE BOOSTER The UK became the first country to approve a bivalent COVID-19 vaccine for use as a booster among adults, as many countries plan late-2022 booster drives to hopefully broaden population immunity to SARS-CoV-2 before winter. The adapted bivalent vaccine is an updated version of Moderna’s original monovalent mRNA vaccine, known as “Spikevax bivalent Original/Omicron.” The vaccine targets the original SARS-CoV-2 strain and the Omicron BA.1 variant, a combination which produces significantly more Omicron BA.1-specific neutralizing antibodies than the original monovalent vaccine and may generate BA.4 and BA.5 neutralizing antibodies at a rate 1.69 times higher than the original vaccine, according to trial data from Moderna. The UK Joint Committee on Vaccination and Immunisation (JCVI) published guidance this week for which vaccines should be used during the UK’s fall COVID-19 booster campaign. For adults, the JCVI recommends using either the newly approved Spikevax bivalent Original/Omicron vaccine, one of the original Moderna or Pfizer-BioNTech booster shots, or, in exceptional circumstances, the Novavax Matrix-M adjuvanted wild-type vaccine (Nuvaxovid). The JCVI also offered advice that a single type of booster be used where possible to facilitate deployment and mobilization.
Drug regulators in the EU may meet as soon as September 1 to consider approving a bivalent vaccine that targets the original SARS-CoV-2 strain and BA.1 and could meet later in the month to review a bivalent vaccine using the original strain and BA.5. Meanwhile, US government health officials have indicated they plan to wait for bivalent vaccines capable of targeting the original SARS-CoV-2 strain and the newer BA.4 and BA.5 Omicron subvariants. The Biden administration is aiming to begin a COVID-19 booster shot campaign for all adults in September, but there remain many considerations for regulators to work through before recommending a booster. One of these considerations is that vaccine-induced immunity can wane over time, so the timing of a booster campaign is important. However, many experts agree that getting a booster too early is better than not getting one at all.
NOVAVAX BOOSTER EUA APPLICATION Novavax announced August 15 that it has submitted an application to the US FDA for emergency use authorization (EUA) of its recently authorized SARS-CoV-2 vaccine as a booster dose. If authorized, the booster dose could be administered to qualifying adults who previously received full courses of Novavax or other SARS-CoV-2 vaccines. The Novavax vaccine is an adjuvanted protein-based vaccine, a more traditional vaccine technology than the platform used in mRNA vaccines. Experts have hoped that this tried-and-true formulation may convince more unvaccinated people to receive their primary courses, although uptake in the US has been slow. Based on clinical trial results, the Novavax vaccine appears to remain relatively effective against SARS-CoV-2 variants, including the Omicron and Delta variants of concern. It is less clear how effective this formulation is against BA.5 specifically, but vaccine experts have been looking forward to Novavax’s EUA booster submission to provide another tool in the fight against the wide variety of Omicron subvariants.
BCG VACCINE The Bacillus Calmette-Guérin (BCG) vaccine continues to offer protection from tuberculosis infection into adulthood when given at birth. The vaccine, which has been in use for nearly 100 years, is routinely given to newborns worldwide but is not part of the standard childhood immunization program in the US. Research has shown that neonatal BCG vaccination confers off-target, nonspecific protection against unrelated infectious diseases in early childhood, and the vaccine has been used in clinical trials to examine its effectiveness to reduce the impact of COVID-19, but with little positive outcome. Now, a small, double-blind, placebo-controlled study published in Cell Reports Medicine by researchers from Massachusetts General Hospital suggests the BCG vaccine is highly effective in protecting patients with type 1 diabetes from COVID-19. The researchers found that 12.5% of the group that received placebo shots and 1% of the group that received 3 BCG doses met the criteria for confirmed COVID-19, yielding an efficacy of 92%. Additionally, the BCG group had fewer infectious disease symptoms and lesser severity, and fewer infectious disease events per patient, including COVID-19. The study provides a basis for additional research into the BCG vaccine’s broad-based infection protection, including against SARS-CoV-2 variants.
US CDC COVID-19 GUIDANCE Late last week, the US CDC updated its guidance on COVID-19 vaccination, quarantine, isolation, and testing. The new “streamlined” guidance is in response to broader levels of immunity among the population, from previous infection or vaccination or both, and the availability of effective COVID-19 prevention and management tools that can reduce the risk for medically significant illness and death. The guidance places significant onus on individuals to assess their personal risk and take steps to prevent infection, transmission, or serious outcomes for themselves or others. One of the most significant changes is that persons who are exposed to SARS-CoV-2 and not up to date on their vaccinations no longer need to quarantine. Instead, the CDC recommends they wear a mask in indoor settings for 10 days after exposure and take a test on day 5. The CDC also removed its recommendations for social distancing, test-to-stay programs, and cohorting of students in schools.
These changes have been met with varied reactions, from acceptance to outrage. Expressing concern over the relaxed guidance, many public health experts cite continuing risk from the predominant BA.5 subvariant; the risk of future, possibly more virulent, variants; and declining adherence to personal protective measures that might inhibit their reinstatement if a new wave of infections begins. On the other hand, many members of the general public and institutional decision makers welcomed the simplified guidance as a sign that COVID-19 should not continue to overburden daily routines, particularly as we move closer to the fourth year of the pandemic. Though 3 years of heightened precautions is a long time to expect a global population to remain vigilant against disease, many public health experts believe the CDC is sending the wrong signal at the wrong time. Of particular controversy is CDC’s “Community Levels” metric that is being used to influence its decision making. Because this indicator is influenced more by hospitalizations than transmission, certain areas can appear as if there is less circulating virus than there actually is. Some argue that community transmission* should be more heavily weighted in decision making, especially while highly transmissible variants are circulating.
*To see community transmission levels, change the “Data Type” dropdown menu to “Community Transmission.”
SERIAL TESTING The US FDA this week recommended that people use serial testing—taking multiple COVID-19 tests over several days—to reduce the risk of a false-negative result and to help prevent people from unknowingly spreading the SARS-CoV-2 virus to others. People who test negative on an at-home antigen test should take a second or third test to confirm their result, even if they do not have symptoms. Specifically, the FDA recommends the second test be taken 48 hours after the first test. For those without symptoms but with a known exposure, the agency goes further to say that a third test should be taken another 48 hours after the second test to be even more confident of a negative result. Repeated testing is not a new concept, but this updated recommendation demonstrates the need for continued vigilance in driving down SARS-CoV-2 transmission. While not at odds with the US CDC’s new COVID-19 guidance on quarantine and isolation, the FDA’s recommendation does appear to place more emphasis on assuring lower likelihood of person-to-person transmission following exposure.
US SCHOOLS On August 11, the US CDC released new operational guidance for K-12 schools, early education programs, and daycares to support safe in-person learning during the ongoing COVID-19 pandemic. The new guidelines largely loosen protocols and leave more of the decision-making responsibility in the hands of local officials. Notably, several states—including California, Colorado, Washington, and West Virginia—have issued their own guidance or taken steps to facilitate testing and vaccinations at schools. Few districts are implementing vaccination mandates for students, as Americans are divided over whether such requirements are needed.
The CDC’s guidance recommends that school staff and students stay up-to-date on vaccinations, stay home when sick, practice proper hand hygiene and respiratory etiquette, and that schools optimize and improve ventilation and clean surfaces at least once a day. The guidance also discusses masking, testing, quarantine, and other mitigation strategies, particularly in relation to local community levels or outbreaks. Though the CDC notes that wearing well-fitting masks reduces the risk of spreading SARS-CoV-2 in schools—with a recent preprint study providing additional supporting evidence—the agency only recommends masking in schools located in localities where SARS-CoV-2 “Community Levels” are high. Additionally, most students no longer are advised to quarantine if they have been exposed to someone with COVID-19 but they should wear a mask for 10 days and get tested. The new guidelines also drop the recommendations for routine testing in K-12 schools, although schools located in areas where COVID-19 Community Levels are high may consider implementing screening testing programs. Approximately 40% of counties in the US are currently experiencing high COVID-19 Community Levels, while “Community Transmission” is high in nearly 94% of the country, according to CDC data.
The CDC’s more relaxed guidelines coincide with increased concern about the social, economic, and mental welfare of students who have had limited social interactions over the last few years. Some of the social concerns expressed by parents include students experiencing depression due to extended isolation, students experiencing distress due to missing key social milestones and events, and suicidal ideation in student populations. Economic concerns stem from the pandemic-related disruption in education. Experts estimate that each year of education can add 10% to an individual’s expected lifetime earnings. As a result, disruptions in education due to the pandemic could mean that the current generation of students might be less competitive when they enter the workforce. Concerns about the mental welfare of students have increased due to reports of more emergency room visits linked to mental health among young people, more reports of eating disorders among adolescent girls, and emotional disturbances that can last for years or decades after a traumatic event.
PREGNANCY COVID-19 directly affects people’s health, but the early pandemic also impacted how and when people accessed health care, with lockdowns, workforce shortages, and supply chain issues forcing many to skip or delay routine medical appointments. A retrospective cohort study published August 12 in JAMA Network Open that included more than 1.6 million pregnant patients in 463 hospitals found that the number of live births decreased by 5.2% during the first 14 months of the pandemic compared with the previous 14 months. Additionally, there were increased odds of maternal death during delivery hospitalization (from 5.17 to 8.69 deaths per 100,000 pregnant patients; OR, 1.75; 95% CI, 1.19-2.58), as well as small but significant increased odds of certain pregnancy complications, including gestational hypertension (OR, 1.08; 95% CI, 1.06-1.11), obstetric hemorrhage (OR, 1.07; 95% CI, 1.04-1.10), preeclampsia (OR, 1.04; 95% CI, 1.02-1.06), and preexisting chronic hypertension (OR, 1.06; 95% CI, 1.03-1.09). While it is unclear whether COVID-19 infection directly caused any of the complications, the study’s authors suggested that missed or delayed prenatal visits may have led to some pregnancy complications going undetected or unmanaged and that increased societal stress could have contributed to the increase in hypertension issues.
Prior to vaccines becoming available in late 2020, mis- and disinformation campaigns to discredit the vaccines had already taken hold and especially created uncertainty among pregnant people. Part of what allowed disinformation to flourish was that pregnant people were not included in the initial clinical trials of SARS-CoV-2 vaccines, creating a dearth of safety data that led to pregnant people having some of the lowest vaccination rates among adults when the vaccines were first authorized. Subsequently, many pregnant people, or those looking to become pregnant, chose to delay or forego vaccination, sometimes with dire outcomes. Unvaccinated pregnant women with COVID-19 have a higher risk of stillbirth and other pregnancy complications, including maternal death, than those who are vaccinated. Multiple studies have shown that the vaccines are safe before and during pregnancy and that SARS-CoV-2 infection can have deleterious impacts on pregnant individuals, including heart complications.
An observational cohort study—conducted in Canada and published last week in The Lancet Infectious Diseases—found that not only were mRNA SARS-CoV-2 vaccines safe for pregnant women, but vaccinated pregnant women reported fewer serious health events than non-pregnant women in the week following vaccination and a similar number of events as a group of unvaccinated pregnant women. Though there are many scientific, legal, and ethical considerations related to research associated with pregnancy and including pregnant people, researchers are working to identify these challenges and develop strategies to overcome them.
INCARCERATED POPULATIONS Several large California (US) counties are ending initiatives meant to keep more nonviolent offenders out of jail to lower incarcerated populations during the COVID-19 pandemic amid rising crime. Los Angeles, San Diego, and Santa Clara counties are among those that recently stopped issuing zero bail for people who committed certain nonviolent felony offenses. Similar public health measures instituted nationwide, meant to depopulate jails to avoid COVID-19 outbreaks, brought the US jail population to its lowest level in nearly a decade, according to federal statistics. But rising crime rates are forcing more progressive district attorneys to end such practices, leading to rising jail populations, which remained below their pre-pandemic levels as of the end of 2021. Incarcerated populations have been disproportionately impacted by COVID-19. In California, nearly half of state prisons had 3 to 4 times more COVID-19 cases than the general population.
WESTERN PACIFIC Officials in the Marshall Islands have declared a national health disaster due to the arrival of the highly transmissible Omicron SARS-CoV-2 variant, shifting from a prevention to mitigation strategy. More than 4,000 people have tested positive in a population of about 60,000 in the past week, and the test positivity rate is about 75% in the capital city, Majuro. The Marshall Islands, with a population of about 59,000, was one of the last countries to claim to be COVID-free because of its strict quarantine rules, and until about one week ago, the nation had not recorded a single case of community transmission. About 70% of the nation’s residents are vaccinated. The health disaster declaration provides the government access to emergency funding and the ability to institute several public health measures, including closing schools. While officials have not instituted lockdowns, many people are choosing to stay at home to prevent further community transmission.
Further south in the Pacific Ocean, the number of new COVID-19 cases in New Zealand dropped to its lowest level in 6 months and the average number of hospitalizations is down, showing hopeful signs the winter wave of infections is subsiding. Cases there spiked in mid-July, when deaths from COVID-19 were essentially on par with those from heart disease, the country’s leading killer. About 90% of people aged 12 years and older have completed a primary vaccination series, according to the New Zealand government. In neighboring Australia, there are signs the recent Omicron surge is in decline there as well. However, the number of hospitalizations and the 7-day average of COVID-19-related deaths remain high, and an unknown number of people are suffering long-term impacts of COVID-19 infection. Wait lists for specialized long COVID rehabilitation clinics are now more than 5 months, and experts in Australia are calling for a nationally coordinated approach to address the condition. Infectious disease experts cautioned that while the worst of the winter surge might have passed, there will be future surges and people should continue to wear masks to help mitigate disease transmission. According to the Australian government, 96% of people aged 16 years and older have received at least 2 doses of vaccine.
by ponchi101
dryrunguy wrote: ↑Tue Aug 16, 2022 5:31 pm
NOVAVAX BOOSTER EUA APPLICATION Novavax announced August 15 that it has submitted an application to the US FDA for emergency use authorization (EUA) of its recently authorized SARS-CoV-2 vaccine as a booster dose. If authorized, the booster dose could be administered to qualifying adults who previously received full courses of Novavax or other SARS-CoV-2 vaccines. The Novavax vaccine is an adjuvanted protein-based vaccine, a more traditional vaccine technology than the platform used in mRNA vaccines. Experts have hoped that this tried-and-true formulation may convince more unvaccinated people to receive their primary courses, although uptake in the US has been slow. Based on clinical trial results, the Novavax vaccine appears to remain relatively effective against SARS-CoV-2 variants, including the Omicron and Delta variants of concern. It is less clear how effective this formulation is against BA.5 specifically, but vaccine experts have been looking forward to Novavax’s EUA booster submission to provide another tool in the fight against the wide variety of Omicron subvariants.
Oh, yes, of course. The reason why all these people refuse to get vaccinated is because they did not have am adjuvanted protein-based vaccine; that was the problem. They did all their research and that was what they were unconvinced about.
We are all fine, now.
dryrunguy wrote: ↑Tue Aug 16, 2022 5:31 pm
NOVAVAX BOOSTER EUA APPLICATION Novavax announced August 15 that it has submitted an application to the US FDA for emergency use authorization (EUA) of its recently authorized SARS-CoV-2 vaccine as a booster dose. If authorized, the booster dose could be administered to qualifying adults who previously received full courses of Novavax or other SARS-CoV-2 vaccines. The Novavax vaccine is an adjuvanted protein-based vaccine, a more traditional vaccine technology than the platform used in mRNA vaccines. Experts have hoped that this tried-and-true formulation may convince more unvaccinated people to receive their primary courses, although uptake in the US has been slow. Based on clinical trial results, the Novavax vaccine appears to remain relatively effective against SARS-CoV-2 variants, including the Omicron and Delta variants of concern. It is less clear how effective this formulation is against BA.5 specifically, but vaccine experts have been looking forward to Novavax’s EUA booster submission to provide another tool in the fight against the wide variety of Omicron subvariants.
Oh, yes, of course. The reason why all these people refuse to get vaccinated is because they did not have am adjuvanted protein-based vaccine; that was the problem. They did all their research and that was what they were unconvinced about.
We are all fine, now.
You forgot to put the "/s" for sarcasm after your comment Ponch.
by ti-amie
by ti-amie
by dryrunguy Here's the latest Situation Report. Haven't read it yet. But the section on pandemic-related fraud caught my eye.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 592 million cumulative cases and 6.45 million deaths worldwide as of August 18. According to the WHO weekly epidemiological update for August 17, the number of new weekly cases decreased by 24% during the week of August 8-14, compared to the previous week. The number of new weekly deaths decreased by 6%, compared to the previous week.
At the regional level, the number of new weekly cases decreased across all six regions: African (-38%), European (-38%), Eastern Mediterranean (-30%), Western Pacific (-18%), Americas (-17%), and South-East Asia (-11%). The number of new weekly deaths increased in the Western Pacific (+31%) and South-East Asia (+12%) regions and decreased or remained stable in the African (-33%), European (-25%), Eastern Mediterranean (-7%), and Americas (-4%) regions.
UNITED STATES
The US CDC is reporting 93 million cumulative cases of COVID-19 and 1,033,332 deaths. The current 7-day moving average of new daily cases is down over last week, dropping to 98,940 on August 16 from 107,899 on August 9. The average daily mortality remains relatively stable, at 398 on August 16. Daily mortality has remained above or around 400 since July 12.** New national ensemble forecasts of new and total deaths predict that the number of newly reported COVID-19 deaths will remain stable or have an uncertain trend over the next 4 weeks, with 1,800 to 5,000 new deaths likely reported in the week ending September 10, 2022, and a total of 1,046,000 to 1,055,000 COVID-19 deaths predicted to be reported by this date.
Both new hospital admissions (-3.5% over the past week) and current hospitalizations (-5.3%) decreased over the previous week, potentially reflecting a downward trend to the latest surge driven by the Omicron BA.5 subvariant. New national ensemble forecasts predict that the number of new daily confirmed COVID-19 hospital admissions will remain stable or have an uncertain trend, with 2,600 to 9,700 new confirmed COVID-19 hospital admissions likely reported on September 9, 2022.
BA.5 is now projected to account for 88.8% of sequenced specimens in the US. The BA.4 sublineage accounts for about 5.3% of cases, while the BA.4.6 sublineage accounts for 5.1% of cases. Together, BA.2.12.1 accounts for only about 0.8% of cases. According to the estimate, Omicron variants represent all new cases in the US.
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
US RESPONSE The US appears to have entered somewhat of a COVID-19 plateau. While there are signs that the latest surge caused by the Omicron BA.5 subvariant might be slowing—the average number of daily infections and hospitalizations are falling—an average of about 400 people have died of the disease every day for the past month. US officials have indicated that Omicron-adapted vaccine boosters could be available for everyone aged 12 and older within the next month, but the US FDA and CDC must act first to authorize and recommend a new vaccine booster. Experts have mixed opinions regarding an FDA plan to base its authorization decision on studies involving mice instead of humans. The UK this week approved a new bivalent booster from Moderna that targets both the original SARS-CoV-2 strain as well as the original Omicron variant, BA.1. The FDA rejected BA.1 bivalent booster versions earlier this year, instead calling on vaccine manufacturers to develop bivalent boosters targeting the Omicron BA.4 and/or BA.5 subvariants.
The federal government has already secured millions of doses of these not-yet-authorized bivalent vaccine boosters from Moderna and Pfizer-BioNTech, but the White House recently announced it is making plans to no longer buy vaccines, treatments, or diagnostic tests, as early as this fall. Without additional funding from the US Congress to purchase those products, availability will shift to the commercial market, raising questions about equitable access. However, the Biden administration is expected to extend the COVID-19 public health emergency for another 90 days in mid-October, which likely would ensure expanded Medicaid coverage, telehealth services, increased payments to hospitals, and other pandemic measures remain in place into early 2023. Meanwhile, the US CDC has loosened its COVID-19 guidance and public health agencies are adapting lessons learned during the pandemic to address other—possibly more pressing—public health and equity challenges, signaling what many see is an attempt to enter a “new normal.”
US CDC REORGANIZATION US CDC Director Dr. Rochelle Walensky on August 17 announced a large-scale reorganization and pivot for the agency, after receiving the results of an external review of the institution that she initiated in April. The review was led by James Macrae, a long-time senior official with the US Department of Health and Human Services, the parent agency of CDC, and was based on 120 interviews with key informants inside and outside the institution. Findings from the review are not yet public. Dr. Walensky announced that, according to the review, the future success of the CDC depends on pivoting from a slower, more academic institution to a swift emergency response agency, providing actionable information to the public and other health authorities in an appropriate and understandable fashion. Initial agency changes to institute this vision include revamping the website, creating a new equity office, creating a new executive council to oversee the overall new vision, hastening time to publication for data needed for response decisions, prioritizing budget allocation for the agency, and promoting staff according to public health impact. Additionally, officials responding to public health crises would now be required to stay in their positions for at least 6 months, and more staff would be trained for those roles as well. Dr. Walensky also is seeking greater authority for the CDC to collect data from states, more quickly finance external partners during health crises, and develop more competitive benefits for prospective staff recruitment. Outside experts have praised the proposed changes to the agency’s vision but some remain skeptical as to whether the proposed shifts are possible or will be enough to address the missteps of the agency during the COVID-19 pandemic.
IMMUNITY AGAINST OMICRON Various studies have indicated that prior SARS-CoV-2 infection may provide some protection against or reduce severity of future infection. However, new studies suggest that prior infection with an Omicron variant may provide increased protection against BA.4 or BA.5 compared to prior infection with Alpha, Beta or Delta variants—although outside experts note the comparison may not be fair because immunity wanes over time. A new preprint study posted August 17 to medRxiv supports this criticism, as it documented rapid waning of protection from an earlier Omicron variant infection against BA.5, particularly 3-5 months post-infection. Furthermore, another study published in Nature Communications suggests that protection post-Omicron infection (BA.1) declines more quickly among unvaccinated individuals compared to their vaccinated counterparts. Altogether, this growing body of literature emphasizes the continued importance of COVID-19 vaccination and the widespread variations in protection based on disease history, and the findings should be taken into consideration for future response planning.
LONG COVID RESEARCH RESULTS People with post-COVID conditions, or long COVID, and their advocates continue to push for more research and clinical treatments for the mix of—and far from uniform—lasting symptoms that make up the condition. Recent developments include a preprint study, posted to medRxiv this month, evaluating the distinguishing symptoms of long COVID. Notably, the researchers found that those with the condition had lower levels of the stress hormone cortisol, in addition to the often-present cognitive deficits—sometimes known as “brain fog”—and fatigue. Similar results have been reported in previous studies, including one published in Cell, which also documented “exhausted T-cells” that result in chronic inflammation indicative of several long COVID symptoms. Impaired memory, fatigue, shortness of breath, and trouble concentrating were among key complaints of participants of a study published August 12 in Clinical Infectious Diseases that followed patients for 12-18 months after infection. Overall, 43% of participants experienced persistent symptoms after mild COVID-19. Researchers also noted that shortness of breath and the number of experienced symptoms at the 12 month mark were significantly linked to specific SARS-CoV-2 spike protein-specific immune responses.
In a 2-year study published August 17 in The Lancet Psychiatry, Oxford researchers retrospectively assessed the risks of 14 neurological and psychiatric diagnoses after SARS-CoV-2 infection among 1.25 million patient records, including children. The researchers matched the COVID-19 patients with patients who had different respiratory infections and found that while common mood disorders typically returned to baseline after 1-2 months in both groups, adults with COVID-19 had an increased risk of psychotic disorder, brain fog, dementia, and epilepsy or seizures by the end of the second year of the follow-up, compared with adults with other respiratory diseases. Children also were at an increased risk for brain fog, in addition to insomnia, intracranial hemorrhage, ischemic stroke, psychotic disorders, and seizures. Children, however, experienced a finite horizon of 75 days for brain fog, nor were they at an increased risk for mood or anxiety disorders in the 6 months following SARS-CoV-2 infection. The study also accounts for the rise of 3 viral variants. The emergence of the Delta variant increased risks of ischemic stroke, seizures, cognitive deficit, insomnia, and anxiety disorders, as well as an increased death rate. The death rate following Omicron emergence was lower than just before, but the risks of neurological and psychiatric symptoms remained similar. Risk profiles remained similar just before and after the emergence of the Alpha variant. The studies all point to the need for more attention to be given to the post-infection risks of SARS-CoV-2, as well as other viruses.
WASTEWATER SURVEILLANCE The COVID-19 pandemic helped bolster an existing surveillance system for infectious diseases: wastewater testing. The method is now being used to track not only older diseases such as norovirus, but also new and emerging viruses including SARS-CoV-2, monkeypox, and polio. Several US states and jurisdictions have taken steps to launch or expand wastewater surveillance programs to provide a better understanding of circulating SARS-CoV-2 levels and variants. The New York Times this week published an interactive exploration into how these systems work and the steps involved in extracting results.
MASKING & INFECTIOUS AEROSOLS Healthcare workers are at an increased risk of SARS-CoV-2 infection, with many required or choosing to wear personal protective equipment such as masks. Those who always wore respirator masks rather than surgical masks had a 40% lower likelihood of infection, irrespective of cumulative exposure, according to a study published August 15 in JAMA Network Open. Among 2,919 healthcare workers included in the study, 749 (26%) tested positive for SARS-CoV-2 between September 2020 and September 2021. Among those with patient exposure, test positivity was 21% among workers wearing respirators compared with 35% among those who used surgical masks or a mix of masks (OR, 0.49; 95% CI, 0.39-0.61). The study was conducted in Switzerland prior to the predominance of the Omicron variant, so the results might not be applicable to newer, more transmissible variants.
A July 29 preprint study posted to medRxiv shows that viral shedding (measured as RNA copies) in exhaled breath aerosol was significantly greater during infections with the more highly transmissible SARS-CoV-2 Alpha, Delta, and Omicron variants than with the ancestral strain and variants not associated with increased transmissibility, even among people who are up to date on vaccinations. The researchers documented the highest viral shedding from a person with Omicron infection. They said the findings provide additional evidence that inhalation of infectious aerosols is the dominant mode of SARS-CoV-2 transmission and support the importance of continued mitigation efforts such as improving indoor air hygiene through ventilation, filtration, and air disinfection, and wearing masks or respirators.
PANDEMIC-RELATED FRAUD The US government has appropriated US$5 trillion in relief programs aimed at helping businesses and individuals during shutdowns due to the COVID-19 pandemic. However, that funding came with minimal oversight leading to an unprecedented amount of fraud, with billions of dollars stolen by thousands of people, through unemployment payouts or business assistance. Now, federal investigators and prosecutors are trying to identify and charge people who committed such crimes, with 500 people working on pandemic-fraud cases across at least 21 government agencies, as well as the FBI, Secret Service, Postal Inspection Service, and the Internal Revenue Service. But with tens of thousands of ongoing investigations, officials are concerned some crimes may never be prosecuted. New laws extend the statute of limitations for some pandemic-era fraud from 5 years to 10 years, and officials hope the extensions will help them find and prosecute more offenders. The costs of loose rules and lax oversight should provide lessons for future pandemic preparedness responses to include planning and prevention efforts for fraud.
UNIVERSAL HEALTHCARE Countries with or close to achieving universal health coverage (UHC)—a system under which all individuals and communities receive needed health services without suffering financial hardship—saw smaller declines in routine childhood vaccinations during the COVID-19 pandemic, according to a study published August 16 in PLOS Medicine. Countries included in a “high UHC index” group had a 2.7% smaller reduction in childhood immunization coverage during 2020 when compared to countries with lower UHC Service Coverage Index rankings. Additionally, a study published August 17 in The Lancet Regional Health found that primary health care coverage in Brazil mitigated socioeconomic disparities in accessing SARS-CoV-2 vaccination. Taken together, these studies provide evidence that UHC guarantees more equitable access to vaccinations and suggest that policymakers should continue to advocate for working toward the goal of achieving access to safe, effective, quality, and affordable healthcare services for all.
by ponchi101 Very odd that the number of cases is dropping, but fatalities are not.
Simplest explanation: cases are the same, people are simply not getting tested as much.
by Deuce Well... the number of deaths always start increasing 2 or 3 weeks after the number of cases and hospitalisations begin increasing... so it would stand to reason that the number of deaths would start decreasing a couple of weeks after the number of cases start decreasing...
by Suliso People either don't test at all or do a self test and usually don't report even a positive test to any official authorities.
by Deuce
Suliso wrote: ↑Fri Aug 19, 2022 8:01 pm
People either don't test at all or do a self test and usually don't report even a positive test to any official authorities.
But that's been the case for about the past 6 months...
by dryrunguy Here's the latest Situation Report. Am I the only one who has become completely lost by the "what vaccine should I be getting next?" debate? Especially given the fact we have no idea what variants will emerge down the road?
::
OMICRON-ADAPTED BOOSTERS Previous COVID-19 Situation Reports have outlined the United States’ and other countries’ decisions to prioritize SARS-CoV-2 vaccines adapted to newer viral variants for future booster campaigns. New variants are differentiated from the original strain of the virus targeted by initial vaccines, showing significant mutations in portions of the spike protein. This differentiation reduces the effectiveness of current vaccines, as well as natural immunity gained through previous infection, and has contributed to surges in COVID-19 cases in many countries.
For many months, public health experts and scientists have discussed the promise of new vaccines, targeted for specific variants. Both Pfizer-BioNTech and Moderna are primed to offer versions of their COVID-19 vaccines specifically tailored to target various sublineages of the globally predominant Omicron variant. The UK became the first country to approve a bivalent COVID-19 vaccine for use as a booster among adults on August 15, authorizing the use of Moderna’s “Spikevax bivalent Original/Omicron,” which targets both the original SARS-CoV-2 strain and the Omicron BA.1 variant. Canada this week announced it has secured 12 million doses of an Omicron-adapted vaccine from Moderna, and the government is currently reviewing bivalent vaccine submissions from both Moderna and Pfizer-BioNTech, with decisions expected in about 2 weeks. Vaccines under review are targeting the original virus and earlier Omicron lineages.
In the US, the government has agreed to purchase 66 million doses of Omicron-adapted vaccines from Moderna and 105 million from Pfizer-BioNTech, but those vaccines are expected to target the original virus and the BA.4 and BA.5 subvariants instead of BA.1. Pfizer and BioNTech this week requested emergency use authorization (EUA) from the US FDA for the companies’ Omicron BA.4/BA.5-adapted vaccine for individuals aged 12 years or older, despite the lack of new clinical data on the shot. In the same announcement, the companies said a trial investigating the safety, tolerability, and immunogenicity of the Omicron BA.4/BA.5-adapted bivalent vaccine is expected to start this month. The companies have provided the FDA with preclinical and manufacturing data on the vaccine, but they have not yet made that information public. Despite the later start researching and making a US supply, the companies say the mRNA platform is well-suited for quick adaptations and federal health officials remain steadfast that the newer bivalent vaccines will be available by mid-September.
Current projections suggest that any person aged 12 or older who has completed a primary COVID-19 vaccination series will be eligible to receive these booster doses when they become available. This projection could change as data come in and are considered, and eligibility could differ among any authorized vaccine boosters. Scientists agree that these new booster doses likely will help improve the nation’s immune protection, but some question how well they will work given that oftentimes, the version of a virus to which an individual has an initial immune response can impact responses to future variants and vaccines. Additionally, many public health experts are worried that the prevailing “COVID is over” sentiment in many countries will negatively impact uptake of vaccine boosters.
NOVAVAX VACCINE EUA On August 19, the US FDA expanded its emergency use authorization (EUA) of Novavax’s protein-based COVID-19 vaccine to include adolescents. The FDA initially authorized the 2-dose primary series vaccine for adults in July, demonstrating 90% efficacy, and the shots will now be available for individuals aged 12 to 17, among whom it showed 80% clinical efficacy. The 2 doses are given 3 weeks apart. The Novavax vaccine uses a more traditional, protein-based technology that teaches the immune system to recognize small, modified pieces of the coronavirus spike protein. This older technology is also used in vaccines for hepatitis B, HPV, and pertussis. The Novavax vaccine also contains the Matrix-M adjuvant, which helps to induce a broader immune response. In July, the company announced that the vaccine shows “broad” immune response to circulating variants, including Omicron BA.4 and BA.5. However, Novavax is also working on an updated version of the vaccine that specifically targets the Omicron variant and subvariants. The company intends to file for authorization for a bivalent vaccine later this year.
PAXLOVID REBOUND The US FDA has requested that Pfizer conduct a study examining an extended course of its antiviral Paxlovid among individuals who experience a rebound of COVID-19 after taking an initial 5-day course. The FDA wants to know if a second 5-day course of the antiviral would help prevent disease rebound, and has requested that Pfizer produce initial results of such a trial by September 30, 2023. While Pfizer claims that disease rebound following Paxlovid treatment remains rare, several high-profile cases have prompted the FDA’s request for further study into the phenomenon.
INCUBATION PERIOD According to a study published August 22 in JAMA Network Open, the incubation period of COVID-19 has decreased gradually as SARS-CoV-2 has continuously evolved and mutated, producing variants with different enhanced transmission and virulence. The incubation period is the interval between exposure and development of symptoms and is an important epidemiologic indicator for understanding transmission. Based on the authors’ meta-analysis, the initial “wild type” strain first detected in Wuhan, China, in 2019 had an incubation period of approximately 5.2 days. Later in 2020, the Alpha variant that quickly became dominant in the UK had an incubation period of about 5 days. The Beta variant was identified shortly after and showed a shortened incubation period of 4.5 days, followed by the Delta variant with 4.41 days. The incubation period for Omicron infection is currently 3.42 days. While a decrease in incubation period often is associated with more severe disease, the decrease with COVID-19 means it makes it much more difficult to control transmission, because the faster someone becomes contagious, the faster an outbreak spreads. Knowledge of this key epidemiological parameter is helpful not only in reducing local transmission but also in understanding presymptomatic transmission.
HOME ANTIBODY TESTS The advent of home antigen tests for SARS-CoV-2 were an important step in helping people gain real-time knowledge of their infection status so they could isolate at home and hopefully stop chains of transmission. Now scientists are working to develop at-home antibody tests to help people determine their level of protection from infection and whether they might need an additional vaccine booster. A new study published this week in Cell Reports Methods describes a finger-prick test to detect neutralizing antibodies against SARS-CoV-2. If the test holds up to large-scale testing, it could provide an inexpensive way for people to learn how well-protected they are against the virus, although they might still be susceptible to newer viral variants capable of evading certain immune system responses.
UK COVID-19 INQUIRY Officially launched in July, the UK COVID-19 Inquiry is an independent panel established to examine the UK’s response to and impact of the COVID-19 pandemic and provide lessons for future pandemic preparedness and responses. Now, a coalition of 9 health and development nongovernmental organizations (NGOs) are calling for the inquiry to expand beyond its focus on the domestic response to also consider in what ways the UK government’s response contributed to growing global inequities during the pandemic. The NGOs—including Oxfam GB, Save the Children UK, Médecins Sans Frontières UK, and Health Poverty Action—sent a letter on August 22 requesting an expansion of the investigation. Another signatory, RESULTS UK, released a report August 16 outlining and assessing various UK government actions in response to the pandemic and providing recommendations for the UK government, including the UK COVID-19 Inquiry be broadened. Inquiry representatives have not yet indicated whether they will expand their examination.
In related news, several US Republican lawmakers have vowed to investigate the role certain individuals played in the US COVID-19 pandemic response if they gain control of the House of Representatives or Senate next year. One figure is Chief Medical Advisor to the White House and NIAID Director Dr. Anthony Fauci, who formally announced his retirement from public service this week.
IRAN In an investigation, the Washington Post outlines how members of Iran’s government and the domestic pharmaceutical company Barkat pushed through the approval of a yet-unproven COVID-19 vaccine during the country’s worst SARS-CoV-2 surge. The company failed to deliver an agreed upon 50 million doses, and most Iranians were vaccinated with a Chinese-produced vaccine. Nevertheless, Barkat’s profits soared, and the company appears to have compensated government officials who sat on its board and pushed the vaccine’s approval.
by ponchi101
dryrunguy wrote: ↑Tue Aug 23, 2022 4:12 pm
Here's the latest Situation Report. Am I the only one who has become completely lost by the "what vaccine should I be getting next?" debate? Especially given the fact we have no idea what variants will emerge down the road?
::
...
You are not the only one. But I am not getting any more Bt/PF or Moderna boosters, unless they carry some new tech.
And I am not getting anything until Jan 2023.
by Deuce I've had the 2 initial vaccines, and 2 boosters. All Moderna.
My most recent booster was in June.
I will continue studying and reading up on the matter, and expect to get another booster in the late fall/beginning of winter, as that will be 5/6 months after my most recent booster.
What the next booster will be, I don't know - maybe the one targeting Omicron, maybe not.
One thing is certain: the boosters specifically targeting a particular variant will always lag behind - because these boosters cannot be created in a day, and so there will always be the potential of a new variant taking over just when the booster targeting the previous variant is being approved. It cannot be otherwise.
by dryrunguy Here's the latest Situation Report. Serious question: Would you take a booster that has not yet cleared human clinical trials to confirm safety and efficacy?
::
EPI UPDATE The WHO COVID-19 Dashboard reports 595 million cumulative cases and 6.45 million deaths worldwide as of August 25. Global weekly incidence decreased for the second consecutive week, down 8% from the previous week. Global weekly mortality appears to have peaked as well, down 13.5% from the previous week.
Regional trends in weekly incidence and mortality also are declining. All regions, with the exception of the Western Pacific, reported decreases in weekly incidence, ranging from -13% to -23% from the previous week. Notably, the Western Pacific reported a slight increase (+1.6%), but the weekly total was still 17% lower than the most recent peak reported the week of August 1. Weekly mortality is declining in all regions except the Eastern Mediterranean and Western Pacific. The Eastern Mediterranean region does appear to be at or near a peak, so if it follows the global trends, we expect weekly mortality to begin decreasing in the next week or two. The Western Pacific region’s weekly mortality continues to increase substantially, up 7.7% over the previous week and 2.5 times the most recent low reported the week of July 11. In light of the region’s sharp peak in weekly incidence several weeks ago, we expect to observe a corresponding decline in mortality over the next week or two.*
*The WHO Dashboard notes that incidence and mortality data for the Africa Region are incomplete.
UNITED STATES
The US CDC is reporting 93.6 million cumulative cases of COVID-19 and 1,036,604 deaths. Average daily incidence continues to decline, down from the most recent high of 129,359 new cases per day on July 21 to 89,698 on August 23—the lowest average since May 12. Average daily mortality appears to have passed a peak, down from 466 deaths per day on August 12 to 390 on August 23. A lag in daily mortality of 2-4 weeks behind daily incidence is consistent with the trends we have observed over the course of the pandemic.**
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to decline, down 3.3% and 6.6%, respectively, over the past week. Both trends peaked around the last week of July, similar to trends in daily incidence.
The BA.5 sublineage is projected to account for 88.9% of sequenced specimens in the US. While BA.5 remains the overwhelmingly dominant variant—and continues to increase in prevalence—the prevalence of the BA.4.6 sublineage is increasing as well. Over the past 2 weeks, BA.4.6 became the #2 variant nationwide, now accounting 6.3% of sequenced cases, while BA.4 fell to #3 (4.3%). It remains unclear whether BA.4.6 is capable of usurping BA.5 in the US, but its increasing prevalence could potentially indicate that it is competing well against the dominant variant. Collectively, the remaining variants account for only 0.5% of cases nationally. All variants reported here are sublineages of the Omicron variant of concern (VOC).
US BOOSTER CAMPAIGN Following recent news regarding the authorization of variant-adapted SARS-CoV-2 vaccine boosters in the UK and applications for emergency use authorization (EUA) of BA.4/BA.5 boosters in the US (both Pfizer-BioNTech and Moderna), US government officials have signaled that variant-adapted booster doses could be available for individuals aged 12 years and older by early September. The bivalent vaccines will target both the original strain of SARS-CoV-2 and both the BA.4 and BA.5 sublineages (since they share common mutations to the spike protein).
While human clinical trials have not yet been conducted, the agency’s Director of the Center for Biologics Evaluation and Research (CBER), Dr. Peter Marks, indicated that he is “extremely confident” that the trials will demonstrate the candidate boosters to be safe and efficacious. In contrast to regulatory review of previous SARS-CoV-2 vaccine candidates, the FDA is not waiting on the completion of human clinical trials. Rather, the agency will base their assessment primarily on data from animal models and previous clinical trial data on BA.1-adapted bivalent candidate vaccines, a process similar to how the FDA reviews seasonal influenza vaccines. Clinical trials for the candidate boosters in humans are expected to begin this month. Reportedly, the FDA does not intend to convene its Vaccines and Related Biological Products Advisory Committee (VRBPAC) to discuss the candidate boosters; however, the CDC’s Advisory Committee on Immunization Practices (ACIP) has tentatively scheduled a meeting for September 1-2 in anticipation of a FDA decision.
Some experts have expressed doubt regarding the need for a BA.4/BA.5-specific booster, as it may provide little additional protection for the millions of people who have already been exposed to one of those variants. Similarly, antibodies generated to protect against BA.4/BA.5 may not provide sufficient protection against other emerging variants, such as BA.2.75. While some experts are concerned that the abbreviated regulatory review risks increasing vaccine hesitancy and mistrust among the public, others argue that it is critical to make variant-adapted boosters available quickly, to provide protection before the virus evolves further and new variants emerge.
PANDEMIC INVESTMENTS Much of the federal funding allocated to the US COVID-19 pandemic response—approximately US$3.9 trillion of US$4.5 trillion—has been spent, and the US Congress has not agreed to authorize additional funding. This leaves many wondering what is worth investing in at this point in the pandemic, when we have many tools to prevent and treat COVID-19 but also uncertainties about future SARS-CoV-2 variants. Many experts agree that funds should be directed toward developing next-generation vaccines—those that can prevent infection instead of only avoiding serious outcomes—and improving indoor air quality, which could help mitigate a host of airborne illnesses and allergens, as well as mitigate the health impacts of air pollution. Overall, they agree investments should be geared toward strategies that provide lasting benefits beyond the COVID-19 pandemic.
The world could be entering a new age of more frequent and intense infectious disease outbreaks, with some infectious disease experts calling attention to the fact that diseases can spread quickly as international travel ramps back up. This highlights the urgent need to improve other public health efforts, including upgrading disease surveillance, data collection, and analysis; rebuilding trust in science and public health systems; taking a holistic view of health to include human-driven environmental change and animal health; closing gaps in health inequities; and boosting funding for pandemic preparedness. With some modeling showing extreme disease events similar to COVID-19 could increase 3-fold in the coming decades, the US and the world must prepare now to mitigate future epidemic, and perhaps pandemic, impacts.
PAXLOVID Several high-profile cases of COVID-19 rebound following treatment with Paxlovid—including White House Science Advisor Dr. Anthony Fauci, US President Joe Biden, and, most recently, First Lady Dr. Jill Biden—raise questions about how often such cases occur. Initial studies of the antiviral suggest that between 1% and 6% of people who take the drug experience rebound, with or without symptoms, around days 10-14 after initially testing positive. But some physicians believe rebound cases are more common, estimating between 20% and 40% of patients who take Paxlovid experience the condition, based on anecdotal evidence. The US FDA has requested that Pfizer, the drug’s manufacturer, conduct clinical trials to better understand the condition and its frequency.
Nevertheless, Paxlovid remains highly effective at preventing serious COVID-19 among people at high-risk of disease progression, according to several studies. In a retrospective cohort study published August 24 in the New England Journal of Medicine, Israeli researchers report that the treatment reduced hospitalizations among people aged 65 years and older who were assessed as being at high risk for progression to severe disease by 73% and reduced the risk of death from complications by 81% when given shortly after infection during the Omicron surge, compared to patients who did not take the treatment. Those findings are consistent with earlier trial results. However, the researchers found Paxlovid showed no evidence of benefit among patients aged 40 to 64 years who were deemed at high risk for disease progression. Across both age groups, a lack of previous SARS-CoV-2 immunity and previous hospitalization were strongly associated with high rates of hospitalization due to COVID-19.
In another study published the same day in The Lancet Infectious Diseases, researchers report that during the Omicron BA.2 wave in Hong Kong, early Paxlovid use was associated with a 66% lower risk of death and early use of molnupiravir—another authorized antiviral, also known as Lagevrio and made by Merck—was associated with a 52% lower risk of death among hospitalized COVID-19 patients who did not need oxygen supplementation. Additionally, patients who took antivirals had a lower risk of disease progression and significantly shorter times reaching low viral burden than those who did not receive the treatments. Taken together, the studies support the continued use of antiviral therapeutics authorized to treat COVID-19 among certain populations, including older patients and those who are hospitalized but not requiring oxygen therapy upon admission, but raise questions for the use of the treatments among the general population. In the US, Paxlovid is authorized for the treatment of mild-to-moderate COVID-19 in certain adult and pediatric patients aged 12 years or older who are at high risk of disease progression, and Lagevrio is authorized for the treatment of mild-to-moderate COVID-19 in high-risk adults aged 18 or older who are at high risk of severe COVID-19 and for whom alternative treatment options are not accessible or clinically appropriate.
VACCINE EFFICACY AMONG YOUNG CHILDREN On August 23, Pfizer and BioNTech announced that their 3-dose primary series SARS-CoV-2 vaccine showed 73.2% efficacy among children younger than 5 years old without evidence of prior infection. The study was conducted during a time when the Omicron BA.2 subvariant was predominant. Among 794 children who were fully vaccinated, 13 were infected, compared with 21 of 351 children who received placebo doses. The vaccine was 75.8% effective among children younger than 23 months old and 71.8% effective among toddlers aged 2 to 4 years old. Sequencing of viral RNA from nasal swabs indicated that cases of COVID-19 among trial participants were primarily caused by Omicron BA.2. Given that the Omicron BA.4 and BA.5 subvariants emerged during the trial and now cause most infections among US adults, the companies indicated their intent to request US FDA emergency use authorization (EUA) of an Omicron BA.4/BA.5-adapted bivalent vaccine in children ages 6 months through 11 years. Though these results continue to illustrate that the Pfizer-BioNTech vaccine is safe, effective, and well-tolerated among children—and despite a national push to vaccinate more children—less than 5% of US children under age 5 have been vaccinated.
LONG COVID/PASC Many researchers are baffled by post-acute sequelae of SARS-CoV-2 infection (PASC) and post-COVID-19 conditions, often referred to as long COVID, a persisting condition affecting some people who have recovered from acute SARS-CoV-2 infection, for which symptoms are vaguely defined, vary in prevalence and severity, and are sometimes difficult to attribute to COVID-19. Despite centuries of evidence showing that viral infections can leave long-term, often debilitating, health complications in their wake, many suffering from long COVID and their advocates are urging more research and support to define and treat the condition. Earlier this month, the Biden administration released 2 reports that outline a national research action plan for the condition and describe federal services available to address the longer-term effects of the pandemic, including long COVID and related conditions.
But without a standardized definition or treatment protocols for long COVID, patients, healthcare workers, and insurers are left wondering how to proceed with care and recovery. Some are turning to unproven treatments and theories about potential underlying causes of the condition, including the hypothesis that tiny, persistent blood clots could be contributing to the wide array of symptoms. Additionally, without workplace protections, universal health care, and adequate medical support, adults with long COVID sometimes are forced to leave their jobs or incur enormous medical debt. In a new report, the Brookings Institution estimates that around 16 million US residents of working age (18 to 65 years old) have long COVID, and 2 million to 4 million of those are out of work due to the condition. The annual cost of those lost wages is estimated to be around US$170 billion annually, and as high as US$230 billion, according to the report, which warns that without sufficient policy actions, those impacts could worsen over time.
In related news, long COVID may be less common among pediatric COVID-19 patients than feared. A study published August 22 in JAMA Pediatrics reported a low burden of PASC among study participants, with only 3.7% of children with COVID-19 experiencing at least 1 systemic, syndromic, or medication feature of PASC when compared with children without COVID-19. The researchers noted that the risks of PASC were higher among participants who had more severe SARS-CoV-2 infection, were younger, or had comorbid complex underlying chronic diseases.
UK COVID-19 MORTALITY The UK is reporting considerably higher COVID-19 mortality in summer 2022 than in 2021. From June 8 through August 12, the UK’s COVID-19 mortality was nearly twice the total from the same period last year. During that span, the UK reported more than 5,700 COVID-19 deaths in 2022, compared to 2,936 in 2021. Overall, the cumulative mortality for 2021 far exceeds the 2022 total to date—65,000 compared to 28,303—however, the data illustrate the severity of the UK’s summer Omicron surge, driven largely by the BA.5 subvariant. In June 2021, the UK had reached the end of its Alpha wave, and the Delta variant of concern (VOC) emerged as a major driver of transmission. In contrast, the BA.5 subvariant grew quickly to predominance in June in the UK and essentially spanned the entire summer. Consistent with the trends over the course of the pandemic, the vast majority of UK COVID-19 deaths in summer 2022 were among older adults. Notably, nearly half of the summer 2022 deaths were among adults aged 85 years and older, compared to 27% in 2021, and there were 77% more deaths among adults aged 75-84 years than the same period in 2021.
The UK also suffered a historic heatwave this summer, which may have contributed to the elevated COVID-19 mortality. During 3 “heat periods” in July, the UK reported overall increases in deaths nationwide—ie, all deaths, not only COVID-19. The average daily mortality during these periods (1,224 deaths per day) was 7% higher than the rest of the month. On July 19 alone, when temperatures in the UK exceeded 40°C/104°F for the first time in history, the UK reported 1,775 deaths, more than 50% higher than the average during non-heat periods. Beyond the overall mortality trends related to the heat, data from the UK’s Office of National Statistics (ONS) shows spikes in COVID-19 deaths corresponding to periods of unusually high temperatures. Specifically, daily COVID-19 deaths were nearly one-third higher during 3 “heat periods” in July, compared to other days that month. Older adults tend to be particularly vulnerable to the effects of heat waves, which could potentially account for some of the increased COVID-19 mortality on those days. Further study is required in order to determine any link between the record temperatures and COVID-19 mortality.
REGULATORY PRESSURE According to a new report from the US House Select Subcommittee on the Coronavirus Crisis, senior officials in the administration of former President Donald Trump, as well as outside allies, pressured the US FDA to authorize SARS-CoV-2 vaccines on an accelerated timeline, prior to the November 2020 election, and to authorize or reauthorize ineffective and potentially dangerous treatments for COVID-19, particularly the antimalarial drug hydroxychloroquine touted by Trump. The committee reviewed emails and texts and heard testimony from high-ranking officials to understand the extent of political interference with the federal public health response to COVID-19. Importantly, there is no evidence that administration or outside efforts changed FDA decisions on vaccines, hydroxychloroquine, or any other therapies.
by ponchi101 Answer to your question: after my two original boosters, no.
by dryrunguy Here's the latest Situation Report. It starts off with a grim milestone. It also summarizes the basis of the Moderna lawsuit against Pfizer, which is... curious.
::
1 MILLION DEATHS IN 2022 WHO Director-General Dr. Tedros Adhanom Ghebreyesus announced during an August 25 briefing that 1 million people have died with COVID-19 in 2022 thus far. Expressing disappointment in the mortality toll, Dr. Tedros blamed lagging vaccination rates and urged all countries to step up and improve vaccination access worldwide, particularly among high-risk groups. "We cannot say we are learning to live with COVID-19 when 1 million people have died with COVID-19 this year alone, when we are 2 and a half years into the pandemic and have all the tools necessary to prevent these deaths,” he said. According to the WHO, 136 countries failed to reach the June target of vaccinating 70% of their populations. Among those countries, 66 have vaccination coverage below 40% and 10 are below 10%, leaving one-third of the world’s population unvaccinated.
GLOBAL VACCINATION CHALLENGES Global COVID-19 vaccination rates have stalled recently. While 67.6% of the world’s population has received at least one dose of a vaccine—close to the WHO’s recently missed goal of 70% by mid-2022—only 20.9% of people in low-income countries have received at least one dose. A new report by the health consultancy Matahari Global Solutions, with support from the International Treatment Preparedness Coalition and the People’s Vaccine Alliance, examines progress on uptake of and access to COVID-19 tools across 14 nations—Bangladesh, Democratic Republic of the Congo, Haiti, Jamaica, Liberia, Madagascar, Nepal, Nigeria, Perú, Senegal, Somalia (and Somaliland), Uganda, and Ukraine. According to the report, the reasons for slow vaccine uptake in these nations are multifaceted and cannot be blamed solely on skepticism about vaccines, or “vaccine hesitancy,” although it does cite influence from “historical memory of experimentation on Black bodies by white colonizers.” The countries also face a range of challenges that contribute to low uptake, including lack of cold chain storage and healthcare workers, unpredictable supply chains, transportation problems related to deliveries or accessing vaccination centers, and insecurity. The report also outlines inequities in access to other COVID-19 tools such as oxygen, diagnostic tests, and therapeutics and discusses actions still needed to address the current pandemic as well as future health emergencies. Notably, experts from the University of Washington's Institute for Health Metrics and Evaluation (IHME) estimate that thousands of lives could be saved if antivirals to treat COVID-19, such as Paxlovid, were more accessible in low- and middle-income countries.
VACCINE PATENT LAWSUIT Moderna on August 26 filed patent infringement lawsuits in the US and Germany alleging that Pfizer and BioNTech violated 3 patents Moderna filed between 2010 and 2016 on its mRNA technology, foundational in developing the company’s SARS-CoV-2 vaccine, Spikevax. Moderna claims that Pfizer and BioNTech copied that technology without permission to produce their vaccine, Comirnaty. Instead of seeking to remove the Pfizer-BioNTech vaccine from the market, Moderna is seeking monetary damages that could include royalties and lost profits incurred since March 2022, when the company began enforcing patents in wealthier nations after pledging not to do so during the emergency phase of the pandemic. Both Pfizer and BioNTech said the litigation was surprising and they remain confident in the intellectual property supporting their vaccine. Notably, some experts say at least one of the patented inventions Moderna included in the lawsuits was patented by two university scientists 6 years earlier than Moderna’s filing. While the earlier patent could weaken Moderna’s argument, the claim likely will not be completely invalidated. Analysts say the lawsuits point toward Moderna’s efforts to profit from the mRNA platform in future endeavors, including to treat and prevent other infectious diseases, cancers, rare diseases, and autoimmune disorders. The patent battle could drag on for years but is unlikely to impact production of the companies’ vaccines against COVID-19.
ACCESS TO COVID-19 TOOLS Most US residents have been able to access COVID-19 vaccines, treatments, tests, and other tools such as masks for low or no cost, largely because the federal government has purchased and allocated them to states and providers. However, because the US Congress has not moved to authorize additional funding for the pandemic response, the government can no longer buy the products for free or low-cost distribution. This week, the Biden administration announced it will pause its program to mail free at-home rapid COVID-19 tests to residents because “Congress hasn’t provided additional funding to replenish the nation’s stockpile of tests,” according to a statement on the Covid.gov website.
In the face of dwindling supplies and funding-related tradeoffs, the Biden administration is aiming to preserve the existing supply of rapid antigen tests in anticipation of a fall surge in cases. If congressional funding becomes available, the program will quickly resume distribution, according to an unnamed administration official. Free tests will continue to be available to order as long as supplies last or through September 2, whichever comes first. After that, they will be available through 15,000 federally supported community sites, such as libraries and pharmacies, as well as community health clinics. Additionally, individuals can be reimbursed for the cost of tests through private and public health insurers.
With funds running low, the Biden administration is beginning to shift the cost of tests, vaccines, and therapeutics to health insurers and consumers. Experts caution that the impending commercialization of COVID-19 tools must account for systemic barriers that prevent equitable access to them, particularly among uninsured people. Already, programs meant to improve access to and uptake of vaccinations have folded, in some cases due to congressional resistance to authorize more pandemic response funds, just as the US prepares to launch a fall booster campaign with updated vaccines. However, due to a lack of funding, coupled with low demand for vaccination and increasingly relaxed federal guidance on preventive measures, many susceptible populations will continue to face barriers in accessing COVID-19 preventive measures and other healthcare.
VACCINE EFFECTIVENESS AGAINST OMICRON A new analysis in JAMA Network Open provides further support that Pfizer-BioNTech or Moderna booster dose administration following a 2-dose primary series provides protection against severe COVID-19 outcomes caused by the Omicron variant of concern. The cohort study of more than 2.4 million individuals estimated that mRNA booster dose effectiveness against severe COVID-19 during Omicron predominance was 87.4% with no waning up to 6 months after receiving the dose, compared to 69.6% effectiveness against severe COVID-19 following a 3-dose series of inactivated vaccine (ie, Sinovac CoronaVac or Sinopharm COVID-19 vaccines). Data from the US CDC, published August 26 in Morbidity and Mortality Weekly Report (MMWR), similarly emphasized the importance of vaccination, showing that while older Americans above the age of 65 faced greater hospitalization rates during the BA.2 predominant period, unvaccinated individuals had a 3 times greater risk of hospitalization compared to vaccinated individuals.
WASTEWATER SURVEILLANCE Wastewater surveillance is a proven method to track disease outbreaks and has provided an accurate and economical way to provide early detection of COVID-19 levels within communities—and even estimate the number of infected people in a specific area—helping to inform health authorities and policymakers throughout the pandemic. Sewage surveillance also is used to track other diseases, including monkeypox and polio, and experts say building and maintaining the infrastructure to expand wastewater-based disease surveillance should be a public health priority. However, funding for the relatively inexpensive systems is inconsistent, leading to pauses in the disease monitoring that, if continuously and thoroughly conducted, can help communities or entire countries save millions of dollars by quickly responding to disease outbreaks. But many governments, including the US Congress, are reluctant to allocate additional money for wastewater surveillance. In some cases, venture capitalists, nonprofit organizations, or academic institutions are stepping up to fill the gaps. But more funding will be needed to grow wastewater epidemiology to help provide warning signals of future potential disease outbreaks.
CHINA Several of China’s largest cities have imposed full or partial lockdowns amid new COVID-19 outbreaks. The measures impact at least 3 million people in the port city of Dalian and an undisclosed number in Chengde and Shijiazhuang in Hebei province. Though the province surrounds Beijing, the capital city is so far relatively unaffected. Partial lockdowns in other areas of the country are affecting millions more people. Measures include the need to show proof of negative test results within 24 hours to enter residential and public spaces, capacity reductions for public spaces, blanket closures of public entertainment and cultural venues, work-from-home mandates, and limits on the number of people that households may send to shop for daily needs. In many areas, the lockdowns will delay the start of the school year. Amid a heat wave, the workers responsible for enforcing the measures face significant occupational health and safety risks, such as heat stroke and exhaustion exacerbated by wearing bulky protective suits. The latest curbs reflect the government’s insistence of adhering to its “dynamic zero COVID” policy, often criticized for being unsustainable, disrupting the economy, and negatively impacting the mental health of residents, particularly teenagers and young adults.
by ti-amie The first paragraph is so disheartening.
by dryrunguy Life expectancy in the U.S. continues to decline--in large part due to COVID. But there's been a shift from 2020 to 2021. Life expectancy fell the most among Native American and White populations. The year before that, which aligns with the first year of COVID, life expectancy fell the most among Black and Hispanic populations.
by ponchi101 White populations that maybe, just maybe, vote for a certain guy and believe C19 is a hoax and are therefore unvaccinated?
A testable hypothesis.
by dryrunguy Here's the latest Situation Report. It includes an explanation and defense for fast tracking the updated vaccines.
::
EPI UPDATE The WHO COVID-19 Dashboard reports nearly 600 million cumulative cases and 6.47 million deaths worldwide as of August 31. Global weekly incidence decreased for the third consecutive week, down 15% from the previous week. Global weekly mortality decreased for the second consecutive week, down 13% from the previous week.
Regional trends in weekly incidence and mortality also are declining. All regions reported decreases in weekly incidence, ranging from -13% to -36.5% from the previous week. Notably, incidence in the Western Pacific appears to have peaked, with weekly incidence down 15% after a slight increase (+1.6%) the week of August 15. Weekly mortality is declining in all regions except the Western Pacific (+3.5%) and South-East Asia (+15.5%). The Eastern Mediterranean region appears to have peaked, with weekly mortality down 35% over the previous week.
UNITED STATES
The US CDC is reporting 94.3 million cumulative cases of COVID-19 and 1,040,314 deaths. Average daily incidence continues to decline, down from the most recent high of 129,363 new cases per day on July 21 to 88,286 on August 30—the lowest average since May 12. Average daily mortality continues to decline, down to 383 on August 30 from a recent high of 486 on August 12.**
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to decline, down 2.9% and 6.3%, respectively, over the past week. Both trends peaked around the last week of July, similar to trends in daily incidence.
The BA.5 sublineage is projected to account for 88.7% of sequenced specimens in the US. While BA.5 remains the overwhelmingly dominant Omicron subvariant, its growth has reversed as the prevalence of the BA.4.6 sublineage is increasing. BA.4.6 remains the #2 subvariant nationwide, now accounting for 7.5% of sequenced cases, while BA.4 now accounts for 3.6% of cases. It remains unclear whether BA.4.6 is capable of usurping BA.5 nationwide, but it appears to be outpacing BA.5 in certain areas, particularly HHS Region 7 (Iowa, Kansas, Missouri, Nebraska), where it accounts for 17.2% of sequenced cases. Collectively, the remaining variants account for only 0.2% of cases nationally. All variants reported here are sublineages of the Omicron variant of concern (VOC).
PANDEMIC VIGILANCE Senior WHO officials are warning that although the overall numbers of COVID-19 cases and deaths are decreasing globally, those numbers could rise as northern nations head into colder months. WHO Director-General Dr. Tedros Adhanom Ghebreyesus on August 31 urged more people—particularly healthcare workers and older adults—to get vaccinated and stay up to date on vaccinations by getting booster doses, where available; wear masks in crowded indoor spaces; and maximize air flow when possible. Dr. Tedros warned that people must remain vigilant against the virus, even if already vaccinated, saying that pretending the pandemic is over is "a huge risk."
In an interview with STAT News, Dr. Maria Van Kerkhove, the WHO’s Technical Lead for COVID-19, echoed these sentiments. She recognized the world is facing many threats—including flooding, war, famine, and several significant disease outbreaks—and acknowledged a global desire for the COVID-19 pandemic to be over. But, instead of forgetting about the deadly disease, Dr. Van Kerkhove said the international community must optimize its response at this point in the pandemic, when we have the tools, knowledge, and, to some degree, immunity to be in a better position against circulating Omicron subvariants and prepare for those that might come next. She too warned that governments and individuals must remain laser-focused on sustaining the actions, systems, and workforce put in place to address the COVID-19 emergency, as those same systems can be used for other disease threats, which appear to be becoming more common as the climate warms.
US BOOSTER CAMPAIGN The US FDA on August 31 granted emergency use authorization (EUA) for 2 Omicron-specific vaccine boosters, one from Pfizer-BioNTech and one from Moderna. Pfizer-BioNTech’s booster is authorized for people aged 12 years and older, and Moderna’s booster is authorized for adults only. The US CDC's Advisory Committee for Immunization Practices (ACIP) is expected to vote today on recommendations for the boosters, and once CDC Director Dr. Rochelle Walensky gives the final approval, the doses can start to be rolled out to states, likely after the Labor Day holiday. The new bivalent boosters target both the original virus strain and the BA.4/BA.5 subvariants, with the hopes that the shots can provide at least some additional protection against currently dominant subvariants as the nation enters colder months. Notably, under the new EUA, the monovalent mRNA COVID-19 vaccines are not authorized as booster doses for individuals 12 years of age and older. The older boosters will be phased out as the updated boosters become more readily available.
However, public health officials face challenges in rolling out the new boosters, including general pandemic fatigue and low uptake of the current boosters. There is also confusion about who should get these newer boosters, particularly among those who were recently boosted for the first or second time with original vaccine formulations. On this question, experts recommend people wait 3 to 6 months after their last immunization or most recent infection to receive the maximum benefit from the new boosters. Otherwise, recently activated immune systems may neutralize the booster components too quickly for the body to develop immune memory for later protection.
Although some people have expressed concern over the rapid timeline with which the new boosters were developed and authorized, public health officials note that annual flu vaccines are updated in much the same manner. Neither shot completed human trials, but experts maintain that safe, effective vaccine formulations with updated antigen profiles are routinely produced using a fast-track model. Therefore, while the targeted strains of SARS-CoV-2 are different, the manufacturing and safety profiles behind these updated boosters remain the same. Additionally, Dr. Walensky said last week that waiting to conduct those trials could potentially risk authorizing an outdated vaccine and that Omicron-adapted vaccines are necessary to help prevent an expected fall and winter surge. Still, data on the boosters’ ability to prevent hospitalizations and deaths will be collected. Now, public health officials must thoughtfully advocate that individuals, especially those at greatest risk of adverse outcomes, choose to receive the updated boosters, just as many in the US and around the world are growing indifferent to COVID-19 in their communities.
US LIFE EXPECTANCY Life expectancy in the US fell for the second year in a row in 2021, representing the first time life expectancy dropped 2 years in a row in 100 years. The Vital Statistics Rapid Release published by the US CDC provides life expectancy estimates calculated using complete period life tables based on provisional death counts for 2021. Someone born in the US in 2019 had a life expectancy of 79 years. But in 2020, life expectancy fell to 77 years, falling further in 2021 to 76.1 years. Notably, there is a 5.9 year gap in life expectancy between males and females. Life expectancy for males born in 2021 was 73.2 years and 79.1 years for females.
The analysis also provides life expectancies by Hispanic origin and race, where the greatest decline between 2020 and 2021 was for non-Hispanic American Indian and Alaska Native (AIAN) males, whose life expectancy declined from 63.8 to 61.5 years, followed by non-Hispanic AIAN females at 70.7 to 69.2 years. Dr. Robert Anderson, Chief of Mortality Statistics at CDC's National Center for Health Statistics, said the type of loss experienced since 2019 is similar to the decline in US life expectancy after the 1918 influenza pandemic. Asian Americans saw the smallest decline in life expectancy from 2020 at 83.1 years, a decline of 0.1 years, and Black Americans lost 0.7 years. COVID-19 accounts for about half of the decline in life expectancy, while accidents and unintentional injuries, including drug overdoses, account for another 16%. COVID-19’s impact on mortality and morbidity, as well as healthcare systems, likely will continue long after the emergency phase of the pandemic ends, as researchers become more aware of the virus’s lasting health implications.
COMMERCIALIZATION PLANNING On August 30, US health officials announced plans to begin shifting COVID-19 vaccine coverage to the commercial market as soon as January 2023. A blog post by US HHS Assistant Secretary for Preparedness and Response Dawn O’Connell noted that while the US government has supported no-cost access to vaccines and therapeutics since the beginning of the pandemic, the ability to do so always had a limited timeframe. However, the timeline to transition to the private market has been accelerated, as the US Congress has shown continued reluctance to authorize additional funds to purchase more medical countermeasures. Assistant Secretary O’Connell advocated for additional funding in order to support an “orderly wind down” of the federal programs, as well as to ensure equitable distribution and coverage for the under- and uninsured.
After the administration recently announced a pause to a program providing free, at-home testing kits, public health experts expressed concern over reduced coronavirus test accessibility for the uninsured or those who live in more remote areas, and others have highlighted the potential impacts that commercialization will have on global equity. HHS recently convened a group of more than 100 representatives from state and local governments, health care providers and insurers, pharmaceutical companies and vaccine manufacturers, patient advocates, and others to discuss first steps in how to move forward with the commercialization process, and the agency plans to continue partner engagement to better implement and communicate a plan.
VACCINATION AMONG US CHILDREN COVID-19-related hospitalizations among US children reached their second highest peak of the pandemic this summer, lower only than the initial Omicron surge earlier this year. Relaxed restrictions allowing for more socialization played a role, as did the more transmissible BA.5 Omicron subvariant, but experts say low vaccination rates also contributed. About 60% of children aged 12-17 are fully vaccinated, but only 30% of younger children, ages 5-11, have received 2 doses. Notably, the COVID-19 vaccination campaign for the youngest children, ages 6 months to 5 years, is off to a very slow start 10 months after the US FDA authorized the vaccines for use among this age group. As of August 16, only 3.4% of children under age 2 had received their first dose, and 5.7% of those aged 2-4 years had gotten their first shot, a significantly slower pace than among older kids and teens, according to US CDC data. Only about 1% of the these children are fully vaccinated.
Several factors are slowing the rate, including parental hesitation and more limited opportunities for vaccine administration. While the slow pace presents a much longer-term challenge to get this age group vaccinated, some of this trend was by design, with most vaccine doses going to pediatricians and community health centers, with the expectation that parents would look to get their children vaccinated by their healthcare providers in familiar, trusted settings. Federal officials said they hope childhood COVID-19 vaccination rates will rise as more children visit their doctors heading into the fall and winter seasons.
by ti-amie
by ponchi101 So. Loony friend sends Twitter about "NIH has approved the use of ivermectin for treating C19". In tweet, the person says that the NIH people should be tried for murder and crimes because they did not approve it earlier. Of course: "The people that wanted to make money from the vaccines already did. Criminals!" (Paraphrase).
Go online. I find three separate stories (AP, Newsweek, another one I can't recall) debunking the story. In each, they directly quote the same tweet I was sent. They clarify: the NIH has approved ivermectin FOR CLINICAL TRIALS; i.e. you can still test it as a possible treatment, but it is not approved as a treatment.
I send all this info.
I get back: "You did not read what I sent. This is new; it was finally approved".
I send back: "Debunks are from yesterday".
I feel sad.
---0---
I feel that there is no way that we can find a consistent epistemology, one that can lead to clarity. Items like these truly divide us; I like my loony friend but it is so hard to engage when we almost live in two parallel universes in which neither one of us is acceptable in the other's.
by dryrunguy IIRC, ivermectin has been studied in clinical trials for COVID treatment since 2021. What's different now?
by ponchi101 There is no difference. The thing is that these people cannot understand that the NIH CANNOT stop you from testing an innocuous treatment; if you want to continue investigating Vitamin C as an effective treatment for the common cold, you are allowed to. If you have the grant money and want to keep testing Ivermectin, in a controlled trial, the NIH allows you.
They truly do not understand methodology in any sense. It is what makes me sad. They are constantly asking you to be "open minded" and, when you are and test the claim, and debunk it, you are still not receptive. They never think "am I applying the same process myself?".
by ti-amie
by dryrunguy Here's the latest Situation Report. Haven't read it yet. BTW, I was over at the Wellspan Health Campus in Chambersburg, PA this morning. They had a sign by the pharmacy indicating that they have the new Moderna bivalent boosters available. I'm shocked they got them so soon. But in an interesting diversion from usual COVID vaccine practice, these will be administered by appointment only. So either they don't have that many doses available or there may be some provision requiring disclosure (e.g., that the bivalent boosters have not been tested in clinical trials?).
::
EPI UPDATE The WHO COVID-19 Dashboard reports nearly 603.7 million cumulative cases and 6.48 million deaths worldwide as of September 7. Global weekly incidence decreased for the fourth consecutive week, down 11% from the previous week. Global weekly mortality decreased for the third consecutive week, down 10.5% from the previous week.
Regional trends in weekly incidence and mortality also are declining. All regions reported decreases in weekly incidence, ranging from -9% to -29% from the previous week. Weekly mortality is declining in all regions except the Western Pacific (+4.5%) and Africa (+15.6%).
UNITED STATES
The US CDC is reporting 94.8 million cumulative cases of COVID-19 and 1,043,171 deaths. Average daily incidence continues to decline, down to 74,803 on September 6 from 88,286 on August 30—the lowest average since the beginning of May. Average daily mortality continues to decline, down to 336 on September 6 from a recent high of 495 on August 12.**
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to decline, down 6.6% and 7.4%, respectively, over the past week. Both trends peaked around the last week of July, similar to trends in daily incidence.
The BA.5 sublineage is projected to account for 88.6% of sequenced specimens in the US. While BA.5 remains the overwhelmingly dominant Omicron subvariant, the prevalence of the BA.4.6 sublineage is increasing. BA.4.6 remains the #2 subvariant nationwide, now accounting for 8.4% of sequenced cases, while BA.4 now accounts for 2.8% of cases. Collectively, the remaining variants account for only 0.2% of cases nationally. All variants reported here are sublineages of the Omicron variant of concern (VOC).
EMERGENCY SPENDING REQUEST The Biden administration on September 2 asked the US Congress to pass US$47.1 billion in new emergency spending as part of a continuing resolution to keep the government open beyond the end of the 2022 fiscal year on September 30. The request includes US$22.4 billion to address the ongoing COVID-19 pandemic, of which US$18.4 billion would go to the US HHS to purchase vaccines, treatments, and diagnostics and conduct research, and US$4 billion would support the global response. The federal government is running out of money for its COVID-19 efforts ahead of a potential fall surge, and Congress has been reluctant to authorize additional spending, with Republican lawmakers insisting that new funding be offset by budget cuts or come from transfers of unspent, previously approved US$5 trillion in pandemic relief funds. The new request is already facing opposition in Congress.
Last week, the White House Office of Science and Technology Policy (OSTP), in collaboration with other relevant government agencies, released the First Annual Report on Progress Towards Implementation of the American Pandemic Preparedness Plan, detailing the nation’s pandemic preparedness efforts, including areas for investment. Notably, the report calls the COVID-19 emergency a “moderate pandemic,” despite more than 1 million US deaths and nearly 6.5 million worldwide, and urges the US government to “seize the moment” to prepare for the likelihood of future pandemics and increasing frequency of biological threats.
UPDATED VACCINE BOOSTERS Last week, the US CDC recommended the use of updated COVID-19 booster vaccines for US residents over the age of 12 who have completed at least a 2-dose primary vaccination series. The recommendation was given to the Pfizer-BioNTech and Moderna mRNA bivalent vaccine boosters that are adapted to address both the original SARS-CoV-2 strain and the Omicron variant of concern, specifically targeting the BA.4 and BA.5 subvariants. The process the companies’ used to modify their vaccines is similar to that of the annual alteration of influenza vaccines. The nimbleness with which scientists can “plug-and-play” variant-specific components into the mRNA platform allowed the rapid updates. However, some individuals have expressed concern over a lack of human clinical data supporting the booster authorizations.
The bivalent boosters are already available for individuals looking to recharge their immune protection against currently circulating variants ahead of what some officials predict will be a surge of cases this fall and winter. Individuals aged 12 and older are eligible for the new booster at least 2 months after completing their 2-dose primary series or their most recent booster. Anyone who is vaccinated and recently recovered from COVID-19 should wait at least 3 months to get their next shot to maximize their immune response. The new boosters are being offered alongside influenza vaccines, with hopes that immunization coverage will increase for both flu and COVID-19. Countries in the southern hemisphere, including Australia, recently experienced a challenging flu season, prompting health officials to call for increased vaccine coverage before influenza activity increases in the United States. Many top US health officials are suggesting that COVID-19 booster shots will become annual vaccinations, similar to those for influenza. Scientists are still hopeful that future COVID-19 vaccines will enable a more durable immune response, but they also note that the current vaccines provide excellent protection from severe disease.
Internationally, the UK has approved bivalent boosters targeting Omicron BA.1 from both Moderna and Pfizer-BioNTech for individuals aged 12 and older. Notably, the UK Health Security Agency (UKHSA) this week said healthy children between the ages of 5-11 years will no longer be offered vaccination against COVID-19, angering some parents and healthcare providers. The European Union has also backed both the Pfizer-BioNTech and Moderna Omicron BA.1-adapted boosters. With the rollout of the new boosters, questions are being raised about remaining stockpiles of old formulations. US officials are debating whether or how to use remaining doses, with some worrying that millions of doses might be wasted. International donations are under consideration, although officials are worried about depleting national stockpiles and falling global demand for the vaccines.
NEEDLE-FREE VACCINES Many scientists and health organizations, including the WHO, have suggested that vaccines delivered nasally or orally may be a crucial step in controlling COVID-19. While the current COVID-19 vaccines, which are administered via intramuscular injection, have shown prolonged effectiveness at preventing severe disease, they are less effective at limiting disease transmission. Many theorize that vaccines administered through nasal drops or oral inhalation may lead to heighted mucosal immunity, a factor that could prolong immunity.
Leading these efforts, both China and India this week approved new needle-free COVID-19 vaccine candidates. China approved the Convidecia Air vaccine made by CanSino Biologics as a booster dose for those who are already fully vaccinated. The vaccine, which is based on the same adenovirus platform as the company’s injected vaccine, is delivered orally via an inhaled mist produced by a nebulizer. India regulators approved a 2-dose primary series vaccine produced by Bharat Biotech, which is administered as drops in the nose. Neither CanSino nor Bharat Biotech have published clinical trial results on the vaccines in peer-reviewed journals, but in-country regulators used preliminary data for their approvals. It is unclear how successful these vaccines will be at preventing disease, but they are a sign of a potential next step for COVID-19 vaccines.
PAXLOVID REBOUND DATA A letter published September 7 in the New England Journal of Medicine provides new data on the occurrence of viral load rebound among COVID-19 patients taking Paxlovid. The data come from a phase 2/3 double-blind, randomized, controlled clinical trial involving nearly 2,250 unvaccinated individuals who had symptomatic COVID-19 infections and at least one risk factor for severe disease. Results regarding viral load rebound were similar in both the treatment and placebo groups, even after controlling for various factors. For those participants for whom viral load data were available, 2.3% of 990 who received Paxlovid experienced viral load rebound between baseline and 14 days after the start of treatment, and 1.7% of 980 patients in the placebo group had viral load rebound within the same timeframe. According to the researchers, the data reaffirm the effectiveness of Paxlovid at preventing severe disease and death, with little difference in instances of rebound between those who took Paxlovid and those who did not. However, Paxlovid remains out of reach for many people who reside in low- and middle-income countries (LMICs), further increasing global disparities in managing COVID-19 disease.
ANTIBODIES Vaccines against COVID-19 are effective at preventing severe illness and death among most individuals, but new SARS-CoV-2 variants are able to circumvent some immune protection induced by these vaccines, which has necessitated the development of new boosters. Additionally, monoclonal antibody therapies, or mAbs, that worked against earlier variants struggle against current variants. Most recently, data in a preprint study posted to bioXiv show that the 2 mAbs that comprise AstraZeneca’s Evusheld—the only therapeutic antibody combination available to protect immunocompromised people against COVID-19—may be less effective against the BA.4.6 subvariant, which is increasing in prevalence. Increased efforts to keep antibody treatments current and updated are important so that immunocompromised people can access reliable and effective treatments against COVID-19.
Two recent studies point to promising new antibodies that could potentially neutralize all SARS-CoV-2 variants and render boosters unnecessary. In a study published August 5 in Communications Biology, Israeli scientists at Tel Aviv University sequenced B cells from the blood of people who had recovered from COVID-19 in Israel and isolated 2 antibodies, TAU-1109 and TAU-2310, that neutralized 84-90% of the Omicron (B.1.1.529) variant and 90-97% of the Delta variant. These findings were successfully corroborated by researchers at the University of California San Diego and Bar-Ilan University. Researchers noted that monoclonal antibodies that prevent SARS-CoV-2 from binding to ACE2 receptors in human cells—a process that current vaccines target—are more susceptible to viral evolution. The 2 TAU antibodies, named after Tel Aviv University, bind to a different part of the virus’ spike protein than most other mAbs.
In another study, published August 11 in Science Immunology, researchers from Boston Children’s Hospital and Duke University modified a humanized mouse model to develop SP1-77, an antibody that can neutralize all currently known variants of SARS-CoV-2. This model initially was developed to look for antibodies that neutralize HIV, another RNA-based virus that mutates often. Instead of blocking SARS-CoV-2 from binding to ACE2 receptors in human cells, the SP1-77 antibody blocks the virus from fusing its outer membrane with human cell membranes. Though this work is in an early proof-of-concept stage, the researchers have applied for a patent for the SP1-77 antibody and mouse model used to create it.
LONG COVID/PASC Myriad questions remain over the long-term health implications of SARS-CoV-2 infection, with an estimated 16 million US residents of working age experiencing symptoms of COVID-19 lasting 4 or more weeks beyond acute infection—a condition often called post-acute sequelae of SARS-CoV-2 (PASC) or long COVID. An ad hoc collaboration of healthcare providers from at least 40 long COVID clinics are trying to fill the knowledge gaps, meeting regularly to compare their experiences treating patients who are often frustrated, and sometimes anxious and depressed, with being dismissed by primary care and specialist providers. The American Academy of Physical Medicine and Rehabilitation collaborative is concerned both the public and the Biden administration are losing focus on the pandemic and its potential long-term impacts. The Biden administration has published 2 reports on long COVID, and congressional lawmakers have introduced several bills on the issue, but until more money, research, guidance, and education is available for those treating the condition, healthcare providers worry the lack of attention will further expose the fragility of the nation’s healthcare system and cases will go undertreated or undiagnosed, particularly in underserved communities.
Few risk factors for long COVID have been identified, although many studies suggest conditions such as immunosuppression, hypertension, obesity or older age are associated with a higher risk of severe outcomes. A new study published September 7 in JAMA Psychiatry suggests that psychological distress prior to infection may be a risk factor for post-COVID-19 conditions. The prospective observational cohort study included nearly 55,000 survey respondents, mostly White and female, and examined whether pre-infection psychological distress early in the pandemic—such as depression, anxiety, loneliness, perceived stress, and worry—was associated with an increased likelihood of developing post-COVID-19 conditions among individuals who were later infected with SARS-CoV-2. The researchers found that all types of distress were significantly associated with an increased risk of long-lasting COVID-19 symptoms, even after adjusting for various demographic and health factors. The relationship was dose-dependent, meaning individuals who reported more types of distress were at higher risk of developing long COVID. The authors emphasized that the findings should not be taken to mean long COVID symptoms are psychological and suggested future research should look at biobehavioral mechanisms linking psychological distress with persistent symptoms.
ORPHANHOOD & CAREGIVER LOSS The COVID-19 pandemic has taken a significant toll on children, many of whom have lost parents and caregivers as a result of COVID-19-related mortality. A research letter published September 6 in JAMA Pediatrics analyzed excess COVID-19-related deaths, estimating that 10.5 million children lost their parents or caregivers to COVID-19 and 7.5 million children experienced orphanhood between January 1, 2020, and May 1, 2022. This is nearly double previous estimates. The study also concluded that the highest amount of orphanhood by primary and/or secondary caregiver loss was found in Southeast Asia (40.6%) and Africa (24.3%). The Imperial College London’s COVID-19 Orphanhood Calculator is updated daily to provide national, regional, and global estimates of children who have lost a parent or caregiver.
There has been a greater push to address the associated economic, social, mental, and health-related consequences that orphanhood and caregiver loss can have on children, particularly as a result of COVID-19-related mortality. In the regions most affected by parent and caregiver loss, aid workers have noticed an increase in issues like child trafficking, early marriage, and exploitative labor practices involving children. The study’s authors recommend the following to mitigate the toll of parent and caregiver loss on children: accelerating vaccination, containment, and treatment efforts to prevent caregiver loss; preparing families to provide safe and nurturing alternative care; and bolstering economic support, violence prevention, parenting support, and school access initiatives. Others recommend funding support programs, such as providing conditional cash transfers to families to ensure that bereaved children continue going to school and remain connected to community resources. Many experts recommend turning to previous research of children who experienced parent and caregiver loss due to the HIV/AIDS epidemic to help identify meaningful solutions.
The United States is one of few countries to have made national commitments to address parent and caregiver loss; the White House released a memorandum in April 2022 promising that families affected by parent and caregiver loss would be able to access necessary support programs and resources. However, there have been no federal efforts to address the needs of children who have lost parents and caregivers as a result of COVID-19.
PANDEMIC LOCKDOWNS Most researchers agree that the rapid onset of the COVID-19 pandemic gave governments little option but to restrict their population’s interactions in early 2020, and those lockdowns likely helped to curb related deaths. But the restrictions had clear costs, including losses in educational gains, and debate remains over the usefulness of lockdown measures implemented after the outbreak’s initial phase. Now, much of the cost-benefit analyses involve value judgments, making lockdowns difficult to study and leading to disagreements. In China, which continues to enforce its “dynamic zero COVID” policies with what is beginning to appear as endless cycles of strict lockdowns and testing measures, experts agree that the restrictions likely will lead to long-lasting political, economic, and social consequences. The country’s leadership seems committed to these highly disruptive methods in an attempt to eradicate COVID-19, while the rest of the world is learning to live with the novel virus. Currently, nearly every Chinese province has recorded infections in recent days, and more than 300 million residents have been placed under partial or full lockdown since the end of August, some indefinitely. These recent actions have left China’s residents scared, frustrated, and feeling helpless.
by Deuce So... the U.S. gets the vaccine that targets Omicron BA.4 and BA.5 - which are the variants currently infecting people... and Canada (and Europe) only get the vaccine which targets BA.1, which was circulating at the end of last winter before being replaced by BA.4 and BA.5.
Why?
What are we waiting for?
It seems that the vaccine targeting BA.1 is not much different than the original COVID-19 vaccines when it comes to taking on BA.4 and BA.5. So it's merely a move sideways, not an advancement. Why bother?
by JazzNU A childhood friend of my mom's passed away last week from covid pneumonia after a few weeks of ups and downs in the ICU. And she was vaccinated. So just a reminder that covid is still around, still kills, and it's not just stats in a news story.
We're well over 2 years into this, so not saying you shouldn't go about your life the way you see fit (within reason), but do hope you are respectful of those that are still scared, and don't make anyone feel uncomfortable that takes more precautions than others.
by dryrunguy Here's the latest. I skimmed it very quickly. Lots of interesting and lots of depressing stuff here.
::
US RESPONSE As the COVID-19 pandemic enters its third fall in the US, the White House has signaled it plans to slowly restructure its response efforts, including the phaseout of the White House COVID-19 Response Team mid-2023. With dwindling federal funds, responsibility for vaccinations and therapeutics is shifting to private industry and consumers within the next 6 months. Any remaining funds are largely being used for vaccination campaigns promoting this fall’s updated boosters and the purchase of at-home, rapid tests for the Strategic National Stockpile and Test-to-Treat locations. Officials are tentatively hopeful that the national public health emergency declaration for the pandemic may be allowed to expire in early 2023. While part of this transition can be attributed to fewer COVID-19 cases, deaths, and related hospitalizations, as well as the widespread availability of vaccinations and therapeutics, most response activities need to wind down due to a lack of new funding from the US Congress. Experts and officials emphasize that the pandemic is far from over, with COVID-19 on track to remain the third leading cause of death in the nation.
At the state level, New York Governor Kathy Hochul allowed the COVID-19 state disaster emergency declaration to expire last night, leaving only 10 states with emergency orders in place—California, Connecticut, Delaware, Illinois, Kansas, New Mexico, Rhode Island, Texas, West Virginia, and Washington. The 10 states with the lowest vaccination rates in the country (Wyoming, Alabama, Mississippi, Louisiana, Idaho, Tennessee, Arkansas, Georgia, North Dakota, Indiana) have yet to vaccinate 60% of their populations with the 2-dose primary series, far below the nationwide total of 67.6% and evidence that an updated booster may have a limited impact in the face of continued unwillingness to get vaccinated.
US WORKFORCE According to a recent Gallup poll, one-third of adults are concerned about COVID-19 exposure in the workplace, a proportion that is relatively unchanged since November 2021. The percentage of people “not concerned at all” has increased from 23% in 2020 to a record high of 39%. The recent survey also shows significant gaps in results by gender—41% of working women are concerned about on-the-job exposure compared with 26% of working men—and political party affiliation—51% of Democrats expressed at least moderate concern compared with 14% of Republicans. Two-thirds of workers said they expect new COVID-19 cases to increase during the colder months, although the poll was conducted prior to the approval of updated booster doses.
Additionally, recent research conducted by economists from Stanford University and Massachusetts Institute of Technology estimates that the labor force shrunk by about 500,000 people due to COVID-19 illness. Millions of people left the workforce for various reasons, including lack of childcare, fear of COVID, and retirement. But this research examines the direct impact of COVID-19 illness, estimating that workers with week-long COVID-19-related work absences are 7 percentage points less likely to be in the labor force one year later compared to otherwise-similar workers who do not miss a week of work for health reasons. In August, the total size of the labor force reached 164.7 million people, exceeding prepandemic levels for the first time. However, workforce recovery is experiencing slow-growth compared to prepandemic numbers, and economic recovery will depend on an expanded workforce in the long term.
BRAIN FOG When the COVID-19 pandemic first began, brain fog was not included in the list of possible symptoms. However, many COVID-19 patients report experiencing the condition, both during acute infection and lasting 3 or more months after recovery. Brain fog symptoms appear to be independent of initial disease severity. According to one review of multiple studies, about 22% of individuals report cognitive impairment 12 or more weeks following their initial diagnosis. Brain fog is often described as a disorder of executive function, the set of abilities that includes holding attention, remembering and recalling information, and blocking out distractions. Cognitive tasks that once seemed simple become excruciatingly difficult, and in some cases, impossible. Some people have had to leave their jobs due to an inability to perform their tasks, and many have faced frustration in obtaining medical care, often being dismissed as having anxiety or depression. Complicating the matter is that few clinicians are aware that many viral infections, not only COVID-19, can lead to brain fog and there are few reliable diagnostic tools.
Other neurological complications have been reported following COVID-19 infection, including stroke, delirium, and encephalitis. A recent study published in the journal Brain showed that patients hospitalized with COVID-19 had elevated levels of sera markers of brain injury, neurofilament light (NfL) and glial fibrillary acidic protein (GFAP). However, no specific pathogenic mechanism was determined responsible. Researchers continue to investigate what leads to brain fog—with possible causes including neuro-inflammation, autoimmune responses, or microclots that inhibit blood flow, and therefore oxygen supply—and are hopeful treatments can be developed.
GENETIC MUTATIONS For years, scientists have known that specific genetic mutations can make certain people less susceptible to infection with HIV, norovirus, or the parasite that causes malaria. Now, scientists worldwide are searching for similar mutations or immune system variations that might explain why some people with known exposures to COVID-19 either never become infected or never show symptoms of SARS-CoV-2 infection. The hope is that if researchers can identify a genetic or immune response explanation for resistance, they can use that knowledge to manufacture treatments or vaccines, which possibly could provide cross-protection from other coronaviruses in the future.
EUROPEAN BOOSTER AUTHORIZATIONS Following recommendations made earlier this month by the European Medicines Agency (EMA), the European Commission (EC) on September 12 approved the expanded conditional marketing authorization (CMA) of the Novavax COVID-19 vaccine, marketed as Nuvaxovid, in the EU as a homologous and heterologous booster for adults aged 18 and older. The protein-based vaccine is now available as a primary series or booster in EU Member States, Japan, Australia, and New Zealand, and is under review in other markets, including as a booster in the US. Only 4,872 people in the US have received the first 2 doses of the Novavax vaccine, which some officials hoped would entice unvaccinated individuals to get vaccinated because of its more traditional protein-based platform.
Also on September 12, the EMA recommended authorizing Pfizer-BioNTech’s adapted bivalent vaccine targeting the wild-type spike protein of SARS-CoV-2 and spike proteins of the Omicron BA.4 and BA.5 subvariants. The EC accepted the recommendation the same day, making the booster doses available for immediate shipment to EU Member States. Earlier this month, the EU authorized both Pfizer-BioNTech’s and Moderna’s bivalent vaccine boosters targeting Omicron BA.1.
CHINA As Chinese President Xi Jinping prepares to leave his country for the first time since the COVID-19 pandemic began in early 2020 to meet with Russian President Vladimir Putin, tens of millions of people in China remain under weeks-long lockdowns as part of the nation’s continued “dynamic zero COVID” strategy. President Xi is expected to seek an unprecedented third term as the nation’s leader, and observers say the lockdowns likely will continue at least through the 20th National Chinese Communist Party Congress set to begin October 16. Experts say President Xi likely does not want any uncontrollable rise in COVID-19 cases until after his next term is secured. However, residents in several cities are warning they are running out of food, have limited to no access to medicines and health supplies, and are suffering from psychological and economic impacts. Experts say the government’s insistence on its zero COVID policy exposes the politics behind the measures, with President Xi taking credit for its apparent success in preventing potentially millions of COVID-19 cases. But growing discontent among the nation’s population, as well as economic harms, raise questions about how long the policies can remain in place.
WESTERN PACIFIC REGION New Zealand dropped many of its COVID-19-related requirements on September 12, bringing an end to some of the most restrictive pandemic mandates in the world. People will no longer be required to wear masks in public places, except healthcare and long-term care facilities; all government-imposed vaccine mandates will end on September 26; and only people with COVID-19, and not their household contacts, will be required to isolate for 7 days. Additionally, the government will no longer require vaccinations for incoming travelers and air crew. New Zealand experienced its worst COVID-19 surge this year when Omicron killed more residents than any other pandemic surge. A total of 1,950 people have died of COVID-19 in New Zealand since March 2020. But the average number of new cases and hospitalizations are down significantly since the beginning of August, when influenza cases also surged. Prime Minister Jacinda Ardern said it is time for Kiwis to “take back control” of the future and thanked the population for its cooperation and endurance throughout the pandemic.
In neighboring Australia, federal health officials accepted a recommendation from the Australian Technical Advisory Group on Immunisation (ATAGI) to approve a bivalent vaccine booster from Moderna targeting the original SARS-CoV-2 strain and the Omicron BA.1 subvariant. The booster, which will be available for people aged 18 years and older, is the first bivalent shot cleared for use in Australia. Additionally, state and territorial health ministers moved this week to begin reporting weekly, instead of daily, COVID-19 metrics, including case numbers, new and total deaths, vaccination rates, and breakdowns of hospitalized ICU and ventilated patients.
In Japan, the government signaled its plans to further ease border restrictions aimed at curbing the spread of COVID-19 by waiving tourist visa requirements from some countries and possibly ditching a daily cap on foreign arrivals by next month.
In the Philippines, President Ferdinand Marcos Jr. this week extended the national state of calamity first declared by former President Rodrigo Duterte in March 2020, primarily to allow continued emergency purchases and provide hazard allowances for healthcare workers. While indoor masking requirements will stay in effect, masking rules for outdoor spaces were immediately lifted, except for crowded places where physical distancing is difficult. The nation reopened schools 3 weeks ago, ending one of the world’s longest pandemic-related school system shutdown.
In other Western Pacific nations, public health officials are warning of the possibility of “twindemics,” a rise of another infectious disease during the COVID-19 pandemic. In South Korea, experts are concerned over simultaneous outbreaks of COVID-19 and influenza during the colder fall and winter months, calling for the development of better diagnostic tests, including one that could detect flu and COVID-19 at the same time, and for healthcare services to offer individuals both vaccines during the same visit. In Vietnam, a severe outbreak of dengue fever is overwhelming healthcare facilities that also must treat COVID-19 patients. Experts say that 2 years of pandemic-related lockdowns caused a reduction in routine mosquito vector surveillance and slowed dengue control. The Philippines, Malaysia, and Singapore have also reported year-on-year increase in the number of reported dengue cases.
by ti-amie I read something yesterday describing what it's like to suffer from Long Covid brain fog. It's horrible.
by ponchi101 I am sure I have been exposed to C19, and yet have never caught it. So, where do I sign for this plan to check for genetic mutations that provide immunity?
Ah, right. I live here...
---0---
The brain fog thing sounds very frightening/interesting. It sounds as if it is truly something that changes your life, forever, and for worse. How do you test for it properly, to ensure that when treatments are developed (hopefully) you can get them?
by ti-amie Ed Yong
I wrote about “brain fog”—one of the most common & disabling symptoms of long COVID (and many other pre-pandemic conditions), and one of the most misunderstood.
First, what it’s not: Brain fog isn't anxiety, or depression. It’s not psychosomatic. It’s really nothing like a hangover, stress, or tiredness, and comments equating it to those things—“hey we all forget stuff”—trivialize what people are going through. 2/
Despite the name, brain fog isn’t a nebulous umbrella term. It’s a disorder of executive function—the mental skills that inc. focusing attention, holding info in mind, & blocking distractors. Without that foundation, one's cognitive edifice collapses. 3/
That’s why people w/ brain fog struggle with concentration, multitasking, & planning—which underlie almost everything. It raises unconscious activities to the level of effortful consciousness, and makes easy tasks absurdly hard. 4/
Executive function problems also affect memory: The brain can’t effectively focus on what to store or retrieve that info. Many long-haulers feel like they lose parts of themselves. Hannah Davis told me: “It feels like I'm a void & I’m living in a void.” 5/
There’s a spectrum. Most people improve & can function normally—but below their old baseline and with MANY accommodations. Some have been sick since the pandemic’s start (900+ days). Others got brain fog from pre-covid illnesses decades ago. 6/
Brain fog isn’t unique to long COVID. The same specific problems affect many HIV patients, epileptics post-seizures, cancer patients w/ chemo brain & folks w/ chronic illnesses like ME/CFS. Many of these conditions have long been stigmatized & neglected 7/
Some people argue that the colloquial term ‘brain fog’ delegitimizes and trivializes the condition. But disability communities have used it for decades; there are many reasons why it & its associated conditions are neglected, the name least among them. 8/
E.g. Most research/teaching about cognitive impairment centers around degenerative diseases of elderly people; docs largely don’t learn about viruses causing neurological problems in young people, and hubris leads to discounting of patient experiences. 9/
Also people w/ brain fog are also good at hiding it—it’s intermittent and they just don’t see people on the worst days. Stigma also motivates them to present as normal in social situations or doctors’ appts, furthering the false idea that they’re fine. 10/
Many docs also use inappropriate tests—like MoCA, which was only validated for elderly people with dementia—that even people with severe brain fog can ace. Hence: more dismissal. Bad testing is a comorbidity of long COVID. 11/
And yet brain-scan studies, blood flow studies, immunological studies, & more all point to physical & chemical changes in the nervous systems of people who have brain fog. It’s a real neurological problem that brings real cognitive impairments. 12/
Also, the basic science and the patients’ experiences *cohere*. The possible mechanisms for why brain fog occurs—as detailed in this piece—make total sense of why it affects executive function, why thinking feels slugging, why the fog waxes and wanes. 13/
Based on those likely mechanisms, many of the scientists I spoke to were also hopeful that brain fog is reversible. It just needs a lot more research, of the kind that hasn’t happened thus far. That’ll take time, and for now, people need help. 14/
Most of the approaches to treating brain fog are about managing symptoms. And that can do a lot. Several people I spoke to can work and do normal things again—but more slowly, at higher cost, with a ton of lifehacks & recovery periods. 15/
The single most important advice I've heard from clinicians & patients: You. Have. To. Pace. Yourself. Because brain fog often goes hand in hand with postexertional malaise—where people crash severely after even minor physical OR MENTAL exertion. 16/
I cannot stress this enough: For most people with brain fog, exercise—and strenuous mental activity counts, because cognitive work IS physical work—is a completely inappropriate treatment, and could make them substantially worse. 17/
I hope this piece makes those of you who have experienced brain fog feel seen. I hope it shows everyone else what it really means. Thanks to everyone who talked to me for this story. 18/
Finally, a very common thing that people with brain fog tell me is that they find it very hard to read. This is an almost 3000 word piece. I’m trying to get an audio version put together, and am told it will happen. More on that when I know more. 19/
PS. I'm spending as little time on Twitter as possible so won't get to read the replies to this thread. But for the many of you sharing brain fog experiences, I'm sorry. I hope this story helps a little, if only to make it easier to explain to others. And now, logging off again.
by ti-amie I had the sense to bookmark the above aggregation by @threadreaderapp.
by MJ2004US criticised for rolling out Covid boosters without human trials
Some health experts say vaccination campaign risks undermining public trust
Health experts have warned that the US decision to roll out new coronavirus boosters without clinical testing on humans risks denting public trust and increasing hesitancy about vaccines.
The Joe Biden administration is using the bivalent boosters, which contain the original Covid-19 strain and the genetic code of the Omicron sub-variants BA.4 and BA.5, to vaccinate more Americans against the virus.
It has bought 171mn doses of the BioNTech/Pfizer and Moderna boosters for $5bn and fast-tracked their authorisation before human trials are complete, hoping that they provide better protection against the dominant variants than existing Covid vaccines.
As doses began arriving at pharmacists for distribution this week, US officials said the rollout marked an “important milestone”. In future people would probably only require annual boosters just as they take a yearly influenza jab, they said.
But several health experts said that the boosters have yielded only limited data from a small number of tests on mice. They said there is no evidence that they provide better protection against infection or severe disease than existing jabs.
“Without the data and getting a human response in at least a limited number of people, you just set it up for the anti-vaxxers, anti-science [people],” said Eric Topol, founder and director of the Scripps Research Translational Institute.
“There are already groups calling it the mouse vaccine . . . We already have a trust problem in this country and we don’t need to make it worse,” he said.
Last month, the UK became the first country to approve a bivalent booster. But it waited for clinical data to greenlight a shot targeting the original Covid strain and the BA.1 sub-variant, which has since been superseded by BA.4/BA.5.
On Monday, Pfizer and BioNTech said the European Medicines Agency had recommended the BA.4/BA.5 bivalent booster for conditional marketing authorisation based on data from the companies’ bivalent jab targeting BA.1 and pre-clinical data.
Both companies said the European Commission would review the EMA recommendation and make a final decision soon.
Experts say vaccine hesitancy is just one of several challenges facing the US booster campaign and have urged caution in prematurely declaring victory over the virus.
Two and a half years into the pandemic there is growing public complacency towards Covid, as most people have already contracted the virus and been vaccinated. The Biden administration has also failed to secure $22.4bn additional funding from Congress, which could restrict its ability to replenish vaccine supplies.
“People have booster fatigue. They feel by this stage they are mostly protected and the pandemic is largely behind them: so I think there will be less interest in these boosters,” said Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia.
Offit was one of two members of a US Food and Drug Administration advisory panel to vote against asking Pfizer and Moderna to develop the bivalent vaccine without clinical data showing it performed better than the existing Covid jab.
“What bothers me in this is that we’re willing to move forward with a vaccine with no human data? I just think that’s a lot to ask people,” he told the Financial Times.
Vaccination and booster rates in the US already lag other developed countries with two-thirds of Americans receiving two Covid jabs and only a third of the population boosted. The comparable figures in France are 83 per cent and 65 per cent.
Health experts say the modest vaccination rate in the US is one of the main reasons it has recorded more deaths from Covid than any other country — 1.04mn. The virus continues to kill about 350 people per day, according to the Centers for Disease Control and Prevention, and yet the number of Americans seeking boosters has fallen sharply this year.
Authorities say the threat posed by waning immunity from vaccination and the potential for a fresh wave of infections in autumn justify its decision to roll out bivalent boosters without clinical data.
They argue that by tailoring the jab to target BA.4/BA.5, sub-variants that account for more than 90 per cent of infections, as well as the original Covid strain, it should boost immunity and do a better job in blocking infections. The vaccine is so similar to the existing Covid jab and a separate bivalent jab targeting the BA.1 variant, which has undergone trials, there is no need to wait for results in ongoing human trials, they say.
Some scientists agree, noting that new clinical data are not always required when the influenza jab is tweaked annually to target the latest strains.
Nancy Jecker, professor at University of Washington School of Medicine, said the risk of approving the boosters was minimal given they are not significantly different to the original Covid jabs.
“Emergency authorising Moderna and Pfizer boosters based on animal studies gives people the chance to minimise their risk of Covid as more people congregate indoors during fall and winter months,” said Jecker.
But Topol and Offit argued the US should have waited for evidence the boosters are better than the existing jabs.
“I don’t think they have proven that this influenza vaccine strategy — where we pick influenza strains every March for a vaccine that comes out in September — makes sense for Covid,” said Offit.
He said there is no evidence showing the BA.4/BA.5 booster provided better protection than existing jabs. Initial clinical data for the BA.1 bivalent booster showed it produced virus-fighting antibody levels that were 1.5 to 1.75 times higher than the existing jab, which was not a clinically significant difference, Offit said.
The CDC cites polling which suggests 72 per cent of respondents would definitely or probably receive bivalent boosters. If uptake of the jabs reach similar levels to the annual flu vaccine — half of US adults — by early autumn CDC modelling predicts it would prevent 100,000 hospitalisations, save 9,000 lives and billions of dollars in healthcare costs.
To boost uptake the CDC has simplified its guidance on eligibility, recommending a single bivalent booster for everyone over 12 years of age who has already received a Covid vaccine.
But workers on the frontline of the inoculation drive are sceptical the public will rush to get another jab.
“I think demand will continue to be sporadic because those people who want to be vaccinated have already got the vaccine and been boosted,” said Rene Rodriguez, owner of Tens Pharmacy in Roseland, a small town in New Jersey.
“There are really two types of people: those who believe in the vaccine, who are generally up to date with their jabs, and those that don’t.”
We're trying to decide when we should get this new booster shot. We had the first booster November last year, so we're not sure if we should get it quickly since it's been ten months, or it's better to wait until Nov again to be freshly boosted before the holiday season/winter travels.
There's very little guidance on the question of when people should be getting boosted.
We're trying to decide when we should get this new booster shot. We had the first booster November last year, so we're not sure if we should get it quickly since it's been ten months, or it's better to wait until Nov again to be freshly boosted before the holiday season/winter travels.
There's very little guidance on the question of when people should be getting boosted.
I've begun timing my boosters to correspond with the time of year and the greater prevalence of COVID in the general community. I got my first booster in January of this year, and my second at the beginning of June so that I could get my next one in November, which is when people are indoors more because of the colder weather, and so more people will be contracting COVID. Here, the suggestion is to get the boosters spaced 5 or 6 months apart.
For the article above, the link requires a subscription. Of course, the entire article is posted above - but for those who want a link to possibly pass onto others, here is one...
MJ2004 wrote: ↑Wed Sep 14, 2022 12:04 amUS criticised for rolling out Covid boosters without human trials
Some health experts say vaccination campaign risks undermining public trust
Health experts have warned that the US decision to roll out new coronavirus boosters without clinical testing on humans risks denting public trust and increasing hesitancy about vaccines.
...
If the slightest thing goes wrong with this booster (a runny nose, 3 hours of hiccups, anything) not only it will be used by anti-vaxxers for their agenda. It will blow a huge hole in any trust in medical science, which is already questioned constantly by all the "alternative" medicine quacks and followers.
It is very risky. You know they cling to any little bit of anecdotal data to sink the entire effort: "I heard that a friend of a cousin of the front man in the apartment next door to the one where my former girlfriend's aunt lives turn into a lizard after he got his booster. I AM NOT GETTING IT".
I agree that it should not have been rolled out so easily.
by dryrunguy Speaking of brain fog... My former anti-vax boss who is now basically my corporate equal has screwed up three proposal submissions in the past 2 weeks since she "recovered" from COVID. And when I look at the errors she made along the way, trust me when I say that all three errors could conceivably be attributed to brain fog. As in, "I never got that email with the business proposal"/"No one ever sent me the file for submission"... But she actually did receive it, and the files actually were sent to her.
Maybe it could be attributed to too many emails (she has a lot of work on her plate)--and important stuff just got buried in Outlook. That's possible. But still... You have to wonder.
She has since been stripped of all proposal submission responsibilities.
EPI UPDATE The WHO COVID-19 Dashboard reports 607 million cumulative cases and 6.50 million deaths worldwide as of September 14. Global weekly incidence continues to decline, for the fifth consecutive week—down 25% from the previous week. Global weekly mortality decreased as well, for the fourth consecutive week—down 19% from the previous week.
Weekly incidence continues to decline in all WHO regions, ranging from -5% in Europe to -36% in the Western Pacific region. Notably, the pace of the decreasing trend in Europe appears to be slowing, and the region may be approaching a local minimum or plateau.
UNITED STATES
The US CDC is reporting 95.2 million cumulative cases of COVID-19 and 1,046,195 deaths. Daily incidence continues to decline, down to 60,558 new cases per day. This is the lowest average since May 1 and a 54% decrease from the most recent peak on July 16. Daily mortality continues to decline as well, down to 350 deaths per day. This is the lowest average since July 9 and a decrease of 30% from the most recent high on August 12. The CDC reported a slight increase in both daily incidence and mortality on September 12, but this is likely due to delayed reporting over the US Labor Day holiday weekend.*
*Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to exhibit downward trends, with decreases of 6.5% and 5.4%, respectively, over the past week. Both trends peaked around the last week of July, similar to trends in daily incidence, and both are approximately 80% lower than the record peak in mid-January 2022.
The BA.5 sublineage continues as the dominant strain in the US, accounting for 87.5% of sequenced specimens; however, growing evidence indicates that BA.4.6 might be capable of outcompeting it. The prevalence of BA.4.6 has steadily increased since at least mid-summer 2022, but the BA.5 prevalence increased more rapidly over much of that period. This is the first week that the CDC’s Nowcast projection shows a noticeable decrease in BA.5 prevalence**, while BA.4.6 continues to account for a larger share of US cases. Since last week, the BA.4.6 prevalence increased from 8.3% to 9.2%, while the prevalence of BA.5 fell slightly from 87.9% to 87.5%. The prevalence of all other reported lineages continues to decline, and together, the Omicron sublineages account for essentially all new US cases.
**From the week of August 27 to the week of September 3, the BA.5 prevalence decreased from 88.0% to 87.9%, but we interpret this as essentially remaining constant over that period.
PANDEMIC RESPONSE EVALUATIONS As daily COVID-19 incidence and mortality continue to decline globally, attention is shifting to pandemic recovery efforts, including lessons for future pandemic preparedness and response. In a long-awaited report published September 14, The Lancet COVID-19 Commission described the tremendous pandemic death toll as “both a profound tragedy and a massive global failure at multiple levels,” underlined by an absence of international cooperation, dismissal of risks by national leaders, influence of misinformation, paucity of governmental and organizational transparency, and disregard for basic public health precautions. As a result, COVID-19 impacted countries in “highly unequal” ways, with particularly severe outcomes for the most vulnerable populations, including children, immigrants and refugees, and those in low- and middle-income countries (LMICs). Additionally, a substantial portion of COVID-19 survivors continue to experience prolonged health effects stemming from SARS-CoV-2 infection, and many people are dealing with the impact of COVID-19-related deaths among family and friends. The report cites the rapid development of vaccines as a positive example of international cooperation, but it also acknowledges substantial disparities in vaccination coverage at the national level, particularly between LMICs and higher-income countries. The report also calls attention to downstream and longer-term effects of the pandemic, including setbacks in progress toward achieving Sustainable Development Goals (SDGs) in many countries.
The report—produced by a panel of 28 experts who consulted more than 170 contributors through 12 task forces—makes several recommendations falling under 5 pillars: prevention, containment, health services, equity, and global innovation. The recommendations include improving multilateral cooperation; implementing a “vaccination-plus” strategy that combines vaccination with other medical countermeasures (MCMs) and nonpharmaceutical interventions (NPIs); improving surveillance and prevention for natural and accidental spillover events; expanding international research and development and manufacturing capacity for vaccines and other products; establishing sustainable financial support for LMICs; and strengthening the WHO and national health systems. The report also calls for intensifying efforts to identify the origins of SARS-CoV-2, noting that the task force examining the pandemic’s origins was ended because “the divisive public discussion about the source of SARS-CoV-2 damaged the trust needed for the task force to complete its work.”
The report has already met pushback from some experts and organizations, including the WHO. The WHO issued a statement in response to criticisms that it acted too cautiously and sluggishly, both to declare a public health emergency of international concern (PHEIC) and warn of the potential for airborne/aerosol transmission. The WHO emphasized that it welcomes the report’s overarching recommendations but argued that there are “several key omissions and misinterpretations,” particularly related to the speed with which the WHO responded to the initial outbreak. Additionally, several experts criticized the report for reviving debate about the virus’ origins and for omitting recent relevant evidence that the novel coronavirus likely emerged through a zoonotic event in a market in Wuhan, China. Notably, the commission’s Chair, Dr. Jeffrey Sachs, has publicly supported the “lab leak” theory as the origin of the virus, and some contest that his personal beliefs unduly influenced the commission’s findings.
Earlier on September 14, WHO Director-General Dr. Tedros Adhanom Ghebreyesus told journalists during his weekly briefing that the world has “never been in a better position to end the pandemic” but is “not there yet.” He called on the international community to “seize this opportunity” and announced the release of 6 WHO policy briefs that outline essential actions for national and subnational policymakers to help reach the goal of ending the pandemic. The briefs include guidance for testing, vaccination, clinical disease management, healthcare facility infection control, combating misinformation, and community engagement. Following those comments, Africa CDC Acting Director Dr. Ahmed Ogwell Ouma emphasized that low vaccination coverage and ongoing transmission across the continent illustrate that COVID-19 remains a major threat.
In related news, an investigation published today by POLITICO and the German newspaper WELT examines the influence of several entities in the COVID-19 pandemic response, including the Bill & Melinda Gates Foundation; the Wellcome Trust; Gavi, the Vaccine Alliance; and the Coalition for Epidemic Preparedness Innovations (CEPI). The investigation concludes that the organizations were better prepared than governments for an infectious disease outbreak; the groups’ leaders were able to routinely meet with high-level government and multilateral organization leaders; they pledged billions of dollars to help close equity gaps for vaccines and treatments but hoarding by high-income nations got in the way; and their initial lack of support for intellectual property waivers might have impeded access to vaccines and therapeutics in LMICs. Several experts have criticized the report for being shortsighted and naïve, including by undervaluing public-private partnerships in pandemic responses and misrepresenting CEPI and Gavi—both financial intermediary funds (FIFs) under the World Bank—as nongovernmental organizations.
US GLOBAL RESPONSE & RECOVERY The Biden administration today released an updated version of its US COVID-19 Global Response & Recovery Framework, meant to help guide the US commitment to a globally equitable end to the emergency phase of the pandemic by working with international partners to use available tools and expertise, integrating COVID-19 response elements into existing health structures, and improving global pandemic preparedness. The plan outlines 3 primary objectives to achieve those goals: vaccinating those who are at highest risk and the hardest-to-reach by ensuring access to vaccines and integrating vaccinations into existing health structures; integrating and scaling testing and treatment efforts into existing health structures without disrupting other health services; and preparing for future variants and pandemic threats by strengthening health security infrastructure to detect and rapidly respond to emerging threats. The updated global framework comes at a time when the US is facing domestic pandemic fatigue, dwindling amounts of federal funding, and hundreds of daily deaths due to COVID-19.
US ECONOMIC IMPACTS Recent data from the US Census Bureau is helping to illuminate impacts of the COVID-19 pandemic and response. The bureau released 1-year estimates from its American Community Survey today, showing various social and economic changes. For example, fewer people moved to a new home, more people gained internet access through expanded coverage and computer ownership, more unmarried couples moved in together, more people spent over 30% of their income on rent, preschool enrollment dropped, and public transportation use dropped by half. Another report, the 2022 Current Population Survey Annual Social and Economic Supplement (CPS ASEC), included some rare good news. Childhood poverty is at a historic low, falling from 9.7% to 5.2% between 2020-2021. Experts attribute much of this improvement to the boosted child tax credit included in the American Rescue Plan that provided families additional money to pay for food, clothes, education, and extracurricular activities. Notably, the overall poverty rate also fell to 7.8% in 2021 from 9.2% in 2020. Additionally, the report shows that insurance coverage expanded in 2021, most likely due to pandemic-related measures that mandated a continuous enrollment provision Medicaid. Many of these measures have already ended or are set to expire, and it is now up to the US Congress to decide whether these measures should be renewed or stay in place.
LONG COVID IN EUROPE An estimated 17 million people across the WHO’s Europe region experienced post-acute sequelae or long-term symptoms of COVID-19, also known as long COVID, during the pandemic’s first 2 years, according to a modeling study conducted by the Institute for Health Metrics and Evaluation (IHME) for WHO/Europe. The region comprises 53 Member States across Europe and Central Asia that are home to nearly 900 million people. The report highlights the ongoing public health challenges posed by the condition, which is characterized by cognitive and mental health problems, fatigue, shortness of breath, and other symptoms experienced 12 weeks or more following a COVID-19 diagnosis.
The report, published September 13, found the number of new long COVID cases identified between 2020 and 2021 rose threefold, driven by the rapid increase in confirmed COVID-19 cases from late 2020 through 2021; women are twice as likely than men to suffer from the condition; and the risk of long COVID increases dramatically among people with severe infections who need hospitalization. WHO officials and the report authors said that although most people fully recover from COVID-19, the findings underline the need for additional analysis and investment to determine the long-term effects of the disease, including implications for the workforce and the need for rehabilitative and support services.
SARS-COV-2 VACCINE BOOSTER DURABILITY Recently published data on SARS-CoV-2 vaccine booster durability indicate that protection wanes by approximately 10-20% each month. Researchers at Ohio State University conducted a longitudinal study of healthcare workers to assess the durability of antibody titers stimulated by booster doses and published their preliminary analysis as a commentary in the New England Journal of Medicine. The study included 46 fully vaccinated participants who received their first booster—24 with the Moderna vaccine and 22 with the Pfizer-BioNTech vaccine*—and serum specimens were collected every 3 months after the booster dose to assess neutralizing antibody titers against the multiple variants, including the Omicron variant of concern (VOC).
*Neither the commentary nor supplementary appendix explicitly indicates whether the booster doses were the monovalent or bivalent formulation, but based on the study timing and duration, we understand them to be monovalent.
Among the participants, 14 had breakthrough infections during the study period, including 9 during the US Omicron variant surges. Notably, the duration of antibody titers was more robust in individuals with prior SARS-CoV-2 infection. Overall, neutralizing antibody titers decayed at a mean rate of 17.53% per month against lineages containing the D614G mutation (ie, Omicon sublineages). More specifically, titers decayed by 19.50% against the B.1 sublineage, 18.44% against BA.2.12.1, and 19.55% against BA.4/5 each month. Among participants with previous SARS-CoV-2 infection, antibody titers decayed 17.07% against lineages containing the D614G mutation, 14.22% against BA.1, 9.97% against BA.2.12.1, and 12.12% against BA.4/5. Additionally, the decay in antibody titers following the first booster dose was slower than after receiving the second dose of the primary series of the vaccines.
Experts note that waning protection is not unexpected for vaccines, emphasizing that this should not dissuade anyone from recommended booster doses. Some experts, however, have called attention to the contrast between this analysis and federal officials’ recent comments about plans for annual boosters, much like seasonal influenza. They argue that if antibody titers wane over a period of several months, annual boosters may not be often enough to provide sufficient protection. Available evidence demonstrates that booster doses do maintain protection against severe disease; however, rapid waning of that protection may necessitate regular booster doses—potentially as frequently as 4 months—especially for those at elevated risk of severe disease and death. Others posed questions regarding barriers to accessing booster doses, particularly in the context of the generally low coverage for annual seasonal influenza vaccinations.
Another issue is the absence of clearly defined and regular seasonal trends for COVID-19. While seasonal influenza tends to peak annually in the winter months, the COVID-19 pandemic has not exhibited traditional seasonality, peaking multiple times each year, across all seasons. Additionally, the emergence of new variants of concern or associated sublineages has occurred more frequently than once per year so far in the pandemic, which White House officials acknowledged could necessitate additional booster doses. Many questions remain regarding future COVID-19 trends and how those will factor into vaccination planning and guidance.
US ECONOMIC IMPACTS Recent data from the US Census Bureau is helping to illuminate impacts of the COVID-19 pandemic and response. The bureau released 1-year estimates from its American Community Survey today, showing various social and economic changes. For example, fewer people moved to a new home, more people gained internet access through expanded coverage and computer ownership, more unmarried couples moved in together, more people spent over 30% of their income on rent, preschool enrollment dropped, and public transportation use dropped by half. Another report, the 2022 Current Population Survey Annual Social and Economic Supplement (CPS ASEC), included some rare good news. Childhood poverty is at a historic low, falling from 9.7% to 5.2% between 2020-2021. Experts attribute much of this improvement to the boosted child tax credit included in the American Rescue Plan that provided families additional money to pay for food, clothes, education, and extracurricular activities. Notably, the overall poverty rate also fell to 7.8% in 2021 from 9.2% in 2020. Additionally, the report shows that insurance coverage expanded in 2021, most likely due to pandemic-related measures that mandated a continuous enrollment provision Medicaid. Many of these measures have already ended or are set to expire, and it is now up to the US Congress to decide whether these measures should be renewed or stay in place.
Another reason the upcoming election is so important.
by ponchi101 If the US electorate were in any way sophisticated (and there are very few that are, worldwide), the configuration of congress would be easily moved. The GOP has proven again and again that they care not one bit for the people of the USA; they care about the corporations.
But we know that the people of the USA cannot make the connection. So, who knows how that ends in November.
by dryrunguy Biden thoroughly deserves to get dragged for his "the pandemic is over" comment. Just because that's what people want to hear doesn't make it true.
Also, be sure to take note of this little gem buried in the latest Situation Report--1200 reported COVID death globally per day (that's probably woefully low), and 400 of those deaths occur in the United States even though the United States only comprises 4% of the global population. Think on that.
Sure, the pandemic is over.
::
“PANDEMIC IS OVER” In an interview with “60 Minutes” at the North American International Auto Show in Detroit, Michigan, US President Joe Biden said he believes that the COVID-19 “pandemic is over” while simultaneously acknowledging that the disease continues to be a “problem.” Notably, a White House team that reviewed the transcript of the interview, which aired September 18 but was taped last week, did not alert its COVID-19 response team about the declaration, leaving senior federal health officials surprised and without a coordinated response for the immediate reactions. President Biden had not originally planned to make headlines on COVID-19, nor had he discussed an end to the pandemic with his health advisors. The day after the interview aired, US HHS Secretary Xavier Becerra supported the president’s comments, saying that effective vaccines, tests, and treatments put the nation on a better path than earlier in the pandemic and noted the administration is reviewing whether it will renew the national declaration of a public health emergency.
But President Biden’s comments drew swift and sharp reactions from public health experts and appeared to further divide opinions over when and how the nation will move out of a pandemic state and into one of endemicity. Some experts supported the president’s comments, noting that while COVID-19 should continue to qualify as a top national priority, much of the nation is settling into a new way of life. Other experts fear that President Biden’s declaration further muddles the messaging surrounding the pandemic and comes at an inopportune time, when the US government is rolling out new bivalent vaccine boosters and asking the US Congress for additional emergency spending. Additionally, virologists are seeing signs of viral resurgence, underlining the enormous amount of uncertainty surrounding the future.
While there are no clear markers to the end of a pandemic, some experts point to 2 ways to determine when an outbreak emergency is over: by looking at what the disease is doing physically and psychologically to a population. To be sure, President Biden’s comments reflect a general national sentiment that people want to move on from the pandemic and that the situation differs significantly from 2 years ago. Schools are open; air travel has returned to pre-pandemic levels; workers are returning to offices at the highest rates since the start of the pandemic, although 1 in 3 say they fear infection by working in offices; and COVID-19 testing labs and at-home test manufacturers are downsizing, but primarily due to a lack of funding.
However, many, including White House Chief Medical Advisor Dr. Anthony Fauci, are worried the nation is not where it needs to be in order to “live with the virus.” The US continues to record more than 400 daily deaths, and the world counts more than 1,600 deaths each day. Notably, this means the US accounts for nearly 25% of the worldwide daily COVID-19 mortality, despite representing only 4% of the global population. A significant portion of the US population remains unvaccinated or under-vaccinated, and therefore at elevated risk of severe disease and death. Nationally, 68% of the population has received a primary vaccine series but only 35% of those over age 5 have gotten a first vaccine booster dose. The president’s remarks could further hinder efforts to increase vaccination and booster rates ahead of what many expect will be a surge in cases over the winter. Additionally, the pandemic has had crippling health, social, and economic impacts on essential workers and vulnerable populations, such as those who are immunocompromised, and on the estimated 18-23 million US residents who are suffering the long-term physical and mental health effects of long COVID.
President Biden’s remarks also likely will undercut his administration’s efforts to procure additional emergency spending for COVID-19. The White House has requested US$22.4 billion from the US Congress, but leading Republicans, who were already skeptical about authorizing additional funding, said the president’s comments essentially shut the door on negotiations as well as raise questions about other pandemic-related measures. Without additional funds for vaccine, treatment, and diagnostic supplies, or for research into next generation vaccines that could prevent SARS-CoV-2 transmission, the burden to pay for pandemic-related tools and stop chains of transmission will shift to the US public, and it remains to be seen whether federal and state policymakers will learn lessons from this pandemic in order to strengthen public health infrastructure to prepare for the next.
US VACCINATION CAMPAIGN The US Department of Health and Human Services last week released a video advertisement to encourage people to get updated SARS-CoV-2 vaccine booster shots. The ad specifically highlights those who are aged 50 and older, and shares the importance of getting the updated, bivalent vaccines, which are expected to provide additional protection against currently circulating SARS-CoV-2 Omicron subvariants. More than 200 million people are eligible for the new vaccines, however demand has dropped considerably with each new round of shots. More than half of people eligible for previous boosters never got them. Nevertheless, several pharmacies and hospitals in California, Hawaii, and Washington, DC, have reported running out of doses of the updated Moderna booster but expect additional supplies soon.
Additionally, several reports have raised concerns over the potential for vaccine administration errors, particularly among children. While there is no evidence vaccine mix-ups have caused more severe adverse events, the complexity involved in keeping straight up to 11 different vaccine brands and formulations has led the US CDC to produce visual guides for vaccine administrators. The potential for errors further undercuts parents’ already low interest in vaccinating their young children. Only about 410,000 children aged 5 and younger have been fully vaccinated since the vaccines became available for this age group in June, according to CDC data. The number of COVID-19 deaths among children is low, but scientists remain concerned about possible long-term complications of COVID-19 among children. Many physicians, and parents, have cited failures among government and local public health agencies to adequately promote the vaccine, communicate about its availability, and debunk circulating myths. Some health officials are concerned that hesitancy to vaccinate children against COVID-19, as well as other diseases, could lead to future outbreaks of other childhood infections.
Public health experts had hoped that another vaccine option—the adjuvanted protein-based SARS-CoV-2 vaccine from Novavax that uses a more traditional platform—would help win over those who were hesitant to receive the newer mRNA-based vaccines. But since it was authorized in July, uptake remains low, with only 6,278 people fully vaccinated using the Novavax vaccine. Outside of the US, the Novavax vaccine has been approved in 38 other countries, including in Japan and Australia, which each recently approved the vaccine for use as a booster.
EU EMERGENCY SUPPLY CHAIN POWERS The European Commission has shared a proposed rule that would make EU Member States prioritize the production of key goods and services to preserve supply chains in a crisis. The Single Market Emergency Instrument would create a crisis governance framework to prevent market fragmentation, drawing on lessons from the COVID-19 pandemic. Among the interventions available to the European Commission, breaking contracts to facilitate the production and stockpiling of critical products would be an option, as well as repurposing production lines and facilitating expansion to prevent bottlenecks like those experienced during the COVID-19 pandemic and the Russian invasion of Ukraine. The emergency powers of the proposal aim to reorganize supply chains as quickly as possible and support the increase and availability of crisis-relevant goods. The proposal includes fines up to 300,000 euros for companies that share incorrect or misleading information. The effort, which echoes similar efforts in the United States and Japan, will likely face pushback from businesses concerned with the expanded power the ruling is overreaching and intrusive.
VACCINE PRODUCTION IN AFRICA Amid slowing global demand for SARS-CoV-2 vaccines, the world’s largest producers of vaccines for COVID-19—Pfizer-BioNTech and Moderna—continue to face pressure to allow low- and middle-income countries (LMICs) to produce their vaccines after much of the supply was purchased by high-income countries. Under a fill and finish agreement with Pfizer-BioNTech, the South Africa-based Biovac Institute, which is partly owned by the South African government, recently produced its first batch of the companies’ vaccine. The doses, the first of Pfizer-BioNTech’s shots to be produced in Africa, will undergo regulatory review and additional batches are expected to be commercially available next year. Aspen Pharmacare, which is authorized to fill and finish vials of the J&J-Janssen SARS-CoV-2 vaccine under its Aspenovax brand for distribution in Africa, earlier this year cautioned it might have to halt its vaccine production lines because it had not received a single order. At the end of August, Aspen announced it signed a deal with the Serum Institute of India to manufacture and sell 4 Aspen-branded vaccines for Africa, effectively keeping the production lines open. Moderna reportedly is seeking a partner on the continent to produce its SARS-CoV-2 vaccine.
In related news, Moderna has allowed the use of its vaccine in clinical trials to test a shot developed by Afrigen Biologics & Vaccines, another South African biotechnology company working with the WHO as part of its mRNA Vaccine Technology Transfer Hub. Afrigen is working to develop mRNA-based SARS-CoV-2 vaccines to increase production and access for LMICs. Instead of supplying the vaccine directly, Moderna approved the Medicines Patent Pool to provide its vaccine to Afrigen for use in early-stage clinical trials; Pfizer-BioNTech refused a similar request because the companies did not see the need as urgent. Afrigen expects to begin human trials of its mRNA vaccine candidate by May 2023. Additionally, Moderna last week said it is open to supplying the Chinese government with its vaccine, although no final decision has yet to be reached. China has not authorized the use of any foreign-made SARS-CoV-2 vaccines, relying on several domestically produced shots.
TREATMENT ACCESS & UPDATES Amid heightened demand from low- and middle-income countries (LMICs) for expanded access to COVID-19 therapeutics, little progress has been made at the World Trade Organization (WTO) toward reaching an agreement to include COVID-19 therapeutics and diagnostics in a limited deal reached earlier this year to temporarily waive patents on SARS-CoV-2 vaccines. High-income countries, including the UK, Switzerland, EU Member States, and the US, as well as pharmaceutical companies, appear opposed to extending the deal to treatments and tests by the end-year deadline.
Separately, a program aimed at bringing oral COVID-19 antivirals to 10 LMICs in sub-Saharan Africa and Asia—Ghana, Kenya, Laos, Malawi, Nigeria, Rwanda, South Africa, Uganda, Zambia, and Zimbabwe—recently launched. With support from nonprofit organizations and other partners, the COVID Treatment Quick Start Consortium will provide Pfizer’s Paxlovid (nirmatrelvir-ritonavir) through pilot programs to evaluate the best ways to implement test-to-treat programs in areas with limited healthcare resources and infrastructure.
In other treatment news, the European Medicines Agency (EMA) last week extended its authorization of AstraZeneca’s preventive COVID-19 therapy Evusheld (tixagevimab co-packaged with cilgavimab) as a treatment for the disease among adults and adolescents with COVID-19 who do not need supplemental oxygen but who are at increased risk of disease progression. Last month, Japan became the first country to approve the monoclonal antibody for COVID-19 treatment. Several nations already have authorized Evusheld as a preventive therapy among people with compromised immune systems who do not respond to vaccination in several nations, including the US.
Additionally, the WHO last week strongly advised against the use of 2 different antibody therapies—sotrovimab as well as casirivimab-imdevimab—to treat patients with COVID-19 because they have limited clinical activity against currently circulating viral variants. The US FDA previously pulled or limited the use of the drugs, and some experts criticized the WHO for waiting to make the updated recommendation. The WHO expanded its conditional recommendation for the antiviral remdesivir to cover patients with severe COVID-19 and those with non-severe infections but who are at high risk of hospitalization.
Only a handful of COVID-19 therapeutics remain useful against currently circulating SARS-CoV-2 strains. While researchers quickly developed 4 effective treatments for hospitalized COVID-19 patients in the year between January 2020 and February 2021, no new therapies for hospitalized patients have been authorized since February 2021, raising concerns about whether treatment advancements have stalled.
by ponchi101 1,200 deaths/day reported worldwide simply means that the rest of the world is not reporting, and the USA is. I really doubt that Colombia even cares anymore; people here have more problems, so nobody is getting tested. One has to wonder how the C19 deaths are reported (but of course, we have very few anti-vaxxers).
Biden's "pandemic is over" comment: eventually, you need to get to RealPolitiks. The mid terms are coming and the last thing you need is the GOP securing both the House and the Senate, and then you can see what is going to happen to any possible legislation or any possible advancement. If the GOP gets the senate, you can bet they will pass a law banning abortion (Biden will veto) and that can lead to more deaths than C19.
So, if in order to get the dumb electorate to vote democrat in November he needs to declare the pandemic is over, do it. Anyway, the people more at risk are those that still refute the science. I feel no pity for them, so be it.
by ponchi101 I caught today the Colombian numbers.
Colombia, with a bit under 50MM people (1/40th the world population) is having 200 deaths a day. 1/8th of the number quoted by the post above, despite smaller than the USA by a lot.
Countries are simply not reporting or counting. In that sense, the pandemic IS over; if people no longer care, there is no phenomenon to report.
by dryrunguy Here is the latest Situation Report. Just when I start to think these things are getting a little redundant and less useful, they send one out that is chock full of interesting stuff. Of particular note in this one:
1) Safety issues discovered upon inspecting the Bloomington, Indiana facility producing Moderna's bivalent booster
2) The lack of interoperability between public health reporting systems (we knew this already, but I didn't know some agencies were actually resorting to fax machines to report data)
3) The largest COVID-19 fraud case to date--47 people got COVID money from the U.S. Department of Agriculture to feed hungry children, but they actually used the money to buy luxury items and real estate. Should have known that was coming. Wonder if Brett Favre's name is going to come up in that one (just kidding, kind of...).
::
EPI UPDATE The WHO COVID-19 Dashboard reports 610.4 million cumulative cases and 6.51 million deaths worldwide as of September 21. Global weekly incidence remained stable, increasing 2% over the previous week. Global weekly mortality continued to decrease, for the fifth consecutive week—down 15% from the previous week.
Weekly incidence declined in most WHO regions, ranging from -8% in South-East Asia to -32% in the African region. As predicted last week, the decreasing trend in Europe reversed, with the region recording a 10% increase in weekly incidence. Weekly incidence in the Western Pacific region remained relatively stable, increasing 3% from the previous week.
UNITED STATES
The US CDC is reporting 95.6 million cumulative cases of COVID-19 and 1,049,101 deaths. Daily incidence continues to decline, down to 55,332 new cases per day. Daily mortality appears to have plateaued, with an average of 356 deaths per day. **
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to exhibit downward trends, with decreases of 6.8% and 11.1%, respectively, over the past week. Both trends peaked around the last week of July, similar to trends in daily incidence.
The BA.5 sublineage continues as the dominant strain in the US, accounting for 84.8% of sequenced specimens. Since last week, however, several other Omicron sublineages show evidence of possible growth advantage over BA.5, including BA.4.6 (10.3%), BF.7 (1.7%), and BA.2.75 (1.3%). The prevalence of BA.4 continues to fall, down to 1.8% the week of September 17.
EMERGING VARIANTS As the Northern Hemisphere moves into its colder months, scientists and officials are following the evolution of SARS-CoV-2 more closely than ever, watching for new variants of interest (VOI) and variants of concern (VOC). As of now, Omicron subvariants are capturing the most international attention, and experts remain uncertain as to which variant will be dominant going into fall. More specifically, the sublineages of the Omicron subvariants BA.2, BA.4, and BA.5 are beginning to show growth advantages compared to their parents. In the United States, prevalence of BA.4 and BA.5 appears to be decreasing, while Omicron sublineage cases have been rising. BA.4.6, a sublineage of BA.4, is now estimated to make up 10.3% of new cases. BF.7, a BA.5 sublineage, now is estimated to make up 1.7% of new cases. BA.2.75, a BA.2 sublineage, is estimated to make up 1.3% of new cases. BF.7 has garnered particular concern among the scientific community, as it has recently made up more than 10%, and even over 25%, of new cases in some Western European nations. However, some experts have argued that BQ.1, a BA.5 sublineage, and BA.2.75.2, a sublineage of BA.2.75 that demonstrates additional immune evasion, also pose a threat. While still too early to tell which sublineage might become predominant, and where, the continuously evolving SARS-CoV-2 promises to keep the attention of scientists and public health practitioners, even as much of the world wants to move on.
BIVALENT BOOSTER FOR YOUNG CHILDREN According to an updated Fall Vaccination Operational Planning Guide released by the US CDC on September 20, bivalent SARS-CoV-2 vaccine boosters could be available for children ages 11 years old and younger starting in October, pending authorization from the US FDA. Dr. Peter Marks, Director of the FDA Center for Biologics Evaluation and Research (CBER), confirmed that the updated boosters for 5- to 11-year-olds are expected to receive emergency use authorization in the next few weeks. The boosters for younger children aged 6 months to 5 years are “a few months away,” according to Dr. Marks.
Currently, the updated bivalent booster shots from Pfizer-BioNTech are authorized for anyone aged 12 years and older who has completed their primary vaccination series, and Moderna’s bivalent booster is available to those aged 18 years and older who have completed the primary series. Pfizer-BioNTech and Moderna are working on bivalent vaccines for children aged 5 to 11 years and 6 to 17 years, respectively. While children aged 6 months and older can now receive primary vaccinations against COVID-19 (3 doses of Pfizer-BioNTech and 2 doses of Moderna), they remain ineligible for booster doses.
More than 1,400 children and teens have died of COVID-19 in the US, according to CDC data, but vaccination rates for the youngest children remain low, worrying health officials. Only 38% of children aged 5-11 and 8% of those aged 6 months to 4 years have received at least one dose of vaccine. Correspondence published today in the New England Journal of Medicine discusses a study showing that immunity from vaccination and previous infection provided considerable protection against hospitalization and death among children 5 to 11 years of age, but that protection rapidly waned over 16 weeks, particularly against the Omicron variant. The authors note that the rapid decline in protection against Omicron infection conferred by vaccination and previous infection provides support for booster doses among this age group. However, children will first need to finish their 2- or 3-dose primary series before becoming eligible to receive an updated booster when authorized.
MODERNA BIVALENT BOOSTER SUPPLY Providers across the US have reported supply shortages of Moderna’s new bivalent SARS-CoV-2 booster, leading pharmacies and local health groups to offer limited appointments for receiving the shot. A Moderna spokesperson anticipated that availability constraints would be resolved in a few days and assured that the company is committed to delivering 70 million doses of the updated bivalent vaccine by the end of the year. No supply issues have been reported for the Pfizer-BioNTech bivalent booster.
The shortage is being attributed to delays in Moderna receiving vaccine supply from its production facility operated by Catalent Inc. in Bloomington, Indiana. The facility was not cleared by the FDA to make Moderna’s new booster shots until recently. The FDA conducted a routine inspection of the facility amid concerns that it was not sufficiently sterile. In its Form 483 notice, the FDA cited observations related to quality control, recordkeeping, failure to follow procedures and address discrepancies in certain batches, misuse of equipment, and contamination in vials packaged at the Catalent facility. The FDA shared that it plans to include doses produced in the Catalent facility in the emergency use authorization (EUA) of the Moderna bivalent vaccine. The FDA also inspected a second production facility, which is operated by Thermo Fisher Scientific, and found no safety issues at that site.
Meanwhile, health officials recommend those eligible to receive Pfizer-BioNTech’s booster shot. The companies have shipped more than 21 million doses of their booster and plan to provide 100 million doses by the end of November. To accommodate locations that cannot switch to the Pfizer-BioNTech shots and need immediate supplies of Moderna’s, the federal government is adjusting ordering thresholds in the coming weeks. Efforts to maintain production of all available booster shots are a crucial component of the fall booster campaign in the US, with the federal government strongly encouraging US residents to receive boosters as new cases are expected to rise this fall and winter.
US FDA TEST AUTHORIZATION The US Department of Health and Human Services’ Office of Inspector General (OIG) on September 21 released a report criticizing the use of the emergency use authorization (EUA) mechanism by the US FDA during the early months of the pandemic. The report cited changing standards for new EUAs for COVID-19 tests from January 2020 to May 2020, sometimes allowing flawed diagnostic and serology tests—such as the initial US CDC assay which was unusable for weeks—to be used to increase testing availability at the cost of quality. Additionally, failure of the FDA to engage with public health laboratories, who were responsible for initial testing efforts, also led to testing challenges. These critiques echo those in a recent study published in the Journal of Public Health Management & Practice describing the experience of public health laboratories in 27 states during the pandemic from 2020 through early 2021. Furthermore, test developers interviewed by OIG noted that, despite FDA support for EUA requests, the EUA process for new COVID-19 tests remained frustrating and confusing to navigate. To help prevent similar issues during future health emergencies, the OIG report recommended that the FDA revise EUA guidance, improve resources for test developers and tracking of EUA submission monitoring, establish better communication between FDA and the lab community, and incorporate lessons learned into a national testing strategy beyond the EUA process.
DATA COLLECTION & ANALYSIS Outmoded and underfunded public health information and data systems in the US are crippling epidemiologists’ and other experts’ ability to fully understand the COVID-19 pandemic and subsequently harming federal, state, and local responses. With state and local health departments having to resort to communicating data through antiquated fax machines, spreadsheets, emails, and phone calls, a lack of interconnected data systems has forced US health officials to extrapolate and make educated guesses about who is being hospitalized with COVID-19, how well vaccines are working, and who is being infected with which variants.
As new SARS-CoV-2 bivalent vaccine boosters are being rolled out in the US, this type of data is more important than ever. Understanding the demographics of the 400-500 people dying of COVID-19 each day in the US would help public health officials better target resources to help prevent these deaths. While we know that vaccination reduces the risk of severe illness and death from COVID-19, there is little data on whether people who end up in intensive care units (ICUs) have been vaccinated or boosted, which shots they received, when they got them, and if they had an immune response. Nor are there data on the COVID-19 treatments they received.
Overall, people are less likely to die of COVID-19 now because of collective immunity from vaccinations or natural infections. But the disease is a leading cause of death and likely will remain so indefinitely. Older adults continue to be at an increased risk of severe illness and death nationwide, and racial and ethnic disparities persist. A recent study published in PNAS suggested that while racial and ethnicity-related mortality disparities among Whites and 6 other groups worsened with the onset of the COVID-19 pandemic, most of those disparities evolved to pre-pandemic levels after the first year. Notably, however, 2 years into the pandemic mortality disparities remained exacerbated for American Indian or Alaska Native people and for Native Hawaiian or other Pacific Islander people when compared to the White population, driven by mortality among those under aged 65 years. The study authors call for new policies and community investments addressing the pandemic’s unequal impacts.
Still, knowing who is dying of COVID-19 will help best target resources to prevent these deaths. Since the beginning of the pandemic, the US CDC has received more funding to help modernize its data and analysis systems, but experts worry the nation’s lawmakers could once again slip into a boom-or-bust funding pattern, leaving the country's public health data systems weak and underfunded.
PANDEMIC FRAUD The US Department of Justice announced charges against 47 people accused of carrying out what officials said is the largest COVID-19 fraud scheme to date. Federal prosecutors said the alleged scheme involved the creation of fake entities that claimed to be providing meals to tens of thousands of children. After being reimbursed more than US$250 million from a US Department of Agriculture child-nutrition program, those charged used the money to purchase luxury items and real estate instead of feeding children, according to prosecutors. The 47 defendants are facing charges related to conspiracy, wire fraud, money laundering, and paying and receiving kickbacks. The Justice Department has recently stepped up its efforts to identify and prosecute those involved in theft from programs meant to provide aid during the COVID-19 pandemic.
by ti-amie More details on what the report summarizes.
by ponchi101 Vaccination.
Reports here in Colombia say that a lot of vaccines are in danger of expiring. But I am not sure if it is because almost everybody has been vaccinated, or people has stopped.
by dryrunguy Here's the latest Situation Report. The cryptic lineages section is really interesting.
BTW, they will be shifting to providing updates just once a week.
::
PANDEMIC PREDICTIONS Recent increases in COVID-19 cases in the UK could signal that the US is heading into a fall and winter COVID-19 surge. Historically, the US lags the UK in case trends by about one month, and the UK trend began rising the week of September 17. Some models predict US case trends will continue to decrease into October before beginning to rise, and while current predictions suggest a big increase in infections, the infection-detection rate likely will remain low due to declines in testing. Because the US population has some underlying immunity, and most experts agree the country has the pandemic under control, the death toll is expected to be rather modest.
But this modeling is based on the Omicron BA.5 subvariant, and the emergence of a new variant or subvariant could upend these predictions, particularly if there is a reduction in cross-variant immunity. BA.5 continues to account for the majority of new COVID-19 cases in the US (83.1%), but BA.4.6 (12%) and BF.7 (2.3%), an offspring of BA.5, are beginning to show growth advantage over BA.5. BF.7 has an additional genetic mutation in the spike protein compared with BA.5, which could reduce the efficacy of the monoclonal antibody treatment Evusheld, one of the few remaining therapies effective against BA.4 and BA.5. The mix of variants in the UK appears to be about the same as the US, although epidemiologists are watching to see whether emerging variants such as BQ.1.1 and BA.2.75 grow in proportion.
US President Joe Biden's declaration that the COVID-19 pandemic is "over" during a "60 Minutes" interview on September 18 raised eyebrows among many experts, most of whom agree that while some countries are in a better place than during the first year of the pandemic—exemplified by the fact that many in the US and elsewhere are returning to their pre-pandemic lifestyles—COVID-19 should remain an urgent priority. In the US, around 400 people die every day due to COVID-19, more than triple the average number who die from influenza.
The declaration by President Biden came shortly after WHO Director-General Dr. Tedros Adhanom Ghebreyesus stated that the end of the pandemic was "in sight." Both statements drew condemnation from WHO Senior Advisor Dr. Bruce Aylward, who called on high-income countries comfortable with the state of the pandemic within their borders to increase aid to low- and middle-income countries (LMICs) that are still struggling to get COVID-19 under control and gain access to vaccines, therapeutics, diagnostics, and other tools. Additionally, allowing the SARS-CoV-2 virus to maintain footholds in LMICs and elsewhere could lead to new variants with the ability to escape immunity. There remains much work to do, experts agree, as many health disparities between high-income nations and LMICs persist and will only get worse if aid is reduced or cut off. While some may feel COVID-19 is under control in places like the US, the pandemic is not over.
US CDC INFECTION CONTROL GUIDANCE The US CDC published changes to its guidance on infection prevention and control recommendations for healthcare personnel during the COVID-19 pandemic. One of the major alterations includes ending the overarching recommendation that everyone wear masks in nursing homes and hospitals. Previously, the guidance asked that everyone wear appropriate masks and respirators in these facilities, but the update only maintains that recommendation in communities experiencing high levels of transmission. The CDC said the change was made to reflect the high levels of immunity derived from vaccinations and prior infection, as well as the availability of effective treatments.
Nevertheless, elderly populations have been hit hard by the pandemic and remain among the most vulnerable. There are concerns that the new recommendation could make life even more difficult for elderly and immunocompromised people to safely navigate healthcare settings, potentially leading to fewer care options and increased stress and isolation among populations that already have suffered greatly. Additionally, many public health experts highlighted the importance of masking in the US as the nation heads into its fall and winter seasons and predictions of a new surge in COVID-19 cases. Appropriately worn masks and respirators serve as source controls that can prevent transmission during a season when many people are gathering indoors, but public appetite for new mask mandates is at an all-time low. The CDC’s guidance leaves the responsibility to take actions to protect vulnerable populations in individuals’ hands.
UPDATED BOOSTERS FOR YOUNGER CHILDREN Updated bivalent booster vaccine doses for younger children in the United States likely will be available before the end of this year. On September 23, Moderna announced in a tweet that the company is requesting emergency use authorization (EUA) from the US FDA for its vaccine booster bivalent vaccine that targets both the original strain of SARS-CoV-2 and the BA.4/5 subvariants of Omicron for adolescents aged 12 to 17 years and children aged 6 to 11 years. The company’s application for the youngest children, ages 6 months to under-6 years, is expected to be completed by year's end.
On September 26, Pfizer-BioNTech announced they have completed a submission to the FDA requesting EUA for the companies' Omicron-adapted bivalent booster for children aged 5 to 11 years. The companies also have begun a Phase 1/2/3 study to evaluate the safety, tolerability, and immunogenicity of different doses and dosing regimens of bivalent vaccine in children ages 6 months through 11 years of age. Additionally, they expect to file for marketing authorization of the bivalent booster for children aged 5-11 with the European Medicines Agency (EMA) in the coming days. Bivalent boosters from both Moderna and Pfizer-BioNTech are already authorized for adults and individuals aged 12 years and older, respectively, in the US. The FDA could make a decision on bivalent boosters for younger children before the next meeting of the US CDC's Advisory Committee on Immunization Practices (ACIP), scheduled for October 19-20.
GLOBAL VACCINE SUPPLY Last year, the US government committed to providing 1.1 billion doses of the Pfizer-BioNTech SARS-CoV-2 vaccine to low- and middle-income countries (LMICs). Last week, however, Pfizer and the US government agreed to lower the number of Pfizer-BioNTech SARS-CoV-2 vaccine doses going to LMICs this year, with Pfizer agreeing to reduce its delivery commitment from 1 billion doses to 600 million doses. Pfizer said while it can meet its previous 1 billion dose commitment, the revised commitment reflects reduced demand for vaccine doses in LMICs, barriers in administration, and vaccine hesitancy, and provides more time for the US and its partners to address delivery and administration challenges. The US will retain an option to purchase the additional 400 million doses for its international program after this year. Under the US contract, Pfizer previously delivered more than 400 million vaccine doses to 79 countries through the COVAX initiative.
During earlier stages of the COVID-19 pandemic, many experts criticized high-income countries for hoarding vaccines and other pandemic supplies, thereby perpetuating inequitable access to lifesaving supplies during the height of the pandemic. The COVAX program was designed to ensure equitable access to vaccines and has donated more than 1.7 billion COVID-19 vaccine doses to 146 countries. While the program ramped up, demand for SARS-CoV-2 vaccines outmatched the supply of approved products and vaccine manufacturers prioritized bilateral customers. Pfizer executives shared that the global effort to develop, manufacture, and distribute vaccines during the COVID-19 pandemic revealed important lessons around how to configure supply chains and design tighter logistics strategies for the future. While some countries are declaring an end to the COVID-19 pandemic, supply chain issues persist in many parts of the world, and only 24% of people in low-income countries have received at least one dose of vaccine. The shift in attention away from the pandemic was highlighted last week during the United Nations General Assembly (UNGA) meetings, where discussions about vaccine equity remained notably absent.
Despite slowing vaccine donation efforts, the US government and Pfizer remain committed to providing other critical supplies to LMICs. On the sidelines of the UNGA at the COVID Global Action Plan Ministerial Meeting, the US government announced plans to establish a clearinghouse of medical supplies to help other countries combat COVID-19, expand its program to distribute therapeutic drugs in 10 countries, expand access to medical oxygen, train healthcare workers in LMICs, and introduce early testing systems that can help healthcare workers identify COVID-19 patients who qualify for treatment. Additionally, Pfizer recently announced its intent to supply up to 6 million treatment courses of Paxlovid, its COVID-19 oral treatment, to the Global Fund as part of its COVID-19 Response Mechanism (C19RM). Depending on local regulatory approvals, 132 Global Fund-eligible LMICs will be able to procure Paxlovid beginning this year. These commitments are a crucial component of a global response to COVID-19, which exposed and continues to worsen concerning gaps in global pandemic preparedness and response systems.
CRYPTIC LINEAGES Nature examines the work of a team of scientists using wastewater surveillance to hunt for the next SARS-CoV-2 variant. In January 2022, the team identified a lineage that shared several mutations with the predominant Omicron variant of concern (VOC) but came from a different branch of the viral family tree. They then traced the cryptic lineage back to one Wisconsin business employing fewer than 30 people. None of the employees tested by nasal swab have shown signs of the lineage, leading the researchers to suspect an individual might be harboring the virus in their gut. While it does not appear the cryptic lineage is spreading, it has gained additional mutations since first being identified. Even if they do not identify the Wisconsin individual in which the virus is evolving, the researchers hope their sleuthing will inform future efforts to identify, track, and forecast emerging SARS-CoV-2, or other virus, variants.
I, myself, am currently sick with some sort of virus. It began rather suddenly on Sunday with a dull, persistent headache and a throat that was increasingly sore when swallowing. On Saturday, I felt perfectly fine - 2 hours of pickleball, plus some biking...
The sore throat has now been replaced by coughing and stuffy sinuses (blowing my nose a lot).
Taste and smell are still ok - though both are always altered with most viruses.
Up to this point, it feels like many other viruses I've had throughout my life - a moderate case... not severe, and not mild, but moderate.
I hesitate to do a rapid COVID test, because, if it shows positive, it simply means that I may have COVID, or I may not. And if it shows negative, it means that I may not have COVID, or I may. When a given form of a test is only 75% - 80% accurate, it really tells you nothing in the end in practical terms. And the rapid test is the only test currently available to me.
And so I will do the responsible thing and avoid others as much as possible over the next 8 days or so... and then we'll see.
This is the first time I've been sick since the pandemic began. I've been very careful - always wearing a mask indoors, and outright avoiding certain situations. Whether I have COVID or not, some type of virus somehow made it through my defences, which is surprising.
by dryrunguy Here's the latest Situation Report. It's packed. I have bolded the paragraphs that really stood out. But all the way to the end, it's just packed.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 617 million cumulative cases and 6.53 million deaths worldwide as of October 6. Global weekly incidence remained relatively steady at slightly more than 3 million cases for the fourth consecutive week, decreasing 2% compared to the previous week. Weekly incidence in Europe increased for the third consecutive week, up 18% over the previous week. All other regions reported decreasing trends. Global weekly mortality continued to decrease, for the seventh consecutive week, down 11% from the previous week. Last week’s total—8,491 deaths—was the lowest since the week of March 16, 2020.*
*The WHO dashboard notes that data from the Africa Region are incomplete.
UNITED STATES
The US CDC is reporting 96.3 million cumulative cases of COVID-19 and 1.06 million deaths. Daily incidence continues to decline, down to 44,414 new cases per day, the lowest average since April. Average daily mortality now appears to be decreasing steadily, down from a recent high of 505 deaths per day on August 12 to 330 on October 4.**
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to exhibit downward trends, with decreases of 6.9% and 8.1%, respectively, over the past week. Both trends peaked around the end of July, approximately 1 week after the peak in daily incidence.
The BA.5 sublineage continues as the dominant strain in the US, accounting for 81.3% of sequenced specimens; however, its estimated prevalence has decreased for 4 consecutive weeks. Several other Omicron sublineages are exhibiting increasing trends over the past several months. Notably, the BA.4.6 sublineage is up to 12.8%, BF.7 is up to 3.4%, and BA.2.75 is up to 1.4%. Relative to the BA.5 sublineage, these estimates are low, but the increasing trends suggest that these subvariants may have some advantage over BA.5.
EMERGING SUBVARIANTS The SARS-CoV-2 virus continues to evolve, with multiple emerging sublineages of the Omicron variant of concern (VOC) poised to play a dominant role in the next surge. As noted above, several sublineages are increasing in prevalence in the US as the current dominant strain, BA.5, begins to wane. At this point, it is unclear if the next principal variant would be capable of evading immunity conferred by vaccination, including Omicron-specific booster doses, or prior infection with other variants, but researchers are already working to identify key mutations and project their impact. In contrast to previous surges, the forecasted fall/winter surge may not be driven by a single variant, as was the case with the Delta and Omicron surges in 2021 and earlier in 2022. In fact, WHO officials recently indicated that they are currently monitoring more than 300 Omicron sublineages.
Several of these sublineages are particularly concerning, including BQ.1 and BQ.1.1 that evolved from BA.5 and BA.2.275 and XBB that evolved from BA.2. The BQ.1 and BQ.1.1 sublineages are currently circulating in Europe, which could forecast a fall/winter surge in other Northern Hemisphere countries. All 4 of these sublineages exhibit resistance to existing treatments and vaccines, and the XBB sublineage, in particular, threatens to render existing vaccines ineffective. In addition to the risk of global spread of a vaccine-resistant vaccine, the decline in testing volume worldwide and barriers to including at-home test results in SARS-CoV-2 reporting systems could make surveillance problematic. And the general absence of COVID-19 protective measures (eg, physical distancing, mask use) could facilitate community transmission. Additionally, governments seem to be unwilling to commit additional funding to COVID-19 responses, including research on future vaccines and therapeutics, as evidenced in the US government’s struggle to secure funding for Project COVID Shield, the follow-on to Operation Warp Speed to develop advanced SARS-CoV-2 vaccines. The world is simply in a much different place than it was in 2020 and 2021, which elevates the threat from these emerging sublineages.
As opposed to more radical antigenic “shifts”—like those observed with the emergence of the Delta variant or the original Omicron variant—the new sublineages of the Omicron variant are exhibiting more subtle antigenic “drift.” This is similar to the evolution observed in annual seasonal influenza epidemics, although on a much shorter timeline. New sublineages appear to be acquiring many of the same mutations, in various combinations, which signals that they may be converging on a common set of traits. Despite the recent pattern, however, it is still possible that the virus could take a more substantial shift, which could result in the emergence of a new major variant with much different characteristics.
FALL/WINTER SURGE POTENTIAL Experts are keeping an eye on whether the United States will experience a surge in SARS-CoV-2 cases, hospitalizations, and deaths during the fall and winter seasons, a potential that looks increasingly likely. Several factors point to a forthcoming wave: the number of new cases is rising in Europe, and the US historically has followed that region’s trend; several emerging SARS-CoV-2 Omicron sublineages appear to be more capable of evading immune system protection and therapies, as discussed above; individual immunity—from vaccination or prior infection—continues to wane, primary vaccinations have stalled, and booster uptake is slow; and policy and behavioral changes have limited the positive impact of previously implemented mitigation measures, such as mask use and physical distancing.
Fifteen countries in Europe are reporting increasing cases. France is experiencing its eighth wave of COVID-19 and hospitals in the UK report resource constraints amid a new wave. New subvariants of SARS-CoV-2 that are evolutionary descendants of BA.2, BA.4, and BA.5 have emerged and are being tracked by scientists. It is still unknown whether one or more of these new strains will outcompete others and drive a fall or winter surge, but scientists are worried that these new sublineages may be able to evade current monoclonal antibody treatments and natural or vaccine-induced immunity.
Many experts stress that waning immunity could be one of the strongest predictors of a fall/winter surge in COVID-19 cases, especially if there is low uptake of new bivalent booster doses authorized in early September. In July, people aged 50 and older who had a primary series of vaccination and only one booster dose had 2 times the risk of dying from COVID-19 compared with individuals in the same age group who had a primary vaccination series and two booster doses targeting the original wild-type virus, showing the impact of continuous boosters. The new bivalent boosters targeting the original virus and the Omicron BA.4/BA.5 sublineages are expected to hold up similarly well and could help protect individuals from experiencing the most severe impacts of SARS-CoV-2 infection. Notably, however, only 7.6 million people have received an updated booster, according to the US CDC, and polling data from the Kaiser Family Foundation support increased efforts to improve messaging surrounding the new vaccines, including better communication about who is eligible to receive the shots.
Policy and behavioral shifts indicate that the US is eager to reach a post-pandemic state of normalcy even though 400-500 people are dying of COVID-19 daily. Most emergency protections established at the onset of the pandemic have been lifted, and government funds for vaccines, treatments, and tests are quickly dwindling. Many experts have cautioned against dropping COVID-19 mitigation efforts too soon.
Additionally, experts are nervous about the impact of any surge in cases on already stressed healthcare and hospital systems. Increases in demand for care—from COVID-19, influenza, or other illnesses—will challenge hospitals that are overloaded and currently experiencing a limited availability of healthcare workers, many of whom are burnt out, having been driven to the point of exhaustion. Public health preparedness and response strategies will need to reckon with these barriers sooner rather than later, as there is evidence COVID-19 cases are set to rise in the US. Data from the Massachusetts Water Resources Authority show that the amount of SARS-CoV-2 in the state’s wastewater is increasing, as are numbers of new COVID-19 cases in several states.
BIVALENT BOOSTER UPTAKE If 80% of eligible individuals aged 5 and older in the US receive an updated bivalent booster dose by the end of 2022, an estimated 90,000 COVID-19 deaths could be prevented and billions of dollars in health care costs could be saved, according to an updated analysis from the Commonwealth Fund. However, if booster vaccinations continue at their current pace, the nation could experience more than 1,000 deaths per day due to COVID-19 this winter, according to the report, which models several scenarios. Currently, between 400-500 people die each day due to the disease. Undoubtedly, vaccination has helped mitigate the burden of COVID-19, likely preventing millions of deaths and hospitalizations since vaccines became available in late 2020. However, vaccine uptake has stalled in the US, with 68% (225 million) of the total population having received a primary series and 49% (110 million) of those receiving a first booster dose. Around 37% (24 million) of eligible people aged 50 years and older have received a second booster dose, and only 7.6 million people have received an updated booster.
The White House and many public health officials are encouraging eligible individuals to receive SARS-CoV-2 vaccines and boosters, as well as influenza vaccinations, early this fall. After a relatively mild flu season last year, health officials are warning that a severe flu season in Australia could portend a similarly severe season in the US. According to a survey from the National Foundation for Infectious Diseases (NFID), only about half of US adult respondents plan to get a flu vaccine this season, and only one-third said they feel safe getting vaccinations against flu and COVID-19 simultaneously.
Notably, messaging around the COVID-19 vaccination campaign appears to be lacking, with guideline complexity possibly playing a role in confusion regarding eligibility. A recent poll from the Kaiser Family Foundation (KFF) found awareness of the new boosters is relatively modest, with only about half of adult respondents saying they had heard “a lot” (17%) or “some” (33%) about the new boosters, and 40% of fully vaccinated respondents said they were not sure whether the updated booster is recommended for them. Only about one-third of adults say they have already gotten a new booster or intend to do so “as soon as possible,” while two-thirds said they plan to “wait and see,” would get a booster only if required, would “definitely not” get a booster, or are not eligible. In a separate analysis, KFF notes that elevated COVID-19 death rates among older adults compared to younger adults through the summer was due in part to relatively lower booster uptake, compared with primary vaccination, and waning immunity. Another poll, the Forbes Health-Ipsos Monthly Health Tracker, shows 63% of adult respondents familiar with the new booster vaccine are “somewhat likely” or “very likely” to get the shot, with only 28% saying they do not plan to get boosted. As the nation heads into the colder months, vaccinations and boosters remain the best method for mitigating a potential COVID-19 surge this winter.
DISRUPTIONS FOR PEOPLE WITH DISABILITIES For many people in the US who have a disability, the COVID-19 pandemic exacerbated the inequities and disparities they already faced in accessing healthcare. According to a recently published study in Health Affairs, adult Americans with disabilities experienced significant disparities in delayed and unmet need for medical care during the first year of the pandemic. The study shows that adults with a disability were much more likely than those without disabilities to report delaying medical care, not getting the medical care they needed for non-COVID-19-related issues, and not getting needed medical care at home from a nurse or other health professional because of the pandemic. These disruptions, as well as elevated rates of comorbidities that people with disabilities may experience, could have increased their risk for severe illness or death from COVID-19.
Several factors contributed to adults with disabilities delaying care during the beginning of the pandemic, including lack of access to technology and internet, financial insecurity, reduced availability of public transportation, or inaccessible COVID-19 risk communication formats. For many adults with disabilities who depend on home- and community-based services, pandemic-related disruptions to and lack of COVID-19 relief support for these programs was a significant barrier. The pandemic has exposed health inequities and disparities that people with disabilities—especially those who experience multiple and intersecting forms of marginalization and discrimination—have faced for a long time.
Despite these notable barriers, several inclusive practices and technologies emerged as the US population tried to adapt to pandemic-related disruptions. When schools initially shifted to virtual learning modalities, some teachers implemented creative solutions to support students with disabilities. At a high school in Indiana, teachers provided supportive technologies for students with visual impairments and leveraged the intuitive accessibility of iPads and digital books. Several broad measures implemented during the onset of the pandemic, such as pivoting to remote or virtual work and learning, providing hazard pay for frontline workers, less punitive action against people who needed to cancel tickets or miss work to stay at home due to an illness, holding online events with closed captions and American Sign Language interpretation, and intentional shopping hours for immunocompromised people, allowed people with disabilities and others to adapt to pandemic-related disruptions.
As many in the US move on from the pandemic, people with disabilities are anxious about being excluded and left behind. This is especially concerning because COVID-19 has increased the number of people with disabilities in the US, as discussed below, thereby necessitating broad policy changes that center disability and help ameliorate individuals’ lived experiences.
LONG COVID/PASC Most US adults experiencing post-acute sequelae of SARS-CoV-2 (PASC), more commonly known as long COVID, have symptoms that interfere with day-to-day activities, according to new data from the US CDC’s National Center for Health Statistics. As of September 26, 14.2% of the more than 50,000 survey respondents said they had experienced long COVID—which is characterized by a host of symptoms including shortness of breath, fatigue, and cognitive difficulties—at some point during the pandemic. Of those with long COVID, 81% said they had some limitations in their daily activities compared to their activities prior to infection. Notably, 1 in 4 adults with long COVID reported significant limitations, with the proportion jumping to nearly 40% of Black or Hispanic/Latino respondents, as well as those already living with disability. The data are limited to adults and do not provide information on whether respondents are vaccinated or the severity of their SARS-CoV-2 infection. Nearly 24 million adults in the US are estimated to currently have long COVID, and researchers are working to define the condition, describe underlying causes, and search for effective treatments. Long COVID is, and likely will remain, a significant cause of disability in the US.
BIVALENT BOOSTER UPTAKE If 80% of eligible individuals aged 5 and older in the US receive an updated bivalent booster dose by the end of 2022, an estimated 90,000 COVID-19 deaths could be prevented and billions of dollars in health care costs could be saved, according to an updated analysis from the Commonwealth Fund. However, if booster vaccinations continue at their current pace, the nation could experience more than 1,000 deaths per day due to COVID-19 this winter, according to the report, which models several scenarios. Currently, between 400-500 people die each day due to the disease. Undoubtedly, vaccination has helped mitigate the burden of COVID-19, likely preventing millions of deaths and hospitalizations since vaccines became available in late 2020. However, vaccine uptake has stalled in the US, with 68% (225 million) of the total population having received a primary series and 49% (110 million) of those receiving a first booster dose. Around 37% (24 million) of eligible people aged 50 years and older have received a second booster dose, and only 7.6 million people have received an updated booster.
by ponchi101 Sister in Law and Niece in Law came down with it, in Vennieland. Mild symptoms, nothing to worry about. But this thing is still all around.
by dryrunguy The notion that both vaccines and existing therapeutics may be powerless and useless against emerging COVID mutations is alarming. And we've only scratched the surface regarding long-term or potentially permanent disability associated with COVID infection.
by ponchi101 Well, I said it in 2019, in TAT1.0. This thing will defeat us, because it is here to stay.
And the concept of permanent disability is a very 1st World Concept; here in the 3rd World, we will not see any sort of compensation or assistance for the simplest of reasons: we can't afford it.
by dryrunguy Here's the latest Situation Report. The section on Long and Medium COVID is interesting as I've been confused as to what constitutes a long but somewhat normal recovery from infection compared to what we know as long COVID. The section on Therapeutics is frightening. The section on US Public Health Measures is downright infuriating.
And for our Canadian friends, Canada got a mention in this--and it's a good one.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 619.8 million cumulative cases and 6.54 million deaths worldwide as of October 12. Global weekly incidence remained relatively steady at slightly more than 3 million cases for the fifth consecutive week, decreasing 6% compared to the previous week. Weekly incidence in Europe increased for the fourth consecutive week, up 5% over the previous week. All other regions reported decreasing trends. Global weekly mortality continued to decrease for the eighth consecutive week, although it appears to be leveling off, down 5% from the previous week.*
*The WHO dashboard notes that data from the Africa Region are incomplete.
UNITED STATES
The US CDC is reporting 96.6 million cumulative cases of COVID-19 and 1.06 million deaths. Daily incidence continues to decline, down to 39,893 new cases per day, the lowest average since mid-April. Average daily mortality is down from a recent high of 505 deaths per day on August 12 to 338 on October 11, but the steadily decreasing trend appears to be leveling off.**
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to exhibit downward trends, with decreases of 2.8% and 5.2%, respectively, over the past week. Both trends peaked around the end of July, approximately 1 week after the peak in daily incidence.
The BA.5 sublineage continues to be the dominant strain in the US, accounting for 79.2% of sequenced specimens; however, its estimated prevalence has decreased for 7 consecutive weeks. Several other Omicron sublineages continue to exhibit increasing trends. Notably, the BA.4.6 sublineage is up to 13.6%, BF.7 is up to 4.6%, and BA.2.75 is up to 1.8%. The increasing trends suggest that these subvariants may have some growth advantage over BA.5.
UPDATED BOOSTERS FOR CHILDREN US health regulators on October 12 authorized the updated SARS-CoV-2 bivalent vaccine boosters for children as young as 5 years old. Specifically, the booster from Pfizer-BioNTech is now available for children aged 5-11 and the shot from Moderna is authorized for children and adolescents aged 6-17. The booster shots—which target the original virus and the currently predominant Omicron BA.5 and BA.4 sublineages—are available to anyone age 5 or older who completed their 2-dose primary series at least 2 months prior. US CDC Director Dr. Rochelle Walensky signed off on the updated bivalent COVID boosters for children shortly after the US FDA issued its authorization. The new formulations will help bolster antibodies that have waned since prior vaccination or infection while targeting newer variants that are more transmissible and immune evasive, particularly important as children are back to in-person schooling and as the US heads into a busy holiday season.
Experts hope the new booster formulation will renew interest in getting children vaccinated before an expected fall and winter surge in cases. As of September 28, only 15.2% of children aged 5-12 years had received a first booster dose, according to CDC data. According to US regulators, there are no safety concerns for the bivalent vaccines, and they stress that vaccination is one of the best ways to keep children healthy and in school. Currently, no bivalent vaccines are approved for children under 5; however, Moderna and Pfizer-BioNTech are expected to have data available later this year. Vaccination continues to be the best way to protect against severe disease and hospitalization, and all eligible individuals are recommended to receive a bivalent booster dose as soon as possible.
LONG & 'MEDIUM' COVID Increasing evidence shows that a significant proportion of people infected with SARS-CoV-2 do not fully recover from acute infection even months later, experiencing a host of post-acute sequelae of SARS-CoV-2 (PASC), more commonly known as long COVID. Research to better understand the condition will help inform the development of care, treatment, and social support systems for people experiencing the condition. A new modeling study, published online this week in JAMA and based on information from a database of more than 1.2 million COVID-19 patients in 22 countries, estimates that 6.2% of people had long COVID symptoms 3 months after symptomatic SARS-CoV-2 infection. The model estimates the proportion of those who had at least 1 of 3 self-reported long COVID symptom clusters: persistent fatigue with bodily pain or mood swings (3.2%), cognitive problems (2.2%), or ongoing respiratory problems (3.7%). Estimated symptom duration for hospitalized COVID-19 patients was 9 months, and 4 months for those who were not hospitalized. Even after one year, 15.1% of those with long COVID continued to experience symptoms.
Another study, published in Nature Communications and performed in Scotland, utilized a matched pair design to evaluate long COVID outcomes in people with and without a previous COVID-19 diagnosis. The cohort of more than 33,000 laboratory-confirmed SARS-CoV-2 infections and nearly 63,000 individuals who had not been infected were evaluated at several time points during the study, including 6, 12, and 18 months. Among those who had symptomatic infection, 6% reported they had not recovered at all, and 42% said they had only partially recovered. No recovery was associated with hospitalization, age, female sex, deprivation, respiratory disease, depression, and multimorbidity. While asymptomatic infection was not associated with adverse outcomes, previous symptomatic infection was associated with poorer quality of life and persistent symptoms—including breathlessness, palpitations, chest pain, and confusion—that impact daily life. Vaccination was associated with a reduced risk of 7 of the 26 symptoms listed in the questionnaire. Further research is ongoing through the COVID in Scotland Study.
Many studies are focusing on the implications of long COVID, but concerns are being raised over “medium COVID”: the middle phase of recovery that stretches to about 12 weeks after infection. Lumping lasting symptoms into the long COVID category and varying definitions of post-COVID conditions have led to little clarity on what classifies as medium COVID. Notably, a few studies indicate that the most severe post-COVID complications may arise in this middle phase of recovery, rather than many months after infection or in the midst of active, symptomatic infection. While time-limited, medium COVID can still cause months of distress and life-altering symptoms. A Swedish study suggests that the risk of developing pulmonary embolism was 32 times higher in the first month after testing positive, twice as likely at 60 days, and indistinguishable from baseline by 3-4 months after infection. Similar risks and trends were found for heart attack and stroke. The findings are supported by similar data from a UK study published over the summer, in which researchers found that new-onset cardiovascular disease was increased early after COVID-19—primarily due to pulmonary embolism, atrial arrhythmias, and venous thrombosis—and new-onset diabetes mellitus incidence remained elevated for at least 12 weeks following COVID-19 before declining. All of these studies have incredible public health implications and show that even if the emergency phase of the pandemic is winding down in many regions, its long-lasting impacts are only beginning to be understood.
THERAPEUTICS Scientists expect numerous countries will experience sizable COVID-19 surges from this month through January, driven by various SARS-CoV-2 Omicron sublineages that will likely be the most transmissible and immune evasive yet. Several nations in Europe—including Germany, France, and Italy—are in the early stages of another wave, and the US typically follows this trend by about 4-6 weeks. Additionally, the new, highly immune-evasive variant XBB—a combination of two different Omicron subvariants—is driving a surge of cases in Singapore. Researchers are concerned over the new strains’ abilities to dodge vaccine-induced or natural immunity, as well as other authorized treatments.
There is evidence that Evusheld, a monoclonal antibody treatment used to bolster protection among immunocompromised individuals, may not be effective against the BA.4.6 Omicron sublineage, which now accounts for about 14% of cases in the US. If BA.4.6 can evade Evusheld, bebtelovimab could be the only monoclonal antibody treatment available to treat circulating strains of the virus. Additionally, Merck and Ridgeback Biotherapeutics released preliminary data last week showing their antiviral molnupiravir (Lagevrio) failed to reduce hospitalizations or deaths compared to placebo among multiply-vaccinated adults mostly under age 65 who were at higher risk of severe disease. The therapy did reduce the time to recovery by 6 days, and use of the drug was associated with earlier recovery across a variety of other symptom measures.
Another antiviral, Paxlovid, is being underused among patients at highest risk of severe disease in the US, experts warn. Some physicians might be reluctant to prescribe the drug due to its known interactions with several types of medications, including some used for cardiovascular disease. Notably, however, several studies show the therapy can reduce hospitalization, death, and time to recovery among older adults and those with at least one high-risk comorbidity, even those who are vaccinated. The US NIH released results from a small study last week showing that a return of COVID-19 symptoms and/or a positive test after completing an initial 5-day course of Paxlovid—commonly called COVID-19 rebound—is likely not caused by impaired immune responses. Instead, the rebound in symptoms could be partially driven by robust cellular immune responses to residual viral RNA in the respiratory tract. Infectious virus was detected in only 1 of 8 rebound participants. The study authors note that larger studies are needed to more fully understand the clinical significance and epidemiological consequences of COVID-19 rebound, but added that the findings do not support the hypothesis that a 5-day course of Paxlovid is too short for the body to mount a robust immune response. Nevertheless, Pfizer, which makes the treatment, plans to study a repeat 5-day course of Paxlovid among people who experience rebound. The US FDA requested such a clinical trial in August, ordering Pfizer to complete such a test by September 30, 2023.
US PUBLIC HEALTH MEASURES The US government, states, and localities implemented various types of public health measures—including mask use requirements, physical distancing recommendations, vaccination mandates, and quarantine rules—during the COVID-19 pandemic to help mitigate transmission of SARS-CoV-2 and protect communities. The results of a new survey, published October 10 in JAMA Network Open, show that nearly 42% of the 1,733 adult respondents reported misrepresenting and/or nonadherence to at least 1 of 9 public health measures. The survey—conducted by researchers from Middlesex Community College in Connecticut and the University of Utah between December 8-23, 2021—showed that 24.3% of respondents told someone they were with or about to be with that they were taking more COVID-19 precautions than they were; 22.5% disobeyed quarantine rules; 21.5% avoided testing when they thought they might be infected; and 20.4% did not divulge that they had a suspected or confirmed infection when entering a doctor's office.
The most common reasons for the diversions were wanting life to feel normal or desiring to exercise personal freedoms, although some people said they felt the pandemic was a hoax or not serious, were following the advice of a celebrity or other public figure, or did not want to miss work. Certain public health measures can be burdensome and highly disruptive, but they are effective, the researchers noted, and nonadherence or dishonesty can have significant consequences, including prolonging the pandemic by leading to more infections, hospitalizations, or deaths. Notably, misrepresentation and nonadherence was more common among those with a greater distrust for science, although the researchers found no association between misrepresentation/nonadherence and political belief, political party affiliation, or religion. Understanding the public’s concerns regarding public health measures could help improve willingness to follow them in the future.
WORSENING INEQUALITY Oxfam and Development Finance International (DFI) published a research report on October 11 that ranks countries on their commitment to reducing inequality between 2020-2022. The report, titled “The Commitment to Reducing Inequality Index 2022,” reviews the spending, tax, and labor policies of 161 governments and finds that both high-income countries (HICs) and low- and middle-income countries (LMICs) pursued policies that worsen inequality since the start of the COVID-19 pandemic. According to the report, 70% of LMICs made cuts to their education budgets, 50% of LMICs cut their health budgets, and nearly 50% of LMICs reduced social protection program spending. In 2021, lower-income countries reportedly spent 27.5% of their budgets to repay debts, about four times the amount those countries spent on health. Additionally, nearly 90% of assessed countries froze tax rates for the rich while poverty levels increased, and many countries failed to raise minimum wages.
The report highlights Norway and Germany as top performers in actions taken to reduce inequality. Other well-performing nations include Australia, Belgium, and Canada. However, the report claims that HICs played a role in exacerbating inequality in LMICs by overseeing lender repayment demands despite the economic hardships imposed by the COVID-19 pandemic. Oxfam accused the International Monetary Fund (IMF) of worsening inequality by demanding new austerity measures to reduce budget deficits. One of the important lessons learned during the COVID-19 pandemic is that health inequality leaves the door open for new and more dangerous viral variants to develop and has the potential to mask the emergence of novel pathogens with pandemic potential. The world must address rapidly deteriorating equality levels to help prepare for and prevent the next pandemic.
SARS-COV-2 ORIGIN A panel of experts examining the origins of SARS-CoV-2—many of whom were originally convened as part of a task force for The Lancet COVID-19 Commission—this week reported their findings in the Proceedings of the National Academy of Sciences (PNAS). Like the Commission’s report, the PNAS analysis stresses the need to apply a One Health lens to help decrease the risk of disease spillover events and to make improvements in the safety of laboratory and field research. While the Commission’s report gave equal weight to theories supporting the virus naturally spilling over to humans and accidentally being leaked from a lab, the PNAS report concludes that increasing scientific evidence is most consistent with the theory that the COVID-19 pandemic began due to zoonosis from wildlife to humans via the wildlife trade or farming. To reach that conclusion, the researchers conducted a literature review, interviewed other experts, and examined major RNA virus outbreaks since 1967 to identify common features as well as opportunities to prevent novel disease emergence. Though the origin of SARS-CoV-2 has not yet been conclusively determined—and may never be—the authors of the PNAS paper say it is time to look beyond trying to answer that question and use lessons learned from the COVID-19 pandemic to improve upon future prevention and preparedness.
BIOSAFETY The COVID-19 pandemic has spurred plans to build more than 40 high-level biosafety laboratories in several nations, prompting concerns from researchers about how these new facilities—which many agree are needed—will obtain sustainable funding to handle dangerous pathogens safely and securely. India, Kazakhstan, Singapore, Philippines, Russia, and the United States plan to establish high-containment facilities. While some researchers question the need for so many new labs and their high operating costs, others maintain that new biosafety centers could lead to improved safety practices, allowing scientists to work more safely than they could without them.
by ti-amie Me after reading the section on US Public Health Measures.
by ponchi101 One thing that OXFAM has never understood about the IMF demands to reduce budget deficits.
3rd world economies do not work like the USA's or the EU's. When one of our countries reach a certain debt/GDP ratio, our economies implode. It is not like the USA, which can have a 2:1 Debt/GDP ratio and nothing happens. In S. America, our currencies immediately devalue and funds quickly find their way to offshore accounts, if our debt reaches a certain level. Greece imploded with just a 1:1 debt/GDP ratio.
And WE DON'T HAVE THE FUNDING to implement social networks, or pass laws to support health programs, because, again, if we run a deficit, our currencies melt. Sure, Chile had the money to buy F16 fighters a few years ago, and because Argentina has defaulted 9 times on previous debt, the premiums charged by the financial markets of their NEW debt are exorbitant and unpayable, but that is why we are a mess.
And I have yet to see any single country, or common market (MERCOSUR, for example) talking to the pharma giants to set up a vaccine manufacturing facility in the continent. Easier to rely on donations.
by dryrunguy
ponchi101 wrote: ↑Thu Oct 13, 2022 11:30 pm
One thing that OXFAM has never understood about the IMF demands to reduce budget deficits.
3rd world economies do not work like the USA's or the EU's. When one of our countries reach a certain debt/GDP ratio, our economies implode. It is not like the USA, which can have a 2:1 Debt/GDP ratio and nothing happens. In S. America, our currencies immediately devalue and funds quickly find their way to offshore accounts, if our debt reaches a certain level. Greece imploded with just a 1:1 debt/GDP ratio.
And WE DON'T HAVE THE FUNDING to implement social networks, or pass laws to support health programs, because, again, if we run a deficit, our currencies melt. Sure, Chile had the money to buy F16 fighters a few years ago, and because Argentina has defaulted 9 times on previous debt, the premiums charged by the financial markets of their NEW debt are exorbitant and unpayable, but that is why we are a mess.
And I have yet to see any single country, or common market (MERCOSUR, for example) talking to the pharma giants to set up a vaccine manufacturing facility in the continent. Easier to rely on donations.
Thank you, ponchi, for reminding me that what I read these things for are not necessarily what other people read them for.
There is, I assume, also a point to be made here regarding to what other countries South American countries are indebted.
by ponchi101 Sure. One the reasons the US debt is not so "detrimental" is because a lot of the debt is held by American institutions. In a sense, the US debt is held by America (although other countries also buy American Treasury Bonds).
This is not related to C19, but an example. In Argentina, the Social & Health system is based on companies called AFJP (an acronym for retirement funds). During the Nestor Kirchner presidency, the administration issued a considerable amount of bonds, to be paid (as expected) in a certain time (10 years). Many of the AFJP's bought this debt, as it seemed like a solid investment. The bonds were traded internationally and well received.
Then, the bonds matured, and the Cristina Kirchner presidency went into default; this lead to most of the AFJP's to go belly up, taking with them the savings of hundreds of thousands of Argentineans. Because the AFJP's were the solid part of the retirement/health system, major companies had their health benefits and insurance policies managed by a given AFJP. Well, those savings were lost. And all this was due to Argentina's default. The bonds started to trade as low as 2% of their face value, as it was impossible to collect, so big international brokerage houses bought them, knowing they had the financial muscle to make the Argentinean government pay. Or at least, pay more than the 2% they funds have bought them for.
These funds were called in Argentina "Vulture Funds", because the government started saying the funds were the ones trying to scrape the "meat off the bones" of the Argentinean economy. The fact that the bonds had dropped 98% in value due to the government's default took a while to percolate down to the population.
And I read these C19 reports for all they have; they have been very valuable. But that section in there was the sole I could comment about. The rest, to me, are facts. I am frequently left like the man in Ti's GIF.
by Deuce I don't like the sensationalistic headline (so I replaced it)...
I find that the article is good and informative, though.
by dryrunguy Here's the latest Situation Report. I have questions about the Boston study.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 623 million cumulative cases and 6.55 million deaths worldwide as of October 19. Global weekly incidence again remained steady at slightly more than 3 million cases for the sixth consecutive week, decreasing only 0.87% compared to the previous week. Weekly incidence in Europe remained relatively steady over the previous week, falling 3% after steady increases for the previous 4 weeks. Weekly incidence increased 11% in the Western Pacific, while all other regions reported decreasing trends. Global weekly mortality continued to decrease for the ninth consecutive week, down 15% from the previous week.
UNITED STATES
The US CDC is reporting 96.8 million cumulative cases of COVID-19 and 1.06 million deaths. Daily incidence continues to decline, down to 37,052 new cases per day, the lowest average since mid-April. Average daily mortality also continues to decline, down to 323 deaths per day on October 18.**
**Changes in state-level reporting may affect the accuracy of recently reported data, particularly over weekends. In an effort to reflect the longer-term trends, the numbers reported here may not correspond to the most recent dates.
Both new hospital admissions and current hospitalizations continue to exhibit downward trends, with decreases of 1.8% and 3.3%, respectively, over the past week. Both trends peaked around the end of July, although the decreasing trend appears to be leveling.
The BA.5 sublineage continues to be the dominant strain in the US, accounting for 67.9% of sequenced specimens; however, its estimated prevalence has decreased for 8 consecutive weeks. Notably, the BA.4.6 sublineage (12.2%) appears to be losing its growth advantage to others, including BQ.1 (5.7%), BQ.1.1 (5.7%), and BF.7 (5.3%). BA.2.75.2 (1.4%) and BA.2.75 (1.3%) also show relative growth advantage over BA.5.
IMMUNE EVASIVE OMICRON SUBVARIANTS While past surges in COVID-19 cases have been driven largely by single SARS-CoV-2 variants, experts are eyeing a collection of Omicron subvariants that could drive an anticipated wave of infections this fall and winter. In the US, BA.4.6 appeared to be gaining momentum, although BF.7, BQ.1, and BQ.1.1 are showing recent potential growth advantage. The same sublineages are also showing evidence of growth advantage over BA.5 in the United Kingdom. Additional variants, including the recombinant variant XBB, are fueling increases in cases in Southeast Asia and Europe. The US has yet to see a large surge due to these subvariants, with the number of new cases continuing to drop. But public health experts warn data on new cases is unreliable—many are turning to wastewater surveillance to help predict where and when surges may occur—and most expect the downward trend to reverse over the next few weeks. The collection of variants, sometimes referred to as “scrabble variants” or “subvariant soup,” accounts for nearly 1 in 3 new infections reported in the US last week. Globally, detecting these variants and developing accurate assessments of the risk they pose to public health is challenging, as many countries have rolled back their surveillance efforts.
While available vaccines remain effective in preventing severe illness and death from COVID-19, there are concerns the emerging subvariants will be more immune evasive than previous variants, particularly due to mutations in the receptor binding domain that would prevent antibodies from docking and attacking the virus. AstraZeneca’s EvuSheld, the only monoclonal antibody authorized to prevent SARS-CoV-2 infection, is ineffective against BA.4.6. Other monoclonal antibodies in development already demonstrate vulnerabilities to newly emerging Omicron subvariants. With this new information, the Biden administration is searching for other potential candidates for use among immunocompromised persons.
US RESPONSE With public vigilance waning and the hopes of new pandemic funding from the US Congress fading, the COVID-19 response in the US is entering a new and uncertain phase. Omicron subvariants remain the predominant circulating lineages, many with high levels of transmissibility and immune evasion. Most places have completely dropped public health measures meant to mitigate transmission, and fewer and fewer Americans are wearing masks indoors or in crowded public spaces. With lower vaccine demand and less federal funding, vaccine manufacturers must soon decide whether and how high to price vaccines and boosters moving forward. While people with health insurance likely will continue to be able to access free or low-cost COVID-19 vaccines and therapies, those who are uninsured or underinsured potentially could lose no-cost access, a factor that would exacerbate underlying inequities. One factor influencing when COVID-19 tools will be commercialized is when the public health emergency declaration ends; however, the Biden administration last week extended the public health emergency for another 90 days, into January 2023, ahead of an expected potential winter surge. This decision aligns with a recent statement from the WHO reinforcing that COVID-19 very much remains a global emergency and calling for nations to sustain efforts to fight against its spread. Still, the US likely will end its public health emergency in 2023, when it will significantly cut back on certain components of its COVID-19 response.
Notably, efforts are underway to prevent such a situation from happening again in the future. On October 18, US President Joe Biden signed a National Security Memorandum to launch the administration’s “National Biodefense Strategy and Implementation Plan for Countering Biological Threats, Enhancing Pandemic Preparedness, and Achieving Global Health Security.” The strategy calls for US$88 billion in funding over the next 5 years to strengthen key areas of pandemic preparedness and biodefense. The strategy will also bring together key government sectors to support its implementation, including the White House, the Intelligence Community, the US Department of State, and the US HHS.
GAIN-OF-FUNCTION STUDY A laboratory at Boston University has come under criticism for its recent gain-of-function experiments on the SARS-CoV-2 virus. Gain-of-function (GOF) refers to laboratory experiments that strategically and specifically enhance the function of one or more genes to study the outcome. They can range from something as simple as overactivating an important enzyme to enhancing the pathogenicity of a virus. In the Boston University (BU) experiments, performed at the BSL-3 level, the original strain of SARS-CoV-2 was modified to contain Omicron variant spike proteins with the aim of studying why some strains of SARS-CoV-2 are more pathogenic and transmissible than others. This work was reviewed internally by the BU institutional review board (IRB) and externally by the Boston Public Health Commission but not by the US NIH or NIAID, which were partial funders. NIH is currently launching a probe to evaluate whether this experiment should have been subject to federal oversight and review before moving forward. BU maintains that the research was not directly funded by the NIH and therefore there was no wrongdoing in not alerting them before beginning the experiment. The federal government takes GOF research very seriously, especially for those manipulating pathogens with potential pandemic potential, as SARS-CoV-2 certainly is. Even before the lab-leak hypothesis of SARS-CoV-2 origins, there was a large amount of controversy surrounding how and when to allow GOF research to move forward.
However, BU refutes that this experiment even should be considered as gain-of-function and maintain that they actually made a less dangerous version of the virus. The school criticized the initial media reports of the experiment, saying they were highly sensationalized; several outlets stressed the study’s finding that the altered strain caused 80% mortality in mice with severe disease, but that proportion is in line with experiments using unaltered SARS-CoV-2. Still, the finding that the resulting strain was less pathogenic does not alter the fact that the methods used fall within the definition of GOF research. Many biosecurity experts have come forward to disagree with BU’s characterization of their research and reiterate that this was in fact GOF research. The NIH inquiry and the renewed conversation among the scientific community will hopefully spur greater understanding and consensus around the risks and benefits of GOF research, in addition to institutionalizing the use of greater safeguards when conducting research with pathogens of pandemic potential.
LIFE EXPECTANCY & PREGNANCY-RELATED MORTALITY The COVID-19 pandemic interrupted decades worth of gains in global life expectancy. According to a study published October 17 in Nature Human Behaviour examining life expectancy losses during the pandemic, those countries that had higher proportions of their populations vaccinated by October 2021 experienced smaller life expectancy deficits in winter 2021. Of the 29 countries included in the analysis, most countries in Western Europe bounced back relatively well from life expectancy losses while most countries in Eastern Europe, the United States, and Chile experienced continuing declines in their pre-pandemic life expectancy. All nations had lower life expectancy than would be expected if pre-pandemic trends had continued. According to data from the US CDC, US life expectancy fell by a total of 2.6 years between 2019 and 2021 to 76.1 years, the lowest level since 1996.
In the US, COVID-19 contributed to about 25% of the more than 2,000 maternal deaths in 2020 and 2021, according to a report published by the US Government Accountability Office. Pregnant people are more vulnerable to severe COVID-19 outcomes, the US CDC has warned. Since 2018, maternal deaths have increased nearly 80%, with COVID-19 associated with 401 of the 1,178 pregnancy-related deaths last year. Additionally, racial and ethnic disparities widened; pregnancy-related deaths among Black people climbed from 44 per 100,000 in 2019 to 68.9 per 100,000 in 2021, rose from 12.6 per 100,000 in 2019 to 27.5 last year for Hispanic individuals, and increased from 17.9 in 2019 to 26.1 in 2021 for White people. Many factors contributed to the increase in maternal deaths, including the emergence of the Delta variant, mental health, lack of access to medical care, and low vaccination rates among pregnant people, among others. Experts note that many of these deaths were preventable, highlighting the urgent need to find solutions.
US CDC VACCINES FOR CHILDREN PROGRAM The US CDC Advisory Committee on Immunization Practices (ACIP) on October 19 recommended that vaccines against COVID-19 be included in the CDC Vaccines for Children program, which provides no-cost vaccines for a variety of diseases to children and adolescents aged 18 and younger whose families cannot afford them. Children are eligible for the program if they qualify for Medicaid, or are uninsured, underinsured, or Native American. The panel of independent advisors voted unanimously to include COVID-19 vaccines in the program to ensure these children can receive the shots for free after the federal government shifts the vaccination program to the commercial market. When the Biden administration decides to end the COVID-19 public health emergency—which it extended again last week—more than 5 million children are expected to lose health insurance under federal programs.
During the meeting, the panel emphasized they were not voting on adding COVID-19 vaccines to the CDC annual vaccination schedule, although a meeting to consider doing is taking place today. While the CDC decides a recommended vaccination schedule for children based on age, US states decide which vaccines are mandatory for entry into schools. Nonetheless, the CDC had to push back on a Fox News contributor who amplified a false claim that the CDC was set to mandate COVID-19 vaccines for schoolchildren. Public health experts agree there is legitimate debate over whether school-aged children should be required to receive the vaccines but warned the erroneous claim represents another example of how quickly misinformation can spread and potentially harm children, erode trust in federal health institutions, or endanger health officials. Experts also agree more states and localities will require children be vaccinated to attend the upcoming 2023 school year.
NOVAVAX BOOSTER On October 19, the US FDA authorized Novavax’s monovalent, protein-based COVID-19 vaccine as a booster for adults. The Novavax booster targets only the original coronavirus strain, although the company is concurrently studying an Omicron-targeting vaccine, in addition to a bivalent booster. The US CDC recommended the monovalent product for use among adults aged 18 years and older who have not yet received any COVID-19 booster but who have completed a primary series vaccination with any authorized or approved vaccine at least 6 months prior. The authorization offers another option for individuals who cannot or are reluctant to receive one of the bivalent mRNA vaccine boosters, or for those who would otherwise not receive a booster.
MODERNA OMICRON BOOSTERS Moderna’s bivalent Omicron-containing booster (mRNA-1273.214), administered as a fourth vaccine dose, produced a stronger immune response to Omicron BA.1 compared to its original booster dose at 90 days, according to the company. Additionally, the updated booster elicited a significantly higher neutralizing antibody response against Omicron BA.4/BA.5 compared to the original version at 28 days, suggesting the booster can produce broad cross-neutralization against Omicron subvariants. Moderna’s BA.1 bivalent booster is central to fall and winter vaccination campaigns in the UK. The company expects to announce interim immunogenicity results of its Omicron BA.4/BA.5-targeting bivalent vaccine (mRNA-1273.222), which is authorized for use in the United States, later this year. It is unclear how well either booster will work against newly emerging Omicron sublineages—including BQ.1.1, XBB, BF.7, and BA.2.75.2—which are expected to be more immune evasive than their older relatives and expected to cause COVID-19 surges in several nations through the end of this year and into the next.
Moderna also announced this week it will work with Gavi, the Vaccine Alliance, to supply more than 100 million doses of its Omicron-adapted bivalent vaccines for purchase at its lowest-tier pricing in 2023 to the COVAX Advance Market Commitment (AMC). Under the new framework, pending orders for Moderna’s original SARS-CoV-2 vaccine will be canceled, and COVAX will instead offer the newer vaccines to low- and middle-income countries (LMICs), which can use them as they see fit. COVAX has delivered nearly 1.8 billion doses of vaccines for COVID-19 to 146 countries, overcoming a rough start to obtain vaccine doses due to hoarding by wealthier nations. Dr. Mike Ryan, executive director of the WHO Health Emergencies Programme, this week at the World Health Summit harshly criticized wealthy nations and pharmaceutical companies for failing to adequately share vaccine doses through COVAX.
by ponchi101 We should also talk about C19 HOAX news.
My looney friend N sent me a tweet (he does not understand that I am averse to tweeter, except when filtered by Ti and other fellow TAT'ers) from Rob Roos, a dutch EU parliament member, who "proved" that pfizer et al "manipulated" the info to promote the vaccine. In reality, the vaccine "skipped" a few testing steps; that was what the emergency use approval was for.
So, his entire sphere (my friend's) is up on arms, because "criminal" Fauci and all these other companies (his literal word) forced us to get this "poison" (quote).
So difficult. We are playing some padel on Saturday, with two more anti-vaxxers/anti-science/anti-corporation people. I may not survive
by ti-amieWhites now more likely to die from covid than Blacks: Why the pandemic shifted
By Akilah Johnson and Dan Keating
October 19, 2022 at 6:00 a.m. EDT
SOMERVILLE, Tenn. — Skill Wilson had amassed more than three decades of knowledge as a paramedic, first in Memphis and then in Fayette County. Two places that felt like night and day.
With only five ambulances in the county and the nearest hospital as much as 45 minutes away, Skill relished the clinical know-how necessary to work in a rural setting. Doing things like sedating patients to insert tubes into their airways.
But when it came to covid-19, despite more than 1 million deaths nationwide, Skill and his family felt their small town on the central-eastern side of Fayette County, with its fields of grazing cattle and rows of cotton and fewer than 200 covid deaths since the start of the pandemic, was a cocoon against the raging health emergency.
“It was a lot easier to stay away from others,” his widow, Hollie Wilson, said of the largely White and predominantly conservative county of about 42,000 residents. “Less people. Less chance of exposure.”
Covid seemed like other people’s problems — until it wasn’t.
The imbalance in death rates among the nation’s racial and ethnic groups has been a defining part of the pandemic since the start. To see the pattern, The Washington Post analyzed every death during more than two years of the pandemic. Early in the crisis, the differing covid threat was evident in places such as Memphis and Fayette County. Deaths were concentrated in dense urban areas, where Black people died at several times the rate of White people.
“I don’t want to say that we weren’t worried about it, but we weren’t,” said Hollie, who described her 59-year-old husband as someone who “never took a pill.” After a while, “you kind of slack off on some things,” she said.
Over time, the gap in deaths widened and narrowed but never disappeared — until mid-October 2021, when the nation’s pattern of covid mortality changed, with the rate of death among White Americans sometimes eclipsing other groups.
A Post analysis of covid death data from the Centers for Disease Control and Prevention from April 2020 through this summer found the racial disparity vanished at the end of last year, becoming roughly equal. And at times during that same period, the overall age-adjusted death rate for White people slightly surpassed that of Black and Latino people.
The nature of the virus makes the elderly and people with underlying health conditions — including hypertension, diabetes and obesity, all of which beset Black people at higher rates and earlier in life than White people — particularly vulnerable to severe illness and death.
That wasn’t Skill.
The virus also attacks unvaccinated adults — who polls show are more likely to be Republicans — with a ferocity that puts them at a much higher risk of infection and death.
That was Skill.
He joined the choir of critics opposing vaccination requirements, his rants in front of the television eventually wearing on Hollie, who, even if she agreed, grew tired of listening and declared their home “covid-talk free.”
So, she said, Skill commiserated with like-minded people in Facebook groups and on Parler and Rumble, the largely unmoderated social networking platforms popular with conservatives.
“We’re Republicans, and 100 percent believe that it’s each individual’s choice — their freedom” when it comes to getting a coronavirus shot, Hollie said in January. “We decided to err on the side of not doing it and accept the consequences. And now, here we are in the middle of planning the funeral.”
Capt. Julian Greaves Wilson Jr., known to everybody as Skill, died of covid Jan. 23, a month after becoming infected with the coronavirus. He fell ill not long after transporting a covid patient to the hospital. At the time he died, infection rates in Fayette County had soared to 40.5 percent among people taking coronavirus tests.
‘A different calculus’
Unequal exposure, unequal spread, unequal vulnerability and unequal treatment concentrated harm in communities that needed protection the most yet had the least. Cumulatively, Black, Latino and Native American people are 60 percent more likely to die of covid.
But as the pandemic progressed, the damage done by the virus broadened, and the toxicity of modern-day politics came to the fore.
The Post analysis revealed the changing pattern in covid deaths. At the start of the pandemic, Black people were more than three times as likely to die of covid as their White peers. But as 2020 progressed, the death rates narrowed — but not because fewer Black people were dying. White people began dying at increasingly unimaginable numbers, too, the Post analysis found.
In summer 2021, the nation saw some of the pandemic’s lowest death rates, as vaccines, shoring up the body’s immune response, became widely available.
Then came the delta variant. The virus mutated, able to spread among the vaccinated. As it did, an erosion of trust in government and in medicine — in any institution, really — slowed vaccination rates, stymieing the protection afforded by vaccines against severe illness and death.
After delta’s peak in September 2021, the racial differences in covid deaths started eroding. The Post analysis found that Black deaths declined, while White deaths never eased, increasing slowly but steadily, until the mortality gap flipped. From the end of October through the end of December, White people died at a higher rate than Black people did, The Post found.
That remained true except for a stretch in winter 2021-2022, when the omicron variant rampaged. The Black death rate jumped above White people’s when the spike in cases and deaths overwhelmed providers in the Northeast, resulting in a bottleneck of testing and treatment.
When the surge subsided, the Black death rate once again dropped below the White rate.
“Usually, when we say a health disparity is disappearing, what we mean is that … the worse-off group is getting better,” said Tasleem Padamsee, an assistant professor at Ohio State University who researched vaccine use and was a member of the Ohio Department of Health’s work group on health equity. “We don’t usually mean that the group that had a systematic advantage got worse.”
(...)
The shift in covid death rates “has vastly different implications for public health interventions,” said Nancy Krieger, professor of social epidemiology at Harvard University’s T.H. Chan School of Public Health. Officials must figure out how to connect with “communities who are ideologically opposed to the vaccine” while contending with “the cumulative impact of injustice” on communities of color.
“Think about the fact that everyone who is age 57 and older in this country was born when Jim Crow was legal,” she said. “What that did was intersect with covid-19, meaning that embodied history is part of this pandemic, too.”
So what contributed to the recent variation in death rates? And why?
The easy explanation is that it reflects the choices of Republicans not to be vaccinated, but the reasons go deeper. The Post interviewed historians and researchers who study the effects of White racial politics and social inequality on health, spoke with relatives and friends of those lost to covid, and compiled data from federal databases and academic studies.
What emerged is a story about how long-standing issues of race and class interacted with the physical and psychological toll of mass illness and death, unprecedented social upheaval, public policies — and public opinion.
Resilience gave way to fatigue. Holes left by rural hospital closures deepened. Medical mistrust and misinformation raged. Skeptics touted debunked alternatives over proven treatments and prevention. Mask use became a victim of social stigma.
Many Republicans decided they would rather roll the dice with their health than follow public health guidance — even when provided by President Donald Trump, who was booed after saying he had been vaccinated and boosted.
Researchers at Ohio State found Black and White people were about equally reluctant to get the coronavirus vaccine when it first became available, but Black people overcame that hesitancy faster. They came to the realization sooner that vaccines were necessary to protect themselves and their communities, Padamsee said.
As public health efforts to contain the virus were curtailed, the pool of those most at risk of becoming casualties widened. The No. 1 cause of death for 45-to-54-year-olds in 2021 was covid, according to federal researchers.
After it became clear that communities of color were being disproportionately affected, racial equity started to become the parlance of the pandemic, in words and deeds. As it did, vaccine access and acceptance within communities of color grew — and so did the belief among some White conservatives, who form the core of the Republican base, that vaccine requirements and mask mandates infringe on personal liberties.
“Getting to make this decision for themselves has primacy over what the vaccine could do for them,” said Lisa R. Pruitt, a law professor at the University of California at Davis who is an expert in social inequality and the urban-rural divide. “They’re making a different calculus.”
It’s a calculation informed by the lore around self-sufficiency, she said, a fatalistic acceptance that hardships happen in life and a sense of defiance that has come to define the modern conservative movement’s antipathy toward bureaucrats and technocrats.
“I didn’t think that that polarization would transfer over to a pandemic,” Pruitt said.
It did.
A lifesaving vaccine and droplet-blocking masks became ideological Rorschach tests.
(...)
The impulse to frame the eradication of an infectious disease as a matter of personal choice cost the lives of some who, despite taking the coronavirus seriously, were surrounded by enough people that the virus found fertile terrain to sow misery. That’s what happened in northern Illinois, where a father watched his 40-year-old son succumb to covid-19...
Stress, and its burden
While almost three years of chaotic public health crises have left Americans of all races uncertain about the future, they have also revealed the enduring nature of racial and class politics — and the cost they exact, including for White Americans.
Those triggers are layered upon each other, stoking stress, said Derek M. Griffith, who co-leads the Racial Justice Institute and directs the Center for Men’s Health Equity at Georgetown University.
“Whether it’s ‘I can’t pay my rent and mortgage as easily as I used to,’ or ‘I want to show I’m not worried about covid,’ your body doesn’t care where the stress is coming from. It’s just experiencing stress,” he said. “Then add to that how people are coping with the stress.”
When it comes to racism, most people think of something that occurs between individuals. But it’s as much about who has access to power, wealth and rights as it is about insults, suspicion and disrespect. Prejudice and discrimination, even if unconscious, can be deadly — and not just for the intended targets.
(,,,)
Perhaps...explaining covid’s unequal burden as part of an enduring legacy of inequality “signaled these disparities were not just transitory epidemiological trends, which could potentially shift and disproportionately impact White people in the future.”
Translation: Racial health disparities are part of the status quo.
Us vs. them
Questions about the government’s role in ensuring the public’s health and well-being hang heavy with historical inflections in states such as Tennessee, once home to the president who argued that Reconstruction-era legislation to help and protect newly freed enslaved people violated states’ rights.
And so in many ways, the roots of the consternation over recent pandemic-control measures began sprouting a century and a half earlier.
But that hasn’t stopped people such as Civil Miller-Watkins from wondering why those roots are choking so many now.
The former Fayette County school board member, who possesses an abiding belief in the power of the common good, said she finds the mind-set “I know what’s good for me, and if it’s harmful for you, you’re going to have to deal with it” worrisome amid a pandemic.
“Living in a rural county is not for the faint of heart, especially as a Black person,” the 56-year-old said. Still, she can’t help but wonder, “if I’m the same neighbor you give sugar to, and you know I have an 84-year-old in my house and a little-bitty baby at home, why wouldn’t you wear a mask around me?”
It’s a question that dogged her over Christmas when two of her grandchildren were infected with the coronavirus days before they were scheduled to be vaccinated.
“We put it on Republicans and politics,” she said, “but I think we should dig deeper.”
That’s what Jonathan M. Metzl, director of Vanderbilt University’s Department of Medicine, Health, and Society, did for six years while researching his book “Dying of Whiteness: How the Politics of Racial Resentment is Killing America’s Heartland.”
Published in 2019, it is a book about the politicization of public health and mistrust of medical institutions. It is a story about how communal values take a back seat to individuality. It’s an exploration of disinformation and how the fear of improving the lives of some means worsening the lives of others.
“I didn’t know it at the time, but I was writing a prehistory of the pandemic,” Metzl said in an interview. “You’re seeing a kind of dying-of-Whiteness phenomenon in the covid data that’s very similar to what I saw in my data.”
Metzl and Griffith, a Vanderbilt professor at the time, conducted focus groups on the Affordable Care Act throughout middle Tennessee including White and Black men who were 20 to 60 years old. Some were small-business owners and security guards. Others were factory workers and retirees.
The divergent medical experiences of Black and White patients permeated Metzl’s focus groups, particularly when the conversation veered toward the politics of health and government’s role in promoting well-being.
“Black men described precisely the same medical and economic stressors as did White men and detailed the same struggles to stay healthy,” Metzl wrote. “But Black men consistently differed from White men in how they conceived of government intervention and group identity. Whereas White men jumped unthinkingly to assumptions about ‘them,’ Black men frequently answered questions about health and health systems through the language of ‘us.’ ”
Tennessee has yet to expand Medicaid under the ACA, a decision fueling rural hospital closures at a rate that eclipses nearly every other state because there isn’t enough money to keep the doors open. Not only would expanding Medicaid have saved hospitals, Metzl wrote, it would have saved thousands of lives — White and Black.
Metzl said watching the pandemic unfold felt like a flashback to past battles over federal health-care reform. Messaging that leaned into quantitative data about masks and vaccines sounded eerily similar to the mistakes made, “at least for this part of the country,” with the ACA, he said.
“The minute public health infrastructure started to talk about the statistical public health benefits of the mask” and not how everyone needed to be on the same page to stay safe, Metzl said, “I just knew that it was going to open a door for the same kind of anti-ACA stuff, which is ‘the government’s telling you what to do.’ ”
As Metzl conducted research for his book in 2016, a 41-year-old uninsured Tennessean named Trevor who was jaundiced and in liver failure told him “I would rather die” than sign up for the ACA. When asked why, Trevor, who was identified by first name only, said: “We don’t need any more government in our lives. And in any case, no way I want my tax dollars paying for Mexicans or welfare queens.”
Now during the pandemic, there are people like 39-year-old Chad Carswell of North Carolina whose kidneys functioned recently at just 3 percent. He was denied a new kidney in January after refusing to take a coronavirus vaccine as required for the transplant at the time, saying: “I was born free. I’ll die free.”
Much like protests to “repeal and replace” the ACA, Metzl said rejecting public health measures is about dogma more so than a mistrust of the science of vaccines or masks.
“We’ve oversimplified this with morality tales about the vaccine is good, and anti-vaxxers are bad, and they’re automatically racist,” Metzl said. “Being anti-vaccine or anti-mask is part of an ideology. When people get more desperate, they get more ideological.”
ponchi101 wrote: ↑Thu Oct 20, 2022 7:24 pm
We should also talk about C19 HOAX news.
My looney friend N sent me a tweet (he does not understand that I am averse to tweeter, except when filtered by Ti and other fellow TAT'ers) from Rob Roos, a dutch EU parliament member, who "proved" that pfizer et al "manipulated" the info to promote the vaccine. In reality, the vaccine "skipped" a few testing steps; that was what the emergency use approval was for.
So, his entire sphere (my friend's) is up on arms, because "criminal" Fauci and all these other companies (his literal word) forced us to get this "poison" (quote).
So difficult. We are playing some padel on Saturday, with two more anti-vaxxers/anti-science/anti-corporation people. I may not survive
You posted this while I was posting the WaPo article. It's all very sobering.
by dryrunguy Here's the latest Situation Report.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 625.7 million cumulative cases and 6.56 million deaths worldwide as of October 26. Global weekly incidence dropped to 2.8 million new cases after remaining steady for 6 weeks, decreasing 12.5% compared to the previous week. Weekly incidence in all regions remained relatively steady or fell over the previous week. Global weekly mortality continued to decrease for the tenth consecutive week, down 11.6% from the previous week.*
*The WHO dashboard notes that data from the Africa Region are incomplete.
UNITED STATES
The US CDC is reporting 97.1 million cumulative cases of COVID-19 and 1.07 million deaths. Incidence for the week ending October 19 remained steady over the previous week, at 260,808 reported cases. Weekly mortality also remained steady for the week ending October 19, at 2,566 reported deaths.**
**Beginning October 20, the US CDC began reporting and publishing aggregate case and death data, and line level data where applicable, from jurisdictional and state partners on a weekly basis rather than daily. As a result, COVID-19 data on cases and deaths are updated every week on Thursdays by 8pm ET.
New hospital admissions remained steady last week, increasing 1.1%, while current hospitalizations continued to exhibit a downward trend, decreasing 2.9% over the past week. Both trends peaked around the end of July and both now appear to be leveling.
The BA.5 sublineage continues to be the dominant strain in the US, accounting for 62.2% of sequenced specimens; however, its estimated prevalence has decreased for 9 consecutive weeks. The second most prevalent sublineage, BA.4.6, appears to be losing its growth advantage to others, decreasing to 11.3% as of October 22. Several other Omicron sublineages continue to exhibit increasing trends, including BQ.1 (9.4%), BQ.1.1 (k7.2%), and BF.7 (6.7%). BA.2.75 (1.6%) and BA.2.75.2 (1.3%) and also show relative growth advantage over BA.5.
GLOBAL PANDEMIC PROJECTIONS The number of new daily global COVID-19 cases is projected to rise slowly over the coming months, increasing from about 17 million now to about 18.7 million by the end of January 2023, the University of Washington Institute for Health Metrics and Evaluation predicts in an analysis published this week. The increase will be impacted by the emergence of various Omicron lineage subvariants, seasonal behavioral changes, and COVID-19 policies in China, where many of the world’s most susceptible population resides. The model’s reference scenario also estimates 245,000 additional reported deaths due to COVID-19 will occur through February 1. The analysis also includes estimates using an 80% mask use scenario and an antiviral access scenario.
‘TRIPLEDEMIC’ Experts in the US are warning the nation could see a convergence of three respiratory diseases—COVID-19, influenza (flu), and respiratory syncytial virus (RSV)—this fall and winter, in what some are calling a “tripledemic.” There are signs that cases of all three infections are rising in parts of the country, likely driven by people feeling confident enough to stop wearing masks and gather more indoors. Newly emerging sublineages of the Omicron variant of concern (VOC) have mutations that potentially make them resistant to existing therapeutics and preventive treatments and possibly immune evasive enough to bypass protections provided by previous infections or vaccination. That is leading the US government to step up efforts to get more people vaccinated and boosted with newer bivalent shots that target the Omicron BA.5 and BA.4 lineages.
Cases of RSV are surging earlier than usual, especially among young children. While many kids contract the virus by age 2 through mingling with other children, there is a potential that nonpharmaceutical interventions—such as lockdowns, social distancing, masking, and increased hygiene—helped to limit the spread of other respiratory diseases, essentially creating an “immunity gap.” Therefore, some toddlers and infants have never been exposed to RSV, leaving them more susceptible to infections. Notably, there is no vaccine and no effective treatment for RSV. Most people recover within a week or two, but RSV can be serious for young children and older adults who have weaker immune systems or underlying health conditions. Already, about three-quarters of pediatric hospital beds nationwide are full and emergency rooms are experiencing long waits.
Additionally, some parts of the country, especially Southern states, are experiencing an early flu season. Flu rates are highest among young children aged 0-4, but the number of cases is increasing in every age group. The past two years saw lower-than-average numbers of cases, and though there is a flu vaccine, protection rates range from 20%-60%. And, unfortunately, flu vaccine uptake dropped during the pandemic. The Southern Hemisphere saw an early flu season with higher case numbers and higher hospitalizations, and many feel nations in the Northern Hemisphere will follow that trend as the weather cools. With hundreds of circulating SARS-CoV-2 variants and increases of other respiratory viruses, taking steps to prevent disease transmission—including getting vaccinated and/or boosted, staying home if sick, wearing masks, and washing hands—remains vital this season to help prevent further strain on the healthcare system, severe disease, and more deaths.
US BOOSTER CAMPAIGN As the US heads into its third winter of the COVID-19 pandemic, US health officials this week announced additional efforts to encourage individuals, particularly those who are older or immunocompromised, to get vaccinated or boosted against COVID-19 at no cost. US President Joe Biden publicly received his fifth shot, coinciding with the release of an updated COVID-19 plan that includes enlisting Walgreens, DoorDash, and Uber to provide free delivery of antiviral prescriptions, calling on educational institutions to hold vaccination clinics for their communities, encouraging employers to provide paid time off for employees to get vaccinated, and urging building operators to improve indoor air quality.
The US appears to be in a better position heading into this winter, with treatments and vaccine doses more widely available, but Biden administration officials are concerned another surge in cases, as well as rising cases of other respiratory diseases, could overwhelm healthcare systems and lead to more deaths. Some experts are concerned a crisis-fatigued public and mixed pandemic messaging are making booster campaign efforts more challenging; only about 19.4 million US residents have gotten the updated shot, accounting for less than 10% of those who are eligible, according to US CDC data. The Omicron subvariants BQ.1 and BQ.1.1 are gaining ground in the US, and for those already vaccinated, receiving an updated booster dose is the best protection from severe disease or death. While some might not look forward to vaccination side effects, a study published October 21 in JAMA Network Open suggests those who experience fever, chills, or muscle pain tended to have more robust antibody responses following the shots. But don’t worry: even among those who experience little to no side effects, vaccines elicit a strong immune response.
BIVALENT BOOSTER IMMUNE RESPONSE Early data on the immunogenicity of the new bivalent booster targeting the Omicron BA.4 and BA.5 Omicron sublineages show the shots appear to work about as well as earlier monovalent booster doses. The two preprint studies—one from researchers from Harvard University and the other from Columbia University—show that neutralizing antibody responses to the bivalent vaccine formulation were about the same as those to the monovalent vaccine formulation when examined 3-5 weeks post-vaccination. Researchers emphasized, however, that the boosters still offer robust and prolonged protection against severe disease or death from COVID-19, and public health officials continue to encourage people to get boosted as soon as possible. Some experts suggested that the studies were not run for a long enough time and included too small of a population to provide a full picture of bivalent vaccine booster immunogenicity.
US COVID DEATH RATES A data brief published October 25 by the National Center for Health Statistics (NCHS) analyzed COVID-19 mortality rates in 2020, illuminating demographic trends early on in the outbreak according to urbanicity, age, and sex. The report’s findings noted that overall age-adjusted COVID-19 death rates ranked highest to lowest were found in large central metropolitan urban counties, noncore rural counties, micropolitan rural counties, large fringe metropolitan urban counties, small metropolitan urban counties, and medium metropolitan urban counties. When broken down by sex, geographic trends remained largely similar, although the highest death rates for women were found in noncore rural counties and the second highest death rates found in large central metropolitan urban counties. Notably, death rates were at least 50% higher for men than women across all counties, with the greatest difference found in large central metropolitan urban counties, where rates were 78% higher for men.
Another data brief by NCHS found that this trend was further exacerbated in adults aged 65 and older, with males experiencing death rates 1.5 times higher than females. Sex differences in COVID-19 death rates in adults aged 65 and over held across all races. Death rates in older men were highest among Hispanic men, followed by non-Hispanic Black men and non-Hispanic American Indian or Alaska Native men. Death rates among older women were highest among non-Hispanic American Indian or Alaska Native women, followed by non-Hispanic Black women and Hispanic women. As has been well-established in other studies, overall COVID-19 death rates increased by age group in adults aged 65 and older. The majority (66.2%) of deaths due to COVID-19 among these older adults occurred in a healthcare setting, compared with 24.3% in a nursing home or long-term care facility, and 4.7% at home.
US WORKFORCE The COVID-19 pandemic has significantly impacted the US workforce, particularly due to the burden of post-acute sequelae of SARS-CoV-2 (PASC), more commonly known as long COVID. Some estimates posit that the economic costs of long COVID could be trillions of dollars. With an estimated 16 million people of working age suffering with long COVID, and as many as 4 million out of work because of their symptoms, many recognize COVID-19 as a mass disabling event. A recent study from the Federal Reserve Bank of New York notes there has been an increase of about 1.7 million people with disabilities since the pandemic began and close to 1 million workers with new disabilities, likely due to an increase in Americans living with long COVID.
Many people with long COVID have reduced the number of hours they work or dropped out of the labor force, but an increase in the number of workers with disabilities suggests that more people with long COVID and disabilities are continuing to work. Some experts believe that the surge of workers with disabilities could also be attributed to a tight labor market and a rise in remote work, which allows people with disabilities to enter and remain in the workplace. As more people with long COVID and disabilities enter and remain in the workplace, experts encourage employers to make reasonable workplace accommodations to retain them. Advocates encourage employers to set a positive example by supporting their employees’ needs regardless of their status under the Americans with Disabilities Act, under which employers are expected to make “reasonable accommodations” for people with disabilities.
Similar to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)— which also often follows viral infection—symptoms of long COVID can include fatigue, brain fog, and muscle/joint pain. The accommodations employers have provided to workers with ME/CFS, such as telework and flexible scheduling, could be extended to workers with long COVID as well, along with other changes that allow workers to control their environment, limit physical exertion and commuting, take breaks as needed, manage symptoms, and access comprehensive health benefits. Although making workplace accommodations requires upfront costs, advocates encourage employers to consider the long-term benefits of creating flexible and inclusive policies.
Relatedly, a recent study from the National Bureau of Economic Research illustrated the phenomenon of “long social distancing” and documented that anxiety around getting COVID-19 has kept close to 3 million people out of the workforce, consequently reducing potential economic output by nearly 1%, or US$250 billion, in the first half of 2022. Long social distancing has ramifications beyond the workforce and economy; many people who continue to protect themselves through social distancing have reported waning social support and increased isolation. Although many in the US seem to be moving on from the pandemic, the long-term economic and social impacts of COVID-19 continue to affect people who struggle to make a complete recovery.
PANDEMIC POLITICIZATION Polling and analysis in the US show Republicans are more likely than Democrats to have lower rates of vaccine uptake and areas with more Republican voters have experienced more COVID-19-related deaths. But viewing the pandemic through a political lens is not useful, Dr. Ashish Jha, the White House COVID-19 Response Coordinator, said last week, urging people to instead view COVID-19 strictly through a public health and medical lens. Nevertheless, partisan messaging surrounding the pandemic is ramping up as US political candidates campaign ahead of mid-term elections. This week, US President Joe Biden publicly received an updated COVID-19 vaccine booster vaccine and called on the country to put politics aside to focus on personal health and the health of friends and family. His public vaccination likely was an effort by the White House to increase awareness that a new booster shot is available—a recent KFF poll found that around half of adults say they have heard “a little” or “nothing at all” about the bivalent boosters—but also a political move to highlight the Biden administration’s COVID-19 efforts, which typically score higher approval ratings than other issues.
Several Republican candidates are arguing that scientific and public health institutions have gained too much power during the pandemic. A new poll from the Pew Research Center suggests that while a majority of respondents agree that government investments in scientific research are worthwhile for society, many expressed a shared concern that the US is failing to gain ground in science globally. Notably, a partisan divide became apparent when respondents were asked about their views on the role of scientists in the policy arena, with Democrats more likely than Republicans to support scientists in active policy roles. Additionally, respondents’ confidence in scientists is lower than the high point seen early in the pandemic but has remained steady over the past year, according to the poll. While other issues appear to be dominating this year’s elections and both parties’ overall spending on COVID-19 messaging has dropped since the 2020 election, the pandemic remains an important issue for voters and elected officials.
US BOOSTER CAMPAIGN As the US heads into its third winter of the COVID-19 pandemic, US health officials this week announced additional efforts to encourage individuals, particularly those who are older or immunocompromised, to get vaccinated or boosted against COVID-19 at no cost. US President Joe Biden publicly received his fifth shot, coinciding with the release of an updated COVID-19 plan that includes enlisting Walgreens, DoorDash, and Uber to provide free delivery of antiviral prescriptions, calling on educational institutions to hold vaccination clinics for their communities, encouraging employers to provide paid time off for employees to get vaccinated, and urging building operators to improve indoor air quality.
In my location when you sign up for your booster you can prearrange for an Uber to pick you up.
At the height of the pandemic the ambulances were very busy and there would be at least two or three ambulances, sirens blaring, audible. Right now in my neighborhood the sirens are almost at the level they were back then.
Anecdotal but I wanted to mention it. There is also a shortage of the flu vaccine.
by dryrunguy Here is the latest Situation Report. Came out yesterday. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 628 million cumulative cases and 6.57 million deaths worldwide as of November 2. Global weekly incidence dropped for a second week after remaining steady for 6 weeks, falling 14% compared with the previous week to 2.5 million new cases. Weekly incidence fell over the previous week in Africa (-40%), Europe (-29%), and the Eastern Mediterranean (-8%); remained relatively steady in South-East Asia (-2%); and increased slightly in the Americas (+5%) and Western Pacific (+5%). Global weekly mortality decreased slightly from the previous week, down 4%.
UNITED STATES
The US CDC is reporting 97.3 million cumulative cases of COVID-19 and 1.07 million deaths. Incidence for the week ending October 26 remained relatively steady over the previous week, rising to 265,839 reported cases from 261,315 cases for the week ending October 19. Weekly mortality also remained relatively steady for the week ending October 26, up slightly to 2,649 reported deaths from 2,591 deaths the week ending October 19.**
**Beginning October 20, the US CDC began reporting and publishing aggregate case and death data, and line level data where applicable, from jurisdictional and state partners on a weekly basis rather than daily. As a result, COVID-19 data on cases and deaths are updated every week on Thursdays by 8pm ET.
Both new hospital admissions and current hospitalizations appear to have leveled over the past week, rising slightly by 2.1% and 0.1%, respectively.
The BA.5 sublineage continues to be the dominant strain in the US, accounting for 49.6% of sequenced specimens, but its estimated prevalence appears to be decreasing more rapidly now. The Omicron sublineages BQ.1 (14%) and BQ.1.1 (13.1%) are exhibiting growth advantages over other sublineages, including BA.4.6 (9.6%) and BF.7 (7.5%). Several other Omicron sublineages continue to exhibit increasing or steady trends, including BA.5.2.6 (2.8%), BA.2.75 (1.8%), and BA.2.75.2 (1.2%).
LONG COVID/PASC Post-acute sequelae of SARS-CoV-2 infection (PASC), commonly referred to as long COVID, continues to pose a heavy yet poorly understood toll on an uncertain proportion of individuals previously infected with SARS-CoV-2. Healthcare providers, scientists, and long COVID patients are hunting for answers regarding the condition, which cuts across all demographic groups and COVID-19 disease severities.
A group of international researchers published a commentary in Nature Reviews Nephrology highlighting recent studies indicating that long COVID increases the risk of adverse long-term kidney events and can have negative effects on the cardiovascular, hematological, and neurological systems, as well as on mental health and glycometabolism. Given the likelihood that long COVID will lead to new noncommunicable diseases in millions of people despite vaccine-mediated protection, the authors call for governments, health systems, and researchers to further investigate prevention and treatment of long COVID, in addition to building health systems capacity for the expected future noncommunicable disease burden. Notably, the US National Institute of Health’s (NIH) RECOVER Initiative has announced a new clinical trial testing Paxlovid as a treatment for long COVID in collaboration with Duke Clinical Research Institute.
A new systematic review from the European Centre for Disease Prevention and Control (ECDC) attempted to better characterize the prevalence of long COVID, stratified by initial COVID-19 disease severity, utilizing recruitment setting as a proxy indicator. Across 74,213 patients from 61 cohort studies in 15 countries assessed at least 12 weeks after initial SARS-CoV-2 infection, at least one long COVID symptom was found in 50.6% (95% CI: 41.1% to 60.2%) of patients recruited in community settings, 66.5% (95% CI: 56.0% to 76.3%) of patients recruited in hospital settings, and 73.8% (95% CI: 62.3% to 83.9%) of patients recruited in intensive care unit (ICU) settings. Prevalence of individual long COVID symptoms (specifically fatigue, shortness of breath, depression, headache, and dizziness) were higher among hospital settings than community settings. While the study only included patients infected pre-Omicron and did not include uninfected individuals as a control, this investigation—one of the largest studies of long COVID—indicates that the burden of the condition is greater than previously estimated and suggests long COVID symptoms may be worse for patients with more severe COVID-19 disease.
Similarly, a study published October 27 in JAMA Network Open assessed the prevalence of COVID-19 symptoms lasting longer than 2 months past infection in 16,091 US survey respondents between February 5, 2021, and July 6, 2022, as well as potential associations between long COVID and sociodemographic factors, prior vaccination status, and predominant variant at the time of infection. According to the results, 14.7% of respondents reported COVID-19 symptoms at least 2 months after infection, reflecting 13.9% of the previously infected US adult population after reweighting. Notably, further analysis indicated that female gender (adjusted odds ratio: 1.91; 95% CI, 1.73-2.13) and older age per decade above 40 years (adjusted odds ratio: 1.15; 95% CI, 1.12-1.19) may be associated with long COVID development, while risk may be less among those who received primary vaccination series prior to infection (odds ratio, 0.72; 95% CI, 0.60-0.86), individuals with a graduate education vs high school or less (adjusted odds ratio, 0.67; 95% CI, 0.56-0.79), and urban vs rural residence (adjusted odds ratio, 0.74; 95% CI, 0.64-0.86). Compared with ancestral COVID-19, infection during periods when the Epsilon variant (OR, 0.81; 95% CI, 0.69-0.95) or the Omicron variant (OR, 0.77; 95% CI, 0.64-0.92) predominated in the US was also associated with lower risk of long COVID symptoms.
VACCINE BOOSTERS With a worrisome mix of SARS-CoV-2 Omicron sublineages expected to drive another cold-weather surge of COVID-19 cases, experts in the US are encouraging people to get vaccinated and boosted using the new bivalent shots. Notably, however, only 7.3% of the US population aged 5 years and older have received the updated boosters, which target both the original SARS-CoV-2 viral strain and the BA.4 and BA.5 Omicron subvariants. Experts expect the new shots to help provide broad protection against these and newly emerging sublineages. Several recent studies posted as preprints—one each from research teams led by scientists from Columbia University Vagelos College of Physicians and Surgeons, Emory University School of Medicine, the University of Texas Medical Branch, and two led by researchers from Beth Israel Deaconess Medical Center—show that the new bivalent BA.5/4 boosters performed as well as or better than the original boosters and have the potential for BA.5 neutralization 4-fold higher than the original booster. These data, taken together with a study published in Science Immunology showing that booster doses (original) help improve neutralizing antibodies without strongly affecting cellular immune responses, further underline the necessity of booster shots to help strengthen waning immunity and protect against severe disease and death from COVID-19.
NON-NEEDLE VACCINE ADMINISTRATION The administration of vaccines through oral or nasal delivery routes offers several probable advantages, including the potential for stimulating immune reactions that could prevent transmission or symptomatic infection. Additionally, needle-free administration could make vaccination more accessible to countries with limited health infrastructure that have struggled with traditional vaccine administration in the past. Plus, those wary of needles could be persuaded to get vaccinated. The Chinese city of Shanghai last week began the rollout of what is believed to be the world’s first inhalable SARS-CoV-2 vaccine. Administration takes less than 20 seconds: a mist containing the vaccine is inhaled slowly through the mouth, then patients hold their breath for five seconds. The CanSino Biologics vaccine was approved in September as a booster dose, but the effectiveness of the inhaled vaccine is not known.
Researchers around the world are investigating another non-needle application, nasal administration. Nasal vaccines, administered through drops or sprays, could offer fast-acting protection, aimed at targeting virus cells where they first take hold in the lining of the nose and throat. Vaccines delivered intranasally differ from traditional vaccines, however, in that they are short-lived compounds aimed at blocking the virus’s ability to enter cells rather than building long-term immunity. They would require frequent application to fully coat the surface where viral cells may enter and likely would need to be used on a regular basis. Regulators in India approved a nasal vaccine in September, but it is not yet in use and efficacy data have not been released. Notably, Oxford and AstraZeneca’s attempt at nasal vaccine administration did not yield significant protection in first-phase human clinical trials. The small trial, which included 30 previously unvaccinated individuals and 12 participants who had received a primary 2-dose vaccination, elicited mucosal membrane antibody responses in only a minority of participants.
A study published October 27 in Science tested an approach the Yale-led researchers dubbed “prime and spike.” The method capitalizes on existing systemic immunity to SARS-CoV-2 gained from primary intramuscular (IM) vaccination to boost the body’s immune response in the respiratory tract using intranasal vaccine delivery. Administered in mice, the nasal spray elicited robust mucosal responses and offered comparable systemic neutralizing antibody booster responses to IM-administered boosters months out from primary vaccination. More research and funding are needed on non-needle vaccines, a key reason why nasal vaccine research has not progressed at the rate of IM-delivered vaccines. In the US, which led the race to develop SARS-CoV-2 vaccines, a lack of funding is preventing promising candidates and methodologies—such as the one tested by Yale researchers—from progressing into human studies and closer to regulatory authorization.
TRAVEL MASK MANDATES The US Supreme Court this week let stand a lower court ruling allowing the Transportation Safety Administration (TSA) to require mask use for travelers on planes, trains, and other methods of transport. The lower court’s ruling, from the US Court of Appeals for the DC Circuit, said the TSA has the authority to maintain safety and security during national emergencies. The TSA dropped its mask mandate in April after a federal judge in a different case ruled the agency had exceeded its authority. As part of a comprehensive strategy, the use of high-quality masks can help reduce the risk of viral transmission, including SARS-CoV-2.
GLOBAL VACCINE ACCESS If SARS-CoV-2 vaccines had been equitably shared among all nations in 2021, 295.8 million infections and 1.3 million deaths due to COVID-19 could have been prevented worldwide by the end of that year, even without any associated changes in behavior, according to a retrospective modeling study published October 27 in Nature Medicine. Additionally, if wealthier nations had kept nonpharmaceutical interventions (NPIs)—such as mask use and limitations on gathering sizes—in place for longer under this scenario, as many as 3.8 million lives could have been saved, the modeling suggests. Vaccine equity has improved globally, although disparities in access persist, according to the WHO. Overall, 68% of the world’s population has received at least one vaccine dose, but that proportion drops to 23% in low-income countries.
Though vaccine access is improving, other challenges remain, including the spread of mis- and disinformation, a lack of laboratory capacity and access, and the need for large capacity storage facilities, among others. Some experts are warning that the emergence of newer variants capable of greater immune evasion could create a critical situation in 2023, particularly in low- and middle-income countries (LMICs) whose populations are undervaccinated. But the situation also provides an opportunity for increased efforts to supply LMICs with next-generation vaccine boosters. Even as access to SARS-CoV-2 vaccines improves, the world needs to seriously look to the future and devise systems that will facilitate the equitable distribution of medical countermeasures during the next disease outbreak.
by dryrunguy Here's the latest Situation Report. I believe this is the first evidence that the bivalent vaccines increase immune response against the most recent subvariants. The section on ending the COVID-19 public health threat by using a "whole of society" or "whole of government" approach made me chuckle, especially the part about rebuilding trust of government.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 630.6 million cumulative cases and 6.58 million deaths worldwide as of November 10. Global weekly incidence dropped for a third week, falling nearly 12% compared with the previous week, to 2.2 million new cases. Weekly incidence fell over the previous week in Europe (-32.5%) and the Eastern Mediterranean (-11%) and remained relatively steady in the Americas (-3%). The South-East Asia (+28%), Western Pacific (+10%), and Africa (+9%) regions experienced increasing weekly incidence. Global weekly mortality decreased slightly from the previous week, down 9%, reaching the lowest level since mid-June 2022.
UNITED STATES
The US CDC is reporting 97.6 million cumulative cases of COVID-19 and 1.07 million deaths. Incidence for the week ending November 2 rose slightly over the previous week, rising to 273,110 from 260,830 for the week ending October 26. Weekly mortality remained relatively steady for the week ending November 2, down slightly to 2,504 reported deaths from 2,581 deaths the week ending October 26.**
**The US CDC updates weekly COVID-19 data on cases and deaths on Thursdays by 8pm ET.
Both new hospital admissions rose 6.2% over the past week, while current hospitalizations remained stable, falling slightly by 0.4%.
The BA.5 sublineage is quickly losing dominance in the US, accounting for 39.2% of sequenced specimens. The Omicron sublineages BQ.1.1 (18.8%) and BQ.1 (16.5%) are exhibiting growth advantages over other sublineages, including BA.4.6 (9.5%) and BF.7 (9%). Several other Omicron sublineages continue to exhibit increasing or steady trends, including BA.5.2.6 (3.1%), BA.2.75 (2.3%), and BA.2.75.2 (1.3%).
DECLINE IN GLOBAL DEATHS The number of global deaths due to COVID-19 has dropped 90% compared to nine months ago, according to the WHO. WHO Director-General Dr. Tedros Adhanom Ghebreyesus this week said the total number of COVID-related deaths reported during the first week in November was slightly more than 9,400, while the number of global weekly deaths in February rose as high as 75,000. The large drop in COVID-19 deaths is cause for optimism, Dr. Tedros said, but he urged governments to remain vigilant. Low global testing rates, waning surveillance activities, vaccination gaps between high-income countries and low- and middle-income countries, and newly emerging SARS-CoV-2 variants could lead to a resurgence in cases.
MASKING IN SCHOOLS A study published November 9 in the New England Journal of Medicine examining universal masking requirements in Boston, Massachusetts, greater metropolitan area schools found that the lifting of those requirements was associated with an additional 44.9 COVID-19 cases per 1,000 students and staff (95% CI, 32.6 to 57.1), corresponding to an estimated 11,901 cases and to 29.4% of the cases in all districts, in the 15 weeks after universal masking ended. Infection rates were lower among masked students than unmasked students, even in the area’s public schools that are often in older buildings with poor ventilation systems, more crowded, and attended by students more often from communities considered to be at-risk. The findings add to evidence underlining the importance of public health mitigation measures to prevent the spread of SARS-CoV-2—and possibly other respiratory viruses—in schools, including universal masking requirements.
PFIZER-BIONTECH BA.4/5 BOOSTER Pfizer and BioNTech released new data last week suggesting their updated Omicron BA.4/BA.5-adapted bivalent vaccine booster offers increased antibody response against the current most commonly circulating variants in populations aged 55 and older. Federal officials hope the news of more significant protection against COVID-19 will encourage people to get the booster shot, as less than 9% of the US population has done so. In a letter published in the New England Journal of Medicine, researchers from Israel detailed data from a 6-month follow-up of more than 11,000 healthcare workers who had 4 doses of the Pfizer-BioNTech vaccine. According to the research, participants had good neutralizing antibody responses, equivalent to those seen after a third dose, but that protection waned more quickly than after the third dose, waning completely after 13 weeks. The researchers said their findings suggest that boosters should be timed wisely to align with projected disease waves or be made seasonally available, similar to influenza vaccination.
Health regulators in the UK approved Pfizer-BioNTech’s bivalent booster targeting Omicron BA.4/5 this week for individuals aged 12 years and older, following the US, Canada, and the European Union. The UK already approved bivalent boosters from Pfizer-BioNTech and Moderna targeting Omicron BA.1. The UK also expanded the conditional marketing authorization for Novavax’s Nuvaxovid (NVX-CoV2373) as a homologous and heterologous booster dose after a primary vaccine series of any authorized SARS-CoV-2 vaccine. Novavax this week said a version of its vaccine targeting Omicron BA.1 (NVX-CoV2515) showed a strong immune response as the fourth dose.
In other vaccine-related news, AstraZeneca announced this week the company has withdrawn its application for authorization of its SARS-CoV-2 vaccine in the US due to waning demand and the availability of other vaccines.
COMBINATION COVID/FLU VACCINE Pfizer and BioNTech announced last week they are once again partnering to test a new vaccine candidate—an mRNA-based combination SARS-CoV-2 and influenza vaccine that incorporates the current bivalent SARS-CoV-2 vaccine with a new quadrivalent influenza vaccine candidate called qIRV (22/23). The Phase 1 trial, which has already begun and aims to enroll 180 healthy volunteers between the ages of 18-64 years in the US, will assess the vaccine candidate’s ability to generate immune response, safety, and tolerability.
In addition to the Pfizer-BioNTech candidate, Moderna and Novavax also are developing combination SARS-CoV-2 and influenza vaccines. If any of the vaccine candidates under development are successful, it would relieve people from the burden of scheduling and receiving separate annual shots for 2 respiratory diseases. Health experts hope an mRNA-based influenza vaccine might improve immune responses in older adults. If successful in trials, a combination vaccine could be ready for use during the 2023-2024 flu season.
THERAPEUTICS The United States is heading into a third pandemic winter with uncertainty surrounding several existing treatments for COVID-19 and few options to boost immune protection for immunocompromised individuals. While there is an updated bivalent vaccine booster, uptake is low; only 8.4% of the US population aged 5 years and older have received the shot. Notably, new data show the newer SARS-CoV-2 Omicron subvariants—including BQ.1, BQ.1.1, XBB, and XBB.1—can evade both vaccine-induced and infection-derived immunity. Additionally, the new sublineages are skirting the protection of the remaining monoclonal antibody therapies, including bebtelovimab, used as a treatment for people at high-risk of severe disease, and Evusheld, given prophylactically to people with compromised immune systems. The newer variants also have multiple pathways that could lead to resistance to the antiviral Paxlovid, one of the most effective treatments available, according to research published in Nature.
As the virus continues to develop ways to skirt available therapeutics, stronger efforts are needed to develop and authorize new drugs. Scientists are examining several new strategies, including targeting the human proteins SARS-CoV-2 uses to reproduce. A study published November 4 in Clinical Infectious Diseases showed that twice daily oral zinc supplementation decreased the 30-day death and ICU admission rate and shortened symptom duration among COVID-19 patients. This week, the US FDA issued an emergency use authorization (EUA) for anakinra (Kineret) injection for the treatment of COVID-19 in certain hospitalized patients at risk of developing severe respiratory failure. Anakinra is an interleukin-1 (IL-1) receptor antagonist currently FDA-approved to treat other conditions, including rheumatoid arthritis. On November 9, an FDA advisory panel voted against authorizing an oral drug, sabizabulin, to treat high-risk hospitalized patients with COVID-19. The panel voted 8-5 against the drug’s use, citing concerns over efficacy and safety data being based on a small clinical trial and hinting that it might reconsider additional data gathered from a larger trial. The FDA is not obligated to follow the panel’s recommendations, although it usually does.
In related news, a preprint study from researchers with the US Veterans Health Administration suggests that taking Paxlovid to treat COVID-19 may reduce the risk of later developing post-acute sequelae of SARS-CoV-2 (PASC), commonly called long COVID. The analysis, which has not yet been peer-reviewed, showed that people treated with Paxlovid within 5 days of a positive test were 26% less likely to develop many long COVID symptoms—including cardiovascular issues, hematologic disorders, neurocognitive impairment, fatigue, and trouble breathing—1 to 3 months after testing positive, compared with people who took a placebo. The study has several limitations, including that most of the people included were White and male. Last month, the US NIH announced it is beginning a study to evaluate Paxlovid as a treatment for people already experiencing long COVID.
ENDING COVID-19 PUBLIC HEALTH THREAT A peer-reviewed research article seeking consensus on how to end the COVID-19 public health threat was published November 3 in the journal Nature. The study convened a panel of 386 experts from academia, health settings, nongovernmental organizations, and governmental organizations from 112 countries and territories to develop the recommendations. Using the Delphi study methodology—a method used to identify consensus views across subject matter experts—the research presents a set of 41 consensus statements and 57 recommendations. In an opinion piece published in STAT, a group of the panel’s co-chairs noted that the process of developing, and agreeing on, the recommendations took approximately 14 months and discussed feeling discouraged at times, because world leaders and the general public seemed ready to move on from a problem that still needs solutions.
Some of the highest-ranking recommendations from the study call for “whole-of-society” and “whole-of-government” approaches to ending the COVID-19 health threat. Other recommendations include calling on governments to improve communication, rebuilding public trust, and engaging with communities while managing the pandemic response. The authors mention that improved indoor air quality is needed, in the form of enhanced air filtration and ventilation, in public spaces to prevent the spread of airborne diseases like COVID-19. Mechanical interventions like enhanced filtration and ventilation can prevent the spread of disease without relying on the actions of individuals. Indoor air quality has received more focus internationally since the start of the COVID-19 pandemic, and some world leaders are taking steps to push for improvements. It remains to be seen if world leaders and the general public will heed the advice from the panel.
CHINA The Chinese government today reaffirmed its commitment to its "dynamic zero" COVID-19 policy, despite growing frustrations from Chinese citizens and heavy economic impacts. This week, the number of new COVID-19 cases in China reached a six-month high, prompting public health officials to reinstate lockdowns, frequent testing, and travel restrictions in some areas, frustrating both Chinese residents and the international community. The country’s restrictions are also interrupting the global economy. China’s 1.4 billion people largely lack immunity due to low infection rates, and Chinese-made vaccines have proven less effective against newer, more transmissible SARS-CoV-2 variants, challenging the nation’s exit from its zero COVID policies.
CORRECTION Due to an editing oversight, a story in last week’s report misrepresented research on nasal vaccines and other experimental compounds that might be used to prevent SARS-CoV-2 infection. Errors in the following paragraph contained in the story Non-Needle Vaccine Administration, which can be read in full here, were corrected to state:
Researchers around the world are investigating another non-needle application, nasal vaccines administered through drops or sprays. Regulators in India approved a nasal vaccine in September, but it is not yet in use and efficacy data have not been released. Notably, Oxford and AstraZeneca’s attempt at nasal vaccine administration did not yield significant protection in first-phase human clinical trials. The small trial, which included 30 previously unvaccinated individuals and 12 participants who had received a primary 2-dose vaccination, elicited mucosal membrane antibody responses in only a minority of participants. Some compounds under investigation that are delivered intranasally differ from traditional vaccines, however, in that they provide short-lived protection aimed at blocking a virus’s ability to enter cells rather than building long-term immunity. They would require frequent application to fully coat the surface where viruses could infect cells and likely would need to be used on a regular basis.
by ponchi101 Well, a bit of good news. The paragraph on declining global deaths is encouraging.
by Deuce
ponchi101 wrote: ↑Thu Nov 10, 2022 9:15 pm
Well, a bit of good news. The paragraph on declining global deaths is encouraging.
Count on deaths rising significantly in the coming weeks - and remaining higher until April or May, as high population areas are headed into the colder/winter months - meaning more people congregating indoors (and largely unmasked this time)...
by atlpam Received my bivalent booster yesterday.
by dryrunguy
atlpam wrote: ↑Fri Nov 11, 2022 3:15 pm
Received my bivalent booster yesterday.
I received my most recent booster (Pfizer) on July 21--right before the bivalent boosters came out. Is it too soon for me to get the bivalent booster? Generally, it seems like the guidance on how often to get boosters is every 6 months. But the regular boosters clearly aren't as effective against today's most prevalent subvariants.
by atlpam Recommendation is to wait 4-6 months, so I would think if you want the extra protection heading into the holiday season, you would be fine to get it the end of Nov. I waited the full 6 months, which worked well for me, timing wise. The hubs is still needing to get his, but he’s always down for a full day after the shot, so he has to plan for a lost day.
by MJ2004 Because I'm under 50, I wasn't eligible for another booster until this Oct (I got the bivalent) - one year from my first booster. Now unless something changes I plan to stay on the fall plan and boost once per year. Every six months is too often for me. I do however continue to wear masks almost everywhere.
by ti-amie I got my booster earlier this month and had no side effects at all. I mask everywhere I go.
by Deuce I was going to get my third booster - a bivalent - at the beginning of this month, which would be 5 months after the previous (second) booster. But a month ago, I became ill with a virus, and the rapid COVID antigen test showed positive... and so I wait, as the medical people say to wait 3 months after you have COVID before getting your next vaccine.
Last month was the first time I've been ill since the pandemic began. I'm still not completely convinced I had COVID. As I have since the spring of 2020, I wear a mask in every indoor setting (except at home), and outright avoid unnecessary indoor locations, and so it's a mystery as to where I contracted it (if it was indeed COVID).
The 3 month wait before the next vaccine is not mandatory (it would be impossible to enforce anyway) - it's simply a recommendation. There is no danger in getting vaccinated right after your COVID symptoms disappear - it's simply a matter of mathematics: when one has COVID, the antibodies remain in the person's system strongly for about 3 months after the fact - and so it makes no sense to waste 3 months of the vaccine's effective protective time range by getting vaccinated right after you have COVID, as you're already protected by the natural antibodies. Getting vaccinated on top of that will not protect you any more.
And so I think I will end up compromising between the two and get the bivalent vaccine 2 months after my positive test, which will be in about a month.
by ti-amie
by ponchi101 :slap to the face: emoji
(We don't have it)
by skatingfan
ponchi101 wrote: ↑Sat Nov 12, 2022 4:03 pm
:slap to the face: emoji
(We don't have it)
by atlpam Cruise ships are floating petri dishes. (my opinion)
by dryrunguy Here's the latest Situation Report. We called the section on long COVID and disability. I thought the last section on the Indian vaccine approval process was interesting.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 633.3 million cumulative cases and 6.59 million deaths worldwide as of November 17. Global weekly incidence increased significantly for the first time since August, rising 5% compared to a decrease of 10% the previous week. A total of 2.4 million cases were confirmed the week of November 7. Weekly incidence fell over the previous week in Europe (-15%) and the Eastern Mediterranean (-12%) and remained steady in Africa (0.42%). The Americas (+17%), South-East Asia (+15%), and Western Pacific (+18%) regions experienced increasing weekly incidence. Global weekly mortality declined from the previous week, down 26%, reaching the lowest level since the beginning of the pandemic.*
*The WHO dashboard notes that data from the Eastern Mediterranean and Africa regions are incomplete.
UNITED STATES
The US CDC is reporting 97.9 million cumulative cases of COVID-19 and 1.07 million deaths. Incidence for the week ending November 2 rose slightly over the previous week, rising to 288,989 from 273,021 for the week ending November 2. Weekly mortality remained relatively steady for the week ending November 9, down slightly to 2,344 reported deaths from 2,489 deaths the week ending November 2.**
**The US CDC updates weekly COVID-19 data on cases and deaths on Thursdays by 8pm ET.
Both new hospital admissions and current hospitalizations remained stable, falling slightly by 0.9% and 0.8%, respectively.
The BA.5 sublineage is expected to lose dominance in the US over the next week. BA.5 now accounts for 29.7% of sequenced specimens. The Omicron sublineages BQ.1.1 (24.1%) and BQ.1 (20.1%) are exhibiting growth advantages over other sublineages, including BF.7 (7.8%) and BA.4.6 (5.5%). The CDC is now tracking the Omicron sublineage BN.1, which is now responsible for 4.3% of cases. Other Omicron sublineages appear to be declining in prevalence, including BA.5.2.6 (2.9%), BA.2.75 (1.2%), and BA.2.75.2 (0.9%).
US RESPONSE The Biden administration is expected to keep in place the public health emergency status of the COVID-19 pandemic through spring 2023 to address a potential winter surge in cases and provide more time to transition vaccines and treatments to the private market, according to 2 unnamed officials. The declaration, most recently renewed in October, was set to expire in January. The US HHS has promised to provide states 60 days’ notice before winding down the emergency, and did not do so on November 11, which marked that date. This week, the White House requested the US Congress authorize an additional US$9.25 billion in pandemic funding for this year. According to officials, about US$8.25 billion would go toward purchasing treatments and vaccines ahead of a possible winter surge, efforts to accelerate research into next-generation vaccines and treatments, and long COVID research, with an additional US$1 billion going toward global vaccination and response efforts. The Biden administration has repeatedly tried to secure additional funding with no success; observers say the best chance might be during the current lame-duck session while Democrats retain control of both congressional chambers.
Though the need remains for additional spending for COVID-19 and general pandemic preparedness and response, public and congressional interest is waning. On November 15, the US Senate voted 62-36 to end the emergency declaration, with support from 12 Democrats. In response, the Office of Management and Budget said abruptly ending the emergency would be “a reckless and costly mistake” and noted US President Joe Biden would veto the measure if passed by Congress. It is unclear whether the US House will take up the resolution.
WINTER SURGE PREDICTIONS The WHO on November 16 announced that the worldwide number of new COVID-19 cases increased last week for the first time in 4 months, warning that the true number of infections is likely higher due to declines in testing. Additionally, upticks in influenza and respiratory syncytial virus (RSV) cases also are straining hospitals, particularly some countries in the Americas.
While many in the US work to find balance between COVID-19 precautions and returning to a sense of normalcy, there are signs the coronavirus has not gone away. The number of new weekly COVID-19 cases are beginning to increase, raising concerns over a potential winter surge amid waning immunity and the emergence of new subvariants. About 330 people die of COVID-10 each day in the US, and around 21,000 are hospitalized with COVID-19 on any given day. Despite low levels of uptake of the bivalent booster vaccine—only 10% of the population aged 5 and older have received the updated shot—some US health officials, including White House COVID-19 Response Coordinator Dr. Ashish Jha, say they are not expecting a large surge in cases during the winter holiday season. Dr. Jha is confident that broad vaccine coverage and widespread previous infections will help keep a large surge at bay. Other experts are not so assured, saying the possibility remains for a substantial surge, with several factors making the US underprepared. Declining support for community vaccination campaigns, a public that is tuning out renewed government vaccination messaging, few remaining treatments effective against emerging Omicron sublineages, waning use of nonpharmaceutical interventions (NPIs) such as mask use, and diminishing surveillance place the US in uncharted territory heading into what is traditionally the height of respiratory virus season.
MODERNA BIVALENT BOOSTER On November 14, Moderna announced data showing its updated Omicron BA.4/BA.5-adapted bivalent vaccine booster offers a strong immune response against BA.5 by increasing antibodies levels, when compared to the company’s original booster. The bivalent vaccine (mRNA-1273.222) demonstrated a 15-fold increase in neutralizing antibody titers compared to pre-booster levels. The data are not yet peer-reviewed or posted to a preprint server. An exploratory analysis of data from 40 participants suggested both of the company’s bivalent boosters—with the other targeting BA.1 (mRNA-1273.214)—showed robust levels of neutralizing antibodies against the emerging Omicron subvariant BQ.1.1, which has the potential to become dominant in the US by next week. Notably, however, the demonstrated antibody responses were lower than those against BA.4 and BA.5. Since Omicron-adapted booster shots began to rollout earlier this fall, acceptance and uptake has been dismal. Only 10% of the US population aged 5 and older have received an updated booster, spurring the Biden administration to launch a new campaign urging residents to get boosted ahead of Thanksgiving.
COVID-19 REBOUND Cases of COVID-19 rebound—the return of test positivity or symptoms after clearance or resolution—following treatment with the antiviral Paxlovid appear to be more common than previously believed, a preprint study posted November 15 to medRxiv suggests. The prospective observational study, which is not yet peer-reviewed, found that viral rebound among the 127 participants who took a 5-day course of Paxlovid was 14.2%, while 9.3% of the control group of 43 people experienced viral rebound. There were no significant differences in viral rebound by demographics, pre-existing conditions, or major symptoms experienced during the acute phase or at 1 month. Additionally, COVID-19 symptom rebound incidence was higher in the Paxlovid group (18.9%) compared with the control group (7.0%). Though the study was not able to determine whether the observed differences were due to chance or as a result of treatment, many researchers agree the results mirror their real-life experiences that rebound is more common in people who take Paxlovid.
Larger studies are being planned to better understand the issue, which hopefully will help alleviate one of the causes for underprescription of Paxlovid. High-profile cases of rebound likely are contributing to underuse of the treatment. In clinical trials, Paxlovid was nearly 90% at preventing hospitalizations and deaths of high-risk patients with COVID-19. Notably, another preprint study suggests treatment with Paxlovid is associated with a 26% reduction in the occurrence of post-acute symptoms, commonly known as long COVID.
PASC/LONG COVID Although many people with COVID-19 recover within weeks, some continue to experience a constellation of symptoms—or start experiencing new ones—that can last long after their acute infection. The US CDC has recognized that post-acute sequelae of SARS-CoV-2 infection (PASC), commonly called long COVID, includes new or ongoing symptoms such as fatigue, brain fog, shortness of breath, headaches, chest pain, loss of taste or smell, and more. Notably, however, there is no widely accepted definition of the condition, often leaving clinics wrestling with how to treat long COVID patients with varying conditions.
To understand the prevalence of post-COVID-19 symptoms, a recent cross-sectional cohort study published in JAMA Network Open compared the presence of post-COVID symptoms in 360 hospitalized and 308 nonhospitalized patients at 2 healthcare centers in Madrid, Spain, 2 years after their initial acute infection early in the pandemic. The study reported that 2 years after initial infection, 59.7% of those who were hospitalized and 67.5% of those who were not hospitalized still had at least one symptom of COVID-19, with the most prevalent symptoms being fatigue (44.7% vs. 47.7%, respectively), pain and headaches (35.8% and 29.9%, respectively), and memory loss (20% and 15.9%, respectively). Overall, the research team observed no significant differences in post–COVID symptoms between hospitalized and nonhospitalized patients, although hospitalized patients experienced slightly higher levels of anxiety.
Similarly, a recent study published in PLOS Medicine investigated post-COVID-associated morbidity in children, adolescents, and adults using comprehensive healthcare data on half of the German population. The study determined that children, adolescents, and adults have the same relative risk of experiencing post-COVID-19 symptoms 90 days after their initial acute infection. Children, adolescents, and adults experienced shared symptoms like cough, fever, headache, malaise/fatigue/exhaustion, and throat or chest pain. Adults were slightly more likely to experience disturbances of smell and taste, fever, and respiratory symptoms, while children and adolescents were slightly more likely to experience malaise, fatigue/exhaustion, cough, throat or chest pain, and adjustment disorder.
This growing evidence base around the characterization and prevalence of long COVID can help inform efforts to support people whose symptoms have a significant impact on their lives. Although the US HHS and US Department of Justice have jointly declared long COVID as a disability, some Americans with long COVID have faced barriers to accessing disability benefits. Long COVID-related disability assistance is frequently denied due a lack of specific guidance on how to evaluate the claims and lack of standard processes for diagnosing the condition. HHS in August released a report outlining federal services and support for people with long COVID, and advocates and researchers are working to raise awareness of these resources. A recent report from the Brookings Institution estimated that long COVID could be contributing to a national labor shortage, with as many as 4 million people out of work due to the condition.
VACCINE MANDATES Vaccine mandates—for COVID-19 and other diseases—are contentious issues in the US. On several occasions, the US Supreme Court has refused to hear arguments or let lower court rulings stand, allowing COVID-19 vaccine mandates to remain in force. Now, the Blackfeet Nation is challenging a Montana law that prohibits businesses and governments from discriminating against people who are not vaccinated against COVID-19 or other diseases, after a meeting on the Blackfeet Indian Reservation that checked attendees’ COVID-19 vaccination status came under scrutiny for potentially violating state law. The case raises the question of whether Montana can enforce its law on the Blackfeet Nation, superseding the tribe’s right to enforce its own ordinances as a sovereign nation within US borders to protect the health of its people. A 1855 treaty allows the Blackfeet tribe to regulate tribal and nontribal members alike on its land. The US CDC has lauded Blackfeet Nation for implementing effective COVID-19 risk mitigation and prevention measures. Relatedly, a separate lawsuit argues that Montana’s law is unconstitutional and prevents hospitals and physicians from protecting disabled patients and employees from exposure to COVID-19.
VACCINE APPROVAL PROCESS IN INDIA India’s national drugs regulator approved a domestically developed vaccine for COVID-19—Covaxin, produced by Bharat Biotech—despite discrepancies in the number of clinical trial participants, questionable changes to trial protocols, and efforts to speed trials along without complete data on safety and efficacy, according to a report from STAT. A lack of transparency surrounding the vaccine’s development efforts, questions over Bharat Biotech’s manufacturing facilities, as well as political and scientific pressure to move testing forward contribute to ongoing concerns over Indian government oversight of and commitment to producing quality medical products. A day after the STAT report’s publication, India’s Health Ministry said any allegations that the government made missteps or rushed Covaxin’s development and testing are “completely misleading, fallacious, and ill-informed,” and Bharat Biotech called the narrative misleading, clarifying that any pressure felt originated within the company. Bharat Biotech also reiterated that Covaxin is safe and effective, having been tested more than any other Indian vaccine and with several million doses administered worldwide.
India’s pharmaceutical industry is one of the world’s largest by volume, exporting medicines to more than 200 countries and contributing a large volume of generic drugs, especially in the US. Last month, the WHO linked an Indian-made cough syrup to the deaths of nearly 70 children in West Africa; India’s drugs regulator disputed the WHO’s findings.
by ponchi101 Agree that Long Covid merits more study. One question that I would like to ask: do people that got Covid BUT WERE VACCINATED, suffer the same range of symptoms and effects as those that were not vaccinated?
We have now two distinct (or even three) populations to study.
by dryrunguy
ponchi101 wrote: ↑Thu Nov 17, 2022 9:53 pm
Agree that Long Covid merits more study. One question that I would like to ask: do people that got Covid BUT WERE VACCINATED, suffer the same range of symptoms and effects as those that were not vaccinated?
We have now two distinct (or even three) populations to study.
Some evidence suggests that unvaccinated people generally suffer worse health outcomes than partially or fully vaccinated people. This applies to general illness (how badly COVID knocks you off your gourd and for how long), hospitalizations, deaths, AND the incidence and severity of long COVID.
by Suliso I have no idea how this will end in China, but not with eradication of covid I'm sure.
by ponchi101 The claim that only 5,200 people have died in China is ludicrous.
by dryrunguy I guess I'll put this here. Today's NY Times e-newsletter featured an interesting analysis of data on the impact of remote learning earlier in the pandemic on student math and reading skills in the U.S.
::
Good morning. Remote learning erased students’ progress in math and reading, but it wasn’t the only factor.
Behind the declines Months into the current school year, most American students are still trying to make up for what they lost during the pandemic. This fall, we saw some of the clearest evidence yet of the extent to which the pandemic — and the school closures that came with it — hurt children’s education.
Nine-year-olds lost the equivalent of two decades of progress in math and reading, according to an authoritative national test. Fourth and eighth graders also recorded sweeping declines, particularly in math, with eighth-grade scores falling in 49 of 50 states.
The data comes from the National Assessment of Educational Progress, a rigorous exam that evaluates thousands of children across the country and is overseen by a research arm of the U.S. Education Department.
Today, I’ll break down the factors that drove these declines and explain an important trend that helps show why these results are so sobering.
Remote learning’s role First, to address one of the most common questions I hear as an education reporter: To what degree is remote learning responsible for these setbacks? The answer is both simple and complicated.
At a basic level, there is good evidence and a growing consensus that extended remote learning harmed students. Some state test results from 2021 help show the damage. In Ohio, researchers found that districts that stayed fully remote during the 2020-21 school year experienced declines up to three times greater than those of districts that mostly taught students in person.
More recently, the national test results capture both the initial academic declines and any recovery, and they offer some nuance. While there was a notable correlation between remote learning and declines in fourth-grade math, for example, there was little to no correlation in reading. Why the discrepancy? One explanation is that reading skills tend to be more influenced by parents and what happens at home, whereas math is more directly affected by what is taught in school.
So remote learning does not explain the whole story. What else does? In a sophisticated analysis of thousands of public school districts in 29 states, researchers at Harvard and Stanford Universities found that poverty played an even bigger role in academic declines during the pandemic.
“The poverty rate is very predictive of how much you lost,” Sean Reardon, an education professor at Stanford who helped lead the analysis, told me.
Comparing two California school districts, one wealthier and the other poorer, illustrates this point. Cupertino Union, a Silicon Valley school district where about 6 percent of students qualify for free or reduced lunch (a marker that researchers use to estimate poverty), spent nearly half of the 2020-21 school year remote. So did Merced City in the Central Valley, where nearly 80 percent of students are eligible for free or reduced lunch, according to the Harvard-Stanford analysis.
Yet despite spending roughly the same amount of time attending classes remotely, students in the wealthier Cupertino district actually gained ground in math, while students in poorer Merced City fell behind.
High vs. low performers While the overall declines in student achievement were stark, the averages mask even deeper divergences between student groups. For example, Black and Hispanic students, who had started out behind white and Asian students in fourth-grade math, lost more ground than those groups during the pandemic.
Notably, the gap is also growing between the country’s highest-achieving students and low-performing students who struggle the most.
That gap — driven by declines among lower performers — was most clear for younger students and in reading. (Middle-school math declines were more significant across the board.)
In fourth grade, the average reading score on the national exam fell three points. But results for students in the top 90th percentile did not fall at all, while those for students in the bottom 10th percentile plunged six points, double the overall average.
In other words: The students who had the least ground to lose lost the most.
There may be a twofold explanation. Recent research from NWEA, a nonprofit academic assessment organization, found that students at the bottom of their classes both experienced sharper setbacks at the start of the pandemic and showed less improvement last school year.
I am sometimes asked: If the pandemic affected all students, how much does it matter? Isn’t everyone behind?
What the latest data affirmed is that while the pandemic affected all students, it did not affect all students equally. That was true with remote learning, and it is playing out now in recovery. The students who had the greatest needs coming into the pandemic have the steepest challenge — and will need the most help — in the future.
by ponchi101 I know this study(ies) are not about this other subject, but: this is also pretty damning evidence that HOME SCHOOLING is bull****. Home schooling is even worse: you would not have a session with a teacher, you would have a session with, most probably, your undereducated parent.
by Deuce No - home schooling is not BS at all. To me, it's preferable to institutionalized schooling.
I've known a few people who were home-schooled, and they are extremely insightful and intelligent. They are 'free thinkers'.
And I've known MANY people who have various diplomas and degrees who are grossly incompetent.
Regular school basically teaches kids how to follow the crowd; how to 'fit in' to the system; how to 'obey'. It does not teach kids to think independently. It does not encourage them to think 'outside the box' - if anything, it teaches them that thinking 'outside the box' is unacceptable. The format is not at all conducive to independent thought, of course - you have 25 to 40 students per class. It's ridiculous. There is no way in hell that ANY of those 25 to 40 students can get the individual attention they need to promote individual and independent thought. It, in fact, stifles independent thought. All that's done is a very generalized learning, where a blanket is thrown over all the students as the teacher teaches one way of doing things at one pace, and the kids who don't catch on are screwed.
“What does education often do? It makes a straight-cut ditch of a free, meandering brook.” ~ Henry Thoreau
I think that kids should learn the basics in school - reading, writing, basic arithmetic. After that foundation is set, they should be able to find a way to focus only on the subjects they are interested in. Their interests may change - and may even change several times in the space of a year - until they realize what they are truly passionate about.
Forcing kids to sit through classes on subjects that they have absolutely no interest in is counterproductive.
by ti-amie The problem with home schooling is that social skills, how to interact with others, end up being lacking for many. If you're only allowed to interact with people who have the same worldview as you've been "taught" by your parents and their friends and relatives your "free thought" is usually regurgitation of the insular views you've been spoon fed all of your life.
There are now parents who make more of an effort to integrate their children into the wider society and welcome the free exchange of ideas so I don't mean to imply all home schooling is bad. It depends on who is doing it and why they're doing it.
by Deuce I've found that the majority of parents who homeschool their kids are more intelligent than average, and are progressive and very open-minded - and they encourage their kids to explore different perspectives.
Exploring different perspectives is not typically taught within the institutionalized schooling system - quite the opposite.
I can understand the concern about developing social skills... But today, social skills are very much lacking for kids and adults alike because of the reliance on technology. Computers and cell phones have done huge damage to social skills. Hell, I've had university students tell me that they are terrified of talking on the phone - because it requires instant responses. They do all of their 'communication' via text messaging, which is pathetic.
Text messaging is fine to let someone know you'll be 10 minutes late in meeting them - but nothing meaningful can be communicated via texts, as it's far too generic, restrictive and limiting. But that is the main means that many people 'communicate' today. The result is that real communication has declined significantly - which inherently makes for less solid and less profound relationships.
Deuce wrote: ↑Mon Nov 28, 2022 11:58 pm
I've found that the majority of parents who homeschool their kids are more intelligent than average, and are progressive and very open-minded - and they encourage their kids to explore different perspectives.
Exploring different perspectives is not typically taught within the institutionalized schooling system - quite the opposite.
I can understand the concern about developing social skills... But today, social skills are very much lacking for kids and adults alike because of the reliance on technology. Computers and cell phones have done huge damage to social skills. Hell, I've had university students tell me that they are terrified of talking on the phone - because it requires instant responses. They do all of their 'communication' via text messaging, which is pathetic.
Text messaging is fine to let someone know you'll be 10 minutes late in meeting them - but nothing meaningful can be communicated via texts, as it's far too generic, restrictive and limiting. But that is the main means that many people 'communicate' today. The result is that real communication has declined significantly - which inherently makes for less solid and less profound relationships.
Roughly 2/3 of home schooling in the USA is religious/grooming based, so not so open minded or progressive here in the USA! USA! USA!
Deuce wrote: ↑Mon Nov 28, 2022 11:58 pm
I've found that the majority of parents who homeschool their kids are more intelligent than average, and are progressive and very open-minded - and they encourage their kids to explore different perspectives.
Exploring different perspectives is not typically taught within the institutionalized schooling system - quite the opposite.
I can understand the concern about developing social skills... But today, social skills are very much lacking for kids and adults alike because of the reliance on technology. Computers and cell phones have done huge damage to social skills. Hell, I've had university students tell me that they are terrified of talking on the phone - because it requires instant responses. They do all of their 'communication' via text messaging, which is pathetic.
Text messaging is fine to let someone know you'll be 10 minutes late in meeting them - but nothing meaningful can be communicated via texts, as it's far too generic, restrictive and limiting. But that is the main means that many people 'communicate' today. The result is that real communication has declined significantly - which inherently makes for less solid and less profound relationships.
Roughly 2/3 of home schooling in the USA is religious/grooming based, so not so open minded or progressive here in the USA! USA! USA!
That is not the case here in Canada.
We're comparatively more progressive.
Politics and religion are both far too prominent in the USA. It seems that EVERYTHING in America is about either religion or politics.
I like it better here.
by Owendonovan Yes, Canada is much more effective at a rationally progressive state, you're lucky! The people we call leaders here....
by Deuce
Owendonovan wrote: ↑Wed Nov 30, 2022 4:53 am
Yes, Canada is much more effective at a rationally progressive state, you're lucky! The people we call leaders here....
It's not that our leaders are better than yours... our leaders are just as dishonest, corrupt, manipulative, and selfish as any leaders anywhere. That's what politics is; that's what politicians are.
The difference in this aspect, I feel, between Canada and the U.S. is that we are much better at ignoring our leaders. We don't obey our leaders as much as people in the U.S. obsessively obey their leaders... and we also don't rebel against them as much as people in the U.S. radically rebel against their leaders. We mostly ignore them and decide for ourselves what is right and what is wrong.
Politics here is very much a trivial sideshow, whereas in the U.S., it's by far the main event.
by Suliso One can ignore politics for a while, but the risk is that politics decides not to ignore you.
by ponchi101
Suliso wrote: ↑Wed Nov 30, 2022 9:42 am
One can ignore politics for a while, but the risk is that politics decides not to ignore you.
My loony friend N is a prime example. He does not care about politics; "it does not affect me".
Yet, here he is, in Colombia, basically one of 6 million Venezuelan refugees around the world, because, you know, Venezuelan politics did not affect him.
sigh...
by dryrunguy Here's the latest Situation Report. Fairly depressing stuff.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 639.5 million cumulative cases and 6.62 million deaths worldwide as of December 1. Global weekly incidence increased for the third week in a row last week, rising 8.9% compared to an increase of 2.36% the previous week. A total of 2.87 million cases were confirmed the week of November 21. Weekly incidence fell over the previous week in Africa (-40%), the Eastern Mediterranean (-17%), South-East Asia (-8%), and Europe (-4%). The Americas (+19%) and Western Pacific (+16%) regions experienced increasing weekly incidence. Global weekly mortality remained relatively steady from the previous week, down 3%.*
*The WHO dashboard notes that data from the Africa region are incomplete.
UNITED STATES
The US CDC is reporting 98.5 million cumulative cases of COVID-19 and 1.07 million deaths. Incidence for the week ending November 23 rose slightly over the previous week, increasing to 305,082 cases from 281,691 cases for the week ending November 16. Weekly mortality increased for the week ending November 23, with 2,644 reported deaths compared to 2,266 deaths the week ending November 16.**
**The US CDC updates weekly COVID-19 data on cases and deaths on Thursdays by 8pm ET.
Both new hospital admissions and current hospitalizations increased last week, up by 18% and 11%, respectively, over the previous week.
The BA.5 sublineage rapidly lost dominance over the past 2 weeks, now accounting for only 19.4% of sequenced specimens. The Omicron sublineages BQ.1.1 (29.4%) and BQ.1 (27.9%) together represent the two most dominant subvariants. A host of other Omicron sublineages—including BF.7, BA.4.6, XBB, BN.1, BA.2.75, BA.5.2.6, BF.11, BA.2, BA.2.75.2, and others—make up the remainder of cases.
US PANDEMIC MORTALITY On average, more than 300 people in the US die each day from COVID-19. While the death toll is significantly lower than during the peak of the Delta wave, the number is 2 to 3 times higher than the average number of deaths from flu. Increasingly, COVID-19 is becoming a disease of the elderly. In summer 2021, about 58% of COVID-19 deaths occurred among adults aged 65 or older. Today, that proportion is 9 of 10 COVID-related deaths, according to US CDC data. This upward trend is expected to continue, and despite the nation’s pursuit of normalcy, is set to cause significant disruptions to the health system.
Mortality trends have shifted throughout the pandemic. A study published this week in the Annals of Internal Medicine by investigators at Brigham and Women’s Hospital in Boston, Massachusetts (US), found that the proportion of younger people who died from COVID-19 in 2021 surpassed that of 2020, with the median age of COVID-related deaths falling from 78 years old in 2020 to 69 years old in 2021. Researchers calculated years of life lost (YLL) and compared timeframes in 2020 and 2021. Using this calculation, the team was able to assess premature deaths based on the number of years an individual would have lived. In 2021, there were about 21% fewer deaths compared to 2020. However, YLL per COVID-19 death increased by 36%. Better understanding age shifts in COVID-19 mortality can help inform prevention and treatment approaches, public policy, and community measures to minimize the impacts of this increasingly preventable disease.
US PUBLIC HEALTH WORKFORCE The US CDC this week announced it will award more than US$3 billion in grants to strengthen the nation’s public health workforce and infrastructure. The funding is the first of its kind, as all US citizens live in a jurisdiction that will receive funds. Notably, the new funding is intended for government-run public health agencies, leaving community health organizations concerned they will be left out. States relied heavily on community and grassroots organizations for vaccine rollout, testing, and other services throughout the COVID-19 pandemic. While it is crucial that government health departments in communities that are economically and socially marginalized or rural, or in communities with people from racial and ethnic minority groups, receive this support, particularly with a growing shortage of healthcare workers, community leaders in these settings feel additional funding is needed to sustain and grow health promotion efforts begun during the pandemic. The CommuniHealth Coalition, led by the Johns Hopkins Center for Health Security and the Department of Anthropology at Texas State University, recently released reports examining the role of community health workers in the COVID-19 pandemic response and recovery and providing guidance for how to build and grow the community health sector.
MONOCLONAL ANTIBODY BEBTELOVIMAB The US FDA on November 30 ended its emergency use authorization (EUA) for Eli Lilly’s monoclonal antibody bebtelovimab because it is not expected to neutralize the two most widely circulating SARS-CoV-2 Omicron subvariants, BQ.1 and BQ.1.1. Known together as the “BQs,” those subvariants account for 57% of cases nationwide, according to US CDC estimates. Bebtelovimab was the only remaining authorized COVID-19 antibody therapy. Several companies are working on updated antibodies, although none appear to be close to authorization. The FDA recommended health providers choose other appropriate approved or authorized treatments, including the antivirals Paxlovid, Veklury, or Lagevrio, or convalescent plasma with high titers of SARS-CoV-2 antibodies. A recent preprint literature review posted to bioRxiv concluded that convalescent plasma from recently vaccine-boosted people who had confirmed COVID-19 neutralized more than 95% of the SARS-CoV-2 Omicron subvariants BQ.1.1, BF.7, and XBB and could be a viable substitute for monoclonal antibodies as passive immunotherapy for both COVID-19 prophylaxis and therapy among immunocompromised patients.
LONG COVID Nearly a third of people in the US with COVID-19 will develop long-term symptoms, according to a recent report from the US Department of Health and Human Services (HHS). Health experts are warning that this collection of post-acute symptoms, commonly known as long COVID, could be the next public health crisis—so far impacting as many as 23 million people, a number expected to grow as COVID-19 continues to circulate. In addition to increased medical expenses, individuals and families dealing with long COVID could face a reduced quality of life, reduced income, higher household debt, and lower retirement savings, further widening existing inequalities and costing the US economy US$3.7 trillion, according to one estimate. A Swiss study published in Nature Communications examined the prevalence of post-COVID conditions among children, with the findings suggesting that risk factors for lingering symptoms included older age, lower socioeconomic status, and having an existing chronic health condition, particularly asthma.
With little known about the underlying causes of lasting symptoms and a lack of a clear definition, healthcare professionals are stuck between wanting more evidence for effective therapies and trying to treat vulnerable and suffering patients. Some people with long COVID are turning to expensive and untested therapies, from vitamin supplements to stem cell treatments. The US NIH created the RECOVER Initiative to learn more about the long-term effects of COVID-19 and recently announced a clinical trial to investigate the antiviral Paxlovid for treatment of long COVID, with results expected in 2024. But many experts argue a more agile research model is needed to more quickly address the growing problem.
FUTURE OF VACCINES Global efforts are underway to prepare vaccine research, development, and production facilities for the next pandemic. This week, the Coalition for Epidemic Preparedness Innovations (CEPI) launched its 100 Days Mission, a US$3.5 billion plan to invest in vaccine research and development and achieve equitable access to vaccines for emerging viruses with pandemic potential, with the goal of producing a safe and effective vaccine within 100 days. This effort, if successful, would significantly shorten the time it took scientists to develop shots for COVID-19, a record 326 days. In Africa, Afrigen Biologics & Vaccines, the Biovac Institute, and a variety of partners are working to bring mRNA vaccines—for COVID-19 and other diseases—to the continent and adapt them for the setting, such as doing away with the need for deep freezing and making them more stable at room or refrigerated temperatures. Those involved in the effort hope more African national governments will prioritize vaccine development and manufacturing, ultimately allowing them to own the intellectual property on domestically produced vaccines that can help protect their own populations.
CHINA At a meeting on November 30, Vice Premier Sun Chunlan, the senior official in charge of China’s COVID-19 response, said that “with the decreasing toxicity of the Omicron variant, the increasing vaccination rate, and the accumulating experience of outbreak control and prevention, China’s pandemic containment faces new stage and mission.” These remarks, as well as state media downplaying the severity of the Omicron variant and a few cities lifting lockdown restrictions, signal a potential shift in China’s pandemic response strategy, though no explicit policy changes have been made yet.
To date, China has relied on its “zero-COVID” policy—comprising isolation for all known cases, quarantining anyone who may have come into contact with COVID-19, strict lockdowns, school and business closures, mandatory testing, and home confinement, sometimes without access to supplies—which has led to entire cities shutting down for weeks or months. Recently, public anger over the human costs of China’s zero-COVID policy sparked public unrest and numerous protests that brought together a diverse group, including workers, students, rural residents, and middle-class people. The events are notable because public protest is rare in China, where the central government strictly cracks down on dissent and has established a high-tech surveillance state.
This week, 2 of China's largest cities, Guangzhou and Chongqing, announced they were easing COVID-19 restrictions. In Chongqing, close contacts of positive COVID-19 cases will be allowed to quarantine at home instead of at centralized, government-run centers. Guangzhou is lifting lockdowns in 4 districts (though lockdowns remain in high-risk areas), allowing close contacts of COVID-19 cases to quarantine at home instead of central facilities, and is no longer launching district-wide mass COVID-19 testing.
Some experts believe the government’s zero-COVID strategy is likely to stay in place until vaccination rates increase, especially among older adults, and a long-term strategy for living with COVID-19 can be established. China’s National Health Commission is launching a national campaign to encourage people who are over 60 years old to be vaccinated and boosted. The campaign will bring vaccines to people in nursing homes, go door-to-door, use mobile vaccination stations for older adults who cannot leave their homes, and press those who are reluctant to give a reason for not being vaccinated. With changes on the horizon, China’s leadership must reckon with the large economic and social toll their blanket approach to controlling COVID-19 is taking while also accounting for the burden that soaring numbers of new infections will place on the country’s health care system.
WORLD AIDS DAY World AIDS Day is commemorated annually on December 1, to show support for people living with and affected by HIV and to remember the approximately 40 million people who have died of AIDS-related illnesses. This year’s theme is “Equalize,” a call to action to address inequalities and continue to work toward ending the AIDS pandemic. Data from UNAIDS, however, show the COVID-19 pandemic and other global crises have impacted progress against HIV/AIDS, shrinking available resources and interrupting access to vital treatment and prevention services. In South Africa, which has the largest population of people living with HIV, some girls and women turned to transactional sex during COVID-19 lockdowns to support their families, increasing their risk of becoming infected. In a joint report, WHO and the European Centre for Disease Prevention and Control (ECDC) said the number of people in Europe living with undiagnosed HIV rose in 2021, when one quarter fewer HIV diagnoses were recorded compared with pre-pandemic levels in the WHO European region. UK Health Security Agency (UKHSA) data show that while new HIV diagnoses fell in England by nearly one-third between 2019 and 2021, progress toward ending HIV transmission has slowed, particularly among heterosexual people. In the US, President Joe Biden outlined steps his administration has taken against the AIDS pandemic, highlighting the ongoing need to better address racial, gender, and other inequities in health systems, through domestic and international programs. The many lessons learned from decades of action against AIDS can serve as a model for how policymakers, public health practitioners, and civil society deal with health threats, including COVID-19, monkeypox/mpox, and other infectious diseases. Importantly, the biomedical, social, and structural actions needed to end AIDS will better prepare the world to address future pandemics.
TWITTER MISINFORMATION POLICY Public health experts, healthcare professionals, and social media researchers are expressing concern after Twitter quietly ended its enforcement of its policy against COVID-19 misinformation on November 23. Twitter implemented the policy in 2020, during the early days of the pandemic, and since then had suspended more than 11,000 accounts and removed more than 100,000 posts for violating the policy. Though many agree the policy was imperfect, the lack of enforcement likely will lead to more false claims about COVID-19, including about the origin of the virus or the safety and effectiveness of vaccines. The move is the latest in a series of rollbacks at Twitter, implemented since the company was purchased by Elon Musk, who himself has spread COVID-19 misinformation.
by Suliso By the way any of you know anyone personally who died from covid or had to be hospitalized? I do not...
by ponchi101
Suliso wrote: ↑Fri Dec 02, 2022 11:30 am
By the way any of you know anyone personally who died from covid or had to be hospitalized? I do not...
My cousin's husband, unvaccinated and a recovering cancer patient. Died.
A lady that was my mom's friend (I did know her). Died.
One close friend that ended up quarantined in Caracas (not hospitalized, so not exactly what you are asking).
But, overall, nobody really close. My mom got it last year and I had to go to Caracas because my sister later admitted she thought I was going for the funeral.
by Owendonovan Ugh, I just tested positive for COVID for the second time. So far asymptomatic. Vaxxed and boosted 3x.
by atlpam A co-worker of mine died of Covid in 2021. Probably the delta variant and if I had to guess, I would say he wasn’t vaccinated. Last night I met a neighbor who revealed she spent 7 weeks in the hospital, including 12 days on a ventilator in 2021 (also unvaccinated).
Other than that, just extended family of people I know, but did not know personally.
by dryrunguy
Suliso wrote: ↑Fri Dec 02, 2022 11:30 am
By the way any of you know anyone personally who died from covid or had to be hospitalized? I do not...
My oldest brother of course. Though he had no fewer than about 8142 risk factors for death.
by Deuce I know one elderly woman (about 80 years old) who died of COVID.
And one woman in her mid-50s who was hospitalized for about a week due to COVID.
A rapid antigen test indicated I had COVID about 2 months ago. I had a fever of 104 degrees, but no hospitalization.
by skatingfan
Suliso wrote: ↑Fri Dec 02, 2022 11:30 am
By the way any of you know anyone personally who died from covid or had to be hospitalized? I do not...
The years that I spent working in a major retailer have meant that I know many people in the community, and the community I live in skews towards seniors, and several of them were seriously ill, hospitalized, and a few died, but also similar to Ponchi in that none of these people were close to me.
My brother dated Dave Dutton's daughter for a number of years. They broke up years ago, but Dave remained a friend of the family, and I used to see him regularly at my previous job. https://ottawacitizen.com/news/local-ne ... ing-editor
by ti-amie Yaneer Bar-Yam
@yaneerbaryam@forall.social
Please let anyone know who is waiting for The CDC to recommend masks, that they are now recommending masks.
"CDC Director Dr. Rochelle Walensky said wearing a mask is an everyday precaution that people can take to reduce their chances of catching or spreading a respiratory virus.
Note: Let them know to wear N95 masks that fit well.
#Covid
by ti-amie
by dryrunguy I received a new Situation Report from Johns Hopkins yesterday and kind of forgot to post it here. Haven't read it yet.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 643 million cumulative cases and 6.62 million deaths worldwide as of December 8. Global weekly incidence remained relatively stable last week, decreasing 1.3% compared to an increase of 16.8% the previous week. A total of 3.04 million cases were confirmed the week of November 28. Weekly incidence fell over the previous week in Africa (-64%)*, South-East Asia (-27%), Western Pacific (-10%), and the Eastern Mediterranean (-4%). The Americas (+14%) and Europe (+4.5%) regions experienced increasing weekly incidence. Global weekly mortality decreased from the previous week, down 17%.
*The WHO dashboard notes that data from the Africa region are incomplete.
UNITED STATES
The US CDC is reporting 98.8 million cumulative cases of COVID-19 and 1.08 million deaths. Incidence for the week ending November 30 remained relatively stable over the previous week, falling to 303,101 cases from 306,856 cases for the week ending November 23. Weekly mortality fell significantly for the week ending November 30, with 1,780 reported deaths compared to 2,634 deaths the week ending November 23. The decline could be a result of delayed reporting due to the US Thanksgiving holiday.**
**The US CDC updates weekly COVID-19 data on cases and deaths on Thursdays by 8pm ET.
Both new hospital admissions and current hospitalizations continue to rise, increasing last week by 20% and 18%, respectively, over the previous week.
The Omicron sublineages BQ.1.1 (32%) and BQ.1 (31%) together represent the most dominant subvariants of sequenced specimens. A host of other Omicron sublineages—including BA.5 (14%), BF.7, XBB, BN.1, BA.4.6, BA.5.2.6, BF.11, BA.2, BA.2.75, BA.2.75.2, and others—make up the remainder of cases.
US SENATE COMMITTEE REPORT Initial efforts to curb the novel SARS-CoV-2 outbreak in early 2020 was “one of the worst public health responses in US history,” according to a 242-page report released today by Democrats on the US Senate Homeland Security and Governmental Affairs Committee. The latest of several federal efforts to evaluate the nation’s pandemic response, the report focuses only on the first few months of the pandemic, saying the federal government “failed to heed critical public warnings” and has many longstanding and ongoing “systemic problems” that hamper US government preparedness and response capacities. Those problems include weaknesses in data collection and analysis, insufficient testing capacity, supply chain vulnerabilities, overlapping government roles, and, critically, “insufficient funding across multiple administrations.”
Some of the report’s recommendations will require new legislation and funding, according to the authors, although they did not offer an amount. US CDC Director Dr. Rochelle Walensky in an interview with Roll Call this week said the agency is running out of funding to help stave off a winter COVID-19 surge and for other near-term activities. In addition to calling for more funding, she urged the US Congress to improve CDC’s authority to collect data. The White House last month requested nearly US$10 billion more for short-term pandemic response needs, but lawmakers so far have refused to include additional COVID-19 spending in a year-end funding bill.
MASK USE The US CDC is once again encouraging people to wear masks to help reduce the spread of respiratory illnesses, as hospitalizations rise due to the so-called “tripledemic” of COVID-19, RSV, and flu. The nation appears to be at the start of another COVID-19 wave, with hospitalizations reaching a 3-month high last week. Hospitals are already feeling strain from earlier-than-normal increases in RSV and flu cases and hospitalizations. The US is experiencing the highest levels of hospitalization from flu that it has seen in a decade this early in the season. Experts warn that holiday gatherings present a prime opportunity for respiratory viruses to spread and urge people to take precautions, including mask use, physical distancing, testing, and increased air ventilation. While it is unlikely that widespread mask mandates will return, masking in crowded areas can lower the risk of infection and help decrease the burden on overwhelmed hospitals.
One more reason to don a mask during the colder months could be to help keep your nose warm. A study published this week in the Journal of Allergy and Clinical Immunology suggests that exposure to cold temperatures hinder immune responses in the upper respiratory tract by killing nearly half of the virus and bacteria-fighting cells in the nostrils, allowing viruses or bacteria to evade this initial immune response.
INDOOR AIR QUALITY The Lancet COVID-19 Commission Task Force on Safe Work, Safe Schools, and Safe Travel recently published a report on air delivery rates capable of reducing the spread of airborne diseases indoors. The report states that air filtration and ventilation targets in current building standards were not designed to prevent the spread of airborne diseases, including SARS-CoV-2, and the authors recommend a set of new non-infectious air delivery rate (NADR) targets that could improve overall occupant health and prevent the spread of respiratory illnesses. The NADR targets include a gradient from good to best of 4 air changes per hour, 6 air changes per hour, and greater than 6 air changes per hour. Some research indicates that 5 air changes per hour can reduce the risk of SARS-CoV-2 transmission by approximately 50%.
Additionally, the Board of Directors of the American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE) this week announced intentions to develop an indoor air quality standard for pathogen mitigation within the next 6 months. ASHRAE’s 2022-2023 President, Farooq Mehboob, further affirmed commitment to the idea that the health and wellbeing of building occupants should be a crucial aspect of building design and operation. The standard is expected to contain aspects related to building design and operation, alternative pathways for clean air, and testing and verification.
The Lancet COVID-19 Commission Task Force report and ASHRAE announcement come at a time when more governments and professional organizations are examining indoor air quality as a means to reduce disease transmission. Mechanical interventions to disease transmission, such as air filtration and ventilation, can be applied throughout an entire building and are not reliant on the individuals' actions to work effectively. The recent increase in attention to indoor air quality has largely been driven by the COVID-19 pandemic, but long-term improvements will continue to reduce the risk of other respiratory diseases such as influenza, measles, RSV, and others.
COST OF TREATMENTS & VACCINES As federal funding to support COVID-19 healthcare runs out, US residents without insurance are finding it increasingly difficult to receive the necessary care that was universally accessible only months ago. The Biden administration’s requests to the US Congress for additional funding for the COVID-19 response so far have been unsuccessful, despite the potential for new variants and a winter surge in cases. The federal government expects to allow manufacturers of COVID-19 vaccines and treatments to move their products to the commercial market by summer 2023, which could further limit access to people without insurance and others who do not have the means to pay.
As a result, public health experts predict that fewer people will seek lifesaving COVID-19 treatments, such as Paxlovid. Paxlovid has been administered at no cost to nearly 6 million US residents, as a result of federal funding; however, with dwindling funding and restrictions preventing Medicare coverage of the treatment, drug pricing is certain to become a substantial barrier for those seeking the therapy. The federal government has been able to purchase Paxlovid for $530 per course—a significantly discounted rate, according to Pfizer, the drug’s manufacturer. Likewise, the Biden administration has announced it no longer has funding to purchase additional COVID-19 vaccines, without action from Congress, and provide them at no cost to consumers. An analysis from KFF shows the cost of the Pfizer-BioNTech and Moderna COVID-19 vaccines is expected to increase at least 3-fold from the pre-purchased federal price when the products reach the commercial market, to approximately US$96 to US$130 per dose.
BIVALENT VACCINES The US CDC last week published its first “real-world” effectiveness data on updated bivalent SARS-CoV-2 mRNA boosters, showing the shots provided significant additional protection against symptomatic SARS-CoV-2 infection among people who previously received 2, 3, or 4 monovalent vaccine doses. Notably, the benefit of the bivalent booster increased with time since receipt of the most recent monovalent vaccine dose. The data were collected from pharmacy-based testing conducted between September 14 and November 11, 2022. Another study, published December 6 in Nature Medicine by researchers from the University of Texas Medical Branch, showed the bivalent boosters elicited a robust antibody response against the Omicron BA.4/BA.5 subvariants but not against the more recent BA.2.75.2, BQ.1.1, or XBB.1 Omicron subvariants, possibly because of their additional mutations in the spike protein. The researchers noted the adaptability of the mRNA platform and suggested future boosters be altered to match newly emerged variants.
In related news, the European Medicines Agency (EMA) this week backed the use of bivalent mRNA vaccines targeting both the original SARS-CoV-2 strain and the Omicron BA.4/BA.5 subvariants as a primary series in previously unvaccinated adults and children. The agency said the decision was based on data suggesting the bivalent vaccines should produce a robust immune response in previously unvaccinated and unexposed individuals and have a similar safety profile to the original mRNA vaccines. This recommendation paves the way for national authorities in Europe to use the bivalent mRNA technology in future vaccine campaigns.
In the United States, Pfizer-BioNTech has asked the US FDA to authorize their bivalent mRNA vaccine for use in children under age 5 as part of the initial vaccine series. Currently, children under 5 receive 3 small doses of the monovalent vaccine formula targeting the original SARS-CoV-2 strain. The series that Pfizer-BioNTech is asking regulators to authorize would replace the 3rd shot in the primary series with a dose of the bivalent vaccine. Pfizer and BioNTech say the new series could help prevent severe illness and hospitalization among children at a time when other respiratory diseases, such as influenza and RSV, are straining hospital systems.
US MILITARY VACCINE MANDATE US House and Senate lawmakers this week released a compromise US$858 billion defense authorization bill that would increase military spending by 8% over fiscal year 2022 levels and rescind the military’s COVID-19 vaccine mandate for service members. The mandate—which required troops to be separated if they refused the vaccine and did not receive a waiver—became a point of contention in recent days’ talks, after conservatives threatened to hold up the bill if the measure was not removed from the final version of the National Defense Authorization Act (NDAA). Both the White House and US Secretary of Defense Lloyd Austin want to keep the vaccine mandate in place to protect the health of military members and national readiness. The White House declined to explicitly state whether US President Joe Biden will sign the annual defense bill if it includes the provision to rescind the mandate. Both the House and Senate need to pass the bill before it heads to President Biden.
CHINA On December 7, China announced significant easing of its strict “zero COVID” policy, including relaxation of frequent mass PCR testing and digital health codes that were required for people to go about their daily life or travel within the country. The changes, released by the State Council in a 10-point plan, also allows those with less severe coronavirus infections to quarantine at home rather than in centralized facilities. The changes, an extension of a November 20-step “optimization” plan aimed at reducing the economic and social costs of restrictions, came after unprecedented protests in more than a dozen cities nationwide over recent weeks. Many residents expressed relief over the policy’s relaxation but some, including health experts, voiced unease over the rapidity of the changes, leaving many concerned that the population is unprepared for what could be an impending surge in cases. Most people in China have not been exposed to the virus, which would have given residents some natural immunity; vaccination and booster rates are lagging, especially among older adults; and the country’s domestically developed vaccines offer suboptimal protection compared to mRNA vaccines. Additionally, some experts say China has not effectively communicated how to move from "dynamic" suppression to mitigation, leaving some people believing they can simply return to pre-pandemic life.
Some are worried a spike in infections will overwhelm the healthcare system and bring a high death toll—as many as 1 million people, according to some models. Already, hospitals are reporting an influx of COVID-19 patients and rationing fever medicines such as ibuprofen and paracetamol because of shortages. The Chinese government appears to be placing some faith in what they say is a “less pathogenic” Omicron variant, but experts warn that all of Omicron’s sublineages remain capable of causing severe disease and post-acute COVID-19 symptoms, particularly in a population with little to no natural immunity. To some experts, it appears China is moving out of its “zero COVID” restrictions without a solid plan—such as strategies implemented by Australia, New Zealand, and Singapore, all of which followed some type of zero COVID approach—and at a time when the dominant viral strains are more transmissible. For now, China—and the world—will have to wait and see how the nation fares.
GLOBAL ACCESS TO MEDICAL COUNTERMEASURES Global demand for COVID-19 vaccines is falling rapidly worldwide. The Board of Directors of Gavi, the Vaccine Alliance, the nonprofit organization that led the COVAX initiative, is set to vote this week on a proposal to allow the vaccine delivery mechanism to lapse sometime in 2023. If approved, no-cost COVID-19 vaccines would be included in Gavi’s standard immunization programming for the 54 low-income nations that traditionally receive the organization’s support, and 37 other middle-income nations would receive a one-time payout to help them establish their own COVID-19 vaccination programs. The Board is also considering other issues, including efforts to bolster or begin routine immunization programs that were delayed during the pandemic and a proposal from the Gavi secretariat to keep a “pandemic preparedness pool” of US$1.8 billion to allow the acquisition of future COVID-19 vaccine doses. Some Board members expressed concern over the latter proposal, saying such a fund could unintentionally broaden Gavi’s mandate and that the organization does not have governance in place to manage those funds.
In related news, the US government has expressed support for extending a December 17 deadline to decide whether the World Trade Organization’s Ministerial Decision on waiving intellectual property protections for COVID-19 vaccines should encompass diagnostics and treatments. US Trade Representative Ambassador Katherine Tai said her agency will ask the US International Trade Commission to investigate certain market dynamics such as pricing, production, access, and supply and demand, a process that usually takes 9-12 months. The move will delay the prospects of a World Trade Organization agreement meant to improve global access to COVID-related medical countermeasures.
ti-amie wrote: ↑Tue Dec 06, 2022 7:47 pm
Yaneer Bar-Yam
@yaneerbaryam@forall.social
Please let anyone know who is waiting for The CDC to recommend masks, that they are now recommending masks.
"CDC Director Dr. Rochelle Walensky said wearing a mask is an everyday precaution that people can take to reduce their chances of catching or spreading a respiratory virus.
Note: Let them know to wear N95 masks that fit well.
#Covid
I've never stopped masking, those not wearing masks on public transportation in NYC is about 80-85%. Masks really only bother me in the summer with humidity. Seems a majority of people just don't care about COVID any longer as we grow more and more numb.
ti-amie wrote: ↑Tue Dec 06, 2022 7:47 pm
Yaneer Bar-Yam
@yaneerbaryam@forall.social
Please let anyone know who is waiting for The CDC to recommend masks, that they are now recommending masks.
"CDC Director Dr. Rochelle Walensky said wearing a mask is an everyday precaution that people can take to reduce their chances of catching or spreading a respiratory virus.
Note: Let them know to wear N95 masks that fit well.
#Covid
I've never stopped masking, those not wearing masks on public transportation in NYC is about 80-85%. Masks really only bother me in the summer with humidity. Seems a majority of people just don't care about COVID any longer as we grow more and more numb.
I've never stopped masking either. It's always seemed a bit reckless to me since the virus is still romping.
ti-amie wrote: ↑Tue Dec 06, 2022 7:47 pm
Yaneer Bar-Yam
@yaneerbaryam@forall.social
Please let anyone know who is waiting for The CDC to recommend masks, that they are now recommending masks.
"CDC Director Dr. Rochelle Walensky said wearing a mask is an everyday precaution that people can take to reduce their chances of catching or spreading a respiratory virus.
Note: Let them know to wear N95 masks that fit well.
I've never stopped masking, those not wearing masks on public transportation in NYC is about 80-85%. Masks really only bother me in the summer with humidity. Seems a majority of people just don't care about COVID any longer as we grow more and more numb.
Owendonovan wrote: ↑Sat Dec 10, 2022 4:11 pm
I've never stopped masking, those not wearing masks on public transportation in NYC is about 80-85%. Masks really only bother me in the summer with humidity. Seems a majority of people just don't care about COVID any longer as we grow more and more numb.
I've never stopped masking either. It's always seemed a bit reckless to me since the virus is still romping.
I have been wearing a mask (N95) in indoor settings, as well, throughout. And I, too, see about 85% to 90% of people in indoor public settings - including buses and subways - being without masks. It's incredibly disappointing. People won't do the right thing unless it's mandated - just like 7 year old children won't do something unless they are threatened with punishment from their parents.
It's pathetic.
That's the thing with human beings - 'comfort' and 'convenience' win out over all else - including basic common sense.
People are so incredibly desperate to be 'comfortable' and to have everything be 'convenient' that they completely ignore the very real consequences of prioritizing these two elements. There is a cost to every comfort and to every convenience.
These people are living in an illusionary state... and they'll be the first to whine "Why is this happening to me - this isn't fair!" once they're hospitalized with COVID.
This mentality of creating illusions is so strong that it is really a game of pretending that everything is fine just because they want it to be. They create their own alternate 'reality' while completely ignoring the facts. Much like children do with their fantasy games, pretending that they are superheroes who can fly, etc. The main difference being that children don't take it as far as adults do - children don't actually attempt to fly...
Not to mention the utter selfishness of these people who won't even mask up to protect others!
It's not that they don't understand - it's that they voluntarily refuse to understand. They prefer their comfortable illusion. This illusionary state reaches far, far beyond just COVID, of course - it goes into all aspects and elements of life.
And then, rather separately, you have the fools who refuse to mask under a very, very misguided definition of 'freedom'... Sigh...
by skatingfan
Owendonovan wrote: ↑Sat Dec 10, 2022 4:11 pm
I've never stopped masking, those not wearing masks on public transportation in NYC is about 80-85%. Masks really only bother me in the summer with humidity. Seems a majority of people just don't care about COVID any longer as we grow more and more numb.
ti-amie wrote: ↑Sat Dec 10, 2022 6:41 pm
I've never stopped masking either. It's always seemed a bit reckless to me since the virus is still romping.
I think the lack of mandates is giving a lot of people mixed messages - it sinks in more if you're being asked to do it everywhere you go.
by ponchi101 WORKERS are supermarkets here are wearing them, on and off.
Most everybody else are not. I am usually one of 3-4 on the bus wearing one. I take it off when I am walking, though.
by Suliso I'd say less than 10% are wearing masks in public transport here. Nobody at work (100+ people). Can't keep masking alll your life...
by Deuce
Suliso wrote: ↑Sun Dec 11, 2022 8:37 am
I'd say less than 10% are wearing masks in public transport here. Nobody at work (100+ people). Can't keep masking alll your life...
Why not?
They've been masking in public settings - even outdoors - in some Asian countries since long, long before COVID appeared.
If I feel that my life stands to endure significantly longer if I mask than if I don't, I'll mask in indoor public settings for the rest of my life. At worst, it's a minor inconvenience and minor expense.
Not to mention, of course, that my masking also protects other people who may be particularly vulnerable. So it's also not as selfish as not masking and pretending that all is as it was pre-COVID.
The only element I don't like about masking is that it creates more garbage, as masks are notoriously difficult to recycle. But hopefully a viable way to recycle masks will be found soon.
by dryrunguy
Suliso wrote: ↑Sun Dec 11, 2022 8:37 am
I'd say less than 10% are wearing masks in public transport here. Nobody at work (100+ people). Can't keep masking alll your life...
Sure we could. Early on in the pandemic, I said to myself, "We should have been masking all along." People in China and some other parts of the world have been doing it as protection against environmental exposures. All personnel in hospitals and medical facilities should have been doing it all along and should still be doing it. Yet, when my brother was in the hospital before he died, there was this huge, muscular dude who was with my brother to keep him under control. He wasn't masked. In a hospital. Watching over someone who had recently had COVID. But he never wore a mask when I was visiting.
It's just good protective hygiene that can help prevent not just COVID but any other airborne germ or environmental exposure. I have no plan to stop. The next airborne disease could be right around the corner. (Not to mention, COVID ain't gone yet--no matter how much people want to pretend it no longer exists).
by Deuce I had an appointment for my 3rd COVID booster vaccine last week. I went to my appointment... but I didn’t get the vaccine.
After doing some research, I decided that I wanted the Moderna bivalent booster which targets the BA.4 and BA.5 variants. I have had Moderna vaccines all along, so I wanted to stay with them, and my research showed that the Moderna booster targeting BA.4 and BA.5 was more efficient than the Moderna booster targeting BA.1.
When it was time for me to get my booster, I asked the person who would be puncturing me which vaccines she had. She said they have the Moderna BA.1 and Pfizer BA.4/BA.5. I asked why that is. She told me that they’ve been told to use up all of the Moderna BA.1 boosters before making the BA.4/BA.5 booster available to people.
I asked when the Moderna BA.4/BA.5 would be available, She asked a supervisor, and he said that he thinks they’ll have it this weekend. He offered to call or text me to let me know when they receive it. But I haven’t heard from him as yet.
Of course, it’s possible that he forgot about me.
In any case, I declined both the Moderna BA.1 and the Pfizer BA.4/BA.5, and plan on waiting until I can access the Moderna BA.4/BA.5.
They also asked if I wanted the ‘flu vaccine, as well (which is free in Canada for everyone). I said ‘No’.
I have never had the ‘flu vaccine, and never contemplated it... but this year, I have thought about possibly getting it, as the ‘flu is more prevalent and more serious this year than in the recent past. I will continue thinking about possibly getting the ‘flu vaccine - but for now, it’s still a ‘No’.
Suliso wrote: ↑Sun Dec 11, 2022 8:37 am
I'd say less than 10% are wearing masks in public transport here. Nobody at work (100+ people). Can't keep masking alll your life...
Sure we could. Early on in the pandemic, I said to myself, "We should have been masking all along." People in China and some other parts of the world have been doing it as protection against environmental exposures. All personnel in hospitals and medical facilities should have been doing it all along and should still be doing it. Yet, when my brother was in the hospital before he died, there was this huge, muscular dude who was with my brother to keep him under control. He wasn't masked. In a hospital. Watching over someone who had recently had COVID. But he never wore a mask when I was visiting.
It's just good protective hygiene that can help prevent not just COVID but any other airborne germ or environmental exposure. I have no plan to stop. The next airborne disease could be right around the corner. (Not to mention, COVID ain't gone yet--no matter how much people want to pretend it no longer exists).
Serious here. C19 will not go away EVER. This thing is too prevalent and mutates with ease. It is here to stay, like almost all infectious and transmittable diseases (flus, STD's, etc).
So, you are willing to spend the rest of your life wearing a mask? I am just asking.
Suliso wrote: ↑Sun Dec 11, 2022 8:37 am
I'd say less than 10% are wearing masks in public transport here. Nobody at work (100+ people). Can't keep masking alll your life...
Sure we could. Early on in the pandemic, I said to myself, "We should have been masking all along." People in China and some other parts of the world have been doing it as protection against environmental exposures. All personnel in hospitals and medical facilities should have been doing it all along and should still be doing it. Yet, when my brother was in the hospital before he died, there was this huge, muscular dude who was with my brother to keep him under control. He wasn't masked. In a hospital. Watching over someone who had recently had COVID. But he never wore a mask when I was visiting.
It's just good protective hygiene that can help prevent not just COVID but any other airborne germ or environmental exposure. I have no plan to stop. The next airborne disease could be right around the corner. (Not to mention, COVID ain't gone yet--no matter how much people want to pretend it no longer exists).
Serious here. C19 will not go away EVER. This thing is too prevalent and mutates with ease. It is here to stay, like almost all infectious and transmittable diseases (flus, STD's, etc).
So, you are willing to spend the rest of your life wearing a mask? I am just asking.
Absolutely, ponchi. Who am I hurting by being masked? Pretty sure it's no one. And the inconvenience to me is beyond minor. To quote the old spiritual, "ain't got time to die." And I certainly don't have time for and cannot afford long COVID. Long COVID alone could decimate me financially, even with the extensive advanced financial planning I've done. No thanks.
The minor inconvenience is a tiny price to pay.
by Suliso You guys are free to keep masking. I certainly don't mind.
by ponchi101 Ok, fair enough.
Marketing ploy for making everybody wear masks: You actually LOOK better when masked. Almost all humans have beautiful eyes. Not everybody has a beautiful nose/mouth combo.
See how people start masking again.
by MJ2004 My parents have COVID. My mom is in the hospital. Her oxygen levels were low so they’re admitting her. They just flew down to Florida on Wed so likely caught it in transit.
Be safe traveling over the holidays as best you can.
We’re flying down tomorrow and rather than cancel we’ve booked a hotel for the first few days so we can stay close.
by ponchi101 I hope she will be fine soon. Keep us posted, and take care too.
Wish you the best.
by ti-amie Wishing your parents the best MJ.
This thing is brutal.
by MJ2004 Thanks. Cases are spiking big time here.
She also has pneumonia. Sigh.
by ti-amie
MJ2004 wrote: ↑Sun Dec 18, 2022 8:15 pm
Thanks. Cases are spiking big time here.
She also has pneumonia. Sigh.
Are you talking about where you live or Florida? According to the governor of Florida there's no spike in the state he governs.
by MJ2004 I meant here in Massachusetts.
Florida, they didn’t even ask my dad to wear a mask in the hospital. I’m sure they’re prohibited from doing so.
by ti-amie
by ponchi101 Part of this is the quality of their vaccine. It really is bad.
My mom's second dose was with that. I have to talk to her about it.
by Deuce
MJ2004 wrote: ↑Sun Dec 18, 2022 4:29 pm
My parents have COVID. My mom is in the hospital. Her oxygen levels were low so they’re admitting her. They just flew down to Florida on Wed so likely caught it in transit.
Be safe traveling over the holidays as best you can.
We’re flying down tomorrow and rather than cancel we’ve booked a hotel for the first few days so we can stay close.
Wishing the best for your parents - and your mom in particular.
Please remember that, though hospital admission is frightening, it's also the best place to be to receive the care that she needs.
And a reminder to everyone - despite what the politicians want us to believe, COVID-19 is not behind us, and is just as present today as it was a year ago, if not more so.
Protect yourself and others by wearing a mask, washing your hands, and keeping your physical distance.
by ti-amie mmalc
@mmalc@mastodon.social
“China's public health officials say that possibly 800 million people could be infected with the coronavirus over the next few months. And several models predict that a half million people could die, possibly more.”
“… about 10% of the planet's population may become infected over the course of the next 90 days.”
by ponchi101 The USA has seen 1 million dead. Out of 360MM people (rough population count).
China has 1,4 Billion. How does the math for ONLY 500,000 work out? The USA has better facilities, and has been using a better vaccine.
Assume mortality rates of 1%, and if the infected population is expected to be 800 MM, the death rate would be 8 million.
Somebody help me here.
by Deuce If anywhere near that many people become infected with COVID-19 in China, that rate of infection risks spreading to other countries with travel to and from China.
But it's ok, because the politicians say that the pandemic is over.
by ti-amie
Deuce wrote: ↑Mon Dec 19, 2022 10:50 pm
If anywhere near that many people become infected with COVID-19 in China, that rate of infection risks spreading to other countries with travel to and from China.
But it's ok, because the politicians say that the pandemic is over.
by Suliso We're all rightly aghast at events in China, BUT it's not so obvious what was a better way out for their government. Lockdowns forever were not sustainable either... You might say buying Western vaccines, but that would be so shameful...
by ponchi101
Suliso wrote: ↑Tue Dec 20, 2022 7:15 am
We're all rightly aghast at events in China, BUT it's not so obvious what was a better way out for their government. Lockdowns forever were not sustainable either... You might say buying Western vaccines, but that would be so shameful...
Who is saying BUYING? Do what the Chinese government has always done: copy them.
It is not as if the Chinese ever have given half a (expletive) about copyrights or anything like that. And, in this case, they may have a point.
by MJ2004 If you look at it as a governmental experiment, China has successfully tested how far they can push the citizens before revolts started. Now time to step back.
by Suliso
ponchi101 wrote: ↑Tue Dec 20, 2022 2:38 pm
Who is saying BUYING? Do what the Chinese government has always done: copy them.
It is not as if the Chinese ever have given half a (expletive) about copyrights or anything like that. And, in this case, they may have a point.
If just copying was so easy to do they would have copied top of the line microchips ages ago. I suspect they simply lack technical know how in this very new mRNA field.
by ti-amie
MJ2004 wrote: ↑Tue Dec 20, 2022 3:17 pm
If you look at it as a governmental experiment, China has successfully tested how far they can push the citizens before revolts started. Now time to step back.
by dryrunguy Here's the latest Situation Report from Johns Hopkins.
::
EPI UPDATE The WHO COVID-19 Dashboard reports 650 million cumulative cases and 6.65 million deaths worldwide as of December 20. Global weekly incidence remained relatively stable last week, increasing 4.8% compared to an increase of 12% the previous week. A total of 3.8 million cases were confirmed the week of December 12. Weekly incidence fell over the previous week in South-East Asia (-36%), Africa (-29%), Eastern Mediterranean (-26%), Europe (-9%). Weekly incidence increased in the Americas (+18%) and Western Pacific (+8%) regions. Global weekly mortality remained relatively stable compared with the previous week, down 5%.
UNITED STATES
The US CDC is reporting 99.7 million cumulative cases of COVID-19 and 1.08 million deaths. Incidence for the week ending December 14 remained relatively stable over the previous week, falling to 455,466 cases from 469,240 cases for the week ending December 7. Weekly mortality fell for the week ending December 14, with 2,703 reported deaths, compared to 3,115 deaths the week ending December 7.
Both new hospital admissions and current hospitalizations began falling last week, both down 10% over the previous week.*
*Due to a change in COVID-19 hospital data reporting guidance, the CDC urges caution in interpreting data immediately reported after December 15, 2022, when the transition to the CDC’s National Healthcare Safety Network (NHSN) began. Additional information on the transition can be found here.
The Omicron sublineages BQ.1.1 (38%) and BQ.1 (31%) together represent the most dominant subvariants of sequenced specimens in the US. BA.5 (10%) accounts for a dwindling proportion of cases, and a growing proportion of cases are due to XBB (7.2%). A host of other Omicron sublineages—including BF.7, BN.1, BA.5.2.6, BA.4.6, BF.11, BA.2, BA.2.75, BA.2.75.2, and others—make up the remainder of cases.
US WINTER PREPAREDNESS PLAN The Biden administration last week announced a COVID-19 Winter Preparedness Plan in an attempt to stay ahead of what many experts believe will be a continued increase in COVID-19 cases this season. The plan involves reopening COVIDTests.gov, through which US residents can order up to 4 tests per household this winter; making more free tests available at community and rural health clinics, schools, food banks, and other convenient locations; offering resources and assistance to increase vaccine uptake, including pop-up and mobile vaccination sites; pre-positioning supplies from the Strategic National Stockpile to help prepare health facilities; monitoring emerging variants and their susceptibility to existing treatments and vaccines; and expanding efforts to increase vaccination rates in long-term care facilities and nursing homes.
White House COVID-19 Response Coordinator Dr. Ashish Jha stressed that the nation is facing other respiratory viruses, including RSV and one of the worst and earliest influenza seasons, which, along with COVID-19, are stressing hospital capacity. Dr. Jha encouraged people to receive an updated bivalent vaccine booster if they are eligible and have not done so already. US CDC data show that while about 69% of the US population has completed the primary 2-dose vaccine series, only about 14% of people aged 5 and older have received the updated booster.
According to recent polling from the Kaiser Family Foundation, many people are unsure about the benefit of the updated COVID-19 vaccine. But 2 new studies published last week in the CDC’s Morbidity and Mortality Weekly Report (MMWR) show the updated shots provide substantial protection against illness and hospitalization, particularly among seniors and including among people who had received 2-4 doses of the original monovalent vaccine. The studies used data from a period during predominance of the Omicron BA.5 subvariant, which the bivalent booster partially targets. Since then, the more immune-evasive Omicron sublineages of BQ.1 and BQ.1.1 have gained traction, and it is unclear how applicable the studies’ findings are to these new subvariants. Additionally, a recent analysis from the Commonwealth Fund shows earlier vaccines’ value. The report estimates that from December 2020 to November 2022, the US COVID-19 vaccination program prevented more than 18.5 million additional hospitalizations and 3.2 million additional deaths, as well as saved more than US$1 trillion in medical costs that would otherwise have been incurred. The analysis estimates there would have been nearly 120 million more COVID-19 infections without vaccination. The US FDA announced it will hold a meeting of its vaccines advisory board next month to discuss the future of COVID-19 vaccines, including whether people who have never received a shot should get the bivalent formulation as their first dose.
With other viruses that cause influenza-like illnesses or stomach flu circulating this season, experts agree taking individual actions can help reduce the risk of serious illness. Some of these actions include:
• Getting vaccinated against COVID-19 or getting the most recent COVID-19 booster*, as well as receiving a flu vaccine
• Wearing a high-quality mask while in crowded, indoor places
• Improving ventilation when possible, including opening doors and windows, running fans on HVAC systems, or installing high-quality air filters
• Practicing proper hand hygiene, including thorough hand washing or use of hand sanitizer when appropriate, especially when preparing or sharing food
• Staying home if showing any symptoms such as runny nose, cough, fevers, chills, nausea, body aches, or sore throat
• Testing for COVID-19 before and after traveling and before gathering indoors, particularly if older adults will be present
• Drinking plenty of water, especially while traveling or if consuming alcoholic beverages.
*The US FDA recently authorized and the CDC recommended bivalent boosters for children down to 6 months of age. Eligibility among this age group can be confusing, as it depends on what vaccine series—and how much of that series—has been received so far:
• Moderna: Children 6 months through 5 years who received the original, 2-dose Moderna vaccine are eligible to receive a single booster of the updated bivalent Moderna vaccine 2 months after completing the primary series.
• Pfizer:
• Children 6 months through 4 years who completed the 3-dose primary series are not eligible at this time.
• Children 6 months through 4 years who have not started the 3-dose primary series or who have not completed the series will receive the updated Pfizer vaccine as their third dose.
LONG COVID-RELATED MORTALITY Post-acute sequelae of COVID-19 (PASC), commonly known as long COVID, contributed to 3,544 deaths in the US from January 2020 through the end of June 2022, according to a recent report from the US CDC’s National Center for Health Statistics (NCHS). The deaths were identified using data entered on death certificates in the National Vital Statistics System, a methodology that could lead to an undercount, the report’s authors and other experts cautioned. The majority of long COVID-related deaths occurred among non-Hispanic white and older individuals.
An estimated 1 in 4 people with COVID-19 experience long COVID, which includes a complex constellation of symptoms—such as breathing problems, heart issues, fatigue, and cognitive and neurological issues—that can last for several months or longer or appear months after acute infection and can affect virtually every organ system. There is no agreed upon definition for the condition, and no diagnostic code for the condition existed until October 2021. Though knowledge about long COVID has improved over the past several years, and the US government earlier this year launched the National Research Action Plan on Long COVID, people impacted by the condition and their clinicians are urging more federal efforts and funding to support research, care, and education on the condition. Some experts warn long COVID could critically impact the nation’s economy and productive capacity in the short and long terms.
LONG-TERM CARE FACILITIES/NURSING HOMES As older adults, usually with underlying health conditions, nursing home and long-term care facility (LTCF) residents are at high risk of infection and death due to COVID-19, and the congregate nature of these facilities increases the risk of SARS-CoV-2 transmission. To examine the disproportionate impact the COVID-19 pandemic has had on LTCF/nursing home residents, the US Government Accountability Office (GAO) conducted an analysis of US CDC and Centers for Medicare & Medicaid Services (CMS) data. According to the report, released December 15, the average COVID-19 nursing home outbreak from June 2020 through December 2021 lasted 4 weeks and transmission of COVID-19 in the community surrounding a nursing home, known as community spread, had the strongest association with the duration of an outbreak. Additionally, the longest outbreaks were associated with nursing home facilities that had more than 100 beds, reported staff shortages, and were government-owned. Staff shortages and low staff morale were identified as critical challenges during interviews with officials from 6 nursing homes in 4 states, according to the report.
As of November 20, only 45% of nursing home residents and 22% of staff were up to date with their COVID-19 vaccines, according to recent analysis from the Kaiser Family Foundation. In light of this, the LCTF/nursing home industry is calling for changes to vaccination practices for residents. In a recent letter to US Health and Human Services Secretary Xavier Becerra, industry groups outlined an “all-hands-on-deck” approach to vaccinating residents, including efforts to better educate residents and their families about COVID-19, influenza, and other vaccines; reaching out to hospitals to vaccinate patients before discharging them to their facilities; mobilizing the National Guard to administer vaccines at facilities when LTCF pharmacies cannot; and reaching out to state and local public health agencies to conduct on-site vaccine clinics when needed. Hesitancy remains the primary obstacle to getting more residents and staff up to date on their vaccinations, which means completing a COVID-19 vaccine primary series and receiving the most recent booster dose recommended.
GLOBAL EXCESS MORTALITY An estimated 14.83 million excess deaths occurred during the first 2 years of the COVID-19 pandemic globally, 2.74 times more deaths than the 5.42 million reported as a result of COVID-19 for 2020 and 2021, according to a new WHO study published last week in Nature. India, Russia, Indonesia, the US, Brazil, and Mexico suffered the most estimated deaths due to COVID-19 during the 2-year period. Overall, 4 of 5 excess deaths in 2020 and 2021 occurred in either Southeast Asia—led by India—Europe, and the Americas. By comparison, heart disease was the leading worldwide cause of death in 2019, resulting in nearly 9 million deaths. The researchers said they expect COVID-19 was among the leading causes of death in 2020 and the leading cause of death in 2021. Knowing exactly how many people have died in the pandemic—including deaths from COVID-19 as well as those indirectly related to the pandemic, such as deaths related to interruptions and disruptions to healthcare—will never be possible.
GLOBAL HEALTH EMERGENCY WHO Director-General Dr. Tedros Adhanom Ghebreyesus last week said he is hopeful the COVID-19 global health emergency can end next year. The International Health Regulations (IHR) Emergency Committee for COVID-19 is expected to begin discussions in January outlining criteria for declaring an end to the COVID-19 Public Health Emergency of International Concern (PHEIC) declaration, first announced on January 30, 2020. Even if the emergency ends, COVID-19 is not going away. During an end-of-the-year press conference, Dr. Tedros noted several challenges, including the growing health burden of post-COVID conditions including long COVID, ongoing vaccine inequity and low vaccine uptake in some areas, remaining gaps and weaknesses in variant surveillance, and rising case numbers in several countries, including China. After highlighting several upbeat developments—such as a declining rate of COVID-19 deaths and falling numbers of mpox and Ebola cases—he called for more investment in pandemic preparedness so the world can be ready for the next emerging health threat. Notably, other experts said COVID-19 remains an emergency, warning the pandemic could worsen over the coming months.
CHINA In a rapid and stark reversal from its “zero COVID” policy, China has largely dropped much of its carefully crafted systems of lockdowns and mass testing. The unpopular policy most recently led to widespread protests, rarely seen in China, before being relaxed. Given the high transmissibility of the Omicron subvariants in circulation, predictions of a massive surge in cases across the country are coming true. COVID-19 is spreading rapidly through the population of 1.4 billion, many of whom are inadequately vaccinated and have little to no natural immunity.
On December 19, the Chinese government reported 2 COVID-related deaths, the first in weeks, but many within the country, as well as outside experts, say the low counts are implausible and ignore the high level of loss and grief the latest wave is causing. One of Beijing’s designated crematoria for COVID-19 patients has received a jump in requests for services, and authorities are rushing to increase the number of intensive care beds and healthcare workers, as well as increase dwindling medication supplies, signs of the human toll of abruptly loosening restrictions. Some provincial governments have suggested that people with mild COVID-19 illness continue to go to work, particularly healthcare and food delivery workers. The surge is also coming ahead of Lunar New Year in January, when millions are expected to travel to be with relatives for the holiday. Multiple models predict a winter wave of COVID-19 infections could kill up to 1 million people over the next several months.
China’s strategy has always been deeply political: President Xi Jinping staked the reputation of the Chinese Communist Party on the ability to control COVID-19 better than Western countries. But with the current COVID-19 situation appearing to spiral rapidly, President Xi is now in the position of deciding whether to accept foreign aid and from whom. European and US officials are in contact with Chinese counterparts, but public statements are being carefully worded to make clear the onus is on China to accept any offers of assistance in obtaining vaccines, treatments, or other countermeasures. China’s state media appear to be positioning the current surge as a pre-planned strategy, an “exit wave,” and promised a return to “normalcy by Spring.” Nevertheless, there remain global concerns that China’s situation will have long-term economic and social impacts and increase the risk of a new variant emerging.
by dryrunguy In other news, I got the Moderna bivalent booster today. And for the first time EVER, I got the flu shot. Too many of my work colleagues have been sick as dogs from the various bugs floating about all over the U.S.
::
BTW, masks are no longer required at the medical campus where I get my vaccines. Either people simply don't care, or they've given up. And not one person working at the pharmacy where I get my vaccines was masked. Not one.
::
While I was waiting to get my jabs, I overheard a very frail elderly woman who had come in to get a booster. She refused to get an mRNA vaccine (Pfizer or Moderna). She didn't say why. She wanted Novavax. They didn't have it. She left without getting a booster. I also overheard the pharmacy technician, basically, validate her and said, "A lot of people are choosing not to get boosters." Not untrue. But as a public health worker, why say that?
by ponchi101 The EXCESS DEATHS section of the report says it all: that 6.65 MM worldwide deaths figure is bull-(expletive). Be generous and only assign 50% directly to C19 (not other related issues). That doubles the figure automatically.
And, as it says: we will never know how many people have really died of it.
Make it a nice, round 16MM. That means that the mortality rate, over 3 years, is 0.2%.
Whether that is significant or not is very, very open to debate.
by Deuce The COVID-19 death rate among the planet's entire population - or among a country's population - is one thing - and is irrelevant.
The death rate of the people who have contracted COVID-19 is what is relevant. Unfortunately, that is impossible to calculate - both because of governments lying about the number of cases and deaths, and because far from every case of COVID is documented.
by MJ2004China estimates 250mn people have caught Covid in 20 days
Figures presented at closed-door meeting are in stark contrast to low official case count
Chinese officials estimate about 250mn people, or 18 per cent of the population, were infected with Covid-19 in the first 20 days of December, as Beijing abruptly dismantled restrictions that had contained the disease for almost three years.
The estimates — including 37mn people, or 2.6 per cent of the population, who were infected on Tuesday alone — were revealed by Sun Yang, a deputy director of the Chinese Center for Disease Control and Prevention in a Wednesday health briefing, said two people familiar with the matter.
Sun said the rate of Covid’s spread in the country was still rising and estimated that more than half of the population in Beijing and Sichuan were already infected, the people briefed on the meeting said.
The explosion in cases followed Beijing’s decision this month to abandon its zero-Covid policy, which kept the virus at bay through mass testing, mandatory quarantine and draconian lockdowns.
Sun’s figures, which were provided in a closed-door meeting, contrast with data put out by the National Health Commission, which reported 62,592 symptomatic Covid cases over the same period. Last week, China stopped publicly trying to tally the total number of infections after authorities curtailed Covid testing.
The lack of published official information has led Washington and the World Health Organization to push Beijing to be more transparent about case counts, disease severity, hospital admission figures and other health statistics that have been made widely available by other countries.
In China’s capital and other cities, the wave of Covid infections has overwhelmed hospitals with an influx of elderly, bedridden patients and left emergency rooms and intensive care units with few available beds.
Yet the country has proceeded with shedding the zero-Covid policy as the medical toll mounts. Hong Kong’s chief executive John Lee on Saturday announced that long-awaited quarantine-free travel between the city and mainland China would resume as early as mid-January.
“The central government has agreed to fully reopen the borders in a gradual and orderly manner,“ Lee told reporters after returning from a four-day trip to Beijing, where he met President Xi Jinping. “Families separated for nearly three years because of the pandemic can be reunited . . . [and] Hong Kong’s economy can be bolstered.”
Business chambers and industry leaders in the financial hub have for months called for a full border reopening as restrictions on movement hampered the territory’s economy, which is expected to suffer an annual contraction of 3.2 per cent this year.
The NHC’s official account of the Wednesday event provided little detail on what the country’s top health officials discussed.
But in the meeting, Ma Xiaowei, director of the NHC, demanded hospitals sort out overflowing emergency rooms and move patients into inpatient departments, said one of the people who participated in the event. He also urged midsized and large hospitals to take in more patients with severe symptoms and promised regulators would not hold them accountable for rising fatality rates.
Meanwhile, the estimate of 250mn cases raised further doubts about the accuracy of official Covid statistics and how authorities account for deaths from the disease.
The NHC reported just 4,103 new local cases on Saturday for the day prior, with no Covid-related deaths for a second consecutive day. Hong Kong, by contrast, reported 20,460 new local cases on Saturday for the previous 24 hours.
China has officially reported only eight deaths since December 1. Top health officials said this week that they had narrowed the definition of what constitutes a Covid death, in a move that reduced the public death tally.
However, crematoriums in China’s capital are struggling to handle a surge of corpses, and bodies were piling up at hospitals visited by the Financial Times in recent days.
Several models, including one partly funded by the Chinese CDC, have forecast that the country could suffer up to 1mn Covid deaths during its reopening.
The National Health Commission did not respond to a request for comment.
FT
Qianer Liu and Cheng Leng in Hong Kong, Sun Yu in Shanghai and Ryan McMorrow in Beijing 9 HOURS AGO
Additional reporting by Chan Ho-him in Hong Kong
by MJ2004China’s botched Covid reopening
Rushed exit from hardline policy shatters myth of Beijing’s competence
China’s mismanaged exit from its “zero-Covid” policy is subjecting its people to widespread disruptions and health risks. It is also exploding a myth that Beijing’s leadership, packed with technocrats and able to exercise authoritarian decisiveness, is inherently superior to western democracies when dealing with crisis scenarios.
As Covid-19 sweeps through the country’s biggest cities, the lack of preparation for China’s opening from strict pandemic controls is becoming painfully clear. Residents of Shanghai, Shenzhen and other cities reported that pharmacies had sold out of fever medicine and Covid tests, while blood banks are battling supply shortages.
Streets in Beijing remain empty and most businesses are closed, with unofficial estimates suggesting about 40 per cent of Beijing’s 22mn people have contracted the Omicron variant. In many other cities, people are sick or staying at home to avoid infections and schools are moving lessons online so that students and teachers can shelter from the wave of contagion.
The scenes of distress not only reflect poorly on President Xi Jinping, who has been widely hailed by state media as the “commander-in-chief of the people’s war against Covid”. They also raise questions about the capacity of China’s administration to make wise and timely decisions.
This is not an academic point. If the world’s emerging superpower — one that exploits a deep sense of historical injustice to fuel its rivalry with the west — is falling prey to the narrowing perspectives of concentrated power, then the risks that Beijing poses to global stability will grow.
With China so central to several of the world’s potential geopolitical flashpoints — on the Korean peninsula, across the Taiwan Strait, in the South China Sea, on its Himalayan border with India and in other arenas — the wider world has a legitimate interest in the quality of Chinese decision-making.
This is not purely a foreign policy concern. Some of the protesters who took to the streets in more than 20 Chinese cities last month to raise grievances about Beijing’s stifling “zero-Covid” regime chanted slogans calling for free speech, the rule of law, democracy and human rights.
Over the course of almost three years of dealing with the pandemic largely through urban lockdowns of varying intensities, China has had ample time to prepare itself for an exit strategy. Yet it has failed to ensure that its most vulnerable age cohort — the 267mn people above 60 — is adequately vaccinated against the virus. Some 32 per cent of this cohort are insufficiently protected, according to official figures.
Beijing also rejected consistent calls to supplement its homegrown vaccines by using foreign mRNA jabs manufactured by Pfizer, Moderna and other groups. This failure to admit highly effective foreign medicines reveals Beijing’s willingness to put national pride before the health and economic welfare of its population.
To be sure, muscular social controls did an impressive job of containing the virus’s spread in early 2020 after its initial outbreak in Wuhan, and China’s official Covid death toll of 5,235 is much lower than that in other large countries. But the current rushed and poorly co-ordinated transition from “zero-Covid” towards living with the virus is undermining China’s own claims to “put people first”.
Simply refusing to report a sharply rising death toll does not obscure a looming humanitarian crisis. With perhaps as many as 1bn people set to travel over the lunar new year holidays starting on January 21, the current wave of infections is only likely to swell.
- FT Editorial Board
by ti-amie
Over the course of almost three years of dealing with the pandemic largely through urban lockdowns of varying intensities, China has had ample time to prepare itself for an exit strategy. Yet it has failed to ensure that its most vulnerable age cohort — the 267mn people above 60 — is adequately vaccinated against the virus. Some 32 per cent of this cohort are insufficiently protected, according to official figures.
Beijing also rejected consistent calls to supplement its homegrown vaccines by using foreign mRNA jabs manufactured by Pfizer, Moderna and other groups. This failure to admit highly effective foreign medicines reveals Beijing’s willingness to put national pride before the health and economic welfare of its population.
When your population is so large you can sacrifice a large portion of it and not even blink is a scary thought. I still can't believe that they didn't find a way to "duplicate" a mRNA vaccine.
by ponchi101 I have worked enough with Chinese companies to know something: you don't tell your boss the truth. You tell your boss what he wants to hear.
So you never know the truth when you work with them. You really, really, have to be a detective. I see no reason why it should be different within the borders.
by Suliso That's also why Russian army is performing so poorly.
But back to the topic Chinese government showed incompetence in both sticking to zero covid this long AND abolishing it so suddenly. It too some effort, but Mr Xi managed it...
Americans could also theoretically sacrifice few millions, but the mindset is different.
by ti-amie
by ponchi101 Serious here. Are countries around the world easing on vaccination entry requirements?
by Suliso In EU all requirements have been abolished as far as I know. Switzerland as well.
by ponchi101 Ok. So I got vaccinated 4 times and now... I can throw away my vaccination card.
It's a wonderful world.
by Suliso
ponchi101 wrote: ↑Thu Dec 29, 2022 4:16 pm
Ok. So I got vaccinated 4 times and now... I can throw away my vaccination card.
It's a wonderful world.
Did you get vaccinated to protect yourself or to show a fancy card when you travel?
by ponchi101 90% to protect myself, 10% because my defunct industry would be adamant about it.
But you know, it is kind of interesting how this thing was, a little over two years ago, biological Armageddon, and now, it is basically a flu in good shape. I did write that it would defeat us (TAT1.0) but the level of flippancy with which it is now being treated is surprising.
So. I will keep my vaccines, and let's see how much it will morph into normalcy. Anyway, I have a strong suspicion I am immune to it. Been exposed too much to it and never got it.
by dryrunguy
ponchi101 wrote: ↑Thu Dec 29, 2022 4:24 pm
Anyway, I have a strong suspicion I am immune to it. Been exposed too much to it and never got it.
Even if you're right, that could change with any given subvariant, right?
by Deuce Yes, people are flippant about COVID now - and that was to be expected, because the human animal cannot bear too much discomfort or inconvenience. And so, when faced with a prolonged degree of discomfort, inconvenience, or otherwise ugly circumstance, it begins to create pretty illusions that all is well.
This is more commonly known as 'being in denial'.
And that is exactly what has occurred with COVID - it's uncomfortable to think of the reality, and so people create pretty illusions. And, of course, that just makes the existing problem worse, because it is not being addressed, and is instead being ignored. And, naturally, when problems are ignored, they grow.
But the FACT remains that more people have died from COVID in 2022 than died in 2021. Here in Canada, more people had died of COVID through 9 months of 2022 than had died in all 12 months of 2021.
It is most definitely NOT "a flu in good shape".
ponchi101 wrote: ↑Thu Dec 29, 2022 4:24 pm
Anyway, I have a strong suspicion I am immune to it. Been exposed too much to it and never got it.
Even if you're right, that could change with any given subvariant, right?
Ergo, I will get my next shots when sub-variant specific doses come.
Don't get me wrong. I know this is not over, nor will it be. It is here to stay. But I am a bit surprised how easily it has become a back thought for so many people.
by Deuce Sadly - actually, tragically - in the great majority of countries, people take their cues from politicians. And the politicians in most countries have decided to put an end to all protective measures against COVID. Not because COVID is no longer dangerous, but because the politicians know that the populace despise discomfort and inconvenience, and the only thing the politicians are interested in is getting votes, and so they knew that if they maintain the protective measures (which remind everyone that COVID is dangerous), they will get less votes.
So they feel it's better (self-servingly) to lie to the people and strongly infer that COVID is no longer dangerous by lifting the protective measures. Governments have helped people to be 'in denial' of the realities of COVID by telling them what they want to hear, rather than telling the truth. Of course, politicians and governments have a very long and well established reputation for not telling the truth...
As a predictable and inherent consequence, when the populace sees that the politicians have lifted the protective measures, they tell themselves 'well, that must mean that COVID is no longer dangerous, because if it were still dangerous, the government would surely protect us from it' - and so they are comfortably in denial.
But no - the government only cares about the populace insofar as it affects them (the politicians). If lifting the protection of the people will get the politicians more votes (because they are telling the people what they want to hear instead of telling them the uncomfortable truth), then they will do exactly that.
And they have.
This is why all through this pandemic, I listen only to independent medical people, and not to any medical people who are employed by any government.
Ultimately, human selfishness and self-deception will be the end of our species - via various avenues.
by MJ2004China’s Covid generation: the surging inequality behind Xi’s U-turn
Lockdowns have often been more relentless in rural areas, upending the education of millions and blocking social mobility
In late September, Tashi, a student in a rural village of fewer than 100 people in south-eastern Tibet, returned to school after a six-week lockdown.
The 15-year-old’s grades had deteriorated markedly after weeks of trying to take classes on a smartphone with patchy internet in a crowded house while being cared for by ageing grandparents. His parents were 750km away in Lhasa, the capital, working.
“It was very difficult to concentrate during the lockdown. My three younger siblings were also taking classes in a noisy house,” he says, sitting next to baskets of dried fungi and herbal medicines, which are his village’s main trade.
“Now we’re back at school, I’m still lagging behind after months of trying. It’s very demoralising.”
Tashi, whose name has been changed to protect his identity, is one of the hundreds of millions who make up China’s “Covid generation” — the children whose lives have been upended through cycles of lockdowns under Xi Jinping’s hallmark zero-Covid policy.
In December, Xi’s administration embarked on a stunning U-turn. The pandemic controls of relentless lockdowns, mass testing and quarantine and fastidious electronic contact tracing are being rapidly unravelled.
The change of course has many causes — from the spontaneous protests that broke out in apartment buildings across the country to the toll the policy was taking on the economy. But one of the least discussed factors has been the way that the zero-Covid policy has sharpened China’s already high levels of social inequality, especially between urban and rural residents — one of the most important political faultlines in society.
Many young people from rural areas or the urban lower classes have been forced to study online and have been separated from their parents for long periods over the past three years. The result is that their education — hitherto their only path to upward social mobility — hangs in the balance.
The sudden abandonment of the zero-Covid playbook has led to an alarming spike in Covid-19 infections and, according to some forecasts, could lead to millions of deaths over the winter. Before the reopening, Chinese doctors and nurses warned that the country was unprepared for an exit wave given thinly resourced hospitals and medical clinics, and nearly 90mn Chinese aged 60 and over who had not received three vaccine doses. Now, the healthcare system is being overwhelmed with a deluge of sick patients and funeral providers cannot keep up with demand for their services.
Beyond the immediate health crisis, which could persist for months, the true extent of the damage wrought upon Chinese society by Xi’s hallmark policy is only just emerging.
For large swaths of the country’s 1.4bn people, the pandemic shattered the fragile balance that once supported the back-and-forth movement of people such as Tashi’s parents from rural areas to large cities. Zero-Covid’s vast web of intersecting restrictions hammered low-income families and in many cases left people cut off from their loved ones.
China-focused economists, market analysts and media have mostly paid attention to the hit to consumer spending and disruptions to factories and supply chains. China’s more developed eastern and southern megacities, such as Shanghai, Chongqing, Shenzhen and Guangzhou have dominated headlines. But many of the areas that have been locked down for the longest have been largely out of sight.
By the time Beijing unveiled its policy pivot, heightened restrictions were still being enforced across more than a dozen regions, including Inner Mongolia, Shaanxi, Heilongjiang and Liaoning in China’s northern rustbelt, as well as Xinjiang in the west and central Hubei.
But as the restrictions have been unwound, it is becoming clear that the pandemic’s scars are deepest among children in many of these areas, experts say. Rising inequality, which is heavily influenced by access to education, will in the coming years carry long-term repercussions for Xi and the ruling Chinese Communist party. Adding to the bleak outlook, China’s youth unemployment rate has been near-record levels and the brunt of the impact is shouldered by those born into poorer households.
The Financial Times spoke to more than 20 children, teachers, academics and mental health experts. Most asked not to be named, citing the risks of repercussions.
“The zero-Covid policy has impacted the poor more than the rich. It exacerbates the Dickensian divide between the haves and have-nots in China,” says Diana Fu, an expert on China’s domestic politics with the Brookings Institution think-tank.
“When young people can’t find jobs, small business owners go bankrupt, migrant workers are evicted, and infected children are separated from their families, it makes people question whether the government is holding up its end of the bargain.”
The coronavirus pandemic has exacerbated educational inequalities globally. At the height of the nationwide lockdowns in 2020, the UN estimated that nearly 1.5bn school children were affected by school closures, a third of which did not have access to remote learning facilities.
However, the problems facing China’s 291mn students stand out because of just how long Beijing persisted in using lockdowns to try to contain the virus.
Before the pandemic struck, China was making progress towards narrowing the educational gap between the country’s urban rich and rural poor. This involved huge state investments in schools in rural areas and fiscal reforms to pay teachers’ wages from the central government coffers rather than strained local accounts.
“It moved from being very, very, very unequal to very, very unequal,” says Scott Rozelle, an expert on educational inequality in China at Stanford University.
In early 2020, as the first outbreak of coronavirus exploded from the central Chinese city of Wuhan, Beijing’s education officials rushed to expand network connectivity to rural areas to ensure schools across the country could shift online.
Yet despite these efforts, Nancy, a maths teacher at a middle school in Qujing, a small town in Yunnan, near the southern border with Myanmar and Vietnam, says there has been a noticeable decline in the quality of her students’ English and maths skills, two subjects that require “high levels of teacher intervention”.
A veteran of more than 20 years in the classroom, Nancy does not blame the children. She feels “clumsy” teaching through video conferencing platforms.
“What a mess,” she says, while checking students’ homework in their first week back to school. More than half of her students are unable to solve mathematical problems taught during lockdown and their basics have also regressed. “Predictable but still heartbreaking.”
“We are teaching easier maths now than prior to the pandemic,” she adds, noting also: “Students from better-off families have done better, especially when parents are around to help them study.”
This chimes with the findings made by researchers at the Institute for Economic and Social Research at Jinan University in south-eastern China. After the first lockdown in 2020, they concluded that the “learning gap” between students with parents who graduated from university and those with parents with primary school education had “enlarged” since before the pandemic.
“The internet supply was there mostly in rural areas, but the quality of the connection wasn’t great, and many of the children in rural areas did not have exclusive access to a mobile or laptop like their urban counterparts,” says Terry Sircular, an economist and expert on social inequality at the University of Western Ontario.
Shelly Lin, an English teacher at a high school in Dongxing, Guangxi, says the deterioration in learning during the lockdown is obvious. Her students took an exam after returning to school after the summer lockdown ended. “The results were poor,” she says. “But we didn’t have time to reteach the material all over again.”
After the arrival of the Omicron variant in late 2021, Xinjiang — the western region where Beijing has been accused of widespread human rights abuses against Uyghurs and other ethnic minority groups — was among the places to return to lengthy periods under lockdown.
Lily, a high-school student from Hotan, in Xinjiang’s south-west, says a stark divide also emerged between students attending China’s equivalent of a grammar school attended by children — both from the majority Han ethnicity and Uyghur Muslims — with good grades and Mandarin skills, and those at the local schools in small cities populated predominantly by Uyghur students.
“The quality of the classes for us who stayed at home for online classes was really poor. Our school buildings were even turned into quarantine facilities,” she says.
China’s household registration system, the “hukou”, has long been derided as a source of entrenched inequality, preventing migrant families from equal access to basic services when they move from rural to urban areas. While there have been some reforms to lower the threshold for hukou registration in some areas, the system still means the vast majority of migrant workers are forced to leave their children in the countryside, typically in the care of grandparents — the so-called left-behind children.
Experts say that this has compounded the hurdles facing poorer children during the pandemic, threatening students’ chances of obtaining a prized place at one of China’s top universities — a setback with potentially life-long consequences.
“They are already at a disadvantage. Add to those months of not being able to access online education. In a highly competitive schooling system, that will have an impact on their ability to get into a good high school and then go to college,” says Rozelle.
In August, a region-wide lockdown was quickly introduced in Tibet following the emergence of dozens of positive coronavirus cases. The school term was delayed and students began to take online classes at home.
In Tashi’s case, the home had three electronic devices: one laptop and two mobile phones. With four children attempting to complete their online classes, one had to watch the playback at night, while Tashi also had to tutor the younger children.
He would try to snatch windows of concentration, sitting outside on the wooden floor straining to read words on a small screen in the harsh sunlight of the Tibetan plateau.
“I couldn’t handle doing my studies and looking after my siblings. I feel so weak using the pandemic as an excuse. But after the lockdown, I feel like my studies, and life, have started to slip,” he says.
“Of course I hoped to find a decent job by studying . . . ” Tashi, suddenly switching from his native Tibetan to Mandarin to emphasise the point, adds: “But after the lockdown, I felt there was no hope for my education . . . when I finish middle school, I’ll quit school and get a job.”
Such despondence among the youth is setting off alarm bells among people involved in mental health services.
Dr George Hu, chair of the mental health department at Shanghai United Family Pudong Hospital, has been on the frontline of psychiatric care in China during the pandemic and says researchers are only “just beginning to scratch the surface” of the period’s long-term impact on mental health.
Hu, a clinical psychologist, believes that for many of China’s young, lockdowns have already “ripped out their previous understanding” of Chinese society and state controls.
“When the lockdowns happened younger people were thinking, ‘How could this happen?’ A lot of the older generation thought, ‘This could happen, and it could be worse.’”
Hu notes that provision of psychiatric services in Chinese hospitals and counselling in the country’s education system had been “tacking in the right direction” with greater accessibility and oversight. But for most people, accessing mental health services requires the ability to both pay upfront and to take the necessary time off work.
Suicide data is patchy in China — data collection is based on certain municipalities as a sampling station and national statistics are not published — making it impossible to know the pandemic’s full toll.
Hu says that in China — and other parts of east Asia — suicide is often linked to a feeling of “perceived burdensomeness” where people feel their presence is a strain for their family and wider community.
“I’m trying to be sensitive here, but the pandemic has increased stress, stress is not good for coping or ‘perceived burdensomeness’. There is a correlation between that and suicide. The exact numbers, I wouldn’t know. But attention has to be paid to this.”
China’s success in tackling poverty in the decades after Mao Zedong’s death — lifting 800mn people over 40 years — has long served to bolster the legitimacy of the Chinese Communist party and its leaders.
Now the collateral damage to the Covid generation is sowing seeds of doubt in the wisdom of the party — and its leader.
Despite the dangers inherent in public displays of dissent, frustration among younger Chinese and opposition to Xi’s policies have become increasingly evident over recent months.
Simmering angst boiled over in November when a fire in a locked-down apartment complex in Ürümqi, the capital of Xinjiang, was blamed for the deaths of 10 people. Since then, monitoring by Nathan Ruser and colleagues at the Australian Strategic Policy Institute think-tank tracked more than 100 protests and acts of public resistance across 39 cities. While not challenging Xi’s grip on power, the number and location of the protests, including the initial spark in remote western Ürümqi, highlighted just how widespread frustrations had become.
No clear explanation has been given by Xi or his top lieutenants for the stunning about-turn. But it came days after the protests and followed months of slowing growth in the world’s second-biggest economy as well as acute financial pressure from local governments who were on the hook for paying for the policy’s draconian enforcement.
Fu, of Brookings, says that the legacy of the protests will go far beyond the zero-Covid policy reversal. The period marks, she says, a turning point for a generation who have no memory or knowledge of the 1989 Tiananmen democracy movement: “China’s Václav Havel moment”.
“Václav Havel had described people living under communist Czechoslovakia as greengrocers who put up signs supporting the regime’s policies, thus becoming a part of the system of oppression,” she says. “Prior to the protests, Chinese citizens had largely complied with the zero-Covid policy as citizens under any authoritarian system would. However, the protests showed that not all Chinese people are greengrocers; some are daring to dissent for the first time.”
Recent online discussion in China has centred increasingly on the folly of the government’s lack of preparation for the zero-Covid U-turn. But for weeks, discussions with sharper political undertones have also raged. On the microblogging site Weibo, a topic entitled “What would university life be like without the Covid?” received more than 550mn views. In another, a discussion based on a popular claim by college students that the pandemic has “stolen their youth” was read more than 4.3mn times on the question-and-answer website Zhihu.
“[Students] were like birds in chains, walking down the road, coming and going with masks, unable to recognise whether each other was crying or laughing,” said a Zhihu user Julya, who offered one of the most popular answers.
As teachers and students are caught up in the overwhelming Covid wave, schools across the country are being forced back to online classes and life-defining exams have been postponed or cancelled.
Yu Jie, a China expert with Chatham House think-tank, observes that the country has not felt such a stark generational divide since Mao’s chaotic rule: “Older people have a clear memory of the cultural revolution and the Great Famine of the 1960s. This [current] period may not be the most drastic period they can remember. It is really the younger Chinese generation who will have the most painful memories of the pandemic.”
She adds that there is also a sense of exhaustion among much of China’s middle class, dashing hopes of an economic recovery based on pent-up consumer demand.
“We’re going to enter a very long phase of stagnation of the Chinese economy . . . For me, that’s the biggest uncertainty,” Yu says, adding that the resulting inequality appears to be “very Dickensian”.
Fu says that ultimately Xi’s zero-Covid policy has put on the line a fundamental pillar of the party’s legitimacy: the promise of a basic living standard for Chinese citizens.
“The party’s social contract with 1.4bn people is that it would provide for needs such as jobs, housing, food and security in exchange for popular support of its rule and acceptance of limitations on political rights,” she says. “To the extent that these basic social rights have been taken away during the pandemic, this poses a legitimacy dilemma for Beijing.”
FT Big Read
Qianer Liu in Hong Kong, Edward White in Seoul and Eleanor Olcott in Tokyo
by ponchi101 More consequences from this pandemic.
And a tick on the side of those that were against lockdowns. It was and is so difficult to make the right call.
by ti-amie It seems some in China have started doing cremations in the street because of the backlog in availability at crematoriums.
by Deuce ^ But... but... but... I was told that the pandemic is finished and COVID-19 is gone!
Was everyone (including the president of the USA) lying?
Or do they just live in a non-existent fantasy world?
by Suliso I remember this guy, but I'm afraid his 15 minutes of fame are over. One could headline never ending new variants forever, but it doesn't really change anything. We have decent vaccines, but they don't sterilize and if so the virus is bound to spread. Just like flu does and no one has ever found a way to stop that from happening either.
by ti-amie
by Deuce
Suliso wrote: ↑Thu Jan 05, 2023 3:08 pm
I remember this guy, but I'm afraid his 15 minutes of fame are over. One could headline never ending new variants forever, but it doesn't really change anything. We have decent vaccines, but they don't sterilize and if so the virus is bound to spread. Just like flu does and no one has ever found a way to stop that from happening either.
There's a lot more than "this guy" warning about this new variant. Many, many medical people are concerned about it.
Yes, we could go on headlining new variants for a long time, encouraging people to protect themselves and others, and trying to get a handle on the new variants of concern as much as possible...
Or we could conveniently stick our heads in the sand and 'comfortably' pretend that everything is fine as the problem persists and grows.
Again - based on medical facts, comparing COVID to the 'flu is irresponsible.
by dryrunguy Here's the first Situation Report of 2023. Damar Hamlin got a mention (see the NFL thread if you haven't been following).
::
EPI UPDATE* As of January 5, the WHO COVID-19 Dashboard reports:
• 657 million cumulative COVID-19 cases
• 6.67 million deaths
• 3 million cases reported week of December 26
• 22% decline in global weekly incidence as of December 26
• 10,794 deaths reported week of December 26
• 12% decline in global weekly mortality as of December 26
Over the previous week, incidence declined 73% in Africa; 42% in Europe; 26% in South-East Asia; 20% in the Americas; 16% in the Eastern Mediterranean; and 12% in the Western Pacific.
UNITED STATES
The US CDC is reporting:
• 100.6 million cumulative cases
• 1.09 million deaths
• 402,525 cases reported week of December 28
• 17% decline in weekly incidence as of December 28
• 2,530 deaths reported week of December 28
• 14% decline in weekly mortality as of December 28
• 17% increase in new hospital admissions
• 8.6% increase in current hospitalizations
*Recent holidays might delay data reporting for the WHO and US.
The Omicron sublineage XBB.1.5 experienced rapid growth over the past 2 weeks, accounting for an estimated 40.5% of all new sequenced specimens. BQ.1.1 (27%) and BQ.1 (18%) fall in line next, with various other Omicron subvariants accounting for the remainder of cases.
THE FOURTH YEAR As the COVID-19 pandemic enters its fourth year, many nations are better positioned to manage the disease due to clinical care management, vaccines, and therapies, WHO Director-General Dr. Tedros Adhanom Ghebreyesus said during a January 4 briefing. Nevertheless, inequities in access to testing, treatment, and vaccination remain, threatening individuals’ health, the global economy, and societies overall, he said, noting that approximately 10,000 people die of COVID-19 worldwide each week. On December 25, the WHO announced it prequalified the first generic version of Paxlovid for production by an Indian manufacturer and said its scientists are closely monitoring and evaluating the emergence of Omicron XBB.1.5, which is quickly spreading in the United States and has been detected in nearly 30 countries. WHO officials also expressed concern over the situation in China, urging health authorities there to regularly share reliable epidemiologic data.
OMICRON XBB.1.5 A new Omicron subvariant, XBB.1.5, has quickly become predominant in the United States, accounting for about 40% of all US cases—and 75% in the Northeast region—this week compared to around 4% of cases during the first week of December. XBB.1.5 is a recombinant Omicron sublineage, a fusion of 2 different BA.2 variants—BJ.1 (BA.2.10.1.1) and BA.2.75 (BA.2.75.3.1.1.1)—making it more closely related to the BA.2 subvariants that were predominant in the earlier part of 2022 than to the BA.5 subvariants that were responsible for most cases in the second half of 2022. Its rapid growth has concerned public health officials and healthcare practitioners alike, with WHO officials calling it the most transmissible subvariant detected yet. Though there is not yet much data on the severity of XBB.1.5, so far there is no indication it makes people more sick than previous subvariants. Hospitals in the US are already under significant stress, however, due to an early flu season as well as widespread incidence of other respiratory viruses such as RSV.
Some experts are concerned about XBB.1.5’s potential to evade prior immunity, with research on the related XBB subvariants showing the potential to escape the protections of antibodies resulting from vaccination, prior infection, or treatments, including Evusheld. In addition to being immune evasive, XBB.1.5 contains a mutation at genomic site 486 that is associated with enhanced viral binding to human ACE2 receptors, which could be boosting its transmissibility and causing it to surge. Notably, many experts highlight that vaccination and quick treatment with Paxlovid remains highly effective at preventing severe illness. It is unclear just how large of a surge may be driven by XBB.1.5, but the nation—and the world—is much better positioned at this point in the pandemic with vaccines, treatments, and nonpharmaceutical interventions such as masking helping to prevent infection, severe illness, and death.
US WINTER SURGE Much of the United States is experiencing a winter surge in COVID-19 cases, driven by waning immunity, holiday gatherings, and the emergence of the highly transmissible Omicron XBB.1.5 recombinant subvariant. Around the time of this report’s last publication on December 20, the nation surpassed 100 million cumulative reported COVID-19 cases, according to the US CDC. Federal data also show the number of hospitalized patients with COVID-19 is set to surpass the number reached during the summer 2022 surge, with new hospital admissions particularly high among individuals aged 70 and older who are most vulnerable to severe disease. Hospitals and clinics are feeling pressure from an influx of people with various respiratory illnesses in addition to COVID-19, including other coronaviruses that cause colds, influenza, and respiratory syncytial virus. Despite this, only 15% of people over age 5—and only 37.5% of those aged 65 and older—have received an updated bivalent vaccine booster dose. While recent data might not provide a clear picture of where the nation stands—due to reporting delays from recent holidays or severe weather as well as a lack of reporting from people using home tests—levels of SARS-CoV-2 detected in wastewater samples are rising in several regions, particularly in the Northeast, where the XBB.1.5 variant accounts for about 75% of new cases. Though health experts and some government officials, including those in New York City and Los Angeles, are urging people to begin wearing masks again and receive the latest booster, much of the country appears to have moved beyond the pandemic.
CHINA Following a reversal of its “zero COVID” containment strategy in early December after widespread protests, China is experiencing an unprecedented surge in cases. The outbreak appears to have spread first in urban areas, overwhelming healthcare facilities and morgues, and officials are concerned that weaker health systems in more rural areas will not fare well. The true impact of the current surge in cases and the number of resulting deaths is not fully understood due to unreliable data. The WHO has urged China to share more geographically based data on COVID-19 hospital admissions, intensive care unit (ICU) patients, and related deaths. Today, the organization said China supplied data on new COVID-19 hospitalizations showing a nearly 50% increase, from 15,161 new hospitalizations for mainland China during the week ending December 25 to 22,416 for the week ending January 1. China continues to report daily COVID deaths in single figures. The numbers likely are undercounts, based on officials’ use of a narrow definition of COVID-19 deaths, anecdotal evidence from individuals, and reports of deaths among prominent public figures.
In addition to the WHO, health and government officials worldwide are struggling to get a true sense of the situation in China and how to respond. Several countries have introduced—and the European Union recommended—pre-departure COVID-19 tests for travelers arriving from China, moves that the Chinese government and others have criticized as useless or even harmful. Some officials are concerned the large outbreak could provide an opportunity for a new SARS-CoV-2 variant to emerge. According to data from China’s CDC, the Omicron variant—specifically sublineages BA.5.2 and BF.7—is the most dominant based on recent genomic sequencing. The data allay concerns, for now, about the potential for a new variant of concern emerging from the outbreak, but some experts say the situation highlights the need to develop an early warning surveillance system using viral genomic data.
THERAPEUTICS Over the past several years, monoclonal antibodies were critical therapies for millions of people who were at high risk of getting sick from COVID-19 but who did not respond to or could not receive SARS-CoV-2 vaccines. However, new immune-evasive Omicron subvariants have rendered them largely ineffective as treatments for currently circulating SARS-CoV-2 variants, and even prophylactic antibody therapies like Evusheld show diminished efficacy. In 2022, the US FDA rescinded emergency use authorizations for major monoclonal antibody treatments including bamlanivimab, etesevimab, sotrovimab, casirivimab, imdevimab, and bebtelovimab, leaving immunocompromised individuals without many treatment options.
Other therapies have mixed benefits for immunocompromised individuals. Although antivirals are available, they have seen lackluster uptake and are not accessible to everyone; Pfizer’s Paxlovid interacts with other widely prescribed drugs, Merck’s Lagevrio shows lower efficacy, and Gilead’s intravenous remdesivir requires infusions over 3 days in hospital or outpatient settings. Although the US government has strongly promoted antivirals like Paxlovid, misinformation and misconceptions about the drug, as well as worries about side effects and viral rebounding after finishing a regimen, have hampered its uptake. Even convalescent plasma, which can be adapted to different strains, is inconsistently available and difficult to administer.
An FDA spokesperson said the agency will work with pharmaceutical companies on expediting the development of preventive therapies for immunocompromised patients, though it is unknown if the agency will accept fact-tracked data gathered from laboratory studies instead of large-scale clinical trials. Additionally, without the support of federal funding that drove drug development during earlier stages of the pandemic, pharmaceutical companies have little incentive to work on new and more effective antibody treatments. The lack of effective, specialized, and widely used therapies leaves many immunocompromised people with limited options if they become sick with COVID-19.
UNFOUNDED VACCINE RUMORS During a primetime US National Football League (NFL) game on January 2, Buffalo Bills player Damar Hamlin collapsed shortly after suffering a blow to his chest and subsequent cardiac arrest. Hamlin was resuscitated on the field and remains in critical condition in a Cincinnati hospital. Although little is known about the true cause of Hamlin’s collapse, cardiologists suspect that the blow to his chest may have disrupted his heart’s rhythm and hindered blood flow to his brain; they note there is no indication Hamlin’s COVID-19 vaccine status played a role. Shortly after the incident, however, unfounded rumors began circulating on social media linking Hamlin’s injury to COVID-19 vaccines, revealing the pervasiveness of false and misleading information 3 years into the pandemic. The November 2022 rollback of Twitter’s ban on COVID-19 misinformation likely helped the rumors spread quickly and widely.
Although certain viral infections and vaccines can lead to myocarditis in some instances, the risk of vaccine-induced cardiac arrest associated with COVID-19 vaccines is inflated. A September 2022 study in the journal Circulation found that the risk of developing myocarditis following a booster dose of the Pfizer-BioNTech vaccine is low, and an August 2022 study published in Frontiers in Cardiovascular Medicine found that the risk of myocarditis is more than 7-fold higher in persons who were infected with SARS-CoV-2 than in those who were vaccinated. Additionally, a July 2020 study in the Clinical Journal of Sport Medicine found that structural abnormalities of the heart muscle or arteries and faulty electric rhythms were the most common causes of sudden cardiac events among competitive professional athletes in the US.
With skepticism surrounding COVID-19 vaccines now threatening other public health priorities, including childhood vaccinations, health officials are struggling to combat misinformation and improve communities’ trust in public health. Experts are concerned that this new wave of misleading information surrounding COVID-19 vaccines threatens the rollout of updated booster doses and ongoing efforts to stop the spread of COVID-19 and other diseases such as measles.
by dryrunguy Here's the latest Situation Report. New format. Haven't read it yet.
::
Lessons of the COVID-19 pandemic should inform future pandemic preparedness and response
The world must heed the “harsh lessons” of the COVID-19 pandemic by making “bold investments” in pandemic preparedness, prevention, and response, UN Secretary-General António Guterres said in a statement marking the International Day of Epidemic Preparedness on December 27, 2022. Many wonder, however, as the pandemic fades from our collective memory, whether the global community is—or will be—prepared to face the next pandemic.
The abilities to detect and analyze potential biological risks are critical to plan for, predict, and respond to disease outbreaks before they reach pandemic levels. Several factors—including climate change and distrust in public health agencies—are accelerating the threat of another pandemic, and various gaps—such as those in leadership, funding, and surveillance—must be filled in order to bolster our ability to face whatever comes next.
In the United Kingdom, scientists this week launched the Respiratory Virus and Microbiome Initiative, supported by the Wellcome Sanger Institute in cooperation with the UK Health Security Agency, to expand genomic sequencing of various common respiratory pathogens, including SARS-CoV-2 and other coronaviruses, various types of influenza, respiratory syncytial virus (RSV), and other microbes. The program’s goal is to elucidate known threats, detect any worrisome mutations, and potentially alert experts to the emergence of new viruses.
In the United States, the US Congress is facing a deadline next year to reauthorize the Pandemic and All Hazards Preparedness Act, which could provide an opportunity for momentum to instill lessons learned. While lawmakers approved some modest changes as part of a December 2022 pandemic preparedness package—including requiring Senate confirmation of future US CDC directors—a proposal to create a bipartisan commission to evaluate the federal pandemic response, identify gaps, and make recommendations for future actions was dropped. In the US House, now under control of Republicans, a Democrat-formed subcommittee—originally focused on the nation’s poor pandemic response and misinformation surrounding vaccines and treatments—will shift its priorities to examining the origin of SARS-CoV-2, investigating gain-of-function research, and probing federal spending and pandemic-related mandates. Though the CDC is expected to roll out changes in the way it addresses health emergencies, the agency continues to require congressional authority to demand data from states. Meanwhile, several states, private foundations, and academic institutions are exploring ways to institute changes on their own or make recommendations for reform.
US renews COVID-19 public health emergency; WHO advisory committee to meet later this month to consider PHEIC declaration
With various sublineages of the Omicron variant of concern (VOC) circulating worldwide—including the XBB.1.5 subvariant that appears to be increasing in prevalence globally—and China facing a severe COVID-19 outbreak, the International Health Regulations (IHR) Emergency Committee for COVID-19 is set to meet January 27 for a fourteenth time to consider whether the pandemic still represents a Public Health Emergency of International Concern (PHEIC). Several leading experts and WHO advisors say it is too early to end the pandemic emergency phase, particularly in light of the situation in China.
In the US, the Biden administration this week quietly renewed the COVID-19 public health emergency for the eleventh time. Several people familiar with the process say this could be the last renewal, although a decision has not been finalized amid yet another surge in cases. If the emergency declaration is allowed to lapse in the spring, it would mark a significant turning point in the pandemic response, triggering a shift in several significant components of the federal response, such as an end to free vaccinations and tests and the resumption of Medicaid enrollment requirements. Moderna this week said it is considering a commercial price of US$110-$130 per shot for its SARS-CoV-2 vaccine, similar to the price Pfizer-BioNTech said it is considering and likely out of reach for many who do not have health insurance. The cost to consumers would be about 4 times the price the federal government paid to secure vaccine doses. In a letter to Moderna’s CEO, US Senator Bernie Sanders (I-VT) chastised the announcement, saying the proposed price tag is “unacceptable corporate greed.”
US government launches new Home Test to Treat initiative, reflecting shift to more at-home health services during the pandemic
The US National Institutes of Health (NIH), in partnership with the Administration for Strategic Preparedness and Response (ASPR) at the US Department of Health and Human Services (HHS), launched a new Home Test to Treat program to provide free at-home rapid tests, free telehealth sessions, and free at-home treatments for COVID-19 in select communities. Berks County, Pennsylvania, will be the first community to pilot the new program, with wider implementation is expected to occur in additional communities that will be selected based on community need, access to healthcare, anticipated COVID-19 incidence rates, and socioeconomic factors. Up to 100,000 individuals may be eligible to take advantage of this program in the coming year. Program leadership hopes the initiative will increase access to COVID-19 health services while potentially reducing community transmission.
The new program model benefits from avoiding some obstacles of the original Test to Treat program launched last year. Some patients faced difficulties accessing the antiviral treatment Paxlovid, including because of a lack of staff at pharmacies able to prescribe the medicine. Additionally, federal subsidies for the treatment are expected to end early this year, and uninsured individuals likely will be confronted with potentially prohibitive price tags.
The new program also reflects the greater shift to at-home health services, associated with high demand from patients and increased health seeking behavior in some cases. A study published January 6 in JAMA Health Forum documented that during the first year of the pandemic, March 2020-December 2020, increases in telehealth services for major depressive disorder, anxiety, and adjustment disorders more than compensated for concurrent drops to in-person appointments, increasing overall mental health service utilization for these conditions. Additionally, there’s been massive patient demand for the expansion of rapid at-home tests for diseases beyond COVID-19, such as RSV and flu.
A useful tool during the pandemic, wastewater surveillance is having a moment
The value of wastewater surveillance rose to prominence during the COVID-19 pandemic. Now, experts are wondering what the method’s future may look like beyond COVID-19, particularly since the 2020 launch of the US CDC’s National Wastewater Surveillance System (NWSS) program, which aggregates data from federal contractors, academic laboratories, state laboratories, and state-contracted commercial laboratories. However, advocates and experts note that while there are numerous advantages to utilizing wastewater surveillance, further evaluation and investment to determine the best applications of wastewater data are needed. An international meeting this week seeks to determine if a global COVID-19 wastewater monitoring system may provide further value, building off existing European Union recommendations and airport wastewater monitoring programs. The WHO this week urged all nations currently experiencing COVID-19 outbreaks to increase genomic sequencing of SARS-CoV-2 and share those sequences, noting that the number of shared sequences has dropped by more than 90% since the peak of the initial Omicron surge.
See also: If interested in learning more about wastewater surveillance, consider listening to this episode of a new Johns Hopkins Center for Health Security podcast series, The BWC Global Forum: Biotech, Biosecurity & Beyond.
Growing body of evidence supports Omicron-targeting bivalent booster’s benefits over original boosters; some experts question need among younger, healthy populations
A growing body of evidence from lab tests and real-world data suggest the bivalent vaccine boosters targeting the Omicron BA.4/BA.5 subvariants provide broad and better protection than the original boosters against severe COVID-19 outcomes. A recent report in the US CDC’s MMWR shows that a bivalent booster dose provided 73% additional protection against COVID-19 hospitalization among immunocompetent adults aged 65 and older, compared to past monovalent mRNA vaccination only. Among the study population, a bivalent booster dose received after ≥2 monovalent mRNA doses provided strong protection against COVID-19–associated hospitalization during a period of Omicron BA.5 or BQ.1/BQ.1.1 predominance. Newer CDC data show that during November 2022, there was a 90% reduction of hospitalizations for people aged 65 and older who had the bivalent booster compared to those who were unvaccinated, a 13.5-fold increased risk of hospitalization for unvaccinated individuals, and a 2.5-fold risk among those who were vaccinated but not a bivalent booster. An Israeli study found similar results—the Omicron-adapted booster provided an 81% reduction in hospitalization among people aged 65 and older who had received the shot.
Another recent MMWR study looking at younger adults aged 18 and older found the bivalent booster was 38-57% effective against hospitalization, consistent with, but at a lower magnitude, than protection among older adults. CDC data also support the bivalent booster’s effectiveness in young adults aged 18-49 years, showing monthly rates of COVID-19-associated hospitalizations were 29.9 times higher in unvaccinated individuals in this age group and 3.2 times higher in vaccinated individuals who did not have an updated booster. Some experts—including Dr. Paul Offitt, a member of the FDA’s Vaccines and Related Biological Products Advisory Committee—say some of these data support booster dosing only among those most likely to need protection against severe disease, such as older adults, people with multiple comorbidities that put them at high risk for serious illness, and those who are immunocompromised. To date, only 15.4% of the US population aged 5 years and older have received the updated booster, including 38.1% of those aged 65 and older.
Most long COVID symptoms resolve 1 year after infection, Israeli study shows; more research needed into multiorgan involvement
The vast range of symptoms known as post-COVID conditions, post-acute sequelae of SARS-CoV-2, or, most commonly, long COVID, can persist for a long time in some people. While more research is needed on exactly how SARS-CoV-2 infection impacts the body, many scientists and doctors are coming to understand that COVID-19 can affect multiple organ systems, as well as cognition and mental health.
A study posted online in the journal Neuropsychology analyzed data from neuropsychological evaluations of 110 adults who had confirmed SARS-CoV-2 infection 12 months prior to enrollment to identify demographic and clinical predictors of cognitive dysfunctions and complaints. Based on the findings, about half the study participants had abnormal performance in at least 1 of 3 cognitive tests, and lower educational background and acute infection-related headache and sleep disturbance were critical predictors of cognitive dysfunction.
Among more than 4,100 US children and adolescents hospitalized with post-COVID multisystem inflammatory syndrome in children (MIS-C), deaths, length of stay, adverse drug reactions, and the proportion of Black patients rose along with the number of organ systems involved, according to a study published January 5 in JAMA Network Open. In related news, the US NIH announced it has awarded 8 research grants to refine new technologies for early diagnosis of severe illnesses resulting from SARS-CoV-2 infection in children, including MIS-C.
For a study published January 11 in the journal BMJ, Israeli researchers examined nearly 2 million patient records, concluding that long COVID symptoms resolve within the first year after infection for most people with mild cases. Notably, several common symptoms of long COVID, such as fatigue, post-exertional malaise, and dysautonomia/POTS, were not included in the study, presenting a major limitation.
What we're reading
VACCINATION DISPARITIES COVID-19 vaccination rates among US children aged 5 to 17 years vary widely, with the highest coverage among Asian youth and the lowest among Black children, according to a study published in the US CDC’s MMWR. The authors state that providers and trusted messengers should provide culturally relevant information and vaccine recommendations to increase overall vaccination coverage and address disparities.
OMICRON NOMENCLATURE Do we really need to be keeping track of the “alphabet soup” of Omicron variant offspring? Do nicknames like “Kraken” help keep it all straight or add another layer of complexity? Does keeping up with the sublineage help people take actions to protect themselves and others, such as getting booster vaccines or wearing masks, or does it confuse such messaging? The Atlantic, STAT, and Fortune examine these questions.
SITUATION IN CHINA China is in the midst of what could be the world’s largest COVID-19 outbreak, but there are no reliable data about who has been infected, hospitalized, or died. The government stopped reporting daily COVID-19 data on January 9, saying it will switch to monthly reports. Both the Washington Post and the New York Times this week published pieces helping to visualize what appears to be a serious situation, using satellite imagery, photos, and videos.
VACCINE DELIVERY IN LMICs An initiative that helped bring COVID-19 vaccines to low- and middle-income countries (LMICs), the COVID-19 Vaccine Delivery Partnership, is winding down in June. The partnership—among Gavi, the Vaccine Alliance; UNICEF; and the WHO—was never meant to be permanent, will continue to support countries’ vaccination campaigns in the coming months, and help examine how to improve future vaccine deliveries, according to reporting by Devex.
Epi update*
As of January 12, the WHO COVID-19 Dashboard reports:
• 661 million cumulative COVID-19 cases
• 6.7 million deaths
• 3 million cases reported week of January 2
• 7% decline in global weekly incidence as of January 2
• 11,467 deaths reported week of January 2
• 9% decline in global weekly mortality as of January 2
Over the previous week, incidence declined 33% in Europe; 27% in South-East Asia; 7% in the Americas; 1% in the Eastern Mediterranean; and 1% in Africa, and increased 3% in the Western Pacific.
UNITED STATES
The US CDC is reporting:
• 101.1 million cumulative cases
• 1.09 million deaths
• 470,699 cases reported week of January 4
• 14% increase in weekly incidence as of January 4
• 2,731 deaths reported week of January 4
• 7.6% increase in weekly mortality as of January 4
• 8.6% decrease in new hospital admissions
• 3.7% increase in current hospitalizations
*Recent holidays might delay accurate reporting of data for the WHO and the US.
The Omicron sublineages BQ.1.1 (34%), XBB.1.5 (28%), and BQ.1 (21%) account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ti-amie SIGH
But it's over right?
/s
by ponchi101
dryrunguy wrote: ↑Fri Jan 13, 2023 3:11 am
VACCINE DELIVERY IN LMICs An initiative that helped bring COVID-19 vaccines to low- and middle-income countries (LMICs), the COVID-19 Vaccine Delivery Partnership, is winding down in June. The partnership—among Gavi, the Vaccine Alliance; UNICEF; and the WHO—was never meant to be permanent, will continue to support countries’ vaccination campaigns in the coming months, and help examine how to improve future vaccine deliveries, according to reporting by Devex.
In the meantime, Colombia is debating which Jet fighter to buy from Europe, to replace aging planes in the Air Force. Because, you know, the ongoing wars with Brazil, Ecuador, Venezuela, Panama and Peru demand a modern air force.
Setting up facilities to produce their own vaccines? Nah, getouttahere!
So when we get another major outbreak, don't send us crap. Really.
by ti-amieChina Reports Nearly 60,000 Covid-Linked Deaths Since Lifting Restrictions
The unexpected disclosure was made as the country faces mounting criticism for providing unreliable data on its latest coronavirus outbreak.
Covid-19 patients on stretchers in a hospital in Tianjin, China, in December. There have been widespread scenes of overflowing hospitals in the country recent weeks.Credit...Noel Celis/Agence France-Presse — Getty Images
By David Pierson and Olivia Wang
Jan. 14, 2023
Updated 4:26 p.m. ET
China said on Saturday that it had recorded nearly 60,000 fatalities linked to the coronavirus in the month since the country lifted its strict “zero Covid” policy, accelerating an outbreak that is believed to have infected millions of people. The disclosure was the first time China has provided an official measure of the Covid wave now sweeping the country, and represents a huge spike in the official death toll.
Until Saturday, China had reported a total of just 5,241 Covid deaths since the pandemic began in the city of Wuhan in late 2019. That measure was narrowly defined as deaths from pneumonia or respiratory failure caused by Covid. The new figure released Saturday included those who had Covid, but also died from other underlying illnesses.
China has faced mounting criticism from other countries and from the World Health Organization for not providing reliable data about the extent of its Covid outbreak and about the number of deaths across the country despite widespread scenes of overflowing hospitals, morgues and funeral homes in recent weeks.
Before the announcement, China said that only 37 people had died of Covid since Dec. 7, the day it ended its “zero Covid” policy.
The lack of transparency prompted several countries, including Japan and South Korea, to impose travel curbs on Chinese visitors after China reopened its borders last Sunday. Experts also warned that playing down the severity of the outbreak could lead people within the country to take fewer precautions.
China recorded 59,938 Covid-related deaths from Dec. 8 to Jan. 12, Jiao Yahui, an official with China’s National Health Commission, said at a news conference in Beijing. That figure included 5,503 people who died of respiratory failure directly caused by Covid. Another 54,435 fatalities were linked to other underlying illnesses, Ms. Jiao said.
Ms. Jiao said China was unable to release the data on Covid-related deaths sooner because it required a comprehensive examination of hospital reporting.
“We organized experts to conduct a systematic analysis on the death cases, so it took a long time,” Ms. Jiao said.
It was unclear whether the new figures mean that China has changed the way it discloses Covid deaths to include people with underlying diseases whose conditions were worsened by the virus. Officials have maintained that China’s official toll counts only those who died from pneumonia or respiratory failure caused by Covid. Other countries, such as the United States and Britain, count Covid deaths more broadly.
Editors’ Picks
A Writer Collapses. As He Recovers, His Dispatches Captivate Readers.
The Power of Instant Pudding Mix
And the 2023 Oscar Nominees Should Be …
Experts said it was too soon to determine whether China had changed tack, but they welcomed the move to provide more data.
“We cannot make a judgment now, but it is obviously more reliable than the previous data saying there were only several deaths,” said Jin Dongyan, a virologist at the University of Hong Kong. “I hope the government will be more transparent now.”
China has narrowly counted deaths from infectious diseases for a long time, including SARS in 2003 and seasonal flu. But during the Shanghai lockdown in the spring of 2022, the authorities made an exception and used a looser definition to justify the lengthy confinement of residents. Of the 588 Covid deaths the Shanghai city government reported at that time, one was ascribed to a heart attack, and the rest to “underlying conditions” or “tumors.” Despite this inconsistency, the National Health Commission has never expunged those deaths from the national toll on Covid deaths.
Ben Cowling, an epidemiologist at the University of Hong Kong, said the actual death toll in China, like that in every country, was almost certainly higher. He said that China could have provided more reliable data on death and infection rates if it had tested hospital patients more vigorously.
“The one thing which is a bit surprising is that China has so much testing capacity but hasn’t been using it to confirm Covid in hospitalized patients,” Mr. Cowling said.
The National Health Commission’s data confirmed longstanding fears that China’s older population would be hit hard by an outbreak because so many did not receive enough vaccine doses. Of the nearly 60,000 fatalities, 56.5 percent involved someone at least 80 years old.
Covid deaths are a particularly sensitive political issue in China, because Xi Jinping, the country’s top leader, had championed a strategy of harsh lockdowns, quarantines and mass testing to try to contain the virus. Mr. Xi boasted that the model could be adopted by other countries after it proved successful in suppressing transmission early in the pandemic.
As the highly infectious Omicron variant picked up steam last year, however, that strategy became untenable. As cases steadily rose across the country, protests erupted in November as more people grew weary of the Covid restrictions. Already under major economic strain, China then abruptly reversed its “zero Covid” policy without providing an opportunity for the country to stock up on medicine.
Officials have said in recent days that infections have peaked in major cities, though concern is growing about how the current coronavirus wave will affect the nation’s countryside, which has a far weaker health care system compared with China’s cities.
Understand the Situation in China
The Chinese government cast aside its restrictive “zero Covid” policy, which had set off mass protests that were a rare challenge to Communist Party leadership.
Rapid Spread: Since China abandoned its strict Covid rules, the intensity and magnitude of the country’s outbreak has remained largely a mystery. But a picture is emerging of the virus spreading like wildfire.
Rural Communities: As Lunar New Year approaches, millions are expected to travel home in January. They risk spreading Covid to areas where health care services are woefully underdeveloped.
Digital Finger-Pointing: The Communist Party’s efforts to limit discord over its sudden “zero Covid” pivot are being challenged with increasing rancor on the internet.
Economic Challenges: Years of Covid lockdowns took a brutal toll on Chinese businesses. Now, the rapid spread of the virus after a chaotic reopening has deprived them of workers and customers.
A Failure to Govern: China’s leadership likes to brag about its governance of the country, but its absence in a moment of crisis has made the public question its credibility.
by Deuce When 'information' is all over the place like this, what's truly happening with COVID in China is really anyone's guess.
I think the only truth is that nobody knows.
by ti-amie
Deuce wrote: ↑Sun Jan 15, 2023 4:37 am
When 'information' is all over the place like this, what's truly happening with COVID in China is really anyone's guess.
I think the only truth is that nobody knows.
If they're admitting to 60,000 deaths and know that pictures of people doing cremations in the streets have circulated around the world I'd add another zero or two to that figure.
by ponchi101 The 60K deaths is obviously not true; that is systemic propaganda from the Chinese govt.
But 2 zeroes would be too much. They could not hide 6MM deaths. 600K maybe.
by ti-amie
ponchi101 wrote: ↑Sun Jan 15, 2023 8:28 pm
The 60K deaths is obviously not true; that is systemic propaganda from the Chinese govt.
But 2 zeroes would be too much. They could not hide 6MM deaths. 600K maybe.
I put nothing past these folks but yeah, I agree with the 600k number.
by ti-amie
by ponchi101 The numbers don't match. If 8 in 10, then: 80% of 1.4 billion is 1.12 billion. But, if you have "only" 72,000 deaths, the mortality rate in China, for C19, is 0.006%.
And that makes no sense.
by ti-amie
ponchi101 wrote: ↑Mon Jan 23, 2023 4:39 pm
The numbers don't match. If 8 in 10, then: 80% of 1.4 billion is 1.12 billion. But, if you have "only" 72,000 deaths, the mortality rate in China, for C19, is 0.006%.
And that makes no sense.
Was it supposed to?
by ponchi101 Within the article, they say something along the lines. But the headline is confusing for the reasons I say.
by dryrunguy Here's the latest Situation Report from Johns Hopkins.
::
Emergency Committee on COVID-19 to discuss PHEIC designation; WHO launches US$2.5B emergency appeal
The Emergency Committee on COVID-19 is set to meet for a 14th time on January 27 to consider whether SARS-CoV-2 continues to merit designation as a Public Health Emergency of International Concern (PHEIC), 3 years after the panel first agreed the outbreak met the criteria. Under the International Health Regulations (IHR), a PHEIC can be declared if a health event meets 3 criteria:
• it is serious, sudden, unusual, or unexpected
• carries implications for public health beyond the affected State’s national border, and
• may require immediate international action.
While COVID-19 has spread globally and is no longer sudden or unexpected, WHO Director-General Dr. Tedros Adhanom Ghebreyesus—who makes the final decision about whether to end the global health emergency, no matter the committee’s recommendation—this week said he is “very concerned” about a rising number of global COVID-related deaths. The US alone is averaging more than 500 deaths per day. The meeting comes as China is experiencing the largest COVID-19 outbreak in the world, raising fears that a new variant of concern could emerge, factors that could influence the committee’s recommendations and Dr. Tedros’s decision.
Notably, there are no guidelines to determine when or how a PHEIC declaration should end. To be clear, ending the PHEIC would not mean that COVID-19 no longer poses a global threat nor would it signal the end of the pandemic, as the IHR do not include mechanisms for formally declaring pandemics or their ends. Many experts say the binary nature of the PHEIC mechanism needs to be reviewed and reformed to better achieve its intended goal of helping to coordinate response and policy.
In related news, the WHO this week launched a 2023 health emergency appeal for US$2.54 billion to address an unprecedented number of intersecting health emergencies worldwide, including COVID-19.
US FDA panel considering shift to regular vaccine boosters; many questions, uncertainties remain
As the SARS-CoV-2 virus continues to mutate, researchers and policymakers are evaluating longer-term vaccination strategies to maintain individual- and community-level protection from COVID-19. In the US, the FDA’s Vaccines and Related Biological Product Advisory Committee (VRBPAC) is meeting today (webcast live) to discuss an array of potential options, including vaccines from multiple manufacturers. Following the availability of bivalent booster doses last year, regulatory officials are considering shifts toward regular boosters, administered either annually or biannually, that could include two or more strains of the virus.
These decisions, however, must also account for individuals who have not yet received their initial course of vaccination, including many infants and young children. Another major concern is the safety and effectiveness of multi-valent boosters, especially the relative benefits and risks for different age groups and other subpopulations. The timing of doses is also a major point of debate. Regulators and health officials will need to walk a fine line between maintaining a high degree of protection, providing significant added benefit from each dose, and establishing a schedule that the public can understand and is willing to follow. And the same schedule may not be appropriate for people with varying degrees of risk. Early studies have yielded mixed results across these areas of concern, and some experts question the value of annual boosters or acknowledge the considerable uncertainty that remains, and research is still ongoing to provide the necessary data.
This week, the UK government announced that it will offer another round of SARS-CoV-2 vaccine booster doses this autumn for those at higher risk of severe COVID-19, based on recommendations from its Joint Committee on Vaccination and Immunisation (JCVI). JCVI also indicated that an additional booster dose for those individuals at greatest risk, such as older adults or those with compromised immune systems, may be recommended for this spring, and plans for the spring 2023 vaccination program will be announced soon.
Two new studies provide evidence bivalent boosters increase protection against Omicron subvariants compared to original vaccines, boosters
Part of the efforts to evaluate longer-term SARS-CoV-2 vaccination strategies necessitates understanding the safety and effectiveness profiles of the recent bivalent booster doses. Two studies published this week offer additional insight into the protective value of these boosters. Both studies provide evidence that bivalent boosters provided increased protection against Omicron subvariants compared to monovalent vaccines and boosters, at least in the short term.
A study conducted by researchers in North Carolina—published as a correspondence in NEJM—evaluated bivalent mRNA vaccine boosters’ effectiveness against severe COVID-19 disease caused by several Omicron subvariants (BA.4.6, BA.5, BQ.1, and BQ.1.1). Based on data from more than 1 million individuals who received bivalent boosters, followed over a 99-day period after vaccination, they estimated the boosters’ effectiveness against hospitalization or death to be 54.0% as the first booster dose*, 64.0% as the second booster dose, and 63.1% as the third booster dose. Across all measured outcomes, the bivalent boosters consistently outperformed monovalent boosters by more than 30 percentage points (pp)**, including in older adults—+37.8pp against hospitalization and +41.2pp against hospitalization or death.
*Marginally not statistically significant (CI: -.03-78.9%).
**Mix of statistically significant and non-significant results.
A study led by the US CDC’s National Center for Immunization and Respiratory Diseases—published in the CDC’s MMWR—evaluated the effectiveness of bivalent mRNA vaccine boosters in preventing symptomatic COVID-19 disease caused by the Omicron BA.5 and XBB/XBB.1.5 sublineages, compared to full vaccination and/or boosting using only the original monovalent vaccines. The study involved data from nearly 30,000 PCR-based SARS-CoV-2 tests conducted among persons with COVID-like illness symptoms at US pharmacies from December 1, 2022, to January 13, 2023. The researchers estimated the bivalent boosters’ additional effectiveness against the BA.5 subvariant to be 52% higher among adults aged 18-49 years, 43% higher in adults aged 50-64 years, and 37% higher among adults 65 years and older. Against the XBB sublineages the bivalent boosters outperformed the monovalent vaccines by 49% among adults aged 18-49 years, 40% in adults 50-64 years, and 43% in adults aged 65 years and older, again with some evidence of waning protection by 2-3 months. Notably, these are some of the earliest data available on protection against XBB subvariants, and the study provides a near-real-time assessment of recent vaccinations.
Number of US cardiovascular deaths rose during pandemic’s first year prior to vaccine availability, especially among some populations
Deaths due to cardiovascular disease (CVD) rose substantially during 2020—the first year of the COVID-19 pandemic and prior to the availability of vaccines—representing the largest single-year increase since 2015 and surpassing the previous single-year total set in 2003, according to new data from the American Heart Association. Notably, the age-adjusted mortality rate increased for the first time in many years, by 4.6%, and the largest overall number of CVD-related deaths were seen among Asian, Black, and Hispanic populations, some of which have been disproportionately impacted by COVID-19.
The COVID-19 pandemic has had both direct and indirect impacts on cardiovascular health. Importantly, infection with SARS-CoV-2 is associated with new-onset clotting and inflammation in some people. According to a study recently published in Cardiovascular Research, COVID-19 disease—including post-COVID conditions commonly known as long COVID—is associated with increased short- and long-term risks of CVD and death from any cause. Additionally, during the beginning months of the pandemic especially, people with new or existing risk factors for CVD outcomes, such as heart disease, hypertension, or stroke symptoms, were reluctant or unable to access medical care. A recent study published in Nature Medicine estimates that the interruption of preventive care could result in more than 13,000 extra cardiovascular events in the UK. Some people are leveraging the association between CVD and COVID-19 to create and spread misinformation surrounding sudden deaths and injuries and vaccine safety, despite a lack of scientific evidence supporting their claims.
Papers, meetings evaluate pandemic-related public health measures
Gaining insight into the effectiveness and impacts of how various nations and institutions responded to the COVID-19 pandemic will provide lessons for future pandemic preparedness and public health measures. Several recent papers and meetings attempt to evaluate these measures, coordinate their use, and identify challenges for future events.
• A paper from the OECD published January 21 draws lessons and provides a synthesis of evidence from 67 national government-level evaluations produced in OECD countries during the first 15 months of the pandemic. Overall, the report finds that pandemic preparedness was insufficient, governments should carefully consider longer-term budgetary costs of actions to mitigate economic and financial pandemic effects, and trust requires transparency and stakeholder engagement, including from the public. The report also notes there is insufficient evidence on critical sectors’ pandemic preparedness and further assessment of lockdowns and restriction measures is needed, including the impact of lockdowns on domestic violence, alcohol consumption, mental health, and youth.
• The leaders of several international organizations—including the WHO, International Labour Organization (ILO), the International Road Transport Union (IRU), and others—met this week to finalize a set of recommendations developed by a Joint Action Group tasked with reviewing the impact of the COVID-19 pandemic, including uncoordinated national rules and restrictions, on transport workers and networks.
• A January 20 commentary published in PLOS Global Public Health by an international group of authors proposes a framework to unite scholarship into the institutional, political, organizational, and governance (IPOG) aspects of the COVID-19 response. Politics and governance are influenced by factors such as institutional norms and the structure and functioning of key public health organizations, they note, contending that “COVID-19 has exposed the need to expand, deepen, and sharpen the focus of investigation to explore the intersection of all of these key contextual factors and how they combine to influence outcomes.”
• An article published January 25 in Scientific Reports aims to explain why models used to project rates of COVID-19 incidence and confirmed cases in the latter part of 2020 were not especially accurate. According to the researchers, "Frequent changes in restrictions implemented by governments, which the modeling team was not always able to predict, in part explains why the majority of model projections were inaccurate compared with actual outcomes and supports revision of projections when policies are changed as well as the importance of modeling teams collaborating with policy experts.”
• Another article published January 25 in Scientific Reports analyzes COVID-19 community transmission risk associated with US colleges and universities. Contrary to rising public sentiment that younger and less-vulnerable populations act as primary introducers of COVID-19 to communities, the findings show that counties with high university enrollments might adhere more closely to public health and safety measures and vaccinations, potentially contributing to safer communities.
What we’re reading
CORONAVIRUS RESEARCH OVERSIGHT A 64-page report from the US Department of Health and Human Services’ (HHS) Office of Inspector General (OIG) says the US NIH did not sufficiently and effectively monitor grant awards to EcoHealth Alliance, limiting the federal agency’s ability to fully understand the nature of the research being conducted—including research on coronaviruses that might fall under enhanced potential pandemic pathogens (ePPPs)—identify potential problem areas, and take corrective action. The report comes as the National Science Advisory Board for Biosecurity (NSABB) is set to discuss new draft recommendations for biosecurity oversight.
RAPID ANTIGEN TESTS At-home COVID-19 tests, also called rapid antigen tests, remain a useful tool in helping to interrupt transmission of SARS-CoV-2, although they are not foolproof. Both NPR and the New York Times recently published articles discussing the tests’ advantages and disadvantages and how to increase testing accuracy (hint: serial testing). To order tests for home delivery in the US, find at-home tests at retailers and pharmacies, and learn about insurance reimbursement, visit covidtests.gov.
MEDICAID CONTINUOUS ENROLLMENT Between 5 and 14 million US citizens and certain legal immigrants are expected to lose their Medicaid coverage when a pandemic-era provision known as “continuous enrollment” ends on March 31. Of those, the US HHS expects 6.8 million people will lose coverage even though they are still eligible, based on historical trends of paperwork and other administrative hurdles. A new analysis from KFF estimates that about two-thirds of those who are disenrolled likely will experience a period of uninsurance. Disruption in Medicaid or other insurance coverage can lead to delayed or missed care, less access to preventive care, and higher healthcare costs, particularly for chronic health conditions.
YOUTH MENTAL HEALTH & NUTRITION Parents are growing increasingly concerned about young people’s mental health, according to a new report from the Pew Research Center, as children and teenagers continue to struggle with depression and anxiety after returning to in-person schooling following widespread school closures and remote learning during the early months of the COVID-19 pandemic. The isolation of remote learning and other pandemic-related stressors may have strained youth mental health, and some children may have experienced adverse childhood experiences (ACEs), such as abuse, neglect, or violence. One such stressor, food insecurity, is increasing among families due to rising food prices and the winding down of pandemic-era assistance programs providing free school meals.
Epi update
As of January 25, the WHO COVID-19 Dashboard reports:
• 665 million cumulative COVID-19 cases
• 6.7 million deaths
• 1.9 million cases reported week of January 16
• 33% decline in global weekly incidence
• 12,937 deaths reported week of January 16
• 16% increase in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in all WHO regions except the Eastern Mediterranean, which recorded a 54% increase in reported cases.
UNITED STATES
The US CDC is reporting:
• 101.9 million cumulative cases
• 1.1 million deaths
• 332,212 cases week of January 18 (down from previous week)
• 3,953 deaths week of January 18 (down from previous week)
• 13.7% weekly decrease in new hospital admissions
• 15.3% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (49%), BQ.1.1 (27%), and BQ.1 (13%) account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by dryrunguy Here's the latest Situation Report.
::
COVID-19 remains international emergency, WHO says, begins discussions on future pandemic preparedness
WHO Director-General Tedros Adhanom Ghebreyesus on January 30 took the advice offered by the International Health Regulations (2005) (IHR) Emergency Committee (EC) regarding COVID-19 following its 14th meeting last week, announcing that the pandemic remains a public health emergency of international concern (PHEIC) for now but is likely at a “transition point.” The WHO acknowledged that COVID-19 continues to cause a high number of deaths globally, particularly compared to other respiratory diseases; vaccine uptake in low- and middle-income countries remains insufficient; and there remains uncertainty about the possibility of newly emerging variants but recognized the world is in a much better place now than even one year ago, when the Omicron variant of concern was predominant.
In a set of temporary recommendations, the WHO called on nations to continue administering COVID-19 vaccines and incorporating them into routine vaccination programs; improve disease surveillance reporting to the WHO and integrate COVID-19 surveillance into existing systems tracking other disease transmission and viral evolution; improve uptake of and assess the regulatory implications of ending the PHEIC for diagnostics, therapeutics, and vaccines; maintain strong healthcare systems and prepare for future health emergencies; and continue to combat misinformation, adjust international travel measures based on risk assessments, and support research. The EC will meet again in 3 months to reconsider the public health emergency designation.
In related news, the WHO Executive Board, which is holding its annual meetings this week and next, is considering its role in addressing the next global health emergency and how it will fund those activities. A 10-point proposal on improving preparedness and response to health emergencies presented at the meeting by Dr. Tedros received mixed reviews from WHO member states. Additionally, the WHO released a “zero draft” of a pandemic treaty to its 194 member states this week, setting the stage for negotiations over how the world should respond to future health emergencies. One of the most significant measures in the draft document proposes that the WHO reserve 20% of all newly developed pandemic products—diagnostics, vaccines, treatments, and the like—for distribution in lower-income countries. Overall, the draft lays out recommendations for how to make the response to the next pandemic more equitable.
US to end emergency declarations on COVID-19 in May; Americans face changes to pandemic-related healthcare coverage
US President Joe Biden announced this week that he will end both the national emergency and public health emergency declarations for COVID-19 pandemic on May 11, marking a new phase of the federal pandemic response as some of the flexibilities and requirements instituted in the pandemic’s early days will end.* The announcement was made alongside a statement opposing resolutions proposed by US House of Representative Republicans to immediately end the COVID-19 emergency (more on House Republican actions below), saying an abrupt end to the declarations “would create wide-ranging chaos and uncertainty.” Though many US residents are fully vaccinated against the virus and have largely returned to a normal way of life, an average of more than 500 people die of the disease in the US every day, making COVID-19 a leading cause of death, even among children and young people.
Once the emergencies end, some things for people in the US will change, particularly in healthcare. Many Americans have been able to access COVID-19 tests and treatments free of charge under the emergency declarations, but the end of those means a return to the nation’s typically fractured healthcare system. As such, many people—even some who have health insurance or qualify for Medicare or Medicaid—will be responsible for some or all of the cost of these medical countermeasures. Most people will continue to be able to access vaccines and boosters at no cost, but there is no guarantee of full coverage under private insurance or social safety net programs. To make matters more confusing, benefits may vary by insurer or state. Additionally, hospitals will lose pandemic-related emergency funding, and some healthcare data reporting may no longer be required. Unrelated to the emergencies’ ends, pandemic-era boosts to the nation’s Supplemental Nutrition Assistance Program (SNAP) will end this month and continuous Medicaid enrollment will end on March 31.
*Notably, the emergency declaration allowing the US FDA to make emergency use authorizations (EUAs) for COVID-19 medical countermeasures will not end on May 11. The timing to conclude the EUA has yet to be determined.
US House Republicans take action to immediately end pandemic emergency, investigate pandemic fraud
The US House of Representatives’ newly sworn-in Republican majority is swiftly taking actions to reverse or investigate COVID-19 policies from previous years. The House, voting on party lines, recently passed the “Pandemic is Over Act” and the “Freedom for Healthcare Workers Act,” both aimed at bringing certain policies and budget lines for COVID-19 response to a close. The “Freedom for Healthcare Workers Act” would end the vaccine mandate for healthcare workers, an action that US President Joe Biden has already stated he would veto should it pass the US Senate. Republicans have long stated their intentions to end many COVID-19 programs and policies, and continue to take action toward doing so, despite an announcement by President Biden this week that he will end some emergency declarations for COVID-19 on May 11 (see story above).
Republicans also have begun investigations into waste, fraud, and abuse of COVID-19 funding. Of the US$5 trillion total spent on emergency relief throughout the pandemic, experts estimate the amount drained by fraud could be anywhere between tens of billions of dollars to more than US$100 billion, but it will take years to understand the total amount.
US FDA advisory committee supports harmonizing COVID-19 vaccines, moving toward annual shots for many
The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) met last week to consider streamlining COVID-19 vaccination schedules and formulations. The committee unanimously voted to replace vaccine manufacturers’ (Pfizer-BioNTech, Moderna, and Novavax) original vaccine formulations targeting only the original wild type virus—currently used for the initial 2-dose series—with the new bivalent shots that target both the original strain and the Omicron BA.4 and BA.5 variants. The bivalent vaccines currently are authorized for use as boosters. The change would only affect individuals who have not yet received their initial shots, and there is no timeline on when the switch might occur if the FDA accepts the panel’s nonbinding recommendation. About 69% of the US population has received the full initial vaccine series, and only 15% of the population has gotten a bivalent booster.
While these are some initial steps toward streamlining the COVID-19 vaccination process, there are still many logistical and scientific questions to be answered on how often, how many, and to whom vaccines should be delivered. For many, the newly proposed schedule would follow a model similar to that of annual flu shots, with most receiving an annual COVID-19 vaccine in the fall that has been updated based on the predominantly circulating variant or variants. Some have termed this strategy the “flu-ification” of COVID-19, in that it will be regarded as a seasonal disease. These assumptions may or may not prove to be accurate in the case of COVID-19, as SARS-CoV-2 mutates at a much different rate and with less predictably than the viruses that cause flu. While flu predictions have decades of research to support the selection of the next year’s vaccine strain, SARS-CoV-2 is much less predictable with much less supporting data to make those predictions. It is also unclear whether it will be necessary for everyone to receive a new booster every year. Given existing challenges in the uptake of annual flu vaccines, marketing COVID-19 vaccines on a similar schedule may prove more difficult than anticipated.
Positive COVID-19 test no longer needed to access antivirals; concerns raised over potential for viral mutations after Lagrevio treatment
The US FDA on February 1 revised the emergency use authorizations (EUAs) for the COVID-19 antivirals Paxlovid (nirmatrelvir and ritonavir) and Lagevrio (molnupiravir), removing the need for individuals to test positive for SARS-CoV-2 before receiving the therapies. Now, healthcare providers can prescribe the drugs to those who have a recent known exposure, are having signs and symptoms, and are at high risk of disease progression but test negative for the virus. Though a positive test is no longer a requirement, the FDA continues to recommend direct testing to help diagnose COVID-19.
The move may be meant to address underuse of Paxlovid, and the much less used Lagevrio, but some experts say the move could lead to overuse of the medications. A new preprint study posted to medRxiv is raising concerns among some about the potential of Lagevrio to cause mutations in SARS-CoV-2 that could be passed along and give rise to new variants. The study, which is not yet peer-reviewed, is the latest of several that could change the risk-benefit calculus for the drug. There is no evidence the mutations have led to the emergence of a circulating variant that is more pathogenic or transmissible, but some say this evidence, along with studies suggesting Lagrevio has limited benefits, call into question whether it should be used.
The Chinese government recently cleared Lagrevio, Paxlovid, and 3 homegrown antivirals for the treatment of COVID-19, but questions remain over how well the Chinese antivirals can minimize severe illness and related deaths and how accessible any of the drugs are to the general population.
US FDA withdraws authorization of Evusheld; US CDC urges those with compromised immune systems to take extra precautions
The US FDA last week withdrew its emergency use authorization (EUA) of Evusheld (tixagevimab co-packaged with cilgavimab) until further notice, as data show the monoclonal antibody is unlikely to be active against the majority of SARS-CoV-2 variants currently circulating in the country. The therapy had been authorized for use as pre-exposure prophylaxis of COVID-19 in people aged 12 years and older who are immunocompromised and not expected to have an adequate response to vaccination, as well as individuals with a history of severe adverse reaction to COVID-19 vaccination or who are allergic to certain vaccine components.
The move led the US CDC to recommend those with weakened immune systems take extra precautions to avoid SARS-CoV-2 infection and have a care plan that includes quick testing at the onset of symptoms and rapid access to antiviral treatments if they test positive for COVID-19. While immunocompromised individuals should stay up to date on their COVID-19 vaccinations, if possible, including receiving an updated bivalent booster, the CDC also recommends wearing a high-quality and well-fitting mask, maintaining physical distance of 6 feet or more from others, improving indoor ventilation, and practicing frequent handwashing.
What we’re reading
LONG COVID The first in-person long COVID summit in the US was held last week in Richmond, Virginia, hosted by US Senator Tim Kaine and the US HHS. Some data suggest the percentage of people experiencing long COVID symptoms after acute infection is declining, but the condition continues to have implications for employment and health care. Multiple studies, including a recent one from New York State, show a significant number of people are missing work because of long COVID, as described in coverage from the New York Times, Guardian, CNBC, and The Hill.
LEARNING DELAYS Children experienced learning delays during the COVID-19 pandemic equivalent to about one-third of a school year’s worth of knowledge and skills, according to a global analysis including data from 15 countries and published this week in Nature Human Behavior. Mathematics skills were more heavily affected than reading skills, the study found, and those learning gaps have not been recovered as of May 2022. The pandemic reinforced inequalities in learning, with the authors predicting the pandemic’s effects on learning will be more severe for children in poorer regions. NPR spoke with several college freshmen to get their take on how the pandemic impacted their high school years.
LESSONS FOR FUTURE RESPONSES Several recent commentaries have touched on the importance of drawing lessons from the pandemic for future responses to be more equitable and nuanced. One published in STAT examines shortcomings in collecting epidemiological data in the US that includes race and ethnicity information. A piece in The BMJ argues that a focus on gender is needed to help shape responses to reduce inequalities in job losses and sustained employment precarity after the pandemic. A perspective piece published in the New England Journal of Medicine argues that one of the key lessons of the COVID-19 pandemic is that policymakers must take into account the ways in which population-wide public health recommendations and policies differentially affect various subgroups of the population and take a more differentiated approach, and recognize that who delivers pandemic-related messages matters.
PANDEMIC ORIGINS The US House Committee on Energy and Commerce’s Subcommittee on Oversight and Investigations held a hearing February 1 to discuss biological investigations and attribution science, focused on the public release of a new report from the US Government Accountability Office (GAO) titled, “Pandemic Origins: Technologies and Challenges for Biological Investigations.” Dr. Tom Inglesby, director of the Johns Hopkins Center for Health Security and professor in the Department of Environmental Health and Engineering at the Johns Hopkins Bloomberg School of Public Health, provided testimony on the importance of bioattribution to pandemic preparedness, national security, and growing the US bioeconomy.
Epi update
As of February 2, the WHO COVID-19 Dashboard reports:
• 754 million cumulative COVID-19 cases
• 6.8 million deaths
• 1.5 million cases reported week of January 23
• 40% decline in global weekly incidence
• 12,793 deaths reported week of January 23
• 49% increase in global weekly mortality
Over the previous week, incidence declined in all WHO regions.
UNITED STATES
The US CDC is reporting:
• 102.2 million cumulative cases
• 1.1 million deaths
• 295,140 cases week of January 25 (down from previous week)
• 3,756 deaths week of January 25 (down from previous week)
• 8.4% weekly decrease in new hospital admissions
• 12.5% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (61%), BQ.1.1 (22%), and BQ.1 (9%) account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ponchi101 We will enter the phase in which this "lives with us, and there is nothing we can do".
I hope the development of variant-specific vaccines will get under way soon. And our yearly shot.
by dryrunguy
ponchi101 wrote: ↑Thu Feb 02, 2023 10:24 pm
We will enter the phase in which this "lives with us, and there is nothing we can do".
I hope the development of variant-specific vaccines will get under way soon. And our yearly shot.
For the time being, I'm getting the jab every 6 months.
by Deuce I'm in a quandary...
I received my last booster (it was my 2nd booster, and 4th vaccine overall) at the beginning of June (2022). A rapid (antigen) test indicated positive for COVID-19 at the beginning of October (2022).
Now, after doing some detailed research, I've decided that I want the bivalent Moderna booster targeting BA.4/BA.5. My research indicates that this is the most effective current Moderna booster (all my COVID vaccines to this point have been Moderna, so I want to stick with them).
But the vaccine centres and pharmacies in my area are offering only the bivalent Moderna for BA.1 (and the bivalent Pfizer BA.4/BA.5). They say that they've been told they must use up all of the Moderna BA.1 before they begin to offer Moderna BA.4/BA.5.
I have been trying to get the Moderna BA.4/BA.5 for over a month now, without success. The big vaccine centre here told me yesterday that they have it in their freezers on site - but they are not allowed to give it out to people.
I find this absurd, and a violation of people's inherent rights.
When I got my 'flu vaccine last month (the first of my life), the person administering the vaccine told me that he thinks it's very wrong that the bivalent Moderna BA.4/BA.5 is being withheld from people...
One of the doctors who is regularly on National TV here discussing COVID-19 (whom I contacted for help about this) told me that he's extremely surprised that the bivalent Moderna BA.4/BA.5 is not available to everyone, as it is an approved vaccine.
I have the right to decide what enters my body. I am not asking for anything special - I am asking simply for a vaccine that is perfectly legal, and which was approved for use in Canada 3 months ago.
But it is effectively being withheld from people - and this is wrong.
by ti-amie Strange indeed Deuce.
All of my jabs have been Pfizer. I'm up to date with boosters too.
by dryrunguy Here's the latest Situation Report. I was especially intrigued by the section on missing students.
::
White House expected to release roadmap to transition out of public health emergency; US House committee holds hearing on pandemic response
The US winter COVID-19 surge appears to be ending, with the increase in reported cases not as bad as initially expected. There was concern in early winter that a combination of COVID-19, RSV, and seasonal influenza would overwhelm hospitals and cause a large surge in deaths. Speculation around why the winter surge was not as bad as expected has centered on people possibly avoiding crowds over the holidays, viral interference among various circulating diseases, and more immunity in the US population due to prior infection and/or vaccination. COVID-19 remains a significant public health threat and a leading cause of death in the US, but there appears to be hope on the horizon. As such, the Biden administration is expected to soon release a roadmap to transition out of the COVID-19 public health emergency, which is set to end on May 11. The end of the public health emergency will also terminate the Trump-era Title 42 orders that US-Mexico border patrol agents have used to return undocumented migrants across the border in the name of COVID-19 prevention. Title 42 has been heavily criticized by public health experts and immigrant advocates, but Republican-led states have sought to keep the orders in place.
Additionally, the Republican-led US House of Representatives is stepping up efforts to investigate the pandemic response. The House Energy and Commerce Committee held a hearing on “The Federal Response to COVID-19” this week. Republicans on the committee used the opportunity to ask leading health officials and scientists about vaccine mandates, mask requirements for children, origin theories of SARS-CoV-2, and the public’s broken trust in health agencies. Additional hearings on similar topics are expected. In a mostly symbolic move, the House on February 8 passed a bill mostly along party lines that would end US CDC-imposed COVID-19 vaccination requirements for foreign travelers entering the US. The White House said it opposes rescinding the order without scientific review, but the travel industry has lobbied for the removal of the requirement, claiming it is an unnecessary barrier to travelers.
WHO releases zero draft of global pandemic treaty; US chairs fourth and final Ministerial of the COVID-19 Global Action Plan
In the last week, two major global efforts to combat future outbreak emergencies and strengthen global health security have reached important milestones in their continuing efforts. Last week, the WHO released a zero draft of a global pandemic treaty, focused on international prevention, preparedness, and response. This would be the first legally binding treaty helping to ensure a more equitable distribution of pandemic-related vaccines, drugs, and diagnostics. WHO member states will now deliberate to negotiate treaty terms and make progress to ensure stronger international collaboration and equity throughout future biological events.
This week, US Secretary of State Anthony Blinken hosted a fourth and final Ministerial of the COVID-19 Global Action Plan (GAP). The GAP has been working for the past year to continue addressing acute pandemic response needs and identifying remaining barriers to fighting the COVID-19 pandemic, as well as planning collaborative prevention, detection, and response methods among many countries and global organizations ahead of the next global health threat. During the meeting, Japan Foreign Minister Yoshimasa Hayashi said that Japan has chosen global health as a priority issue when the nation hosts a Group of Seven summit in May, partly because of the continuing challenge of equitable vaccine access.
Cochrane Library review examines effectiveness of various nonpharmaceutical interventions; most experts agree future pandemics will require more nuanced responses
More than 3 years into the COVID-19 pandemic, experts continue to discuss whether masking definitively slows transmission of respiratory viruses, and by how much. Throughout the pandemic, numerous studies have been published with conflicting results and conclusions, culminating in a recent review published by the Cochrane Library. The review found that masking, either with surgical masks or N95 respirators, made little to no difference in the outcome of laboratory‐confirmed influenza/SARS‐CoV‐2 compared to not wearing masks; however, the review emphasized that the findings could be due in part to multiple factors such as poor study design, low adherence to mask rules, quality of masks used, and incorrect mask usage. Notably, several individual studies have shown an association between community mask use and a reduction in COVID-19 cases. The review also found that hand hygiene programs may help slow the spread of respiratory diseases. Results of the review have split infectious disease experts, leading some to critique its methodologies and emphasize the importance of public messaging on nonpharmaceutical interventions (NPIs) to prevent disease transmission. More research is needed into various NPIs and public health interventions and their use in future disease outbreaks likely will need to be more nuanced.
Clinical trial shows promise for interferon therapy but regulatory hurdles exist; experts say additional treatment options desperately needed
Monoclonal antibodies have been an important tool in treating COVID-19 and as pre-exposure prophylaxis for those at high risk of severe disease, especially individuals with compromised immune systems. Following the US FDA’s suspension of emergency use authorization (EUA) for Evusheld last month, however, no monoclonal antibodies are authorized for use in the US because of inactivity against currently circulating variants of SARS-CoV-2. Other treatments exist, including the antivirals Paxlovid and molnupiravir, but each comes with its own concerns, including worry over viral rebound, drug interactions, or viral mutations.
Newer medicines that remain active against various SARS-CoV-2 lineages are needed to help shore up the nation’s therapeutic toolbox, and potentially help protect people who are immunocompromised. The results of a clinical trial involving nearly 2,000 patients published this week in the New England Journal of Medicine show that people with early COVID-19 who had a single injection of a treatment called pegylated interferon lambda (PEG-lambda) were 51% less likely to be hospitalized or to go to an emergency room, compared with those who received a placebo shot. Most of the study participants were vaccinated—an already low-risk group—but the treatment was even more effective in unvaccinated participants.
Interferons are a part of the body’s natural immune response, and PEG-lambda is a synthetic version of a naturally produced interferon. Even with promising results, the treatment faces hurdles to regulatory approval by the FDA, which has signaled it needs data from a larger trial with sites located in the US, an expensive and multi-year process. Some experts worry the barriers are indicative of problems threatening the future development of next-generation COVID-19 medical countermeasures, some of which might help prepare for the next pandemic.
Black Americans, others face barriers to long COVID treatment, care; caregivers need support too
Though the medical community is learning more about long COVID, also called post-COVID condition or post-acute sequelae of COVID-19, much remains unknown about how many people have the condition, why and what their prospects for recovery are, or the long-term impacts on society. In the US Black community, already disproportionately impacted by the pandemic, many with symptoms lingering a month or longer after recovering from acute COVID-19 are struggling to find the care they need. According to the latest data from the US Census Bureau Household Pulse Survey, nearly 30% of Black respondents said they currently have or have had long COVID and about 35% of those with long COVID reported severe limitations on their ability to perform day-to-day activities. Additionally, caregivers of people with long COVID, many of whom suffer from the same or other health conditions, need to establish their own support systems, sometimes in the form of support groups such as those with Survivor Corps or Body Politic. Online support groups and other forms of telerehabilitation are useful for both people with long COVID and their caregivers, some face barriers to access because of internet and digital literacy considerations.
What we’re reading
SARS-COV-2 VARIANTS No new variants of SARS-CoV-2 were detected in China between November 14 and December 20, 2022, during a time when the nation began experiencing a surge of COVID-19 cases, according to a study published February 8 in The Lancet. A majority of the sequenced samples were the already circulating Omicron subvariants BF.7 and BA5.2. Notably, the study only looked at samples from Beijing and only covered a few weeks after the government lifted its strict “zero COVID” policies, which some experts warn would be too early to detect new lineages. Scientists have their eye on another variant—CH.1.1—that emerged in November 2022 in Southeast Asia and now accounts for about 25% of cases in the UK and New Zealand, and about 12% of overall cases in Europe. According to a preprint report posted on bioXriv, the lineage contains the mutation L452R seen in Delta, but not Omicron, and has “a consistently stronger neutralization resistance available than XBB, XBB.1, and XBB.1.5,” which is worthy of monitoring.
EXCESS MORTALITY Between March 2020 to December 2021, 622 more physicians died in the US than expected, according to a study published in JAMA Internal Medicine this week. Excess mortality among physicians was substantially lower than for the general population during this time, and there were no excess deaths among physicians after April 2021, concurrent with the availability of COVID-19 vaccines. In related news, the New York Times examined the obituaries of China’s top academics to gain some insight into the nation’s true death toll since it dropped its “zero COVID” strategy, finding significantly higher numbers of published obituaries in December 2022 and January 2023 than in preceding months.
HONORING THOSE LOST More than 1.1 million people in the US have died of COVID-19 since the beginning of the pandemic, and about 3,500 people continue to die each week of the disease. Colorado Public Radio/NPR reports on the desire—some say need—to memorialize individuals who died of COVID-19, to recognize and remember their lives but also to help those left behind heal from the trauma of losing loved ones. In October 2022, the Johns Hopkins Center for Health Security, in collaboration with the Center for Health and Economic Resilience Research at Texas State University, held a 2-day virtual symposium, titled Post-Pandemic Recovery: From What, For Whom, and How?, to consider how to operationalize the process of holistic recovery from the COVID-19 pandemic, including a focus on trauma recovery centered on safety, memorialization, and social connection.
LEARNING LOSSES & MISSING STUDENTS Half of US students began this academic year below their grade level in at least one subject, according to new federal survey data based on reports from schools nationwide. Nearly all schools said some students were behind in reading and math, 80% reported students behind in science, and 70% reported lags in social studies. The results, along with other research, show students and educators have a long road ahead to reverse pandemic impacts. Worse, an analysis by the Associated Press, Stanford University’s Big Local News project, and Stanford professor Thomas Dee found an estimated 240,000 students in 21 states who disappeared from public schools during the pandemic and whose absences cannot be accounted for. Some students who left public schools moved out of state or switched to private schools or home-schooling, but nearly a quarter million remain “missing” and the true number is likely much higher.
ANTIMICROBIAL RESISTANCE According to a study published recently in The Lancet Microbe, antimicrobial resistance (AMR) is highly prevalent in patients with laboratory-confirmed COVID-19 and bacterial infections. In another recent analysis published in eClinical Medicine, researchers found that increases in antibiotic sales were associated with increases in COVID-19 cases, according to data collected during the first 2 years of the pandemic in 71 countries. Despite less than 10% of COVID-19 patients having a bacterial coinfection, an estimated 75% of COVID-19 patients are prescribed antibiotics, underlining the need for greater antibiotic stewardship in the context of COVID-19. In related news, the United Nations Environment Programme (UNEP) published a report this week warning that up to 10 million people could die annually by 2050 due to AMR, making it one of the top 10 global threats to health requiring a multisectoral response that recognizes the intertwined health of people, animals, plants, and the environment, referred to as One Health.
Epi update
As of February 9, the WHO COVID-19 Dashboard reports:
• 755 million cumulative COVID-19 cases
• 6.8 million deaths
• 1.35 million cases reported week of January 30
• 13.5% decline in global weekly incidence
• 13,440 deaths reported week of January 30
• 16% decrease in global weekly mortality
Over the previous week, incidence declined or remained stable in all WHO regions. The WHO notes that the case and death data for the Eastern Mediterranean region are incomplete and will be updated as soon as possible.
UNITED STATES
The US CDC is reporting:
• 102.4 million cumulative cases
• 1.1 million deaths
• 280,911 cases week of February 1 (down from previous week)
• 3,452 deaths week of February 1 (down from previous week)
• 6.2% weekly decrease in new hospital admissions
• 11.3% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (66%), BQ.1.1 (20%), and BQ.1 (7%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ponchi101 Especially, how does the "missing student" phenomenon relates to C19?
by skatingfan
ponchi101 wrote: ↑Fri Feb 10, 2023 3:33 pm
Especially, how does the "missing student" phenomenon relates to C19?
Tens of thousands of American children lost a primary, or secondary caregiver to COVID. I wonder how many young people have dropped out of school to start earning money for a family now missing an income earner.
by Owendonovan I have found my kindergartners, 1st and 2nd grade boys are very immature at this age compared to pre covid.
by Deuce After fighting for almost 2 months, I finally received my Moderna Bivalent BA.4/BA.5 booster yesterday.
About 10 days ago, I was able to contact one of the head doctors in the province, and we had a correspondence for a few days... As a result, she contacted the regional director of vaccines, who then asked for and received 'permission' from the provincial government health services to free up this vaccine to the population.
Prior to this, the region was insisting on using up all of the Moderna Bivalent BA.1 boosters before allowing access to the Moderna Bivalent BA.4/BA.5 boosters. This made no sense, as both vaccines were approved for use in Canada, and the BA.4/BA.5 boosters effectively rendered the BA.1 boosters more or less obsolete.
by MJ2004 My parents had the bivalent vaccine and both had COVID two months later- my mom ended up in the hospital for five days.
Given the constantly shifting variants and sub variants, I’m not convinced it makes much difference which vaccine is administered, which was likely the logic behind the decision to first use up the original supply.
by ponchi101 I will assume that you parents came out of it and are doing well. Happy for you, and them (and hoping my assumption is correct).
by Deuce
MJ2004 wrote: ↑Sun Feb 12, 2023 3:51 pm
My parents had the bivalent vaccine and both had COVID two months later- my mom ended up in the hospital for five days.
Given the constantly shifting variants and sub variants, I’m not convinced it makes much difference which vaccine is administered, which was likely the logic behind the decision to first use up the original supply.
Yes - there's no doubt that it's a moving target due to the evolving and different variants...
But I did some rather profound research, and concluded that this vaccine was the best currently approved booster.
That's unfortunate about your mom - and surprising, as we keep reading and hearing that the vaccines will help to lower - not eliminate - the chances of contracting COVID, and will go a long way toward greatly reducing the chances of severe symptoms of COVID. But nothing is 100%.
I hope your mom has recovered fully.
by MJ2004 Yes, both are now recovered. In that sense, the vaccine did its job. Thank you!
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
US House committees begin investigations into SARS-CoV-2 origins, reviews of federal pandemic response; WHO pandemic origin inquiry to continue under SAGO panel
As the Biden administration prepares to wind down the federal Public Health Emergency (PHE) for COVID-19 on May 11—releasing a transition roadmap on February 9—the Republican-controlled US House of Representatives is ramping up its efforts to investigate the origins of SARS-CoV-2 and examine how the federal government responded to the pandemic. At least 2 House committees are investigating the pandemic’s origins, setting the stage for overlap and possible tension over priorities. The House Energy and Commerce Oversight and Investigations Subcommittee held hearings early this month delving into biological event origin investigations and the federal pandemic response. The House Select Subcommittee on the Coronavirus Pandemic of the Committee on Oversight and Accountability recently received 900 pages of records from the US Department of Health and Human Services (HHS) it requested to begin its review of similar topics. It remains unclear how the committees will differentiate their investigations. Some outside of government are calling for the establishment of a COVID commission to conduct a broad inquiry into the federal response.
Little is known of how SARS-CoV-2 originated—though most experts agree the pandemic began in China—and definitive answers about whether the virus began spreading among humans in a market or as the result of a laboratory accident may never be known, as much of the world moves beyond the pandemic. WHO officials have expressed frustration with efforts to investigate the pandemic’s origins, with politics hampering collaboration and damaging trust among Chinese counterparts. Additionally, the amount of time elapsed since the first recorded cases in China has made investigations into the pandemic’s origin increasingly difficult. The WHO last week said there will not be a “phase 2” of its original coronavirus investigation but another WHO panel—the Scientific Advisory Group for the Origins of Novel Pathogens (SAGO)—will continue looking for answers.
Multiple studies examine aspects of long COVID, including neurological symptoms, organ damage, racial/ethnic disparities; WHO releases clinical case definition for children, adolescents
Researchers continue their work to learn more about post-COVID-19 condition (PCC), also known as post-acute sequelae of COVID-19 (PASC) and most commonly as long COVID.
• A study published February 14 in the Journal of the Royal Society of Medicine examined the prevalence of organ impairment in long COVID patients at 6 and 12 months after initial symptoms. Symptoms such as extreme breathlessness, cognitive dysfunction, and poor health-related quality of life were common at 6 and 12 months and associated with female gender, younger age, and single-organ impairment. Overall, 59% of 331 patients followed for 1 year experienced single organ impairment and 29% had multi-organ impairment with implications for persistent symptoms and reduced function. Researchers observed mild damage in patients’ hearts, lungs, kidneys, livers, spleens, and pancreas.
• Some of the most common symptoms among people living with long COVID are neurological, and a few experts are beginning to focus on these persistent brain and nervous system issues of their patients. A study published February 23 in The Lancet Regional Health Europe found that among 165 people with PCC in Sweden, cognitive, sensorimotor, and fatigue symptoms were the most common symptoms persisting at 24 months. Some studies suggest SARS-CoV-2 might trigger an immune response leading to ongoing inflammation in the brain, and understanding these inflammatory processes might point to potential treatment options. Still, more research is necessary to understand the mechanisms behind the possible neurological impacts of COVID-19 and differentiating those symptoms from functional neurological disorder (FND), according to a recent study published in the European Journal of Neurology.
• A preprint posted January 26 to medRxiv found SARS-CoV-2 infection is associated with an increased risk of developing new-onset autoimmune diseases after acute infection, with the highest incidence rate ratio (IRR) observed for the rather uncommon autoimmune diseases of the vasculitis group, such as small vessel inflammatory processes. The large matched cohort study, which is not yet peer-reviewed, included 641,704 patients with COVID-19.
• New evidence from US NIH-supported studies shows that long COVID symptoms and diagnostic experiences vary among different racial and ethnic groups. Two studies show that Black and Hispanic Americans seem to experience more symptoms and health problems related to long COVID than White Americans; however, they are less likely to receive a long COVID diagnosis. This is even more concerning given findings from other studies showing that patients with long COVID report higher rates of unemployment, underemployment, new-onset symptoms, disabilities, and financial problems 6 months after hospitalization.
• Efforts are being made to better define long COVID but there is no consensus on its prevalence, what symptoms it comprises, or standard diagnosis protocol. Some experts question the need for a standard diagnosis, arguing that treating symptoms of the condition is sufficient, though others disagree. The WHO previously released a clinical case definition for PCC and last week published a clinical case definition for PCC in children and adolescents. Both definitions were developed using robust protocol-based methodologies and engaged diverse groups of representative patients, caregivers, and other stakeholders.
Emergency US SNAP benefits ending March 1; older adults, rural populations, communities of color most likely impacted by increased food insecurity, hunger
During the pandemic, numerous families have received additional assistance through the US Supplemental Nutrition Assistance Program (SNAP); however, these emergency allotments will end on March 1 in 32 states as well as Washington, DC; Guam; and the US Virgin Islands. With more than 41 million US residents relying on SNAP benefits, this upcoming change—dubbed by some experts as a “hunger cliff”—is expected to strain family finances, with the average recipient losing an estimated $82–$90 per month in benefits, shifting aid burdens to food banks and other similar local programs that most likely will not be able to make up the difference in assistance. Coupled with food price inflation since 2020, the end of emergency allotments is expected to hit older individuals, rural populations, and communities of color the hardest with increased food insecurity and poverty-related hunger. If you are or know someone in need of food security assistance who may be impacted by this upcoming change, contact your local SNAP office and/or call the US Department of Agriculture’s (USDA) Hunger Hotline: 1-866-3-HUNGRY (1-866-348-6479) or 1-877-8-HAMBRE (for Spanish), Monday through Friday, 7 am to 10 pm ET.
Popular figures influenced public opinion, discourse on COVID-19 through social media networks; US FDA working to dispel medical myths
Through the use of online social networks, people in the public eye (PIPE)—including news anchors, politicians, athletes, entertainers, and others—helped shape public opinion and discourse on the COVID-19 pandemic and related public health efforts, according to an analysis of 45,255 tweets posted between January 2020 and March 2022 published in BMJ Health & Care Informatics. Overall, the related sentiments shared by subgroups of public figures were found to be more negative than positive, and posts shared by politicians and news anchors appeared to be the most influential. The researchers note the analysis underscores the importance of cooperation among health professionals, public health organizations, and community groups to proactively and efficiently share clear, correct, and population-relevant health messaging to inform and educate the public about mis- and disinformation in response to future disease outbreaks.
According to US FDA Commissioner Dr. Robert Califf, some people are dying of COVID-19 because they are “misinformed” and influenced by “distortions and half-truths.” To counter misinformation, the FDA is stepping up its presence on social media outlets to debunk medical myths. But some experts are concerned the agency’s reputation as a trusted messenger might have been damaged by contentious drug approvals and other controversies. Experts also warn that the agency’s messaging is reaching a small audience and that its language, particularly surrounding decisions on COVID-19 vaccine boosters, needs to be simplified.
The Johns Hopkins Center for Health Security is engaged with several projects working to combat health-related misinformation and disinformation through conducting research, identifying best practices, educating public health professionals and policymakers, and furthering policy solutions to the problem. Read more here.
What we’re reading
MASK USE EFFECTIVENESS The January 30 publication of a Cochrane review that found masking, either with surgical masks or N95 respirators, made little to no difference in the outcome of laboratory‐confirmed influenza/SARS‐CoV‐2 compared to not wearing masks has reignited the debate over mask use. As we mentioned in our February 9 coverage of the meta-analysis, the review emphasized that the finding could be due in part to multiple factors such as poor study design, low adherence to mask rules, quality of masks used, and incorrect mask usage. Several sources have since reviewed the publication, including The Atlantic, Vox, and Your Local Epidemiologist, outlining the Cochrane review’s potential shortcomings and highlighting evidence showing that masking works to reduce the risk of respiratory disease transmission. Additionally, the WHO reiterated its firm recommendation that wearing masks is an effective method to prevent the spread of COVID-19, along with vaccination and physical distancing when possible.
LIFE EXPECTANCY & ECONOMIC IMPACTS An article published in Scientific Reports assessed the impact of 1 million COVID-19 deaths in the US between February 2020 and May 2022, focusing on economic and life expectancy losses. The researchers estimated that COVID-19 deaths contributed to a drop in US life expectancy at birth by 3.08 years, effectively reversing all gains made in the last 40 years. Economic welfare losses estimated in terms of national income growth supplemented by the value of lives lost were around US$3.57 trillion. Hispanic and Black populations were disproportionately impacted. The results of the analysis underscore the need for additional investments in pandemic preparedness to prevent economic shocks from future disease outbreaks.
DEATHS IN US PRISONS The New York Times examined data on deaths in US state and federal prisons during the beginning of the COVID-19 pandemic, reporting that prisoner deaths rose nearly 50% during 2020, more than twice the increase in the US overall and exceeding the estimate of the percentage increase in nursing homes. In several states—particularly those with histories of elevated prison deaths including Alabama, Arkansas, South Carolina, and West Virginia—deaths more than doubled, and many states had high death rates continue into 2021. Though COVID-19 drove the higher death rates, inmates also died of other illnesses, suicide, and violence, according to the data collected by researchers at UCLA Law. The higher death rates were due to a variety of factors, including older inmate populations, many with other known or undiagnosed health problems; crowded and often harsh conditions; inadequate or delayed access to testing and care, for COVID-19 and other conditions; and prison worker understaffing.
CORONAVIRUS VACCINE ROADMAP The Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota this week released the Coronavirus Vaccines Research and Development (R&D) Roadmap (CVR), a strategy to develop broadly protective vaccines that are suitable for use in all world regions. With US$1 million in funding from the Rockefeller Foundation and the Bill & Melinda Gates Foundation, CIDRAP convened 50 international scientists who mapped out a strategy to develop new vaccines. The roadmap—a summary of which was published in the journal Vaccine—covers a 6-year timeframe, is organized into 5 topic areas—virology, immunology, vaccinology, animal and human infection models, and policy and finance—and includes 20 goals and 86 R&D milestones, 22 of which are ranked as high priority. In a separate effort reported on by NPR, the Coalition for Epidemic Preparedness Innovations (CEPI) is funding an initiative to develop a better way of coding mRNA that makes it more stable and does not require the use of ultra-low temperature freezers for storage and transport.
Epi update
As of February 21, the WHO COVID-19 Dashboard reports*:
• 757 million cumulative COVID-19 cases
• 6.85 million deaths
• 1.08 million cases reported week of February 13
• 13% decrease in global weekly incidence
• 8,013 deaths reported week of February 13
• 22% decrease in global weekly mortality
Over the previous week, incidence declined in all WHO regions except the Eastern Mediterranean region (+25%) and Europe (+3.5%).
*Starting this week, the WHO will update the dashboard once per week on Wednesdays.
UNITED STATES
The US CDC is reporting:
• 103 million cumulative cases
• 1.1 million deaths
• 259,339 cases week of February 15 (down from previous week)
• 2,838 deaths week of February 15 (down from previous week)
• 5.7% weekly decrease in new hospital admissions
• 6.7% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (80%), BQ.1.1 (12%), and BQ.1 (4%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by dryrunguy And these are the same fools who freely and carelessly scream words like "freedom"...
Idaho bill would criminalize giving mRNA vaccines – the tech used in popular COVID vaccines
by ti-amie Jonathan-FL
@AmerLiberal@mastodon.social
Former Sen. Jim Inhofe (R-Okla.) attributed his decision to retire due to the long-term effects of COVID-19, telling local newspaper Tulsa World that certain symptoms were still affecting him day-to-day.
by ponchi101 The gig is up.
All the evidence needed to prove that this entire C19 thing was a hoax, planned by Pfizer et al, in order to sell a bogus vaccine, was exposed and we can no longer deny it.
How? When?
Woody Harrelson monologue in SNL. Since SNL is live, the PTB that control the media could not stop him, and he told the entire truth.
Do NOT, repeat, DO NOT be surprised if he has "an accident".
---0---
Some friendships are hard to keep. Next thing that we can expect: this was planned by the The illuminatti. In the late 1800's.
by ti-amie
ponchi101 wrote: ↑Tue Feb 28, 2023 4:53 pm
The gig is up.
All the evidence needed to prove that this entire C19 thing was a hoax, planned by Pfizer et al, in order to sell a bogus vaccine, was exposed and we can no longer deny it.
How? When?
Woody Harrelson monologue in SNL. Since SNL is live, the PTB that control the media could not stop him, and he told the entire truth.
Do NOT, repeat, DO NOT be surprised if he has "an accident".
---0---
Some friendships are hard to keep. Next thing that we can expect: this was planned by the The illuminatti. In the late 1800's.
by ti-amie
This issue of Myocarditis or Pericarditis Events After BNT162b2 vaccine has become a talking point for some because of the recent death of the brother of actor Hayden Panettiere which was reported in his autopsy report as being the result of an enlarged heart. There is no evidence of it being vaccine related but every highly publicized death is, according to these people, related to the vaccine.
by Deuce I've had 5 mRNA COVID-19 vaccines. I just checked my pulse, and can confidently state that I am alive.
Prior to COVID, I avoided vaccines, and medication in general. I didn't even take Aspirins. But COVID has scared me - so I got the 2 primary COVID vaccines, and 3 boosters. I even got my first 'flu vaccine ever this past December.
I keep up to date on the evolving information about the vaccines and about COVID-19 - I only take information from independent, non-government affiliated medical sources, such as independent doctors in the infectious diseases department, and historically trusted sources like the Mayo and Cleveland Clinics.
I wish that none of us had to deal with COVID, of course - it has changed life immeasurably - but it is a fact of life, and I, for one, chose not to pretend that it isn't.
by dryrunguy Here's the latest Situation Report. Haven't read it yet.
::
US Department of Energy concludes with ‘low confidence’ COVID-19 pandemic began as result of lab incident, prompting congressional hearing; experts call for actions to improve biosafety, biosecurity
After assessing new intelligence, the US Department of Energy (DoE) concluded with “low confidence” that the SARS-CoV-2 virus likely emerged from a potential laboratory incident in China, according to a classified intelligence report delivered recently to the White House and key members of the US Congress. The DoE joins the FBI as the only other US intelligence agency to conclude that the COVID-19 pandemic most likely began as the result of a laboratory leak. The FBI arrived at its conclusion with “moderate confidence,” according to FBI Director Christopher Wray. Four other unidentified government agencies and the National Intelligence Council maintain their positions with “low confidence” that the pandemic arose as a result of natural zoonosis. The US CIA and one other unnamed government intelligence agency have yet to arrive at conclusions about the pandemic’s origin. Despite the divide, all agencies currently agree that the virus was not released as an intentional weapon. The new intelligence that led the DoE to change its previous position from undecided remains classified. Some officials briefed on the new intelligence said it is relatively weak, likely leading to the DoE saying its decision was made with “low confidence.” Notably, DoE shared the intelligence with other agencies and none have changed their previous conclusions.
White House National Security Advisor Jake Sullivan this week said there is “no definitive conclusion” on the pandemic’s origin. Many scientists and virologists point to data and what some say is “overwhelming evidence” of a zoonotic origin. Some of these same scientists are curious to learn more about the intelligence information that led the DoE to its conclusion. In the US Congress, reactions to the report have been mixed. Some lawmakers are calling for the declassification of information related to the pandemic’s origin, the establishment of a nonpartisan commission to investigate the virus’s beginnings, and restrictions on data-sharing with Chinese scientists. Others, however, are requesting classified intelligence briefings and warned against too much focus on the past at the expense of current threats. The US House Select Subcommittee on the Coronavirus Pandemic announced it will hold a hearing March 8 focused on investigating the origins of the COVID-19 pandemic. The chairs of the subcommittee and the Committee on Oversight and Accountability this week sent a letter to DoE Secretary Jennifer Granholm requesting the release of certain documents and information related to the pandemic’s origins. Additionally, US Senator John Barrasso, ranking member of the Senate Committee on Energy and Natural Resources (ENR), requested the DoE hold a classified briefing for all members of Congress on the new intelligence that led to its revised conclusion.
Notably, the DoE assessment likely will create more tension for US-China relations already strained by recent events. US Ambassador to China Nicholas Burns this week called on China to be “more honest” about the origins of the pandemic and increase cooperation with the WHO. In response, Chinese Foreign Minister Mao Ning said China has been “open and transparent” in matters related to origin investigations and shared information and data with the international community, including the WHO, in “a timely manner.” Foreign Minister Mao also said the US government is politicizing origin investigations and called for a stop to efforts that she said are “disrupting social solidarity and origins cooperation.”
Several experts say the debate over whether the pandemic arose due to a lab leak or a viral jump from animals to humans detracts from efforts that could help prevent either scenario in the future. Several experts previously have outlined specific steps governments and scientific institutions should take to address uncertainties about the origin of the COVID-19 pandemic. Dr. Caitlin Rivers, an epidemiologist and Senior Scholar at the Johns Hopkins Center for Health Security, this week wrote about the importance of taking actions to strengthen biosafety and biosecurity despite the likelihood that the world will never have a definitive answer on where COVID-19 originated. Such actions could include enhanced oversight of research with high consequence pathogens, better mechanisms for providing proper equipment to laboratories in low-resource settings, and the adoption of a code of conduct for biological scientists. Dr. Katelyn Jetelina, an epidemiologist and science communicator, echoed this sentiment, writing that accidental laboratory leaks, intentional laboratory leaks, and natural spillover events all need to be addressed for a safer future. She also called for more transparency, because without concrete evidence, people are forming narratives based on incomplete or sometimes downright false information, leading to the resurgence of conspiracy theories that have been disproven, as well as the emergence of new, unproven theories.
Most US states with pandemic-related emergency declarations will allow them to expire this month
Three years into the pandemic, the few US states that still have COVID-19 emergency declarations are allowing them to wind down, for the most part, offering symbolic endings to a period marked by pandemic-related challenges and the loss of more than 1.1 million lives to the disease. California’s emergency declaration ended on February 28, although some local emergencies remain in place. One of those localities is Los Angeles County, which is expected to end its COVID-19 emergency on March 31.
According to the National Academy for State Health Policy, 7 other states have ongoing emergency declarations related to public health, disaster recovery, or supply chain issues, but all are set to expire in March unless renewed. The exception is Illinois, which is ending its disaster declaration on May 11 to coincide with the end of the federal emergency. Notably, in Texas, Governor Greg Abbott has continued to extend the state’s emergency declaration to prevent cities from imposing their own restrictions, including mask and vaccine requirements. Governor Abbott has indicated that the state’s emergency declaration will stay in place until the Texas legislature passes laws to prevent local governments from imposing these types of restrictions. The state’s Republican-controlled legislature is currently considering several bills to forbid what the sponsor called “restrictions on our personal liberties.”
US CDC advisory panel supports annual COVID-19 vaccine booster for high-risk populations; Pfizer-BioNTech request EUA for bivalent vaccine as booster for youngest children
There is insufficient evidence to support SARS-CoV-2 vaccine boosters more than once a year for older adults and people with compromised immune systems, the COVID-19 working group of the US CDC's Advisory Committee For Immunization Practices (ACIP) said on February 24. The working group supported an annual COVID-19 vaccine booster, likely in the fall, for high-risk populations, although ACIP advised showing flexibility in booster frequency recommendations, particularly for individuals at risk of severe COVID-19. CDC advisors did not vote on new recommendations, and both the CDC and US FDA continue to explore how best to annually update the vaccines to target circulating variants, in a way similar to annual influenza vaccines.
In February, the CDC added the COVID-19 vaccine to its child and adolescent immunization schedule. The schedule recommends that children between the ages of 6 months and 18 years receive 2 doses of a primary series 4-8 weeks apart and a booster dose at least 8 weeks after the second dose. On March 1, Pfizer-BioNTech requested emergency use authorization for their Omicron-adapted bivalent vaccine as a booster dose for children aged 6 months to 4 years. The bivalent vaccine is already authorized as a third dose of the 3-dose series for this age group, but a new EUA would allow children under age 5 to get a fourth dose using the updated vaccine, at least 2 months after completing their primary series.
Incidence of long COVID could be declining; people with condition more likely to develop cardiac complications, suffer from orthostatic tachycardia
Several recent studies, as well as anecdotal evidence, suggest the incidence of post-acute sequelae of COVID-19 (PASC), commonly known as long COVID, has decreased over time. Nevertheless, there are an enormous number of people who are suffering with lasting symptoms—at least 65 million people worldwide, according to one study. Notably, a recent study published in Preventive Medicine found the prevalence of SARS-CoV-2 infections and incidence of long COVID among US adults during the Omicron BA.4/BA.5 surge was higher than previous estimates that focused primarily on people who were hospitalized or sought medical care, which has key implications on the burden of long COVID.
A study published in Clinical Infectious Diseases earlier this year showed prolonged symptoms of COVID-19 were more common among participants during the beginning of the pandemic, before the Delta and Omicron variants of concern emerged. When the researchers adjusted for vaccination status, the differences were no longer significant, suggesting vaccination, or possibly immunity from prior infection, has a beneficial effect on the risk of long COVID. Two other studies published this week in BMJ Medicine, as well as another published in JAMA Network Open, also support the theory that vaccination reduces case severity and the risk of developing long COVID, although it is not known to what degree and additional studies are needed.
According to a meta-analysis to be presented next week at the American College of Cardiology (ACC)/World Congress of Cardiology Annual Scientific Session, people with long COVID are at more than double the risk of new-onset cardiovascular symptoms than people who were never infected with SARS-CoV-2. The researchers noted that clinicians need to be aware of the association between long COVID and cardiac complications, which some speculate could be caused by chronic inflammation. Another condition that impacts up to 30% of patients with long COVID is postural orthostatic tachycardia syndrome, or POTS, a disorder of the autonomic nervous system that can result in symptoms such as dizziness, fainting, fatigue, and a significant increase in heart rate upon standing or exertion. Few clinicians know how to care for POTS patients, and The BMJ recently published a Practice Pointer on orthostatic tachycardia after COVID-19 to raise awareness.
To help better understand the long-term implications of post-COVID conditions, the US CDC recently expanded its guidelines for certifying deaths to include PASC as the reason for or an underlying cause of death, even if the original SARS-CoV-2 infection occurred months or years prior.
US FDA authorizes first-ever at-home COVID-19, flu test kit
The US FDA on February 24 issued an emergency use authorization (EUA) for the first over-the-counter (OTC) at-home diagnostic test that can differentiate and detect influenza A and B, commonly known as the flu, and SARS-CoV-2, the virus that causes COVID-19. The Lucira COVID-19 & Flu Home Test, a single-use at-home test kit, uses nasal swab samples to provide results in about 30 minutes. Notably, Lucira Health, the California-based test manufacturer, filed bankruptcy on February 22, blaming the FDA’s “protracted” authorization process for its financial troubles. Questions remain about the company’s manufacturing capacity, how much the test will cost, and when such a combined test—from Lucira or other companies—will be widely available to consumers.
What we’re reading
VACCINE RESEARCH PUBLIC INVESTMENTS According to a study published March 1 in BMJ, the US government invested at least US$31.9 billion to develop, produce, and purchase mRNA COVID-19 vaccines, including significant investments made in the 30 years prior to the pandemic. Moderna recently made a US$400 million payment for the rights to a chemical technique that its scientists said they borrowed from government-funded research to make the company’s mRNA-based SARS-CoV-2 vaccine. The payment will be shared among the US NIH and 2 US universities where the method was invented. Moderna and NIH continue to dispute who owns the rights to information that makes up the central component of the vaccine.
PRETERM BIRTHS Across a group of mostly high-income countries—including Belgium, Canada, Chile, Denmark, Switzerland, and the United States—about 4% fewer preterm births than expected occurred in spring 2020, when most of the world was in lockdown at the onset of the COVID-19 pandemic. According to the research, published in Nature Human Behavior, this translates to nearly 50,000 premature births averted globally in the first month of lockdown alone. The finding could help researchers better understand what leads to preterm birth, which is the leading cause of infant mortality worldwide.
SURVEILLANCE TECHNOLOGIES In the beginning of the COVID-19 pandemic, the use of surveillance technologies—such as overhead infrared thermometers and wearable tracking devices—ramped up quickly. These technologies often forced essential workers to change how they worked, sometimes made workplaces less safe, and typically did not offer clear and accurate information to help workers protect their own health, according to a new report by the nonprofit Data & Society. The report assessed the impact of COVID-19 surveillance on the employees—who were mostly Black, Latino, and low-income—of several industries such as meatpacking and food processing, warehousing, grocery retail, and manufacturing.
ASYMPTOMATIC TRANSMISSION Initially, SARS-CoV-2 was thought to spread only from symptomatic infected people, as SARS-CoV did, but was later understood to also transmit from people without symptoms. This covert transmission potential prompted public health officials to encourage widespread mask use, physical distancing, and testing to help prevent the virus’s spread. Now, enthusiasm for these protective measures is waning, partially because people have more immune protection from vaccination and/or prior infection; however, asymptomatic transmission still occurs, leaving questions about how many people experience COVID-19 without becoming symptomatic.
PANDEMIC TREATY In a commentary published in The BMJ, Dr. Alexandra Phelan, Senior Scholar at the Johns Hopkins Center for Health Security, discusses the importance of operationalizing equity through international law surrounding infectious diseases, specifically within a draft pandemic treaty currently under negotiation among WHO member states. Dr. Phelan calls for the “effective participation of all member states, strong civil society engagement, and transparency” in the negotiation processes, as well as the incorporation of legal measures aimed at decolonization and benefit sharing, as all will help prepare the world to better respond to the next disease threat.
Epi update
As of February 28, the WHO COVID-19 Dashboard reports:
• 758 million cumulative COVID-19 cases
• 6.86 million deaths
• 1.02 million cases reported week of February 20
• 13% decrease in global weekly incidence
• 6,958 deaths reported week of February 20
• 13.5% decrease in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in all WHO regions except the South-East Asia (+9.35%).
UNITED STATES
The US CDC is reporting:
• 103 million cumulative cases
• 1.1 million deaths
• 236,131 cases week of February 22 (down from previous week)
• 2,407 deaths week of February 22 (down from previous week)
• 7.5% weekly decrease in new hospital admissions
• 7.3% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (85%), BQ.1.1 (9%), and BQ.1 (3%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by Suliso At the height of the pandemic there were so many opinions and articles proclaiming that this and that will never be the same. Those of us with some life experience recognized that most of it was nonsense. So I was just thinking with a benefit of hindsight what has changed at a society level and is likely to remain so. The only thing I can think off is a rise of remote work and associated technologies which make it feasible. Anything else?
Of course there is also all the mRNA medical technology, but it hasn't yet made any impact beyond covid vaccines and it remains to be seen if it ever will.
by Deuce ^ I think that not much has changed in the lives of those who are pretending either that COVID-19 is no more serious than the 'flu, and/or those who are pretending that COVID-19 is no longer a viable serious threat to health, and are living now as they did pre-pandemic.
For those of us who realize that COVID-19 is still present, and is still a realistic threat, it has changed a lot of elements, and likely for the long term. I, for one, cannot envision entering indoor public spaces or public transit without wearing a mask for the foreseeable future - at least until things with the virus change drastically for the better - and if/when that will occur is largely unpredictable at this point.
How much it has changed things, then, is, in my opinion, directly related to the level of comfortable illusion that individuals adopt.
It has also drastically changed the landscape of providing help to homeless people here - namely because the homeless are generally often not very careful about the state of their health, and are not very disciplined when it comes to mask wearing, physical distancing, washing their hands, and getting vaccinated. As a result, there has been a lot of COVID-19 transmission among the homeless and the people working with them - including hospitalizations and deaths.
As well, homeless shelters typically cram several people together - both for meals and for sleeping. All of that has has to be re-thought.
Also among the long-term changes are that every time a person (in the general population) - and particularly an elderly or otherwise vulnerable loved - one becomes physically ill, there will be anxiety about whether it is COVID-19 or not, and whether it will kill them or not. Much more anxiety than pre-pandemic.
The pandemic has also changed the ways that medical professionals at various levels and hospitals function, as well as homes for the elderly, as the pandemic has all too often exposed the inefficiency of these systems.
Let's also hope that it has radically changed the way that everyone - from governments to the private individual, and every person and entity in between - will react to the next deadly virus/pandemic.
by Suliso I was talking about society level not about individuals. I personally don't wear masks and I rarely see anyone in Switzerland doing that. Therefore I strike that out as a possibility.
I can't really comment about the homeless so perhaps you're right on that.
by dryrunguy
Suliso wrote: ↑Sat Mar 04, 2023 10:09 am
At the height of the pandemic there were so many opinions and articles proclaiming that this and that will never be the same. Those of us with some life experience recognized that most of it was nonsense. So I was just thinking with a benefit of hindsight what has changed at a society level and is likely to remain so. The only thing I can think off is a rise of remote work and associated technologies which make it feasible. Anything else?
Of course there is also all the mRNA medical technology, but it hasn't yet made any impact beyond covid vaccines and it remains to be seen if it ever will.
Three things I can think of, but I'm not quite sure if these are unique to the United States or if, to some degree, they also apply to other wealthy nations that implemented lockdowns.
1) LONG COVID. I'm pretty sure this is not unique to the United States, but it appears the United States is paying more attention to it than many other countries. We are already seeing fairly dramatic increases in the number of people applying for and receiving disability status due to Long COVID. It's very curious, though, that Long COVID appears to be disproportionately associated with older COVID strains rather than the newer strains. I don't think we can attribute that to improved treatments or increased vaccination rates, either, because we have a significant portion of the U.S. population that has never been vaccinated, and they don't seem to be developing Long COVID at the same rates as previous strains. That story is unfinished, though, and will remain so for a long time.
2) MISSING STUDENTS. This story is also unfinished. Chances are many of these missing students in the U.S. were already at high risk for not completing their education. COVID just sped things up a bit in terms of quitting school. But where are they? What are they doing? How are they making money? I have A LOT of questions about that.
3) MENTAL HEALTH. The literature on the impact of COVID on young people's mental health is already fairly robust, and it appears girls are especially negatively affected. Yet again, that story is unfinished.
::
On a more positive note... I can't prove it and am not aware of any data on this. But it SEEMS to me that more people are making a concerted effort to grow more of their own food rather than relying on supply chains that broke down during COVID. But that's just an observation. I can't prove it.
by ponchi101
Suliso wrote: ↑Sat Mar 04, 2023 11:53 am
I was talking about society level not about individuals. I personally don't wear masks and I rarely see anyone in Switzerland doing that. Therefore I strike that out as a possibility.
I can't really comment about the homeless so perhaps you're right on that.
It was TAT1.0 where I wrote that C19 would defeat us in the sense that we would not vanish it and we would "learn" to live with it.
In Colombia, it is like in Switzerland (what you describe). Very few people wearing masks anymore. The people have other problems to deal with (high unemployment and subemployment, inflation, the usual latin America mess).
Remote work here is almost gone. People are expected to go back to work, and people are willing to. Human contact was needed.
So, it seems that there are very few permanent changes. My sister (the shrink) has gone almost back to normal with patients that live in Caracas. They do not want to Skype, they want face to face interaction.
We are a social species. To think that interaction could be cut in 50% was not realistic. Or even desirable for too many.
2) MISSING STUDENTS. This story is also unfinished. Chances are many of these missing students in the U.S. were already at high risk for not completing their education. COVID just sped things up a bit in terms of quitting school. But where are they? What are they doing? How are they making money? I have A LOT of questions about that.
...
::
On a more positive note... I can't prove it and am not aware of any data on this. But it SEEMS to me that more people are making a concerted effort to grow more of their own food rather than relying on supply chains that broke down during COVID. But that's just an observation. I can't prove it.
That phenomenon is probably relegated to the USA. Here in Colombia, where there is no such concept as "home schooling", students are all back in class. The problems about education remain the same, in that there are sectors of the population with little or no access to education. But that was structural before, not something that C19 affected one way or another.
by Suliso 50% would be really bad in my line of work, but I'm certainly enjoying my one day of home office per week. It allows me to sleep an hour more and whenever necessary do extra business in the city (shopping, bank etc). My sister in Latvia still works remotely 70-80% of the time. She's working for an advertising agency.
by Suliso Indeed, I've not heard anything about any missing students in Switzerland or Latvia either.
by ponchi101 And after a bit more thought.
The divide between trust and mistrust of the pharmaceutical industry has never been larger. The believe in "alternative medicines" took a huge boost, with Hydroxychloroquine and Ivermectin showing that people will accept these alternatives prima facie. We are also now clearly divided, once more, on accepting that Big Pharma, for all its faults, is needed, or Big Pharma has to be destroyed to the ground.
If another pandemic starts, having people accepting treatments in accordance to either canon will be harder than ever. Last, public trust on government validated policies will be very low.
We have been divided even more.
by ti-amie
Deuce wrote: ↑Sat Mar 04, 2023 11:35 am
^ I think that not much has changed in the lives of those who are pretending either that COVID-19 is no more serious than the 'flu, and/or those who are pretending that COVID-19 is no longer a viable serious threat to health, and are living now as they did pre-pandemic.
For those of us who realize that COVID-19 is still present, and is still a realistic threat, it has changed a lot of elements, and likely for the long term. I, for one, cannot envision entering indoor public spaces or public transit without wearing a mask for the foreseeable future - at least until things with the virus change drastically for the better - and if/when that will occur is largely unpredictable at this point.
How much it has changed things, then, is, in my opinion, directly related to the level of comfortable illusion that individuals adopt.
It has also drastically changed the landscape of providing help to homeless people here - namely because the homeless are generally often not very careful about the state of their health, and are not very disciplined when it comes to mask wearing, physical distancing, washing their hands, and getting vaccinated. As a result, there has been a lot of COVID-19 transmission among the homeless and the people working with them - including hospitalizations and deaths.
As well, homeless shelters typically cram several people together - both for meals and for sleeping. All of that has has to be re-thought.
Also among the long-term changes are that every time a person (in the general population) - and particularly an elderly or otherwise vulnerable loved - one becomes physically ill, there will be anxiety about whether it is COVID-19 or not, and whether it will kill them or not. Much more anxiety than pre-pandemic.
The pandemic has also changed the ways that medical professionals at various levels and hospitals function, as well as homes for the elderly, as the pandemic has all too often exposed the inefficiency of these systems.
Let's also hope that it has radically changed the way that everyone - from governments to the private individual, and every person and entity in between - will react to the next deadly virus/pandemic.
The pandemic is not over and no amount of wishing it to be will change that.
by Suliso Not medically perhaps, but sociologically and politically it is over.
by Deuce
Suliso wrote: ↑Sun Mar 05, 2023 3:22 am
Not medically perhaps, but sociologically and politically it is over.
^ For the reasons I previously mentioned (comfort and convenience).
Also, I think Djokovic fans would not agree that it's over politically.
by ti-amie Augie Ray
@augieray@mastodon.social
New US CDC report: "Emerging
evidence suggests that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes #COVID19, can have lasting effects on nearly every organ and organ system of the body weeks, months, and potentially years after infection. Documented serious post-COVID-19 conditions include cardiovascular, pulmonary, neurological, renal, endocrine, hematological, and gastrointestinal complications, as well as death." https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.pdf
ti-amie wrote: ↑Sun Mar 05, 2023 8:48 pm
Augie Ray
@augieray@mastodon.social
New US CDC report: "Emerging
evidence suggests that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes #COVID19, can have lasting effects on nearly every organ and organ system of the body weeks, months, and potentially years after infection. Documented serious post-COVID-19 conditions include cardiovascular, pulmonary, neurological, renal, endocrine, hematological, and gastrointestinal complications, as well as death." https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.pdf
@shayz0rz@mastodon.online
@augieray And yet, they’re still recommending we do nothing to avoid this and acting like it’s no big deal.
by dryrunguy Here's the latest Situation Report. It's packed. A few things. The short section near the end on Neanderthal genes is absolutely fascinating. The lying parents part made my head hurt.
And finally, am I the only one who has THOROUGHLY lost interest in the origins of COVID? We'll never know. So why bother? And why invest all of this time and resources on investigations and hearings?
::
US House Select Subcommittee holds hearing on origin theories of SARS-CoV-2; Democrats, Republicans agree further investigation needed
The US House Select Subcommittee on the Coronavirus Pandemic held a hearing March 8 on “Investigating the Origins of COVID-19” to examine theories about the origination of SARS-CoV-2. Many say determining whether the virus emerged in Wuhan, China, because of a laboratory-related incident or natural animal-to-human transmission is important to help inform efforts that could prevent another novel disease and pandemic, while others say that crucial steps to improve the security and safety of labs and to study and track the spread of diseases in nature can be taken now, without knowing the origin of this novel coronavirus. The hearing, which included a panel of scientists, most of whom support a lab leak theory, produced no new evidence and made it clear that uncovering evidence to prove either theory will be difficult. While the hearing involved some political theater, Democrats and Republicans on the committee appeared to agree that both theories are plausible, and that further investigation is needed. How to go about doing that is in question, as several witnesses noted that China has not been forthcoming in offering cooperation in the search for answers.
Dr. Robert Redfield, former director of the US CDC, who suspects the virus emerged due to a lab leak, said he was cut out of early discussions about where the virus came from because of his beliefs and called for a moratorium on gain-of-function research. To be clear, most experts and US officials, including US intelligence agencies, do not believe the virus was intentionally created in or released from a Chinese lab. A panel of the US NIH recently convened experts to discuss boosting oversight of research involving enhanced potential pandemic pathogens (PPPs), but so far the federal government has not moved to ban this type of research entirely. The renewed debate over the origins of COVID-19 comes after the release of assessments by several federal agencies. The House is expected to vote this week on a US Senate-passed bill calling for the declassification of information related to the origins of COVID-19 (more below).
US Intelligence Community discusses health security in Annual Threat Assessment; lawmakers push for declassification of information related to COVID-19 origin investigations
The US Office of the Director of National Intelligence this week released its 2023 Annual Threat Assessment of the US National Intelligence Community (IC), which focuses on the most direct, serious threats to the nation in the next year. In a section on health security (pages 24-25), the report discusses infectious diseases and impacts from the COVID-19 pandemic—including economic, human security, political, and national security implications that will persist over the next year and for years to come—and says the IC continues to investigate whether the novel coronavirus arose due to a laboratory-associated incident or natural exposure to an infected animal. Additionally, the assessment finds countries worldwide remain vulnerable to the emergence or introduction of a novel pathogen that could lead to a new pandemic, briefly outlining drivers for disease emergence. The report also discusses threats related to the development of biological weapons and occurrence of anomalous health incidents.
IC leaders from across the US government appeared before the US Senate Intelligence Committee on March 8 to discuss the threat assessment’s findings. Director of National Intelligence Avril Haines outlined the IC’s various findings regarding the origin of SARS-CoV-2. Several Republican Senators this week sent a letter to Director Haines requesting the independent IC assessments on the pandemic’s origin be delivered to members of US Congress so they can be evaluated “without filters, ambiguity or interpretations of the intelligence.” Last week, the Senate passed a bill by unanimous consent to require the Director of National Intelligence to declassify information related to the origins of COVID-19. The US House is scheduled to vote on the bill on March 10.
Health Affairs studies examine trust in public health agencies, exodus of state, local public health employees
In its March 2023 issue focused on lessons learned regarding public health during the COVID-19 pandemic, the journal Health Affairs includes a study surveying 4,208 US adults to learn their reasons for trust in federal, state, and local public health agencies’ information during the COVID-19 pandemic. Among respondents, 37% said they have a "great deal" of trust in the US CDC's health recommendations, whereas state and local health departments were highly trusted by about one-quarter of respondents. Between 37%-51% of respondents trusted these public health agencies somewhat, and <10% reported no trust at all in the health information provided by these agencies. Respondents who expressed a “great deal” of trust in public health agencies associated those beliefs with agencies’ abilities to make clear, science-based recommendations instead of abilities to control the spread of COVID-19. Scientific expertise was cited more commonly as a reason for a “great deal” of trust in the CDC, whereas state and local agencies garnered more trust due to perceptions of hard work, compassionate policies, and direct services.
Compared with a similar survey conducted in 2021, the Health Affairs study shows the US public’s trust in the CDC has dropped. Respondents’ reduced trust was influenced by their beliefs that health recommendations were politically influenced and inconsistent, concerns about private-sector influence, and dislike of excessive restrictions. To begin to address the public’s concerns, the CDC conducted an internal review of its shortcomings during the COVID-19 pandemic and is undergoing a reorganization, with greater focus on disseminating scientific evidence more rapidly, focusing on health communication, and transitioning into becoming a more response-based agency.
Notably, a 2022 survey found that 90% of adults think public health departments play an important role in creating a healthy community. Nonetheless, another study published in Health Affairs shows that nearly half of all employees of state and local public health agencies left their positions between 2017 and 2021. Among employees aged 35 or younger or those with shorter tenures, the proportion rose to three-quarters. Reasons for the exodus are multifaceted but include low salaries, work overload and burnout, stress, harassment, and lawsuits and legislation that have stripped the public health system of its powers and authority to address health risks. Legislators in more than half of US states have proposed—and, in some cases, successfully passed—bills to curb public health authorities’ power to implement preventive measures such as mask mandates, quarantine or isolation requirements, vaccine mandates, school closures, and more. The study notes that if the separation trend continues, more than 100,000 workers—about half of the total governmental public health workforce—could leave their posts by 2025, causing significant gaps in the nation’s vital public health-related knowledge base and a lack of a pipeline for future public health leaders.
Systematic ethnic inequalities in COVID-19 health outcomes exist, study shows
The COVID-19 pandemic exacerbated existing racial and ethnic inequalities in health. A global meta-analysis of 77 studies involving more than 200 million participants published online March 5 in eClinicalMedicine highlights the ethnic inequalities in COVID-19-related clinical health outcomes. When compared to White majority populations, an increased risk of testing positive for COVID-19 was observed for Black, South Asian, Mixed, and Other ethnic populations. Black and Hispanic ethnic groups and Indigenous populations had an increased risk of hospitalization, with an increased risk of ICU admission among the same groups as well as among South Asian, East Asian, and Mixed ethnic groups. Mortality risk was increased among Hispanic, Mixed, and Indigenous groups. Additionally, the risk for severe disease among hospitalized cases was greater for minority ethnic groups in low- and middle-income countries compared with those in higher-income countries. Prognosis following hospitalization varied among groups, with South Asian, East Asian, Black, and Mixed ethnic groups having an increased risk of ICU admission, and Mixed ethnic groups showing a greater mortality risk. Studies from the US NIH support these findings, showing that Black and Hispanic Americans are more likely than White Americans to have post-COVID conditions, also known as long COVID; experience higher rates of hospital admission; and are more likely to die from COVID-19.
New studies support increased risk of cardiovascular events, symptoms following even mild SARS-CoV-2 infection
Several recent studies have examined cardiovascular risks associated with the COVID-19 pandemic and SARS-CoV-2 infection, which can induce inflammation and blood clotting, further predisposing people to related adverse events. In February 2022, a seminal study published in Nature Medicine showed that people with COVID-19, even mild infections, are at increased risk of incident cardiovascular disease of various types more than 30 days out from acute infection. Since then, other studies have reported similar findings. A study published March 3 in JAMA Health Forum observed that US adults with post-COVID-19 conditions and symptoms were at elevated risk for cardiovascular conditions such as ischemic stroke and blood clots in the lungs 1 year after acute SARS-CoV-2 infection. Another study, presented recently at the American College of Cardiology's Scientific Conference and not-yet peer-reviewed, found that patients who tested positive for COVID-19 had significantly higher rates of chest pain up to 1 year after infection, compared with a control group of matched patients seen for other indications. Though no other increases in cardiovascular events were observed, the study signals that even mild initial COVID-19 infections could be a sign of future cardiovascular complications.
A study in Nature Cardiovascular Research found that there were 90,160 excess cardiovascular deaths, or 4.9% more cardiovascular deaths than expected, between March 2020 to March 2022. Time periods of excess cardiovascular deaths coincided with peaks of COVID-19 deaths, suggesting at least some of the excess deaths may be attributable to disruptions in cardiovascular medical care during the pandemic and patients’ risk-mitigation-related reluctance to seek healthcare. Together, these findings show the need for improved access to healthcare services during health emergencies and greater awareness of the potential for cardiovascular risks posed by even mild SARS-CoV-2 infections.
What we’re reading
TRAVEL RESTRICTIONS US officials are expected to lift COVID-19 testing restrictions on travelers from China as soon as March 10, based on a decline in the number of new cases in the country. Australia’s testing restrictions on travelers from China, Hong Kong, and Macau will end at midnight on March 11. Other countries that imposed similar restrictions, such as Japan, have recently eased testing rules.
MENTAL HEALTH The COVID-19 pandemic has been associated with worsening mental health, for people in the United States and worldwide. The Pew Research Center examines findings from its surveys, as well as those conducted by other organizations, about US residents’ mental health during the pandemic. Noting that concerns about mental health in the US were increasing prior to COVID-19, the piece summarizes findings about mental health among US adults, high school students, younger children, and parents. Another study, published in BMJ this week, reviewed 137 studies and compared general mental health, anxiety symptoms, or depression symptoms assessed during the pandemic with similar data collected between January 2018 and December 2019. The researchers, from McGill University in Canada, found symptom changes were of minimal to small magnitudes and called for more rigorous study into the nuance of mental health.
INDOOR AIR QUALITY The COVID-19 pandemic has shed light on the importance of indoor air quality (IAQ), prompting a focus on efforts to make lasting improvements to the air we breathe, Nature reports. SARS-CoV-2, as well as myriad other viruses that cause chickenpox, measles, tuberculosis, and influenza, are primarily spread in indoor spaces. To address the issue, national governments and US state legislatures have enacted laws and rules to improve ventilation and air quality in indoor spaces. IAQ experts—including a group involving scientists from the Johns Hopkins Center for Health Security that is drafting a Model State Indoor Air Quality Law—are hoping long-term changes can be made to lower the infection risks inside buildings.
US SCHOOL PANDEMIC RELIEF FUNDS US states and school districts have spent less than half of their allotted COVID-19 education relief funds, according to the latest data by the Education Stabilization Fund, and are now working to spend or allocate those funds to close COVID-19-related learning gaps. A January 2023 report estimates that it could take decades to recover from the drastic learning losses due to academic disruption during the pandemic. The Elementary and Secondary Schools Emergency Relief funds must be allocated or spent by September 2024, or be lost. Of educational relief funds that have been spent, federal and state auditors say some have been spent questionably. The US Department of Education’s Office of Inspector General found faulty awards, improper contracts, and double payments in a sampling of US$280 billion in federal pandemic funds. The audits cover at least 9 pandemic-related programs. Thus far, 46 districts and 3 states have been evaluated, with the rest ongoing.
DISHONESTY AMONG PARENTS In a survey including 580 parents of children younger than 18 years living with them, 26% reported "misrepresentation of and nonadherence to COVID-19 recommendations" in at least 1 of 7 COVID-related public health measures pertaining to exposure, quarantine, vaccination and testing, according to a study published this week in JAMA Network Open. Of those who lied, 52.4% said they did so to exercise their parental autonomy, 47.6% said their child did not feel very sick, 44.4% said they did not want to miss a fun event, and 42.9% said they did not want their child to miss school. Other reasons parents listed included that they wanted their child’s life to feel normal; were following advice from a public figure, like a politician or celebrity; or could not miss work or other duties. Of the respondents, who volunteered and were not chosen randomly, 70% identified as women. The researchers said the results suggest better support mechanisms, such as paid sick leave for family illnesses, might help prevent dishonest behavior in the future.
NEANDERTHAL GENES Since the beginning of the pandemic, researchers have been working to better understand why some people appear to be more susceptible to severe COVID-19 than others. A new study from an international group of scientists has identified 4 specific gene variants of Neanderthal origin that strongly modulate the regulation of the CCR1 and CCR5 genes, which are important receptors for chemokines, small proteins within the cytokine family that play significant roles in the activation of immune responses. Cytokine storms—during which the body releases too many cytokines into the blood too quickly, leading to severe immune reactions—are characteristic of severe COVID-19. Additional study is needed into the role of these gene variants and other genetic risks in immune responses to COVID-19.
Epi update
As of March 7, the WHO COVID-19 Dashboard reports:
• 759 million cumulative COVID-19 cases
• 6.87 million deaths
• 999,848 million cases reported week of February 27*
• 7% decrease in global weekly incidence
• 6,021 deaths reported week of February 27
• 24% decrease in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in all WHO regions except the South-East Asia (+28%) and Eastern Mediterranean (+36%) regions.
*Marks first time global reported cases have dropped below 1 million since June 8, 2020
UNITED STATES
The US CDC is reporting:
• 103.5 million cumulative cases
• 1.1 million deaths
• 226,618 cases week of March 1 (down from previous week)
• 2,290 deaths week of March 1 (down from previous week)
• 7.9% weekly decrease in new hospital admissions
• 9.9% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (90%), BQ.1.1 (6.7%), and BQ.1 (2%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ponchi101 I am still interested in knowing where it came from, and how.
Because the Chinese will never cooperate, we won't know if any of the possibilities, from the most farfetched (it was an attempt to genetically manipulate a virus that went terribly wrong) to a more normal one (the virus was discovered and was being studied, and was accidentally released) is the one. But, if we were to know the truth, protocols and procedures could perhaps be revised and improved. If it was the second case I pose, protocols to ensure that when the next such virus is discovered, it will be handled properly, could be in place.
About parents lying. Heck, there is a reason I never had kids. Can't imagine being locked in a house with a hyperactive 9 yo. Who knows in what level of despair these moms were in.
by ti-amie I agree with Ponchi on both of the points he's making and want to add that I think the mental health aspects really need to be studied and disseminated.
As for covid idiocy Savannah Guthrie of NBC has tested positive for Covid three times and when Al Roker, who is severely immunocompromised tried to get out of being in a photograph with her he's the one the idiots went after.
by dryrunguy Just to clarify, I would LIKE to know the origins of COVID for the same reasons you cite, ponchi. But I'm confident we'll NEVER really know because the answer is unknowable.
by ponchi101 Only thing I would add, then, is that NEVER is a very long time.
We may get lucky. I doubt it, but we may.
by Deuce"DISHONESTY AMONG PARENTS In a survey including 580 parents of children younger than 18 years living with them, 26% reported "misrepresentation of and nonadherence to COVID-19 recommendations...""
^ If 26% admitted to it, you can bet that the real number of parents who lied is closer to about 60% (or more).
by Deuce Today is the 3rd anniversary of the COVID-19 virus being declared a pandemic.
It is reported that approximately 7 Million people have died from the virus.
I agree it's true that the majority have stopped believing the science in favour of believing in a comfortable and convenient (and selfish) illusion...
by dryrunguy Here is the latest Situation Report. A question: What do they mean by cosmopolitan Singapore? I've never seen that term before.
::
WHO calls COVID-19 origin investigations scientific, moral imperative; US Congress passes bill calling for declassification of intelligence information
Understanding the origin of COVID-19 by exploring all hypotheses constitutes both a scientific and moral imperative, to help prevent future outbreaks and “for the sake of the millions of people who died and those who live with long COVID,” WHO Director-General Dr. Tedros Adhanom Ghebreyesus said March 11 on Twitter, reiterating that the UN health agency remains committed to finding out how SARS-CoV-2 arose.
The day before, the US House voted unanimously to declassify all US intelligence information on the origins of the coronavirus, as part of US congressional efforts to investigate the pandemic’s origin. The US Senate passed the bill by unanimous consent on March 1. If signed into law by US President Joe Biden, the measure would require the declassification within 90 days of “any and all information relating to potential links between the Wuhan Institute of Virology and the origin of the Coronavirus Disease,” including information regarding research and other activities at the lab, such as whether any researchers fell ill. Biden has not indicated whether he will sign the legislation. If he does not, it will mark his first veto as president. In addition to Congress, 8 US government agencies are investigating the origin of COVID-19, but their findings remain divided and uncertain. Evidence from the scientific community largely supports the theory that SARS-CoV-2 arose from zoonotic transmission from an infected animal to a human.
COVID-19 pandemic exacerbated health workforce shortages, WHO says, calls for health worker migration agreements
At least 55 countries are facing serious healthcare worker (HCW) shortages, an existing situation exacerbated by workers leaving their home nations to seek better paid opportunities in wealthier nations amid the COVID-19 pandemic, the WHO said this week. The WHO health workforce support and safeguards list 2023 includes 8 additional countries since it was last published in 2020. African nations are the worst-hit, with 37 countries on the continent facing shortages of HCWs, threatening their chances of achieving the Sustainable Development Goal (SDG) of universal health care by 2030. The WHO list notes that the 55 countries have: 1) a density of doctors, nurses, and midwives below the global median (ie, 49 per 10 000 population), and 2) a universal health coverage service coverage index below a certain threshold. Though the list does not prohibit international HCW recruitment, it does recommend governments establish health worker migration agreements and implement the WHO Global code of practice on the international recruitment of health personnel (WHO Global Code) to ensure the international movement of health workers is ethically managed, supports those workers’ rights and welfare, and maintains health service delivery objectives.
4 vaccine doses provide protection against severe COVID-19, restore waning immunity; US FDA authorizes bivalent booster for youngest children but mum on spring boosters for individuals at high-risk
Four vaccine doses, including a primary 2-dose series and 2 booster shots, were the most effective way to protect against critical Omicron BA.5 infection, according to a large population-based study from South Korea published in JAMA Network Open. A 4-dose booster regimen was associated with higher protection against critical BA.5 infection, irrespective of a history of SARS-CoV-2 infection, according to the study, which highlights the importance of booster shots. Notably, subsequent boosters appear to restore waning immunity. In another study, published in Nature Communications, a fourth dose of monovalent mRNA vaccine restored strong protection against severe outcomes for at least 3 months after vaccination.
With these and other supportive findings, many countries, including the US, are looking to the future of vaccine schedules. The UK and Canadian governments plan to offer additional booster shots to people at high risk of severe COVID-19 this spring. In the US, the FDA has remained silent on the issue of spring boosters for those most at risk, creating frustration among a small number of people who do not want to wait until the fall to receive their next dose. Notably, only 16.3% of the total US population has received an updated bivalent booster. This week, the FDA amended the emergency use authorization (EUA) of the Pfizer-BioNTech bivalent COVID-19 vaccine to allow for a single booster dose of the vaccine in children aged 6 months through 4 years, to be administered at least 2 months after completion of the primary 3-dose series of the companies’ monovalent vaccine. So far, no US resident has had to pay for a COVID-19 vaccine dose, but that could soon change. Experts are concerned that if people have to pay an expected US$110-$130 per shot, they will forego the jabs that, based on ongoing research, continue to provide significant protection from serious COVID-19 disease.
US maternal mortality climbed significantly during pandemic, with communities of color more dramatically impacted
The rate at which people in the US died of medical conditions caused or aggravated by pregnancy increased from 23.8 deaths per 100,000 live births in 2020 to 32.9 deaths per 100,000 live births in 2021, with the burden of death disproportionately borne by communities of color, according to a report published today by the US CDC National Center for Health Statistics. In 2021, 1,205 women died of maternal causes in the United States compared with 861 in 2020 and 754 in 2019. These numbers represent an overall 40% increase compared to 2020, which itself had a 60% increase compared with 2019. Racial and ethnic disparities were particularly stark, with Black women experiencing 69.9 maternal deaths out of 100,000 births, compared to 26.6 maternal deaths per 100,000 births among White women. The US maternal mortality rate—the highest among high-income nations—increased for the third year in a row and the increases were significant in all race and Hispanic-origin groups and all age groups.
Though the report does not mention the pandemic, experts highlighted the likely role COVID-19 played in worsening the number of maternal deaths. They said there is a clear need to understand what factors, both social and biological, impacted the health of pregnant women during COVID-19. Additionally, scientists attribute some maternal stressors to the contextual factors of living through a tumultuous worldwide event, such as disrupting income or experiencing grief from deaths. Notably, social determinants of health are already an identified factor in the likelihood of having a preterm birth. Strong and lasting changes are needed to prevent these outcomes in future pandemic and non-pandemic scenarios and must be applied through an equity-focused lens in order to best serve expectant women.
Studies, articles show pandemic’s negative impacts on health and wellbeing of children, adolescents
Several new articles and studies highlight the severe, adverse impacts of the pandemic on the health and wellbeing of children and adolescents in the United States and around the world, as well as associated factors:
• A survey on adolescent mental health and substance use in Iceland documented increased depressive symptoms and worsened mental wellbeing for the first 2 years of the pandemic, as well as a decrease in alcohol intoxication that reversed after the easing of social restrictions. Parental social support and average sleep duration of 8 hours or more were significantly associated with better mental health outcomes and lessened substance use among adolescents.
• A survey of adolescents in cosmopolitan Singapore examining resilience during the pandemic noted that approximately half of the participants had normal resilience scores, while about one-third had low scores, according to the Brief Resilience Scale (59.6%/32.7%) and Hardy-Gill Resilience Scale (49.0%/29.0%). Chinese ethnicity, low socioeconomic status, and lower coping abilities related to school life, staying home, sports, and friends were associated with lower resilience scores.
• A Kaiser Health News article highlighted various studies showing how the effects of the pandemic and other recent events have heightened the gun violence crisis affecting children and adolescents. This is further echoed in a JAMA viewpoint published this week describing increases in pediatric all-cause mortality. Between 2019 and 2020, pediatric all-cause mortality increased 10.7% and increased an additional 8.3% between 2020 and 2021, with injuries (particularly from gun violence) and COVID-19 as the major culprits.
• A JAMA Network Open study noted that family financial disruptions were associated with a 205.2% [95% CI, 52.9%-509.0%] increase in perceived stress, 112.1% [95% CI, 22.2%-268.1%] increase in sadness, 32.9% [95% CI, 3.5%-53.4%] decrease in positive affect, and a 73.9 [95% CI, 13.2-134.7] percentage-point increase in COVID-19–related worry among a sample of 6,030 US children in late 2020. There was no association between in-person schooling disruption and mental health.
US FDA briefing document supports Paxlovid use in high-risk COVID-19 patients ahead of expert meeting to discuss full approval
A US FDA briefing document prepared by the Antimicrobial Drugs Advisory Committee and released this week addresses the question of whether or not Paxlovid is associated with COVID-19 rebound, a phenomenon wherein patients test positive or symptoms recur after initial recovery. The briefing document is meant to inform a panel of experts meeting today to determine whether to recommend Paxlovid for full approval for mild-to-moderate COVID-19 in adults at high risk of hospitalization or death. Since it received emergency use authorization (EUA) in 2021, more than 8 million people in the US have taken Paxlovid, which consists of a 5-day course of nirmatrelvir and ritonavir for COVID-19 treatment that has shown to reduce the chances of hospitalization, death, and experiencing long COVID.
The briefing concluded that Phase 2 and 3 clinical trials conducted by the drug’s manufacturer, Pfizer, support that Paxlovid’s benefits outweigh its risks. The document also acknowledged the COVID-19 rebound phenomena but concluded that rebound is likely a natural course of COVID-19 and likely not significantly associated with Paxlovid treatment. Notably, an ongoing clinical trial may indicate if re-treatment would aid patients who experience COVID-19 rebound, and another ongoing trial is investigating optimal treatment duration in immunocompromised patients. Data indicate that COVID-19 rebound rates range from 10-16% across patients, with no significant difference based on infection with either the Omicron or Delta variant. The FDA’s review of whether or not Paxlovid should receive full approval is expected to be completed in May this year.
by ponchi101 Let me set my watch for when my friend N will send me the tweet with praise for this.
by ti-amie
by ti-amie
by ti-amie AnthropoceneMan
@Anthro@universeodon.com
The guy who snuck me into the cattle call at our convention center for the first #Covid vaccine came back from a conference last week with…Covid.
That makes son’s friend, several students in wife’s class, and others around me that have fallen prey recently.
There is a wave of Covid that is happening in Oregon that is not showing up in the official stats.
#CovidIsNotOver
Mar 20, 2023, 13:28 · · havenkt@artisan.chat
Kristen, digital version
@havenkt@artisan.chat
@Anthro I have a feeling the official stats are not including home testing results, so the numbers we're seeing are artificially low.
by Deuce The PBS 'American Masters' series this week focussed on Dr. Anthony Fauci.
I found it to be extremely interesting.
About 80% of it deals with his work on COVID-19, and the other 20% is about his work with AIDS beginning in the 1980s.
Here is the link to watch it. I don't know if it's available to watch online yet - if not, it very likely will be soon.
You can also check your local PBS TV listings for it this week. It really is worth the watch...
New analysis appears to link SARS-CoV-2 origin to raccoon dogs in Wuhan market, raises questions about completeness of data shared by China; US law requires declassification of intelligence information
More than 3 years into the COVID-19 pandemic, the origin of the SARS-CoV-2 virus remains a hotly contested topic. In the absence of a “smoking gun,” it is unclear exactly how the virus first infected humans, and it may never be definitively determined whether the virus evolved naturally among animals or escaped a laboratory setting. Investigations into the emergence of SARS-CoV-2 have been hindered by insufficient access to facilities, personnel, specimens, and data in China, and intense political divisions—in the US and elsewhere—have made public debate over the available evidence difficult.
Recent revelations regarding early genetic data from specimens collected at the Huanan Seafood Wholesale Market in Wuhan, China, in early 2020 provide additional support for theories that the pandemic emerged as a result of natural zoonotic transmission. Dr. Florence Débarre, a researcher from France, recently identified a previously undisclosed trove of genetic data published on the GISAID platform. Among the viral genetic data, she identified DNA from multiple mammal species, including raccoon dogs, which are known to be susceptible to coronaviruses. The presence of raccoon dog DNA among the viral sequences indicates that these animals were present at the market and may have been infected with the SARS-CoV-2 virus. Notably, the Chinese government previously asserted that these types of animals were not present at the market. Reportedly, after Dr. Débarre reached out to Dr. George Gao, former Director of the China CDC, to collaborate on further research, the data were removed from GISAID “at the request of the submitter.” Following a briefing by Dr. Débarre’s team last week, WHO Director-General Dr. Tedros Adhanom Ghebreyesus chastised China for withholding the data and called on the Chinese government to share all of the available data immediately. The researchers published their findings (preprint) on March 20. While the new data still do not provide definitive proof, they demonstrate that the Chinese government has more data available than what it has shared.
Following unanimous approvals in both houses of the US Congress, President Joe Biden signed a bill requiring US intelligence agencies to declassify all information related to investigations on the origin of SARS-CoV-2 and the Wuhan Institute of Virology in China. To date, various public reports from the US intelligence community indicate that agencies have reached different conclusions regarding the likely origin of the pandemic. Following the release of its report that concluded—albeit with “low confidence”—that a laboratory incident was the most likely origin, the US Department of Energy briefed the Senate Energy and Natural Resources Committee on March 16 about classified information underpinning that analysis.
End of US public health emergency to impact various healthcare programs, rules; US House Republicans eye canceling unspent COVID-19 aid to help rein in federal spending
The WHO said this week that its experts are confident that the public health emergency of international concern (PHEIC) declaration for COVID-19 will be able to be declared over by the end of this year. Similarly, the Biden administration previously announced an end to the US public health emergency for COVID-19 in May, and this week said it will disband its White House COVID-19 Response Team at the same time. The end of the public health emergency will bring with it changes to healthcare access and benefits for many residents nationwide. Millions will lose healthcare coverage with the end of continuous Medicaid enrollment, a change likely to disproportionately impact Black and Hispanic adults, according to a recent Commonwealth Fund report. Additionally, training rules for nursing home staff will become stricter; rollbacks of broader access to certain controlled substances threaten treatment for people recovering from addiction; hospitals and other care facilities will have to comply with stricter capacity and staffing rules; and federal COVID-19 surveillance reporting requirements for states will end.
Additionally, Republicans in the US House are targeting unspent COVID-19 relief money in a plan to cut federal spending. Though a small amount—less than US$80 billion unspent as of January out of the total US$5.2 trillion relief aid allocated—canceling the funds would have huge repercussions for union pension funds, healthcare for veterans, COVID-19 research efforts, and aid for small businesses and transportation systems.
US Senate HELP Committee hears testimony from Moderna CEO about expected commercial market price increase for vaccine
In early 2023, reports emerged publicly that Moderna planned to increase the price of its SARS-CoV-2 vaccine, quadrupling it from between US$15–$26.36 to US$110–$130 per dose, when it shifts its sales to the commercial market later this year. The end of the COVID-19 public health emergency in May will shift the burden of purchasing vaccines to the private sector. Moderna earned about US$40 billion from sales of its COVID-19 vaccines alone over the past 2 years. On March 22, Moderna CEO Stéphane Bancel testified regarding those plans before the US Senate Committee on Health, Education, Labor and Pensions (HELP Committee). Mr. Bancel argued that, while Moderna received considerable funding from the federal government—on the order of US$12 billion for research, development, and procurement—the company will need to implement new production and logistics as the pandemic enters an endemic phase. The combination of new manufacturing processes, storage, wastage, and significantly lower demand necessitates higher costs per dose, he said. Some Senators on the committee argued in favor of Moderna, noting that the success of Moderna’s vaccine illustrates the benefits of capitalism. While the purchase cost of the vaccine is expected to increase, Moderna has committed to ensuring the vaccines remain fully covered by health insurance. Patient assistance programs also will help uninsured or underinsured individuals access the vaccines, but some Senators noted that the paperwork for these programs can be difficult to navigate. Pfizer and BioNTech also plan to increase the cost of their SARS-CoV-2 vaccine to US$110–$130 per dose, but the companies did not use US government funding in developing the shot.
US FDA expected to soon decide on authorization of additional bivalent booster dose; Canada, UK move forward with shots for some individuals
The US FDA is discussing the possibility of authorizing a second round of vaccine boosters targeting the Omicron variant for certain people at high risk of severe COVID-19 illness. The agency is expected to decide within a few weeks, according to people familiar with the deliberations. The bivalent booster is currently recommended for anyone aged 6 months and older after completion of any FDA-approved or FDA-authorized primary series or previously received monovalent booster dose(s), with an exception for the youngest children who received the bivalent vaccine as the last dose in their 3-dose primary series.
While only 16.4% of the total US population has received the updated booster, a small percentage of people are anxiously wondering when they can get another shot. People aged 65 and older are contributing a larger proportion of COVID-19-related deaths over time, particularly those who have underlying health conditions. Additionally, though people who are immunocompromised make up about 3% of the US population, they account for 25% of people hospitalized with COVID-19. For both of these populations, vaccine effectiveness against hospitalization and symptomatic infection begins to drop significantly 2–4 months following their last booster. Canada and the United Kingdom are offering the bivalent booster to older adults, residents of care homes and other senior living settings, and certain people who are immunocompromised. We should know soon whether the US will authorize boosters for similar groups.
What we’re reading
CHILDREN & FAMILIES The COVID-19 pandemic had an unprecedented impact on the lives of children and their families in the United States, and greater focus and investment are needed to address the critical social, emotional, behavioral, educational, mental, physical, and economic health and well-being challenges that the pandemic caused or exacerbated, especially among families identifying as Black, Latino, and Native American, and those with low incomes, that have disproportionately borne the stress of these negative effects, according to a report published March 16 by the National Academies of Sciences, Engineering and Medicine. The report makes several recommendations for federal- and state-level legislatures and agencies to address the short- and long-term effects on children and families and to prepare for the next pandemic.
PAXLOVID A panel of expert advisors to the US FDA voted 16-1 last week to endorse the antiviral Paxlovid (nirmatrelvir-ritonavir) as a treatment for adults with COVID-19 who are at high risk for progression to severe illness. Notably, the committee highlighted potentially harmful drug interactions. Experts later said there is not enough data to determine exactly who would benefit most from the drug and a poor understanding of the treatment among the medical community, hindering its prescription. According to a recently released analysis, Paxlovid use could “lead to 1,500 lives saved and 13,000 hospitalizations averted each week in the United States,” based on COVID-19 data from January 2023. Another study, published March 17 in JAMA Health Forum, modeled population-level impacts of a Paxlovid rollout during a surge like the 2022 winter Omicron wave. The panel’s endorsement likely will lead to full approval of the drug by FDA, although the agency is not required to follow the advice of its advisory committees. A final decision is expected in May. In related news, a study by the Yale School of Medicine is testing whether a 15-day course of Paxlovid can improve the health of people with long COVID.
PANDEMIC-RELATED STATE LAWS, LEGISLATION & REGULATIONS On March 17, KHN published 2 articles examining various state-level legislative actions or laws with pandemic-related roots. One article discusses legislation and proposed regulations in more than a dozen states aimed at controlling healthcare staffing agency wage rates for temporary workers during health emergencies, as well as steps hospitals and health facilities are taking to retain their workers with the acute challenges of the pandemic now in the past. Another article examines how California’s COVID-19 misinformation law, which is meant to discipline doctors who provide false information about COVID-19 patients, is mired in legal limbo after 2 federal judges issued conflicting rulings in recent lawsuits.
CHINA China this week authorized a domestically produced mRNA vaccine against COVID-19, after showing reluctance to use similar vaccines produced in the US and European nations. According to CSPC Pharmaceutical Group Ltd., which makes the vaccine, known as SYS6006, a large clinical trial showed the vaccine is safe and effective against several Omicron subvariants. The WHO urged CSPC to share its full data so the health agency can assess the vaccine for use on the international market. China’s other homegrown vaccines, which use more traditional platforms, proved less effective against newer Omicron variants. According to a report from the Associated Press, China’s sudden scrapping of its strict “zero COVID” policy in late 2022 went against the advice of experts and led to hundreds of thousands of COVID-19-related deaths, some of which could have been avoided with better vaccination coverage and more prepared healthcare facilities.
EQUITABLE VACCINE DISTRIBUTION Equitable worldwide distribution of COVID-19 vaccines would increase global economic benefits by about US$950 billion per year by improving health gains, helping to ease lockdowns, and supporting supply chain recovery, when compared with a scenario focused on vaccinating the entire populations of vaccine-producing countries first then distributing vaccines to other nations, according to an analysis published this week in Nature Communications. The researchers propose a benefit-sharing mechanism that allows all stakeholders to benefit and provides a model to analyze distribution strategies in different infectious and socioeconomic contexts. They note that the need for equitable vaccine distribution is one of the most important lessons to be learned from COVID-19, though global collaboration continues to present a challenge. Notably, wealthy nations already appear to be repeating their COVID-19-era vaccine hoarding tendencies with avian influenza vaccines.
UN CLIMATE REPORT A report released this week by the UN Intergovernmental Panel on Climate Change (IPCC) warned that the world is likely to fail at meeting its most ambitious climate target—limiting warming to 1.5 degree Celsius (2.7 degrees Fahrenheit) above preindustrial temperatures—by the early 2030s. This change could bring about catastrophic damage to the Earth, causing climate disasters and other impacts—such as heat waves, famines, and infectious disease outbreaks—so extreme that humans will have difficulty adapting. The authors said humanity has reached a “critical moment in history” and needs to accelerate actions to achieve its climate goals.
Epi update
As of March 21, the WHO COVID-19 Dashboard reports:
• 761 million cumulative COVID-19 cases
• 6.88 million deaths
• 734,302 million cases reported week of March 13
• 18% decrease in global weekly incidence
• 4,897 deaths reported week of March 13
• 22% decrease in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in all WHO regions except the South-East Asia (+57%) and Eastern Mediterranean (+47%) regions.
UNITED STATES
The US CDC is reporting:
• 103.8 million cumulative cases
• 1.12 million deaths
• 149,955 cases week of March 15 (down from previous week)
• 1,706 deaths week of March 15 (down from previous week)
• This is the lowest weekly mortality since March 2020
• 7.8% weekly decrease in new hospital admissions
• 12.1% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (90.2%), BQ.1.1 (3.5%), XBB (2.5%), and XBB.1.5.1 (2.2%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ponchi101
dryrunguy wrote: ↑Thu Mar 23, 2023 5:31 pm
UN CLIMATE REPORT A report released this week by the UN Intergovernmental Panel on Climate Change (IPCC) warned that the world is likely to fail at meeting its most ambitious climate target—limiting warming to 1.5 degree Celsius (2.7 degrees Fahrenheit) above preindustrial temperatures—by the early 2030s. This change could bring about catastrophic damage to the Earth, causing climate disasters and other impacts—such as heat waves, famines, and infectious disease outbreaks—so extreme that humans will have difficulty adapting. The authors said humanity has reached a “critical moment in history” and needs to accelerate actions to achieve its climate goals.
Meanwhile, in Colombia.
NO new exploration permits will be issued to any new oil and gas projects. But.
No plan to encourage solar or wind has been seen.
No plan to construct or invest in an electric train system, for transport of goods, is in place.
No plan to build or assemble electric vehicle in the country is in place.
All O&G needs for the country must therefore be imported (Colombia is not O&G self sufficient) meaning that transport of such needs is an energy expenditure, leading to more CC gases being released.
One thing is to be oblivious to CC. Another is to be stupid. Here I live.
by dryrunguy Here's the latest Situation Report.
::
White House disbanding COVID-19 Response Team as end of pandemic emergency nears; No movement seen on establishing new preparedness and response office
The White House is disbanding the COVID-19 Response Team that led the federal response to the pandemic since February 2020. The move makes sense, according to officials, as the nation prepares to wind down the COVID-19 national emergency and public health emergency on May 11. The end to those declarations could come even sooner, however, as the US Senate last week voted to end the national emergency order that was first implemented during the Trump administration. The US House of Representatives passed the measure in February, and US President Joe Biden said he will sign it despite his opposition. Meanwhile, the US Congress in December 2022 asked the White House to stand up a new, permanent office to coordinate the government’s preparedness activities before the next pandemic threat, but there has been little movement to do so. With only a month, or less, remaining before the pandemic emergency ends—which has implications for millions of US residents—it appears the political will to create a new pandemic preparedness and response office already is dwindling, perpetuating the cycle of “panic and neglect” so often experienced in health emergencies.
US FDA expected to announce authorization of second bivalent booster for certain people; UK, Canada move forward with spring shots for high-risk populations
The US FDA is expected to announce authorization of a second bivalent booster for certain high-risk groups within the next few weeks. The second Omicron-specific booster—with the same formulation as the first—likely will be authorized for individuals aged 65 years and older or with those with weakened immune systems, to be given at least 4 months or 2 months, respectively, after the first bivalent booster. According to officials familiar with the plan, the new policy will be “permissive,” allowing people to choose to get the shot rather than standing as a formal recommendation. About 42% of people aged 65 and older have received the bivalent booster shot, according to the US CDC.
Once the FDA makes a final decision, the CDC will have to recommend use of the second booster, but it is unclear whether the agency will convene a meeting of its vaccine advisory committee. A reformulated booster is anticipated for summer or early fall rollout to align with a proposed plan made in January by the FDA's Vaccines and Related Biological Products Advisory Committee (VRBPAC) to switch to annual COVID-19 boosters for the majority of people. Data from CDC’s vaccine advisory committee February meeting confirms earlier real-world reports that bivalent vaccines provide better protection against serious illness in adults than monovalent boosters. While data collection is ongoing, studies show that an additional booster may be particularly beneficial to older adults, but experts note that boosters likely will need to be updated to keep up with emerging variants, to maintain immunity levels as the virus evolves.
Last month, health officials in the UK and Canada recommended additional boosters this spring for the elderly, residents of nursing homes, or immunocompromised people. Today, the UK Joint Committee on Vaccination and Immunisation (JCVI) said children between the ages of 6 months to 4 years with underlying medical conditions be offered 2 doses of the Pfizer-BioNTech vaccine, with an interval of 8 to 12 weeks between the first and second doses. UK health regulators authorized the vaccine for children in that age group in December 2022, but the JCVI did not advise vaccination of children of that age who are not in a clinical risk group. On April 5, the European Centre for Disease Prevention and Control (ECDC) released guidance calling on countries in the region to plan for continued rollout of COVID-19 vaccines in 2023, with efforts focused on protecting older adults and other vulnerable groups, such as those with underlying comorbidities and the immunocompromised, irrespective of age.
WHO monitoring XBB.1.16 Omicron subvariant driving surge of cases in India
The WHO is monitoring a new SARS-CoV-2 Omicron subvariant called XBB.1.16, which is driving a surge of cases in India. Dr. Maria Van Kerkhove, WHO's COVID-19 technical lead, said the subvariant has replaced other variants in India and noted it is “one to watch.” The WHO added XBB.1.16 to its list of monitored variants on March 22. XBB.1.16—which is a recombinant variant from BA.2.10.1 and BA.2.75—is similar to the XBB.1.5 variant that is currently dominant in the US and accounts for 45% of global cases, but additional mutations in the spike protein may give it some growth advantages over the older subvariant. The mutations have the potential for increased infectivity and potential increased pathogenicity, although reports do not indicate a rise in hospitalizations, ICU admissions, or deaths due to XBB.1.16, the WHO noted.
So far, there are about 800 sequences of XBB.1.16 from 22 countries, primarily India, which is reporting its highest number of COVID-19 cases in 6 months. In its weekly situation report, the WHO noted that while overall COVID-19 cases and deaths continue to decline, several other countries in the Eastern Mediterranean and South-East Asia regions—which comprises India—are reporting significant increases in cases, including Iran, Kuwait, Libya, United Arab Emirates, and Qatar. In the US, the 7-day average for new daily cases continues to decline to around 20,000, down 9.2% compared to the previous 7-day average. XBB.1.5 has reached saturation, accounting for 87.9% of samples, while 3 other Omicron subvariants show positive growth: XBB.1.9.1, XBB, and XBB.1.5.1. The XBB.1.16 subvariant has been detected in at least 18 US states, and a descendant of the new subvariant that is raising concern among experts, XBB.1.16.1, has been found in 15 states.
Though many people are weary of the pandemic, health experts note it is important to remain vigilant, as past experience with variants shows that things can change quickly. In the US, XBB.1.5 accounted for less than a quarter of COVID-19 cases in late December 2022, but it became the dominant variant over the ensuing week. In the US, XBB.1.16 has shown a 188% growth advantage over XBB.1.5 in the past 3 months, and a 64% growth advantage in India. While the WHO is closely monitoring this new subvariant, as well as several others, it said maintaining and developing surveillance systems to track known variants and detect emerging strains is critical to healthcare system and response agility. Additionally, the WHO urged people to continue taking precautions against COVID-19, including vaccination, social distancing, and wearing masks.
Nature publishes first peer-reviewed data on SARS-CoV-2 origin from Chinese scientists
The journal Nature this week posted a peer-reviewed but unedited study from Chinese scientists examining the results of surveillance samples taken from the Huanan Seafood Market in Wuhan, China, in January 2020, once again reigniting the debate surrounding the origin of SARS-CoV-2. The study examined 923 environmental swabs taken from locations around the market and 457 swabs collected from 18 animal species. The animal swabs were taken from fish tanks, stray animals, and unsold refrigerator and freezer contents. Sample analysis through RT-PCR detected SARS-CoV-2 in 73 environmental samples, but no evidence of SARS-CoV-2 was detected in the animal samples. Three live viruses were isolated from the SARS-CoV-2-positive samples, and the viruses shared a 99.99-100% nucleotide identity with the wild-type virus isolated from humans.
The first version of the article was originally posted to a preprint server in February 2022 and downplayed the possibility of animal infections at the market. But recently, Dr. Florence Débarre, a researcher from France, identified a previously undisclosed trove of genetic data published on the GISAID platform. A group of international researchers led by Dr. Débarre released their own analysis of the data on the preprint server Zenodo, which identified DNA from multiple mammal species, including raccoon dogs, which are known to be susceptible to coronaviruses. The presence of raccoon dog DNA among the viral sequences indicates that these animals were present at the market and may have been infected with the SARS-CoV-2 virus, but the preprint did not provide definitive data to support their infection. Notably, the Chinese government previously asserted that these types of animals were not present at the market. However, in the recently published Nature article, the Chinese scientists confirm the presence of raccoon dogs in the Huanan Market, but the authors stress the remaining uncertainty surrounding the virus’s origins. The authors state that the virus could have been transmitted from humans to raccoon dogs in the Huanan Market or that the virus could have been imported on cold-chain products such as frozen foods.
The release of the Nature publication and the Zenodo preprint analysis has led to varied reactions from the international community. Dr. Alice Hughes, a conservation biologist with the University of Hong Kong, questioned whether the Nature data could have been improperly processed or contaminated, particularly because the Chinese research team found genetic traces from animals such as pandas and chimpanzees, which would not have been in the market. Similarly, Dr. Angela Rasmussen of the University of Saskatchewan said the Nature study is “deeply flawed” because the Chinese researchers used a reference database that excluded the genome of the raccoon dog for sequencing. Meanwhile, authorities in China continue to promote the cold-chain import theory. The WHO has called on China to immediately share all relevant data with the international scientific community.
While the origin of SARS-CoV-2 is unlikely to be definitively proven at this point, scientific evidence points to a natural origin. Full transparency within the scientific community is necessary for the mystery surrounding the virus’s origin to be resolved. Nonetheless, work can begin now to put measures in place to help lower the likelihood of future viral events, including improving standards and guidance for animal markets to lower the risk of disease transmission between humans and animals and enhancing international biosafety and biosecurity standards at laboratories globally.
Researchers, patient advocates call on US government to more effectively respond to long COVID, urge global consensus on definition of condition
Long COVID, also called post-COVID condition (PCC) or post-acute sequelae of SARS-COV-2/COVID (PASC), is a multifaceted and often disabling condition that can affect the neurologic, cardiovascular, pulmonary, hematologic, and endocrine systems of people of all ages, including children. As many as 23 million US adults and 65 million people worldwide have developed long COVID, which involves a variety of symptoms lasting more than 3 months after initial COVID-19 infection. This week, the US Department of Health and Human Services (HHS) marked 1 year of its whole-of-government response to long COVID with a press release outlining its progress and actions moving forward. As part of the initial federal response to long COVID, the US NIH is working with Palantir Technologies Inc. to build an enormous, collaborative database of deidentified data collected from people with COVID-19 or related conditions and launched the Researching COVID-19 to Enhance Recovery (RECOVER) Initiative, which selected a network of enrollment sites or hubs across 24 states, Puerto Rico, and the District of Columbia, with each site collecting clinical and biobank data from about 1,000 participants.
Over months of collaboration, the RECOVER principal investigators (PIs) say they have identified gaps in the response to care for patients with long COVID and developed strategies to address those gaps, and this week they called on the federal government to evolve its response. To do so, the PIs are urging the US Congress to include US$37.5 million in Fiscal Year 2024 funding for the Department of Health and Human Services (HHS) to competitively select Long COVID Centers of Excellence that could gather, develop, and disseminate data regarding evidence-based treatment; educate and train providers on best practices; conduct outreach to affected populations and community organizations; and coordinate access to care, with the aim of coordinating long COVID care, reducing healthcare disparities, and improving psychosocial and medical outcomes. Other experts are calling for the federal government to support an “Operation Warp Speed” for long COVID like it did to develop vaccines, therapeutics, and diagnostics for COVID-19. Such a program could help define, diagnose, treat, and classify the condition, as well as help improve the understanding of risk factors or the protective effect of vaccines or other therapies.
Additionally, advocates for and patients with long COVID are calling on the US NIH to reconsider plans to include exercise trials in its RECOVER initiative to find treatments for the condition. A large proportion of people with long COVID report experiencing post-exertional malaise (PEM), which can cause a worsening of symptoms such as fatigue, poor body temperature regulation, and cognitive dysfunction after even light exercise. Advocates fear that some trial participants could be harmed if they are not properly informed of the risks or the trials do not include adequate screening or post-exercise monitoring. Through a petition and letters, they also are asking researchers to share their rationale and trial protocols so potential risks can be assessed. Trial protocols for the RECOVER initiative are still under development, and a statement sent to Nature on behalf of NIH said patient representatives are included in that process.
Separately, in a commentary published in JAMA Network Open on April 5, experts argue that if the condition is universally defined, more effective treatments for it can then be developed. They say working toward this consistency can be accomplished in 3 parts: agreeing on a universal definition of this condition, with 1 name that can be adopted by all studies in the future; characterizing those who may be experiencing PCC unknowingly in studies, particularly among those who are at highest risk of exposure and severe disease; and conducting longitudinal research to collect data on symptoms and different outcomes over time. In an accompanying JAMA Network Open research letter, researchers aimed to describe how post-COVID-19 condition has been defined to date in studies on this topic.
What we’re reading
GLOBAL HEALTH WORKFORCE On the occasion of its 75th anniversary this week, the WHO called for global action to address health inequities and protect the health workforce, many of whom are facing burnout from the COVID-19 pandemic. Millions of health and other care workers were infected during the pandemic, thousands died, and many suffer from anxiety, depression, and other declines in mental health wellbeing. The agency urged governments to invest in education, skills-building, and decent jobs to meet the rapidly growing demand for healthcare and avert a projected shortage of 10 million health workers by 2030, particularly in low- and middle-income countries. The agency stressed the importance of upholding labor rights; investing in decent working conditions, fair pay, training, and leadership; and addressing gender inequalities in the health sector. Additionally, the WHO, in conjunction with the World Health Professions Alliance, recently published a report comparing the experiences of dentists, nurses, pharmacists, physicians, and physiotherapists during the COVID-19 pandemic and summarizing those 5 professions were impacted in common and different ways.
US PUBLIC SCHOOLS The COVID-19 pandemic affected all US schools in profound ways, but in a system where inequities existed prior to the national health emergency, those that were already the most vulnerable suffered the deepest and most lasting impacts. The Washington Post examines the experiences of 2 Alabama school districts that diverge on socioeconomic status, and the New York Times Magazine highlights the experiences of teachers, parents, and students in one Los Angeles County public school in a neighborhood that suffered immense stress and grief. In one fifth grade class alone, 17 of the students had a loved one die during the first year of the pandemic.
VILOBELIMAB EUA The US FDA issued an emergency use authorization (EUA) for vilobelimab, also known as Gohibic, to treat COVID-19 in hospitalized adults when initiated within 48 hours of receiving invasive mechanical ventilation or extracorporeal membrane oxygenation (ECMO). The drug is a monoclonal anti-human complement factor C5a antibody, which works to control a part of the immune system that is thought to lead to inflammation and COVID-19 disease progression. The clinical trial supporting the authorization showed that patients treated with Gohibic had a lower risk of death by day 28 and day 60 of treatment compared to those who received a placebo. InflaRx, the treatment’s manufacturer, said it currently has a supply of the drug available and is working to increase production at a contractor facility. The EUA is expected to offer another potentially life-saving treatment option for the most critically ill COVID-19 patients.
MONOCLONAL ANTIBODIES Monoclonal antibodies (mAbs) administered to high-risk COVID-19 patients within 2 days of diagnosis reduced their risk of hospitalization or death by 39%, according to a hypothetical randomized study using observational data published this week in the Annals of Internal Medicine. Researchers at the University of Pittsburgh Medical Center assigned 7,706 high-risk COVID-19 patients aged 12 years or older to receive either mAbs (bamlanivimab, bamlanivimab-etesevimab, sotrovimab, bebtelovimab, or casirivimab-imdevimab) or no treatment between December 8, 2020, and August 31, 2022. The risk of hospitalization or death by 28 days was 4.6% among mAb recipients, compared with 7.6% among control patients. Notably, the US FDA revoked or suspended emergency authorization for all 5 mAbs during the study period after in vitro studies showed little to no benefit against newer SARS-CoV-2 variants. In the study, the benefit was greatest amid the Alpha and Delta variants, potentially reflecting the more virulent earlier strains and lower levels of immunity early in the pandemic. Using one of the largest US databases of patients treated with mAbs, the study confirms that the therapies saved lives and prevented hospitalizations.
NASAL VACCINE CANDIDATE In a study published April 3 in Nature Microbiology, researchers from Germany describe the results of a nasal vaccine candidate made with a live-attenuated form of COVID-19 that they claim can block SARS-CoV-2 from copying itself in the upper airways, where the virus generally gains a foothold. The team used a technique called codon pair deoptimization to manipulate the virus’s genetic material and weaken it so it can be shown to the immune system without making the body sick. In experiments conducted on hamsters, 2 doses of the nasal vaccine candidate, sCPD9, elicited the most robust immunity when compared with homogeneous and heterologous vaccination regimens using the Pfizer-BioNTech mRNA vaccine and Ad2-Spike, an adenovirus-vectored spike protein vaccine candidate. Notably, it remains unclear how effective nasal vaccines may be in humans. As of July 2022, there were at least 12 nasal vaccines under development worldwide. China, India, Iran, and Russia have authorized nasal vaccines, but little is known about their effectiveness.
LATIN AMERICA & CARIBBEAN The Lancet Regional Health Americas discusses the challenges faced by Latin America and the Caribbean (LAC) in rebuilding after the COVID-19 pandemic. In January, representatives from the World Bank, PAHO, and UNICEF met with health ministers and decision-makers from the region to discuss the extensive and enduring effects of the pandemic, which include high mortality rates, economic contraction, increased unemployment, and poverty. The pandemic also revealed vulnerabilities in the region’s healthcare systems with knock-on effects on primary health care, noncommunicable diseases, and education. Additionally, the pandemic disproportionately impacted the mental health of people in the region, with a 35% increase in depression and a 32% increase in anxiety, and mental health care services were disrupted. Representatives at the meeting emphasized the urgent need to address mental health, strengthen essential public health services, provide timely primary care, increase healthcare coverage, and include climate change in rebuilding efforts.
Epi update
As of April 6, the WHO COVID-19 Dashboard reports:
• 762 million cumulative COVID-19 cases
• 6.89 million deaths
• 711,352 million cases reported week of March 27
• 12% decrease in global weekly incidence
• 4,745 deaths reported week of March 27
• 25% decrease in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in all WHO regions except the South-East Asia (+90%) region.
UNITED STATES
The US CDC is reporting:
• 104.1 million cumulative cases
• 1.12 million deaths
• 139,991 cases week of March 29 (down from previous week)
• 1,596 deaths week of March 29 (down from previous week)
• 10.2% weekly decrease in new hospital admissions
• 11.4% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (87.9%), XBB.1.9.1 (4.6%), XBB (2.5%), and XBB.1.5.1 (2.1%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
The New York Times this week launched a “build-your-own-dashboard” to track COVID-19 in US locations.
by ti-amie Yesterday I heard a horror story at the hair salon. One of the young hairdressers four year old son woke up unable to walk and very sick. At the hospital they said he'd been hit by both Covid and the flu, and an MRI was scheduled to be done yesterday. This particular woman, not out of her 20's, and the daughter of a correction officer, wore a mask but it seems she herself was never vaccinated judging by comments she'd made.
This pandemic is not over and while everyone wants to live in the fantasy that it is I'm not part of that collective delusion. I continue to mask in public and will get recommended boosters when available. I'm really worried about this baby and hope he makes a full recovery.
by Deuce Drugs somehow couldn't kill David Crosby - but COVID-19 could...
so not his first bout with Covid - he was certainly in a high risk category and no mention of whether he was ever vaccinated.
I read that he did get the two original COVID-19 vaccines (the 2 which came as a pair, a few weeks apart). I don't know if he received any of the boosters, or how many.
I know that he was in favour of the vaccines, objected to vaccine misinformation, and argued with people who were anti-vaccine.
And, yes, I suppose he was in a higher risk category, based on his age and the myriad stupid abuses he subjected his body to over the years.
by dryrunguy Here's the latest Situation Report. I think they're only coming out once a week now. Because, you know, COVID is in our past. Except it's not.
::
COVID-19 pandemic still volatile, WHO says; disease remains a leading cause of death in US
The WHO this week said the COVID-19 pandemic remains volatile, warning that the virus could bring further trouble before settling into a predictable pattern. The agency noted that in the past 28 days, 23,000 people have died of COVID-19 and 3 million new cases have been reported, even with much lower levels of testing. In the US, COVID-19 remains a leading cause of death, with an average of about 245 deaths per day over the past 4 weeks, primarily among older adults or those who are immunocompromised. The WHO Emergency Committee on COVID-19 is set to meet in the beginning of May to once again reconsider whether the pandemic constitutes a public health emergency of international concern (PHEIC), which it has reaffirmed at its previous meetings since first making the declaration in January 2020.
Additionally, SARS-CoV-2 continues to mutate, with the Omicron subvariant XBB.1.16—first detected in India earlier this year—now accounting for more than 7% of US cases. Another Omicron subvariant, XBC.1.6, a combination of the Delta and Omicron variants of concern first detected in Southern Australia where it caused a wave of cases and hospitalizations, could provide competition to XBB.1.16. Even if many feel the pandemic is over, the virus remains a threat, particularly to vulnerable populations.
US health agencies authorize additional bivalent vaccine booster for certain populations, simplify recommendations; Biden administration launching effort to maintain equitable access to COVID-19 vaccinations
Following US FDA regulatory action earlier this week, the US CDC on April 19 took steps to simplify COVID-19 vaccine recommendations and allow more flexibility for individuals at higher risk of severe disease who would like an additional vaccine dose. Adults aged 65 years and older and people who are immunocompromised may now receive a second dose of updated bivalent mRNA booster targeting both the original viral strain and Omicron BA.4 and BA.5 subvariants at least 4 months or 2 months after their last dose, respectively. Additionally, people who are immunocompromised will now be able to receive more doses if their healthcare provider feels the shots are necessary. About 250 people die each day of COVID-19-related causes in the US, the majority of whom are age 70 or older or have weakened immune systems.
Most US residents who have had one dose of the bivalent vaccine are not currently eligible for an additional jab, although authorization for another shot is expected for the autumn. However, the CDC recommends everyone aged 6 and older receive a bivalent vaccine, regardless of whether they have previously completed their primary series with the original monovalent vaccine. In fact, the monovalent mRNA vaccines are no longer authorized for use in the US. People who are unvaccinated will now require only a single dose of bivalent mRNA vaccine to be considered vaccinated. The guidelines for children remain complicated, with recommendations varying by age, vaccine, and which shots they previously received. The CDC is expected to post a detailed chart with recommendations for children under age 6.
In related news, the Biden administration plans to spend more than US$1 billion on a new public-private partnership to maintain broad access to COVID-19 vaccines, treatments, and tests for millions of uninsured Americans when the medical countermeasures move to the commercial market later this year. The US Department of Health and Human Services (HHS) Bridge Access Program For COVID-19 Vaccines and Treatments Program would allow officials to purchase COVID-19 vaccines for uninsured individuals after the current federal supply is exhausted and when vaccine manufacturers plan to charge as much as $130 per dose. People with private insurance or who are covered under Medicare or Medicaid will also not be expected to pay out-of-pocket expenses for vaccines once the public health emergency ends in May.
Additionally, HHS officials told state governors last week that it will maintain its authority allowing pharmacists, pharmacy technicians, and pharmacy interns to administer COVID-19 and flu vaccines after the COVID-19 public health emergency declaration ends. The extension, set to last through December 2024, is based on the Public Readiness and Emergency Preparedness (PREP) Act, which offers extra protections to companies and providers making, distributing, and administering medicines and vaccines in times of emergency. The White House “Test to Treat” initiative, which allows pharmacists to test people for COVID-19 and prescribe the antiviral Paxlovid, will also continue.
US Congress continues investigations into COVID-19 pandemic origin with Republican-led Senate report, House hearing
Republicans in both houses of the US Congress continued their efforts to investigate the origin of SARS-CoV-2. The investigations, shaped by tensions between scientific knowledge and political discourse, have broad political implications and some say are detracting from the need to take steps to prevent another disease emergency. On April 18, the US House Select Subcommittee on the Coronavirus Pandemic held a second hearing on the origins of COVID-19, with testimony from former intelligence officials discussing the intelligence community’s understanding of COVID-19 origins and the Chinese government’s lack of transparency in providing data and evidence. The hearing raised the ire of the Chinese Embassy, after Li Xiang, the embassy’s liaison to Congress, emailed a staff member of the subcommittee’s chair, Rep. Brad Wenstrup, on April 14 asking “the US side to respect science and facts,” “refrain from targeting China,” “put a stop to the intelligence-led, politics-driven origins-tracing,” and “help promote international solidarity against the pandemic.”
Earlier this week, US Senate Republicans who hold minority leadership on the health subcommittee released a 300-page report that concludes the pandemic most likely began from at least one unintentional lab-related incident—possibly resulting from failures of biosafety containment during vaccine-related research—rather than naturally, via an animal infecting a human; however, the document concedes both theories are plausible but lack key supporting evidence. The report is the result of former Sen. Richard Burr's investigation into the pandemic’s origin, began when he served as the minority leader of the Health, Education, Labor and Pensions Committee, although staffers noted Sen. Burr did not review the full report nor did it go through the vetting process that was afforded an executive summary publicly released last year.
Speaking at a London summit on pandemic preparedness last week, former China CDC Director Dr. George Gao said there is no evidence yet to show an animal host or reservoir for SARS-CoV-2. The WHO has repeatedly called on China to immediately share all available data on the virus, with Chinese officials and scientists rejecting the agency’s accusations that they are hiding information. The WHO says all origin hypotheses remain plausible, while many international scientists say evidence points to a natural origin for the pandemic.
Experts debate universal masking recommendations for healthcare settings; about half of healthcare workers go to work sick with COVID-19, study shows
Most COVID-19-related mask mandates have ended—including those for the subway system in Beijing, China—but debate over whether to mask in healthcare settings is ongoing. While most US states have phased out mask mandates for healthcare settings, many healthcare facilities maintain mask requirements for all staff and patients, but they are increasingly dropping those rules. In a recent commentary published in the Annals of Internal Medicine, a group of infectious disease experts and epidemiologists notes that while “universal masking” was critically important during the pandemic—particularly when there was no population immunity, limited testing capacity, and no medical countermeasures (eg, vaccines, therapeutics)—they argue against masking becoming a required component of Standard Precautions, as COVID-19 transitions from a pandemic to an “endemic phase.” The authors conclude that mandatory masking remains an important infection prevention and control (IPC) strategy that could be employed in the future as “part of a dynamic approach to infection prevention policy that adapts to changing circumstances.”
However, some healthcare workers and other infectious disease epidemiologists have voiced opposition to dropping universal masking, noting that other disease transmission precautions are not scrapped simply because a disease is endemic. In a commentary published in February in the journal Infection Control & Hospital Epidemiology, a separate group of infectious disease experts propose an update to Standard Precautions in healthcare settings, including permanently implementing universal masking in routine patient-care interactions. They say masking prioritizes safety for patients, healthcare providers, and visitors. Other experts fall somewhere in the middle, saying masks remain important in all patient-facing interactions or recommending them to patients who have underlying conditions that put them at higher risk of severe COVID-19.
Notably, a study published last week in the journal Infection Control & Hospital Epidemiology showed that about half of healthcare workers (HCWs) with COVID-19 worked for at least some time during a day when diagnosed but returned to work for additional days with symptoms. The study found that presenteeism rates did not vary for HCWs working directly with patients, suggesting that the potential for disease transmission to patients did not influence HCWs’ choices about whether to go to work. The researchers note that new strategies are needed to help HCWs with COVID-19 reconcile their duties to do no harm and to provide or support care. Additionally, a study presented this week at the European Congress of Clinical Microbiology and Infectious Diseases (ECCMID) in Copenhagen, Denmark, suggests requirements to wear surgical masks in a large London hospital during the first 10 months of Omicron activity (December 2021 to September 2022) made no discernible difference to reducing hospital-acquired SARS-CoV-2 infections. Another study published today in Scientific Reports uses a COVID-19 model showing that a combination of mask wearing and vaccination may be more effective and reasonable in preventing and controlling SARS-CoV-2 infection and suggests infection control departments strongly recommend the use of both strategies to protect unvaccinated individuals from becoming infected.
People with long COVID, advocates frustrated with lack of attention to, actionable research on condition
Americans suffering from post-COVID condition, commonly known as long COVID, are beginning to get frustrated—and for good reason. There is still no clear medical definition, diagnostic framework, or treatment for the condition. The US NIH has received more than US$1 billion to study the condition but it has yet to recruit patients to test potential therapeutics and has released minimal findings from observational studies conducted over the last 2 years, all with allegedly insufficient accountability or oversight. Patients are frustrated that the observational studies conducted so far seem redundant to already completed research and that there are no ongoing efforts to support private sector companies or researchers trying to study long COVID through the NIH. Additionally, one treatment option under consideration—exercise—has the real potential to worsen patients’ condition, causing advocates to raise alarm. Still, other researchers are currently exploring more promising candidates for the treatment or prevention of long COVID, such as metformin, Paxlovid, and low-dose naltrexone. In the meantime, patients continue to feel dismissed by peers, healthcare providers, and institutions, as their lives are disrupted by the condition, sometimes leading to unemployment and homelessness.
Wastewater surveillance gains traction as advantageous disease monitoring system in US, South Korea, globally
The COVID-19 pandemic has provided ample case studies on the value of conducting wastewater surveillance for infectious diseases. The process has certain advantages over hospital-based surveillance in that it can detect viral markers from people with mild cases who did not seek out healthcare or who may have been asymptomatic. Wastewater surveillance has also been instrumental in detecting new viral variants, even as fewer and fewer daily PCR tests are being performed that could provide sequencing material. The US National Wastewater Surveillance System currently has more than 1,000 sites across the country that feed into their data analysis to track SARS-CoV-2 incidence and new variant profiles.
In South Korea, the Korea Disease Control and Prevention Agency (KDCA) is looking to pursue this strategy by implementing a wastewater surveillance system in most major cities and towns. In their current system, hospitals must report all positive tests, which the KDCA director described as an expensive and laborious process. The switch to wastewater surveillance is anticipated to be more cost effective and will provide a broader perspective of the country’s COVID-19 situation. There are also proposals to create a global wastewater surveillance system using airport wastewater. While this endeavor would be useful for disease monitoring, possible disincentives to participation include fear of the imposition of travel restrictions should a disease be detected.
What we’re reading
INFLUENZA PANDEMIC PREPAREDNESS Countries and international bodies must immediately revise existing pandemic influenza preparedness and response plans to incorporate lessons learned from and the impacts of COVID-19, experts from the Johns Hopkins Center for Health Security and colleagues write in Nature Medicine. The authors note these steps are “particularly urgent given both the emergence of a number of influenza spillover threats and exhausted and depleted public health systems globally.” They make recommendations about how revisions could be achieved, concluding, “The world is in a precarious public health position that warrants weighing potential pandemic risks more seriously. The next pandemic may not be influenza, but the risk calculus for such a pandemic must be prepared now.”
VACCINE MANDATE RULING A panel of the San Francisco-based 9th US Circuit Court of Appeals ruled on April 19 that President Joe Biden had the authority under the federal Procurement Act—which enables the president to adopt rules that promote economy and efficiency in federal contracting—to mandate COVID-19 vaccination for millions of federal contractor employees in 2021. The decision reverses a previous ruling by an Arizona court that blocked the mandate last year and creates a split with 3 other appeals courts that have said President Biden likely exceeded his authority. In October 2022, the White House told agencies not to enforce the contractor mandate in light of ongoing and pending legal challenges.
US PRISON POPULATION The United States is known for having the highest incarceration rate on the planet, with significant bias by class and race. COVID-19 reduced the country’s prison population by 17%, but a new study in Nature shows that racial disparities worsened with this decrease, as the proportion of incarcerated Black and Latino people sharply increased. The authors cited changes in typical distribution of those admitted into prisons, disruptions in court proceedings, disruptions in transfers from county jails, as well as ongoing racial disparities in sentence length, pre-trial case dismissals, and pre-trial plea deals as contributors to these trends. They also noted potential structural and racial inequalities in decarceration policies. Unfortunately, these trends reverse some of the progress made in the last decade to reduce prison populations and racial disparities within them.
TYPE 2 DIABETES In a study published this week in JAMA Network Open, Canadian researchers found that people who have had COVID-19 were significantly more likely to be diagnosed with Type 2 diabetes within a year of their infection, compared with those who had not been exposed to SARS-CoV-2. Notably, men were more likely than women to develop diabetes, and people who were hospitalized or in intensive care with COVID-19 were 2 and 3 times as likely to develop the condition, respectively, when compared with individuals who were not infected. The researchers concluded that 3–5% of new diabetes diagnoses could be related to COVID-19. At least 11 other studies have shown an increased risk of developing diabetes after SARS-CoV-2 infection, with one meta-analysis showing a 66% increased risk of diabetes following COVID-19. Some evidence exists suggesting that vaccination might have a protective effect but also that multiple reinfections could raise the risk of Type 2 diabetes. Healthcare organizations and medical professionals should be mindful of the potential long-term outcomes of COVID-19, including monitoring patients for diabetes.
CHILDHOOD VACCINATIONS The COVID-19 pandemic, conflict, and a loss of confidence in vaccines due to misleading information led to 67 million children missing out on at least one routine vaccination between 2019 and 2021, according to UNICEF’s State of the World’s Children 2023 report. A trend of declining confidence in childhood vaccines of up to 44 percentage points in several countries is a “worrying warning signal” of rising vaccine hesitancy, decreasing trust in governments, and increasing politicization, UNICEF Executive Director Catherine Russell said. The report stressed that vaccine confidence can shift and the findings may not indicate a long-term trend.
GLOBAL VACCINATION KNOWLEDGE The Global Compendium of Country Knowledge on COVID-19 Vaccination is now available online from TechNet-21, the WHO announced. The Compendium, which stores more than 140 documents, provides country experiences, case studies, and country evaluations on COVID-19 vaccination and is a resource for national authorities managing or making key decisions on the deployment, implementation, and monitoring of COVID-19 vaccinations, as well as for partners who can provide technical support based on the best practices.
Epi update
As of April 19, the WHO COVID-19 Dashboard reports:
• 763.7 million cumulative COVID-19 cases
• 6.9 million deaths
• 536,422 million cases reported week of April 10
• 24% decrease in global weekly incidence
• 2,289 deaths reported week of April 10
• 48% decrease in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in the Africa (+4%), Europe (-11%), Eastern Mediterranean (-26%), Western Pacific (-30%), and Americas (-55%) regions but increased in South-East Asia (+79%).
UNITED STATES
The US CDC is reporting*:
• 104.3 million cumulative cases
• 1.13 million deaths
• 101,437 cases week of April 12 (down from previous week)
• 1,327 deaths week of April 12 (down from previous week)
• 6.1% weekly decrease in new hospital admissions
• 11.4% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (78%), XBB.1.16 (7.2%), XBB.1.9.1 (6.5%), XBB.1.9.2 (2.5%), XBB.1.5.1 (2.4%), and FD.2 (1.7%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
*According to the CDC, as of April 1, 2023, the state of Iowa no longer reports aggregate COVID-19 case data to CDC. As a result, case counts from Iowa will no longer be reported at the national, regional, state, or county-levels on COVID Data Tracker or data.cdc.gov.
by ponchi101 I don't think that it is because it is in the past. It is that there is very little else to do. When they come with new vaccines for specific variants, we will get them (those, I assume, that got the original ones). But for most people, it is just that we cannot go back to any sort of shot down or isolation.
Some industries never recovered. For example. My friends/colleagues and I used to keep a list of countries we would not go to work: Ethiopia, Pakistan, Southern Colombia, Yemen. The list has been reduced to one single location: East Ukraine. That's how hard we were hit, and we simply can't accept the world shutting down again.
by ti-amie
by ponchi101 If they got tired of masks and such....
I said it in 2020, when this started. This virus would defeat us. It is here to stay. Fortunately, it has mutated towards the "benign".
by dryrunguy Here's the latest Situation Report. The bit about the ivermectin lawsuit was interesting.
There won't be a Situation Report next week. It's safe to say this is winding down.
::
Surveillance efforts decline as US prepares to wind down public health emergency; WHO panel meets to discuss whether to continue PHEIC
As the COVID-19 pandemic enters its fourth year, surveillance of the disease has declined dramatically, both in the US and internationally. The US public health emergency is set to expire on May 11—bringing an end to most federal COVID-19 vaccine requirements—and the US CDC plans to stop reporting its color-coded COVID-19 Community Levels, switching to tracking hospitalizations in some areas. Hospitalizations, however, are a lagging indicator, as it takes about a week to 10 days for a person to be hospitalized with a serious infection. Additionally, most states have stopped public reporting of COVID-19 cases and related deaths, or stopped surveillance efforts altogether, leaving little information to enable scientists to determine how the virus is trending. While most feel the nation, and the world, has moved beyond the days of massive case surges and overwhelmed hospitals, the new normal remains unknown but likely will entail a series of smaller “wavelets.” The virus’s evolution remains unpredictable, however, and without better surveillance, experts are unable to say whether this period of the lowest levels of reported cases and deaths since the beginning of the pandemic is the beginning of a post-pandemic stability or a temporary reprieve.
A panel of global health experts is meeting today to discuss whether COVID-19 still constitutes a public health emergency of international concern (PHEIC). Although there is no consensus on what course the panel may recommend, and whether WHO Director-General Dr. Tedros Adhanom Ghebreyesus follows that advice, several experts feel it is time to wind down the emergency declaration. Regardless of its decision, COVID-19 will remain a complex public health challenge into the future, requiring countries to transition their emergency response activities to longer-term sustained disease prevention, control, and management.
Experts begin to assess pandemic responses, glean lessons learned to prepare for next pandemic
As the COVID-19 public health emergency comes to an end in the US, health officials are working to assess the nation’s response to the COVID-19 pandemic and ensure we are prepared for future health emergencies. In one such effort, 34 experts who were gearing up for the establishment of a 9/11-style commission instead formed the COVID Crisis Group, led by Dr. Philip Zelikow. When the call to establish a National COVID Commission never came, the group pivoted to develop a nonpartisan, dispassionate review of the pandemic response, which was often marred by politicization and infighting. In a report titled, Lessons from the COVID War: An Investigative Report—published by PublicAffairs as a book—the authors outline what went right and wrong with the pandemic response, including why people made certain choices, the availability of information necessary for decision makers to make choices, and the tools that were available and those that necessitated development.
The report includes information from interviews with nearly 300 people and often compares the pandemic response to a military conflict, saying the efforts in the US unraveled like fighting a war with no army or battle plan. According to the report, a lack of human coordination due to a fragmented US public health system, rather than scientific limitations, was one of the major points of failure in the response. Another major lesson centers around communication, with the report highlighting overall emergency communications as a point of failure, during both the Trump and Biden administrations. Poor communication likely exacerbated a loss of trust in US public health institutions, according to the authors. Notably, however, efforts that reached out to local community leaders were often more successful, and future responses will need practical toolkits to aid decision makers in implementing effective communications and mitigation efforts.
The European Centre for Disease Prevention and Control (ECDC) this week published its own assessment of its pandemic response. The report, titled Lessons from the COVID-19 Pandemic, contains 4 main lesson areas: investment in the public health workforce, preparation for the next public health crisis, risk communication and community engagement, and collection and analysis of data and evidence. The collection of pandemic response lessons and recommendations is a crucial task, but political buy-in is needed to implement many of the changes recommended by these assessments that are necessary for preventing and responding to the next pandemic.
Journal articles review progress made, lessons learned on COVID-19 treatment; studies into new treatments, repurposed drugs continue
The journals Nature Reviews Drug Discovery and The BMJ recently published articles examining therapeutic strategies for COVID-19, including progress made, lessons learned, and global standard of care development. Authorized or approved therapies that reduce mortality, length of hospital stay, or time on a ventilator for patients with severe disease include systemic corticosteroids (such as dexamethasone), interleukin-6 receptor antagonists (such as tocilizumab), and Janus kinase inhibitors (such as baricitinib). Additionally, marketed antivirals, including molnupiravir (Lagevrio), nirmatrelvir/ritonavir (Paxlovid), and remdesivir (Veklury), are effective against non-severe COVID-19, particularly when given within 10 days of symptom onset. More than 400 randomized clinical trials have been conducted worldwide on treatments for COVID-19, and research into new therapies continues.
• AstraZeneca’s investigational new antibody drug AZD3152 neutralizes all known variants of SARS-CoV-2 in laboratory studies and could help protect people with compromised immune systems who do not respond well to vaccination. Studies are ongoing, but AstraZeneca is aiming to make the treatment available later this year.
• A study published in the Annals of Internal Medicine evaluated the use of 2 repurposed drugs, the oral selective serotonin reuptake inhibitor (SSRI) fluvoxamine plus the inhaled corticosteroid budesonide, among nonhospitalized adults with early symptomatic COVID-19 and at least one risk factor for severe disease in Brazil. Though a lower proportion of patients in the treatment group than in the placebo group were seen in an emergency setting for COVID-19 for more than 6 hours or were hospitalized within 28 days, no differences were noted in secondary outcomes.
• Another study published in the Annals of Internal Medicine assessed the safety and efficacy of the monoclonal antibodies amubarvimab plus romlusevimab among patients at high risk for poor outcomes in the US, Brazil, South Africa, Mexico, Argentina, and the Philippines during the first half of 2021. Cumulative incidence of hospitalization or death was significantly lower in the treatment group than in the placebo group, regardless of treatment timing. A subgroup analysis of patients with variant data showed the combination was equally effective against Delta and pre-Delta strains, but the researchers speculated the therapy likely would have limited efficacy against the currently predominant Omicron variant.
Vaccine effectiveness studies support use of bivalent formulations, show monovalent vaccines highly effective against severe disease, death but effectiveness waned quickly against Omicron
Advisors to the US FDA are scheduled to meet on June 15 to discuss and make recommendations on future vaccinations against COVID-19 for the general public, now that a second round of bivalent boosters is available for older adults and other people at high risk of severe disease. The FDA will make decisions after the panel meets, but officials previously indicated a desire to recommend annual shots that are possibly updated to match currently circulating variants, similar to flu vaccines. In a study published in Open Forum Infectious Diseases, researchers report that the effectiveness of both Omicron BA.1-containing and BA.4/BA.5-containing bivalent COVID-19 mRNA vaccines against symptomatic infection during the BA.5-dominant period in Japan was high compared to no vaccination (65% and 76%, respectively) and moderate compared to monovalent vaccines administered over half a year earlier (46% combined). Notably, however, the bivalent vaccines were not as effective against Omicron subvariants as the original, monovalent vaccines were against the ancestral strain (Alpha) and Delta variants.
Though the monovalent mRNA vaccines are no longer authorized for use in the US, having been replaced by the bivalent versions, several recent studies show they provided substantial, durable protection against severe COVID-19 disease and death. A study published last week in Morbidity and Mortality Weekly Report found monovalent mRNA vaccination was 76% effective in preventing COVID-19-associated invasive mechanical ventilation (IMV) and death less than 6 months after the last dose and remained 56% effective at 1–2 years. Vaccine effectiveness was higher among older adults, supporting optional, additional bivalent boosters for individuals at highest risk of severe disease. A meta-analysis published in JAMA Network Open shows that vaccine effectiveness of the monovalent vaccines waned quickly and significantly against laboratory-confirmed Omicron infection and symptomatic disease, although the type of vaccine played some role. These studies support the use of updated, bivalent mRNA vaccines and boosters moving forward, and provide some evidence for reformulating the vaccines to match future dominant variants.
Decreasing US racial disparities in COVID-19 deaths possibly due to more deaths among Whites, study shows
A study published this week in JAMA Network Open examines the factors driving changes in mortality rate disparities among racial and ethnic groups over the course of the COVID-19 pandemic. Mortality rates for Hispanic and non-Hispanic Black US residents were much higher than mortality rates for non-Hispanic White residents during the initial wave of the pandemic in 2020. However, those mortality rate disparities decreased in 2021. According to the study, 60.3% of the decrease in mortality disparities are attributable to higher mortality among non-Hispanic White adults and a shift in higher mortality rates to nonmetropolitan areas, where more non-Hispanic White adults reside. The findings highlight a continued need to prioritize racial health equity despite recent reports of decreased mortality disparities, according to the authors, who also make several policy recommendations that could address health equity, including: paid medical leave for essential workers, extended unemployment benefits, and further moratoriums on eviction and foreclosure.
The Kaiser Family Foundation recently released a brief examining the impact of the COVID-19 pandemic by race and ethnicity through the lens of premature mortality, using the measures of premature mortality rate and years of life lost among excess deaths that occurred during the pandemic. The analysis shows that for all groups of color, the pandemic was associated with a steeper increase in the premature death rate than for White people. Notably, the increase in the premature death rate for Hispanic people (33%) was more than twice that of White people (14%) from 2019 to 2022.
What we’re reading
HEALTH SYSTEM RECOVERY According to a new interim report from the WHO, health systems in many countries are beginning to show the first major signs of recovery after 3 years of the COVID-19 pandemic. By early 2023, most countries reported experiencing reduced disruptions in the delivery of routine health services but highlighted the need to apply lessons learned to build more prepared and resilient health systems for the future, according to the report. Despite signs of recovery, service disruptions persist across countries in all regions and income levels, and additional support is needed for recovery, resilience, and preparedness.
US CDC CONFERENCE OUTBREAK The US CDC is investigating several dozen COVID-19 cases linked to its own annual conference held near the agency’s headquarters in Atlanta, Georgia, last week. About 35 people have tested positive as of May 2, according to a CDC spokesperson. The 3-day 2023 Epidemic Intelligence Service conference was the first time in 4 years that EIS officers and alumni gathered in-person. Around 2,000 people attended the conference, and while attendees said many people at the conference did not wear masks or socially distance, most were likely fully vaccinated. The CDC is working with state health officials to determine transmission patterns. The outbreak serves as a reminder that while COVID-19 may not pose the serious risks it did at the beginning of the pandemic, the virus continues to circulate, maybe especially easily at large indoor gatherings.
IVERMECTIN The Wisconsin Supreme Court this week ruled that a hospital cannot be forced to administer ivermectin to a COVID-19 patient. The 6-1 ruling overturned a lower court's order that required Aurora Health Care to treat John Zingsheim, who was placed on a ventilator due to COVID-19 complications, with the anti-parasitic medication. Zingsheim's nephew, Allen Gahl, who was authorized to make medical decisions for Zingsheim, requested his uncle be treated with the drug, but Aurora determined that ivermectin did not meet the standard of care for treating Zingsheim's symptoms. Gahl then sued after doctors refused to administer a prescription for ivermectin that he received from a doctor outside Aurora. The court found that the lower court had no legal basis for its order, citing no law in either its written or oral ruling. The FDA has not approved ivermectin for the treatment of COVID-19, and its misuse can be harmful, even fatal. The lawsuit is one of dozens filed across the US seeking to force hospitals to administer ivermectin to treat COVID-19.
BRAZIL INVESTIGATION Brazil's federal police on May 3 raided the home of former President Jair Bolsonaro as part of an investigation into the alleged falsification of COVID-19 vaccine cards. Authorities seized his phone, searched more than a dozen homes in Rio de Janeiro and Brasília, and arrested 6 people, including some of Bolsonaro’s closest aides. In a statement, the police said the investigation is focused on whether officials in Bolsonaro's inner circle created false vaccination certificates so that unvaccinated travelers, including Bolsonaro, his family members, and assistants' relatives, could circumvent mandatory immunization requirements to enter the US. Bolsonaro confirmed to reporters that he is not vaccinated against COVID-19 but denied playing a role in any fraud.
Epi update
As of May 3, the WHO COVID-19 Dashboard reports:
• 765.2 million cumulative COVID-19 cases
• 6.9 million deaths
• 630,979 million cases reported week of April 24
• 15% decrease in global weekly incidence
• 3,568 deaths reported week of April 24
• 18% decrease in global weekly mortality
Over the previous week, incidence declined or remained relatively stable in all regions except Africa (+17%).
UNITED STATES
The US CDC is reporting:
• 104.5 million cumulative cases
• 1.13 million deaths
• 88,330 cases week of April 26 (down from previous week)
• 1,052 deaths week of April 26 (down from previous week)
• 13.7% weekly decrease in new hospital admissions
• 15.2% weekly decrease in current hospitalizations
The Omicron sublineages XBB.1.5 (69%), XBB.1.16 (12%), XBB.1.9.1 (69%), XBB.1.9.2 (4%), XBB (2.4%), XBB.1.5.1 (2.2%), and FD.2 (1.3%) currently account for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ti-amie My doctor recommended that I get the latest booster but specified Pfizer. I'm going one day next week.
by dryrunguy Figured this was imminent. Here is the final Situation Report.
::
End to COVID-19 pandemic emergency phase brings focus on preparedness, response efforts for future health threats
The COVID-19 pandemic’s impacts, in the US and globally, will be felt for years to come. Though the global COVID-19 emergency has officially ended, SARS-CoV-2 continues to kill at least 1 person every 4 minutes, and questions remain about how to move forward living with a dangerous virus, especially for vulnerable people and countries with less or no access to vaccines and treatments. Meantime, the world must also prepare for the threat of new variants or other pathogens with even deadlier potential, WHO Director Dr. Tedros Adhanom Ghebreyesus said recently at the World Health Assembly, calling on nations to be “ready to answer decisively, collectively, and equitably.”
Discussions about how to ensure equitable access to medical countermeasures during future pandemics are underway, as are negotiations of a wide-reaching treaty laying out new rules for dealing with pandemics. A draft document sent to member states and nongovernmental organizations this week included feedback from previous versions, as well as a clause calling on countries with greater “capacities and resources” to bear a “commensurate degree” of responsibility in global health threat preparedness and response efforts. Separately, discussions are underway to reform the 2005 International Health Regulations (IHR), which describe countries’ obligations during public health events that have the potential to cross borders. Both the pandemic treaty and IHR amendments are on track to be presented at next year’s World Health Assembly.
In related news, the co-chairs of the Independent Panel for Pandemic Preparedness and Response and more than 15 scientists and public health experts called on G7 leaders to make specific commitments to pandemic preparedness and response at their summit in Hiroshima, Japan, last weekend. In their communique, the leaders committed to “further enhancing political momentum toward more coordinated and sustained leader-level governance for health emergency prevention, preparedness and response (PPR) that ensures legitimacy, representation, equity, and effectiveness,” and recognized the importance of the WHO pandemic negotiations to break the cycle of panic and neglect.
Additionally, efforts to track and anticipate the next outbreak from an unknown pathogen, sometimes referred to as Disease X, are ongoing. The WHO on May 20 launched the International Pathogen Surveillance Network (IPSN), a platform using technology to map out the genetic code of disease-causing organisms that will connect countries and regions with an aim of improving systems for collecting and analyzing samples. Though many countries scaled up their genomics capacity over the past 3 years, the IPSN will allow nations to more efficiently share data and use it to drive public health decision-making.
US debt ceiling negotiations consider takeback of unused COVID-19 emergency relief funds
The United States is rapidly approaching the date at which the government can no longer pay its bills, with Treasury Secretary Janet Yellen setting a fast-approaching June 1 deadline to avoid a potential debt default. Debt ceiling negotiations are zeroing in on several key issues, including remaining COVID-19 relief funds. The potential for the redistribution of unused COVID-19 emergency money is an item of contention between US House Democrats and Republicans. Though President Joe Biden has said he is willing to consider a takeback of the remaining funds, many congressional Democrats worry about the consequences such an action would have for public health initiatives the money is intended to support, including efforts to develop vaccines and therapeutics for future SARS-CoV-2 variants and to fortify medical supplies for the Strategic National Stockpile, among others. House Republicans argue that the remaining US$30 billion of the total US$4.6 trillion of pandemic-related funding should be put toward raising the nation’s debt limit because the COVID-19 pandemic emergency is over. While it seems likely that the Biden administration and House Democrats will cede some of the funding, the unspent COVID-19 funds are only a drop in the bucket, dwarfed by the more than US$31 trillion in debt the nation owes.
WHO advisory group recommends updating COVID-19 vaccines to include XBB subvariant; US FDA set to discuss vaccine composition in June
The WHO Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC) last week released new recommendations for updating the antigen composition of COVID-19 vaccines. Current vaccines based on the index SARS-CoV-2 virus offer broad protection against severe disease; however, experts are recommending that new vaccines tailored only to the Omicron XBB.1 subvariant, which is now the most commonly circulating strain, will improve durability and breadth of protection. Some COVID-19 vaccine producers, including Pfizer-BioNTech, Moderna, Novavax, and others, have already begun research and development on vaccines targeting currently circulating variants like XBB.1.
The US FDA is set to meet in mid-June to discuss next-generation vaccine composition and rollout ahead of cold and flu season in the fall. Using the influenza vaccination as a model for future COVID-19 vaccination strategies, the FDA will likely move toward recommending once-a-year COVID-19 boosters that are updated annually to match the most widespread circulating SARS-CoV-2 variant or variants. Pfizer-BioNTech and Moderna are already innovating new approaches for their vaccines against COVID-19, including combination shots that could protect against multiple viral threats.
Pandemic worsened racial/ethnic disparities in health, highlighting need to confront structural inequities
Over the course of the COVID-19 pandemic, racial disparities in cases and deaths have widened and narrowed, but overall, Black, Hispanic, and American Indian and Alaska Native (AIAN) people in the US have borne the heaviest health impacts of the pandemic. New findings renew concerns over these disparities:
• Research from KFF released earlier this week found widening racial disparities in US life expectancy from 2019 to 2021, noting the trend was largely driven by COVID-19 mortality. Researchers said life expectancy declined 2.7 years overall, with decreases of 2.1 years for Asian people (85.6 to 83.5), 2.4 years for White people (78.8 to 76.4), 4 years (74.8 to 70.8) for Black people, 4.2 years (74.8 to 70.8) for Hispanic people, and 6.6 years (71.8 to 65.2) for AIAN people.
• A study published in JAMA last week examined excess deaths and years of potential life lost for the Black population of the US, compared to the White population, from 1999 to 2020. Researchers found that Black Americans have suffered 1.63 million excess deaths and more than 80 million years of potential life lost compared to White Americans. These disparities seemed to be improving until they stalled and then worsened in 2020. Heart disease was the leading cause of excess mortality.
• Black adults are more likely than White adults to suffer from high blood pressure (56% vs 48%, respectively) and less likely to have the condition under control with medication (25% vs 32%, respectively). This disparity, which is expected to worsen in the coming decades, further exacerbates COVID-19 racial disparities, as high blood pressure is listed as a contributing factor in 21.4% of COVID-related deaths among Black patients and 15.5% of COVID-related deaths among White patients.
With the end of the public health emergency in the US ushering in the termination of several policies implemented during the COVID-19 pandemic meant to help people access care, including continuous enrollment for Medicaid and the Children’s Health Insurance Program (CHIP), many fear these health disparities could widen even further. Federal, state, and local governments must work to raise awareness of health disparities and focus on implementing solutions that include confronting structural inequities affecting health insurance coverage and access to care, as well as other socioeconomic factors that impact health.
China experiencing new wave of COVID-19 cases due to XBB subvariants; authorities working to update vaccines
Chinese authorities are working to develop, approve, and distribute vaccines updated for the XBB subvariants, which are driving a new wave of COVID-19 cases. Authorities have approved 2 new vaccines for the subvariants, with the approvals of 3-4 more expected soon. The wave of new infections is expected to peak in June, with up to 65 million cases per week under the worst-case scenarios. China last faced a surge in cases over the 2022-23 winter after dropping its “zero COVID” policy, causing as much as 85% of the population to become infected. Although officials believe this wave will be less severe, public health experts are stressing the need for an aggressive vaccine booster program and ample antiviral supplies to prevent a spike in deaths, particularly among the elderly population. While some hospitals have advised precautions, and some concerts and other events have been canceled without explanation, most residents are continuing life as usual.
Research into new monoclonal antibody therapies moving forward but threatened by lack of long-term investments
Treatment with a monoclonal antibody (mAb) within 2 days of a COVID-19 diagnosis reduced the risk for hospitalization or death by almost 40%, according to one study. With the emergence of the Omicron variant, however, the US FDA withdrew the emergency use authorizations (EUAs) for 5 mAbs because they are ineffective due to mutations in SARS-CoV-2. Now, researchers are working to redesign antibody treatments to target parts of the virus that are less prone to mutation, Science reports. One approach involves creating antibody-like compounds that can bind to multiple sites on viral proteins simultaneously, making it harder for the virus to evade treatment. Other strategies include targeting conserved regions of the spike protein that have not changed among variants and modifying the structure of antibodies to enhance their potency.
But with the US emergency declaration expired, concerns over waning interest and lack of investment in research threaten the development of these new therapies. In April, President Biden’s administration launched a US$5 billion Project NextGen to help commercialize vaccines, mAbs, and other therapeutics, but that funding could fall victim in ongoing debt ceiling negotiations (see story above). What is clear is that long-term investments are needed for COVID-19 therapy research and development, especially for people who are immunocompromised, about 3% of the US population.
What we’re reading
ORIGIN INVESTIGATIONS The Atlantic looks at the state of current scientific investigations into the origin of SARS-CoV-2, including how prior beliefs can affect data interpretation and lead researchers into heated battles. All evidence and options remain on the table, however, “the world probably won’t ever get data that will conclusively end the debate.”
US FEDERAL PRISON RESPONSE In an analysis of nearly 1,500 pages of data, obtained through multiple Freedom of Information Act requests, STAT provides a detailed look at the US federal prison system’s COVID-19 response, finding many prisons implemented substandard mitigation measures throughout the pandemic, including facilities meant to take care of the sickest incarcerated people. The article highlights 4 shortcomings, such as delays in vaccinating high-risk residents, failures to provide widespread screening testing, a lack of reliable data from the Bureau of Prisons on testing activities, and low rates of vaccine booster administration among prison populations.
AFRICA’S TRUST Devex examines the structural and systemic issues that led to a further erosion of trust among African nations during the COVID-19 pandemic and how efforts moving forward might help improve that trust. The article features comments made by Dr. Ayoade Alakija, the WHO’s special envoy for the ACT-Accelerator, who spoke on the sidelines of the World Health Assembly.
WORLD HEALTH STATISTICS REPORT The COVID-19 pandemic is estimated to have resulted in nearly 15 million excess deaths in 2020 and 2021, with each resulting in an average loss of more than 22 years of life, or more than 330 million years of life lost globally, according to the WHO’s 2023 World Health Statistics report. Though global life expectancy increased from 67 years in 2000 to 73 years in 2019, progress against many global health indicators began to slow or stagnate beginning in 2015, prior to the pandemic. The pandemic set things back even further, however, overwhelming health systems and badly disrupting essential health services, the report notes. The WHO warned of the growing threats of noncommunicable diseases (NCDs), air pollution, and antimicrobial resistance but also highlighted successes, such as reductions in exposure to many health risks—including tobacco use, violence, and unsafe water and sanitation—as well as declines in new HIV infections and HIV-related deaths. Global life expectancy at birth is projected to reach 77 years by 2048, according to the report.
CANINE OLFACTORY DETECTION A meta-analysis of 27 studies published in the Annals of Epidemiology adds to the evidence that dogs are able to detect SARS-CoV-2 in humans. According to the analysis, dogs have a high sensitivity of more than 80% and specificity of more than 90% in detecting SARS-CoV-2 in humans through scent. The studies tested dogs on their capacity to detect SARS-CoV-2 in various samples such as sweat, saliva, masks, and urine. In 6 studies with high-quality data, the sensitivity ranged from 82% to 97% and specificity from 83% to 100%. The researchers suggest that canine detection can be beneficial in public spaces and events, providing a relatively cost-effective testing strategy alongside other measures in controlling pandemics.
Epi update
As of May 24, the WHO COVID-19 Dashboard reports:
• 766.9 million cumulative COVID-19 cases
• 6.9 million deaths
• 434,032 confirmed cases reported week of May 15
• 24% decrease in global weekly incidence
• 1,977 deaths reported week of May 15
• 55% increase in global weekly mortality
Over the previous week, case incidence declined or remained relatively stable in all WHO regions.
UNITED STATES
The US CDC is reporting:
• 1.13 million cumulative deaths
• 9,186 weekly COVID-19 hospital admissions (decrease of 4.9%)
The data for variant proportions have not changed since last week, as the CDC now updates only every other week. As of March 13, the Omicron sublineages XBB.1.5 (64%), XBB.1.16 (14%), XBB.1.9.1 (9%), XBB.1.9.2 (4%), XBB.2.3 (3.5%), XBB.1.5.1 (2.4%), and FD.2 (1.8%) accounted for a majority of all new sequenced specimens, with various other Omicron subvariants accounting for the remainder of cases.
by ti-amie The Washington Post :press:
@washingtonpost@press.coop
More than 200 lingering symptoms have been reported in patients who suffer ongoing health problems after a covid infection.
Now a new study has identified 12 key symptoms that best define the debilitating condition known as long covid. https://wapo.st/428KV2j #press
dryrunguy wrote: ↑Thu May 25, 2023 9:04 pm
Figured this was imminent. Here is the final Situation Report.
::
...
Txs for posting all these reports during these times.
You were extremely useful, as were the reports.
by ti-amie Thank you for keeping us informed for the last few years dry. I will miss these updates.
by ti-amie
by ti-amie
by dryrunguy Instead of receiving the Johns Hopkins Situation Report, which ceased publication several weeks ago, I now receive their Health Security newsletter that covers information beyond the bounds of just COVID. In any case, here's an excerpt from the one that just arrived this afternoon.
::
US CDC COVID-19 indicators show increase, beginning of possible summer wave
Two metrics the US CDC uses to keep track of the COVID-19 pandemic—the number of new hospital admissions with COVID-19 and the percentage of emergency room visitors diagnosed with COVID-19—are rising across the country, according to data reported for the week of July 15. Though still at near historic lows after 7 months of steady declines, the markers have been increasing for about 4 weeks, indicating the US likely is entering its fourth summer COVID-19 wave, although it is currently small. Rises in early indicators, including test positivity and wastewater levels, preceded the increase in hospitalizations seen this week, according to a CDC spokesperson. Only the Midwestern region—including Illinois, Indiana, Michigan, Minnesota, Ohio, and Wisconsin—did not record an increase in weekly COVID-19 hospitalizations.
COVID-19 tracking is not as comprehensive as it once was, as many people do not test, and if they do, they likely use home tests and do not report results to authorities. Many localities are turning to wastewater surveillance to provide some warning that an increase in COVID-19 cases might be coming. A new study published July 26 in JAMA Network Open found that levels of SARS-CoV-2 in a community's wastewater were closely in line with local case and hospitalization rates. Those indicators fell out of sync by fall 2022, but that likely was due to case counts becoming more unreliable because of at-home tests and more people developing immunity or receiving treatments that protected them from hospitalization. Wastewater surveillance remains a dependable metric to keep track of how much virus is circulating in a community.
No single or new variant is responsible for the increase in cases. A mix of descendants from the XBB Omicron subvariant are likely driving the increase in cases, according to current CDC projections. Among these is EG.5, a descendant of XBB.1.9.2, with one extra spike mutation, which accounts for approximately 11.5% of new cases. The WHO last week added EG.5 to its list of Omicron variants under monitoring (VUM). Updated COVID-19 vaccine boosters, expected to roll out this fall, will be a monovalent composition targeting the XBB.1.5 subvariant. According to the CDC, many people may wait to receive the updated vaccine, as it is expected to provide more robust protection against currently circulating variants, although some individuals may need or want a booster shot prior to the release of the new formulation.
by Owendonovan My husband and I are the only people we know who still pay attention to COVID. (outside this forum)
by ti-amie Tara C. Smith :verified:
@aetiology@med-mastodon.com
I love it when people claim our founding fathers would be against vaccination, when there's so much evidence otherwise. Just released from the American Society for Microbiology archives: Thomas Jefferson from 1826, establishing a public clinic at the University of Virginia providing medical advice, smallpox vaccines (free!), and surgery to all peoples.
by ponchi101 One of the groups of most forward thinking people in the history of the world, would have been against vaccination.
Sure.
by skatingfan
ponchi101 wrote: ↑Wed Aug 16, 2023 10:22 pm
One of the groups of most forward thinking people in the history of the world, would have been against vaccination.
Sure.
Particularly at a time when infectious disease was not well understood, and was a constant threat to everyone.
by ti-amie New York is in the midst of a spike right now.
by ti-amie Ars Technica
@arstechnica
FDA finally nabs alleged quack who claimed silver vibrations cure COVID
Gordon H. Pedersen of Utah was on the run from fraud charges for three years.
by ponchi101 Silver VIBRATIONS, P, silver VIBRATIONS, not silver VIBRAT....
(I have to stop trying to read everything in one gulp)
by ti-amie
ponchi101 wrote: ↑Wed Aug 16, 2023 11:36 pm
Silver VIBRATIONS, P, silver VIBRATIONS, not silver VIBRAT....
(I have to stop trying to read everything in one gulp)
You and me both!
by ti-amie Eric Topol
@erictopol@mstdn.social
There are 2 new publications today on Covid follow-up at 2 years that shed light on #LongCovid, but there are still many known unknowns...
by ti-amie
Patient Mike Camilleri works with physical therapist Beth Hughes in St. Louis on March 1. A mild covid-19 case set off a chain reaction that left Camilleri with dangerous blood pressure spikes, a heartbeat that raced with slight exertion and episodes of intense chest pain. (Angie Wang/AP)
Many long-covid symptoms linger even after two years, new study shows
By Amy Goldstein
August 21, 2023 at 11:00 a.m. EDT
by ti-amie Ron Chusid :verified:
@rchusid@med-mastodon.com
Hollywood often had the strictest Covid precautions earlier in the pandemic as they couldn't afford the financial hit of hard to replace stars getting sick. One studio is reinstating masking after a recent Covid outbreak.
#Covid #CovidIsNotOver
by ti-amieGottaLaff@mastodon.social
Safe Schools Coalition BC
@SafeSchoolsBC@zeroes.ca
Just a few weeks into the school year, some USA states are having to cancel classes due to rampant illness. (Proof that “immunity debt” was false and most likely “immunity theft” from COVID is to blame.)
Therefore, BC schools need to employ protections like masks & clean air to avoid the same fate. BC NDP?
by dryrunguy Johns Hopkins latest newsletter (today) led off with what's below:
Number of sequenced cases of BA.2.86 doubles this week but still too early to predict course of new variant
The number of sequenced cases of the new SARS-CoV-2 variant BA.2.86 doubled this week. As of writing, 27 cases have been reported in 8 countries—Denmark (10), Sweden (4), Portugal (2), UK (3), Israel (1), South Africa (2), Canada (1), and the US (4)—according to a dashboard created by Dr. Raj Rajnarayanan, Assistant Dean of Research and Associate Professor at NYITCOM at Arkansas State University. The variant has been detected in wastewater in several additional countries, including Switzerland and Thailand, as well as 4 US states and New York City. Scientists remain on alert but say it is still too early to predict whether the variant will become widespread or cause disruption like the original Omicron variant.
In the US, COVID-19 hospitalizations rose nearly 19% in the most recent week and COVID-19 deaths rose 21.4%, according to US CDC data. Only a few states—Alaska, New Hampshire, and North Dakota—saw COVID-related hospital admissions fall last week, while 26 states experienced a "substantial increase" in COVID-19 hospitalizations. Despite increasing week by week, hospitalizations remain at historic lows, and while general hospital departments can better manage the care of COVID-19 patients now compared with the beginning of the pandemic, healthcare practitioners would welcome better medications, especially products that do not interact with other drugs.
Updated vaccines are expected to be available in the US in mid-September, and the UK announced this week it is moving up its planned COVID-19 and flu vaccination campaign from October to September. Because of its large number of spike protein mutations, BA.2.86 may be more able to skirt existing immunity and cause infection in people who have previously had COVID-19 or been vaccinated against it. The updated vaccines, which will be monovalent and target the XBB.1.5 Omicron subvariant, are expected to be effective against the most currently predominant subvariant, EG.5, which is a descendent of the XBB lineage. As the US heads into the Labor Day weekend, when gatherings of family and friends are common, people should consider their circumstances and utilize mitigation measures—such as mask wearing, gathering outside, improving indoor ventilation, and testing—as appropriate.
by ponchi101 Dear John Hopkins.
Don't tell us the percentage increase. If you say deaths increased 21.4%, putting the absolute numbers is also good to know.
Also, by now we have almost 4 years of data. Tell us the trend.
by MJ2004 And.. my husband has symptoms and tested positive. I'm feeling ok, but we'll see over the next few days. Only a matter of time for everyone, it seems.
Absolutely nobody is masked around here.
by ponchi101 Hope you will escape, and hope your husband will get better soon.
by Oploskoffie
MJ2004 wrote: ↑Sun Sep 10, 2023 12:18 pm
And.. my husband has symptoms and tested positive. I'm feeling ok, but we'll see over the next few days. Only a matter of time for everyone, it seems.
Absolutely nobody is masked around here.
Hopefully both of you will come out of it just fine and yes, sooner or later it will reach (nearly) everyone, everywhere. Is there still a level of mask requirement of expecation where you live?
Here in the Netherlands the public mask requirement was lifted in february 2022 for most locations, with (I think) airports being the last to lose it. Hospitals and other medical locations kept the requirements for far longer. The government choice, for now, has pretty much been to "learn to live with it" and have it gradually take its place amongst the annual disseases like the flu. There's a lot of opinions to go around where that's concerned but for now it has seemed to work and after a brief spike late last year, things have continued to stabilize. Fingers crossed for this fall.
by MJ2004
Oploskoffie wrote: ↑Sun Sep 10, 2023 7:33 pm
Is there still a level of mask requirement of expectation where you live?
Not at all. And while I somewhat understand the perspective of "learn to live with it", it's just aggravating to see people out and about in the middle of a "mini-COVID wave" while sick and with no masks. I fall into the camp of it's really not that hard to wear one, especially when out in crowded public spaces.
We think it was caught on the subway - my husband was masked, but the man across from him coughing up a storm with no mask on. In the meantime, I've seen people at work sick, with "colds and coughs" and no masks. People have thrown any level of precaution and consideration for others out the window.
by Oploskoffie
MJ2004 wrote: ↑Mon Sep 11, 2023 12:34 am
Not at all. And while I somewhat understand the perspective of "learn to live with it", it's just aggravating to see people out and about in the middle of a "mini-COVID wave" while sick and with no masks. I fall into the camp of it's really not that hard to wear one, especially when out in crowded public spaces.
We think it was caught on the subway - my husband was masked, but the man across from him coughing up a storm with no mask on. In the meantime, I've seen people at work sick, with "colds and coughs" and no masks. People have thrown any level of precaution and consideration for others out the window.
For the record, I'm in your camp when it comes to mask usage.
What I think one of the big issues is, especially with the current covid variants, is that for many people the symptoms are mild at worst and too similar to pre-2020 having a cold or a flu-like symptoms for which hardly anyone would stay at home (or be expected to) nevermind wear something as "extreme" as a facial mask. Working from home, in my organization, was reserved for people with disabilities of some sort. As for the rest... Feeling under the weather? Come into work anyway and see how it goes, right? Been home for a few days? Expect a call from the manager, asking about your return to work. Though certainly not in all companies/businesses, we do appear to be heading back in that direction. Same for schools, colleges and universities.
For some part, it probably is a variant of simply being selfish. Then there's the part of the population that never considered covid an issue/reality to begin with, so for them it's merely a continuation of what would be considered "normal". And then there is, in my opinion, a large part of society who are not consciously/deliberately being selfish/disregarding the worries of a shrinking minority, but as a response to the experiences of the last couple of years have a stronger need for a semblance of normality wherein mask usage and other covid reminders have no place. I see it all around me, especially with my partner's two children, the youngest of whom really struggled socially during the lockdowns and other restrictions and has now completely gone into FoMO-mode, only sleeping between his neverending social engagements and, for as much as he feels like attending, his college classes. None - and I mean zero - of his friends ever do a covid test these days, while we still regularly hear about people having symptoms that could be caused by it. It's not deliberate, it's simply left their mindset.
by atlpam After 3.5 years, it finally caught up with us. Still no clue where I was exposed as our summer life is mostly outdoors with minimal interactions with the public other than an occasional restaurant or the grocery store. We took precautions going to Boston for a memorial service, wearing masks since we would be around many people, but it turns out I was the one likely to expose people as I started experiencing symptoms as the day went on. Was still hoping it was ‘just the flu’, but no such luck and the hubs got symptoms 4 days later. Had to cancel a visit from friends that we had been looking forward to all summer. Now hoping to test negative by end of week so I can visit family (an aunt I haven’t seen in 10 years).
by mmmm8
atlpam wrote: ↑Mon Oct 02, 2023 1:40 pm
After 3.5 years, it finally caught up with us. Still no clue where I was exposed as our summer life is mostly outdoors with minimal interactions with the public other than an occasional restaurant or the grocery store. We took precautions going to Boston for a memorial service, wearing masks since we would be around many people, but it turns out I was the one likely to expose people as I started experiencing symptoms as the day went on. Was still hoping it was ‘just the flu’, but no such luck and the hubs got symptoms 4 days later. Had to cancel a visit from friends that we had been looking forward to all summer. Now hoping to test negative by end of week so I can visit family (an aunt I haven’t seen in 10 years).
Wishing you a quick recovery and a complete one too!
atlpam wrote: ↑Mon Oct 02, 2023 1:40 pm
After 3.5 years, it finally caught up with us. Still no clue where I was exposed as our summer life is mostly outdoors with minimal interactions with the public other than an occasional restaurant or the grocery store. We took precautions going to Boston for a memorial service, wearing masks since we would be around many people, but it turns out I was the one likely to expose people as I started experiencing symptoms as the day went on. Was still hoping it was ‘just the flu’, but no such luck and the hubs got symptoms 4 days later. Had to cancel a visit from friends that we had been looking forward to all summer. Now hoping to test negative by end of week so I can visit family (an aunt I haven’t seen in 10 years).
Wishing you a quick recovery and a complete one too!
Thankfully I have already recovered, it was equivalent to having the flu for me. If the husband’s is on a similar trajectory, he should start improving tomorrow.
by ti-amie A friend of mine came to NYC for her annual visit and when she got home she was, as the saying goes, sick as a dog. She says she feels better but her voice is still "pneumonia breathy" and her family is encouraging her to go to a doctor.
Pam I'm glad to hear that you're better.
by ti-amie MARCH 13, 2024
COVID-19 Leaves Its Mark on the Brain. Significant Drops in IQ Scores Are Noted
Research shows that even mild COVID-19 can lead to the equivalent of seven years of brain aging
BY ZIYAD AL-ALY & THE CONVERSATION US
The following essay is reprinted with permission from The Conversation, an online publication covering the latest research.
From the very early days of the pandemic, brain fog emerged as a significant health condition that many experience after COVID-19.
Brain fog is a colloquial term that describes a state of mental sluggishness or lack of clarity and haziness that makes it difficult to concentrate, remember things and think clearly.
Fast-forward four years and there is now abundant evidence that being infected with SARS-CoV-2 – the virus that causes COVID-19 – can affect brain health in many ways.
In addition to brain fog, COVID-19 can lead to an array of problems, including headaches, seizure disorders, strokes, sleep problems, and tingling and paralysis of the nerves, as well as several mental health disorders.
A large and growing body of evidence amassed throughout the pandemic details the many ways that COVID-19 leaves an indelible mark on the brain. But the specific pathways by which the virus does so are still being elucidated, and curative treatments are nonexistent.
Now, two new studies published in the New England Journal of Medicine shed further light on the profound toll of COVID-19 on cognitive health.
I am a physician scientist, and I have been devoted to studying long COVID since early patient reports about this condition – even before the term “long COVID” was coined. I have testified before the U.S. Senate as an expert witness on long COVID and have published extensively on this topic.
Here are some of the most important studies to date documenting how COVID-19 affects brain health:
Large epidemiological analyses showed that people who had COVID-19 were at an increased risk of cognitive deficits, such as memory problems.
Imaging studies done in people before and after their COVID-19 infections show shrinkage of brain volume and altered brain structure after infection.
A study of people with mild to moderate COVID-19 showed significant prolonged inflammation of the brain and changes that are commensurate with seven years of brain aging.
Severe COVID-19 that requires hospitalization or intensive care may result in cognitive deficits and other brain damage that are equivalent to 20 years of aging.
Laboratory experiments in human and mouse brain organoids designed to emulate changes in the human brain showed that SARS-CoV-2 infection triggers the fusion of brain cells. This effectively short-circuits brain electrical activity and compromises function.
Autopsy studies of people who had severe COVID-19 but died months later from other causes showed that the virus was still present in brain tissue. This provides evidence that contrary to its name, SARS-CoV-2 is not only a respiratory virus, but it can also enter the brain in some individuals. But whether the persistence of the virus in brain tissue is driving some of the brain problems seen in people who have had COVID-19 is not yet clear.
Studies show that even when the virus is mild and exclusively confined to the lungs, it can still provoke inflammation in the brain and impair brain cells’ ability to regenerate.
COVID-19 can also disrupt the blood brain barrier, the shield that protects the nervous system – which is the control and command center of our bodies – making it “leaky.” Studies using imaging to assess the brains of people hospitalized with COVID-19 showed disrupted or leaky blood brain barriers in those who experienced brain fog.
A large preliminary analysis pooling together data from 11 studies encompassing almost one million people with COVID-19 and more than 6 million uninfected individuals showed that COVID-19 increased the risk of development of new-onset dementia in people older than 60 years of age.
Autopsies have revealed devastating damage in the brains of people who died with COVID-19.
Most recently, a new study published in the New England Journal of Medicine assessed cognitive abilities such as memory, planning and spatial reasoning in nearly 113,000 people who had previously had COVID-19. The researchers found that those who had been infected had significant deficits in memory and executive task performance.
This decline was evident among those infected in the early phase of the pandemic and those infected when the delta and omicron variants were dominant. These findings show that the risk of cognitive decline did not abate as the pandemic virus evolved from the ancestral strain to omicron.
In the same study, those who had mild and resolved COVID-19 showed cognitive decline equivalent to a three-point loss of IQ. In comparison, those with unresolved persistent symptoms, such as people with persistent shortness of breath or fatigue, had a six-point loss in IQ. Those who had been admitted to the intensive care unit for COVID-19 had a nine-point loss in IQ. Reinfection with the virus contributed an additional two-point loss in IQ, as compared with no reinfection.
Generally the average IQ is about 100. An IQ above 130 indicates a highly gifted individual, while an IQ below 70 generally indicates a level of intellectual disability that may require significant societal support.
To put the finding of the New England Journal of Medicine study into perspective, I estimate that a three-point downward shift in IQ would increase the number of U.S. adults with an IQ less than 70 from 4.7 million to 7.5 million – an increase of 2.8 million adults with a level of cognitive impairment that requires significant societal support.
Another study in the same issue of the New England Journal of Medicine involved more than 100,000 Norwegians between March 2020 and April 2023. It documented worse memory function at several time points up to 36 months following a positive SARS-CoV-2 test.
Taken together, these studies show that COVID-19 poses a serious risk to brain health, even in mild cases, and the effects are now being revealed at the population level.
A recent analysis of the U.S. Current Population Survey showed that after the start of the COVID-19 pandemic, an additional one million working-age Americans reported having “serious difficulty” remembering, concentrating or making decisions than at any time in the preceding 15 years. Most disconcertingly, this was mostly driven by younger adults between the ages of 18 to 44.
Data from the European Union shows a similar trend – in 2022, 15 percent of people in the EU reported memory and concentration issues.
Looking ahead, it will be critical to identify who is most at risk. A better understanding is also needed of how these trends might affect the educational attainment of children and young adults and the economic productivity of working-age adults. And the extent to which these shifts will influence the epidemiology of dementia and Alzheimer’s disease is also not clear.
The growing body of research now confirms that COVID-19 should be considered a virus with a significant impact on the brain. The implications are far-reaching, from individuals experiencing cognitive struggles to the potential impact on populations and the economy.
Lifting the fog on the true causes behind these cognitive impairments, including brain fog, will require years if not decades of concerted efforts by researchers across the globe. And unfortunately, nearly everyone is a test case in this unprecedented global undertaking.
ZIYAD AL-ALY is the chief of research and development at the VA St. Louis Health Care System. He is a clinical epidemiologist at Washington University in St. Louis
by ponchi101 How about the people that had the vaccine AND still got the virus? The vaccines, we know, just made the symptoms less severe and gave you a better chance of not dying of the thing. Did they also protect you from this brain fog and cognitive decay?




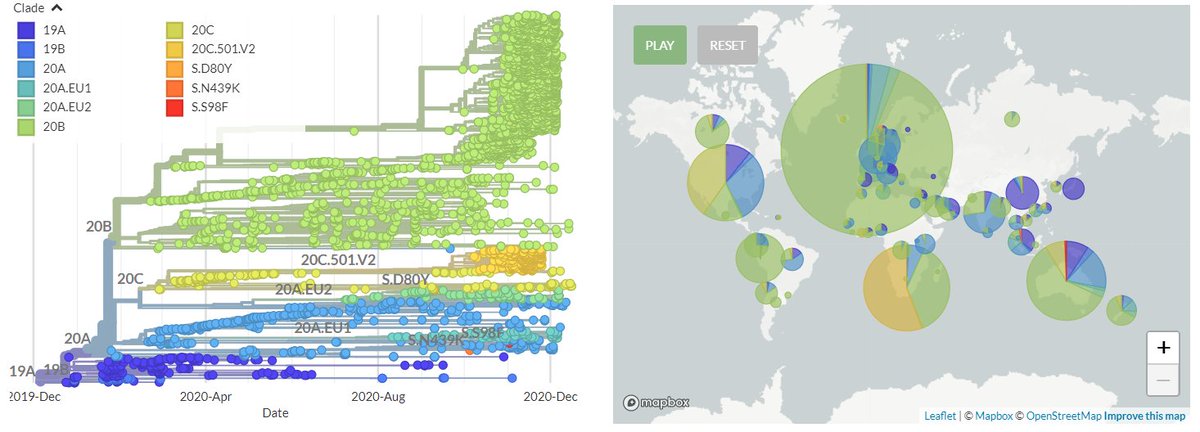

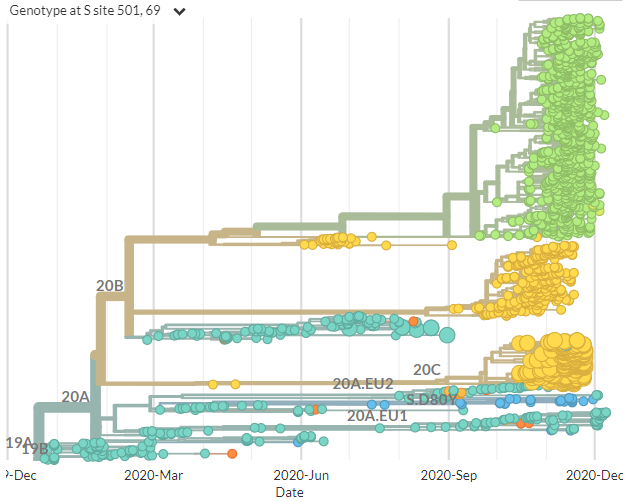
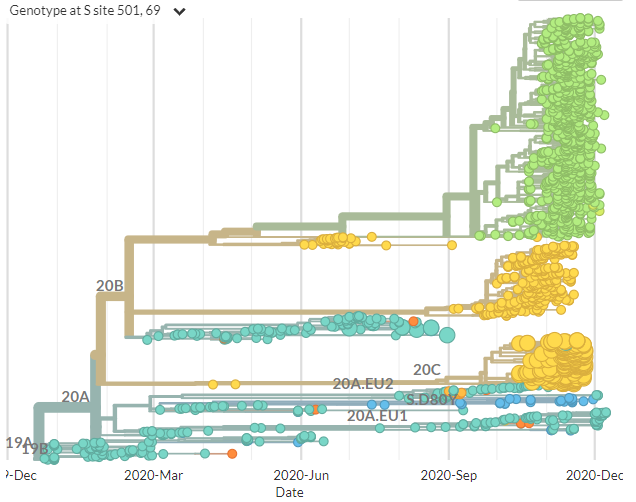



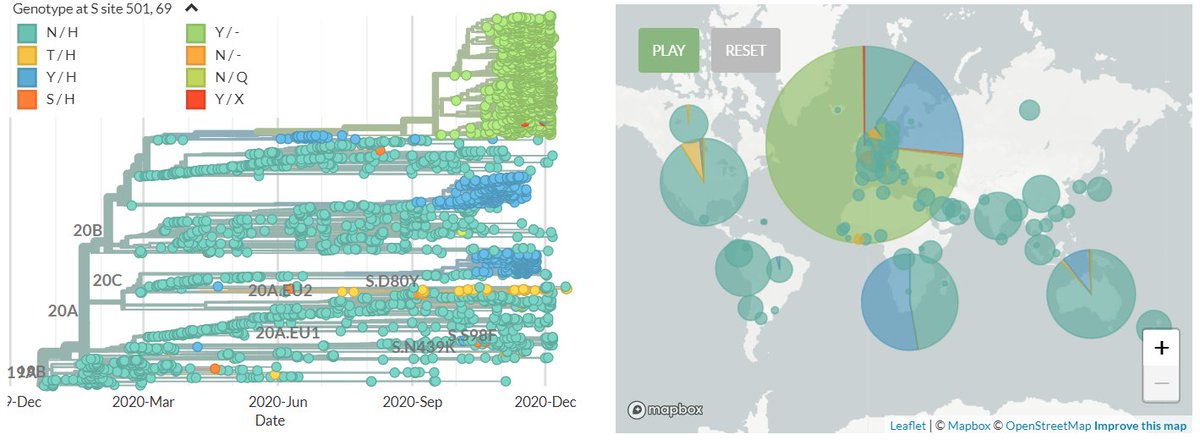


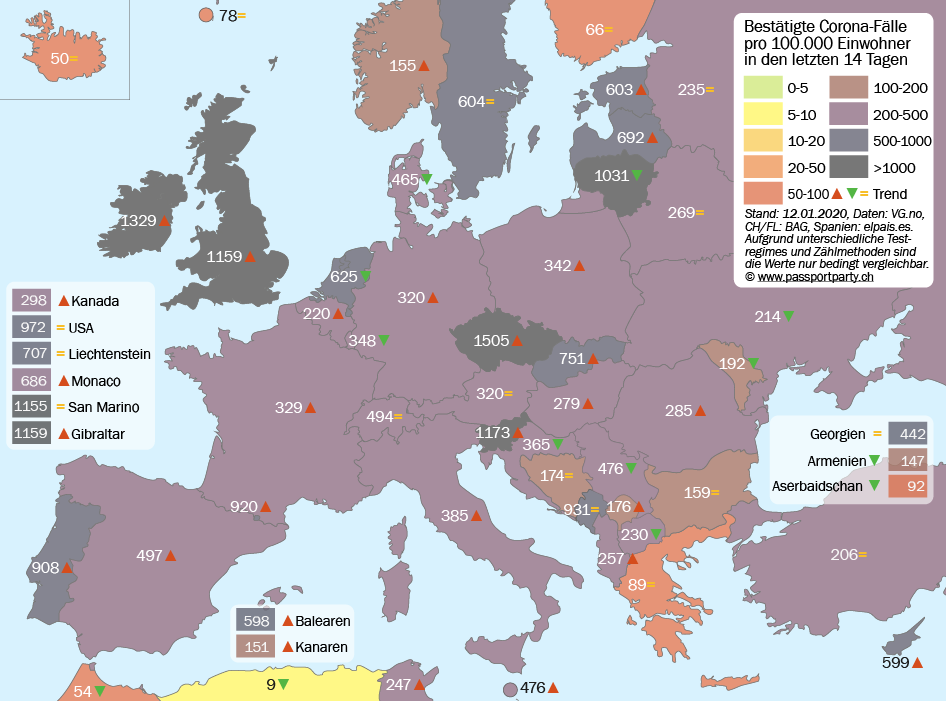
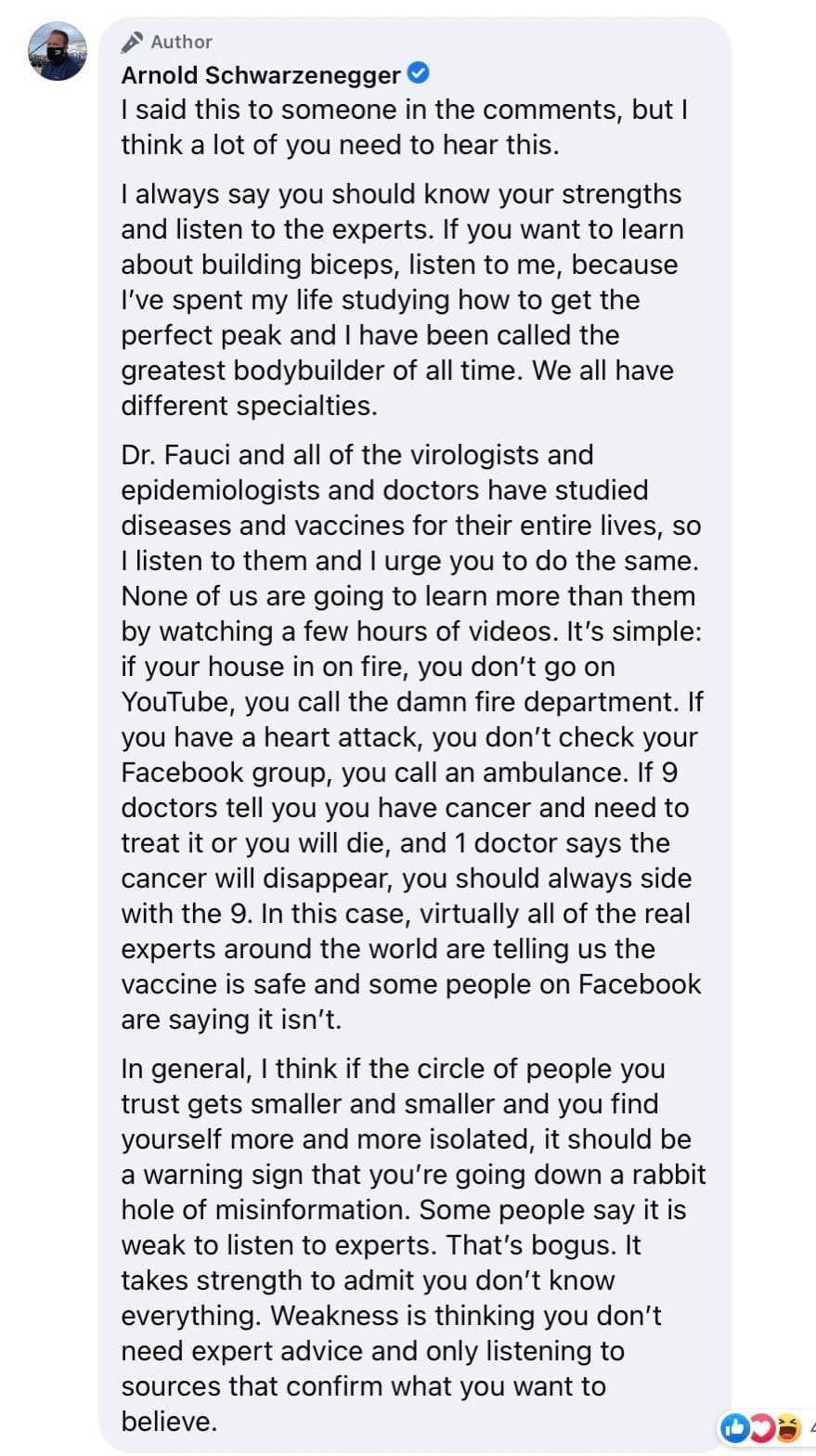


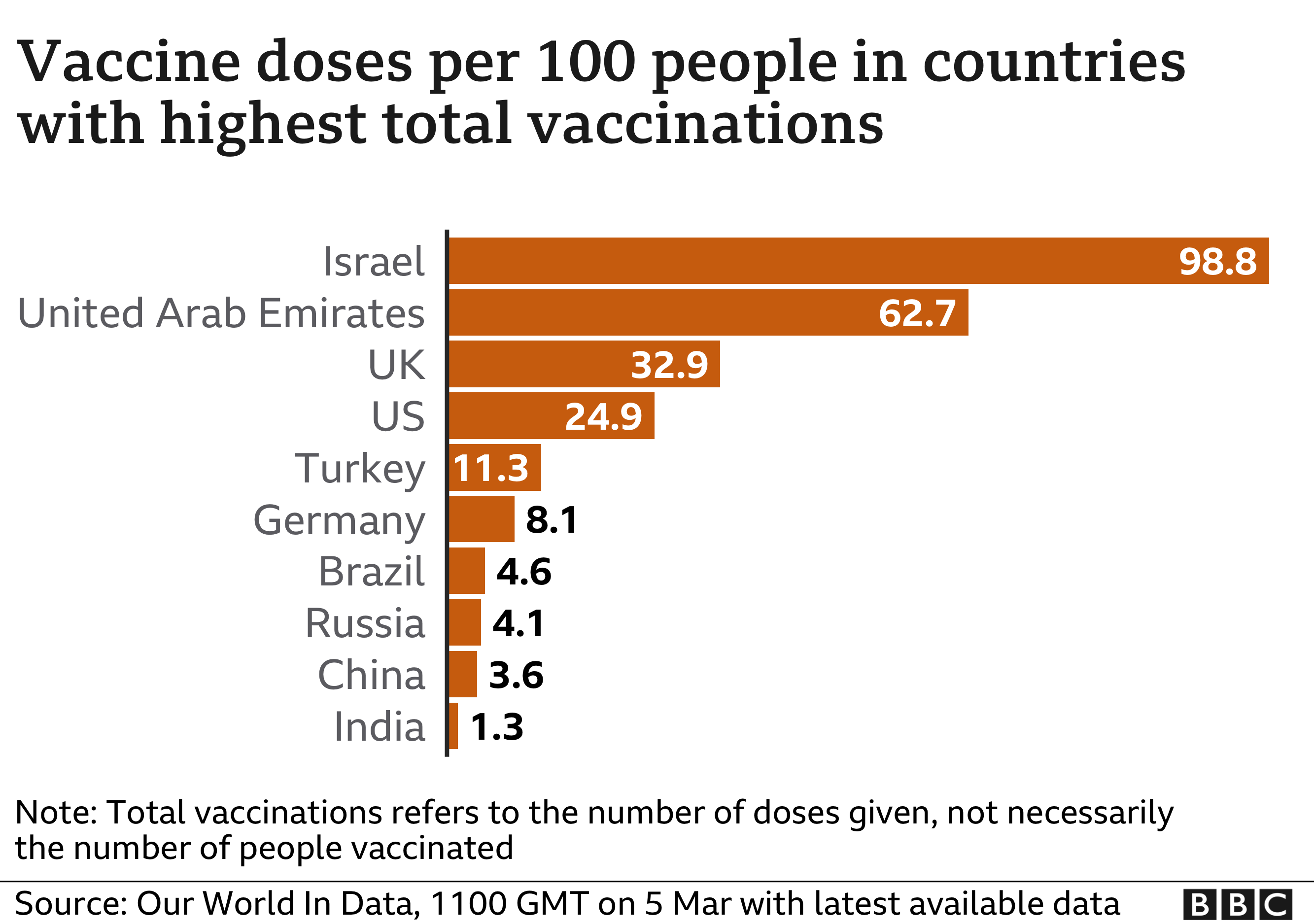

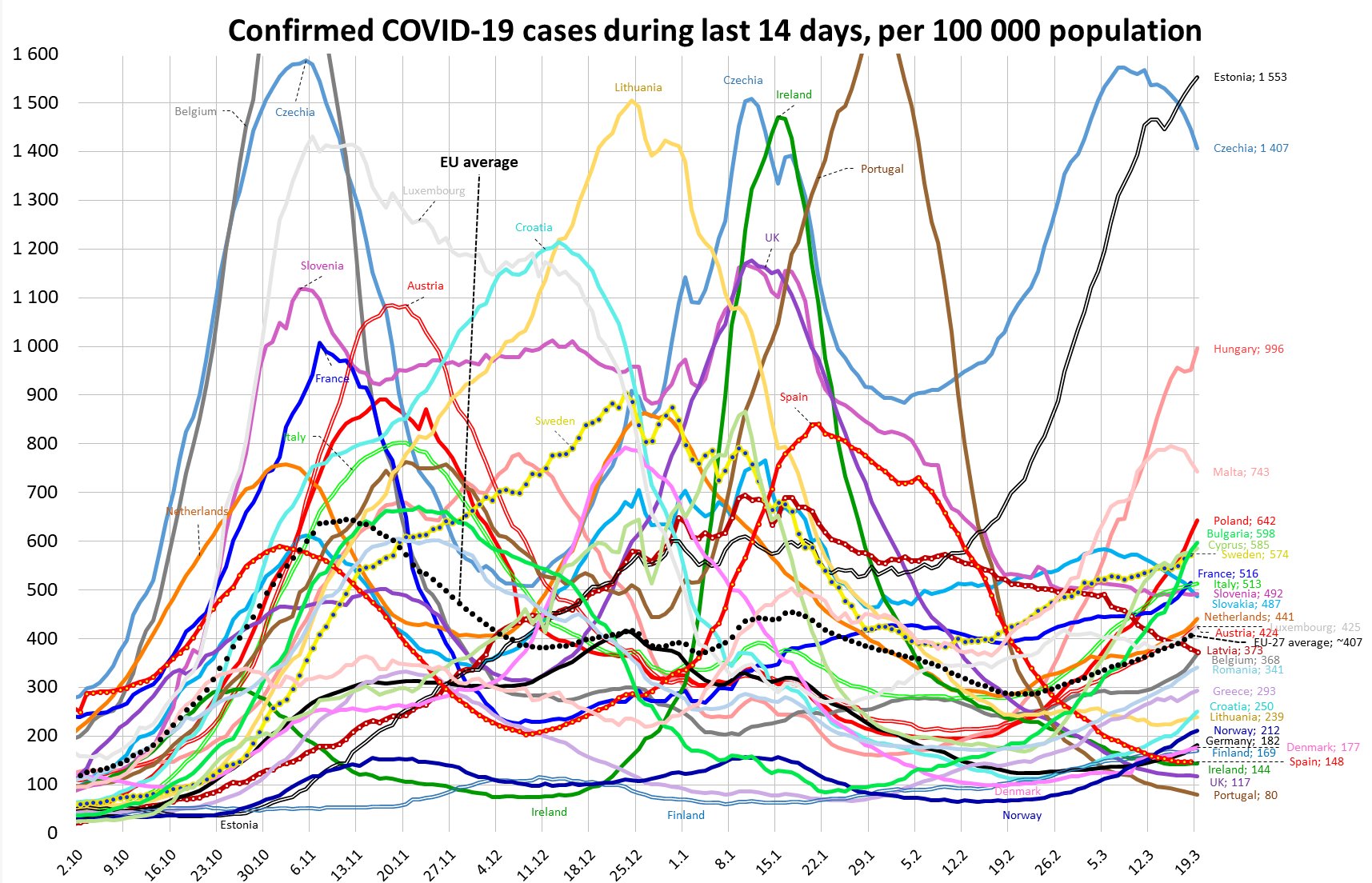





 (click for a graph)
(click for a graph)
 #COVID19
#COVID19











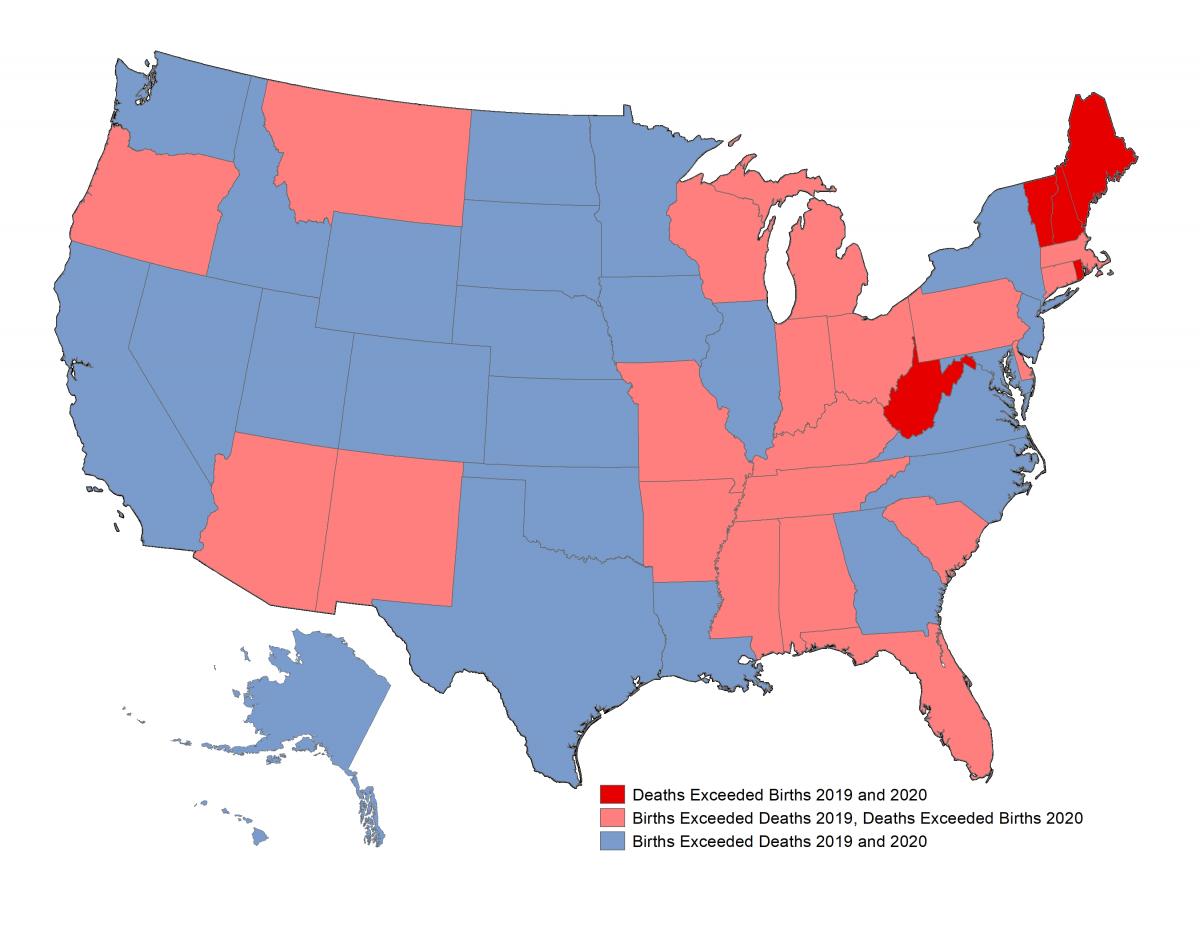






 study found that after adjusting for factors, Omicron is only slightly intrinsically milder—2%-12% (red)
study found that after adjusting for factors, Omicron is only slightly intrinsically milder—2%-12% (red)
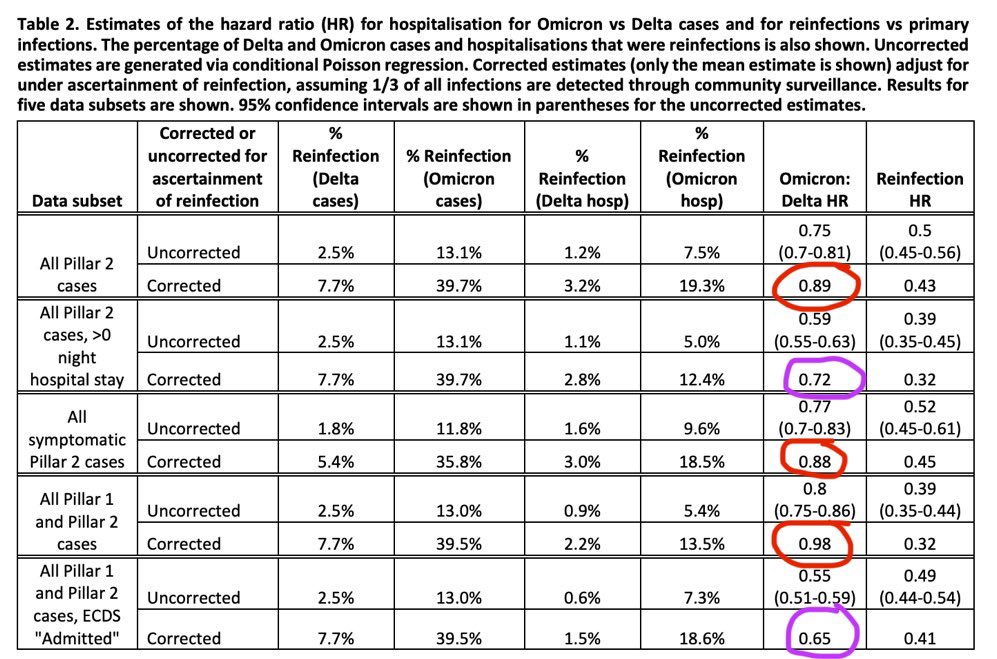
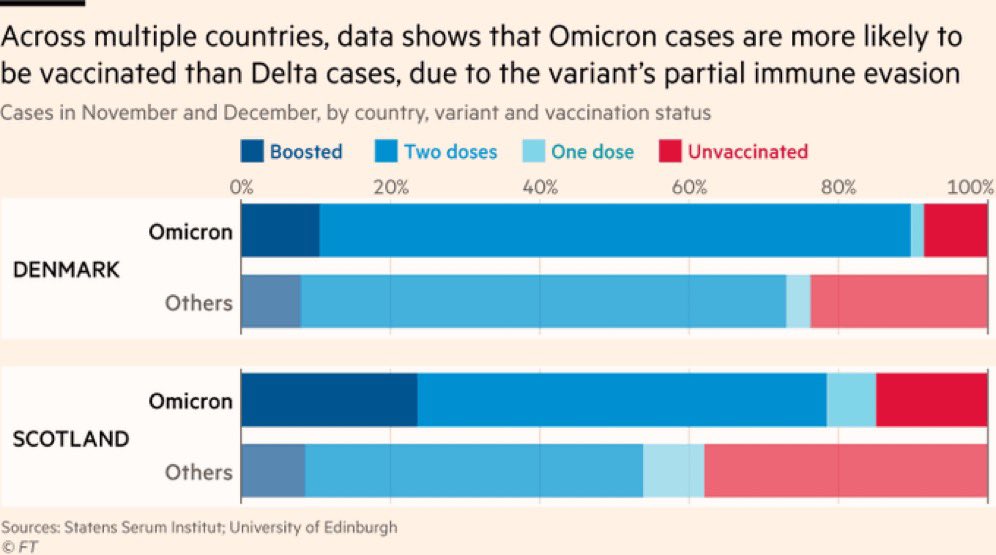
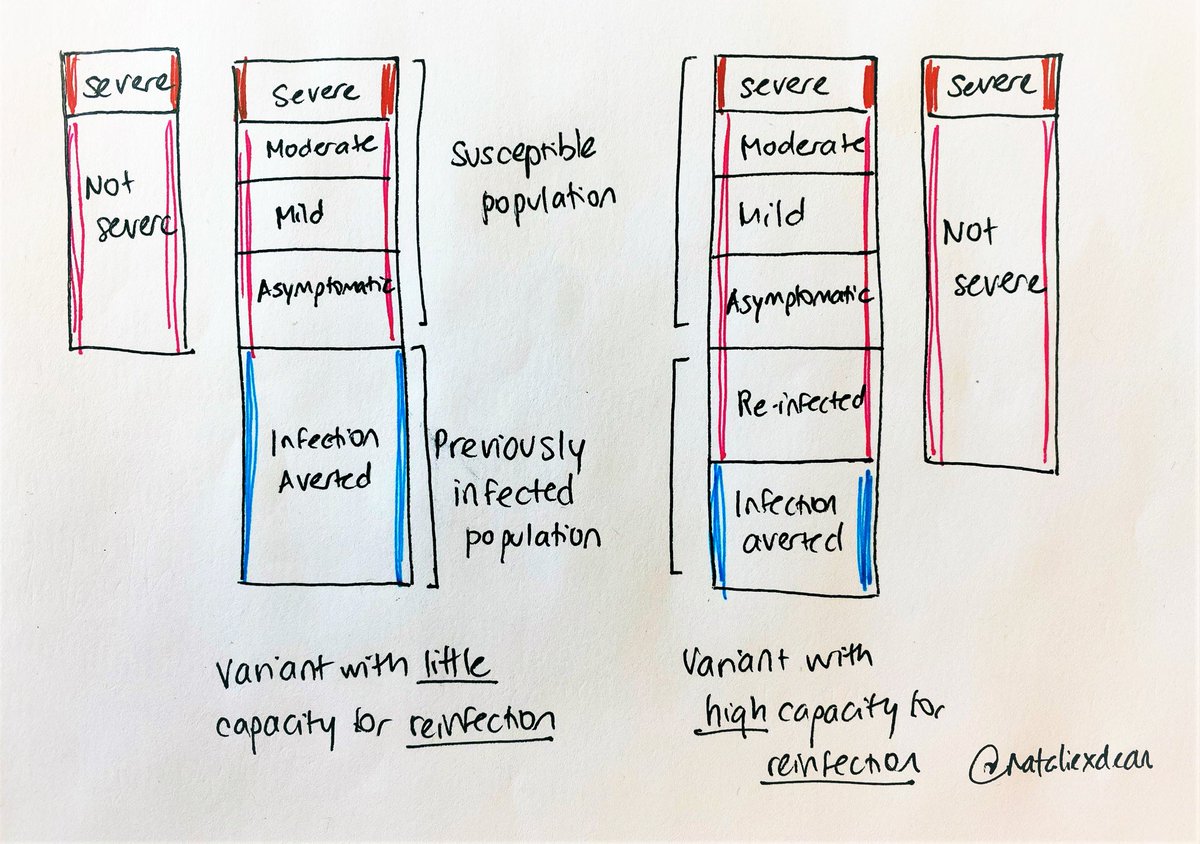
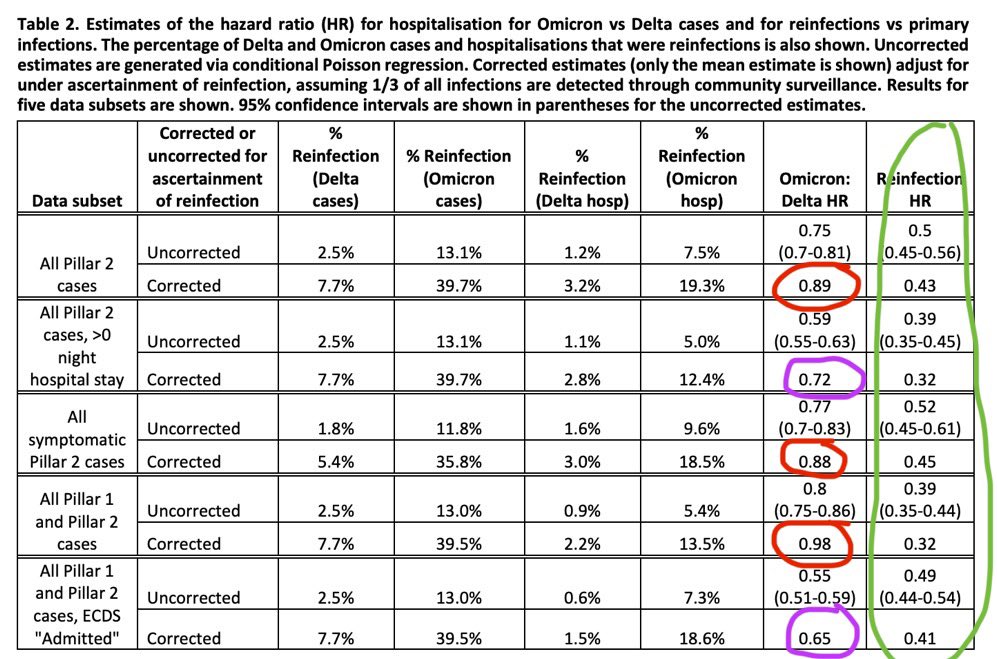













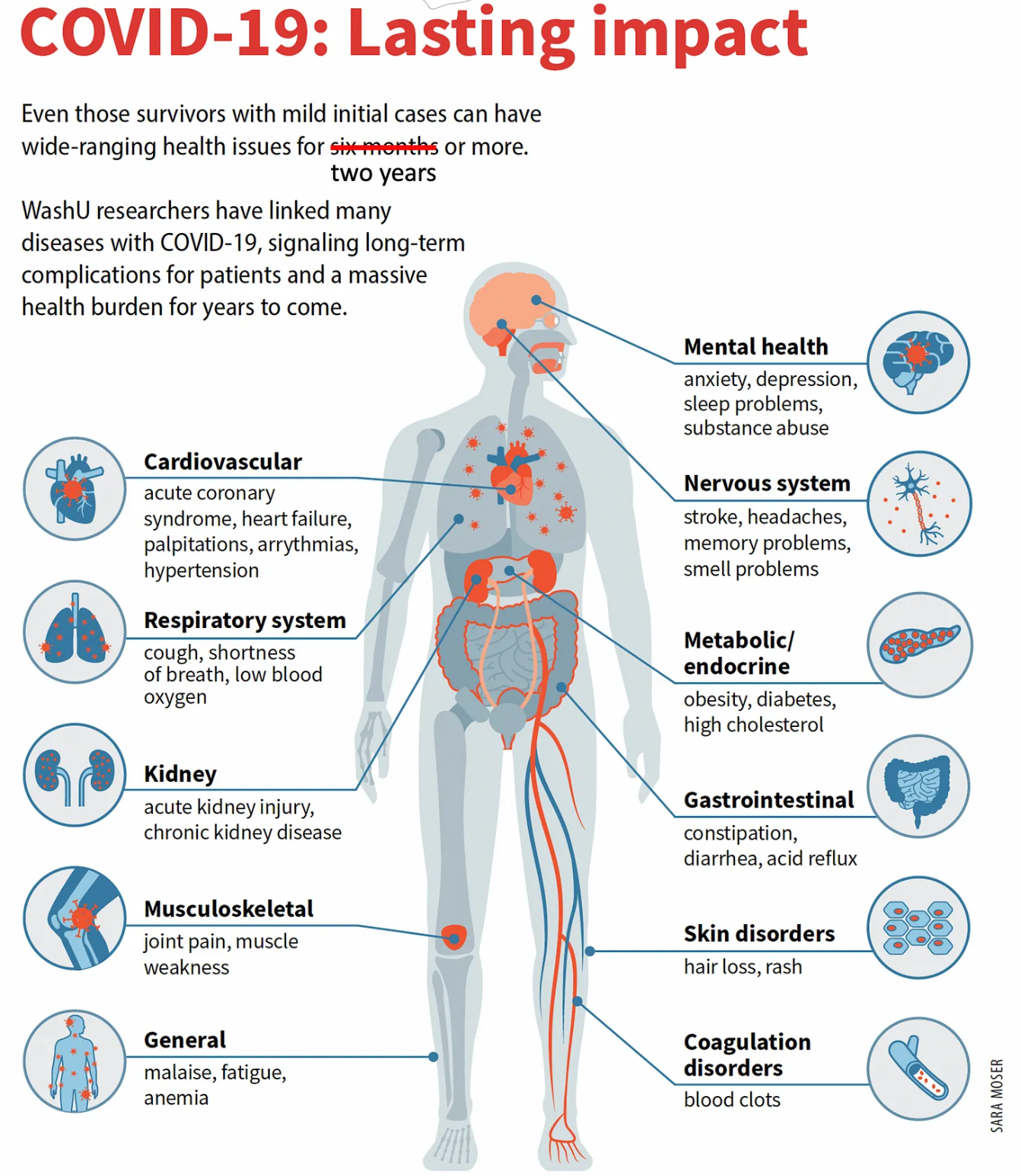


{kind=link}